-
7/27/2019 Hardiness and Coping Strategies.pdf
1/18
Journal of Behavioral Medicine, Vol. 23, No. 3, 2000
The Relationship of Hardiness, Coping Strategies,and Perceived
Stress to Symptoms of Illness
Mike Soderstrom,1 Christyn Dolbier,1 Jenn Leiferman,1
and Mary Steinhardt1,
2
Accepted for publication: January 12, 2000
We proposed a conceptual model based on research supporting the
relation-ship between symptoms of illness and the determinants of
hardiness, copingstrategies, and perceived stress. In this model,
hardiness, avoidance coping, andapproach coping have paths to
perceived stress, perceived stress has a path to
symptoms of illness, and hardiness also has a path to symptoms
of illness. Weexamined the goodness of fit of this model using path
analysis and tested its
stability, as well as the presence of gender effects, in
corporate (N = 110) anduniversity (N=271) samples. The proposed
model was a good fit for the data inthe corporate sample, and no
gender effects were found. The proposad modelwas not a good fit for
the data in the university sample, therefore we added two
paths that have received some support in the research: from
approach copingto symptoms of illness and from avoidance coping to
symptoms of illness.This model was a good fit for the data in the
university sample, however, the
path from approach coping to symptoms of illness had a critical
ratio
-
7/27/2019 Hardiness and Coping Strategies.pdf
2/18
312 Soderstrom, Dolbier, Leiferman, and Steinhardt
INTRODUCTION
It is well documented that psychological stress is associated
with a vari-
ety of physical and mental health illnesses (Dohrenwend and
Dohrenwend,1974, 1981; Sapolsky, 1994). However, the magnitude of
these correlations ismoderate (Rabkin and Struening, 1976),
suggesting that stress accounts foronly a portion of the variance
in illness. Such data have led researchers toconclude that stress
does not inevitably lead to illness (Wiebe and McCallum,1986). As a
result, research has focused on identifying those factors that
havedirect, indirect or modifying effects on illness.
Although there has been an abundance of research over the past
twodecades focused on hardiness, coping strategies, perceived
stress, and ill-
ness, the nature of the relationships among these variables
remains inconclu-sive. Much research indicates that a hardy
personality (Kobasa et al., 1982a)and approach-oriented coping
behaviors (Williams et al., 1992) moderate orbuffer the effect of
stress on health. However, other research indicates thata hardy
personality is not a moderating variable in the relationship
betweenstress and illness, but rather hardiness has a direct effect
on illness indepen-dent of its effect on stress (Orr and Westman,
1990). Simultaneously, it hasbeen proposed that coping strategies
mediate the relationship between har-diness and health (Gentry and
Kobasa, 1984; Williams et al., 1992). Research
has yet to examine concurrently the direct, indirect, and
modifying effects ofhardiness, coping strategies, and perceived
stress on symptoms of illness.
Hardiness
The hardiness concept was originally developed by Kobasa (1979).
Theconcept emerged from an existential theory of personality
(Kobasa andMaddi, 1977) and is defined as a personality
characteristic describing an in-dividual with three closely related
tendencies: challenge, commitment, andcontrol. The term challenge
reflects an outlook on life that enables an indi-vidual to perceive
change as an opportunity for growth rather than a threatto ones
sense of security or survival. Change rather than stability is seen
asthe normative mode of life. Individuals strong in commitment
believe in thetruth and value of who they are and what they are
doing. They have a senseof meaning and purpose in work and
relationships and are deeply involvedrather than alienated out of
fear, uncertainty, or boredom. The term controlreflects a belief
that one can influence the course of life events within rea-sonable
limits. Hardy individuals have an internal sense of personal
mastery,confronting problems with confidence in their ability to
implement effectivesolutions, rather than feeling powerless,
lacking self-confidence and initiative,and manipulating others.
-
7/27/2019 Hardiness and Coping Strategies.pdf
3/18
Hardiness, Coping, Stress, and Illness 313
It was originally hypothesized that a hardy personality improves
healthby buffering or moderating the effects of stress. Some
studies support thisoriginal hypothesis (Kobasa et al., 1982a;
Rhodewalt and Zone, 1989); how-
ever, other research has found hardiness to have a direct effect
on health in-dependent of stress (Banks and Gannon, 1988; Kobasa,
1979; Kobasa et al.,1981, 1982a, 1983, 1985; Kobasa and Puccetti,
1983; Nowack and Hanson,1983; Pollock, 1986; Wiebe and McCallum,
1986). Comprehensive analysesof this research base have found that
the buffering effect of hardiness onstress is weaker than its
direct effects on health (see reviews by Funk, 1992;Gentry and
Kobasa, 1984; Hull et al., 1987; and Orr and Westman, 1990).
Still other studies revealed that hardiness has an indirect
effect onhealth through improved health practices (Wiebe and
McCallum, 1986) and
approach-oriented coping strategies (Williams et al., 1992).
High-hardy indi-viduals engage in behaviors positively associated
with health and greater ap-proach or problem-focused coping
strategies, whereas low-hardy individualsengage in behaviors
negatively associated with health and greater avoidanceor
emotion-focused coping strategies. These studies suggest that
health prac-tices and coping strategies mediate the stressillness
relationship differentlyfor high-hardy and low-hardy
individuals.
Kobasas initial finding that hardiness was predictive of health
outcomeswas based solely on male samples, raising the issue of
generalizability of these
findings to women. Studies examining gender differences are
inconsistent.Some studies have found that the relationship between
hardiness and healthoutcomes seen in male samples is generalizable
to female samples (Ganellenand Blaney, 1984; Gentry and Kobasa,
1984; Rhodewalt and Agustsdottir,1984; Rhodewalt and Zone, 1989).
However, other studies have shown thatthe predictive nature of
hardiness found in males is not generalizable tofemales (Schmied
and Lawler, 1986; Shepperd and Kashani, 1991; Wiebe,1991). It has
been suggested that these gender differences in hardiness aredue to
differences in coping strategies (Wiebe, 1991; Williams etal.,
1992). Forinstance, several studies have found that males and
females employ differentcoping strategies in the face of stress
(Billings and Moos, 1981; Kvam andLyons, 1991; Pearlin and
Schooler, 1978), suggesting that the mechanismby which coping
influences the hardinessillness relationship is different formales
and females.
Coping Strategies
Coping refers to the cognitive and behavioral efforts to manage
situa-tions appraised as taxing or exceeding personal resources.
Researchers makea common conceptual distinction in the focus of
coping strategies. There arethose strategies that are
approach-oriented and deal with confronting the
-
7/27/2019 Hardiness and Coping Strategies.pdf
4/18
314 Soderstrom, Dolbier, Leiferman, and Steinhardt
problem and those that are oriented to avoiding dealing directly
with theproblem (Roth and Cohen, 1986, Moos et al., 1990). While
their focus is dif-ferent, both approach and avoidance coping use
cognitive and behavioral
methods to address the stressful situation and have been likened
to transfor-mational and regressive coping, respectively (Gentry
and Kobasa, 1984), aswell as problem-focused and emotion-focused
coping, respectively (Lazarusand Folkman, 1984). Approach coping
strategies are aimed at problem solv-ing or active attempts to
resolve the stressor. Avoidance coping strategiesare aimed at
avoiding active confrontation of the stressor or reducing
emo-tional tension associated with the stressor. Coping strategies
that fall underthe approach-oriented domain have been associated
with less stress (Pearlinand Schooler, 1978) and illness (Blake and
Vandiver, 1988; Olffet al., 1993),
while those falling under the avoidance-oriented domain have
been associ-ated with more stress (Pearlin and Schooler, 1978) and
illness (Blake andVandiver, 1988; Holahan and Moos, 1985; Kobasa,
1982).
It has been proposed that high-hardy individuals engage in
approachcoping styles for the purpose of transforming stressful
events into situationsthat seem to be more manageable. In contrast,
low-hardy individuals tend toengagein avoidancecopingstylessuch as
cognitiveand behavioral disengage-ment and denial to deal with a
stressful situation (Gentry and Kobasa, 1984).These coping styles
neither transform the situation nor solve the problem
thought to be the source of stress. Several studies show support
for a rela-tionship between hardiness and coping strategies,
whereby high-hardy indi-viduals use more approach- or
problem-focused types of coping strategiesand low-hardy individuals
use more avoidance- or emotion-focused copingstrategies (Florian et
al., 1995; Williams et al., 1992).
Although based on conceptualizations of traditional sex roles,
it is com-monly assumed that men tend to be more analytical and
task-oriented in re-sponse to stressful situations, while women
respond more emotionally. Thisassumption infers that men are more
inclined to use approach-oriented cop-ing strategies aimed at the
problem, whereas women use avoidance-orientedcoping strategies
aimed at reducing emotional tension. In fact, a pattern ofgender
differences in coping strategies consistent with part of this
assump-tion has been observed, showing that women appear somewhat
more likelyto report using avoidance- or emotion-focused coping
strategies, includingventing or expressing emotions, becoming
depressed, and avoiding the situa-tion (Billings and Moos, 1981;
Fondacaro and Moos, 1989; Kvam and Lyons,1991; Pearlin and
Schooler, 1978; Ptacek etal., 1992). In terms of approach-
orproblem-focused coping, as of yet there is not a clear pattern of
gender differ-ences. Some studies show that men report using more
approach- or problem-focused coping (Holahan et al., 1995; Kvam and
Lyons, 1991; Ptacek et al.,1992, 1994). Additional research
supports these findings, but only in certain
-
7/27/2019 Hardiness and Coping Strategies.pdf
5/18
Hardiness, Coping, Stress, and Illness 315
situations (Folkman and Lazarus, 1980), and still other research
has foundthe opposite, with more problem-focused coping in women
(Vitaliano et al.,1985) or no differences between men and women
(Holahan and Moos, 1985).
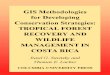
Based on the above research, we proposed a conceptual model
illustrat-ing the relationships among hardiness, coping strategies,
perceived stress,and symptoms of illness. We predicted that
hardiness would have a negativerelationship to symptoms of illness
independent of perceived stress (Banksand Gannon, 1988; Kobasa,
1979; Kobasa et al., 1981, 1982a,b, 1983, 1985;Kobasa and Puccetti,
1983; Nowack and Hanson, 1983; Pollock, 1986; Wiebeand McCallum,
1986). On the basis of previous research, we also hypothe-sized
that perceived stress would demonstrate a positive relationship
withsymptoms of illness (Dohrenwend and Dohrenwend, 1974, 1981;
Sapolsky,
1994).Inaddition,onthebasisofcopingresearch,wepredictedthatapproachcoping
would have a negative relationship to perceived stress and
avoidancecoping would have a positive relationship to perceived
stress (Pearlin andSchooler, 1978).
This set of predictions is shown graphically in Fig. 1 as a
nonreciprocalpath model. The purpose of this study was to examine
the goodness of fit ofthe proposed model using path analysis and
test its stability in two differentsamples. These were convenience
samples of corporate employees and uni-versity students.
Additionally, because some research indicates that gendermay be a
differentiating variable, we also examined whether or not the
pro-posed model differed by gender. This study extends earlier
research in that
Fig. 1. Model 1 for the corporate sample.
-
7/27/2019 Hardiness and Coping Strategies.pdf
6/18
316 Soderstrom, Dolbier, Leiferman, and Steinhardt
it examines the constructs of hardiness, coping strategies,
perceived stress,and symptoms of illness concurrently.
METHODS
Subjects
Corporate Sample
Data for the corporate sample were collected from full-time
employeesof 3M in Austin, Texas. The overall subject pool included
a convenience sam-ple of employees (N= 110) with a mean age of 42.4
8.5 years who were
members of 3Ms employee wellness program. 3M has approximately
1900employees located in Austin, 1200 of whom are members of the
wellnessprogram. All subjects were assured that their decision
regarding whether ornot to participate would have no effect on
their relationship with 3M or theuniversity.
University Sample
Data for the university sample were collected from students
enrolled in
undergraduate introductory psychology classes at The University
of Texasat Austin. Two hundred seventy students with a mean age of
19.2 3.0 yearsvolunteered to participate. All subjects were assured
that their decision re-garding whether or not to participate would
have no effect on their grade inthe class or their relationship
with the university.
Procedures
The study involved a cross-sectional research design using
survey data.Both corporate and university subjects completed a
questionnaire in smallgroups of approximately 1520 individuals in
quiet classroom conditions.Study procedures were approved by The
University of Texas InstitutionalReview Board, and data were
collected and recorded so as to protect theanonymity of
subjects.
Instrumentation
Hardiness
Bartone et al.s (1989) 30-item dispositional resilience scale
was se-lected as a measure of hardiness because it represents one
of the best third
-
7/27/2019 Hardiness and Coping Strategies.pdf
7/18
Hardiness, Coping, Stress, and Illness 317
generation measures of hardiness (Funk, 1992), assessing each of
the closelyrelated tendencies of challenge, commitment, and
control. The internal con-sistency of the hardiness scale was = .81
for the corporate sample and
= .78 for the university sample. For both samples, the internal
consistencyof the composite measure of hardiness was higher than
for each of the threesubscales, thus supporting the use of the
composite measure.
Coping Strategies
Coping strategies were assessed using the dispositional version
of theCoping Orientations to Problems Experienced (COPE) scale
(Carver et al.,
1989), which measures a broad range of cognitive and behavioral
copingstrategies that individuals typically use in stressful life
situations. The totalscale contains 53 items and measures 14
subscales of coping styles. For ourpurposes, 8 of the 14 subscales
of the COPE were used to measure approachand avoidance coping
strategies. Each subscale contained four items.
Four subscales were combined to assess approach coping
strategies: ac-tive coping, planning, positive reinterpretation and
growth, and suppressionof competing activities. Active coping
measures behavioral attempts to takeaction to deal directly with
the problem (I take direct action to get around
the problem). Planning assesses cognitive attempts to come up
with actionstrategies (I think hard about what steps to take).
Positive reinterpretationand growth measures cognitive attempts to
construe the problem in positiveterms while accepting the reality
of the situation (I try to grow as a personas a result of the
experience). While some researchers regard this type ofcoping as
emotion-focused (Lazarus and Folkman, 1984), others classify it
asan approach-oriented coping strategy whose value exceeds merely
reducingdistress (Holahan et al., 1997; Moos et al., 1990; Carver
et al., 1989). Suppres-sion of competing activities assesses
cognitive and behavioral attempts toavoid becoming distracted by
other events in order to deal with the problem(I keep myself from
getting distracted by other thoughts or activities). Theinternal
consistency of approach coping was = .89 for the corporate
sampleand = .87 for the university sample.
Four subscales were also combined to assess avoidance coping
strategies:denial, behavioral disengagement, mental disengagement,
and focus on andventing of emotions. Denial measures cognitive
attempts to refuse to believethat the problem exists (I pretend
that it hasnt really happened). Behav-ioral disengagement assesses
behavioral attempts to reduce ones effort todeal with the problem
(I just give up trying to reach my goal). Mentaldisengagement
measures behavioral attempts to distract the person fromthinking
about the problem (I turn to work or other substitute activities
to
-
7/27/2019 Hardiness and Coping Strategies.pdf
8/18
318 Soderstrom, Dolbier, Leiferman, and Steinhardt
take my mind off things). Focus on and venting of emotions
assesses be-havioral attempts to focus on the distress associated
with the problem and toventilate those feelings (I get upset and
let my emotions out). The internal
consistency of avoidance coping was = .79 for the corporate
sample and = .80 for the university sample.
Perceived Stress
Perceived stress was defined as the degree to which situations
in oneslife during the past month were perceived as stressful, as
measured by the14-item Perceived Stress Scale (Cohen et al., 1983).
The scale has shown to
be a good predictor of stress in that it correlates highly with
symptomatogicalmeasures and life event scores (Cohen et al., 1983).
The internal consistencyof the perceived stress scale was = .89 for
the corporate sample and = .86for the university sample.
Symptoms of Illness
Psychosomatic symptoms of illness were measured by the
SymptomsChecklist (Bartone et al., 1989), which includes 20 items
measuring the ex-
tent to which subjects had experienced various physical and
psychologicalsymptoms over the past few weeks, such as the
commoncold or flu, headaches,upset stomach, and feeling nervous or
tense. The internal consistency of thesymptoms checklist was = .89
for the corporate sample and = .82 forthe university sample.
Data Analysis
Descriptive statistics including means and standard deviations
were cal-culated for men, women, and total sample on all variables
for both the cor-porate and university subjects. Gender differences
among variables wereexamined using Hotellings multivariate tests of
significance with follow-upunivariate tests. One analysis was
conducted on the variables hardiness, ap-proach coping, avoidance
coping, perceived stress, and symptoms of illness.A second analysis
was conducted using the subscales of hardiness, approachcoping, and
avoidance coping. In addition, Pearson correlation coefficientswere
calculated to examine the relationships among all variables for
eachsample.
To test the proposed conceptual model, path analysis was used in
boththe corporate and the university samples to examine
therelationship betweensymptoms of illness and the set of
determinants including perceived stress,
-
7/27/2019 Hardiness and Coping Strategies.pdf
9/18
Hardiness, Coping, Stress, and Illness 319
hardiness, and approach and avoidance coping. Gender differences
wereexamined by comparing a multiple-group or less restricted
model, where thepath coefficients for men and women were allowed to
be different, to the
more restricted single-group model, where the path coefficients
for men andwomen were forced to be the same.
Goodness-of-fit indices were examined using the chi-square test,
thenormed fit index (NFI), the comparative fit index (CFI), and the
TuckerLewis index (TLI). The chi-square statistic provides a test
of the null hypoth-esis that the reproduced covariance matrix has
the specified model structure(i.e., that the model fits the data).
The NFI ranges from 0 to 1, where 0 rep-resents the goodness of fit
associated with a null model (one specifying thatall the variables
are uncorrelated) and 1 represents the goodness of fit as-
sociated with a saturated model (a model with 0 degrees of
freedom thatperfectly reproduces the original covariance matrix).
The CFI and TLI aresimilar to the NFI. Values over .95 on the NFI,
CFI, and TLI indicate a goodfit between model and data (Schumacker
and Lomax, 1996).
RESULTS
Mean scores and standard deviations for men, women, and total
sam-
ple for all variables in the corporate and university subjects
are shown inTables I and II, respectively. Several mean differences
between males and
Table I. Means and Standard Deviations for Hardiness, Coping
Strategies, Perceived Stress, andSymptoms of Illness in the
Corporate Sample
Women Men Total(N= 70) (N= 40) (N= 110)
Hardiness 60.5 9.0 63.8 8.0 61.7 8.8Challenge 18.0 3.5 18.9 2.6
18.3 3.2
Commitment 21.2 4.4 22.6 3.9 21.7 4.3Control 21.2 3.7 21.9 4.1
21.5 3.6
Approach coping 48.7 8.4 49.4 5.6 49.0 7.5Active 12.4 2.3 12.8
1.6 12.5 2.1Planning 12.9 2.7 13.4 1.8 13.1 2.4Positive
reinterpretation and growth 12.7 2.7 12.5 2.1 12.6 2.5Suppression
of competing activities 10.7 2.3 10.8 2.0 10.8 2.2
Avoidance coping 32.1 6.6 28.1 6.0 30.4 6.8Denial 6.0 2.6 5.6
1.8 5.9 2.3Behavioral disengagement 7.0 2.3 6.3 2.3 6.7 2.3Mental
disengagement 8.6 2.4 8.0 2.4 8.4 2.4Focus on and venting of
emotions 10.3 2.7 7.8 2.5 9.4 2.9
Perceived stress 24.5 8.6 19.5 7.3 22.7 8.5Symptoms of illness
12.5 9.1 8.2 6.3 11.0 8.4
p < .01, two-tailed.
-
7/27/2019 Hardiness and Coping Strategies.pdf
10/18
320 Soderstrom, Dolbier, Leiferman, and Steinhardt
Table II. Means and Standard Deviations for Hardiness, Coping
Strategies, Perceived Stress,and Symptoms of Illness in the
University Sample
Women Men Total
(N= 168) (N= 102) (N= 270)
Hardiness 58.8 9.0 57.9 8.3 58.5 8.7Challenge 17.5 4.1 17.3 3.9
17.4 4.0Commitment 21.1 3.9 20.3 4.4 20.8 4.1Control 20.4 3.5 20.3
3.2 20.4 3.4
Approach coping 47.2 7.4 45.3 7.3 46.5 7.4Active 11.6 2.3 11.2
2.2 11.4 2.2Planning 12.6 2.5 11.9 2.7 12.5 2.6Positive
reinterpretation and growth 12.4 2.5 11.5 2.4 12.1 2.5Suppression
of competing activities 10.6 2.3 10.2 2.3 10.5 2.2
Avoidance coping 32.0 6.7 29.8 6.8 31.2 6.8
Denial 5.7 2.0 5.8 2.0 5.7 2.0Behavioral disengagement 6.2 2.2
6.6 2.6 6.4 2.4Mental disengagement 9.2 2.4 9.6 2.4 9.3 2.5Focus on
and venting of emotions 10.6 3.3 8.0 2.7 9.7 3.3
Perceived stress 26.0 8.3 24.8 7.6 25.5 8.0Symptoms of illness
15.4 7.6 12.5 6.8 14.3 7.4
p < .05, two-tailed.p < .01, two-tailed.
females were found. Hotellings multivariate overall test of
significance forthe variables hardiness, approach coping, avoidance
coping, perceived stress,and symptoms of illness was significant
for both the corporate [F(5,101) =3.9, p < .01] and the
university [F(5,239)= 5.8, p < .01] samples. The univar-iate
tests indicated that females used greater avoidance coping
strategiesin both the corporate [F(1,105)= 11.8, p < .01] and
the university [F(1,243) = 11.3, p < .01] samples. In addition,
females reported more symp-toms of illness in both the corporate
[F(1,105)= 9.4, p < .01] and the univer-sity [F(1,243)= 13.6, p
< .01] samples. Females in the corporate sample alsoreported
greater perceived stress [F(1,105)= 12.6, p < .01]. Hotellings
mul-tivariate overall test of significance for the subscales of
hardiness, approachcoping, and avoidance coping was also
significant for both the corporate[F(11,95)= 2.4, p < .01] and
the university [F(11,236)= 5.5, p < .01] sam-ples. The
univariate tests indicated that females in the university sample
usedgreater positive reinterpretation and growth coping strategies
[F(1,246) =5.1, p < .05] than males. In addition, females in
both the corporate [F(1,105)= 20.1, p < .01] and the university
[F(1,246)= 47.1, p < .01] samplesused greater focus on and
venting of emotions coping strategies.
Pearson productmoment correlations among the variables are
shownin Table III for the corporate and university samples. As
expected, higherlevels of hardiness are related to lower levels of
perceived stress and fewer
-
7/27/2019 Hardiness and Coping Strategies.pdf
11/18
Hardiness, Coping, Stress, and Illness 321
Table III. Correlations Among Variables in the Corporate and
University Samples
Approach Avoidance PerceivedHardiness Challenge Commitment
Control coping coping stress
Corporate sample
HardinessChallenge .64
Commitment .89 .39
Control .81 .22 .65
Approach coping .53 .39 .47 .41
Avoidance coping .48 .36 .42 .38 .29
Perceived stress .71 .51 .60 .58 .52 .60
Symptoms of .65 .50 .51 .54 .45 .51 .70
illnessUniversity sample
Hardiness
Challenge .68
Commitment .81 .24
Control .79 .27 .59
Approach coping .46 .17 .46 .43
Avoidance coping .39 .21 .34 .34 .21
Perceived stress .60 .32 .55 .50 .37 .62
Symptoms of .33 .11 .35 .31 .16 .52 .61
illness
p < .05, two-tailed.p < .01, two-tailed.
symptoms of illness for both the corporate and the university
samples. Hardi-ness is also associated with more approach coping
and less avoidance copingin both samples. Approach coping is
related to less perceived stress and fewersymptoms of illness for
the corporate and university samples, whereas avoid-ance coping is
related to greater stress and more symptoms of illness forboth
samples. Finally, greater levels of perceived stress are related to
moresymptoms of illness for both samples.
Corporate Sample Model
There was a nonsignificant gender effect with respect to the
relation-ship of hardiness, coping strategies, and perceived stress
to symptoms ofillness. The multiple-group model, where the path
coefficients for men andwomen were allowed to be different, was not
significantly different from themore restricted single-group model,
where the path coefficients for men andwomen were forced to be the
same [ 2(8, N= 110)= 8.77, p= .362]. There-fore, the path model for
the corporate sample assessed men and women com-bined. Results of
the path analysis supported the proposed model (Model 1),as
presented in Fig. 1. Estimation of the model revealed a
nonsignificantchi-square value [ 2(2, N= 110)= 2.52, p= .283] and
accounted for a large
-
7/27/2019 Hardiness and Coping Strategies.pdf
12/18
322 Soderstrom, Dolbier, Leiferman, and Steinhardt
Table IV. Goodness-of-Fit Indices for the Final Corporate and
University Models
Model 2 df p NFI CFI TLI RFI
CorporateModel 1 2.52 2 .283 .999 1.000 .998 .989
UniversityModel 1 15.14 2 .001 .996 .997 .977 .974Model 2 .62 1
.430 1.000 1.000 1.001 .998Model 3 1.79 2 .409 1.000 1.000 1.000
.997
amount of the variance in both symptoms of illness (R2= .54) and
perceived
stress (R2= .
62), indicating that the model fit the data well. All values of
thedescriptive goodness-of-fit tests exceeded .95, also indicating
a very good fitbetween the model and the data (see Table IV). Path
coefficients for theproposed model appear in Table V.
University Sample Model
There also was a nonsignificant gender effect with respect to
the rela-
tionship of hardiness, coping strategies, and perceived stress
to symptomsof illness for the university sample. The multiple-group
model, where thepath coefficients for men and women were allowed to
be different, was notsignificantly different from themore
restricted single-groupmodel, where the
Table V. Path Coefficients for the Final Corporate and
University Modelsa
Predicted Predicting Unstandarized Standarizedvariable variable
estimate estimate SE CR
Corporate modelStress Resilience .44 .46 .07 5.95Stress Approach
coping .20 .18 .08 2.52Stress Avoidance coping .40 .33 .09
4.78Symptoms of illness Stress .47 .47 .09 5.00Symptoms of illness
Resilience .30 .32 .09 3.39
University model
Stress Resilience .44 .46 .07 5.95Stress Approach coping .20 .18
.08 2.52Stress Avoidance coping .40 .33 .09 4.78Symptoms of illness
Stress .41 .47 .10 4.02
Symptoms of illness Resilience .29 .32 .09 3.26
a All path coefficients exceeded the absolute critical ratio
(unstandardized estimate/standarderror) value of 2.0 and thus are
significant beyond the .05 level.
-
7/27/2019 Hardiness and Coping Strategies.pdf
13/18
Hardiness, Coping, Stress, and Illness 323
path coefficients for men and women were forced to be the same [
2(8, N=270) = 6.75, p= .564]. Therefore, the path model for the
university sampleassessed men and women combined. However, results
of the path analysis
for the university sample did not support Model 1. Estimation of
the modelrevealed a significant chi-square value [ 2(2, N= 270)=
15.14, p= .001], in-dicating that the model did not fit the data
well. The path coefficient fromresilience to symptoms of illness
was the only path with a CR value less than2.0 (B= .05, = .06, SE=
.06, CR= .91), therefore, this path was removed.
Given that Model 1 did not fit the data for the university
sample, weadded two paths, from approach coping to symptoms of
illness and fromavoidance coping to symptoms of illness. Adding
these paths from copingstrategies to symptoms of illness have some
support in the literature. Ap-proachcoping hasbeen associated with
less illness (BlakeandVandiver, 1988;Olffet al., 1993) while
avoidance coping has been associated with more illness(Blake and
Vandiver, 1988; Holahan and Moos, 1985; Kobasa, 1982). For
thismodel (Model 2), there was a nonsignificant gender effect with
respect to therelationship of hardiness, coping strategies, and
perceived stress to symptomsof illness. The multiple-group model,
where the path coefficients for menand women were allowed to be
different, was not significantly different fromthe more restricted
single-group model, where the path coefficients for menand women
were forced to be the same [ 2(9, N= 270)= 10.64, p=
.301].Therefore, Model 2 assessed men and women combined. Results
of thisanalysis supported the proposed model. Estimation of the
model revealeda nonsignificant chi-square value [ 2(1, N= 270)=
.62, p= .430], indicatingthat the model fit the data well. However,
the path from approach coping tosymptomsofillness had a CRvalue
oflessthan2.0 (B= .06, = .06, SE= .05,CR = 1.09), thus we removed
this path and ran the model again. This model(Model 3) is shown in
Fig. 2.
There was a nonsignificant gender effect for Model 3 with
respect to therelationship of hardiness, coping strategies, and
perceived stress to symptomsof illness. The multiple-group model,
where the path coefficients for men andwomen were allowed to be
different, was not significantly different from themore restricted
single-group model, where the path coefficients for men andwomen
were forced to be the same [ 2(8, N= 270)= 10.88, p= .209].
There-fore,Model3assessedmenandwomencombined.Thismodelrevealedanon-significant
chi-square value [ 2(2, N= 270)= 1.79, p= .409] and accountedfor a
large amount of the variance in both symptoms of illness (R2= .40)
andperceived stress (R2= .54), indicating that the model fit the
data well. Allvalues of the descriptive goodness-of-fit tests
exceeded .95, also indicatinga very good fit between the model and
the data (see Table IV). Path coeffi-cients for the university
model appear in Table V, and all exceeded a valueof 2.0.
-
7/27/2019 Hardiness and Coping Strategies.pdf
14/18
324 Soderstrom, Dolbier, Leiferman, and Steinhardt
Fig. 2. Model 3 for the university sample.
DISCUSSION
This study examined the relationships of hardiness, coping
strategies,and perceived stress to symptoms of illness using
corporate and universitysamples. A conceptual model of these
relationships was proposed based onthe research and examined using
path analysis. We also examined genderdifferences among these
relationships.
Comparing the means of men and women in both samples, several
gen-der differences among coping strategies were found. Consistent
with otherresearch (Billings and Moos, 1981; Fondacarao and Moos,
1989; Kvam andLyons, 1991; Pearlin and Schooler, 1978; Ptacek et
al., 1992), women in bothsamples reported more avoidance coping
than men, and most distinctly thefocus on and venting of emotion
strategy. The finding that women from bothsamples did not have
significantly lower approach coping strategies is in-consistent
with some of the research that supports men use more approachcoping
strategies than women (Holahan et al., 1995; Kvam and Lyons,
1991;Ptacek et al., 1992, 1994). In fact, that university women
reported significantlymore of the positive reinterpretation and
growth strategy is consistent withresearch in this area that
supports the opposite stance, that women use moreapproach coping
than men (Vitaliano et al., 1985).
The correlational results for both samples in our study support
the re-lationships depicted in the literature. The well-documented
relationship be-tween perceived stress and illness was supported
(Dohrenwend and
-
7/27/2019 Hardiness and Coping Strategies.pdf
15/18
Hardiness, Coping, Stress, and Illness 325
Dohrenwend, 1981; Sapolsky, 1994). Consistent with the research
literature,hardiness and approach coping were inversely related to
stress and symp-toms of illness (Blake and Vandiver, 1988; Olffet
al., 1993; Orr and Westman,
1990; Wiebe and McCallum, 1986), whereas avoidance coping was
directlyrelated to stress and symptoms of illness (Blake and
Vandiver, 1988; Holahanand Moos, 1985; Kobasa, 1982; Pearlin and
Schooler, 1978). The finding thathardiness was directly related to
approach coping and inversely related toavoidance coping is also
consistent with other research (Florian et al., 1995;Williams et
al., 1992). The relationship between hardiness and symptoms
ofillness was also supported, thus supporting the preponderance of
researchin this area (Banks and Gannon, 1988; Kobasa, 1979; Kobasa
et al., 1981,1982a, b, 1983, 1985; Kobasa and Puccetti, 1983;
Nowack and Hanson, 1983;
Pollock, 1986; Wiebe and McCallum, 1986).Consistent with
previous research, the path of hardiness to symptoms
of illness was found in the corporate sample (Funk, 1992; Orr
and Westman,1990). This path was not, however, found in the
university sample. This dis-crepancy may be attributed to the age
difference between the corporate(mean age = 42.4) and the
university (mean age = 19.2) samples. It seemslogical to assume
that the more life experiences one has, the hardier onebecomes.
Perhaps the more pronounced hardiness becomes, the more di-rect
influence it has on health. For example, Schmied and Lawler
(1986)found that hardiness was associated with being older. Thus,
the relationshipof hardiness to health outcomes may be influenced
by age, with hardinesspredicting health outcomes among older but
not younger individuals.
Another interesting finding was the addition of the path from
avoidancecoping to symptoms of illness in the university sample.
This difference mayalso be attributed to the age differences
between the two samples. Accordingto the growth and maturity
hypothesis, older individuals may have a moreeffective and mature
repertoire of coping styles (Diehl et al., 1996; Labouvie-Vief et
al., 1987; McCrae, 1982). Therefore, the subjects in the
universitysample, being of a young age, may not have developed the
more effectivecoping styles characteristic of approach coping.
Several applications for intervention are implied by these
findings. Mostimportantly, the finding that the personality trait
of hardiness and copingstrategies impact the stressillness
relationship suggests that these are nec-essary components of an
effective intervention. Due to the negative im-pact of avoidance
coping, particularly in the university sample with the ad-ditional
path from avoidance coping to symptoms of illness,
interventionstargeted for college-aged populations should focus on
increasing aware-ness and understanding of the influence these
strategies have on health.Finally, interventions targeted at
corporate employees should reflect thestronger role hardiness has
in the stressillness relationship as illustrated by
-
7/27/2019 Hardiness and Coping Strategies.pdf
16/18
326 Soderstrom, Dolbier, Leiferman, and Steinhardt
the paths hardiness has to both perceived stress and symptoms of
illness in thissample.
The results of the study should be considered in light of
several limita-
tions. First, as with all survey data, self-report has inherent
limitations. Evenso, the instruments used were previously published
and possess adequatepsychometric properties. Second, the use of
convenient samples of corporateemployees and university students
limits the generalizability of the findings.Further research is
necessary using demographically diverse populations tostrengthen
the validity of the study findings. Finally, the design of the
study iscross-sectional, therefore causation cannot be determined
and the possibilitythat some third variable may be accounting for
some of the effects cannot bedismissed. The use of a longitudinal
design in future research would enable
examination of the effects of targeted interventions on
perceived stress andsymptoms of illness.
ACKNOWLEDGMENTS
We are grateful to 3M Wellness for allowing us to collect data
at 3M.Specific appreciation goes to Nancy Cherwitz, Health
Management Admin-
istrator, and Rebecca Ryan Swift, Health Management
Coordinator.
REFERENCES
Banks, J. K., and Gannon, L. R. (1988). The influence of
hardiness on the relationship betweenstressors and psychosomatic
symptomatology. Am. J. Commun. Psychol. 16: 2537.
Bartone, P. T., Ursano, R. J., Wright, K. M., and Ingraham, L.
H. (1989). The impact of a militaryair disaster on the health of
assistance workers: A prospective study. J. Nerv. Ment. Dis.177:
317328.
Billings, A. G., and Moos, R. H. (1981). The role of coping
responses and social resources inattenuating the stress of life
events. J. Behav. Med. 4: 139157.Blake, R. L., and Vandiver, T. A.
(1988). The association of health with stressful life changes,
social supports, and coping. Family Pract. Res. J. 7:
205218.Carver, C. S., Scheier, M. F., and Weintraub, J. K. (1989).
Assessing coping strategies: A theo-
retically based approach. J. Person. Soc. Psychol. 56:
267283.Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global
measure of perceived stress.
J. Health Soc. Behav. 24: 385396.Diehl, M., Coyle, N., and
Labouvie-Vief, G. (1996). Age and sex differences in strategies
of
coping and defense across the life span. Psychol. Aging 11:
127139.Dohrenwend, B. S., and Dohrenwend, B. P. (eds.) (1974).
Stressful Life Events: Their Nature and
Effects, Wiley, New York.
Dohrenwend, B. S., and Dohrenwend, B. P. (1981). Stressful Life
Events and Their Contexts,Neale Watson Academic, New York.Florian,
V., Mikulincer, M., and Taubman, O. (1995). Does hardiness
contribute to mental
health during a stressful real-life situation? The roles of
appraisal and coping. J. Person.Soc. Psychol. 68: 687695.
-
7/27/2019 Hardiness and Coping Strategies.pdf
17/18
Hardiness, Coping, Stress, and Illness 327
Folkman, S., and Lazarus, R. S. (1980). An analysis of coping in
a middle-aged communitysample. J. Health Soc. Behav. 21:
219239.
Fondacaro, M. R., and Moos, R. H. (1989). Life stressors and
coping: A longitudinal analysisamong depressed and nondepressed
adults. J. Commun. Psychol. 17: 330340.
Funk, S. C. (1992). Hardiness: A review of theory and research.
Health Psychol. 11: 335345.Ganellen, R. J., and Blaney, P. H.
(1984). Hardiness and social support as moderators of the
effects of life stress. J. Person. Soc. Psychol. 47:
156163.Gentry, W. D., and Kobasa, S. C. (1984). Social and
psychological resources mediating stress-
illness relationships in humans. In Gentry, W. D. (ed.),
Handbook of Behavioral Medicine,Guilford Press, New York.
Holahan, C. J., and Moos, R. H. (1985). Life stress and health:
Personality, coping, and familysupport in stress resistance. J.
Person. Soc. Psychol. 49: 739747.
Holahan, C. J., Moos, R. H., Holahan, C. K., and Brennan, P. L.
(1995). Social support, coping,and depressive symptoms in a
late-middle-aged sample of patients reporting cardiac
illness.Health Psychol. 14: 152163.
Holahan, C. J., Moos, R. H., Holahan, C. K., and Brennan, P. L.
(1997). Social context, copingstrategies, and depressive symptoms:
An expanded model with cardiac patients. J. Person.Soc. Psychol.
72: 918928.
Hull, J. G., Van Treuren, R. R., and Virnelli, S. (1987).
Hardiness and health: A critique andalternative approach. J.
Person. Soc. Psychol. 53: 168177.
Kobasa, S. C. (1979). Stressful life events, personality, and
health: An inquiry into hardiness.J. Person. Soc. Psychol. 37:
111.
Kobasa, S. C. (1982). Commitment and coping in stress resistance
among lawyers.J. Person. Soc.Psychol. 42: 707717.
Kobasa, S. C., and Maddi, S. R. (1977). Existential personality
theory. In Corsini, R. J. (ed.),Current Personality Theories,
Peacock, Itasca, IL.
Kobasa, S. C., and Puccetti, M. C. (1983). Personality and
social resources in stress resistance.J. Person. Soc. Psychol. 45:
839850.
Kobasa, S. C., Maddi, S. R., and Courington, S. (1981).
Personality and constitution as mediatorsin the stress-illness
relationship. J. Health Soc. Behav. 22: 368378.
Kobasa, S. C., Maddi, S. R., and Kahn, S. (1982a). Hardiness and
health: A prospective study.J. Person. Soc. Psychol. 42:
168177.
Kobasa, S. C., Maddi, S. R., and Puccetti, M. C. (1982b).
Personality and exercise as buffers inthe stress-illness
relationship. J. Behav. Med. 5: 391404.
Kobasa, S. C., Maddi, S. R., and Zola, M. A. (1983). Type A and
hardiness. J. Behav. Med. 6:4151.
Kobasa, S. C., Maddi, S. R., Puccetti, M. C., and Zola, M. A.
(1985). Effectiveness of hardiness,exercise, and social support as
resources against illness. J. Psychosom. Res. 29: 525533.
Kvam, S. H., and Lyons, J. S. (1991). Assessment of coping
strategies, social support, and general
health status in individuals with diabetes mellitus. Psychol.
Rep. 68: 623632.Labouvie-Vief, G., Hakim-Larson, J., and Hobart, C.
J. (1987). Age, ego level, and the life-spandevelopment of coping
and defense processes. Psychol. Aging 2: 286293.
Lazarus, R. S., and Folkman, S. (1984). Stress, Appraisal, and
Coping, Springer, New York.McCrae, R. R. (1982). Age differences in
the use of coping mechanisms.J. Gerontol. 37: 454460.Moos, R. H.,
Brennan, P. L., Fondacaro, M. R., and Moos, B. S. (1990). Approach
and avoidance
coping responses among older problem and nonproblem drinkers.
Psychol. Aging 5: 3140.Nowack, K. M., and Hanson, A. L. (1983). The
relationship between stress, job performance,
and burnout in college student resident assistants.J. College
Student Personnel24: 545550.Olff, M., Brosschot, J. F., and
Godaert, G. (1993). Coping styles and health. Person. Ind.
Diff.
15: 8190.Orr, E., and Westman, M. (1990). Does hardiness
moderate stress, and how?: A review. In
Rosenbaum, M. (ed.), Learned Resourcefulness: On Coping Skills,
Self-Control, and Adap-tive Behavior, Springer, New York.Pearlin,
L. I., and Schooler, C. (1978). The structure of coping. J. Health
Soc. Behav. 19: 221.Pollock, S. E. (1986). Human responses to
chronic illness: Physiological and psychosocial adap-
tation. Nurs. Res. 35: 9095.
-
7/27/2019 Hardiness and Coping Strategies.pdf
18/18
328 Soderstrom, Dolbier, Leiferman, and Steinhardt
Ptacek, J. T., Smith, R. E., and Zanas, J. (1992). Gender,
appraisal, and coping: A longitudinalanalysis. J. Person. 60:
747770.
Ptacek, J. T., Smith, R. E., and Dodge, K. L. (1994). Gender
differences in coping with stress:When stressor and appraisals do
not differ. Person. Soc. Psychol. Bull. 20: 421430.
Rabkin, J. G., and Struening, E. L. (1976). Life events, stress,
and illness. Science 194: 10131020.Rhodewalt, F., and
Agustsdottier, S. (1984). On the relationship of hardiness to the
type A
behavior pattern: Perception of life events versus coping with
life event. J. Res. Person. 18:212223.
Rhodewalt, F., and Zone, J. B. (1989). Appraisal of life change,
depression, and illness in hardyand nonhardy women. J. Person. Soc.
Psychol. 56: 8188.
Roth, S., and Cohen, L. J. (1986). Approach, avoidance, and
coping with stress. Am. Psychol.41: 813819.
Sapolsky, R. M. (1994). Why Zebras Dont Get Ulcers, W. H.
Freeman, New York.Schmied, L. A., and Lawler, K. A. (1986).
Hardiness, type A behavior, and the stress-illness
relation in working women. J. Person. Soc. Psychol. 51:
12181223.Schumacker, R. E., and Lomax, R. G. (1996). A Beginners
Guide to Structural Equation Mod-
eling, Lawrence Erlbaum Associates, Mahwah, N.J.Shepperd, J. A.,
and Kashani, J. H. (1991). The relationship of hardiness, gender,
and stress to
health outcomes in adolescents. J. Person. 59: 747768.Vitaliano,
P. P., Russo, J., Carr, J. E., Maiuro, R. D., and Becker, J.
(1985). The Ways of Coping
Checklist: Revision and psychometric properties. Multivar.
Behav. Res. 20: 326.Wiebe, D. J. (1991). Hardiness and stress
moderation: A test of proposed mechanisms.J. Person.
Soc. Psychol. 60: 8999.Wiebe, D. J., and McCallum, D. M. (1986).
Health practices and hardiness as mediators in the
stress-illness relationship. Health Psychol. 5: 425438.Williams,
P. G., Wiebe, D. J., and Smith, T. W. (1992). Coping processes as
mediators of the
relationship between hardiness and health. J. Behav. Med. 15:
237255.