Embed Size (px)
Citation preview
Haematology
Learning objectives
• Blood and its composition• Hematopoiesis• Erythrocyte, Leukocyte and Platelet Physiology• Hemostasis• Blood types• Transfusion and compatibility testing
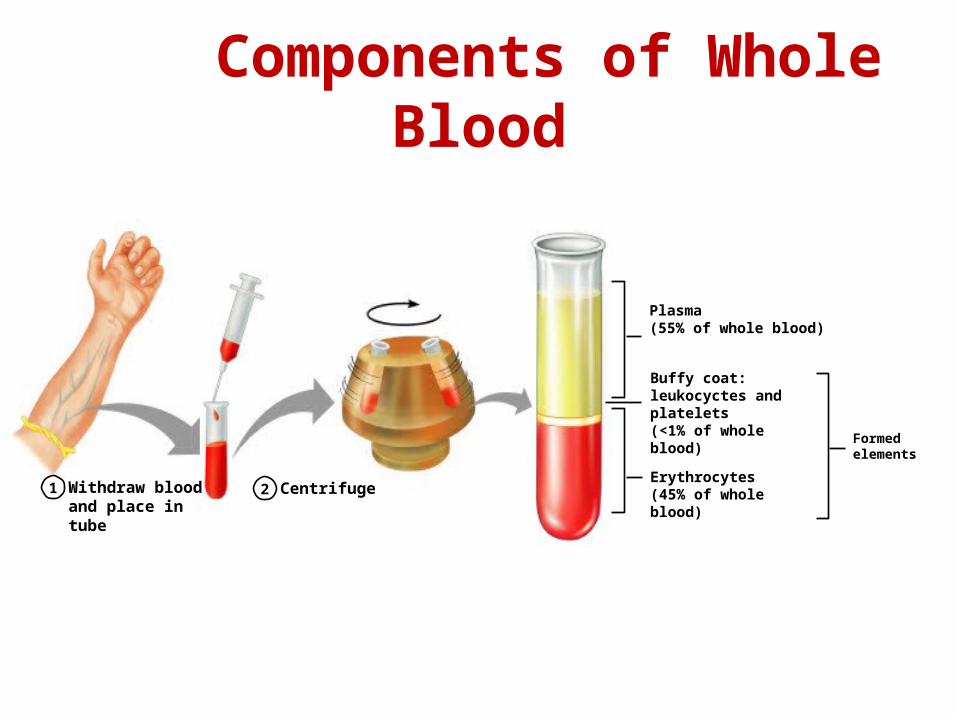
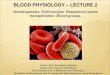
Components of Whole Blood
Withdraw blood and place in tube
1 2 Centrifuge
Plasma(55% of whole blood)
Formed elements
Buffy coat:leukocyctes and platelets(<1% of whole blood)
Erythrocytes(45% of whole blood)
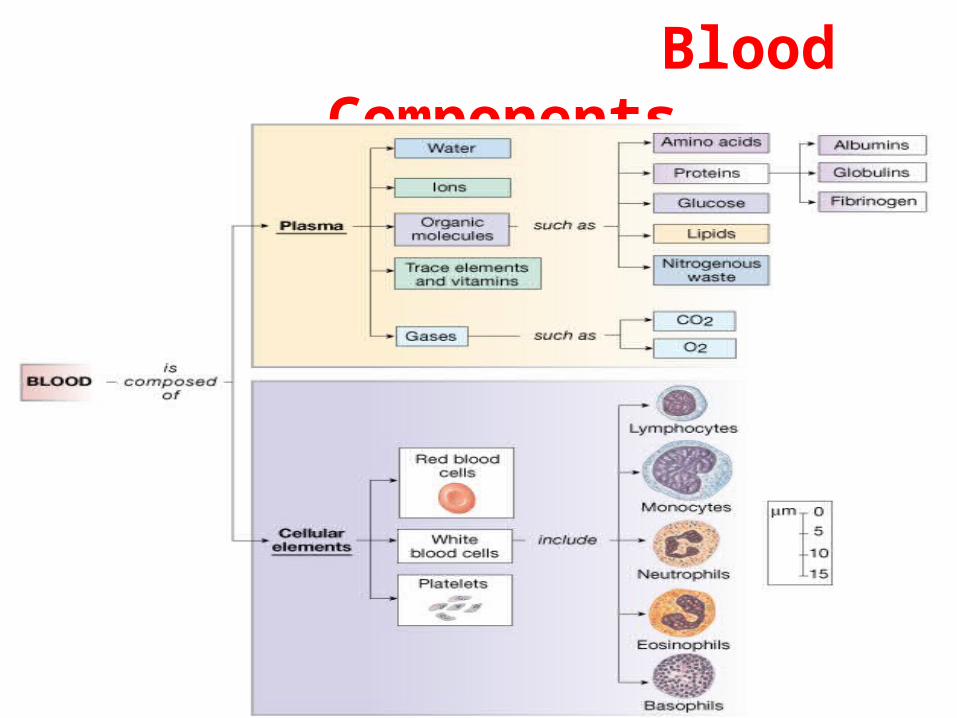
Blood Components
Figure 16-1: Composition of blood
5
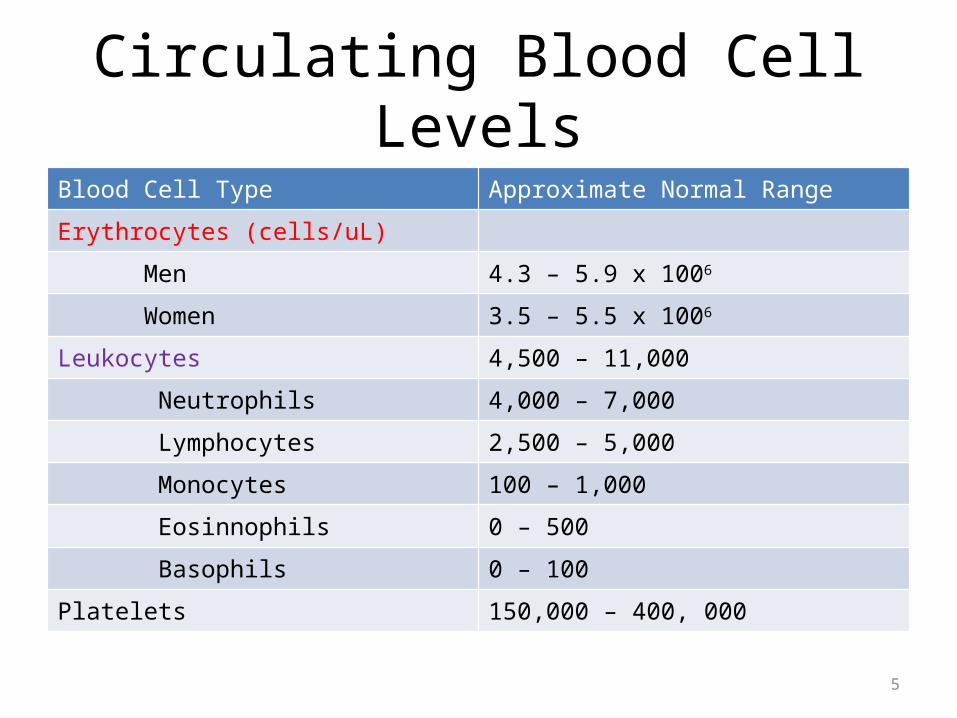
Circulating Blood Cell LevelsBlood Cell Type Approximate Normal Range
Erythrocytes (cells/uL)
Men 4.3 – 5.9 x 1006
Women 3.5 – 5.5 x 1006
Leukocytes 4,500 – 11,000
Neutrophils 4,000 – 7,000
Lymphocytes 2,500 – 5,000
Monocytes 100 – 1,000
Eosinnophils 0 – 500
Basophils 0 – 100
Platelets 150,000 – 400, 000
Blood Plasmacomponents:
1. Water = 90-92%2. Proteins = 6-8%
• Albumins; maintain osmotic pressure of the blood• Globulins
• Alpha and beta globulins are used for transport purposes• Gamma globulins are the immunoglobulins (IgG, IgA, etc)
• Fibrinogen; a clotting protein3. Organic nutrients – glucose, carbohydrates,
amino acids4. Electrolytes 5. Nonprotein nitrogenous substances – lactic
acid, urea, creatinine6. Respiratory gases
7
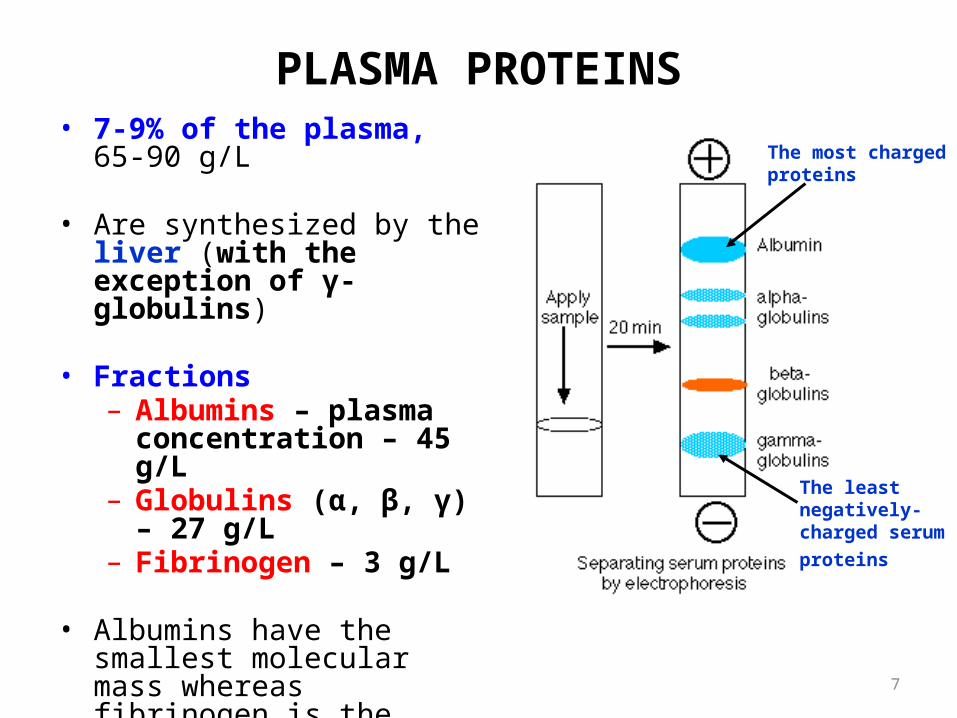
PLASMA PROTEINS• 7-9% of the plasma, 65-90 g/L
• Are synthesized by the liver (with the exception of γ-globulins)
• Fractions– Albumins – plasma
concentration – 45 g/L– Globulins (α, β, γ) – 27 g/L– Fibrinogen – 3 g/L
• Albumins have the smallest molecular mass whereas fibrinogen is the largest
The least negatively-charged serum proteins
The most charged proteins
8
GENERAL FUNCTIONS OF PLASMA PROTEINS
• Create colloid osmotic pressure (25 mmHg) → retaining water within the capillaries
• Binding and transport of hormones, enzymes, lipids, vitamins, metals, bilirubin, drugs, etc.
• Contribution to the blood viscosity
• Buffer properties – capability of accepting both H+ and base ions
• Protection of body against microorganisms and toxic substances
• Mediate blood coagulation
• Precursors of some hormones (angiotensinogen, erythropoietin)
• Protein reserve – source of AA for tissues in case of starvation
9
PROPERTIES & FUNCTIONS OF VARIOUS FRACTIONS OF PLASMA PROTEINS
• Albumins– 60% of the total plasma protein– High concentration and small size → 80% of the total colloid osmotic
P of the plasma
• 1 globulins (glycoproteins)– Transport of glucose and lipids– Include anti-protease
• 2 globulins– Carriers for different substances (high affinity, low binding capacity)
• Ceruloplasmin – copper• Thyroxin-binding protein• Transcobalamin – Vit B12• Bilirubin binding globulin• Transcortin – cortisol, etc.
10
PROPERTIES & FUNCTIONS OF VARIOUS FRACTIONS OF PLASMA PROTEINS (cont.)
• -globulins– Carriers for lipids (lipoproteins), polysaccharides and metals (i.e.,
transferrin – iron and cupper)
• -globulins– Are immunoglobulins (antibodies)– Quantity and composition fluctuate
• ↑ in almost all diseases (inflammation and infections)
• Fibrinogen– A dissolved precursor of fibrin – blood clotting– Serum – plasma without fibrinogen (and clotting factors)
11
HYPOPROTEINEMIA• ↓ blood level of proteins
• Results from – Malnutrition– Liver diseases (depression of protein synthesis)– Intestinal disease (malabsorption)– Kidney diseases (lost of albumins in urine)
• Results in – ↓ plasma oncotic pressure (especially due to ↓ albumin
concentration) and edema formation– Depression of specific functions (i.e., ↓ in globulins – ↓ resistance to
infections, ↓ in fibrinogen – defective blood clotting)
Formed Elements
• Formed elements comprise 45% of blood• Erythrocytes, leukocytes, and platelets make
up the formed elements– Only WBCs are complete cells– RBCs have no nuclei or organelles, and platelets
are just cell fragments
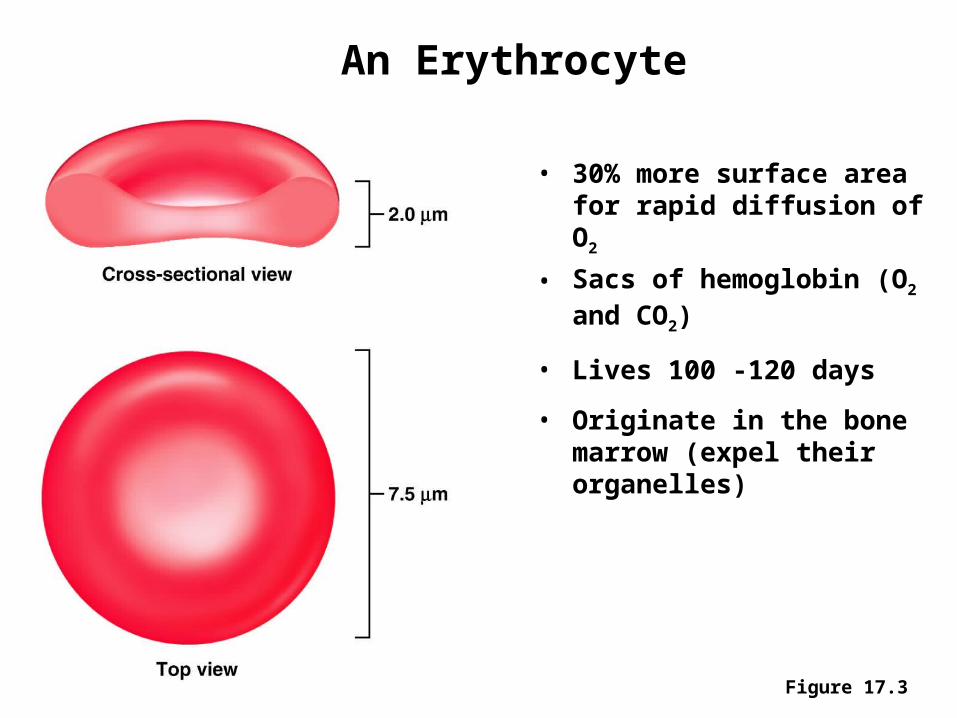
An Erythrocyte
• 30% more surface area for rapid diffusion of O2
• Sacs of hemoglobin (O2 and CO2)
• Lives 100 -120 days
• Originate in the bone marrow (expel their organelles)
Figure 17.3
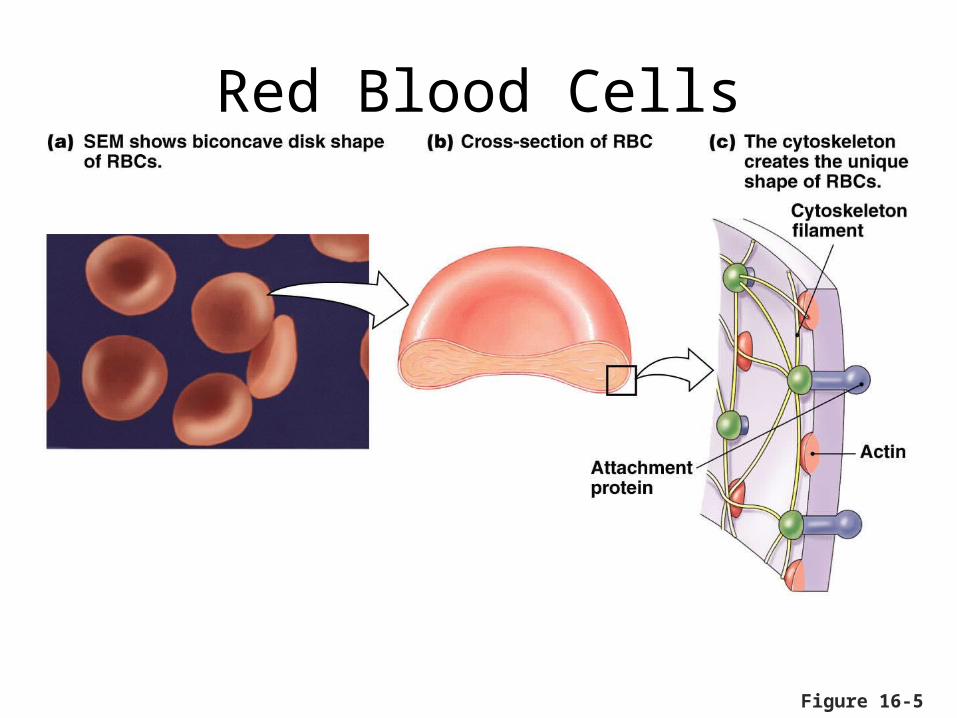
Figure 16-5
Red Blood Cells
16
RBC COUNT
• Normal values– Adult males: 4 600 000 – 6 200 000/mm3 (5.4million/mL)– Adult females: 4 200 000 – 5 400 000/mm3 (4.8million/mL)
• Abnormally high count – polycythemia
• Abnormally low count – anemia
17
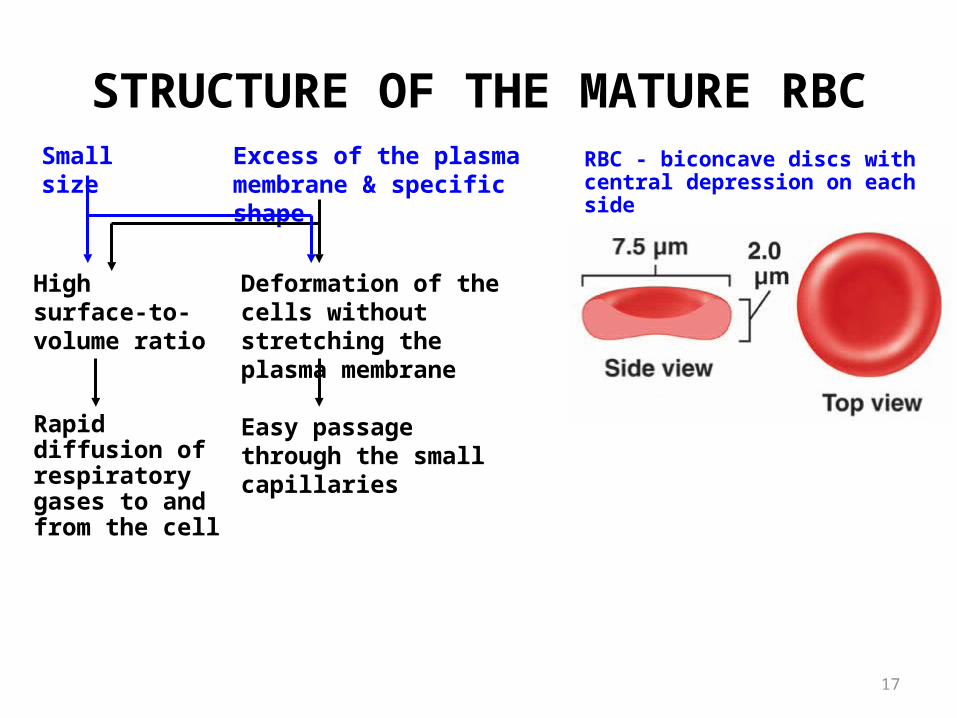
STRUCTURE OF THE MATURE RBC RBC - biconcave discs with central
depression on each sideSmall size Excess of the plasma membrane
& specific shape
High surface-to-volume ratio
Rapid diffusion of respiratory gases to and from the cell
Deformation of the cells without stretching the plasma membrane
Easy passage through the small capillaries
18
STRUCTURE OF THE MATURE RBC (cont.)
• Membrane contains special proteins and polysaccharides that differ from person to person – blood groups
• Lack of the nucleus and organelles– Cannot undergo mitosis– Generate ATP anaerobically → do not use oxygen they transport– Can not synthesize new cellular components to replace damaged ones
Life span - 120 days
• Contain a red pigment, hemoglobin (red color of the blood) – Occupies 1/3 of cellular volume– 280 million Hb molecules/RBC
19
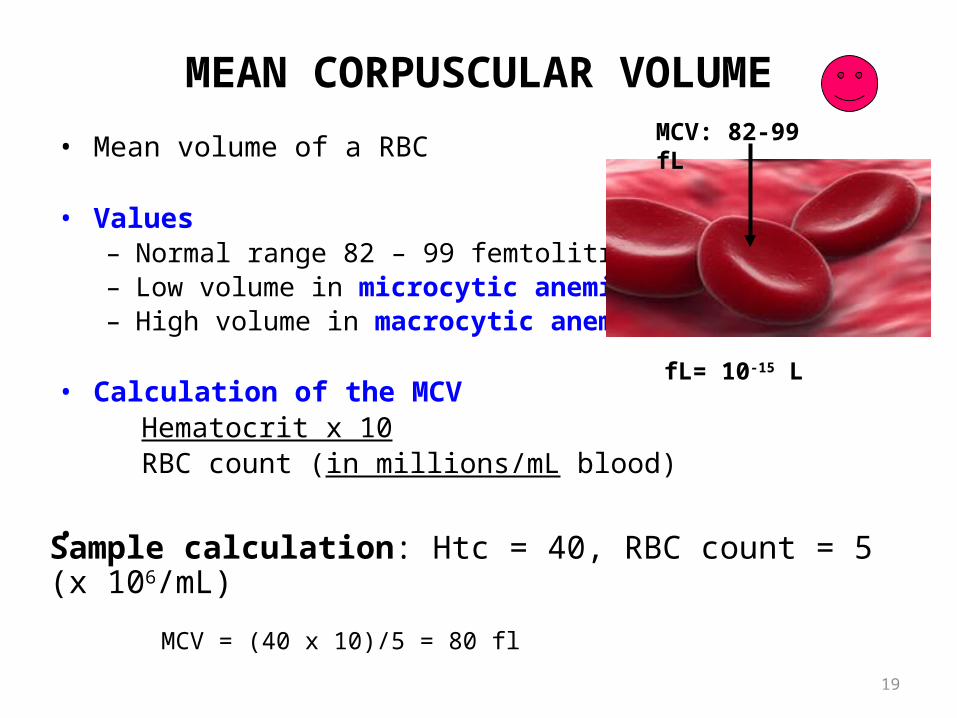
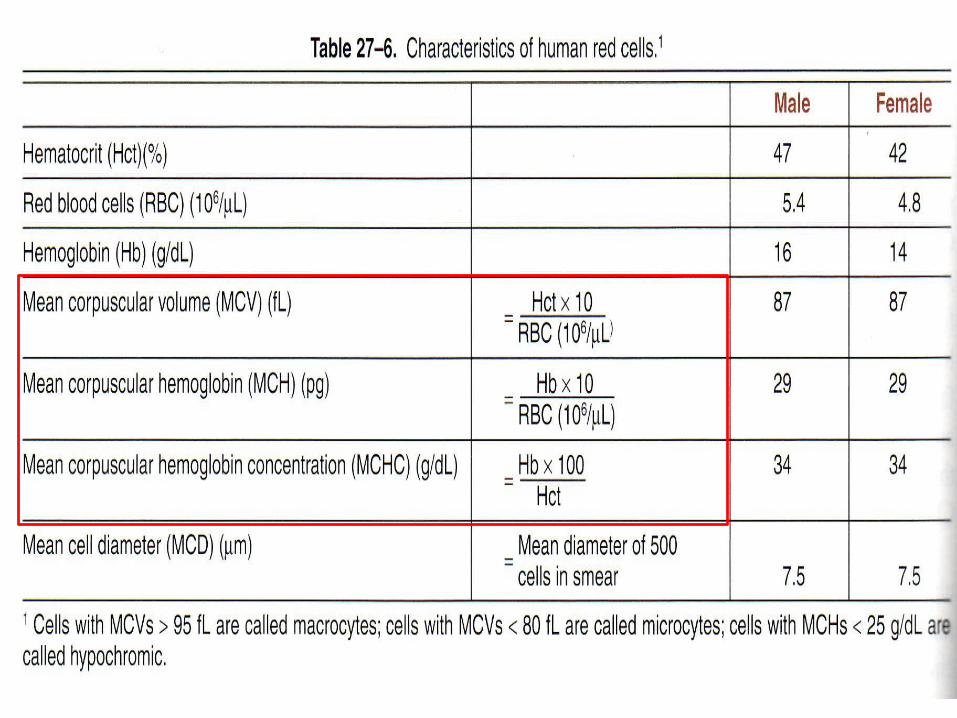
MEAN CORPUSCULAR VOLUME
• Mean volume of a RBC
• Values– Normal range 82 – 99 femtolitre (fL)– Low volume in microcytic anemia– High volume in macrocytic anemia
• Calculation of the MCVHematocrit x 10RBC count (in millions/mL blood)
•
MCV: 82-99 fL
fL= 10-15 L
Sample calculation: Htc = 40, RBC count = 5 (x 106/mL)
MCV = (40 x 10)/5 = 80 fl
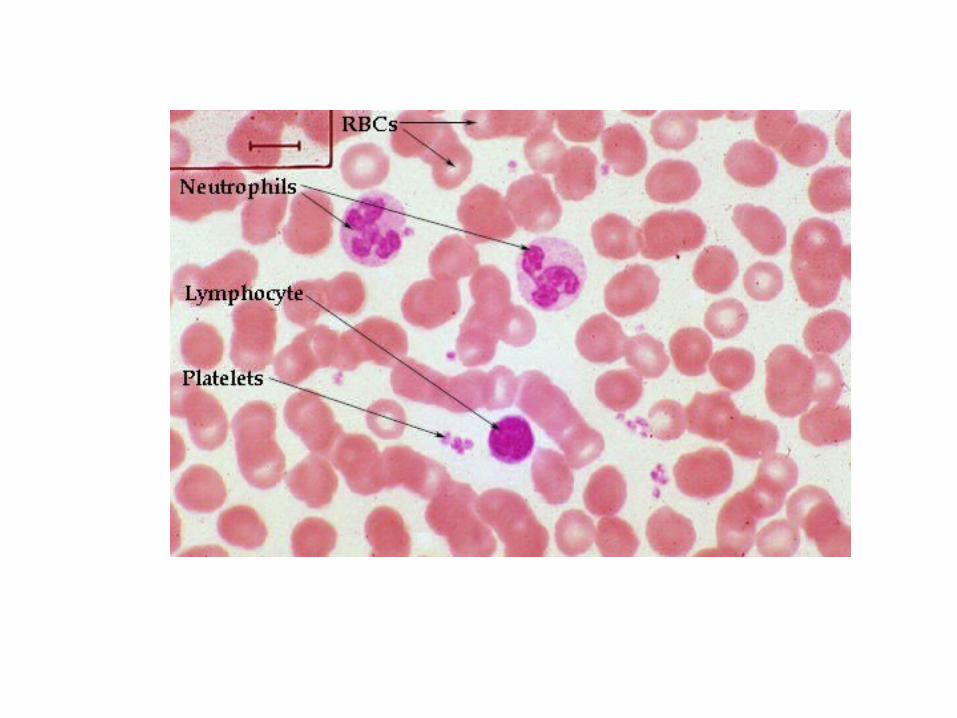
Erythrocytes (RBC’s) Small, oxygen-transporting cells, biconcave disc– 7.5 m in diameter
(capillary diameter 8 – 10 m) Have no organelles or nuclei- anucleate, no centrioles, no
organellesEnd result - no cell division No mitochondria means they generate ATP anaerobically.
Prevents consumption of O2 being transported Cytoplasm packed with hemoglobin- 97% of cell contents
Hb functions in gas transport Hb + O2 HbO2 (oxyhemoglobin)
Most numerous of the formed elements – females: 4.3 – 5.2 million cells/cubic ml of blood
males: 5.1 – 5.8 million cells/cubic ml of blood
Packed Cell Volume
• Percentage of the cellular elements (RBC’s,WBC’s and platelets) in the whole blood.
• PCV is considered equivalent to the volume of packed red cells or the so called haematocrit value, as the volume of WBC’s and platelets is very less.
• In 100ml of blood PCV is 45ml.• Haematocrit is the volume of RBC’s expressed as
percentage• Haematocrit value in males is about 45% Haematocrit value in females about 42%
22
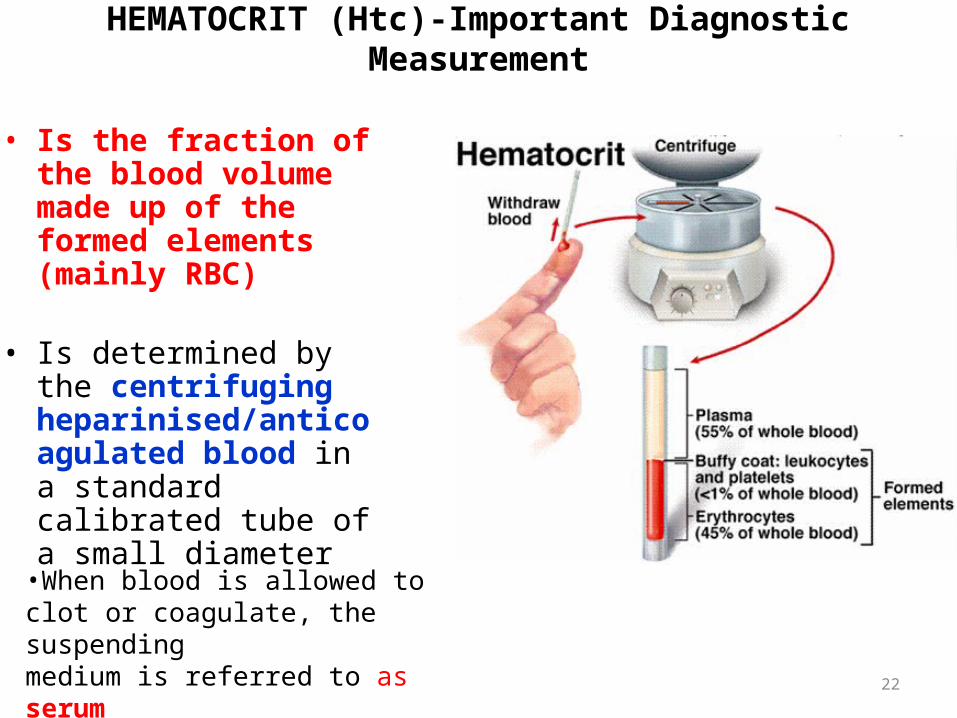
HEMATOCRIT (Htc)-Important Diagnostic Measurement
• Is the fraction of the blood volume made up of the formed elements (mainly RBC)
• Is determined by the centrifuging heparinised/anticoagulated blood in a standard calibrated tube of a small diameter
•When blood is allowed to clot or coagulate, the suspendingmedium is referred to as serum
23
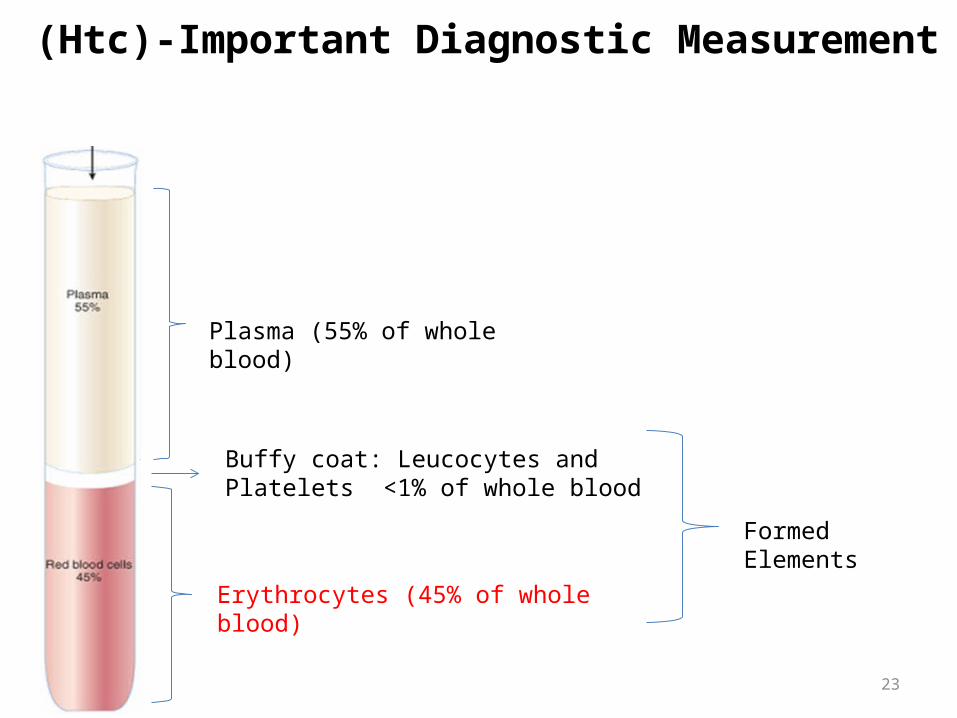
(Htc)-Important Diagnostic Measurement
Plasma (55% of whole blood)
Erythrocytes (45% of whole blood)
Buffy coat: Leucocytes and Platelets <1% of whole blood
Formed Elements
24
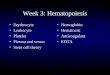
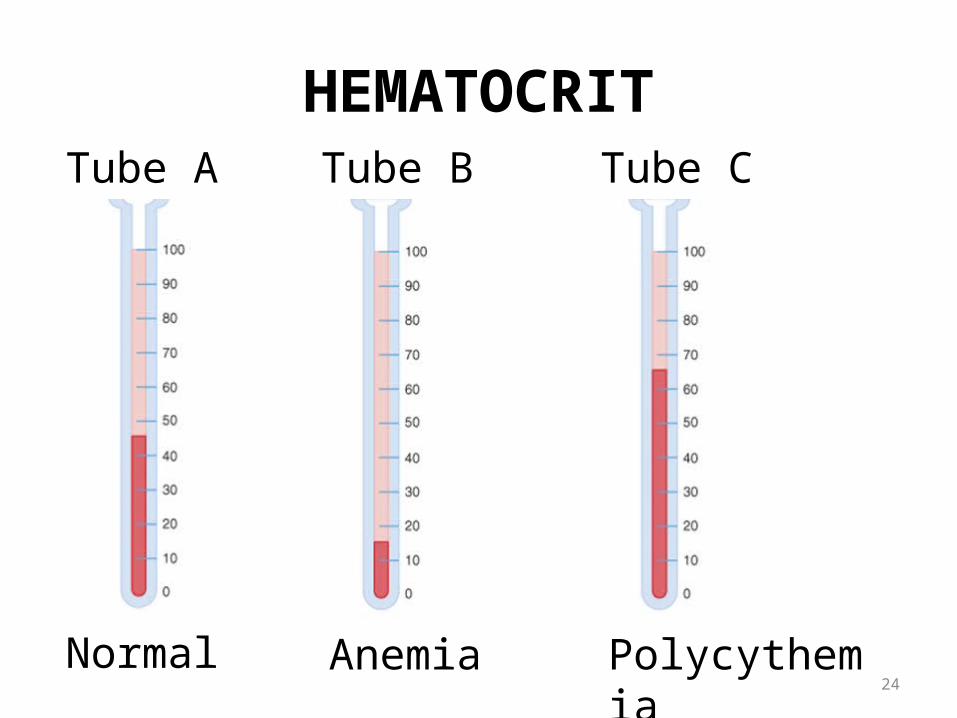
HEMATOCRIT
Normal Anemia Polycythemia
Tube A Tube B Tube C
25
HEMATOCRIT
• Values– Males: 40 – 54 vol% (mean – 47%; 0.47)– Females: 38 – 46 vol% (mean – 42%, 0.42)
• ↑ in persons leaving at high altitudes, in dehydrated state, polycythemia, etc.
• ↓ in anemia, leukemia, bone marrow failure
• Importance– Determines blood viscosity– ↑ Htc → ↑ resistance to blood flow, load on the heart & BP
Determination of hematocrit values is a simple and important screening diagnostic procedure in the evaluation of hematological disease
The contribution of the WBC to hematocrit is only 0.08%. WBCs are lighter than the RBCs, they form a thin whitish layer between the sedimented RBCs and the plasma.
26
Rouleaux formation
• Tendency of RBC’s to pile one over the other like a pile of coins.
• Their discoid shape and protein coating play major role in rouleaux formation
• Does not occur in normal circulation under physiological conditions
• This is reversible phenomenon.
Erythrocyte sedimentation rate• Citrated blood when allowed to stand in a narrow
vertical tube, the cells settle down leaving a layer of clear plasma above.
• The erythrocyte sedimentation rate is the mm of plasma separated per hour.
• Normal values- males 3-7 mm/hr females5-9 mm/hr
29
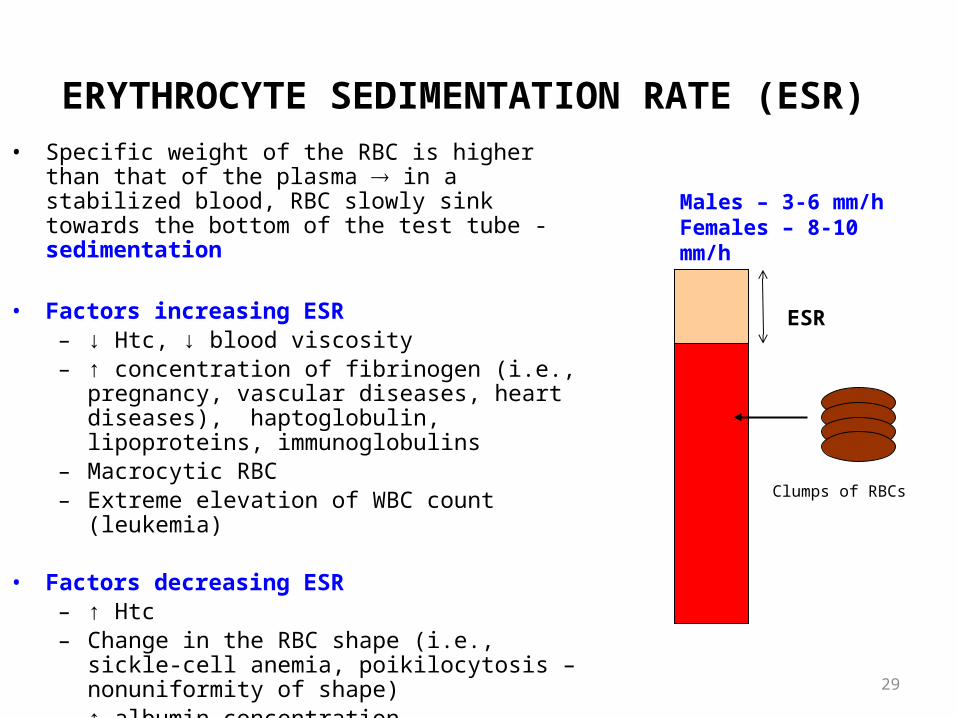
ERYTHROCYTE SEDIMENTATION RATE (ESR) • Specific weight of the RBC is higher than that of the
plasma in a stabilized blood, RBC slowly sink towards the bottom of the test tube -sedimentation
• Factors increasing ESR– ↓ Htc, ↓ blood viscosity– ↑ concentration of fibrinogen (i.e., pregnancy,
vascular diseases, heart diseases), haptoglobulin, lipoproteins, immunoglobulins
– Macrocytic RBC– Extreme elevation of WBC count (leukemia)
• Factors decreasing ESR– ↑ Htc – Change in the RBC shape (i.e., sickle-cell anemia,
poikilocytosis – nonuniformity of shape)– ↑ albumin concentration
ESR
Clumps of RBCs
Males – 3-6 mm/hFemales – 8-10 mm/h
Hematopoiesis: Blood Cell Formation
• Include erythropoiesis, leucopoiesis and thrombopoiesis.
• Mostly in bone marrow from haemopoietic stem cells.
• Rate regulated by cytokines & growth factors-like
IL-1,IL-3,IL-6,G-CSF,M-CSF,GM- CSF, Erythropoietin,Thrombopoietin………………
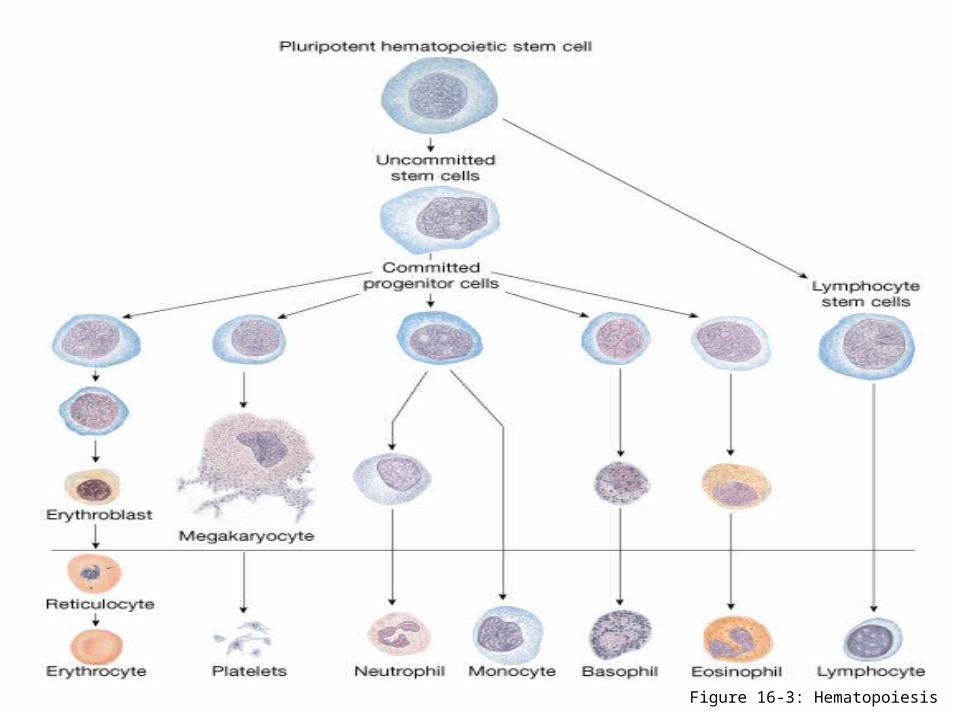
Figure 16-3: Hematopoiesis
32
Sites of haemopoiesis
•Yolk sac -Mesoblastic period (3rd wk
• Liver & spleen-Hepatic period(3rd mth
• Bone marrow -Myeloid period(5th mth
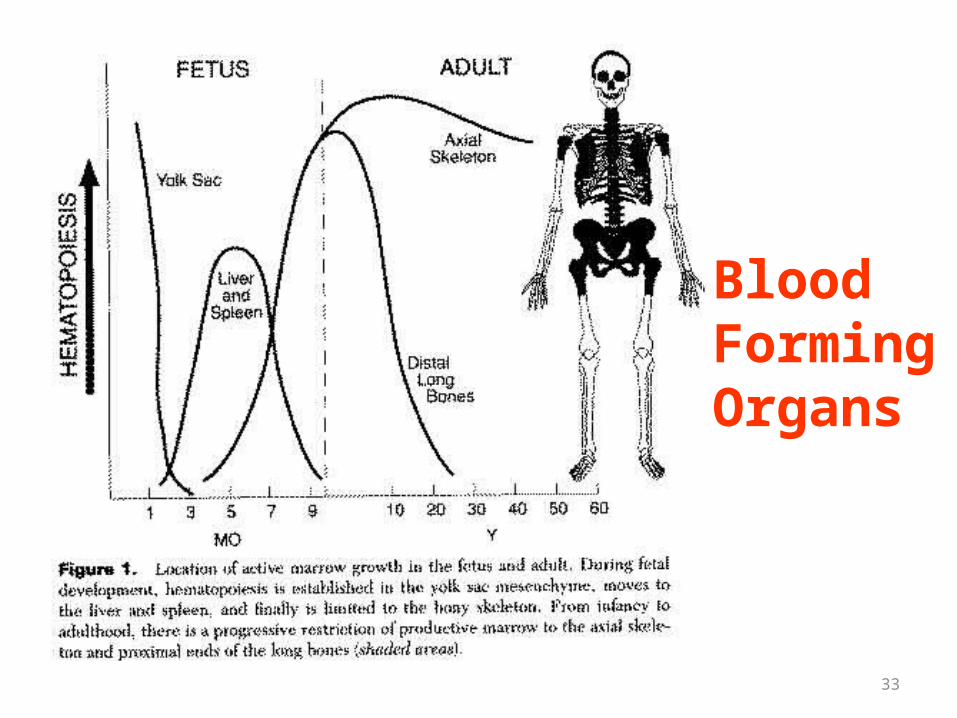
33
Blood FormingOrgans
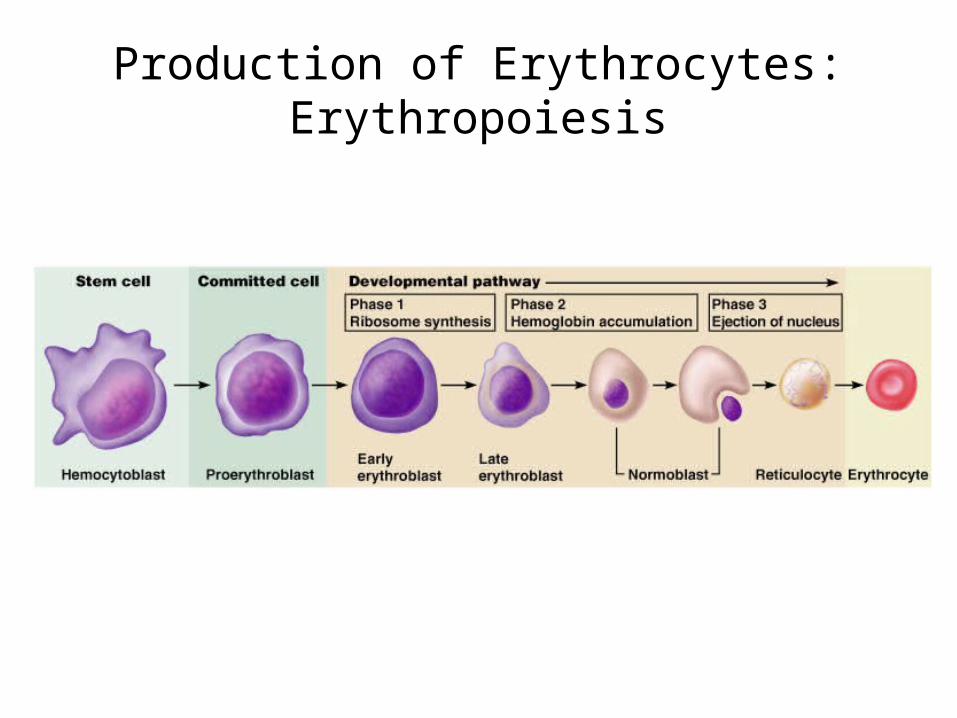
Production of Erythrocytes: Erythropoiesis
• A hemocytoblast is transformed into a committed cell called the proerythroblast
• Proerythroblasts develop into early erythroblasts• The developmental pathway consists of three phases
Phase 1 – ribosome synthesis in early erythroblastsPhase 2 – hemoglobin accumulation in late
erythroblasts and normoblastsPhase 3 – ejection of the nucleus from normoblasts
and formation of reticulocytes• Reticulocytes then become mature erythrocytes
Reticulocytes make up about 1 -2 % of all circulating erythrocytes
35
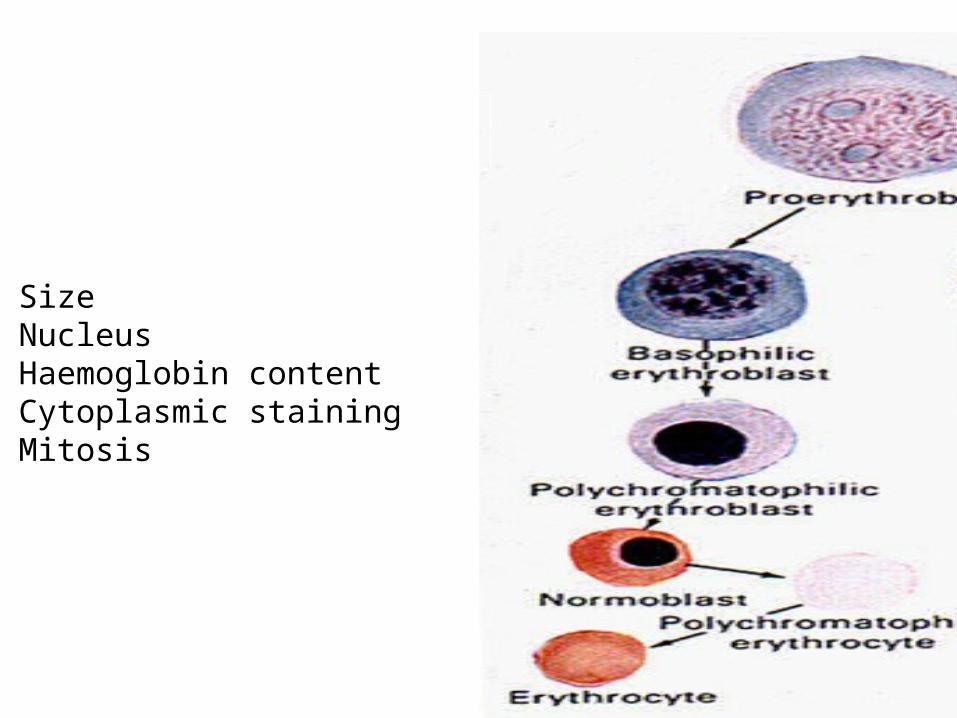
SizeNucleusHaemoglobin contentCytoplasmic stainingMitosis
Production of Erythrocytes: Erythropoiesis
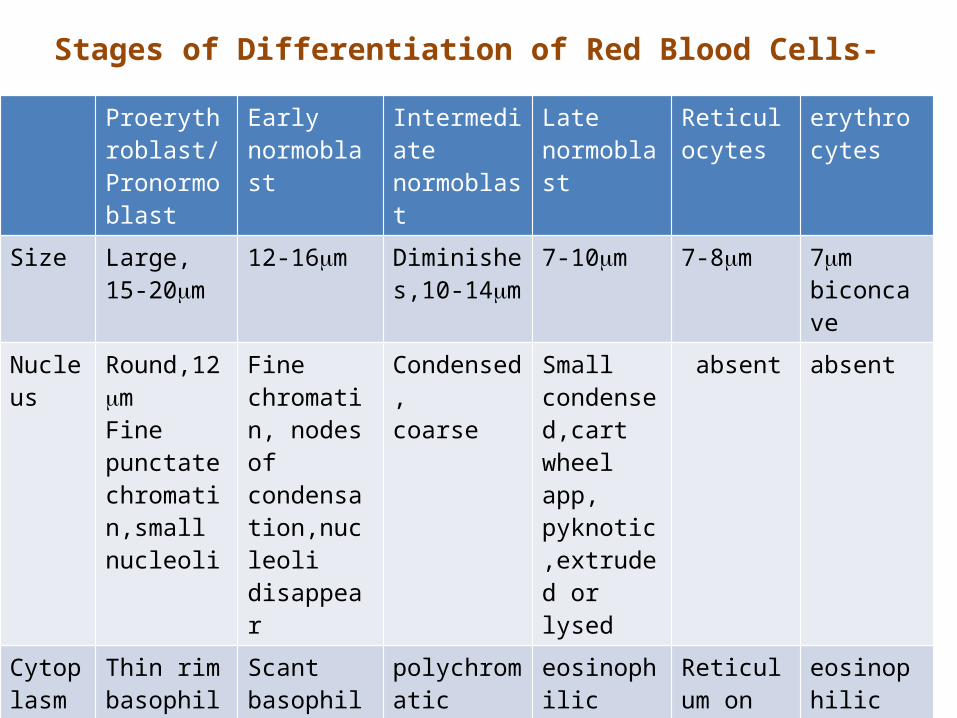
Stages of Differentiation of Red Blood Cells-Proerythroblast/Pronormoblast
Early normoblast
Intermediate normoblast
Late normoblast
Reticulocytes
erythrocytes
Size Large, 15-20m
12-16m Diminishes,10-14m
7-10m 7-8m 7mbiconcave
Nucleus
Round,12mFine punctate chromatin,small nucleoli
Fine chromatin, nodes of condensation,nucleoli disappear
Condensed,coarse
Small condensed,cart wheel app, pyknotic,extruded or lysed
absent absent
Cytoplasm
Thin rim basophilic
Scant basophilic
polychromatic
eosinophilic Reticulum on supra vital staining
eosinophilic
Hb absent Formation starts
Content rises increases increases max
Mitosis +nt +nt +nt -nt -nt -nt
Regulation of erythropoiesis1. Hypoxia decreased availability of oxygen decreased oxygenation of haemoglobin low blood vol /poor blood flow2. Erythropoietin• glycoprotein,• Site of formation- JG cells in kidney, liver
3. Maturation factors necessary for erythropoiesis
• Vitamin B12 and folic acid • Both are required for DNA synthesis,
nucleus maturation and cell division .• In their deficiency cells remain large
(megaloblast),making them less efficient and fragile.
4. Factors necessary for haemoglobinization
• Proteins• Iron • Copper• Cobalt• Calcium• Bile salts• Vitamin C
Anemia
Defination
It is the qualitative or quantitative diminution of haemoglobin or RBC or both in respect to the age and sex of the individual.
The net effect is failure in transport of adequate amount of oxygen to the tissues.
43
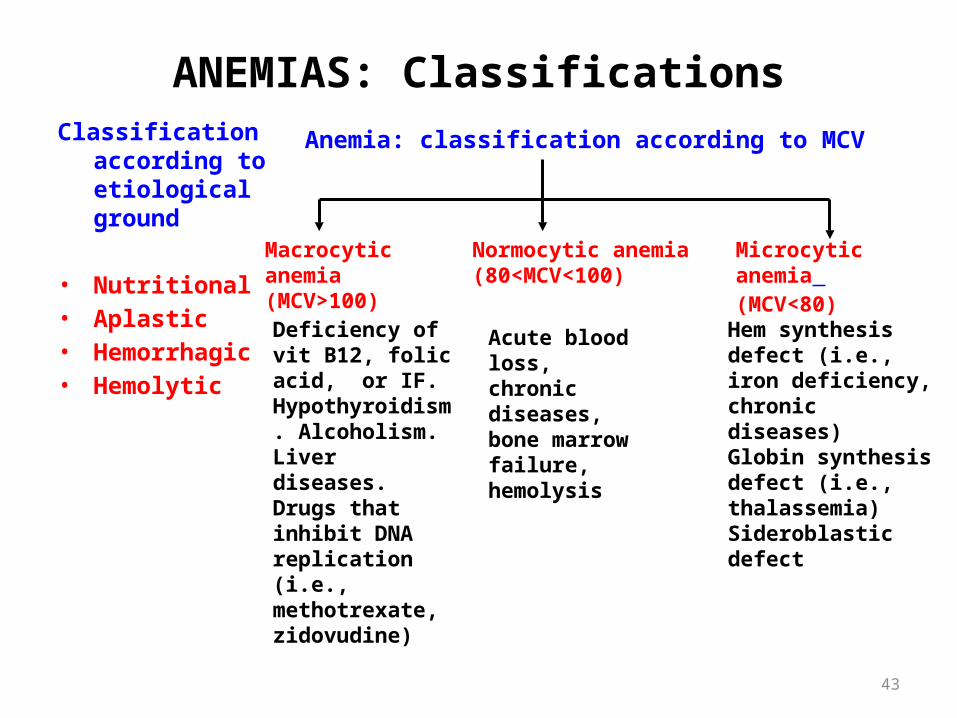
ANEMIAS: ClassificationsClassification
according to etiological ground
• Nutritional• Aplastic• Hemorrhagic• Hemolytic
Anemia: classification according to MCV
Macrocytic anemia (MCV>100)
Normocytic anemia (80<MCV<100)
Microcytic anemia (MCV<80)
Hem synthesis defect (i.e., iron deficiency, chronic diseases) Globin synthesis defect (i.e., thalassemia) Sideroblastic defect
Deficiency of vit B12, folic acid, or IF. Hypothyroidism. Alcoholism. Liver diseases. Drugs that inhibit DNA replication (i.e., methotrexate, zidovudine)
Acute blood loss, chronic diseases, bone marrow failure, hemolysis
44
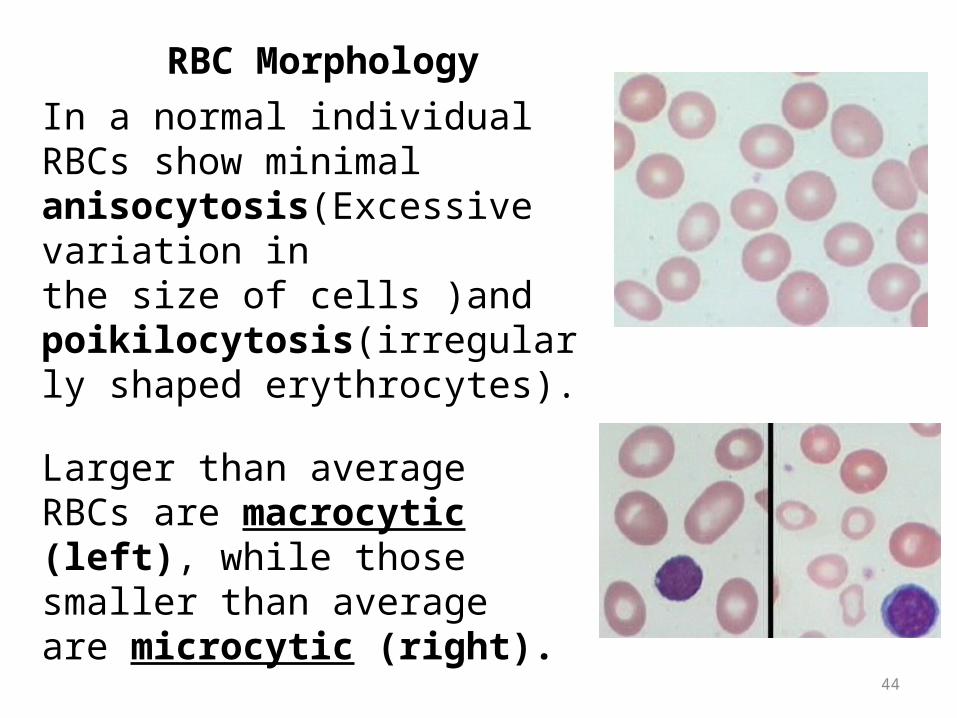
In a normal individual RBCs show minimal anisocytosis(Excessive variation inthe size of cells )and poikilocytosis(irregularly shaped erythrocytes).
Larger than average RBCs are macrocytic (left), while those smaller than average are microcytic (right).
RBC Morphology
45
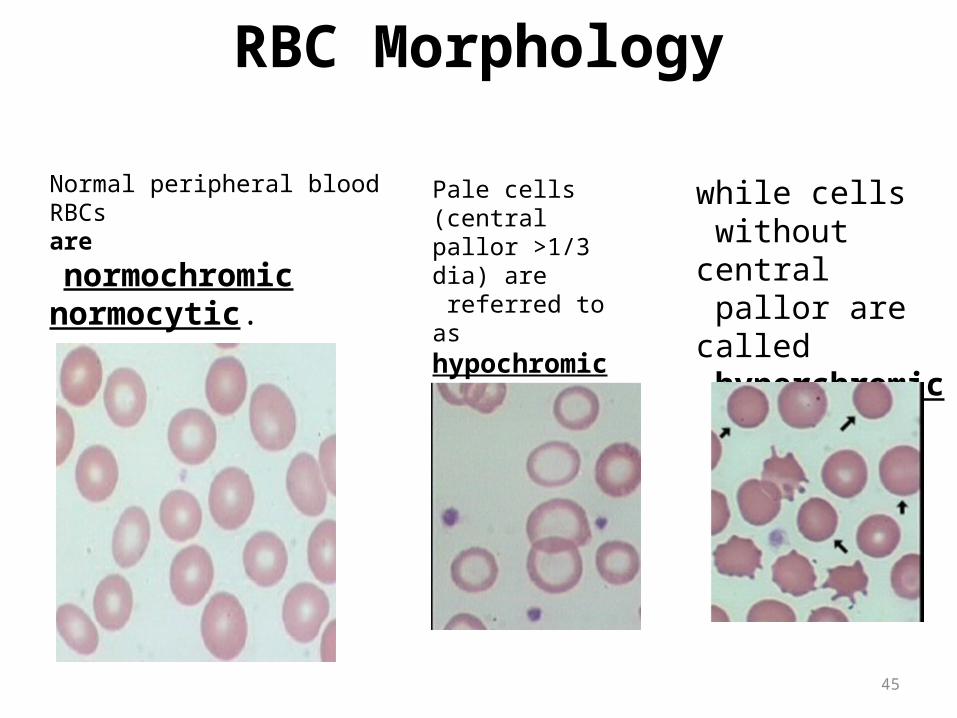
RBC Morphology
Normal peripheral blood RBCs are
normochromic normocytic.
while cells without central pallor are called hyperchromic
Pale cells (central pallor >1/3 dia) are referred to as hypochromic
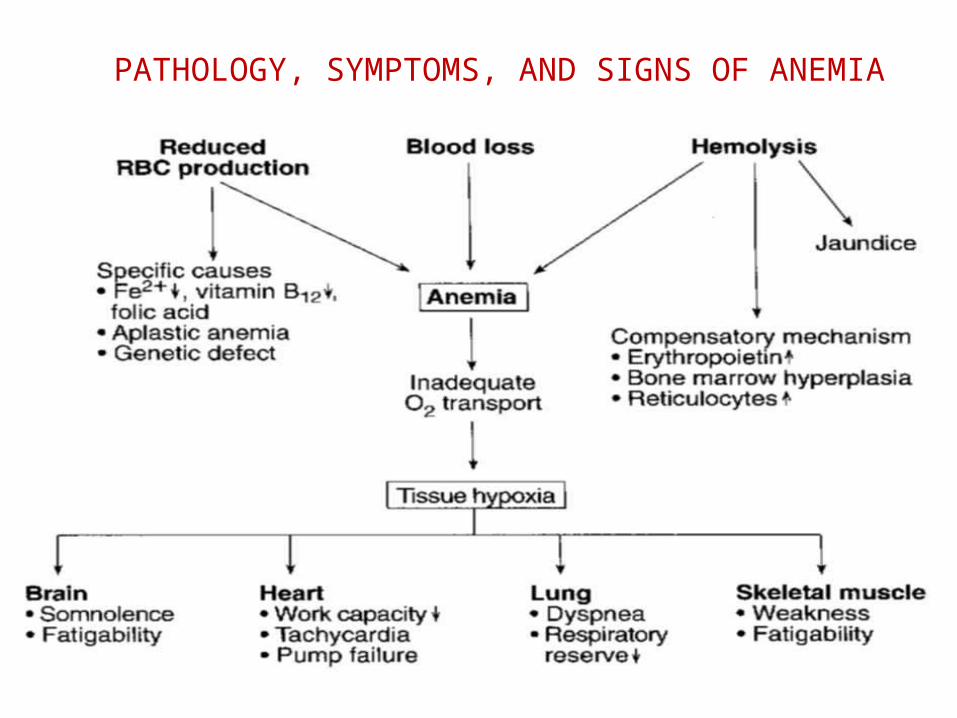
PATHOLOGY, SYMPTOMS, AND SIGNS OF ANEMIA
47
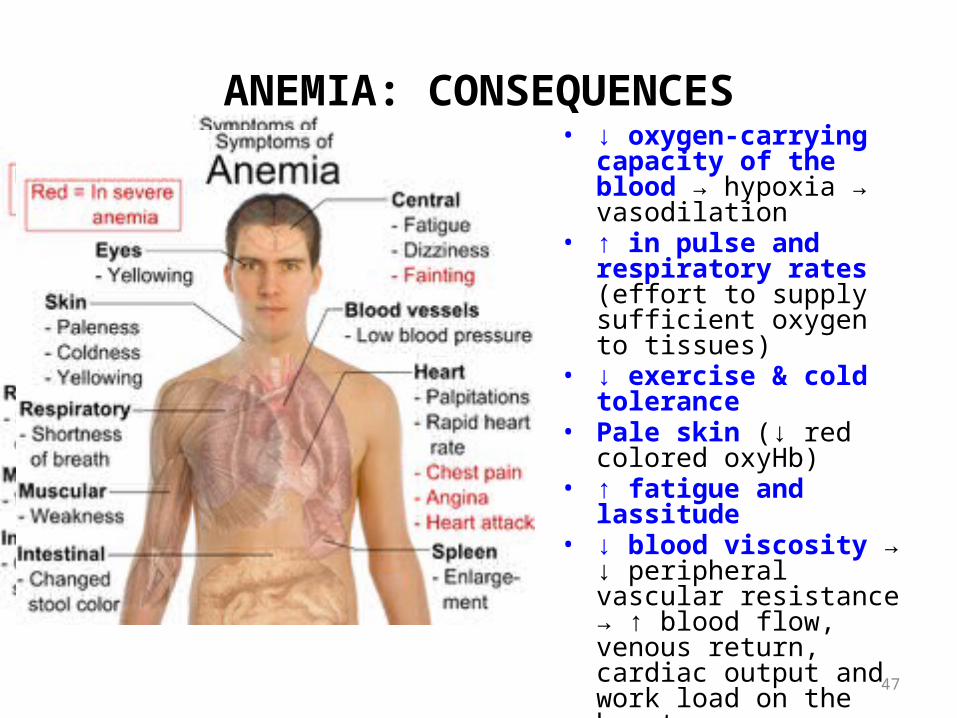
ANEMIA: CONSEQUENCES• ↓ oxygen-carrying capacity
of the blood → hypoxia → vasodilation
• ↑ in pulse and respiratory rates (effort to supply sufficient oxygen to tissues)
• ↓ exercise & cold tolerance
• Pale skin (↓ red colored oxyHb)
• ↑ fatigue and lassitude• ↓ blood viscosity → ↓
peripheral vascular resistance → ↑ blood flow, venous return, cardiac output and work load on the heart
Eyes- yellowing
48
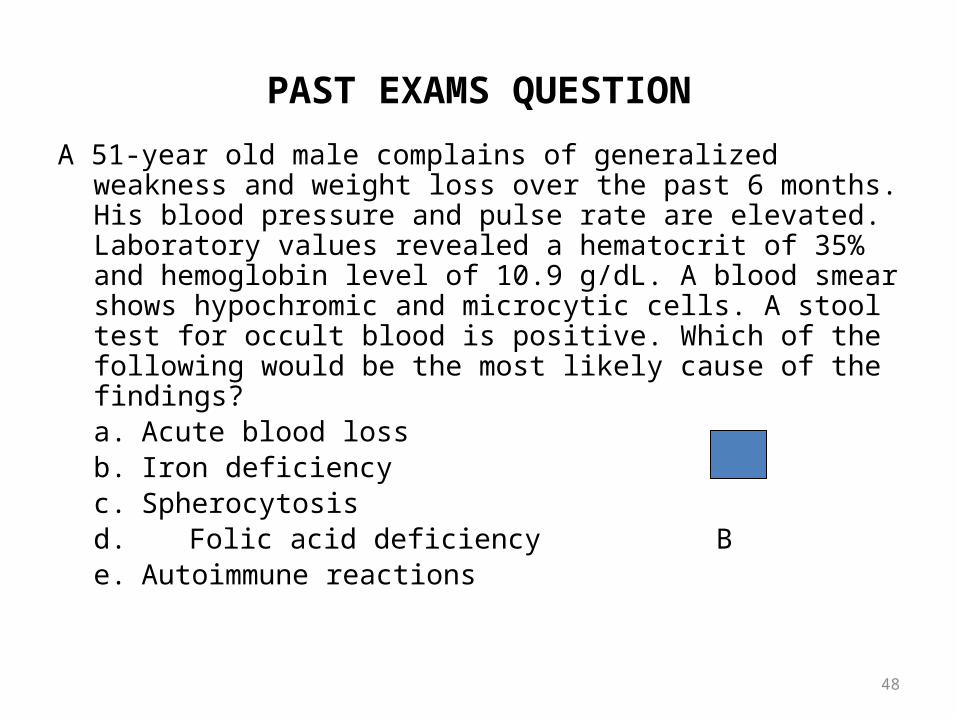
PAST EXAMS QUESTION
A 51-year old male complains of generalized weakness and weight loss over the past 6 months. His blood pressure and pulse rate are elevated. Laboratory values revealed a hematocrit of 35% and hemoglobin level of 10.9 g/dL. A blood smear shows hypochromic and microcytic cells. A stool test for occult blood is positive. Which of the following would be the most likely cause of the findings?a. Acute blood lossb. Iron deficiencyc. Spherocytosisd. Folic acid deficiency Be. Autoimmune reactions
Blood Groups
• Discovered by Landsteiner• Awarded Nobel Prize • Blood group Systems ABO ABO System Rh System Lewis SystemMN system Luthern System
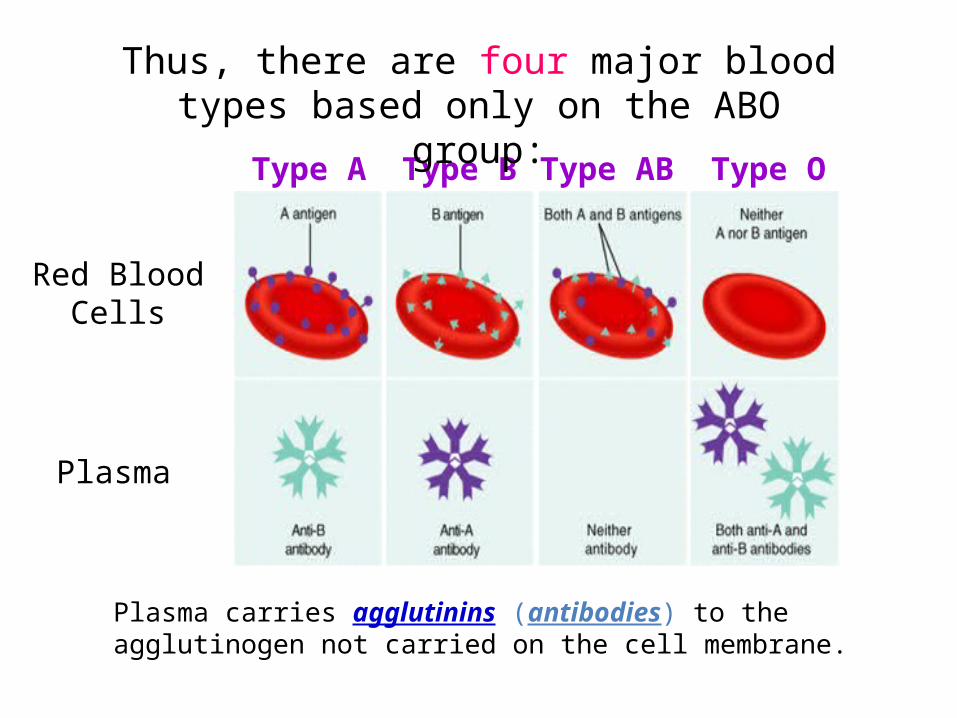
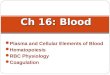
Red BloodCells
Plasma
Type A Type B Type AB Type O
Thus, there are four major blood types based only on the ABO group:
Plasma carries agglutinins (antibodies) to the agglutinogen not carried on the cell membrane.
Landsteiner’s Law
• If an agglutinogen is present on the RBC, corresponding agglutinin will be absent
• If the agglutinogen is absent corresponding Agglutinin will be present [Exception to the 2nd part is Rh System]
• Rh-ve people will not have Rh Antibodies
52
ABO blood group• But why are these agglutinins produced in people
who do not have the respective agglutinogens in their red blood cells?
• Small amounts of type A and B antigens enter the body in food, in bacteria, and in other ways, and these substances initiate the development of the anti-A and anti-B agglutinins.
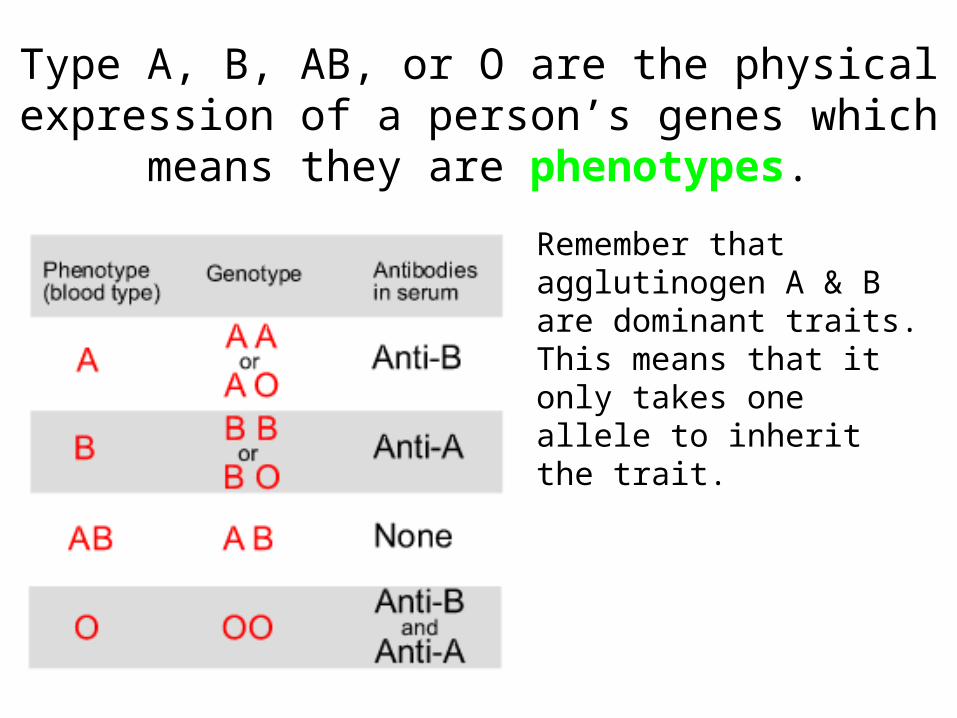
Remember that agglutinogen A & B are dominant traits. This means that it only takes one allele to inherit the trait.
Type A, B, AB, or O are the physical expression of a person’s genes which means they are phenotypes.
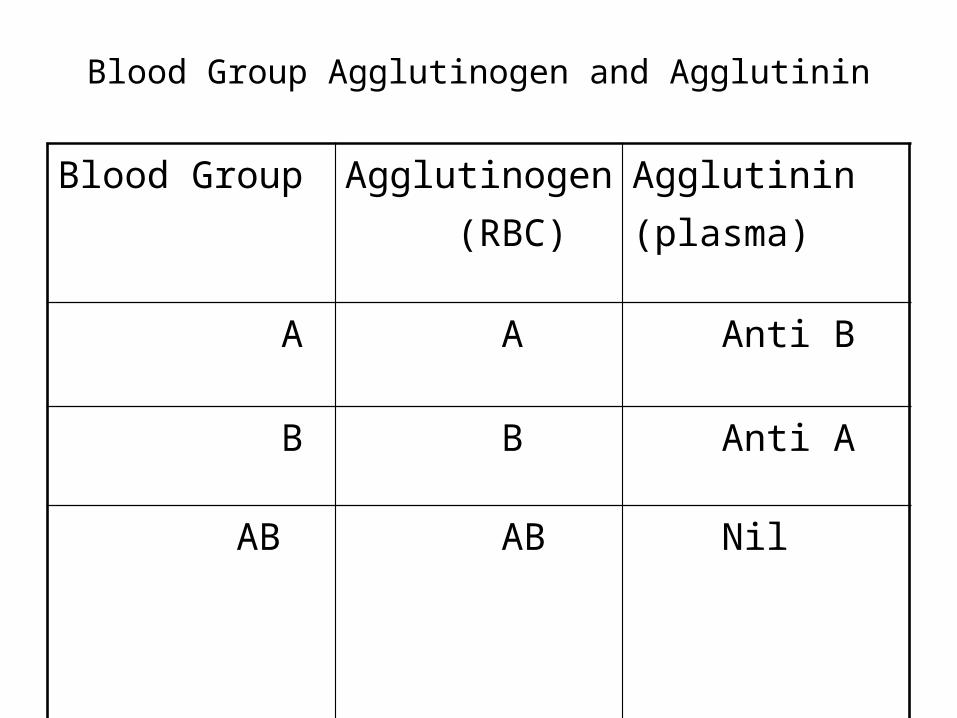
Blood Group Agglutinogen and Agglutinin
Blood Group Agglutinogen (RBC)
Agglutinin(plasma)
A A Anti B
B B Anti A
AB
AB Nil
O
Nil Anti A Anti B
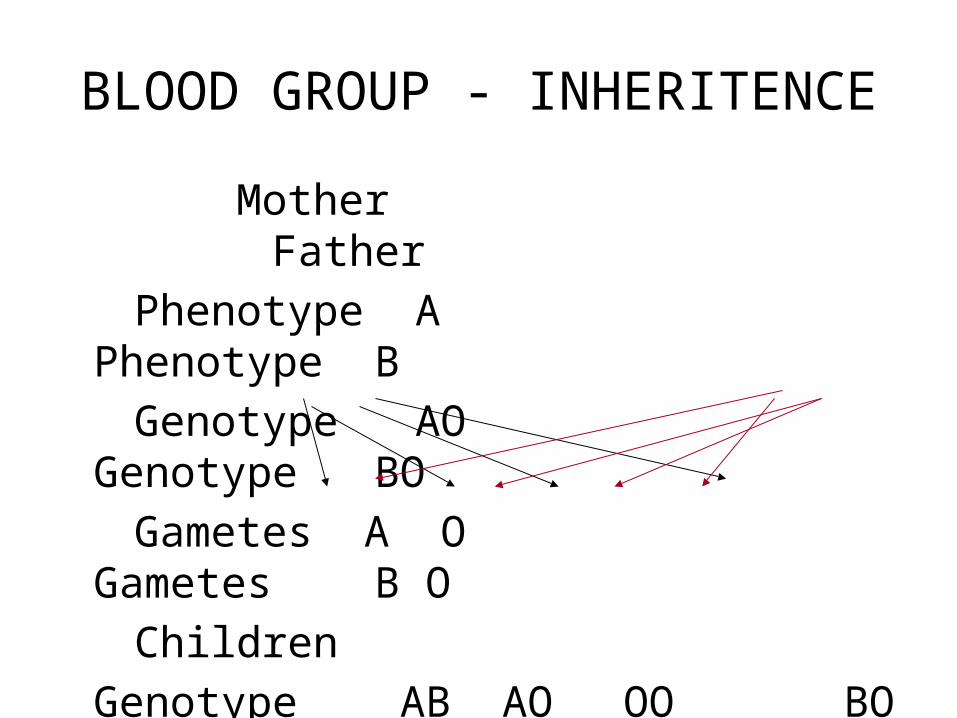
BLOOD GROUP - INHERITENCE
Mother Father Phenotype A Phenotype B Genotype AO Genotype BO Gametes A O Gametes B O Children
Genotype AB AO OO BO Phenotype AB A O B
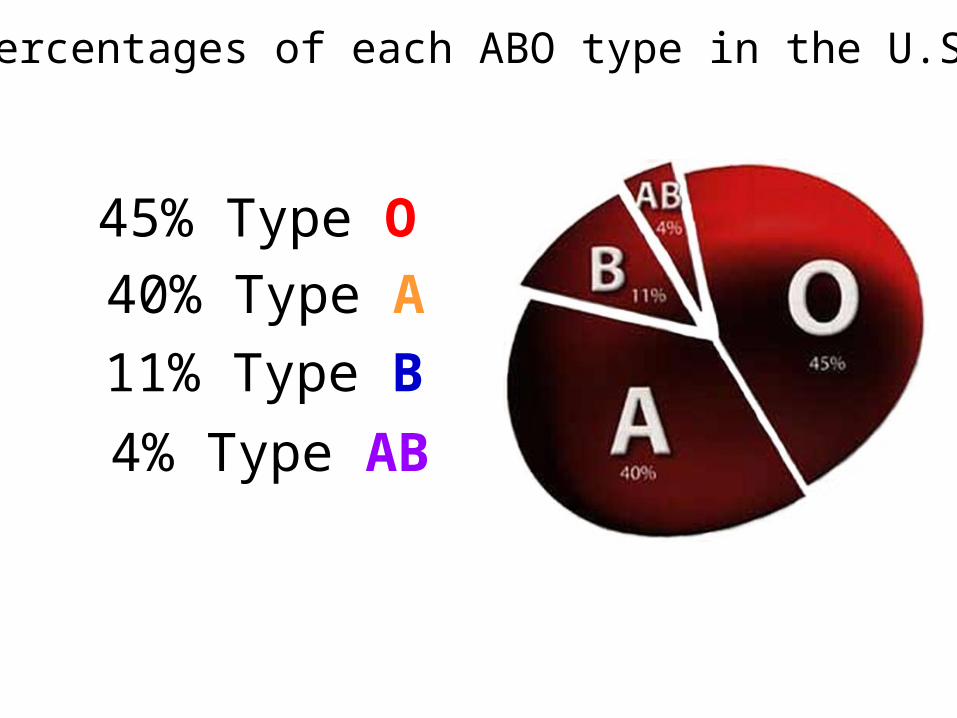
Percentages of each ABO type in the U.S.
45% Type O40% Type A11% Type B4% Type AB
• A man who is blood type AB marries a woman who is heterozygous type B. If they had children, what would their genotypes and phenotypes be?
58
Rh BLOOD GROUP SYSTEM• Rh (rhesus factor)
– Is named after the rhesus monkey in which it was found– Rh is an antigen present on the RBC membrane – transmembrane proteins,
which may act as ionic channels– 6 types of Rh AG
• C, D, E, c, d*, and e (+ 43 other Rh antigens, which are less common)
• Antigen D is the most common and potent– Presence of D antigen - Rh+ (RhD+)– Lack of D antigen - Rh- (RhD-)
• Population data on RhD+– 85% of Caucasians– 90% of African Americans– 99% of Asians– 100% of Africans
Inheritance of Rh GroupRh gene is inherited from both the parentsIf both the parents Contribute D antigen the
Genotype of the offspring is DD (Homozygous) Rh +ve
If the Gametes carry D and d (allelomorph when D is absent) the Genotype of the offspring is Dd (heterozygous) Rh+ve
If both the gametes carry d the offspring genotype is dd (homozygous) Rh-ve
60
Rh BLOOD GROUP SYSTEM: Antibodies
• Blood of normal individual does not contain anti-Rh antibodies (with exception of anti-E)
• Production of anti-Rh antibodies can be evoked by– Transfusion of Rh- individual with Rh+ blood (only 0.5 ml may
suffice)– The presence of Rh+ fetus in a Rh- mother
61
Rh IMMUNE RESPONSE
• Transfusion of RhD+ blood to un-immunized RhD- recipient– No immediate reaction– Sensitization of recipient’s blood to RhD AG - slow formation of
anti-RhD AB– Delayed transfusion reaction – hemolysis of the donor’s RBC
that still circulate in the recipient’s blood
• Transfusion of RhD+ blood to immunized RhD-recipient – Enhanced transfusion reaction – acute hemolysis
62
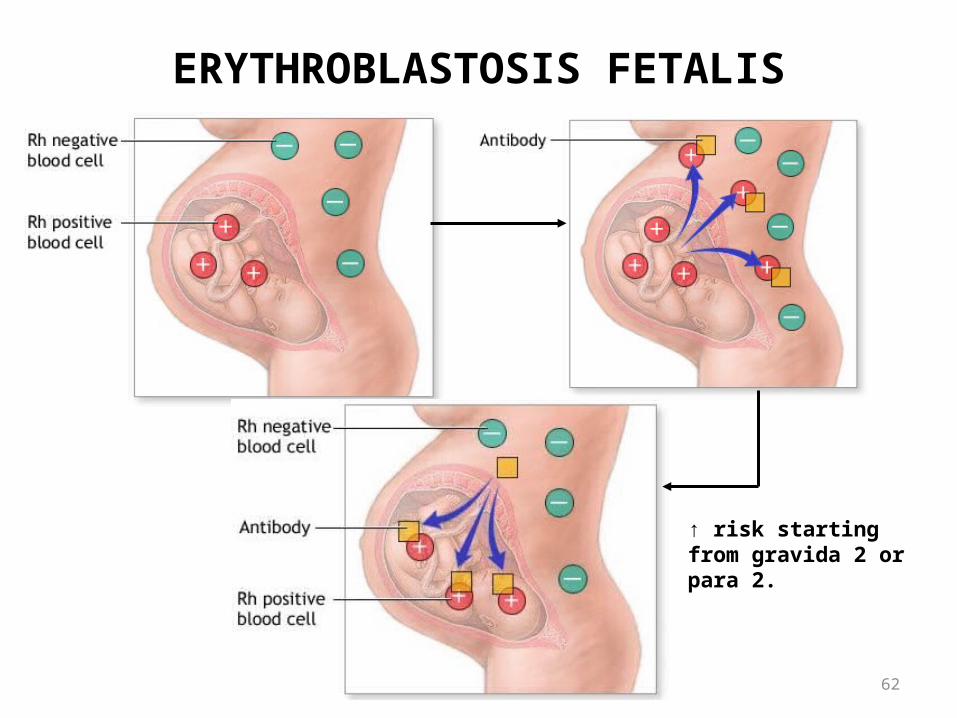
ERYTHROBLASTOSIS FETALIS
↑ risk starting from gravida 2 or para 2.
63
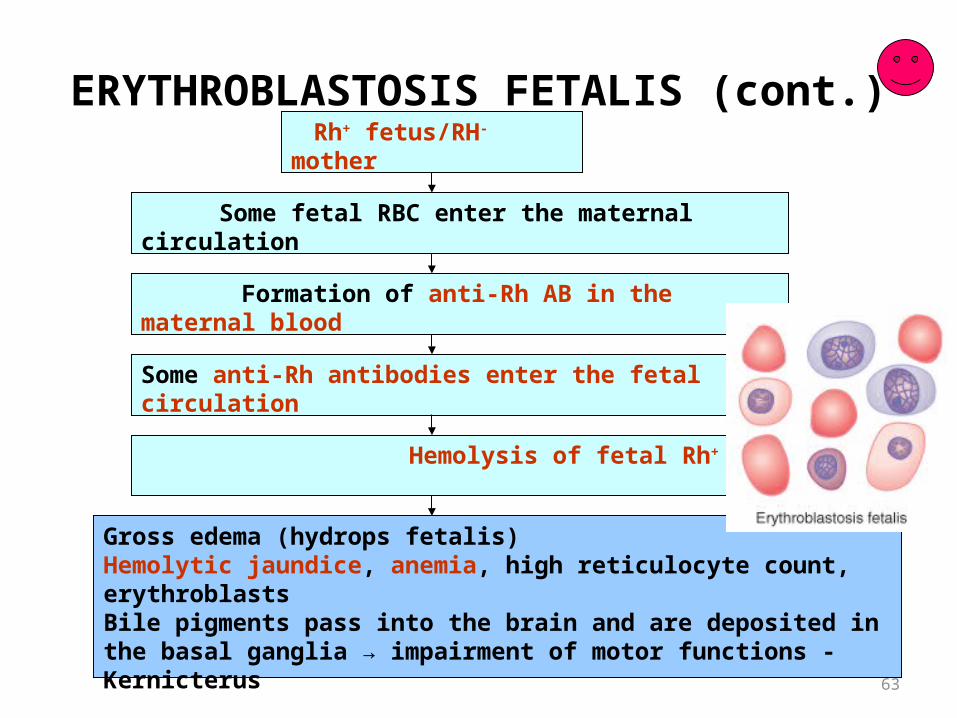
ERYTHROBLASTOSIS FETALIS (cont.) Rh+ fetus/RH- mother
Some fetal RBC enter the maternal circulation
Formation of anti-Rh AB in the maternal blood
Hemolysis of fetal Rh+ RBC
Some anti-Rh antibodies enter the fetal circulation
Gross edema (hydrops fetalis)Hemolytic jaundice, anemia, high reticulocyte count, erythroblastsBile pigments pass into the brain and are deposited in the basal ganglia → impairment of motor functions - Kernicterus
Gross edema
64
ERYTHROBLASTOSIS FETALIS (cont.)• Treatment
– Replacement of the neonate’s blood with Rh- blood – removal of Rh AB and damaged RBC
• Prevention– Administration of anti-D AB to the Rh- pregnant woman who
expects RhD+ baby• Destruction of Rh+ RBC, which cross the placenta and
enter the maternal circulation• Inhibition of AG-induced AB production by B
lymphocytes in the pregnant woman
Transfusion Blood transfusion is a lot like marriage. It should not be
entered upon lightly, unadvisedly or wantonly, or more often than is absolutely necessary” - Beal
Blood transfusion• Blood transfusion is the process of
receiving blood products into one's circulation intravenously.
• Transfusion can be of whole blood or blood components like packed cells, fresh frozen plasma, platelet rich plasma, albumin, cryoprecipitate, etc.
• Blood transfusion can be autologous or allogenetic; most commonly allogenetic.
68
Agglutination and hemolysis in transfusion reaction
When bloods are mismatched so anti-A or anti-B plasma agglutinins are mixed with red blood cells that contain A or B agglutinogens respectively, agglutinins will make the red cells adhere to each
other – agglutination. The clumps of red cells will plug small blood
vessels throughout the circulatory.
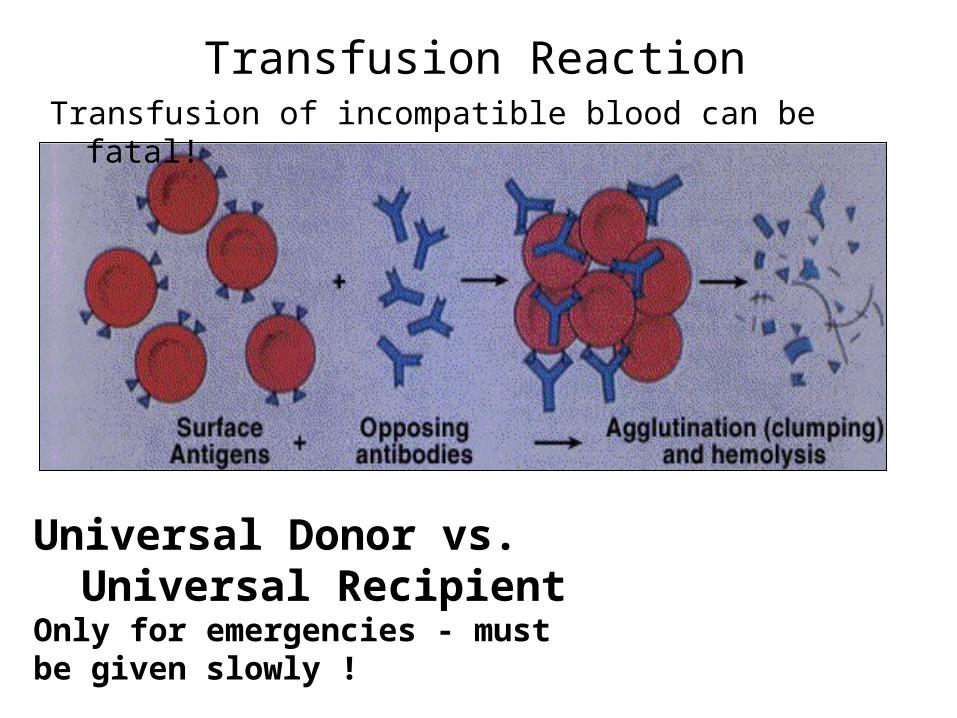
Transfusion ReactionTransfusion of incompatible blood can be fatal!
Universal Donor vs. Universal RecipientOnly for emergencies - must be given slowly !
70
Agglutination and hemolysis in transfusion reaction
During the ensuring few hours to a few days, either physical distortion of the cells or
attack by phagocytic white cells destroys the agglutinated cells,
releasing hemoglobin into the plasma, which is called “hemolysis” of the red blood
cells. Type II hypersensitivity reaction
71
agglutination
During severe hemolytic reaction, fever, chills and shock may occur.
One of the most lethal effects of transfusion reactions is kidney shutdown, which can begin within few minutes to a few hours.
If the shutdown is complete and fails to open up, the patient die of renal failure.
72
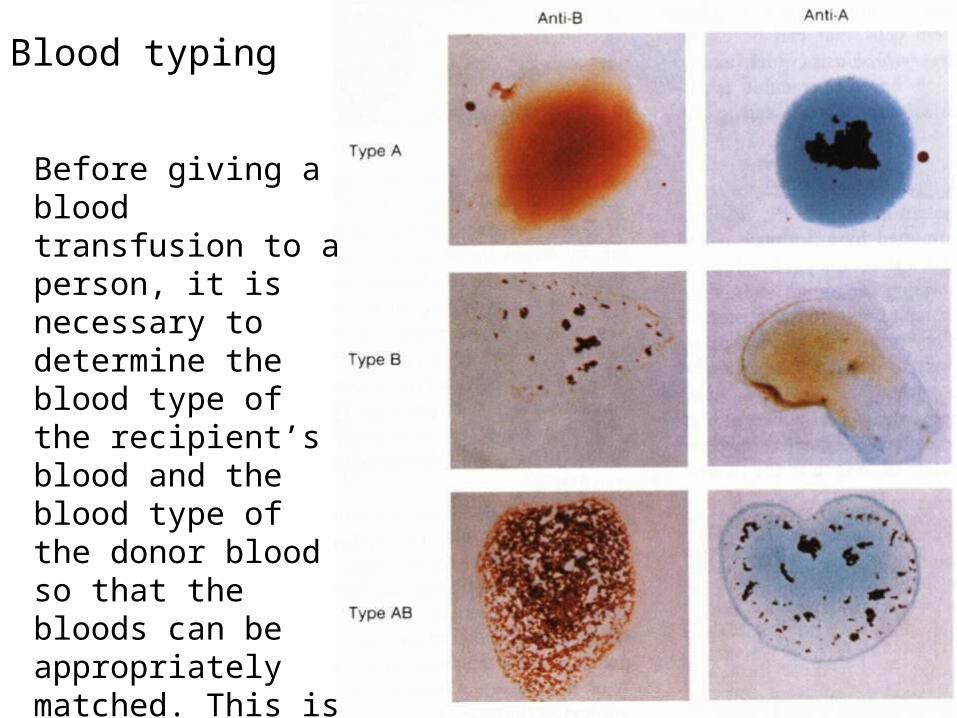
Blood typing
Before giving a blood transfusion to a person, it is necessary to determine the blood type of the recipient’s blood and the blood type of the donor blood so that thebloods can be appropriately matched. This is calledblood typing and blood matching.
73
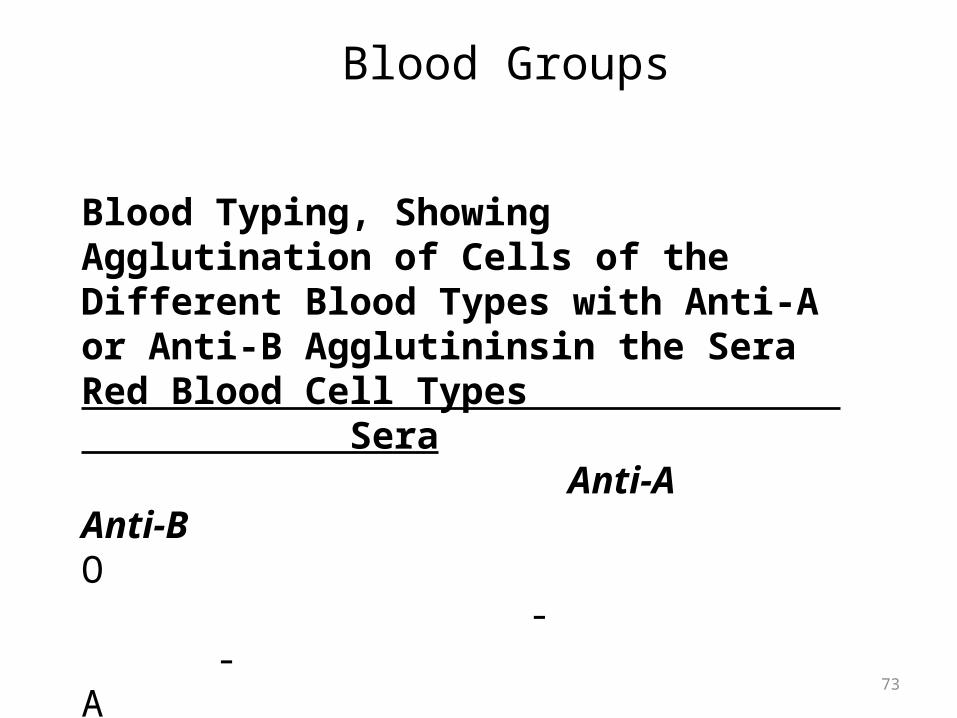
Blood Groups
Blood Typing, Showing Agglutination of Cells of the Different Blood Types with Anti-A or Anti-B Agglutininsin the SeraRed Blood Cell Types Sera Anti-A Anti-BO - -A + -B - +AB + +
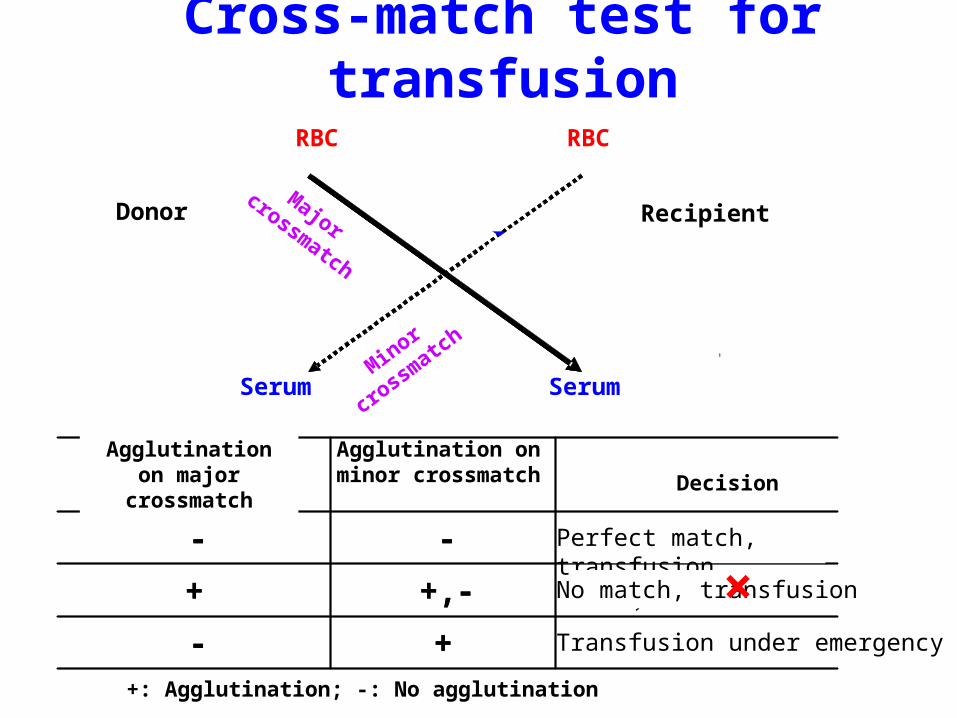
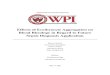
Cross-match test for transfusion
红细胞
供血者
受血者
血清
红细胞
血清
红细胞
供血者
受血者
血清
红细胞
血清
应急情况下输血+-
不合,不能输血+, -+
相合,可以输血--
次侧凝集反应主侧凝集反应
应急情况下输血+-
不合,不能输血+, -+
相合,可以输血--
次侧凝集反应主侧凝集反应
RBC RBC
Donor Recipient
Major crossmatch
Minor
crossm
atch
Serum Serum
Agglutination on major crossmatch
Perfect match, transfusion
No match, transfusion
Transfusion under emergency
×
Agglutination on minor crossmatch Decision
+: Agglutination; -: No agglutination
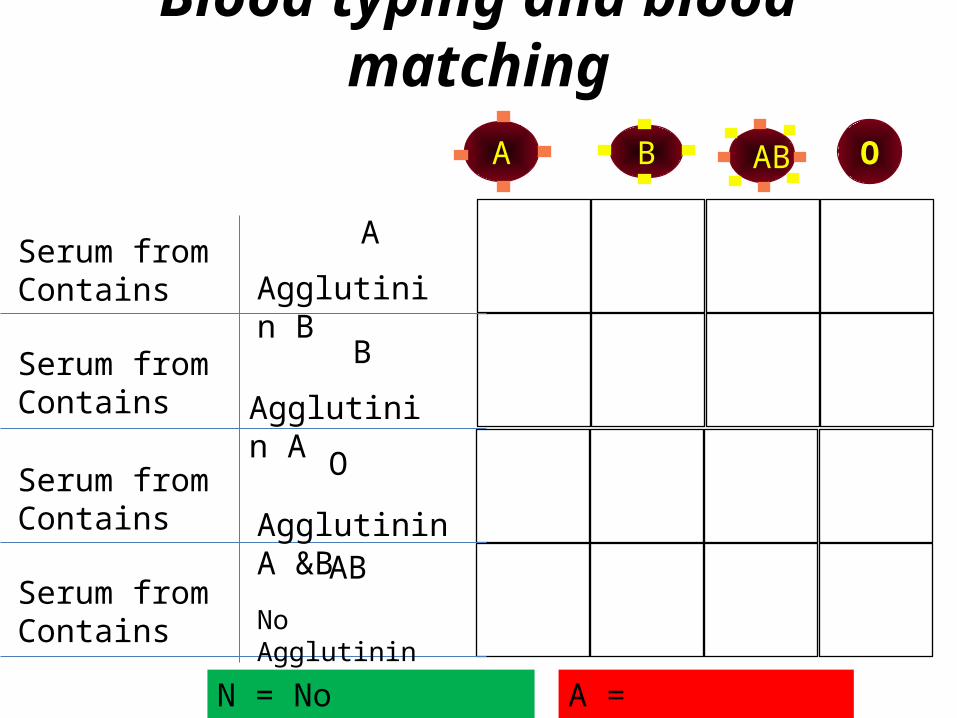
Blood typing and blood matching
Serum fromContains
Serum fromContains
Serum fromContains
Serum fromContains
A
Agglutinin B
B
Agglutinin A
O
Agglutinin A &BAB
No Agglutinin
N = No Agglutination A = Agglutination
A B O AB
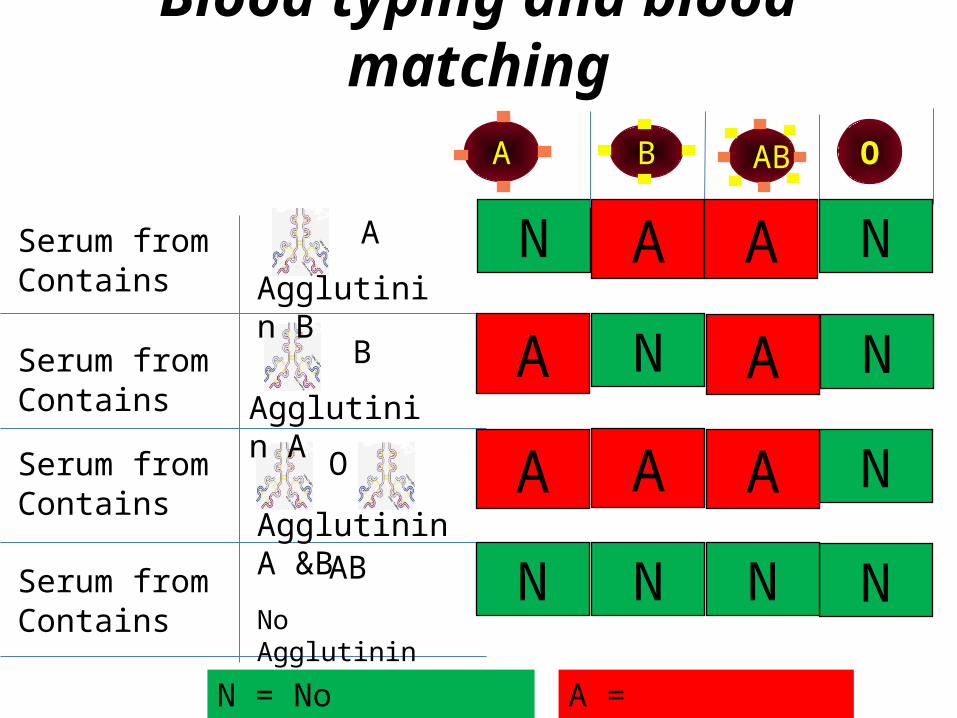
Blood typing and blood matching
ANSerum from A
Agglutinin B
B
Agglutinin A
O
Agglutinin A &BAB
No Agglutinin
N
N
N
N
A
A
A
A
N N N
N
A A
Contains
Serum fromContains
Serum fromContains
Serum fromContains
N = No Agglutination A = Agglutination
A B O AB
Structure & functions of WBC
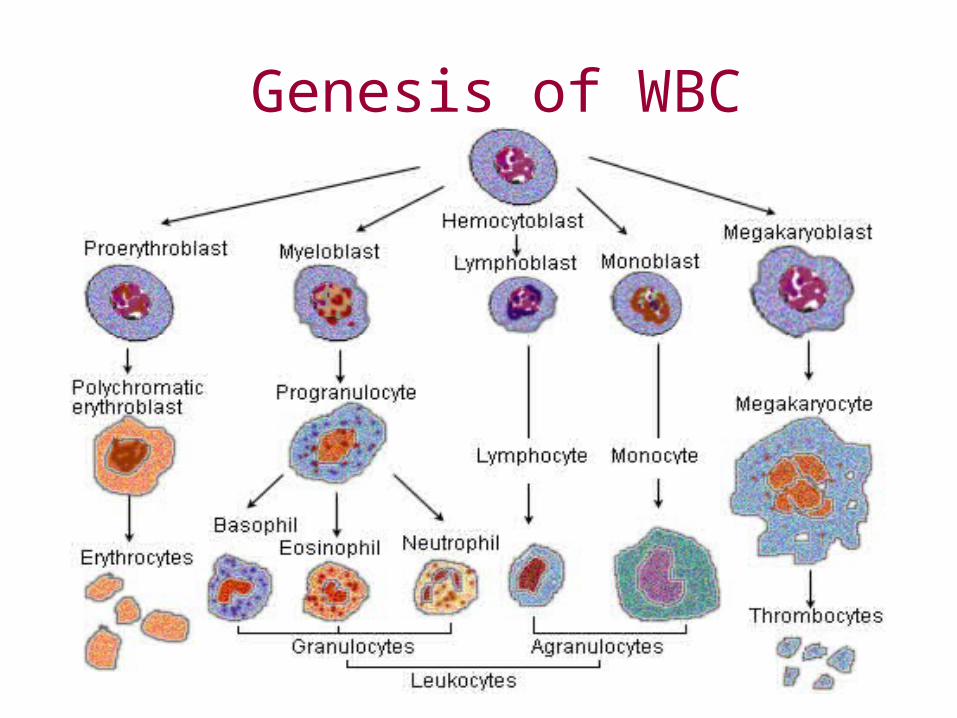
Genesis of WBC
WHITE BLOOD CORPUSCLES
Mobile units of body’s protective system Soldiers defending against microorganism Seek out & destroy foreign invaders
Phagocytosis Forming Ab & sensitised lymphocytes
Differ from RBC Formed in bone marrow & lymphoid organs Average lifespan is short Myeloid : Erythroid – 75% : 25%
CLASSIFICATION
WBC
Granulocytes Agranulocytes
Neutrophil Eosinophil Basophil Monocyte Lymphocyte
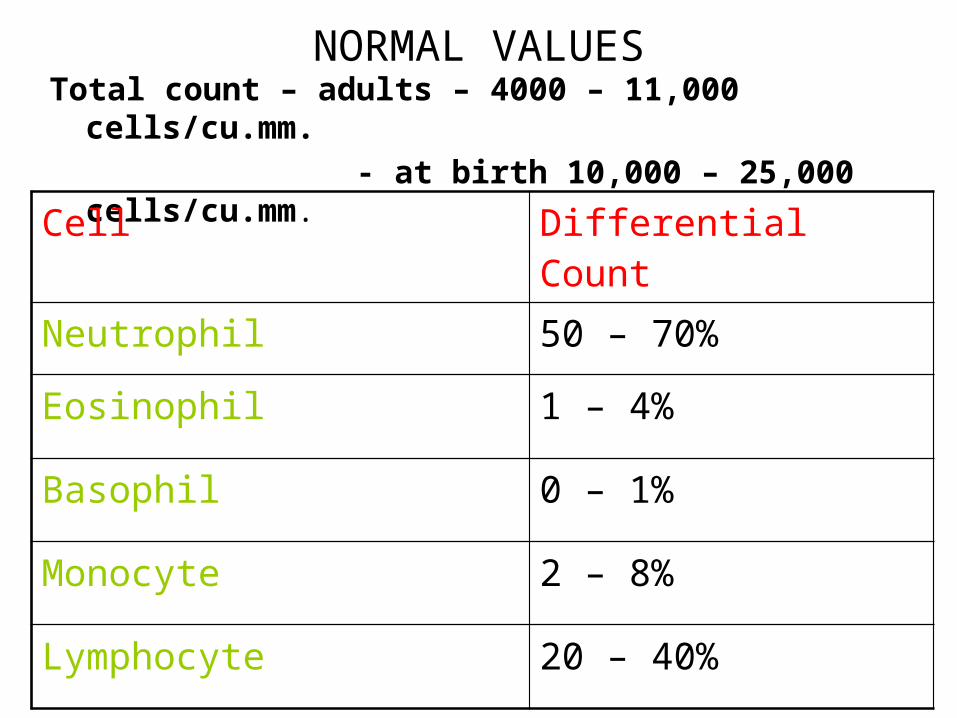
NORMAL VALUESTotal count – adults – 4000 – 11,000 cells/cu.mm. - at birth 10,000 – 25,000 cells/cu.mm.
Cell Differential Count
Neutrophil 50 – 70%
Eosinophil 1 – 4%
Basophil 0 – 1%
Monocyte 2 – 8%
Lymphocyte 20 – 40%
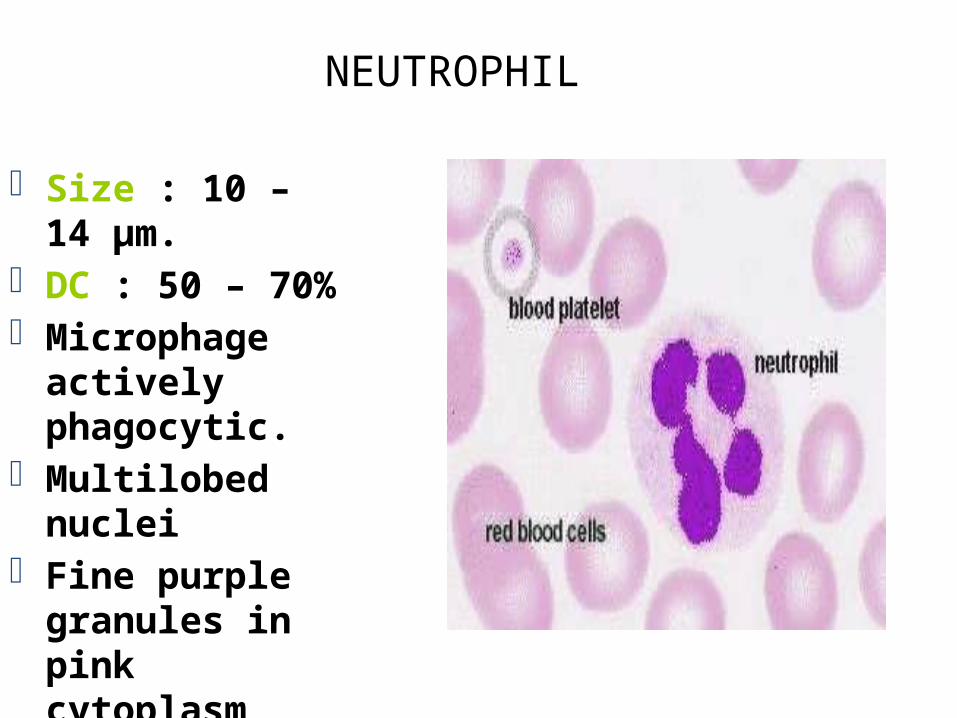
NEUTROPHIL
Size : 10 – 14 µm. DC : 50 – 70% Microphage actively
phagocytic. Multilobed nuclei Fine purple
granules in pink cytoplasm
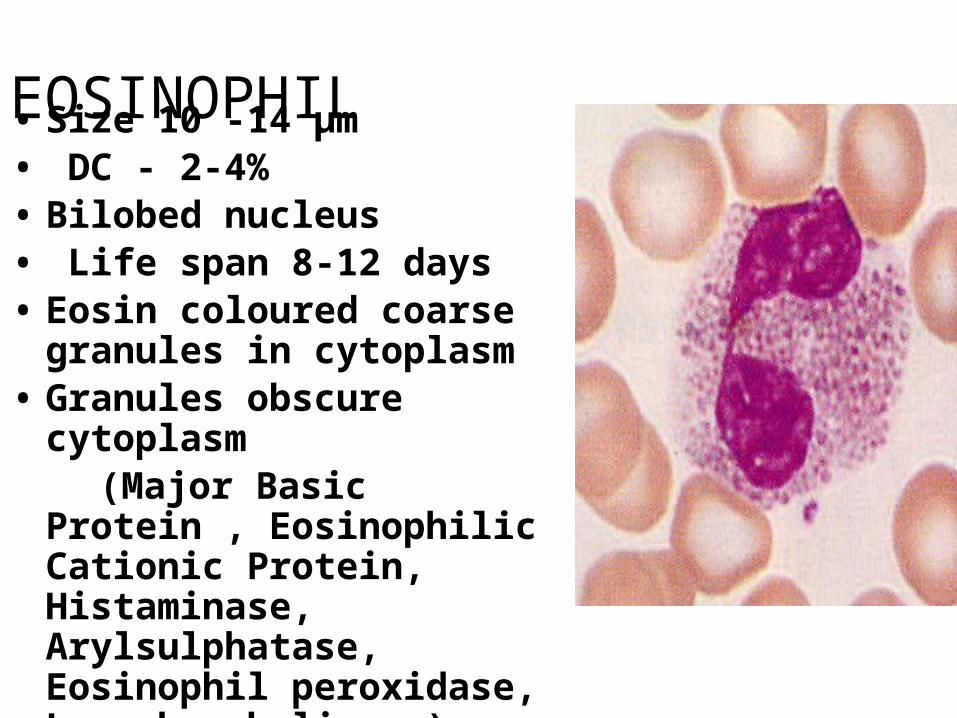
EOSINOPHIL• Size 10 -14 µm• DC - 2-4% • Bilobed nucleus• Life span 8-12 days• Eosin coloured coarse granules in
cytoplasm• Granules obscure cytoplasm (Major Basic Protein , Eosinophilic
Cationic Protein, Histaminase, Arylsulphatase, Eosinophil peroxidase, Lysophospholipase)
EOSINOPHIL
• Functions♠ Defends body from allergic reactions (Neutralise allergen, larvicidal,
parasiticidal)♠ Weakly phagocytic♠ Limits the effects of antigen antibody
reactions
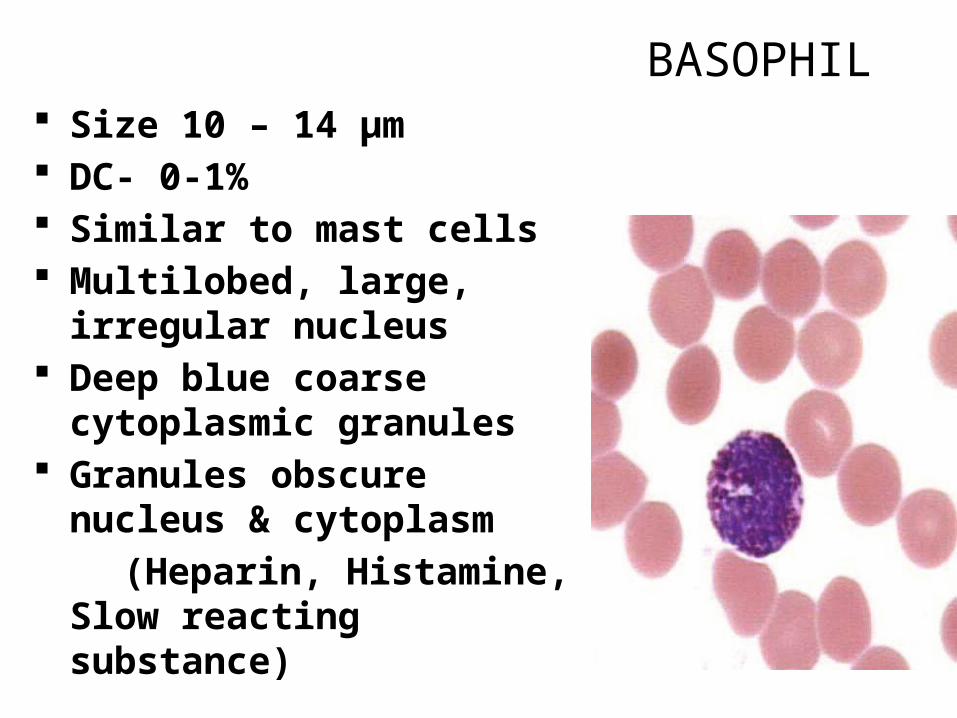
BASOPHIL Size 10 – 14 µm DC- 0-1% Similar to mast cells Multilobed, large, irregular
nucleus Deep blue coarse cytoplasmic
granules Granules obscure nucleus &
cytoplasm (Heparin, Histamine, Slow
reacting substance)
BASOPHIL
Functions: Phagocytic Heparin - prevents intravascular clotting Histamine & SRS - take part in IgE mediated
allergic reactions along with mast cells.
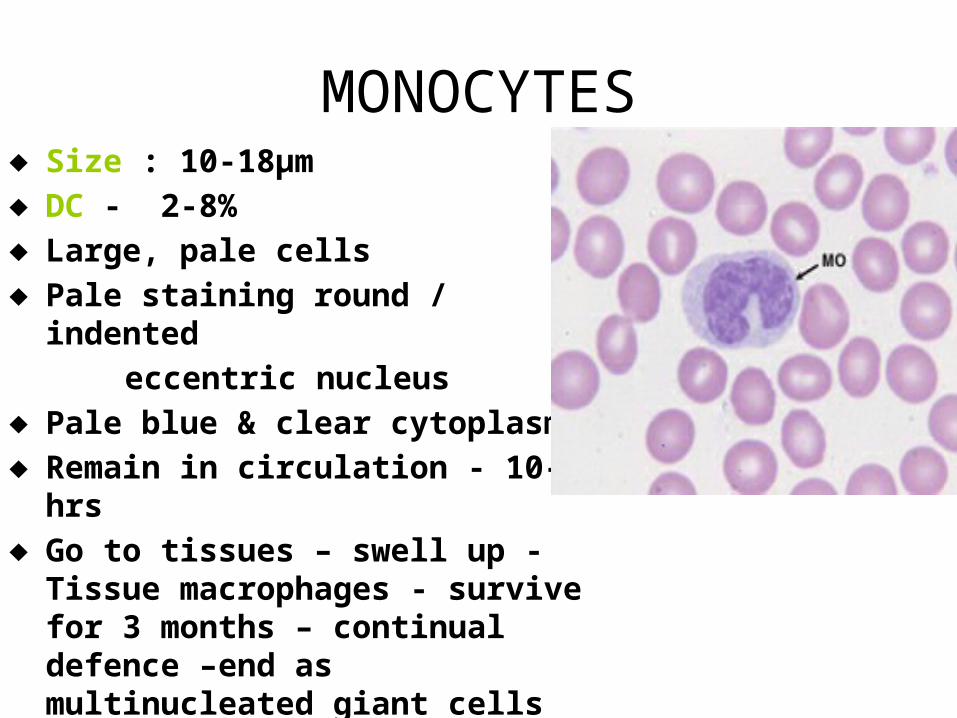
MONOCYTES♦ Size : 10-18µm♦ DC - 2-8%♦ Large, pale cells♦ Pale staining round / indented eccentric nucleus ♦ Pale blue & clear cytoplasm♦ Remain in circulation - 10-20 hrs♦ Go to tissues – swell up - Tissue
macrophages - survive for 3 months – continual defence –end as multinucleated giant cells
FUNCTIONS OF MONOCYTES
Actively phagocytic – Mononuclear macrophage-engulf 100 bacteria
Participate in immune response –process and present antigen to T & B lymphocyte
Monocytes on stimulation secrete IL -1, promotes proliferation and maturation of T lymphocytes
Destroy senescent RBC - initiate catabolism of Hb
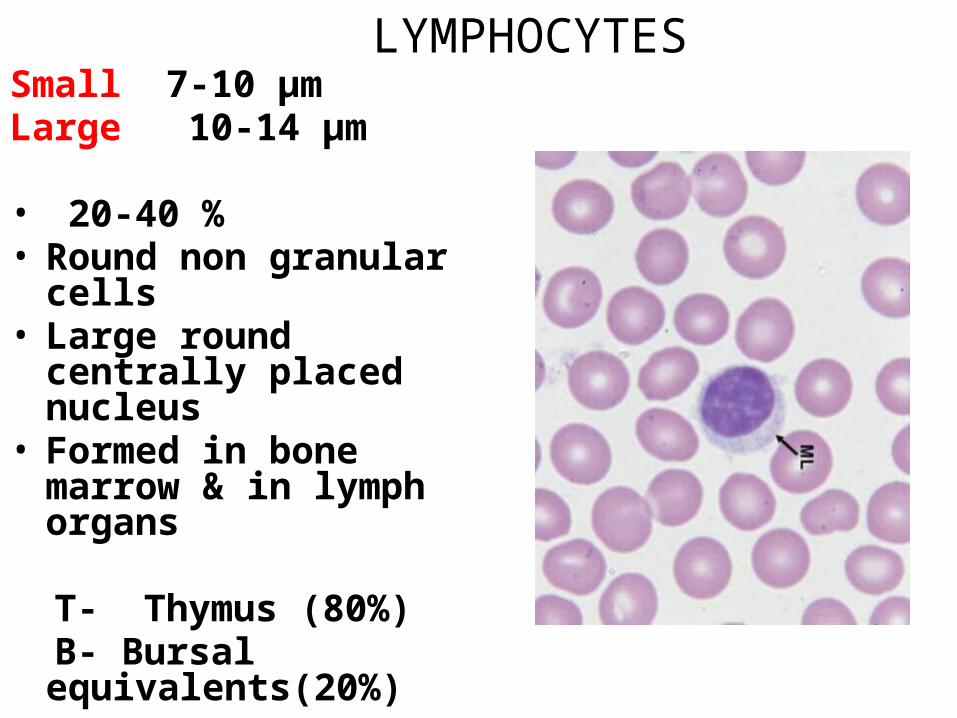
LYMPHOCYTESSmall 7-10 µmLarge 10-14 µm
• 20-40 % • Round non granular cells • Large round centrally
placed nucleus • Formed in bone marrow &
in lymph organs
T- Thymus (80%) B- Bursal equivalents(20%)
LYMPHOCYTESSite of Formation --- circulation---
TissuesLife span - weeks to months FUNCTIONS • Mediate immune responses T- Cellular Immunity B- Humoral Immunity
DEFENSIVE FUNCTIONS OF NEUTROPHIL AND MONOCYTE
• NEUTROPHIL Attack and destroy bacteria ,virus & injurious agents , Can destroy
even in circulation• MONOCYTES A little ability to kill in circulation Become macrophages (80 µm) in tissue - Actively phagocytic • PHAGOCYTOSIS – Cellular ingestion of offending agent
Basis of selection • Rough surface• No protective protein coat • Antibodies & Complement adhere to bacterial membrane
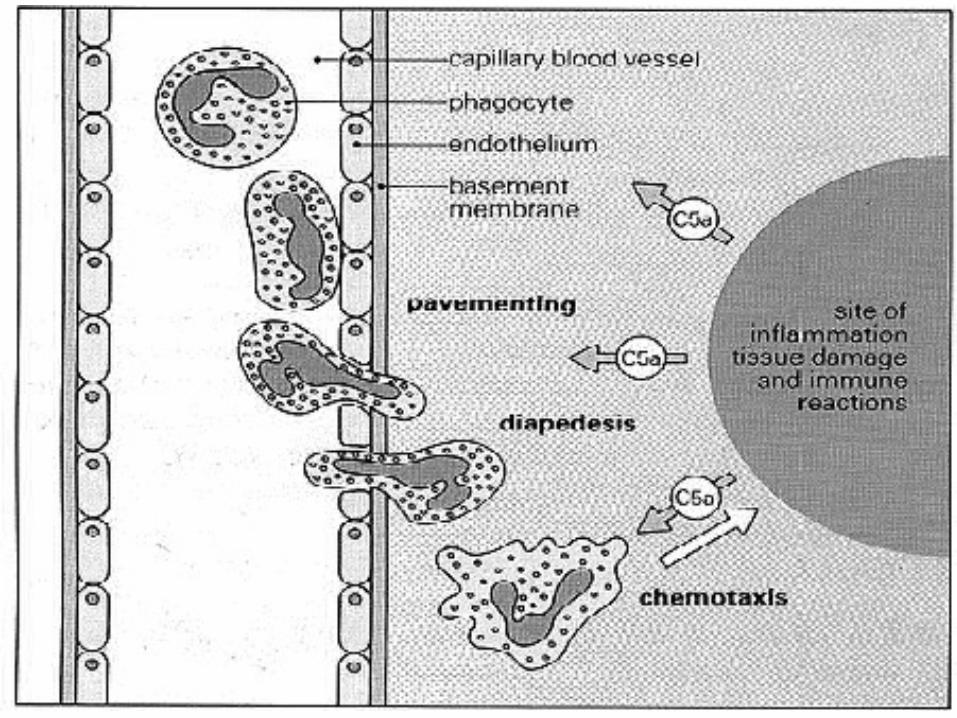
STEPS INVOLVED IN DEFENCE
Margination Diapedesis Chemotaxis Opsonisation Phagocytosis
• Phagosome formation• Degranulation• Respiratory Burst• Discharge of myeloperoxidase• Digestion by intracellular enzyme
Walling off effect
Phagocytosis (Capture, Ingest & Destroy)• Neutrophils – Microphages• Monocytes - Macrophages• Projects pseudopodia• Enclose bacteria• Invaginates• Breaks from cell membrane • Fusion of lysosome with phagosome • Exocytosis of granules • Digestion by intracellular enzymes
“Blood is still the best possible thing to have in our veins” - Woody Allen