Embed Size (px)
Citation preview
Hem philiaTODAY
N e w s m a g a z i n e o f t h e C a n a d i a n H e m o p h i l i a S o c i e t y • S p r i n g 2 0 0 3 • V o l 3 8 N o 1
Hem philiaTODAY w w w . h e m o p h i l i a . c a
FOCUS ON BLEEDING DISORDERS SEE P.6
2003 is a landmark year for the Canadian HemophiliaSociety. In 1953, people with hemophilia and theirfamily members and caregivers got together to create anorganization that would lead to a better quality of life for
Canadian hemophiliacs and also to some of the bestmedical treatment in the world. Celebrations to
highlight our 50th anniversary will include a commemorative
book, a public exhibit on the history of hemophilia and the
CHS, a research symposium as well as a medical symposium, a poster
exhibit of volunteers over the years and, finally, a celebratory banquet
with a few surprises in store. These activities will all be taking place in Montreal on
May 8-11TH, 2003. You’ll find details
on how you can take
part in these cele-
brations on page 17 of this issue.
Don’t miss out on this chance to
join the biggest hemophilia-family gathering
ever and to commemorate 50 years
of tragedy and triumph in the care
of people with bleeding disorders.
50 YEARS TO REMEMBER
I N S I D E
EDITOR’S KEYBOARD......................................................2PRESIDENT’S MESSAGE ................................................3NEWS UPDATE ................................................................4FOCUS ON BLEEDING DISORDERS....Introduction ....................................................................6....Von Willebrand Disease ....................................................6....Five people… Five bleeding disorders ................................7....Bleeding Disorders at a Glance ......................................10
FEATURES....Families in Touch ..........................................................11....Chapter Spotlight ..........................................................11....Medical News: Pain ......................................................12....The Blood Factor ..........................................................13....The Global Perspective ..................................................15....The Female Factor ........................................................16
CHS FIFTIETH ANNIVERSARY....CHS 50th Anniversary Celebrations ................................17....1st Canadian State of the Art Conference on ....von Willebrand Disease ..................................................18....Frank Schnabel: Founder of the CHS and WFH ................19....50th Anniversary Registration Form ................................20

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 32
Hem hiliaTODAY
FALL 2002 • VOL 37 • NO 3
Hemophilia Today625 President Kennedy Avenue, Suite 1210
Montreal, Quebec H3A 1K2www.hemophilia.ca
Phone: (514) 848-0503Fax: (514) 848-9661
Toll Free: 1(800)668-2686
Hemophilia Today is the official publication of the Canadian Hemophilia Society (CHS)
and appears three times yearly.
The Canadian Hemophilia Society exists toimprove the quality of life for all persons with
hemophilia and other inherited bleedingdisorders and to find a cure.
The purpose of Hemophilia Today is to inform the hemophiliaand bleeding disorders community about current news andrelevant issues. Publications and speakers may freely use the
information contained herein, provided a credit lineincluding the volume number of the issue is given. Opinions
expressed are those of the writers and do not necessarilyreflect the views of the CHS.
The CHS consults medical professionals before distributingany medical information. However, the CHS does not
practice medicine and in no circumstances recommendsparticular treatments for specific individuals. In all cases, it is
recommended that individuals consult a physician beforepursuing any course of treatment.
Brand names of treatment products are provided forinformation only. They are not an endorsement of a
particular product or company by the writers or editors.
EDITORFrançois Laroche
PRESIDENTTom Alloway, Ph.D.
EXECUTIVE DIRECTORDaniel Lapointe
EDITORIAL COMMITTEEHélène Bourgaize
Clare CecchiniFrançois Laroche
David PagePatricia Stewart
CONTRIBUTING WRITERSTom Alloway, Ph.D.
Clare CecchiniKaren CreightonFranços Laroche
David Lillicrap, MDDavid Page
Jeff RicePatricia Stewart
Eric StolteMarion Stolte
Candace TerpstraPam Wilton
PRODUCTION COORDINATORDavid Page
PRODUCTION ASSISTANT AND FRENCH VERSION COORDINATOR
Hélène Bourgaize
GRAPHIC DESIGNPaul Rosenbaum
TRANSLATORSNormand LatulippeHélène Morissette
PRINTINGIntegria Inc.
Four days of information,testimonials and celebrationsawait attendees at the
Canadian Hemophilia Society’s 50TH
anniversary, May 8 to 11. Exhibits, amedical research symposium, acommemorative book, a state-of-the-art conference on vonWillebrand Disease and asumptuous banquet are just someof the activities featured during thefour days of festivities. The publicdisplay on the history ofhemophilia and its treatmentthrough the ages, with a link tohockey (after all, isn’t MarioLemieux our Honorary President?),is not to be missed. All of this willtake place in Montréal, where oursociety was founded in 1953.
In passing, we will all have alaudatory thought for the founderof the CHS — who was also thefounder of the World Federation ofHemophilia (WFH) — FrankSchnabel, who did so much toimprove the quality of life ofpeople with hemophilia. This willbe the ideal occasion to reminisceon the early days of the Society, inan era when treatment wasnothing like it is today; some ofyou will remember only too wellhaving lived through it yourselves.
This opens the door for me topoint out once again the privilegewe have here in Canada to be ableto count on the latest treatments,efficacious and safe, while 75percent of hemophiliacs in theworld are completely deprived. Theefforts deployed by the WFH tofoster cooperation amonghemophilia organizations both inindustrialized countries and indeveloping countries deserve bothmention and encouragement.Several international twinningpartnerships have been set in
EDITOR’S KEYBOARD
Please feel free to respond to this editorial or to any other article that hasappeared in Hemophilia Today by writing toThe Editor, Hemophilia Today, 119Thomassin, Beauport, QC, G1B 2W6 or by Email at [email protected].
FrançoisLaroche
January 8, 2003
Dear members of the CHS Board ofDirectors,
I just read that you are preparingfor your 50TH anniversary.
It is my hope that it will be asgreat a success as the Society hasbeen in the past 50 years. Your workhas been appreciated, even in thesmall towns that are miles awayfrom your office. Thanks to the workof your past and present directors, Iwill also be celebrating my 72ND
anniversary a couple of weeks afteryour 50TH.
I was born in 1931 in NewLiskeard which at that time had apopulation of about 3,500. Includedin that figure were four GPs and asmall hospital. I spent a lot of mypre-teens in that hospital. Whenthey could not handle my needs itfell upon my father to drive the 350miles to Sick Children’s Hospital inToronto. I was to learn that therewas only a 10 percent chance that Iwould live until I reached 20 years ofage. I have been given a few monthsto live twice and told I would neverwalk again.
I married at age 24, when advisedby a doctor that my hemophiliawould be passed on by my sister’schildren but not mine. That waslater proved wrong, of course, but bythen I had 4 children. I think it wasabout the mid-60s that I heard about
LETTERSTO THEEDITOR
motion in our provincial chapters. Theyare proof of the fact that together wecan contribute to improving the qualityof life of people with hemophiliaaround the world.

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 3
Dear editor,
I want to congratulate Michael Kingon his excellent and informativearticle on “I Feel the Need...”.However, I would like to point out
one small (perhaps editing) mistake.It appears twice—once in the second
paragraph of the body of the articleand in point 3 of “the Top Eight”—the minimum age recommended forthe influenza vaccine is 6 months,not 6 years. (Reference: CanadianImmunization Guide, 6th Edition, 2002,page 124).
I look forward to the second vaccinearticle, and many more.
Best regards,
Bill MindellDirector, Infectious Diseases ControlDivision York Region Health Services
This issue of Hemophilia Today contains articles on von WillebrandDisease (VWD) and other inherited bleeding disorders, topics which fit in wellwith the launch of the Bleeding Disorders Initiative, a programme whichaffirms the fact that the CHS is an organization which exists to improve thequality of life for Canadians with all inherited bleeding disorders. In addition,this spring in conjunction with our fiftieth anniversary celebrations, the CHSis hosting the world’s first international medical symposium on VWD. Theseevents are very dear to my heart. They represent things that I’ve been workingfor since I first became active in the society in 1990.
In 1985, I met a man named Santo Caira, who was working for theHemophilia Society in Toronto and told him over coffee one evening that,even though doctors had assured me that I was not a hemophiliac, I hadnevertheless experienced a number of episodes of excessive bleeding. Indeed,once after surgery, I had almost bled to death. In addition, my mother died asa result of a hemorrhage when I was born. Santo suggested that I go see Dr.Jerry Teitel at St. Michael’s Hospital in Toronto; and Dr. Teitel diagnosed myvon Willebrand Disease. It was comforting to know that my excessive bleedingcould be controlled if the need ever arose. And arise it did in the fall of 1989when I was unlucky enough to be standing next to a large mirror when it felloff the wall and cut me rather badly. That day it was very fortunate indeedthat the comprehensive care team knew what to do. Afterwards, I realizedthat I owed a debt of gratitude not only to Dr. Teitel and the other doctors atSt. Michaels Hospital, but also to the Hemophilia Society. If it hadn’t been forSanto Caira’s good advice, the aftermath of my encounter with the mirrorwould have been much worse than it was.
When I first started attending Hemophilia Society events in Toronto andeventually joined the boards of the Toronto and Central Ontario RegionalHemophilia Society (TCOR), Hemophilia Ontario and the CHS, I was a bit of acuriosity. Many of the people I met had never even heard of VWD; and thosewho had heard of it didn’t know much about it. I was the very first “vonWillie” that most of the hemophiliacs had ever met.
In those days, the Hemophilia Society at all levels was heavily engaged inattempts to obtain compensation for people infected with HIV through theblood system. Then we realized that we needed to work for an inquiry into theCanadian blood system and obtain compensation for people infected withHCV. However, while working to make these extremely important thingshappen, a few of us also quietly worked to have the CHS gather and publishinformation about VWD and the other inherited bleeding disorders and tobegin to reach out to people with these diseases through a VWD Educationand Awareness Campaign. And this spring, the Medical Symposium on VWDand the launch of the Bleeding Disorders Initiative are making these effortseven more visible. I’m not a “lonely little von Willie in a hemo patch” anymore.
your organization and joined to getyour newsletters, which have nowbecome a book. They have kept meup to date on what was being doneto ease our lives.
Then the Northeastern OntarioChapter was formed in Sudbury. I andmy two grandsons traveled the 160miles to their clinics. Nurse Betty-Anne Paradis still routes me out tothem, even though I feel like adinosaur when compared to theothers that turn out. I have grand-children older than them. I am blindin one eye, have a prosthetic leg andnumerous joints that don’t work theway they were supposed to, but mymotto is, “As long as I keep moving,they won’t shovel no dirt on me.”
I have rambled on enough. Myoriginal idea was to let you guys andgals know how much you havehelped me through the rocky roadof life and to wish you all the VERYBEST ANNIVERSARY possible.
Yours truly,
William J. BondNew Liskeard, Ontario
PRESIDENT’SMESSAGE Tom Alloway, Ph.D.
“I was the very first ‘von Willie’ that most of the hemophiliacs had ever met”
LETTERS
H E M O P H I L I A T O D A Y S P R I N G 2 0 0 34 n e w s u p d a t e
NOTICE
The Annual General Meeting of theCanadian Hemophilia Society will conveneas follows:
Saturday, May 10th, 2003 9:00 a.m.at the Sheraton Hotel in Montreal, Quebec
11.. To receive the report of the NominatingCommittee
22.. To acknowledge the designatedDirectors of each Chapter
33.. To nominate candidates for the Directorat Large positions on the CHS Board for2003-2004
44.. To receive the audited financial state-ments of the Canadian HemophiliaSociety for the year ended December 31,2002
55.. To appoint an auditor for the ensuingyear
66.. To transact such other business as mayproperly come before this AnnualGeneral Meeting of the members of theCanadian Hemophilia Society
James KreppnerSecretary
◗ CHS MARITIME OFFICE MOVES
Please note the new address and phonenumbers for the CHS Maritime Office.
Tradina Meadows, CHS RegionalCoordinator for the [email protected]: 506-854-5695Fax: 506-854-4379
CHS Maritime OfficeP.O. Box 29194Moncton, NBE1G 4R3
◗ CHS SCHOLARSHIP AND BURSARYPROGRAMME
Applications for the 2003 CHS scholar-ship and bursary programme have beenavailable as of February 1 on the CHSwebsite at www.hemophilia.ca. Copieswere also sent to chapters and clinics fordistribution to interested people.Annually, CHS awards one $4000 aca-demic scholarship, one $4000 bursary,and one $4000 mature student bursary.The deadline for applications is April 30,2003.
This programme is funded through aneducational grant from Baxter.
NOW AVAILABLE!
HEPATITIS C:An Information Booklet for
People Infected With theHepatitis C Virus, and Their
Families and Friends, published by the Canadian
Hemophilia Society.
Originally introduced in April 1995,the fourth edition of this extremely
popular publication is now available.The revised edition provides updated
information on: hepatitis C,diagnosis, symptoms, getting
treatment and treatment options,hepatitis C and HIV co-infection,
standards of care, healthy lifestyle,alternative therapies, psychosocial
aspects, as well as a number of usefullinks to other sources of information.
Order yours today, for free. Quantities are limited!
Place your order by FAX to 1-514-848-9661, or send us an e-mail at [email protected]. You may also order by phone by
calling, in the Montreal area: 514-848-0503, or toll-free at
1-800-668-2686. Order by mail by writing to:
Canadian Hemophilia Society, 625 President Kennedy Avenue,
Suite #1210, Montreal, QC H3A 1K2.
◗ CHS ORGANIZES 2ND NATIONALINHIBITOR WORKSHOP
The second national workshop forfamilies dealing with inhibitors,sponsored by NovoNordisk, will be heldin Montreal, October 17-19, 2003. Furtherdetails will be available on the CHSwebsite in the spring.
NEWS UPDATE
continued on page 14
◗ RENEWED SUPPORT FOR HTCS INONTARIO
The Ontario Ministry of Health hasrecently agreed to support the fiveprovincial Comprehensive Care Clinics /Hemophilia Treatment Centres byproviding funding for clerical support.The Ministry will also support the hiringof a Provincial Co-ordinator.Representatives of Hemophilia Ontarioand the clinics have been asked to sit onthe Steering Committee to oversee thisinitiative. Members of HemophiliaOntario and the medical communitylook forward to working with theMinistry in this capacity to improvecomprehensive care for people withbleeding disorders in Ontario. More inupcoming issues.
◗ FDA PROPOSES NEW WARNING ONNONOXYNOL 9
In January 2003, The Food and DrugAdministration in the United Statesproposed new warnings labels for over-the-counter contraceptive drugs thatcontain the spermicide Nonoxynol 9.
The warning would state that vaginalcontraceptives containing Nonoxynol 9do not protect against infection fromHIV or other sexually transmitteddiseases. The proposed label warningswould also tell consumers that the useof these contraceptives can increasevaginal irritation, which may increasethe possibility of transmitting the AIDSvirus and other STDs from infectedpartners. The proposals are based onrecent studies using Nonoxynol 9,including data from a World HealthOrganization study of 991 HIV-negativesex workers in Africa and Thailand. Thestudy showed Nonoxynol 9 to beineffective in the prevention of HIVinfection.
PATIENT NOTIFICATION
SYSTEM
A N N O U N C E M E N T
NEW SYSTEM FOR PLASMA PRODUCTRECALL INFORMATION
Canadian Blood Services is pleased toannounce that the Patient NotificationSystem is now available in Canada, inboth French and English, at no cost tothe consumer.
H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 5
Eric Stolte, Chair CHS National Awards Committee
Some might say that for altruism to be authentic, it must go unrecognized. If that were true, then an Awards Committeewhich honours altruistic service would be counter-productive. But when we see the selfless devotion of the people who receiveacknowledgment, and whose sacrifice we deeply appreciate, we’re spurred on to greater service.
At the November 2002 Awards Banquet, the CHS recognized a group of dedicated volunteers, health care providers and staffwho made a significant contribution to the bleeding disorders community during the year 2001. The Awards Committee truststhat by recognizing the following people, you’ll be inspired to even greater levels of service yourself!
CHAPTER RECOGNITION AWARDS
This award is designed to recognizechapters who have demonstrated anachievement over the preceding year in aspecific area such as fund-raising,patient services, education, or chapter/regional development.
Newfoundland and LabradorChapter – for outstanding efforts toadvocate, in collaboration with the clin-ic, for improved funding for comprehen-sive care.
Alberta Chapter – for outstandingefforts to provide peer support to mem-bers and to educate the general publicabout bleeding disorders.
AWARD OF APPRECIATION
This award honours individuals whohave demonstrated outstanding serviceto the care of people with inheritedbleeding disorders.
DR. CECIL HARRIS AWARD
This award hon-ours distinguishedcontributions in theareas of hemophilia-related research orthe advancement ofthe care of patientswith hemophilia orother inheritedbleeding disorders.It is named after thelate Dr. Cecil Harris,in recognition of hiscontribution as oneof the pioneers inthe care and treatment of hemophiliacsin Canada and around the world.
Dr. John J. AkabutuPast Clinic Director, Edmonton, Alberta
CHAPTER LEADERSHIP AWARD
This award is given to an individualwho has merited special national recog-nition for having provided exceptionalleadership and devotion to a specificCHS Chapter over many years and foroutstanding efforts to further thegrowth and development of the chapter.
Left to right: Tanya Wright and her three children, Kirk, Lanaand Ashley
Craig Wright (posthumously)Saskatchewan
Eric StolteSaskatchewan
PIERRE LATREILLE AWARD
This award forexcellence is givento a staff member ofthe CHS working ateither the national,chapter or regionallevel who demon-strates outstandingqualities of devotionand support for vol-unteers and of hisor her other staffmembers.
Clare Cecchini
CHS Program Development Coordinator
FRANK SCHNABEL AWARD
This award wasinitiated to honourthe outstandingservice of FrankSchnabel, thefounder of theCanadianHemophilia Society.The award is pre-sented in his nameto honour a volunteer who, over a num-ber of years, has rendered distinguishedservices and noteworthy contributions tothe mission and objectives of theCanadian Hemophilia Society.
Michael McCarthyOntario
AWARDS BANQUET held in NovemberCHS honours volunteers, health care providers and staff
Kathy Mulder (left), BPT,Physiotherapist, Winnipegreceiving the Award ofAppreciation from ErmaChapman
Wilma McClure (left), R.N.,Edmonton receiving theAward of Appreciation fromBob Verreau
Maybe you know of more “hiddenheroes” – people sacrificing their owntime and energy for the greater good of improving the quality of life for ALL people with bleeding disorders. If you doand would like to nominate them for anaward, we’re requesting people forwardnominations to CHS for 2002 by June30th, 2003.
The awards package will be availableon the CHS website as of the end ofMarch. We’re eager to read yournominations and honour a newgroup of devoted volunteers, healthcare providers and staff this year.
Dr. John J. Akabutu (left),retired Director of the John J.Akabutu Bleeding DisordersClinic in Edmonton receivingthe Dr. Cecil Harris Awardfrom Bruce Ritchie
Clare Cecchini (left), CHSProgram DevelopmentCoordinator, receiving thePierre Latreille Award fromPam Wilton
Michael McCarthy (right),receiving the Frank SchnabelAward from James Kreppner

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 36
FIVE PEOPLE…FIVE BLEEDINGDISORDERS
David Page
In the coming months, the
CHS will be launching its
Bleeding Disorders
Initiative, a programme
intended to raise awareness
among the general public,
health care providers and
decision-makers about the
whole range of inherited
bleeding disorders —
von Willebrand Disease
(VWD), platelet function
disorders, rare factor
deficiencies and, of course,
hemophilia. The longer-
term goal is improved care
and treatment for all people
with bleeding disorders.
The Bleeding Disorders Initiative isnot a radical departure from the pastmission of the CHS. People with VWDand the rarer factor deficiencies havebeen active members of the CHS formany years; indeed, a major element ofCHS programming in recent years hasbeen the VWD Awareness Campaign.
Hemophilia A and B are the mostcommon severe bleeding disorders, andwill remain a focus of the work of theCHS and the Hemophilia Treatment
Centres which treat bleeding disorders.However, they affect fewer than 3,000Canadians. An estimated 300,000Canadians suffer from other inheritedbleeding disorders. These are usually,but not always, milder conditions. Manyof these people remain undiagnosed;their lives can be in danger after serioustrauma, surgery or even a banal eventsuch as a nose bleed.
This article features five peopledescribing the reality of five differentbleeding disorders. Its goal is to raiseawareness among the members of theCHS about the individuals we serve.
Six-year-old Albertcan have intra-cranial bleeds
S ylvie Ferlatte is the mother ofAlbert Bourdages, a six-year-oldboy with severe factor VII deficien-
cy who this year started to attend kinder-garten. Sylvie and her husband, BernardBourdages, and daughter Laurence, livein St-Siméon, a small town near the tipof the Gaspé Peninsula, and a nine-hourdrive from Sainte-Justine Hospital inMontreal where Albert is now treated.
Albert’s deficiency in factor VII wasdiscovered at the age of three weekswhen a tiny intra-cranial bleed caused ablockage in his head, and a fluid build-up inside the skull. An operation wasnecessary to insert a valve; over the next18 months, six more operations wereperformed to counter the build-up of flu-
ids. Fortunately, there was no neurologi-cal damage.
Albert was treated in several hospitalsin Quebec City. “It was hell,” Sylvie saystoday. “Each time we went to the hospitalwe saw different doctors. It was crazy —there were too many doctors at too manyhospitals. Albert had to get his factor VIIconcentrate three times a week to pre-vent the intra-cranial bleeding. He hadfour or five Port-a-caths but they keptgetting infected, andhad to be changed.”
Four years ago,Albert was referredto the HemophiliaTreatment Centre atSte-Justine Hospitalin Montreal. “It iswonderful. I can’tcompare it to whatwe went throughbefore. All the servic-es are in one place.Everything is con-nected together.Everybody knowsAlbert. They seem toknow exactly what todo.”
At Ste-Justine,Sylvie and Bernard learned to infuseAlbert with factor VII through IV injec-tions. For the last four years, they havebeen successfully taking charge ofAlbert’s treatment with infusions everytwo days. “The goal,” says Sylvie, “is tocompletely prevent the intra-cranial hem-orrhages. Albert accepts the infusionswhen we do them. He’s very brave.”
Albert is not affected by joint or mus-cle bleeds, or even bruising. The dangerfor people with factor VII deficiency isintra-cranial bleeding. “That’s why roughsports are forbidden for Albert. It’s justtoo dangerous,” says his mother. “But hehas started school and he’s a normal lit-tle boy.”
Only 1 person in 500,000 has factor VIIdeficiency. Sylvie says, “We sometimesfeel isolated. We’d love to talk to otherparents with the same problem, but wedon’t know anyone. There’s a lack ofinformation about factor VII deficiency.The nurses recently wrote a booklet onthe condition and that helps. We canshow people what the condition is.”
Sylvie has a very positive outlook. “Youcan’t have pity for Albert just because hehas this bleeding disorder. We see it asjust one part of his life. We want to makesure he is not isolated because of it.”
Only 1 person in 500,000 hasfactor VIIdeficiency.Sylvie says,“We sometimesfeel isolated.We’d love totalk to otherparents with thesame problem,but we don’tknow anyone.”)
f o c u s o n b l e e d i n g d i s o r d e r s

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 7f o c u s o n b l e e d i n g d i s o r d e r s
Factor XI deficiency— much more common thanbelieved?
R ichard Yampolsky, a 46-year-oldhusband and father of two girls,is one of an unknown number of
Canadians with factor XI deficiency, alsocalled hemophilia C. He was diagnosedat the age of 12. “I had a tooth out and itbled for weeks. The resident suggested Ibe tested for hemophilia. My mother wasappalled. Six months later, I had an eyeoperation. There was no problem post-op, but after I got home, I sneezed andthe entire side of myface turned purple.”
Soon after, at theRoyal Vic inMontreal, Richardwas diagnosed withfactor XI deficiency.But instead of refer-ring him to theHemophiliaTreatment Centre, hewas referred to theJewish General. Thedoctor consideredfactor XI deficiency a“Jewish disease”because of its dispro-portionately highrate amongAshkenazi Jews.There is also a largepopulation in Iraq.
“Factor XI affects 1in 100,000 people inthe general popula-tion,” says Richard,who worked asExecutive Director ofHemophilia Ontariobefore accepting aposition with theOntario Ministry of Health. “However,the defective gene affects as many as 8percent of Ashkenazi Jews. This means itcould affect more than 25,000Canadians, most of whom don’t knowthey have it. This underlines the criticalissue of proper diagnosis and referral tobleeding disorder clinics. It’s too bad,but the importance of factor XI deficien-
“Factor XI affects 1in 100,000 peoplein the generalpopulation.However, thedefective geneaffects as many as8 percent ofAshkenazi Jews.This means it couldaffect more than25,000 Canadians,most of whomdon’t know theyhave it. Thisunderlines thecritical issue ofproper diagnosisand referral tobleeding disorderclinics.”
cy is not evenrecognized inthe Jewish com-munity.”
“To compli-cate mattersmore, the sever-ity of bleedingis unpre-dictable. Somepeople withquite high lev-
els of factor XI in their blood streamexperience frequent, severe bleeding.Others with much lower levels havealmost no problems. And levels seem tofluctuate,” according to Richard.
People with factor XI deficiency donot suffer from joint and muscle bleedsas do those with hemophilia A and B. Infact, Richard recently ran a 6.5 km leg ofthe Toronto Marathon. Bleeding afterdental extractions, surgery and traumaare the main symptoms. Women can suf-fer from heavy, prolonged bleeding dur-ing menstruation and complicationsafter childbirth.
Treatment is provided on-demand tostop bleeding. Fresh frozen plasma isstill extensively used. Factor XI concen-trates derived from plasma exist and areavailable in Canada, but have been asso-ciated with thrombosis, the formation ofunwanted clots in the blood stream. InIsrael, where many people are livingwith factor XI deficiency, research hastried to evaluate the effectiveness ofdesmopressin to treat bleeding; however,the results are not convincing. Fibringlue is used during dental work. Thesmall numbers of patients makes itunlikely that recombinant factor XI con-centrate will ever be developed.
“I was lucky,” recounts Richard. “Ihappened to read about the opening ofthe St. Michael’s Hemophilia Clinic in1983 in the newspaper and have beengoing there ever since. It seems that doc-tors and hospitals just don’t think torefer patients to where they should betreated — in a specialized centre like St.Mike’s. I know one woman with factor XIwho was treated in another Toronto hos-pital. She went into cardiac arrest fromcirculatory overload with fresh frozenplasma and almost died.”
Richard says having factor XI deficien-cy has its positive side. “I’ve learned a lotmore about my body and my own careand treatment than most people. AndI’ve had the privilege to be involved inthe bleeding disorders community overthe years.”
Type 2B VWD can cause life-threat-ening bleeds
F rance Drapeau, 44, and her two chil-dren, aged 12 and 3, have Type 2Bvon Willebrand Disease, a type of
VWD in which the von Willebrand factorin the blood stream binds to platelets.The clumping togeth-er of platelets causeslow levels of plateletswhich, in turn, con-tributes to bleeding.Type 2B VWD repre-sents about 5 percentof all the cases ofVWD, or approxi-mately 15,000Canadians. Somecases can be associat-ed with serious, life-threatening bleeding.
As is often thecase, it’s a familyaffair; France’s fourbrothers also haveVWD. One of them died from complica-tions caused by contaminated bloodproducts.
“I’ve always been treated at Ste-Justinein Montreal,” says France. “People arealways complaining about hospital serv-ices these days; I have only praise. I can’tfind the words to express all my grati-tude for what they have done for me overthe years.
“Von Willebrand Disease is not wellknown outside the hemophilia clinic. If Isee other health care providers and say Ihave VWD, they don’t say anything.Maybe they don’t want to seem ignorant.As soon as I say it’s a type of hemophilia,they know what it is, they know it’s ableeding problem.”
France was treated with cryoprecipi-tate in her youth. Dental extractionswere often a cause of bleeding. Both herchildren were born by Caesarian sectionand each time she suffered extensivebleeding. “The last time the doctors werevery worried because I lost a lot ofblood,” she remembers. Nowadays, she istreated with Humate-P, a concentrate offactor VIII and von Willebrand factor.France is no longer able to use desmo-pressin to prevent bleeding as she hasangina and the side effects of the med-
“I can neversay thankyou enoughto the people whotake thetime to giveblood.”

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 38 f o c u s o n b l e e d i n g d i s o r d e r s
ication could be dangerous.Both her son and daughter are treated
with sub-cutaneous desmopressin andanti-fibrinolytics (Cyklokapron). “It’smagic,” says France. “I haven’t had to takemy daughter to the hospital since lastfall. When she was younger she had anose bleed so severe her hemoglobin fellto .50 — she was gray and waxy looking —and she needed a blood transfusion. I cannever say thank you enough to the peoplewho take the time to give blood.”
Because of nose bleeds her son has togo to the Ear-Nose-and-Throat Centre andthe hemophilia clinic four or five times ayear. “He’s only twelve. He sees VWD as anegative thing in his life, especially whena bleed stops him from participating inhis regular activities. But I know it’s notall negative. Medication is excellent now.My insurance pays 100 percent of thedrug costs, though I had to get a letterfrom Dr. Rivard to convince them it wasnecessary. And I don’t worry about thelittle things in life. At the hematologyclinic, I see all the kids with cancer. Itkeeps things in perspective.”
“I have two wishes,” France said at theend of the interview. “That research con-tinues to find a cure and that, in themeantime, people continue to donateblood.”
Factor XIII deficiency… and an 8-hour driveto the clinic
“Drake is a pretty awesome boy,” sayshis mother, Gwenn Bodie ofThompson, Manitoba. Drake has
severe factor XIII deficiency. The familylearned of his condition when he was 13days old. Bleeding began from the umbil-
France Drapeau (right) and her children, Kevin and Elizabeth
ical cord after the stump fell off, a clas-sic sign of factor XIII deficiency. Therewas no history of abnormal bleeding inthe family.
As a 7-year-old, the main symptoms ofhis condition are prominent bruisingand poor wound healing. “Cuts andscrapes take forever to heal,” says Gwenn.“First, the bleeding lasts longer than nor-mal, then a large scab forms and staysfor a long periodand finally, scar tis-sue can form.”
The other dangeris the potential forintra-cranial bleed-ing. “He receives apreventative infu-sion of factor XIIIconcentrate,Fibrogammin P,every four weeks.Fortunately the half-life of factor XIII islong, 19 days, so fre-quent infusions arenot necessary,” saysDrake’s mother.
“He went to theER for treatment forthe first three and ahalf years, but thenthe staff at thehemophilia clinic inWinnipeg taught usto home infuse. Henever had a port.There were times atthe beginning when it took two of us tohold him down. Drake didn’t understandwhy he was getting a needle. But it’smuch better now. He has great veins andit only takes ten minutes. There are stilloccasions when he tries to get out of itand we have to insist. He’s at the pointnow where he often does all the prepara-tions for the infusion, except the poke.That’ll come when he’s a little older.”
Drake doesn’t experience joint ormuscle bleeds so, with his prophylactic
therapy, he isable to playsports. “Wefollow thephysicalactivityguidelinesdevelopedfor hemo-philia A andB,” saysGwenn. “Heplays hockeybut withoutcontact.”
Nor are mucosal bleeds from the noseor mouth a problem in Drake’s case.
“His condition could have been over-whelming,” says Gwenn. “When he was ababy, we lived in Terrace, BC, and nowThompson. It’s an 8-hour drive to thehemophilia clinic in Winnipeg. Therewas no one to talk to about it and we feltso alone, so isolated. But I’m an RN andthat has helped with the hospital situa-tions. Our reaction was to get all theinformation we could find. In the end wehad so much the physicians asked uswhat we knew. And home treatment hasmade it so much easier.”
“I think this has opened a lot of doorsfor us as a family,” concludes Gwenn.“We’ve met so many nice people atHemophilia Manitoba and at the clinic.We go to the family camp and reallyenjoy that. Once Drake learns to managehis own disease, he’ll benefit from hiscondition in a lot of ways.”
An inherited bleeding disorder…but which one?
Inherited bleeding disorders are notalways easy to diagnose. Just ask
Marlene Permanand of Winnipeg,Manitoba.
“For years I was told I had a plateletfunction disorder,” says Marlene. “That’seven what’s written on my MedicAlertbracelet. But after a recent lab work-up,the doctors can no longer say I do. Thelab work just doesn’t match my symp-toms.”
Those symptoms started at a veryyoung age. “I had horrible lengthy nosebleeds as a child. I bled on-and-off for twoor three days. My mother remembers Iwas anemic. I had no energy. I was soanemic I used to chew on the coal deliv-ered for the neighbour’s furnace. Mybody craved the iron.”
Marlene continues to have problemsas an adult. “I’ll bleed into the tissues ofmy fingers just from carrying groceries,”she says. Her most serious problems haveresulted from bleeding after surgery. Onetime after back surgery, bleeding dam-aged the sciatic nerves. As a result, shelives with chronic pain. The pain forcedher to shorten her nursing career.
Marlene wasn’t the only person in thefamily with bleeding problems. “Mymother and six or seven of her brothersbled after tooth extractions or surgery.
“His condition couldhave been over-whelming. It’s an 8-hour drive to thehemophilia clinic inWinnipeg. There wasno one to talk toabout it and we feltso alone, so isolated.But I’m an RN andthat has helped withthe hospital situa-tions. Our reactionwas to get all theinformation we couldfind. In the end wehad so much thephysicians asked uswhat we knew.”

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 9f o c u s o n b l e e d i n g d i s o r d e r s
One time, onealmost died. Mymother’s motheralso bled abnor-mally. But sinceeverybody had it,they thought itwas normal.”
“In the 1980s,”Marlene recounts,“my son was diag-nosed with vonWillebrandDisease. He wentback recently to bere-assessed andnow they’re not so
sure. We’re a real mystery.”Marlene’s difficulties in getting a defi-
nite diagnosis, even in a specializedbleeding disorders clinic, underline theneed to continue to conduct research inthis area. “I’m close to retirement. We’regoing to be traveling alot. What do I put onmy MedicAlertbracelet?” Marleneasks. “I want people toknow what I have andwhat to do if I’m in anaccident.”
Despite the lack of adefinite diagnosis,health care providershave found effectivetreatments. “I’m treat-ed with desmopressinbefore surgery. Thetimes I didn’t have it, Ihad bleeding complica-tions. The times I tookdesmopressin, theproblems were muchless severe. I don’tknow what would’vehappened the last timewithout it.”
“I’ve had to become very knowledge-able about my body. A few years ago, Istarted taking vitamin E and noticed Iwas getting increased bruising. I calledthe bleeding disorders clinic and thenurse said to stop taking it – the vitaminwas the cause.
“I’ve also made a point to informeverybody in my family of the symptomsthrough a family letter. That’s how mysister and her sons were diagnosed withVWD. Family awareness about our bleed-ing tendency has really improved.”
Marlene says her links withHemophilia Manitoba and the localbleeding disorders clinic are excellent.“And,” she concludes, “I’m so grateful foruniversal health care.”
“Marlene’sdifficulties ingetting adefinitediagnosis, evenin a specializedbleedingdisorders clinic,underline theneed to continueto conductresearch in thisarea.”
The inherited bleeding disorder vonWillebrand Disease (VWD) isextremely common, particularly
in its mildest form, called Type 1. In fact,it’s thought that one in 100 people haveVWD, though the vast majority are undi-agnosed. On the other hand, the moresevere form, Type 3, occurs in only onein 500,000 people. I’m one of those rareType 3s.
I was diagnosed as a
child, but I didn’t realize
until adulthood that I
have Type 3. It’s funny to
think of it now. All those
bleeds into muscles and
joints, Emerg visits, hospi-
tal stays, missed school-
days, crutches, tears,
never-ending bleeding
times... and I thought I
had a mild disorder.
Although the treatment
back then was a far cry
from today’s options, I
coped and my family
coped, so I thought every-
thing was close to normal.
My experience helps me understandhow so many can have VWD and yet beunaware of their condition. The mainsymptoms of VWD are easy bruising,heavy menstrual periods, frequent orprolonged nosebleeds, and prolongedbleeding after injury, surgery, childbirthor dental work. Both males and femalescan have VWD and exhibit symptoms.Sounds straightforward; you mightexpect people to be getting diagnosed indroves. It seems that most people with
Von Willebrand Diseaseundiagnosed VWD don’t realize thattheir symptoms are symptoms of any-thing. But just because someone doesn’trealize that, say, her period is muchheavier than normal (after all, flow vol-ume is not a common topic of conversa-tion) doesn’t mean that she shouldn’t berelieved of the burden of excessive bleed-ing, if possible. Even someone with mildVWD can experience significant bleed-ing. It’s always better to have a properdiagnosis and know the facts so that onecan prevent or treat problems.
For Type 1s, treatment is oftendesmopressin, also known by the brandname DDAVP, a pharmaceutical productwhich causes the body’s stored vonWillebrand factor (VWF) to be releasedinto the bloodstream where it can get towork in clotting — VWF carries and stabi-lizes Factor 8. DDAVP can be used preven-tatively or to treat bleeding. There areseveral ways to administer it. My chil-dren, who have Type 1, have received itonly intravenously. Fortunately, they’vehad few problems, but they havereceived treatment before significantdental work as well as after a headinjury.
Type 3s don’t respond to DDAVP. Wehave little VWF, and not enough is ware-housed in our cells to make a differencewhen it gets released. When I need toprevent or stop bleeding, I sometimesuse Humate P. It’s a heat-treated, virallyinactivated blood product.
There is also Type 2 VWD. Unlike 1sand 3s, 2s have normal amounts of VWFin their bloodstreams, but their VWFdoesn’t function properly. Type 2s mayuse Humate P or other treatmentoptions (excluding DDAVP.)
For all of us, prevention is obviouslythe best medicine. My kids and I wearhelmets to ride and skate, and our sportsactivity is low impact. But there aresome things that can’t be prevented. Oneof my worse bleeds occurred from ovula-tion. It may sound trivial; it was bad. ButI knew where and when to get treat-ment, and the treatment worked well.That’s what I wish for all girls, boys, menand women with VWD: knowledge, rightoff the bat, and effective treatment ifand when they need it.
(The writer’s name has been withheldon her request.)
10 H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3f o c u s o n b l e e d i n g d i s o r d e r s
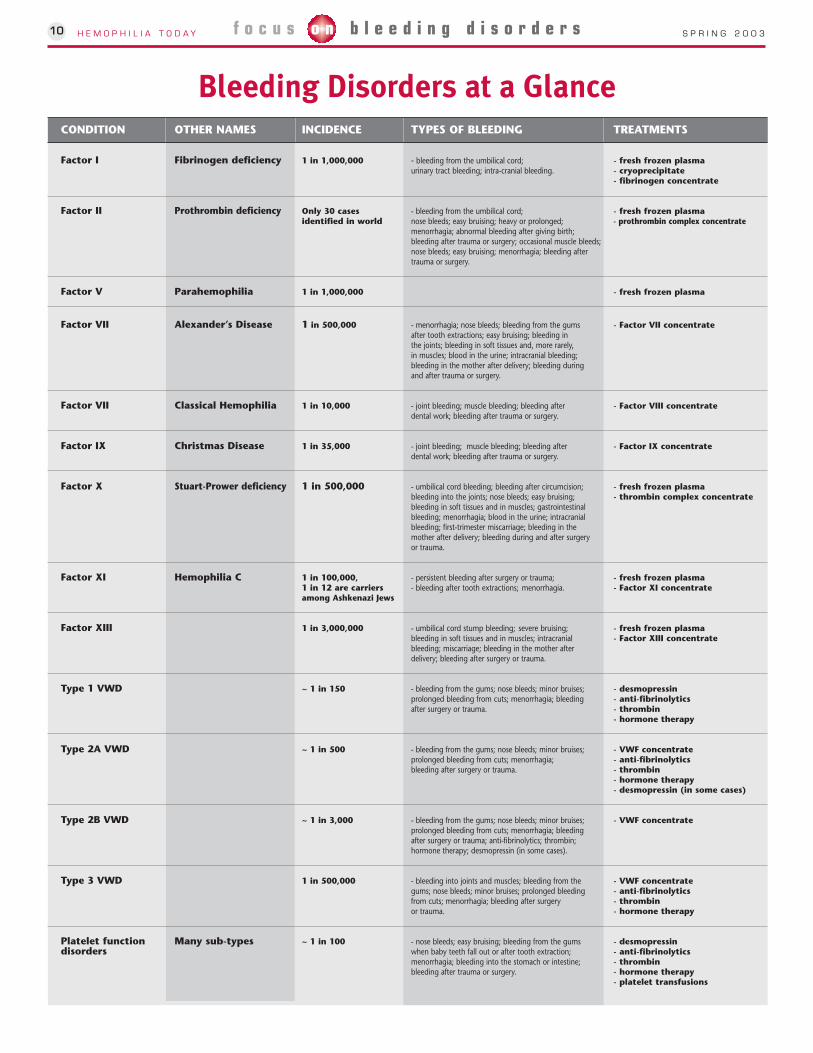
Bleeding Disorders at a GlanceCONDITION OTHER NAMES INCIDENCE TYPES OF BLEEDING TREATMENTS
Factor I Fibrinogen deficiency 1 in 1,000,000 - bleeding from the umbilical cord; - fresh frozen plasmaurinary tract bleeding; intra-cranial bleeding. - cryoprecipitate
- fibrinogen concentrate
Factor II Prothrombin deficiency Only 30 cases - bleeding from the umbilical cord; - fresh frozen plasma identified in world nose bleeds; easy bruising; heavy or prolonged; - prothrombin complex concentrate
menorrhagia; abnormal bleeding after giving birth;bleeding after trauma or surgery; occasional muscle bleeds;nose bleeds; easy bruising; menorrhagia; bleeding after trauma or surgery.
Factor V Parahemophilia 1 in 1,000,000 - fresh frozen plasma
Factor VII Alexander’s Disease 1 in 500,000 - menorrhagia; nose bleeds; bleeding from the gums - Factor VII concentrateafter tooth extractions; easy bruising; bleeding in the joints; bleeding in soft tissues and, more rarely,in muscles; blood in the urine; intracranial bleeding;bleeding in the mother after delivery; bleeding duringand after trauma or surgery.
Factor VII Classical Hemophilia 1 in 10,000 - joint bleeding; muscle bleeding; bleeding after - Factor VIII concentratedental work; bleeding after trauma or surgery.
Factor IX Christmas Disease 1 in 35,000 - joint bleeding; muscle bleeding; bleeding after - Factor IX concentratedental work; bleeding after trauma or surgery.
Factor X Stuart-Prower deficiency 1 in 500,000 - umbilical cord bleeding; bleeding after circumcision; - fresh frozen plasmableeding into the joints; nose bleeds; easy bruising; - thrombin complex concentratebleeding in soft tissues and in muscles; gastrointestinal bleeding; menorrhagia; blood in the urine; intracranial bleeding; first-trimester miscarriage; bleeding in the mother after delivery; bleeding during and after surgery or trauma.
Factor XI Hemophilia C 1 in 100,000, - persistent bleeding after surgery or trauma; - fresh frozen plasma1 in 12 are carriers - bleeding after tooth extractions; menorrhagia. - Factor XI concentrateamong Ashkenazi Jews
Factor XIII 1 in 3,000,000 - umbilical cord stump bleeding; severe bruising; - fresh frozen plasmableeding in soft tissues and in muscles; intracranial - Factor XIII concentratebleeding; miscarriage; bleeding in the mother afterdelivery; bleeding after surgery or trauma.
Type 1 VWD ~ 1 in 150 - bleeding from the gums; nose bleeds; minor bruises; - desmopressinprolonged bleeding from cuts; menorrhagia; bleeding - anti-fibrinolyticsafter surgery or trauma. - thrombin
- hormone therapy
Type 2A VWD ~ 1 in 500 - bleeding from the gums; nose bleeds; minor bruises; - VWF concentrateprolonged bleeding from cuts; menorrhagia; - anti-fibrinolyticsbleeding after surgery or trauma. - thrombin
- hormone therapy- desmopressin (in some cases)
Type 2B VWD ~ 1 in 3,000 - bleeding from the gums; nose bleeds; minor bruises; - VWF concentrateprolonged bleeding from cuts; menorrhagia; bleedingafter surgery or trauma; anti-fibrinolytics; thrombin;hormone therapy; desmopressin (in some cases).
Type 3 VWD 1 in 500,000 - bleeding into joints and muscles; bleeding from the - VWF concentrategums; nose bleeds; minor bruises; prolonged bleeding - anti-fibrinolyticsfrom cuts; menorrhagia; bleeding after surgery - thrombinor trauma. - hormone therapy
Platelet function Many sub-types ~ 1 in 100 - nose bleeds; easy bruising; bleeding from the gums - desmopressindisorders when baby teeth fall out or after tooth extraction; - anti-fibrinolytics
menorrhagia; bleeding into the stomach or intestine; - thrombinbleeding after trauma or surgery. - hormone therapy
- platelet transfusions
Bleeding Disorders at a Glance

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 11f e a t u r e s
families inTOUCHby Karen Creighton
Reaching OutThis isn’t the first time this column has
been devoted to the theme of supportingeach other nor, I venture, the last. It is oneof the founding principles of our national,provincial and local chapters. Much goodhas come over the years from talking andsharing our experiences with each other.We have the challenge of bleedingdisorders in common. Our family iscomprised of those who have a bleedingdisorder and those of us who are parents,siblings, grandparents, friends and familyof people with bleeding disorders. It seemsfitting to highlight a new pilot projectbeing planned in London, Ontario as wecelebrate the anniversary of 50 years ofcaring and support.
At SWOR (South Western OntarioRegion), this age-old tradition of supportbetween families is getting an overhaul!Julie Serrador is the Regional ServiceCoordinator at SWOR. She joined SWORthis fall and has taken over the challengeof launching a pilot project to pair familiestogether, one a newly diagnosed familyand the other a family with some livingexperience with a bleeding disorder.(Watch out, Julie, the “It’s a Boy/GirlPrograms” are in need of an overhaul andyour initiative fits in nicely with that goal,too!)
Julie is setting up a pilot project to pairfamilies together. She is able to do so,through the financial support of Bayer Inc.Julie has an extensive non-profitbackground. She has worked as aneducation and service coordinator, runcommunity outreach programs and evenworked at a camp for kids with sight andhearing disabilities. She is enthusiasticabout the new pilot project.
“It’s a great opportunity for me to get toknow the bleeding disorder communityand the need for this type of program isstrong. I’ve had great feedback so far andlook forward to getting the project off theground.”
The pilot project will start off with 10pairs of families from across the country.One of the challenges of the project is toidentify host families to work with the new
families. For the pilot project, SWORfamilies will be trained to work withfamilies from across the country. Once thepilot phase is completed the ideal situationwill be to recruit host families from acrossCanada to draw on their diverseexperiences and expertise to provide thebest-suited match for the newly diagnosedfamily. The host family will be trained inpreparation for their role as mentor.Training will include what families shouldand should not say, what the host/mentorrole is meant to be, active listening, howinvolved to get and not to get, when torefer matters back to Julie, and participantfeedback.
Julie has researched 12 other programsin operation including those at The WarAmps and at the AIDS Committee of
London. These programs have verysuccessfully provided support amongstfamilies in similar situations. Like theseprograms, this pilot project will providesupport and reassurance to new familiesand provide them with a connection to ourcommunity.
Many of us have worked with familieswho are dealing with a newly diagnosedcase of hemophilia or von WillebrandDisease. I think the participants in thisproject will find they are not only helpingthe new families, but they will also receivegreat satisfaction and support from theirbuddy family. Many of us have benefitedfrom the support, kindness and interest offamilies with older children or from thesame support from adults with bleeding
CHAPTER SPOTLIGHT
Hemophilia Saskatchewanexpands fundraising activities in 2002
Marion Stolte, Saskatchewan ChapterRegional Coordinator
◗ Lifespring 2002 raffle
This year we increased the profile andproductivity of our raffle. We had sevenprizes – all in the “electronic entertain-ment” category. Our members success-fully sold tickets, through tables at sever-al Wal-Mart locations in the province aswell as to friends and family. First prizewas a home entertainment system, val-ued at $2500. Herbert Mogge, one of oursociety members from up north, was thewinner of the first prize.
continued on page 14
Funds raised are going to awarenessand educational workshops/events foradults and youth. We received “in-kind”donations from NEXT Communications,the company that designed and printedour display boards and tickets. Our othersponsors were: Audio-Warehouse, BaxterPharmaceuticals, NovoNordisk, Wal-Martand Wyeth.
Thank you to each volunteer who soldtickets and to our wonderful sponsorsfor their generous contributions!
◗ Old Elephant’sChristmas Benefit Concert
Brenda Baker, an acclaimedchildren’s entertainer, partnered withHemophilia Saskatchewan to bring herinteractive performance/concert, The OldElephant’s Christmas, to Saskatoon inDecember. What a great time everyonehad! Brenda’s enthusiasm and engagingpersonality enthralled even the adults!Hemophilia Saskatchewan volunteershosted the reception for all three con-certs, as well as participated on the plan-ning committee. A number of sponsors
were found, some of whom pur-chased tickets so children from BigSisters and Big Brothers couldattend. Thanks to all the volunteersand the following sponsors for yourgenerous contributions: TheStarPhoenix, C95 FM, 650 CKOM,Baxter Bioscience, Bayer BiologicalProducts, Canada Safeway (severallocations) IGA Garden Market,SaskTel, The Refinery, Joe Bean’sCoffee, Wal-Mart.
12 H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3f e a t u r e s
PAIN - THE FIFTH VITAL SIGN
Maureen Brownlow, Social worker, IWKGrace Health Centre, Halifax, Co-Chair, CHSPain Management Working Group
This is the second in a series of articles onpain and pain management that will appearin Hemophilia Today over the coming months.The article is written by Dr. Peter Leung, PainSpecialist, St. Michael’s Hospital Pain Clinicin Toronto and a member of the CHS PainManagement Working Group. It presents theappropriate assessment and treatment ofpain as essential to quality medical care. Dr.Leung has promoted this philosophy as apractitioner and as a volunteer within theCHS community. To learn more about strate-gies for managing pain, we encourage con-sumers to attend the workshop, Pain - the 5thVital Sign, which will be held on May 10thduring the CHS 50th Anniversary Weekend.And, if you have an experience with painmanagement that you’d like to share with theworking group, please write, e-mail or call usthrough CHS. Improved pain managementfor persons with bleeding disorders is ourgoal.
PAIN – THE FIFTHVITAL SIGN
Dr. Peter Leung Pain Management ServiceSt. Michael’s Hospital
Most health care providers and con-sumers are used to having the four routinevital signs recorded. Blood pressure, pulserate, temperature and respiratory rate aredocumented every time a patient presentsfor a medical assessment. Yet the most com-mon reason for seeking medical care ispain. In 1995, the President of the AmericanPain Society, Dr. James Campbell, coined theabove captioned title suggesting that “quali-ty care means that pain is measured andtreated”. When we add the measurement of“pain” as one of the essential records for allpatients, then we are finally focusing on themain cause for access to medical care.
Health Regulatory Boards in many U.S.states have legislated guidelines to mandatepain assessment with all patient contacts.Pain is now officially considered the fifthvital sign by the Joint Commission onAccreditation of Healthcare Organizations;in other words, all health facilities have toinclude pain as the fifth vital sign for thatfacility to be accredited. The CaliforniaGovernor recently signed into law theHealth and Safety Code (HSC). As part ofthis bill, HSC 1254.7 reads:
(a) It is the intent of the Legislature thatpain be assessed and treated promptly,effectively, and for as long as pain persists.(b) Every health facility licensed pursuantto this chapter shall, as a condition oflicensure, include pain as an item to beassessed at the same time as vital signsare taken. The health facility shall insurethat pain assessment is performed in aconsistent manner that is appropriate tothe patient. The pain assessment shall benoted in the patient’s chart in a mannerconsistent with other vital signs.
Surveys report 14% of the populationhave sick days due to pain, 75% use over thecounter pain medications and 35% use pre-scription pain medications. Chronic painaccounts for more total annual costs thanother chronic conditions such as heart dis-ease, high blood pressure and diabetes.In the hemophilia community, a new bleed-ing episode is recognized primarily becauseit causes pain. Hemarthrosis — bleedinginto the joint — is most common. The painfrom the inflammatory reaction of blood inthe joint can become severe; the jointswelling then further aggravates the pain.Bleeding into the muscle also gives rise topain and swelling and, if unabated, candamage nerves, tendons or other structures.Other sites may or may not be as painfuland each person with hemophilia will havedifferent common sites.
What then is pain? Pain is very difficultto define in words but the InternationalAssociation for the Study of Pain did try.“An unpleasant sensory and emotional
MEDICALNEWSexperience associated with actual or poten-tial tissue damage, or described in terms ofsuch damage.”
Pain is always subjective. The personwith pain is the one who decides if there ispain or not. It is always unpleasant andsince we learn of pain from injury in earlychildhood, it is described in “damage”terms. Lastly, it is an emotional experience.We should note that there does not have tobe actual damage to specific areas of thebody to cause pain. In other words, whenpain becomes chronic, we may not see theactual injury or the physical response suchas changes in heart rate, blood pressure oreven grimacing and crying out.
Some books or pamphlets on hemophiliamight talk about individual differences ofpain perception but the pain level is yoursand yours alone. Do not feel that your painis less significant than that of others, andcertainly you must not feel guilty or embar-rassed because you need medication ortreatment for both acute and chronic pain.Actually, inadequate initial pain manage-ment may be a cause for future abnormalpain behaviour.
The aim of pain control within the firstfew hours of a bleeding episode is relief ofsuffering. With chronic pain control thereis the added aim of maintaining daily func-tion. The balance between the efficacy ofpain relief, the side effects if any, and theability to be as functional as possible is thefinal goal of management. Any and allmodalities of paxin management — physi-cal, pharmacological and psychological —should be incorporated into the scheme ifbeneficial.
How do we measure pain?
Unlike its vital sign counterparts, howev-er, there is no gadget to measure pain; itmust be evaluated by asking questions andobserving behaviour. And unlike tempera-ture or blood pressure, getting accuratedata about pain depends on two-way com-munication between the health careprovider and the patient. These are somehelpful tools:
Numeric Rating Scale:Instructions: Choose a number from 0 to 10 which indicates how strong your pain is right now.
No pain at all = 0 1 2 3 4 5 6 7 8 9 10
Visual Analog Scale:Instructions: Mark on the line below how strong your pain is right now.
No pain at all __________________________________________________ The worst pain imaginable
Category Scale:Instructions: Choose the word below which best describes how your pain feels right now.
Mild Disconforting Distreeing Horrible Excruciating

13HEMOPHILIA TODAY S P R I N G 2 0 0 3f e a t u r e s
BLOODDavid Page, CHS Blood Safety Coordinator
THE
FACTOR
Once we measure the level of pain, wecan go ahead with the treatment plan. Theclinician may quantify it on a single dimen-sion using, for example, a single VAS, butthis approach risks being too simplistic. Painhas sensory, emotional, motivational, cogni-tive, and behavioural dimensions. We mustbe aware that clinical pain intensity doesnot necessarily vary directly with the extentor severity of clinical pathology. Hence theindividual’s subjective response overridesthe clinician’s bias of labeling the patient.Every patient deserves the most effectivetreatment, not what the provider feelshe/she should have. Many barriers impedehumane and competent assessment andmanagement. Patients and health care pro-fessionals also often differ culturally andsocially. Treatment for chronic pain andchronic illness may be unavailable, unaf-fordable, or not covered by health insurers.The variability and unpredictability of painin hemophilia make effective coping diffi-cult, and thus contribute to an adversarialrelationship so often observed betweenpatients and health care professionals.
Fortunately, there is already a major shiftin attitudes toward pain medications. Not solong ago, there was a reluctance to prescribepain killers because they might cause addic-tion or interfere with recovery. Research hasshown that the risk of clinical addiction isoverestimated and, in fact, quite rare at thedosages used for pain management. What’smore, recovery takes place faster when painis properly managed. Unrelieved pain canactually interfere with healing and turnacute pain into a chronic problem.
I believe that recognizing the 5th vitalsign puts assessment at the forefront andsets the tone for cooperation. “What level isyour/your child’s pain?” brings the familyand the provider into an alliance againstthe suffering.
Once we have all parties on the sameside, the therapeutic plan can be developedfor future episodes and daily chronic pain.Then, there is no fear of the agony of thenext episode because the patient canassume “control” and knows there is a pathto follow with back up plans in place.
This all stems from a simple assessmenttool, what we refer to as the “vital signs”.
Reports of cyro being usedto treat hemophilia A
At the January 25-26 meeting of theCHS Blood Safety Committee, it wasreported that cryoprecipitate is stillbeing used to treat some people withhemophilia A. These unconfirmedreports came to light at the time of theplasma and cryoprecipitate recalls forWest Nile Virus in late December. Theprovinces mentioned were Quebec andOntario.
Note that cryoprecipitate continues tobe supplied to hospitals by both CBS andHéma-Québec to treat certain condi-tions; however, since the arrival ofenhanced viral-inactivated factor concen-trates in the late 1980s, cryoprecipitatehas not been the recommended treat-ment for hemophilia A both because ofits lesser efficacy and continued verysmall risk of transmitting human virus-es. In addition, with the availability ofenhanced viral-inactivated vonWillebrand factor, physicians have pre-ferred to use factor concentrates, such asHumate-P®, in those situations wheredesmopressin and other hemostaticagents are not effective for VWD.
After discussion, the followingmotion was made: “In the opinion of theBlood Safety Committee, notwithstand-ing exceptional circumstances andpatient preferences based on informedchoice, given the safety record of high-purity factor concentrates over the lastten years, cryoprecipitate represents asub-standard form of care for hemophil-ia A.”
If chapters are able to identify anyphysicians continuing to prescribe cryo-precipitate, the following actions aresuggested:i) provide them the AHCDC guidelines(http://ahcdc.medical.org/)ii) refer them to specialists in the nearestHemophilia Treatment Centre.
Preparations for summer West Nile Virus seasonunderway
In the summer of 2002 at least oneCanadian was infected with West NileVirus (WNV) through a bloodtransfusion. At least thirteen casesoccurred in the U.S. As the 2003mosquito season nears, concerns mountabout the integrity of the Canadianblood supply should the West Nile Virusepidemic in mosquitoes, birds, horsesand humans continue, or worsen.
Huge efforts are underway to developa test to screen blood donations for WNVand introduce it across Canada by July.Fresh frozen plasma and cryoprecipitatecollected during the winter months arebeing stockpiled in case the test is notready. Other creative strategies are beingevaluated in an effort to reduce the riskto patients.
WNV can be transmitted through redblood cells, platelets, fresh frozenplasma, cryoprecipitate andcryosupernatant. Risks in 2002 wereextremely small, but real. Risk estimatesfor 2003 are difficult to make as thescope of the epidemic cannot bepredicted.
Products manufactured from plasmasuch as factor concentrates,immunoglobulins and albumin havebeen shown not to transmit WNV.
Baxter announces ADVATE as brand name for its third-generation FVIII recombinant product
Baxter International Inc. announced in February that ADVATE is the proposed pro-prietary name for its investigational factor VIII therapy - Antihemophilic Factor(Recombinant), Plasma/Albumin-Free Method (rAHF-PFM). This announcement followsthe provisional acceptance of the brand name by both the U.S. Food and DrugAdministration (FDA) and the European Medicines Evaluation Agency (EMEA).
Hemophilia Today reported on the early results of clinical trials with ADVATE in thespring 2002 issue (Vol 37, No 1). ADVATE is expected to be the first FVIII recombinantproduct made without the addition of human or animal proteins at any stage of theproduction process to come to market.
For children aged 3 and older, a range oftools is available for self-reporting andbehaviour observation; children fromapproximately age 5 are able to reliablycomplete a VAS (Visual Analog Scale) score.One useful tool might be the “Face Scales”.
H E M O P H I L I A T O D A Y S P R I N G 2 0 0 314 f e a t u r e s
More data on prion removal
Aventis Behring has announced that studies show its procedure for cleaning the pro-duction equipment for plasma-derived therapies has the capacity to eliminate the theo-retical risk of prion contamination. Although prions have never been found in the bloodor plasma of people with CJD or vCJD, a study published in a supplement of Blood, sug-gests that even if prions did contaminate equipment, they would not adhere to the sur-face of the equipment and would be removed by standard cleaning procedures.
Individual lots of ReFacto released for use in Canada
In February Health Canada approvedthe release of individual lots of ReFacto®,a second-generation recombinant factorVIII concentrate used to treat hemophil-ia A, manufactured by Wyeth. ReFactoobtained its Notice of Compliance inJune 2002.
This brings to four the number ofrecombinant factor VIII products on theCanadian market: Kogenate® FS, manu-factured by Bayer; Recombinate®, madeby Baxter; Helixate® FS, from Aventis-Behring; and now ReFacto.
Note that Kogenate FS and Helixate FSare identical products manufactured byBayer. Under a licensing agreement,Aventis-Behring distributes a significantpercentage of the production of Bayer’sBerkeley manufacturing facility.
Both Wyeth and Aventis Behring arecontinuing talks with the CanadianBlood Services and Héma-Québec inefforts to have their products made avail-able on a regular basis.
The Canadian Hemophilia Society hasconsistently made known its position tothe operators: physicians and patientsshould have freedom of choice in select-ing the most appropriate therapy. Inaddition, the Canadian blood systemshould establish permanent relation-ships with multiple distributors so as tominimize risks to supply.
Bayer, Aventis Behring merger off, Aventis startstalks with CSL
Bayer and Aventis Behring have can-celled plans to combine their plasma prod-ucts units after a year of talks. Bayer hassaid that it will continue to run its biologi-cal products unit on its own. Aventis said ina statement that it is “proactively exploringalternative options for the future of AventisBehring.”
Only weeks later, Aventis Behringannounced that it had entered into prelim-inary negotiations with CSL Limited regard-ing the acquisition of Aventis Behring.
CSL is an Australian company whichmanufactures products derived fromhuman plasma. The company has growndynamically over the last few years throughthe acquisition of ZLB in Switzerland in2000 and the NABI plasma collection cen-tres in the United States in 2001. Today, CSLis ranked number three in fractionationvolume and number four in sales revenuein the plasma protein industry, with astrong focus on immunoglobulins.
In the hemophilia field Aventis Behringmanufactures and/or distributes theseproducts in the Canadian market: Helixate®FS, a recombinant factor VIII; Monoclate® P,a monoclonal antibody purified plasma-derived factor VIII; Mononine, a monoclon-al antibody purified factor IX; and Humate-P® to treat von Willebrand Disease.
disorders. Families In Touch was started asa support group at TCOR (Toronto CentralOntario Region), over 5 years ago for thevery same reasons Julie is undertaking thisproject.
On the day we founded FIT (Families inTouch), mostly as a group of moms,Margaret Plater joined us. Margaret is afounding member and long time supporterof our associations. She is, of course, JohnPlater’s mother. On that day Margarettalked about sending a child to camp forthe first time, the interaction of siblingswith and without a bleeding disorder andabout the day she was left outside the
Reaching Out continued from page 12doctor’s office at John’s first appointmentat St. Michael’s Hospital. I’ve already sentkids to camp, although I have a few yearsleft before we graduate to St. Mike’s. I doknow that every hug and sharedexperience from all the moms and dads Ihave met will help me along the way.
Good luck, Julie. Keep up the greatwork. You have a wonderful opportunity todo something outstanding. If anyone hasany suggestions on what to call thisproject, or if you are interested in being apart of it, please contact Julie at the SWORoffice.
[email protected]: 519-432-2365
The Patient Notification System is aconfidential, 24-hour communicationsystem providing information on plasma-derived and recombinant productwithdrawals and recalls. It was created toprovide a single, convenient source for up-to-date product withdrawal and recallinformation.
The Patient Notification System wasdeveloped in the U.S. by the PlasmaProtein Therapeutics Association ofWashington, D.C. (made up of 11manufacturers), in conjunction withrelevant consumer groups. NNC Group,based in Indianapolis, Indiana, is theSystem Operator. It has been adapted forCanadian use by an advisory panel ofCanadian companies, and relevantmedical and patient groups who workedwith Canadian Blood Services and Héma-Québec. In Canada, the system is offeredwith funding from plasma and proteintherapy producers and distributors.
The system is entirely voluntary. InCanada, notification of a recall orwithdrawal of blood or blood products isthe primary and legal responsibility ofthe treating physician and/or hospitalofficials. Registering or choosing not toregister with PNS does not alter currentpatient notification by treating physiciansand hospitals.
If you would like to register, you cando so by visiting the Web site atwww.patientnotificationsystem.org,calling the toll-free phone number (1-888-UPDATE-U), or by sending an applicationform by mail to NNC Group, Attention:PNS Manager, 5250 West 76th Street,Indianapolis, IN, 46268. There is no costto the consumer and you will be asked toprovide your name, contact information,password, password hint and a list of theproduct(s) you would like information on.You can choose to be contacted by U.P.S.Express, telephone, fax or e-mail. You willalso receive a follow-up notification byregular mail. Detailed information can befound on the Web site. Please note thatpromotional pamphlets containingapplication forms are available uponrequest by sending an email [email protected] or calling 613-260-6800.
The Patient Notification System iscompletely confidential. It is operated by NNCGroup, an independent organization thatspecializes in pharmaceutical notifications. All patient information is held in strictconfidence by NNC Group. Every attempt willbe made to reach you within 24 hours of anyrecall or withdrawal.
continued from page 4

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3 15f e a t u r e s
THEGLOBAL PERSPECTIVEEric Stolte Chair, International Projects Committee
INTERNATIONALPROJECTS REPORT
TCOR Twins withJordan
Candace Terpstra
Jordan is a small county — 100,000square kilometres of land, mostlydesert — sandwiched between Israel and Saudi Arabia and also bordering
on Syria and Iraq. It is not an oil richcountry. The population of the countryis five million and, just like everycountry in the world, some people havehemophilia. There is no hemophiliatreatment centre in the entire countryof Jordan and factor concentrates areextremely scarce.
On November 8th, 2002, the WorldFederation of Hemophilia officiallyrecognized the partnership between theToronto and Central Ontario RegionalHemophilia Society and the JordanBlood Diseases Patients Friends’Association (Hemophilia Committee).When you learn that hemophilia affects400,000 people worldwide, seventy-fivepercent of whom have little or notreatment, and when you knowthat national hemophilia care
programs have been proven to increasethe life expectancy of people withhemophilia, you realize there is much tobe done. The World Federation Twinningprogram is one way of supporting localhemophilia organizations to improvenational hemophilia care programs intheir own countries.
In the fall of 2002, Karttik Shah and Itraveled as representatives of TCOR toAmman, Jordan. It was a pleasure tomeet the members of the JordanHemophilia Committee: Arafat Awajan,Wael Hudhoud, Mohammed Jaber, Alla,and Mahera Hamza. Without realizing it,they form quite a dynamic little group.They remind me of the early days of theCanadian Hemophilia Society whenpassion and commitment kept membersgoing, working, moving forward, onestep at a time to the next task. Alreadythey have formed a Committee, part of alarger organization officially recognizedby the Queen of Jordan. More recently,they rented separate office space inAmman and the office was freshlypainted just prior to the visit. They havebeen in contact with about 350 membersthus far and are reaching out to find
more. And so it continues.
As for my impressions, there are nowords to describe the incrediblehospitality with which we were treated.We were personally greeted at theairport at 3:00 a.m., met families in theirhomes, attended a packed members’meeting in the new office, werepersonally accompanied on all visits andshared many wonderful meals withmembers of the Committee.
The assessment visit also includedmore formal activities such as meetingwith key personnel in local hospitals andthe blood bank, as well as a meetingwith the Minister of Health. As part ofthe Fourth International BiotestHemophilia Forum for physicians, wewere able to visit the site of the ancientcity of Petra and the Dead Sea. This wasespecially enjoyable as our hosts fromthe Jordanian Hemophilia Committeeaccompanied us on these trips.
Twinning is a two-way street andalready we have learned a tremendousamount about Jordanian culture andreligious customs in the Middle East.There will be lots more to come as wecontinue to work together at educatingfamilies through meetings andnewsletters, and planning a symposiumfor the fall of 2003. These initialactivities will set the stage for lateradvocacy efforts to improve hemophiliacare and treatment in the country ofJordan.
I invite all our members to thinkabout what they can do to supportWorld Federation Twinning Programs. It is surely a worthwhile endeavour.
Left to right: Mohammed Jabber, JordanHemophilia Committee; Karttik Shah andCandace Terpstra, Toronto HemophiliaSociety; Dr. Arafat Awajan, JordanHemophilia Committee

H E M O P H I L I A T O D A Y S P R I N G 2 0 0 316 f e a t u r e s
EndometrialAblation
Menorrhagia (heavy or prolongedmenstrual bleeding) often leadsto problems including severe
anemia. When the problem cannot becontrolled with hormone therapy orother medication, surgical options maybe the only way to control blood loss.
In the past only a hysterectomy couldstop menstrual bleeding altogether.Today, for many patients, a simple safeoutpatient procedure called uterine orendometrial ablation (EA) in which theuterine lining is removed will often alle-viate excessive menstrual blood loss. Incontrast to a hysterectomy which mayrequire up to 8 weeks for recovery, mostwomen who have EA are able to returnto most normal activities within 2-3days.3 Gynecologists have been success-fully performing endometrial ablationsince 1990.
Preparations
Before undergoing any procedure, awoman should be examined to eliminateany other mechanical disorder such as afibroid tumor or a polyp in the lining ofthe uterus which could cause bleedingto occur. The existence of a bleeding dis-order does not rule out these problems.Other tests could include blood tests,uterine lining sampling (biopsy), and asaline sonohysterogram or office hys-teroscopy to evaluate the size and config-uration of the woman’s endometrial cav-ity.3 These procedures are usually donein the physician’s office and are quickand relatively painless. Proper treatmentprecautions should be taken to preventfurther bleeding in women with a bleed-ing disorder.
For 1 to 2 months before the proce-dure anti-hormones may be prescribedto decrease the thickness of theendometrium. Thinning the uterine lin-ing exposes the lower (basal) layer ofendometrial cells; this is the tissue thatwill be removed.
This section is related specifically towomen with bleeding disorders and theirfamilies. All articles are reviewed byphysicians to ensure medical accuracy. If you have any questions, comments orideas, feel free to contact me, PatriciaStewart, at the following addresses:Phone & Fax: 418-884-2208 or e-mail:[email protected] or simplyput pen to paper and mail to: 389, R.R. # 4, La Durantaye, Quebec G0R 1W0
Patricia Stewart
Procedure options
Hysteroscopic endometrial ablationor “RollerBarrel system”: Developed inthe early 1990s, this is a first-generationEA technique and an experienced gyne-cologic endoscopic surgeon is required.The patient receives a general anesthe-sia. Endometrial ablation is performedby inserting a narrow viewing tubethrough the vagina and the cervix intothe uterus. A tiny camera attached to theviewing tube (hysteroscope) allows theuterine cavity to be shown on a TV moni-tor. The uterus is filled with a harmlessliquid to make the procedure easier. Thelining of the uterus is then burned awayor vaporized, using a laser or electrosur-gical tool inserted through the viewingtube.
Second-generation EA devices havenow been developed including uterineballoon technique (UBT) and theMicrowave technique, among others.Benefits of these procedures are thatthey are easier to perform, easier tolearn by physicians, have very high suc-cess rates, are safer than first generationdevices, and in contrast to first genera-tion devices, can often be performed inyour doctor’s office, taking less than 15minutes, and requiring only local anes-thesia.
These second-generation devicesrequire less operator skill than for hys-teroscopic endometrial ablation and noirrigant or distending solutions. All uti-lize heat to destroy the endometrium.Both UBT and Microwave techniquesavoid the use of laser or electrosurgicalenergy, liquid uterine distention media,and their associated complications.3 Thewoman will normally stay in the recov-ery area for 1-2 hours, and then be dis-charged. There may be some mild men-strual cramping and vaginal bloody dis-charge for the next few days.
Potential risks
Most potential complications of EAinvolve use of the hysteroscopic endome-trial ablation devices. These include therisks of anesthesia, uterine perforation,and absorption of large volumes of fluid
used during the ablation procedure(fluid overload).
The global endometrial ablation pro-cedures have the advantage of not usinghigh volumes of, or dangerous, fluids,requiring less anesthesia, requiring lesstime to complete, and in many cases, canbe performed in a gynecologist’s officerather than a hospital.3
Post ablation
Most women cannot have childrenafter endometrial ablation. However,because there is still a slight possibilityof pregnancy, contraceptive methodsshould continue to be used untilmenopause.
It’s important to realize that theseprocedures are not guaranteed to pro-duce amenorrhea (cessation of menses).Most studies have shown that the rate ofabsolute stoppage is 50%, while another25% of patients have very little bleed-ing.1
Approximately 10 percent of womenwill move on to hysterectomy and 10 per-cent will require a repeat endometrialablation for failed initial treatment. Re-operation rate at five years may be up to40 percent with rollerbarrel ablation.Patients undergoing surgery after theage of 40 appear to have a better out-come.5
1. Centre for endometriosis care:www.centerforendo.com/index.htm
2. www.ivf.com/eablate.html
3. D.I. Galen, M.D., FACOG - Bay AreaFertility & Gynecology Medical Groupwww.rscbayarea.com/articles/formendo.html
4. womenshealth.medscape.com www.power-surge.com/headlines/abla-tion.htm
5. SOGC CLINICAL PRACTICE GUIDE-LINES, No. 106, August 2001www.sogc.org/SOGCnet/sogc_docs/com-mon/guide/pdfs/ps106.pdf
FEMALEFACTORTHE
17H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3c h s f i f t i e t h a n n i v e r s a r y
Commemorative book – 50 Years to Remember
In order to have a written and pictorialhistory of the CHS, a commemorativebook will be distributed during theweekend. People active in the Societyover the last five decades will becontributing their memories of livingwith hemophilia. Many volunteers andhealth care professionals who have mademajor contributions will also beincluded. This limited edition book willbe available to all members.
MSAC research symposium
Medical personnel will give an update onthe most recent research in hemophilia-related areas and answer questions. Thiswill take place Friday afternoon.
Youth dinner
Young people from 18-25 years of agewill be attending a dinner on Fridayevening giving them a chance to gettogether and discuss their vision of thefuture of the CHS. It’s also a chance forthem to meet others from across thecountry who will eventually become thelead volunteers in the CHS.
Medical Symposium
During the weekend there will a medicalsymposium for patients on a variety oftopics including pain management,visiting the ER, the safety and supply ofblood and blood products, and the latestin HCV treatment and women’s issues.This is a chance to get the latestinformation from specialists and findanswers to your questions.
CHS 50TH ANNIVERSARY Celebrations
Poster exhibit
One of the strengths of the CHS is thededication of its volunteers. A posterexhibit will be displayed at the hotelduring the weekend on a variety oftopics. You may find faces from the pastand perhaps even see yourself in thisexhibit. This will be the CHS giantfamily photo album and a reminder ofmuch that has happened in the fiftyyears since its founding.
Pioneer Award
This award was created to acknowledgethe founders of each chapter, peoplewho had a dream of improving care forthe hemophiliacs in their own province.This award is to be presented by eachChapter to the recipients during theyear.
50th Anniversary Banquet
No celebration would be completewithout a feast. The banquet will takeplace on Saturday evening. This is achance for people to renewacquaintances and see old friends. AllPast-Presidents and Honorary LifeMembers have been invited making thisa truly multi-decade celebration.
Make sure you send in your registration as soon as possible. Don’t miss outon this once-in-a-lifetimeopportunity to commem-orate 50 years of tragedyand triumph in the care ofpeople with bleedingdisorders.
Patricia Stewart, Chair, CHS 50thAnniversary Celebrations
Celebrations for the 50th Anniversary of thefounding of the CanadianHemophilia Society will betaking place May 8-11th,2003, at the Centre SheratonHotel in Montreal. The CHSis planning a number ofactivities to highlight thisimportant occasion.
Public exhibit on bleedingdisorders
Located in the Complexe Desjardins indowntown Montreal, the CHS willpresent a public display on the history ofhemophilia, its treatment and theachievements of the CHS. MarioLemieux, the CHS Honorary President,and M.J. O’Grady, will be the virtualguides for visitors along this fifty-yeartimeline. Mario’s family has graciouslyoffered some Mario Lemieuxmemorabilia to make the exhibit evenmore attractive. At the same time, Héma-Québec is working with the CHS and issetting up a blood donor clinic besideour exhibit. We’re looking for volunteersto man the exhibit and to thank donorsfor giving blood. Buses have beenarranged on Thursday night and Sundaymorning to take you to the exhibit. Theexhibit itself will later be available totravel across the country to be sharedwith all chapter members.
H E M O P H I L I A T O D A Y S P R I N G 2 0 0 318 c h s f i f t i e t h a n n i v e r s a r y
Dr. David Lillicrap, Chair, ConferenceSteering Committee
On May 8th and 9th 2003 inMontreal, the CHS will be hostingthe 1st Canadian State of the Art
Conference on von Willebrand Disease tocoincide with the 50th anniversary cele-brations for the Society. The conferencepromises to be an excellent forum forreviewing the diagnostic, treatment andpatient-related issues associated withthis condition, in light of recentadvances in knowledge.
Despite the fact that von WillebrandDisease (VWD) has been recognized as adistinct clinical condition for more than75 years, there are still many unresolvedquestions about its genetic basis, themost effective way to diagnose it and theoptimal forms of treatment in differentclinical settings. Furthermore, untilvery recently, critically important issuessuch as quality of life measurementshave not been investigated in the con-text of VWD. There even remains uncer-tainty about the population prevalenceof the condition, with figures rangingfrom 1 in 100 to 1 in 100,000 being quot-ed in the medical literature. Overall,these many remaining questions, alongwith recent advances in our understand-ing of the biology of von WillebrandFactor (VWF), suggest that this confer-ence comes at a time when a compre-hensive re-assessment of VWD will bevery informative for the professional andpatient communities alike.
In considering the best way to reviewthis topic, the Steering Committee forthe conference has developed a programthat we hope will be informative andengaging to all attendees, whether they
be a professional care giver or a patient.The meeting will begin with a series offour “stage-setting” plenary talks byinternational experts in this area. DrsBob Montgomery and David Ginsbergwill talk about the clinical and laborato-ry presentation, and genetic basis of thedisease, respectively, and will, in particu-lar, address the challenging questions ofhow to diagnose and sub-classifypatients with this disorder. The thirdpresentation, by Dr. Craig Kessler, willfocus on treatment issues, and will con-sider the best forms of therapy for specif-ic hemostatic challenges as well as sug-gesting optimal ways to evaluate treat-ment outcome. Finally, Dr. Christine Leewill address the issue of clinical manage-ment of VWD in women, the patientgroup in which the most adverse qualityof life outcomes have now been docu-mented in VWD.
For the remainder of the meeting, thechallenge for the attendees will be toplace the information presented by the
CHS to host 1st Canadian State of the Art Conference on von Willebrand Disease
VWD1ST Canadian State of the Art Conference on von Willebrand Disease
plenary speakers into the context of aseries of “ConferenceRecommendations” relating to VWDdiagnosis, treatment, specific manage-ment issues in women and patient advo-cacy matters. These recommendationswill be developed through a series ofinteractive forums that will be overseenby members of the Planning Committee.Finally, the conclusions of each of thefour forums will be presented to all con-ference attendees at a summary sessionon the Friday morning of the meeting.This will enable input and discussion byall attendees on each of the forum topicsand recommendations.
We hope that you will be able toattend this conference for what we thinkwill be an outstanding review of this,the commonest inherited bleeding disor-der in humans. Further details about the1st Canadian State of the Art Conferenceon von Willebrand Disease including theregistration form are available on theCHS website at www.hemophilia.ca.
A 2-DAY CONFERENCE for physicians, nurses andother medical professionals in the fields of:
• Inherited bleeding disorders• Hematology• Obstetrics / Gynecology• Nursing• Family Practice
We invite you to attend this conference in order to increaseyour understanding of the diagnosis and clinical managementof the bleeding patient with von Willebrand Disease.
Managing the Bleeding Patient: von Willebrand DiseaseDiagnosis, Treatment and Gynecological Considerations
May 8-9, 2003 • Le Centre Sheraton Hotel • Montreal, Quebec

H E M O P H I L I A T O D A Y S U M M E R 2 0 0 219H E M O P H I L I A T O D A Y S P R I N G 2 0 0 3c h s f i f t i e t h a n n i v e r s a r y
As a young boy with hemophilia in Montreal in the 1950s,whose parents and grandparents were active in theCanadian Hemophilia Society, I grew up hearing about
‘Frank’. In my house he was portrayed as a sage. I knew he was-n’t a doctor, yet he was the one whose words counted. “Franksays there’s a new blood product. It means surgery could besafe.” “Frank says he’s getting his plasma as an out-patient—he’snot being admitted to hospital anymore.” “Frank says we needto push for comprehensive care.”
I knew Frank had hemophilia like I did, yet he was doing themost amazing things. He was the Consul-General for CostaRica—this was very mysterious—and was always travelingaround the world. He had a huge office at the top of Montreal’stallest skyscraper—even more impressive—which I visited onoccasion. (I now know he worked as an investment analyst atThe Imperial Trust.) And, best of all, he had season tickets forthe Montreal Canadiens hockey team and, when I was verylucky, invited me to go with him. Watching the game,we discussed everything under the sun, includinghemophilia. It was in researching this article that Icame across these words of Frank’s from the 1960s.
“I wanted to be like everyone else. I didn’t wantto be different. So I never told anyone what waswrong with me. Then it occurred to me that if allhemophiliacs hid their problem, how could we everexpect to make any progress? I felt we had to educatepeople about hemophilia, and then push, and pushhard, for better treatment and more career opportunities.So I went to the other extreme and just refused to stop talkingabout hemophilia.”
I remember my parents’ pride that this young Montrealer,who had rounded up patients, parents and physicians to foundthe Canadian Hemophilia Society in 1953, went on to create theWorld Federation of Hemophilia ten years later, with six found-ing National Members—Argentina, Australia, Belgium, Canada,France and United Kingdom. And, only five years later, hebrought many more countries to our city for one of the firstWorld Congresses. Imagine how proud Frank would be today tosee the number of WFH National Member Organizations sur-pass one hundred!
As I grew up, Frank’s youthful face, with the dark horn-rimmed glasses, was the face of hemophilia. It looked out at mefrom newspaper and magazine articles which my mother care-fully preserved in scrapbooks. Words like these influenced myparents and parents around the world in rearing children withhemophilia.
“My parents decided that they didn’t want me to live a cot-ton wool existence and they did everything possible to allow mea normal childhood. My mother later told me it was the hardestthing she ever had to do—to stand back and let me do all thethings kids normally do—and then rush me to hospital when Igot hurt.”
In these newspaper and magazine photographs, Frank wasoften flanked by prominent physicians in hemophilia care. Suchcollaboration was unheard of at the time. Chris Tsoukas,Frank’s Montreal physician, once said:
FRANK SCHNABEL: FOUNDER OF THE CANADIAN HEMOPHILIA SOCIETY
AND THE WORLD FDERATION OF HEMOPHILIA
by David Page
“Frank was the one who dared break into the medical estab-lishment and propose a meeting of minds, a cooperationbetween the care givers and the care receivers. He was the onewho by organizing and bringing together hemophiliacs madethem feel they were not alone.”
Frank’s contribution was more than that of a patient advo-cate. He became as competent on hemophilia issues as any ofthe trained medical personnel. Again, in the words of ChrisTsoukas.
“Professionally, he was invaluable to me, in helping mebegin my research career. He was my sounding board, the per-son I knew I could talk freely and openly with. He was a greatlistener and always gave me good advice and encouragement.He helped me to keep my enthusiasm for my work, even duringtimes of gloom.”
Frank’s contribution was recognized outside the hemophiliacommunity. Among many other decorations, he was awarded
in 1967 the Centennial Medal by the Government ofCanada. In 1970 the International Society for the
Rehabilitation of the Disabled designated Frank‘Representative to the Assembly’ in recognition ofdistinguished service rendered to advance the wel-fare of disabled persons throughout the world.
It is without doubt that Frank’s most importantachievements were on the world stage. One observer
commented, “To most people the world is a big placeto live in; to Frank Schnabel, the world was his back-
yard. He used the newspapers, telex and the telephone toshrink the world to manageable size.” Imagine what he
would have accomplished in the era of E-mail and Internet!Frank’s extensive travel on behalf of WFH could not have
been without sacrifice. The Reverend Alan Tanner, formerChairman of the WFH, said of Frank:
“I think he must have been one of the most widely traveledpeople ever. And on all those occasions I have seen his singleminded devotion to the national member organizations and toindividuals who came to him for advice and guidance. He wasthe pioneer in establishing this great blood brotherhood. Andall of this was achieved at great personal cost to himself,because he never spared himself. Lesser men would not havestarted the journey.”
I happened to be in hospital in Montreal at the same time asFrank just before his death in 1987 at the age of 61. His hospitalroom had become the nerve centre of the WFH. Frank was sum-moning people to his bedside so that his work could continue.Few of us could tell how ill he was. Only weeks later, TheReverend Tanner spoke these words in Frank’s eulogy.
“For many years to come, the names of the World Federationof Hemophilia and Frank Schnabel will be synonymous; andmany boys and men throughout the world look to FrankSchnabel as their model and their hero because he demonstrat-ed so clearly that they could rise above the complications ofhemophilia and turn adversity into triumph.”
This tribute to Frank Schnabel first appeared in the March 2003 issue ofHaemophilia World, on the occasion of the 40th anniversary of theWorld Federation of Hemophilia.
H E M O P H I L I A T O D A Y S U M M E R 2 0 0 2
REGISTRATION FORMFIFTY YEARS TO REMEMBER! • MAY 8-11, 2003CANADIAN HEMOPHILIA SOCIETY 50TH ANNIVERSARY CELEBRATION
Hotel Accommodation
Le Centre Sheraton Montreal is the site of all meetings. For your convenience, arrangements have been made with Le Centre Sheraton Hotel as well as with the alternativehotels listed below. As shown on the map, all these hotels are at a walking distance or accessible by bus from the Conference site. Please reserve directly with these hotelswhere rooms are set aside until the dates indicated. Late reservations are subject to availability and Conference rates may not apply. When making your reservation, makesure to identify yourself as a participant at the CHS 50th Anniversary Celebrations. Space is limited so reserve early.
Hotel Conference Rate For Reservations Deadline (Plus taxes) for Reservations(Single or double)
Le Centre Sheraton $189 1-800-325-3535 March 141201 Boul. René Levesque West
Le Nouvel Hotel1740 Boul. René-Levesque West $139 (514) 931-8841 March 24
Days Inn Metro Centre $129.95 (514) 938-4611 April 71005 Guy Street
Please fill in the form below and return it as soon as possible to:Canadian Hemophilia Society, 625 President-Kennedy Ave, Suite 1210 Montreal, Quebec H3A 1K2
NAME:
ADDRESS:
CITY: PROVINCE: POSTAL CODE:
TELEPHONE NUMBER: E-MAIL ADDRESS:
ARRIVAL DATE: DEPARTURE DATE:
Registration fees: BEFORE APRIL 15TH AFTER APRIL 15TH
FULL BANQUET FULL BANQUETCONFERENCE* CONFERENCE*
PERSON WITH A BLEEDING DISORDER $100 $ 50 $125 $ 60
FAMILY MAXIMUM $150 $100 $175 $120
HEALTHCARE PROVIDERS — $ 50 — $ 60
*Full conference includes Research Symposium, Consumer Workshops, Tour of CHS Public Display and Banquet.(Please be advised that these registration fees do not include registration for the 1st Canadian State of the Art Conference on von Willebrand Disease). Cheques should be payable to the Canadian Hemophilia Society.
I would like to register for the following consumer workshops. Please print name of participant(s) beside your choice(The following sessions will only be offered depending upon sufficient registration.)
Navigating the Emergency Room ❑ English ❑ French
Name(s)
Treatment Update on Hepatitis C ❑ English ❑ French
Name(s)
Women with Bleeding Disorders ❑ English
Name(s)
Current Issues in the Safety & Supply of Blood Products ❑ English ❑ French
Name(s)
Pain: The Fifth Vital Sign ❑ English
Name(s)
St. Catherine Street
René Levesque Boul.
Guy
Str
eet
Nou
ntai
n St
reet
St. Antoine Boul.
DAYSINN
LE CENTRESHERATON
LENOUVELHOTEL