Embed Size (px)
Citation preview

770
in the same solution, as are all non-absorbable suturematerials and implants before use.
3. Handbowls contain 1 in 10,000 chlorhexidine.4. Dressings are wrung out in 1 in 2000 chlorhexidine
before application to the wound. All changes of dressingare similarlv treated.
The above represents my own practice, but there are, nodoubt, other methods of applying antiseptics to surgicalwounds before closure. I believe that if those who are plaguedby postoperative sepsis were to adopt a similar policy of woundantisepsis, they would experience a dramatic vindication ofListerian principles.
It must be emphasised that the application of anti-biotic powders to wounds before closure is not adequateantisepsis. A powder cannot completely sterilise a woundand local antibiotic therapy may interfere with propersystemic treatment by inducing resistance.
Bridgend General Hospital,Quarella Road,
Bridgend, Glamorgan. A. W. FOWLER.
RESPIRATORY FUNCTION TESTS IN MINERS
SIR,-Dr. Catterall has now kindly supplied 1 theinformation I sought in my letter (Jan. 23).
All her 35 miners, except 3 concerning whom there were nodetails, were known to be smokers or ex-smokers. 23 were
smoking cigarettes at the time of the trial, only 2 consumingless than ten a day; 4 of the remainder were pipe-smokers, but3 of these had previously smoked 20-30 cigarettes daily; andthere were 5 men who had not smoked for two or more years.
Against this background, it is interesting to note thatFletcher said: "... it is probable that the dyspnoea and coughin those (with simple pneumoconiosis) who complain of it aredue chiefly to associated chronic bronchitis and emphysemarather than to the pneumoconiosis itself." One must hopetherefore that the detailed lung-function tests so wiselyrecommended by Dr. Catterall and Mr. Hunter (Jan. 16) willprove of value not only in assessing the extent of any respiratorydisability but also in evaluating the relative xtiological import-ance of industrial and addictive inhalations.
Phillips et al. have written that "... in studies of chronicrespiratory complaints of all types, unless the factor ofcigarette smoking is considered and comparisons are
drawn between smokers and non-smokers, the conclusionsdrawn may not be valid ". This essential clinical principleis peculiarly important in the assessment of obstructiveairway disease affecting cigarette-smoking miners whoclaim compensation for pneumoconiosis.Taunton Isolation and
Chest Hospital,Somerset. J. P. ANDERSON.
HÆMODIALYSIS IN
THE HÆMOLYTIC-URÆMIC SYNDROME
SIR,-We read with great interest the article by Dr.Moorhead and his colleagues (March 13) on the treatmentof acute renal failure in the Gasser syndrome. In 1964
we observed four patients with the haemolytic-uraemicsyndrome. Because of the severity of the syndrome inthree of these cases peritoneal dialysis was used.One of these, a girl aged 21’2 years, had diarrhoea for 7 days.
She became very pale and virtually anuric. She was admittedto the University Hospital on the 9th day of her illness. Purpuracould not be detected. There was no oedema. Blood-pressurewas 135 80 mm. Hg, erythrocyte-sedimentation rate 125 mm.in the first hour, haemoglobin 6.5 g. per 100 ml., reticulocytes82% of red cells, platelets 64,000 per c.mm. The blood-smear revealed anisocytosis, poikilocytosis, spherocytosis, andnumerous burr cells and triangular cells. Blood-chemistry was1. Catterall, M Personal communication,2. Fletcher, C. M. in The Practice of Medicine; p. 135. London, 1960.3. Phillips, A. M., Phillips, R. W., Thompson, J. L. Ann. intern. Med. 1956,
45, 216.
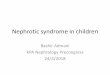
Urine production and blood-findings in patient with hxmolytic-uraemic syndrome treated by peritoneal dialysis.
as follows: potassium 6-4, sodium 126, and chloride 87 mEq.per litre; urea 340, creatinine 9-3, phosphate 9,2, and bilirubin2-5 mg. per 100 ml. Urine production was very low. Ureacontent of the urine was about 800 mg. per 100 ml. The urinecontained protein, red cells, and casts.The patient received 10% glucose solution intravenously, and
an anabolic steroid, ’ Orgabolin’, 2 mg. per day. Treatmentwith heparin, 4000 i.u. per day, was started.1 Blood-transfu-sions were given because of the low hxmoglobin concentration.The diarrhoea was very persistent and the faeces containedoccult blood. Feeding was very difficult and the girl vomitedseveral times a day. Urine production increased to 480 ml. perday, and urea concentration to 1100 mg. per 100 ml. (seeaccompanying figure).
Peritoneal dialysis was started on the 12th day. Blood valuessome hours before dialysis were: urea 360, creatinine 9-8, andphosphate 12.7 mg. per 100 ml.; pH 7.24; and standard bicar-bonate 12.2 mEq. per litre. Blood-potassium was rather low(5-2 mEq. per litre) after treatment with ’Resonium A’. The
peritoneal dialysis was easily performed, and was repeated fourtimes. Bacterial infection of the peritoneal cavity did not occur.Blood-urea decreased to 190 mg. per 100 ml., acidosis wascorrected, but phosphate remained high (9-1 mg. per 100 ml.).Despite this symptomatic treatment resulting in improvementof the blood-chemistry, the clinical condition deteriorated.Urine volume decreased to less than 100 ml. per day. The
patient developed severe intestinal haemorrhage and died onthe 21st day of illness.Two of the other patients with the Gasser syndrome (a girl
aged 21/2 years and a boy aged 2) were treated by peritonealdialysis which led to biochemical correction. Despite sympto-matic treatment they died on the 9th and 46th days after onsetof illness. The fourth patient, a 5-month-old boy, also hadrenal impairment though normal diuresis. He recoveredwithout dialysis.For the treatment of young children and infants with
1. Kunzer, W., Aalam, F. Lancet, 1964, i, 1106.

771
acute renal failure peritoneal dialysis is a safe and simplemethod, preferable to hasmodialysis. It can be performecfor 10-12 hours per day and if necessary repeated next dayThe danger of cerebral oedema with acute brain-sterr
compression from too rapid dialysis can be avoided. Th(
risks of bacterial contamination and biochemical dis-turbances are low. Accurate and repeated laborator)investigations during and after peritoneal dialysis arc
necessary. Despite this treatment the prognosis of thehaemolytic-urasmic syndrome remains grave.
Department of Pædiatrics,State University,
Groningen, The Netherlands.
J. A. TROELSTRAH. K. A. VISSER.
RETRACTOR FOR PROSTATECTOMY
SIR,-In 1962 I described a retractor for prostatectomy,3but it appears that I was not specific enough in describingthe method of its use.
The retractor is normally used with the arms angled, theangle varying according to the thickness of the anteriorabdominal wall. It is inserted over the symphysis pubis; andthe assistant, standing on the patient’s right side, can controlthe retractor quite easily with his right hand. A slight down-ward pressure on the retractor, which normally opens to
about two inches in the prostatic bed, will expose the wholeof the cavity.
Civil Hospital,Omdurman,
Sudan. H. H. BARST.
REACTION TO CHLORHEXIDINE AND
CETRIMIDE
SIR,-As Dr. Birdwood writes (March 20), " severereactions to savlon have not previously been reported ",and in view of the frequency with which chlorhexidineand cetrimide are used they must be regarded as amongthe safest of agents applied to the skin, which from timeto time will react to almost anything.On the evidence presented I do not think that he is
justified in attributing the reaction to chlorhexidine. Ihave personal experience of four patients showingextreme sensitivity to cetrimide itself.The first reacted alarmingly to a proprietary shampoo con-
taining cetrimide, and, 2 years later, to cetrimide applied to acut. The next two patients developed eruptions after pre-operative skin preparation, one of them on two separate occa-sions in the same hospital. The fourth was a small boy seenonly last week who was given 1 %,aqueous solution of cetrimidefor the cleansing of a mild balanitis. This was followed by analarming bullous eruption, with shedding of the whole of theskin of the penis and scrotum, and severe dermatitis spreadingto the thighs and abdomen.The condition of two of these patients, especially the last,
was so severe as to require systemic corticosteroid therapy.The first three patients were investigated by patch-testing.
Patch-tests with cetrimide may be difficult to interpret, becauseat dilutions of about 1 % primary irritant reactions are seen innormal persons. All these patients reacted strongly or violentlyto 0-1% and two to 0.01 % and 0-001%, while the third gave adetectable reaction to a dilution of one in a million-thisreaction was at first attributed to maceration, but it was positivewhen repeated, controls using water and saline being negative.For a variety of reasons these rare but alarming re-
actions are of great dermatological interest, but fortun-ately they are so rare that they do not seriously limit theusefulness of cetrimide. On the other hand, I have riot
encountered, or at least have not recognised, reactions tochlorhexidine.
DENIS SHARVILL.2. Segar, W. E., Gibson, R. K., Rhamy, R. Pediatrics, 1961, 27, 603.3. Lancet, 1962, ii, 1150.
SEVERITY OF RESPIRATORY FAILURE
SIR,-Of course we agree with Dr. Palmer (March 6)" that it cannot be assumed when the alveolar ventilationis halved that dangerous hypoxia will not occur ".We are distressed to think that anything in our paper could
be taken to imply the opposite. And, of course, the alveolar-arterial Po, difference is usually greater than 15 mm. Hg-thefindings reported in fig. 1 and table n of our paper (Feb. 13)show that it is usually over 30 mm. Hg and may be greaterthan 50. But we were attempting to predict the highest toler-able Pc02, and the rules of this sort of game required us toassume the smallest likely alveolar-arterial difference.
Dr. Simpson (March 6) tries to draw us beyond thelimited field of our paper.We reluctantly cannot agree with his proffered rephrasing of
our remarks about oxygen therapy because it begs certain
important questions. He may be right that " there is no bar togiving pure oxygen so long as the mental state remains.clear ",just as there may be no bar to overtaking on a blind corner solong as nothing is coming the other way. A skilful physicianpaying close attention can get out of difficulty if the patientsubsides into coma, but he may have to use dramatic measures
-just as a skilful driver can get out of trouble if he meets anoncoming car. But we believe there is no need to take theserisks.
Central Middlesex Hospital,London, N.W.10. M. W. MCNICOL.
Postgraduate Medical School of London,London, W.12. E. J. M. CAMPBELL.
ANTIBODY-LIKE ACTIVITY IN DIABETIC AND
NORMAL SERUM
SIR,-My colleagues and I pointed out 1 that the
findings by Pav et aI.,2 of positive complement consump-tion in the sera of 33% of diabetic and 4% of non-dia-betic subjects when insulin was added, raised implicationsof considerable importance in the setiology of diabetes.
If the complement-consumption technique provides a reli-able index of complement fixation by antigen-antibody com-plexes, then these observations may be interpreted as indicatingthe formation of autoantibodies against insulin in non-diabeticindividuals as well as in some diabetic subjects who have neverreceived exogenous insulin therapy. Certain of our own obser-vations dealing with the binding in the tissues of fluorescein-conjugated insulin were cited as supporting the formation ofautoantibodies against insulin in diabetic individuals who havenever received insulin therapy.
Recently Dr. Chetty and Dr. Watson (Jan. 9) haverepeated the studies of Pav et al. with some minor modi-fications in technique, and have obtained even higherproportions of positive complement consumption indiabetic subjects who have never received exogenousinsulin, and in non-diabetic individuals. They draw twoconclusions, however, with which we would take issue.
1. They cite several studies showing non-immune bindingof insulin to various serum-proteins including i:J-globulins; -,Yagi et all 4 have shown that certain ,3-globulins of insulin-immunised animals may indeed be immune globulins. Ofeven greater importance is the assumption by Dr. Chetty andDr. Watson that non-immune insulin protein complexes maybind complement. This is at variance with a very basic tenetof immunology, and, if true, would invalidate all immuno-
logical procedures based on complement fixation.2. They fail to find any definite correlation between the age
of onset of diabetes and positive complement consumption,and suggest that there may thus be no relation between theoccurrence of autoantibody against insulin and the age-related1. Blumenthal, H. T., Berns, A. W., Owens, C T, Lancet, 1963, ii, 7832. Páv, J., Ježková, Z., &Sbreve;krha, F. ibid. 1963, ii, 221.3. Yagi, Y.. Maier, P., Pressman, D. J. Immunol. 1962, 89, 442.4. Yagi, Y, Maier, P., Pressman, D., Arbesman, C. C., Reisman, R. E.,
Lenzner, A. R. ibid. 1963, 90, 760.