Embed Size (px)
Citation preview

Hashimoto's Thyroiditis Presenting with Severe Pressure Symptoms --A Case Report--
Tsukasa TSUNODA, Nobuo MOCHINAGA, Toshifumi ETO, Masazumi TERADA and Ryoichi TSUCHIYA
ABSTRACT: A extremely rare case of Hashimoto's thyroiditis presenting with pressure symptoms is described herein. A 50 year old Japanese woman was referred to our department with swelling of the anterior neck, facial edema and recent heavy snoring. Oto-rhinolaryngological examinations revealed no movement of the bilateral vocal cords, severe laryngeal edema and diffuse edema of the tongue and pharynx. These findings had apparently been induced by compression of the bilateral recurrent nerves and internal jugular veins by an enlarged thyroid gland. The results of thyroid function and autoimmune tests were compatible with a diagnosis of Hashimoto's disease and thus, total thyroidectomy with a tracheostomy was performed uneventfully. The resected specimen weighed 168 grams and was confirmed histologically to be Hashimoto's disease. Following her opera- tion, all the above symptoms disappeared and 4 months later, the patient is well and asymptomatic.
KEY WORDS: Hashimoto's thyroiditis, pressure symptoms, recurrent nerve palsy, laryngeal edema
INTRODUCTION
H a s h i m o t o ' s disease, or lymphocytic thy- roiditis, has become common and the num- ber of cases may even be increasing since antithyroid antibody examinations are now widely used for it s diagnosis. 1,2 Usually, long- term suppressive therapy with the thyroid hormone is recommended for patients with symptomatic goiter or hypothyroidism with surgical intervention being justified only when the goiter shows pressure symptoms, cosmetic problems and /o r a suspicion of
The Second Department of Surgery, Nagasaki Uni- versity School of Medicine, Nagasaki, Japan
Reprint requests to: Tsukasa Tsunoda, MD, The Second Department of Surgery, Nagasaki University School of Medicine, 7-1, Sakamoto, Nagasaki 852, Japan
associated malignant lesions. 1-3 There are very few reports of a huge goiter of Hashi- moto's thyroiditis being treated surgically because of pressure symptoms.
In this paper, we report a case of Hashi- m0to's d i sease with pressure symptoms, namely, bilateral recur ren t nerve palsy, severe laryngeal edema and facial edema, which was treated successfully by a total thyroidectomy.
A CASE REPORT
A 50 year old Japanese woman was ad- mitted to the Second Department of Surgery, Nagasaki University Hospital on December 5, 1989, complaining of facial swelling, hoarse- ness and recent heavy snoring, and swelling of t h e anterior neck. The swelling of the anterior neck had first been pointed out by a
JAPANESE JOURNAL OF SURGERY, VOL. 21, No. 4 pp. 450-453, 1991

Volume 21 Number 4 Hashimoto's thyroiditis 451
ne ighbor 4 years prior to the admission, however, there were no other symptoms at this timel In September, 1989, her voice b e c a m e husky and by November , 1989, general fatigue, hoarseness, facial swelling and heavy snoring during sleep had de- veloped, which prompted her to visit a physi- cian, The physician referred her to Nagasaki University Hospital.
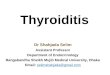
Fig. 1. Front view of the neck and face showing a huge goiter and facial edema. Note the edema around the eyes.
Physical examination revealed the patient to be in a good nutritional state and have a good appetite. Her height was 155 cm and weight 76 kg. There Was no edema of the trunk or extremities. A hard cartilage-like mass was palpable at the site o f the thyroid gland, the size o f which was 8.5 X 4.0 cm in the right lobe and 7.5 X 3.5 cm in the left lobe. No bruit was audible over the thyroid gland. Her face was edematous, especially around the eyes ~(Fig. 1) and her voice showed a severe husky change with heavy snoring that disturbed the sleep of other in- patients even on the opposite side of the ward. She had inspiratory and expiratory stridor but no dyspnea or a sense of choking.
T h e p reopera t ive l abo ra to ry data are shown in Tables l a and lb. Thyroid function tests revealed low levels of T 3 and T~, and a high level of TSH, indicating hypothyroid- ism. The thyroid autoantibodies, namely, antithyroglobulin antibodies and antimicro- somal, antibodies, were elevated and blood chemistry showed abnormally high levels of SGOT, LDH, CPK, aldolase, T I T , ZTT, total
Table la. Thyroid Function and Autoimmune Tests
T 3 : 24 ng/dl (80-180) free T3: 0.6 pg/ml (2.3-5.8) T~ : 0.5 ug/dl (6-13) free T,: 0.0 ng/dl (0.8-2.2) TSH : 68.4 uU/ml (0.3-3.2) T~ uptake: 22.8% (25-35) TBG : 22.5 ug/ml (15-28) TSH receptor antibody: (+) TGHA: 5120 ~ MCHA: 5120 ~
( ): normal value, TBG: thyroxine-binding globulin, TGHA: thyro- globuline hemagglutination antibodies, MCHA: microsomal hemag- glutination antibodies.
Table lb. Blood Chemistry
SGOT: 98 IU/1 (11-39) CPK: 1418 IU/1 (0-52) SGPT: 31 IU/1 (4-33) LDH: 1308 IU/1 (202-435) Ch-E; 0.59 ApH/H (0.6 1.3) Albumin: 11.0 IU/1 (2.0-7.0) Al-p: 123 IU/1 (88-270) T Chol: 256 mg/dl (111-247) LAP: 60 IU/1 (40-100) Total protein: 9.3 g/dl (6.2-8.0) y-GTP: 20 IU/1 (0-50) Albumin: 51.5%, al-globulin: 2.2% TIT: 20.9 Kunkel (0• a2-globulin: 5.0%, t-globulin: 6.9% ZTT: 29.9 Kunkel (4.0-12.0) y-globulin: 34.4%
Ch-E: cholinesterase, Al-p: alkaline phosphatase, LAP: leuicine amino- peptidase, y-GTP: y-glutamyltranspeptidase, CPK~ creatine phosphokinase, LDH: lactate dehydrogenase, T Chol: total cholesterol.

452 Tsunoda et al. Jpn. J.
Fig. 3. ACT scan of the neck demonstrat- ing the enlarged thyroid, deformity of the trachea and dilated right internal jugular vein.
Fig. 2. Lateral X-ray of the neck Showing the expanded retrotracheal space.
cholesterol and y-globulin, all be ing com- patible with a diagnosis of Hashimoto ' s dis- ease. An analysis of arterial b lood gases was done in room air, the result o f which was withifi normal limits.
A lateral X-ray of the neck showed that the retrotracheal space between the posterior wall o f the trachea and anterior rim of the cervical vertebrae had expanded to 2.8 cm (Fig. 2). A C T scan of the neck revealed the enlarged homogeneous thyroid mass to com- press the trachea, and that the right internal jugular vein was unusually dilated (Fig. 3). Ukrasonography revealed the bilateral inter- nal jugular veins to be c o m p r e s s e d by a goiter at the caudal level o f the neck and dilated at the cephalad part o f the neck. 6~Ga scintigraphy showed diffuse and scanty ac- cumulations in the area of the thyroid gland.
The oto-rhinolaryngological findings in- c luded severe l a ryngea l e d e m a , diffuse edema of the tongue and pharynx and no movement of the bilateral vocal cords.
Under the diagnosis of Hashimoto ' s dis- ease associated with c o m p r e s s i o n o f the
bilateral recurrent nerves and internal jugu- lar veins, a total thyroidectomy was carried out on December 18, 1989. The operat ion was more difficult than a typical total thy- roidectomy because of the enormous size and hardness of the goiter, and a tracheo- storey was also pe r fo rmed to prevent post- operative respiratory distress. The resected thyroid gland weighed 168 grams. The ad- ministration of thyroxine (100/2g/day) was started on the 5th postoperative day. A his- tological examinat ion of the resected speci- men confirmed the diagnosis o f Hashimoto 's disease, which was cons ide red to be in an advanced stage because the connective tis- sues were evenly distributed.
Oto-rhinolaryngological examinations on the 8th postoperative day revealed improved movement of the bilateral vocal cords and the absence of edema except for the ary- tenoid. The t racheostomy tube was removed on the 17th postoperative day and her voice returned to normal. Serum calcium levels were normal, and a marked improvement was seen in all the blood tests.
The patient was discharged on the 21st postoperative day and has been well since.

Volume 21 Number 4 Hashimoto's thyroiditis 453
Discussion
Hashimoto's thyroiditis is an autoimmune disease which may be associated with varying degrees of thyroid enlargement. It has occa- sionally been reported that the goiter of Hashimoto's disease causes mild pressure symptoms such as a sensation of fullness in the neck or o f chokifig ordysphagia, but in general, these symptoms can be alleviated successfully by medical treatment.
Our patient, however, developed symp- toms of pressure on the bilateral recurrent nerves and internal jugular veins: The facial and laryngeal edema in this patient was also regarded as a pressure symptom because there was no edema on the trunk or ex- tremities as is usually observed in myxedema. LucarottP reported 3 cases of vocal cord paralysis as a very uncommon symptom in Hashimoto's disease in which the right re- current nerve alone was paralyzed by pres- sure from a diffuse goiter. Shaw ~ reported a patient with venous compression, presenting with superior/vena cava obstruction while L i n d e m ~ r epo r t ed 41 surgically t rea ted Hashimoto's patients, among whom 21 had pressure symptoms involving e i ther the esophagus , t rachea, r ecu r ren t nerve or carotid artery. However, we were unable to find a case similar to ours in the literature and therefore consider it to be extremely rare.
What type of thyroidectomy should be employed to relieve the pressure symptoms of Hashimoto 's goiter? In a discussion of the report by Thomas, Letton recommended cutting of the isthmus and resection of the anterior portion o f the gland for' patients with mild pressure symptoms? His method may be appropriate for patients complaining of a pressure sensation without any evidence of compressio n to the adjacent structures after failure o f medical treatment. Lindem ~ recommended near total thyroidectomy by the "off the.trachea" technique, emphasizing that the remaining port ion of the goiter
could cause pressure symptoms again. He u s e d the "off the trachea" technique for complete removal of the goiter in the retro- tracheal area. This method may be effective for patients with marked compression to the esophagus, trachea a n d / o r internal jugular vein, however, near total thyroidectomy may fail to relieve the compression to the recur- rent nerve because the posterior part of the thyroid adjacent to the nerves is left com- pressed. Shaw ~ performed total thyroidec- tomy on a patient with venous compression symptoms without any complications. In our case, total thyroidectomy was employed be- cause a huge goiter occupied even the retro- tracheal space and compressed both the recurrent nerves and internal jugular veins. Near total tyroidectomy was not performed due to the possibility that recurrent nerve palsy would persist. Thus, total thyroidec- tomy seems the most reliable and efficient method when pressure symptoms are very severe. Moreover, it can be performed by a trained surgeon without damage to the re- current nerve or parathyroid glands. 7
(Received for publication on Apr. 20, 1990)
REFERENCES
1. Ingbar SH. Hashimoto's disease (Lymphocytic thy- roiditis, Struma lymphomatosa) In: Wilson JD, Foster DW, eds. Textbook of Endocrinology. W.B. Saunders Co. 1985; 806-808.
2. Volpe R. Autoimmune thyroiditis, In: Ingbar SH, Bravennan LE, eds. The Thyroid, Philadelphia: J.B. Lippincott Co. 1986; 1266-1286.
3. Thomas CGJr, Rutledge RG. Surgical intervention in chronic (Hashimoto's) thyroiditis. Ann Surg 1981; 193: 769-776.
4. Lucarotti ME, Holl-Allen RTJ. Recurrent laryngeal nerve palsy associated with thyroiditis. BrJ Surg 1988; 75: 1041-1042.
5. Shaw JFL, Tayler MJ. Superior vena cava obstruc- tion dueto Hashimoto's thyroiditis. BrJ Clin Pract 1983; 37: 73-74.
6. Lindem MC, Clark JH. Indication for surgery in thyroiditis. AmJ Surg 1969; 118: 829-831.
7. Attie JN, Khafif RA. Preservation of parathyroid glands during total thyroidectomy. AmJ Surg 1075; t30: 399-404.








![Riedel’s thyroiditis presenting as large retropharyngeal ... · in literature are multinodular goiters[2,8,9] with one large study failing to mention the pathology of the goiter.[3]](https://img.pdfslide.us/doc/110x75/5b6a1e7a7f8b9af6098bb781/riedels-thyroiditis-presenting-as-large-retropharyngeal-in-literature.jpg)