Embed Size (px)
Citation preview

HAART for the treatment HAART for the treatment experienced patientexperienced patient
Prema Menezes PA-CPrema Menezes PA-C

Treatment FailureTreatment FailureDefinition and ReasonsDefinition and Reasons
ImmunologicImmunologic No increase in CD4 Decrease in CD4
ClinicalClinical HIV related event at
least 3 months after ART
VirologicVirologic HIV RNA >400
(24wks), >50 (48 weeks)
VirusVirus Resistant
Drug TherapyDrug Therapy Sub optimal Sub therapeutic
PatientPatient Non adherence
Managing virologic failure:Managing virologic failure: make a distinction make a distinction between limited, intermediate, and extensive between limited, intermediate, and extensive prior treatment exposure and resistanceprior treatment exposure and resistance
Goal of treatment:Goal of treatment: re-establish maximal re-establish maximal virologic suppressionvirologic suppression
March 2004: Preservation of immune function and prevention of clinical progression
May 2006: Re-suppress HIV RNA levels maximally and prevent further selection of resistance mutations
DHHS Treatment GuidelinesDHHS Treatment Guidelines

New AgentsNew Agents
Protease InhibitorsProtease Inhibitors Tipranavir Darunavir
NNRTIsNNRTIs Etravirine
Integrase InhibitorIntegrase Inhibitor Raltegravir
CCR5 InhibitorCCR5 Inhibitor Maraviroc

Limited Treatment FailureLimited Treatment Failure
Case 1: First Line Virologic FailureCase 1: First Line Virologic Failure
31 yo woman s/p bilateral tubal ligation began 31 yo woman s/p bilateral tubal ligation began [fdc ZDV/3TC] + EFV 36 months ago[fdc ZDV/3TC] + EFV 36 months ago
Initial CD4 = 162; VL = 56,000Initial CD4 = 162; VL = 56,000 After starting HIV therapy, CD4 increased to 365 After starting HIV therapy, CD4 increased to 365
and VL fell to 340 and then to < 50 c/mLand VL fell to 340 and then to < 50 c/mL Difficulty taking medication over the past 2 Difficulty taking medication over the past 2
months due to relapse of substance abusemonths due to relapse of substance abuse Now returns with weight loss and thrushNow returns with weight loss and thrush

What is your next step?What is your next step?
1.1. Obtain HIV RNA, CD4, continue therapy and Obtain HIV RNA, CD4, continue therapy and have her return within a monthhave her return within a month
2.2. Obtain HIV RNA, CD4, stop therapy and have Obtain HIV RNA, CD4, stop therapy and have her return within a monthher return within a month
3.3. Obtain a resistance testObtain a resistance test
4.4. Choice 1 and 3Choice 1 and 3
5.5. Choice 2 and 3Choice 2 and 3

GS934: Resistance Development Through Week 96
TDF + FTC(n = 244)
ZDV/3TC(n = 243)
Patients genotyped, n 14 29
Wild-type, n 4 7
Any resistance, n 10 20
EFV resistance mutations, n
10 18
M184V/I, n 2 9*
TAMs, n 0 1
K65R, n 0 0
Gallant J, et al IAC 2006. Abstract TUPE0064.Comparative trial of ZDV/3TC/EFV vs. TDF/FTC/EFV in treatment naïve patients

KLEAN: Resistance FPV/r vs. LPV/rKLEAN: Resistance FPV/r vs. LPV/r(with ABC/3TC FDC)(with ABC/3TC FDC)
Eron JJ Jr, Lancet 2006.
FPV/r, n
LPV/r, n
Confirmed virologic failuresConfirmed virologic failures 1616 2424
Unable to sequenceUnable to sequence 22 33
No treatment-emergent mutationsNo treatment-emergent mutations 99 1414
Treatment-emergent mutations
TAMs (M41M/L)TAMs (M41M/L) 00 11
3TC-associated mutations (M184I, M184V, 3TC-associated mutations (M184I, M184V, M184M/V)M184M/V) 33 44
NNRTI-associated mutations (V106V/A)NNRTI-associated mutations (V106V/A) 00 22
PI-associated mutations: all minor (I54I/L, I93I/L, PI-associated mutations: all minor (I54I/L, I93I/L, K20K/R, I62I/V)K20K/R, I62I/V) 33 22
Case 1: First Line Virologic FailureCase 1: First Line Virologic Failure
CD4 now = 98 and VL = 29,000CD4 now = 98 and VL = 29,000 Genotype reveals Genotype reveals 184V184V and and 103N103N mutations mutations ART is discontinued and PCP prophylaxis ART is discontinued and PCP prophylaxis
prescribed. The patient enters in-patient detox prescribed. The patient enters in-patient detox and 6 weeks later returns to restart HIV and 6 weeks later returns to restart HIV medications. medications.
She begins a series of adherence counseling She begins a series of adherence counseling sessionssessions
What ART to use?What ART to use?

1.1. Atazanavir + NRTIsAtazanavir + NRTIs
2.2. Atazanavir/ritonavir + NRTIsAtazanavir/ritonavir + NRTIs
3.3. Lopinavir/ritonavir + NRTIsLopinavir/ritonavir + NRTIs
4.4. Fos-Amprenavir/ritonavir + NRTIsFos-Amprenavir/ritonavir + NRTIs
5.5. [fdc ZDV/3TC/ABC] + tenofovir[fdc ZDV/3TC/ABC] + tenofovir
6.6. OtherOther
Case 1: First Line Virologic FailureCase 1: First Line Virologic Failure

If you chose NRTI + PI – which NRTIsIf you chose NRTI + PI – which NRTIs
1.1. Abacavir + 3TC or FTCAbacavir + 3TC or FTC
2.2. Abacavir + tenofovirAbacavir + tenofovir
3.3. Didanosine plus 3TC or FTCDidanosine plus 3TC or FTC
4.4. Didanosine plus tenofovirDidanosine plus tenofovir
5.5. Tenofovir + 3TC or FTCTenofovir + 3TC or FTC
6.6. Tenofovir, ZDV + 3TC or FTCTenofovir, ZDV + 3TC or FTC
7.7. Something elseSomething else
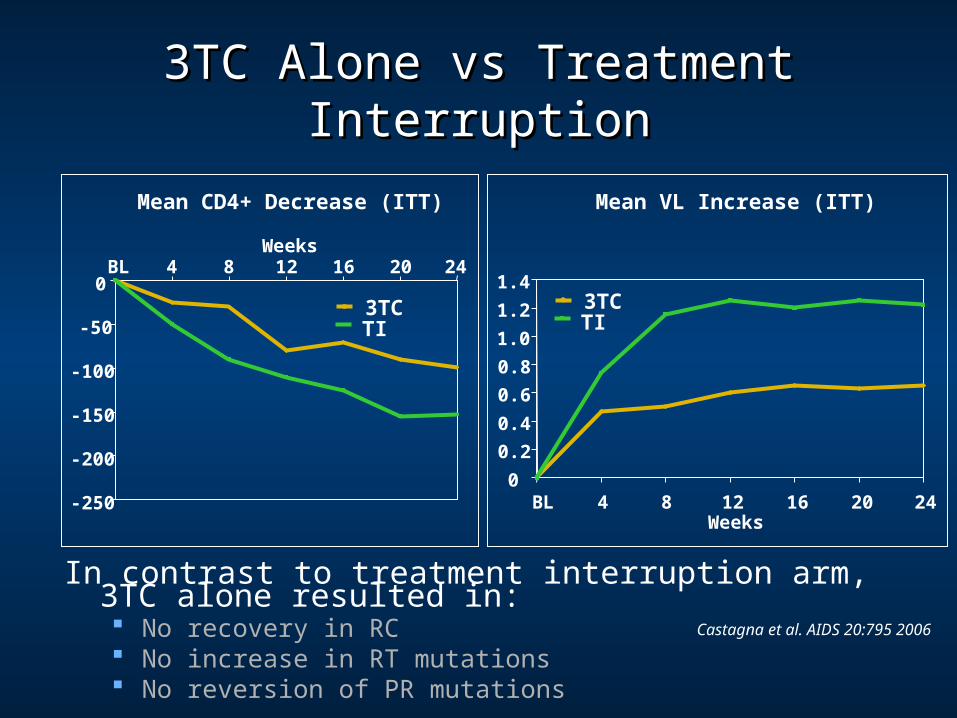
3TC Alone vs Treatment Interruption3TC Alone vs Treatment Interruption
Castagna et al. AIDS 20:795 2006
-250
-200
-150
-100
-50
0BL 4 8 12 16 20 24
Weeks
3TCTI
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
BL 4 8 12 16 20 24Weeks
3TCTI
Mean CD4+ Decrease (ITT) Mean VL Increase (ITT)
In contrast to treatment interruption arm, 3TC alone resulted in: No recovery in RC No increase in RT mutations No reversion of PR mutations

Effects of M184V on other NRTIEffects of M184V on other NRTI Increases in susceptibilityIncreases in susceptibility
Zidovudine Stavudine Tenofovir
Minimal Change or decrease in susceptibilityMinimal Change or decrease in susceptibility Abacavir Didanosine
− Both of these agents can select for M184V in vivo.

First Line Virologic FailureFirst Line Virologic Failure
Good newsGood news Lots of treatment options
ConsiderationsConsiderations Keep 3TC/FTC in new regimen Genotype Resistance appears to be limited in first
HAART failure

ART Options for Extensively ART Options for Extensively Treatment Experienced PatientsTreatment Experienced Patients
Newer AgentsNewer Agents
DarunavirDarunavir
TipranavirTipranavir

*Based on IAS-USA March 2003 at start of studies; updated to October 2004 list during studiesVL = viral load, OBR = optimized background regimen (NRTIs ± enfuvirtide [ENF])
Investigator-Investigator-selected CPI(s) selected CPI(s) + OBR (without + OBR (without
NNRTIs)NNRTIs)
POWER 1 and 2 trials: designPOWER 1 and 2 trials: design
Investigator-selected CPI(s) + OBR
TMC114/r 400/100mg qd + OBR
TMC114/r 800/100mg qd + OBR
TMC114/r 400/100mg bid + OBR
TMC114/r 600/100mg bid + OBR
• PI-, NRTI- and NNRTI-PI-, NRTI- and NNRTI-experiencedexperienced
• ≥≥1 PI mutation1 PI mutation* *
• PI-based regimenPI-based regimen
• VL >1,000 copies/mLVL >1,000 copies/mL
Randomization
• The highest dose of TMC114/r (600/100mg bid) provided the greatest virologic response in the Week 24 analysis and is the selected dose for treatment-experienced patients
• The combined 48-week efficacy and safety interim analysis at this dose versus CPI(s) is reported here
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104

POWER 1 and 2: BL characteristicsPOWER 1 and 2: BL characteristicsTMC114/r TMC114/r
600/100mg bid600/100mg bidn=131n=131
CPI(s)CPI(s)n=124n=124
DemographicsDemographicsGender (% male)Gender (% male)Mean age (years)Mean age (years)
89894444
88884444
Disease characteristicsDisease characteristicsCDC class C (%)CDC class C (%)Mean duration of infection (years)Mean duration of infection (years)Mean VL (logMean VL (log1010 copies/mL; SD) copies/mL; SD)Median CD4 count (cells/mmMedian CD4 count (cells/mm33; range); range)
363612.012.0
4.61 (0.69)4.61 (0.69)153 (3–776)153 (3–776)
434312.912.9
4.49 (0.78)4.49 (0.78)163 (3–1,274)163 (3–1,274)
Previous ARV experiencePrevious ARV experienceMean duration (months; SD)Mean duration (months; SD)
NRTINRTINNRTINNRTIPIPIFusion inhibitor (ENF)Fusion inhibitor (ENF)
100 (48)100 (48)28 (24)28 (24)65 (29)65 (29)14 (11)14 (11)
106 (45)106 (45)23 (15)23 (15)65 (28)65 (28)11 (9)11 (9)
Genotypic and phenotypic informationGenotypic and phenotypic informationMedian primary PI mutations* (n; range)Median primary PI mutations* (n; range)Median PI resistance-associated mutations* (n; range)Median PI resistance-associated mutations* (n; range)≥≥1 sensitive1 sensitive†† PI available (%) PI available (%) ≥≥1 sensitive1 sensitive†† NRTI in OBR (%) NRTI in OBR (%)
3 (0–5)3 (0–5)8 (0–12)8 (0–12)
36367272
3 (0–5)3 (0–5)8 (1–13)8 (1–13)
39397373
ARV = antiretroviral; SD = standard deviation*IAS-USA October 2004, †susceptibility was determined by Antivirogram®
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104

POWER 1 and 2: patients with VL <50 copies/mL POWER 1 and 2: patients with VL <50 copies/mL over time to Week 48 (ITT-TLOVR)over time to Week 48 (ITT-TLOVR)
TMC114/r 600/100mg bidCPI(s)
45%*(n=59/131)
12% (n=15/124)
46%* (n=50/110)
10% (n=12/120)
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48Weeks
Pat
ient
s (%
)
12
*p<0.001 vs CPI(s)ITT = intent-to-treat, TLOVR = time to loss of virologic response
Not all patients had reached Week 48 at the time of analysis; patients who had not reached Week 48 were censored at their last available visit
TMC114/r n= 131 131 131 130 120 110CPI(s) n= 124 124 124 124 121 120
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104

POWER 1 and 2: virologic response defined as VL POWER 1 and 2: virologic response defined as VL
<50 copies/mL by BL subgroups at Week 48<50 copies/mL by BL subgroups at Week 48 (ITT-TLOVR)(ITT-TLOVR)P
atie
nts
(%
)
70
60
50
40
30
20
10
0ENF used
(naïve)ENF used
(non-naïve)ENF
not used
TMC114/r 600/100mg bidCPI(s)
21
/36
1/1
5 7/7
0
0 sensitive ARV
in OBR
≥1 sensitive ARV
in OBR5
/25
0/1
8
44
/82
11
/10
0
4/3
5 2/1
3
27
/61
ARV = antiretroviral drug; OBR = optimized background regimen; ENF = enfuvirtide.Use of ENF was not randomized in POWER 1 and 2.
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104
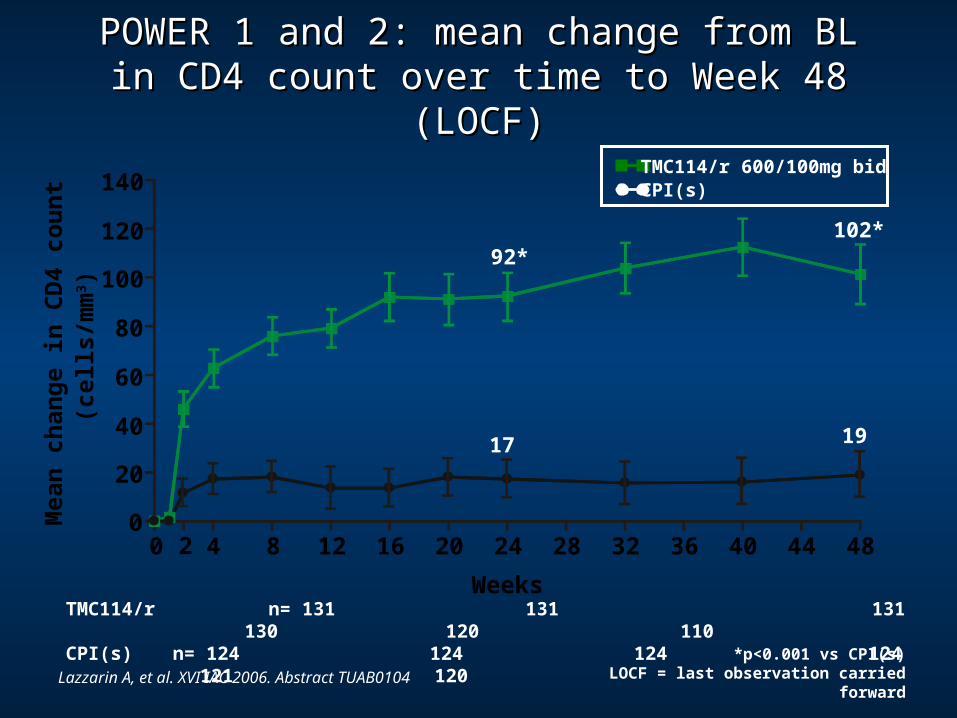
POWER 1 and 2: mean change from BL in CD4 POWER 1 and 2: mean change from BL in CD4 count over time to Week 48 (LOCF)count over time to Week 48 (LOCF)
TMC114/r 600/100mg bidCPI(s)
92*102*
17 19
*p<0.001 vs CPI(s)LOCF = last observation carried forward
2
20
40
60
80
100
120
140
0 4 8 12 16 20 24 28 32 36 40 44 48
Weeks
Mea
n c
han
ge
in C
D4
cou
nt
(cel
ls/m
m3 )
0
TMC114/r n= 131 131 131 130 120 110CPI(s) n= 124 124 124 124 121 120
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104

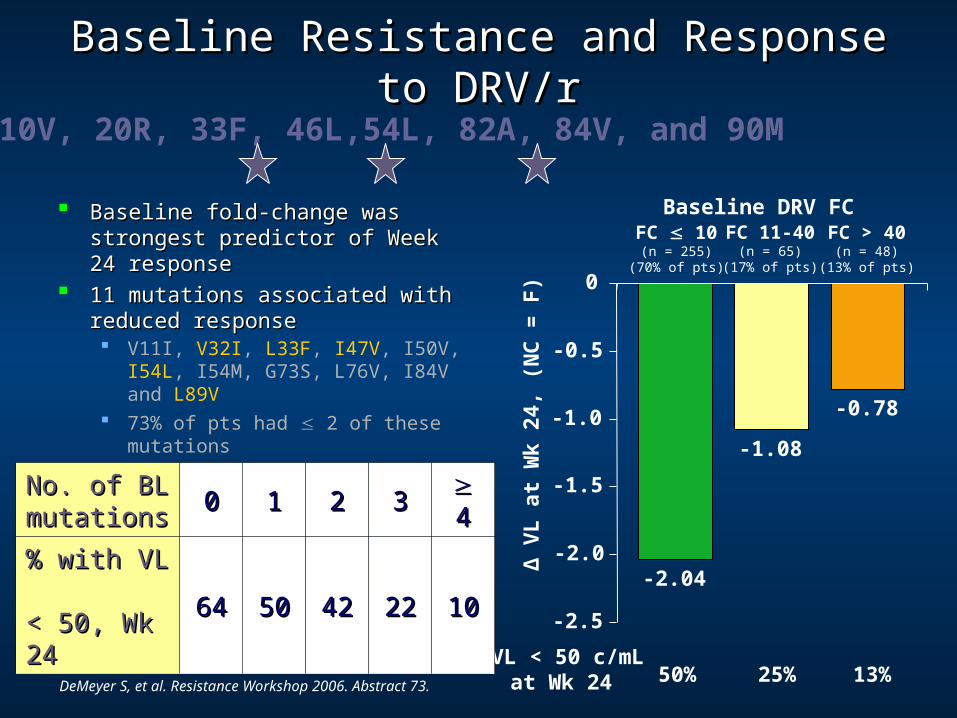
Baseline Resistance and Response to DRV/rBaseline Resistance and Response to DRV/r
Baseline fold-change was strongest Baseline fold-change was strongest predictor of Week 24 responsepredictor of Week 24 response
11 mutations associated with 11 mutations associated with reduced responsereduced response V11I, V32I, L33F, I47V, I50V,
I54L, I54M, G73S, L76V, I84V and L89V
73% of pts had 2 of these mutations
DeMeyer S, et al. Resistance Workshop 2006. Abstract 73.
Δ V
L a
t W
k 24
, (N
C =
F)
FC 10(n = 255)
(70% of pts)
FC 11-40(n = 65)
(17% of pts)
FC > 40(n = 48)
(13% of pts)
VL < 50 c/mLat Wk 24 50% 25% 13%
Baseline DRV FC
No. of BL No. of BL mutationsmutations 00 11 22 33 44
% with VL % with VL < 50, Wk 24< 50, Wk 24 6464 5050 4242 2222 1010 -2.04
-1.08
-0.78
-2.5
-2.0
-1.5
-1.0
-0.5
0

POWER 1 and 2: observed incidence of the POWER 1 and 2: observed incidence of the most common treatment-emergent AEs* most common treatment-emergent AEs*
during treatment, regardless of severity and during treatment, regardless of severity and causalitycausality
*AEs = adverse events reported in ≥10% of patients and excluding ENF-associated injection site reaction (TMC114/r: 28%; CPI: 22%)
80
70
60
50
40
30
20
10
0Diarrhea Nausea Headache Naso-
pharyngitisFatigue
Pat
ien
ts (
%)
Pyrexia
TMC114/r 600/100mg bidCPI(s)
Upper respiratory
tract infection
Herpes simplex
Lazzarin A, et al. XVI IAC 2006. Abstract TUAB0104

TITANTITAN DRV/RTV vs LPV/RTV in DRV/RTV vs LPV/RTV in
Tx-Experienced, LPV-Naive PatientsTx-Experienced, LPV-Naive Patients
Intermediate treatment experience Intermediate treatment experience Stratified by treatment site, NNRTI in OBR, HIV Stratified by treatment site, NNRTI in OBR, HIV
RNA > or < 50,000 c/mLRNA > or < 50,000 c/mL
Darunavir/ritonavir met criteria for superiority to Darunavir/ritonavir met criteria for superiority to lopinavir/ritonavir in proportions with HIV-1 RNA lopinavir/ritonavir in proportions with HIV-1 RNA < 400 copies/mL and < 50 copies/mL at week 48< 400 copies/mL and < 50 copies/mL at week 48
Safety comparable between darunavir/ritonavir Safety comparable between darunavir/ritonavir and lopinavir/ritonavirand lopinavir/ritonavir

The Randomized Evaluation of The Randomized Evaluation of Strategic Intervention in Multidrug Strategic Intervention in Multidrug
Resistant Patients With Resistant Patients With Tipranavir (RESIST) Tipranavir (RESIST)

Proportion of patients with viral load <400 and <50 copies/ml at week 96
Resist 1 and 2 – 96 weeks

Resist 1 and 2 – 96 weeks
Proportion of patients who took Enfuvirtide as a new drug and achieved virologic suppression.


TPV/r (%) CPI/r (%)
Grade 3/4 AST 6.1 1.8
Grade 3/4 ALT 9.7 4.2
Grade 3/4 total cholesterol 2.1 0.4
Grade 3/4 triglycerides 24.9 13.0
Safety - laboratory Safety - laboratory abnormalitiesabnormalities
Patients with Grade 3/4 elevations in liver enzymes or lipids Patients with Grade 3/4 elevations in liver enzymes or lipids were able to continue TPV/r therapy without developing were able to continue TPV/r therapy without developing clinical AEsclinical AEs

Highly Treatment ExperiencedPatients

Highly Treatment ExperiencedHighly Treatment Experienced
48 yo white man HIV + since 1991 (CD4 180)48 yo white man HIV + since 1991 (CD4 180) Received ZDV from 1994 to 1996, added 3TC Received ZDV from 1994 to 1996, added 3TC
then indinavirthen indinavir VL on this regimen was initially BDL and CD4 VL on this regimen was initially BDL and CD4
rose to 300 cells over two years. rose to 300 cells over two years. VL rose to 5,600 then 10,100, CD4 was 390.VL rose to 5,600 then 10,100, CD4 was 390. In 2000 treatment was interrupted VL peaked at In 2000 treatment was interrupted VL peaked at
386,000 and CD4 fell to 220386,000 and CD4 fell to 220

Case: Multi-drug ResistanceCase: Multi-drug Resistance
Over several years he was on a series of Over several years he was on a series of regimens:regimens: EFV, SQV/RTV, d4T Abacavir, ddI, LPV/r TDF, FTC, LPV/r plus SQV HIV RNA rebound was eventually observed on each regimen
He feels well and has had no AIDS defining He feels well and has had no AIDS defining illness. His current CD4 is 310 and his VL illness. His current CD4 is 310 and his VL repeated several times is between 10,000 and repeated several times is between 10,000 and 15,000 on therapy15,000 on therapy

Case: Multi-drug ResistanceCase: Multi-drug Resistance
Given long treatment history with only Given long treatment history with only intermittent suppression of HIV RNA to BDL you intermittent suppression of HIV RNA to BDL you order a genotypeorder a genotype This is the test available to you
RT mutations include:RT mutations include: 41L, 74V, 118I, 184V, 215Y and 219Q
Protease mutations include:Protease mutations include: 10V, 20R, 33F, 46L,54V, 82A, 84V and 90M

Case: Multi-drug ResistanceCase: Multi-drug Resistance
What will you do at this point?What will you do at this point?1. Change to > 1 NRTI, tipranavir/r and enfuvirtide
2. Change to > 1 NRTI, darunavir/r and enfuvirtide
3. Interrupt therapy and after 6 months begin > 1 NRTI, darunavir/r and enfuvirtide
4. Continue current therapy
5. Holding regimen

Need to Know Likelihood of Need to Know Likelihood of SuccessSuccess
CD4 310, clinically stableCD4 310, clinically stable

Let’s Look at GenotypeLet’s Look at Genotype
RT mutations include:RT mutations include:41L, 74V, 118I, 184V, 215Y and 219Resistance predicted to 3TC, FTC, ddI, ABC,
ZDVIntermediate activity to TDF and d4T
Protease mutations include:Protease mutations include:10V, 20R, 33F, 46L,54L, 82A, 84V and 90M

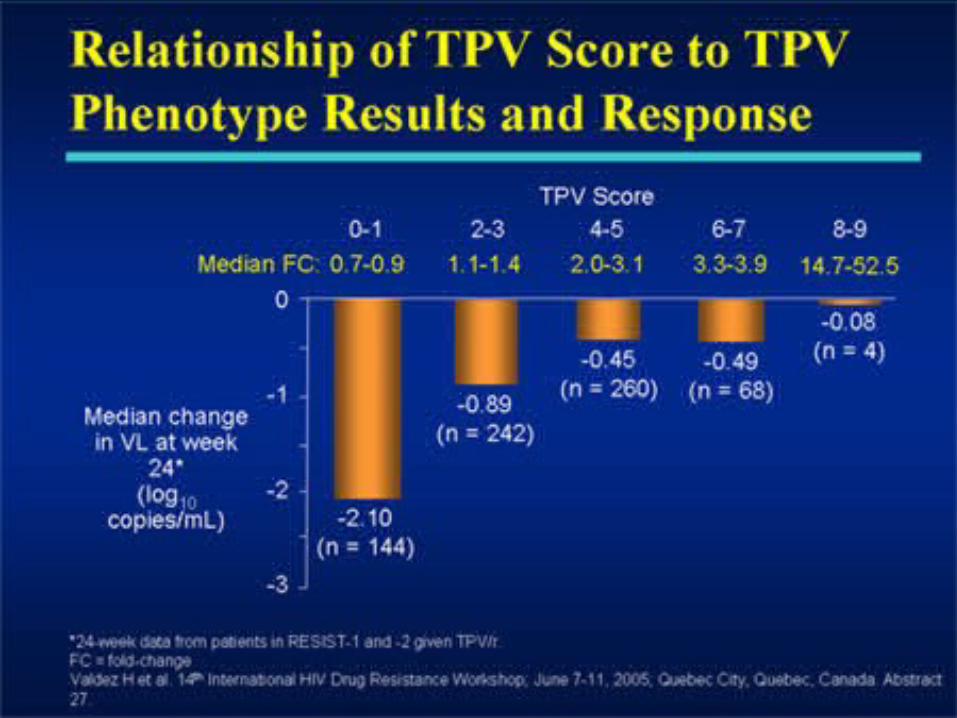
TPV Score and Treatment ResponseTPV Score and Treatment Response
Valdez H, et al. Resistance Workshop 2005. Abstract 27.
-2
-1
0
-3
Med
ian
Ch
ang
e in
VL
at
Wk
24*
(lo
g10
co
pie
s/m
L)
0-1 2-3 4-5 6-7 8-9
-2.10(n = 144)
-0.89(n = 242)
-0.45(n = 260)
-0.49(n = 68)
-0.08(n = 4)
TPV Score
Median FC: 0.7-0.9 1.1-1.4 2.0-3.1 3.3-3.9 14.7-52.5
*24-week data from patients in RESIST-1 and -2 given TPV/r
TPV Score Mutations10V, 13V, 20M/R/V, 33F, 35G,
36I, 43T, 46L, 47V, 54A/M/V, 58E, 69K, 74P, 82L/T, 83D, 84V
10V, 20R, 33F, 46L,54L, 82A, 84V, and 90M
Baseline Resistance and Response to DRV/rBaseline Resistance and Response to DRV/r
Baseline fold-change was strongest Baseline fold-change was strongest predictor of Week 24 responsepredictor of Week 24 response
11 mutations associated with 11 mutations associated with reduced responsereduced response V11I, V32I, L33F, I47V, I50V, I54L,
I54M, G73S, L76V, I84V and L89V 73% of pts had 2 of these
mutations
DeMeyer S, et al. Resistance Workshop 2006. Abstract 73.
Δ V
L a
t W
k 24
, (N
C =
F)
FC 10(n = 255)
(70% of pts)
FC 11-40(n = 65)
(17% of pts)
FC > 40(n = 48)
(13% of pts)
VL < 50 c/mLat Wk 24 50% 25% 13%
Baseline DRV FC
No. of BL No. of BL mutationsmutations 00 11 22 33 44
% with VL % with VL < 50, Wk 24< 50, Wk 24 6464 5050 4242 2222 1010 -2.04
-1.08
-0.78
-2.5
-2.0
-1.5
-1.0
-0.5
0
10V, 20R, 33F, 46L,54L, 82A, 84V, and 90M
Multi-Drug ResistanceMulti-Drug Resistance This case illustrates several points to This case illustrates several points to
consider when making the difficult decision consider when making the difficult decision of when to switchof when to switch
This patient is in no clinical danger.This patient is in no clinical danger. His CD4 cell count is above 300 His viral load is over 1 log10 lower than a peak off
therapy. He has had no AIDS defining illness and feels well
On the other hand his current therapy is On the other hand his current therapy is not optimal with sustained viral replicationnot optimal with sustained viral replication Continued current therapy may lead to CD4 cell
decline and further accumulation of resistance mutations

Case: Multi-drug ResistanceCase: Multi-drug Resistance There is no clinical urgency; what are treatment There is no clinical urgency; what are treatment
options?options? He is naïve to T-20 therefore likely very active initially
− T-20 low barrier to resistance; incomplete suppression leads to rapid resistance evolution
He has no NNRTI mutations− By history he had previous viral rebound while on EFV− NNRTI may add modest activity, − NRTI will likely have modest ADDITIONAL activity
There are substantial PI mutations limiting PI options
− He has 5 TPV-associated mutations decreasing the likelihood of a sustained response
− He has 3 DRV mutations which will impact activity
Should He Wait for New Should He Wait for New Agents?Agents?
How quickly will new mutations How quickly will new mutations evolve?evolve?

Risk of Delayed Switch on Stable HAARTRisk of Delayed Switch on Stable HAART
SCOPE cohort of ART-experienced SCOPE cohort of ART-experienced subjects (nsubjects (n = 106)= 106)[1][1]
Stable HAART for 120 days
HIV-1 RNA > 1000 c/mL
1 resistance mutation
Resistance testing every 4 mos until HAART modification
Emergence of new mutns at 1 yrEmergence of new mutns at 1 yr Any: 44% (95% CI: 33%-56%)
NAMs: 23% (95% CI: 15%-34%)
PI: 18% (95% CI: 9%-34%)
Those with persistent viremia on Those with persistent viremia on HAART run risk of limiting future HAART run risk of limiting future treatment optionstreatment options
Other studies show similar resultsOther studies show similar results[2-4][2-4]
1. Hatano H, et al. CROI 2006. Abstract 615. 2. Lafeuillade A, et al. IAC 2004. Abstract WeOrB1293. 3. Margot NA, et al. JAIDS. 2003;33:15-21. 4. Napravnik S, et al. JAIDS. 2005;40:34-40.
Pro
po
rtio
n W
ith
ou
t
New
Mu
tati
on
1 new major PI mutation1 new NRTI mutation*Any new mutation
Number of available antiretrovirals from the following: ZDV,
3TC, ddI, ABC,TDF, EFV, IDV, NFV, SQV, RTV, APV, LPV 0
0.25
0.50
0.75
1.00
0 4 8 12 16 20 24Time (Mos)
Time to loss of 1 drug equivalent
0 4 8 12 16 20 24
*PI-treated subjects (n = 71)0
0.25
0.50
0.75
1.00
Pro
po
rtio
n W
ith
ou
t
Lo
ss o
f 1
Dru
g
Case 1Case 1
Patient now has CD4 cell count of 120Patient now has CD4 cell count of 120 VL is 15,000VL is 15,000 Repeat Genotype – virtual phenotype Repeat Genotype – virtual phenotype
show no new mutationsshow no new mutations DRV fold change = 45 (cut-offs 3.4 – 96.8) TPV fold change = 4.0 (cut-offs 1.2 – 5.4) Intermediate susceptibility to TDF resistant to all NRTI No NNRTI mutations (failed EFV in the past)

Case 1Case 1
If you were to start the patient on new drugs If you were to start the patient on new drugs which would you use?which would you use?A. Maraviroc
B. Raltegravir
C. Etravirine
D. Raltegravir/Etravirine
E. Maraviroc/Etravirine
F. Maraviroc/Raltegravir

HIV-infected patients with VF on current HAART regimen,
history of ≥ 1 NNRTI resistance mutations, ≥ 3 primary PI mutations,
HIV-1 RNA > 5000 copies/mL
(DUET-1: N = 612; DUET-2: N = 591)
Placebo+ DRV/RTV-containing OBR*
(n = 604)
Etravirine 200 mg BID+ DRV/RTV-containing OBR*
(n = 599)
Week 48
*Investigator-selected OBR to consist of DRV/RTV (600/100 mg/mL) + ≥ 2 NRTIs ± enfuvirtide.†Planned Week 24 analysis: primary endpoint HIV-1 RNA < 50 copies/mL (TLOVR).
Week 24†
DUET-1 and -2: Etravirine + DRV/RTV-Containing OBR Phase III Trials
Madruga JV, et al. Lancet. 2007;370:29-38. Lazzarin A, et al. Lancet. 2007;370:39-48. Mills A, et al. IAS 2007. Abstract WESS204.1. Katlama C, et al. IAS 2007. Abstract WESS204.2. Cahn P, et al. ICAAC 2007. Abstract H-717.

DUET-1 and -2: Pooled Virologic and DUET-1 and -2: Pooled Virologic and Immunologic Responses Immunologic Responses
Outcome at Week 24 Etravirine(n = 599)
Placebo (n = 604)
P Value
HIV-1 RNA < 50 copies/mL, %
59 41 < .0001
Mean change in HIV-1 RNA from baseline, log10
copies/mL-2.4 -1.7 < .0001
Mean change in CD4+ cell count from baseline, cells/mm3
+86 +67 < .0001
In patients using enfuvirtide for the first time (n = 201), the difference between treatment In patients using enfuvirtide for the first time (n = 201), the difference between treatment arms (67% and 62% for etravirine vs placebo, respectively) was not significant (arms (67% and 62% for etravirine vs placebo, respectively) was not significant (P P = .427)= .427)
Cahn P, et al. ICAAC 2007. Abstract H-717.

DUET-1 and -2: Response Based on DUET-1 and -2: Response Based on Active Agents in OBR Active Agents in OBR
Cahn P, et al. ICAAC 2007. Abstract H-717.
0
20
40
60
80
100
HIV
-1 R
NA
< 5
0 co
pie
s/m
L a
t W
eek
24 (
%)
45
8
60
74
30
67
Etravirine + OBR Placebo + OBR
n = 88 25725821119991
No. of Fully Active Agents in OBR (assessed by PSS)0 1 ≥ 2

DUET-1 and -2: BL ETR Mutations and DUET-1 and -2: BL ETR Mutations and Virologic Response at Week 24Virologic Response at Week 24
0 1 2 3
Pat
ien
ts W
ith
HIV
-1
RN
A <
50
cop
ies/
mL
(%
)
0
102030
4050607080
90100
4 5
No. of BL ETR Mutations
Patients (%) 40 30 16 8 5 1
13 mutations associated with ETR resistance
V90I A98G
L100I K101E/P
V106I V179D/F
Y181C/I/V G190A/S
Presence of ≥ 3 ETR mutations associated with response similar to placebo + OBR
– 70% of patients had 0 or 1 ETR resistance mutations at BL
– 14% of patients had ≥ 3 ETR resistance mutations at BL
– Response diminished by ~ 20% in presence of 1 or 2 mutations
Katlama C, et al. IAS 2007. Abstract WESS204.2.
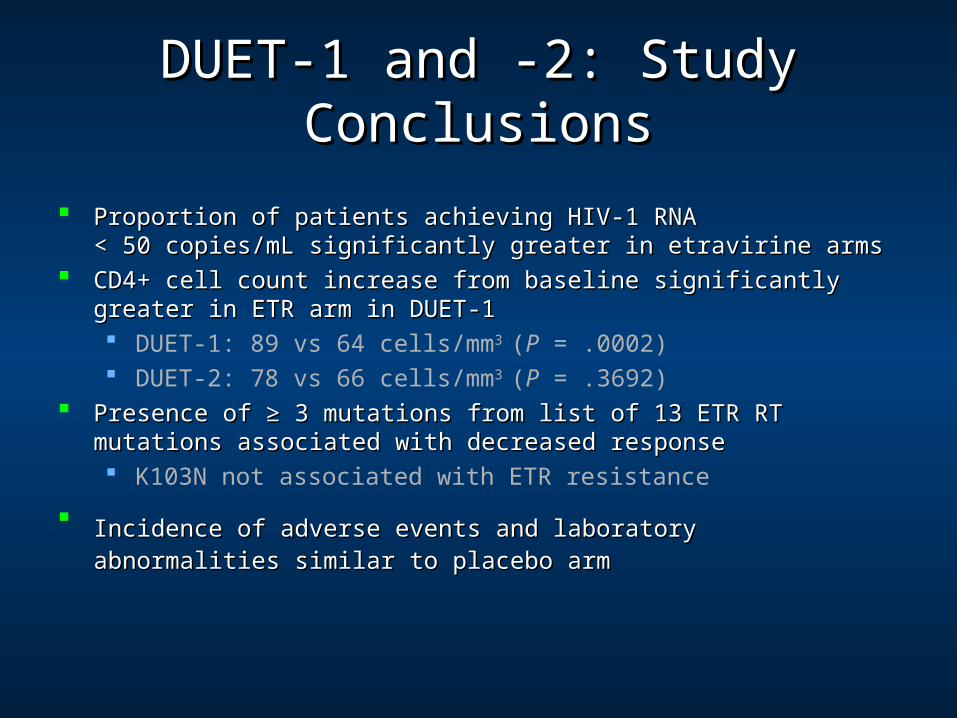
Proportion of patients achieving HIV-1 RNA Proportion of patients achieving HIV-1 RNA < 50 copies/mL significantly greater in etravirine arms< 50 copies/mL significantly greater in etravirine arms
CD4+ cell count increase from baseline significantly greater in ETR arm in CD4+ cell count increase from baseline significantly greater in ETR arm in DUET-1DUET-1 DUET-1: 89 vs 64 cells/mm3 (P = .0002) DUET-2: 78 vs 66 cells/mm3 (P = .3692)
Presence of ≥ 3 mutations from list of 13 ETR RT mutations associated with Presence of ≥ 3 mutations from list of 13 ETR RT mutations associated with decreased responsedecreased response K103N not associated with ETR resistance
Incidence of adverse events and laboratoryIncidence of adverse events and laboratory abnormalities similar to placebo abnormalities similar to placebo armarm
DUET-1 and -2: Study ConclusionsDUET-1 and -2: Study Conclusions
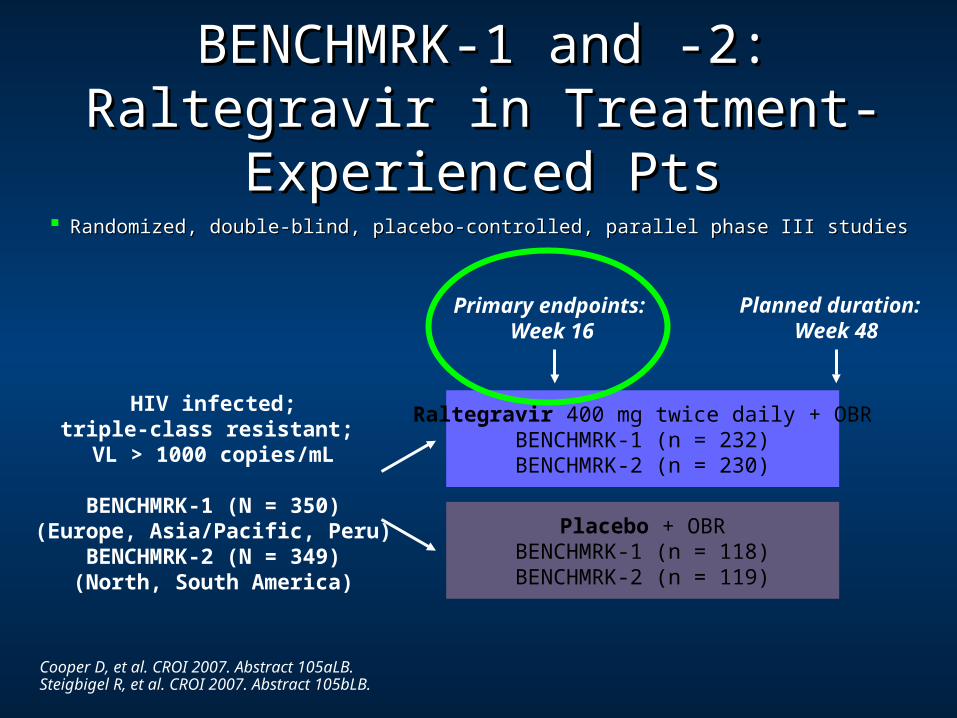
BENCHMRK-1 and -2: Raltegravir in BENCHMRK-1 and -2: Raltegravir in Treatment-Experienced PtsTreatment-Experienced Pts
Cooper D, et al. CROI 2007. Abstract 105aLB. Steigbigel R, et al. CROI 2007. Abstract 105bLB.
Randomized, double-blind, placebo-controlled, parallel phase III studiesRandomized, double-blind, placebo-controlled, parallel phase III studies
Raltegravir 400 mg twice daily + OBRBENCHMRK-1 (n = 232)BENCHMRK-2 (n = 230)
Placebo + OBRBENCHMRK-1 (n = 118)BENCHMRK-2 (n = 119)
HIV infected;triple-class resistant; VL > 1000 copies/mL
BENCHMRK-1 (N = 350)(Europe, Asia/Pacific, Peru)
BENCHMRK-2 (N = 349)(North, South America)
Primary endpoints: Week 16
Planned duration: Week 48

Benchmark 1 and 2Patient Disposition at study entry

BENCHMRK 1 and 2: HIV-1 RNA < 50 BENCHMRK 1 and 2: HIV-1 RNA < 50 copies/mL (ITT, NC = F)copies/mL (ITT, NC = F)
Cooper D, et al. CROI 2007. Abstract 105aLB. Steigbigel R, et al. CROI 2007. Abstract 105bLB.
P < .001 at Week 16
Per
cen
t o
f P
ati
en
ts w
ith
HIV
RN
A <
50 C
op
ies/
mL
P < .001 at Week 16
BENCHMRK-2
Weeks
0 2 4 8 12 16 240
20
40
60
80
100
0 2 4 8 12 16 240
20
40
60
80
100BENCHMRK-1
Weeks
61%
33%
62%
36%
Raltegravir + OBR Placebo + OBR

BENCHMRK 1 and 2: HIV-1 RNA < 400 BENCHMRK 1 and 2: HIV-1 RNA < 400 c/mL at Wk 16 by Agents in OBRc/mL at Wk 16 by Agents in OBR
Cooper D, et al. CROI 2007. Abstract 105aLB. Steigbigel R, et al. CROI 2007. Abstract 105bLB.
+ : First use in OBR– : No use in OBR
Overall Efficacy Data
––
% of Patients
0 20 40 60 80 100
n
447230
Efficacy by Agents in OBR
Enfuvirtide Darunavir
+
+
+
+
–
–
879844
23
639042
24
559080
47
2974191
90
7943
Raltegravir + OBR Placebo + OBR

BENCHMRK 1 and 2: HIV-1 RNA < 400 BENCHMRK 1 and 2: HIV-1 RNA < 400 c/mL at Wk 16 by PSS/GSS of OBRc/mL at Wk 16 by PSS/GSS of OBR
Cooper D, et al. CROI 2007. Abstract 105aLB. Steigbigel R, et al. CROI 2007. Abstract 105bLB.
(PSS)
0
1
2 or more
(GSS)
0
1
2 or more
Overall Efficacy Data
% of Patients
615
6244
7641
14168
8757
222110
5710
11163
8543
17093
8971
15970
0 20 40 60 80 100
n
447230
7943
Raltegravir + OBR Placebo + OBR
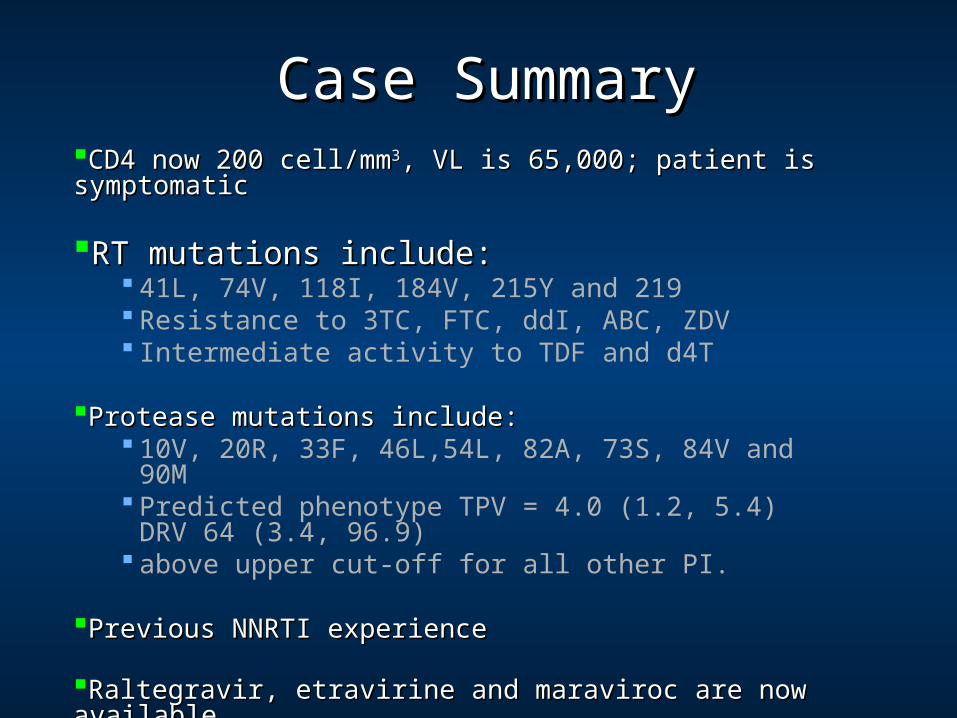
Case SummaryCase SummaryCD4 now 200 cell/mmCD4 now 200 cell/mm33, VL is 65,000; patient is symptomatic , VL is 65,000; patient is symptomatic RT mutations include:RT mutations include:
41L, 74V, 118I, 184V, 215Y and 219 Resistance to 3TC, FTC, ddI, ABC, ZDV Intermediate activity to TDF and d4T
Protease mutations include:Protease mutations include: 10V, 20R, 33F, 46L,54L, 82A, 73S, 84V and 90M Predicted phenotype TPV = 4.0 (1.2, 5.4) DRV 64 (3.4,
96.9) above upper cut-off for all other PI.
Previous NNRTI experiencePrevious NNRTI experience
Raltegravir, etravirine and maraviroc are now available.Raltegravir, etravirine and maraviroc are now available. Entry phenotype is dual-mixed

SummarySummaryTreatment experienced patientsTreatment experienced patients
Re-suppress HIV RNA levels maximally Re-suppress HIV RNA levels maximally and prevent further selection of resistance and prevent further selection of resistance mutationsmutations
Need to know likelihood of successNeed to know likelihood of success Must have at least two active drugsMust have at least two active drugs

World AIDS Day 2006

What Is the “Resistance Penalty” of What Is the “Resistance Penalty” of Continued Nonsuppressive Therapy?Continued Nonsuppressive Therapy?
Studies of resistance accumulation in states of Studies of resistance accumulation in states of “incomplete viral suppression”“incomplete viral suppression” 68% with new mutations after median of 22 mos[1]
33% with new TAMs, 2% K65R during 96 wks of FU[2]
60% with new mutations after median of 9.3 mos, but no shift on virtual phenotype[3]
Studies lack results of subsequent switches Studies lack results of subsequent switches No fully powered randomized studies of early vs deferred No fully powered randomized studies of early vs deferred
switchingswitching
1. Lafeuillade A, et al. IAC 2004. Abstract WeOrB1293. 2. Margot NA, et al. J Acquir Immune Defic Syndr. 2003;33:15-21. 3. Napravnik S, et al. J Acquir Immune Defic Syndr. 2005;40:34-40.