Embed Size (px)
Citation preview

Annals of the Rheumatic Diseases, 1988; 47, 957-960
Case report
Ischaemic necrosis of the ilium complicatinghaemolytic anaemia due to an unstable haemoglobinN W McGILL, P WARBURTON, H KRONENBERG, J E HASSALL, ANDM A ROSSLEIGH
From the Royal Prince Alfred Hospital, Camperdown, Australia
SUMMARY A case of ischaemic necrosis of bone (INB) affecting the right hemipelvis in a 57 yearold woman with an unstable haemoglobinopathy is presented. The rarity of INB in this site, theusefulness of nuclear scanning, and the relation between haemolytic anaemia and INB arediscussed.
Key words: avascular necrosis, aseptic necrosis, osteonecrosis, haemoglobinopathy.
In adults ischaemic necrosis of bone most commonly,affects the epiphyseal (especially the femoral andhumeral heads) and metadiaphyseal marrow cavitiesof long tubular bones. Occasionally, the small roundbones of the wrist and ankle are affected. Involve-ment of large flat bones such as the ilium is rare andto our knowledge has only previouslr been de-scribed complicating sickling diseases, Gaucher'sdisease,2 and in two patients who received largedoses of corticosteroids in the course of renaltransplantation.3We report a case of ischaemic necrosis affecting
most of the right hemipelvis in a 57 year old womanwith haemolytic anaemia due to an unstablehaemoglobin. Despite a lifelong history of haemoly-sis there was no evidence of previous episodes ofischaemic necrosis, nor did she have a sicklingdisorder.
Case report
A 57 year old woman presented in January 1987with severe pain in the region of the right hip. Shewas diagnosed as having an unstable haemoglobin-opathy at the age of 19 years when noted to beanaemic during her first pregnancy. Over the next30 years she received only occasional blood transfu-
Accepted for publication 21 March 1988.Correspondence to Dr N W McGill, Rheumatology Unit, BristolRoyal Infirmary, Bristol BS2 8HW, UK.
sions but for the eight years before this presentationreceived transfusions of four or five units of packedcells approximately every six weeks. Her unstablehaemoglobin was characterised by the presence ofsmall numbers of Heinz bodies and numerous otherinclusion bodies which have been shown to containhaemoglobin. Attempts in the early 1970s to analyseher haemoglobin using various forms of haemoglo-bin electrophoresis and peptide analysis (fingerprinting) were unsuccessful owing to the instabilityof her haemoglobin. Further attempts to charac-terise the haemoglobin, including amino acidsequencing, are currently being undertaken.As a consequence of her chronic haemolysis she
had a cholecystectomy for pigment stones in 1969and a splenectomy for abdominal discomfort due tomassive splenomegaly in 1973. She had noted in-creasing skin pigmentation for the five years beforepresentation.
Since 1975 she had suffered from a non-deformingpolyarthritis which affected her hands, wrists,ankles, and shoulders. She had mild intermittentjoint swelling and prominent early morning stiff-ness. Rheumatoid factor was negative and x rays ofher joints were normal. Although she was initiallythought to have seronegative rheumatoid arthritis,the subsequent course of her arthritis was more inkeeping with the arthropathy of iron overload whichshe was recorded to have. In 1985 she developedtransient pain in the region of the right hip. A bone
957
copyright. on O
ctober 11, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.47.11.957 on 1 N
ovember 1988. D
ownloaded from

958 McGill, Warburton, Kronenberg, Hassall, Rossleigh
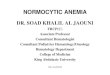
scan was normal (Fig. 1), and no further investiga-tion was considered necessary. In 1986 she sufferedan osteoporotic crush fracture of Ti1.She also had a number of intercurrent illnesses
Fig. 1 Technetium-99m methylene diphosphonate bonescan: normal; November 1985.
including peptic ulceration, hypertension, ischaemicheart disease, and aortic incompetence.She was a non-smoker, drank minimal alcohol,
and took isorbide nitrate, nifedipine, pindolol,ranitidine, folic acid, indomethacin, paracetamol-dextropropoxyphene, and temazepam. She hadnever taken corticosteroids.
In January 1987 she developed over a few hourssevere pain in the region of her right hip, whichprevented her from walking and required largeamounts of narcotic analgesia to achieve adequatepain relief even while lying in bed.On examination she was distressed by pain and
had a low grade fever to 37-8°C, which persisted forfive days. Her right iliac crest was exquisitelytender, but movements of the right hip were onlymoderately restricted by pain. Her bones and jointswere otherwise normal. Neurological examinationwas difficult because of her pain and subsequentsedation but was felt to be normal apart from a smallarea of longstanding hypoaesthesia on the lateralaspect of her right thigh. She had slate greypigmentation, a liver edge palpable 3 cm below thecostal margin, and signs consistent with moderateaortic incompetence.
Investigations at that time were haemoglobin 90g/l, white cells 17*2x109/1, platelets 181x107/1. Liverfunction tests had been and remained chronically
9,; .i
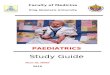
Fig. 2a Fig. 2b
Fig. 2 (a) Technetium-99m methylene diphosphonate bone scan: reduced tracer uptake in the right ilium, most marked inthe iliac crest and extending into the acetabulum; January 1987. (b) Technetium-99m sulphur colloid bone marrow scan:absent bone marrow uptake throughout most ofthe right hemipelvis; January 1987.
copyright. on O
ctober 11, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.47.11.957 on 1 N
ovember 1988. D
ownloaded from

Ischaemic necrosis of the ilium 959
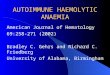
Fig. 3a Fig. 3b
Fig. 3 (a) Technetium-99m methylene diphosphonate bone scan: persistence ofreduced tracer uptake in the right ilium,only marginally less marked than in January 1987 (Fig. 2); March 1987. (b) Technetium-99m sulphur colloid bone marrowscan: persistent absence ofbone marrow uptake throughout most ofthe right hemipelvis, unchangedfrom January 1987(Fig. 2); March 1987.
abnormal (alkaline phosphatase 179 U/1, aspartateaminotransferase 76 U/i, alanine aminotransferase83 U/i, y-glutamyltransferase 46 U/i), but thebiochemical screen was otherwise normal. An x rayof the pelvis showed some generalised loss of bonedensity but was otherwise normal. A 99mTcmethylene diphosphonate bone scan showedreduced tracer uptake in the right ilium, mostmarked in the iliac crest and extending into theacetabulum (Fi. 2a). In view of the bone scanappearance a mTc sulphur colloid bone marrowscan was performed and showed absent bonemarrow uptake throughout most of the righthemipelvis-the abnormality being more extensivethan that present on the bone scan (Fig. 2b). Thecombined studies strongly sdpported the diagnosisof bone infarction. A computed tomographic scan ofthe abdomen and pelvis showed replacement of thenormal fatty marrow in the femoral head consistentwith increased haemopoiesis, and increased liverdensity consistent with iron overload, but no mass orbony erosion.The patient was treated with rest and analgesia
and improved rapidly, being able to walk again 11days after the onset of pain. Unfortunately, trouble-some low grade right pelvic pain persists eightmonths after onset.
Repeat bone and bone marrow scans performedafter two months showed little change (Figs 3a andb) and pelvic x ray after seven months was un-changed. A trephine biopsy of the right iliumconfirmed the presence of osteonecrosis (Fig. 4).
Fig. 4 Trephine biopsy ofthe right ilium. Absentosteocyte nuclei indicate necrotic bone trabeculi. Themarrow spaces revealed numerous siderophages,sparse haemopoietic cells, and afewfibroblastic cells.(Haematoxylin and eosin.)
copyright. on O
ctober 11, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.47.11.957 on 1 N
ovember 1988. D
ownloaded from

960 McGill, Warburton, Kronenberg, Hassall, Rossleigh
Discussion
We have presented a case of ischaemic necrosis ofbone (INB) occurring in an unusual site in a patientwith an unstable haemoglobinopathy.INB has been reported in association with a
number of conditions (traumatic disruption of theblood supply, sickle cell disease and other sicklingdisorders, corticosteroid treatment, Cushing'sdisease, irradiation, alcoholism, Gaucher's disease,caisson disease, haemophilia, rheumatoid arthritis,systemic lupus erythematosus, and pancreatitis) butnot to our knowledge with non-sicklinghaemoglobinopathies.4
Ischaemic necrosis of the ilium is rare but hasbeen re orted in sickle cell disease,' Gaucher'sdisease,1'and after large doses of corticosteroids forrenal transplantation.3 In sickle cell diseaseischaemia is thought to result from sludging ofsickled red cells in small vessels and vascularsinusoids,4 and in Gaucher's disease ischaemia maybe due to compression of vessels as a result ofincreased intraosseous pressure resulting frominfiltrating Gaucher cells. The blood supply of theilium comes via the iliac branches of the obturatorand iliolumbar arteries (branches of the internaliliac), which anastomose with each other and withbranches of the superior gluteal artery (branch ofthe external iliac) to give off numerous small vesselswhich supply the bones of the pelvis.5 6As occlusionof a major vessel could not account for ischaemicnecrosis of the bones of the pelvis without also pro-
ducing visceral ischaemia it is not plausible that ourpatient's illness resulted from such an occlusion.Our patient does not have a sickling disorder nor
any of the other diseases associated with INBmentioned above. Although our patient's bonemarrow was hyperplastic, INB is not associated withother non-sickling haemolytic anaemias with similardegrees of marrow hyperplasia, and thus the rela-tion between our patient's unstable haemoglobino-pathy and the occurrence of INB remains unclear.
This report describes INB occurring in an unusualsite and demonstrates the value of bone and bonemarrow scanning in patients with undiagnosed acutesevere musculoskeletal pain and normal x rays.
We would like to thank Dr S McCarthy for his help andhistopathological expertise.
References
1 Diggs L W. Bone and joint lesions in sickle-cell disease. ClinOrthop 1967; 52: 119-43.
2 Davidson A, Kalff V, Ryan P F J. Bone crisis of Gaucher'sdisease due to bone ischemia: a case report. Arthritis Rheum1985; 28: 218-21.
3 Spencer J D, Maisey M N. The incidence of avascular necrosisof bone following renal transplantation using radionuclidc boncscanning. In: Arlet J, Ficat R P, Hungerford D S, eds. Bonecirculation. Baltimore/London: Williams and Wilkins, 1984:259-64.
4 Middlemiss H. Aseptic necrosis and other changcs occurring inbone in the hcmoglobinopathies. In: Davidson J K, ed. Asepticnecrosis of bone. Amsterdam: Excerpta Medica, 1976: 271-300.
5 Williams P L, Warwick R (eds). Gray's anatomy. 36th cd.Edinburgh: Churchill Livingstone, 1980: 719-25.
6 Brookes M. The blood supply of bone. An approach to bonebiology. London: Butterworth, 1971: 65-6.
copyright. on O
ctober 11, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.47.11.957 on 1 N
ovember 1988. D
ownloaded from