Embed Size (px)
DESCRIPTION
Haemolytic Anaemia. Elliot Catchpole PCMD. Recap. Mean Cell Volume = The size of each RBC. MACROCYTIC >96. Normocytic 76-96. Microcytic
Citation preview

Haemolytic Anaemia
Elliot CatchpolePCMD

Recap• Mean Cell Volume = The size of each RBC
Microcytic<76
Normocytic76-96
MACROCYTIC>96
-IRON deficiency
-Thalassaemias
-Sideroblastic
Chronic Disease
Haemolysis
B12 and
Folate
-Alcohol-Liver Disease-MYLODYSPLASIA
Megaloblastic
Non-Megaloblastic
-G6PD Deficiency-Hereditary spherocytosis-Paroxysmal Nocturnal Haemoglobinurea-Autoimmune Haemolysis-Sickle Cell

• What is haemolysis?

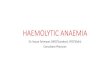
Haemoglobin Cycle
Haem
Iron
Bilirubin
Blood
ALBUMIN
BilirubinHaem
SPLEEN
LIVER
‘Unconjugated/indirect’
(destruction)
Bilirubin
‘Conjugated/direct’
CONJUGATION!!!Water solubility
K
Bilirubin
GIUrobilinogen

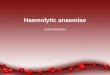
Haemolysis
HaemolysisMCV =
Normal/raised
Generally ACUTE
Indirect Bilirubin
Haptoglobin
(Intravascular)
LDH
Reticulocyte
•?Dark urine?•?Jaundice?•Gallstone risk

Sickle Cell• CAUSES: SCD = homozygote, Trait = heterozygote
• *PRESENTATION* - Trait = only haematuria in normal circumstancesSCD = PAIN Parvovirus B19 = HCT drops precipitously
• INVESTIGATIONS – Blood smear – best initialShows Sickled cells for SCD, nothing for trait - Hb electrophoresis
• TREATMENT – Pain = Supportive (O2, fluids, pain meds) Fever/infection = above + antibiotics Parvovirus = Transfusion/Ig for virus CNS = give exchange transfusion Prophylaxis = Folate + Hydroxyurea
• COMPLICATIONS - GallstonesOcclusion problems = leg ulcers, osteomyelitis, CNS complications (stroke, visual disturbance)
Intravascular

Autoimmune Haemolysis
• CAUSES: Autoimmune – PHx of autoimmune conditions, medications (penicillin, quinidine)
• *PRESENTATION*Warm = chronic haemolysis (extravascular)Cold = in the cold (<4*) (intravascular)
• INVESTIGATIONS – COOMBS TEST based on the 2 risks (autoimmune Hx and medications)
• TREATMENT – Steroids stop Recurs? More steroids stop Constant recurrence? SPLENECTOMY
Either

Hereditary Spherocytosis
• CAUSES: Autosomal dominant RBC membrane defect.
• *PRESENTATION* - Young – extravascular – splenomegaly, jaundice
• INVESTIGATIONS – Osmotic fragility test – cells will burst
• TREATMENT – Splenectomy
Extravascular

PNH (Paroxysmal Nocturnal Haemoglobinurea)
• CAUSE: Genetic defect in creating DAF/CD55 • *PRESENTATION* - Dark urine IN MORNING
(haemolysis at night)• INVESTIGATIONS – Test for DAF/CD55• TREATMENT + Steroids
+ Anticoagulation (prevent thrombosis)
+ SCT (stem cell transplant, curative)
• COMPLICATIONS – Large vessel thrombosis (so give anticoagulants) - Associated with Leukaemia and Aplastic Anaemia
Intra.

G6PD deficiency
• CAUSES: X-linked recessive – defective G6PD enzyme
• *PRESENTATION* - Oxidising crisis (jaundice + anaemia) on oxidising stressors (e.g. Henna, infection)
• INVESTIGATIONS – G6PD levels >8weeks ‘Heinz Body’ smear Exclude other causes
• TREATMENT – Avoid stressors
Intravascular

Questions
• A patient comes to the ED with sudden onset of fatigue and SOB. The HCT is 20 and the MCV is slightly elevated. The reticulocyte count, LDH, and indirect bilirubin are all elevated, with a low haptoglobin.1) History SLE and Lymphoma2) Recurrent episodes with a large spleen, with a European family history 3) Sudden onset of haemolysis in a male with acute infection. A similar reaction occurs when certain medications are used.

Questions
• An African American man comes into the ED with back, chest and thigh pain. He has a history of sickle-cell disease. He has a temperature of 38.5C. CXR and urinalysis are normal. Oxygen, fluids and analgesics are started. His HCT is 28.
1) What is the most urgent step at this time?2) How would you confirm a Parvovirus infection?3) How would you treat this?