Embed Size (px)
Citation preview

Our Child has Seizures
2850
57 /
202
402
Our child has seizure
Supported by:
DESITIN ARZNEIMITTEL GMBHWeg beim Jäger 214 · 22335 HamburgTel.: +49 40 59101-0 · Fax +49 40 59101-400E-mail: [email protected] www.epinews.de · www.desitin.de
Edited by:Epilepsiezentrum Kork D-77694 Kehl-Kork
This booklet is mainly adress-ed to parents with a child ex-periencing epileptic seizures.The authors answer ques-tions regarding ”epilepsy” incommon language. This bro-chure cannot replace the per-sonal communication withyour child’s doctor. But, inaddition to this, it is meant tohelp you understand the oftencomplex medical back-gro-und and inform you aboutdiagnostic and therapeuticmanagement opportunitiesfor your child.
A guide for parents byProfessor Dr. Ansgar Matthesand Dr. Hansjörg Schneble
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 1

EPILEPSY IN CHILDREN
A guide for parentsbyProfessor Dr. Ansgar Matthes and Dr. Hansjörg Schneble
Edited by:Kork Epilepsy Centre (D-77694 Kehl-Kork, Germany)in cooperation with the German Section of the International League against Epilepsy
The printing of this brochure was made possible by the kind support of Desitin Arzneimittel GmbH, Hamburg, Germany
OUR CHILD HAS SEIZURES!
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 3

You are probably anxious and concerned because your child has just had an epi-leptic seizure for the first time or because he or she has been suffering fromrecurrent seizures for some time. Perhaps your child has so far experienced“only” minor seizures, or maybe you have been alarmed by a major seizure thatappeared to be life-threatening.
In this situation, many questions arise concerning the disease, its origin, the opti-ons for treatment and any possible effects on your child’s future.
No doubt you have already consulted your family doctor who will have given youthe most important preliminary information. Perhaps your child has already beenreferred to a specialist or admitted to hospital. However, experience has shownthat initial discussions with the family doctor or the specialist leave many questi-ons unanswered – maybe because there wasn’t enough time to deal with all thequestions in enough detail, or maybe because important questions did not occurto you until after your doctor’s appointment was over.
This is where this information booklet is designed to help you. It is the result ofdoctors‘ discussions with parents of epileptic children who had the same worriesand questions as you. Take your time to study this brochure, and if you still havequestions or problems, do not hesitate to consult your doctor.
One thing you will not find in this brochure is specific suggestions about how yourchild’s disease should be treated. Since each case is different, only your doctorcan decide which is the best path to take towards improving or curing your child’sdisease.
We hope that you will find this small brochure helpful. It is ment to encourage youand show you ways in which you can join your doctor in achieving the best foryour child.
Kork Epilepsy Centre, April 2004
Ansgar MatthesHansjörg Schneble
Dear Parents,
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 5

Epilepsy – what does it really mean? 4
How common is epilepsy in children? At what age does it begin? 5
What are epileptic seizures like? 6
What different types of epilepsy are there? 10
Is epilepsy a hereditary disease? 11
What are the causes of epilepsy? 12
Do external circumstances contribute to an individual seizure
being triggered? 13
Does epilepsy lead to mental deficiency or behavioural disorders? 14
How does the doctor diagnose epilepsy? 16
What is an EEG? 17
Are all convulsions in children a sign of epilepsy? 18
What should I do if a seizure occurs? 19
Does epilepsy have to be treated? 21
How is epilepsy treated today? 22
How can I help in treating my child’s epilepsy? 23
Are the drugs harmful? 25
Is it also possible to treat epilepsy surgically? 26
What are the chances of success of epilepsy treatment? 27
Are there ‘alternative‘ methods for the treatment of epilepsy? 28
Should a child go to kindergarten if it has epilepsy? 29
What is the right kind of school for epileptic children? 30
What are the job prospects for epileptic children? 31
Is an epileptic child allowed to play sports? 32
Is an epileptic child allowed to watch TV? 33
What do I do if my child needs vaccinations or an operation? 34
When should an epileptic child be cared for in a home? 35
Address index 36
Index 38
Table of Contents
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 7

4 5
The expression “epilepsy” is derivedfrom a Greek word (“epilambanein”)which basically means “to seize,attack”. In other words, “epilepsy”means “seizure”, or even better “con-vulsive disease”. However, since thereare different types of convulsive dis-ease, it is more accurate to refer to epi-lepsies.(You will encounter some of the differ-ent epilepsies in this brochure, althoughnot all of the ones known to date (first-ly, because it would go way beyondthe scope of this booklet to describeevery possible type, and secondly,because some of the known types ofepilepsy are extremely rare).
Anybody can suffer an epileptic sei-zure under certain circumstances, e.g.due to electric shock, oxygen deficien-cy or a severe head injury. However,one only refers to epilepsy if epilepticseizures occur without any recognis-able cause, i.e. in an otherwise ap-parently healthy person, and if theytend to recur. Among other things, thismeans that epilepsy is a chronic, i.e.longer-lasting disease (although itdoes not have to last a life-time by anymeans!).
Some people – including doctors! –are afraid of using the word “epilepsy”for this disease, because the term hasbecome stigmatised. In ancient times,
people believed in a supernatural ori-gin of the disease and that the suf-ferer was possessed by demons, evi-denced by the frightful outbreak ofgreat convulsions. This superstition is athing of the past. Nevertheless, manypeople think that epilepsy is a mentaldisorder or a disease that inevitablyleads to the loss of mental capacity, ora hereditary and incurable disease. Allthese stigmas that make life so difficultfor an epileptic child and its parentshave long been refuted by modernscience.
Epilepsy is a disease that starts in thebrain. It has nothing to do with mentaldisorders and only in exceptionalcases does it lead to a decline in intel-ligence. As in many other diseases,there are benign and malignant types.Epilepsy can be treated and, in verymany cases, completely cured.
It is a matter of individual choice whe-ther to use the term “seizures” or “con-vulsive disease” instead of the word“epilepsy”. The choice of words makesno difference to the reality of the di-sease. It is more important to look forthe right mode of treatment than for anagreeable name.
In Europe, with its population of approxi-mately 400 million people, around2,000,000 children suffer from epilep-sy. Epilepsy is thus more common inchildhood than the much better knownchronic diseases rheumatism, diabe-tes or tuberculsis.
Precise figures are not available forepilepsy, because of course it is not adisease that doctors have to notify tothe authorities. However, another rea-son is that many parents fear that thefamily will lose face if it comes out thattheir child has epilepsy, so instead oftaking their child to the doctor, theyplace their trust in people who advo-cate ‘alternative‘ (unproved) methods.
As we have already seen, the occur-rence of a single epileptic seizure doesnot necessarily signal the beginning ofepilepsy. The number of children whosuffer one or more seizures as babiesor infants without chronic epilepsydeveloping is many times greater thanthe number of children with epilepsystated above.
Epileptic seizures can start at any timeof life, even immediately after birthunder certain circumstances. In three-quarters of all epilepsy patients, thefirst epileptic seizures occur before theage of 20, especially in the first threeyears of life and around puberty.
The age at which the first seizuresoccur does not allow any reliable con-clusions to be drawn about the causeof the epilepsy, its further course or thechances of a cure.
Epilepsy - what does it really mean? How common is epilepsy in children?At what age does it begin?
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 9
6 7
There a many different types of epi-leptic seizures, and this booklet canonly deal with the most importantones.
“Major” and “minor” seizures.Until recently, epileptic seizures weremainly divided into “minor” and “major”ones. In medical jargon, especiallywhen the doctor is talking to patientsand relatives, these two terms are stillused today to describe the differentseizures, and you will frequently comeacross them in this booklet. However,it is important that you are clear that“major” seizures can be an expressionof an epilepsy with an overall mildcourse, while epilepsies with an un-favourable course may sometimesonly result in “minor” seizures.
“Major” seizures.Major seizures especially include thegrand mal seizure. In this type of sei-zure, the child suddenly falls uncon-scious to the ground, in most caseswithout warning, often letting out somekind of sound (scream, moaning); thechild rolls its eyes, the whole body goesstiff (tonic phase), and this culminatesin spasms in the arms, legs and face(clonic phase). Due to the course of thistype of seizure, doctors call it “tonic-clonic grand mal”. At the height of thisapparently threatening process, thechild salivates or may even foam at themouth, has difficulty breathing and thelips and hands turn a bluish-red.
In general, the major symptoms sub-side after 1 to 3 minutes. The child isthen exhausted and difficult to arousefor a prolonged period. The child oftenpasses urine or faeces during such aseizure. Bite injuries to the tongue andcheeks can occur at the beginning ofthe seizure, due to spasms of the jawmuscles (jaw seizure).
If such major seizures occur duringsleep, attention might be drawn to thisby the bed shaking or by gurglingsounds. The child feeling worn out orhaving a headache the next morning,large saliva stains on the pillow orabnormal bed-wetting may indicatethat a seizure occurred during thenight.
Grand mal seizures sometimes lastless than one minute. They occasion-ally only affect one side of the body(hemispasm). Consciousness may bemaintained or may be restricted to agreater or lesser degree. Despite thesemilder manifestations, such seizuresare also classified under the group of“major seizures”.
Some children are irritable, depressedor whiny hours or even days before amajor seizure. There are experiencedparents who can very reliably predictwhen their child is going to have a sei-zure on the basis of these signs. Inother children, a major seizure is some-times announced a few seconds inadvance by abdominal pain, nausea,dizziness, indeterminate aural or visu-al impressions or by a feeling of anxi-ety. Such brief “precursors”, which old-er children can often describe veryaccurately, are called an “aura”.
“Minor” seizures.The appearance of so-called minorseizures is far less dramatic than thatof a grand mal seizure. The mildestform of a minor epileptic seizure is abrief lapse in consciousness (absence).The child is “absent” and unrespon-sive for a few seconds, usually inter-rupting or slowing down in what it isdoing and staring fixedly or dreamilyat one point. Especially at the onset ofthe disease, such seizures often fail tobe recognised or are considered to bea bad habit or stupid behaviour.
In infancy, minor seizures mostly oc-cur in the form of an abrupt spasmwhich may be repeated several times(lightning convulsions). Sometimes,the infants bend in two for 1 to 3 sec-onds at a time, rather like an orientalgreeting (salaam convulsions). This
type of seizure is sometimes misinter-preted as nervousness or colic-like sto-machache.
Mainly among small children, smallepileptic seizures are evidenced by atic-like blinking of the eyes (winkingspasms) or a pronounced noddingmotion (nodding spasms). If these sei-zures are more pronounced, the childoften falls abruptly backwards or for-wards (drop attack ), often sufferinginjury.
The term minor seizure is also usedeven if the seizure (spasms, stiffness,sensory disorder – e.g. experiencedas a tingling sensation, numbness orstrange sensation) only affects onepart of the body (e.g. arm, leg or oneside of the face). In such cases, thechild‘s consciousness is not impaired.
Another type of minor seizure is simi-lar to a “behavioural abnormality”(psychomotor or complex partial sei-zure): The children may make unpro-voked swallowing or licking move-ments, fiddle with their hands, talknonsense or run around aimlessly.Such psychomotor seizures may last30 seconds, one or even two minutes.
What are epileptic seizures like?
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 11

8 9
Minor seizures often tend to occur at aparticular stage in life – which is whythey are referred to as age-related orage-dependent (minor) seizures:lightning and salaam convulsions areobserved almost exclusively in babies,winking spasms and drop attacksmainly in small children and absenceseizures predominantly in schoolchil-dren. The other minor seizures – andthe majority of major seizures – occurat all times of life, which is why theyare often referred to as age-independ-ent seizures.
“Generalised” and “partial” seizures.In today’s medical terminology, wetend to talk about “generalised” and“partial” seizures instead of “major”and “minor” seizures.
A generalised seizure is one whichaffects both sides of the body equallyfrom the outset or – viewed from thepoint of origin – in which both halvesof the brain are simultaneously besetby the seizure activity.
The whole body does not necessarilyhave to be affected by the seizure – theimportant thing is that both sides areaffected from the outset. Of the exam-ples of seizures mentioned so far, thefollowing can be called “generalised”seizures: grand mal and absence sei-zures, lightning and salaam convulsi-ons, winking and nodding spasms,and drop attacks.In contrast to this, we refer to partial orfocal seizures if, at the beginning of theseizure, only one side of the body oronly a limited part of the body on oneside is affected by the seizure. (Thisnaturally also means that only a limi-ted part of one side of the brain isinvolved in the seizure activity.)According to this definition, the follow-ing are partial seizures: hemispasm;grand mal seizures preceded by anaura; spasms, stiffness or sensory dis-turbances affecting one side only; psy-chomotor seizures (complex partialseizures).
Moreover, the classification of epilep-tic seizures into generalised and partialseizures is not affected by the fact thatan initially partial seizure can developinto a generalised one over the courseof the seizure. For example: The sei-zure begins with spasms in one hand(partial seizure!) which then rapidlyspread throughout the whole body(generalised seizure!). The beginningof the seizure activity alone is impor-tant for classifying the seizure as “gen-eralised” or “partial”. However, it issometimes only possible to decidewhether a seizure is partial or gener-alised to begin with by means of anelectroencephalogram (EEG) whichmeasures the electrical activity in thebrain (see the chapter “What is anEEG?” later on in this brochure).
Status epilepticus.All epileptic seizures can recur at shortintervals (minutes to hours) under par-ticular circumstances; if the patientrecovers consciousness between theindividual seizures, we refer to a seriesof seizures. If a single seizure lasts morethan 15 minutes or if the patient doesnot recover consciousness betweenseveral seizures, we refer to status epi-lepticus (“epileptic state”).
In the case of major seizures (grandmal seizures), such a state is alwayslife-threatening and can only be alle-viated in the hospital.Although a state of minor seizures isless dangerous, it is often misinter-preted. For example, if one absenceseizure follows another, the child ap-pears sluggish and tired. It hardly spe-aks at all and its movements are likethose of a puppet. If they are not trea-ted, such states of minor seizures canlast for hours, days or even weeks.
Generalised seizurePartial seizure
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 13

10 11
At the beginning of this brochure, wementioned that there are differenttypes of epilepsy and that it is there-fore more accurate to talk about epi-lepsies rather than about epilepsy as asingle disease.
You now know about the modern (in-ternational) classification of the diffe-rent types of seizures – namely the clas-sification into generalised and partialseizures. The modern classification ofepilepsies follows the same lines:There are generalised and partial epi-lepsies. We talk about generalised epi-lepsy when this epilepsy involves(“major” or “minor”) generalised sei-zures; epilepsy characterised by par-tial seizures is called partial epilepsy.
Epilepsy with grand mal seizures is ageneralised epilepsy (generalisedgrand mal epilepsy), as is an epilepsywith frequent absence seizures (themedical term for which is “pyknolep-sy”; it is the most common type of gen-eralised epilepsy in childhood).
Epilepsy with hemilateral or psycho-motor (complex partial) seizures orwith major seizures that are heraldedby an aura (see p. 7) is classified aspartial epilepsy. The most common par-tial epilepsy in childhood is calledjacksonian or rolandic epilepsy whichcan occur between the age of 3 and 12and is characterised by seizures thatmostly occur during sleep:
The children are often woken by astrange sensation around their mouthor on one side of their face, there maybe spasms in one corner of the mouthor in one cheek, usually accompaniedby pronounced salivation. The child-ren are unable to speak, but oftendraw their parents‘ attention to theproblem by making gestures or un-intelligible sounds; they generally re-main conscious during such seizures.
The most important and characteristicsymptom of any particular type of epi-lepsy is the individual epileptic sei-zure. For the doctor to make an exactdiagnosis and decide on the right tre-atment, it is very important that youobserve your child’s seizures carefullyso that you can describe them as pre-cisely as possible to your doctor lateron.
Not only the seizures themselves, butalso the origin, course and prognosis(the expected outcome of the disease)can be very different in the individualtypes of epilepsy.
Speaking in very general terms, thereare two basic conditions that lead tomost diseases developing: An (inner)predisposition and an (external or ac-quired) trigger: There are diseases inwhich predisposition plays a partic-ularly important role (e.g. diabetes orgout), and others in which external(acquired) conditions are the mainreason for the disease being triggered(e.g. lung cancer).
The extent of the predisposition to-wards a particular disease is connec-ted with heredity (the genes) and ispassed on from parents to their chil-dren: We therefore talk about a gen-etic or familial predisposition. For ex-ample, some families have a greaterpredisposition towards diabetes thanothers; nevertheless, diabetes is not ahereditary disease. We only talk about a hereditary dis-ease when the disease itself (not onlya predisposition towards this disease!)is transmitted according to specific lawsof heredity.
Epilepsy is not a hereditary disease,i.e. the disease epilepsy is not passeddown from the father or mother to theirchild. However, the extent of the pre-disposition towards epilepsy can varyfrom family to family.This explains why several members ofone family may suffer from epilepticseizures or develop chronic (persist-ent) epilepsy – although the predispo-
sition always has to be accompaniedby an additional triggering factor.
Certainly, there are epilepsies in whichgenetic predisposition plays the crucialrole in the development of the disease(and not the external triggering fac-tors); we refer to such epilepsies as“primarily genetically-related epilep-sies” (the medical term for this is “idio-pathic epilepsies”). Examples of this inchildhood are epilepsy with frequentabsence seizures (pyknolepsy) and jack-sonian or rolandic epilepsy (see p. 10).
However, in the development of mostepilepsies, the external (acquired) fac-tors play a much more important rolethan the genetic predisposition; suchtypes of epilepsy are called “symp-tomatic epilepsies” (see the next chap-ter in this brochure).
The widespread misconception thatepilepsy is a hereditary disease hasbrought great unhappiness to many afamily. So don‘t reproach yourself anddon‘t torture yourself with the questionof whether or not you might be “to bla-me” for your child‘s disease, but con-centrate your efforts on finding theright treatment.
Is epilepsy a hereditary disease?What different types of epilepsy are there?
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 15

12 13
Epilepsy is caused by a malfunction ofnerve cells in the brain. Electrical dis-charges occur, similar to what happenswhen you have a short-circuit. The epi-leptic seizure results from a rapid se-quence of such discharges in the nervecells of the brain. In the previous chap-ter, we discussed the fact that both a(genetic) predisposition and an (ex-ternal or acquired) trigger are requiredfor epilepsy to develop. As alreadymentioned, if the acquired triggersplay the decisive role in the epilepsydeveloping, we call such an epilepsy“symptomatic”.
There are many different external trig-gers or causes for the abnormal be-haviour of the nerve cells, i.e. for thedevelopment of symptomatic epilep-sy. The most common ones in chil-dren are:• Impaired development of the brain
during pregnancy – for instance dueto chromosomal disorders, anoma-lies, alcohol abuse, poisoning, infec-tions (e.g. German measles in earlypregnancy!), heavy bleeding (lea-ding to oxygen or nutrient deficiencyin the foetus).
• Brain haemorrhage, contusion of thebrain or oxygen deficiency during birth(damage to and/or loss of nervecells).
• Encephalitis or meningitis (which mayalso occur during apparently harm-less childhood illnesses like measles,mumps, whooping cough or chicken-pox).
• Brain injuries caused by accidents(bleeding into the brain, contusion ofthe brain).
• Progressive brain diseases, like braintumours, premature decay of the greymatter or metabolic disorders.
Months or even years can pass bet-ween the occurrence of these causa-tive diseases and the onset of epilepsy.
Your doctors will do their very best tofind out which of these causes is res-ponsible for your child‘s epileptic sei-zures in order to provide important in-formation on the right treatment andthe chances of a cure. Despite the useof the very latest test methods, the ori-gin of the seizures cannot be found insome children. But even in such cases,treatment is necessary and a comple-te cure is often still possible.
No doubt you have already thoughtabout the external circumstances thatmay cause individual seizures in yourchild, or at least make them more likely.
Experience has shown that, in almostall cases, the onset of seizures is un-foreseeable, occurring out of the blue.Poor diet is often blamed for causingseizures, but this does not play anyrole whatsoever.
However, infections accompanied byfever, a change in the weather andphysical or mental stress, especiallylack of sleep, can trigger seizures ormake them more likely in some children.
Alcohol is like poison for a child‘s ner-ves. It goes without saying that allforms of alcohol are prohibited forchildren and adolescents who sufferfrom seizures.
In some particularly predisposed chil-dren, certain everyday sensory stimulican cause epileptic seizures; this es-pecially includes optical stimuli (light-dark contrasts, flickering light) and,much more rarely, even startling sounds,unexpected contact or being given astart. Such “stimulus-induced” sei-zures are called “reflex-induced” sei-zures (in this connection, also see thechapter “Is an epileptic child allowed towatch TV?”!). However, we only talkabout “epilepsy” in such children if, inaddition to the triggered seizures, theyexperience seizures without any rec-ognisable stimulus.
What are the causes of epilepsy? Do external circumstances contribute to an individual seizure being triggered?
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 17

14 15
Epilepsy has nothing to do with men-tal disease.
Most children who suffer from epi-lep-sy are mentally healthy – as regardsboth their intelligence and their be-haviour.
Nevertheless, there are more mentallyabnormal children among epilepticchildren than among children withoutepilepsy of the same age-group. Whatis the reason for this?
We already know that epilepsy is oftenthe result of organic brain damage(“symptomatic epilepsy” - e.g. due todamage caused at birth, encephalitisor brain injuries; see page 12). If severebrain damage occurs, it is clear that thedevelopment of intelligence may alsobe delayed or remain retarded. In thiscase, epilepsy and reduced intellectualability are two symptoms of the sameorigin – in other words, the severe braindamage. (This reduced intelligence isnot a result of the epilepsy, but of thebrain damage which also causes theepilepsy!). However, brain damagedoes not always lead to a reduction inoverall intelligence, but leads to weak-ness in certain areas of performance:e.g. in reading, writing or arithmetic orin spatial orientation; or the child simp-ly has difficulty keeping up with otherchildren of the same age.
In such cases, the doctor refers to parti-al deficiencies in performance.
The same may also apply to abnor-mal behaviour : Severe brain damage(with or without epilepsy) can alsocause abnormal behaviour (with nor-mal or reduced intelligence). Exam-ples of such abnormal behaviour areforgetfulness, poor concentration, poorattention span, being easily distracted;some children are also very agitated,“nervous” or overaggressive; on theother hand, others are slow, awkwardor ponderous. However, none of thesepossible symptoms are caused by epi-lepsy, but are the result of precisely thesame brain damage which is at theroot of the seizures.
Some abnormal behaviour is not basedon disease-related malfunctions in thenerve centres of the brain, but onexternal influences: If parents and tea-chers do not recognise or take intoaccount the fact that the child‘s per-formance is impaired by a disease, thechild becomes overstrained. Suchchildren often react to this by clown-ing around at school and showingdefiance, aggression and refusal to dowhat they‘re told at home.
Does epilepsy lead to mental deficiency orbehavioural disorders?
Overanxious and overprotective par-ents prohibit their ill children fromdoing too much and dare not placeany demands on them. This leads tochildish behaviour even in older chil-dren.
Abnormal behaviour caused by func-tional impairment of the nervous sys-tem is often combined with that causedby the external influences mentionedabove. This can make it difficult toseparate one cause from the other.
In rare cases, epileptic seizures canalso lead to a loss of mental abilities -e.g. if grand mal seizures occur in rapidsuccession (series) or as an epilepticstate (see page 9).
Occasionally, adverse reactions ofdrugs that have to be taken to treat theepilepsy can also lead to changes inbehaviour (see page 25).
The person to turn to whenever youhave any such problems is the doctortreating your child. If necessary, hemay refer you to an experienced psy-chologist who can provide you with theright counselling.
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 19

16 17
The first thing the doctor needs is pre-cise information about the onset, thefrequency and the appearance of theseizures. He also needs details aboutthe course of pregnancy, birth, deve-lopment and any previous diseasesthe child has had. Information aboutany epileptic seizures or seizure-likeconditions in other family members isalso extremely important for the doc-tor to determine the type and origin ofthe seizures.
Normally, the child is then given athorough examination, particularly ofthe nervous system. An EEG examina-tion is also carried out (see page 17).These measures are often sufficient todetermine whether or not epilepsy isinvolved. Sometimes, the cause of theepilepsy can only be determined bymeans of special test methods forwhich the child may (but certainly notalways) have to be admitted to thehospital (e.g. metabolic tests of theblood and urine, computerised tomo-graphy or magnetic resonance imag-ing which produce pictures of thebrain, tests of the spinal fluid).
Under normal circumstances, thesespecial tests are hardly any bother atall for the child. The need for such testmethods, which parents often incor-rectly assume to be unpleasant, verypainful or even dangerous, is solely forthe doctor to decide.
How does the doctor diagnose epilepsy? What is an EEG?
Each nerve cell is a highly complexstructure on the surface of which elec-trical (and chemical) processes takeplace. EEG is the abbreviation for “elec-troencephalogram”, by means ofwhich it is possible to amplify and re-cord the sum of the electrical proces-ses that take place in the many billionsof cells in the cortex of the brain. Inother words, it is a kind of brain-wavecurve.
Like the better known EKG or electro-cardiogram (which is used to recordthe electrical processes in the heart),the EEG is an absolutely harmless andpainless test method that can be re-peated as often as you like. It involvesattaching electrodes (metal discs) tothe child’s scalp using rubber bands. (Itis not necessary to remove the hair atthese measuring points!).
The electrodes receive the normal andabnormal electrical currents from thebrain which are then amplified by theEEG device. These brain waves areregistered in the form of a compli-cated curve, called an electroence-phalogram. Normally, this recordinglasts 20 to 30 minutes. It is sometimespossible to identify the desired infor-mation during sleep only. This is calleda sleep EEG (which is easiest to per-form after depriving the child of sleep).
Today, the EEG is the most importanttechnical method for diagnosing epi-lepsy. In most cases, it can also beused to locate the point in the brainfrom which the epilepsy originates.Finally, the EEG shows whether andhow rapidly the abnormal stimulationof the nerve cells diminishes duringtreatment. The EEG says nothing aboutintelligence or character.
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 21

18 19
Some children have seizures that arenot signs of epilepsy, although theseseizures really are epileptic seizures.However, these seizures occur exclu-sively in certain situations, namely incertain short-term health disorders. Since such seizures are associatedwith very specific situations and neveroccur spontaneously ( i.e. never occurother than in such situations ), they arecalled occasional seizures or occasio-nal convulsions.
Convulsions sometimes occur in olderbabies or infants, e.g. in particularlypredisposed children at the beginningof infectious diseases accompanied bya high fever (called febrile convul-sions). They may recur in later febrileinfections and cease spontaneously ataround the age of 6.
However, such an attack with fever isnot necessarily a harmless event; inrare cases, convulsions accompaniedby fever can also be a sign of the be-ginning of encephalitis or anotherserious disease. Therefore, alwaysapply the rule: Whenever the first epi-leptic seizure occurs – with or with-outfever – call the doctor.
Other “occasions” on which “occasio-nal seizures” can occur (even withoutfever) are, for instance, lack of essen-tial minerals (e.g. calcium or sodium),low blood-sugar levels (especially indiabetic children), poisoning, contactwith electric current (“electric shock”),overheating (“heat stroke”).
Ill-informed people often dismiss suchconvulsions as “teething troubles”,“growing pains”, “infant spasms” or“goutiness”. This attitude can lead tothe right moment for curing the dis-ease being missed and epilepsy de-veloping later on.
Contrary to a widely held belief, teeth-ing in children is never the cause ofconvulsions.
The reasons for convulsions occurringin each individual case can only bedetermined by the doctor or hospital.
Normally, a major seizure (grand mal)stops on its own after 1 to 3 minutes;despite its dangerous appearance, it isnot life-threatening. For this reason, inthe vast majority of cases, medicalmeasures do not have to be takenduring a major seizure. However, if amajor seizure lasts longer than usual(i.e. longer than 3 to 5 minutes), spe-cial measures must be taken to inter-rupt this seizure activity (see below).
First of all: Which measures are gener-ally recommended in the case of amajor seizure?• If there are warning signs (“aura”– see
page 7) just before the seizure, placethe child flat on the bed or floor andloosen its clothing, especially a-round the neck.
• Move the patient away from any pos-sible danger zones (e.g. traffic,water, sharp objects and edges).
• Calmly wait for the seizure to pass andwatch the child attentively. Carefuldetails about the appearance andduration of the seizure are of greatimportance for the doctor later on(see page 10).
• If the child salivates profusely, turn itshead to one side to prevent chok-ing. Vomiting sometimes occurs dur-ing or immediately after the seizure;in such cases, instead of just turningthe head, it is best to place the childin a stable position on its side (if thiscan be done without difficulty – donot use force!).
• After the seizure, the child is usuallysluggish and does not respond oronly responds with difficulty, or it fallsinto a deep sleep. Do not disturb thechild at all, giving the exhausted ner-ve cells in the brain a chance to reco-ver. The seizure is sometimes follo-wed by a state of restlessness. Onceagain, wait patiently for this to passand do not use force to restrain thechild, but accompany it calmly.
• Your doctor may have prescribed youan anticonvulsant which can beintroduced into the child‘s intestinesthrough the rectum without profes-sional help (e.g. diazepam supposi-tories). In general, this step is recom-mended if a major seizure has notstopped after 2 minutes or if it hasnot clearly subsided after 2 minutes.(In rare cases, two or more supposi-tories have to be used – althoughthis must be discussed with yourdoctor beforehand!)
Are all convulsions in children a sign ofepilepsy?
What should I do if a seizure occurs?
Unser_Kind_03/04_engl 30.03.2005 10:48 Uhr Seite 23

20 21
What you should not do during a sei-zure?• Do not use force to release the spasms
that occur in the arms and legs duringa seizure;
• Do not hold down the convulsing limbsby force;
• Do not use force or hard objects to pryopen the clenched jaws (even if thechild has bitten its tongue, leading tobleeding);
• Do not pour water on the child duringthe seizure or try to resuscitate thechild;
• Do not try to wake the child after theseizure by shaking, hitting, smellingsalts or other resuscitation measures.
Children who experience minor sei-zures (e.g. absence seizures, psycho-motor seizures - see page 7) need tobe accompanied calmly and protec-tively and to be observed carefully;interruption of the seizure activity (e.g.by administering a suppository) is notgenerally necessary, even if the sei-zure lasts for several minutes.A doctor only has to be called if the sei-zure lasts for a prolonged period.Here, too, it is better to observe care-fully than to take unthinking action.
Although epilepsy can occasionally becured without treatment, treatment isgenerally necessary. The notion thatthe problem disappears anyway duringpuberty or after getting married usuallyturns out to be mistaken. Seizures mustbe treated for the following reasons:1. The abnormal reaction of the seizure
becomes increasingly “ingrained” inthe brain and each seizure pavesthe way for the next one (“facilitati-on”). A cure can only be achieved ifthis vicious circle is broken. This iswhy it is important that early diagno-sis is followed by early treatment.The later the right treatment is given,the poorer the chances of a cure.
2.So-called minor seizures are oftenjoined by major seizures at a laterstage-sometime no until manymonths or even years after the onsetof the epilepsy. This is why it is alsoimportant to treat minor seizures.
3. Since most seizures occur withoutwarning, epileptic children are indan-ger of having accidents duringsei-zures that are accompanied byloss of consciousness, a twilight sta-te, disturbances of balance or falling– e.g. when climbing trees, in traffic,when riding a bike, on stairs, in thebathtub or when swimming. Fromthis point of view, even a briefabsence seizure lasting just a fewseconds can represent a major dan-ger for the child.
In general, the epileptic seizures them-selves – regardless of whether they areminor or major – do not lead to anydamage to brain cells. Only in the caseof a large number of convulsions (grandmal seizures), especially if they occurin the form of an epileptic state, mightbrain cells be destroyed as a result ofoxygen deficiency and other disorders(see page 15). However, the right treat-ment will considerably reduce preciselythis risk of longer lasting seizures (sta-tus epilepticus)!
Does epilepsy have to be treated?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 25

22 23
The most important form of treatmentis to administer drugs that reduce theabnormal stimulability of the nervecells and make it possible for the brainto function normally. Only your doctorcan decide which drugs and whichdose will have the best effect on yourchild.
There is no such thing as a “guaran-teed medicine” that will alleviate sei-zures in all patients. The drug that helpsthe neighbour’s child might just beprecisely the wrong one for your ownchild.
It sometimes takes many weeks oreven months for the doctor to find theright “adjustment” to the medication.The parents have to place their trust inthe doctor’s ability and experience andthey sometimes have to be very pati-ent. However, frequently changingdoctors can be disastrous when treat-ing epilepsy. Your doctor will certainlyconsult a specialist if he is uncertain orhas not the right experience. Treat-ment in outpatient departments canbe unsatisfactory if the size of the de-partment leads to a frequent changein hospital doctors.
In most cases, the medication has tobe taken for several years every dayon a regular basis – even if treatmenthas prevented further seizures fromoccurring. Suddenly stopping takingthe tablets can lead to life-threateningconvulsions and prevent a cure. Onlythe doctor can decide when it is safe togradually stop taking the tablets.
The best help that parents can givetheir epileptic children to begin with isto accept their child with its epilepsy.However, this does not signify resig-nation – but rather the call to join thedoctor in the search for the best pos-sible treatment for the ill child.
As parents, you must pay special atten-tion to the following points during thetreatment phase:• Make sure your child takes the drugs
regularly as prescribed – a little edu-cational pressure may have to beapplied from time to time; childrensometimes refuse to take their medi-cation, particularly at the beginningof treatment. If this happens, it maybe helpful to change from tablets tosugar-coated tablets or syrup (con-taining the same active substance,of course). A pill box (with daily orweekly dose compartments) is oftena great help.
• Keep careful records, i.e. fill out a seizu-re calendar or seizure diary. Youshould keep an exact record of thefrequency, duration, time of day andappearance of the seizures, if possi-ble including the situations that mighthave contributed to the seizure occur-ring (e.g. fever, lack of sleep, month-ly period in girls). You should bringthese records with you when you goto see your doctor.
• Keep your doctor ’s appointments.It is absolutely necessary that yourdoctor sees and examines your childat regular intervals – depending onthe type of epilepsy and the courseof the disease – and gives you detai-led advice.
• Avoid situations that contribute to sei-zures. Beside drug treatment, ahealthy and sensible lifestyle alsohelps to cure epilepsy. Physical andmental overexertion must be avoi-ded, as must disturbances in thesleeping and waking cycle. Lack ofsleep particularly contributes to sei-zures in predisposed children. Youshould therefore make sure that yourepileptic child gets sufficient sleep;experience has shown that the pro-blem of insufficient sleep increasesin adolescence – but precisely aro-und the time of puberty, sufficientsleep is especially important for peo-ple at risk of having seizures.
How is epilepsy treated today? How can I help in treating my child’s epilepsy?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 27

Your epileptic child’s diet should not beany different from a normal diet withplenty of vitamins and minerals. Nonutritional substances are known totrigger seizures or promote a tendencyto seizures; conversely, dietary regi-mens cannot prevent the occurrenceof epileptic seizures.
One exception to this is the so-calledketogenic diet which has a beneficialeffect on seizures in children in veryrare cases; it mainly consists of fat andprotein and produces a seizure-inhi-biting over-acidification of the blood.However, since this diet by no meansalways helps and often loses its effectafter initial improvement, and since it isoften poorly tolerated and rejected bythe children after prolonged intake, itcan only be used in exceptional cases.
Alcohol can contribute to the occur-rence of epileptic seizures (see page 13).Certain types of epilepsy are “alcohol-sensitive”, especially in older school-children and in puberty. Alcohol shouldtherefore be completely avoided byolder children and adolescents whosuffer from epilepsy.
24 25
In principle, all drugs can have adver-se reactions, i.e. side effects, in addi-tion to their desired action. At the dosesprescribed by the doctor, most drugsagainst epileptic seizures have no oronly mild side effects that are not da-maging in the long-term. Your doctorwill try to “adjust” your child‘s epilepsywith medication in such a way that thedrug has only the desired effects, andcauses no or only insignificant sideeffects. In exceptional cases, more seri-ous side effects can also occur fromtaking anti-epileptic drugs. Before star-ting the treatment, your doctor will talkto you in detail about such possi-bleside effects and their earliest possibledetection. Thankfully, most epilepticchildren tolerate their medication with-out any problem.
In order to recognise rare side effectsas quickly as possible, your child mustbe kept under regular medical supervi-sion for the entire duration of treat-ment. The control examinations willnaturally be more frequent at the be-ginning of treatment than after the so-called adjustment phase. At regularintervals, your doctor will perform drugtolerability tests in which he will exam-ine the blood count and liver func-tions, and also the urine in rarer cases.He will also measure the blood levels(plasma concentration) of the drugs todetermine whether the dose is suffi-cient, too low or too high, and whetherthe drugs have been taken regularly.
As is true of most drugs, the agentsused to treat epileptic seizures canoccasionally cause hypersensitivity re-actions (allergies), e.g. in the form ofskin rashes, swollen glands and fever.
Overdosage can occur if too muchmedication is given and is evidencedby symptoms like drowsiness, mood-iness, shivering, visual impairment oruncertain gait. Usually, such symptomscan be rapidly eliminated by loweringthe dose.
You should immediately tell your doc-tor about any abnormal symptomsthat you observe in your child so thathe can change the treatment if this isrequired.Under no circumstances may you in-crease or reduce the daily amount ofthe prescribed medication on yourown initiative!
Are the drugs harmful?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 29
26 27
In the vast majority of cases, epilep-sies are treated with drugs. However,in rare cases, surgical treatment ofepilepsy may also be possible andadvisable (surgical epilepsy therapy,epilepsy surgery). In principle, suchepilepsy surgery only comes into que-stion under the following circum-stances:• Partial epilepsy is present (see page 10).• Thorough examinations must be per-
formed and repeated several timesto confirm that all of the patient‘s sei-zures always start in the same partof the brain. (The epilepsy may nothave “several focal points”.)
• Treatment with drugs failed to producethe desired result.
• The seizures lead to a pronounced deterioration in the patient‘s qualityof life – or, put another way: Eliminati-on of the seizures would lead to adecisive improvement in the pati-ent‘s quality of life.
• The risk of a “defect” as a result of thesurgery must be minimal.
• The child (if possible) and the parentsdefinitely want the operation to beperformed.
It goes without saying that epilepsysurgery should only be considered andperformed after very careful exami-nations. These examinations (espe-cially complicated EEG recordings,imaging procedures) must be perfor-med at specialised centres.
These “preoperative diagnostics” (ex-aminations before the operation) areoften more complicated and stressfulthan the operation itself. On the otherhand, precisely in desperate cases,epilepsy surgery can often achieveextraordinarily good results. There isno lower age limit for epilepsy surgery– even babies can be given an opera-tion for epilepsy; in fact, the youngerthe patient, the better seems to be theoutcome of surgery. However, onlyabout 2 to 4% of all epilepsy patientscan currently be considered as candi-dates for epilepsy surgery.
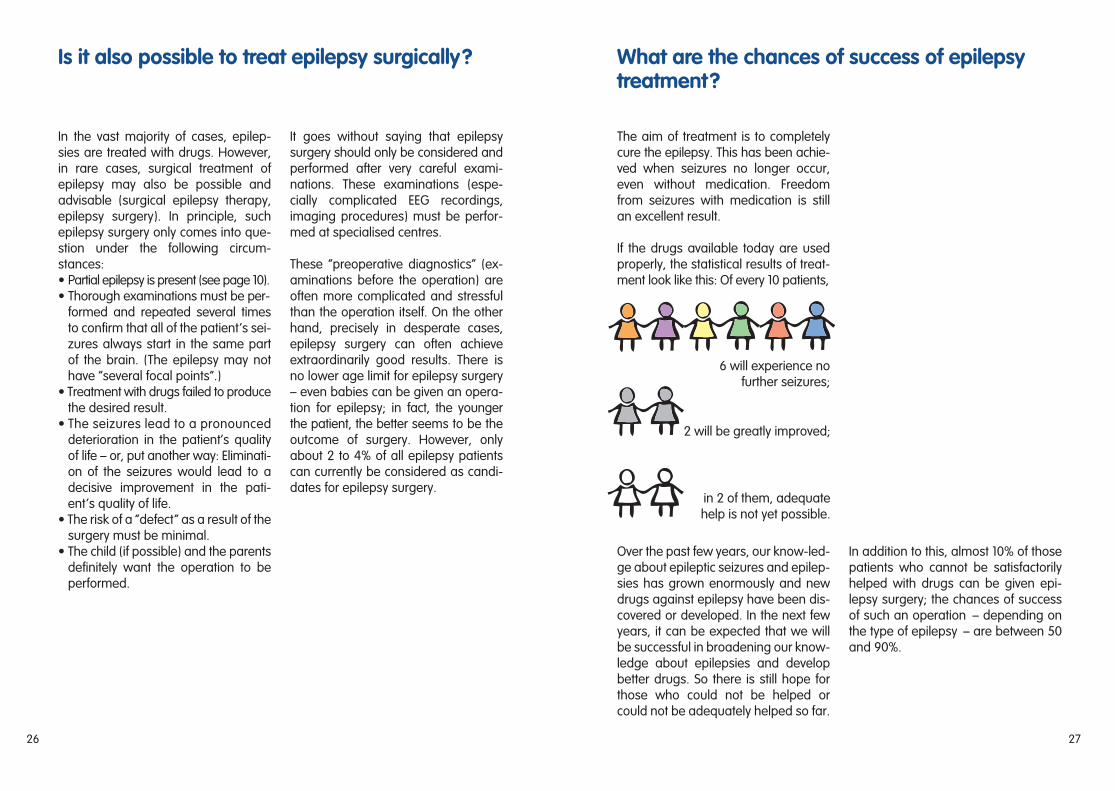
The aim of treatment is to completelycure the epilepsy. This has been achie-ved when seizures no longer occur,even without medication. Freedomfrom seizures with medication is stillan excellent result.
If the drugs available today are usedproperly, the statistical results of treat-ment look like this: Of every 10 patients,
Over the past few years, our know-led-ge about epileptic seizures and epilep-sies has grown enormously and newdrugs against epilepsy have been dis-covered or developed. In the next fewyears, it can be expected that we willbe successful in broadening our know-ledge about epilepsies and developbetter drugs. So there is still hope forthose who could not be helped orcould not be adequately helped so far.
In addition to this, almost 10% of thosepatients who cannot be satisfactorilyhelped with drugs can be given epi-lepsy surgery; the chances of successof such an operation – depending onthe type of epilepsy – are between 50and 90%.
Is it also possible to treat epilepsy surgically? What are the chances of success of epilepsytreatment?
6 will experience no further seizures;
2 will be greatly improved;
in 2 of them, adequatehelp is not yet possible.
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 31

28 29
Alternative methods of treatment arethose which are applied instead of thestandard and generally acceptedtherapy (in particular instead of drugtreatment and epilepsy surgery) andwhich have yet to be fully tested for theireffectiveness.
With the use of such therapeutic mea-sures, it is especially hoped that theactual or suspected side effects of drugtreatment can be avoided and that atleast an equivalent effect against theepileptic seizures can be achieved.
At the moment, there are no alternati-ve forms of treatment available for epi-leptic seizures that would be equivalentor even superior to the standard thera-peutic options.
Acupuncture is not capable of impro-ving the seizure situation in epilepticchildren. The biofeedback method, inwhich the patient is supposed to learnhow to suppress impending seizuresand in principle reduce the seizurepotential through self-control, has notproved sufficiently effective in the treat-ment of epilepsy to date. In older child-ren or adolenscents, this treatmentmethod can at most be regarded as asupporting measure to accompanydrug therapy.
The ketogenic diet has already beendescribed above ( see p. 24). The possi-ble risk of such a strict, one-sided dietmust again be pointed out here.
So-called vagus stimulation (electricalstimulation of the vagus nerve [in thearea of the neck] by means of surgicallyimplanted electrodes – comparable toa pace-maker in the heart has led to areduction in seizure frequency in a fewselected patients over the past fewyears; however, this treatment optioncan only play a supporting role inexceptional cases and has not beenproperly tested on children and adoles-cents.
Psychotherapeutic measures are notsuitable as a “treatment for epilepsy“,although their importance in helpingepileptic patients, including children, tocope with their psychological problemsis unquestioned.
As soon as the seizures have improv-ed or disappeared, there is no pro-blem with sending small children tokindergarten. Particularly in epilepticchildren, early integration into a groupis of considerable importance in pre-venting feelings of inferiority.
If you believe there is a possibility thatyour child might have an epileptic sei-zure during kindergarten, you shouldtell the teachers about this and informthem about the main features of yourchild's disease. If necessary, ask yourdoctor to provide this information, es-pecially if certain measures should betaken in the event of a seizure in thekindergarten (e.g. administering aDiazepam Desitin® rectal tube).
Are there ‘alternative‘ methods for the treat-ment of epilepsy?
Should a child go to kindergarten if it has epilepsy?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 33

30 31
If the epileptic child has a normal men-tal age, there is no reason not to sendit to primary and secondary school orlater to any other more advancedschools.
Mental exercise reduces the tendencytowards seizures; however, all mentaloverexertion should be avoided. Forexample, it is wrong to try and improveyour child‘s school performance byforcing it to do hours of homework.Sufficient relaxation in games is extra-ordinarily important, especially for theepileptic child. As regards informingthe teachers about your child‘s epi-lepsy, the same applies as for the kin-dergarten situation (see page 29).
Occasionally, it may be necessary –particularly if your child is not yet freeof seizures – to make special arrange-ments for the journey to and fromschool. The options range from youaccompanying your child personally,having it taken by other parents (alter-nately) or by a responsible school-friend,to special transportation (if available).
The decision about whether or notyour child should go to an advancedschool should not be based primarilyon the child‘s epilepsy; as with other chil-dren, the most important considera-tions should be your child‘s talents andinclinations and your own ideas concer-ning your child‘s education and future.
If normal school is too much for yourchild, do not be afraid to send it to apreparatory school or a special schoolfor the physically handicapped, espe-cially if the teacher or doctor advisesthis. It is not a disgrace to go to a spe-cial school. Apart from this, just asmuch knowledge can be conveyed intoday‘s special schools, particularlysince the classes are smaller here andthe teachers can devote more time toyour child‘s individual difficulties. Anddon‘t forget, some children who attendspecial schools are more successful inlater professional life than childrenwho are tortuously forced through pri-mary school with excessive pressureand obedience.
If your child shows very little ability anddoes not fulfil the requirements of apreparatory school, it can still often makeextraordinary progress in a specialschool for the mentally handicappedand discover a joy in life when the con-stant pressures to perform are removed.
What is the right kind of school for epilepticchildren?
The history books tell us of many peoplewho suffered from epilepsy and stillachieved greatness, like the states-man Caesar, the poet Dostoyevsky,the painter van Gogh, the composerHändel and the naturalist Helmholtz.
Even in today‘s technological world,many of our epileptic citizens are able,under the protection of modern treat-ment, to take up a wide variety of dif-ferent professions and pursue them tothe full.
If the seizures can be greatly improvedor brought completely under controlwith medication, and if your child hasthe necessary mental ability and cha-racter, nothing stands in the way oftheir being trained in the majority ofprofessions.
Jobs that involve the danger of falling,jobs on unprotected machines or jobsthat include driving public vehicles arenaturally unsuitable for epileptics.
In professional life, you have undoubt-edly already discovered that intelli-gence alone is not the only way ofmeasuring professional success. Be-ing good with your hands, reliabilityand conscientiousness are sometimesmore important-qualities often heldby epileptics. But even if your childcannot be adequately helped with thetreatment methods offered by modernmedicine, or if it has a physical ormental disability in addition to the epi-lepsy, integration into a profession isby no means ruled out.
What are the job prospects for epilepticchildren?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 35

32 33
Physical exercise, games and sportsare ways in which the child can freelyexpress itself. The epileptic childshould not be deprived of this: Thedevelopment of self-assurance, co-ming together with children of thesame age, experiencing the sense ofsuccess, but also coming to terms withdefeat, obeying rules, physical train-ing – all these things are just as impor-tant for an epileptic child as for ahealthy one. In addition to this, beingin good physical shape has a benefi-cial effect on the outcome of treatment.
Nevertheless, certain restrictions arenecessary: Overexertion (e.g. long-dis-tance running and high-performancesports) should be avoided, along withsports in which there is a danger of fal-ling (apparatus gymnastics, climbingbars, riding) and those involving “dan-gerous” sports equipment (e.g. ham-mer, fencing sword).
Although seizures only occur very ex-ceptionally when swimming, the epi-leptic child should never go swimmingwithout adult supervision; swimmingin open water (sea, river, lake) shouldnot be allowed unless a life-jacket isworn that will keep an unconsciouschild‘s head above water; likewise,any child that is taken in a boat mustwear a life-jacket.
Even in the bathtub at home, the epi-leptic child should always be undersupervision.
Cycling can be extremely hazardousfor the epileptic child and other roadusers if a seizure occurs. Cycling shouldtherefore be completely prohibited inheavy traffic until the patient has beenfree of seizures for at least one yearand should otherwise only be allowedif the patient has been free of seizuresfor at least 3 months.
In some epileptic children, the flicker-ing of a television or computer screencan lead to an increased stimulabilityof the nerve cells in the brain and maytrigger seizures (called photogenic epi-lepsy-see page 13).
Using the EEG, it is easy for the doctorto determine whether the child hassuch a hypersensitivity to light stimuli.However, it is not necessary to com-pletely prohibit such “photosensitive”children from watching television, al-though a certain amount of “TV ma-nagement” is necessary. Here are somespecific points you should bear inmind:• Do not allow your child to spend too
much time in front of the TV screen(the time allowed should mainly bedecided along the lines of educatio-nal considerations, but should not belonger than 1 to 1 1/2 hours).
• Do not allow your child to sit too closeto the TV; the place farthest awayfrom the TV is always best.
• Do not allow your child to darken theroom too much when watching TV sothat the light-dark contrasts are nottoo pronounced.
• Place additional lamps near the TV - also to moderate the light-dark con-trasts.
• The television picture should be incolour (not black and white) and thecontrast setting should not be toobright.
• Lack of sleep and tiredness furtherincrease the likelihood of seizures,so the TV should be turned off whenthe first signs of tiredness are obser-ved.
In particularly predisposed children withpronounced photosensitivity, it may benecessary to darken the monitor withan anti-glare screen or to give the childa pair of dark-tinted glasses.
The small screen on Game-Boys (li-quid-crystal display) is not capable oftriggering epileptic seizures in photo-sensitive children; therefore, the deci-sion about whether or not to allowchildren to use Game-Boys, even ifthey have photogenic epilepsy, can bemade from a purely educational pointof view.
Again, you should discuss any specificquestions you have on this subjectwith your doctor.
Is an epileptic child allowed to watch TV?Is an epileptic child allowed to play sports?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 37

34 35
Most vaccinations are no more of arisk for epileptic children than they arefor healthy children – this particularlyapplies to vaccinations against teta-nus, measles, mumps, German meas-les, diphtheria and polio.However, caution is recommendedconcerning whooping cough vaccin-ation; only the acellular vaccine shouldbe used (not the whole vaccine).Neither should epileptic children begiven inoculations against typhoid fever,paratyphoid fever or cholera.
If your child should require surgery(e.g. appendix, tonsils, hernia) theanaesthetist and the surgeon must beinformed about the disease and thedrugs being taken. In general, the riskof the operation is not increased byepilepsy; just a few of the drugs usedagainst epilepsy can reduce the abilityof the blood to clot; however, if the an-aesthetist has been informed aboutthese drugs, he will have the agentsnecessary to counteract this ready athand, just in case they are needed.
It is important to ensure that the drugtreatment is not interrupted during thestay in hospital. Discuss this with thedoctor on the ward or the anaesthetist,especially if the tablets have to be tem-porarily discontinued to ensure anempty stomach before the operationand in gastrointestinal operations. Insuch cases, antiepileptic medicationmust be injected into the muscles ordirectly into the blood-stream or admi-nistered rectally (through the intestines).
Just like all other children, epilepticchildren obtain the right kind of secu-rity and care within the family. Never-theless, under certain circumstances, itmay be necessary to place such achild in a home for a certain time orpossibly even permanently.
Unlike the way it used to be, suchhomes and institutions are no longerdesigned purely for custody and care.They often have experienced doctors,teachers and medical counsellors. Somehomes also offer vocational training.Many different things are done in theinterest of the patients‘ medical andsocial rehabilitation.
For the parents, it is naturally a difficultdecision to part from their child, parti-cularly when the child is ill. However, iffrequent seizures occur despite experttreatment and the teaching staff of thelocal school feel that they are unableto cope with the severe and frequentseizures, or if the local school cannotoffer adequate support and therapy,or ultimately if relatives are unable tocare for the child due to ill-ness, age orother family circumstan-ces, the deci-sion will be taken to place the child inthe care of a home.
On the other hand, when taking thisundoubtedly very difficult decision toplace an epileptic child in a home, it iscertainly worth bearing in mind that lifein a home may well open up newopportunities for the child in certainareas: e.g. with regard to educationaladvancement, vocational training, re-creation, and contact with other dis-abled children who have very similarproblems.
Your doctor may advise you aboutwhich home might come into question.
What do I do if my child needs vaccinations oran operation?
When should an epileptic child be cared for in a home?
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 39

36 37
Address index – Where do I go from here?
In Austria:
Sekretariate der Österreichischen Sektion der Internationalen Liga gegen Epilepsie(Austrian Section of the International League against Epilepsy)Hospital for Neurological of the UniversityAnichstraße 35 · A-6020 Innsbruck · Tel.: ++ 43 512 504-38 79
Hospital for Neurological of the UniversityWähringer Gürtel 18 - 20 · A-1090 Wien · Tel.: ++ 431 / 40 400-34 33
Elterninitiative anfallskranker Kinder (EIAK)Breitenseerstr. 9/5, A-1140 Wien, Tel. 01 / 650 813 37 37, E-mail: [email protected]
In the Czech Republic:
Ceská sekce mezinárodni ligy proti epilepsii(Czech Section of the International League against Epilepsy)Vídenská 1083 · CZ-142 00 Praha 4 · Tel.: ++ 42 2 471 31 55
Spolecnost „E“(Czech Epilepsy Association)Novodvorská 994, CZ-142 21 Praha 4 · Tel.: ++ 42 2 476 15 57
Nadace Detsky mozek(Child Brain Foundation)Rimská 16 · CZ-120 00 Praha · Tel.: ++ 42 2 269 62 25
In Germany:
Deutsche Epilepsie-Vereinigung e.V. (DE)(German Epilepsy Alliance-alliance of self-help groups)Administrative office: Zillestr. 102 · D-10585 Berlin · Tel.: ++ 49 30 3 42 44 14
Deutsche Sektion der Internationalen Liga gegen Epilepsie(German Section of the International League against Epilepsy)Administrative office: Herforder Str. 5-7, D-33602 Bielefeld · Tel.: ++ 49 521 12 41 92 (10-12 a.m. daily)
Informationszentrum Epilepsie (IZE)(Epilepsy Information Centre)Herforder Str. 5-7, D-33602 Bielefeld, Tel.: ++ 49 521 12 41 17 (9-12 a.m. daily)
Stiftung Michael zur Bekämpfung von Anfallkrankheiten(Michael Foundation for Combating Convulsive Diseases)Münzkamp 5, D-22339 Hamburg, Tel.: ++ 49 40 5 38 85 40
In Hungary:
Hungarian Section of ILAEHüvösvölgyi út. 116 · H-1021 BudapestMH Budai Honvédkórház · Királyhágó út. 1/3. · H-1126 Budapest
In Poland:
Polish league against Epilepsy (medical association)Department of Neurology and Epileptology, Medical Center of Postgraduate Educationul. Czerniakowska 231 · PL- 00416 Warsaw · Tel.: ++ 48 22 625 41 26 · Fax.: ++ 48 22 625 10 14
Polish Association of People suffering from Epilepsy(self-supporting organization of patients and parents,a member of International Bureau for Epilepsy)ul. Fabryczna 57 · PL-15482 Bialystok · Tel./Fax.: ++ 48 85 75 44 20
Foundation of Epileptology(Editor of „Epileptologia“, journal of PLAE)Al. Niepodeeglosci 214 m. 4 · PL- 00608 Warsaw · Tel./Fax.: ++ 48 22 25 21 06
In Slovakia:
Slovenská liga proti epilepsii(Slovakian Section of the International League against Epilepsy)SL-975 17 Banská Bystrica · Slovakia · Tel.: ++ 42 88 71 27 05
In Switzerland:
Schweizerische Liga gegen Epilepsie (SLgE)(Swiss League against Epilepsy)Dorfstr. 2 · Postfach 233 · CH-8712 Stäfa · Tel.: ++ 41 1 9 26 89 71
Schweizerische Vereinigung der Eltern epilepsiekranker Kinder (ParEpi)(Swiss Alliance of Parents of Epileptic Children)Rothstr. 17 · Postfach · CH-8042 Zürich
Epilepsie-Vereinigung Schweiz (E-V-CH)(Swiss Epilepsy Alliance)Alpenstr. 66 · CH-8200 Schaffhausen · Tel.: ++ 41 52 6 24 56 75
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 41

38 39
Absence seizure 7, 8, 10, 20Acupuncture 28Age 5Age of onset 5Alcohol 13, 24Allergy 25“Alternative” methods 28Anomalies 12Aura 7, 8, 19
Bathtub 21, 32Behavioural disorders 14, 15Biofeedback 28Bite injury 6Blood levels 25Brain haemorrhage 12Brain tumour 12
Causes 12Chromosomal disorders 12Computerised tomography 16Contusion of the brain 12Convulsive disease 4Cycling 21, 32
Damage at birth 12, 14Danger of falling 31Diagnostics, preoperative 26Diazepam suppositories 19Diet 23Diet, ketogenic 24Disposition, genetic 11Drop attacks 7Drugs 22, 27Drugs, adverse reactions 15, 25
Electric shock 4Electrodes 17Electroencephalogram (EEG) 9, 17
Encephalitis 12, 18Epilepsy (definition) 4, 10, 11
focal 10, 26generalised 10genetically-related; idiopathic 11surgery 26symptomatic 11, 12, 14
Facilitation 21Febrile convulsions 18Fever 13Frequency 5
Game-Boy 33Glasses, Polaroid 33Goutiness 18Grand mal 6, 8, 19, 21
Head injury 4Hemilateral seizure 6, 8, 10Hereditary disease 11Home 35Homoeopathy 28Hypersensitivity 25, 33
Infant spasms 18Intelligence, reduced 14
Jaw seizure 6Job prospects 31Job-seeking scheme 31
Kindergarten 29
Lapse in consciousness 7Lifestyle 23Lightning convulsions 7Liver function 25
Magnetic resonance imaging 16Meningitis 12Mental disorder 4, 14Metabolic disorders 12
Nodding spasms 7Notification to the authorities 5
Occasional seizures, convulsions 18Operations 34Overdosage 25Overexertion 14Oxygen deficiency 4, 12
Performance, partial deficiencies 14Phase, clonic 6Phase, tonic 6Photogenic epilepsy 33Photosensitivity 33Pill box 23Plasma concentration 25Precursors 7Predisposition 11, 12Predisposition, familial 11Prognosis 10Puberty 5, 21, 23Pyknolepsy 10, 11
Reading/writing weakness 14Reflex-induced seizures 13Rehabilitation 31, 35Rolandic epilepsy 10, 11
Salaam convulsions 7Salivation 6, 10, 19School 30School, journey to and from 30Seizure 4, 5, 6, 10, 13
age-independent 8age-related 8complex partial 7diary 23focal; 8generalised 8major 6minor 7, 9psychomotor 7, 8, 10series 9, 15
Sensation, strange 7Sensory disorder 7Sleep EEG 17Sleep, lack of 13, 23Sleep, seizures during 6Special kindergarten 29Special school 30Sports 32Status epilepticus 9, 15, 21Suppository 19, 29Swimming 21, 32
Teething troubles 18Test methods 16Tolerability tests 25Treatment 21, 22, 23, 27Trigger 11, 13Television 33TV epilepsy 33TV management 33
Vaccinations 34Vocational training centre 31
Warning signs 7Winking spasms 7Workshop for the disabled 31
Index
Unser_Kind_03/04_engl 30.03.2005 10:49 Uhr Seite 43