Embed Size (px)
DESCRIPTION
Endodoncia
Citation preview


Problem Solving in Endodontics
Prevention, Identification, and Management

James L. Gutmann DDS, Cert Endo, PhD (honoris causa), FACD, FICD, FADI Professor Emeritus, Department of Restorative Sciences
Baylor College of Dentistry
Texas A&M University System, Health Science Center
Dallas, Texas;
Diplomate, American Board of Endodontics
Honorary Professor, School of Stomatology
Wuhan University
Wuhan, China
Paul E. Lovdahl DDS, MSD, FACD, FADI Practice Limited to Endodontics
Sea Mar Community Health Center
Bellingham, Washington
with 1663 illustrations
Problem Solving in Endodontics
Prevention, Identification, and Management
5th Edition

3251 Riverport LaneMaryland Heights, Missouri 63043
PROBLEM SOLVING IN ENDODONTICS: PREVENTION, IDENTIFICATION, AND MANAGEMENT ISBN: 978-0-323-06888-8
Copyright © 2011, 2006, 1997, 1992, 1988 by Mosby, Inc., an affiliate of Elsevier Inc.
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Cataloging-in-Publication Data or Control Number
Gutmann, James L. Problem solving in endodontics : prevention, identification, and management / James L. Gutmann, Paul E. Lovdahl.—5th ed.
p. ; cm.Includes bibliographical references and index.ISBN 978-0-323-06888-8 (hardcover : alk. paper) 1. Endodontics. I. Lovdahl, Paul E. II. Title.[DNLM: 1. Dental Pulp Diseases. 2. Endodontics—methods. 3. Root Canal Therapy—methods.
WU 230 G9835p 2011]RK351.G88 2011617.6′342—dc22
2010015577
Working together to grow libraries in developing countries
www.elsevier.com | www.bookaid.org | www.sabre.org
Vice President and Publishing Director: Linda DuncanExecutive Editor: John DolanDevelopmental Editor: Brian S. LoehrPublishing Services Manager: Catherine JacksonSenior Project Manager: Rachel E. McMullenDesign Direction: Teresa McBryan
Printed in China
Last digit is the print number: 9 8 7 6 5 4 3 2 1

v
Preface
The discipline of endodontics seems to be at the cross-roads in its evolutionary process and growth as a specialty of dentistry. Over the past few years, the
practice of endodontics has been enhanced by remarkable technologic innovations and evidenced-based research. A wealth of new information has led to a better understanding of the biological basis for treatment, which has resulted in improved clinical treatment and more predictable outcomes. Interest in the provision of quality endodontic procedures and tooth retention remains foremost with many dental practitioners.
At the same time, however, our educational processes within this discipline are ailing. Recruitment to full-time faculty positions in endodontics has been a major challenge, especially from the ranks of recent graduates of endodontic specialty programs in the United States and Canada. The same is true in many countries around the world. The modest success of filling some teaching positions from the ranks of the retired military is offset by the comparatively short career potential of these people. Furthermore, many of these indi-viduals are choosing a more lucrative “second career” in private practice. Moreover, whereas part-time faculty do play a role in the educational process, most do not possess peda-gogic expertise. Teaching, therefore, may often be empiri-cally-based, which at times can undermine even the most sophisticated and well-structured curricula. Despite the addi-tion of many foreign trained educators in the United States and elsewhere, numerous faculty positions remain unfilled with no prospects in the offing. In some schools, endodontic departments have lost autonomy and have been consolidated into megadepartments, which ultimately weakens the posi-tion of endodontics in the competition for curriculum time. Who then will teach the students of tomorrow?
The astute observer will also note that over the course of recent years there has been the loss of many enduring and influential figures in endodontic education. Not only are these individuals remembered for their inspirational teaching but also for their self-sacrificial commitment to excellence in all aspects of endodontics. An attempt at a complete list would be futile as the definition of “great” is elusive. Never-theless, today one wonders who are the leaders that can replace Irving Naidorf, Gerry Harrington, I.B. Bender, Sam Seltzer, Hank Van Hassel, Don Arens, Harold Gerstein, Tom Mullaney, Gene Natkin, Thom Dumsha, and Ed Osetek? Who will be the stalwarts of the future or have we
seen the twilight of the “endodontic professor?” Who will be remembered for their intellects, the rigor of their educational programs, and their enduring influence on students? Who will bring the necessary passion to the teaching of endodon-tics and the inquisitive energy to the research that is essential within this discipline?
Unlike many popular novelists or screen writers of our time, we did not conclude the previous editions of this book with visions of a “sequel” or plans for the “next install-ment.” The impetus for the creation of a fifth edition arose gradually during many think tank endeavors and reflective sessions in the years since the publication of the fourth edition. It is obvious that there have been significant con-tributions from research that have impacted on current practice. Some concepts that were novel at the time of the fourth edition are now fully integrated into modern theory and practice. Other prompts came from readers and com-mentaries on our previous efforts. Our own experience and observations have led to certain additions and changes as well as an increasing need to present the information within from a global perspective. For example, tooth numbering systems differ widely throughout the world. Since this book has achieved a surprising and gratifying international pres-ence, revisions were required to rename each tooth using international standardized terminology, e.g., maxillary first molar, etc. In the same way, we have attempted to use diction that will be as clear as possible to nonnative English readers.
Many excellent endodontic texts currently available are anthologies of chapters written by a multitude of different and varied authors. A distinct disadvantage of this approach is the paucity or lack of communication among writers. The fifth edition of Problem Solving in Endodontics is the product of two of the original authors. The intense collaboration during the long creative process has resulted in a uniquely cohesive and integrated text. For example, concepts and figures are frequently cross referenced from other chapters where additional information will be helpful. A cursory examination of the table of contents will reveal a complete restructuring of the text material into sections of related topics. There are several completely new chapters. Every chapter carried forth from the previous edition has been almost completely rewritten.
In terms of content, the first obvious change is the expansion of diagnosis in this edition. It has become clearer

vi Preface
that problem solving must include a more complete process of diagnosis. Observations of referred cases in the private practice experience of the authors underscore diagnostic and treatment planning errors which in some cases, have led to a succession of calamities in treatment. Occasionally, endodontic treatment was completely unwarranted. Our objective in expanding the diagnostic section is to give the reader a diagnostic process that can confirm or rule out pathoses related to issues of the pulp and supporting peri-odontium in the vast majority of clinical situations. Likewise, it was not our intention to be encyclopedic. Rare condi-tions are omitted as we believe the practitioner provides better service by ruling out the most common possibilities and referring the patient when a diagnosis cannot be reached. For our international audience, we have included as many alternate diagnostic and treatment procedures as possible so that proper diagnosis can be done with the materials available.
A second major expansion is the section on surgical pro-cedures. The ability to treatment plan and perform a multi-plicity of surgical procedures are hallmarks of the specialty of endodontics, and therefore it will be obvious that tooth retention is a paramount objective of this text. The discussion of periapical surgery is intentionally limited to the anterior teeth and it is presumed that readers who will use this text for acquiring surgical techniques will be novices. The text is written with this in mind and with increased attention to detail. Periapical surgery on posterior teeth is a subject that
requires extensive surgical experience and is not within the scope of this text.
A third addition in content consists of references through-out the text. The amount of research since the previous edition is staggering. We have endeavored to include as many of the relevant sources as possible to support the advocated philosophy. Whenever possible, evidence-based or best evi-dence references are cited to support the clinical choices. Furthermore, because textbooks can often be out of date by the time they go through the gymnastics and gyrations of publishing, a recommended additional reading list is included with updates added as close as possible to the final process of publication. It is anticipated that references will be website based and usable for academicians and lecturers.
Fourth, entire chapters are spent on irrigation and disin-fection and on working length determination, with extensive literature assessments and clinical directives, because of the importance that these two entities play in the achievement of success. Furthermore, issues of diagnosis and treatment of tooth hypersensitivity along with vital pulp therapy have been expanded and put into clinical perspective, as well as techniques to revitalize the compromised tissues in teeth with immature apical development—often referred to erroneously at this early stage of its evolution as “regenerative endodon-tics.” In doing so it should be understood by the reader that endodontic therapy does not equal root canal treatment, as this discipline encompasses many diagnostic and treatment modalities.

vii
Acknowledgmentstext of this nature requires the input from many inter-ested and loyal supportive individuals who believed in the passion and commitment of the authors.
PEL would like to express appreciation for the immeasur-able contribution made by his daughter, Jennifer Ludwigson in the production of digital images, location of charts and records, and willingness to be a subject in clinical photo-graphic demonstrations. Thanks also to Lorrie Ebergson, who has the most amazing memory for cases and patient names. Thanks to Diane Edson for setting up photographic demonstrations and sometimes being the subject as well. Thanks to Joe Ludwigson for help with the skull photogra-phy. I appreciate the cases provided by the colleagues who are referenced in the legends. Finally thanks to my wife Kathy, for longsuffering patience and grace throughout the project.
JLG would like to express appreciation to all of his former graduate students and to all the professionals, globally in 51 countries, that he has had the honor and privilege to teach and guide in the achievement of quality, predictable
endodontic procedures. I have learned from you in the process and furthermore you have kept my passion for teach-ing alive and well. I would also like to thank the endodontic staff members at the Medical College of Virginia, University of Maryland at Baltimore and Baylor College of Dentistry for their support in my vision of endodontic excellence during my 27 years of full-time teaching. Gratitude goes out to the enthusiastic and supportive dental assistants and administrative staff that have assisted me in the practice of endodontics. Finally, for the many hours of patience, under-standing, and support provided to me by my wife Marylou, I express my deepest gratitude.
We also wish to thank John Dolan, Executive Editor, for believing in us and using a gentle prod to move us forward with this edition; to Brian Loehr, Developmental Editor, for his creative ideas and excitement in the editing of this text and preparation of the layout and presentation of the mes-sages within; and Rachel McMullen, our Senior Project Manager, for keeping on schedule and ensuring that we always strove for excellence every step along the way.
A

viii
Dedication
It is both a privilege and honor for the two authors of this text to dedicate this vastly revised edition of Problem Solving in Endodontics to Dr. Sonia Ferreyra of Córdoba,
Argentina. We have come to recognize that Sonia is an indi-vidual with a unique vision for dental education and the will to bring it into reality. Early in her teaching career, she was recognized by her peers and her students for her ability to incorporate the science of dentistry with the highest stan-dards of clinical care. Gradually, the needs and requests of her postgraduate students led to a formalized program of study that now encompasses a 30-month curriculum focus-ing on the areas of endodontics and dental trauma.
Today, Dr. Ferreyra is the President of FUNDECO, a Scientific Foundation for Continuing Education in Dentistry in Argentina. She established this Foundation in 2002 with the goal to educate highly qualified dental professionals in formative knowledge and clinical skills. Her vision “to save teeth” includes education, patient care, and clinical research, which is most laudable in this day and age. In addition to continuing educational programs at the highest possible level, FUNDECO has established school educational programs, sports educational programs, and emergency unit programs to manage dental trauma in local hospitals. Under her astute guidance, treatment protocols and rehabilitation programs for patients have been developed with services provided free of charge. She has initiated research programs that would contribute to the ultimate delivery of quality and predictable clinical care to the community at large. She has been directly responsible for 359 postgraduate students, of which 185 have successfully completed their studies and remain active with the workings of the Foundation. Another 174 are presently in various stages of their educational and research pursuits. She continues to influence dental professionals in Uruguay, Paraguay, Chile, Argentina, and Spain.
Sonia has become a beacon of hope for many dental professionals and a life-line to tooth retention and quality oral health care for so many residents of these countries in South America. She is passionate about her mission; deliber-ate in choosing her students; unrelenting in her pursuit of science and both educational and clinical excellence; and compassionate and caring in all of her undertakings. She is loved by all of her students and through both good times
and challenging times in the establishment of FUNDECO, she has endeared herself to so many dentists, imbuing them with her wisdom, her impeccable values, and her staunch professional integrity. Dr. Ferreyra holds both a DDS and PhD degree and is a member of both the American Asso-ciation of Endodontists and International Association of Dental Traumatology.
For JLG as a contributor to Dr. Ferreyra’s efforts for the past 10 years, this has been an amazing and rewarding rela-tionship, especially during the evolution and growth of her Foundation. For PEL, the past 5 years of contributions have expanded his horizons and his love for teaching on all levels, spurred on by the thirst for knowledge and enthusiasm dis-played by all of Sonia’s students. Together, we are both humbled and proud to dedicate our efforts to this extraordi-nary and enthusiastic young lady, who is both a true “amiga” and an inspiration for so many colleagues. Sonia we salute you and thank you for your immense contribution to end-odontics and dental trauma.
James L. GutmannPaul E. Lovdahl
From left: Dr. James Gutmann, Dr. Sonia Ferreyra, and Dr. Paul Lovdahl.

ix
Es un honor y privilegio, como autores de este libro, dedicar esta ampliamente revisada edición de “Resolvi-endo Problemas Endodónticos” a la Dra. Sonia Fer-
reyra de Córdoba, Argentina. Hemos llegado a reconocer, que Sonia es una persona con una visión única por la edu-cación odontologica y el deseo de llevarlo a la realidad. Tem-prano en su carrera de docente, fue reconocida por sus colegas y estudiantes por su habilidad de incorporar la ciencia odon-tológica con los más altos niveles de cuidado clínico. Gradu-almente, las necesidades y demandas de sus alumnos de post-grado, resultaron en un programa formal de estudio, que hoy en día consta de un currículo de 30 meses de duración, enfocado en áreas de endodoncia y trauma dental.
Hoy, la Dra. Sonia Ferreyra es la presidente de FUNDECO, una Fundación científica para Educación Continuada en Odontología en Argentina. Ella estableció esta Fundación en el año 2002, con el propósito, de formar odontólogos alta-mente calificados, en conocimientos formativos y habilidades clínicas. Su visión de “salvar dientes” incluye, educación, cuidado del paciente y investigación clínica, la cual es elo-giable en estos tiempos. Además de programas educación continuada del más alto nivel, FUNDECO estableció pro-gramas educativos en escuelas, programas educativos de deportes y programas de unidades medicas para poder manejar el trauma dental en hospitales locales. Bajo su astuta guía, han sido desarrollados protocolos de tratamiento y de programas de rehabilitación con servicios prestados sin costo alguno para el paciente. Ella ha iniciado programas de inves-tigación que contribuirían en grande la entrega de calidad y cuidado clínico predecible para una amplia comunidad. La Dra. Sonia Ferreyra es directamente responsable de 359 egresados de Post-grado, de los cuales 185 han completado satisfactoriamente sus estudios, y se encuentran activos tra-bajando con la Fundación. Otros 174 están actualmente en varias etapas de sus carreras educacionales y de investigación.
Ella continúa influenciando a odontólogos en Uruguay, Para-guay, Chile, Argentina y España.
Sonia se ha convertido en faro de esperanza para muchos odontólogos, y en una línea de vida, para la retención de dientes y calidad en el cuidado oral para muchos residentes de estos países en Sur América. Ella tiene pasión por su misión; selecciona muy bien a sus estudiantes; persistente en su destino, en cuanto a la investigación científica y en su búsqueda de la excelencia educacional y clínica; también en cuanto al cuidado compasivo de sus pacientes. Es una doctora muy querida por sus alumnos y en todo momento ya sea bueno o desafiante en FUNDECO, ella se ha puesto siempre en disposición muchos Odontólogos, enseñándoles de su experiencia y sabiduría, con valores impecables y su gran integridad profesional. La Dra. Ferreyra posee 2 diplomas, uno como Odontóloga y otro de PHD, es miembro de la Sociedad Americana de Endodoncia, y de la Sociedad Inter-nacional de traumatología dental.
Para JLG como contribuyente a los esfuerzos de la Dra. Ferreyra durante los últimos 10 años, esta ha sido una relación de gran satisfacción, especialmente durante la evo-lución y el crecimiento de su Fundación. Para PEL, los últimos 5 años de contribuciones han expandido sus hori-zontes y su amor por enseñar a todos los niveles, empujado por la sed de conocimiento y el entusiasmo demostrado por todos los alumnos de la Dra. Sonia. Juntos, nos sen-timos al mismo humildes y orgullosos de dedicar nuestros esfuerzos a esta extraordinaria y entusiastica joven mujer, quien significa una verdadera amiga y una inspiración pro-funda para muchos colegas. Sonia, te saludamos y te agra-decemos por tu inmensa contribución a la endodoncia y al trauma dental.
James L. GutmannPaul E. Lovdahl
Dedicación

x
New to this EditionTo help you make the best clinical decisions,
this edition contains new chapters and new sections on diagnosis
and treatment planning!
Use of new material in vital pulp therapy.Expands the endodontists’ capabilities into differential diagnosis.
The Surgery section has been expanded with new case studies, and more
in-depth coverage of indications and applications for surgeries!

xi
New Illustrations!
Drawings and radiographs that identify clinically-important and potential anatomic problems.
Controversies in the biologic and clinical aspects of working length determination

1
part 1 Problem Solving in Diagnosis and Treatment Planning
Chapter 1
Problem Solving in the Diagnosis of Odontogenic Pain
Problem-Solving ListProblem-solving challenges and dilemmas in diagnosis addressed in this chapter are:
Taking an Accurate Dental History
Interpretation of Historical Data and Subjective Findings
Clinical Examination: Objective Findings
Visual inspection
Use of the explorer
Palpation
Percussion
Bite pressure test
Periodontal probing
Mobility
Radiographic Interpretation
Differential Tentative Diagnosis
Sensibility (Vitality) Testing
Theory
Applicable and Pertinent Testing Techniques
Cold test
Heat test
Dental (rubber) dam application for thermal pulp testing
Electric pulp test
Anesthetic test
Test cavity
Clinical Diagnostic Scheme Based on Test Responses
Normal
Reversible pulpitis
Irreversible pulpitis
Irreversible pulpitis not localized
Necrotic pulp
Aerodontalgia/Barodontalgia
Putting It All Together: the Final Pulpal Diagnosis
A few moments’ consideration of the original cause of trouble at the apex of roots enables us to realize what is required to be accomplished in the way of successful treatment. If the original cause is admitted to be irritation from decomposing pulp, its removal will in most cases affect a cure.27
W. WHITEHOuSE, 1884
Making an accurate endodontic diagnosis is a problem for many dentists. The solution to this problem is neither easy nor lends itself to a method that can be reduced to a series of simple steps. A further complication is that most clinicians find it difficult to challenge long-held concepts and practices and resist the notion that these beliefs may be biased. Their experience, under examination, may be limited. There is also a tendency to place trust in authorities without asking how these authorities came to be dominant influences in clinical thinking and practice. When attending a continuing educa-tion course, it is not unusual to have thoughts, such as “I already know this,” or “I have heard this before,” or “There is nothing new to be learned here.”
Dentists attend continuing education courses or read pro-fessional literature with the intent to improve their knowl-edge and abilities. In reality, most of the information in a course may not be new to an experienced clinician. What is often missed by clinicians, however, is the importance of detail, relative significance of concepts, and how this unique information can enhance their diagnostic acumen and clini-cal data gathering. Upon returning to the practice of den-tistry, the information presented in the educational experience is often forgotten, and the clinician is destined to repeat the same errors they have been perpetuating for years. In an attempt to minimize this nonproductive process, and in the hope that ingrained patterns of erroneous thinking in the diagnosis of pulpal and periapical pathosis states will be clari-fied, simplified, and enhanced for the dental clinician, this chapter will provide detailed diagnostic methods used by the authors and most endodontic specialists.

2 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
• “Can you recall what you were experiencing prior to thetreatment performed by the other dentist?”
Hearing the patient describe their pain is essential to under-standing their problem, interpreting the information gath-ered, and asking additional probing questions when necessary. Some patients may be accompanied by a spouse, parent, or friend who wishes to contribute to the interview. Generally, this is not very helpful. It is best to address the patient for this information.
• “When do you feel this pain?”• “Is it a constant pain? If not, describe when or how it
occurs and how long it might last.”• “Has the pain occured more frequently or lasted longer
in the past few days or weeks?”• “Is the pain stimulated by something hot or cold?”• “Is there a time of day when the pain seems to be
worse?”• “Does the pain awaken you at night?”• “How would you describe the pain? Is it dull? Is it sharp,
like an electric shock?”
At this point, it is appropriate to ask the patient about any physical perceptions or concerns.
• “Have you noticed any swellings, or do you feel swollenin any specific area?”
• “Is there an area of your face that is tender to touch?”• “Are there any teeth that hurt or are uncomfortable
when you chew or after you have eaten?”• “Do any of your teeth feel loose, or are you biting on
any tooth sooner than other teeth?”
Interpretation of Historical Data and Subjective Findings
Interpreting historical data and subjective findings usually occurs simultaneously as they are secured, and these initial impressions usually direct the subsequent questioning. As a broad overview, let us consider these questions in the order they have been presented. Responses to the initial questions about the basic dental complaint can often lead directly to a clinical examination and a rapid diagnosis. If the problem were an acute abscess, for example, the patient would probably give enough information in the first two or three sentences to make a tentative diagnosis of abscess. Subsequent questioning would then concentrate on the pres-ence of physical signs and symptoms of infection. It would remain to be determined if the abscess is of pulpal, peri-odontal, or other etiology.
Patients who have been experiencing chronic pain prob-lems may not be feeling any pain at the moment of examination but can describe the chronic nature of it in detail. Endodontic problems can develop episodically over a period of time but will most often show a pattern of decreasing periods of comfort and increasing periods of
Most concepts may already be familiar; the intent of this chapter is to provide a context for each method or test that will emphasize its unique importance in a problem-solving format. Not all diagnostic tests, examination methods, weighing of historical information, or patient subjective data are relevant to every case. Through clinical examples, the value of each approach will be emphasized to assist the clini-cian in reevaluating the entire diagnostic process and the incorporation of a realistic and meaningful approach to making a final diagnosis.
Taking an Accurate Dental History
The most common complaint that brings people to the dentist is pain. It is usually an acute problem termed “an emergency” by the patient, who typically characterizes it as being swollen, having pain to biting, being unable to tolerate temperature changes, or the statement, “I have an infection in my tooth.” Occasionally the dental problem is the result of trauma that is usually obvious by appearance; or the patient arrives with complaints of vague or nonlocalized pain. In some cases, pain may not be a reason for the dental con-sultation at all. The specific nature of the problem is sorted out during the consultation interview, where patient state-ments and other critical information are collected. In addi-tion to revealing much information about the dental problem, this initial contact, if done in an open and nonthreatening manner, will usually disclose patients’ expectations, previous experiences, fears, and their understanding of the nature of their dental problem.
Because pain is so variable and its perception so subjective, history taking will require gathering and interpreting appro-priate information. Patients frequently have strongly held preconceptions that may not be true or relevant. For example, often they believe they know which tooth is causing the problem. The clinician must be able to distinguish informa-tion that is useful, such as “I cannot bite on this tooth,” from that which is subjective, such as “The pain hurts me in these three teeth.” It is highly unlikely there are three teeth creating the patient’s problem, but it is quite common for pain to be referred to an area larger than the area of the offending tooth. A few pertinent questions to obtain greater insight into the patient’s specific problem may include:
• “Is there a tooth that is bothering you at this time?”• “Are you experiencing pain?”• “How would you rate the pain on a scale of 1 to 10?”• “How long has the pain been present?”• “When did you first experience pain?”
In some cases, pain has continued after another clinician has attempted to manage the patient’s problem. In these cases, the following questions may be appropriate.
• “Is the pain you are now experiencing any different fromthe pain you had before the previous treatment?”

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 3
discomfort. This may even be followed by periods of com-plete comfort.
The overall time frame for tooth problems is much shorter than for myofascial pain problems, which often come and go over a period of years. It is helpful to find out if there have been periods of complete resolution. This kind of history is also consistent with myofascial pain related to nocturnal bruxing or clenching, which is discussed in Chapter 6 on nonodontogenic pain. Within this diagnostic theme, it is common to awaken in the morning with facial pain. Both endodontic problems and myofascial pain problems can awaken patients from sound sleep, which is one of the few relatively objective measures of the severity of pain. Other typical symptoms of myofascial pain problems may mimic endodontic pathosis as well. As will be discussed in detail in Chapter 6, patients who have developed trigeminal neuralgia may experience severe and debilitating episodes of electric shock–type pain but are curiously never awakened from sleep with pain.
If the patient has not experienced appreciable pain, responses to the probing questions during data gathering often focus on a nodule or “bump” noticed on the mucosal surface or an area that is noticeably tender to touch. These findings may indicate a developing periapical lesion or a draining sinus tract. Other possibilities could include a wide range of possibilities, from a normal but previously unrecog-nized exostosis to a small swelling associated with blocked ducts of minor or major (Stensen’s duct) salivary glands. Diagnosis and treatment of many of these etiologies is beyond the intended scope of this book. Our purpose here is to rule these out as having a pulpal or periapical origin or focus.
Finally, some patients who come for a routine examina-tion are found to have a clinical lesion of possible pulpal or periapical origin or a radiographic lesion discovered on the routine radiographic survey (see Chapters 2 and 3). It is still important to inquire about any history associated with these lesions. Many people may recall episodes of pain or local swelling in the past that may assist in clarifying these findings and providing a more accurate diagnosis. On the other hand, the radiographic lesion or interpretation of such may not be of pathologic origin.
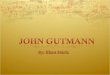
CLINICAL PROBLEMProblem: A 52-year-old male was seen on an emergency basis. His chief complaint was of acute, spontaneous pain episodes in the mandibular left molar area (Fig. 1-1, A). Visual examination revealed no caries or fracture lines in either the left maxillary or mandibular teeth. There was a very large amalgam restoration in the mandibular first molar, which was the area where the patient felt the pain was originating. Thermal sensibility (pulp) tests, however, elicited normal responses from all teeth in this area.
Solution: Failure to reproduce the patient’s chief complaint during the examination of this quadrant of teeth resulted in conducting further tests in other areas of the left side. Further tests were then conducted on the opposing teeth. The heat test elicited an acute, severe painful response on the maxillary second molar. A radiograph of this area revealed gross caries (see Fig. 1-1, B). Although there was no visual evidence of caries clinically, on removal of the occlusal composite resin, gross marginal leakage was apparent. Root canal treatment was indicated only on the maxillary second molar.
BA
FIGuRE 1-1 A, Left mandibular molars respond normally to thermal tests. B, Maxillary second molar with evidence of gross caries.
Clinical Examination: Objective Findings
Visual InspectionClinical examination specifically for an endodontic diagnosis will focus on two areas: causative factors in the teeth (pulpal inflammation, infection, etc.) and signs of periapical pathosis in the soft tissues due to spread of an inflammatory/infectious process from the pulp.1,2 All of the teeth on the side of pain should be visually inspected. Gross caries is an obvious etiol-ogy for painful symptoms. Occasionally in a case of sponta-neous pain, gross caries may be observed in a tooth, almost invariably a molar, in the opposing arch from where the pain has been felt. Further testing in such a case often indicates that the teeth in the area of felt pain are normal, whereas the opposing carious tooth is the source of the referred pain.

4 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
FIGuRE 1-2 Coronal fracture evident on intact marginal ridges. The mesial fracture line is obvious (black arrows). The distal extension of the same fracture is not as apparent but is visible (red arrow).
BA
FIGuRE 1-3 A, Coronal fracture extending over distal marginal ridge. B, Periodontal defect from extension of crack below crestal bone (arrows).
A B
FIGuRE 1-4 A, Fracture lines evident on distal marginal ridge and lingual developmental groove of mandibular second molar. B, In this case, the fracture resulted in complete separation of the cusp from the crown.
Another important process in the clinical examination is to search for the presence of coronal fracture lines.5 The majority of fractures occur in a mesial-distal direction, and frequently these are obscured by coronal restorations (Fig. 1-2). It is often possible to observe them only on the intact marginal ridges, but they may extend to or below the level
of crestal bone on the interproximal surface (Fig. 1-3). Frac-tures may also be observed on the buccal or lingual surfaces.26 Two fracture lines on different surfaces may be evidence of a complete cusp fracture. For example, the combination of a deep lingual fracture line in the lingual groove of a mandibular molar and a fracture line on the distal marginal ridge distal could indicate the fracture of the distal lingual cusp, which is a common factor in the initiation of pulpal inflammation (Fig. 1-4).
The soft tissues should be examined for physical signs of redness and swelling that may indicate that the periapical tissues have become inflamed or infected. Typically these specific physical signs would be evidence of a sinus tract, local swelling over the apices, or regional swelling (Fig. 1-5). Dis-coloration and edema may also be clues in a site of recent acute infection. In view of the original complaint of the patient, the clinician must be careful to avoid being misled by the accidental discovery of additional problems. For example, if the original complaint included a current history of acute thermal sensitivity, the visual observation of a sinus tract in the alveolar mucosa or attached gingiva on a single-canal tooth may be evidence of a pulpal problem, but it would probably not be the source of the symptoms for which the patient is seeking treatment. In this situation, the patient may have at least two distinct problems.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 5
FIGuRE 1-5 Swelling resulting from an acute periapical abscess.
FIGuRE 1-6 Pericoronitis associated with a partially erupted third molar (arrow).
Occasionally there may be signs of infection that are likely to be the source of the patient’s complaint but unlikely to be of pulpal or periapical origin. Pericoronitis around a partially erupted third molar is usually recognizable owing to its loca-tion; an endodontic problem with the second molar may have to be ruled out (Fig. 1-6). Much more common are periodontal abscesses, which may be more difficult to dif-ferentiate from periapical abscesses if periodontal disease is evident throughout the dentition.3,14 This diagnostic problem will be discussed further in the subsequent section on peri-odontal probing.
The clinical examination is conducted with a series of instruments and techniques that might be considered the “tools of problem solving.” Each test or assessment technique can reveal a clue that may impact or confirm the ultimate
diagnosis. Seldom will it be necessary to do all of the tests or techniques listed, but it is equally important not to jump to conclusions too early in difficult diagnostic cases. The process of clinical examination is intended to both identify the source of the symptoms or observed pathosis and to rule out pathosis on adjacent teeth. It may be difficult in some cases to repro-duce reported symptoms, but it often will be possible to reach a confident opinion about the normality of certain teeth, thereby reaching a diagnosis through the process of elimination.
During a clinical examination, data are gathered using a multitude of tests and evaluative procedures. While some tests will focus on the status of the pulp, others will be used to ascertain the extent of the spread of pulp inflammation or infection to the supporting periodontium. At times, it is dif-ficult to separate information that is pulpally related from information related to extension of the disease process or periapically related. It is the intent of this first chapter to focus on the gathering of key information that will initially provide evidence of pulpal status. Other findings gleaned in this problem-solving process must be correlated and inte-grated with a thorough examination of the supporting peri-odontium, along with quality radiographs. These data will then be integrated into a periapical diagnosis that will be addressed in Chapter 3.
Use of the ExplorerFor diagnostic purposes, the No. 23 explorer or the DG16 endodontic explorer (both explorers can feature a No. 17 tip when the instruments are double ended) are useful for the detection of caries, open restorative margins, fractures, loose cusps, and fracture lines (Fig. 1-7). Interproximally, the extent of caries buccal lingually can be ascertained. If a cracked tooth is located in the area of pain, it is useful to explore the interproximal surface of the tooth with a fine
FIGuRE 1-7 No. 23 explorer (left) and DG 16 endodontic explorer (right).

6 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
A B C
FIGuRE 1-8 A, No. 17 explorer. B, Use of the No. 17 explorer to detect vertical fractures in the crown. C, Use of the No. 17 explorer interproximally for the detection of fractures.
No. 17 explorer (Fig. 1-8). Often it is possible to feel the presence of a deep fracture line and follow it vertically along the proximal surface. Obviously, the more apical the fracture is felt, the more likely there is pulpal involvement. If the fracture extends below crestal bone, periodontal breakdown may also occur, a finding with serious prognostic implica-tions. This will be discussed in more detail in the section on periodontal probing and also in Chapter 3 on radiographic interpretation.
PalpationOne of the most informative but often overlooked evaluative procedures of the clinical examination is palpation. While not crucial for a pulpal diagnosis, for teeth with pulpal necro-sis, palpation soreness or pain may reveal the presence of inflammation associated with periapical periodontitis.10 Reflecting on the anatomy of this environment is important in the interpretation of findings in this examination. Teeth with roots that lie close to the surface of the alveolar process will more likely exhibit palpation sensitivity or tenderness. Roots covered by relatively thin labial plates of bone or no bone at all are usually in the maxilla, with the apices of the central incisors, the canines, the buccal root of the first pre-molar, and the buccal roots of the molars often located ana-tomically superficial to the bony surface.12 Examination of teeth in human skulls indicates that fenestration of the apex or sections of the root surface is common in the absence of pathosis (Fig. 1-9).8 Periapical lesions of teeth in other areas are less likely to exhibit palpation tenderness, owing to the thickness of the buccal plate or the external oblique ridge in the case of the mandibular molars (Fig. 1-10).12 Nevertheless, in conditions of an acute periapical abscess, palpation tender-ness, local swelling, and drainage through the gingival sulcus are not unusual even where the buccal bone is very thick.
PercussionPain or tenderness to tapping on a tooth (percussion) is not crucial to a pulpal diagnosis but is symptomatic of
FIGuRE 1-9 Fenestration is a normal anatomic finding.
FIGuRE 1-10 Apices of mandibular molars covered with thick, dense cortical bone. Palpation signs are less common in this area.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 7
BA
FIGuRE 1-11 A, Percussion in the vertical axis of tooth. B, Percussion perpendicular to vertical axis of tooth.
three other conditions. It may be a sequela of trauma, which applies to virtually all anterior teeth and is easy to identify by the history. A root canal procedure may not be indicated, because there may be no pulpal damage. Sensibil-ity testing (formerly known as vitality testing) would be indicated. There may or may not be concomitant palpation tenderness with traumatized teeth, but if palpation tender-ness is found, it will usually not be confined to the region over the apex.
Second, tenderness to percussion may be the result of periapical inflammation due to either a necrotic or an acutely inflamed pulp.1,10 In these cases, concomitant pal-pation tenderness may or may not be found only over the apices. Depending on the acuteness or chronicity of the underlying pathosis, both the percussion tenderness and concomitant palpation tenderness can be either mild or extremely acute. Included in this category are teeth that have coronal fractures, since it is the pulp that becomes painful from the flexing of the cracked cusp. However, sensibility tests would be necessary to establish a pulp diagnosis.
Third, tenderness to percussion may be a symptom of occlusal trauma, most often the result of nocturnal clenching or bruxing.1 The presence of a concomitant tenderness to palpation with this condition is rare. Fur-thermore, the pulps of affected teeth respond normally to sensibility testing. It is common to find more than one tooth equally sensitive and a history of episodes of dis-comfort separated by intervals of complete comfort. The reader is referred to Chapter 6 for additional information on this topic.
Percussion testing can be done using the handle of a mouth mirror to tap several teeth in the opposite dental arch along their long or vertical axis (occlusal direction) to estab-lish in the patient’s mind the condition of normality (Fig. 1-11, A). Ideally a contralateral tooth from the tooth in question should be chosen; if available, a previously root-treated, symptom-free tooth may be used. Every effort should be made to “standardize” the degree of force used as each
tooth is tapped, even though it is not possible to measure the force.
Following percussion of the teeth along the vertical axis of the tooth, the teeth are also tapped with the mirror handle on the inner slopes of the cusps (on posterior teeth) and at 90 degrees to the long axis of the tooth (see Fig. 1-11, B). A traumatically injured tooth and a tooth with periapical periodontitis will be sensitive in any direction. Teeth that have become sensitive to percussion from bruxism may be sensitive to percussion in only one direction. If the tooth responds normally to percussion tests when performed occlu-sally but is sensitive to lateral percussion, the underlying cause is most likely an occlusal prematurity or wear pattern in lateral excursion. Visual assessment will often identify smoothed, flattened cusps or marginal ridges when wear facets are present. If the tooth is sensitive in an occlusal direction, the prematurity or wear pattern is usually in the centric contacts. Articulating paper is often helpful in survey-ing the occlusal contacts. Treatment for this problem is described in Chapter 6.
Bite Pressure TestThis is a corollary test to the percussion test. At times, patients describe an inability to chew comfortably on a side or a tooth. It is often difficult to reproduce this symptom with the per-cussion test. A bite pressure test is performed by having the patient bite directly onto a device or material placed between the teeth.5,8 This is done tooth by tooth. Do the test first on the opposite side to inform the patient what is expected and what is normal. Various materials have been used for this purpose. The wooden handle of a cotton applicator, the cotton end of a cotton applicator, an orangewood stick, the commercially available “Tooth Slooth” (Professional Results Inc., Laguna Niguel, CA, USA), and temporary dental stop-ping have all been recommended (Fig. 1-12). Most clinicians prefer a semi-hard gutta-percha type stopping material or orangewood stick. Additional information about this test is described in Chapter 6.

8 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
with the symptomatic tooth. Acute periapical abscesses will occasionally drain spontaneously through the sulcus, and upon probing in the area of swelling, purulent drainage will ensue. In most cases, the attachment will return rapidly after the initial removal of the infected pulp tissue from the root canal, often within 1 week (Fig. 1-13).
For the purposes of routine periodontal examination, the sulcus depth is usually measured and recorded at the mesial, midtooth, and distal points on both buccal and lingual surfaces. During an endodontic evaluation, however, probing should be as circumferential as possible in 1-mm increments.14 This technique will characterize the physical architecture of any infrabony defect associated with attach-ment loss. It is diagnostically important to know if the defect is narrow or wide across the circumference of the root and to determine whether the defect has a precipitous architecture or a rather gradual pattern of probing to the deepest point. Periodontal pockets tend to have a steplike or gradual archi-tecture. They are shallow at the limits and step gradually to the deepest level (Fig. 1-14, A).
The most common cause of attachment loss is periodontal disease. It is possible to confuse an acute periapical abscess with an acute periodontal abscess.3 If the symptomatic tooth
A B
CD
FIGuRE 1-12 Bite pressure test with a wooden stick. See Chapter 6 for alternative techniques.
FIGuRE 1-13 A, Local swelling associated with an acute periapical abscess. B, Probings are normal circumferentially except for a narrow 10 mm defect in the furcation. C, Post treatment radiograph indicating the bone loss associated with the apical lesion on the distal root. D, Three and a half weeks after treatment. The symptoms and the swelling have resolved completely. Probings indicate complete periodontal reattachment in the area of the former defect.
Periodontal ProbingThe value of periodontal probing in diagnosing and differ-entiating problems of pulpal or periapical origin cannot be overemphasized. Loss of periodontal attachment has a signifi-cant influence on the prognosis of treatment and the prog-nosis for tooth retention. Periodontal probing should begin

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 9
but will be distinguished chiefly by the fact that the tooth will have had a root canal procedure. Vertical root fractures of teeth without previous root canal treatment are rare. Though symptomatic, many such defects will be discovered only on probing, because they lack radiographic signs of pathosis, including a periapical lesion. Another clinical finding unique to vertical fractures is the consistent location on either the midfacial or the midlingual surface of the involved root. If the root is fractured completely through, this probing pattern will be found on both buccal and lingual sides (see Fig. 1-14, B).
Chapters 3, 4, and 19 explore the topic of fractures more fully, but from a diagnostic standpoint, the probing pattern virtually defines the presence of fracture. Whenever a defect is present for which the diagnosis may be unclear, surgical exposure is a procedure that may reveal the cause, especially following a previous root canal procedure.
Many defects will be discovered interproximally. A deep mesial-distal coronal fracture extending below crestal bone will cause the formation of a narrow periodontal pocket only present at the site of the fracture line. Probings 1 mm to either side may be normal. The difficulty of probing in a vertical direction in the interproximal space can make this discovery a challenge if the periodontium is healthy. Anes-thesia is sometimes necessary for this clinical evaluation. Some defects of this type will not be evident on radiographs, so the probings may be the only objective evidence found. This is critical to the diagnosis, since a deep, narrow inter-proximal defect would suggest a poor long-term prognosis that may be best managed by extraction.
The fracture illustrated in Fig. 1-3 has an associated inter-proximal periodontal defect. Probings confirmed that the defect extended well below the general crestal bone level of the area, and the tooth was extracted.
MobilityMobility is most often found on teeth with advanced peri-odontal disease. It can also occur in cases of acute periapical
is found to have a deep defect on probing, it will be impor-tant to know if there is generalized periodontal bone loss by probing in other areas of the dentition. The discovery of generalized bone loss and multiple deep defects would support a possible periodontal diagnosis for the symptomatic problem.11 Usually periodontal abscesses can be distinguished by normal pulp sensibility tests and a lack of periapical bone loss. If the symptomatic tooth is found to have a unique defect, the differential diagnosis would still include periodon-tal pathosis that must be ruled out by sensibility testing and assessment of the defect by the probing pattern.
If sensibility tests are negative and there is probing to the apex, the loss of attachment may be due to a draining sinus tract from a periapical abscess. A distinguishing feature of a sinus tract is the precipitous architecture of the probing pattern. Where periodontal defects tend to be broad and stepwise, a sinus tract will be characterized by normal prob-ings circumferentially and an abrupt drop into a deep and typically narrow defect.14 The probing should correspond to a periapical lesion evident on the radiograph. Continued probing beyond the tract circumferentially will reveal normal sulcus depth. On molars, the drainage tracts are often found to exit the sulcus over the furcation or interproximally. Occa-sionally, drainage tracts probe quite wide circumferentially, in some cases up to 3 or 4 mm. The closure of a sulcular drainage tract following root canal procedures should be monitored during a reevaluation appointment with new probing assessments. Many take up to a month to close, especially if the tract is wide. If there is no reattachment after 1 month, the prognosis would be very poor. Periodontal surgery for such lesions is not very successful.
The presence of chronic sinus tracts through the sulcus can be problematic and may only be discovered on routine probing. The soft tissues associated with the pulpally involved tooth may not exhibit obvious clinical signs of infection, so it is important to develop the habit of probing carefully around all teeth that have radiographic lesions.
A deep, narrow defect can also be a sign of a vertical root fracture.8 The probing pattern may resemble a drainage tract
A B
FIGuRE 1-14 A, Probing of crestal bone levels found in lesions of chronic periodontitis. B, Probing pattern of a periodontal lesion associated with a vertical root fracture. NOTE: Adjacent bone levels are typically normal.

10 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
abscess and occasionally, occlusal trauma.10 During the exam-ination, note any mobility and check the occlusion. Regard-less of etiology, occlusal reduction should be done in all cases of teeth having excessive occlusal contact, although its value has been questioned.9,25 Heavy occlusal contact will remain a contributing factor for postoperative pain and prolonged healing time.
Radiographic InterpretationChapter 3 on radiographic interpretation will cover a broad range of topics that digress from the issue at hand: odonto-genic pain. Nevertheless, it is essential to the development of a pulpal and periapical diagnostic system to include a discussion of some important concepts regarding the value
BA
FIGuRE 1-15 A, Maxillary left posterior teeth where pain is felt. Note lack of periapical signs of pathosis. B, Diagnostic testing revealed that the second premolar was the cause of pain.
FIGuRE 1-16 Typical appearance of a periapical lesion.
CLINICAL PROBLEMProblem: A 50-year-old female with a 2-month history of acute pain to heat in the maxillary left quadrant was referred to an endodontist. The symptoms began slowly, and initially the woman felt only mild pain of brief duration. The symptoms had progressively become more acute. The patient was now experiencing spontaneous pain almost continuously. She stated that her dentist has been unable to diagnose the problem because nothing has appeared on any of the several radiographs taken during this time (Fig. 1-15, A).
Solution: The diagnosis of this case will never be made on the basis of a radiograph. In almost all cases, there are no radiographic changes in cases of thermal sensitivity. The diag-nosis will always be made on the basis of thermal tests and clinical examination. In this case, though the molar teeth were heavily restored and likely candidates for endodontic involve-ment, the tooth causing the problem proved to be the second premolar (see Fig. 1-15, B).
of radiographs. First, it should not be the expectation that every pulpally involved tooth will have radiographic signs of pathosis. It is impossible to determine the condition of the pulp itself on a radiograph. The only changes to be discov-ered radiographically in these cases are those representing the loss of hard tissue, usually bone surrounding the apex. Periapical pathosis is, in turn, a consequence of pulpal necrosis and (occasionally) extreme pulpal inflammation. Routinely, teeth with pulpal symptoms (i.e., discomfort to thermal changes, etc.) will not have radiographic changes, yet they still require a root canal procedure. This is of crucial diagnostic significance.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 11
desire of the clinician is to know the physiologic condition or relative health of the pulp tissue, the tests provide only an indirect assessment through stimulation of the nerve tissue or possible blood flow.16 Fortunately, although the pulp is a complex tissue composed of fibrous connective tissue, vascular supply, nerve supply, and odontogenic cells, there seems to be a reasonable correlation between the way the nerves react to sensibility tests and the health or pathologic condition of the pulp as a whole.2 Research approaches during the middle of the 20th century sought to correlate clinical symptoms with the histopathologic status of the pulp.10,16 However, all histopathologically defined conditions were found to have a wide variety of clinical signs and symptoms. A clinically based diagnostic system emerged based on symptoms alone.22 Diagnostic pulpal entities were defined clinically and primarily by responses to thermal tests. This system, with some modifications, has withstood the test of time and clinical practice.
There are two valuable aspects to thermal testing. First, the pulp either responds or it does not. This positive or nega-tive aspect to the response indicates whether there is vital tissue, or specifically, vital neural tissues in the root canal. In this sense, the value of the thermal test is the same as the electric pulp test. In fact, if a tooth responds to either hot or cold, the electric pulp test may be redundant. As a conse-quence, electric pulp testing has value only with teeth that are unresponsive to thermal tests. The same qualifications apply to the value of a test cavity.
The second value of thermal testing is the qualitative aspect of the response. It is not only whether the pulp responds but also how it responds. This testing always begins with establishing what is normal for the patient by testing multiple teeth outside the symptomatic area. Ideally this is done by testing the tooth contralateral to the tooth in ques-tion and the teeth on either side of the suspected tooth.7 Responses of the symptomatic tooth are evaluated in com-parison to the other tested teeth. This is extremely important when there are no clinical signs of pathosis other than a history of sensitivity. The magnitude of response and the duration have significant meaning in determining the status and prognosis of the pulp. Generally, the magnitude of the response is less important than the duration. Any test response which lasts 10 seconds or longer is considered abnormal and the status of the pulp is unlikely to improve. Theoretically this is a sign of irreversible pulpal degeneration. Teeth responding in this manner are indicated for root canal treatment.
Ideally, the object of thermal testing is to reproduce symp-toms reported by the patient. Most of the time this will occur, and the diagnosis will be established rapidly. In many cases, however, this will not be possible. Degeneration of the pulp is a dynamic process in which the symptoms tend to change over time. Symptoms felt a week prior to the visit may no longer be felt at the time of examination. Neverthe-less, it is extremely unlikely that the pulp has recovered to complete normality. In these cases, any abnormal responses
Inflammation and infection of the periapical tissues are the result of necrotic tissue products and bacteria that emanate from the apical foramen and sometimes from lateral canals that can be present at a separate location on the root. The same process occurs in cases of failure of previous root canal treatment. This disease process will cause eventual resorption of the surrounding bone. It is the loss of bone that produces the characteristic radiolucency observed in the periapical area (Fig. 1-16). In some cases of acute periapical abscess, there are no radiographic changes even though there may be swell-ing and acute pain. These situations can be explained by the suddenness of onset. Radiographic evidence of apical bone resorption will require as much as 7 days or more to occur after the onset of an acute periapical abscess. In these cases, while no lesion is observed at the time of emergency treat-ment, a lesion may be present at a subsequent appointment when the tooth is comfortable and ready for completion of the treatment. The reader is referred to Chapter 3 for a discussion of the radiographic progression of periapical pathosis.
Differential Tentative Diagnosis
A differential diagnosis is an intermediate step in the diag-nostic process. Diagnostic possibilities are narrowed to two or three plausible choices, and other possibilities are elimi-nated. This concept can apply to etiologic entities such as periodontal abscesses or vertical root fractures. Identification of the final diagnosis from the narrowed list will require a further but more focused examination. For endodontic cases, a frequent problem is identifying the correct tooth. After evaluating radiographs and doing the clinical examination, further testing is often required, but the area of interest will be more limited.
Sensibility (Vitality) TestingTheoryFortunately for dentistry, pulpal diagnosis has the benefit of some reasonably reliable tests. However, the value of these tests has been questioned to some extent as to their direct correlation with the disease process at hand.16 Tests for the measurement or assessment of the depth of cracks in teeth do not exist. Hot, cold, and electrical stimulation have existed in dentistry for a very long time.10,16 Histori-cally, the last test to arrive was the electric pulp tester, invented in 1867.20 Curiously, with all the developments in modern technology, no new testing methods have been refined for clinical application, and a problem or disconnect actually exists with all presently used tests. Whereas the

12 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
An equally viable option for the cold test is ethyl chloride (Fig. 1-20) or carbon dioxide sprayed onto a cotton-tipped applicator (Fig. 1-21) or a cotton pellet and then applied to the tooth. An advantage of this choice is convenience and consistency in temperature without affecting the soft tissues.19,21 It is always ready to use, and no special prepa-ration is needed to maintain a supply in the office (other than to reorder spray cans).
Again, testing with any of these materials should begin on a contralateral tooth when possible to establish in the mind of the practitioner what would be considered normal for that patient. Presumably, normal teeth within the quadrant of the suspected tooth should also be used (Fig. 1-22).
on a particular tooth are significant, even if they do not resemble the symptoms reported by the patient.
Applicable and Pertinent Testing Techniques
Cold TestCold testing is a more reliable test than heat.23 The test may be conducted with ice, crystals of ethyl chloride, carbon dioxide spray, or cold water. Ice sticks or ice pencils can conveniently be made by filling and freezing the discarded plastic sheaths from disposable anesthetic needles (Fig. 1-17). The advantage of ice is that it is readily available and easy to use (Fig. 1-18). The chief disadvantage to ice is the possible effect of the melting cold water on adjacent teeth or the gingival tissues. To counter this, the adjacent teeth and gingiva can be protected by cotton rolls or gauze (Fig. 1-19). The ice stick should be blotted to remove any melted water immediately prior to the test. Another minor disadvantage is the need for someone in the office to maintain the supply of ice sticks in the freezer.
FIGuRE 1-17 Anesthetic carpules used to make ice sticks for testing.
FIGuRE 1-18 Testing with an ice stick.
FIGuRE 1-19 Protecting adjacent teeth with gauze while ice testing.
FIGuRE 1-20 Endo Ice.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 13
Again, all exposed surfaces may be tested in this way. If no response is obtained on any surface while other com-parative teeth respond readily, the pulp may be presumed to be necrotic.
Heat TestUnlike cold testing, historically there was no heat test that applied a stimulation at a known temperature or maintained the stimulation at any constant temperature. Contemporar-ily, there are instruments that can be used to apply heat to the tooth at specific temperatures (BeeFill 2in1, VDW, Munich, Germany; Calamus Dual, Dentsply Tulsa Dental Specialties, Tulsa, OK, USA; Elements System, Sybron Dental, Orange, CA, USA). These are actually root canal obturation devices that use heat applied with a specific tip for contacting tooth structure. If not available, a commonly used applicator for heat is temporary gutta-percha-type stopping material warmed in a flame (Fig. 1-25). Other options for applying heat are the rubber polishing wheel
Furthermore, a previously root-treated tooth will serve as an excellent negative control. A normal response to these other teeth will educate the patient as to what to expect or antici-pate when testing the tooth or teeth in question. Testing is limited to one location on one tooth at a time. It is wise to develop a habit of placing the stimulus on the same position on each tooth—for example, along the gingival margin on the buccal or the midbuccal surface.
In cases where responses seem uncertain or vague, con-sider testing all exposed surfaces of each tooth, because it will be seen with experience that responses will often vary on the same tooth (Fig. 1-23). Some teeth may react more strongly to the same test on the lingual, on a metal restoration, or on the lingual metal band of porcelain fused to metal crowns (Fig. 1-24). In some patients, responses to cold may be minimal or delayed initially on every tooth tested. This must be considered when testing teeth in the symptomatic area. If the suspected tooth does not respond to testing, the cold should be reapplied and left in place longer, since some responses may be delayed.
BA
FIGuRE 1-21 A, Ice crystals formed on cotton applicator. B, Testing with Endo Ice.
FIGuRE 1-22 Testing presumably normal teeth first.FIGuRE 1-23 Testing on the lingual surface. All exposed surfaces should be tested.

14 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
cervical margins, the dental dam may actually prevent an accurate response to the testing.
Electric Pulp TestThe electric pulp tester, as indicated before, has no qualitative aspect to the response (Fig. 1-28). In cases where there is no reaction to hot or cold, the reasonable presumption might be that the pulp is necrotic. This would be a valid conclusion if all the teeth tested provided comparable responses. Occasion-ally in a given dentition, heat and cold tests elicit little response on any of the teeth. The electric pulp test (EPT) can at least provide the information of response or no response that may help differentiate normal from necrotic pulps. During usage, a medium such as tooth paste or gel is used to ensure the electrical contact between the tooth and the tip of the tester. Ideally the tip of the tester is placed at the incisal edge for the anterior teeth (Fig. 1-29).4 On posterior teeth, the favored location for placement of the tester is on the buccal cusp tip (Fig. 1-30).18 Many clinicians tend to favor the midfacial or buccal surfaces, but false readings may occur.15
The relative number or reading on the tester is not an indication of the relative health or pathosis of the pulp. Because EPTs apply an increasing power on a logarithmic (not linear) scale, responses at the very highest power levels cannot be reasonably accepted as normal. EPTs can provide false positives and false negatives up to 20% of the time.17
A further limitation of the EPT is lack of response on teeth with immature root development; this can be particularly confusing.17 Such teeth commonly have open apices and periapical-type radiolucencies associated with the develop-ment of the dental papilla. In these cases, a widened apical periodontal ligament space is also typical and completely normal (Fig. 1-31). If any diagnostic questions arise regard-ing pulpal pathosis in teeth with immature apical develop-ment, pulp testing will be unhelpful. It is appropriate to monitor such teeth over time for the emergence of periapical symptoms or lack of continued root development before making the diagnosis of pulpal pathosis.
Traumatically injured teeth may also fail to respond reli-ably and predictably immediately following the traumatic event,17 but many teeth will regain sensibility within 3 to 6 months. Once again, long-term monitoring is in order. Development of periapical pathosis either clinically or radiographically would support endodontic intervention. The same is true for sensibility testing of teeth during orth-odontic tooth movement, where responses may be highly unreliable6,13 (see Chapter 20).
Anesthetic TestWhen patients are experiencing pain at the time of exami-nation, or pain is elicited by thermal testing, the use of an anesthetic test may sometimes be valuable to confirm the diagnosis. In the maxilla, teeth can often be anesthetized selectively by infiltration. A small amount of anesthetic is
FIGuRE 1-24 Testing on the metal portion of a metalloceramic crown.
or the rubber prophylactic cup (Fig. 1-26). It may be necessary to test multiple surfaces with more than one method. Delayed responses to heat are more frequent than to cold on both normal and pathologic teeth.23 For this reason, it is wise to proceed slowly from one tooth to the next. If tests are performed too rapidly on multiple teeth, a delayed reaction may occur for which it is not possible to identify the source. On occasion, more than one stick of warmed stopping may be applied simultaneously to dif-ferent surfaces to increase the temperature and duration of the heat stimulus. The most useful application of the heat test is the case where the chief symptom is heat sensitivity or actual pain to heat that must be relieved with cold water or ice.
Dental (Rubber) Dam Application for Thermal Pulp TestingThe application of a dental dam is sometimes advantageous for routine pulp testing to allow more complete isolation. All pulp tests can be performed more conveniently because it can serve to retract the cheek and tongue. The retraction effect is especially useful during heat testing to avoid accidental burning of the cheek or tongue (Fig. 1-27). With this method, the dam is placed on each tooth separately with the rubber dam clamp. There is no need to establish a complete seal by working the dam interproximally, so the dam can be quickly moved from tooth to tooth.
The dental dam also can be applied for the use of cold or warm water as a test. The advantage of this test could be the bathing of the tooth in liquid, similar to what occurs in reality. Theoretically, the thermal stimulus would most likely reproduce the symptoms experienced by the patient. The disadvantage is that the dam must be applied separately to each tooth to ensure a complete seal. If sensitivity is due to loss of enamel or cementum covering the dentin at the

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 15
B
C
A
FIGuRE 1-25 A, Hygienic Temporary Stopping®. B, Heating the stopping with a butane torch. C, Application of heated stopping.
A B
FIGuRE 1-26 A, Rubber wheel used to generate heat by friction. B, Alternative use of dry prophylaxis cup.
deposited in the periapical region of the suspect tooth (Fig. 1-32). After a minute or two, the pain should resolve if the diagnosis is correct. This test should only be done after all other examination techniques have been used, and the diagnosis is reasonably firm. It is also possible to achieve this effect by using periodontal ligament injection on some mandibular molars, but since the method is not effective for all, the lack of pain resolution could be due to anesthetic failure.
A second circumstance in which the anesthetic test can be useful is a case where the patient is in pain, and the clinician
is unable to elicit responses from one or more teeth. The usual diagnostic procedures have been done, and most of the teeth have been ruled out. It is still unclear that the pain is of tooth origin. Of the teeth remaining after testing, the most likely candidate that may be etiologic for the pain is selected. If the pain resolves after the deposition of a small amount of anesthetic solution over the apex, that tooth is likely to be the problem. The anesthetic can be placed via infiltration or periodontal ligament injection. If the pain does not resolve after administering the solution, it is possible that the pain is not of pulpal or periapical origin.

16 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
BA
FIGuRE 1-27 Rubber dam retraction allows multiple heat applications without burning soft tissues.
FIGuRE 1-28 The Sybron Endo Vitality Scanner.
FIGuRE 1-29 Electric pulp test on the incisal edge.
FIGuRE 1-30 Electric pulp test on cusp of molar.
FIGuRE 1-31 Immature teeth with radiographically and histologically normal periapical tissues with various shapes resembling periapical pathosis. A, Maxillary incisors. B, Mandibular second molar.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 17
areas. If there is gingival recession, the exposed gingival areas of the crown are somewhat hypersensitive, as are large metal-lic restorations. Often these areas will be found around gin-givally placed metallic restorations, in which case any thermal testing that touches the metallic restoration may cause an accentuated response.
If the electric pulp tester has been used, data support testing on incisal edges of anterior teeth and buccal cusps of posterior teeth.
Reversible PulpitisThis clinical diagnosis is characterized by accentuated response to cold and/or hot, compared to neighboring and contralateral teeth. Once again, the response will cease imme-diately or very soon upon withdrawal of the stimulus. There is no spontaneous pain. The patient reports an undesirable need to avoid foods or beverages of either temperature extreme.
This type of pulpal sensitivity is best exemplified by a tooth with a new restoration. Other common causes are root exposure from periodontal inflammation, periodontal treat-ment, or recent extraction of an adjacent tooth. There is an occasional onset after minor trauma. Some teeth will develop symptoms without an apparent cause. If an etiology such as caries, exposed cervical margins of dentin, or fractured cusp is discovered, the majority of cases will resolve after appropri-ate restorative treatment (see Chapter 7).
Test CavityAnother sensibility test that has limited application is the test cavity. If all other methods of testing are ineffective or inap-propriate, as in the case of the electric test on a full crown, a test cavity may reveal dentinal sensitivity as an indication of vitality. The test cavity is generally made in the same position as an endodontic access cavity. The value of this test would be similar to the result of an EPT. The test consists of making a small access cavity without the use of anesthetic. Clearly this is an invasive and irreversible procedure from a restorative standpoint, so it should only be used when it is essential to the diagnosis, all other methods of testing have proven unsuccessful, and the patient is well informed. As soon as the patient feels sensation from penetration into the dentin, the cavity is closed with a bonded restoration. In teeth with calcified pulpal spaces, the patient may not feel any sensation until the pulp has been exposed, which would commit the tooth to completion of root canal treatment, regardless of diagnosis.
Clinical Diagnostic Scheme Based on Test Responses
Normal
The clinical definition of normal is a response to cold at a low level of magnitude and immediate cessation of the response on withdrawal of the stimulus. A normal tooth will respond the same way to heat, though in practice somewhat fewer normal teeth seem to react to heat at all. There is no injury imparted to the tooth by this testing. The same tooth may be confidently retested any number of times. Generally, thermal testing that is done using the gingival areas will respond more consistently than the midbuccal or cusp-tip
FIGuRE 1-32 Anesthetic test. A small amount of anesthetic solution is deposited adjacent to the apex of the suspect tooth.
CLINICAL PROBLEMProblem: A 23-year-old female complained of increasing thermal sensitivity in the maxillary left second molar. Clinical examination revealed a fractured and leaking restoration (Fig. 1-33, A). Pulp tests indicated a pulpal state of reversible pulpitis.
Solution: In the absence of evidence of irreversible pulpal pathosis, the decision was made to replace the restoration. The existing restoration was removed. Only slight incipient caries was observed below fracture lines in the previous res-toration. There was no evidence of a coronal fracture in tooth structure. The restoration was replaced using cavity varnish (see Fig. 1-33, B). The symptoms resolved completely within 72 hours.
In no case does the inflammation spread into the perira-dicular tissues, so no periapical changes are seen in these types of cases (Fig. 1-34). On occasion, the patient might experi-ence continued mild pulpal pain from a minimal restorative procedure (class I amalgam or class III composite restora-tion). Remember that restorative procedures will have an inflammatory effect on the pulp in addition to any preexist-ing inflammation caused by other etiologies.

18 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
In these situations, if the sensitivity is not improving after 2 weeks or so, removal of the new restoration and placement of the base or sedative dressing may alleviate the symptoms. The problem with this approach, however, is that any addi-tional restorative procedure has the potential to cause addi-tional pulpal inflammation. Consequently, replacement of a new restoration with a sedative temporary restoration may have the opposite effect.
Reversible pulpitis generally will resolve spontaneously and gradually in 4 to 6 weeks upon removal of the etiologic factors. Root canal procedures are generally not indicated for reversible pulpitis; monitoring the patient is indicated. Occasionally when pulp testing reveals that symptoms are due to root exposure, desensitizing solutions or toothpastes may be recommended to decrease sensitivity. In some cases, this type of hypersensitivity may not resolve after many months of monitoring, which may indicate that the pulp is inflamed beyond its ability to heal (irreversible pulpitis; see later). Chapter 7 discusses identification and management of a hypersensitive tooth in greater detail.
BA
FIGuRE 1-33 A, Multiple fractures in the amalgam. B, Completed restoration.
BA
FIGuRE 1-34 A, Preoperative radiograph of carious tooth with reversible pulpitis symptoms. B, Postoperative radiograph of completed restoration. Symptoms resolved. There is no radiographic sign of periapical pathosis.
Irreversible PulpitisIrreversible pulpitis is defined by the symptom of prolonged, painful responses to thermal stimulation or the presence of spontaneous tooth pain with no obvious stimulus. Unlike reversible pulpitis, painful reactions to temperature may last from minutes to hours. This symptom is the typical reason patients seek dental treatment. If present, the spontaneous pain can also last for hours and awaken patients from sound sleep. Often teeth with irreversible pulpitis become painful to biting pressure as well. The diagnosis of irreversible pul-pitis with localized pain can usually be made within a few minutes of taking the patient history and performing sensibil-ity tests.
During clinical testing, any tooth that exhibits a reaction longer than about 10 seconds is considered to have irrevers-ible pulpitis and is indicated for root canal treatment. This response occurs with either temperature extreme and occa-sionally both extremes simultaneously. It is not unusual to observe dramatic painful responses from relatively mild

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 19
communications. The location of this pathologic process makes possible the clinical signs of percussion sensitivity or pain, palpation sensitivity, swelling, and draining sinus tract. Gradually the apical bone resorbs, and as a result, apical and sometimes lateral rarefaction (loss of bony integrity) appears on the radiograph (Fig. 1-35). Radiographic inter-pretation of these findings is discussed in great detail in Chapter 3.
Aerodontalgia/BarodontalgiaA small subset of cases with significant pulpal degeneration or pulpal necrosis exhibit the unusual symptom of spontane-ous pain that occurs when there is a significant change in atmospheric pressure.24 Patients most often experience this during commercial aviation flights in which the cabin is pressurized (aerodontalgia). The pain may subside or be eliminated by reducing altitude or on landing; however, in some cases the pain may continue for several hours. This phenomenon has also occurred from changes as slight as driving over mountain passes where the altitude change may only be on the magnitude of 5000 to 7000 feet. People in deep underwater diving conditions have also experienced these symptoms (barodontalgia).
When patients present for dental treatment, they are often symptom free. It is clinically impossible to reproduce changes in atmospheric pressure, so it may be impossible to reproduce the symptoms by means of routine thermal tests. Nevertheless, thermal testing is usually the most effec-tive means to localize the offending tooth. Testing will at least rule out the normal teeth that could not be the problem. Once the number of possible etiologic teeth has been reduced, continued testing, often with heat, will help confirm a diagnosis.
temperature stimulation, and the resultant pain can last until anesthesia is obtained. Teeth that react with pain to cold can either be unaffected by heat, or pain is intensified by the application of heat. Cold, on the other hand, will frequently temper or completely relieve pain in teeth due to heat stimu-lation. Patients with acute heat sensitivity and experiencing prolonged or spontaneous pain will sometimes arrive for examination sipping ice water to control the pain. Upon access opening in these teeth, a small amount of purulence is often seen, followed by excessive hemorrhage due to the presence of an intrapulpal abscess.
Irreversible Pulpitis Not LocalizedPatients with irreversible pulpitis often present with a history of severe pain, either spontaneous in nature or stimulated by cold foods or liquids. Although the patient identifies a particular tooth or area in which the pain is felt, the clini-cian is unable to reproduce the symptoms. Likewise, the radiographic presentation is completely normal. Typically several teeth may have large restorations or crowns. The patient may be convinced that a particular tooth is causing their discomfort, but the clinician cannot elicit any thermal or percussion sensitivity from the indicated tooth or any other. In these not-so-rare instances, the clinician should resist the inclination to begin treatment based upon the patient’s diagnosis or insistence. Clinical data and diagnostic findings are often confusing and do not lend themselves to a rapid or logical diagnosis. It is best to wait until valid, integrated data can be obtained that will facilitate an accurate diagnosis.
Initially, it is common for the radiographic presentation to be normal or show subtle or suggestive but not definitive changes. This is especially true of mandibular posterior teeth in which the cortical plate is extremely dense. Changes in the periapical bone will not become obvious until significant destruction has taken place.
Necrotic PulpThe physiologic health or pathosis of the dental pulp might be thought of as a continuum that begins on one end with the normal pulp and progresses through stages of increasing pulpal inflammation and degeneration. Ultimately, the pulp becomes necrotic. Though pulpal necrosis is the endpoint of a pulp with irreversible pulpitis, symptoms for the two diagnostic states have a completely different manifestation. Whereas thermal sensitivity is the hallmark of inflammatory conditions, there is no thermal sensitivity with a necrotic pulp. The patient experiences no symptoms of pain from thermal stimulation, and the clinician elicits no responses on testing.
Patient symptoms in the presence of pulpal necrosis arise in the periapical tissues as an inflammatory or infectious reaction to necrotic materials and to bacteria that diffuse out of the apical foramen and associated accessory
FIGuRE 1-35 Typical periapical lesion of pulpal etiology.

20 chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain
5. Cameron CE: Cracked-tooth syndrome, J Am Dent Assoc 68:405-411, 1964.
6. Cave DG, Freer TJ, Podlich HM: Pulp-test responses in orthodon-tic patients, Aust Orthod J 18:27-34, 2002.
7. Chilton NW, Fertig FW: Pulpal responses of bilateral intact teeth,Oral Surg Oral Med Oral Pathol 33:797-800, 1972.
8. Cohen S, Blanco L, Berman L: Vertical root fractures: clinical andradiographic diagnosis, J Am Dent Assoc 134:434-441, 2003.
9. Creech JL, III, Walton RE, Kaltenbach RJ: Effect of occlusal reliefon endodontic pain, J Am Dent Assoc 109:64-67, 1984.
10. Gutmann JL, Baumgartner JC, Gluskin AH, et al: Identify anddefine all diagnostic terms for periapical/periradicular health anddisease states, J Endod 35:1658-1674, 2009.
11. Gutmann JL, Dumsha TC, Lovdahl PE: Problem solving in end-odontics, ed 4, St. Louis, 2006, Mosby-Elsevier.
12. Gutmann JL, Harrison JW: Surgical endodontics. Boston, 1991,Blackwell Scientific Publications.
13. Hall CJ, Freer TJ: The effects of early orthodontic force applicationon pulp test responses, Aust Dent J 43:359-361, 1998.
14. Harrington GW: The perio-endo question: differential diagnosis,Dent Clin North Am 23:673-690, 1979.
15. Jacobson JJ: Probe placement during electric pulp-testing proce-dures, Oral Surg Oral Med Oral Pathol 58:242-247, 1984.
16. Levin LG, Abbott P, Holland R, et al: Identify and define all diag-nostic terms for pulpal health and disease states, J Endod 35:1645-1657, 2009.
17. Lin J, Chandler NP: Electric pulp testing: a review, Int Endod J41:375-388, 2008.
18. Lin J, Chandler N, Purton D, et al: Appropriate electrode place-ment site for electric pulp testing first molar teeth, J Endod33:1296-1298, 2007.
19. Linsuwanont P, Palamara JE, Messer HH: Thermal transfer inextracted incisors during thermal pulp sensitivity testing, IntEndod J 41:204-210, 2008.
20. Magitot E: Ètudes sur les alterations de tissus dans la carie dentaire.Paris, 1867, Bailliere & fils.
21. Miller SO, Johnson JD, Allemang JD, et al: Cold testing throughfull-coverage restorations, J Endod. 30:695-700, 2004.
22. Morse DR, Seltzer S, Sanai I, et al: Endodontic classification, J AmDent Assoc 94:685-689, 1977.
23. Petersson K, Söderström C, Kiani-Anaraki M, et al: Evaluation ofthe ability of thermal and electrical tests to register pulp vitality,Endod Dent Traumatol 15:127-131, 1999.
24. Robichaud R, McNally ME: Barodontalgia as a differentialdiagnosis: symptoms and findings, J Can Dent Assoc 71:39-42,2005.
25. Rosenberg PA: Clinical strategies for managing endodontic pain,Endod Topics 3:78-92, 2002.
26. Schweitzer JL, Gutmann JL, Bliss RQ: Odontiatrogenic toothfracture, Int Endod J 22:64-74, 1989.
27. Whitehouse W: New mode of treating dead teeth and alveolarabscess, Br J Dent Sci 27:238-240, 1884.
RECoMMENDED ADDITIoNAL READINgAbd-Elmequid A, Yu DC: Dental pulp neurophysiology: part 1.
Clinical and diagnostic implications, J Can Dent Assoc 75:55-59, 2009.
Bender IB: Pulpal pain diagnosis—a review, J Endod 26:175-179, 2000.
Figdor D: Aspects of dentinal and pulpal pain. Pain of dentinal and pulpal origin—a review for the clinician, Ann R Australas Coll Dent Surg 12(4):131-142, 1994.
Putting It All Together: The Final Pulpal Diagnosis
The final pulpal diagnosis is derived from a synthesis and analysis of data obtained relative to the patient’s complaint, the clinical examination, evaluation of radiographs, and the objective signs elicited from various tests. As a rule of good clinical judgment, no tooth should ever be relegated to root canal treatment unless the clinician is 90% or better assured that the correct diagnosis has been made and the correct tooth identified. From the history and description of symp-toms, the clinician will sometimes know that a root canal procedure is indicated but be unable to identify the specific tooth upon clinical examination. Although contrary to the desire to provide pain relief for the patient, it may often be better to send the patient home with palliative support rather than risk treatment of the wrong tooth. It is especially dif-ficult to send the patient away without treatment when the diagnosis cannot be made in the case of moderate to severe pain. The clinician fears that the patient will lose confidence in his or her diagnostic ability. In reality, however, if the clinician has conducted a thorough examination and has presented the diagnostic dilemma in a compassionate manner, the patient will understand that the symptoms will localize in time to a specific tooth. It will then be possible to diagnose the problem accurately and provide definitive treatment. The best solution to difficult diagnostic problems in endodontics is: Don’t initiate a root canal procedure with the attitude of “let’s try this and see if it works.”
This chapter focused primarily on problem-solving con-cepts in the diagnosis of odontogenic pain, but the authors fully realize that accurate radiographs are essential in the overall diagnosis of the patient’s problem. Many problems with achieving an accurate or most probable diagnosis stem from not having quality radiographs and interpretation of the data they contain. Chapter 2 will address proper radiographic techniques necessary in the endodontic diagnostic scheme, and Chapter 3 will address interpretation of (1) radiographic findings relative to information that may or may not assist tracking pulpal pathosis etiology and (2) findings that will enable a more focused periapical diagnosis. Information gleaned from Chapter 3 will enable the clinician, through problem solving, to create a more accurate patient diagnosis for both pulpal and periapical pathoses.
REfERENCES1. Abbott PV: Classification, diagnosis and clinical manifestations of
apical periodontitis, Endod Topics 8:36-54, 2004.2. Baumgartner JC: Pulpal infections including caries. In Hargreaves
KM, Goodis HE, editors: Seltzer and bender’s dental pulp, CarolStream Il, 2002, Quintessence Publishing Co.
3. Belk CE, Gutmann JL: Perspectives, controversies and directiveson pulpal-periodontal relationships, Can Dent J Assoc 56:1013-1017, 1990.
4. Bender IB, Landau MA, Fonsecca S, et al: The optimum place-ment-site of the electrode in electric pulp testing of the 12 anteriorteeth, J Am Dent Assoc 118:305-310, 1989.

chapter 1 | Problem Solving in the Diagnosis of Odontogenic Pain 21
in the pulp, Oral Surg Oral Med Oral Pathol 16:846-871; 969-977, 1963.
Sigurdsson A: Pulpal diagnosis, Endod Topics 5:12-25, 2003.Weisleder R, Yamauchi S, Caplan DJ, et al: The validity of pulp testing.
A clinical study, J Am Dent Assoc 140:1013-1017, 2009.
Jararzadeh H: Laser Doppler flowmetry in endodontics: a review, Int Endod J 42:476-490, 2009.
Keiser K, Hargreaves KM: Building effective strategies for the manage-ment of endodontic pain, Endod Topics 3:93-105, 2002.
Seltzer S, Bender IB, Ziontz M: The dynamics of pulp inflammation: correlation between diagnostic data and actual histologic findings

22
Chapter 2
Problem-Solving Techniques in Making Radiographic Images
Problem-Solving ListProblem-solving challenges and dilemmas relative to making diagnostic radiographic images addressed in this chapter are:
The Ideal Dental Radiographic Image
Handling of Film and Digital Sensors
Controlling Variables
Exposure
Film/sensor position
Radiation beam angulation
Problem Solving in Evaluation of Image Quality
Correct and accurate images
Effects of Incorrect Angulation on Images of the Teeth
Foreshortening
Elongation
Anterior-posterior angulation
A Quality Dental Image Revealing Normal Structures
Advances in Radiology: Digital and Cone-Beam Computed Tomography
Clinical Directives
The most commonly used clinical tool to assist in making a diagnosis is without doubt the x-ray. It has been an invaluable boon to mankind, giving him a sixth sense to penetrate into the otherwise unknown. It leads us out of the dark as no other diagnostic can. Without x-rays one can hardly practice dentistry in an adequate manner or render the patient a satisfactory oral health service.7
L.I. GRoSSmAN, 1946
Before a meaningful discussion of the diagnostic interpreta-tion of radiographs can begin, the technical quality of the image must first be assessed. A poorly made radiographic image will not contribute as much to the process of diagnosis as a well made one, but this self-evident concept is missed by many clinicians. The process of diagnosis may be entirely subverted by erroneous conclusions drawn from inadequate radiographs and could lead to inappropriate treatment. Tension arises when the clinician has made an inadequate image and a decision must be made. Is the information to be gained by remaking the image worth the added exposure of the patient to radiation? This ethical dilemma is usually resolved by remaking the image if the first fails to provide necessary information. Fortunately, modern dentistry has
both low-exposure radiographic film and low-exposure digital radiography, so additional exposures have far less long-term risk than in the past. Nevertheless, it is incumbent on the clinician to review the cause of the radiographic error and correct it prior to additional exposures. It is the purpose of this chapter to review principles and practical techniques for obtaining diagnostically useful dental radiographic images, primarily for diagnosis in endodontics.
The Ideal Dental Radiographic Image
What is an ideal radiographic image? There are several aspects to be considered in answer to this question. First, the image should be neither too light nor so dark that it fails to show desired detail. It should have clarity of detail and be free of marks and blemishes. The image should represent the teeth without overlapping of proximal surfaces or roots. It should also represent the teeth as dimensionally accurate as possible, which occurs when the film is able to be placed in a position that is exactly parallel to the long axis of the tooth and the x-ray beam exposes the film at right angles. Clinically, this ideal is difficult to achieve in some areas because of the anatomy of the location into which the intraoral film or digital sensor is to be placed.

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 23
Handling of Film and Digital Sensors
Improper handling of film and poor darkroom technique can ruin otherwise excellent images. Dark spots, general foggy darkening, or a completely black film can indicate exposure to radiation or light, either by leaving unexposed film unpro-tected in the area where films are exposed or by natural light leaking into the darkroom during processing. It can also result from storage in areas where the temperature may exceed 80°F. Blemishes can be due to chemicals on the hands while handling undeveloped film and scratching of the emulsion before complete drying. Problems such as too much or too little contrast may indicate that the kVp is too high or too low. Discoloration such as brown staining of finished radio-graphs may indicate a problem with the fixer, either insuffi-cient time for fixing or an exhausted fixer solution. If any of these problems arise with persistence, it is wise to review the recommendations of the manufacturer for both the x-ray machine and film to be sure the exposures and film are well matched. Secondly, it is worthwhile to review film handling and darkroom technique with all auxiliary personnel.
Digital sensors are less affected than film by environmental factors. There are no problems with exposure to light or radiation of the sensors not in use. The most frequent prob-lems arise from infection control, frequent use and wear of connections, mechanical degradation, mishandling, the sensor itself wearing out, and patient concerns.5
Controlling VariablesGood image making with appropriate equipment consists in the control of three variables: exposure, film or digital sensor position, and beam angulation. A good radiographic image for endodontic diagnostic and treatment purposes is obtained when the center of the x-ray beam passes through the apex and projects the tooth on the receptor film or sensor at a right angle (Fig. 2-1).
ExposureAlways follow the recommended exposure settings provided by the manufacturer of the radiographic equipment. For
FIGURE 2-1 Art diagram.
B
A
FIGURE 2-2 A, Radiograph that is underexposed. B, An ideal, clinically useful exposure.
conventional film, the film type and speed must also be con-sidered. Underexposure results in the loss of details such as the periodontal ligament space and lamina dura around the apex (Fig. 2-2, A). There is also a loss of contrast which makes it difficult to detect pathosis that lacks clear borders, such as caries. Increasing the exposure to recommended guidelines will result in a clinically useful film (see Fig. 2-2, B).
Overexposure tends to make normal structures appear pathologic. Radiolucency is observed in areas such as the cervical regions of teeth just above crestal bone, often referred to as cervical burnout, which resembles caries. There can also be loss of detail owing to excessive contrast in the film (Fig. 2-3).
FIGURE 2-3 Radiograph that is overexposed.

24 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
FIGURE 2-4 Radiograph that fails to capture the root apices. Use on an increased angulation cannot compensate for this error.
FIGURE 2-5 The Rinn XCP film positioner.
FIGURE 2-6 The Rinn XCP in place for exposure of a mandibular molar. Note how the bite block device holds the film at full depth. The upper edge of the film is even with the occlusal plane.
CLINICAL PROBLEMProblem: Even with a hemostat/holder, the patient is unable to keep the film deep enough to capture the apices of a man-dibular molar on a preoperative image.
Solution: The film is placed in position with the hemostat/holder, and the patient is instructed to bite together. This will force the film/sensor downward to the proper depth, and at the same time the musculature of the floor of the mouth will relax (Fig. 2-8). There is also less of a tendency to lose this position if the patient should swallow before the film/sensor is exposed. This approach will be effective even with the rubber dam in place.
The hemostat can function similarly to the film positioner. The film packet is clamped along the edge and positioned in the mouth so that the instrument rests on the incisors or premolar. This positions the film to the maximum depth. The patient can maintain the film in position extraorally (Fig. 2-7). Digital sensors come with holders of similar design, and once the film/sensor is in place, the hemostat/holder also provides a measure of safety. A film packet or sensor held by a finger might easily become loose in the mouth.
Maxillary teeth are always a greater challenge in imaging because of the limited depth of the palatal vault and the anatomic lack of parallelism between the long axes of the teeth and the surface of the palate. To counter this, it is not necessary to have the film in contact with the tooth. For maxillary imaging, having the film or sensor in contact with
Film/Sensor PositionIf a film packet or digital sensor is not completely behind the tooth to be studied, the tooth or portion of interest will not be on the image. In endodontics, the area of interest is almost always the apex (Fig. 2-4). Commercially available intraoral film positioners such as the Rinn XCP (Dentsply Rinn, Elgin, IL, USA) are designed to place the film or sensor in the ideal position to capture the entire tooth (Fig. 2-5). When the patient bites on the film holder, the film is posi-tioned to the maximum depth, and the apices will inevitably be present on the image (Fig. 2-6). The use of positioners can eliminate many problems in preoperative and postopera-tive image making.
The major challenge during root canal treatment is to make accurate images while the dental dam is in place.6

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 25
CLINICAL PROBLEMProblem: The patient has a narrow mandibular arch which makes placement of the film packet/sensor difficult for imaging the anterior teeth.
Solution: A conventional film packet can be bent at the edges to allow placement in the narrow space (Fig. 2-9, A and B). Pediatric-sized radiographic films can also serve but are shorter in length and may not capture the apices. The only option with digital radiography is to obtain a sensor of narrow width, which is available with some systems. If the mandibular arch is very narrow, as is sometimes the case with mandibular exostoses (tori), the film packet can be bent in half and clamped in the hemostat. Using a sensor in the presence of an exostosis can be most challenging and requires careful placement of the sensor. It is equally important to position the film/sensor as parallel as possible to the long axis of the tooth. The mandibular molars are the easiest teeth to make images of, since placement of the film/sensor is almost always auto-matically parallel to the tooth (Fig. 2-10). In the mandibular anterior region, the floor of the mouth and the attachment of the tongue to the genial tubercles are impediments to place-ment of the film/sensor to the proper depth. Images of the anterior teeth often appear very short. So long as the film/sensor is parallel to the tooth, it can be placed farther back into the mouth to allow the base of the tongue to be depressed (Fig. 2-11). It is not necessary to have the film/sensor immedi-ately adjacent to or in contact with the tooth. By placing the film/sensor farther back into the mouth, the base of the tongue may be depressed. Placing a plastic cushion along the lower border of the film/sensor where it contacts the soft tissues is more comfortable for the patient (Fig. 2-12).
CLINICAL PROBLEMProblem: The patient has a muscular tongue and has a dif-ficult time maintaining the film in position behind the anterior teeth, even though the tongue can be depressed.
Solution: Position the film/sensor using the hemostat/holder. Instruct the patient to maintain the handle of the hemostat/holder in contact with an incisor to the side as the hemostat exits the mouth. This will usually work with or without the dental dam in place but may require anesthesia (Fig. 2-13).
the crowns (Fig. 2-14, A) is actually counterproductive. In this position, the film/sensor is never parallel to the long axis of the tooth and will lead to elongated teeth on the image. In ideal palatal placement, the apical edge of the film/sensor is usually in the midline of the vault, and the incisal edge is far from the crown of the tooth (see Fig. 2-14, B). This is the exact position obtained with a film positioner. When the dental dam is in place, the same positioning can be obtained using the hemostat/holder. The dental dam and clamp
actually help to keep the occlusal edge of the film/sensor away from the tooth.
The maxillary anterior teeth, especially the canines, present a challenge in film placement, since all sensors and film packets tend to be rectangular. The corners of these image receptors inhibit the most anterior placement, and parallel-ism is difficult to maintain. With conventional film, it is possible to bend a small portion of the corner to counter this limitation. No such option exists for rigid digital sensors (Fig. 2-15).
Radiation Beam AngulationThe third aspect of image making is simply to expose the film or sensor at a right angle to the beam of radiation. If the film is in the proper position, it would seem that this step would be the easiest, but orientation of the radiation beam is diffi-cult to master. Examination of the Rinn film holder demon-strates that if the cone is placed against the alignment ring, the radiation beam will be perpendicular to the film/sensor (Fig. 2-16). In addition, the center of the beam will focus on the center of the film/sensor. With these controls, the object tooth will always appear properly on the film.
When the dental dam is in place, it is difficult to use a film positioner. If the hemostat is used, it is useful to lift the
B
A
FIGURE 2-7 A, Hemostat holding the film or sensor. B, If the dental dam were in place, the hemostat could function like the film holder.

26 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
FIGURE 2-10 The anatomy of the lingual space is usually ideal for placement of the film or sensor parallel to the tooth.
FIGURE 2-11 For mandibular anterior teeth, film placement should be as parallel as possible. Contact or proximity to the teeth is not important.
BA
FIGURE 2-9 A, Standard sized film packet can be adapted to variable anatomic situations by bending the sides or corners. This will leave a line on the resultant image. Do not place the bend where it will interfere with the desired image of the tooth. B, A standard sized film adapted to a narrow arch.
A B
FIGURE 2-8 A, It is difficult for some patients to hold the film sufficiently deep in the floor of the mouth. B, The hemostat will aid in maintaining the proper position by resting on the incisors. It also helps to have the patient close the mouth.

FIGURE 2-12 Edge-Ease cushions make placement of films in the sublingual spaces more comfortable.
FIGURE 2-13 For muscular tongues, instruct the patient to force the hemostat down to rest on the incisor. Most patients can tolerate this without anesthesia. A film positioner functions in exactly the same way.
FIGURE 2-15 Digital sensors are rigid, which can impair placement.
B
A
FIGURE 2-14 A, If the film or sensor is in contact with the crown, the resultant image may be elongated. B, Ideal film placement should be as parallel as possible to the teeth. The superior edge of the film or sensor may be in the midline of the palate.
A B
FIGURE 2-16 A, The ring on the film positioner orients the x-ray beam perpendicular to the film. In addition, the center of the beam is oriented to the center of the film. B, The cone is oriented extraorally without requiring visualization of the film/sensor position.

28 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
FIGURE 2-17 When using the hemostat technique, the dental dam can be retracted to view the film position for orienting the x-ray cone.
FIGURE 2-18 Film with a cone cut. The x-ray beam was not centered on the receptor sensor or film.
A
B
C
dam or remove the dental dam frame to view the film/sensor while aligning the cone (Fig. 2-17). This also reduces the possibility of a “cone cut” that occurs when the collimated beam is not centered on the film/sensor, missing a portion and leaving a section of the image blank (Fig. 2-18).
Problem Solving in Evaluation of Image Quality
There are numerous issues to be considered in the interpreta-tion of pathosis on radiographic images.12 Before any diag-nostic problem can be considered, however, the quality of the radiograph itself must be assessed. Only limited informa-tion can be obtained from a poor-quality image.
The issues already discussed—namely underexposure, overexposure, and failure to have the target tooth on the image—can be corrected by film position and proper expo-sure. The problems associated with beam angulation are more pervasive and often so subtle as to escape detection until other images are made of the same area (Fig. 2-19). All three images in Fig. 2-19 appear familiar and acceptable clinically,
FIGURE 2-19 A, Clinically acceptable radiograph of mandibular incisors. A comparison with C indicates that in this image, the teeth are actually elongated. B, A foreshortened image of the same teeth. It is not unusual to see images like this used for clinical diagnosis. C, Mandibular incisors exposed with the film parallel to the long axes of the teeth. This is an ideal clinical radiograph.

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 29
A
B
CLINICAL PROBLEMProblem: A 48-year-old female presented to her dentist with the chief complaint of recurring episodes of severe spon-taneous pain in the mandibular right posterior area. A radio-graph was made of the mandibular left molars (Fig. 2-22, A). No radiographic abnormalities could be identified, and the patient was referred to the endodontist for evaluation.
Solution: A properly exposed radiograph demonstrated gross caries under the mesial margin, as documented in the postoperative radiograph (see Fig. 2-22, B). Another clue to excessive upward angulation in the posterior mandible is the appearance of the inferior border of the mandible on the image (Fig. 2-23).
FIGURE 2-21 Exaggerated superior angulation of the x-ray beam on a skull.
but only Fig. 2-19, C approximates the true dimensions of the teeth. This is of significant importance in endodontics if the image is to be used to estimate tooth length.
Images exhibiting obvious distortion due to errors in beam angulation also define the source of the error. The error can usually be remedied by returning to the principles of correct film placement and correct beam angulation.
Correct and Accurate ImagesWithin the realm of clinically acceptable radiographs, there are still variations the prudent clinician would be wise to minimize as much as possible. There are a few clues or signs that indicate the assurance of high-quality radiographs, assuming the exposure is correct. On the mandibular poste-rior teeth, as stated previously, placement of the film/sensor in the lingual space almost invariably results in a parallel relationship with the long axes of the teeth. If the teeth are parallel to the film, the occlusal surfaces are perpendicular to the film. A quality image should not have any aspect of the occlusal surfaces visible (Fig. 2-20). Despite the favor-able anatomic relationship between the lingual aspect of the mandible and the long axes of the posterior teeth, many clini-cians or other authorized personnel engaged in radiography have the tendency to angle the beam upward (Fig. 2-21). There is an apparent fear that the image will not capture the apices. Although the resultant image may appear clinically satisfactory, important diagnostic information may be missed, especially around large metallic restorations.
In the maxilla, it is seldom possible to make images of the posterior teeth without an indication of the occlusal surfaces. The molar teeth can still provide an important clue to film quality, however. Although the palatal root is usually the longest root, the buccal roots are generally within 2 to 6 mm of the length of the palatal root. A film indicating excessively short buccal roots would be questionable, and as often as possible, the buccal roots should appear to frame the palatal root (Fig. 2-24).
A third clue is the position of the zygomatic arch. The normal anatomy is widely variable, and many teeth are dif-ficult to radiograph without superimposition of this struc-ture. An image on which the arch obscures most of roots of the molar teeth would be suspect and of little diagnostic value (Fig. 2-25).
FIGURE 2-20 A, Occlusal surfaces of the mandibular posterior teeth will not be visible on an ideal exposure. B, Occlusal surfaces of the same mandibular posterior teeth are visible on a less-than-ideal exposure.

A B
FIGURE 2-22 A, Radiograph of the mandibular left posterior teeth provided by referring dentist. B, Posttreatment radiograph indicating gross caries under mesial margin not evident on referral film.
FIGURE 2-23 Visualization of the inferior border of the mandible is a clue to foreshortening of the mandibular teeth. Superimposition of the mylohyoid ridge over apices of the mandibular posterior teeth is seldom found when angulation is correct.
FIGURE 2-24 Acceptable radiograph of the maxillary posterior teeth made using a skull. The palatal root is depicted between the buccal roots.
A B
FIGURE 2-25 A, Exaggerated inferior angulation of the x-ray head for the exposure of maxillary posterior teeth. B, Diagnostic radiograph made with the same angulation. Note foreshortened roots. The zygomatic arch obscures much of the detail in the area of the apices.

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 31
A B C
FIGURE 2-26 A, Exaggerated inferior angulation in the anterior maxilla would capture a portion of the nasal cavity. B, Clinical radiograph made at an exaggerated inferior angulation. Note the nares at the top of the film. The teeth are excessively foreshortened. C, Correct angle for maxillary anterior exposures.
Unfortunately, images of the anterior teeth have few clues that reveal less-than-optimal angulations within the range of clinical acceptability, as seen in the examples in Fig. 2-19. Some possible clues in the maxillary anterior area might be superimposition of the nasal nares. The angulation of the x-ray cone in Fig. 2-26, A demonstrates how the nasal struc-tures can be captured (see Fig. 2-26, B). The correct angula-tion is depicted in Fig. 2-26, C. In the anterior mandible, excessive upward angulation (Fig. 2-27) might be indicated by the presence of the inferior border of the mandible (mental protuberance) or the genial tubercles, as depicted in Fig. 2-28, A.
FIGURE 2-27 Exaggerated superior angulation for exposure of mandibular anterior teeth. Note how the inferior border of the mandible would be captured on the radiograph.
C D
C, Correct inferior angulation. D, Radiograph of same teeth at correct inferior angle. Roots appear longer, and apical detail is now visible.FIGURE 2-25, cont’d

32 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
B
A
FIGURE 2-28 A, Foreshortening of the mandibular anterior teeth. Note the genial tubercles. B, Image of same teeth made at the correct angle.
Effects of Incorrect Angulation on Images of the Teeth
ForeshorteningTeeth can appear much shorter on a radiographic image than they are in reality (see Fig. 2-28; review Fig. 2-26, B). The image may be clear and possess fine detail, but such films are of poor diagnostic quality. The relationship of bone to tooth, such as assessment of crestal bone levels, is impossible. The appearance of pathosis may be hidden or completely dis-torted. In the mandible, foreshortening is usually another result of the attempt to capture the apices by angling the beam upward, but it can also occur with normal angulation
ElongationElongation is the opposite of foreshortening; in this case, the teeth appear much longer than they are in reality. Detail may be completely distorted in the elongated area. Elongation is most often a problem in making images of the maxillary posterior teeth. One aspect of the problem is the low angle of the x-ray beam, which approaches parallelism with the occlusal plane (Fig. 2-31, A). The resultant image does not appear abnormal until it is compared with an ideal image of the same teeth (see Fig. 2-31, B and C ). Maxillary exposures always require a distinctively downward angle relative to the occlusal plane (see Fig. 2-25, C ).
A second contributing factor is film or sensor placement. A film/sensor held against the crown of the tooth (see Fig. 2-14, B) and exposed will accentuate elongation (Fig. 2-32).
A third complication pertains to film only. Radiographic film packets are pliable. If the film is held firmly with finger pressure directly against the palate, the superior edge of the film may curve to conform to the shape of the palate (Fig. 2-33, A). The resultant image will generally have good detail in the coronal half and elongation in the apical half (see Fig. 2-33, B).
The maxillary canine is a particularly difficult tooth to capture without elongation. This problem is made more acute in view of the wide variation in the anatomic shape of the anterior palate and the variable length of canine teeth. As mentioned earlier, placement of the film/sensor is limited by the anterior palate. If film is used, it is possible to bend the corner slightly to improve adaptation, but every effort should
CLINICAL PROBLEMProblem: A 50-year-old female was referred for root canal treatment of a symptomatic mandibular left first molar. The patient had been advised that the tooth may require extrac-tion because of the apparent severe calcification observed on the image. The digital image was emailed to the endodontist (Fig. 2-29, A) prior to the arrival of the patient. The film was reviewed and found to be inadequate due to foreshortening and lack of diagnostic clarity.
Solution: At the examination appointment by the special-ist, a new image was made with the film positioner. In the laboratory, the change in angulation is exemplified by photos of the angulation of the x-ray cone on a skull (see Fig. 2-29, B). It is apparent that the tooth is not calcified (see Fig. 2-29, C). Root canal treatment was completed without difficulty. Fore-shortening can drastically affect root canal treatment when radiographic techniques are used to determine length or monitor quality during treatment1,6 (Fig. 2-30).
if the molar teeth have a lingual inclination of the long axis. For these teeth, proper exposure would actually require a slight downward angulation of the radiation beam.

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 33
B
C
A
FIGURE 2-29 A, Referral film showing foreshortened and possibly calcified mandibular left first molar. B, Laboratory view of x-ray cone placed at an exaggerated superior angulation. C, Radiograph made at optimal angle. There is no apparent calcification.
FIGURE 2-30 Mid-treatment film to assess quality of obturation. Exaggerated superior angulation resulted in extreme foreshortening. This image could not be used.
Anterior-Posterior AngulationAn analysis of the film positioner reveals that the ideal anterior-posterior angulation of the x-ray beam is exactly perpendicular to the segment of dental arch in which the target tooth is located. For posterior teeth, this equates to perpendicular to the posterior sextant (Fig. 2-34).
Often, multiple radiographically angled views must be taken to reveal anatomic features not evident on the optimal clinical view. Documentation for this approach has existed for almost 90 years, with recommendations for taking radio-graphs from three distinct angles.8 The technique is to bring the x-ray head anteriorly so the cone will be angled in a more posterior direction (mesial angulation) while maintaining the correct upward or downward cone angle (Fig. 2-35). If pos-sible, it is advisable to attempt to angle the film/sensor across the arch to approximate a perpendicular relationship with the beam (Fig. 2-36).20 Fig. 2-37 illustrates a clinical example of the view of the tooth and roots from this angulation. The same altered-angle view can be taken from the posterior but this configuration is difficult to use clinically, especially in the maxilla as the zygomatic arch is projected forward over the apices of the teeth. Secondly, the curve of the palate posi-tions the film unfavorably for a beam angle approaching from the posterior.
be made to avoid curvature of the entire film packet, which would result in elongation of the apical half of the root. The best way to compensate for these complications is to place the film as far back into the mouth as possible and maintain parallelism.

34 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
A
B C
FIGURE 2-31 A, Low beam angle. Angle of x-ray cone is approximately parallel to the occlusal plane. This is ideal for mandibular teeth, but the contour of the palate will cause elongation in exposures of maxillary teeth. B, Image of maxillary posterior teeth exhibiting elongation due to the beam angulation depicted in A. C, Ideal image for comparison made at the angle depicted in Fig. 2-25, C.
FIGURE 2-32 Excessive elongation results if film/sensor is held against the crown of the tooth, as in Fig. 2-14, A.

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 35
A B
FIGURE 2-33 A, Maintaining film in position with finger. Finger pressure causes deformation and undesired curvature of the film. B, Film exposed with the combination of low beam angulation and curvature of the film packet as it is formed to the palate with pressure.
FIGURE 2-34 Ideal anterior-posterior angulation provided by film positioner. Ideal anterior-posterior angulation is perpendicular to the dental arch, here depicted in the posterior sextant of either the mandibular or maxillary teeth.
FIGURE 2-35 Anterior angle variant position of the x-ray cone for additional views.
A B
FIGURE 2-36 Demonstration of variable angle techniques with a film packet in a skull. A, Normal position perpendicular to the segment. B, Beam position altered anteriorly. It is very difficult to obtain a film in which the angulation of the beam is altered posteriorly. Buccal roots of maxillary molars can be projected anteriorly if the tooth is in a rotated position.

36 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
FIGURE 2-38 Length determination film made with excessive anterior angulation. Distortion makes interpretation impossible.
A
B
FIGURE 2-37 A, Application of variation in angle technique. By shifting the beam anteriorly, buccal objects such as buccal roots or canals will “move” distally. B, Completed treatment. Distal buccal canal is on far left.
FIGURE 2-39 Normal periodontal ligament space is of uniform width around entire root. The lamina dura on this tooth is normal and continuous.
FIGURE 2-40 The normal lamina dura is routinely variable in visibility and width around many teeth.
Excessive angulations from the mesial will displace buccal roots of the molars severely to the distal, overlapping roots and proximal surfaces of the crowns (Fig. 2-38). An image made in this manner will be of little clinical use (see Fig. 2-38). The same is true with excessive angulations from the distal. Another sign of excessive anterior angulation is the appearance of the canine or even the lateral incisor on a molar image.
A Quality Dental Image Revealing Normal Structures
What is the definition of radiographic normality of the peri-apical tissues? The two anatomic features of normality with respect to endodontic diagnosis and root canal treatment are a periodontal ligament space of uniform width and an intact lamina dura around the entire root (Fig. 2-39).1,6 The lamina dura in general tends to vary in appearance even on the same root. The periodontal ligament is highly consistent and reli-able in almost all anatomic areas (Fig. 2-40).

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 37
Advances in Radiology: Digital and Cone-Beam Computed Tomography
Digital radiography has revolutionized and streamlined end-odontic diagnosis and treatment. There are several advan-tages of digital x-ray imaging over analog film imaging that can benefit the clinician5: reduced time, reduced radiation, ability to take multiple exposures without repositioning the sensor, storage and maintenance of the images, and elec-tronic transmission of images. Clinical challenges are inabil-ity to sterilize the sensors and the thickness of sensors, which can create discomfort for some patients and difficulty in the detection of small endodontic files when radiographi-cally determining working length (Fig. 2-41).3 When
BA
FIGURE 2-41 A, Digital radiograph of a mandibular first molar with somewhat indistinct root canals. B, When a digital clear view enhancement is used, even No. 10 K-files are easily distinguishable on the digital film.
A B
FIGURE 2-42 A, Radiograph of maxillary molars using a digital radiograph. Note superimpostion of zygomatic process that obscures root apices. B, Same film inverted using digital radiographic techniques. Details are somewhat enhanced over A.
appropriately sized working length files are used, digital radiology has superior accuracy to traditional radiographic exposures. Within this perspective, and when the various capabilities of digital radiology (clear views, inverted pictures, etc.) are used to view the films (Fig. 2-42), both normal and pathologic details can be seen more clearly than on standard radiographic film16 (Fig. 2-43). An exhaustive look at digital radiography is beyond the scope of this text, but its diagnostic and treatment advantages are worth noting (Fig. 2-44). Although there are some potential technical issues with these devices, they are irrelevant to the problem-solving focus of this chapter. Scientific validation of the best exposure strategies for optimizing specific diagnostic imaging tasks in endodontics is warranted.5
There has been a major movement of cone-beam com-puted tomography (CBCT) into endodontics.2,11,13 This technology can be quite accurate,9,15 and its impact on

38 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
A
CB
FIGURE 2-43 A-C, These three digital radiographs are the same, except that A is a normal view, B is the enhanced clear view, and C is the inverted view. Different details of the roots, lamina dura, periodontal ligament space, sinus outline, poorly filled root canal, and crown margins can be gleaned from each different view, demonstrating the value of digital radiography for anatomic assessments.
PS PS
C D
C, Digital radiograph of mandibular molars enhanced with a clear view option. D, Same film inverted in appearance. Both of these enhancing options assist in radiographic assessment. Note clarity of the pulp stone (PS) in the chamber in both pictures and the linear calcification positioned in both mesial and distal canals (arrows).
FIGURE 2-42, cont’d

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 39
A B
E F
C D
FIGURE 2-44 A, Normal digital exposure of maxillary premolars that exhibit decay and large pulpal spaces. B, Enhanced clear view of the same teeth. C, Maxillary molar with crown and small root canals as seen in a normal digital radiograph. D, Inverted view enhances view of root structures, especially the large periapical radiolucency on the palatal root (arrows) and the lamina dura and periodontal ligament space around the roots. E, Mandibular molar with large lesion on a normal digital radiograph. F, Same tooth as seen in an inverted format, showing extent of bone loss. Tooth had a large crack on the distal margin ridge and could be probed to the depth of the lesion on the distal.
diagnosis of periapical lesions and possibly their etiologies is significant4,10,14,17-19 (Fig. 2-45). Presently, cost factors for both the clinician and the patient may limit integration of this technology into private-practice settings; larger radiology centers can provide this expertise. Within 5 to 10 years,
however, owing to the potential of technology to vastly improve patient care,11 CBCT may very well be considered the standard of care in providing accurate endodontic diag-noses and treatment, in particular surgical intervention and case revision.19

40 chapter 2 | Problem-Solving Techniques in Making Radiographic Images
A
B
C D E
FIGURE 2-45 A, Cone-beam computed axial tomography (CBCT) of the entire mouth. The tooth in question is the maxillary right central incisor that exhibits invasive external resorption. B, Sections 95 to 98 (red outline) demonstrate the nature and location of the resorptive defect, enhancing both diagnosis and treatment planning. C, Pretreatment periapical digital film. D, Following root canal treatment and location of the defect. E, Defect filled with mineral trioxide aggregate. CBCT enabled identification of the defect and its management. (Courtesy Dr. Paul Buxt.)

chapter 2 | Problem-Solving Techniques in Making Radiographic Images 41
Clinical DirectivesRadiography is an essential and indispensable part of end-odontic diagnosis and root canal treatment. Excellence in diagnosis requires excellence in the quality of dental images. A poor-quality radiograph can only invite error in diagnosis and possibly result in harm to the patient. Concepts and techniques for producing good-quality images have been dis-cussed to aid in trouble-shooting current techniques and unsatisfying results. Good diagnosis also requires a grounding in the definition of radiographic normality so that changes that represent abnormal anatomic structures or pathosis can be easily recognized and considered in the overall treatment plan of the case.12
REFEREnCES1. Bridgman JB, Campbell DJ: Radiography in endodontics, N Z
Dent J 91:62-64, 1995.2. Cotton TP, Geisler TM, Holden DT, et al: Endodontic applica-
tions of cone-beam volumetric tomography, J Endod 33:1121-1133, 2007.
3. Eikenberg S, Vandre R: Comparison of digital dental x-ray systemswith self-developing film and manual processing for endodontic file length determination, J Endod 26:65-67, 2000.
4. Estrela C, Bueno MR, Leles CR, et al: Accuracy of cone beamcomputed tomography and panoramic and periapical radiology for detection of apical periodontitis, J Endod 34:273-279, 2008.
5. Farman AG, Ramamurthy R, Hollwnder LG: Diagnostic Imaging.B. Digital Imaging for Endodontics. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc, Chap 15, pp 573-589.
6. Fava LF, Dummer PM: Periapical radiographic techniques duringendodontic diagnosis and treatment, Int Endod J 30:250-261, 1997.
7. Grossman LI: Root canal therapy, ed 2, Philadelphia, 1946, Lea &Febiger.
8. Hinman TP: The interpretation of x-ray pictures of apical granula-tions, giving differential diagnosis of cases favorable and cases unfavorable for treatment root-canal filling, J Nat Dent Assoc 8:83-87, 1921.
9. Lascala CA, Panella J, Marques MM: Analysis of the accuracy oflinear measurements obtained by cone beam tomography (CBCT-New Tom), Dentomaxillofac Radiol 33:291-294, 2004.
10. Lofthag-Hansen S, Huumonen S, Gröndahl K, et al: Limitedcone-beam CT and intraoral radiolography for the diagnosis ofperiapical pathology, Oral Surg Oral Med Oral Pathol Oral RadiolEndod 103:114-119, 2007.
11. Nesari R, Rossman LE, Kratchman SI: Cone-beam computedtomography in endodontics: are we there yet? Compend ContinEduc Dent 30:312-314, 316, 318, 320, 322, 324, 2009.
12. Ørstavik D, Larheim TA: Radiographic interpretation. In Ingle JI,Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Ham-ilton, Ontario, 2008, BC Decker Inc, Chap 16, pp 600-625.
13. Patel S, Dawood A, Whaites E, et al: The potential applicationsof cone beam computed tomography in the management of end-odontic problems, Int Endod J 40:818-830, 2007.
14. Patel S, Dawood A, Mannocci F, et al: Detection of periapicalbone defects in human jaws using cone beam computed tomogra-phy and intraoral radiography, Int Endod J 42:507-515, 2009.
15. Pinsky HM, Dyda S, Pinsky RW, et al: Accuracy of three- dimensional measurements using cone-beam CT, DentomaxillofacRadiol 35:410-416, 2006.
16. Schmitd LB, Lima Tde C, Chinellato LE, et al: Comparison ofradiographic measurements obtained with conventional and indi-rect digital imaging during endodontic treatment, J Appl Oral Sci16:167-170, 2008.
17. Simon JHS, Enciso R, Malfaz JM, et al: Differential diagnosis oflarge periapical lesions using cone-beam computed tomographymeasures and biopsy, J Endod 33:291-294, 2006.
18. Tyndall DA, Rathore S: Cone-beam CT diagnostic applications:caries, periodontal bone loss assessment, and endodontic applica-tions, Dent Clin North Am 52:825-841, 2008.
19. Velvart P, Hecker H, Tillinger G: Detection of an apical lesion andthe mandibular canal in conventional radiography and computedtomography, Oral Surg Oral Med Oral Pathol Oral Radiol Endod92:682-688, 2001.
20. Walton RE: Diagnostic Imaging. A. Dental radiography. In IngleJI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6,Hamilton, Ontario, 2008, BC Decker Inc, Chap 15, pp 554-572.
RECommEndEd AddItIonAl REAdIngPatel S: New dimensions in endodontic imaging: Part 2. Cone beam
computed technology, Int Endod J 42:463-475, 2009.Patel S, Dawood A, Whaites E, et al: New dimensions in endodontic
imaging: Part 1. Conventional and alternative radiographic systems, Int Endod J 42:447-462, 2009.
Sewerin IP: Radiographic examination. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.

42
Chapter 3
Problem Solving in Interpretation of Dental Radiographic Images
Problem-Solving ListProblem-solving challenges and dilemmas relative to the interpretation of dental radiographic images addressed in this chapter are:
Evaluation of Tooth Anatomy: Problem Prevention
Radiographic Changes Associated With Dental Caries
Radiographic Changes Associated With Tooth Fractures
Coronal fractures
Midroot fractures
Vertical root fractures
Radiographic Tooth Changes Associated With Resorption
Influence of Radiolucent Anatomic Structures on Radiographic Interpretation
Influence of Radiopaque Structures on Radiographic Interpretation
Radiographic Changes Associated With Pulpal Necrosis in Periapical Tissues
Lateral Radiographic Changes Associated With Pulpal Necrosis
Radiographic Changes Associated With Cases of Endodontic Failure
Radiographic Changes Associated With Nonendodontic Pathoses Mimicking Potential Endodontic Problems
Cementoma
Developmental cysts
Healed endodontic lesions
Periodontal lesions
The radiographic picture is only one means of diagnosis. It seems absurd for a dentist to bring to a diagnostician a radiographic picture and ask his opinion . . . the picture may show a tremendous area of rarefaction, but to use it as the sole means of diagnosis is unwise.17
T.P. HINMAN, 1921
Within the scope of endodontics, radiographic images serve a double purpose: the confirmation of normality and the indication or details of pathosis. Radiographic images are produced by the differential absorption of radiation by mineralized tissues through which the x-ray beam passes before exposing the receptor film or digital sensor. There are only three types of tissues that can be identified rou-tinely on dental radiographs: bone, enamel, and dentin. Cementum or a cementum-type material can be identified when it is reparative or regenerative. Normal radiographic details and appearance are learned by correlating the knowledge of the physical anatomy of structures discussed in Chapter 1 with their radiographic representations. The model of normality includes a range of variations and implies concepts such as average, commonality, typicality, and rarity.
Deviations from normality include radiographic changes in the anatomy of the teeth and bony structures. Most often, changes are represented as radiolucency or loss of mineralized structure, as in the case of caries, resorption, or infrabony periodontal defects.30 Occasionally, change can also be rep-resented by radiopacities, as in the case of iatrogenically introduced materials or odontogenic tumors. In this chapter, the aspects of radiographic normality and abnormality rele-vant to endodontic diagnosis and case assessment will be discussed.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 43
Evaluation of Tooth Anatomy: Problem Prevention
The process of radiographic interpretation should begin with examination of the teeth. Assessment is limited in all areas of dentistry by the fact that the intraoral radiograph is a two-dimensional representation of three-dimensional objects. For example, even with well-made digital or film images, it is rarely possible to confirm or rule out the presence of a second canal in the mesial buccal root of a maxillary molar. Three-dimensional radiography is available in dentistry in the form of cone-beam computed tomography (CBCT),10,24,30 which is developing but not yet sufficiently refined to rou-tinely produce the detailed images required for endodontic diagnosis and treatment.6,10,24 When combined with digital radiography, however, CBCT can significantly enhance end-odontic care.
Once a quality radiographic film is obtained, knowledge of dental anatomy is crucial for extrapolating two- dimensional representations into three-dimensional mental images. For example, anatomic examination of mandibular molar roots teaches that these roots are narrow in the mesial-distal dimension and very wide in the buccal-lingual dimen-sion. A very wide root buccal-lingually will appear narrow on an optimal clinical radiograph. If the radiograph is made using variable angulations of the radiation beam (from the mesial or distal), the root will appear wider.31 More than one periodontal ligament space may be observed, and the image may be more difficult to interpret if roots of adjacent teeth are overlapped.
One objective of tooth evaluation will be to confirm ana-tomic form and any variations: it is sometimes possible to see two roots on a mandibular canine (Fig. 3-1, A), but it is equally important to know that a mandibular canine can have two roots, and many such cases will not be discoverable on radiographs.13 Additional roots and canals must be found by internal exploration during treatment, and CBCT images can assist in this anatomic assessment (see Fig. 3-1, B and C ).
Teeth that may be indicated for root canal treatment should be examined for relative length, the number of roots, calcification of canals, and general morphology. Once assessment has been completed, anatomy confirmed, and treatment initiated, canal morphology should be clearly visu-alized in the mind of the clinician and retained throughout treatment. Variations in the anatomy of posterior teeth such as the mandibular first molar are seen routinely (Fig. 3-2). Fig. 3-2, A shows a molar with two divergent mesial roots; Fig. 3-2, B shows a molar tooth with two divergent distal roots. Even more variations may exist in various ethnic populations.
CLINICAL PROBLEMProblem: A 53-year-old male with a current history of acute pain to heat stimulation in the maxillary right posterior area was evaluated for treatment. The periapical film indi-cated that the second molar had past root canal treatment, but no carious lesions were seen radiographically or upon clinical exam. There was no evidence of periapical pathosis (Fig. 3-3, A).
Solution: Routine sensibility tests were performed. The maxillary right first molar and two premolars responded nor-mally to cold but did not respond to heat. The second molar responded abnormally to heat, with lingering pain. The patient stated this was the pain he had been experiencing. Examina-tion of the radiograph revealed that the treated canals appeared asymmetrically located to the mesial of the root with respect to the overall morphology of the root anatomy. An untreated canal was suspected in the distal buccal root. Following access opening, the canal was identified, cleaned, shaped, disinfected, and obturated (see Fig. 3-3, B). The patient reported that once anesthesia was gone, the previous discom-fort to heat was absent.
A similar case is seen in Fig. 3-4, A to C. The patient was referred for root canal treatment on the maxillary left second molar. She had been experiencing intermittent episodes of a dull ache in the maxillary premolar area for 1 year. At examination, the patient pointed to the pontic area as the felt location of the pain. Root canal treatment had been completed on the left first premolar 8 years previously. Sen-sibility testing with heat clearly identified the premolar as the source of pain. Preoperative radiographs were made at different angles (see Fig. 3-4, A and B). Careful analysis of the radiograph (see Fig. 3-4, B) suggested that filling material might have been compacted into the orifice of an untreated canal. An occlusal access opening was made, but locating the orifice of the third canal was a challenge. Once the untreated canal was located, the pulp was found to be vital. Following successful treatment of this root canal, the symp-toms resolved (see Fig. 3-4, C).
The number of roots treated should be noted in each case of a previously treated tooth, as well as the quality of treat-ment (length of fill, density of fill, shape of canal, etc.). Although no abnormal changes may be found radiographi-cally, the tissue remaining in uncleaned canals can give rise to symptoms of thermal sensitivity, percussion sensitivity, and spontaneous pain. Any teeth found to have poor or questionable root canal treatment could be possible sources of symptoms and potential candidates for treatment revision. Further clinical examination of these teeth would be indicated.

44 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
A B
C
FIGURE 3-1 A, Mandibular canine with a bifurcated root. B, Another case of a mandibular canine investigated using cone-beam computed tomography (CBCT); occlusal view (arrow indicates tooth being evaluated). C, Proximal view of the two-rooted canine tooth using CBCT. Note sections 94 to 97; not only do they provide a good view of the two roots and two canals, but they also provide valuable information as to the location of the lingual canal and the challenges faced in access opening and orifice location.
A B
FIGURE 3-2 A, Mandibular molar with two mesial roots. B, Mandibular molar with two distal roots.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 45
A B
FIGURE 3-3 A, Maxillary second molar with confirmed heat sensitivity. B, Posttreatment image indicating previously untreated distal canal.
B
A
C
FIGURE 3-4 A, Initial radiograph of the maxillary left first premolar with heat sensitivity. B, Second view angulated slightly from the distal. Note the small bulge in the gutta percha extending mesially in the coronal third. C, Posttreatment image indicating a previously untreated canal. (Courtesy Dr. Ryan Wynne.)

46 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
A B
FIGURE 3-5 A, Carious exposure of mesiobuccal pulp horn in a maxillary second molar. B, Bitewing digital radiograph showing the location and extent of dental caries.
Radiographic Changes Associated With Dental Caries
The radiographic appearance of dental caries is basic to all dental education, and ample resources exist in the dental literature for further reading on detecting dental caries on routine radiographic surveys.23 For endodontic diagnostic purposes, the depth of caries past or present is an important radiographic indicator of teeth with pulpal pathosis. While carious exposures of the pulp cannot be seen radiographically, gross caries that approximates the radiographic outline of the pulp chamber is frequently evident even in the absence of symptoms (Fig. 3-5, A). Pulp exposure would be a logical
expectation following excavation of such lesions, and root canal treatment of this tooth would be a necessary part of the treatment plan. Bitewing radiographs greatly assist identification of caries and its proximity to the dental pulp; they can be taken with traditional film or as digital images (Fig. 3-5, B)
Carious lesions that appear near pulp horns also are likely to be carious exposures upon excavation. Demineralization of dentin that occurs in the process of caries is progressive and lacks a clear clinical or radiographic border. Most carious lesions extend deeper into the dentin than what can be ascer-tained radiographically. Fig. 3-6, A represents a symptomatic tooth with a carious lesion in close proximity to the mesial pulp horn. Excavation revealed a gross carious exposure and necrotic pulp. Root canal treatment was indicated (see Fig. 3-6, B).
A B
FIGURE 3-6 A, Caries near mesiobuccal pulp horn. B, Excavation revealed carious exposure and necrotic pulp. Root canal treatment was indicated.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 47
FIGURE 3-7 Large occlusal carious lesion. The tooth responds normally to sensibility tests.
A B
FIGURE 3-8 A, Large occlusal carious lesion in a 10-year-old patient. B, 12 month re-evaluation after vital pulp therapy using mineral trioxide aggregate (MTA) for a direct pulp cap. The patient was asymptomatic and the tooth responded normally to sensibility tests. (Courtesy Dra. Silvina Díaz.)
For many teeth with large carious lesions, there may be no history of symptoms, and sensibility tests may provide normal responses (Fig. 3-7). The most reasonable approach to treatment is to advise the patient that the caries should be excavated, and the decision to treat endodontically or with vital pulp therapy will depend on the remaining dentin thick-ness (RDT).5,21,22 Although dentistry has no instrument to measure this dimension, there is a good clinical indicator: if the RDT is 0.5 mm or less, the proximity of the pulp will make the dentinal wall appear pink. Studies show that with an RDT of less than 0.5 mm, the prognosis for pulp survival is doubtful.21,22 The majority of teeth in this situation will develop symptoms of acute irreversible pulpitis after restoration, and root canal treatment will be necessary. On the other hand, vital pulp therapy has a good chance of success regardless of dentinal thickness, if the patient is young (Fig. 3-8). (Chapter 7 will address vital pulp therapy in detail.)
The decision to treat a tooth endodontically can some-times be influenced by the economic situation of the patient; successful vital pulp therapy could avoid additional expense.
CLINICAL PROBLEMProblem: A 57-year-old male patient was examined for the chief complaint of recurrent spontaneous pain in the man-dibular right teeth (Fig. 3-12, A). Sensibility tests indicated normal responses from the central incisors through the second premolar, but there was no response to testing on the second molar. Radiographs showed no periapical pathosis, but recur-rent caries was noted around the margins of the second molar bridge abutment. No other signs of pathosis or abnormalities were noted. The patient had a full maxillary denture.
Solution: The diagnosis centered on the mandibular second molar, since all other teeth were ruled out as having normal pulps. A shepherd’s hook explorer (No. 23) was placed under the solder joint immediately anterior to the crown of the second molar. Lifting the bridge with the explorer confirmed that the bridge was loose on this tooth but well retained on the second premolar. Not only was vertical mobility observed, but bubbles appeared in the saliva along the margins of the crown as the bridge was elevated and reseated. The decision was made to cut the bridge distal to the second premolar. Gross caries was found to have undermined the entire clinical crown of the second molar (see Fig. 3-12, B). Following excava-tion, there was no remaining clinical crown (see Fig. 3-12, C), and the pulp was nonvital. The tooth was eventually retained and restored with a new bridge following a crown-lengthening procedure (see Chapter 17).
If it fails, the patient will still be able to receive root canal treatment (Fig. 3-9).
The radiographic appearance of recurrent decay is most often obvious at the margins of existing restorations. Caries beginning at the depth of a previous caries excavation will almost invariably involve the pulp (Fig. 3-10). Caries under existing crowns appears along the margin but may extend extensively under the clinical crown (Fig. 3-11). Bridge abut-ments are occasionally completely undermined and have no retention.

FIGURE 3-9 Pulpal necrosis and periapical pathosis following vital pulp therapy. Endodontic treatment was then indicated.
FIGURE 3-10 Recurrent caries is deeper than original carious lesion. A carious exposure is likely.
A B
FIGURE 3-11 A, Recurrent caries under the buccal (or lingual) margin of crown. B, Clinical view of excavated caries shown in A.
A
B C
FIGURE 3-12 A, Radiograph of the abutment teeth of a mandibular right posterior bridge. Note the caries at margins of the crown on second molar. B, Following bridge removal, gross caries was found to involve the entire clinical crown on the molar abutment. C, Gross caries excavated. There is no clinical crown remaining.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 49
A B
FIGURE 3-13 A, Typical traumatic coronal fracture of maxillary incisor in a young person. Note open apex. B, An anterior crown fracture in an elderly patient. Note calcification of canal.
Radiographic Changes Associated With Tooth Fractures
Coronal FracturesRadiographically, the most commonly observed fracture is the posttraumatic image of an anterior tooth with coronal tooth loss (Fig. 3-13, A). Generally, the diagnosis does not depend on radiographic findings, but it is wise to make a radiograph to rule out additional fractures below the level of the crestal bone. Complete coronal fractures often occur in older individuals owing to combined factors of heavy occlusal contacts, full crown preparations and calcification. While these patients are frequently asymptomatic, the teeth are functional and exhibit no periapical pathosis. The diagnostic radiograph is important to assess the degree of canal calcifica-tion and the overall root morphology (Fig. 3-13, B). Short roots with severely calcified canals might be treatment planned for extraction.
Coronal fractures in posterior teeth generally occur in a mesial–distal orientation (Fig. 3-14, A), consequently, radio-graphic evidence of the fracture is seldom visible in the tooth structure (Fig. 3-14, B). The most typical radiographic signs of coronal fracture are changes in the coronal alveolar bone mesially, distally and in the furcation extending apically as far as the midroot level (Fig. 3-14, C ) also review Fig. 1-3.
Midroot FracturesTrauma can also result in midroot fractures. If the fracture occurs just submarginally, the crown will be extremely
mobile (Fig. 3-15, A). Radiographically the root is not connected to the crown. If the fracture is more apical, the coronal segment may not be mobile, and the radio-graph will be essential in making an assessment and deter-mining the level and extent of the fracture. Midroot fractures will usually not be evident on clinical examination (Fig. 3-15, B). Chapter 19 offers in-depth discussion on treating these teeth.
Vertical Root FracturesVertical root fractures are a frequent cause of tooth loss almost unique to root-treated teeth. A second unique feature of this problem is the consistent location of the crack lines on the midfacial/buccal or 180 degrees on the midlingual/palatal regions of most roots. Occasionally a root is found with fractures in both positions. Lack of separation of the fractured segments of the root makes vertical root fractures seldom visible radiographically. The characteristic radiographic change is in the adjacent bone, which is the result of bone resorption along the fracture line. Early changes are typified by lateral widening of the periodontal ligament space. Often there is no apical involvement. As bone resorption continues, a distinct lateral radiolucency develops parallel to the root surface (Fig. 3-16).
When a fracture is visible and significant separation of the fractured segments of the root has occurred, the fracture has probably been present for a long time (Fig. 3-17). A number of causes of root fractures have been suggested by many authors. The etiology is said to involve anatomic, restorative, periodontal, or endodontic factors.27 No doubt this is probably a multifactorial problem. Endodontically, excessive removal of root structure during cleaning and

50 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
A
B C
FIGURE 3-14 A, Coronal fractures in posterior teeth tend to be mesial-distal in direction. B, Unusual buccolingual fracture in maxillary molar crown is visible on radiograph. C, Mandibular molar with coronal fracture extending to a level below the furcation; note bone loss. The patient did not have evidence of periodontal disease in other areas of the dentition.
A B
FIGURE 3-15 A, Root fracture near crestal bone level. B, Midroot fracture. Note ovoid appearance of the fracture line.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 51
shaping can weaken a root. During obturation, using exces-sive lateral compaction pressure in the presence of an improp-erly shaped canal and using a spreader that is too large for the shape of the canal can cause a fracture (Fig. 3-18).27 (See Chapter 12.)
Curiously lacking in most discussions is the consideration of the forces of occlusion, specifically in the context of bruxism. A common denominator of teeth with vertical root fractures is the presence of heavy wear facets or other signs of excessive occlusal loading.27 Conversely, it is very rare to see a vertical fracture in a tooth which is out of occlusion. The subject of vertical root fractures is discussed in greater detail in Chapters 5 and 19.
A B
FIGURE 3-16 A, A vertical root fracture is not usually visible on a radiograph. B, Lateral bone loss associated with a vertical root fracture.
FIGURE 3-17 Wide separation of root segments after vertical root fracture. Clinically, deep narrow periodontal defects are found on both buccal and facial surfaces in cases of complete root fracture.
FIGURE 3-18 Vertical root fracture in a second premolar caused by excessive condensation pressure during obturation. Note the widened periodontal ligament space on the distal from crestal bone to the apex. Lateral and longitudinal extrusion of filling materials is a possible sign that fracture occurred during the procedure.

52 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
(Fig. 3-20). This type of external resorption is also referred to as cervical resorption.15,16
External resorptive defects can sometimes resemble defects of internal resorption.12 A key distinguishing factor in most cases is the continued presence of the canal through the resorptive defect (Fig. 3-21). This problem is not of pulpal origin, so the shape of the root canal space is unaltered.
Resorptive defects can have a varied presentation from very early (Fig. 3-22, A) to very severe (Fig. 3-22, B) to the point where a pathologic fracture is possible (Fig. 3-23). There can also be variation in the degree of vertical involve-ment on the root surface from a localized lesion to one that involves the full root length (Fig. 3-24). Note that in Fig. 3-24, B, root canal treatment was done with the apparent and erroneous assumption that the resorption was of pulpal origin.
External invasive resorption is a subset of external resorp-tion.12 The radiographic feature of this type is a honey-combed appearance in which the root canal appears to avoid invasion. At surgery, the root canal is often found to be sur-rounded by a thin layer of intact dentin in an area of advanced resorption (Fig. 3-25). This is due mainly to the fact that the surrounding dentin is actually predentin that lacks mineral content.15,16
To confirm a buccal or lingual location of a resorptive defect, radiographs are made using ideal angulations and at angles divergent from ones taken perpendicular to the tooth.31 The beam is usually angled from the mesial on posterior teeth and from the distal on anterior teeth. Comparison of the films will show that the lesion appears to have “moved” on the angulated film. If the resorptive lesion is on the labial surface of the root, it will appear to move to the distal in comparison with a straight-on view. If the lesion is on the lingual surface of the root, it will appear to have moved mesi-ally. Compare Fig. 3-25, A with the divergent-angle film in Fig. 3-25, B of the same resorptive lesion. In Fig. 3-25, B, which is exposed from the distal, the lesion on the mandibu-lar right central incisor (far right) appears to have moved mesially, indicating it is located on the lingual surface of the root. The radiographic techniques referenced here are detailed in Chapter 2.
Inflammatory resorption is a pathologic process exclu-sively associated with an infected degenerating or necrotic pulp.2 It is usually seen in the presence of a periapical radio-lucency. The affected root may be shortened, and the external surface may appear mottled or irregular in shape (Fig. 3-26). In most cases, the resorptive process is arrested by nonsurgical root canal treatment.
Replacement resorption is often a sequel following replacement of an avulsed tooth or intentional replantation.2 The onset may be weeks or months after clinical healing. It initially appears as an alteration of root-surface contour far below crestal bone. As the process advances, the root appears to become extremely mottled, and the affected areas are asso-ciated with radiolucency in the adjacent bone (Fig. 3-27). Ultimately, the resorbed root may be completely replaced by normal bone.
FIGURE 3-19 A classic example of internal resorption. Signs of pulpal vitality would indicate an active process and warrant immediate endodontic intervention.
Radiographic Tooth Changes Associated With Resorption
There are four types of resorption of tooth structure that can be identified radiographically.1,2,29 In this section, the radio-graphic features of these pathologic entities will be described and compared. Further discussion of etiology, histologic characteristics, and treatment options will be found in Chap-ters 13, 18, and 19.
Internal resorption is characterized by a relatively sym-metric radiolucency located in the mesial-distal center of the root.29 Radiographs taken at any angle other than perpen-dicular to the tooth will confirm the central location of the defect in the root. A key distinguishing radiographic finding is the loss of the canal outline in the resorptive defect. Note the large midroot radiolucency in Fig. 3-19. No canal outline is visible on the large defect, owing to enlargement of the canal space from within. The process is a function of vital yet inflamed pulp. Often at the time of discovery, the pulp may have already become necrotic, so internal resorption may be observed on a tooth with an apical lesion as well as on a tooth without an apical lesion.
External root resorption, as the name implies, originates from the periodontium and invades the tooth on the external surface of the root.1,29 The defects are usually characterized by an irregular shape and are not centrally located in the root. Many seem to originate at the level of crestal bone in the marginal periodontium and are discovered clinically as a defect in the root surface below the free gingival margin

A
C D
B
FIGURE 3-20 A, Radiograph of external resorption in the marginal periodontium. B, Clinical appearance of same case. C, Clinical view of the defect during repair procedure. D, Cervical external resorption on the distal of a maxillary right first molar.
FIGURE 3-21 External resorption can resemble internal resorption on radiographs. Note that root canal is unaltered in this case (left arrows indicate margin of lesion, right arrows indicate canal continuity). Within the resorption defect, the appearance of the canal is lost in cases of internal resorption. Compare with Fig. 3-19.

A B
FIGURE 3-22 A, Early external resorption. B, External resorption can be extremely destructive. This tooth required extraction.
FIGURE 3-23 Pathologic fracture of the crown from internal resorption.
A
B
FIGURE 3-24 A, A small lesion of external resorption localized to the marginal periodontium. B, Lesions of external resorption which have a distinct vertical component radiographically have a very poor prognosis. Root canal therapy will not alter or arrest the process of external resorption.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 55
A
B
FIGURE 3-25 A, Cases of extracanal invasive external resorption involving multiple teeth are relatively uncommon. B, A second off-angle image of the same teeth exposed from the distal. Utilizing the “SLOB” (same lingual, opposite buccal) rule, note that the lesion in the mandibular right central incisor (far right) has “moved” mesially. This indicates a lingual location, which is common on the mandibular anterior teeth.
Influence of Radiolucent Anatomic Structures on Radiographic Interpretation
The maxillary sinus is a highly variable radiolucency that is commonly superimposed over the apices of the posterior teeth, occasionally extending anteriorly to include the canine. Careful examination of good-quality films will almost invari-ably reveal that the width of the periodontal ligament remains constant even though root tips may appear radiographically to extend well into the maxillary sinus (Fig. 3-28). This will be an important constant in differentiating normality from pathosis in cases with true pathosis as well (Fig. 3-29), although there are occasional exceptions to this general obser-vation. The normal sinus can resemble a pathologic lesion in which the lamina dura and periodontal ligament space sur-rounding superimposed root tips will not be evident. Fortu-nately, these exceptions are quite infrequent (Fig. 3-30). Sensibility testing will be required to differentiate pathosis from normality.
The only other normal radiolucency in the maxilla is the incisive canal. Anatomically, it is in the midline and would rarely if ever be confused with periapical pathosis (Fig. 3-31). Where it appears large enough, the periodontal ligament space on the adjacent root surfaces will still appear of normal width (Fig. 3-32). Pathologic problems in this area will be discussed in a later section.
The mandibular canal, mental canal, and mental foramen most often are located anatomically and radiographically at some distance from the apices of the teeth so that no diag-nostic confusion occurs (Fig. 3-33). Within the range of anatomic variation, however, these structures can present diagnostic challenges. The mandibular canal can alter the
FIGURE 3-26 External inflammatory resorption. The pulp is always necrotic with this pathologic process.
FIGURE 3-27 External replacement resorption.

56 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
normal periodontal ligament space around the apices, similar to the effect of the sinus on maxillary apices (Fig. 3-34). The mental canal and mental foramen can also be superimposed over the apices. If there is no pathosis, the apical periodontal ligament space and lamina dura will remain intact. The pres-ence of periapical pathosis, however, can pose a diagnostic challenge (Fig. 3-35). The position of the mental foramen has been found to be located between the two premolars 50% of time, distal from this central location 25% of the time, and mesial to it 25% of the time.13
FIGURE 3-28 Roots of normal healthy teeth which radiographically extend into the maxillary sinus have an uninterrupted periodontal ligament space and lamina dura.
FIGURE 3-29 Most frequently, an apical lesion will be radiographically distinct from the sinus cavity.
FIGURE 3-30 An unusual case in which the normal sinus appears as an apical lesion. Pulp testing results were completely normal for all teeth in the area. This person had been referred for endodontic treatment. Note the normal periodontal ligament space and lamina dura on the roots associated with the radiolucency.
A B C
FIGURE 3-31 A, The incisive canal is typically located between the roots of the maxillary central incisors. B, With anatomically short roots, the incisive canal may appear above the apices but still in the midline. It is usually easy to distinguish from an apical lesion. C, Large apical lesion of pulpal origin on the apex of the maxillary right central incisor. Asymmetry and loss of normal apical anatomic structures identifies this lesion as pathologic in contrast to the appearance of a normal incisive canal.

FIGURE 3-32 The periodontal ligament space remains intact in the case of an unusually large incisive canal. Compare this normal incisive canal with the pathologic lateral lesion depicted in Fig. 3-50.
A
B
FIGURE 3-33 A, The typical mandibular canal is located at some distance inferior to the apices of the premolar teeth. B, Frequently, the mandibular canal is not evident on routine periapical radiographs.
FIGURE 3-34 Superimposition of apices of teeth over the mandibular canal can suggest possible periapical pathosis. In this image, close examination reveals intact periodontal ligament spaces around all apices.
A
B
C
FIGURE 3-35 A, The mental canal and foramen can resemble lesions of periapical pathosis. Note the intact periodontal ligament space around the apex of the second premolar. B, A mental foramen in close proximity to the apex of the second premolar. C, An apical lesion superimposed over the mental foramen.

58 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
Rarely, an anatomic depression on the medial surface of the body of the mandible, known as Stafne’s defect, will appear as a periapical lesion. Sensibility tests will provide normal pulp responses (Fig. 3-36).20,28
Influence of Radiopaque Structures on Radiographic Interpretation
Anatomic or iatrogenic impediments to radiographic inter-pretation occur when teeth are superimposed over one another or a metallic object obscures the apex. It is not unusual to see impacted maxillary third molars obscuring the apices of maxillary second molars (Fig. 3-37). Impacted teeth in other areas can produce the same effect (Fig. 3-38). Metallic objects that obscure the apex are often permanent ligature wires or plates placed during orthognathic surgery or the reduction of traumatically induced fractures (Fig. 3-39). Implants sometimes have the same effect (see Fig. 3-39). For endodontic purposes, the value of these images is limited by the inability to evaluate the width of the peri-odontal ligament space or the continuity of the lamina dura at the apex. It is possible, however, to theorize about a possible etiology by evaluating other radiographic aspects of the teeth such as caries, the depth of existing restorations, and the periodontal condition of the supporting bone. Accu-rate assessment will rely on clinical examination; sensibility testing will usually be the most important component (Fig. 3-40). During root canal procedures in such cases, an elec-tronic apex locator is the only alternative for length determination.
FIGURE 3-36 Staphne’s defect. The tooth responds normally to all vitality tests. Note the intact apical periodontal ligament space.
CLINICAL PROBLEMProblem: A 38-year-old female presented with a recent onset of mild percussion sensitivity on the mandibular left first premolar. Approximately 8 months earlier, implants had been placed in the positions of the mandibular left first molar and second premolar (Fig. 3-41, A). The periapical image indi-cated what appears to be superimposition of the implant in the second premolar position over a portion of the apex of the first premolar. Clinical examination confirmed percussion ten-derness only on the first premolar. Sensibility tests were non-contributory due to lack of sensitivity on the first premolar and several other presumably normal anterior teeth tested for comparison. The dilemma: How was the diagnosis going to be made?
Solution: The spontaneous onset of percussion tenderness was due to one of two possible etiologies. Either the tooth had pulpal pathosis or the tooth was under traumatic occlusal forces, usually associated with bruxism. In this case, the reasonable course was to check the occlusion and eliminate any heavy or premature contact. Occlusion was in fact found to be heavy, and appropriate adjustment was done. The patient was discharged with the advice to monitor the problem. When a diagnosis cannot be confirmed, it is appro-priate to wait.
Seventeen months later, the patient returned with more acute percussion tenderness than that observed on the first visit. She related that over the months since the occlusal adjustment, she had experienced occasional episodes of recurrent percussion tenderness lasting 2 to 3 days but not severe enough to seek a consultation. Three days prior to the present visit, the tooth had become acutely tender to percus-sion. The periapical image did not reveal any deleterious changes, and the occlusion was no longer a factor that could explain the symptoms. A clinical decision was made to initiate root canal treatment. Not only was the pulp necrotic, but during cleaning and shaping of the canal, endodontic files would not extend to the estimated length of the root. The files in fact were in contact with the threaded surface of the implant. Root canal treatment was completed in the usual manner, and the symptoms resolved (see Fig. 3-41, B).
FIGURE 3-37 Superimposed impacted third molars can obscure anatomy of the roots of the second molars.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 59
A
B
FIGURE 3-38 A, Impacted canine obscuring the apex of a maxillary central incisor. Apical resorption of the incisor is possible. B, Superimposition of the crown of an impacted maxillary premolar over the mesiobuccal root of the first molar. Close examination reveals that the periodontal ligament surrounding the apex of the mesiobuccal root is intact.
FIGURE 3-39 Apices of a maxillary molar obscured by fixation device secured with screws. It is not unusual to see apices obscured with ligature wires, arch bars, and implants.
A
B
FIGURE 3-40 A, Radiographic assessment of distal apex of second molar is limited by superimposition of impacted third molar. Apical resorption of distal root of second molar is possible and difficult to confirm. Pulpal assessment must depend on testing, but depth of caries is useful diagnostic information. B, In treatment, the electronic apex locator is necessary for length determination. Radiographic assessment of outcome is difficult.
Occasionally the bone itself may obscure the root apex (Fig. 3-42). The traditional name for this area of increased density is condensing osteitis, and it is found more often in the mandibular molar and premolar regions. There is some evidence that these lesions may be related to long-term, chronic pulpal inflammation/degeneration7,23 but no evi-dence to suggest the bone is actually inflamed, so treatment is not required. There is conflicting evidence that these bony lesions may or may not disappear after root canal treat-ment.8,14 It is possible to have an inflamed pulp in an area where condensing osteitis exists, but the two conditions may or may not be related. The decision to treat the tooth asso-ciated with such an area must be based on diagnostic assess-ment of the pulp and not the mere radiographic presence of an opacity.

60 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
Radiographic Changes Associated With Pulpal Necrosis in Periapical Tissues
The only pulpal conditions that cause periapical pathosis are pulpal necrosis and (occasionally) severe irreversible pulpitis (see Chapter 1). At the time of onset of apical inflammation, there may be no changes on a radiograph, yet the tooth will often be acutely tender to percussion, with radiographic changes usually following within a few days. The radio-graphic lesion which appears is the result of bone resorption caused by the necrotic pulpal tissue and bacteria emanating from the apical foramen. Many lesions develop slowly over a relatively long period of time. Even in cases of acute apical
infection without a preexisting lesion, a radiographic lesion may not become evident for as long as 10 days.3,4
The earliest change will be observed as a widening of the periodontal ligament space in the region of the apical foramen. This can sometimes be subtle and difficult to distinguish from the variation seen in the normal apical anatomy. For this reason, the radiograph alone is insufficient to make a final diagnosis. A history of symptoms would be very impor-tant, and sensibility testing and the other forms of clinical evaluation would have to be done.
CLINICAL PROBLEMProblem: A 48-year-old female with a 1-week history of mild tenderness to percussion on the mandibular left second molar was seen for examination. Sensibility testing was limited by the presence of porcelain veneer crowns on both the first and second molars, and neither tooth responded to hot or cold. Heavy wear facets were observed on the second molar, found to be the symptomatic tooth. A radiograph was made (Fig. 3-43, A), but interpretation was difficult because of the super-imposition of the mandibular canal over the apices.
Solution: Without a firm diagnosis, it was wise to proceed cautiously. Occlusal adjustment was done, and the patient was advised to monitor the situation. If the symptoms resolved within a few days, the presumptive diagnosis of bruxism would be confirmed. In this case, the woman returned about 10 days later with increasing pain to percussion. A new radiograph now confirmed a widened apical periodontal ligament space consistent with periapical pathosis of pulpal etiology. Root canal treatment was initiated, and a necrotic pulp was con-firmed (see Fig. 3-43, B).
A B
FIGURE 3-41 A, Apex of premolar is obscured by implant. B, During treatment, it became apparent that the apex was cut in preparation for the implant.
FIGURE 3-42 Radiopaque bone is superimposed over distal apex of second molar.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 61
A B
FIGURE 3-43 A, Mandibular canal makes it difficult to radiographically interpret periodontal ligament surrounding apices of second molar. B, Ten days following initial examination, radiographic evidence of periapical pathosis is more apparent.
A B
FIGURE 3-44 A, Early signs of periapical pathosis on maxillary central and lateral incisors. Teeth had sustained traumatic injury approximately 2 months previously. B, Early signs of periapical pathosis in a mandibular molar. This tooth had a coronal fracture to the level of the pulp chamber.
FIGURE 3-45 Periapical lesions such as these are virtually diagnostic for a tooth with complete pulpal necrosis.
As periapical pathosis progresses, the loss of apical bone will increase, causing a more characteristic periapical lesion. At this point, the pulp will be necrotic. The apical periodontal ligament space will be found to be widened and become continuous with the apical radiolucency; the lamina dura in the apical area is lost. It is still necessary, however, to complete a clinical evaluation to confirm pulpal necrosis (Fig. 3-44). Ultimately a periapical lesion will reach a size that will be virtually diagnostic for a necrotic pulp (Fig. 3-45).
Periapical lesions of pulpal origin always exhibit loss of normal periodontal ligament space and lamina dura in the affected area. As the lesion enlarges to approximate the roots of adjacent teeth, the periodontal ligament space may be lost on these teeth as well, but it cannot be assumed that all

62 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
A
B
FIGURE 3-46 A, Pretreatment film indicating a large apical lesion encompassing the apices of four mandibular incisors. Pulp tests indicated normal pulpal vitality on the lateral incisors. B, The 11-month reevaluation film indicates excellent healing is in progress.
involved teeth are necrotic or need root canal treatment. Once again, sensibility tests are indicated. When root canal treatment is completed on the appropriate teeth, healing of the periapical lesion will follow, and the periodontal ligament space will be restored radiographically on both the involved and the uninvolved teeth. Evidence of radiographic healing can occur in as little as 3 months for small lesions and up to 1 year or longer for larger lesions (Fig. 3-46).
Radiolucencies that develop on the apices of maxillary posterior teeth will initially elevate the thin bone of the sinus floor and the schneiderian membrane lining the sinus (Fig. 3-47). Eventually most larger lesions will form a sinus tract to the buccal or palatal mucosal surface (Fig. 3-48).
FIGURE 3-47 Periapical lesions can elevate the sinus floor and expand the thin bone covering the apices into the sinus cavity.
A
B
FIGURE 3-48 A, Apical lesions frequently develop sinus tracts which drain through the mucosa. B, Opening of a sinus tract on the mucosal surface.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 63
A B
FIGURE 3-49 A, Rarely, a chronic periapical lesion can expand directly into the sinus cavity. Apical surgery was performed in which the sinus cavity was completely enucleated. B, Reevaluation radiograph after more than 12 years.
Pathologic perforation through the schneiderian membrane is fortunately rare but not impossible. It is difficult to make this determination radiographically, because the anatomic relationship between the apices of the teeth and the floor of the sinus is highly variable. Many apices of healthy teeth lie inside the sinus cavity and are covered only by periodontal ligament and the sinus membrane. Loss of these radiolucent structures will be very difficult to discern, even on the best of images. Fig. 3-49, A demonstrates a case of acute apical abscess extending into and occupying the entire sinus cavity. The extent of involvement was only confirmed after surgical intervention during which the entire sinus cavity was enucle-ated. A 12-year, 3-month reevaluation is seen in Fig. 3-49, B. Note that the healing process resulted in almost complete occlusion of the sinus cavity.
Lateral Radiographic Changes Associated With Pulpal Necrosis
Interruptions in the periodontal ligament or lamina dura laterally can occur at the site of a lateral canal (Fig. 3-50). The process is identical to the development of an apical lesion in which the lateral lesion develops as a reaction to the emer-gence of necrotic pulpal material and bacteria. Rarely, a tooth with a lateral canal lesion may actually respond to an electric pulp test if the pulp apical to the lateral canal is still vital. These responses are usually much higher on the arbitrary scale of the electric pulp tester compared to those of the presumably normal adjacent or contralateral teeth. Usually there is no response to a cold test.
Periapical lesions of pulpal origin may extend coronally and drain clinically. The radiographic appearance of a sinus tract is similar to a lesion of severe periodontitis (Fig. 3-51). Drainage will usually follow the tract along the root
FIGURE 3-50 Lateral lesion associated with a necrotic pulp.
FIGURE 3-51 Apical lesion with a sinus tract along the root surface.

64 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
CLINICAL PROBLEMProblem: A 34-year-old male was referred for routine root canal treatment of the maxillary left central incisor due to fracture of the clinical crown. The existing crown was cemented temporarily (Fig. 3-53, A). The root treatment was uncomplicated, and the patient was returned to the referring dentist with the crown cemented using a temporary post. Twenty years later, the patient was referred again to the endo-dontist with the tentative diagnosis of treatment failure (see Chapter 5). There was a recent history of local swelling, and a sinus tract stoma was observed near the gingival margin of the same tooth.
Solution: Review of the radiograph indicated that despite the overextension of the intraradicular post, there was no sign of failure (see Fig. 3-53, B). Probings ruled out a vertical root fracture but did indicate that there was a periodontal defect on the mesial that probed 9 mm. The presence of cal-culus was evident radiographically and was clinically palpable with the explorer. The diagnosis of periodontal abscess was confirmed.
FIGURE 3-52 Molar sinus tracts may involve the furcation.
surface and emerge through the mucosa as a sinus tract stoma (sometimes referred to as a fistula) or through the gingival sulcus. Probings of sulcular drainage tracts will be distinctly narrow and on molars, may or may not involve the furcation (Fig. 3-52). Radiographically, a distinguishing feature of drainage tracts is the lack of periodontal bone loss on adjacent teeth. Chronic periodontitis is most often characterized by radiographic evidence of bone loss in mul-tiple areas but without involvement of the periapical tissues (unless an advanced state of deterioration exists).
A
B
FIGURE 3-53 A, Original referral film from 1980. B, Reevaluation after 20 years. Note the advanced periodontal lesion on the mesial.
Radiographic Changes Associated With Cases of Endodontic Failure
Root-treated teeth that fail will develop lesions that are radiographically identical to lesions that result from the extension of pulpal infection to the periapical bone (Fig. 3-54, A). Lesions may occur at the apex or the site of a

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 65
A B
FIGURE 3-54 A, Periapical lesions resulting from failed endodontic treatment appear radiographically identical to lesions of primary infection. B, Four year reevaluation after nonsurgical revision indicating complete resolution of the apical lesion.
BA
FIGURE 3-55 A, Lateral lesion associated with a lateral canal communicating with unsealed canal space around intraradicular post. B, Five-year reevaluation of the revised root canal treatment, indicating complete healing of the lateral lesion.
lateral canal (Fig. 3-55, A). Most will respond to nonsurgi-cal revision, after which the periodontal ligament and lamina dura will reappear as a result of healing (Fig. 3-54, B and 3-55, B).
If an asymptomatic periapical lesion is discovered on routine examination, it is wise to ask the patient when the treatment was performed. Lesions typically take 3 to 12 months to resolve following root canal treatment. Sometimes larger lesions require more time. If the treatment in question was completed less than 12 months prior to examination, the appropriate course of action would be radiographic reevalu-ation of the lesion in 6 months. If the treatment had been completed more than 2 years previously, the tooth may be presumed to have recurrent pathosis and would be indicated for treatment revision in most cases.
Diagnosis of recurrent periapical pathosis is discussed in depth in Chapter 5. The techniques for revision of previous root canal treatment are discussed in Chapter 14.
Radiographic Changes Associated With Nonendodontic Pathoses Mimicking Potential Endodontic Problems
CementomaA cementoma, also known as a periapical ossifying fibroma or cemento-osseous dysplasia, is a lesion that occurs primarily in the mandibular anterior area.25 More than one tooth may be involved, and initially there is a developing radiolucency. In time, the lesion will begin to undergo mineralization (Fig. 3-56). Sensibility tests are critical for making this diagnosis. Teeth with cementomas will invariably respond normally to testing and do not require root canal treatment.

66 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
Developmental CystsThe incisive canal cyst, also known as the nasopalatine duct cyst, is a developmental cyst that occurs in the incisive canal (or nasopalatine duct).9 Radiographically, the lesion appears much larger than the incisive canal foramen. It can involve the apices of the central incisor teeth, and the apical peri-odontal ligament space and lamina dura can be lost. Internal positive pressure can gradually displace the roots of the
CLINICAL PROBLEMProblem: A 42-year-old male sought dental consultation for acute pain in the maxillary left anterior area. The dentist found a large radiolucent lesion between the apices of the maxillary left lateral incisor and canine (Fig. 3-58, A). On opening, the dentist recorded that there was profuse drainage. The patient was referred to an endodontist for completion of the treat-ment. Four months later, the patient was seen by the endo-dontist for the first time. The patient had been symptom free. Note the periapical anatomy on the preoperative film (see Fig. 3-58, A). While the periodontal ligament space appears intact, the lamina dura is interrupted. On opening, there was no drainage, and the root canal treatment was completed. Almost 10 years later, the patient returned to the endodontist for reevaluation of the same tooth. He was experiencing recur-rent symptoms of pressure and pain in the area. The periapical film indicated that the lesion had failed to heal, but the apical periodontal ligament space was of uniform width, and the lamina dura was intact (see Fig. 3-58, B).
Solution: Periapical surgery was performed, during which no communication with the apex of the tooth was observed. The curetted soft-tissue lesion was submitted for histologic examination, and a diagnosis of “benign fibro-osseous lesion, possibly representing cemento-osseous dysplasia” was reported by the pathologist. The symptom-free patient returned for reexamination 3 months later, and a posttreat-ment radiograph indicated excellent healing (see Fig. 3-58, C).
FIGURE 3-56 Early onset of periapical ossifying fibromas involving three mandibular incisors. The teeth respond normally to tests.
FIGURE 3-57 Incisive canal cyst. Note the intact periodontal ligament spaces around the apices of both central incisors. The teeth responded normally to sensibility tests.
central incisors laterally. This is not a lesion of pulpal origin; the teeth will respond normally to tests, and root canal treat-ment is not indicated (Fig. 3-57).
The term globulomaxillary cyst has been questioned as not describing a distinct histologic entity but rather a group of lesions which occur in the suture line between the maxillary lateral incisor and the canine.18,25,32 Although most lesions have been found to be of odontogenic origin, some lesions are distinctly nonapical lesions for which endodontic inter-vention is not indicated. Sensibility testing is critical to estab-lishing the correct diagnosis.
Healed Endodontic LesionsLarge lesions in the anterior maxilla are often treated surgi-cally. On surgical exposure of the defect, the entire buccal plate of bone may be missing due to destruction from infec-tion and enlargement of the lesion. Following complete peri-apical curettage, it is sometimes found that the palatal plate is missing as well. After such through-and-through lesions heal, sometimes the radiolucency will remain above and radiographically separate from the apices of the teeth. This condition is a form of scarring.19,26 The lesion is caused by the infilling of fibrous connective tissue instead of bone, yet is perfectly healthy. There is no indication for treatment (Fig. 3-59).

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 67
A B C
FIGURE 3-58 A, Referral film of a suspected periapical lesion of pulpal origin supplied by the referring dentist. Subsequent to making this film, the tooth was opened for root canal treatment due to acute symptoms of pain. Referral report stated that copious amounts of straw-colored fluid had drained from the canal on opening, no drainage was observed by the endodontist, and root canal treatment was completed on the initial visit. B, Recurrent symptoms in the area 9 1
2 years later warranted reevaluation of the lesion. Periapical surgery was performed, and the apical tissue was submitted for histologic examination. C, Three-month reevaluation image indicating healing of lesion.
FIGURE 3-59 Reevaluation 15 years after apical surgery. At surgery, the lesion was observed to fenestrate both the labial and palatal plates of bone (through and through). The apparent “apical lesion” represents normal healing of these lesions.
FIGURE 3-60 Lateral periodontal cyst presented similarly to a lateral lesion. Both teeth responded normally to vitality tests.
Periodontal LesionsLesions of periodontal disease do not normally involve areas of the root which would resemble lesions of endodontic origin. Periodontal disease is a process that causes destruction
of bone in a coronal-to-apical direction, whereas endodontic lesions generally progress from the apex coronally. Neverthe-less, there are some clinical problems which can cause diag-nostic confusion.
A lateral periodontal cyst is a lesion of unknown origin that arises predominantly in the mandibular premolar areas.11

68 chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images
FIGURE 3-61 A lateral periodontal cyst discovered superior to a periapical lesion on an endodontically treated tooth. Acute apical symptoms warranted apical surgery. The lateral periodontal cyst was a completely separate lesion.
It is not of pulpal origin but appears similar to a lateral lesion in the presence of a necrotic pulp and lateral canal. Even though there is a draining sinus tract present clini-cally, both adjacent teeth respond normally to pulp tests in Fig. 3-60, A. This would be considered a lateral peri-odontal cyst.
Occasionally, lesions of advanced periodontitis will cause severe bone loss in a local area, resembling apical lesions. In Fig. 3-61, the periapical lesion appears to be a classic lesion of pulpal origin until the clinical examination reveals complete dehiscence of the lingual surface of the root to the apex. Root canal treatment would be of no benefit to this person. Chapter 4 will explore this area of diagnosis more completely.
This chapter has presented a selective overview of radio-graphic diagnosis limited to endodontic pathosis. Definitions of normality have been discussed that provide a basis for distinguishing abnormal findings associated with pathosis. Some commonly encountered lesions in the bone that mimic disease of pulpal origin have also been presented.
REFEREnCES1. Andreasen JO: External root resorption: its implications in dental
traumatology, paedodontics, periodontics, orthodontics and end-odontics, Int Endod J 18:109-118, 1985.
2. Andreasen JO, Bakland LK: Pathologic tooth resorption. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc.
3. Bender IB, Seltzer S: Roentgenographic and direct observation of experimental lesions in bone: I 1961, J Endod 29:702-706, 2003.
4. Bender IB, Seltzer S: Roentgenographic and direct observation of experimental lesions in bone: II 1961, J Endod 29:707-712, 2003.
5. Bergenholtz G, Spångberg L: Controversies in endodontics, Crit Rev Oral Biol Med 15:99-114, 2004.
6. Cotti E, Campisi G: Advanced radiographic techniques for the detection of lesions in bone, Endod Topics 7:52-72, 2004.
7. Douglass GD, Trowbridge HO: Chronic focal sclerosing osteomy-elitis associated with a cracked tooth. Report of a case, Oral Surg Oral Med Oral Pathol 76:351-355, 1993.
8. Elliasson S, Halvarsson C, Ljungheimer C: Periapical condensing osteitis and endodontic treatment, Oral Surg Oral Med Oral Pathol 57:195-199, 1984.
9. Escoda Francoli J, Almendros Marqués N, Berini Aytés L, et al: Nasopalatine duct cyst: report of 22 cases and review of the litera-ture, Med Oral Patol Oral Cir Bucal 13:E438-E443, 2008.
10. Estrela C, Bueno MR, Leles CR, et al: Accuracy of cone beam computed tomography and panoramic and periapical radiology for detection of apical periodontitis, J Endod 34:273-279, 2008.
11. Formoso Senande MF, Figueiredo R, Berini Aytés L, et al: Lateral periodontal cysts: a retrospective study of 11 cases, Med Oral Patol Oral Cir Bucal 13:E313-E317, 2008.
12. Frank AL: Extracanal invasive resorption: an update, Compend Contin Educ Dent 16:250-254, 1995.
13. Gutmann JL, Harrison JW: Surgical endodontics. Boston, 1991, Blackwell Scientific Publications.
14. Hedin M, Polhagen L: Follow-up study of periradicular bone con-densation, Scand J Dent Res 79:436-440, 1971.
15. Heithersay GS: Invasive cervical resorption: an analysis of potential predisposing factors, Quintessence Int 30:83-95, 1999.
16. Heithersay GS: External root resorption, Ann R Australas Coll Dent Surg 12:46-59, 1994.
17. Hinman TP: The interpretation of x-ray pictures of apical granula-tions, giving differential diagnosis of cases favorable and cases unfavorable for treatment root-canal filling, J Nat Dent Assoc 8:83-87, 1921.
18. Hollinshead MB, Schneider LC: A histologic and embryologic analysis of so-called globulomaxillary cysts, Int J Oral Surg 9:281-286, 1980.
19. Huumonen S, Ørstavik D: Radiological aspects of apical periodon-titis, Endod Topics 1:3-25, 2002.

chapter 3 | Problem Solving in Interpretation of Dental Radiographic Images 69
20. Katz J, Chaushu G, Rotstein I: Stafne’s bone cavity in the anterior mandible: a possible diagnostic challenge, J Endod 27:304-307, 2001.
21. Murray PE, About I, Lumley PJ, et al: Cavity remaining dentin thickness and pulpal activity, Am J Dent 15:41-46, 2002.
22. Murray PE, Smith AJ, Windsor LJ, et al: Remaining dentin thick-ness and human pulpal responses, Int Endod J 36:33-43, 2003.
23. Ørstavik D, Larheim TA: Radiographic interpretation. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc, Chap 16, pp 600-625.
24. Patel S, Dawood A, Mannocci F, et al: Detection of periapical bone defects in human jaws using cone beam computed tomogra-phy and intraoral radiolography, Int Endod J 42:507-515, 2009.
25. Resnick CM, Novelline RA: Cemento-osseous dysplasia, a radio-logical mimic of periapical dental abscess, Emerg Radiol 15:367-374, 2008.
26. Rud J, Andreasen JO, Möller Jensen JE: Radiographic criteria for the assessment of healing after endodontic surgery, Int J Oral Surg 1:195-214, 1972.
27. Schweitzer JL, Gutmann JL, Bliss RQ: Odontiatrogenic tooth fracture, Int Endod J 51:64-74, 1989.
28. Solomon LW, Pantera EA, Jr, Monaco E, et al: A diagnostic chal-lenge: anterior variant of mandibular lingual bone depression, Gen Dent 54:336-340, 2006.
29. Tronstad L: Root resorption—etiology, terminology and clinical manifestations, Endod Dent Traumatol 5:255-265, 1989.
30. Tyndall DA, Rathore S: Cone-beam CT diagnostic applications: caries, periodontal bone loss assessment, and endodontic applica-tions, Dent Clin North Am 52:825-841, 2008.
31. Walton RE: Diagnostic Imaging. A. Dental radiography. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc.
32. Wysocki GP, Goldblatt LI: The so-called “globulomaxillary cyst” is extinct, Oral Surg Oral Med Oral Pathol 76:182-184, 1993.
RECoMMEnDED ADDitionAL READingMjör IA: Pulp-dentin biology in restorative dentistry. Chicago, 2002,
Quintessence Publishing Co.Ørstavik D: Radiology of apical periodontitis. In Ørstavik D,
Pitt Ford TR, editors: Essential endodontology—Prevention and treatment of apical periodontitis, Oxford, 1998, Blackwell Science.
Sewerin IP: Radiographic examination. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.

70
Chapter 4
I have never found a pulp removed from a pyorrhetic tooth to be normal . . . where a pathologic pulp is present, a pyorrhetic condition cannot be cured by treatment applied exclusively to the external surface of the root, with no treatment of the pulp itself.12
L.R. Cahn, 1927
Problem Solving in the Differential Diagnosis of Bony Defects Resulting from Pulpal and Periodontal Pathosis
Problem-Solving ListProblem-solving challenges and dilemmas that deal with the differential diagnosis of bone defects resulting from pulpal and periodontal pathosis addressed in this chapter:
Controversies and highlights of Disease Interactions
an Endodontic Perspective on Chronic Periodontitis
Periodontal Lesions of Bone that Can Be Confused With Pulpally Induced Bony Lesions
Acute periodontal abscess
Lesions of chronic periodontitis
Periodontal lesions involving the furcation
Lesions associated with aggressive forms of periodontitis
External root resorption
Cemental tears
Pulpally Induced Lesions that Can Be Confused With Periodontal Lesions
Furcation or lateral lesions without loss of attachment
Acute periapical abscess
Chronic sinus tracts of pulpal origin with drainage through the gingival sulcus
Chronic sinus tracts of pulpal origin with permanent periodontal attachment loss
Response of the periodontium to mechanical root perforations
Bony Lesions of the Periodontium that Do not Originate from Either Periodontal or Pulpal Pathosis
Deep coronal fractures
Vertical root fractures
Developmental lingual groove on maxillary lateral incisors and similar lesions
Other possible rare lesions
The relationship of disease processes coming from the pulp of the tooth to the supporting periodontium is a subject that has received much attention in endodontic literature for almost 90 years.10,12,18 The reverse situation has also been controversial: the impact of periodontal pathosis on the dental pulp.* Clinically, two important issues must be kept in focus. Pulpal pathosis and its extension into the peri-odontium causes a localized periodontitis with the potential for further extension into the oral cavity.26 Periodontal patho-sis and its extension have little short-term effect on the dental pulp.26 However, the long-term effect of periodontal
Interradicular periodontal lesions can be initiated and perpetuated by inflamed or necrotic pulps. Extension of the inflammatory lesions from the dental pulp apparently occurs through accessory or lateral canals situated in the furcation regions of premolars and molars.45
S. SELtzER, I.B. BEnDER, h. nazImOv, 1967
*References 15, 21, 28, 37, 46, 60, and 63.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 71
inflammatory substances and/or bacteria. For our purposes, the pathophysiologic relationships that exist between the pulp and periodontium are less important than an accurate diagnosis or one based on the best clinical evidence available on clinical problems and lesions that present on a daily basis. In general, inflammation or bone loss in the periodontium caused by lesions of pulpal origin will heal following a wide range of endodontic treatments. These types of cases are seen as a radiolucent lesion around the root apex, in an isolated furcation that has no other etiology, or on the lateral surface of a root. Specific periodontal treatment in these cases is rarely if ever warranted. The vast majority of lesions of the periodontium do not affect the dental pulp. The incidence of cases in which a connection between a lesion of pulpal origin and one of periodontal pathosis is even suspected is small.27,42
This chapter has three objectives: (1) to clarify the most important diagnostic characteristics of lesions of the peri-odontium, with emphasis on those that resemble the exten-sion of pulpal pathosis to the supporting root tissues; (2) to clarify the distinguishing diagnostic characteristics of perira-dicular lesions of pulpal origin that resemble or are mistaken for periodontal defects; and (3) to discuss the characteristics of lesions that are the result of neither inflammation/ infection of the pulp or periodontium, yet may share char-acteristics of both. Treatment suggestions will accompany the lesions described.
An Endodontic Perspective on Chronic Periodontitis
The etiology and pathophysiology of chronic periodontitis is extremely complex. Briefly summarized, lesions of the disease are the result of microbiologic and immunologic effects of a biofilm that forms on the surfaces of roots.4,35,62 Fortunately, an accurate clinical diagnosis of periodontitis can usually be made on the basis of physical examination35 and radiographic findings of bone destruction.39 The clinical characteristic of this disease may be summarized as a “top-down” process, meaning simply that it begins with inflammation of the marginal periodontium and progresses apically with the gradual destruction of the crestal supporting bone (Fig. 4-1, A and B).
For the dentist/endodontist, the periodontal probe is absolutely indispensable to clinical diagnosis. During assess-ment of the periodontium, measurement of attachment loss is the standard by which progression or remission of the disease is assessed.62 Within the discipline of endodontics, the discrimination between periodontal lesions and those origi-nating from the dental pulp can usually be made by identify-ing the physical characteristics of the lesion itself.27,28 The technique of diagnostic periodontal probing should be done using a relatively small-diameter instrument (0.05 mm at the tip) with standard markings (Fig. 4-2).62 Probing should be done with as uniform a pressure as possible, slightly angling the tip of the probe toward the surface of the root.30
pathosis, especially in conjunction with concomitant restor-ative procedures, must be considered in all diagnostic and treatment planning considerations.
Controversies and Highlights of Disease Interactions
Pulp tissue degenerates after a multitude of insults—caries, restorative procedures, chemical and thermal insults, trauma, and some periodontal treatment. When products from pulp degeneration, in particular inflammatory exudates and bac-teria, reach the supporting periodontium, many changes may occur, including a rapid onset of inflammation, lateral or furcation bone loss, tooth mobility, and sinus tract formation through the buccal mucosa or gingival sulcus. If this occurs in the apical region, a periapical lesion forms (see Chapter 3). If this occurs with crestal extension of the inflammation, a periodontitis of pulpal origin is formed.49 However, the lesion formed has little anatomic similarity to a defect of periodontal pathosis.
Periodontal disease is generally a slow-developing process that may have a gradual atrophic effect on the dental pulp. Complete pulpal necrosis caused by periodontal pathosis, however, is uncommon. Changes in the pulp include chronic inflammation, localized tissue death (infarction), fibrosis, decrease in cellular populations, resorptions, local coagula-tion necrosis, or dystrophic calcification.32,43,46,50 Periodontal procedures such as deep scaling and curettage54 (with the use of localized medicaments) and gingival injury or wounding53 may enhance further pulpal inflammation and perpetuate the interrelated disease process in a small number of cases.
The most intimate and demonstrable relationship of the communication of inflammation between the two tissues is via the vascular system,9,20,31,54 as demonstrated anatomically at the apical foramen and adjacent to aberrant accessory com-munications.11,18,25,36,43 These channels, when patent, may serve as potential routes of inflammatory interchange. Still other channels, covered by cementum, may be exposed during scaling or other periodontal therapeutic procedures.54 To what extent these vascular communications must be dis-rupted to cause a resultant overwhelming inflammatory process is unknown and a major concern.32
The main anatomic pathways must be considered as potential pathways in the exchange of inflammatory products and bacteria between the pulp and the periodontium (and vice versa) and include lateral/accessory canals that branch off the main root canal, open dentinal tubules (sometimes due to cemental agenesis), the presence of lingual grooves, removal of cementum during periodontal or restorative pro-cedures or loss due to resorptive defects, and root or tooth fractures.
For intact teeth, the principle avenues of communication would be the main foramen, lateral/accessory canals, and dentinal tubules. In the clinical setting, however, there are few means to determine that these particular avenues of com-munication are actively involved in the exchange of

72 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
differentiation of lesions of pulpal origin from periodontal lesions, probings in the area of principle concern should be performed circumferentially on each tooth in small (1-mm) increments. The intent is to explore the physical morphology or bony architecture of a lesion. There is a distinction between “probing” the attachment levels and “sounding” the location of the crestal bone.27 In the technique of sounding, the probe is inserted past the level of attachment directly to bone. This is a more accurate method of assessment but will usually require some level of local anesthesia. Generally, probing will yield adequate diagnostic information, especially in combina-tion with radiographs.
Osseous defects resulting from chronic periodontitis are routinely found to be of varying depth but similar in form. Probing circumferentially across a broad root surface will usually indicate a gradual increase in depth until the deepest area of the defect is reached. Continuing past this point, the probing depths will then gradually decrease. The typical con-tours of crestal bone found in bony lesions of advanced periodontitis are illustrated in Fig. 4-3. Note the general increase in root exposure from mesial to distal, which would be reflected as a gradually increasing probing depth on a clinical examination.
The normal periodontium is known to have fairly pre-dictable dimensions.23 The average distance from the gingival margin to crestal bone has been found to be approximately 2.5 mm. Increased probing depths represent the loss of periodontal attachment to the tooth and crestal bone. Since chronic periodontitis is usually generalized, osseous defects are typically found in multiple areas of the denti-tion, particularly in the posterior sextants. This can be an important finding in the diagnosis of potential end-odontic problems. In the diagnosis of a localized defect of unknown origin, begin the diagnostic examination by probing multiple random locations throughout the denti-tion.27 Findings of osseous defects in several locations well apart from the area of chief concern would tend to support a tentative diagnosis of periodontitis for the area in ques-tion. In contrast, random probings that reveal no indication of periodontal bone loss in any other area would suggest a possible nonperiodontal etiology for the localized defect being evaluated.
Traditionally in routine periodontal examinations, probing depths have been recorded in six locations for each tooth: the mesial, midsurface, and distal of both the buccal and lingual surfaces.4 For the purposes of endodontic diagnoses and the
FIGURE 4-2 Periodontal probes with small-diameter tips are preferable. FIGURE 4-3 Surgical exposure of advanced lesion of chronic
periodontitis. Note altered contours of the crestal bone.
A B
FIGURE 4-1 a, Typical radiographic presentation of periodontal bone loss on mesial of mandibular first molar. B, 5 years later, bone loss has progressed to a deeper level.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 73
Periodontal Lesions of Bone that Can Be Confused With Pulpally Induced Bony Lesions
Bony lesions of periodontal disease are usually not difficult to distinguish from bony lesions of pulpal origin. Periodontal defects begin in the marginal periodontium, and even deep periodontal pockets are usually far removed from the root apex (Fig. 4-4). Confusion in diagnosis usually arises in cases of acute periodontal abscess, periodontal infection causing chronic sinus tracts in the mucosa, or localized periodontal bony lesions extending deep enough to involve the apex of a tooth. The severity of periodontal bone destruction, however, varies in the same dentition. At times it may be quite localized and extend to the root apices. The following discussion of pathologic entities will include diagnostic pro-cedures necessary to (1) arrive at the best diagnosis based on the gathered information and (2) determine the appropriate treatment plan.
Acute Periodontal AbscessAn acute periodontal abscess is clinically identical to many acute periapical abscesses of pulpal origin. The patient may experience severe swelling (Fig. 4-5, A) along with the usual symptoms of acute infection such as pain, fever, and malaise. The location of swelling near the gingival margin is common to both types (see Fig. 4-5, B).
Diagnostic procedures usually begin with a good radio-graph. In this case (see Fig. 4-5, C ), significant information
FIGURE 4-4 Lesions of advanced chronic periodontitis with severe bone loss do not generally involve the apex, as seen on the second molar. Lesion on first molar is endodontic, with a drainage tract coursing coronal and exiting near the furcation. Circumferential probings of first molar reflect a level of attachment consistent with bone levels seen on radiograph and do not involve the furcation. Prognosis for root canal treatment of first molar and long-term tooth retention is good. Second molar is hopeless periodontally, regardless of pulpal status.
A
B
C
FIGURE 4-5 a, Acute facial swelling associated with periodontal abscess is identical to the swelling of acute periapical abscess. B, Clinical view of same acute periodontal abscess. C, Radiograph of periodontally involved teeth. Note bone loss between molars and lack of periapical involvement.
is immediately apparent: there is loss of crestal bone inter-proximally, indicating a lesion of periodontitis as opposed to one of pulpal origin. There is no radiolucency at the apices. Since it is possible to have an acute periapical abscess without obvious or significant radiographic evidence of a periapical

74 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
Although there may be ample evidence of a general chronic periodontitis in the oral cavity, some localized areas may have developed extremely severe bone destruction. If periodontal defects extend to the apex, the radiographic lesion present
CLINICAL PROBLEMProblem: A 57-year-old male with a history of recurrent swelling on the palatal aspect of the maxillary left first molar was referred for root canal treatment. The referring dentist noted a large periapical lesion encompassing the apex of the palatal root (Fig. 4-11, A). The radiograph also shows evidence of severe bone loss around the buccal roots that was not noted by the dentist. The molar had no restorations, and there was no evidence of a fracture in the crown.
Solution: Sensibility tests should be performed early in the examination. In this case, results were normal—in fact, the tooth was hypersensitive to a cold stimulus. Periodontal prob-ings indicated that there was bone loss to the apex of the palatal root and confirmed severe attachment loss around the other two roots. As in the previous case, root canal treatment would have no effect on this problem, so the tooth was extracted. In these cases, calculus deposits are commonly seen covering the entire root surface (see Fig. 4-11, B).
may be confused with a periapical lesion of pulpal origin. The patient in Fig. 4-10 was sent for completion of root canal treatment on a second premolar. Note the endodontic access cavity in the crown of this tooth. The loss of bone radio-graphically correlated with the loss of attachment circumfer-entially by clinical probing. The extreme mobility of this tooth was another consequence of bone loss. A root canal procedure would have no effect on this condition, so the tooth was extracted.
FIGURE 4-6 Sinus tract of periodontal etiology found in attached gingiva over maxillary left central incisor.
or lateral lesion, the next step in diagnosis is sensibility testing. In this case, all of the maxillary right posterior teeth respond normally to thermal and electrical sensibility tests. This finding eliminates the possibility of a pulpal etiology. The diagnosis of acute periodontal abscess is confirmed by signs, symptoms, and periodontal probings. Treatment plan-ning will be based on probing depths. Probings that are found to confirm attachment loss to the level of the apical third would support tooth extraction as the treatment of choice. Probings to the level of the midroot might favor periodontal surgery to reduce or eliminate pocket depth.
Lesions of Chronic PeriodontitisBony lesions of chronic periodontitis are sometimes confused with lesions of pulpal origin because of a draining sinus tract. In Fig. 4-6, the patient was referred for endodontic evalua-tion because of the drainage tract in the attached gingiva over the left central incisor (arrow). In a similar case (Fig. 4-7), probings are consistent with a deep periodontal lesion. The radiograph clearly shows no apical rarefaction on either of the central incisors (see Fig. 4-7, D), and sensibility tests elicit normal responses. Surgical exposure illustrates the morphology of the defect (see Fig. 4-7, E). Contrast these cases with the endodontic case presented in Fig. 4-8. Clini-cally, the sinus tracts appear nearly identical (see Fig. 4-8, A; also see Fig. 4-6), but surgical exposure of the tooth reveals not only the periapical lesion but also intact crestal bone (see Fig. 4-8, B).
CLINICAL PROBLEMProblem: A 52-year-old male was seen for recurrent local swelling and drainage in the area of the maxillary right second premolar. Clinical examination revealed a draining sinus tract in the attached gingiva near the second premolar. A radio-graph indicated that there was a widened apical periodontal ligament space consistent with a developing periapical lesion in addition to a deep periodontal defect interproximally on the distal (Fig. 4-9, A). At this point, the origin of the sinus tract was unknown.
Solution: Sensibility testing was performed. No responses were obtained from the second premolar, and the first molar previously had root canal treatment. A sinus tract exploration was done by placing a gutta-percha cone in the tract and exposing an additional radiograph (see Fig. 4-9, B). This exami-nation indicated that the drainage was of periodontal origin. No communication between the two lesions was evident on the film, and none was found during probing. The diagnosis was concomitant periodontal and periapical lesions.6 Both root canal treatment and periodontal treatment will be required to resolve the infections in this case (see Fig. 4-9, C).
Occasionally a periodontal bone lesion may resemble a periapical lesion and, at least radiographically, lack other obvious signs of generalized periodontitis.26 At the close of Chapter 3, an excellent example was depicted in Fig. 3-60. What appears to be a typical periapical lesion of pulpal origin is in reality a lesion of severe periodontitis. Once again, root canal treatment would have been of no benefit in this case.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 75
A B
C
E
D
FIGURE 4-7 a, Periodontal probing depth normal interproximally. B, Probing depth normal in midlabial area. C, Deep probing pattern associated with periodontal bone loss. D, Radiograph of same lesion. Note absence of periapical involvement. E, Surgical exposure of periodontal lesion.
CLINICAL PROBLEMProblem: A 38-year-old male presented with a history of recur-rent acute abscesses in the buccal vestibule adjacent to the maxil-lary left first molar. The radiograph showed a “classic” periapical lesion on the apex of the mesial buccal root (Fig. 4-12, A). The lesion was noted to extend coronally along both the mesial and distal surfaces of the root.
Solution: Sensibility tests indicated normal responses on this tooth, confirming that this is not a pulpal problem. Periodontal
probing revealed complete loss of attachment over the entire buccal surface of the root (see Fig. 4-12, B). Large deposits of calculus were seen and felt on the root surface with the probe. The diagnosis of periodontal abscess was made. Since there was minimal periodontal involvement of the other two roots, the optimal treatment plan was to resect (amputate) the mesial buccal root; pulp exposure resulting from the amputation would necessitate root canal treatment on the remaining roots.
Periodontal Lesions Involving the FurcationLoss of bone in the furcation of a molar due to periodontal disease is sometimes difficult to distinguish from bone loss
due to a necrotic pulp (communication via furcation canals)25 or a sinus tract that is traced to the furcation. As cited earlier, the periodontal probe may reveal a sometimes subtle distin-guishing difference. Periodontal defects tend to affect the space in the furcation more or less symmetrically, whereas

76 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A B
FIGURE 4-8 a, Sinus tract similar to Fig. 4-6 but of pulpal etiology. B, Surgical exposure of apical lesion. Note normal crestal bone contours.
A
B C
FIGURE 4-9 a, Maxillary right premolar area with history of recurrent drainage suspected to be of pulpal origin. There is both apical and periodontal pathosis evident on the second premolar. B, Sinus tract exploration with gutta-percha cone, revealing source of drainage is the periodontal lesion. C, Completed root canal treatment will only resolve the periapical lesion. Periodontal surgery is also indicated to eliminate the pocket. This will resolve both associated infection and the drainage tract.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 77
FIGURE 4-10 Localized lesion of advanced chronic periodontitis. Note tooth has been opened for root canal treatment that will have no effect on this lesion.
FIGURE 4-11 a, Radiograph of maxillary left first molar area with apical lesion of chronic periodontitis. Pulp test results are completely normal. B, Following extraction. Note calculus deposits covering entire palatal root.
A
B
sinus tracts tend to align with one root and more directly with a lesion at the apex. Therefore periodontal defects will tend to probe both vertically (parallel to the root) and hori-zontally (buccal-lingually, parallel to the occlusal plane). Sinus tracts of pulp origin tend to probe in a vertical direction only, but in some cases the tract may take a tortuous path, depending on the nature of the bone around the tooth, so straight probes will be of less value in the differential
A
B
FIGURE 4-12 a, Maxillary left first molar with a “classic” periapical lesion on mesial buccal root. B, Clinical examination reveals periodontal etiology. Sensibility test results are normal.
diagnosis of a lesion of this type. This emphasizes the need to have both straight and curved probes (Nabers or Cattoni probes, Hu-Friedy Co., Chicago, IL, USA). The furcation defect in Fig. 4-13, A was suspected to be the result of inad-equate root canal treatment of the mesial buccal root. Peri-odontal probings indicated there were deep vertical and horizontal components to the defect. Surgical exploration showed the extent of the bone loss (see Fig. 4-13, B). The entire furcation was devoid of bone in addition to loss of the buccal plate covering the buccal roots, which accounted for the preoperative probing patterns. The diagnosis of advanced periodontitis was confirmed, and the tooth was extracted.
Lesions Associated With Aggressive Forms of PeriodontitisAggressive periodontitis in young people, once known as juvenile periodontitis, affects less than 1% of the population.4 This disease process is now associated with a specific patho-gen, Aggregatibacter actinomycetemcomitans (formerly Actino-bacillus).24 This pathogen has also been found to be dominant in some global environments,19 and therefore may be used as a specific diagnostic marker for the disease. However, studies have also indicated that other global populations may have different markers, such as Treponema lecithinolyticum40 or inflammatory cells and serum globulins that may be associ-ated with the degree of periodontal destruction.47

78 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A
B
FIGURE 4-14 a, Deep periodontal defect discovered on a 12-year-old patient. B, Radiograph of same lesion. Diagnosis is aggressive periodontitis.
CLINICAL PROBLEMProblem: A 64-year-old male was referred for evaluation of the maxillary left central incisor. His chief complaint was recurrent swelling and drainage in the roof of his mouth adja-cent to the tooth. The periapical film showed previous root canal treatment and a periapical lesion (Fig. 4-16, A). The patient related that the treatment was done at least 35 years ago. A small radiolucency was also apparent in the coronal half of the root. Clinical examination confirmed tenderness to pal-pation in the midapical region on the facial aspect of the tooth. Circumferential probing indicated no bony defects, but a subgingival defect on the mesial palatal aspect of the root was identified.
Solution: Treatment options included periradicular surgery (see Chapter 18) with repair of the resorption defect or extrac-tion. Removal of the sectional silver cone in the root canal was judged to be impossible. In evaluating the tooth for surgery, the size of the silver cone suggested that apical removal would also be impossible without severe reduction in the length of the root. At the same time, preparation of the resected root apex for a root-end filling would also be difficult with the silver cone in place. The lingual angulation of the long axis of the tooth placed the resorption defect in a very difficult location for repair. Extraction was elected as the treatment of choice (see Fig. 4-16, B).
A
B
FIGURE 4-13 a, Furcation lesion in bone, suspected to be the result of extension of pulp pathosis into periodontium. B, Surgical exposure confirms the diagnosis of chronic periodontitis.
Owing to the diagnostic confusion with an acute periapi-cal abscess and the rarity of periodontal pathosis in children, a necrotic pulp with a periapical lesion is sometimes sus-pected as the cause of this disease. The case depicted in Fig. 4-14 illustrates a bony lesion in a 12-year-old female who was referred for root canal treatment of the maxillary right first molar. After confirming the presence of a normal pulp with sensibility tests, the patient was referred for a periodontal consultation.
External Root ResorptionExternal root resorption that occurs in the marginal peri-odontium is often confused with internal resorption of the root. Internal resorption is a pathologic process of pulpal origin.22,44,58,61 External resorption infrequently involves pulp.22 Root canal treatment may or may not affect this problem but is often necessary because of pulp exposure or near exposure during repair of the defect (Fig. 4-15).22 A more detailed discussion of resorption is found in Chapters 3, 13, 18, and 19.
Cemental TearsA cemental tear is a rare periodontal condition often associ-ated with a root-treated tooth.57,59 This condition appears

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 79
A B
C
FIGURE 4-15 a, Lesion of external resorption in marginal periodontium, resembling internal resorption. B, Probings suggest a periodontal defect. C, Surgical exposure confirms diagnosis of external resorption that arises in the periodontium.
A B
FIGURE 4-16 a, Maxillary left central incisor with recurrent periapical pathosis and a palatal draining tract. B, Following extraction, external resorption lesion is seen on the palatal surface.

80 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
Pulpally Induced Lesions that Can Be Confused With Periodontal Lesions
There are also periapical lesions of pulpal origin that share clinical and radiographic features with lesions of periodontal origin. Most periapical lesions arise in the bone adjacent to the apical foramen, and there is usually no radiographic con-fusion with lesions of periodontitis (Fig. 4-18). Diagnosis on the basis of radiographic findings alone can be misleading, however, if a periapical lesion or evidence of a sinus tract should extend to the alveolar crest (Fig. 4-19; see Chapters 2 and 3).
Furcation or Lateral Lesions Without Loss of AttachmentPeriapical (periradicular) lesions can become quite large and approach crestal bone. Radiographically, the appearance is similar to periodontal lesions with advanced bone loss, par-ticularly because of the loss of crestal or furcation bone (Fig. 4-20, A). Careful circumferential probing will often indicate that there is no loss of attachment in the sulcus. Clearly, a normal probing pattern rules out a periodontal etiology for the lesion. Root canal treatment alone is usually effective to bring about resolution of the radiolucency (see Fig. 4-20, B).
CLINICAL PROBLEMProblem: Root canal treatment was completed on a man-dibular right lateral incisor for an 85-year-old male. There was no indication of periodontal pathosis at the time of treatment. The patient was seen 18 months later for evaluation of a local swelling associated with the same tooth. Periodontal probings revealed a 7-mm localized periodontal defect on the distal aspect of the tooth; all other probing depths were within normal limits. The presumptive diagnosis was a recurrent periapical lesion due to inadequate root canal treatment or a vertical root fracture. A periapical radiograph showed a radio-lucency on the distal aspect of the root, extending from the apex to crestal bone level (Fig. 4-17, A).
Solution: Exploratory surgery revealed a cemental tear on the labial surface of the root (see Fig. 4-17, B). Fragments of separated cementum were found attached to the elevated tissue and removed. The area of cemental separation was lightly recontoured with a composite finishing bur to remove the irregular margins of the tear, and the root surface was treated with citric acid for 30 seconds to enhance reattachment of the periodontal ligament fibers. After rinsing, the tissue was repositioned and sutured. Reevaluation at 6 months (see Fig. 4-17, C) indicated that probing depth had returned to normal.
clinically as a periodontal infection with rapid loss of attach-ment. Although the etiology is unknown, there is a higher incidence in the elderly.59 At time of surgery, small segments of the cementum are often observed to have fractured away from the surface of the root. The literature has a number of case reports with some success in treatment outcomes, but
A
B
C
FIGURE 4-17 a, Radiograph of a mandibular right lateral incisor 1 12 years after root canal treatment. Clinically there was local swelling and a periodontal defect in this location. Preoperatively, there had been no evidence of periodontal pathosis. B, Surgical exposure of defect, revealing cemental tear. Note margins of cemental defect on root surface. C, Six months post treatment, indicating normal probings.
the level of evidence for the best way to manage these cases is less than ideal.57,59

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 81
FIGURE 4-18 Typical periapical lesion of pulpal etiology. FIGURE 4-19 Typical periapical lesion of pulpal etiology with a draining sinus tract along the distal root surface. There was no periodontal disease.
A B
FIGURE 4-20 a, Mandibular right first molar with large radiolucent lesion. Bone loss appears to extend from distal interproximal crest to apex, but clinically there was no break in the sulcular attachment. B, Reevaluation at 15 months, indicating healing of periapical lesion and restoration of interproximal bony architecture.
A B
FIGURE 4-21 a, Mandibular left first molar with radiographic evidence of furcation and lateral bone loss. There were two draining tracts in the attached gingiva but probings were normal. B, One year reevaluation, indicating complete healing.
Some teeth with periodontal attachment and bone loss will develop large periapical lesions that may appear radio-graphically to merge with the periodontal bone loss (Fig. 4-21, A). These lesions have been identified by many as perio-endo lesions.6,48,63 Once again, however, periodontal
probing is the key to diagnosis. In this case, there is definite loss of bone from periodontitis. Nevertheless, cir-cumferential probings identified a normal sulcus depth in the interproximal space, with no break in the attachment. This cannot be a so-called perio-endo lesion in the absence of the

82 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A
B
FIGURE 4-22 a, Local swelling secondary to acute periapical abscess. A narrow defect into the furcation was probed. B, One week following routine endodontic emergency procedures, swelling had subsided, and reattachment in the furcation had occurred.
periodontal disease component communicating with a lesion of pulpal origin. Root canal treatment was completed and a 1-year reexamination demonstrates healing of the interproxi-mal crest of bone as well as the periapical lesion itself (see Fig. 4-21, B).
Acute Periapical AbscessSome acute periapical abscesses of pulpal origin will cause localized swelling of the marginal gingiva (Fig. 4-22, A). Additionally, probings may reveal a break in the attachment, and it is not unusual to observe purulent drainage around the probe tip during oral examination. Probings will also quickly rule out a periodontal etiology if no other defects are found. Routine endodontic examination should include sen-sibility tests. In the case of acutely abscessed teeth, the pulp is invariably necrotic, as was explained in Chapter 1. A radio-graph most often will indicate the presence of a periapical radiolucency. Once the diagnosis is established, the tooth is customarily opened for root canal treatment (see Chapter 15), although in some cases an incision and drainage may also be indicated. The most important difference between acute periapical and periodontal abscesses is that attachment loss in the endodontic cases will be recovered, often within 1 week (see Fig. 4-22, B). Probings will return to normal in
the affected site once the infection heals and the drainage ceases. There are rarely any residual defects.
Chronic Sinus Tracts of Pulpal Origin With Drainage Through the Gingival SulcusSeldom are sinus tracts of pulpal origin mistaken for peri-odontal lesions when they appear on the surface of the mucosa.27,28 Confusion arises most often when the tract exits through the gingival sulcus. Fig. 4-23, A illustrates a maxil-lary left first molar with an acute swelling on the mesial palatal surface. Probings identified a possible periodontal eti-ology, and the patient was referred to a periodontist for
A
B
C
FIGURE 4-23 a, Local swelling on mesial palatal surface of maxillary left first molar, which was presumed to be periodontal. B, Sectioned periodontal probe in the defect. C, Surgical exposure confirms diagnosis of a sinus tract of pulpal origin.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 83
CLINICAL PROBLEMProblem: An 18-year-old female college student presented for evaluation of the maxillary right molar area. She related a history of recurrent soreness, local swelling, and a foul taste in the area between the first and second molars. Her family dentist had placed a large temporary restoration in the second molar just before she left for school (Fig. 4-24, A). Probings in the area identified a narrow sinus tract–type probing inter-proximally on the palatal side. A periapical film with a peri-odontal probe in the tract indicated the source of the drainage was a large periradicular lesion encompassing the apices of both the first and second molars (see Fig. 4-24, B). Sensibility testing showed that the pulp in the second molar was necrotic, but the first molar responded normally.
Solution: Evaluation of the periodontal status revealed a normal, healthy periodontium throughout the dentition. This was consistent with the crestal bone levels on the periapical film. Furthermore, osseous defects of advanced periodontitis would be extremely rare in an 18-year-old individual, so a periodontal etiology was ruled out. The periapical lesion was large and draining through the gingival sulcus. Root canal treatment of the second molar resulted in closure of the sinus tract in 2 weeks.
Chronic Sinus Tracts of Pulpal Origin with Permanent Periodontal Attachment LossSome periapical lesions that drain through the sulcus can become periodontal lesions as well. In addition to bacteria, biofilm and calculus can form on the root surfaces,1 within sinus tracts, and even on the apices of roots in chronically draining periapical lesions (Fig. 4-25). Fig. 4-26 illustrates the case of a 24-year-old male with no clinical signs of periodontal pathosis. His chief complaint was a local swell-ing on the vestibular side of the mandibular right first molar
evaluation. Probings were essentially normal except for a narrow tract in the area of the swelling. The periodontist did a sinus tract exploration using a sectioned periodontal probe (see Fig. 4-23, B). The tissue was reflected in the area, and a sinus tract was observed to be a small defect without a change in the general contour of the bone (see Fig. 4-23, C ). This image illustrates the bone contours that characterize a “sinus tract–type probing” pattern.27,28 The probing depths along root surfaces with these defects are usually within normal limits until the defect is encountered. The probing depth at this point will precipitously become very deep as the probe enters the tract. Continuing circumferentially, the probing depth will just as precipitously return to normal. Root canal treatment of the molar was subsequently completed and the sinus tract healed uneventfully.
A
B
FIGURE 4-24 a, Maxillary right molar area with a history of symptoms. Probing indicates a narrow sinus tract on the distal-palatal surface. The sulcus depth was normal in all other areas. B, Radiograph indicating probe extending to the large periapical lesion through a sulcular drainage tract.
FIGURE 4-25 Calculus on apex of a root with history of chronic drainage from a periapical lesion of pulpal origin.

84 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A B
FIGURE 4-26 a, Radiograph indicating furcation bone loss. Normal bone levels around adjacent teeth. There was no evidence of chronic periodontitis. B, Probing indicating horizontal bone loss. Even though the defect is due to chronic drainage from a periapical lesion of pulpal origin, the prognosis for healing in the furcation is guarded.
that had been present for several months. The periapical radiograph showed no evidence of infrabony defects from periodontitis, but a large periapical radiolucency was present on the first molar and extended into the furcation (see Fig. 4-26, A). Clinically, probings confirmed both vertical and horizontal bone loss in the furcation (see Fig. 4-26, B). The outcome of root canal treatment in these cases is uncertain. Many cases will regain attachment after débridement of the root canal, but some will not. See Chapter 1, Fig. 1-13 for review of a case that healed satisfactorily in less than 1 month.
If reattachment has not occurred approximately 1 month after treatment, it is not likely to occur at all. The prog-nosis for such a tooth is poor, so complete root canal treatment is not advisable until a prognosis has been estab-lished. The treatment of choice would be access to the chamber, canal débridement, and closure with calcium
CLINICAL PROBLEMProblem: A 70-year-old male was seen for a chief complaint of recurrent swelling and drainage on the buccal of the man-dibular left lateral incisor The periapical film made at the examination showed a periapical radiolucency on the apex of the lateral incisor (Fig. 4-27, A). Sensibility tests indicated a nonvital lateral incisor. Periodontal probings indicated that there was a narrow drainage tract on the labial surface of the root (see Fig. 4-27, B). Root canal treatment was started and the canal was sealed with calcium hydroxide. One month later, the tooth was reevaluated. The patient felt better and was optimistic about retaining the tooth. The tissue color had improved, but probings revealed no change in the sinus tract.
Solution: The chance for reattachment after 1 month in treatment is very poor. The prognosis was hopeless, so the tooth was recommended for extraction.
hydroxide.34,38,51 Some authors and investigators would rec-ommend using a combination of 2% chlorhexidine along with the calcium hydroxide for better bacterial control.5 The completion of root canal procedures would be indicated as soon as reattachment is observed, which can occur in as few as 10 days.
Response of the Periodontium to Mechanical Root PerforationsMechanical perforations into the periodontium that may occur during root canal procedures result in one of two types of periodontal lesions. Those found below the level of the attachment have characteristics similar to radicular abscesses that occur adjacent to a lateral canal in the presence of necrotic pulp abscesses. Those that occur in the marginal periodontium have characteristics of periodontal pockets. The prognosis of treatment for each is comparable; lesions have a much better prognosis for complete healing if the attachment is not involved.2 As a general rule, if a perforation occurs during root canal procedures, immediate repair is very important to prevent contamination of the periradicular tissues by bacteria or materials/solutions used in root canal treatment.3 Many materials have been used for sealing a perforation, with mineral trioxide aggregate (MTA) the most contemporary and possibly the most favorable for healing.13,41 Zinc oxide eugenol has also been used with some degree of success, but materials will be of no value if the site becomes infected.
The case presented in Fig. 4-28 illustrates that if the peri-odontal attachment is normal preoperatively, attachment will most likely return following surgical repair. During surgery, the attachment area of the root surface should not be curet-ted. This case also illustrates the general observation that small perforations have a better outcome than large ones. Location is also important in assessing prognosis. Lateral perforations on broad accessible root surfaces have a better

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 85
CLINICAL PROBLEMProblem: A 40-year-old female requested endodontic con-sultation for a local swelling in the gingiva over the maxillary right canine (Fig. 4-28, A). She related a history of a recent emergency visit to a dentist while on vacation in a distant city. The tooth felt better after the emergency treatment, but upon returning from the trip, the labial gingiva over the tooth became very sore to touch. In the last 3 days, the swelling appeared. Clinical examination confirmed that an endodontic access was made on the palatal aspect of the crown and was sealed with a temporary restoration. A periapical film showed a very generous access cavity. Periodontal probing depths were normal, so a diagnosis of perforation during access to the root canal was considered the most likely problem.
Solution: The mucoperiosteal tissues were elevated, and a small perforation was located. Without enlarging the orifice of the perforation, the defect was cleaned with an ultrasonic endodontic file and sealed with MTA (see Fig. 4-28, B). The elevated tissue was repositioned and stabilized with a sling suture. The root canal treatment was completed (see Fig. 4-28, C), and a photograph was made at an 8-month (see Fig. 4-28, D) reexamination appointment, at which time peri-odontal probings were normal.
CLINICAL PROBLEMProblem: A 70-year-old male was examined for a complaint of chronic soreness in the facial gingiva of the maxillary left lateral incisor. The periapical image confirmed that a perforation during post space preparation had occurred (Fig. 4-34).
Solution: The mucoperiosteal tissues were elevated over the area, revealing a large perforation and severe localized interproximal bone loss. The perforation was repaired, and the tissue was positioned apically to eliminate the pocket as much as possible. The patient was advised that the area is likely to heal with a large space between the incisors due to lack of crestal bone support for the papilla.
A B
FIGURE 4-27 a, Periapical lesion of pulpal etiology. Pulp tests indicated pulpal necrosis. B, Probings confirm chronic draining tract through gingival sulcus. Root canal débridement was performed and the tooth closed with calcium hydroxide for monitoring. One month later, probings were unchanged. If healing has not occurred in this time interval, it is unlikely to occur at all. Extraction was recomended.
prognosis for healing after repair than those on inaccessible surfaces or in the furcations (Fig. 4-29).
Perforations can occur below the periodontal attachment. Strip-type perforations may occur during intracanal cleaning and shaping and during post space preparation (Figs. 4-30 and 4-31). Especially with misdirected post preparations,
severe defects in both tooth and bone can occur (Fig. 4-32). These types of perforations are very difficult to manage suc-cessfully because of inaccessibility and the presence of metal in the perforation defect. If repair is attempted, it is usually best if the post can be removed first to avoid the necessity of trying to cut back the metal during surgery in preparation for the repair material.
Perforations into the periodontal attachment are disas-trous events which cause irreversible damage to the crestal bone (Fig. 4-33). Regardless of the repair material, recovery of a more coronal attachment level is highly unlikely. In this sense, the lesion must be treatment planned for pocket elimi-nation or extraction. Aesthetics will also be a major factor in the anterior teeth.

86 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
FIGURE 4-29 Perforation during access cavity preparation into the furcation with associated periodontal breakdown.
FIGURE 4-30 Strip perforation in the course of canal shaping.
A
C
B
D
FIGURE 4-28 a, Localized swelling in attached gingiva over maxillary right canine which had been opened for endodontic treatment one month earlier. B, Surgical exposure of perforation. Note interruption of crestal bone, yet preoperative probings were normal. Surgical repair was completed with mineral trioxide aggregate (MTA without enlargement of perforation defect). C, Root canal treatment completed after surgical repair. D, Eight-month reexamination, indicating complete healing.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 87
FIGURE 4-32 Misdirected post preparation resulting in extension of post into lateral periodontium.
FIGURE 4-31 Strip perforation resulting from intraradicular post placement.
FIGURE 4-33 Access perforation into marginal periodontium. Without realizing the error, the clinician completed root canal treatment; result was acute periodontal abscess. Remedial root canal and periodontal treatment failed to improve severe periodontal defect, and tooth was extracted.
Bony Lesions of the Peridontium that Do Not Originate from Either Periodontal or Pulpal Pathosis
The following lesions have similarities to pulpal and peri-odontal lesions described in the two previous sections but have entirely unrelated etiologies.
Deep Coronal FracturesThe subject of coronal fractures is discussed as an etiology of pulpal pathosis in Chapter 1. Most coronal fractures in teeth with pulpal symptoms are found to extend to the level of the pulp chamber and no farther. Root canal treatment followed by full coronal coverage provides an excellent long-term prognosis, the latter treatment depending on the age of the patient.
Unfortunately at present, technology does not exist to measure the depth of a coronal fracture preoperatively. Since most fractures develop in a mesial-distal plane, they are not evident on two-dimensional radiographs. Cone-beam com-puted tomography (CBCT) may serve as an excellent tool in these situations (see Chapter 3). Clinically, fractures can usually be confirmed by visual examination (Fig. 4-35) and transillumination (Fig. 4-36), but the depth and direction cannot be determined with any reliability. If the fracture is
FIGURE 4-34 Radiograph of lateral perforation into marginal periodontium post space preparation. The post was not protruding through the perforation defect. Surgical repair of perforation defect was possible but periodontal defect was irreparable.

88 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
FIGURE 4-36 Transillumination of fractured tooth. The transmission of light stops at the fracture line.
FIGURE 4-35 Clinical examination of fracture line with an explorer.
A
B
C
FIGURE 4-37 a, Oblique coronal fracture of maxillary left canine. B, Fractured crown showing angle and extent of fracture. C, Following crown lengthening, tooth is again restorable.
relatively new and deep enough to extend into the periodon-tal attachment, there may be slight to no initial changes in the probing depth. One useful early indication is increased tenderness to probing in the location of the fracture com-pared to other areas around the tooth.
In some cases, coronal fractures are often deep enough to result in mobility of the coronal segments. Mobility is a good clue to the severity of depth and also the likely direction of the fracture line. If a fractured cusp is highly mobile while the remainder of the tooth is firm, the fracture is likely to be oblique with respect to the long axis of the tooth and not extend very far below the free gingival margin. These frac-tured segments are held only by gingival attachment. Crown lengthening can often make such teeth restorable (Fig. 4-37; see Chapter 17).
A fractured molar is seen in Fig. 4-38. Separation in the fracture line is possible with an instrument, but neither segment is very mobile. This is a grave sign in terms of prog-nosis. The fracture most likely extends deep and parallel to
the long axis of the tooth. Severe periodontal destruction is inevitable along the fracture lines. Fig. 4-39 illustrates a case of a tooth with a deep cuspal fracture that presents as an acute periodontal abscess. The swelling on the buccal is an exten-sion of the infection that originated in the periodontium along the fracture line.
Periodontal complications can present a serious diagnostic dilemma with recent fractures, because signs and symptoms of periodontal involvement are often lacking. As a conse-quence, some teeth are restored but later develop the peri-odontal sequelae, and extraction is the unfortunate outcome.
Deep coronal fractures in maxillary molars may follow a different course and extend into the furcation. Clinical exam-ination will usually identify the fracture, but there are seldom any significant radiographic changes. The effect is to divide

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 89
FIGURE 4-38 Mandibular left first molar with deep, unrestorable coronal fracture. Both coronal halves exhibit only slight mobility.
A
B
C
FIGURE 4-39 a, Mandibular right first molar presenting with acute periodontal abscess. B, Occlusal view. Note fracture lines on distal and lingual. C, Fracture of distal-lingual cusp was quite mobile, indicating that fracture may not be very deep.
CLINICAL PROBLEMProblem: A 50-year-old male complained of acute cold sensi-tivity in the maxillary right premolar area. He could not chew comfortably, and clinical examination revealed a mesial-distal fracture line through the crown of the second premolar. There was no mobility of either half of the crown. Sensibility tests con-firmed the presence of an irreversible pulpitis. Root canal treat-ment was completed, followed by placement of a full crown.
Five months later, the patient returned with the complaint of drainage around the tooth and occasional episodes of swell-ing in the area. Clinical examination showed draining tracts on both vestibular and palatal surfaces but probings on these surfaces were normal. Interproximal probings, however, iden-tified deep narrow defects on both the mesial and the distal surfaces (Fig. 4-40, A), The periapical radiograph confirmed deep periodontal defects interproximally (see Fig 4-40, B).
Solution: The diagnosis of deep coronal fracture was made, and the tooth was extracted. Postoperative examination con-firmed the presence of fracture lines on both mesial and distal surfaces (see Fig. 4-40, C and D). These locations were consis-tent with a coronal fracture rather than a vertical root fracture (discussed in the following section). A possible treatment plan for coronal fractures without periodontal signs of deep exten-sion would be placement of circumferential protection (e.g., an orthodontic band), removal of occlusal contact, and observ-ing for 1 to 2 months. If no signs of periodontal destruction appear, the tooth could be assumed to be restorable. When multiple sinus tracts are present on an individual tooth, there is a high likelihood of the tooth being fractured, whether a deep coronal fracture or a vertical root fracture.52, As this case illustrates, placement of a full crown over a tooth with a deep coronal fracture will not prevent periodontal deterioration and eventual extraction.
the tooth in half buccal-lingually (Fig. 4-41). The patient will typically present with an acute abscess in the furcation that will probe normally on the buccal and palatal surfaces. Inter-proximal probings will reveal a loss of attachment and bone in the furcation.
Vertical Root FracturesA vertical fracture of the root is a much different entity than vertical fracture of the crown, though the etiology of both may be the same.7,8,17 Generally, vertical root fractures tend to develop from the apex and extend coronally (Fig. 4-42). The clinical presentation is a sinus tract–type periodontal probing pattern that surfaces in the specific areas where the fractures occur, namely the midbuccal or midlingual/palatal

90 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A B
FIGURE 4-41 a, Clinical view of maxillary right second molar with obvious mesial-distal fracture. B, Extracted tooth, demonstrating that fracture extended directly into furcation and divided tooth in half.
A B
DC
FIGURE 4-40 a, Probing on the mesial demonstrates deep, narrow defect, indicating periodontal defect. Distal has similar defect but probings on the buccal and palatal surfaces were normal. B, Radiograph indicating periodontal bone loss on mesial and distal surfaces, extending to midroot level. C, Mesial view of extracted tooth, showing fracture line extending from crown to midroot level. D, Distal view of tooth, showing fracture line to same level.

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 91
CLINICAL PROBLEMProblem: A 72-year-old male presented with low-grade discomfort in a mandibular central incisor. The discomfort had been vague for 2 or 3 months but now was more focused on this particular tooth. He reports having seen pus coming from around the tooth when he pushed on the gum tissue. Clinical examination revealed a small sinus tract at the muco-gingival junction overlying the severely worn mandibular right central incisor. The tooth was slightly tender to percussion and definitely tender to palpation. A radiograph revealed a previously root-treated tooth with a large radiolucency (Fig. 4-45, A). Two canals were obturated in the tooth, and the quality of the root canal treatment appeared adequate. The initial impression gave a tentative diagnosis of endodontic failure.
Solution: A tentative diagnosis of subacute suppurative periapical periodontitis was appropriate, since the tooth had an apical lesion following root canal treatment, and purulence was present. Incremental circumferential probing was per-formed and normal sulcus depths found on the mesial and distal line angles (see Fig. 4-45, B and C). Probing between these points indicated a deep, narrow sinus tract–type defect that was pathognomonic of a vertical fracture (see Fig. 4-45, D), and extraction was the treatment of choice. This case emphasizes the use of probing to assess teeth that appear to have failed root canal treatment.
FIGURE 4-42 Surgical exposure of typical vertical root fracture.
FIGURE 4-44 Unusual vertical root fracture on endodontically untreated tooth.
FIGURE 4-43 Vertical root fractures can be caused by excessive spreader pressures during lateral compaction. Extrusion of sealer and gutta-percha document that this occurred during this procedure.
surfaces of teeth or individual roots. Signs and symptoms include percussion tenderness and local palpation tenderness or swelling of the overlying soft tissues similar to a periodon-tal abscess.17 In contrast to deep coronal fractures, vertical root fractures tend to occur in the buccal-lingual plane.17 Most are found to involve only one surface of the root, but if the fracture extends completely through the root, fracture lines will be found on both buccal and lingual. When this occurs, two sinus tracts may be noted.56
Fractures of this type can be induced by excessive pressures with a spreader during lateral compaction of gutta-percha (Fig. 4-43; see Chapter 12).26 However, with present-day shaping techniques that have better divergent canal prepara-tions, this occurrence is minimal.
The etiology of the majority of vertical root fractures is not well understood, but two of the most common denomi-nators seem apparent: previous root canal treatment and evidence of heavy occlusal forces. Except for a reported high incidence of vertical root fractures in untreated teeth found
It is uncommon for vertical root fractures to be visible on radiographs. Many fractured roots have no radiographic signs of pathosis at all (Fig. 4-46). This is not surprising, consider-ing the minimal osseous breakdown of a narrow drainage tract as compared to a typical periodontal defect. Since most fractures occur on the buccal or lingual surfaces, bone loss would also be obscured by the root itself. Infrequently, the fractured segments may separate, and the fracture may become radiographically apparent (Fig. 4-47).
in a study of Chinese teeth,14 the occurrence of such fractures generally is rare (Fig. 4-44).7

92 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
A B
C D
FIGURE 4-45 a, Radiograph indicating previous root canal treatment and periapical lesion on a mandibular central incisor. B, Normal probing depth on mesial-labial line angle. C, Normal probing on distal-labial line angle. D, Sinus tract–type probing diagnostic for vertical root fracture in this location.
As described in the preceding chapter, the most common diagnostic radiographic finding is a widened periodontal ligament space extending from the apex of the fractured root to crestal bone (Fig. 4-48, A).17 The dimension or actual radiographic width may vary and it may be observed on one proximal surface or both (see Fig. 4-48, B ). Chronic lesions in the periodontium from root fractures can reach significant dimensions and resemble primary periodontal lesions (Fig. 4-49). The diagnostic distinctions will be in the results of probings. Periodontal lesions will tend to probe deeply with a wide base in a circumferential pattern, whereas bone loss associated with vertical fractures will probe deeply on buccal and/or lingual surfaces only. Unfor-tunately, there is no remedy for a vertical root fracture. On single-rooted teeth, extraction is indicated. On mul-tirooted teeth, root resection (amputation) is a possibility (see Chapter 18).
Developmental Lingual Groove on Maxillary Lateral Incisors and Similar LesionsThe maxillary lateral incisor will occasionally develop with a groove on the lingual surface of the root.32,33 Although the periodontal status may remain normal for many years, the groove appears susceptible to periodontal breakdown.29 Patients eventually experience signs and symptoms of either acute or chronic periodontal abscess (Fig. 4-50, A), and the defect probes much like a sinus tract (see Fig. 4-50, B). The periapical film in this case demonstrates the groove (see Fig. 4-50, C and D). There is no treatment; extraction is indicated.
The same phenomenon can occur on molars with fused roots.16,55 The most typical presentation is on the buccal surface of mandibular second molars, but the phenomenon

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 93
A
B
C
FIGURE 4-46 a, Fracture of mesial buccal root without typical radiographic signs of pathosis. B, Probings reveal fracture defect. C, Surgical exposure of defect.
FIGURE 4-47 Vertical fracture line at apex of maxillary canine. Visible fractures on radiographs are unusual.
is possible on any multirooted tooth with this anatomic varia-tion. Fusion of the roots sometimes creates a groove similar to the lingual developmental groove of the lateral incisor.16 Once again, a deep, narrow periodontal defect will be found on the midbuccal surface. Most teeth with these defects will respond normally to pulp tests. Prognosis is poor and depen-dent on the success of any possible periodontal treatment. When these fusions occur in mandibular molars or premo-lars, usually a C-shaped canal is present internally.16,55
Other Possible Rare LesionsAfter traumatic injury, some maxillary incisors will be found to have a deep probing defect in the palatal sulcus. This is
A
B
FIGURE 4-48 a, A widened periodontal ligament space identifying vertical root fracture. In this case the radiographic sign may be slight but extends the full length of the root. B, Widened periodontal ligament space occasionally seen on both sides of root.

94 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
FIGURE 4-49 Mandibular left molar with severe bone loss related to longstanding vertical root fracture.
A B
C D
FIGURE 4-50 a, Sinus tract on labial surface of maxillary lateral incisor. B, Circumferential probings are normal except in the location of the lingual developmental groove. C, Groove evident on radiographic image of tooth. D, Lingual groove demonstrated on an extracted tooth (arrows).

chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects 95
the direct result of luxation and will generally close spontane-ously without treatment.
Periodontal defects associated with enamel pearls are gen-erally found in the furcation areas of molars. Rarely they will cause periodontal breakdown but could present as an acute abscess. Probings are similar to periodontal pockets. Once again, prognosis for the tooth will depend on the possibility of periodontal treatment.
REFEREnCES1. Adriaens PA, De Boever JA, Loesche WJ: Bacterial invasion in root
cementum and radicular dentin of periodontally diseased teeth in humans. A reservoir of periodontopathogenic bacteria, J Periodon-tol 59:222-230, 1988.
2. Albaricci MF, de Toldeo BE, Zuza EP, et al: Prevalence and features of palate-radicular grooves: an in vitro study, J Int Acad Periodon-tol 10:2-5, 2008.
3. Alhadainy HA: Root perforations. A review of the literature, Oral Surg Oral Med Oral Pathol 78:368-374, 1994.
4. Axelsson P: Diagnosis and risk prediction of periodontal diseases, Chicago, 2002, Quintessence Pub Co.
5. Basrani B, Ghanem A, Tjäderhane L: Physical and chemical prop-erties of chlorhexidine and calcium hydroxide-containing medica-tions, J Endod 30:413-417, 2004.
6. Belk CE, Gutmann JL: Perspectives, controversies and directives on pulpal-periodontal relationships, Can Dent J Assoc 56:1013-1017, 1990.
7. Bender IB, Freedland JB: Adult root fracture, J Am Dent Assoc 107:413-419, 1983.
8. Bender IB, Freedland JB: Clinical considerations in the diagnosis and treatment of intra-alveolar root fractures, J Am Dent Assoc 107:595-600, 1983.
9. Bender IB, Seltzer S: The effect of periodontal disease on the pulp, Oral Surg Oral Med Oral Pathol 33:458-474, 1972.
10. Black GV: Amputation of the roots of teeth. In Litch WF, editor: The American system of dentistry, Philadelphia, 1886, Lea Brothers.
11. Burch JG, Hulen S: A study of the presence of accessory foramina and the topography of molar furcations, Oral Surg Oral Med Oral Pathol 38:451-455, 1974.
12. Cahn LR: The pathology of pulps found in pyorrhetic teeth, Dent Item Int 49:598-617, 1927.
13. Casella G, Ferlito S: The use of mineral trioxide in endodontics, Minerva Stomatol 55(3):123-143, 2006.
14. Chan CP, Tseng SC, Lin CP, et al: Vertical root fractures in non-endodontically treated teeth—a clinical report of 64 cases in Chinese patients, J Endod 24:678-681, 1998.
15. Chen S-Y, Wang H-L, Glickman GN: The influence of endodontic treatment on periodontal wound healing, J Clin Periodontol 24:449-456, 1997.
16. Cleghorn BM, Christie WH, Dong CC: Root and root canal morphology of the human permanent maxillary first molar: a lit-erature review, J Endod 32:813-821, 2006.
17. Cohen S, Blanco L, Berman L: Vertical root fractures: clinical and radiographic diagnosis, J Am Dent Assoc 134:434-441, 2003.
18. Coolidge ED: Anatomy of the root apex in relation to treatment problems, J Am Dent Assoc 16:1456-1465, 1929.
19. Cortelli JR, Cortelli SC, Jordan S, et al: Prevalence of periodontal pathogens in Brazilians with aggressive or chronic periodontitis, J Clin Periodontol 32:860-866, 2005.
20. Cutright DE, Bhaskar SN: Pulpal vasculature as demonstrated by a new method, Oral Surg Oral Med Oral Pathol 27:678-683, 1969.
21. Czarnecki RT, Schilder H: A histological evaluation of the human pulp in teeth with varying degrees of periodontal disease, J Endod 5:242-253, 1979.
22. Fuss Z, Tsesis I, Lin S: Root resorption—diagnosis, classification and treatment choices based on stimulation factors, Dent Trauma-tol 19:175-182, 2003.
23. Gargiulo AW, Wentz FM, Orban B: Dimensions and relations of the dentinogingival junction in humans, J Periodontol 32:261-267, 1961.
24. Guentsch A, Puklo M, Preshaw PM, et al: Neutrophils in chronic and aggressive periodontitis in interaction with Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans, J Periodontol Res 44:368-377, 2009.
25. Gutmann JL: Prevalence, location, and patency of accessory canals in the furcation region of permanent molars, J Periodontol 49:21-26, 1978.
26. Gutmann JL, Dumsha TC, Lovdahl PE: Problem solving in end-odontics, ed 4, St Louis, 2006, Mosby Elsevier.
27. Harrington GW: The perio-endo question: differential diagnosis, Dent Clin North Am 23:673-690, 1979.
28. Harrington GW, Steiner DR, Ammons WF, Jr: The periodontal-endodontic controversy, Periodontol 2000 30:123-130, 2002.
29. Hou GL, Tsai CC: Relationship between palate-radicular grooves and localized periodontitis, J Clin Periodontol 20:678-682, 1993.
30. Kahn S, Cabanilla LL: Periodontal probing depth measurement: a review, Compend Contin Educ Dent 30:12-21, 2009.
31. Kramer IHR: The vascular architecture of the human dental pulp, Arch Oral Biol 2:177-189, 1960.
32. Langeland K, Rodrigues H, Dowden W: Periodontal disease, bac-teria, and pulpal histopathology, Oral Surg Oral Med Oral Pathol 37:257-270, 1974.
33. Lara VS, Consolaro A, Bruce RS: Macroscopic and microscopic analysis of the palate-gingival groove, J Endod 26:345-350, 2000.
34. Law A, Messer H: An evidence-based analysis of the antibacterial effectiveness of intracanal medicaments, J Endod 30:689-694, 2004.
35. Lindhe J, Lang NP, Karring T: Clinical periodontology and implant dentistry, ed 5, Oxford, 2008, Blackwell Munksgaard.
36. Lowman JV, Burke RS, Pelleu GB: Patent accessory canals: inci-dence in molar furcation region, Oral Surg Oral Med Oral Pathol 36:580-584, 1973.
37. Mazur B, Massler M: Influence of periodontal disease on the dental pulp, Oral Surg Oral Med Oral Pathol 17:592-603, 1964.
38. Peters LB, et al: Effects of instrumentation, irrigation and dressing with calcium hydroxide on infection in pulpless teeth with perira-dicular bone lesions, Int Endod J 35:13-21, 2002.
39. Pitiphat W, Crohin C, Williams P, et al: Use of preexisting radio-graphs for assessing periodontal disease in epidemiologic studies, J Public Health Dent 64:223-230, 2004.
40. Riep B, Edesi-Neuss L, Claessen F, et al: Are putative periodontal pathogens reliable diagnostic markers? J Clin Microbiol 47:1705-1711, 2009.
41. Roberts HW, Toth JM, Berzins DW, et al: Mineral trioxide aggre-gate use in endodontic treatment: a review of the literature, Dent Mater 24(2):149-164, 2008.
42. Rotstein I, Simon JH: The endo-perio lesion: a critical appraisal of the disease condition, Endod Topics 13:34-56, 2006.
43. Rubach WC, Mitchell DF: Periodontal disease, accessory canals, and pulp pathosis, J Periodontol 36:34-38, 1965.
44. Seltzer S, Bender IB: The dental pulp, ed 3, Philadelphia, 1984, JB Lippincott.

96 chapter 4 | Problem Solving in the Differential Diagnosis of Bony Defects
45. Seltzer S, Bender IB, Nazimov H: Pulpitis-induced interradicular periodontal changes in experimental animals, J Periodontol 38: 124-129, 1967.
46. Seltzer S, Bender IB, Ziontz M: The inter-relationship of pulp and periodontal disease, Oral Surg Oral Med Oral Pathol 16:1474-1490, 1963.
47. Shi D, Meng H, Xu L, et al: Systemic inflammation markers in patients with aggressive periodontitis: a pilot study, J Periodontol 79:2340-2346, 2008.
48. Simon JHS, Glick DH, Frank AL: The relationship of endodontic-periodontic lesions, J Periodontol 43:202-208, 1972.
49. Simring M, Goldberg M: Pulpal pocket approach: retrograde peri-odontitis, J Periodontol 35:22-48, 1964.
50. Sinai I, Soltanoff W: The transmission of pathologic changes between the pulp and the periodontal structures, Oral Surg Oral Med Oral Pathol 36:558-568, 1973.
51. Siqueira JF, Jr, de Uzeda M: Disinfection by calcium hydroxide pastes of dentinal tubules infected with two obligate and one fac-ultative anaerobic bacteria, J Endod 22:674-676, 1996.
52. Slutzky-Goldberg I, Tsesis I, Slutzky H, et al: Odontogenic sinus tracts: a cohort study, Quintessence Int 40:13-18, 2009.
53. Stahl SS: Pathogenesis of inflammatory lesions in pulp and peri-odontal tissues, Periodontics 4:190-195, 1966.
54. Stallard RE: Periodontic-endodontic relationships, Oral Surg Oral Med Oral Pathol 34:314-326, 1972.
55. Sutalo J, Simeon P, Tarle Z, et al: “C”-shaped canal configuration of mandibular second permanent molars, Coll Antropol 22:179-186, 1998.
56. Tamse A, Fuss Z, Lustig J, et al: An evaluation of endodontically treated vertically fractured teeth, J Endod 25:506-508, 1999.
57. Tai T-F, Chiang C-P, Lin C-P, et al: Complex cementodentinal tears in a maxillary central incisor—a case report, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103:e55-60, 2007.
58. Tronstad L: Pulp reactions in traumatized teeth. In Gutmann JL, Harrison JW, editors: Proceedings of an international conference on oral trauma, Chicago, 1986, American Association of Endodontists.
59. Tulkki MJ, Baisden MK, McClanahan SB: Cemental tear: a case report of a rare root fracture, J Endod 32:1005-1007, 2006.
60. Wang H-L, Glickman GN: Endodontic and periodontic interre-lationships. In Cohen S, Burns RC, editors: Pathways of the pulp, ed 8, St Louis, 2002, Mosby.
61. Wedenberg C, Linkdskög S: Experimental internal resorption in monkey teeth, Endod Dent Traumatol 1:221-227, 1985.
62. Wilson GW, Kornman KS: Fundamentals of periodontics, Chicago, 1996, Quintessence Pub Co.
63. Zehnder M, Gold SI, Hasselgren G: Pathologic interactions in pulpal and periodontal tissues, J Clin Periodontol 29:663-671, 2002.

97
Chapter 5
Problem Solving in the Diagnosis of Treatment Failure
Problem-Solving ListProblem-solving challenges and dilemmas addressed in this chapter:
Nonsurgical Treatment Success
Incomplete Nonsurgical Treatment
Alternative Diagnoses often Confused With Treatment Failure
Diagnosis of Treatment Failure
Causes of Treatment Failure
Uncleaned, contaminated canal space
Persistence or occurrence of pathosis due to an inadequate apical seal
Persistence or occurrence of pathosis due to an inadequate coronal seal
Persistence or occurrence of pathosis on roots with presumably nonnegotiable canals
Instrument separation preventing thorough canal cleaning, shaping, disinfection, and obturation
Emerging Clinical Directives
In attempting to assign the success or failure of operations upon diseased teeth to their proper causes, factors of the greatest importance are frequently left out of account, and the results ascribed to some agent which may have been entirely indifferent. One of these factors, which forms the very foundation of successful root-treatment, is the manner in which the mechanical cleansing of the canal is carried out.18
R.H. HoFHEINz, 1892
The patient’s subjective data and objective clinical findings to confirm a pulpal diagnosis are discussed in Chapter 1. In many cases, teeth that may be present in the newly symptomatic area have already had a root canal procedure. The process of establishing an accurate diagnosis in these situations must then also include an evaluation of both the treated and untreated teeth. It is a common misperception—at least among many patients, if not some dentists—that once a root canal procedure has been completed, the tooth no longer has the potential for developing problems (radicu-lar pathosis, spontaneous or functional symptoms). This chapter will explore the subjective and objective findings in these cases and highlight the clinical and radiographic criteria that will enable the clinician to determine the outcomes of previous treatment procedures. The approach to this assess-ment will assume that other diagnostic considerations, as highlighted in Chapter 1 (odontogenic pain) and Chapter 4 (pulpal-periodontal problems) have already been elimi-nated in the diagnostic scheme.
Nonsurgical Treatment Success
A simplified definition of favorable outcomes with nonsurgi-cal treatment procedures might be: If there is no radiographic evidence of periradicular pathosis prior to root canal
treatment, no radiographic signs of pathosis should ever appear following treatment (Fig. 5-1).11 If there is radio-graphic evidence of periradicular pathosis at the time of treat-ment, periodic postoperative reexamination radiographs should indicate that the pathosis is healed or is healing.11 As characterized radiographically, this would mean a return to a normal periodontal ligament space and lamina dura, and a normal bony pattern surrounding the root apex (Fig. 5-2). Subjective and clinical corollaries to these findings would refer to the presence or absence of objective signs or patient symptoms. If there are no preoperative symptoms, none should arise postoperatively. Conversely, any preoperative symptoms should resolve completely with treatment.
With these concepts for success in mind, a clinical diag-nostic case involving a mixed dentition of root-treated treated and untreated teeth would require a separate and distinct evaluation of the treated teeth, as opposed to just dismissing them as not being the cause of the patient’s symptoms.

98 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
A B
FIGURE 5-1 A, Routine endodontic case without radiographic evidence of periapical pathosis at the time of treatment in February 1978. B, Reevaluation June 2006. The tooth is asymptomatic with normal function.
A B
FIGURE 5-2 A, Large periapical lesion secondary to necrotic pulp on a mandibular right first molar. Lesion appears to have a periodontal complication, but clinical probings were normal. There was a draining sinus tract on the edentulous ridge distal to the tooth. B, One-year posttreatment reexamination. The apical and distal bone is completely restored along with a periodontal ligament space of uniform and normal width.
CLINICAL PROBLEMProblem: A 46-year-old patient complained of a periodic dull pain in the lower right quadrant. There was discomfort on chewing but no history of thermal sensitivity. The radio-graph indicated previous root canal treatment of the man-dibular second premolar and second molar, which according to the patient was completed 7 to 10 years previously (Fig. 5-3, A). Radiographs from the time of the original treatment were unavailable. The only questionable radiographic finding was a slightly widened apical periodontal ligament space on the apex of the distal root on the second molar. The patient had acute tenderness to percussion on the mandibular first molar, but the second premolar and second molar had no discomfort. Periodontal probings indicated moderate general periodontal bone loss, but there was no evidence
of defects potentially related to a vertical root fracture on any tooth.
Solution: The challenge was to arrive at the correct diagnosis. The differential diagnosis included bruxism, possible recurrent periapical pathosis on either of the treated teeth, or pulpal disease in the first molar. Occlusion was evaluated, and no occlusal pre-maturities were found that would account for the percussion tenderness on the first molar. Thermal sensibility tests on the first molar failed to elicit a response. The diagnosis of pulpal necrosis of the first molar was made; root canal treatment of the other two teeth was judged to be successful. The completed root canal treatment of the first molar is seen in Fig. 5-3, B. All symp-toms subsequently resolved.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 99
A B
FIGURE 5-3 A, Mandibular left posterior dentition in which patient is experiencing pain. Note questionable radiographic appearance of apical periodontal ligament space on distal root of second molar. B, Post treatment of first molar, which clinical examination identified as the cause of symptoms. The two adjacent teeth were judged to have successful root canal treatment.
CLINICAL PROBLEMProblem: The patient was a 55-year-old female with an acute apical abscess. She gave a history that the maxillary left first molar had root canal treatment approximately 3 years previ-ously (Fig. 5-4, A). Clinically there was acute apical palpation tenderness over the apex of the mesial buccal root. There was a radiolucency around the apex of the mesial buccal root; bone associated with the other two apices appeared to be normal.
Solution: What was the differential diagnostic parameter? The root canal filling material in both buccal roots suggested that the canals were adequately but not ideally cleaned and shaped, and therefore a true failure was a possibility. A more likely diagnosis for this root was the presence of a second canal or irregular canal configuration.3,47 Fig. 5-4, B shows a file in a second canal clearly separate from the previously treated canal. Fig. 5-4, C shows the completed treatment of this canal only. Arguably, this canal may be the most frequently over-looked canal, owing to its small diameter, the lack of radio-graphic signs of its presence, and the fact that it is not present in all cases (Fig. 5-5, A to D). Nevertheless, if a maxillary molar presents with a lesion only around the apex of the mesial buccal root in an otherwise adequately treated tooth, an untreated second mesial buccal canal must be the first diag-nostic consideration. An uncleaned, contaminated second canal would be one of several possible etiologies for pathosis in a case of inadequate root canal treatment involving the mesiobuccal root (Fig. 5-6).
One of the more perplexing clinical circumstances with the maxillary first molar (and any other tooth that may have a second canal located in the buccal-lingual dimension) is when there is no radiolucency seen on the radiograph, or when the presence of a radiolucency is questionable no matter what angle the film is exposed. In these cases, there may be a lesion present directly behind the root, which is blocked from view by the widening of the mesial buccal root as it approaches the cervical portion of the tooth. An example would be the mesial buccal root of a maxillary first molar with a small palatally located second canal orifice well below the mesial buccal apex. Clinically, the only finding may be tenderness to percussion that is different on the mesial buccal root than on the other roots. Some cases may exhibit local-ized tenderness to palpation over the root as well. In these cases, it is reasonable to consider either nonsurgical or surgi-cal revision of this root, the choice depending on the other circumstances surrounding the case.20,62
A second common way in which infected/inflamed pulpal tissue in untreated canals causes a symptomatic clinical problem is the onset of acute thermal sensitivity.57 Symptoms will be typical of acute or chronic pulpitis, and thermal stimu-lation will cause lasting pain. Episodes of spontaneous pain are also typical, but there are seldom any radiographic signs. The diagnostic challenge is to determine which tooth is causing the symptoms. It should not be assumed that a multirooted tooth should be eliminated from consideration because it has had root canal treatment. Thermal sensibility tests should be con-ducted on all teeth in the area, including the root-treated tooth.57 Since the onset of an abnormal reaction to thermal stimulation may be delayed in cases of untreated canals, it is wise to test one tooth and pause before continuing to the next tooth. If tests are conducted too rapidly, it may be difficult to identify which tooth is the cause of a delayed response.
In the evaluation of recurrent pathosis on root-treated teeth, it is important to consider an untreated canal in any tooth that anatomically could have one. These generally are present in a buccal-lingual dimension, as discussed earlier with the maxillary first molar.4 Mandibular molars com-monly have two distal canals and occasionally two distal roots
Incomplete Nonsurgical Treatment
Occasionally the cause of periapical pathosis on a multicanal pulpless tooth can easily be identified when it is obvious that one of the canals has no root filling. It is a matter of semantics whether or not to label this condition as a treatment failure, since the canal in question was never treated. At the same time, it is clearly a failure on the part of the clinician to locate and treat all canals present in the tooth.

A B
C
FIGURE 5-4 A, Apical lesion at apex of mesiobuccal root of an endodontically treated maxillary left first molar. B, Endodontic file in an untreated second mesial buccal canal. C, Post treatment. Existing root canal treatment of the other canals was judged adequate.
A B
C D
FIGURE 5-5 A, Cross-section of typical mesial buccal root, indicating a treated mesial buccal canal and an untreated second mesial buccal canal connected by an isthmus (arrows). B, Radiographic view palatal root (left) and lateral view buccal root (right) of same tooth. C, Pulp chamber with identification of mesial buccal, distal buccal, and palatal canals. D, Identification of the second mesial buccal canal.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 101
A B
FIGURE 5-6 A, Inadequate root canal treatment of a maxillary left first molar in which there is also an untreated second mesial buccal root. Clinically, there was local swelling and palpation tenderness localized to the area over the apex of the mesial buccal root. B, Completed revision. Note treatment of second mesial buccal root.
A B
FIGURE 5-7 A, Previously treated mandibular right first molar with an apical lesion on the distal apex. An untreated second canal in the distal root was the suspected etiology. B, Postrevision radiograph indicating treatment of two distal canals.
A B
FIGURE 5-8 A, Mandibular left second molar with a lesion caused by failure to treat a second distal root. The endodontic treatment present in the other three canals was judged to be adequate. B, Post revision radiograph.
(Figs. 5-7 and 5-8). Mandibular incisors and all premolars may also have two canals or sometimes even three canals (Figs. 5-9 through 5-11).
A second concept of incomplete root canal treatment may be identified as any treatment falling far below the standard of care with respect to obturation as evaluated on a good
periapical radiograph. Cleaning and shaping are undoubtedly included as a cause of failure, but inadequacy of obturation is most obvious upon radiographic examination (Fig. 5-12). Root canal procedures completed with such disregard for traditional and proven concepts of cleaning, shaping, disin-fecting, and sealing are doomed to failure.

FIGURE 5-9 Mandibular right lateral incisor with two canals. FIGURE 5-10 Mandibular first premolar with two canals.
A B
FIGURE 5-11 A, Root treated maxillary first premolar with an apical lesion. B, Postrevision radiograph indicating treatment of a third canal that was the cause of continuing pathosis. (Courtesy Dr. Ryan Wynne.)
A B
FIGURE 5-12 A, Maxillary central incisor with inadequate root canal treatment. B, Mandibular first molar with inadequate root canal treatment and continuing periapical pathosis.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 103
radiographic features that mimic those of root treatment failure but in reality are unrelated. The two categories are lesions associated with root fracture and lesions associated with chronic periodontal pathosis.
Chapter 4 provides a broader and more detailed discussion of root fractures, but it is appropriate to review those aspects of lesions associated with fractures that might be confused with failure of root canal treatment. Vertical fractures of the root are almost always associated with root-treated teeth, although some can be seen in other circumstances. The typical lesion associated with a root fracture is a narrow peri-odontal defect which develops along the course of the frac-ture line. In many cases, it will resemble a halo or J and is often referred to as a J-shaped lesion (Fig. 5-14).53 The peri-odontal probe will be of great value in the discovery and diagnosis of these lesions. If the fracture line extends through the sulcus, the clinical manifestation will be a narrow, deep periodontal pocket usually found on the midfacial or midlin-gual/palatal surface of the root (Fig. 5-15, A to C ). In some cases, if the fracture extends completely through the root, defects will be found on both the buccal and lingual surfaces.
It is common to find chronic sinus drainage tracts associ-ated with these lesions; oftentimes two tracts will appear.49,52 The buccal and lingual locations of these fractures and super-imposition of the narrow defect over the root itself seldom offer any radiographic evidence of the fracture itself. Infre-quently, in cases of complete fracture through the root, the fractured segments may separate, and the fracture line may become visible (Fig. 5-16). Other than exploratory surgery, periodontal probings are often the only means by which root fracture can be differentiated from a developing periapical lesion of pulpal origin.
Clinical and radiographic changes that typify vertical fractures often take time. Tenderness to percussion or con-tinuous low-grade pain may begin at the time the fracture occurs, but development of a periodontal defect that can be probed may not occur for weeks or months. Radiographic
A
B
FIGURE 5-13 A, Maxillary left second molar with inadequate root canal treatment. Patient was seen for an acute apical abscess. B, Reexamination image at 28 months indicates complete restoration of normal osseous anatomy around the apex.
FIGURE 5-14 A, J-type radiographic lesion (dashed line) associated with vertical root fracture.
CLINICAL PROBLEMProblem: A 42-year-old patient had a maxillary second molar with only one large canal (Fig. 5-13). The original root treatment was incomplete and led to failure. In addition, there was significant loss of periodontal attachment on the tooth that resulted in increased mobility. The resultant lesion was large, and the prognosis for revision was doubtful.
Solution: Following removal of the original gutta-percha filling material, copious purulent drainage was observed. The canal was cleaned, and a calcium hydroxide intracanal dress-ing was placed. Fortunately all symptoms resolved quickly. After 1 month, sulcular probing depths had returned to normal, mobility had disappeared, and there was no drainage from the canal upon reentry. The revision was completed and a 31-month reexamination indicated complete regeneration of bone in the previous periapical radiolucency (see Fig. 5-13, B).
Alternative Diagnoses Often Confused With Treatment Failure
If the possibility of incomplete root canal treatment has been eliminated from the differential diagnosis, alternative diag-noses should be considered. These entities have clinical and

104 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
CLINICAL PROBLEMProblem: The patient was a 63-year-old female with a recent history of local swelling and tenderness in buccal gin-gival tissues in the mandibular right molar area. The tooth was an abutment for a fixed bridge in place for many years. The radiograph indicated that the tooth had had root canal treat-ment. There was also a widening of the periodontal ligament space around the distal root (Fig. 5-19, A).
Solution: Periodontal probings were made in 1-mm incre-ments circumferentially around the tooth. A normal sulcus depth of 3 mm was found circumferentially on the mesial half of the tooth. Deep narrow periodontal defects on both the buccal and lingual aspects of the distal root indicated a through and through vertical fracture (see Fig. 5-19, B and C). A joint decision made between the patient and clinician was to reflect the buccal soft tissue and examine the bone and root. This diagnostic surgical procedure confirmed the pres-ence of a vertical root fracture. The crown was removed, and the distal root was resected, thereby preserving the mesial half of the tooth to be restored as a functional premolar (see Chapter 18).
A B
C
FIGURE 5-15 A, Normal probing depth found to the mesial of midlabial. B, Normal probing depth found to the distal of midlabial. C, Probing to the apex in the midlabial position.
FIGURE 5-16 Vertical root fracture line visible in the distal root of a mandibular molar.
changes will not occur until there has been a sufficiently wide zone of bone resorption along the fracture line. The patient in Fig. 5-17 presented with a toothache in the man-dibular left first molar and was referred to the endodontist with the presumptive diagnosis of root canal treatment failure (see Fig. 5-17, A). The patient elected to postpone the end-odontic examination. One month later, the patient was seen on an emergency basis, having developed an acute infection. A second periapical radiograph documents significant loss of bone around the distal root (see Fig. 5-17, B). The lateral
location of the bone loss is an important distinction from lesions that develop with the failure of root canal treatment, which tend to involve the periapical tissues. Nevertheless, occasional lesions associated with vertical fracture can be difficult to diagnose radiographically (Fig. 5-18). A detailed

A
B
FIGURE 5-17 A, Mandibular left first molar referred with provisional diagnosis of “endodontic failure.” B, One month later, new radiograph displays bone loss consistent with vertical root fracture.
FIGURE 5-18 Maxillary central incisor with apparent apical lesion. Note vertical fracture line visible in apical third. Lesion was found to probe as a sinus tract–type probing in both midlabial and midpalatal positions. This probing pattern is consistent with a complete fracture through the root.
B C
A
FIGURE 5-19 A, Mandibular second molar with history of recurrent local swelling. Tentative diagnosis was “endodontic failure.” Normal probings were found around mesial half of root. B, Probing to the apex on the buccal of the distal root. C, Probing to the apex on the lingual of the distal root that completes a probing pattern consistent with a vertical fracture extending completely through the distal root from buccal to lingual.

106 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
CLINICAL PROBLEMProblem: A 61-year-old female was referred to the endo-dontist for revision of root treatment in the mandibular right first molar. The referring dentist initiated root treatment approximately 2 months previously. The patient states that there was no improvement in the persistent infection that appeared to be draining through the gingival sulcus, and that her dentist was convinced there was some irregularity in the root canal anatomy that he was unable to clean properly. A radiograph showed a periapical radiolucency on the distal root of this tooth that extended coronally along the distal root surface (Fig. 5-20, A). There did not appear to be any bone in the interproximal space between the first and second molars. There was advanced periodontal bone loss associated with the second molar as well. Periodontal probing circumferentially in 1-mm increments indicated loss of attachment from the furca-tion on the buccal surface completely around the distal surface to the lingual surface of the distal root on the first molar. (Fig. 5-20, B). This probing pattern is typical of an infrabony defect of advanced periodontal disease (see Chapter 4).
Solution: A surgical procedure in which the buccal soft tissues are reflected revealed the extent of bone loss (see Fig. 5-20, C). A root resection (amputation; see Chapter 18) was performed and a 12-month reexamination radiograph (see Fig. 18-50, C ) indicated complete healing of the original defect. The tooth and the bridge it supports remained functional, the patient had no symptoms, the periodontal pocket was elimi-nated, and the crestal bone regenerated to a maintainable level.
A B
C
FIGURE 5-20 A, Mandibular right first molar with large apical lesion associated with distal root. B, Probings indicated loss of attachment to apex from midbuccal to distal lingual through interproximal space. Pattern is consistent with severe periodontal bone loss. C, Surgical exposure of periodontal lesion. Note bone contours which actually produce the probing pattern.
analysis of the radiographic interpretation of these lesions is found in Chapter 3.
Periodontal defects associated with chronic periodontitis may involve the apical tissues and could be confused with failure of a root-treated tooth. Generally, lesions of periodon-tal origin that extend to the apex of a tooth occur in dentition with generalized periodontal bone loss. This concept may be a helpful radiographic clue in determining the etiology of bone loss. Chapter 4 discusses the interrelationship of defects of periodontal origin and bony defects of pulpal origin in great detail. A case is presented here to preserve the continu-ity of the diagnostic process.
Diagnosis of Treatment Failure
Having discussed the sequelae of inadequate and incomplete root canal treatment, we will now consider cases that techni-cally appear to meet the standard of care on radiographic examination and do not exhibit clinical signs of the alternate diagnoses discussed in the preceding sections. Based on our simplified definition of success with root canal treatment, the first statement suggests that a root-treated tooth without a periapical lesion would be considered successful if the symp-toms resolve and no lesion ever appeared following the pro-cedure. Failure then would be seen as the posttreatment emergence of symptoms and the gradual appearance of

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 107
FIGURE 5-21 Palatal root of first molar obturated well short of apical terminus of prepared canal.
A B
FIGURE 5-22 A, Adult maxillary central incisor with open apex and inadequate apical seal. B, Following an 18-month course of apexification with calcium hydroxide, an apical barrier was obtained and the canal was refilled.
radiographic signs of bone destruction at the apex or a spe-cific lateral site.
With the singular exception of an untreated canal with remaining pulpal tissue (discussed earlier), the symptoms of root treatment failure will arise in periradicular tissues in a manner virtually identical to routine pulpal necrosis. Early onset is often characterized by symptoms of percussion sensi-tivity and possibly palpation sensitivity that may precede radio-graphic signs of pathosis. As with many cases of pulpal necrosis, developing apical or lateral lesions may become symptomatic, causing the patient to seek consultation. In other cases, lesions of unknown duration may be discovered on routine radio-graphic examination. Clinically, lesions associated with teeth that have had root treatment may present as acute abscesses or with chronic sinus tracts. The reader is referred to the sections on diagnosing pulpal necrosis in Chapter 1 and Chapter 15 for management of endodontic emergencies.
The second statement at the beginning of the chapter with regard to outcomes suggests that success following root canal procedures would be defined as the healing of any periradicu-lar lesion that exists at the time of original treatment. A number of studies recognize that healing of existing lesions following root treatment is variable and dependent on many factors.11 Recent investigations into the area of causes for root treatment failure have contributed to our understanding of why periradicular lesions may not heal.48
Causes of Treatment FailureUncleaned, Contaminated Canal SpaceBecause the persistence or occurrence of periapical pathosis following initial root canal treatment may have multiple causes,5 treatment planning for revision (see Chapter 15) must first determine etiology. One should presume that all possible causes are present, although it can almost always be anticipated that there is untreated root canal space that con-tains necrotic, infected, or inflamed tissue.
Chapter 1 discussed failure to débride the canal system of its irritating contents as a prime cause for failure.2,46 When coupled with other identifiable entities such as ineffective three-dimen-sional filling of the canal space, incomplete fills using only sealers or medicated pastes, and gross overextension of filling materials, the percentage of treatment failures will increase.25,48 The common threads in these failures are incomplete removal of tissue debris and bacteria from the canal system and lack or failure of a radicular seal, both apically and coronally.17,43,51
Persistence or Occurrence of Pathosis Due to an Inadequate Apical SealSome cases of failed root canal treatment have obvious radio-graphic signs of inadequacy in the canal obturation. Fig. 5-21
illustrates an example of a palatal canal that is clearly prepared to within 2 mm of the radiographic apex but is obturated 2 to 3 mm short of the prepared stop.
A failed case of nonsurgical management of an open-apex tooth is seen in Fig. 5-22. Radiographically, the gutta-percha filling fails to fill the canal properly; by a priori reasoning, an apically sealed canal probably does not exist. At this stage of root development, the canal space appears radiographically to have parallel walls. When considering the anatomy of an immature root, in the labial-lingual plane, the canal is actu-ally divergent and wider apically than in a mesial-distal

108 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
This case amplifies the main causes for the occurrence of periradicular disease and supports initial nonsurgical revision of inadequacies in root canal treatment in most situations. The existing and original crown appeared well done, with excellent marginal fit. It is still possible, however, that coronal leakage developed around the crown margin or the margin of the restoration. There are other possible causes such as regrowth of latent bacteria in the dentinal tubules or
dimension.7 It would never have been possible to obturate this canal adequately with standard techniques. The plan for revision included apexification with calcium hydroxide prior to any attempt to seal the canal.60 The previous gutta-percha filing was removed using Gates-Glidden burs and large Hed-ström files. Treatment time for apexification on the 35-year-old patient shown was 2 years, 9 months. This is essentially the same time frame for treatment on a young patent when using calcium hydroxide. Presently, however, the use of mineral trioxide aggregate (MTA) may enhance and hasten the process59 (see Chapter 14).
Unfortunately in most cases of failed root canal treatment, the quality of the obturation at the apical foramen cannot be directly assessed radiographically. A second limitation is the inability to assess the quality of the débridement. It is reason-able to assume that if the canal is not properly débrided, it will be impossible to obtain an adequate seal. This is espe-cially true in the contemporary use of resin-bonded root canal filling materials that claim to develop a monoblock-type of bonding in the root canal.15,54,55 If the canal cannot be débrided properly, bonding will not occur, the filling will leak, and it may suffer further from enzymatic breakdown due to the impact of tissue debris and retained bacteria on the resin-based core material and sealer.54
CLINICAL PROBLEMProblem: A relatively uncomplicated endodontic case was completed by a general dentist (Fig. 5-23, A). No periradicular lesions were present at the time of treatment. Five years later, the tooth became sensitive to percussion, and an apical lesion on the mesial root was discovered on a radiograph (see Fig. 5-23, B).
Solution: The patient was referred for revision of the root canal treatment, which was completed only on the mesial canals. Reexamination 4 years later demonstrated healing of the periradicular tissues (see Fig. 5-23, C).
A
B C
FIGURE 5-23 A, Posttreatment radiograph of root canal treatment on mandibular right first molar. B, Film of same tooth 5 years later, indicating an apical lesion on the mesial apex. Nonsurgical revision of mesial root completed at the same time. C, Reevaluation after 4 years, indicating complete healing.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 109
inaccessible areas of the canal system.16 Obtaining a clean canal in a revision is a much greater technical challenge than to achieve cleanliness in a primary treatment.6,37,50 These issues will be discussed in further detail in the next sections. In some cases, after thorough assessment and explanation to the patient, a surgical revision may be the treatment of choice6,62 (see Chapter 16).
Persistence or Occurrence of Pathosis Due to an Inadequate Coronal SealResearch supports that coronal leakage following root canal treatment can cause periradicular pathosis or result in its persistence.36,48 This theory has been long held based on empirical observation. The problem of coronal leakage is known to occur in a variety of situations. The most obvious is the case of a root-treated tooth that has lost its coronal restoration, leaving the gutta-percha filling material exposed to the oral environment (Fig. 5-24). Studies indicate that in as little as 20 to 90 days, bacteria may penetrate along and apically beyond a well-placed gutta-percha filling.27,51 Other common pathways are recurrent caries in contact with the pulp chamber (Fig. 5-25). Marginal leakage can occur around crowns (Fig 5-26), faulty access cavity restorations (Fig. 5-27), or inadequate core buildups. This is a particular problem with composite materials placed using a bulk tech-nique as opposed to incremental placement (Fig. 5-28). Also, posts that are exposed to saliva or become loose under failing
FIGURE 5-24 Periapical pathosis secondary to coronal leakage due to loss of the clinical crown.
FIGURE 5-27 Faulty restoration of the access cavity establishes a pathway for coronal leakage. See Fig. 20-3.
FIGURE 5-26 Leakage under the crown was not discovered until an access cavity was made and the crown came off.
FIGURE 5-25 Periapical pathosis secondary to coronal leakage due to caries into the pulp chamber.
restorations provide ready access for bacteria into the canal (Fig. 5-29). While these concepts are widely held as true in clinical scenarios, data are based on retrospective evaluations. The same type of retrospective data, only in a more extensive and in-depth histologic evaluation, have strongly suggested

110 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
that well-prepared and filled root canals seem to resist bacte-rial penetration even upon frank and long-standing oral exposure by caries, fracture, or loss of restoration.38,39
A seldom identified etiology for failure, or one that may even be thought of as a source of coronal leakage and con-tamination of the untreated or treated root canal, is the long-term persistence of bacterial plaque and calculus around the restorative margins. Dentinal tubules may serve as portals of entry for external irritants into the root canal58 (Fig. 5-30, A; also see recommended readings at end of chapter). Ana-tomic alterations in the tooth structure can also exist in this area. Between 5% and 10% of the cemental-enamel junction presents with open, uncovered dentinal tubules14,22,32 (see Fig. 5-30, B). This presents a perfect avenue for com-munication between the periodontium/oral cavity and the pulp canal space, whether rapidly through virulent
FIGURE 5-28 Failure of composite buildup due to marginal leakage. This led to leakage into root-treated canals as well.
FIGURE 5-29 Intact post, core, and crown restoration, or that loosened and came out. Marginal leakage into post space destroyed cement bond and continued apically to defeat endodontic seal. Note corrosion of silver cones.
pathogenic invasion or slowly through a chronic invaginating process. This usually does not present a problem in teeth that are meticulously maintained through oral hygiene practices or teeth with well-adapted restorative margins that are prop-erly maintained. However, the potential for this etiology to be the cause of failure in teeth with even the best root canal treatment cannot be overlooked in the following situations:
• If the margin is not well adapted (see Fig. 5-30, C ) or if there is a small area of undetectable caries (both clinically or radiographically), this may serve as a long-term source of leakage58 (see Fig. 5-30, A). Bitewing radiographs are recommended during the evaluative phase (see Chapters 2 and 3), but their diagnostic capabilities may be limited. In the non–root-treated tooth, this will create a long-term sensitivity or sometimes a vague pulpal problem, whereas in the root-treated tooth, the patient will be symptom free but may have signs of apical or lateral pathosis.
• If the tooth was prepared for a crown and the impression did not clearly mark the finish line, or if the crown was not adapted to cover the entire area of cut, exposed tubules, there will be exposed dentin that can serve as potential avenues of communication to the pulpal space (see Fig. 5-30, D, arrows). In the non–root-treated tooth, this will create a great deal of sensitivity or sometimes outright pain, whereas in the root-treated tooth, the patient will be symptom free but may have signs of apical or lateral pathosis.
• In teeth that undergo periodic root planing and curettage, often the cementum is removed along with the adherent plaque, which opens additional pathways for irritants to gain access to the root canal space.58 Coupled with the degree or severity of root instrumentation, this may cause severe discomfort in the non–root-treated tooth, whereas in the root-treated tooth, the patient may be symptom free but will often manifest signs of periapical or lateral pathosis following multiple episodes of periodontal treatment intervention.
The implications of this phenomenon of coronal leakage and treatment failure are significant (see Fig. 5-30, E) is pos-sible (see Fig. 5-5, A-B). It may be wise to consider revision of any root canal obturation that has been exposed to saliva, caries, or a failing restoration, whether or not it is symptom-atic or the root shows any radiographic signs of periapical pathosis.62 This scenario, however, must be discussed at length with the patient before proceeding. During case assess-ment following root canal treatment, consider the following questions: Are the restorative margins possibly leaking? Is there recurrent decay around the restorative margins? Is there leakage around a core buildup or post? Is the post possibly loose? Are there excessive amounts of plaque and calculus around the restorative margins?

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 111
BT
A
Den
tin
Den
tin
Den
tin
Crown
Cementum
Crown
Cementum
Crown
Cementum
60%-65%Enamel overlaps
cementum
30% Edge to edge
5%-10%Enamel andcementum
do not meetB
C D
E
FIGURE 5-30 A, Histologic section of a tooth that had a crown. Above margin, debris can be seen. This represents an area where the crown was leaking; presence of bacteria penetrating cut dentinal tubules all the way to pulpal space (BT) can be seen (Brown and Brenn stain ×4). B, Relation of cementum to enamel at the cemento-enamel junction. Overlap, meet, and gap (OMG) describe the order of frequency of these conditions. C, Note poor marginal adaptation of the crown to the tooth, presenting a perfect opportunity for bacterial invasion. D, Newly placed crown that does not adapt to cut dentin margins. Patient had severe pain when this area was stimulated. E, Demineralized and cleared root specimen illustrating leakage from the coronal direction. Arrows indicate uncleaned canal and leakage. (B, Modified from Daniel SJ, Harfst SA: Mosby’s dental hygiene: concepts, cases, and competencies, 2004 update, St Louis, 2004, Mosby, p 288.)
Persistence or Occurrence of Pathosis on Roots With Presumably Nonnegotiable CanalsOften root canals may either not be found or are not nego-tiable. There is a presumption that these canals are calcified, so treatment may not be necessary. However, if there is a
periapical lesion present at the end of the root or on its lateral aspect or if one develops over time, this is prima facie evi-dence of the presence of a canal space and necrotic, infected tissue, even when a canal does not appear patent on radio-graphs. Studies have shown that there is a greater risk for these cases to develop periapical periodontitis or have persis-tence of such following root canal procedures.31

112 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
fracture occurred may make the attempt to remove such fragments unwise.19,20,26,45 As with calcified canals, a reason-ably successful strategy is to complete revision or treatment of the second canal when the root has multiple canals in a case in which the instrument fragment cannot be removed or bypassed (see Fig. 5-32, B). Many canal systems merge to a single common apical foramen. By treating the alternate canal, the instrument fragment may effectively be bypassed. The unknown factor with this approach is that there is no means by which this canal configuration can be confirmed.4 Consequently, the patient should be informed of the problem, the strategy to be employed, and a plan for peri-odic reexamination.
Attempts to remove instrument fragments deep in the root canal space invite a number of serious procedural errors such as stripping perforation, instrument perforation, and exces-sive thinning of the root canal walls.10,19 Although citations appear in the literature documenting successful removal,12 postoperative radiographs typically indicate extremely generous excavation cavities, which begs the question of restorability or at least the prognosis of restoration. Occasion-ally it may be possible to bypass a fractured instrument segment. With the use of ultrasonically energized root canal files, it is sometimes possible to remove the fractured segment (Fig. 5-33).
If the fragment cannot be removed, the canal is cleaned, shaped, disinfected, and obturated incorporating the frac-tured segment into the root canal filling material. However, the instrument may not play a significant role in sealing the canal from bacterial penetration via coronal or apical leakage at a later date.28 Attempts to bypass any fractured instrument segment must be monitored radiographically. In such cases, the prognosis of a successful obturation would depend chiefly on (1) the degree to which the instrument fragment influ-enced the direction and final diameter of the canal prepara-tion and (2) the presence of contaminated space beyond the instrument. Total blockage of the canal lumen by the
Persistence of pathosis on a mandibular molar filled short of the apical constriction in all the canals is seen in Fig. 5-31, A. Radiographically, no canal space is apparent beyond the present radicular filling material. The patient presented clini-cally with a long-standing gingival sinus tract. The tooth also contains intraradicular posts, which should not prevent non-surgical revision, since in some molars surgery is not a viable option (see Chapter 16). Limited anatomic access, short roots, certain tooth angles, or medical contraindications fre-quently limit the choices to nonsurgical revision or extrac-tion. Fortunately, the distal canal and one of two mesial canals were negotiable to the apex after post removal. Clinical examination confirmed healing of the sinus tract after the canals were débrided. Fig. 5-31, B is the appearance at the 1-year reassessment. The ability to negotiate one of two canals in roots such as this greatly improves the prognosis because of the frequent joining of two such canals into one at the apex.
Instrument Separation Preventing Thorough Canal Cleaning, Shaping, Disinfection, and ObturationA separated root canal instrument is seldom if ever the sole cause of failure.23 Since instruments are stainless steel or nickel-titanium alloy, it would be extremely rare for these materials to cause periradicular inflammation. The real problem is that the separated instrument prevents thorough cleaning, shaping, disinfection, and canal obturation23 (Fig. 5-32, A). When these instruments can be removed, successful revision of treatment invariably ensues.19 Although it is occasionally possible to remove these instrument frag-ments with methods to be described (see Chapter 14), the majority cannot be removed nonsurgically. Factors such as canal curvature, overall root width, and the depth at which
A B
FIGURE 5-31 A, Root treated mandibular molar with apical lesion. Distal root appears to be filled short owing to complete calcification of apical half of canal. Presence of lesion confirms there is canal space with infected necrotic tissue. Following post removal, the apical canal space was negotiated. B, One-year reexamination radiograph indicating complete osseous healing.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 113
resection may be considered (see Chapters 16 and 18). While surgical intervention has a high degree of success (see Chapter 16), residual bacteria in the apical dentinal tubules or extremely irregular anatomic spaces that could not be addressed nonsurgically may not be removed totally during the surgical procedure, regardless of the radiographic quality
fractured segment will almost always make an attempt to bypass unsuccessful, with the potential for a root perforation. Alternative treatment planning generally includes cleaning the canal up to the fractured segment and sealing the canal space; the case should be observed for subsequent signs or symptoms. If unsuccessful, periapical surgery or root
A B
FIGURE 5-32 A, Mandibular left first molar referred for revision and removal of fractured instrument in the mesial lingual canal. B, Off-angle radiograph indicating revision might be possible in the mesial buccal canal. If the instrument cannot be bypassed or retrieved, revision of one canal is often successful if the canals merge.
A B
C
FIGURE 5-33 A, Length determination exhibiting instrument fragment in mesial buccal canal. B, Successful bypass of the instrument (arrows). C, Posttreatment image suggesting that the instrument fragment was removed during the course of canal shaping. With use of ultrasonic instrumentation, fragments are often suctioned without notice.

114 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
of the resection and root-end filling. This may be due to the nature of the root-end resection and these contaminated irregularities,24 and signs and symptoms may persist. These problems create both diagnostic and treatment-planning challenges regarding the etiology and choice of management (e.g., second surgery or extraction).44 Clinically, the patient is usually given antibiotics “in hopes” that the symptoms will diminish. Only too often, this delays necessary treatment-planning alternatives.
These cases emphasize the importance of preventing instrument separation by (1) considering the canal anatomy, (2) paying attention to the objectives of canal cleaning and shaping, and (3) exercising caution when choosing to provide root canal treatment for posterior teeth with complex root canal systems. New file systems made from highly flexible yet durable metals and single-use endodontic files for each case may minimize instrument-separation incidents in the future.1 Further details on problem solving the management of anatomic complexities will be found in Chapter 13.
Fractured instruments in the root canals of molars are sometimes impossible to remove. They can be beyond reach around curves in small canals or in surgically inoperable roots. Root or tooth resection may be a feasible alternative to extraction (Fig. 5-35). If periradicular surgery or root or tooth resection cannot or should not be done, intentional replantation or extraction are usually the only options remaining.
CLINICAL PROBLEMProblem: A 33-year-old female presented with long-standing pain in the mandibular left posterior quadrant. She was convinced that her problem was coming from the first molar, though she could not be sure. She recalled that she had had root canal treatment on one of the molars and was told that that tooth could not cause her any difficulty. Her pain was beginning to be accentuated by biting. Clinical examination indicated pain to percussion and palpation on the second molar, with a more subdued response on the first molar. Both teeth were unresponsive to thermal stimulation, and peri-odontal probings were within normal limits. A radiograph showed a large radiolucency on the distal root of the first molar and a small radiolucency on the mesial apex of the second molar. The second molar appeared to be filled with a paste filling. The canals of both roots were filled well short of the radiographic apices and there was a separated instrument fragment at the mid root level of the mesial root.
Solution: Because of the patient’s symptoms and chief complaint, a decision was made to treat both teeth simultane-ously. After significant attempts to remove the fractured instrument segment in the mesial root of the second molar, the metallic object was bypassed with a file (Fig. 5-34, B). Both teeth were obturated with gutta-percha and sealer, and the patient’s symptoms ceased (Fig. 5-34, C). The fractured instru-ment segment was incorporated into the root canal filling. A 4-year reevaluation shows excellent healing for both teeth, and the patient was symptom free (see Fig. 5-34, D).
A B
C D
FIGURE 5-34 A, Mandibular left second molar with fractured instrument in mesial root. B, Successful bypass of the instrument (arrows). C, Completed revision. Note fragment is now located more apically than originally and may compromise the apical seal (arrows). D, Four-year reevaluation. Apical healing appears excellent.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 115
buildups over minimal clinical crowns are not likely to survive extraction in one piece. If these conditions are favor-able, replantation can be very successful (Fig. 5-36). In all cases, the patient should be informed of the potential outcome of extraction alone.
Intentional replantation is only an option in selected cases.8,34,61 One criterion for selection is an anatomic root morphology that is conducive to extraction without tooth fracture, such as a fused or cone shape. The restorative condi-tion of the tooth is also important. Teeth with posts and core
A B
FIGURE 5-35 A, Instrument fragment in distal lingual canal of mandibular molar. Nonsurgical removal has not been possible using conservative techniques. Apical surgery is not possible. B, Distal lingual root amputation was performed to retain the tooth as a terminal abutment for a removable partial denture.
A
CB
FIGURE 5-36 A, Maxillary second molar with chronic apical lesion. Presence of posts in two canals and a lesion involving the palatal root made intentional replantation the treatment of choice. B, A conical root morphology is ideal for successful extraction. The orifices were filled with MTA. C, Eight-year reexamination. The tooth was asymptomatic and had normal function.

116 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
Emerging Clinical DirectivesIn the area of microbiology, residual infections primarily caused by E. faecalis have become the subject of numerous studies.* Statistically, this organism is isolated relatively infre-quently from primary infections of the root canal system.56,63 In isolates from posttreatment lesions, the percentage rises significantly,13,20,34 although in specific geographic popula-tions, other organisms have been identified to be just as criti-cal.41 This is important because these microorganisms have proven to be difficult to eliminate from the root canal system by all methods now in clinical use.40 The resurgence of inter-est in endodontic irrigants and disinfectants, along with the issue of biofilms, are examples of concerns about this problem (see Chapter 12).
Many authors have described multiple conditions that may cause posttreatment disease.34 The most obvious are vertical root fractures, true cysts, foreign body reactions, extrusion of materials through the apical foramen, and extra-radicular infections, such as with yeasts or fungi.10,29,30,62 Of these entities, only vertical root fractures can be diagnosed clinically. The treatment for this problem is always extraction or root removal. Since the etiology of most cases of persistent periapical pathosis cannot be confirmed preoperatively, non-surgical revision is usually indicated, with a plan for postop-erative monitoring. However, a significant percentage of these cases will eventually require apical surgery.
The radiographic and clinical appearance of root canals obturated with a paste filling material that was extruded through the apical foramen during treatment is seen in Fig. 5-37. It is not surprising that subsequently, periapical lesions developed. Although nonsurgical revision was necessary to correct the inadequate root canal treatment, apical surgery was required to remove the excess material.
Of the remaining conditions cited for failure in the litera-ture, inadequate root canal treatment without alteration of the canal morphology is considered to be the only cause of posttreatment disease that has a good chance for success with
nonsurgical revision. Two other conditions for failure that are cited are inadequate root canal treatment with alteration of the root canal morphology and infection remaining in inaccessible areas in the apical portion of the root canal system.16,40 Nonsurgical revision of root canal treatment is not very likely to result in healing in many of these cases, even with an extensive revision. The recommendation for all of these conditions is periapical surgery. A final condition may be the presence of excessive material extruded beyond the apical foramen.25 More often than not, surgery will be indicated if the patient is symptomatic.
The diagnosis of treatment failure begins with the elimina-tion of alternative etiologies. Using the criteria for determin-ing treatment success, treated teeth can be assessed for relative success or failure. Although the success rate for nonsurgical root canal treatment is high, there are known conditions that will cause treatment failure. In the presence of symptoms, a diagnostic pathway has been described in a problem-solving format to yield the proper diagnosis and potential courses of treatment. Problem solving the technical aspects of these choices is detailed in Chapters 13, 14, and 18.
RefeReNCeS1. Bachall JK, Carp S, Miner M, et al: The causes, prevention, and
clinical management of broken endodontic rotary files, Dent Today 24(11):74, 76, 78-80, 2005.
2. Cheung GS: Endodontic failures, Int Dent J 46(3):131-138, 1996.
3. Cleghorn BM, Chjristie WH, Dong CC: Root and root canal morphology of the human permanent maxillary first molar: a lit-erature review, J Endod 32:813-821, 2006.
4. Cleghorn B, Goodacre CJ, Christie WH: Morphology of teeth and their root canal systems. In Ingle JI, Bakland LK, Baumgsartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc.
5. Crump MC: Differential diagnosis in endodontic failure, Dent Clin North Am 23:617-635, 1979.
6. Del Fabbro M, Taschieri S, Testori T, et al: Surgical versus non-surgical endodontic re-treatment for periradicular lesions. Cochrane Database Syst Rev 18(3):CD005511, 2007.
7. Duell R: Conservative endodontic treatment of the open apex in three dimensions, Dent Clin North Am 17:125-134, 1973.
8. Dumsha TC, Gutmann JL: Clinical guidelines for intentional replantation, Compend Contin Educ Dent 6:604, 606-608, 1985.
9. Fabricius L, Dahlén G, Sundqvist G, et al: Influence of residual bacteria on periapical tissue healing after chemomechanical treat-ment and root filling of experimentally infected monkey teeth, Eur J Oral Sci 114:278-285, 2006.
10. Friedman S: Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure), Endod Topics 1:54-78, 2002.
11. Friedman S: Prognosis of initial endodontic therapy, Endod Topics 2:59-88 2002.
12. Gencoglu N, Helvacioglu D: Comparison of the different tech-niques to remove fractured endodontic instruments from root canal systems, Eur J Dent 3(2):90-95, 2009.
13. Gomes BP, Pinheiro ET, Jacinto RC, et al: Microbial analysis of canals of root-filled teeth with periapical lesions using polymerase chain reaction, J Endod 43:537-540, 2008.
FIGURE 5-37 Extrusion of paste filling material into maxillary sinus. Note inadequate root canal treatment that failed.
*References 9, 21, 33, 35, 42, and 59.

chapter 5 | Problem Solving in the Diagnosis of Treatment Failure 117
36. Ray HA, Trope M: Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and coronal restoration, Int Endod J 28:12-18, 1995.
37. Reit C: Factors influencing endodontic retreatment. In Bergen-holtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
38. Ricucci D, Bergenholtz G: Bacterial status in root-filled teeth exposed to the oral environment by loss of restoration and fracture or caries—a histobacteriological study of treated cases, Int Endod J 36:787-802, 2003.
39. Ricucci D, Gröndahl K, Bergenholtz G: Periapical status of root-filled teeth exposed to the oral environment by loss of restoration or caries, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90:354-359, 2000.
40. Rucucci D, Siqueira JF, Jr: Anatomic and microbiologic challenges to achieving success with endodontic treatment: a case report, J Endod 34:1249-1254, 2008.
41. Rôças IN, Hülsmann M, Siqueria JF, Jr: Microorganisms in root-canal treated teeth from a German population, J Endod 34:926-931, 2008.
42. Sakamoto M, Siqueria JF, Jr, Rôças IN, et al: Bacterial reduction and persistence after endodontic treatment procedures, Oral Microbiol Immunol 22:19-23, 2007.
43. Saunders WP: Apical and coronal leakage. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
44. Saunders WP: Considerations in the revision of previous surgical procedures, Endod Topics 11:206-218, 2005.
45. Shen Y, Peng B, Cheung GS: Factors associated with the removal of fractured NiTi instruments from root canal systems, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98:605-610, 2004.
46. Sjögren U, Figdor D, Persson S, et al: Influence of infection at the time of root filling on the outcome of endodontic treatment in teeth with apical periodontitis, Int Endod J 30:297-306, 1997.
47. Somma F, Leoni D, Plotino G, et al: Root canal morphology of the mesiobuccal root of maxillary first molars: a micro-computed tomographic analysis, Int Endod J 42:165-174, 2009.
48. Spångberg LSW, Haapasalo M: Rational and efficacy of root canal medicaments and root filling materials with emphasis on treatment outcomes, Endod Topics 2:35-58, 2002.
49. Slutzky-Goldberg I, Tsesis I, Slutzky H, et al: Odontogenic sinus tracts: a cohort study, Quintessence Int 40:13-18, 2009.
50. Sundqvist G, Figdor D: Life as an endodontic pathogen. Ecologi-cal differences between the untreated and root-filled root canals, Endod Topics 6:3-28, 2003.
51. Swanson K, Madison S: An evaluation of coronal microleakage in endodontically treated teeth. Part I. Time periods, J Endod 56-59, 1987.
52. Tamse A, Fuss Z, Lustig J, et al: An evaluation of endodontically treated vertically fractured teeth, J Endod 25:506-508, 1999.
53. Tamse A, Kaffe I, Lustig J, et al: Radiographic features of vertically fractured endodontically treated mesial roots mandibular molars, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:797-802, 2006.
54. Tay FR, Pashley DH, Loushine RJ, et al: Susceptibility of a poly-caprolactone-based root canal filling material to degradation. Evi-dence of biodegradation from a simulated field test, Am J Dent 20:365-369, 2007.
55. Teixeira FB, Twixeira EC, Thompson J, et al: Dentinal bonding reaches the root canal, J Esthet Restor Dent 16:348-354, 2004.
14. Gottlieb B, Orban B, Diamond M: Biology and pathology of the tooth and its supporting mechanism, New York, 1938, Macmillan.
15. Gutmann JL: Biologic perspectives to support clinical choices in root canal treatment, Aust Endod J 31(1):9-13, 2005.
16. Haapasalo M, Udes T, Endal U: Persistent, recurrent, and acquired infection of the root canal system post-treatment, Endod Topics 6:29-56, 2003.
17. Heling I, Gorfil C, Slutzky H, et al: Endodontic failure caused by inadequate restorative procedures: a review and treatment recom-mendations, J Prosthet Dent 87:674-678, 2002.
18. Hofheinz RH: Immediate root filling, Dent Cosmos 34:182-186, 1892.
19. Hülsmann M, Schinkel I: Influence of several factors on the success or failure of removal of fractured instruments from the root canal, Endod Dent Traumatol 15:252-258, 1999.
20. Karabucak B, Setzer F: Criteria for the ideal treatment option for failed endodontics: surgical or nonsurgical? Compend Contin Educ Dent 28:391-397, 2007.
21. Kavaoglu G, Ørstavik D: Virulence factors of Enterococcus faecalis: relationship to endodontic disease, Crit Rev Oral Biol Med 15(5):308-320, 2004.
22. Lehmann U, Schmeisser S: Variations of cemento-enamel junction of human teeth. Literature review (in German), Dtsch Stomatol 41:516-519, 1991.
23. Lin LM, Rosenberg PA, Lin J: Do procedural errors cause endodontic treatment failure? J Am Dent Assoc 136:187-193, 2005.
24. Lin S, Platner O, Metger Z, et al: Residual bacteria in root apices removed by diagonal root-end resection: a histopathological evalu-ation, Int Endod J 41:469-475, 2008.
25. Love RM, Firth N: Histopathological profile of surgically removed persistent periapical radiolucent lesions of endodontic origin, Int Endod J 42:198-202, 2009.
26. Machtou P, Reit C: Non-surgical retreatment. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
27. Magura ME, Kafrawy AH, Brown CE, Jr, et al: Human saliva coronal microleakage in obturated root canals: an in vitro study, J Endod 17:324-331, 1991.
28. Mohammadi A, Khademi AA: Effect of separated instrument on bacterial penetration of obturated root canals, J Clin Dent 17(5): 131-133, 2006.
29. Nair PNR: Non-microbial etiology: periapical cysts sustain post-treatment apical periodontitis, Endod Topics 6:96-113, 2003.
30. Nair PNR: Non-microbial etiology: foreign body reaction main-taining post-treatment apical periodontitis, Endod Topics 6:114-134, 2003.
31. Negishi J, Kawanami M, Ogami E: Risk analysis of failure of root canal treatment for teeth with inaccessible apical constriction, J Dent 33:399-404, 2005.
32. Noyes FB, Schour I, Noyes HJ: A textbook of dental histology and embryology, ed 5, Philadelphia, 1938, Lea & Febiger.
33. Peciuliene V, Maneliene R, Balcikonyte E, et al: Microorganisms in root canal infections: a review, Stomatologija 10:4-9, 2008.
34. Peer M: Intentional replantation—a “last resort” treatment or a conventional treatment procedure? Nine case reports, Dent Trau-matol 20:28-55, 2004.
35. Portenier I, Waltimo TMT, Haapasalo M: Enterococcus faecalis: the root canal survivor and “star” in post-treatment disease, Endod Topics 6:135-159, 2003.

118 chapter 5 | Problem Solving in the Diagnosis of Treatment Failure
56. Theilade E: The microbiology of the necrotic pulp. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontol-ogy, Oxford, 2003, Blackwell Munksgaard.
57. Tidwell E, Witherspoon DE, Gutmann JL, et al: Thermal sensitiv-ity of endodontically treated teeth, Int Endod J 32:138-145, 1999.
58. Tronstad L: Clinical endodontics, Stuttgart, 1991, Georg Thieme Verlag.
59. Tronstad L, Sunde PT: The evolving new understanding of end-odontic infections, Endod Topics 6:57-77, 2003.
60. Witherspoon DE, Small JC, Regan JD, et al: Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate, J Endod 34:1171-1176, 2008.
61. Wolcott J, Rossman LE: Intentional replantation of endodonti-cally treated teeth: an update, Compend Contin Educ Dent 24:68-72, 74, 2003.
62. Wu MK, Dummer PM, Wesselink PR: Consequences of and strategies to deal with residual post-treatment root canal infection, Int Endod J 39:343-356, 2006.
63. Zehnder M, Guggenheim B: The mysterious appearance of entero-cocci in filled root canals, Int Endod J 42:277-287, 2009.
ReCOmmeNDeD ADDITIONAl ReADINgHals E: Observations on giant tubules in human coronal dentin by
light microscopy and microradiography, Scan J Dent Res 91:1-7, 1983.
Tronstad L: Ultrastructural observations on human coronal dentin, Scan J Dent Res 81:101-111, 1973.
Tronstad L, Langeland K: Electron microscopy of human dentin exposed by attrition, Scan J Dent Res 79:160-171, 1971.

119
Chapter 6
Problem Solving in the Diagnosis of Nonodontogenic Pain
Problem-Solving ListProblem-solving challenges and dilemmas in the diagnosis of nonodontogenic pain addressed in this chapter are:
Occlusal Discrepancies
Trigeminal Neuralgia
Atypical Facial Pain
Temporomandibular Disorder
Further observations on the diagnosis of TMD: maxillary symptoms
Dental signs of temporomandibular disorder
Dental symptoms of temporomandibular disorder
Treatment of Heavy Occlusal Contacts and Prematurities
Additional and Effective Pain-Relieving Strategies
Maxillary Sinusitis
Other Etiologies of Pain in the Oral Cavity and Head
The condition (tic douloureux) frequently results from chronic irritation of the fifth cranial nerve. The pain is very acute, and occurs in distinct paroxysms, gradually increasing in severity, until it reaches a climax, when it quickly subsides. The attack may occur at any time and is provided by speech, laughing, talking, the movement of a muscle, etc., and even slight noise or light touch, as placing the hat on the head, may cause a paroxysm. The patient lives in constant dread of an attack.6
J.P. BuCklEy, 1910
observed.12 The majority of these conditions (e.g., temporal arteritis, otitis media, sialolithiasis) have an array of signs and symptoms that usually manifest in the tissues of origin. The reported dental symptoms are not typical, and it is extremely unlikely that these conditions would present with primary oral symptoms that would be confused with pulpal or peri-apical pathosis. In all cases, if the source is not of odontogenic origin, a careful and thorough examination of the teeth will typically rule out a dental etiology.
If a case of oral-facial pain is encountered for which no dental etiology can be found, the patient should be referred to an oral surgeon or physician for further evaluation. It is not the responsibility of the dentist to make the diagnosis or manage the treatment of such a case. It is the responsibility of the dentist to rule out a dental etiology and assist the patient in resolving the problem through an appropriate referral. To facilitate this problem-solving endeavor, various nonodontogenic pain scenarios will be presented in the
In the course of clinical practice, it is typical that pain is the reason many patients seek a consultation. Some symptoms are virtually diagnostic for pulpal and periapical pathosis. When a patient reports protracted pain that results from thermal stimulation, for example, there is a high likelihood it is of pulpal etiology; only the dental pulp is capable of such painful responses. The main diagnostic task is to find out which tooth is the problem.
In other cases, the history of symptoms is not so specific for pulpal or periapical pathosis. Through diagnostic proce-dures and radiographic interpretation described in Chapters 1 and 3, an etiology can usually be identified, or the facts can be narrowed for further assessment. Nevertheless, it is common to encounter patients with pain problems for which the etiology is quite elusive. It is the purpose of this chapter to discuss some of the most common and often perplexing oral-facial pain problems that are not attributable to teeth but are nonodontogenic in origin.
It is not the goal of this chapter to be encyclopedic. Other sources in the endodontic and dental literature have already described an extensive array of medical conditions from which oral and facial pain symptoms have occasionally been

120 chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain
manner they are most commonly encountered: thorough analysis of clinical cases.
Occlusal DiscrepanciesOcclusal discrepancies are a common source of patient dis-comfort. Many are not tooth related, but with data gathering and problem-solving techniques, the source of the patient’s distress can usually be identified and eliminated rapidly.
PROBLEM SOLVINGProblem: A 31-year-old female was referred for root canal treatment on her mandibular left first molar. She stated that she could not chew comfortably on the tooth. She had no thermal sensitivity and was not experiencing any spontaneous pain. A radiograph gave no evidence of dental caries, periapi-cal pathosis, or periodontal disease (Fig. 6-1). Pulp sensibility tests were performed on all the mandibular left posterior teeth, all of which responded normally to cold. Further inquiry indicated that 3 months earlier, a crown was placed on the first molar. The patient recalled that the symptoms actually began around that time. The occlusion was checked with articulating paper (Fig. 6-2), and a large premature contact was found. The occlusion was reduced and refined in this area, and the patient felt some immediate relief.
Discussion: An examination should always begin with an accurate and detailed history of symptoms. Occasionally the patient may not recall all pertinent details, or the clinician may follow a line of inquiry that initially does not reveal important clues. It is appropriate to treat the case as having a potential problem and perform usual tests to confirm or rule out a pulpal diagnosis that requires treatment. In this case, having performed tests, it was clear that the pulp was normal in all three teeth, and the pain was from another source. Since the only symptom has been sensitivity to occlusal pressure, it was logical to assess the occlusion, which proved to be the problem. A simple occlusal adjustment of the prematurity was the only treatment required.
PROBLEM SOLVINGProblem: A 53-year-old male was seen on referral. For several weeks, he had been unable to chew comfortably on the mandibular right first molar. When he awoke, there was usually a particular soreness in the tooth. He had not had recent dental treatment, and there was no history of thermal sensitivity. A radiograph indicated no caries, periapical patho-sis, or periodontal disease (Fig. 6-3). Full porcelain veneer crowns had been done approximately 10 years previously on the mandibular right posterior teeth. Pulp sensibility tests were limited to heat and cold, owing to the lack of exposed tooth structure necessary for an electric pulp test. Multiple tooth surfaces were tested, and each tooth was tested at least three times, with no responses to either hot or cold that would indicate a pulpal problem. Analysis of the occlusion with artic-ulating paper indicated heavy wear facets on almost all the posterior teeth including the first molar, yet this tooth was only mildly tender to percussion. Occlusal adjustment was performed on this tooth, and the patient related that there was an immediate improvement.
Discussion: This case differs from the first case in the fact that the presence of pulpal pathosis can neither be confirmed nor ruled out. It is inappropriate to proceed with root canal treatment, because there is no confirmation of pathosis. In this case, the occlusal adjustment is both a diagnostic proce-dure and a potential final treatment.
FIGuRE 6-1 Mandibular left first molar with symptoms of percussion tenderness.
FIGuRE 6-2 Almore articulating paper (Almore International Inc., Portland, OR, USA).
As for the prematurity found in the first case, occlusal adjustment may be the only treatment required. On the other hand, if sensitivity to percussion is of pulpal origin, (degen-erative or irreversible pulpitis), an occlusal adjustment will improve but not eliminate the problem. In time, more defini-tive signs or symptoms of pulpal pathosis will become appar-ent, with the potential for radiographic changes at the end of the root (increase in the width of the periodontal ligament space and loss of the lamina dura; see Chapter 3). If the tooth

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 121
FIGuRE 6-3 Mandibular right posterior teeth that fail to respond to all pulp tests. Only the first molar is percussion tender.
becomes increasingly sensitive or painful to percussion, the etiology would be primarily pulpal in origin, since occlusal contact has already been eliminated. Greater changes in the apical periodontal ligament space may also be seen radio-graphically, depending on the position of the root or roots in the bone.1,2 Under these circumstances, what also may have to be considered is a root or tooth fracture (see Chapters 4 and 5).
The appropriate course of action at this point is to wait and watch. The patient is now informed of the possible outcomes and should be encouraged to return if the symp-toms become worse at any point in the future. It is impossible to predict when a true pulp problem and its sequelae may evolve. It may occur in a relatively short period of time, such as a gradual increase in symptoms over a span of days, or it may not become apparent for months.
A B
C
FIGuRE 6-4 A, Immediate posttreatment radiograph of mandibular left first molar supplied by referring dentist. The chief complaint is continuing pain. B, Same tooth 10 months later. C, After 16 months, gutta-percha was removed from distal canal. There was no improvement in symptoms.

FIGuRE 6-5 Patient feels the pain along the inferior border of the mandible.
FIGuRE 6-6 No signs of tenderness or swelling around the teeth.
CLINICAL PROBLEMProblem: The patient was a 35-year-old female with a 17-month history of continuing pain following root canal treatment of the mandibular left first molar. A postoperative radiograph of treat-ment was provided by the referring dentist (Fig. 6-4, A). The fol-lowing history was also provided:Case HistoryReferring clinician notes: Root canal treatment was completed on the mandibular left first molar for “local swelling and the feeling of warmth” over the area of the apices. Following treatment, the symptoms persisted to the present time despite antibiotics, one complete retreatment/revision, and a third reopening to remove the filling material in the distal canal. This is the status of the tooth at present.
Patient-related information: Subsequent to the initial treat-ment, the symptoms resolved for a time then returned. The pain had been continuous in the area of initial treatment and was the same pain felt prior to treatment. At no time were there symp-toms specific to the tooth (i.e., cold, hot, or percussion sensitiv-ity). Ten months following treatment, a feeling of external swelling developed on the inferior border of the left mandible, which prompted a return to the dentist.
A radiograph was made on return to the treating dentist 10 months post treatment (see Fig. 6-4, B).
• On this date, antibiotics were prescribed.• Later in the same month, the dentist decided to do a com-
plete retreatment of the tooth.• Over the next 2 months or so, two more prescriptions for
antibiotics were given.• Neither the retreatment/revision nor the courses of antibi-
otics had any lasting effect.• Six months after her return, 16 months from the original
treatment, the patient returned again with the same complaint.
At this point, the dentist chose to remove the gutta-percha root filling from the distal canal, which was done on a subsequent visit 2 weeks later (see Fig. 6-4, C).
• Removal of the gutta-percha filling had no effect on this pain.• The patient was referred for specialist evaluation.
Clinical examination on referral appointment: The patient stated that the swelling had always been felt externally in the area along the inferior border of the mandible (Fig. 6-5). At no time was there any swelling noted intraorally, which was confirmed by the clini-cal examination (Fig. 6-6). There was no swelling or tenderness to palpation found lateral to the first molar or anywhere in the vestibule. Further clinical examination indicated there were no caries, no fracture lines, and normal periodontal probings. The other teeth in this quadrant responded normally to pulp sensibil-ity tests.
From a problem-solving standpoint, it is worthwhile to con-sider some important questions in establishing a tentative dif-ferential diagnosis: First, is there a tooth/pulp etiology for the pain in this case?
Discussion: A review of historical data reveals no evidence to support a diagnosis of pulpal pathosis other than the original conditions as stated by the dentist. There was no preoperative record of sensibility tests on the first molar, and the patient relates a history of symptoms uncharacteristic of pulpal or peri-apical pathosis. In addition, the history does not include any symptoms directly related to a tooth/pulp, such as an abnormal thermal response or sensitivity to percussion. A review of radio-graphs throughout the period of observation and treatment indi-cated a consistently normal apical periodontal ligament space around the apices of the first molar. The clinical findings indicated a remote location of discomfort relative to the alveolar arch. There was no evidence of pathosis in the vestibule lateral to the first molar, and the sensibility test responses on all adjacent teeth were normal, as were the periodontal probings. Conclusion: The patient’s problem is not related to the tooth or the treatment rendered.
Second, what are the diagnostic possibilities for oral and facial pain that might fit this dental history?
Discussion: Diagnostic possibilities are trigeminal neuralgia, atypical facial pain, and temporomandibular disorder.

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 123
found with laboratory or imaging studies.12 Frequently, psy-chiatric symptoms of depression and anxiety are also experi-enced by persons suffering this pain, further obscuring its etiology.
Although this entity would be a convenient solution to many diagnostic dilemmas, it is a relatively rare final diag-nosis. It would be appropriate to refer the patient for medical evaluation if such a diagnosis were suspected. In the case of the 35-year-old woman under consideration, there were clinical signs of pathosis. There was an area of palpation tenderness and the feeling of swelling in a consistent, well-differentiated area of the mandible. Conclusion: Atypical facial pain, or PIFP, can be confidently ruled out in this case.
Temporomandibular DisorderTemporomandibular disorder (TMD) is a complex entity that can involve chronic inflammation and pain in any or all of the following tissues: temporomandibular joint, teeth, and the muscles of mastication and associated tendons and liga-ments. There may also be degeneration of the articular sur-faces of the joint.15 TMD is a problem involving not only the hard and soft tissues but also the personality and is strongly influenced by social and environmental factors. It is not unusual to encounter older individuals with ample evi-dence of a long history of bruxing, who only recently have developed symptoms. Extraordinary stress is a typical precipi-tating factor. Because of the complexity of the subject, this descriptive section will focus on the types of signs and symp-toms that might be confused with pain of tooth/pulpal origin.
The majority of patients with TMD report symptoms associated with the muscles.12,15 The most common causes for muscle symptoms are overuse of the masticatory muscles through parafunctional habits such as bruxism or clenching. In the observations of the authors, the symptoms are almost invariably unilateral. Frequently, patients suffering from this pain are unaware of any tendency to clench or grind, giving credence to the probability that most of this activity occurs during sleep. For this reason, during a diagnostic inquiry, it is worth asking whether the patient is ever awakened from sleep with the pain or has pain on awakening in the morning. Another related symptom is the feeling of muscle fatigue. The masseter muscle is easy to palpate and can be found to be tender at either its origin or insertion, seldom both.
In reviewing the facts in the case of the 35-year-old woman presented in the Clinical Problem box, the examination indi-cated that the patient experienced swelling and pain over the insertion of the masseter. Anyone who does strenuous physi-cal work or exercises recognizes that a muscle exercised to the point of fatigue will become sore from lactic acid accumula-tion in addition to becoming hard, enlarged, and warm. This fits perfectly with the history of “local swelling and feeling warm,” and it explains why there are no intraoral signs or symptoms.
Trigeminal NeuralgiaTrigeminal neuralgia affects about 155 per 1 million people and most often occurs after the age of 50.12,17 Its devastating effects have been known for over 100 years, and a wide variety of attempts have been made to identify its etiology and deter-mine a successful treatment.5 It is unilateral and follows the distribution of either the mandibular or the maxillary branch of the trigeminal nerve, occasionally both. There is evidence that trigeminal neuralgia is also found in some people afflicted by disorders such as multiple sclerosis that affect the myelin sheath of the nerves.7,13
Trigeminal neuralgia is characterized by short episodes or bursts of pain described as intense and similar to electric shocks.3 Onset is usually random and unpredictable, but occasionally the sufferer will describe a “trigger zone,” an area of the face or a locus in the oral cavity that initiates the pain upon physical stimulation. This may occur during face washing, teeth brushing, experiencing a cold breeze, or simply moving the facial muscles. Painful attacks are not initiated by hot or cold stimulation of the teeth. Most often the diag-nosis can be recognized from the history, since the symptoms are unique compared to pain of pulpal or dental origin.
Episodes of pain with trigeminal neuralgia do not occur during sleep and usually last from a few seconds to a minute. There are no physical signs of pathosis, and pain is unrespon-sive to analgesics. Most often, the history and routine pulp tests will easily rule out the teeth as a cause. The importance of taking a complete history cannot be overemphasized. In many cases, the diagnosis of trigeminal neuralgia can be quickly ruled out on that basis alone.
In the case of the 35-year-old female described in the previous problem box, the pain is not spasmodic but lasts for extended periods of time. It is described as a continuous dull aching, and there has never been an episode of acute sharp pain. Physically, there is an area of tenderness externally, along the mandibular border, the palpation of which does not initiate the pain. Conclusion: Trigeminal neuralgia can be ruled out as an etiology for this patient.
Atypical Facial PainAtypical facial pain, also known as persistent idiopathic facial pain (PIFP), is a diagnosis that was introduced in the mid-1920s.8,10,11 It is basically a diagnosis of exclusion. If all other entities are ruled out, it must be atypical facial pain. Some neurologists believe the term falsely gives the patient a sense that they have a diagnosis, when in fact a better term might be undiagnosed facial pain. It is easy to see that this is not the place to start when attempting to diagnose an oral pain problem. The International Headache Society defines atypi-cal facial pain as pain that is present daily and persists most of the day. At onset, it is confined to a limited part of the face, is deep and poorly localized, is not associated with sensory loss or neural symptoms, and no abnormalities are

124 chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain
Further Observations on the Diagnosis of TMD: Maxillary SymptomsThere are far more patients with symptoms in the area of the origin of the masseter (the zygomatic process) than the insertion (the external inferior border of the mandible). The typical reason for referral to the endodontist is the presump-tion of periapical pathosis at the apices of the maxillary first molar. Once again, the chief complaints are soreness “over the apices,” tenderness to palpation, and often “swell-ing.” On clinical examination, in addition to the lack of evidence of pulpal disease and its extension to the support-ing bone, there is no palpation tenderness over the apices on the lateral surface of the maxilla (Fig. 6-7, A). Palpation should be continued laterally under the zygoma, with the area of tenderness typically found laterally on the anterior aspect of the zygoma (see Fig. 6-7, B [arrow] ). This can
The bruxing or clenching habit is characterized by periods of symptoms lasting days or weeks interspersed with periods of relative comfort. When interviewed about their history, many patients will recall that symptoms have come and gone over a long period of time. Clearly these findings are vastly different from what is identified with pulpal pathosis that develops rapidly and localizes to a specific tooth. Even in cases of pulpal degeneration that develop over a longer time frame, there is an ultimate progression to a more acute and localized condition.
Conclusion: The patient described in the Clinical Problem box is most likely suffering from chronic TMD manifesting in the left masticatory muscles. There may or may not have been any indication to perform root canal treatment on the mandibular molar in this case, though at this point, it was necessary to complete what had been initiated. The definitive treatment for her symptoms at this point would be treatment for TMD.
A B
C D
FIGuRE 6-7 A, No palpation tenderness over the apices of the teeth. B, Anatomically, there is an approximate distance of 1 cm between the facial surface of bone over the apices and the prominence of the zygomatic arch. C, Palpation tenderness is frequently found over the anterior zygomatic arch. D, The location of the palpation tenderness intraorally is the attachment of the masseter muscle to the anterior aspect of the zygomatic arch.

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 125
FIGuRE 6-8 Physical signs of bruxism are often lacking in younger people.
be felt both intraorally and externally (see Fig. 6-7, C and D).
Dental Signs of Temporomandibular DisorderThe teeth are valuable resources for diagnostic signs of TMD as well as being the objects of its destructive effects. Some patients, usually the young, may present without visual evi-dence of bruxism or clenching (Fig. 6-8). The typical older sufferer, however, will usually exhibit signs such as wear facets, coronal facture lines, multiple fractured cusps, and pitting of gold restorations (Fig. 6-9, A to D).
A B
C D
FIGuRE 6-9 A, Wear patterns and facets of bruxism. B, Coronal fracture lines. C, Broken cusps. D, Pitting on occlusal surfaces of gold restorations.
Dental Symptoms of Temporomandibular DisorderIn addition to the restorative problems like wear and cuspal fractures, TMD often is the cause of deep coronal fractures which affect the pulp. Coronal fractures can lead to acute pulpitis or pulpal necrosis (Fig. 6-10). They can occasion-ally extend well beyond the pulp chamber level and cause periodontal bone loss (Fig. 6-11). After an evaluation of the oral soft tissues, a clinical examination should always evaluate all aspects of the teeth and not just focus on the presence or absence of caries. The history, pulp tests, and radiographs will confirm or rule out endodontic pathosis. More than likely, a patient with pulpal disease from a coronal fracture of TMD origin will have symptoms of both problems.
The usual dental symptom of TMD is sensitivity to occlu-sal pressure, which may present as sensitivity only from verti-cal pressure or only from lateral pressure or both. A single tooth may be affected or several teeth in the posterior sextant. Discomfort from vertical pressure typically only occurs from a heavy or premature contact in centric occlusion. Lateral sensitivity typically occurs from heavy or premature contact in lateral excursion, particularly on balancing-side inclined planes. These nuances can be easily tested. Devices like the Tooth Slooth (Professional Results Inc., Laguna Niguel, CA, USA) are available for testing occlusal sensitivity (Fig. 6-12, A). These tests can also be done with a cotton applicator (see Fig. 6-12, B) and temporary stopping (see Fig. 6-12, C).

126 chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain
FIGuRE 6-10 Endodontic complications associated with coronal fractures. Transillumination for confirmation of deep fractures.
A
B
C
FIGuRE 6-11 A, Periodontal abscess associated with a deep coronal fracture. B, Coronal fracture extending past the periodontal attachment, causing infrabony defects similar to lesions of advanced periodontitis. C, Transillumination of the fracture line in the tooth depicted in A and B.
A
B
C
FIGuRE 6-12 A, Occlusal pressure testing with the Tooth Slooth. B, Testing with the wood handle of a cotton applicator. C, Testing with dental stopping.
Stopping has some advantages in that both vertical and lateral occlusal forces can be analyzed independently.
It usually helps the process of testing to start on the unaf-fected side as a demonstration. The patient is instructed to bite through the stopping like biting through a nut (Fig. 6-13). First, the fact that the material is somewhat soft gives qualitative information relative to the degree of pain. If, for example, the patient cannot bite on the material at all, the pain problem is severe, possibly an indication of pulpal pathosis. If there is visual evidence of coronal fracture, pain on biting through the stopping may separate the fracture slightly. This will cause acute pain of pulpal origin if the pulp is vital. It will also cause acute pain in the periodontal liga-ment. The patient will seldom be able to bite with much

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 127
A BB
FIGuRE 6-13 A, Assessment of relative occlusal pressure sensitivity tooth by tooth. B, Testing whether the patient is able to bite through the material at all in a vertical direction only.
A B
FIGuRE 6-14 A, Testing whether the patient can grind laterally on the material in left excursion. B, Grinding in right lateral excursion.
A B
FIGuRE 6-15 A, Articulating paper revealing a heavy wear facet on the distobuccal cusp. B, After reduction of heavy contacts only.
pressure on the material. Conversely, most people who have pain on occlusion from TMD will be able to slowly bite through the material. A symptom-free tooth will have no pain biting forcibly through the stopping.
Second, the direction of bite force can be tested. If the patient can bite through the material but cannot tolerate moving in lateral excursion while maintaining the bite on the
material, the tooth will probably need adjustment of the balancing-side cusps (Fig. 6-14).
Once the painful teeth are identified and the direction of pain has been determined, articulating paper can be used to identify the contact that needs adjustment (Fig. 6-15). A selection of stones and finishing burs will be needed to relieve the occlusal contacts (Fig. 6-16).

128 chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain
FIGuRE 6-16 A selection of stones, diamonds, and finishing burs are for occlusal adjustment. It is also appropriate to polish areas which have been ground.
only in centric occlusion. After marking the occlusion with the articulating paper, have the patient tap only vertically. Once the contacts have been identified, a finishing bur or a diamond bur (for porcelain) should be used to reduce the heaviest centric contacts. In addition, large surface-area con-tacts should be reduced to small areas. It is not the objective to eliminate all contact completely. After the initial reduc-tion, another check is done with the paper. If necessary, the procedure is repeated until the contacts are relatively uniform on all teeth (Fig. 6-17). Next, the procedure is repeated by having the patient clench and grind in lateral excursion. Balancing-side contacts should be eliminated, and heavy contacts on the functioning cusps should be reduced (Fig. 6-18).
The strategy of occlusal adjustment will generally alleviate the symptoms of occlusal pressure pain, but some patients will need additional support for relief.16 The night guard or occlusal appliance is relatively easy and inexpensive to fabri-cate (Fig. 6-19).
A
B C
FIGuRE 6-17 A, Pretreatment photo showing heavy wear facets on mandibular left first and second molars. B, Occlusal contacts marked in centric occlusion first. Instruct the patient not to grind at this point. C, Centric contacts reduced; large areas of contact reduced to small areas of contact. Note heavy contact on distal marginal ridge of second premolar. This should be reduced from a “doughnut” or circular mark to a contact similar to what has been produced on the molars.
Treatment of Heavy Occlusal Contacts and Prematurities
The general approach to the treatment of occlusion-induced pain is reduction of the occlusal contacts. It is best to begin

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 129
A
B C
FIGuRE 6-18 A, Preoperative view of a percussion-tender maxillary left second molar. B, Marking of heavy occlusal contacts with articulating paper. Note heavy contact on balancing (buccal) cusps. C, Posttreatment photo demonstrating elimination of balancing-side contacts and reduction of centric contacts to smaller areas.
A B
FIGuRE 6-19 A, Rigid night guard. B, Night guard in place. If the patient already has a night guard and continues to have symptoms, the night guard should be examined with articulating paper and the occlusion should be adjusted.
Additional and Effective Pain-Relieving Strategies
• Educate the patient about the relationship between stress and TMD. Knowledge can help reduce the symptoms and the stress caused by them. The patient may be able to reduce stress or at least see an end to their present circumstances.
• Hot, moist compresses over the masseter may increase circulation and relieve the ache, in conjunction with the short-term use of prescription-strength NSAIDs (800 mg
ibuprofen every 6 hours). Many patients will experience rapid relief.
• Also for short periods of time, a prescription for muscle relaxants may provide relief, especially at night.
Maxillary SinusitisWhen patients present with symptoms primarily in the maxilla, maxillary sinusitis must be included in the initial differential diagnosis. While an odontogenic etiology accounts for 10% to 12% of the maxillary cases of diagnosed

130 chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain
sinusitis,4,12,14 sinus infections can also give rise to generalized tooth pain that is often mistaken for a pulpitis. Sinusitis may be due to either a bacterial infection or an allergen. With an acute infectious maxillary sinus, there will usually be an acute ache in the dentition in close proximity or contact with the sinus floor. Percussion tenderness is common on all teeth in a specific quadrant. Once again, pulp-testing procedures will most often rule out the dentition as the etiology. There may be an increase in thermal sensitivity, but the teeth will still respond within normal limits. Radiographically, the sinus will appear cloudy or completely radiopaque (Fig. 6-20).
Cases of allergic sinusitis are more difficult to diagnose, although it is generally easy to rule out the teeth with the usual tests. Allergic inflammation of the sinus membrane will result in a thickening of the lining on the films, but this finding cannot confirm the etiology of the pain, since most sinus cavities with thickened membranes are asymptomatic. Patients report a dull, continuous ache in the posterior area, and the teeth usually do not develop tenderness to percus-sion. The most convincing aspect in making the diagnosis of allergic sinusitis is its occurrence in springtime when other allergic conditions are also on the increase.
Other Etiologies of Pain in the Oral Cavity and Head
The remaining list of pain-inducing pathologic entities are known to cause facial pain.12 Generally these entities will not present with oral or specifically pulpal-type pain, especially as the primary or initial symptom. In fact, dental symptoms are rare for most of these lesions. In any case, routine testing of the dentition should rule out a dental etiology if there is any question.
• Cluster headache—severe unilateral pain is located around the eye (photophobia), comes in groups, and is debilitating.
FIGuRE 6-20 A periapical radiograph indicating a cloudy sinus cavity consistent with maxillary sinusitis. Patient should be referred to the physician.
• Cardiogenic—affects the left mandible and is an extension of the area commonly affected by angina pectoris. It is caused by ischemia of the coronary arteries.
• Sialolithiasis—blockage of a salivary duct. Most often the primary symptom is swelling of the gland, especially at mealtime. Commonly found in Stensen’s duct adjacent to the maxillary posterior teeth.
• Neoplasm—pain will depend on location and tissues involved, but other signs and symptoms will make confusion with endodontic pathosis extremely unlikely but not impossible.9
• Otitis media—pain and signs of pathosis will be localized in the affected ear. Will not be a diagnostic challenge for the physician.
• Post herpetic—a significant facial pain problem that follows about 20% of cases of infection with herpes zoster (shingles). Patients with this problem will have already suffered through the disease.
Pulpal pathosis is the most common cause of oral and facial pain. There are several nonpulpal pathologic entities that can also cause symptoms of oral and facial pain; TMD is the most common. In fact, in the experience of the authors, it is the most common nonendodontic reason for referral to a specialist for evaluation. The diagnostic procedures and treatment strategies have been presented.
Should a patient present with a painful problem that does not fall into one of these diagnostic categories, a presumptive diagnosis can be made, but the task of final diagnosis should be left to specialists in the fields of oral maxillofacial surgery or medicine. The appropriate task of the dentist is to rule out a possible dental etiology, if possible make a tentative diag-nosis, and refer the patient for evaluation.
ReFeRenceS1. Bender IB, Seltzer S: Roentgenographic and direct observation of
experimental lesions in bone: I 1961, J Endod 29:702-706, 2003.2. Bender IB, Seltzer S: Roentgenographic and direct observation of
experimental lesions in bone: II 1961, J Endod 29:707-712, 2003.3. Bennetto L, Patel NK, Guller G: Trigeminal neuralgia and its
management, Br Med J 334(7586):201-205, 2007.4. Brook I: Sinusitis of odontogenic origin, Otolaryngol Head Neck
Surg 135:349-355, 2006.5. Brophy TW: Oral surgery—a treatise on the diseases, injuries and
malformations of the mouth and associated parts, Philadelphia, 1915. P. Blakiston’s Sons & Co.
6. Buckley JP: Modern dental materia medica, pharmacology and therapeutics, ed 2, Philadelphia, 1910, P. Balkiston’s Son & Co.
7. Cruccu G, Biasiotta A, Di Rezze S, et al: Trigeminal neuralgia and pain related to multiple sclerosis, Pain 143:186-191, 2009.
8. Frazier CH: Pain phenomena in the face, Brit Dent J 46:1169-1170, 1925.
9. Gutmann JL, Tillman JL: Rhabdomyosarcoma of the maxillary antrum: a case report, J Endod 2:250-252, 1976.
10. Harrison SD, Balawi SA, Feinmann C, et al: Atypical facial pain: a double-blind placebo-controlled crossover pilot study of subcu-taneous sumatriptan, Eur Neuropsychopharmacol 7(2):83-88, 1997.

chapter 6 | Problem Solving in the Diagnosis of Nonodontogenic Pain 131
11. Headache Classification Subcommittee of the International Head-ache Society: The international classification of headache disorders: 2nd edition, Cephalalgia 24(Suppl 1):9-160, 2004.
12. Jaeger BJ, Reyes MR: Non-odontogenic toothache and chronic head and neck pain. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker, Inc.
13. Jensen TS, Rasmussen P, Reske-Nielsen E: Association of trigemi-nal neuralgia with multiple sclerosis: clinical and pathological fea-tures, Acta Neurol Scand 65:182-189, 1982.
14. Mehra P, Jeong D: Maxillary sinusitis of odontogenic origin, Curr Allergy Asthma Rep 9:238-243, 2009.
15. Okeson JP: Management of temporomandibular disorders and occlusion, ed 5, St. Louis, 2003, Mosby.
16. Patel K, Hemmings KW, Vaughan S: The provision of occlusal splints in primary dental care, Prim Dent Care 7(3):109-113, 2000.
17. van Kleef M, van Genderen WE, Narouze S, et al: 1.Trigeminal neuralgia, Pain Pract 9(4):252-259, 2009.
RecOMMenDeD ADDiTiOnAl ReADingGibbs JL, Hargreaves KM: Mechanisms of odontogenic and non-
odontogenic pain. In Ingle JI, Bakland LK, Baumgartner JC (eds): Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker Inc.
Mattscheck D, Law A: The nonodontogenic toothache. In Cohen S, Hargreaves KM (eds): Pathways of the pulp, ed 9, St Louis, 2006, Mosby.
Ram S, Teruel A, Kumar SKS, et al: Clinical characteristics and diag-nosis of atypical odontalgia, J Am Dent Assoc 140:223-228, 2009.

132
The task of keeping alive the exposed healthy pulp demands an undamaged pulp, capable of reacting to treatment. Damage to the enamel, be it of a chemical, mechanical, or bacterial nature and to a greater degree similar damage to the dentine of the tooth, may affect the pulp and the adjoining odontoblasts. Apart from caries prophylaxis and the early treatment of carious defects in the human dentition, dental treatment if carried out with the necessary understanding of the basic physiology of the dental tissue, can often keep alive the vital pulp of the tooth, which as an organ for nourishing and registering stimulation has to fulfill an important function.38
W. Hess, 1950
Problem-Solving ListProblem-solving challenges and concerns with dentin hypersensitivity and vital pulp therapy addressed in this chapter are:
Dentin Hypersensitivity: Patient Considerations, etiologies, and Treatment Issues from an endodontic Viewpoint
Directives for Considering Vital Pulp Therapy
Are vital treatment procedures viable options in contemporary dentistry?
When is treatment of the vital pulp preferable to root canal treatment?
When is root canal treatment preferable to vital pulp treatment procedures?
Materials for Vital Pulp Therapy
Treatment Modalities to Maintain Pulpal Vitality
Stepwise excavation and indirect pulp capping
Indirect pulp cap
Direct pulp cap
Pulpotomy procedures
part 2 Problem-Solving Treatment Procedures in Nonsurgical Root Canal Procedures
Chapter 7
Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
Dentin Hypersensitivity: Patient Considerations, Etiologies, and Treatment Issues from an Endodontic Viewpoint
One of the more challenging problems to deal with in den-tistry is to maintain teeth in symptom-free function over the life of the patient. Over time through normal wear, function, and maintenance, some teeth create a “sensitivity” problem for the patient to a point where the patient is alerted to teeth
that give them a shooting sensation, a tingling sensation, sometimes a painful sensation, or at times just a different feeling during normal daily activities. The teeth may or may not be painful, depending on the patient’s perception, pain threshold, and emotional and physical factors.52 Yet they grab the patient’s attention when they ingest certain foods or liquids, chew, brush their teeth, and even just take in a cool breath. For the patient, the quality of life, defined in this case as a pain-free oral cavity, has been altered.
In some cases, the patient can identify the problem tooth and go directly to the sensitive part of it; in other situations, the problem is not focused and rather vague but very real. Daily, these patients are referred for an endodontic evalua-tion or are sent to have root canal treatment. In most cir-cumstances, root canal treatment is unwarranted, but the patient feels that their dentist does not know what to do about the sensitivity that is present and has been for a period

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 133
groove of posterior teeth, with exposed dentin beneath the groove; or the presence of giant dentinal tubules36,75,76 on a cusp tip for which there was no enamel covering or enamel has worn away.
5. A small area of initial or recurrent caries that cannot be readily identified.
6. Identifiable abfractions, attritions, abrasions, and erosions.9,10,64
7. Vital tooth bleaching.35,37,39,55,70
The two most common etiologies have been identified as gingival recession and attrition,9 but this should not bias the clinician. Exhaustive evaluation of the patient’s problem is warranted because different patient populations may present with a much wider range of etiologic factors. For example, recession or tooth wear that may be identified as etiologies may in themselves be caused by acid diets and irregular or excessive tooth-brushing habits.2 Moreover, the overwhelm-ing consumer craze for teeth whitening has contributed greatly to dentin hypersensitivity.39
With the first etiology, a simple evaluation using a fiber-optics (transillumination),47,72 biting tests, and magnifica-tion23 can determine the extent of the problem and a possible solution (see Chapters 1, 3, and 4). In the second situation, simple desensitization procedures are indicated.7,45,46,59 With etiologic factors 3 through 6, simple restorative procedures and possible changes in oral home-care practices would be advised. In the last scenario, vital bleaching, desensitization would seem to be the treatment of choice.20,37,39 Without supporting data and a diagnosis to indicate that root canal treatment is warranted, the patient should not be subjected to needless procedures.20 A final procedure that may in time serve to provide rapid and lasting desensitization for the patient is the use of lasers. There has been limited success thus far, but their use to block the permeability of dentinal tubules on a predictable basis seems both reasonable and attainable67 (see Recommended Additional Reading).
Desensitization techniques and minimally invasive proce-dures to eliminate the patient’s hypersensitivity would seem to be the treatments of choice to manage the patient’s chief complaint in these situations. This approach goes hand in hand with the initial phases of vital pulp therapy. Many clini-cians may not identify this approach to management as being within the scope of endodontics, because too often endodon-tics and the everyday use of the term are erroneously equated only with root canal treatment. Treatment modalities for vital pulp therapy do fall within the scope of endodontics and should be considered first before doing a root canal procedure.33
Directives for Considering Vital Pulp Therapy
It is a reasonable goal of endodontic research to seek diagnos-tic and treatment methods that more predictably determine
of time. A root canal procedure will certainly solve the problem. This is the quick fix and unfortunately occurs in many private-practice settings. However, the real question is whether this degree of treatment is truly indicated and in the best interest of the patient. In the bigger picture, the patient needs a diagnosis and treatment plan to maintain the vitality of the dental pulp in a particular tooth or teeth and if possible to restore symptom-free function.20 This approach to the problem is neglected or simply cast aside when even more extensive insults to the tooth in the form of a crown or root canal treatment and crown are offered. This is the antithesis to problem solving and turns dental treatment planning and treatment into nothing more than a technical trade that provides an identified service for a fee. Such “care” is driven by business models that dictate the need to treat with high-end services to be profitable, as opposed to managing patients’ problems in a preventive manner that maintains both tooth integrity and symptom-free function whenever possible. In dental practices that are run as managed profit centers, an investigative, compassionate, and caring approach may not be a priority that ensures the bottom line of fiscal solvency.
Tooth hypersensitivity, or more frequently identified as dentin hypersensitivity, is defined as a short pain arising from exposed dentin in response to stimuli. Typically, thermal, evaporative, tactile, osmotic, or chemical stimuli produce responses which cannot be ascribed to any other form of dental defect or disease3,26 (except for incipient, undiagnosed, or unidentified caries). Mostly, the sensations dissipate quickly and completely when the stimulus is removed. While many theories have been proposed for this problem (see Recommended Additional Readings at the end of this chapter), the most likely is a change in fluid flow with the dentinal tubules that excites neural endings at the pulpal-dentin interface (classic hydrodynamic theory).3,19,29,62 The size and patency of the dentinal tubules also have a direct bearing on the degree of sensitivity.41 Essential to patient management in these situations is (1) an understanding of what causes dentin hypersensitivity, (2) a thorough clinical assessment and identification of the etiologic factors, and (3) a diagnosis and reasonable treatment plan.13 Common etiolo-gies for this malady have been identified as:
1. A small crack in the tooth that exposes dentinal tubules.12
2. An area of dentinal tubule exposure along the cervical line at or slightly below the crest of free gingival. This may be due to wear; to gingival recession1,2,9 with exposed tubules at an incompletely sealed, abnormal cemental-enamel interface* or as a result of cemental agenesis48; or due to tissue shrinkage subsequent to periodontal surgery.41
3. A leaking margin around a restoration or a cracked restoration exposing dentinal tubules.12
4. An occlusal area in which the inner slopes of the enamel have not fused in the region of the central
*References 16, 21, 31, 36, 57, 75, and 76.

134 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
hemorrhage is normal and will usually slow with sterile water, saline, or sodium hypochlorite lavage.60,71 The use of chlorhexidine has also been shown to be effective in these situations.60 Care must be taken to not probe into the expo-sure or otherwise mechanically irritate the pulp. The prepara-tion should be kept moist because desiccation is a strong irritant to the vital pulp.69 If the hemorrhage is profuse, the prognosis for maintaining pulpal vitality by pulp capping is poor. The use of strong hemostatic agents such as ferric sulfate or racemic epinephrine should not be used; the infu-sion of strong chemicals into the blood clot that forms may be deleterious to the pulp.69
When Is Treatment of the Vital Pulp Preferable to Root Canal Treatment?Possibly the most important indication for vital treatment procedures is in the case of pulpal exposures on teeth with incomplete root formation. In these cases, preservation of pulpal vitality is an essential objective for all exposures—whether traumatic, mechanical, or carious—to permit normal apexo-genesis. Removal of the pulp immediately eliminates the pos-sibility of further root development, leaving the root canal with an open apex and the root itself with thin dentinal walls that cannot undergo thickening, owing to loss of the radicular pulp. Root canal procedures in teeth with open, immature apices are more complicated, more time consuming, and less predictable in terms of outcome. Teeth with large-diameter
the status of the dental pulp and preserve the vitality of the pulp under all conditions, especially when the vital pulp has exposed. Preserving pulpal vitality would have several advan-tages. The current techniques of vital pulp capping or pulp-otomy are much less complicated and time consuming than root canal procedures. From a public health perspective, reduction of the number of teeth requiring root canal treat-ment would lessen the economic burden of dental care and increase tooth retention.42,49 In the lower-income sectors of the economy on a global basis, the choice of a root canal procedure is currently not a viable option.
Are Vital Treatment Procedures Viable Options in Contemporary Dentistry?Yes, pulp capping can play a major role in pulp and tooth reten-tion. Recent studies have provided a great insight into the pulpal responses to irritants (see Recommended Readings). Early, careful intervention to eliminate the etiologies for pulpal disease and prevent further damage to the pulp generally yields a positive outcome.54 Research confirms the inherent capability of the dental pulp to heal, but at this point—with the currently avail-able imprecise methods of pulpal assessment, variations in opera-tive techniques, and variety of pulp treatment materials—there are limitations to an ideal response.
When challenged by irritants, the pulp has an amazing capacity to form a hard, reparative tissue, sometimes in the form of its original tissue, tubular dentin (Fig. 7-1), and sometimes in the form of a gnarled, irregular or irritational dentin (Fig. 7-2, A). The nature and intensity of the insult and the host’s response will usually determine the nature of the reparative tissue. The pulp tries to stand its ground, so to speak, by forming a calciotraumatic line to block the ingress of both bacterial toxins and bacteria themselves (see Fig. 7-2, B).
Ideally, the clinician should strive to prevent a pulpal exposure, especially under optimal conditions when there are no signs or symptoms of pulpal pathosis. A step-wise approach to caries excavation known as an indirect pulp cap is one possible treatment option that may prevent an expo-sure and allow for remineralization of the affected dentin or stimulate the formation of dentinal sclerosis and irrita-tional dentin.18,54,73 Unfortunately, there is no correlation between symptoms and the degree to which the pulp may be affected by the invasion of caries. The extent to which bacteria may have invaded the pulp cannot be determined preoperatively. Nevertheless, the pulp possesses some capa-bility to respond favorably even in the presence of bacteria (Fig. 7-3).
When signs or symptoms are not of consideration and an exposure occurs, the visual appearance of the exposure (Fig. 7-4, A) and the amount of hemorrhage (see Fig. 7-4, B) must be assessed. Small exposures would have a better prognosis than large or multiple exposures. A small amount of
FIGURe 7-1 Normal tubular dentin showing mineralized, unmineralized, and partially mineralized dentin.

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 135
canals and thin-walled roots are more prone to fractures of all types.5,27,28,72
Fortunately, the pulps of teeth with immature root formation have a more generous blood supply than teeth with fully formed roots and apical closure. As a consequence, they are more tolerant
A BA B
FIGURe 7-2 A, Gnarled dentin in apposition to normal dentin. B, Gnarled, irregular, irritational dentin (left) with evidence of the calciotraumatic line. Note normal dentin (right) and bacteria that have penetrated the tubules.
FIGURe 7-3 Irregular, irritational dentin (left), presence of the calciotraumatic line, and bacteria in the tubules. Note how some of the bacteria have passed through the calciotraumatic line into tubules that formed with the irritational dentin.
of injury and exposure to microorganisms. Vital treatment pro-cedures are far more likely to succeed in teeth with open, imma-ture apical development than in teeth with mature root formation. With these factors in mind, vital techniques should be considered even when symptoms of pulpitis are present.
There is growing evidence that vital pulp treatment is effective for carious exposures on permanent teeth. Clinicians must remember that a carious exposure does not necessarily imply that bacteria actually reached the dental pulp. Often the demineralized front of dentin that contains bacterial byproducts has reached the pulp, but not the bacteria them-selves. Studies have found that with techniques to be described, both direct pulp caps and coronal pulpotomies can preserve pulpal vitality with a very high degree of predict-ability.11,17,32,33 Although the majority of patients in these studies were in the 10- to 13-year age range, one study included cases with patients as old as 45.17 These findings open up new and exciting avenues of research. With currently available materials and the potential of more new develop-ments, vital therapy in many cases of carious exposure may be a viable and predictable treatment option in the future.24
When Is Root Canal Treatment Preferable to Vital Pulp Treatment Procedures?Preoperative pulp sensibility testing would be appropriate for teeth with large carious lesions, but some teeth may respond posi-tively to tests and still have localized intrapulpal inflammation and tissue degeneration. Factors that have been cited as

PROBLEM SOLVINGProblem: A 9-year-old male was brought to the dentist with a fractured maxillary right central incisor. The tooth had symptoms of irreversible pulpitis. There were prolonged pain reactions to cold, and the patient had experienced episodes of moderate spontaneous pain relieved by over-the-counter analgesics. The parent related that the tooth was fractured in a playground acci-dent at school a month earlier. There had been little pain initially, and because of the Christmas holidays, no treatment was sought. Clinical examination indicated a complete midcoronal horizontal fracture with exposure of the coronal pulp. The periapical film indicated that the tooth had an open, immature apex and the apical periodontal ligament space was widened 2 to 3 mm more coronally than what would be typical of a normal physiologic apical formation (Fig. 7-5, A).
Solution: Although the symptoms and radiographic appear-ance of the periapical tissues suggested an irreversible pulpitis, the potential problems associated with root canal treatment of the open apex highlighted the need to consider a form of vital therapy. A direct pulp cap (partial pulpotomy, also known as the Cvek technique), was performed with calcium hydroxide,25 in which a sterile high-speed diamond bur is used under copious water irrigation to surgically excise the inflamed pulp tissue. The
excision is considered complete when the pulp stump no longer bleeds profusely. The intent is to remove the contaminated, degenerating tissue and create a new surgical wound that will respond favorably to the placement of calcium hydroxide. The pulp cap was covered and sealed with an amalgam restoration (see Fig. 7-5, B). Postoperatively, the symptoms gradually resolved. Sensibility testing in the subsequent months indicated a return to normal pulpal responses. One year later, a reevaluation radio-graph indicated normal physiologic completion of apical forma-tion (see Fig. 7-5, C). Root canal treatment was then completed in preparation for a post-retained restoration.
Discussion: This case was treated more than 30 years ago with materials available at the time, which were limited. Fortunately, the choice of materials has improved, and the prognosis for pulpal healing has improved as well. Nevertheless, the preoperative con-ditions were no different than many cases today, so this case illustrates the reparative potential of pulp tissue in teeth that exhibit immature root development. Had this treatment approach failed, apexification (techniques for nonvital pulps) would have been indicated (see Chapter 13), which 30 years ago would have consisted of multiple applications of calcium hydroxide over an 18- to 24-month period of time.28
A B C
FIGURe 7-5 A, Traumatic fracture of a maxillary right central incisor in a 9-year-old boy. The tooth was examined approximately 1 month after the accident and was symptomatic of irreversible pulpitis. B, Postoperative radiograph of Cvek pulpotomy with calcium hydroxide. C, One-year reevaluation radiograph. The tooth responded normally to pulp testing, and the apex was closed.
A B
FIGURe 7-4 A, Mechanical exposure of a presumed normal pulp with no hemorrhage or exudates. B, Carious exposure of a pulp with hemorrhagic exudates.

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 137
FIGURe 7-6 Exposure of a pulp with an intrapulpal abscess and purulent exudate.
In teeth with mature root formation, caries extending directly into the pulp, resulting in multiple exposures or complete unroof-ing of the pulp chamber, would be indicated for pulpectomy and root canal treatment (Fig. 7-7, A and B).
Materials for Vital Pulp Therapy
Historically, the standard material indicated for both indi-rect and direct pulp capping has been calcium hydroxide.38 In the treatment regimen of indirect pulp capping, calcium hydroxide has been shown to cause remineralization of affected (but not infected) dentin while maintaining pulpal vitality.50 Application of this material to direct pulp expo-sures usually results in a relatively symptom-free postopera-tive course, with gradual dentinal bridging of variable type and quality over the exposure site. Unfortunately, calcium hydroxide use is associated with a potential risk of continued calcification of the entire root canal system. Histologically, this is a very irregular process, leaving portions of the canal spaces that may not be visible radiographically. Despite a lack of symptoms or radiographic evidence of apical patho-sis, it is unwise to conclude that the canal space is com-pletely calcified to the apex and that root canal treatment will never be required (Fig. 7-8, A). The pulp tissue in these spaces often degenerates and becomes necrotic at highly variable lengths of time postoperatively. Signs and symp-toms of apical inflammation or apical lesions may develop from a few years to decades after the pulp capping procedure.
Some teeth that appear to have calcified canals may in fact have canal spaces that can be penetrated and successfully treated (see Fig. 7-8, B). The techniques for treating these difficult cases are discussed in Chapter 13. Unfortunately, calcium hydroxide used in either a direct pulp cap (Fig. 7-9, A) or pulpotomy (see Fig. 7-9, B) may stimulate significant calcification to a point where the tooth may be untreatable with nonsurgical techniques.
Mineral trioxide aggregate (MTA) was introduced in the mid-1990s.74 Marketed under the name Pro-Root MTA (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), it is essentially a derivative of Portland cement (Fig. 7-10). The original formulation was gray and discolored anterior teeth, so a white formulation was subsequently introduced. This material has withstood the rigor of extensive histologic inves-tigation as a pulp capping and pulpotomy material. One study using human third molars compared dentinal bridging of pulp exposures using MTA and calcium hydroxide. The teeth were extracted after 2 months and examined histologi-cally and histochemically. Dentinal bridging was observed in 100% of MTA cases but only 60% of calcium hydroxide cases.53 Furthermore, less dystrophic calcification has gener-ally been observed with MTA than with calcium hydroxide. MTA has been shown to have a much better success rate than traditional formocresol for pulpotomies in primary teeth4,32
A
B
FIGURe 7-7 A, Clinical photograph of a severely carious mandibular right first molar. B, Radiograph of same tooth. This molar is indicated for root canal treatment.
indications for pulpectomy are uncontrollable hemorrhage from the exposure site,51 purulent exudates emanating from the expo-sure site, and complete lack of bleeding. Purulent exudate (Fig. 7-6) would indicate an intrapulpal abscess for which no evidence exists that suggests a positive outcome for either pulp capping or pulpotomy. Similarly, if the exposure site is pale yellow and without hemorrhage or exudates of any type, the pulp may already be partially necrotic.

138 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
A B
A B
FIGURe 7-8 A, Mandibular right second premolar with apparent calcification of the root canal when viewed radiographically. It would appear no pathosis could develop in this tooth. B, The completed root canal treatment following the onset of acute apical periodontitis. The canal was very small but patent to the apex.
FIGURe 7-9 A, Severe dystrophic calcification of a mandibular left first molar after a calcium hydroxide pulp cap. B, Severe dystrophic calcification of a mandibular left first molar after a calcium hydroxide pulpotomy.
FIGURe 7-10 Mineral trioxide aggregate (MTA) marketed as ProRoot in the original gray formulation. (Courtesy Dentsply.)
and is now recommended as the material of choice for pulp-otomies in primary teeth.34,68
The use of MTA in pulpotomies on permanent teeth has also been studied clinically.11,30,78,79 The findings compare favorably with the results of MTA pulpotomies in primary teeth and are more favorable when calcium hydroxide is used.30 MTA has also been studied clinically as a direct pulp capping agent,17,79 and excellent clinical responses17 have been noted, with the majority of teeth responding normally to sensibility testing.
The clinical preference for either gray or white MTA has been controversial, but data that support significant differ-ences in the outcomes are limited.4 Only white MTA is presently available in the United States. Other countries have begun to produce various versions of the gray material. However, the physical make-up of the powder may not be micronized or have its impurities removed, in addition to being a little more challenging to mix and place. There has

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 139
A
B C
FIGURe 7-11 A and B, Preparation of mineral trioxide aggregate (MTA) by mixing MTA powder with water. C, Excess water may be removed with a cotton roll.
been a major global research and development impetus for a more user-friendly MTA with better mixing, manipulating, placing, compacting, and setting-speed properties.
The MTA powder is mixed with water into a thick paste (Fig. 7-11, A and B). Setting time is lengthy, so the material can be carried to the prepared tooth with any spoonlike instru-ment. For pulp capping procedures (e.g., open excavation), a rather wet mix will flow easily over the exposed pulp. Bleeding should be controlled by rinsing with sterile water, saline, or sodium hypochlorite. If the mix contains too much water, the excess may be removed by blotting with a cotton roll on the mixing pad (see Fig. 7-11, C) or with dry cotton pellets in the tooth. A drier mix is preferred for placement into smaller preparations (described later in the partial pulpotomy tech-nique, Cvek pulpotomy).27 Special tools are available for car-rying and placement of this material (see Chapter 16).
Treatment Modalities to Maintain Pulpal Vitality
Stepwise Excavation and Indirect Pulp CappingSubstantial research evidence supports indirect pulp capping as a viable and successful approach to deep carious lesions.18 Criteria for case selection include minimal preoperative symptoms, a carious lesion radiographically deep enough to
involve the pulp, no apical pathosis, and a positive response to pulp testing. The technique requires thorough excavation of caries peripheral to the pulp. Only the softest caries is removed from the central area over the pulp chamber. Pulp exposure is avoided if possible. Calcium hydroxide is then applied to the carious dentin, and a temporary restoration is placed. The choice of temporary restorative material is based on the desired length of recall, usually 6 to 12 months. However, what is most important in this regard is that the restoration seal the cavity margins to prevent any bacterial leakage.14,42,71
On the subsequent reevaluation, if the patient is symptom free and the tooth appears normal radiographically, the carious lesion is reentered, the caries is removed to the den-tinal bridge, and a permanent restoration is placed.18 The more recent evidence of the success rate of MTA pulp cap-pings and pulpotomies32,33,78,79 raises the question of whether or not there is any advantage to a two-step treatment regimen in indirect pulp capping. In fact, there may be two important disadvantages. The first is the requirement of patient compli-ance. In many practices, the assurance of a return visit in 6 to 12 months for additional excavation and restoration is of concern. Secondly, the two-step treatment is more expensive, requiring twice as much operator and office time. Thirdly, as already noted, a bacteria-tight seal is essential between visits.14,42,71 Current evidence regarding vital treatment with MTA in both primary and permanent teeth leads to the conclusion that indirect pulp treatment may not be worth the additional time or expense.17,32,33,65,79

140 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
because it is hydrophilic and compatible with the moisture in the MTA and the cavity preparation. After setting, the entire cavity preparation and the glass ionomer cement base can be etched for the placement of a permanent, bonded composite restoration (see Fig. 7-12, E and F ).
Direct Pulp CapTechniques for vital pulp capping are useful in two types of pulp exposures: carious and some mechanical (iatrogenic) exposures. The conditions of the pulp and the physical pre-sentation of the exposure sites requires a separate consider-ation of the treatment of each type.
Carious ExposureCase selection is important to successful outcome. The importance of maintaining pulp vitality in open apex cases cannot be overemphasized (Fig. 7-12, A and B). All studies consider preoperative symptoms important in the selection of teeth for vital treatment. Preferably, teeth should be free of symptoms, but teeth with symptoms of reversible pulpitis such as increased thermal sensitivity and episodic mild spon-taneous pain may be considered. Preoperatively, the routine sensibility testing of teeth is indicated; some carious expo-sures may have already caused partial to complete pulpal necrosis. Teeth with symptoms of irreversible pulpitis or developing apical pathosis are not suitable for vital treatment (see Chapter 1).
Unlike indirect pulp capping procedures, the caries are excavated thoroughly and a final restoration is placed to create a “bacteria-proof ” seal.14,42,71 Most clinicians favor a large, low-speed round bur for caries removal, but some suggest completing the excavation in the area of potential exposure with a coarse, high-speed diamond bur.78,79 Bleed-ing will often occur with small exposures. The operative field can be rinsed with water until bleeding ceases (see Fig. 7-12, C). If there is significant bleeding, 3% sodium hypochlorite or 2% chlorhexidine can be placed in the cavity preparation and left for up to 10 minutes for hemostasis.
The operative field should be left moist at all times. MTA is then placed over the floor of the cavity preparation (see Fig. 7-12, D). Some clinicians favor a flowable compomer to cover the MTA, others use a layer of glass ionomer cement
CLINICAL PROBLEMProblem: A 13-year-old female presented with a chief com-plaint of a hole in her tooth. She had no symptoms but was getting food caught in her tooth. She had a previous restora-tion in the tooth and could not understand how the food was being caught in her tooth (Fig. 7-13). Examination showed that the restoration had broken down, and caries had penetrated beneath the filling.
Solution: Upon removal of the old restoration and excava-tion of the caries, the pulp was exposed when the last vestiges of the demineralized dentin was removed. The pulp was capped with MTA, and a restoration was placed. At the 3-month reevaluation, the patient was symptom free, and the tooth was functional and responded normally to sensibility tests (see Fig. 7-13, B). As cited earlier, only one study included teeth in older individuals with closed apices for pulp capping, in which similar success with direct MTA was achieved.17
CLINICAL PROBLEMProblem: A 23-year-old female presented with a chief com-plaint of her tongue being sore because it was being caught in a hole in her last tooth in the upper left jaw. Upon examina-tion, a large carious lesion was present, and it appeared that she had lost a restoration (Fig. 7-14, A). The patient claimed she had not had any tooth pain, but sensibility testing with cold indicated a pulpal condition of reversible pulpitis (sensi-tivity without prolonged pain). The patient had limited finan-cial resources but wished to retain the tooth if possible.
Solution: The caries was excavated carefully using both a bur and sharp spoon excavator. When the last vestiges of demineralized dentin were removed, the pulp began to bleed, but the hemorrhage was controlled within a few minutes with chlorhexidine. The pulp was capped with MTA, and the tooth was restored with a composite resin (see Fig. 7-14, B). The patient was lost to follow-up until she returned 3 years later, inexplicably with a fractured amalgam restoration in the same tooth (see Fig. 7-14, C). At that time, sensibility tests gave normal responses. Note the dentinal bridging in the pulp chamber adjacent to the MTA (arrows).
Even in some cases of a large carious exposure with minimal symptoms, a pulp cap may be successful in an adult patient. The patient in Fig. 7-15, A was a 30-year-old male with no complaints other than having a “hole” in his tooth. The tooth was restored in the manner described earlier using an MTA direct pulp cap, a glass ionomer base, and an amalgam restoration. A 4-year reexamination radiograph showed no adverse findings, and the tooth responded nor-mally to sensibility testing (see Fig. 7-15, B).
CLINICAL PROBLEMProblem: A 41-year-old male patient presented with a large carious lesion in the mandibular left second molar. He had experienced occasional episodes of spontaneous pain in the past month that were relieved using mild analgesics. The peri-apical radiograph indicated the presence of deep coronal caries but no obvious pulp or periapical pathosis (Fig. 7-16, A). Following thorough excavation of caries in the mesial pulp horn area, there was a large carious exposure with a hemor-rhagic pulp (see Fig. 7-16, B).
Solution: Treatment and retention of the vital pulp in this tooth was judged to have a poor chance of success, and root canal treatment was completed (see Fig. 7-16, C).

A B
C D
E F
FIGURe 7-12 A, Mandibular right first molar with a potential carious exposure in an 8-year-old female patient. The tooth was asymptomatic. B, Clinical photograph if same tooth. C, After excavation, a pinpoint exposure of the mesial lingual pulp horn is apparent. D, Placement of mineral trioxide aggregate (MTA). e, Completed composite restoration. F, Postoperative radiograph of the restored tooth. Note the distinct layers of MTA, glass ionomer base, and final composite resin restoration. (Courtesy Dr. Sid Williams.)
A B
FIGURe 7-13 A, Carious exposure in mandibular right first molar of a 13-year-old female patient. B, Reevaluation radiograph after 3 months. Patient was asymptomatic and tooth responded normally to testing.

142 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
A
B C
FIGURe 7-14 A, Carious exposure in maxillary left second molar of a 23-year-old female patient. B, Posttreatment radiograph indicating a direct pulp cap with mineral trioxide aggregate (MTA) and final restoration with composite resin. C, Three-year reevaluation radiograph. Patient sought treatment of a fractured amalgam on the same tooth. No history why the composite restoration had been replaced. The patient was asymptomatic, and the tooth responded normally to testing. Note dentinal bridging (arrows).
A B
FIGURe 7-15 A, Carious exposure in tooth of a 30-year-old male patient. The tooth had preoperative symptoms of reversible pulpitis. B, Four-year reevaluation radiograph. The patient was asymptomatic, and the tooth responded normally to testing.
Since the probability of pulpal repair is less predictable in mature teeth, large exposures or excessive hemorrhage would be indications to proceed with pulpectomy and complete root canal treatment.
Mechanical (Iatrogenic) ExposureMechanical, or iatrogenic, exposures are those that occur acci-dentally in a noncarious area of a tooth (Fig. 7-17). Mechanical
exposures that would be appropriate for pulp capping by the techniques described in the previous section would be those that occur in the course of cavity preparation. For example, a pulp horn may be inadvertently exposed in a young tooth because of its relatively high extension toward the occlusal surface. Mechanical exposures that occur on the external surface of the prepared tooth, as in a crown preparation, are discussed in the following section on pulpotomy procedures.

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 143
Recent attempts to promote the use of direct bonded composite to mechanical pulpal exposures23 have met with mixed results. The focus of this approach was to seal the environment from bacterial ingress and thereby minimize or eliminate the demise of the pulp from bacterial influences.44 If optimal conditions for the preservation of pulpal health are to be ensured, dental restorations should provide an impervious seal against the surrounding tooth structure. However, polymerization shrinkage and contraction stresses induced during setting, as well as a variety of technical dif-ficulties encountered during the clinical operation, often produce less than perfect results. Therefore, modern restor-ative procedures involving resin and resin-bonded restor-atives must still rely on the ability of the pulp to cope with the injurious elements to which it may be exposed during and after the procedure.14,15 In this respect, direct placement on the dental pulp and residual dentin thickness appear to be key determinants of pulp responses after restorative dental treatment. In deep and pulpally exposed cavities in posterior teeth, composites have been associated with greater pulpal demise, requiring root canal treatment.77 Whereas some studies have claimed that pulp capping with bonded resin composites provides the lowest incidence of bacterial leakage,25 pulpal inflammation, and pulpal necrosis,14,15
The prognosis for mechanical exposures in all cases would seem to be quite good if the exposure is treated carefully in an aseptic environment. Even in the hands of a neophyte, success rates for capping mechanical exposures with calcium hydroxide can exceed 90%.6
A
B C
FIGURe 7-16 A, Mandibular left second molar with a gross carious exposure in a 41-year-old male patient. The tooth had been mildly symptomatic. B, Large carious exposure was found with a hemorrhagic pulp after thorough excavation. C, Completed root canal treatment.
FIGURe 7-17 Mechanical exposure of the dental pulp with no evidence of an inflammatory response.

144 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
others have found that some bonding systems should be avoided because they were not compatible with the technique and resulted in failure when compared to the use of calcium hydroxide in mechanically exposed pulps.60,61,66,69 Of major concern with the use of these materials are reports suggesting that hard tissue is often not formed; healing is delayed, result-ing in a lingering chronic inflammatory state; the potential exists for deficiency in bonding over time, especially if bridg-ing does not occur; and there are no properly designed clini-cal trials with adequate long-term follow-ups.14
Pulpotomy ProceduresPulp Exposure from CariesPulpotomy is the term for removal of the coronal pulp with the intent of maintaining the vitality of the remaining radicu-lar pulp tissue.54 Pulpotomy techniques using formocresol on primary teeth have been a standard in pediatric dentistry for decades. The indication was primarily the presence of a carious exposure and desire to retain the primary tooth until exfoliation. However, formocresol has been labeled as a car-cinogen, and its use is being abandoned.22,43 Other tech-niques that have been investigated with positive outcomes include the use of ferric sulfate63 and electrosurgery.8 Evi-dence of the effectiveness of MTA pulpotomies in primary teeth is positive and encouraging,4,32,40,56 in addition to its
A
B C
FIGURe 7-18 A, Mandibular left first molar with gross recurrent occlusal caries in a nine-year-old male patient. B, Immediate post pulpotomy radiograph indicating MTA in pulp chamber and permanent restoration. C, 24-month reevaluation radiograph indicating normal periapices on the treated tooth. The tooth responds normally to sensibility testing. Note the root development of the two rooted second premolar during the period of observation. (Courtesy Dra. Silvina Díaz.)
successful outcomes for permanent teeth (Fig. 7-18).56 Research must still pursue the conditions in which a pulp-otomy is the preferred treatment regimen rather than a direct pulp cap. On an empirical basis, some clinicians currently make the decision based on the amount of pulpal hemor-rhage from the exposure.
Pulp Exposure from Traumatic FractureFractures that result in pulpal exposure are mainly limited to the anterior teeth. Although posterior teeth are sometimes traumatically fractured with pulp exposure, root canal treat-ment is almost always indicated if the tooth can be saved. Traumatic fracture of posterior teeth with open apices is rare, and vital treatment of traumatically exposed pulps is indi-cated only when the root development of the tooth is imma-ture, exhibiting an open apex and thin root walls. For all teeth with fully developed roots and apical closure, root canal treatment is uncomplicated, predictable, and often necessary for restorative purposes.
There are two significant differences between carious and traumatic exposures. Pulps of traumatically fractured teeth usually have no history of bacterial involvement, and the patients rarely have symptoms prior to the trauma. The prog-nosis for pulp survival is excellent; even after several days, the superficial layer of the pulp is only slightly inflamed when exposed.28 However, the longer the exposure time, the smaller the chance for healing, because the quantity of bacteria that

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 145
placement of approximately 1 mm of the pulp capping mate-rial with another 1-mm space remaining for a bonded restor-ative material to seal the cavity (Fig. 7-20), taking care to avoid compaction of the MTA material too forcefully into the prepared canal space. Although the material is well toler-ated, the pressure alone may result in pulpal damage (Fig. 7-21). Following this procedure, dentinal bridging is usually observed in the pulp chamber adjacent to the reparative material (Fig. 7-22).
As previously noted, white MTA was formulated to address the problem of discoloration in the anterior teeth. Clinical experience with the white formulation has not always been satisfactory. Although no statistical evidence exists as yet, some cases treated with the white material still develop discoloration due to apparent darkening of the material in the coronal part of the tooth (Fig. 7-23). There are multiple speculations for this occurrence, including the inadvertent presence of residual blood products, interaction with residual bacterial toxins, and interactions with proteinaceous matter from the dentinal tubules. Fortunately, the tooth structure is not stained in the process. The usual remedy is complete removal of the MTA material, since dentinal bridging has usually occurred. The cavity preparation is then restored with a suitable bonded composite resin.
invade the pulp and the formation of irreversible inflamma-tory reactions increase.58
A second difference is that carious exposures generally occur in the depth of a carious excavation. The cavity prepa-ration presents a convenient and effective location for the protection and seal of the pulp with the capping material. On the other hand, traumatic fractures leave the pulp exposed on the surface of the tooth. Pulp capping materials do not adhere to the tooth and present a problem in both retention of the material and prevention of leakage. As with root canal treatment, coronal leakage of bacteria will cause failure of a pulp capping procedure and result in pulpal necrosis.
In addition to time of exposure, other issues that must be considered in the presence of a traumatic fracture are health of the pulp prior to trauma, diameter of the pulp exposure (1.5 mm diameter is the critical but empirical guideline), age of the tooth, no concomitant luxation injury, and the stage of root development.58 To address many of these challenges, a partial pulpotomy (Cvek) procedure27 was developed in which a cavity preparation is cut in the dentin around the exposure site. The depth of the cavity is approxi-mately 2 mm (Fig. 7-19). The original pulp capping material was calcium hydroxide, but MTA would be the current material of choice. The cavity preparation allows for the
A B
CC
FIGURe 7-19 A, Small pulp exposure resulting from a traumatic fracture. B, Preparation into the surrounding dentin for partial (Cvek-type) pulpotomy. Cavity preparation will allow for placement of mineral trioxide aggregate (MTA) and a secure protective restoration. C, Favorable repair on an exposed pulp using MTA. Note dentinal bridge. (C, Courtesy Dr. Mercedes Dominguez.)

146 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
A B
FIGURe 7-20 A, Two maxillary anterior teeth with vital exposures from traumatic fractures. Note open apices on both teeth. B, Completed Cvek partial pulpotomies with mineral trioxide aggregate (MTA).
A B
FIGURe 7-21 A, Traumatic fracture of a maxillary left central incisor with pulp exposure. B, Cvek pulpotomy with mineral trioxide aggregate (MTA), which was possibly overcompacted into the preparation.

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 147
DP
MTA
A B
FIGURe 7-22 A, Dentinal bridging observed with partial pulpotomies with MTA after traumatic exposure (DP, dental pulp; MTA, mineral trioxide aggregate). B, Radiograph of two maxillary central incisors showing dentinal bridging (arrows).
A B
C D
FIGURe 7-23 A, Traumatically fractured maxillary right central incisor with exposure of pulp. A partial pulpotomy was completed with white mineral trioxide aggregate (MTA). B, Two-year reevaluation radiograph indicating normal root development and no apical pathosis. Tooth responded normally to all pulp tests. C, Clinical photograph at 2-year reevaluation, indicating midcoronal discoloration. D, Reentry into pulp chamber revealed that white MTA had become discolored but did not stain adjacent tooth structure. Dentinal bridging meant MTA could be safely removed.

148 chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy
22. CDC: NIOSH pocket guide to chemical hazards, 9/2005. Avail-able at: http://www.cdc.gov/niosh/npg/npgd0293.html. Accessed March 24, 2009.
23. Clark DJ, Sheets CG, Paquette JM: Definitive diagnosis of early enamel and dentin cracks based on microscopic evaluation, J Esthet Restor Dent 15:391-401, 2003.
24. Coll JA: Indirect pulp capping and primary teeth: Is the primary tooth pulpotomy out of date? J Endod 34:S34-S39, 2008.
25. Cox CF, Hafez AA, Akimoto N, et al: Biologic basis for clinical success: pulp protection and the tooth restorative interface, Pract Periodontics Aesthet Dent 11:819-826, 1999.
26. Cummins D: Dentin hypersensitivity: from diagnosis to a break-through therapy for everyday sensitivity relief, J Clin Dent 20:1-9, 2009.
27. Cvek M: A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture, J Endod 4:232-237, 1978.
28. Cvek M: Prognosis of luxated non-vital maxillary central incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study, Endod Dent Traumatol 8:45-55, 1992.
29. Dowell P, Addy M: Dentine hypersensitivity—a review. Aetiology, symptoms and theories of pain production, J Clin Periodontol 10:341-350, 1983.
30. El Meligy OAS, Avery DR: Comparison of mineral trioxide aggre-gate and calcium hydroxide as pulpotomy agents in young perma-nent teeth (apexogenesis), Pediatr Dent 28:399-404, 2006.
31. Ehnevid H, Jansson L, Lindskog S, et al: Endodontic pathogens: propagation of infection through patent dentinal tubules in trau-matized monkey teeth, Endod Dent Traumatol 11:229-234, 1995.
32. Farsi N, Alamoudi N, Balto K, et al: Success of mineral trioxide aggregate in pulpotomized primary molars, J Clin Pediatr Dent 29:307-311, 2005.
33. Farsi N, Alamoudi N, Balto K, et al: Clinical assessment of mineral trioxide aggregate (MTA) as direct pulp capping in young permanent teeth, Bottom of Form J Clin Pediatr Dent 31:72-76, 2006.
34. Fuks AB: Vital pulp therapy with new materials for primary teeth: new directions and treatment perspectives, J Endod 34:S18-S24, 2008.
35. Guide to clinical endodontics, ed 4, Chicago, 2004, American Association of Endodontists.
36. Hals E: Observations on giant tubules in human coronal dentin by light microscopy and microradiography, Scan J Dent Res 91:1-7, 1983.
37. Haywood VB: Treating sensitivity during tooth whitening, Compend Contin Educ Dent 26(9 Suppl 3):11-20, 2005.
38. Hess W: The treatment of teeth with exposed healthy pulps, Int Dent J 1:10-35, 1950.
39. Hewlett ER: Etiology and management of whitening-induced tooth hypersensitivity, J Calif Dent Assoc 35:499-506, 2007.
40. Holan G, Eidelman E, Fuks AB: Long-term evaluation of pulp-otomy in primary molars using mineral trioxide aggregate or formocresol, Pediatr Dent 27:129-136, 2005.
41. Holland GR: Morphological features of dentine and pulp related to dentine hypersensitivity, Arch Oral Biol 39(Suppl):3S-11S. 1994.
42. Hørsted-Bindslev P, Løvschall H: Treatment outcome of vital pulp treatment, Endod Topics 2:24-34, 2002.
43. IARC monographs on the evaluation of carcinogenic risks to humans. Lyon, France. Available at: http://monographs.iarc.fr/ENG/Monographs/vol88/mono88.pdf. Accessed March 24, 2009.
REFEREnCES1. Addy M: Tooth brushing, tooth wear and dentine hypersensitiv-
ity—are they associated? Int Dent J 55:261-267, 2005.2. Addy M: Tooth brushing, tooth wear and dentine hypersensitiv-
ity—are they associated? [republication], J Ir Dent Assoc 51:226-231, 2006.
3. Addy M, Urquhart E: Dentine hypersensitivity: its prevalence, aetiology and clinical management, Dent Update 19:407-412, 1992.
4. Agamy HA, Bakry NS, Mounir MMF, et al: Comparison of mineral trioxide aggregate and formocresol as pulp-capping agents in pulpotomized primary teeth, Pediatr Dent 26:302-309, 2004.
5. Al Ansary MAD, Day PF, Duggal MS, et al: Interventions for treating traumatized necrotic immature permanent anterior teeth: including a calcific barrier and root strengthening, Dent Trauma-tol 25:367-379, 2009.
6. Al-Hiyasat AS, Barrieshi-Nusair KM, Al-Omari MA: The radio-graphic outcomes of direct pulp-capping procedures performed by dental students: a retrospective study, J Am Dent Assoc 137:1699-1705, 2006.
7. Arrais CA, Micheloni CD, Giannini M, et al: Occluding effect of dentifrices on dentinal tubules, J Dent 31:577-584, 2003.
8. Bahrololoomi Z, Moeintaghavi A, Emtaizi M, et al: Clinical and radiographic comparison of primary molars after formocresol and electrosurgical pulpotomy: a randomized clinical trial, Indian J Dent Res 19:219-223, 2008.
9. Bamise CT, Olusile AO, Oginni AO: An analysis of the etiological and predisposing factors related to dentin hypersensitivity, J Contemp Dent Pract 9(5):52-59, 2008.
10. Barbour ME, Rees GD: The role of erosion, abrasion and attrition in tooth wear, J Clin Dent 17(4):88-93, 2006.
11. Barrieshi-Nusair KM, Qudeimat MA: A prospective clinical study of mineral trioxide aggregate for partial pulpotomy in cariously exposed permanent teeth, J Endod 32:731-735, 2006.
12. Bartlett DW, Ide M: Dealing with sensitive teeth, Prim Dent Care 6:25-27, 1999.
13. Bartold PM: Dentinal hypersensitivity: a review, Aust Dent J 51:212-218, 2006.
14. Bergenholtz G: Evidence for bacterial causation of adverse pulpal responses in resin-based dental restorations, Crit Rev Oral Biol Med 11:467-480, 2000.
15. Bergenholtz G: Advances since the paper by Zander and Glass (1949) on the pursuit of healing methods for pulpal exposures: historical perspectives, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100:S102-S108, 2005.
16. Berutti E: Microleakage of human saliva through dentinal tubules exposed at the cervical level in teeth treated endodontically, J Endod 22:579-582, 1996.
17. Bogen G, Kim JS, Bakland LK: Direct pulp capping with mineral trioxide aggregate: an observational study, J Am Dent Assoc 139:305-315, 2008.
18. Bjørndal L: Indirect pulp therapy and stepwise excavation, J Endod 34:S29-S33, 2008.
19. Brännström M: Sensitivity of dentine, Oral Surg Oral Med Oral Pathol 21:517-526, 1966.
20. Canadian Advisory Board on Dentin Hypersensitivity: Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity, J Can Dent Assoc 69:221-226, 2003.
21. Carneiro SR, Todescan JH, Friedman MT, et al: Zone between plaque and attached periodontal tissues on chronic periodontitis-affected teeth: an SEM study, Int J Periodontics Restorative Dent 23:261-267, 2003.

chapter 7 | Problem-Solving Challenges in Dentin Hypersensitivity and Vital Pulp Therapy 149
66. Silva GA, Lanza LD, Lopes-Júnior N, et al: Direct pulp capping with a dentin bonding system in human teeth: a clinical and his-tologic evaluation, Oper Dent 31:297-307, 2006.
67. Slutzky-Goldberg I, Nuni E, Nasralla W, et al: The effect of CO2 laser on the permeability of dentinal tubules: a preliminary study, Photomed Laser Surg 26:61-64, 2008.
68. Sonmez D, Sari S, Çetinbas T: A comparison of four pulpotomy techniques in primary molars; a long-term follow-up, J Endod 34:950-955, 2008.
69. Stanley HR: Pulp capping: conserving the dental pulp—can it be done? Is it worth it? Oral Surg Oral Med Oral Pathol 68:628-639, 1989.
70. Swift EJ, Jr: Tooth sensitivity and whitening, Compend Contin Educ Dent 26(9 Suppl 3):4-10, 2005.
71. Swift EJ, Jr, Trope M, Ritter AV: Vital pulp therapy for the mature tooth—can it work? Endod Topics 5:49-56, 2003.
72. Thomas GA: The diagnosis and treatment of the cracked tooth syndrome, Aust Prosthodont J 3:63-67, 1989.
73. Thompson V, Craig RG, Curro FA, et al: Treatment of deep carious lesions by complete excavation or partial removal—a criti-cal review, J Am Dent Assoc 139:705-712, 2008.
74. Torabinejad M, Hong CU, McDonald F, et al: Physical and chemi-cal properties of a new root-end filling material, J Endod 21:403-406, 1995.
75. Tronstad L: Ultrastructural observations on human coronal dentin, Scan J Dent Res 81:101-111, 1973.
76. Tronstad L, Langeland K: Electron microscopy of human dentin exposed by attrition, Scan J Dent Res 79:160-171, 1971.
77. Whitworth JM, Myers PM, Smith J, et al: Endodontic complica-tions after plastic restorations in general practice, Int Endod J 38:409-416, 2005.
78. Witherspoon DE: Vital pulp therapy with new materials: new directions and treatment perspectives—permanent teeth, J Endod 34:S25-S28, 2008.
79. Witherspoon DE, Small JC, Harris GZ: Mineral trioxide aggregate pulpotomies: a case series outcomes assessment, J Am Dent Assoc 137:610-618, 2006.
RECOMMEnDED ADDITIOnAl READIngGillam DG, Bulman JS, Newman HN: A pilot assessment of alterna-
tive methods of quantifying dental pain with particular reference to dentine hypersensitivity, Commun Dent Health 14:92-96, 1997.
Jacobsen PL, Bruce G: Clinical dentin hypersensitivity: understanding the causes and prescribing a treatment, J Contemp Dent Pract 2(1):1-12, 2001.
Kiatwateerantana T, Kintarak S, Piwat S, et al: Partial pulpotomy on caries-free teeth using enamel matrix derivative or calcium hydrox-ide: a randomized controlled trial, Int Endod J 42:584-592, 2009.
Ni Chaollai A, Monteiro J, Duggal MS: The teaching of management of the pulp in primary molars in Europe: a preliminary investigation in Ireland and the UK, Eur Arch Paediatr Dent 10(2):98-103, 2008.
Pashley DH, Tay FR, Haywood VB, et al: Consensus-based recom-mendations for the diagnosis and management of dentin hypersen-sitivity, Inside Dent 4(9 Special Issue):1-37, 2008.
Ritter AV, de L Dias W, Miguez P, et al: Treating cervical dentin hypersensitivity with fluoride varnish, J Am Dent Assoc 137:1013-1020, 2006.
West NX: Dentine hypersensitivity, Monogr Oral Sci 20:173-189, 2006.
44. Kakehashi S, Stanley HR, Fitzgerald R: The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats, Oral Surg Oral Med Oral Pathol 20:340-349, 1965.
45. Kobler A, Kub O, Schaller H-G, et al: Clinical effectiveness of a strontium chloride-containing desensitizing agent over 6 months: a randomized, double-blind, placebo-controlled study, Quintes-sence Int 39:321-325, 2008.
46. Lee SY, Kwon HK, Kim BI: Effect of dentinal tubule occlusion by dentifrice containing nano-carbonate apatite, J Oral Rehabil 35: 847-853, 2008.
47. Liewehr FR: An inexpensive device for transillumination, J Endod 27:130-131, 2001.
48. Lindskog S, Blomlöf L: Cementum hypoplasia in teeth affected by juvenile periodontitis, J Clin Periodontol 10:443-451, 1983.
49. Maryniuk GA, Haywood VB: Placement of cast restorations over direct pulp capping procedures: a decision analytic approach, J Am Dent Assoc 120:183-187, 1990.
50. Massler M: Pulpal reactions to dental caries, Int Dent J 17:441-460, 1967.
51. Matsuo T, Nakanishi T, Shimizu H, et al: A clinical study of direct pulp capping applied to carious-exposed pulps, J Endod 22:551-556, 1996.
52. McGrath PA: The measurement of human pain, Endod Dent Traumatol 2:124-129, 1986.
53. Min KS, Park HJ, Le SK, et al: Effect of mineral trioxide aggregate on dentin bridge formation and expression of dentin sialoprotein and heme oxygenase-1 in human dent pulp, J Endod 34:666-670, 2008.
54. Mjör IA: Pulp-dentin biology in restorative dentistry, Chicago, 2002, Quintessence Publishing Co. Inc.
55. Nathanson D: Vital tooth bleaching: sensitivity and pulpal con-siderations, J Am Dent Assoc 128(Suppl):41S-44S, 1997.
56. Ng FK, Messer LB: Mineral trioxide aggregate as a pulpotomy medicament: an evidence-based assessment, Eur Arch Paediatr Dent 9(2):58-73, 2008.
57. Noyes FB, Schour I, Noyes HJ: Oral histology and embryology, ed 6, London, 1948, Henry Kimpton.
58. Olsburgh S, Krejci I: Pulp response to traumatic crown fractures, Endod Topics 5:26-40, 2003.
59. Orchardson R, Gillan DG: Managing dentin hypersensitivity, J Am Dent Assoc 137:990-998, 2002.
60. Pameijer CH, Norval G: Pulpal responses to restorative treatment. In Duke ES, editor: The changing practice of restorative dentistry, Indianapolis, 2002, Indiana University Press.
61. Pameijer CH, Stanley HR: The disastrous effects of the “total etch” technique in vital pulp cappings in primates, Am J Dent 11(Spec No):S45-S54, 1998.
62. Pashley DH: Dentine permeability and its role in the pathobiol-ogy of dentine sensitivity, Arch Oral Biol 39(Suppl):73S-80S, 1994.
63. Peng L, Ye L, Guo X, et al: Evaluation of formocresol versus ferric sulphate primary molar pulpotomy: a systemic review and meta-analysis, Int Endod J 40:751-757, 2007.
64. Rees JS, Hammadeh M, Jagger DC: Abfraction lesion formation I maxillary incisors, canines and premolars: a finite element study, Eur J Oral Sci 111:149-154, 2003.
65. Sawicki L, Pameijer CH, Emerich K, et al: Histological evaluation of mineral trioxide aggregate and calcium hydroxide in direct pulp capping of human immature permanent teeth, Am J Dent 21:262-266, 2008.

150
The first step in the treatment of a tooth . . . is the adjustment of the rubber dam over the diseased tooth to preclude the possibility of the entrance of any germs in the oral secretions into the pulp chamber. This should be the invariable rule.14
Anonymous, 1900
Chapter 8
Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
Problem-Solving ListProblem-solving issues and challenges in pulp chamber access addressed in this chapter are:
Critical Factors in Tooth Isolation Within the standards of Care
major Problems or Errors in Endodontic Access openings
Techniques for safe and Accurate Access Cavity Preparations
Problem-solving Challenges in Access openings
Pulp chamber calcifications
Use of magnification during access preparation
Preventing and managing coronal perforations
Potential problems in access openings through crowned teeth or teeth with excessively large restorations
Clinical considerations in preventing and managing problems in tooth isolation and access preparation
Problem Solving in Recognizing or Locating Canal Orifices
Calcification of the dental pulp and pulp canal space
Maxillary central and lateral incisors and canines
Maxillary premolars
Maxillary molars
Mandibular incisors, canines, and premolars
Mandibular molars
Clinical considerations in preventing and managing problems in orifice identification
The main purpose of a lingual or occlusal endodontic access opening is to develop an unimpeded passageway to the pulpal space and apical foramen of the tooth. This unrestricted opening should be specifically designed for each tooth to facilitate proper canal cleaning, shaping, and obturation. In some cases, a problem-solving approach may dictate the need to initiate the access opening in a surface other than the lingual or occlusal (Figs. 8-1 and 8-2). Although rare, these creative approaches should only be used when standard entries to the canal system are impossible or the loss of tooth structure permits. A properly prepared access opening can eliminate many technical difficulties encountered in root canal treatment.42,43 In fact, many of the problems discussed in this book regarding locating and negotiating fine and calci-fied canals, cleaning and shaping, disinfection, obturation,
The first essential in getting at any root-canal is to gain direct access, and not to try to work around corners, whatever tooth-structure may have to be sacrificed.24
R.H. HoFHEInz, 1892

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 151
A
B
FIGuRE 8-1 A, Rotated mandibular canine. B, Access is made through the facial surface.
A B C
FIGuRE 8-2 A, Maxillary molar exhibits extensive buccal cervical erosion and abrasion. B, Initial access is made in a buccal-palatal direction without a dental dam. C, Closer view shows access after the canal orifices are opened.
and revision of treatment may be avoided or eliminated with a proper coronal access opening.
The major consideration in all access openings is that coronal tooth structure should not be retained if its preser-vation prevents direct pathways to the canal orifices. This admonition does not imply that radical removal of the coronal tooth structure is necessary simply to obtain unim-peded access to the pulpal space; caution is also advised in creating excessively large access cavities for the convenience of operating microscope visualization. Rather, the statement implies that the clinician must be thoroughly knowledgeable
CLINICAL PROBLEMProblem: A 37-year-old female presented with acute pain to biting on her mandibular left first molar. Following diagnostic testing, a diagnosis of irreversible pulpitis with acute apical periodontitis was made. Root canal treatment was initiated on the tooth, and the final radiograph showed poorly filled canals with significant canal space apical to the gutta-percha filling in all canals (Fig. 8-3). The mesial canals were prepared to a size No. 30 K-file and the distal canal to a size No. 35 K-file. The working length was established 1 mm from the radio-graphic apex, and the final file sizes were used to the full length in the root. The general dentist was concerned about not being able to obturate the canals well, even after the instruments would go to the working length, so the patient was referred to a specialist.
Solution: An assessment of the tooth indicates that the roof of the pulp chamber had not been removed (see Fig. 8-3, arrow). Failure to remove this anatomic obstruction forces the clinician to prepare and obturate the canals through the pulp horns. A major constriction of this nature due to an improper access opening significantly influences access to the canals, quality of canal cleaning and shaping, canal disinfection, and obturation. Clearly not all inflamed/infected pulp tissue has been removed, yet the clinician’s problem focused on errors in obturation.
about pulpal and external root anatomy and must be capable of proper radiographic assessment of the three-dimensional relationship of the pulpal space within the con-fines of the tooth.38 When these factors are all considered, a properly placed and shaped access opening can be made. Failure to approach this initial technical step in root canal treatment in this manner not only invites problems during access opening preparation but also unleashes a plethora of technical problems in all phases of treatment. Subsequently, treatment will be compromised or teeth will be lost unnecessarily.

152 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
Critical Factors in Tooth Isolation Within the Standards of Care
Proper tooth isolation is essential to all phases of root canal treatment, particularly patient protection and asepsis.3,8,21,40,63 Tooth isolation with a dental dam (formerly known as a rubber dam), using creative approaches to ensure these attain-ments is often required (Fig. 8-4).4 Questions or concerns frequently asked include:
“Do I really need to use a dental dam all the time? It is so hard to place.”
“The patient does not want to have the dental dam used in their mouth.”
“I was taught that in dental school, but is it really relevant in dental practice?”
These are important issues because what is being taught in dental education may not be viewed seriously by the dental clinician once in practice.* Nevertheless, use of the dental dam is the standard of care in providing root canal treatment
FIGuRE 8-3 Mandibular molar had been accessed, and clinician could not penetrate canals fully with the filling materials. All the cleaning, shaping, and obturation had been done through the pulp horns, and the roof (arrow) of the pulp chamber had never been removed.
FIGuRE 8-4 A, Maxillary premolar with subgingivally fractured palatal cusp. B, An oral sealing agent is placed along the palatal margin. C, A rubber dam is sealed in place. D, Clamping of adjacent teeth facilitates isolation of a tooth prepared for a crown.
*References 23, 35, 36, 50, 51, and 57.
A B
C
D

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 153
FIGuRE 8-5 Well-fitted rubber dam prior to disinfection and access opening.
and certainly can and should be used in other aspects of restorative dentistry.9,16,18,63
There are several directives that should be considered for all cases of root canal treatment. Prepare access openings after a well-fitted and disinfected dental dam is placed, isolating the tooth to be treated. This is followed by disinfecting the dental dam with 2.5% sodium hypochlorite or alcohol before access to enhance asepsis (Fig. 8-5).22 The dental dam will
protect the patient’s tissues and seal the mouth from root canal irrigants and disinfectants. This will prevent patient ingestion of irrigants and aspiration of instruments or materi-als during root canal procedures. The dental dam also facili-tates procedures by creating a clear, dry field while enhancing infection control.3,31,32 In some cases, the initial access opening outline can be prepared immediately before placing the dental dam, so long as the tooth is not contaminated further before placing the dam (see Fig. 8-3).
Major Problems or Errors in Endodontic Access Openings
Many problems can occur during access opening preparation that will impact greatly on the subsequent phases of root canal treatment. Major shortcomings tend to occur in the following areas. First, all caries and unsupported weak tooth structure must be removed. This will enable the determina-tion of tooth restorability and identification of any defects such as cracks (Fig. 8-6).33 Developing straight-line access to the pulp chamber and root canal system and establishing an aseptic environment for treatment procedures are critical
E F
G
E, Two central incisors are isolated using two clamps. F, The tooth is isolated with excessive amounts of temporary material. This approach may prevent the necessary excavation and determination of restorability before root canal procedures. G, Temporary material adjacent to two mesial canals is used to isolate the tooth. Scraping the material with files and carrying it into the canal create a strong possibility of blocking the canal.
FIGuRE 8-4, cont’d

154 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
A B
C D
FIGuRE 8-6 A, Apparent small crack on the marginal ridge of a mandibular molar (arrow). B, Same tooth as in A after removal of the restoration. Note the crack line extending almost completely across the pulpal floor. This is an obvious cause of pulpal pathosis but may not be significant in treatment planning if it does not extend apically to the pulpal floor. C, Coronal fracture extending across the pulpal floor. Careful assessment of the periodontal attachment in this area should be done to rule out extension of the fracture below crestal bone. Note the use of Methylene Blue 1% to stain fracture line. D, Large crack on the mesial floor of cavity preparation in a maxillary molar. A large crack at the level of the gingival margin could easily extend apically below the level of crestal bone.
steps. Moreover, stable coronal reference points can be estab-lished, and loosening of restoration debris that may be pushed into the canal is avoided.48
During the removal of carious tooth structure, the periph-eral decay is removed first, and then the carious material is
removed inward toward the pulp chamber (Fig. 8-8, A). Penetrating a pulp chamber in which pulp is hyperemic or purulence has accumulated creates the difficulties of working in a confined space in a pool of blood or pus (see Fig. 8-8, B). Attempts to unroof a chamber or enlarge the access at
CLINICAL PROBLEMProblem: A 54-year-old male presented with episodic pain in the mandibular left quadrant. All teeth in this quadrant had extensive restorations. He believed his pain was coming from the first molar, but he was not sure. Pain was evident in response to percussion on the first molar; all other teeth responded normally. Cold elicited prolonged pain on the first molar, with normal responses on the adjacent and contralateral teeth. Periodontal probings and palpation were normal, but an explorer was easily placed under the mesial buccal margin of the crown on the first molar. A radiograph showed an invasive carious lesion on the mesial of the first molar, along with radiolucencies at the apices of both roots (Fig. 8-7, A). The diagnosis was irreversible pulpitis with acute apical periodontitis. The dilemma with this case
focused on the access opening. Preparation of an access through the crown creates a situation in which all the previous problems described can occur.
Solution: All potential problems with gaining access to the pulpal space can be prevented with crown removal. In this case, the tooth was isolated, and the crown was cut off using a bur to cut a groove from buccal to lingual (see Fig. 8-7, B and C). Attempt-ing to retain this crown is futile because there is loss of marginal integrity. Complete removal and excavation of the caries pro-vided the opportunity to evaluate the remaining coronal tooth structure (see Fig. 8-7, D and E), which contributed greatly to the treatment plan for this tooth.

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 155
A
C D E
B
C
B
FIGuRE 8-7 A, Radiograph showing apical lesions on both roots and recurrent caries under mesial margin of the crown. B, Cutting of the crown from the tooth. C, Crown has been removed, and decay is evident under the old restoration. D, Removal of the old restoration shows significant decay. E, Final excavation that allows for evaluation of the tooth structure and facilitates direct access to the pulp chamber.
A B
FIGuRE 8-8 A, Caries around margins and under cusps must be excavated before the endodontic access opening is made. B, Excessive hemorrhage from inflamed pulp tissue can impair visualization of the pulp chamber.

156 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
accentuated manner to enhance straight-line access (Fig. 8-10). This approach also prevents scraping metallic margins with the intracanal instruments and carrying metallic parti-cles into the canal and blocking its pathway. Removal of foreign debris inadvertently carried into the canal is possible with gentle ultrasonic canal instrumentation.41 In cases in which a temporary restorative material such as zinc oxide eugenol is present, removal of the entire restoration is recom-mended,48 except in those areas where avenues of leakage may be opened. However, crown lengthening may be the pre-ferred alternative to leaving deep temporary restorations in place (see Chapter 17). (Indications for restoration removal can be found in Boxes 8-1 and 8-2.)
A BB CA C
FIGuRE 8-9 A, Maxillary molar requires root canal treatment. Exploration showed evidence of decay around distal margins of amalgam. B, Removal of amalgam reveals a vertical fracture on the palatal margin. C, Complete cleaning and shaping of canals are shown. Fracture lines are still visible, but no periodontal defects are present.
FIGuRE 8-10 Crowned tooth with endodontic access opening is shown. All canals are visible when viewed from the occlusal perspective.
BoX 8-1 Compelling Reasons to Remove Restorations
• Evidence of continued leakage of salivary contaminants into the canal during treatment
• Unexpected carious invasion beneath restorations, especially full crowns
• Fractures uncovered during access preparation• Loose, defective, or undermined restorations• Treatment-planned restoration replacement
BoX 8-2 Reasons of Convenience to Remove Restorations
• Malpositioned teeth or restorations that impede direct access to the canals
• Need to search for calcified orifices• Need to establish tooth restorability, especially with
possible chamber perforations• Need to enhance clinician orientation
this point can lead to crown or furcation perforation. Careful excavation around the pulp chamber before penetration will generally prevent this problem.
Along with caries excavation, removal of unsupported tooth structure and weakened or faulty restorations enhances access to the canal system and visibility of tooth fractures (see previous Clinical Problem) and helps prevent fracture of fragile enamel walls and possibly the entire tooth during treatment33 (Fig. 8-9). Further excavation will also remove restorations from the borders of the access opening, thereby preventing the loosening of alloy or composite particles that may enter and block the root canal system—a common occurrence when large pin restorations or crowns are present. If the restoration is intact and provides an adequate seal, total removal is unnecessary. In these cases, the clinician should (1) use water during the access opening preparation to elimi-nate debris and (2) flare the cavity walls occlusally in an

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 157
compound this situation, extra canals are commonly found (Fig. 8-12), and failure to identify and clean these anatomic variants will often lead to treatment failure. The best way to manage such problems is to prevent them. Continuous rec-ognition of deviations thorough periodic radiographic review and the possible use of magnification are essential. See Chapter 3 for additional discussion and examples.
Coupled with a smaller or calcified pulp chamber or canal, failure to take into account altered coronal-radicular relationships will usually lead to irreparable damage to the tooth structure (Fig. 8-13). Additionally, the location of the canal or canals will often be missed. Pulp chamber spaces are generally located in the center of the crown.59,60 Many teeth that have had multiple restorative procedures over time exhibit pulpal response to these irritations. The result is usually a reduction in the dimensions of the root canal space
Oftentimes the crown of the tooth is not in direct align-ment with the long axis of the root, so preparation of the access with only the angle of the crown in mind invites a coronal perforation or gouging of the crown. Teeth that normally exhibit significant altered crown-root angulations are maxillary lateral incisors and mandibular first premolars,19 but any tooth in the mouth may present this anatomic chal-lenge (Fig. 8-11). In molar teeth during access opening in the presence of these altered angular relationships, misiden-tification of canals (e.g., mistaking the mesial lingual canal for the mesial buccal canal) may occur.7 Subsequent search-ing for the other canals often results in gouging or perforating areas far removed from the true canal orifice(s).
Undermining and weakening coronal or radicular tooth structure is inevitable when anatomic relationships are not readily identified, even if a perforation does not occur. To
A B
FIGuRE 8-11 A and B, Two mandibular molars with the occlusal surface at divergent angles to the long axes of the roots. Occlusal surface orientations are indicated by the black lines on both teeth. Root angulations are indicated by the red arrows on both teeth. Penetration perpendicular to the occlusal surface may lead to ultimate chamber/furcation perforation.
A B
FIGuRE 8-12 A, Both canine and lateral incisors have multiple canals. B, Distal roots of a mandibular molar with two distinct roots/canals.

158 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
that is visible on a good-quality, two-dimensional radio-graph.1 In many cases, especially when large restorations are present, bite-wing radiographs are necessary for proper visu-alization of the chamber space relative to the alignment of the crown to the root. Often, angled radiographs from the mesial and distal aspects will also be necessary when teeth are rotated or have abnormal root configurations28 (see Chapter 2).
Access openings in artificial crowns or excessively large restorations also invite possible perforation if the three-dimensional relationship of the pulp chamber in relation to the altered crown anatomy (due to restorations) is not con-sidered.37,53 Here again, the use of angled radiographs is most useful for determining relationships prior to preparing an access opening. Additional concerns with access into these teeth are the distribution of metallic or composite debris into the chamber and root canals that may ultimately block the canals or be pushed beyond the end of the root, creating potential long-term sources of irritation and lack of healing of the periapical tissues.34,62 High-speed suction and frequent irrigation are essential.
Techniques for Safe and Accurate Access Cavity Preparations
Access opening preparation is a dynamic, three-dimensional process.23 The old adage in access opening preparation, “Go for the pulp horns,” is reasonable in most cases. The pulp horn areas are targets in the process of early excavation (Fig. 8-14). In more routine cases in which the pulp chamber is
FIGuRE 8-13 Access perforation in a mesially tipped mandibular molar with calcified canal orifices. Access was cut through a large composite restoration. Despite its eventual removal, the clinician remained disoriented as to the location of the second mesial orifice. A preoperative bitewing radiograph might have established the true orientation of the long axis of the tooth with the occlusal plane.
C
BA
FIGuRE 8-14 A, Diagram of mandibular molar shows anticipated parameters of the pulp chamber. Access entry must proceed into the center of these parameters (arrow). B, Access entry may be directed to the largest canal (arrow) in cases of tooth misalignment, calcification, or lack of visible pulp chamber. C, With a crown in place and evidence of calcifications in the pulp chamber, a direct-line access opening into the center of this tooth is recommended.
visible on the preoperative film, location of the pulp horns is an early confirmation of spatial orientation (Fig. 8-15). In anterior teeth, the lingual surface is penetrated at right angles to the lingual/palatal surface of the crown. After pen-etration through the enamel (or artificial crown), the bur is reoriented as much as possible to the long axis of the root. Some clinicians describe this as “keeping the bur to the lingual of the initial opening.” From this standpoint, the pulp horns, if present, should be located. Once the pulp chamber has been accessed, the lingual ledge or shoulder is removed by “cutting on the outstroke.” This will establish a straight-line access opening into the root canal (Fig. 8-16). If removal of the lingual ledge is done with a “cutting-in stroke” there is a greater chance for gouging or even a buccal/facial perforation.
Complete removal of the lingual ledge will often uncover extra canals in mandibular incisors, canines, and premolars (Fig. 8-17). Failure to locate these canals often leads to severe postoperative pain or ultimate treatment failure (see Chapter

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 159
A B
FIGuRE 8-15 A and B, Two molars requiring root canal treatment, each with pulp horns visible even in the presence of some calcifications. Once these pulp horns are reached with a bur, there is initial spatial confirmation of the pulp chamber location and dimensions.
FIGuRE 8-16 Access opening in maxillary central incisor demonstrates straight-line access to the pulp space.
A B
FIGuRE 8-17 Access opening in mandibular incisor (A) extends lingually. The second canal located under the cingulum is noted. B, Two canals in a maxillary lateral incisor.

160 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
FIGuRE 8-18 Anterior Access Kit (Dentsply Maillefer, Ballaigues, Switzerland).
FIGuRE 8-20 Posterior Access Kit (Dentsply Maillefer, Ballaigues, Switzerland).
5). The blame for failure of this nature is often transferred to the patient or tooth, when in fact the clinician should have full knowledge and control in these situations.
Burs that are recommended for access to anterior teeth include small to medium round burs, tapered diamonds and/or Endo-Z burs for refinement of the access outline, and possibly Gates-Glidden burs or X-Gates to assist in lingual ledge removal (Fig. 8-18: Anterior Access Kit [Dentsply Maillefer, Ballaigues, Switzerland]).
In posterior teeth, failure to remove the entire roof of the pulp chamber is a common problem that precludes locating the wide variety and often complex canal systems in these teeth (Fig. 8-19). Initially the size and depth of the pulp chamber space on the radiograph should be measured by holding the mounted bur in the handpiece next to the image of the crown on the radiograph (see Fig. 8-30); or if a digital image is being used, measurement tools are available for this purpose. After the pulp horns have been identified, remove the dentin between the horns. Once the dentin has been removed, a safe-ended bur can be placed adjacent to the overhanging roof, which is removed by cutting laterally to unroof the overlying dentin and to flare the walls of the access opening occlusally. A No. 17 or No. 23 explorer is used to evaluate the removal of the roof or dentin overhangs, fol-lowed by an inspection of the chamber to ensure an unob-structed entry into the canal orifices. Burs recommended for this procedure include medium to large round burs, a safe-sided diamond bur or Endo-Z bur, and a Gates-Glidden bur or X-Gates for refinement. For both anterior and posterior access openings, various bur access kits have been created to facilitate clinician choice and usage (Fig. 8-20: Posterior Access Kit [Dentsply Maillefer, Ballaigues, Switzerland]), and the instruments within provide a wide range of tried and tested tools to ensure a proper access opening.
Once the pulp chamber of the posterior tooth is opened to good visualization, recognition of the commonly observed anatomic relationships seen on the floor of the chamber is essential to determine the location of the orifices and prevent perforations. Fig. 8-21 depicts commonly seen pulp chamber
A
B
FIGuRE 8-19 A, Mandibular molar with access opening is shown. Patient is referred for treatment because of constant pain during attempts to enter the canal orifices. Only the pulp horns are exposed, and the pulp chamber roof is intact. B, Ideal access is shown with roof removed.
floor anatomy in a maxillary two-rooted pre-molar, maxillary first molar, and mandibular first and second molars. Recogni-tion of these anatomic designs12,29 and integration of this information with the radiographic findings will prevent problems during both access preparation and canal orifice location.
In refining posterior access openings, removing cervical ledges or bulges (Fig. 8-22) is important because these often impede straight-line entry into the canal or cover up addi-tional canals (Fig. 8-23).30 Removal of the ledges/bulges must

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 161
A B
C D
FIGuRE 8-21 Commonly seen anatomy on the pulp chamber floors is evident in posterior teeth. A, Maxillary premolar. B, Maxillary first molar with two canals in the mesial buccal root (arrows). C, Mandibular first molar with one distal canal. D, Mandibular second molar with two distal canals (arrows).
AA B
FIGuRE 8-22 A, Radiograph of a maxillary molar with cervical ledges (arrows). B, A sectioned maxillary molar that depicts what happens in the layering of irritational dentin and development of ledges (arrows) that may impede access to the canal system.

162 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
A B
C D
FIGuRE 8-23 A, Access opening in a maxillary molar showing cervical ledges on mesial and distal walls. B, Top of the ledge on the mesial is removed. C, Probing with a DG-16 explorer discovers the mesial palatal (MP) canals (arrow). D, The final canals cleaned and shaped, showing all four canals.
be performed carefully, using lateral cutting while tapering the internal walls occlusally and avoiding any apical penetration.
Problem-Solving Challenges in Access Openings
Not every tooth is amenable to a straightforward access preparation. In fact, teeth with artificial crowns or large restorations usually have significantly diminished pulp chambers and pulp canals as a result of increases in irri-tational dentin or the presence of pulp stones.1,13,39 Artificial crowns often completely block the view of the chamber space radiographically even on bite-wing radiographs. Large restorations cannot only obscure the pulp chamber radio-graphically, but also can block the orifices physically (Fig. 8-24). These impediments can make access preparations most challenging. There are at least three issues that come into consideration in these cases: (1) the presence of cal-cifications in the pulp chamber, (2) the use of magnifica-tion during access preparation, and (3) the potential for perforation of the floor of the pulp chamber or its encom-passing walls.53
Pulp Chamber CalcificationsIn teeth with diminished or severely calcified pulp chamber spaces (see Fig. 8-24, A), the pulp horns are usually no longer present. Excavation through solid tooth structure cannot be done without being oriented to the external anatomy of the tooth. Once the target areas are reached, the excavation should be inspected (preferably with some level of magnification and good light—loupes or microscope) for calcified discoloration,1 indicating the previous location of the pulp chamber. Probing with an endodontic explorer is also necessary, and although the canal orifices may not be obvious, they are often soft to probing with the explorer. An ultrasonic instrument for excavation, removal of calcified pulp chamber inclusions, and opening orifices is indispens-able41 (Fig. 8-25, A and B: ProUltra Tips [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]; Fig. 8-25, C: Smart X Tips [Dentsply Maillefer, Ballaigues, Switzerland]). If used without irrigation, the excavation process is easily observed through the operating microscope or loupes. Irrigation during the use of ultrasonic instruments may block visibility, but it also rinses materials, especially calcifications, from the field of operation. Both approaches should be considered in these situations.

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 163
A
B C
FIGuRE 8-25 A, ProUltra Tips as a group, showing a wide range of sizes and shapes (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA). B, Four of the more commonly used ProUltra tips. C, Start X Tips (Dentsply Maillefer, Ballaigues, Switzerland).
C
BA
FIGuRE 8-24 A, Blockage of diminished pulp chamber by a coronal restoration in a maxillary molar. B, Significant pulp chamber calcifications (arrows) that will impede direct access to canal orifices. C, Crown on the maxillary first molar that completely blocks the view of the pulp chamber.

164 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
FIGuRE 8-26 Loupes with magnification at ×3.5.FIGuRE 8-27 Multiple perforations of a mandibular molar due to aggressive and perhaps careless access procedures.
Use of Magnification During Access PreparationA special caution is in order regarding the use of magnifica-tion in the location of canals that are calcified or difficult to find. Under very high power magnification (×30), the depth of field is very shallow, and the field of vision is very narrow. In this situation, it is easy to become completely disoriented with the external anatomy of the tooth and the actual loca-tion of the ongoing excavation. To compound the problem, in a calcified tooth, every speck and slight discoloration can begin to look like the orifice of a canal under high magnifica-tion (×30) when using a microscope. This can lead to serious procedural errors. Continued reorientation under low-power magnification is essential during such excavation. This can be accomplished with loupes at ×2.5 or ×3.5 magnification (Fig. 8-26).
Under magnification, the pulpal horns must be distin-guished from the canal orifices. In some cases, the bur may need to be directed toward the largest or the only visible chamber and canal space, such as the distal canal of man-dibular molars or the palatal canal of maxillary molars (see Fig. 8-14). Time must be spent reviewing the radiograph prior to access to assess pulp chamber morphology—noting the coronal-apical and mesial-distal dimensions of the chamber space—and if possible the position of the orifices as they leave the pulp chamber floor. If calcifications are present, this task is even more challenging (see Fig. 8-24, B).
During access opening under magnification, a radiograph may be occasionally necessary to check the position of the excavated cavity. A second and vitally important technique to the successful location of all canals in a multicanaled tooth is to enlarge each orifice individually as it is located and before excavation is performed to locate others. This tech-nique will help provide proper spatial and visual orientation of the pulp chamber anatomy. Either the location of all canals will be confirmed, or the orientation will act as a guide to the location of the other unidentified canal orifices. Further, the potential of excavating in areas where no canal could possibly be found or (worse yet) perforating the wall or pulp
chamber floor will be avoided using the careful stepwise approach.
Preventing and Managing Coronal PerforationsAlthough many errors can occur during access preparations, the most deleterious is perforation of the pulp chamber space into the oral cavity or periodontal tissues.37,49,53 Attention to the radiographic position of the pulp chamber space before access opening preparation will often prevent this problem. Similarly, maintaining an orientation to the external anatomy and possessing knowledge of the anatomy of the floor of the pulp chamber and the location of the canal orifices will con-tribute to the prevention of perforations. Other consider-ations include making the initial bur preparation and access outline form in the tooth prior to dental dam isolation. At any time during the access preparation, the alignment and position of the bur can be verified radiographically (Fig. 8-27). In more difficult situations, such as the patient not having the ability to open the mouth sufficiently, specific portions of the tooth may be removed, such as a wall or cusp. In anterior teeth that are severely lingually inclined, prepara-tion of the access in the facial tooth surface is often a reason-able consideration.58
If, however, a perforation should occur, it should be rec-ognized as soon as possible. This can only be done through constant vigilance and assessment during access preparation. Early recognition will prevent needless irritation and further insult to the periodontal tissues.5 If the perforation occurs above the osseous crest in the gingival sulcus or above the free gingival margin, careful management is essential. Usually any hemorrhage can be controlled with a dry cotton pellet impregnated with a hemostatic agent if necessary (see later). The defect can be sealed temporarily or permanently at that time with a material appropriate for the location of the per-foration. Temporary materials may include zinc oxide eugenol (ZOE) or glass ionomer (GI), and permanent materials may include a bonded composite or core paste, a modified glass

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 165
materials can be covered with a fast-setting glass ionomer. This is essential with the present formulation of MTA to prevent rinsing it from its placement; present formulations take 2 to 4 hours to set firmly. Try to prevent or minimize pushing the repair material into the periradicular tissues. Once sealed, identification of the canal can proceed, and when it is identified, normal root canal procedures should be performed. Generally the prognosis is better with small per-forations that are discovered early and repaired immediately. Internal repairs can be successful with minimal damage to the supporting periodontium. If there has been significant damage to the periodontium, all forms of repair have a very guarded prognosis.
Large perforations in the furcation of premolars and molars are more problematic.20,54 If significant portions of the floor of the pulp chamber have been destroyed, the chance of successful repair is remote (Fig. 8-29, A). Similarly, cases that have been repaired with materials other than MTA20 or ZOE may have poorer long-term outcome owing to the lack of biocompatibility, especially if the material is forced through the defect into the periodontal tissues15 (see Fig. 8-29, B). It is usually impossible to remove the excess nonsurgically, but the attempt is likely to make the perforation larger and irritate the surrounding periodontium.
ionomer (compomer), or even amalgam if it will be included in and covered with a full crown.
If the perforation is at or below the osseous crest or into the furcation region, these procedures can be considered. First, attempt to control the hemorrhage with a dry, sterile cotton pellet or the large end of a sterile paper point. A hemostatic agent in small amounts may be considered, such as epinephrine 1:50,000 on a cotton pellet (various percent-ages of racemic epinephrine—#2 Pellets have 1.15 mg, and #3 pellets have 0.55 mg [Pascal Company Inc., Bellevue, WA, USA]). Ferric sulfate is another option (Cut-Trol [Ichthys Enterprises, Mobile, AL, USA]). Hemostatic agents provided for tissue retraction prior to tooth impressions may also work (Astringedent [Ultradent Products, South Jordan, UT, USA]; Traxodent [Premier Dental Products Co., Phila-delphia, PA, USA]). Avoid strong hemostatic agents that may cause significant damage and do not use formocresol. If the perforation is close to a canal orifice, locate the canal orifice and enlarge the orifice as much as possible away from the perforation before repair. Second, once the hemorrhage has been controlled, sealing with a thick mix of mineral trioxide aggregate (ProRoot MTA) (Dentsply Tulsa Dental Special-ties, Tulsa, OK, USA) would be ideal2,25-27 (Fig. 8-28). If MTA is not available, a thick mix of ZOE can be used. These
A B
C
FIGuRE 8-28 A, Perforation of chamber floor of a mandibular molar during access. B, Defect sealed with mineral trioxide aggregate. C, One-year reevaluation shows good tissue response, and patient functions without discomfort on the tooth.

166 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
of bur penetration should not be left to chance. Consider measuring the approximate depth by holding the bur against the radiograph to estimate relative positions of both the chamber and the furcation in molar teeth before cutting the access opening (Fig. 8-30).
In all situations, a thorough assessment of each tooth that has a crown and requires a root canal procedure can facilitate good treatment planning. Additional important information can be obtained by using bitewing radiographs (see Chapters 2 and 3). Options exist for crown retention when there is no damage due to caries, with the occlusal surface repaired after root canal procedures. If caries is present under the crown margins or potential avenues of caries under crown margins exist, the extent must be identified and eliminated. This may very often mean removal of the crown, especially when the tooth margins appear subgingival on either a periapical or bitewing radiograph. In the latter cases, crown lengthening may be indicated prior to doing any root canal procedures (see Chapter 18).
When full metallic crowns are present and made of non-precious alloys, access may be very difficult; burs may dull
Perforations in the coronal third, in particular in the furca-tion, have a highly guarded prognosis. With adjunctive peri-odontal, surgical, or orthodontic treatment (see Chapters 17 and 18),44 management with a simple surgical repair or root extrusion may result in a successful outcome. In some cases, however, internal repair cannot be accomplished, and an external surgical approach must be taken. Even in these cases, extraction may be indicated.
Because crown perforations can be devastating and result in tooth loss, a preventive approach to access opening is always advocated. In some cases, the initial outline form of the access can be made without the dental dam in place. This is especially helpful when there is a discrepancy between the long axis of the crown and the root. Upon placement of the dental dam and as the access opening is being cut, bur align-ment can be evaluated with radiographs. Sometimes specific portions of the crown must be removed to facilitate safe access to the chamber. Creative approaches and access prepa-rations done with a sound rationale are highlights of problem solving in this area.
Potential Problems in Access Openings Through Crowned Teeth or Teeth With Excessively Large RestorationsA significant number of all root canal procedures are per-formed through existing crowns. The presence of these metallic and metalloceramic restorations can add additional problems and challenges to those discussed previ-ously.17,45,51,52,58 Most of these concerns can be addressed (problems prevented or challenges met) when preparing an access opening through an artificial crown.
As with naturally occurring crown-root angulations, a thorough radiographic evaluation is necessary to identify divergently angled roots or rotated teeth. This may be diffi-cult if the pulp chamber is not visible. The exact location of the chamber may not be readily seen, and therefore the depth
A B
FIGuRE 8-29 A, Attempted repair of a large access perforation with zinc oxide eugenol cement resulted in acute onset of symptoms. The tooth was extracted. B, There would be minimal chance of successful removal of the excess repair material. Extraction was recommended.
FIGuRE 8-30 Estimation of pulp chamber depth by holding a bur mounted in the handpiece against a radiograph of the tooth to be operated.

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 167
In all cases, open the coronal outline of the access slightly greater than a standard-sized access to facilitate identification of possible avenues of leakage or fractures and canal location and exploration if necessary.48 The integrity of the crown resides in the gingival margins, not in the occlusal surface. As previously mentioned, conservation of tooth (crown) anatomy does not preclude using the necessary avenue of access (see Figs. 8-1 to 8-4), especially if restorations are to be remade.
Clinical Considerations in Preventing and Managing Problems in Tooth Isolation and Access Preparation• Clamping adjacent teeth should be considered if the
dental dam clamp cannot be positioned on the tooth to be treated (see Fig. 8-4, D). Further control of moisture can be achieved with dental and medical adhesives, a rubber base, floss, or temporary filling materials.4 Buildups can be done prior to access preparation, but oftentimes these are hollowed out, weakened, result in excess debris that may be pushed into the canals, or redone prior to final coronal restoration.35
• Crown lengthening should be considered before any root canal procedures are performed if isolation can only be achieved by clamping the tissue (see Chapter 18).33
• Temporary crowns should be removed before isolation and access whenever possible. Removal prevents dislodgment during canal preparation, potential contamination during or after treatment, unstable reference points, and leakage of irrigant into the mouth.
• A line can be drawn on the crown to indicate the angle of the root when creating an access opening under a
easily or break during use. Also, failure to use water spray and good evacuation during access preparation may leave large metallic particles in the chamber or orifices or even in the root canals.
In the case of artificial crowns (metalloceramic or com-plete ceramic), if the crown is to be retained, significant care must be taken to prevent fracture of the ceramic mate-rial.17,52,58,61 This is especially true if the crowns are of an older vintage. In cases of ceramic-type crowns, use water spray and new high-speed round diamond burs to gain access through the initial layer, which is a porcelain-type material.17 Cut the porcelain in a light, shaving manner as opposed to using heavy pressure and long cutting times. If the crown is metal-loceramic, a metal core will be present which requires the use of a Transmetal Bur (Dentsply Maillefer, Ballaigues, Switzer-land) (Fig. 8-31, A). This is then followed by a bur of choice to complete the access into the pulp chamber. Then the walls of the access opening are flared to the occlusal side for pos-terior teeth or the lingual side for anterior teeth to prevent contact with the intracanal instruments. This can be done safely with an Endo-Z bur (see Fig. 8-31, B).
If the crown is zirconium based, the initial cut is made with a coarse, medium to large, round diamond bur or special diamond bur (KS2 turbo-type diamond bur [Axis Dental Corp, Coppell, TX, USA]), which will expose a dense, white zirconia layer.17 The opening should be slightly larger than the anticipated final access opening. Once the initial layer has been penetrated, the thin zirconia substrate can be penetrated with a round diamond bur; it should be smaller than the initial outline to prevent cutting the lateral walls of the opening, which may promote fractures in the veneering porcelain. Advise the patient ahead of time of a possible fracture in these situations. New technologies using air abrasion to access these crowns appear to prevent the problems of damaging the porcelain veneer that overlies the zirconium base.45
A B
FIGuRE 8-31 A, Transmetal Bur (top) and Endo-Z bur (bottom) (Dentsply Maillefer, Ballaigues, Switzerland). B, The transmetal bur has many uses in addition to assisting in access openings. Here it is being used to section a crown prior to removal from a tooth.

168 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
response to a continual low-grade irritation1 (Fig. 8-35). Radiographically, calcification will appear complete, with histologic confirmation of complete canal closure except for a few small areas that contain minimal tissue remnants. Cal-cification is also known to occur as a result of vital pulp treatment with calcium hydroxide and other materials. See Chapter 7 for examples and discussion of these topics.
Successful identification of the parameters of the pulp chamber and canal orifice in this type of tooth is extremely difficult (see Chapter 13 for canal penetration in the presence
rubber dam. Failure to determine excessive root angulation often leads to a perforation (Fig. 8-32).
• Although their use is effective and indicated in many teeth, care must be exercised in crown penetration when using long-shank or surgical-length burs.
Problem Solving in Recognizing or Locating Canal Orifices
Calcification of the Dental Pulp and Pulp Canal SpaceDystrophic and excessive linear calcification in the root canal system is a frequently encountered problem in root canal procedures.1,13 The clinician must understand that pulpal calcifications are signs of pathosis, not the cause of them.39,47 The nature of the calcification is often unpredictable and can create significant clinical challenges. Over the life of the tooth, deposition of secondary dentin—whether normal or irritational—occurs in every tooth.1 When the pulp is sub-jected to rapid, overwhelming bacterial invasion or traumatic insult, little time may be available for normal reparative dentin formation. In these situations, the dental pulp may die rapidly, leaving the canal space patent but full of necrotic and often infected tissue (Fig. 8-33). Clinically and radio-graphically, the pulp chamber and canal system remain patent and easily accessible. However, if irritants impact the tooth slowly over a long period, both the pulp chamber and the pulp canal system undergo calcific changes that may impede access and canal identification during initial root canal procedures (Fig. 8-34).
The histologic appearance of the calcifying pulp, pulp chamber, and root canal space generally reflects a long-term
A B
FIGuRE 8-32 Incorrect angle of the handpiece and bur leads to serious subosseous perforations in a canine (A) and a premolar (B).
FIGuRE 8-33 Abscess is present in the dental pulp. No reparative dentin has formed on the walls; patency is ensured (H&E stain ×100).

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 169
the location of the orifice is best accomplished using an ultrasonic instrument (see Fig. 8-25) if available. If not, care must be exercised in penetrating farther with a high-speed bur to prevent a perforation. This approach to access and orifice identification requires knowledge of the normal pulp chamber location, root canal anatomy, and long axis of the roots, especially in posterior teeth. Accurate radiographs are essential for preoperative visualization and periodic assess-ment of bur penetration and orientation. Ultimately, the calcified orifice must be recognized when it has been reached.
For teeth with single canals, textbooks on root canal mor-phology have often overlooked an important anatomic fact:
of calcifications). Of the numerous techniques available to penetrate the chamber and locate the canal orifices, only those procedures known to be most effective in clinical prac-tice are considered here.
Initially the clinician must mentally visualize and project the normal spatial relationship of the pulp space onto a radiograph of the tooth. Then information from the two-dimensional radiographic image is correlated, if possible, with the three-dimensional morphology of the tooth (Fig. 8-36).19 Thereafter, access preparation is initiated with the rotary instrument directed toward the presumed location of the pulpal space. Refining this preparation and identifying
A
C D E
B
FIGuRE 8-34 A, Reparative dentin has built up in the coronal portion of a mandibular molar with evidence of dystrophic calcification and canal closure (B&B stain ×10). B, Diffuse calcification in the dental pulp appears as complete calcification on a radiograph (H&E strain ×40). C, Pulp stones block the canal pathway (H&E stain ×100). D, Tooth section showing the flow of the canal from the chamber may be patent, but calcification may be evident as the canal is entered. E, Coronal portion of a canal with partial mineralization of the pulp. While an explorer may stick into this material, penetration with a file may be difficult (H&E stain ×100).

170 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
the canal space is always located in the cross-sectional center of the root.19 Similarly, the pulp chamber is (or was, before calcification) located in the cross-sectional center of the crown.
Prior to access preparation in a tooth with a calcified pulp chamber, the distance from the occlusal surface to the pro-jected pulp chamber floor is measured from the preoperative periapical radiograph or preferably from a bite-wing radio-graph, which maximizes accuracy. This can also be done using a wide range of digital radiographic systems. An access cavity of normal size and shape is created in the crown to a depth equal to that of the pulp chamber floor in a noncalci-fied chamber (see Fig. 8-36).
A second important aspect of normal root canal anatomy is the geometric pattern of canal orifices found in the pulp chambers of teeth with multiple canals.60 These geometric patterns and their potential variations must be mentally pro-jected on the calcified pulp chamber floor with consideration for the direction of the canals as they leave the pulp chamber. This requires an astute integration of two-dimensional radio-graphic findings with three-dimensional tooth anatomy,6,29 coupled with a safe and dexterous movement of the rotary
A B C
FIGuRE 8-36 A, Normal mandibular molar without dystrophic calcification. Broken lines delineate anatomic central location of pulp chamber. B, A similar tooth with severe dystrophic calcification characterized by obliteration of the pulp chamber and apical recession of the canal orifices. Broken lines delineate the location of the former pulp chamber. C, Access preparation is shown diagrammatically to the precise depth and lateral extension as with a normal pulp chamber.
A B
C
FIGuRE 8-35 A, Mandibular incisors show evidence of severe calcification. B and C, Histologic appearance of what may be occurring in A is visualized. Canal narrowing and blockage is noted. (C, B&B stain ×10.)

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 171
45º
A
B
C D E
FIGuRE 8-37 A, Diagram of a maxillary incisor with dystrophic calcification. Broken lines delineate central location of former pulp chamber similar to the previous figure. B, Angle of access penetration is approximately 45 degrees to the long axis of the root. The access opening should extend incisogingivally to include the full middle third of the crown. C, No pulp chamber is found in the calcified canal. Continued bur penetration may result in a facial perforation. D, Facial perforation results from excessive bur penetration without adequate radiographic control for bur angulation and pulp canal depth. E, To prevent perforation, angle of bur is changed from 45 degrees to an angle as close to parallel as possible with the long axis of the root.
instrument or ultrasonic tip on the pulpal floor. To facilitate this approach to the location of fine or calcified canals, the following discussion is a consideration of access preparation of the calcified pulp chamber by each tooth type with canal variations.
Maxillary Central and Lateral Incisors and CaninesA maxillary incisor with dystrophic calcification is dia-grammed in Fig. 8-37, A. The root canal is located in the cross-sectional center of the root. If aesthetics and structural integrity were disregarded, the ideal location of the access preparation would be through the incisal edge58; however, the standard access preparation for this tooth is in the exact center of the palatal surface of the crown, buccal lingually and incisal gingivally (Fig. 8-38, A). At an angle of roughly 45 degrees to the long axis, bur penetration of 3 to 4 mm will generally intersect with the pulp chamber in average-sized teeth (see Fig. 8-38, B). In a calcified chamber, however,
continued penetration at 45 degrees to the long axis will eventually pass over the canal entirely and result in perfora-tion of the labial root surface below the gingival attachment. Therefore when the chamber is calcified and the canal has not been located after 3 to 4 mm of penetration, the bur must be rotated to be as parallel as possible to the long axis of the tooth to prevent perforation. Penetration proceeds down the lingual aspect of the access preparation with fre-quent exploration with the DG-16 endodontic explorer for the orifice. In deep excavations, the bur may be changed to a long-shank No. 2 round bur (or switch to an ultrasonic tip). Visual and radiographic reassessment of direction is frequently necessary. Sometimes the canal is never found, and treatment plans must be revised.
Maxillary PremolarsThe point of coronal penetration for access begins in the center of the occlusal surface and follows the long axis of the tooth.12,59 Because the pulp chamber is wide buccal lingually in both one- and two-canaled premolars, the chamber must

172 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
A B
FIGuRE 8-39 Typical access shape and canal morphology of a single-canal premolar (A) and a two-canal premolar (B). Access is wide buccal lingually and narrow mesial distally.
XXXXX
A B
FIGuRE 8-40 A, Occlusal view of a maxillary molar shows a standard access preparation. By locating and flaring the orifices of two canals, the location of the third canal (X) is consistently and accurately determined. B, After the three primary canals have been located, the orifice of the second mesial buccal canal can be located by troughing 0.5 to 5.0 mm toward the palatal canal orifice. Most second canals will be found 1 to 3 mm from the primary mesial buccal canal orifice (X).be cut wide buccal lingually but should remain narrow mesial
distally (Fig. 8-39, A-B, see also Fig. 8-21, A).
Maxillary MolarsThe most common design for access preparation is a triangle formed by the orifices of the two buccal canals and the palatal canal.7,11,29,55,60 In many molars with calcified cham-bers or canals, it is common to find one or two orifices initially without much difficulty. However, the other orifices may not be readily identified. In these situations, a mental image of the geometric pattern of the canals is invaluable6,7 (Fig. 8-40, A). In the case of maxillary molars, these teeth have a high potential for having four orifices and possibly four separate canals (see Fig. 8-40, B). For a second canal in the mesial buccal root,46,56 a slot or trench is usually exca-vated in a straight line toward the palatal orifice from the primary mesial buccal canal orifice. Generally if a second mesial buccal orifice or mesial palatal is present, it will be anywhere from 0.5 to 5 mm toward the palatal orifice and
often located under a cervical ledge. Occasionally the orifice to the fourth canal will actually be located 1 to 2 mm into the mesial buccal orifice or even the palatal orifice (see Fig. 8-23, C and D).
Mandibular Incisors, Canines, and PremolarsThe most common canal morphology for mandibular inci-sors, canines, and premolars is a single canal; a second canal, if present, will almost invariably be found lingual to the first canal19 (see Fig. 8-15, A and B). In the incisors and canines, second canals are particularly difficult to locate (even when minimal calcification is present) because of the angulation of the anatomic crown or the location of the standard access cavity on the lingual aspect (Fig. 8-41). After the main canal
A B
FIGuRE 8-38 A, Central incisor with calcified chamber and questionable canal. B, After deep penetration the canal could still not be found, although it appears visible on the radiograph. Patient opted for periapical surgery.

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 173
CBA
FIGuRE 8-41 A, In a two-canal mandibular incisor, the standard access preparation will invariably place the initial instrument in the facial canal, passing over the orifice of the second canal. B, Second canals in mandibular canines and premolars are almost always found on the lingual aspect. Most diverge at significant angles from the facial canals and require negotiation with very fine instruments. C, Radiograph of an extracted first premolar exhibits two distinct canals from a proximal view.
M D
X
A B
FIGuRE 8-42 A, Mandibular molar with a two-canal morphology will have both orifices on the mesial distal midline. B, If two canals are located in a mandibular molar, and the mesial orifice is distinctly buccal or lingual to the mesial distal midline, a second canal in the mesial root (X) is probable.
is located and débrided, it is important to widen the orifice lingually and probe for the second orifice using a No. 10 or 15 K-file with an abrupt curve placed 1 or 2 mm from the tip of the file. If the canal is not located with this technique, using Nos. 2, 3, and 4 Gates-Glidden drills or orifice shapers on the lingual surface may be helpful in uncovering the orifice of a lingual canal. The drill is used in the manner of the round bur and is drawn up the lingual surface in a sweep-ing motion. Breakage may occur during this motion, but the fracture typically occurs high on the shank, and such a posi-tion allows easy removal of the segment. If the canal is found with either technique, even a normal-sized second canal is usually as fine as any calcified canal.
Mandibular MolarsThe most common morphology for access preparation in mandibular molars is a trapezoid formed by the two canals in the mesial root and the oval canal in the distal root7,11,19 (see Fig. 8-21, C and D). The distal canal is commonly found to be wide buccal lingually, with a morphology that requires separate preparation of the buccal and lingual aspects of the canal. In roughly 30% to 50% of cases, the distal canals will be separate, making it necessary to make a wide buccal- lingual excavation in the distal root in calcified canals. A small percentage of second molars will have only one canal in each root. If one canal is located in the mesial root, it is wise to enlarge its orifice as previously described and assess the symmetry of the orifice geometry. In a two-canal mor-phology, both canals will be in the mesial distal midline (Fig. 8-42, A). If after orifice widening, the mesial canal is asym-metrically located to the buccal or lingual side relative to the distal canal, the mesial root probably has two canals. The
second canal can be envisioned as completing the trapezoid initially described (see Fig. 8-42, B). Again, making a groove in excavating for the calcified orifice is recommended because it may be either quite close to the located canal or as far as 3 to 4 mm away. As with the fourth canal in the maxillary molar, the orifice of either the mesial buccal or the mesial lingual canal may be located 1 to 2 mm into the singly identi-fied mesial orifice.
Although the majority of attempts to locate canal orifices in the presence of severe calcification will be successful, the potential for perforation always exists. Probing with the explorer will yield the characteristic “stick,” if in fact the excavation has come too close to the root surface and the explorer is actually penetrating a thin area of remaining dentin. This type of procedural accident must be detected as early as possible to ensure that injury to underlying bone can be kept to a minimum. Another common sign of accidental perforation is bleeding. The clinician must immediately

174 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
explorer should be in the position where the canal is believed to be and the probe should be positioned at the angle at which the excavation is being done. Often, the radiograph will confirm that the direction of excavation is accurate (Fig. 8-43). Occasionally, the direction of excavation is found to be in error. With the aid of the radiograph, the direction of excavation can be corrected and the canal can be located (Fig. 8-44).
Details on the initial and subsequent problem-solving techniques for the penetration of orifices and canals that exhibit calcifications will be found in Chapter 13, which deals with anatomically compromised root canal systems. However, once the orifice has been located, the use of heated
discern whether a bleeding point is the true canal orifice with a hemorrhagic pulp or a perforation to an external surface. First, a visual analysis of the external and internal anatomy will give an indication if the bleeding point is reasonably close to the position of a canal. Secondly, a radiograph can be made with very small file (.06 or .08) inserted into the bleeding point. This exposure is for location only. No attempt effort should be made to enlarge the orifice until it is confirmed that it is the canal. At the earliest point of discovery of a perforation, repair with MTA should be done.
To assist in the location of a calcified canal and to avoid possible perforation it is often helpful to radiograph the tooth with an endodontic explorer in the excavation. The tip of the
A B
FIGuRE 8-43 A, mandibular molar under endodontic treatment with calcified distal orifice. Endodontic explorer is radiographed in excavation to confirm location and direction of access procedure. B, Successful location and negotiation of canal.
A B
FIGuRE 8-44 A, Maxillary lateral with calcified canal under endodontic treatment. Endodontic explorer indicates aberrant excavation pathway. B, Successful completion of root canal treatment after correction of pathway direction and location of canal.

chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations 175
(37°C) sodium hypochlorite (NaOCl) solution is recom-mended10 as a soak in the chamber; this will assist in the digestion of any debris with an organic component. While room temperature NaOCl is also effective, a heated solution (even up to 45°C) will act rapidly to assist the clinician in débridement. This may actually include some of the debris located in the orifice, especially if the explorer can begin to penetrate 1 to 3 mm into the canal.
Clinical Considerations in Preventing and Managing Problems in Orifice Identification• Locating the orifice is best accomplished using a DG-16
explorer. The explorer will not penetrate and stick in solid dentin, but if an orifice is present, firm pressure will slightly force the instrument into the orifice, and it will resist dislodgement or stick.
• The location of the canal can be confirmed radiographically, leaving the explorer in place. Magnification in the form of telescopic loupes or an operating microscope is extremely useful. However, it is often more useful to excavate the area where an orifice is likely to be found under lower magnification to maintain an awareness of the overall anatomy of the tooth.
• The location of the orifice can often be determined by the color of the dentin, sometimes referred to by the term dentinal mapping. The orifice may appear as a whitish spot in a general field of yellowish dentin. If such a location is consistent with the expected anatomic position of the orifice, the area should be firmly probed with the DG-16 explorer.
• Calcifications over the orifice can be removed with the ultrasonic instrument and a probe-type tip. The
ultrasonic instrument can be used either wet or dry to excavate calcification. As excavation proceeds, the DG-16 explorer is used frequently to probe for the orifice. If the canal cannot be located, a radiograph of the excavation should be exposed to check the position at the deepest point of penetration. Placing an endodontic instrument or an explorer in the excavation before radiographic exposure will often aid in assessing direction and position.
• Fiberoptic light transmission from the buccal or lingual surface when an artificial crown is not present may also assist in orifice location (Fig. 8-45).
• Using a small amount of methylene blue 1% on the pulp chamber floor (see Fig. 8-6, C) may help identify the pooling of poorly mineralized dentin that may fill a partially calcified orifice. It may also help identify or confirm the presence of fractures.45
REfEREnCES1. Amir FA, Gutmann JL, Witherspoon DE: Calcific metamorphosis:
a challenge in endodontic diagnosis and treatment, Quintessence Int 32:447-455, 2001.
2. Bargholz C: Perforation repair with mineral trioxide aggregate: a modified matrix concept, Int Endod J 38:59-69, 2005.
3. Barkmeier WW, Cooley RL, Abrams H: Prevention of swallowing or aspiration of foreign objects, J Am Dent Assoc 97:473-476, 1978.
4. Bramwell JD, Hicks ML: Solving isolation problems with rubber base adhesive, J Endod 12:363-367, 1986.
5. Beavers RA, Bergenholtz G, Cox CF: Periodontal wound healing following intentional root perforations in permanent teeth of Macaca mulatta, Int Endod J 19:36-44, 1986.
6. Chogle S, Mickel AK, Self M, et al: A correlation study of occlusal and pulp chamber anatomy: the maxillary first molar, Gen Dent 55:218-220, 2007.
7. Christie WH, Thompson GK: The importance of endodontic access in locating maxillary and mandibular molar canals, J Can Dent Assoc 60:527-532, 535-536, 1994.
8. Cochran MA, Miller CH, Sheldrake MA: The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment, J Am Dent Assoc 119:141-144, 1989.
9. Cohen SC: Endodontics and litigation: an American perspective, Int Dent J 39:13-16, 1989.
10. Cunningham WT, Balekjian AY: Effect of temperature on collagen dissolving ability of sodium hypochlorite endodontic irrigant, Oral Surg Oral Med Oral Pathol 49:175-177, 1980.
11. Deutsch AS, Musikant BL: Morphological measurements of ana-tomic landmarks in pulp chambers of human maxillary and man-dibular molar pulp chambers, J Endod 30:388-390, 2004.
12. Deutsch AS, Musikant BL, Gu S, et al: Morphological measure-ments of anatomic landmarks in pulp chambers of human maxil-lary furcated bicuspids, J Endod 31:570-573, 2005.
13. Dodds RN, Holcomb JB, McVicker DW: Endodontic manage-ment of teeth with calcific metamorphosis, Compend Cont Educ Dent 6:515-520, 1985.
14. Editorial: Treatment of blind abscess (root canal treatment), Dominion Dent J 12:231-233, 1900.
15. ElDeeb ME, ElDeeb M, Tabibi A, et al: An evaluation of the use of amalgam, Cavit, and calcium hydroxide in the repair of furca-tion perforations, J Endod 8:459-466, 1982.
FIGuRE 8-45 Placement of a fiberoptic light on the buccal wall to enhance intrachamber visibility when searching for canal orifices.

176 chapter 8 | Problem Solving in Tooth Isolation, Access Openings, and Identification of Orifice Locations
16. European Society of Endodontology: Quality guidelines for end-odontic treatment: consensus report of the European Society of Endodontology, Int Endod J 39:921-930, 2006.
17. Graham L, Little DA: Endodontic access in zirconia restorations, Contemp Esthet Restor Pract 7:2-3, 2003.
18. Gutmann JL: Prevention and management of endodontic proce-dural errors, N Z Soc Endod Newsl 23:15-36, 1983.
19. Gutmann JL, Harrison JW: Surgical endodontics, Boston, 1991, Blackwell Scientific Publications.
20. Hamad HA, Tordik PA, McClanahan SB: Furcation perforation repair comparing gray and white MTA: a dye extraction study, J Endod 32:337-340, 2006.
21. Heling B, Heling I: Endodontic procedures must never be per-formed without the rubber dam, Oral Surg Oral Med Oral Pathol 43:464-466, 1977.
22. Hermsen KP, Ludlow MO: Disinfection of rubber dam and tooth surfaces before endodontic therapy, Gen Dent 35:355-356, 1987.
23. Hill EE, Rubel BS: Do dental educators need to improve their approach to teaching rubber dam use? J Dent Educ 72:1177-1181, 2008.
24. Hofheinz RH: Immediate root filling, Dent Cosmos 34:182-186, 1892.
25. Holland R, Bisco Ferreira L, de Souza V, et al: Reaction of the lateral peridontium of dog’s teeth to contaminated and uncontami-nated perforations filled with mineral trioxide aggregate, J Endod 33:1192-1197, 2007.
26. Holland R, Filho JA, de Souza V, et al: Mineral trioxide aggregate repair of lateral root perforations, J Endod 27:281-284, 2001.
27. Juárez Broon N, Bramante CM, Assis GF, et al: Healing of root perforations treated with mineral trioxide aggregate (MTA) and Portland cement, J Appl Oral Sci 14:305-311, 2006.
28. Khabbaz MG, Serefoglou MH: The application of the buccal object rule for the determination of calcified canals, Int Endod J 29:284-287, 1996.
29. Krasner P, Rankow HJ: Anatomy of the pulp-chamber floor, J Endod 30:5-16, 2004.
30. Leeb IJ: Canal orifice enlargement as related to biomechanical preparation, J Endod 9:463-470, 1983.
31. Liebenberg WH: Access and isolation problem solving in end-odontics: anterior teeth, Can Dent J Assoc 59:663-671, 1993.
32. Liebenberg WH: Access and isolation problem solving in end-odontics: posterior teeth, Can Dent J Assoc 59:817-822, 1993.
33. Lovdahl PE, Gutmann JL: Periodontal and restorative consider-ations prior to endodontic therapy, J Acad Gen Dent 23:38-45, 1980.
34. Love RM, Firth N: Histopathological profile of surgically removed persistent periapical radiolucent lesions of endodontic origin, Int Endod J 42:198-202, 2009.
35. Lynch CD, McConnell RJ: Attitudes and use of rubber dam by Irish general practitioners, Int Endod J 40:427-432, 2007.
36. Mala S, Lunch CD, Burke FM, et al: Attitudes of final year dental students to the use of rubber dam, Int Endod J 42:632-638, 2009.
37. Martin LR, Gilbert B, Dickerson AW: Management of endodontic perforations, Oral Surg Oral Med Oral Pathol 54:668-677, 1982.
38. Moreinis SA: Avoiding perforation during endodontic access, J Am Dent Assoc 98:707-712, 1979.
39. Moss-Salentijn L, Hendricks-Klyvert M: Calcified structures in human dental pulps, J Endod 14:184-189, 1988.
40. Oswald RJ: Procedural accidents and their repair, Dent Clin North Am 23:593-616, 1979.
41. Plotino G, Pameijer CH, Grande NM, et al: Ultrasonics in end-odontics: a review of the literature, J Endod 33:81-95, 2007.
42. Robinson D, Goerig AC, Neaverth EJ: Endodontic access: an update, part I, Compend Contin Educ Dent 10:290-292, 294-296, 298, 1989.
43. Robinson D, Goerig AC, Neaverth EJ: Endodontic access: an update, part II, Compend Contin Educ Dent 10:328-330, 332-333, 1989.
44. Roda RS: Root perforation repair; surgical and nonsurgical man-agement, Pract Proced Aesthet Dent 13:467-474, 2001.
45. Sabourin CR, Flinn BD, Pitts DL, et al: A novel method for creat-ing endodontic access preparations through all-ceramic restora-tions: air abrasion and its effect relative to diamond and carbide bur use, J Endod 31: 616-619, 2005.
46. Seidberg BH, Altman M, Guttuso J, et al: Frequency of two mesio-buccal root canals in maxillary permanent molars, J Am Dent Assoc 87:852-856, 1973.
47. Selden HS: Radiographic pulpal calcifications: normal or abnormal—a paradox, J Endod 17:34-37, 1991.
48. Shankle RJ: Extension for convenience in root canal therapy, J Acad Gen Dent 29:62-64, 1981.
49. Sinai IH: Endodontic perforations: their prognosis and treatment, J Am Dent Assoc 95:90-95, 1977.
50. Stewardson DA: Endodontics and new graduates: Part I, practice vs training, Eur J Prosthodont Restor Dent 10(3):131-137, 2002.
51. Stewardson DA: Endodontic standards in general practice—a survey in Birmingham, Part I, Eur J Prosthodont Restor Dent 9(3-4):107-112, 2001.
52. Sutherland JK, Teplitsky PE, Moulding MB: Endodontic access of all-ceramic crowns, J Prosthet Dent 61:146-149, 1989.
53. Tidmarsh BG: Accidental perforation of the roots of teeth, J Oral Rehabil 6:235-240, 1979.
54. Tsai YL, Lan WH, Jeng JH: Treatment of pulp floor and stripping perforation by mineral trioxide aggregate, J Formos Med Assoc 105:522-526, 2006.
55. Velmurugan N, Venkateshbabu N, Abarajithan M, et al: Evaluation of the pulp chamber size of human maxillary first molars: an institu-tion base in vitro study, Indian J Dent Res 19(2):92-94, 2008.
56. Weine FS, Healey HJ, Gerstein H, et al: Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance, Oral Surg Oral Med Oral Pathol 28:419-425, 1969.
57. Whitworth JM, Seccombe GV, Shoker K, et al: Use of rubber dam and irrigant selection in UK general dental practice, Int Endod J 33:435-441, 2000.
58. Whitworth JM, Walls AWG, Wassell RW: Crowns and coronal restorations: endodontic considerations: the pulp, the root-treated tooth and the crown, Br Dent J 192:315-327, 2002.
59. Wilcox LR, Walton RE: The shape and location of mandibular premolar access openings, Int Endod J 20:223-227, 1987.
60. Wilcox LR, Walton RE, Case WB: Molar access: shape and outline according to orifice locations, J Endod 15:315-318, 1989.
61. Wood KC, Berzins DW, Luo Q, et al: Resistance to fracture of two all-ceramic crown materials following endodontic access, J Prosthet Dent 95:33-41, 2006.
62. Yusuf H: The significance of the presence of foreign material peri-apically as a cause of failure of root treatment, Oral Surg 54:566-574, 1982.
63. Zinman EJ: Endodontic records and legal responsibilities. In Cohen S, Hargreaves KM, editors: Pathways of the pulp, ed 9, St Louis, 2006 Mosby Elsevier.

177
Chapter 9
Problem Solving in Working Length Determination
Problem-Solving ListProblem-solving issues and challenges in working length determination addressed in this chapter are:
Anatomic Basis for Challenges With Working Length Determination
Apical Root Anatomy and Its Impact on Working Length
Working length determination: radiographic technique
Working length determination: electronic apex locator
Working length determination: other clinical techniques
Controversies and Challenges With the Pulpal and Periapical Status and Their Impact on Working Length Determinations and Choices
Posttreatment Implications and Outcomes of Root Canal Treatment Based on Working Length Philosophies
The healing processes after removal of a pulp occur in the tissue immediately adjacent to the point where the pulp was severed. It is, therefore, of great importance to retain the vitality of these tissues in order to make healing possible.35
R. KROnfeLD, 1933
For many years, the tooth apex has been the focus of many anatomic and treatment studies.* Anatomic variations in this region have been accepted as the norm, but contemporary treatment parameters involving these aberrations still present challenges and controversies.
Anatomic Basis for Challenges With Working Length Determination
The apex of the mammalian tooth is a complex biological unit composed of cementum, dentin, blood vessels, nerves, and connective tissues. One of the factors determining the long-term success of root canal treatment has been shown to be the relationship between instrumentation and obturation procedures and the anatomy of the apex.41,47,53 A clear under-standing of the morphology of the root canal system, includ-ing the apex, is imperative.
Root formation and development are determined by the Hertwig’s epithelial root sheath (HERS), which maps out the external form of the root. The HERS is a double layer of epithelial cells derived from a proliferation of the internal and external dental epithelium (Fig. 9-1). The rim of this sheath, the epithelial diaphragm, encloses the primary apical foramen. Multirooted teeth form as a result of the division of the primary apical foramen into two or more sections by “tongues” of epithelium growing inwards from the HERS.
If the tooth is uncomfortable, however, or presents an area of rarefaction, apical access must be obtained in order to negotiate the canal throughout its entire length to reach the periapical tissues.24
L.I. GROSSmAn, 1946
Factors that may influence a difference [in the method used for working length determination] include the quality of radiographs, superimposed anatomic structures, or anomalous positions of root canal foramen.
D.H. PRATTen, n.J. mCDOnALD, 1996
*References 2-5, 11, 12, 15, 25, 26, 31, 35, and 36.

178 chapter 9 | Problem Solving in Working Length Determination
Internal morphology at the end of the root canal is deter-mined by the odontoblasts responsible for development of the dentin. The transition from internal to external morpho-logic features occurs at the cementum-dentin junction (CDJ), delineated histologically by the odontoblasts. Coronal to this position, the tissue is classified as pulp tissue. However, the soft tissue contained within that portion of the canal apical to the CDJ is not dental pulp but a fibrous connective tissue that originates from the periodontal ligament and supplies the vessels and nerves leading to and from the pulp (Fig.
Therefore, the root sheath determines the number, size, and external morphology of the roots. Following initiation of root formation, the HERS becomes fragmented and forms a fenestrated network known as the epithelial cell rests of Malas-sez. As the root sheath disintegrates, cells of the connective tissue differentiate into cementoblasts, and cementum is deposited on the dentin. Should the HERS disintegrate before dentin is elaborated, a lateral canal will be formed (Figs. 9-2 to 9-4)—an anatomic entity that has its own clini-cal implications (see Chapter 18). Development of root length is complete approximately 3 to 4 years after tooth eruption, with apical closure occurring some years later.
Extensive variability exists in the external apical root mor-phology of human permanent teeth with completed root apices (Fig. 9-5). In young teeth with incompletely formed apices, a funnel-shaped opening containing connective tissue (the dental papilla) is the typical appearance (Fig. 9-6). As the apex matures, the opening closes, and cementum is deposited on the apex continuing throughout life to com-pensate for loss of coronal tooth structure due to erosion, abrasion, or attrition. This gradual change in the morphology of the “normal” apical complex has been demonstrated,35 with further studies indicating that with increasing age, the center of the foramen deviates more and more from the vertex or apical center.55 Resorptive processes will also alter the morphology of the apical complex (Figs. 9-7 and 9-8; also see Chapters 3, 13, and 19). These resorptive processes may be the result of normal remodeling, orthodontic tooth movement, or inflammation of the pulp or periradicular tissues.
HERS
fIGURe 9-1 Remnants of the Hertwig epithelial root sheath (HERS) (arrow) in the developing root structure. This is a layer of inner and outer enamel epithelium responsible for root formation as it invaginates into the alveolar bone.
fIGURe 9-3 Large lateral canal leaving the mesial canals and exiting on the distal surface of the mesial root, as evidenced by filling during obturation. Note lateral lesion.
fIGURe 9-2 Palatal view of a mesial buccal root from a maxillary first molar, showing multiple foramina in the apical third of the root.

chapter 9 | Problem Solving in Working Length Determination 179
A B
fIGURe 9-4 A, Histologic evidence of a large lateral canal in cross-section of the mandibular premolar. Note development of a cystic lesion on the lateral surface of the root. B, SEM (scanning electron microscopy) view of a lateral canal (×1800).
fIGURe 9-5 Multiple apical terminations pose clinical problems for working length determination, cleaning and shaping, disinfection, and obturation.
P
fIGURe 9-6 Overall view of an immature root that is forming shows a large dental papilla and advancing root sheath, left and right. Arrow indicates remnants of the epithelial sheath.
A B
fIGURe 9-7 A, Resorbed root apex. B, SEM (scanning electron microscopy) of the same root apex shows significant irregularities. (×2000).

180 chapter 9 | Problem Solving in Working Length Determination
fIGURe 9-8 Radiograph showing apical resorption of the root apices of two teeth. Tooth on the left has an apical invaginating external resorptive defect that alters the position of the cemental-dentinal junction.
PDL
RCF
fIGURe 9-9 Root apex following root canal filling (RCF) short of the actual root length. Histologic evidence of hard-tissue formation (black arrows) that has formed from cells of the periodontal ligament (PDL) adjacent to root filling material. Note cementum formation (white arrows) on internal aspect of apical foramen.
fIGURe 9-11 Apical delta formation in a demineralized and cleared tooth. Note presence of pulp stones in multiple small canals.
fIGURe 9-10 Multiple possibilities for canal termination at the cemental-dentinal junction.
9-9).5 The walls of that portion of the canal as it enters the periodontal ligament (PDL) are covered with cementum. The root canal system tapers from the coronal end to its nar-rowest part, the constriction (minor foramen), which is usually but not necessarily within dentin. Early investigations indicated that the “pulp canal anatomy becomes extremely variable in the apical third.”5 Contemporarily, the internal morphology of the constriction has been classified into five main types: single constriction point, tapering constriction, multiple constriction, parallel constriction, and blocked (Fig. 9-10).17 Apical to the constriction, the root canal system diverges again to the major foramen that is within cementum. This hourglass shape dictates that canal cleaning, shaping, and obturation should be confined within dentin and not extend beyond the apical constriction or minor foramen.
The apical portion of the root canal system presents the greatest number of ramifications, with 27.4% of teeth dem-onstrating accessory and lateral canals or an extensive arbori-zation, also known as an apical delta (Fig. 9-11; also see Fig.

chapter 9 | Problem Solving in Working Length Determination 181
P
A B
fIGURe 9-12 A, Position of apical foramen is coronal to root apex. B, Histologic evidence and verification of this position (H&E stain ×4).
extrusion of debris, medicaments used in root canal proce-dures, and obturation materials can be minimized, thereby preventing postoperative complications.10,14,31,37,60
The seventh edition of the Glossary of Endodontic Terms defines the working length of a tooth as the distance from a coronal reference point to the point at which canal prepa-ration and obturation should terminate.21 To this purpose, the ideal apical terminus of the working length has been identified histologically as the CDJ. This junction is typified by a constriction or narrowing of the canal space (minor constriction) that provides an ideal point to prepare an apical seat in sound dentin. However, as previously mentioned, there can be vast variability in the nature of this constriction that will have an impact on any technique of working length determination.26,43,44 Furthermore, the constriction should not be confused with the apical foramen (major constric-tion), since the constriction is rarely if ever at the tip of the root.7,8,10,27-29
The distance from the foramen to the constriction depends on a multitude of factors such as increased cemental deposi-tion or radicular resorption (Fig. 9-13, A). Both processes are strongly influenced by multiple factors. Especially in peri-odontal disease states, the CDJ location has no predictable anatomic appearance or location, owing to resorptive pro-cesses or cemental depositions that may extend well into the root canal (see Fig. 9-13, B). The foreman and CDJ position on the root can be highly variable and exist anywhere from the direct radiographic apex up to 3 mm or more coronal to the radiographic apex, depending on a particular root mor-phology (Fig. 9-14). These potential anatomic variances have had a major impact on the precise region or location for determining the working length and termination of root canal instrumentation and obturation.
9-5).16 Their existence necessitates the use of adjuncts to mechanical cleaning and shaping to ensure thorough débride-ment of the root canal system (see Chapters 10 and 11). In all likelihood, the cleaning of these aberrant structures is all but impossible; in actuality, the tissues contained within these ramifications may contribute to ultimate apical healing.3,31
Studies have shown that the major foramina of most human teeth are distant from both the radiographic and anatomic apex9,36 (Fig. 9-12). Likewise, the major foramen is distant from the minor foramen or constriction by an average distance of 0.5 mm (see Fig. 9-12, B).9 All these anatomic variations directly affect clinical decisions made during root canal treatment, such as where shall the root filling end?30 It is easy to conjecture where this ideal position should be located, but more often than not, achieving this goal may elude the clinician. Ultimate clinical success and radiographic findings usually confirm or disprove this choice in treatment.41,47,53
Apical Root Anatomy and Its Impact on Working Length
It is frequently impossible to know exactly where the apical foramen and apical constriction are located until after the canal has been obturated.30 However, knowledge of the pos-sible three-dimensional variations (e.g., resorption or changes due to age, trauma, orthodontic movement, periradicular pathology, or periodontal pathosis) may prevent significant damage during working length determination and instru-mentation to the cementum that has formed around the apical dentin and to the periapical tissues.18 In addition,

182 chapter 9 | Problem Solving in Working Length Determination
Current concepts of initial canal penetration recommend preflaring techniques for a coronal-to-apical approach to working length determination rather than immediate pene-tration to the apex region.39,54 Emphasis is placed on straight-line access to the radicular third of the canal, and considerable time and effort is spent preparing the coronal two-thirds of the root prior to apical penetration.39,54 This eliminates coronal impingements on the working length instrument and enhances penetration to the CDJ.
In curved canals, however, after obtaining straight-line access, the working length can change, especially if debris is packed around the curvature and not removed on a regular basis. Techniques have been advocated for this purpose, and cognizant use of them is recommended.38 If working length is obtained prior to straight-line access, it may be 1 mm less or even shorter after preparing the coronal two-thirds. Straight-line access eliminates the bend at the canal orifice and places the file in a more upright position closer to the reference point. A more accurate working length will be obtained after straight-line access in the canal is established (Fig. 9-15). This does not preclude obtaining a preliminary working length prior to preparing the coronal two-thirds if necessary to assist in overall knowledge of root shape, canal morphology, foramen patency, and to prevent canal block-age. Knowledge of average tooth length, tactile feel, or the use of digital radiography may provide tools for this purpose. However, once straight-line access is achieved, a more precise working length should be obtained.
During access opening preparation, all caries, unsup-ported enamel, and faulty restorations are removed in an effort to secure stable reference points as aids in working length determination (see Chapter 8). This is especially helpful when more than one appointment is required to complete treatment. Typical reference points are those that are closest to the file and can be identified accurately as the cleaning and shaping process develops.18 If significant coronal destruction exists and extensive restorative procedures are
Prior to establishing a definitive working length, coronal access to the pulp chamber must provide a straight-line avenue into the canal orifice, thereby facilitating subsequent canal penetration (see Chapter 8). In anterior teeth, failure to remove the lingual ledge or incisal edge often impedes this straight-line access, resulting in lack of depth penetration to the CDJ, failure to locate all canals present, or instrument penetration into the canal wall with ledge formation. In posterior teeth, primarily molars, or multirooted premolars, failure to remove cervical ledges or bulges results in missed canals or binding of the penetrating instrument in the coronal third of the canal with ledge formation (see Chapter 8). The ability to penetrate unimpeded to the CDJ is crucial to deter-mining the working length of the root canal.
A B
fIGURe 9-13 A, Mandibular molar with apical root resorption due to a necrotic, infected dental pulp that destroyed the natural cemental-dentinal junction. B, Histologic evidence of apical resorption on external cementum (black arrows) and layering of cementum (white arrows) into apical foramen (H&E stain ×10).
fIGURe 9-14 Apical view of tooth with a C-shaped root formation. Note root morphology around the canal exits as cementum invaginates into the foramen. K-files (arrows) are exiting from the canal long before they reach the actual root surface. Actual foramina are much larger than canal exits, as indicated by widths of the red lines. Working length determination to the root length in these cases would be destructive to periapical tissue.

chapter 9 | Problem Solving in Working Length Determination 183
lingual resorption cannot be discerned until 20% to 40% of the root structure has been demineralized and evidences some type of replacement resorption.1 If apical resorption presents radiographically with a scalloped or uneven proximal margin, significant three-dimensional resorption has already occurred, further complicating working length determination. Cre-ation of an apical stop or enhancing an apical narrowing or
fIGURe 9-15 When curves are present, as seen in the mesial buccal root, straight-line access is essential.
A B
fIGURe 9-16 A, Histologic demonstration of invasive apical resorption and how it destroys the cemental-dentinal junction. B, Working length established at the most narrow point in the canal when invasive apical resorption is present (arrow).
anticipated, it is helpful to reduce unsupported tooth struc-ture to prevent possible fracture between appointments, which may not only complicate the working length measure-ment already established but may also prevent associated periodontal and restorative problems should the fracture occur through the periodontal ligament (see Chapter 17).
Pathologic processes resulting in apical resorption can destroy the natural constriction of the CDJ (Fig. 9-16). This will create difficulty in locating a biologically acceptable posi-tion at which to establish the working length. The resorptive process generally produces a root end with an uneven, irregu-lar radiographic appearance with few clues about where to prepare an apical stop. While the extent of proximal surface root end resorption may be discernible, the degree of buccal and lingual tooth loss is distinctly ambiguous. Buccal or
CLINICAL PROBLEMProblem: A 19-year-old male presented with mild discom-fort in his maxillary left canine. He had been wearing orth-odontic appliances for 18 months. The tooth was slightly tender to percussion and palpation and gave a significantly reduced response to sensibility testing compared to the con-tralateral canine. A radiograph showed evidence of significant resorption on the mid-mesial surface and a suggestion of resorption at the apex (Fig. 9-17, A).8 Of concern was the extent of the mesial resorption and whether or not a simple root canal procedure would stop the resorptive process. At issue was the location of the working length termination; invariably these teeth have experienced apical resorption or remodeling at some level during 18 months of orthodontic tooth movement. (Note that adjacent lateral incisor and pre-molar exhibited extensive resorption.)
Solution: The working length of the tooth was determined to be short of the discerned apical resorption (see Fig. 9-17, B). Note the scalloped apex that was enhanced using digital radi-ography. The root canal was cleaned, shaped, disinfected, and obturated using gutta-percha and sealer staying short of the anticipated resorbed apex. A 6-month reevaluation showed good bony response and cessation of the lateral resorption (see Fig. 9-17, C).

184 chapter 9 | Problem Solving in Working Length Determination
fIGURe 9-18 Improperly placed file stops can significantly alter accuracy of the working length.
constriction in these situations must rely on the clinician’s judgment, drawing on experience, tactile sensation, and reli-able diagnostic radiographic techniques. If the root end is wide open from the resorptive destruction, electronic apex locators are unreliable and of little clinical value. Conse-quently, the coronal-most point on the root above the resorbed apex that exhibits sound radiodensity must be iden-tified.28,52 This position is used as the new radiograph apex, and the working length is established 1 to 2 mm coronal to that point.28 In cases of extensive irregular apical resorption, the new working length can conceivably be 5 mm or more coronal from the original root apex.
A silicon stop is a common aid for evaluating the working length measurement and returning to a secure reference point (see Chapter 10). Care must be taken to assure that the stop is placed on the file and measured at a right angle to the file (Fig. 9-18). Otherwise, differences in length of a millimeter or more between files may occur, leading to either perforation and stripping of the apical foramen or inadequate cleaning and shaping of the apical seat, with corresponding loss of length. Commercially produced stops are teardrop shaped or notched and can be positioned to indicate instru-ment curvature as dictated by the canal; these are essential in maintaining working length once established. Most if not all intracanal instruments, both nickel-titanium (NiTi) and stainless steel, come with stops already positioned on their shafts.
Working Length Determination: Radiographic TechniqueRadiography is paramount to the successful practice of endodontics during diagnosis, treatment, and postoperative evaluation (see Chapters 2 and 3).6,29,36,42 Radiographic assessment of the tooth and periradicular structures prior to treatment will provide the clinician with essential informa-tion necessary to form a mental image of the apical complex.42
B CA
fIGURe 9-17 A, Maxillary canine undergoing orthodontic tooth movement. Note the lateral resorptive defect (arrow). B, Working length is determined. C, Six-month reexamination shows a stable environment. Radiographs are digital clear-view enhanced. (Case courtesy Dr. Paul Buxt, Dallas, TX.)
The generally accepted method for establishing the working length of a root canal is to expose a periradicular radiograph with an endodontic instrument (stainless steel K-file or NiTi file) placed in the canal.18,34 This method provides acceptable results in most instances (Fig. 9-19), especially when using enhanced digital radiographic tech-niques in the posterior teeth. However, other factors may complicate the decision-making process during this phase of root canal treatment, and this method has several drawbacks or limitations that can affect the ultimate accuracy of the working length used. The primary problem focuses on the

chapter 9 | Problem Solving in Working Length Determination 185
A
B C
fIGURe 9-19 A-C, Enhanced digital radiography using clear view provides a good assessment of treatment on this maxillary second molar.
quality of the radiograph produced, which is a composite of proper film placement, tubehead angulation, exposure time, and film processing (see Chapter 2). Attempts to read and interpret findings (e.g., position of a file tip in a root canal, angle of root curvature) from an exposed film that fails to meet accepted standards for diagnostic dental radio-graphs immediately alters the quality of the entire root canal treatment. It also destroys the concept of problem solving, which is based on the step-by-step assessment process, identifying variances from accepted standards and eliminat-ing them before the process is completed. Using erroneous data from a nondiagnostic, unreadable, or otherwise unintel-ligible dental radiograph will result in additional problems during treatment, such as instrumentation beyond the end of the root, canal ledging, loss of length, and associated complications (see Chapters 2 and 3).18 Often errors in film quality can be attributed to the inability of the clinician to properly manage factors such as a patient gag reflex, macro-glossia, shallow floor of the mouth, or shallow palate. These can only be managed by initially identifying that these problems may exist. Technical skill, authority, and assurance will more often than not overcome these potential impedi-ments to obtaining a quality dental radiograph, especially when the dental dam21 is in place. Failure to do so often
leads to unnecessary exposure of the patient to additional radiation.
Dental radiographs also have inherent limitations, perhaps the most important being that they provide only a two-dimensional image of a three-dimensional object. Coupled to the anatomic variability of the apical foramen and the apical constriction relative to the root end, radiographs fall far short of the ideal tool for determining the working length.17 Additionally, radiographs are subject to the super-imposition of normal anatomic features and pathologic changes on normal apical tooth anatomy.18 The presence of a radiolucency can aid in the interpretation of a radiographic image because of the change in density it produces. Likewise, the presence of a radiopacity such as the zygomatic arch (Fig. 9-20) can obscure the maxillary first and second molar apices. This occurrence has been shown to affect 20% of the first molar apices and 42% of the second molar apices.18
Regardless of these problems, the radiograph is an indis-pensable part of root canal treatment, and a variety of ways have been identified to determine the working length. In the method described by Ingle,34 an estimated working length is initially established by measuring from an accurate preopera-tive radiograph. A file, preferably ISO size 15 or greater, is then placed to the estimated working length, and a second

186 chapter 9 | Problem Solving in Working Length Determination
A B
fIGURe 9-20 A, Anatomic landmarks that block the view of the root apex in determining working length. B, Enhanced digital and inverted view provides some additional detail but will not suffice for a properly placed and exposed radiograph.
radiograph is exposed. If the tip of the file is within 1 mm of the ideal location, the radiograph can be accepted as an accurate representation of the tooth length. Other investiga-tors have recommended reconfirming working lengths with a new radiograph if adjustments of 2 mm or more have to be made.13 This method usually provides acceptable results, especially when the pulp is inflamed yet vital.
Controversies still exist, however, when the pulp is con-sidered nonvital, especially in the presence of an obvious periapical radiolucency and/or when the patient is experi-encing pain (Fig. 9-21).57 The success of the approach to working length determination is predicated on two things: (1) the accuracy of the radiograph exposed with the file in place in the canal and (2) ensuring that the file does not move from its original position before it can be removed safely from the canal after examining the working length film.28 It is incumbent upon the clinician to examine the working length film not only for the position of the file in the tooth but also for proper angulation, eliminating films that are foreshortened or elongated as being nondiagnostic. For rapid access to clear and diagnostic films, digital radiog-raphy that can provide enhanced imaging is preferred (see Chapter 3).58
Once a quality working length radiograph is obtained, the major challenge facing the clinician is interpreting the find-ings. Numerous studies have identified problems in radio-graph interpretation, both in inter- and intra-examiner reliability.22 Films exposed using a right-angle paralleling technique may result in magnification of the findings; some believe that using a paralleling device coupled with a grid for the pretreatment radiograph provides a consistent method for measurement control. Using the bisecting-angle technique, the radiographic distance of files placed in teeth from the apical vertex was 0.7 mm shorter than the actual anatomic file position.55
Radiographic working length determination for single rooted teeth is usually a simple task of exposing a film that is parallel to the front surface of the x-ray tubehead (Fig.
9-22). Few if any anatomic structures are superimposed on the root in this situation, and length determination is straightforward. With multirooted teeth, the superimposi-tion of files on one another and the presence of anatomic structures may often impede easy assessment of the working length.
An often misunderstood method of radiographically assessing the working length is the buccal object rule or SLOB (same lingual, opposite buccal) rule, in which buccal or lingual anatomic structures can be placed predictably on the x-ray film (see Chapter 3).18 By using this rule, individual files in the buccal and lingual roots of many anterior teeth with two canals or roots and all posterior teeth can be visualized and distinguished from each other (Fig. 9-23). Mesial buccal and distal buccal roots of maxil-lary premolars and molars can be shifted to expose the palatal root, and the zygomatic arch can be displaced from molar root apices for clear viewing of working length files (Fig. 9-24).
Clinical experience suggests that the major reason for not using the buccal object rule is the inability of the clinician to rapidly and easily interpret the findings. Simply stated, when the x-ray tubehead is moved in any direction, the file or structure to the lingual will move with the tubehead. Like-wise, if the tubehead is moved to a mesially or distally angu-lated position, the buccal object will move in the opposite direction, or to the distal or mesial, respectively. A slight shift of 20 to 30 degrees will in most cases allow an unobstructed view of the desired target. This rule works equally well in the horizontal or vertical plane. For example, with working length files in the mesial buccal and mesial lingual canals of a mandibular molar, and a horizontal shift of the x-ray tube-head 20 to 30 degrees to the mesial, the lingual canal (file) will move to the mesial—the same direction as the tubehead (Fig. 9-25). The buccal canal (file) will move opposite the tubehead or to the distal. Likewise, because the zygomatic arch is located buccal to the root apices of the maxillary molars, a decrease in the tubehead vertical angulation to a

chapter 9 | Problem Solving in Working Length Determination 187
A B
C
fIGURe 9-21 A, Mandibular canine that has a periapical radiolucency is presumed to be nonvital. Many clinicians would subscribe to the penetration of the apical foramen and filling to the root length in these cases, claiming that healing will not occur without this approach. B, Working length is established short of the root length but at the natural constriction, and the canal is filled. C, Twelve-month reexamination shows evidence of healing, and the patient is symptom free. (Case courtesy Dr. Erick Menegazzo, Dallas, TX.)
fIGURe 9-22 Simple radiographic exposures in maxillary anterior teeth at proper angles that assist in a more accurate working length determination.
more parallel position will move the arch apical to (above) the root apices. To move the mesial buccal root away from the palatal root, a distal horizontal angle of the tubehead would be used.
Using a parallel technique and constant reproducible angles, a slight 20- to 30-degree horizontal or vertical tube-head shift can predictably shift roots and structures to aid in accurate working length determination. Although it takes time and experience to develop this reliable technique, once mastered it greatly simplifies working length determination by minimizing problems encountered in the interpretation of undiagnostic radiographs. Hence the quality of root canal treatment can be enhanced.
Working Length Determination: Electronic Apex LocatorElectronic apex locators (EALs) have been available for almost 40 years for measuring the length of the root canal.56 These instruments work on the principle that the resistance between

188 chapter 9 | Problem Solving in Working Length Determination
A B
fIGURe 9-24 Applying the buccal object rule or SLOB (same lingual, opposite buccal) rule using enhanced clear-view digital radiography to determine the working length for a maxillary premolar with two aligned roots. A, Preoperative, using digitally enhanced clear view. B, Radiograph taken with a slight distal inclination of the radiographic beam using clear view.
fIGURe 9-25 Mandibular molar working length radiograph taken with the cone angled from the mesial, with the beam going distally.
A B
fIGURe 9-23 Applying the buccal object rule or SLOB (same lingual, opposite buccal) rule using digital radiography to determine the working length for a maxillary premolar with two divergent roots. A, Preoperative film. B, Cone position from the mesial with the beam directed distally. The buccal root is the most distally placed root.
the periodontal membrane and the oral mucosa is a constant 6.5 kilo-ohms. More recently, the resistance-type apex loca-tors have been superseded by impedance and frequency-type instruments which have been reported to be accurate to within 0.5 mm greater than 90% of the time.51 Apex locators can be used as an adjunct in determining working lengths where problems with anatomic variations obscure visualiza-tion of the periradicular area.40 In addition, they may be used to determine perforations or in patients where radiation expo-sure needs to be reduced.23
One issue of concern with EALs was their ability to work in the canal in the presence of various fluids such as blood and irrigants. Initially this was a problem, but most EALs have resolved this issue.19 Another issue was the size of the root canal, in particular the size of the apical constriction and the use of various file sizes. For best results, the use of a file that closely approximates the width of the constriction is recommended.32,33 What must be recognized, however, is

chapter 9 | Problem Solving in Working Length Determination 189
A
B C
fIGURe 9-26 Digital radiographic series of a mandibular molar using the clear-view option. Pulp is vital and inflamed. A, Preoperative. B, Working length with files positioned at the natural constriction protecting the vital tissue at the root apex. Patency filing is NOT used in these cases; there is no scientific evidence to support its use. C, Obturation to the natural constriction.
that apex locators are no substitute for high-quality radio-graphs that yield invaluable information regarding root mor-phology and curvature, calcification, number of canals and roots, and anatomic anomalies.
A comparison between radiographs and the apex locator found the apex locator to be significantly more reliable than the radiograph for determining working length.40,50 These findings suggest serious consideration be given to the use of apex locators as the primary means of determining the working length during endodontic procedures.
Working Length Determination: Other Clinical TechniquesTwo other techniques have been advocated for determining the working length of the root canal: (1) the use of paper points45,46 and (2) tactile sensation as a small instrument is placed slowly in the canal. Paper points may be helpful in determination of the canal exit if the canal can be dried of any periapical fluid. Inflamed tissues will moisten the tip of
the paper point at the level of the canal exit (Fig. 9-26). If, however, there is significant bleeding or the paper point is not made of tightly compacted paper, it may absorb a lot of blood and not provide a reasonable accurate indication of the position of the constriction. This technique is empiri-cally based and has no scientific evidence to support its routine use.
The use of tactile sensation also has the potential for sig-nificant variables, especially in light of the wide variety of apical constrictions that may occur.17 The first file to bind in its apical movement may not define the constriction accu-rately.59 To overcome this problem, initial flaring or preflar-ing of the canal is recommended to eliminate any false coronal interferences to instrument passage apically and enhance tactile sensation apically.17,39
There is no one technique that will work in all situations. Often, using more than one of the available techniques in a particular case will be necessary to achieve a reasonable esti-mate of the working length. Even then, anatomic factors that may influence the determination of working length may not always be evident or identified.

190 chapter 9 | Problem Solving in Working Length Determination
regrowth and multiplication.57 This is an empirical and contemporary approach to working length determination (including cleaning and shaping; see Chapters 10 and 11) that is promulgated by many in today’s practice of endodon-tics. However, because the root apex can be highly irregular, especially in the presence of obvious or even unidentified apical resorption,8 files placed to the apical extent of the root as viewed radiographically will likely be outside the confines of the canal and create potential damage to the root anatomy at that point.43 It is also possible that this technique may serve to inoculate the apical tissues with bacteria and material debris.37,60 Here also, a middle-of-the-road philosophy has been proposed: clean and shape the canal to the entire length of the root, then (1) back up or retreat into the canal suffi-ciently to develop a constriction or (2) stop inside the root for further intracanal procedures.52 However, even with this choice, the movement of materials past the root apex into the periapical tissues usually cannot be prevented.
Controversies and Challenges With the Pulpal and Periapical Status and Their Impact on Working Length Determinations and Choices
The wide range of anatomic variables and technical interpre-tations regarding the apical location for determining the working length have been identified. Because the location of this variable terminal position for working length, cleaning, shaping, and obturating the root canal has resulted in signifi-cant clinical opinions, applications, and advocacies, at least two camps of polarized thought and a vast array of multiple outliers have evolved. Advocates have been driven by passion, concern for radiographic appearance, and incorporation of cognitive dissonance into their decision making and proffer-ing.48 One major philosophy is to retain all procedures within the confines of the root. As determined by the position of the apical constriction, while the other philosophy espouses con-fining the determination of working length, cleaning, shaping, and obturation to the anatomic root apex or root length. In most teeth, overlap or agreement may occur in some cases, but these two philosophies are incompatible. In light of the controversy, there seems to be a middle-of-the-road position that most clinicians can travel comfortably and that will yield success. While the choices can vary, it would seem to be dependent on the status of the dental pulp, access to the end of the root, and the clinician’s skill, expertise, and experience that demonstrates that particular choices provide positive outcomes in the majority of cases. However, there does not appear to be any evidence-based data at the highest level to verify this approach, and therefore it is empirically driven.
If the dental pulp is vital (inflamed; irreversible pulpitis, see Chapter 1), the working length is established clinically as close to the constriction as possible, and all procedures are retained within the root canal.49 This position has been advo-cated as approximately 1 mm from the radiographic apex, but this dictate is flawed.43 The thought behind it is that the tissue that invaginates into the canal from the periodontal ligament (periodontal in nature) is not disturbed by the sub-sequent cleaning, shaping, and obturation accomplished within these confines (Fig. 9-27).27,29 This recommendation is based on sound wound-healing principles in that severance of the tissue at its narrowest point will create the smallest wound possible for healing.43,44 It also encourages the poten-tial for tissue regeneration, not just repair, with the formation of cementum as opposed to only fibrous connective tissue or persistent chronic inflammation.29
If the dental pulp is nonvital (obvious necrosis; presence of a periapical radiolucency), the working length is initially established as close as possible to the canal exit or slightly short of the apical foramen to clean the entire length of the canal,51 thereby eradicating bacteria as much as possible and removing the substrates that could encourage bacterial
CLINICAL PROBLEMProblem: A 52-year-old male presented with a large swelling over the maxillary right lateral incisor, with drainage evident from the sulcus. The tooth was painful to touch, and he was told he had a cyst that would require surgery or extraction. The tooth had been opened and left open by the referring dentist to “drain the cyst.” A radiograph showed a significantly large area of bone loss (Fig. 9-28, A). The patient was provided with a number of options, including an immediate root canal proce-dure followed directly by surgical procedure. After discussing treatment options, the patient chose to try to save the tooth with a nonsurgical root canal procedure and would consider surgery if this first choice did not work. The lesion failed to heal.
Solution: The tooth was isolated and irrigated extensively prior to placing any instrument in the canal. The working length was determined at 1 mm short of the radiographic apex (see Fig. 9-28, B). The canal was cleaned again with small files to the terminus of the root, then further cleaning and shaping occurred at the chosen working length. The patient failed to show for his appointments for the next 7 months. When he returned, the canal was again cleaned and shaped to the working length, followed by disinfection and obturation during which a small amount of sealer was exruded beyond the apical foramen. The 1-year reevaluation (see Fig. 9-28, C) shows significant healing, with the residual filling material being compacted against the root end by the inwardly advanced bone. Under these circumstances, the clinician would consider this outcome a success, especially if the patient functions symptom free. However, the residual mate-rial will unlikely encourage a regenerative response in the tissues and may serve as a focused area of chronic inflamma-tion for a long period of time (Fig. 9-29).37,60
Ironically, both of these philosophical and clinically prac-ticed positions have no evidenced-based data to support them as the ideal working length technique. Only when the teeth are obturated can one conjecture where the exact working length was terminated during root canal procedures. Data to

chapter 9 | Problem Solving in Working Length Determination 191
RCFRCF
CC
PDLPDL
RCF
CIRCIR
RCF
PDLC
A B
C
fIGURe 9-27 A, Histologic evidence for healing at the apical foramen when intracanal procedures are maintained inside the canal (RCF, root canal filling; PDL, periodontal ligament; C, new invaginated cementum into the root canal foramen and layered on the root surface [H&E stain ×10; canine model, 120 days]). B, Pushing obturation materials beyond the apical constriction, with resultant periapical chronic inflammatory response (CIR). Yellow arrow shows extent of root filling and an attempt at fibrous encapsulation. NO cementum is formed (H&E stain ×10; canine model, 120 days). C, Histologic evidence for healing at the apical foramen when procedures and materials are retained in the root canal (RCF, root canal filling; C, cementum; PDL, periodontal ligament). Arrow indicates the presence of a cemental barrier that has formed from the cells of the periodontal ligament. If the filling had gone beyond the constriction, the PDL cells would not have been able to differentiate and form a new cemental layer (B&B stain ×4; human specimen).
A B C
fIGURe 9-28 A, Maxillary lateral incisor with significant periapical bone loss. B, Working length determination; patency filing was NOT used. C, Twelve-month reexamination; healing stable but not complete. In these situations it is not uncommon to have healing with fibrous scar tissue. (Case courtesy Dr. John Kostohryz, Dallas, TX.)

192 chapter 9 | Problem Solving in Working Length Determination
A B
C D
fIGURe 9-30 A, Maxillary premolar with broken post, periapical lesion, and poor root canal filling with open apex possibly due to resorption. B, Post is removed and working length is established short of the end of the root. C, Root canal filled, staying short of the resorbed apex. D, 20 months. Patient is symptom free, tooth is functional, and the periapical lesion appears to be healed.
CLINICAL PROBLEMProblem: A 55-year-old male requested a second opinion regarding his maxillary right second premolar. He had been advised to have the tooth removed and replaced with an implant. The tooth had a broken post, the fractured tooth margins were below the soft tissue, the root canal did not appear to be ade-quately filled, the apex was open, and a large periapical lesion was present (Fig. 9-30, A). The patient was experiencing minimal symptoms but did want to retain the tooth if possible.
Solution: The challenges in this case were many, such as post removal and management of the tooth margins and open apex. A crown lengthening procedure was performed, and the post was removed (see Chapters 14 and 17). The working length was established short of the root apex, and all cleaning and shaping were confined to this length (see Fig. 9-30, B). A custom gutta-percha cone was used along with a sealer that contained some MTA (mineral trioxide powder only); the canal was filled to the working length with minimal to no extrusion of sealer (see Fig. 9-30, C). The tooth was restored with a post, core, and crown. Reevaluations at 3, 7, 12, and 20 months indi-cated a symptom-free patient with a functioning tooth and evidence of bony healing around the root end, possibly into the open apex (see Fig. 9-30, D). This case highlights the vari-ability of working length determination based on anatomic treatment factors and choices based on experience and skill.
RCF
CIR
fIGURe 9-29 Histologic evidence for an adverse tissue response with the expression of material beyond the confines of the root canal (RCF, root canal filling, CIR, chronic inflammatory response [H&E stain ×10; canine model, 120 days]).
support either position is elusive and unfounded, except for information gleaned from outcome studies that take into account all phases of root canal procedures. Many of these studies are retrospective, however, and have questionable bearing on contemporary practices. Lengthy and thorough assessments of outcomes relative to termination of the working length, cleaning, shaping, and obturation of the root

chapter 9 | Problem Solving in Working Length Determination 193
canal system suggest that “No scientific basis exists in the litera-ture to support the notion that the apical foramen should be pierced and root canals be overfilled for a successful outcome.” 20
Posttreatment Implications and Outcomes of Root Canal Treatment Based on Working Length Philosophies
Historically, great emphasis was placed on proper manage-ment of the root apex during root canal treatment.42 Philo-sophically, most authors and clinicians were in agreement that the tissues beyond the apical constriction must be pro-tected and not injured with excessive instrumentation or caustic drugs. Authors such as Grove,25,26 Blayney,2-5 Coolidge,11,12 Kronfeld,35 and Davis15 all agreed that termina-tion of root canal procedures should occur in a manner that would allow for proper healing, that is, deposition of cemen-tum at the root apex to secure a complete biological seal (see Figs. 9-9 and 9-28, C ). Hatton31 probably best summed up the philosophy of the time by saying:
Because the smaller accessory foramina react in all respects like the principal ones, the assumed risk of inserting pulp-canal filling into canals with tortuous accessory or terminal foramina may be considered discounted, and root-canal filling need not, therefore, be condemned because all acces-sory canals and the apical portion cannot be reached. . . . It is not wise to assume that a partial filing of pulp canals is a safe and justifiable routine procedure. The junction of the cementum and the dentin of the apex is the ideal ter-mination of such a filing. . . . Such regeneration as the preceding must be greatly hampered by unnecessary injury of the apical structures by instrumentation or the corrosive action of many drugs used in root canals. A rigidly aseptic, gentle and accurate root-canal technic should favor these restorations.
The ideal healing response in the periradicular tissues fol-lowing root canal treatment would result in deposition of cementum over the apical foramina (see Fig. 9-28, C ), with regeneration of the periodontal apparatus. However, repair, not regeneration, is the usual outcome. Most obturation materials available today possess no regenerative potential,14 having neither inductive nor conductive properties. Studies have demonstrated the negative effect of gutta-percha and calcium hydroxide on the extracellular matrix tissues and on alkaline phosphatase activity.14 Therefore, it would appear logical that extrusion of obturation material beyond the con-fines of the root canal system will further irritate the perira-dicular tissues and delay healing.37,49,60
Controversies will continue to surround the management of the root apex, even though contemporary root canal treat-ment has a high rate of clinical success. With patients demanding a greater degree of tooth retention using modern treatment modalities, there will be continued efforts to
identify an all-compassing technique and material to achieve the goals of successful treatment on a predictable basis. These expectations can only be achieved by establishing an evidenced-based and problem-solving approach to treatment that reflects a biological basis for the therapy rendered.
REfEREnCES1. Andreasen JO: Luxation of permanent teeth due to trauma: a clini-
cal and radiographic follow-up study of 184 injured teeth, Scand J Dent Res 78:273-286, 1970.
2. Blayney JR: The biological aspect of root canal therapy, Dent Items Int 49:681-708, 1927.
3. Blayney JR: Present conception of vital reactions which occur within apical tissues after pulp removal, J Am Dent Assoc 16:851-860, 1929.
4. Blayney JR: Tissue reactions in the apical region to know types of treatment, J Dent Res 9:221-249, 1929.
5. Blayney JR: Fundamentals governing pulp-canal therapy, Dent Cosmos 74:635-653, 1932.
6. Bramante CM, Berbert A: A critical evaluation of some methods of determining tooth length, Oral Surg Oral Med Oral Pathol 37:463-473, 1974.
7. Briseño Marroquin B, El-Sayed MAA, Willerhausen-Zönnchen B: Morphology of the physiological foramen. I. Maxillary and man-dibular molars, J Endod 30:321-328, 2004.
8. Brynolf I: A histological and roentgenological study of the periapi-cal region of human upper incisors, Odont Revy 18(Suppl 11):1-176, 1967.
9. Burch JG, Hulen S: The relationship of the apical foramen to the anatomic apex of the tooth root, Oral Surg Oral Med Oral Pathol 34:262-268, 1972.
10. Certosimo FJ, Molor MF, Walker T: Endodontic working length determination—where does it end? Gen Dent 47(3):281-286, quiz 287-288, 1999.
11. Coolidge ED: An aseptic root canal technique for the preparation and filling of roots, J Natl Dent Assoc 8:180-195, 1921.
12. Coolidge ED: An aseptic root canal technique for the preparation and filling of roots, J Am Dent Assoc 16:1456-1465, 1929.
13. Cox VS, Brown CE, Bricker SL: Radiographic interpretation of endodontic file length, Oral Surg Oral Med Oral Pathol 72:340-344, 1991.
14. Craig RG, Zuroff M, Rosenberg PA: The effect of endodontic materials on periodontal ligament cell proliferation, alkaline phos-phatase activity, and extracellular matrix protein synthesis in vitro, J Endod 23:494-498, 1997.
15. Davis WC: Anatomy of the apical third of the roots of teeth, Dent Items Int 45:649-722, 1923.
16. De Deus QD: Frequency, location and direction of the lateral, secondary and accessory canals, J Endod 11:361-366, 1975.
17. Dummer PM, Mc Ginn JH, Rees DG: The position and topogra-phy of the apical canal constriction and apical foramen, Int Endod J 17:192-198, 1984.
18. Dumsha TC, Hovland EJ: Problems in radiographic technique and interpretation. In Gutmann JL, Dumsha TC, Lovdahl PE, Hovland EJ, editors: Problem solving in endodontics, ed 3, St Louis, 1997, Mosby-Year Book Inc, 23-46.
19. Ebrahim AK, Yoshioka T, Kobayashi C, et al: The effects of file size, sodium hypochlorite and blood on the accuracy of the Root ZX apex locator in enlarged root canals: an in vitro study, Aust Dent J 51:153-157, 2006.
20. Gesi A, Bergenholtz G: Pulpectomy—studies on outcome, Endod Topics 5:57-70, 2003.

194 chapter 9 | Problem Solving in Working Length Determination
43. Ricucci D: Apical limit of root canal instrumentation and obturation, part 1. Literature review, Int Endod J 31:384-393, 1998.
44. Ricucci D, Langeland K: Apical limit of root canal instrumentation and obturation, part 2. A histological study, Int Endod J 31:394-409, 1998.
45. Rosenberg DB: The paper point technique. Part 1, Dent Today 22(2):80-86, 2003.
46. Rosenberg DB: The paper point technique. Part 2, Dent Today 22(3):62-64, 66-67, 2003.
47. Swartz DB, Skidmore AE, Griffin JA: Twenty years of endodontic success and failure, J Endod 9:198-202, 1983.
48. Seltzer S, Bender IB: Cognitive dissonance in endodontics, Oral Surg 20:505-516, 1965.
49. Seltzer S, Bender IB, Turkenkopf S: Factors affecting successful repair root canal therapy, J Am Dent Assoc 67:651-662, 1963.
50. Shanmugaraj M, Nivedha R, Mathan R, et al: Evaluation of working length determination methods: an in vivo/ex vivo study, Indian J Dent Res 18(2):60-62, 2007.
51. Shabahang S, Goon WWY, Gluskin AH: An in vivo evaluation of Root ZX electronic apex locator, J Endod 22:616-618, 1996.
52. Simon JHS: The apex: how critical is it? Gen Dent 42:330-334, 1994.
53. Smith CS, Setchell DJ, Harty FJ: Factors influencing the success of conventional root canal therapy; a five-year retrospective study, Int Endod J 26:321-333, 1993.
54. Stabholz A, Rotstein I, Torabinejad M: Effects of preflaring on tactile sense of the apical constriction, J Endod 2:92-94, 1995.
55. Stein J, Corcoran JF: Nonionizing methods of locating the apical constriction (minor foramen) in root canals, Oral Surg Oral Med Oral Pathol 71:96-99, 1991.
56. Sunada I: New method of measuring the length of the root canal, J Dent Res 41:375-387, 1962.
57. Wesselink P, Bergenholtz G: Treatment of the necrotic pulp. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
58. Woolhiser GA, Brand JW, Hoen MM, et al: Accuracy of film-based, digital, and enhanced digital images for endodontic length determination, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:499-504, 2005.
59. Wu M-K, Barkis D, Roris A, et al: Does the first file to bind cor-respond to the diameter of the canal in the apical region? Int Endod J 35:264-267, 2002.
60. Yusuf H: The significance of the presence of foreign material peri-apically as a cause of failure of root treatment, Oral Surg 54:566-574, 1982.
RECOmmEnDED ADDiTiOnAL READingHülsmann M, Schäfer E: Apical patency: fact and fiction—a myth or
a must? A contribution to the discussion, ENDO (Lond Engl) 3:285-307, 2009.
21. Glossary of endodontic terms, ed 7, Chicago, 2003, American Association of Endodontists.
22. Goldman M, Pearson AH, Darzenta N: Reliability of radiographic interpretations, Oral Surg Oral Med Oral Pathol 38:287-293, 1974.
23. Gordon MP, Chandler NP: Electronic apex locators, Int Endod J 37:425-437, 2004.
24. Grossman LI: Root canal therapy. Philadelphia, 1946, Lea & Febiger.
25. Grove CJ: Nature’s method of making perfect root fillings follow-ing pulp removal with a brief consideration of development of secondary cementum, Dent Cosmos 63:968-982, 1921.
26. Grove CJ: The value of the dentinocemental junction in pulp canal surgery, J Dent Res 11:466-468, 1931.
27. Gutmann JL: Biologic perspectives to support clinical choices in root canal treatment, Aust Endod J 31(1):9-13, 2005.
28. Gutmann JL, Leonard JE: Problem solving in working-length determination, Comp Contin Educ Dent 16:288, 290, 293-294 passim; quiz 304, 1995.
29. Gutmann JL, Regan JD: Historical and contemporary perspectives on the root apex, Arab Dent J 3(6):9-15, 1998.
30. Hasselgren G: Where shall the root filling end? N Y State Dent J 60:34-35, 1994.
31. Hatton EH: The possibility of apical regeneration after root canal filling from the histopathological point of view, J Am Dent Assoc 9:192-198, 1922.
32. Herrera M, Abalos C, Planas AJ, et al: Influence of apical constric-tion diameter on Root ZX apex locator precision, J Endod 33:995-998, 2007.
33. Hoer D, Attin T: The accuracy of electronic working length deter-mination, Int Endod J 37:125-131, 2004.
34. Ingle JI: Endodontics. Philadelphia, 1965, Lea & Febiger.35. Kronfeld R: Histopathology of the teeth and their surrounding
structures, Philadelphia, 1933, Lea & Febiger.36. Kuttler Y: Microscopic investigation of root apexes, J Am Dent
Assoc 50: 544-552, 1955.37. Love RM, Firth N: Histopathological profile of surgically removed
persistent periapical radiolucent lesions of endodontic origin, Int Endod J 42:198-202, 2009.
38. Parris J, Wilcox L, Walton R: Effectiveness of apical clearing: histological and radiographical evaluation, J Endod 20:219-224, 1994.
39. Pecora JD, Capelli A, Guerisoli DM, et al: influence of cervical preflaring on apical file size determination, Int Endod J 38:430-435, 2005.
40. Pratten DH, McDonald NJ: Comparison of radiographic and electronic working lengths, J Endod 22:173-176, 1996.
41. Ng Y-L, Mann V, Rahbaran S, et al: Outcome of primary root canal treatment: systemic review of the literature—part 2. Influ-ence of clinical factors, Int Endod J 41:6-31, 2008.
42. Provan WF: Roots and their treatment, Dent Summary 36:675-680, 1916.

195
Chapter 10
Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
Problem-Solving ListProblem-solving issues and challenges in enlarging and shaping the root canal system addressed in this chapter are:
Prevention of Procedural Errors in Canal Enlarging and Shaping Using Traditional Techniques and Stainless Steel or Nickel-Titanium Instruments
Loss of working length
Deviations from the canal anatomy
Inadequate or inappropriate enlarging and shaping that hinder the provision of quality treatment
Enlarging and shaping beyond the canal terminus
Excessive removal of root dentin
Failure to properly enlarge and shape the canal
Prevention and Management of Procedural Errors in Canal Enlarging Using Contemporary Techniques and Rotary Nickel-Titanium Instruments
Importance of the crown-down technique
In attempting to assign the success or failure of operations upon diseased teeth to their proper causes, factors of the greatest importance are frequently left out of account, and the results ascribed to some agent which may have been entirely indifferent. One of these factors, which forms the very foundation of successful root-treatment, is the manner in which the mechanical cleansing of the canal is carried out.24
R.H. HofHEINz, 1892
Problem-solving principles in enlarging and shaping the root canal system are predicated on the guidelines presented in Chapters 8 and 9: access to the canal and establishing a proper working length. Application of these concepts will minimize or prevent problems that may be encountered in enlarging and shaping the root canal system. Even though the principles of canal enlarging imply that cleaning is being done, true cleaning occurs through the use of irrigants, important enough to be addressed in a separate chapter (see Chapter 11). But while addressing the principles of enlarg-ing and shaping, be cognizant that they go hand in hand with using irrigants and methods of debris and irritant removal that cannot be achieved with instruments alone. This concept has been firmly established in the endodontic literature.10,14,41,43,44
Application of traditional techniques in canal enlarging and shaping using stainless steel root canal instruments has received volumes of attention historically.35,50 Likewise, there are abundant articles and textbooks detailing these traditional approaches to enlarging and shaping.37,45 The global popula-tion of dental clinicians has either adopted or is moving
forward with contemporary techniques using newer instru-ments and philosophies of canal treatment,26,37 so minimal time will be spent on problem solving the traditional approaches to treatment. However, the reader should not feel that these principles are being neglected. These concepts and their solutions have served the clinician well for decades and are just as important today for anyone who picks up a stain-less steel file and inserts it into the root canal at any time during treatment. Even with the advent of rotary nickel-titanium (NiTi) instruments and their global adoption for routine root canal procedures, in almost all cases, the use of stainless steel instruments is still indicated at some time during the procedures (e.g., pathfinding, initial penetration, severely curved canals, etc).

196 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
with some subtle exceptions, is almost exclusive to the use of hand stainless steel instruments in the root canal. The main shortcomings that promote loss of working length are listed below, and logic would support preventing the problem by eliminating these shortcomings.
• Failure to irrigate frequently and copiously with a tissue-dissolving irrigant (sodium hypochlorite [NaOCl])
• Failure to recapitulate (Fig. 10-3) (periodically passing a small file to the desired working length to ensure debris is not being packed); in some circles, referred to as apical clearing, defined as removal of debris from the apical portion of the preparation but not going past the canal constriction52,54
• Failure to radiographically verify the working length during the enlarging process if necessary
• Malpositioned instrument stops (Fig. 10-4, A)• Failure to record and regularly use stable reference
points (see Fig. 10-4, B)• Skipping instrument sizes, especially in curved canals• Fracturing an instrument without realizing it has
occurred• Aggressive use of instruments in small, tight, and
curved canals
Each one of these errors is easily avoided with (1) attention to detail during instrument application and (2) generous use of irrigants during enlarging and shaping.
If nickel-titanium (NiTi) rotary instruments are used properly during canal enlarging and shaping, the same short-comings may enter into the process, but loss of working length occurs infrequently. The major cause of loss of working length with NiTi rotary files appears to be excessive use of these instruments, retaining them in the canal for longer than 1 to 3 seconds while they are achieving their goals apically.
Prevention of Procedural Errors in Canal Enlarging and Shaping Using Traditional Techniques and Stainless Steel or Nickel-Titanium Instruments
The safe and efficacious practice of endodontics, specifically root canal procedures, is based on both biological and clinical parameters, with prevention being the operative word. This discussion precludes a focus on management of problems. Most if not all can be prevented with a knowledgeable and thoughtful approach to providing care at all times. In the discussion of endodontic outcomes, only too often when cases fail, they are labeled as “endodontic failures,” or the “persistence of what is generically termed endodontic disease.”17,18 In actuality, clinician failure is responsible for the vast majority of cases in which there is persistent pathosis, newly developed inflammatory processes, or patient symp-toms. Clinician failure constitutes not practicing in a preven-tive manner, not applying sound principles of diagnosis, and not adhering to appropriate treatment planning and treat-ment. A procedural error in itself may not be the cause of the failure but rather serve as an impediment to positive out-comes.33 Sadly, this scenario may not be identified by the clinician, and in fact the clinician only too often informs the patient the treatment did not work and recommends extrac-tion in favor of a fixed prosthesis (primarily implant). This message is for all who choose to do endodontic procedures: heed the signals, assess what has caused the problems, and change clinical practice procedures to prevent these unfortu-nate occurrences. Moreover, recommend these cases of clini-cian failure be sent to a specialist for revision considerations (see Chapter 14).
Loss of Working LengthLoss of working length during cleaning and shaping is a common and frustrating procedural error. The problem is often only noted on the master-cone radiograph or when the master apical file (MAF) is short of the intended or initial working length. Even worse, it is often not noted until the canals are filled and a crown is placed. Too many times it is never noted (Fig. 10-1). Assuming that a clean, dry canal with proper shape has been developed, reestablishing canal length becomes time consuming, tedious, and often hopeless. Loss of working length may be secondary to other procedural errors (e.g., canal blockages, ledges, perforations, fractured instruments) which occur during the canal enlarging and shaping process and can be identified early in the procedures (Fig. 10-2).21,27,29 In most instances, however, the loss of working length is due to the packing of dentin chips in the apical third of the canal. The occurrence of this problem,
fIGURE 10-1 A 39-year-old presented with pain to biting on the mandibular first molar. He related that he could not understand why he was having pain; root canal treatment and a crown had been completed only 2 weeks prior to this painful episode. Note the incomplete root canal treatment with possible ledges in the mesial canals.

chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal 197
particles and canal wall; see Fig. 10-5, C ).31 Once the catch is felt, the file is carefully rotated in a stem-winding fashion along with a slight in-and-out motion until the tip of the instrument bypasses the obstruction and negotiates the canal to length. Placing a relatively straight instrument into a milieu of metallic filings or dentin debris may push the
It is not the packing of chips that occurs, but rather there is a tendency of these instruments to move laterally in the canal, especially in larger sizes and when placed apically over and over during the enlarging and shaping process.
Should loss of working length occur that is due to packed dentinal and tissue debris (Fig. 10-5, A) the clinician should choose a small but stiff instrument (e.g., No. 15 K-file) to bore through the obstruction. If the obstruction is caused by particles of temporary or permanent restorative materials, an instrument smaller than the last instrument placed into the canal system is used (e.g., No. 8, 10, or 15 K-file or C+ file [Dentsply Maillefer, Ballaigues, Switzerland]). A 45-degree curve is placed at the apical 3 to 4 mm of the instrument (see Fig. 10-5, B), and the file is inserted into the canal and slowly rotated circumferentially to detect a catch (the space between
fIGURE 10-3 Packed amalgam particles in the apical extent of the canal block the apical 3 mm of the root canal.
B CA
fIGURE 10-2 A, Preoperative radiograph showing significant curvature of the mesial canals, which should warn the clinician that ledging is more likely to occur if instrumentation is not performed cautiously. B, Master apical file radiograph shows that canals were instrumented larger than appropriate for size and curvature of mesial roots. Notice the loss of canal length and ledge formation. C, Mesial canals are fully ledged, and distal canal is partially ledged.
A B
fIGURE 10-4 A, Improperly placed stop on a file can significantly change the accuracy of the working length and maintenance of canal length during enlarging and shaping. B, Cross-section of extracted tooth with files and stops in place. Stops are positioned at a proper angle with respect to the shaft of the file and the reference point on the tooth surface.

198 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
B
C D
A
fIGURE 10-5 A, Diagram showing dentinal chips and tissue debris packed in the apical portion of the canal. B, A stiff file is curved in the apical 1 to 3 mm at a 30- to 45-degree bend and placed to the level of the blockage. C, The file is rotated slowly until it catches in the debris then advanced slowly in millimeter strokes to remove the blocking debris. D, Once the catch is felt, the file is carefully rotated in a stem-winding fashion along with a slight in-and-out motion until the tip of the instrument bypasses the obstruction and negotiates the canal to length.
B CA
fIGURE 10-6 A, Note the block (most likely a ledge) in the mesial canals of a mandibular molar. B, After placement of a 45-degree bend, one of the canals was penetrated and negotiated to the working length. The other canal could not be penetrated, or possibly it joined the patent canal. C, Obturation with a softened gutta-percha and sealer technique.
particles more apically into the canal or periapical tissues, making them irretrievable. All recovery procedures should be performed with a lubricant in the canal.
Once the instrument begins to advance further into the canal, or if it expediently reaches the estimated working length, a radiograph is obtained to verify the position of the file. The instrument should not be removed until it can be used in small-amplitude strokes, moving circumferentially to dislodge the packed debris. When sufficient space has been developed
through or along the side of the blockage, a smaller-sized Hedström file can be placed to length. Moving this instrument on the outstroke will eliminate the debris. To bore through dense blockage with dentinal chips, chelating agents such as RC-Prep, REDTAC, or liquid ethylenediamine tetraacetic acid (EDTA; see Chapter 11) may be used to soften the plug to facilitate penetration. If the plug has not been penetrated, the file may be creating a false canal in the dentinal wall.
Whenever there is failure to penetrate or bypass blockage, complete enlarging and shaping at a new working length coronal to the blockage (Fig. 10-6) are recommended.33 Variations in obturation techniques such as diffusion, ther-moplasticized gutta-percha, warm vertical compaction, or core-carrier procedures can be used to enhance penetration of the gutta-percha and sealer around or through the block-age (see Chapter 12). Periodic reassessment is necessary, and if further treatment is deemed appropriate, surgical interven-tion to correct the problem may be warranted (Fig. 10-7).9 If surgery is not feasible, intentional replantation15,57 or extraction and replacement with an artificial prosthesis such as an implant may be indicated if symptoms persist.
Many authors and clinicians would also list separation or breakage of intracanal instruments, especially in curved canals, as a major cause of canal blockage or loss of working length (Fig. 10-8).28 This problem has been addressed in Chapters 5 and 14. However, during the application of NiTi rotary instruments, there are unique circumstances that tend to predispose to instrument separation and canal blockage (Fig. 10-9). In many respects, the concern for instrument breakage has prevented many clinicians from adopting the use of rotary NiTi instruments. This is unfortunate because the minimal potential for instrument separation does not have to be a deterrent to usage if some basic principles are followed. First, these instruments are always to be used in a crown-down technique after a tapered pathway for the instru-ments has been developed. The pathway will ensure ease of

chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal 199
*References 5, 22, 26, 34, 42, and 55.
A B
fIGURE 10-7 A, Maxillary molar with a separated instrument segment around the curve in the mesial buccal canal. The tooth was symptomatic. B, Following apical surgery and a root-end filling in the mesial buccal canal; 3-month reevaluation.
movement with minimal pressure, binding, and torque on the instrument during canal penetration. The pathway can be created with stainless steel hand K-files (No. 06 to 20) intended for this purpose4 or with NiTi rotary PathFiles (Dentsply Maillefer, Ballaigues, Switzerland). The pathway that is developed favors variably tapered NiTi instruments and small constant-tapered instruments (0.04 to 0.06, Nos. 15 and 20). When time is taken to develop the pathway, additional important information is identified by the clini-cian, such as canal curves, the joining of canals, rapid devia-tions, and multiple canals. In light of these findings, most causes for loss of working length can be prevented.
A final note on this issue concerns the cost of the newer NiTi instruments and their value in problem prevention and the quality of the final enlarging and shaping process. While stainless steel instruments can still be used for these proce-dures,28 the higher incidence of errors and problems that occur would seem to compel the clinician to switch to instru-ments that can prevent these problems, thereby minimizing
unacceptable treatment, need for revision, or the wholesale extraction of teeth. A word of caution to the clinician who continues to use the stainless steel file for canal enlarging and shaping, especially in curved canals: When using stainless steel instruments, placing a small, accentuated curve in the apical 1 to 3 mm is essential prior to placement in any canal during initial penetration and canal negotiation.
Deviations from the Canal AnatomyDeviations from the normal canal anatomy are usually in the form of ledges that can occur anywhere along the length of the canal (Fig. 10-10): zips, that usually occur at the apical extent of the canal (Fig. 10-11); false canals, which occur if a ledge is accentuated with aggressive instrument activity of the instrument tip against the wall until the instrument creates its own exit out of the root (some refer to as a root perforation) (Fig. 10-12); or strip perforations that occur with the lateral cutting of an instrument anywhere along the root wall (primarily in areas of root wall thinness or natural external root invaginations), resulting in a longitudinal lac-eration of the root structure (Figs. 10-13 and 10-14).*
As with the loss of working length, these errors occur primarily with the use of stainless steel hand instruments (K-files). However, in any given root canal anatomy, these problems may also occur when using NiTi rotary instruments with lack of attention during instrument application. In this regard, deviations with NiTi instruments are prevented by (1) developing a smooth, clean pathway in the canal before placement of specific NiTi instruments used for enlarging and shaping, and (2) using the instruments only to their desired length for only a few seconds. Repeated placement of these instruments to length or holding them at length during rotation will result in canal deviations and possible breakage, especially if excessive pressure is placed on the instrument by the clinician.
fIGURE 10-8 Broken instrument segment around the curve at the junction of the mesial buccal and distal canals—a common canal blockage.

200 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
E
F
G
A
B
C
D
fIGURE 10-9 Diagrammatic representations of the four most common reasons for breakage of any endodontic intracanal instrument: canal convergence (A), S-shaped canals with multiple curves (B), abrupt canal deviations (C), and severe and rapid apical curvatures (D). These anatomic complexities are especially important in the application of NiTi rotary instruments. E, Histologic evidence for the complexities in the case of the severe apical curvature. f, Radiograph showing the severe apical curve in the distal root of the second molar. G, Radiograph shows three of the four anatomic challenges. In the mesial root of the first molar, there is evidence of canal convergence (black arrow) and an S-shaped apical curve below the convergence (white arrow). The mesial root of the second molar has an abrupt deviation (white arrow) of the root and canal anatomy in the mesial root (highlighted in red).
Inadequate or Inappropriate Enlarging and Shaping That Hinder the Provision of Quality TreatmentEnlarging and Shaping Beyond the Canal TerminusThe excessive movement of instruments (overinstrumenta-tion) beyond the apical constriction violates the periodontal ligament and alveolar bone.7 Many problems may arise from
this error. Loss of the apical constriction creates an open apex with an increased likelihood of pushing debris past the con-fines of the root canal,32,51 overfiling, lack of an adequate apical seal, and pain and discomfort for the patient.23,39 Excessive instrumentation beyond the constriction may be recognized when hemorrhage is evident in the apical portion of the canal, with or without patient discomfort. Another way some clinicians recognize this problem is the presence of what is referred to as a weeping canal, which results from tissue fluids backing up into the canal due to damage to the

chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal 201
fIGURE 10-10 Diagrammatic representation of a ledge (see Fig. 10-2, B for a radiographic image).
ElbowZip
A B C
fIGURE 10-11 A, Diagrammatic representation of a zip. B, Cleared tooth specimen showing a zip (red arrow) with narrowing (elbow black arrow). C, Radiograph with canal zip in the apical portion of the distal canal of the first molar.
periapical tissues. With an apical foramen that has been opened arbitrarily, the fluid can back up into the canal and make obturation and sealing of the canal challenging. Fur-thermore, if the tissues have been inoculated with bacteria from the root canal, persistent weeping may be due to local-ized tissue destruction from bacterial invasion.30,47 If the apical environment is bacteria free, the trauma of overinstru-mentation should not affect the ultimate healing potential of the tissues.30,47 Thus performing all instrumentation within the confines of the root system is imperative, especially in cases of a necrotic pulp.
Prevention is key to this problem. First, good radiographic techniques should be used to accurately determine the apical constriction of the root canal, and sound reference points should always be used (see Chapters 2 and 3). Using stable instrument stops placed perpendicularly to the shaft of the instrument is essential and will allow predictable retention of all instruments within the confines of the canal system. Occlusal reduction or refinement are always done before working length determination, enlarging, and shaping. Sub-sequent to working length determination and some initial
enlargement, the working length can be verified when neces-sary. Attention to detail during all enlarging and shaping procedures is the modus operandi.
If the apical constriction has been lost after excessive instrumentation, there are a number of ways to manage this dilemma. First, a new apical stop can be established within the confines of the root canal. This position will be approxi-mately 1 to 2 mm from the radiographic apex; the stop is equivalent to two to three sizes larger than the first file used to bind at that position. Second, a plug of dentin chips or pharmaceutical-grade calcium hydroxide (Ca[OH]2) can be placed apically to control the movement of gutta-percha and sealer during compaction procedures (Fig. 10-15). A Hed-ström file can be used short of the working length in a dry canal to obtain the dentin chips during canal enlarging and shaping and in the middle and coronal thirds of the canal. The chips are packed apically to the working length with a paper point or small plugger. If the dentin chips are contami-nated, a plug of mineral trioxide aggregate (MTA), such as ProRoot MTA (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), can be placed apically. A measured plugger that fits in the canal to the desired length is used to carry the material apically to the desired depth, followed by gentle apical compaction.
Some clinicians and authors recommend the use of patency filing. This is described as the passage of small instruments (No. 08 to possibly even a No. 20 K-file) beyond the canal terminus.16,48 The rationale for this pro-cedure varies and is empirical; there are no substantial studies that support the concept and technique.19 In fact, the repeated movement beyond the canal terminus with larger instruments and in the presence of canal curves may or may not alter the canal anatomy sufficiently to make

202 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
perforation of the apical constriction. A rotary NiTi file may not cause the problems associated with variably tapered instruments but may create problems associated with constant-tapered instruments, especially if left to rotate in the canal longer than 1 to 2 seconds.
There are studies that claim that unless the apical portion of the canal is taken to larger sizes, it will not be clean with regard to surface cleaning and bacterial removal or reduc-tion.11,36,40,45,49 Larger, however, is not always better for many root canal systems as far as the final apical diameter—unless this can be done using instruments with larger tapers but not necessarily larger diameters.3,11-14 For example, an apical size 50 prepared with a K-File will develop a 2% taper, but a variably tapered instrument that is only a size 30 apically may have as much as a 9% taper. In the former case, more tooth structure may have to be removed that may not align with the external root anatomy. In the case of the latter, the shape follows the external anatomy, and the size still allows for good cleaning with irrigants and disinfectants; the pro-gressive size apically is 30 at the tip, 39 one millimeter coro-nally, 48 two millimeters coronally, and 57 three millimeters coronally. With the size 50 K file, it will only be a size 56 three millimeters coronally from the apical working length. Another solution would be to retain the smaller sizes in the apical portion of the canal using rotary instruments, and then to further clean the apical 1 to 3 mm with hand instru-ments that can be curved subtly if necessary to contact the canal walls.2
Overpreparation is a special concern in the apical portion of the canal system, but it can easily occur in the middle and coronal portions of the canal as well. Excessive canal flaring or shaping increases the chances of stripping and perfora-tion.1 When flaring the canal, a step-back or step-down pro-cedure is recommended to create a continuously tapering funnel preparation for obturation with gutta-percha. If neces-sary, careful and conservative use of rotary instruments (e.g., variably tapered NiTi files) can be considered to assist in refining canal shape. Excessive removal of tooth structure is not necessary; overprepared (overflared) canals are potentially weaker and subject to fracture during compaction and restor-ative procedures.
complete cleaning and obturation difficult.20 Each case is dependent on the three-dimensional apical anatomy and clinician application of the instruments.8,48,53 Furthermore, instrumentation into the apical periodontal tissues may impair or delay positive outcomes, depending ultimately on the nature and impact of the root filling material.25
Excessive Removal of Root DentinExcessive removal of tooth structure (overpreparation) in a mesial distal and buccal lingual direction can result in root weakening, laceration of the root wall, or perforation. During canal enlarging and shaping, the size of the apical preparation should correspond to the respective size, shape, and curvature of the root. For example, attempts to produce an apical seat equivalent to a No. 40 K-file in a moderately curved (10 to 20 degrees) mesial buccal canal of a mandibular first molar are likely to cause not only zipping of the root apex but also
A B
fIGURE 10-12 A, Diagrammatic representation of a false canal. B, Radiograph showing two false canals in the mesial root of the first molar.
BA
fIGURE 10-13 A, Extracted root with strip perforation (arrow). B, Paper point can be used to identify the position of a strip perforation—blood on the lateral wall.

A B
C D
E F
fIGURE 10-14 A, Mandibular molar with signs or symptoms requiring treatment. Note the root invagination on the distal surface of the mesial root. B, Two years later, the tooth exhibited significant bone loss apically and in the furcation. C, Working length determination. D, Obturation with strip perforation. E, Nonsurgical removal of the protruding gutta-percha cone and placement of mineral trioxide aggregate. f, Nine-month reevaluation shows good healing.
AB
1.5-2 mm
fIGURE 10-15 A, Diagrammatic representation of a root canal in which the apical constriction has been violated and the canal has been overinstrumented to a large size. B, Preparation of a new apical constriction 1.5 to 2 mm inside the root.

204 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
subsequent apical perforation (lack of apical stop and constriction).
Underprepared canals are best managed by adhering to sound principles of proper length determination, canal enlarging and shaping, and recapitulation when necessary. Copious irrigation, with proper irrigation needle penetration (see Chapter 11) and attention to detail during instrumenta-tion will ensure a properly cleaned canal. Before obturation, spreaders and pluggers must be fitted to determine their depth of placement and ensure proper canal shape.6 A critical assessment of the preparation can often be made only by evaluating the final obturation, but this will not provide a true three-dimensional appraisal of the overall accomplish-ment, especially the cleanliness of the root canal system.
Prevention and Management of Procedural Errors in Canal Enlarging Using Contemporary Techniques and Rotary Nickel-Titanium Instruments
The introduction of NiTi alloy to endodontics46 is purported to have problem solved many of the negative features associ-ated with stainless steel instruments, even in the hands of neophytes.38 Endodontic files made from this superelastic alloy are significantly more flexible and highly resistant to fracture and corrosion. This is particularly true with the newer instruments that are made of M-wire (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), a technologic improve-ment over the superelastic wire that was used initially for these types of instruments. M-wire files include Dentsply’s ProFile Vortex; GT Series Xfiles. Other new developments include heat-treated metals that change the crystalline struc-ture of the metal (R-phase [SybronEndo, Orange CA, USA]), resulting in more durable instruments, and Twisted Files or instruments with asymmetrical cross sections that increase flexibility and decrease stresses during application (Micro-Mega, Thônex, Switzerland). The advantages of NiTi files for canal cleaning and shaping seem to be enhanced canal negotiation, especially in curved canals; decreased canal transportation and ledging; reduced chance for breakage; faster and more efficient instrumentation; and no requisite precurving,56 as for stainless steel instruments.
The clinician must understand that NiTi instrumentation is not without its problems. A long learning curve may be necessary, and many unknowns remain. This is especially true as many newer instruments are appearing in the market-place on a regular basis. For example, when stressed, these instruments undergo a microscopic phase transformation and become structurally weaker. However, no visible or macro-scopic indication that the metal has become fatigued is usually exhibited. Thus a NiTi file may break without warning (unwinding), especially if used improperly.
Failure to Properly Enlarge and Shape the CanalFailure to remove pulp tissue, dentinal debris, and microor-ganisms from the root canal system (underpreparation or inadequate preparation) is a common error in root canal procedures, even with the vast array of NiTi instruments available.36 If the canal system is improperly shaped, it can prevent three-dimensional obturation, unless possibly a soft-ened core-carrier technique is used (see Chapter 12). This problem is usually not present when using greater-tapered NiTi instruments to the working length, unless the instru-ments are not applied properly to the canal anatomy. For example, some studies have questioned the ability of rotary NiTi instruments to enlarge and shape canals that are wide buccal-lingually.58 It is not the inability of the instruments during application that falls short of ideal, but rather how they are used by the clinician.
Inadequate preparation (which includes enlarging, shaping, cleaning, and disinfecting) of the canal system occurs in one or more of the following ways:
1. Insufficient preparation of the apical dentin matrix or apical third of the canal to control filling materials in the canal. This occurs when the shape of the apical portion of the canal is irregular, and minimal instrumentation is done in favor of small apical sizes36; when the canal is reasonably round, and the enlarging is insufficient to contact all the canal walls; or when NiTi rotary instruments are only used in a vertical direction—a major flaw in using NiTi rotary instruments, not understood by many clinicians—and not used in a lateral or shaving motion when the canal anatomy indicates this type of enlarging and shaping are necessary.
2. Insufficient use of tissue-dissolving and bactericidal irrigants (NaOCl) or their inability to reach the apical third because of inadequate shaping due to small apical sizes with minimal tapers. In such a case, the canal will be underprepared.
3. Inadequate canal shaping (flaring) that prevents depth of spreader or plugger penetration during compaction. In this case, there will be incomplete obturation with voids.
4. Establishing the working length short of the apical constriction, especially in cases of pulpal necrosis.
5. Inadvertent development of ledges and blockages that prevent complete canal preparation.
Inadequate canal preparation can generally be prevented by adhering to the principles of problem solving previously dis-cussed in this chapter. The existence of this problem is usually identified at the time of obturation when the compacting instruments cannot be placed to the appropriate length for the filling technique chosen; when the master apical file cannot reach the working length; or when the master apical file penetrates beyond the established working length, with

chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal 205
• Easy removal of obstacles that prevent access to the root apex (e.g., pulp stones)
• Enhanced tactile feedback with all instruments by removal of coronal interferences
• Enhanced movement of instruments apically into the canal
• Enhanced working length determination as a result of minimal tooth contact in the coronal third
• Increased space for irrigant penetration and débridement
• Rapid removal of the bulk of dental pulp tissue located in the coronal third
• Straight-line access to root curves and uniting canal junctions
• Enhanced movement of dentinal and soft-tissue debris coronally
• Decreased deviation of instruments in canal curvatures by reducing root wall contact
• Decreased canal blockages• Minimization of instrument separation by reducing
contact with the root canal walls• More ideal canal shapes that facilitate and promote
enhanced canal obturation• Predictable levels of quality canal cleaning and
shaping• Facilitation of one-visit root canal procedures within a
reasonable period
Biologically, many of the benefits attained with the crown-down technique mirror or complement the clinical benefits and ultimately contribute significantly to the overall case success. These include:
• Rapid removal of contaminated, infected tissue from the root canal system
• Removal of tissue debris coronally, thereby minimizing the pushing of debris apically
• Reduction in postoperative pain that may occur with the apical extrusion of debris
• Better dissolution of contaminated tissue, with increased irrigant penetration
• Easy smear layer removal because of better contact of chelating agents with canal walls
• Enhanced disinfection of canal irregularities as a result of irrigant penetration in patent canals and patent tubule orifices after removal of the smear layer
• More accurate management of the working length, canal cleaning and shaping, and control of obturation materials with respect to the biology of the apical root tissues and surrounding periradicular tissues
A collage of cases that highlight the more common errors encountered in canal enlarging and shaping when the dictates of prevention described in this chapter are not adhered to is seen in Fig. 10-16.
K-files, Hedström files, S-files, Flex-R files, reamers, and compactors are available in NiTi alloy, but because of their extreme flexibility are not designed for creating a pathway in the canal, for negotiating small, calcified curved canals, or for bypassing ledges. Stainless steel instruments should be used initially for pathfinding because of their enhanced stiffness. The recent introduction of the C+ file or ProFinder files (Dentsply Maillefer, Ballaigues, Switzerland) exclusively for this purpose supports this need.
Once the canal has been negotiated or the ledge has been bypassed and removed, NiTi instruments can then be used. Because a reduced tactile sensation may exist when NiTi hand instruments are used, the clinician may feel that the file is not cutting. On the contrary, NiTi files can be as aggressive as stainless steel files, and excessive removal of root dentin can occur if filing pressures and instrumentation times are not carefully monitored. If NiTi hand files are used in a conventional push-pull or filing motion, especially K-files and S-files, deviations in anatomy may occur, with a ten-dency of the outer wall of the preparation to belly out below the height of curvature. This is probably attributable to the file’s predisposition to unflex or straighten out during appli-cation. Research suggests that NiTi files may function best and cause less transportation and deviation in anatomy when used in a reaming or rotary motion, as that found with hand greater-taper (GT) files or hand ProTaper instruments. In turn, the evolution of mechanized or rotary instrumentation, using specially designed NiTi files in gear-reduction or elec-trically driven high-torque hand pieces, has revolutionized root canal procedures because of their speed (ranging from 250 to 500 rpm) and efficacy in canal shaping and maintain-ing canal curvature. Although such variably shaped NiTi files are quite flexible, NiTi metal, like any other metal, will eventually fail when rotated in a curved canal and definitely in a multicurved canal. Strict monitoring of instrument use should be maintained so that NiTi files can be periodically disposed of before failure. In addition, care must be taken to use these systems per the manufacturer’s instructions (e.g., a crown-down approach with light pressure is essential when using most NiTi rotary instruments). These systems require a significant learning curve to achieve mastery. Rotary NiTi instruments are used in the coronal-to-apical technique or crown-down technique, thereby eliminating many of the pre-viously discussed problems with stainless steel instruments.
Importance of the Crown- Down TechniqueThe clinical benefits of using the crown-down technique are many and greatly influence the achievement of predict-able success with nonsurgical root canal procedures. These benefits can be achieved with all instrument types, but efficiency favors rotary NiTi instruments. However, inte-grated enlarging and shaping techniques with a wide range of instruments will often be necessary, given the anatomic challenges posed by the root canal system. These benefits include:

206 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
BB
C D
E F
A
fIGURE 10-16 A, Fractured NiTi instrument segment in the apical portion of a significantly curved canal; removal not recommended. B, Maxillary molar and premolar with poorly shaped and obturated canals short of ideal. Patient has had continuous pain for weeks after treatment; revision recommended. C, Mandibular molar with poorly shaped and obturated canals and broken instrument in the mesial buccal canal. All canals short of ideal; revision recommended. D, Maxillary molar with poorly shaped and obturated canals short of the ideal; revision recommended. E, Mandibular molar with multiple enlarging and shaping errors, strip perforation in the mesial root, broken instrument in the mesial root, and post perforation in the distal root; extraction recommended. f, Even with NiTi instruments, major errors can occur when not paying attention to detail. Note strip perforation in the mesial buccal root (red arrow), apical deviation in the mesial buccal root (white arrow), and failure to gain full length in the palatal root (black arrow). The palatal curves to the buccal approximately 85% of the time.

chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal 207
REFEREnCES1. Abou-Rass M, Frank A, Glick D: The anticurvature filing method
to prepare the curved root canal, J Am Dent Assoc 101:792-794, 1980.
2. Ahlquist M, Henningsson O, Hultenby K, et al: The effectiveness of manual and rotary techniques in the cleaning of root canals: a scanning electron microscopy study, Int Endod J 34:533-537, 2001.
3. Albrecht LJ, Baumgartner JC, Marshall JG: Evaluation of apical debris removal using various sizes and tapers of ProFile GT files, J Endod 30:425-428, 2004.
4. Allen MJ, Glickman GN, Griggs JA: Comparative analysis of endodontic pathfinders, J Endod 33:723-726, 2007.
5. Alliët P, Berghmans J: Pitfalls to avoid in the cleaning and shaping of the pulp canal (French), Rev Belge Med Dent 54:282- 308, 1999.
6. Allison DA, Weber CR, Walton RE: The influence of the methods of canal preparation and the quality of apical and coronal seal, J Endod 5:298-304, 1979.
7. al-Omari MA, Dummer PM: Canal blockage and debris extrusion with eight preparation techniques, J Endod 21:154-158, 1995.
8. Arias A, Azabal M, Hidalgo JJ, et al: Relationship between postendodontic pain, tooth diagnostic factors and apical patency, J Endod 35:189-192, 2009.
9. Block RM, Lewis RD: Surgical treatment of iatrogenic canal block-ages, Oral Surg Oral Med Oral Pathol 63:722-732, 1987.
10. Byström A, Sundqvist G: Bacteriological evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy, Scand J Dent Res 89:321-328, 1981.
11. Card SJ, Sigurdsson A, Ørstavik D, et al: The effectiveness of increased apical enlargement in reducing intracanal bacteria, J Endod 28:779-783, 2002.
12. Chuste-Guillot MP, Badet C, Peli JF, et al: Effect of three nickel-titanium rotary file techniques on infected root dentin reduction, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:254-258, 2006.
13. Coldero LG, McHugh S, MacKenzie D, et al: Reduction in intra-canal bacteria during root canal preparation with and without apical enlargement, Int Endod J 35:437-446, 2002.
14. Dalton BC, Ørstavik D, Phillips C, et al: Bacterial reduction with nickel-titanium rotary instrumentation, J Endod 24:763-767, 1998.
15. Dumsha TC, Gutmann JL: Clinical guidelines for intentional replantation, Compend Contin Educ Dent. 6:604,606-608, 1985.
16. Flanders DH: Endodontic patency. How to get it. How to keep it. Why it is so important, N Y State Dent J 68(3):30-32, 2002.
17. Friedman S: Considerations and concepts of case selection in the management of post-treatment endodontic disease (treatment failure), Endod Topics 1:54-78, 2002.
18. Friedman S: Prognosis of initial endodontic therapy, Endod Topics 2:59-88, 2002.
19. Gesi A, Bergenholtz G: Pulpectomy—studies on outcome, Endod Topics 5:57-70, 2003.
20. Goldberg F, Massone EJ: Patency filing and apical transportation: an in vitro study, J Endod 28:510-511, 2002.
21. Greene KJ, Krell KV: Clinical factors associated with ledged canals in maxillary and mandibular molars, Oral Surg Oral Med Oral Pathol 70:490-497, 1990.
22. Griffiths IT, Chassot AL, Nascimento MF, et al: Canal shapes produced sequentially during instrumentation with Quantec SC
rotary nickel-titanium instruments: a study in simulated canals, Int Endod 34:107-112, 2001.
23. Gutiérrez JH, Brizuela C, Villota E: Human teeth with periapical pathosis after overinstrumentation and overfilling of the root canals: a scanning electron microscopic study, Int Endod J 32:40-48, 1999.
24. Hofheinz RH: Immediate root-filling, Dent Cosmos 34:182-186, 1892.
25. Holland R, Sant’Anna Júnior A, Souza V, et al: Influence of apical patency and filling material on healing process of dogs’ teeth with vital pulp after root canal therapy, Braz Dent J 16:9-16, 2005.
26. Hülsmann M, Peters OA, Dummer PMH: Mechanical preparation of root canals: shaping goals, techniques and means, Endod Topics 10:30-76, 2005.
27. Jafarzedeh H, Abbott PV: Ledge formation: review of a great chal-lenge in endodontics, J Endod 33:1155-1162, 2007.
28. Jain N, Tushar S: Curved canals: ancestral files revisited, Indian J Dent Res 19:267-271, 2008.
29. Kapalas A, Lambrianidis T: Factors associated with root canal ledging during instrumentation, Endod Dent Traumatol 16:229-231, 2000.
30. Kirkevang L-L, Hørsted-Bindslev P: Technical aspects of treatment in relation to treatment outcome, Endod Topics 2:89-102, 2002.
31. Lambrianidis T: Ledging and blockage of root canals during canal preparation: causes, recognition, prevention, management and outcomes, Endod Topics 15:56-74, 2006.
32. Lambrianidis T, Tosounidou E, Tzoanopoulu M: The effect of maintaining apical patency on periapical extrusion, J Endod 27: 696-698, 2001.
33. Lin LM, Rosenberg PA, Lin J: Do procedural errors cause end-odontic treatment failure? J Am Dent Assoc 136:187-193, 2005.
34. Marroquin BB: An anti-zipping preparation system (method and instrument) for curved canals: a preliminary report, J Endod 22:85-89, 1996.
35. Mullaney TP: Instrumentation of finely curved canals, Dent Clin North Am 23:575-592, 1979.
36. Paqué F, Ganahl D, Peters OA: Effects of root canal preparation on apical geometry assessed by micro-computed tomography, J Endod 35:1056-1059, 2009.
37. Peters OA, Peters CI: Cleaning and shaping of the root canal system. In Cohen S, Hargreaves KM, editors: Pathways of the pulp, ed 9, St Louis, 2006, Mosby-Elsevier.
38. Pettiette MT, Metzger Z, Phillips C, et al: Endodontic complica-tions of root canal therapy performed by dental students with stainless-steel K-files and nickel-titanium hand files, J Endod 25: 230-234, 1999.
39. Pi GL, Yin SH: A study of the related factors and prophylactic measures of endodontic interappointment emergencies (Chinese), Hua Xi Kou Qiang Yi Xue Za Zhi 22:471-473, 2004.
40. Rollison S, Barnett F, Stevens RH: Efficacy of bacterial removal from instrumented root canals in vitro relative to instrumentation technique and size, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94:366-371, 2002.
41. Schäfer E, Erier M, Dammaschke T: Comparative study on the shaping ability and cleaning efficiency of rotary M two instruments. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth, Int Endod J 39:203-212, 2006.
42. Schäfer E, Dammaschke T: Development and sequelae of canal transportation, Endod Topics 15:75-90, 2006.
43. Schäfer E, Schlingemann R: Efficiency of rotary nickel-titanium K3 instruments compared with stainless steel hand K-Flexofile. Part 2. Cleaning effectiveness and shaping ability in severely curved

208 chapter 10 | Problem-Solving Clinical Techniques in Enlarging and Shaping the Root Canal
tics, Philadelphia, 1989, WB Saunders.53. Tsesis I, Amdor B, Tamse A, et al: The effect of maintaining
apical patency on canal transportation, Int Endod J 41:4341-4435, 2008.
54. Walton RE: Current concepts of canal preparation, Dent Clin North Am 36:309-326, 1992.
55. Weine FS, Kelly RF, Lio PJ: The effect of preparation procedures on original canal shape and on apical foramen shape, J Endod 1:255-262, 1975.
56. Weine FS, Healey HJ, Gerstein H, et al: Precurved files and incre-mental instrumentation for root canal enlargement, J Can Dent Assoc 4:155-157, 1970.
57. Wolcott J, Rossman LE: Intentional replantation of endodontically treated teeth: an update, Compend Contin Educ Dent 24:68-72, 74, 2003.
58. Wu MK, Wesselink PR: A primary observation on the prepara-tion and obturation of oval canals, Int Endod J 34:137-141, 2001.
RECommEnDED ADDITIonAL READIngHüslmann M, Schäfer E: Apical patency: fact and fiction—a myth or
a must. A contribution to the discussion, ENDO (Long Engl) 3:285-307, 2009.
root canals of extracted teeth, Int Endod J 36:208-217, 2003.44. Schäfer E, Vlassis M: Comparative investigation of two rotary
nickel-titanium instruments: ProTaper versus RaCe. Part 2. Clean-ing effectiveness and shaping ability in severely curved root canals of extracted teeth, Int Endod J 37:239-248, 2004.
45. Senia ES, Wildey WL: The LightSpeed root canal instrumentation system, Endod Topics 10:148-150, 2005.
46. Serene TP, Adams JD, Saxena A: Nickel titanium instruments: applications in endodontics, St Louis, 1994, Ishiyaku EuroAmerica.
47. Siqueira JF, Jr.: Reaction of periradicular tissues to root canal treat-ment: benefits and drawbacks, Endod Topics 10:123-147, 2005.
48. Souza RA: The importance of apical patency and cleaning of the apical foramen on root canal preparation, Braz Dent J 17:6-9, 2006.
49. Tan BT, Messer HH: The quality of apical canal preparation using hand and rotary instruments with specific criteria for enlargement based on initial apical size, J Endod 38:658-664, 2002.
50. Tidmarsh BG: Preparation of the root canal, Int Endod J 15:53-61, 1982.
51. Tinaz AC, Alacam T, Uzun O, et al: The effect of disruption of apical constriction on periapical extrusion, J Endod 31:533-535, 2005.
52. Torabinejad M, Walton RE: Principles and practice of endodon-

209
Chapter 11
Problem Solving in Cleaning and Disinfecting the Root Canal System
Problem-Solving ListProblem-solving issues and challenges in cleaning and disinfecting the root canal system addressed in this chapter are:
What Is the Key Role of and the Rationale for the Use of Intracanal Irrigants?
What Is the Purpose of and the Rationale for the Use of Chelator Solutions in Root Canal Procedures?
What Is the Role of Disinfectants in Root Canal Procedures?
What Are the Best Disinfectants and How Should They Be Used to Achieve the Goals of Root Canal Disinfection Without Causing Problems?
One of the most neglected phases of endodontic treatment is the removal of minute fragments of organic debris and dentinal shavings from the root canal. It is an axiomatic principle of surgery that before a wound is ready for chemotherapy, all necrotic material and debris must be removed. Many dentists have failed to appreciate the importance of this basic rule of surgery and have relied principally on drug therapy rather than on thorough cleansing and irrigation of the root canal.26
L.I. GRoSSmAn, 1955
The concepts of cleaning and shaping the root canal system have been with us for years. In many respects, the two activi-ties are incompatible when there is sole reliance on intracanal instruments to accomplish these goals. Instruments can shape the canal, but true cleaning relies on irrigants.
What Is the Key Role of and the Rationale for the Use of Intracanal Irrigants?
The key role of root canal irrigants is to clean the canal during the enlarging and shaping process. Specifically, the objectives of the cleaning and shaping process are to remove the vital or necrotic dental pulp tissue and neutralize or eliminate bacteria and their associated metabolic byproducts. Although the shaping of the root canal has been enhanced with advances in metal technology, the actual cleaning of
the canal still relies heavily on the adjunctive use of chemi-cal rinses and soaks to achieve these goals because of the anatomic complexity and irregularity of the tooth (Fig. 11-1). In this respect, the use of irrigants that possess multiple characteristics, such as tissue-dissolving attributes and bacteriostatic or bactericidal capabilities, is warranted at all times. Other advantageous properties include rinsing away debris created during cleaning and shaping, lubricat-ing the instruments, and demineralizing and removing the smear layer.
No one solution as yet possesses all the properties of an ideal irrigant, but it is important to emphasize that the use of neutral solutions for the irrigation process (e.g., water, saline, anesthetic solutions) serves no useful purpose in the root canal system.
The effectiveness of NaOCl in cleaning and disinfection depends on the concentration of available chlorine and the pH of the solution. Hypochlorous acid (HOCl) is a weak acid and dissociates to the hypochlorite ion (OCl−) and

210 chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System
susceptible to percentages as low as 0.5%,7 but these species may not reflect bacterial populations found in the tooth with a necrotic infected pulp.64 Clinical use for both bacterial control and tissue dissolution favors percentages from 1% to 6%, with studies claiming various levels of superiority with a particular percentage. Manipulations that enhance the effi-cacy of NaOCl include warming the solution to at least 37°C.1 Within the bacterial species studied, bactericidal rates for NaOCl more than doubled for each 5°C rise in tempera-ture in the range of 5°C to 60°C.14 In particular when using steady-state planktonic E. faecalis cells, a temperature rise of 25°C increased the efficacy of NaOCl by a factor of 100.51 Within this framework of heating NaOCl, the capacity of a 1% solution at 45°C to dissolve human dental pulps was found to be equal to that of a 5.25% solution at 20°C.51 While apparently effective in a laboratory setting, there are no evidenced-based clinical studies to verify this efficacy as it relates to successful outcomes.
Using the NaOCl solutions for periods of 5 to 30 minutes in the root canal has also been advocated to enhance its effectiveness, but optimal times have not been determined.67 The application of sonics and ultrasonics to the NaOCl solu-tion have also been advocated,57 but the efficacy of these combinations has shown mixed results.27,60,63 Techniques for
proton (H+) depending on the solution pH. It is generally believed that HOCl is the active species in the germicidal action, whereas the concentration of OCl− is a key factor determining cleaning efficiency. This implies that the optimal pH region of the germicidal activity of NaOCl differs from that of its cleaning activity.22
The concentrations of NaOCl that are used during root canal procedures vary among clinicians and may very well be chosen empirically. Some bacterial populations are
B
C D
A
FIGURE 11-1 A, Tissue debris sandwiched in the anastomoses between the mesial buccal and mesial lingual canals of the mandibular molar after cleaning and obturation. B, Tissue debris that remains in a C-Shaped canal system after cleaning and shaping (H&E stain ×10). C, Scanning electron micrograph (SEM) shows the smear layer that is present during the shaping of the root canal is packed with tissue debris, dentin chips, and bacteria (×750). D, SEM showing surface tissue debris in anatomic irregularities after shaping and cleaning the root canal with irrigants (×2000).
CLINICAL PROBLEMProblem: What is the best irrigant to use during root canal procedures and why?
Solution: The best irrigant is sodium hypochlorite (NaOCl) in various concentrations. NaOCl is a highly effective irrigat-ing solution that is both antimicrobial and has tissue- dissolving capabilities.22,67 Additionally, it possesses bleaching and lubricating properties and has been shown to inactivate endotoxins,48 although calcium hydroxide is much better in this latter regard.53

chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System 211
Specialties, Tulsa, OK, USA). This innovative device agitates irrigation solutions during endodontic treatment. Evidence has indicated that dynamic movement of the irrigant signifi-cantly improves débridement.40 The system is designed to safely energize the hydrodynamic phenomenon. Claims are made that activated fluids promote deep cleaning and disin-fection into lateral canals, fins, webs, and anastomoses, with minimal apical extrusion because the activator tip is placed short of the working length in the canal.12
Claims have also been made relative to the application of ultrasonic irrigation devices alone and during canal cleaning and shaping.6,10,27 Significant débridement of canal irregulari-ties and bacterial reductions have been noted, but the exact nature of the process has been challenged as to mechanism of action.63
A development that has claimed to eliminate problems with the delivery of NaOCl is the EndoVAC (Discus Dental, Culver City, CA, USA). The device offers an apical negative pressure system that uses microcannulas to deliver irrigants to the canal and draws fluid away by evacuation. Claims are made that cleaning occurs to within 1 mm of the apex,31,43 without apical extrusion of solution.12 However, there are no data available at this time to indicate what happens in the last millimeter of the canal, or if this activity can penetrate into the dentinal tubules to eliminate biofilms, bacteria, or embedded endotoxins.
The most recent addition to this foray of irrigation devices is the ProUltra PiezoFlow irrigation device (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA). ProUltra PiezoFlow Ultrasonic Irrigation Needles are used to deliver irrigants by application of ultrasonic vibration. The PiezoFlow irrigation needles are used in conjunction with a piezo-electric ultra-sonic energy-generating unit to provide the energy for tip oscillation. A syringe or other irrigation source is attached to the Luer-lock connection on the ultrasonic needle. Removal of irrigant is through the operatory vacuum source. Compat-ible irrigants include sodium hypochlorite (up to 6%), EDTA (up to 17%), Chlorhexidine (up to 2%) and BioPure MTAD, however working times with each irrigant may vary.
NaOCl contact with dentin has been questioned as to its impact on the mechanical, chemical, and structural composi-tion of dentin.13,39,49 Evaluations were done ex vivo using different concentrations and different time frames to deter-mine the impact on the inorganic phase of dentin. While higher concentrations of NaOCl affected the elastic modulus and the flexural strength of dentin, no clinical relevance has been drawn or shown from these studies.
NaOCl should not be used as the final rinsing agent when resin-based bonded root canal filling materials are planned for canal obturation. The bonding of the sealer to the dentin may be altered. Alternatives are to finish with EDTA, chlorhexidine (CHX),8,9 or BioPure MTAD (Dentsply Tulsa Dental Specialties, Tulsa OK, USA). Studies have shown that a soft chelating solution (1-hydroxyethylidene-1, 1-bisphosphonate [HEPB]) not only removes the smear layer effectively but also enhances the bond strength of intracanal resins.11,68 However, the use of EDTA or MTAD as a final
this approach have been detailed in literature, but here again, meaningful clinical studies are lacking.61,62 Even with longer time periods, replenishment may be necessary to increase its effectiveness, especially in the presence of significant amounts of tissue and bacteria that may be encountered in highly irregular canal anatomies in cases of long-standing necrotic pulp. Similarly, when NaOCl has been used for long periods, the potential for altering the physical properties of dentin have been highlighted in vitro but not clarified in vivo.13,39,49 When used in conjunction with ethylenediamine tetraacetic acid (EDTA) or 10% citric acid,38 its antibacterial properties are not necessarily enhanced.45 When these solutions are used alternatively during canal cleaning and shaping, bacterial loads may be efficiently reduced.7
NaOCl should always be delivered passively to the canal to prevent a forceful extrusion beyond the apical foramen. This delivery is best accomplished by avoiding wedging the delivery needle in the canal, expressing the solution slowly, and using specially tipped side-delivery needles that enhance the cleaning of the dentin walls while minimizing potential risks during its use (Fig. 11-2). The passive movement of small amounts beyond the apical foramen should not create problems for the patient. Forceful movement of greater volumes of NaOCl will, however, be deleterious, and the literature is replete with “sodium hypochlorite accidents.”30 Newer technologies that prevent this extrusion but at the same time are effective in removing the smear layer include the intracanal aspiration technique, in which the irrigant is delivered from the tip of an injection needle connected to an electric apex locator (EAL) placed 2 to 3 mm short of the root end. Studies indicate that there is limited extrusion of the irrigant when applied in this manner.21 A further develop-ment is the EndoActivator (Dentsply Tulsa Dental
FIGURE 11-2 Side-delivery needle enables delivery of irrigating solutions to the root canal walls to enhance canal cleaning. (Courtesy Dentsply Maillefer, Ballaigues, Switzerland.)

212 chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System
What Is the Purpose of and the Rationale for the Use of Chelator Solutions in Root Canal Procedures?
Chelates are stable complexes of metal ions with organic substances as a result of ring-shaped bonds.45,67 The stability is a result of the bond between the chelator, which has more than one pair of free electrons, and the central metal ion. Chelates bind and inactivate metallic ions, in particular during their demineralizing effect on dental hard tissues when used in the form of EDTA. Detergents have been added to solutions of EDTA to reduce the surface tension of the chelate, thereby facilitating the wetting of the root canal wall and increasing the chelator’s ability to penetrate the dentin. Citric acid has also been used for this purpose but may be more aggressive than EDTA. In essence, these solu-tions soften and dissolve inorganic dentin particles, thereby either preventing the accumulation of debris on the root canal walls or removing it once it is present.28
For root canal procedures, chelating agents are available commercially in liquid and paste forms. These substances may assist in penetrating calcified orifices and root canals, enhancing the removal of the smear layer during cleaning and shaping and serving as excellent lubricants for both hand and rotary instruments (Figs. 11-4 and 11-5). Chelating agents are used primarily as “soaks” in the root canal after cleaning and shaping, or alternating with NaOCl during the cleaning process. Their application with ultrasonics appears beneficial even in the apical portion of the canal.32 When used in con-junction with NaOCl for 1-, 3-, and 5-minute periods in laboratory studies, the smear layer was effectively removed.56
These solutions have relatively limited antiseptic capaci-ties45 but may assist in bacterial reduction through the removal of debris on the canal wall, possibly including biofilms.67,68 Both clinically relevant solutions (EDTA and 10% citric acid) do have an impact on the effectiveness of NaOCl4 by imme-diately reducing the available chlorine, thereby rendering the NaOCl ineffective against bacteria and necrotic tissue. The same is true for chelates in paste form, such as RC-Prep (10% urea peroxide, 15% EDTA, and glycol in an aqueous oint-ment base [Premier Dental, Plymouth Meeting, PA, USA]), Glyde file (15% EDTA and 10% urea peroxide in an aqueous solution [Dentsply, Surrey, UK]), and File-EZE (19% EDTA in an aqueous, water-soluble solution [Ultradent Co., South Jordan, Utah, USA]). Recent studies have identified other chelators that may be more effective than EDTA, but there are no clinical data to support their efficacy or outcomes.58
An additional solution designed to remove the smear layer (in conjunction with NaOCl) is BioPure MTAD (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), which is a mixture of tetracycline (doxycycline) and acid detergent (citric acid).41 Because of its components, it also qualifies as a disinfectant. Studies have shown mixed results in its efficacy.
rinse may actually cause a collapse of the dentin matrix struc-ture on the surface of the dentin, thereby impeding root canal sealer infiltration and formation of a high-quality hybrid layer bonding.23,54,55
NaOCl has strong support as being the best intracanal irrigant67 because it fulfills most of the ideal requirements for this purpose, but it will not dissolve and remove the smear layer created during canal enlargement and shaping (Fig. 11-3).35 Other solutions (or a combination of solu-tions) or mechanisms must be considered for this purpose. Smear layer removal is discussed later; elimination of this bioburden-packed debris is essential in contemporary root canal procedures to achieve a long-term positive outcome in treatment.
Clinicians must understand that challenges that must be overcome in the root canal system relative to tissue removal, bacterial elimination, and complete disinfection of the root canal system cannot be met successfully without the use of NaOCl. There is no rationale or scientific basis for the use of water, saline, hydrogen peroxide, or alcohol as the primary root canal irrigant.60 Even if rinsing of debris is considered a main objective, these solutions are not effective.67 While some may choose to use chlorhexidine as the primary irrig-ant, it also is ineffective in achieving the stated goals for root canal irrigation and disinfection (see section below on the best disinfectants).67
FIGURE 11-3 After cleaning and shaping with sodium hypochlorite, the smear layer (arrows) can still be seen in this low-power magnification of the root canal wall (H&E stain ×10).

chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System 213
C
A
B
FIGURE 11-4 A, Apical calcifications in a cleared root apex will require the use of chelating agents to assist in removal and canal penetration. B, Calcifications in the midroot portion in small, irregular canal areas make cleaning very difficult. C, Multiple canal closures and narrowings (arrows) due to increased formation of irritational dentin (B&B stain ×100).
FIGURE 11-5 A, Scanning electron micrograph (SEM) showing cross-section of dentin on which a thick smear layer has formed when irrigants and chelating agents are not used during cleaning and shaping. The degree of smear layer formation is increased with the use of rotary instruments (×2000). B, Longitudinal SEM appearance of smear layer that covers the dentinal tubules and harbors undesirable irritants (×1000).
A B
Continued

214 chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System
What Are the Best Disinfectants and How Should They Be Used to Achieve the Goals of Root Canal Disinfection Without Causing Problems?
Historically, root canal procedures relied heavily on a wide range of phenolic and formaldehyde preparations to disinfect the canal. Sadly, little effort was expended in tissue removal from the canal; the disinfecting agents alone were relied on to sterilize the canal. More often than not, these agents created significant problems for the patient and a false sense of achieve-ment for the clinician if the patient appeared symptom free.
Within the modern tenets of root canal treatment, tissue removal is still the first step in root canal disinfection. When
What Is the Role of Disinfectants in Root Canal Procedures?
Disinfectants are to be used to minimize or eliminate bacte-rial populations in the shaped root canal system. The ability of disinfectants to achieve their goals during root canal pro-cedures is predicated on the removal of the gross debris in the canal system and the effective dissolution of the remain-ing pieces of tissue and fragmented predentin following canal shaping. This is accomplished most effectively with NaOCl when the canal has been opened and shaped sufficiently to allow for a proper flow of irrigants apically and into irregu-larities. Disinfectants are also more effective when the smear layer has been removed, in particular with disinfection of the exposed dentinal tubules. Finally, disinfectants will only be effective in a canal system that is sealed from oral fluids.
C D
E
F
C, Use of appropriate irrigants and chelating agents during cleaning and shaping can reduce the smear layer to loose particles (rather than the matted layer seen in B) that can be removed from the canal with copious soaking and rinsing with chelating agents (×1500). D, SEM showing complete removal of the smear layer in the apical portion of the canal (×1000). Note the fewer tubules and greater amounts of peritubular and intertubular dentin. E, SEM showing complete removal of the smear layer in the coronal portion of the canal with patent dentinal tubules (×1200). F, Low magnification of the root canal and dentin wall after the smear layer has been removed (H&E stain ×10).
FIGURE 11-5, cont’d

chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System 215
some studies to be efficacious when mixed with calcium hydroxide in the root canal for initial treatment,5,46 and revision,68,69 while others have indicated that CHX was more efficacious alone.15,25 Heat can enhance the antibacterial activity of both substances individually.18
Basically, three disadvantages are found with all presently used disinfectants. First, if the smear layer is not removed, the agent has no access to the dentinal tubules and the bac-teria that may be present within (Fig. 11-6). Second, move-ment of the disinfectants beyond the apical foramen into the periradicular tissues may cause adverse sequelae. Therefore, all disinfectants are to be placed carefully in the canal without application of pressure. This may be a challenge with those products that come in syringes and have long needles or tips for delivery to the canal. The delivery tips must not be bound against the canal wall. Ideally, if the materials are placed in the coronal third of the canal, a hand K-file can be used to safely carry the material apically. Likewise a rotary NiTi instrument that fits loosely in the canal can be used in reverse to place the material apically; the file is placed only to the middle third, and the rotary action will carry the material apically. Also, there are rotary instruments (PacMac Conden-sor [SybronEndo, Orange, CA, USA]) designed to carry the materials (primarily calcium hydroxide slurries) apically. Third, although disinfectants are not designed to be used as canal irrigants during cleaning and shaping procedures, some clinicians use various concentrations or gels of CHX (pre-dominately 0.12%) as the irrigant of choice.20 This solution will not dissolve tissue,42 chemically clean the root canal system, or have an impact on bacteria embedded in tissue debris in the canal. Therefore, the efficacy and safety of this
performed with NaOCl as the irrigant, significant disinfec-tion is achieved; only in cases in which additional agents are warranted are disinfectants indicated. This includes teeth with necrotic pulps that are being treated in more than one visit and teeth that are undergoing revision of failed root canal procedures.64 (For teeth that have suffered luxation or avulsion trauma, the use of disinfecting agents will be dis-cussed in Chapter 19; for teeth undergoing apexification see Chapter 13.) Common agents indicated for use during routine root canal procedures include:
• Calcium hydroxide19,33: Can be mixed in sterile water to create a water slurry that is carried to the root canal or is available premixed in a syringe (Calcigel [Dental A2Z Ltd., UK]; Pulpdent Paste/Forendo Paste [Pulpdent Corp., Watertown MA, USA]; Calasept Plus [Nordiska Dental, Ängelholm, Sweden]; Vitapex [Neo-Dent International Inc., Federal Way, WA, USA]). Calcium hydroxides have a range of pH, but ideally the higher the pH, the more effective the material. They will kill bacteria on contact and are effective in tissue dissolution.64
• Iodine37: When used in the form of iodine potassium iodide (IKI 2%), it is very effective and efficacious but not available in a commercial form.
• Ledermix paste3: A composition of 3.21% demethylchlortetracycline and 1% triamcinolone acetonide is available in a water-soluble cream. Not approved for use in the United States.
• Chlorhexidine*: Commonly used as a 2% solution of chlorhexidine gluconate, CHX has been shown in
NP
A B
FIGURE 11-6 A, Gross movement of bacteria into the dentinal tubules (B&B stain ×40). B, Necrotic pulp (NP) and infected canal space, with movement of bacteria into the tubules (Brown & Brenn stain ×100).
*References 15, 17, 25, 29, 46, 50, and 59.

216 chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System
14. Dychdala GR: Chlorine and chlorine compounds. In Block SS, editor: Disinfection, sterilization and preservation, Philadelphia, 1991, Lea & Febiger.
15. Ercan E, Dalli M, Dülgergil CT: In vitro assessment of the effec-tiveness of chlorhexidine gel and calcium hydroxide paste with chlorhexidine against Enterococcus faecalis and Candida albicans, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102(2);e27-e31, 2006.
16. Estrela C, Estrela CR, Decurcio DA, et al: Antimicrobial efficacy of ozonated water, gaseous ozone, sodium hypochlorite and chlorhexidine in infected human root canals, Int Endod J 40:85-93, 2007.
17. Estrela C, Silva JA, de Alencar AH, et al: Efficacy of sodium hypo-chlorite and chlorhexidine against Enterococcus faecalis—a system-atic review, J Appl Oral Sci 16(6):364-368, 2008.
18. Evanov C, Liewehr F, Buxton TB, et al: Antibacterial efficacy of calcium hydroxide and chlorhexidine gluconate irrigants at 37 degrees C and 46 degrees C, J Endod 30:653-657, 2004.
19. Fava LR, Saunders WP: Calcium hydroxide pastes: classification and clinical indication, Int Endod J 32:257-282, 1999.
20. Ferraz CC, Gomes BP, Zaia AA, et al: Comparative study of the antimicrobial efficacy of chlorhexidine gel, chlorhexidine solution and sodium hypochlorite as endodontic irrigants, Braz Dent J 18:294-298, 2007.
21. Fukmoto Y, Kikuchi I, Yoshioka T, et al: An ex vivo evaluation of a new root canal irrigation technique with intracanal aspiration, Int Endod J 39:93-99, 2006.
22. Fukuzaki S: Mechanisms of action of sodium hypochlorite in cleaning and disinfection processes, Biocontrol Sci 11(4):147-157, 2006.
23. García-Godoy F, Loushine RJ, Itthagarun A, et al: Application of biologically-oriented dentin bonded principles to the use of end-odontic irrigants, Am J Dent 18:281-290, 2005.
24. Giardino L, Ambu E, Savoldi E, et al: Comparative evaluation of antimicrobial efficacy of sodium hypochlorite, MTAD, and Tetra-clean against Enterococcus faecalis biofilm, J Endod 33:852-855, 2007.
25. Gomes BP, Souza SF, Ferraz CC, et al: Effectiveness of 2% chlorhexidine gel and calcium hydroxide against Enterococcus faecalis in bovine root dentine in vitro, Int Endod J 36:267-275, 2003.
26. Grossman LI: Root canal therapy, 4 ed, Philadelphia, 1955, Lea & Febiger.
27. Gutarts R, Nusstein J, Reader A, et al: In vivo debridement efficacy of ultrasonic irrigation following hand-rotary instrumentation in human mandibular molars, J Endod 31:166-170, 2005.
28. Hülsmann M, Heckendorff M, Lennon Á: Chelating agents in root canal treatment: mode of action and indications for their use, Int Endod J 36:810-830, 2003.
29. Kanisavaran ZM: Chlorhexidine gluconate in endodontics: an update review, Int Dent J 58:247-257, 2008.
30. Kleier DJ, Averbach RE, Mehdipour O: The sodium hypochlorite accident: experience of diplomats of the American Board of End-odontics, J Endod 34:1346-1350, 2008.
31. Kratchman GM: Improving endodontic success through use of the EndoVac irrigation system, Endod Pract 12(1):17-20, 2009.
32. Kuah HG, Lui JN, Tseng PS, et al: The effect of EDTA with and without ultrasonics on removal of smear layer, J Endod 35:393-396, 2009.
33. Law A, Messer H: An evidence-based analysis of the antibacterial effectiveness of intracanal medicaments, J Endod 30:689-694, 2004.
choice has not been demonstrated, and its use reflects a lack of understanding regarding the procedures of cleaning, shaping, and disinfecting the root canal system. Because the disinfectants available to the contemporary clinician are effec-tive in achieving their goals in the root canal, the use of phe-nolic agents and formaldehyde products in the root canal system is not indicated and should be abandoned.
Future projections for the elimination of bacterial species include applications of ultrasonic energy during final irriga-tion protocols10; light-activated/photo-activated disinfection (PAD)34,36,65; and ozonated water or gaseous ozone.16 All ini-tiatives require significant development and both laboratory research and clinically relevant prospective studies. In addi-tion to attempts to eradicate bacteria, further attempts have also been made to eliminate bacterial biofilms that tend to be present when bacteria are present in the root canal spaces over long periods of time.47 Attempts at biofilm elimination have included dynamic irrigation protocols,40,63 varying irrigants and times of application,2,44,66 and using alkaline hypochlo-rites and chlorosulfamates52 or newly developed irrigants.24
RefeRenceS1. Abou-Rass M, Oglesby SW: The effects of temperature, concentra-
tion , and tissue type on the solvent ability of sodium hypochlorite, J Endod 7:376-377, 1981.
2. Arias-Moliz MT, Ferrer-Luque CM, Espigares-García M, Baca P: et al: Enterococcus faecalis biofilms eradication by root canal irrig-ants, J Endod 35:711-714, 2009.
3. Athanassiadis B, Abbott PV, George N, et al: An in vitro study of the antimicrobial activity of some endodontic medicaments and their bases using an agar well diffusion assay, Aust Dent J 55(2):141-146, 2009.
4. Baumgartner JC, Ibay AC: The chemical reaction of irrigants used for root canal debridement, J Endod 13:47-51, 1987.
5. Basrani B, Ghanem A, Tjäderhane L: Physical and chemical prop-erties of chlorhexidine and calcium hydroxide-containing medica-tions, J Endod 30:413-417, 2004.
6. Burleson A, Nusstein J, Reader A, et al: The in vivo evaluation of hand/rotary ultrasound instrumentation in necrotic, human man-dibular molars, J Endod 33:782-787, 2007.
7. Byström A, Sundqvist G: The antibacterial action of sodium hypo-chlorite and EDTA in 60 cases of endodontic therapy, Int Endod J 18:35-40, 1985.
8. Carrilho MR, Geraldeli S, Tay F, et al: In vivo preservation of the hybrid layer by chlorhexidine, J Dent Res 86:529-533, 2007.
9. Carrilho MR, Tay FR, Donnelly AM, et al: Host-derived loss of dentin matrix stiffness associated with solubilization of collagen, J Biomed Mater Res B Appl Biomater 90(1):373-380, 2009.
10. Carver K, Nusstein J, Reader A, et al: In vivo antibacterial efficacy of ultrasound after hand and rotary instrumentation in human mandibular molars, J Endod 33:1038-1043, 2007.
11. De-Deus G, Namen F, Galan J, Jr, et al: Soft chelating irrigation protocol optimizes bonding quality of Resilon/Epiphany root fill-ings, J Endod 34:703-705, 2008.
12. Desai P, Himel V: Comparative safety of various intracanal irriga-tions systems, J Endod 35:545-549, 2009.
13. Driscoll CO, Dowker SE, Anderson P, et al: Effects of sodium hypochlorite solution on root surface dentine composition, J Mater Sci Mater Med 13:219-223, 2002.

chapter 11 | Problem Solving in Cleaning and Disinfecting the Root Canal System 217
52. Stewart PS, Rayner J, Roe F, et al: Biofilm penetration and disinfec-tion efficacy of alkaline hypochlorite and chlorosulfamates, J Appl Microbiol 91:525-532, 2001.
53. Tanomaru JM, Leonardo MR, Tanomaru Filho M, et al: Effect of different irrigation solution and calcium hydroxide on bacterial LPS, Int Endod J 36:733-739, 2003.
54. Tay FR, Pashley DH, Loushine FJ, et al: Ultrastructure of smear layer-covered intraradicular dentin after irrigation with BioPure MTAD, J Endod 32:218-221, 2006.
55. Tay FR, Gutmann JL, Pashley DH: Microporous, demineralized collage matrices in intact radicular dentin created by commonly used calcium-depleting endodontic irrigants, J Endod 33:1086-1090, 2007.
56. Teixeira CS, Felippe MC, Felippe WT: The effect of application time of EDTA and NaOCl on intracanal smear layer removal: an SEM analysis, Int Endod J 38:285-290, 2005.
57. Townsend C, Maki J: An in vitro comparison of new irrigant and agitation techniques to ultrasonic agitation in removing bacteria from a simulated root canal, J Endod 35:1040-1043, 2009.
58. Tripodi D, D’Ercole S, De Fazio P, et al: Demineralizing action of EDTA in endodontics, Int J Immunopathol Pharmacol 20 (1 Suppl 1):93-96, 2007.
59. Vahdaty A, Pitt Ford TR, Wilson RF: Efficacy of chlorhexidine in disinfecting dentinal tubules in vitro, Endod Dent Traumatol 9:243-248, 1993.
60. van der Sluis LW, Gambarini G, Wu MK, et al: The influence of volume, type of irrigant and flushing method on removing artifi-cially place dentine debris from the apical root canal during passive ultrasonic irrigation, Int Endod J 39:472-476, 2006.
61. van der Sluis LW, Wu MK, Wesselink PR: The efficacy of ultrasonic irrigation to remove artificially placed dentine from human root canals prepared using instruments of varying pluggers, Int Endod J 38:764-768, 2005.
62. van der Sluis LW, Wu MK, Wesselink PR: A comparison between a smooth wire and a K-file in removing artificially placed dentine debris from root canals in resin blocks during ultrasonic irrigation, Int Endod J 38:593-596, 2005.
63. van der Sluis LW, Versluis M, Wu MK, et al: Passive ultrasonic irrigation of the root canal: a review of the literature, Int Endod J 40:415-426, 2007.
64. Wesselink P, Bergenholtz G: Treatment of the necrotic pulp. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
65. Williams JA, Pearson GJ, Colles MJ: Antibacterial action of pho-toactivated disinfection {PAD} used on endodontic bacteria in planktonic suspension and in artificial and human root canals, J Dent 34:363-371, 2006.
66. Williamson AE, Cardon JW, Drake DR: Antimicrobial suscepti-bility of monoculture biofilms of a clinical isolate of Enterococcus faecalis, J Endod 35:95-97, 2009.
67. Zehnder M: Root canal irrigants, J Endod 32:389-398, 2006.68. Zehnder M, Schmidlin P, Sener B, et al: Chelation in root canal
therapy reconsidered, J Endod 31:817-820, 2005.69. Zerella JA, Fouad AF, Spångberg LS: Effectiveness of a calcium
hydroxide and chlorhexidine digluconate mixture as disinfectant during retreatment of failed endodontic cases, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100:756-761, 2005.
34. Lee MT, Bird PS, Walsh LJ: Photo-activated disinfection of the root canal: a new role for lasers in endodontics, Aust Endod J 30(3):93-98, 2004.
35. Lester KS, Boyde A: Scanning electron microscopy of instru-mented, irrigated and filled root canals, Br Dent J 143:359-367, 1977.
36. Lim Z, Cheng JL, Lim TW, et al: Light activated disinfection: an alternative endodontic disinfection strategy, Aust Dent J 54(2): 108-114, 2009.
37. Lin S, Kfir A, Laviv A, et al: The in vitro antibacterial effect of iodine potassium iodide and calcium hydroxide in infected den-tinal tubules in different time intervals, J Contemp Dent Pract 2(10):59-66, 2009.
38. Loel DA: Use of acid cleanser in endodontic therapy, J Am Dent Assoc 90:148-151, 1975.
39. Marending M, Luder HU, Brunner TJ, et al: Effect of sodium hypochlorite on human root dentine—mechanical, chemical and structural evaluation, Int Endod J 40:786-793, 2007.
40. McGill S, Gulabivala K, Mordan N, et al: The efficacy of dynamic irrigation using a commercially available system (RinsEndo) deter-mined by removal of collage “bio-molecular film” from an ex vivo model, Int Endod J 41:602-608, 2008.
41. Mozaveni MA, Javaheri GH, Poorroosta P, et al: Effect of 17% EDTA and MTAD on intracanal smear layer removal: a scanning electron microscope study, Aust Dent J 35(1):13-17, 2009.
42. Naenni N, Thoma K, Zehnder M: Soft tissue dissolution capacity of currently used and potential endodontic irrigants, J Endod 30:758-787, 2004.
43. Nielsen BA, Baumgartner JC: Comparison of the EndoVac system to needle irrigation of root canals, J Endod 33:611-615, 2007.
44. Ozok AR, Wu MK, Luppens SB, et al: Comparison of growth and susceptibility to sodium hypochlorite of mono- and dual-species biofilms of Fusobacterium nucleatum and Peptostreptococcus (micromonas) micros, J Endod 33:819-822, 2007.
45. Patterson SS: In vivo and in vitro studies of the effect of the diso-dium salt of ethylenediamine tetra-acetate on human dentine and its endodontic implications, Oral Surg Oral Med Oral Pathol 16:83-103, 1963.
46. Podbielski A, Spahr A, Haller B: Additive antimicrobial activity of calcium hydroxide and chlorhexidine on common endodontic bacterial pathogens, J Endod 29:340-345, 2003.
47. Sena NT, Gomes GP, Vianna ME, et al: In vitro antimicrobial activity of sodium hypochlorite and chlorhexidine against selected single-species biofilms, Int Endod J 39:878-885, 2006.
48. Silva LA, Leonardo MR, Assed S, et al: Histological study of the effect of some irrigating solutions on bacterial endotoxin in dogs, Braz Dent J 15:109-114, 2004.
49. Sim TP, Knowles JC, Ng YL, et al: Effect of sodium hypochlorite on mechanical properties of dentine and tooth surface strain, Int Endod J 34:120-132, 2001.
50. Siqueira JF, Jr, Paiva SS, Rôcas IN: Reduction in the cultivable bacterial populations in infected root canal by chlorhexidine-based antimicrobial protocol, J Endod 33:541-547, 2007.
51. Sirtes G, Waltimo T, Schaetzle M, et al: The effects of tempera-ture on sodium hypochlorite short-term stability, pulp dissolution capacity, and antimicrobial efficacy, J Endod 31:669-671, 2005.

218
Chapter 12
Problem-Solving Challenges in Root Canal Obturation
Problem-Solving ListProblem-solving challenges and dilemmas in obturation of the enlarged, shaped, cleaned, and disinfected root canal system addressed in this chapter are:
Root Canal Sealers: Their Role and Use
Gutta-Percha Obturation Techniques
Lateral compaction
Vertical compaction
Thermoplasticized injection techniques
Thermoplasticized core-carrier techniques
Resin-Bonded Obturation Techniques
Guiding Principles for All Obturation Techniques
Problems Preparing to Obturate the Canal
Problems During Canal Obturation
Problems Identified After Obturation
Gutta-percha . . . for convenience, utility, and harmlessness withal, it is invaluable.19
A. HIll, 1848
The evolution of root filling materials and techniques has a long and challenging history, but not much has changed in this regard. Gutta-percha, the use of which is credited to Dr. Asa Hill in 1847, is still being used to obturate prepared root canals.19 Many teeth have been retained in symptom-free function thanks to this material filling the root canals, and any failures were not due to the material. During the past 80 years, there have been efforts to change the way root canals are filled. Materials have included paste fills, silver cones, synthetic gutta-perchas, and resin-bonded materials. In each case, there must have been a clinical problem the dental clinician faced that prompted the need for a better product or an easier and more thorough way to achieve the goal of root canal obturation. That goal: to fill completely and seal the enlarged, shaped, cleaned, and disinfected space created when the dental pulp of the tooth was removed. What were those problems, those challenges? What were their effects on what is done today? Have the problems been
rectified? Is the clinician in a better position to provide predi-cate outcomes with the present-day obturation materials and techniques?
Dr. Neil Postman, a noted author and professor of media and communications at New York University, once posed a very useful question in an interview on PBS: “When con-fronted with a new technology, whether it’s a cellular phone or high-definition television or cyberspace or Internet, the question, the one question, should be What is the problem to which this technology is the solution?” Later in the inter-view, he concludes with the observation, “It is very easy to be swept up in the enthusiasm for technology, and of course all the technophiles around, all the people who adore tech-nology, are promoting it everywhere you turn.”33
Turning these concepts to root canal obturation, pastes were developed to speed the tedious process of obturation and more effectively move filling material into canal irregu-larities.16 Innovative clinicians, who were also dabbling scientists, thought they could create a more biological filling material, one that would destroy bacteria while sealing the root canal. Silver cones were brought to the clinician to enhance bacterial control and create a more radiopaque root canal filling on the radiograph (possibly the beginning
Perhaps there is no technical operation in dentistry or surgery where so much depends on the conscientious adherence to high ideals as that of pulp-canal filling.17
E.H. HATTOn, 1924

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 219
Ideally, all sealers should be antimicrobial and biocompat-ible; some sealers or portions of substances within them may be absorbed when exposed to tissues and fluids.5,29,37 Sub-stances used for radiopacity within the sealer are generally insoluble and may remain in the tissues either engulfed by macrophages or surrounded by fibrous capsules (Fig. 12-4). If large amounts are pushed beyond the canal confines, the patient may experience discomfort, especially if the sealer has a slow set, or chronic inflammation may persist and create problems at a later time.5,25,37 Sealer may be consolidated during the healing process and remain pushed up against the root of the tooth by the encapsulating tissue (Fig. 12-5), never really allowing the tissue to heal fully, although clini-cians attempt to identify this as healing so long as the patient is symptom free.
Sealers are generally grouped based on their primary com-ponent or chemical make up (e.g., zinc oxide eugenol, poly-ketone, epoxy, calcium hydroxide, silicone, glass ionomer, or resin based). Ideally, none of these sealers should be extruded beyond the end of the root canal, because chronic inflammation may persist (see Chapter 9). However, many clinicians attempt to extrude the sealer with their obturation technique and empirically claim that when they see sealer extruded beyond the confines of the canal, the canal is “per-fectly sealed.” The fallacies in this position are that (1) a seal cannot be seen on a radiograph, (2) the radiograph only represents a two dimensions of a highly variable three-dimensional object, and (3) there is no evidence-based infor-mation to support this claim.10 As noted earlier, there is evidence to support the long-term presence of chronic inflammation.34
of esthodontics within endodontics). Silver cones also sped up the obturation process as placement was easy, especially in small, tortuous root canals—and in some respects served as compactors of the root canal sealer into canal irregulari-ties.21 Synthetic gutta-perchas were developed to address the decrease in availability of naturally occurring gutta-percha and eliminate the possibility of impurities and allergic reactions related to latex allergies. Warmed gutta-percha delivered on a core focused on the need for better methods of easily and predictably obturating and sealing the canal.22 Resin-bonded materials were brought to market in hopes of creating a better seal and (potentially) strength-ening the root canal system by taking advantage of the bonding capacity of the newer restorative materials and techniques that were being used in the coronal portion of the tooth.42
Yet as we enter the second decade of the 21st century, gutta-percha still dominates. The gutta-percha cones that have been available for decades and gutta-percha on core carriers that have been used extensively over the past 20-plus years are still the filling material of choice globally—used, of course, with some type or root canal sealer or cement and compacted into the prepared root canal space.
When all the more recent developments in root canal obturation materials and techniques are considered, there appear to be recurring themes that beg Dr. Postman’s question: What is the problem to which this technology is the solution? The list includes developing ways to manage the intricacies of the root canal system, ensuring complete obturation, sealing the canal system, providing a radiographic appearance of the filled root that signifies to the clinician they have achieved their goal (and, of course, provided that needed signature of expertise), and strengthening the root canal to prevent potential fracture during function (see Chapter 20). A missing link in these themes only came into the clinician’s hands in the middle to late 1990s: new tools (nickel-titanium instruments; see Chapter 10) necessary to prepare the root canal system for proper obturation.
Root Canal Sealers: Their Role and Use
A root canal sealer or cement is essential with any gutta-percha technique, just as an etching agent and bonding mate-rial are required when using resin-filling techniques.15,46 These products serve many functions, such as being a lubri-cant to facilitate obturation and adhesiveness to enhance the seal and stability of the root canal filling. When mixed prop-erly, they can be elevated from a mixing slab approximately 1 inch (2.54 cm) and held there for 5 to 10 seconds without flowing off the elevating instrument (Fig. 12-1). The sealer will flow into the dentinal tubules if the smear layer has been removed,6,13,15,23 depending on the obturation technique used,6 (Fig. 12-2; also see Chapter 11) and may be expressed through lateral or accessory canals (Fig. 12-3).
FIGURE 12-1 Properly mixed sealer can be strung out at least 1 inch.

220 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
FIGURE 12-2 Sealer penetration into the dentinal tubules (Rhodamine B dye). (Courtesy Ronald Ordinola-Zapata, São Paulo, Brazil.)
BA
FIGURE 12-3 A, Sealer penetrating into dentinal tubules and accessory communications in a tooth that has been demineralized and cleared for visualization. B, Mandibular molar showing the movement of root canal sealer into accessory communication into the furcation.
FIGURE 12-4 Photomicrograph showing chronic inflammation surrounding the extrusion of root canal sealer beyond the root canal (H&E ×10).

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 221
A B
FIGURE 12-5 A, Obturated mandibular premolar that exhibits multiple accessory communications and extrusion of sealer. B, Six-month reexamination shows what most clinicians would consider as healing; however, healing cannot occur with the presence of the irritating sealer that contributes to long-term chronic inflammation.
Gutta-Percha Obturation Techniques
Popular methods of canal obturation are lateral compaction, vertical compaction, thermoplasticized gutta-percha injec-tion techniques, and thermoplasticized core-filler tech-niques.15,46 Although other variations on these themes exist, such as thermatically executed lateral compaction and ther-momechanical compaction, specific problems occur with these techniques, and their overall popularity at present is variable. Similarly, problem solving the standard techniques should aid in the execution of these alternative approaches to gutta-percha compaction. A brief synopsis of each technique is provided in the following text; however, the reader is encouraged to seek complete descriptions of each technique in the references cited and in other “how-to-do-it” endodon-tic textbooks. Each technique presumes proper canal prepara-tion prior to commencing obturation. For the first two techniques and any technique that requires the use of a master cone, a gauge is available to assist in choosing a master cone with the proper diameter and length to match the canal preparation size and shape (Fig. 12-6).
Lateral CompactionA spreader that reaches the working length or within 0.5 mm is chosen and fitted in the canal (Fig. 12-7, A).15,31,46 A stan-dard or variably sized gutta-percha cone (master cone taper .02, .04, .06, .08) is chosen to correspond to the final size of the last K-file to the apex (master apical file; see Fig. 12-7,
B). The cone is fitted to the working length with close adap-tation in the apical 1 to 3 mm (snugness of fit, or tugback); A radiograph is obtained to verify the position of the master cone. Subsequently, the master cone is coated with a root canal sealer in the apical half and seated to the working length in the canal (see Fig. 12-7, B). A metal root canal spreader is placed beside the master cone, compacting the cone apically and laterally and at the same time creating space adjacent to the master cone (see Fig. 12-7, C ). A smaller, nonstandard-ized accessory cone is placed in the void created by the spreader (see Fig. 12-7, D). The spreader is reinserted and the second cone is compacted (see Fig. 12-7, E ). This pro-cedure is continued until the spreader cannot penetrate into the apical two-thirds of the canal (see Fig. 12-7, F ). The excess coronal gutta-percha is seared off at the orifice, and the coronally softened gutta-percha is compacted apically with a large plugger. The adaptation of the master cone api-cally should be noted when the spreader can be placed to the working length (see Fig. 12-7, G and H ). Compaction per-formed in this manner results in well-filled root canals (see Fig. 12-7, I ) even in long, narrow, or curved canals and the filling of accessory communications (Figs. 12-8 and 12-9). Variations on this approach include softening the master cone with solvents such as chloroform to achieve a better adaptation to the intricacies of the apical portion of the canal.
If the shape of the canal is developed with a hand instru-ment, the taper usually closely corresponds to a cone that is .02 or slightly larger. Cleaning and shaping is often accom-plished using the step-back technique or variation thereof. A .02 master cone is chosen for obturation that provides suf-ficient taper or space lateral to the master cone for root canal

222 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
BA C D
E F G H
I
FIGURE 12-7 A, Fit of the spreader is visualized to the working length in a prepared canal. B, Fitting of the master cone to the working length. C, The spreader is placed alongside the master cone to length to compact the apical portion of the cone and seal the canal. D and E, Adding additional cones are followed by compaction apically and laterally. F, Finished compaction. G and H, Adapting the master cone to the root canal walls and apical preparation when the spreader is placed to the working length during lateral compaction. Failure results in a single uncompacted master cone in a sea of cement—an invitation to failure! I, Mandibular molar shows well-adapted and laterally compacted gutta-percha fillings.
A
B
FIGURE 12-6 A and B, Measuring gauge is shown for both length and apical sizing. (Courtesy Dentsply Maillefer, www.maillefer.com.)

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 223
• The cone must fit to the prepared length with snugness of fit or tugback.
• Space exists laterally to the cone for the fit of the spreader during compaction.
• Accessory cones must be slightly smaller or basically equal to the size of the spreader (Fig. 12-10, A).
• The spreader must reach to within 0.5 to 1 mm of the working length without binding in the canal1 (see Fig. 12-10, B-D ). If binding should occur, there is a chance for tooth fracture with excessive pressures32 (Fig. 12-11).
• The sealer and core material (with the spreader) are adapted into the prepared apical third of the canal.
sealer and placement of the spreader to within 1 mm or less of the working length.
If the shape is developed with a rotary instrument at larger taper sizes (.04, .06), the chosen master cone corresponds to the last instrument placed to the working length. The size of the cone may have a specific taper, or it may be a nonstan-dardized cone (e.g., fine-medium, medium) cut to fit the taper and length of the prepared canal. These cones can be cut to fit into the apically prepared space more accurately using a metallic standardized gauge (see Fig. 12-6). With ALL techniques of canal preparation and choice of lateral compaction:
FIGURE 12-8 Obturation of a mandibular molar with long, curved canals. (Courtesy Dr. David P. Rossiter III.)
FIGURE 12-9 Mandibular molar is obturated using the lateral compaction technique; note lateral canal in the distal root. (Courtesy Dr. David Stamos.)
CLINICAL PROBLEMProblem: At the point of cone selection, it appears that there is insufficient room for the spreader to extend to the proper depth as described in the preceding section.
Solutions: The interrelationship between the shape of the canal and the technique for obturation cannot be overempha-sized. Furthermore, the understanding of the balance between preparation and obturation varies from person to person. It involves such subjective aspects as experience, the “feel” of the canal shape, the “feel” of the cone fit and the “fit” of the spreader. There are a number of objective remedies if there are problems with the fitting of master cone or the fitting of the spreader. For most clinicians, the majority of the problems seem to occur in the mid-root areas. Usually, there is insuffi-cient enlargement of the canal space, but there may be other contributing factors.
To address this issue, there are a number of effective remedies:
• The orifice can be further enlarged with orifice wideners, Gates Glidden drills or Peeso reamers.
• The canal can be reshaped by hand with larger file sizes in a step-back manner principally in the middle and coronal thirds.
• If rotary instruments are in use, the canal can be reshaped with the same rotary instruments applying more lateral pressure to “plane” the canal walls.
• The canal can be reshaped with rotary instruments having a greater taper.
• If .06 tapered gutta-percha cones are being used, a .04 or .02 tapered gutta-percha cone of identical apical size could be used. It is generally unwise to choose a smaller apical size gutta-percha cone as it will not provide an adequate filling of the apical portion of the canal.
• Try different brands of gutta-percha products as the sizing varies somewhat among manufacturers.
• Choose a spreader of smaller diameter and taper. Spreaders are available in many sizes.
Some of these concepts will be revisited in greater detail later in this chapter in the discussion of obturation problem areas in general.

224 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
Vertical CompactionA nonstandardized master gutta-percha cone (master cone taper .02, .04, .06, .08) is chosen to ensure that it has a slightly smaller taper than the prepared root canal space (Fig. 12-12, A.15,46 The cone is fitted snugly 1 to 2 mm from the prepared apical constriction. Root canal pluggers are also prefitted to ensure depth of penetration into the apical third of the canal without binding on the canal walls. A light coating of root canal sealer is placed on the apical half of the master cone, which is then seated in the canal short of the apical constriction. A heated instrument is used to sear off and remove coronal segments of gutta-percha and transfer heat to the remaining portion of the master cone (see Fig. 12-12, B). A cold vertical plugger is used to compact the softened portion of the cone apically and laterally (see Fig. 12-12, C). This process of heating, removing, and compact-ing (see Fig.12-12, D and E) is continued until softened gutta-percha is delivered into the apical 1 to 2 mm of the prepared apex (see Fig. 12-12, F ). Subsequently, softened segments are added and compacted to obturate the canal from the apical segment to the canal orifice see Fig. 12-12, G). Figure 12-13 illustrates the clinical application of this technique.
With ALL techniques of canal preparation and choice of vertical compaction for obturation:
• Canal tapers should be .04 or larger. In these cases, selection of a corresponding master cone with the same taper and apical size is routine.
• If a nonstandardized cone (e.g., fine-medium, medium) is selected, it must be cut to the appropriate apical size and have a taper that allows it to penetrate to within 0.5 to 1 mm of the length of the prepared canal (see Fig. 12-6). The vertical compaction process will move the cone apically into the prepared canal.
• With canal preparation using NiTi rotary instruments, the taper will also be variable and may even be greater
A
B
RT
C
D
FIGURE 12-10 A, Accessory gutta-percha and resin-bonded accessory cones are chosen based on the size of the compacting instrument. The cones should be slightly smaller. B, Spreader inserted into a root canal only reached to the position of the arrow, far short of the ideal length (RT). Note there is no compaction of the gutta-percha apical to the arrow. C, Spreader reaches to the desired length at the extent of the master cone. D, Spreader reaching the reference point for the working length adjacent to the master cone in a molar tooth.
FIGURE 12-11 Excessive use of apical compaction with a large spreader resulted in a root fracture.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 225
A needle or applicator tip designed to deliver the softened gutta-percha is introduced into the canal to the junction of the middle and apical thirds, with care taken to ensure that the needle does not bind against the canal walls (Fig. 12-14, A). The gutta-percha is passively injected into the root canal system, avoiding apical pressure on the needle (see Fig. 12-14, B). In 5 to 10 seconds, the softened material will fill the apical segment and begin to lift the needle out of the tooth. During this lifting by the softened, flowing mass, the middle and coronal portions of the canal are continuously filled until the needle reaches the canal orifice. Compaction of the material follows to adapt the gutta-percha to the prepared canal walls (see Fig. 12-14, C ). With some techniques, compaction is optional, depending on the type of gutta-percha used, because the softened material flows into the canal preparation. If necessary, additional amounts of gutta-percha can be easily injected into the canal to achieve complete obturation. Another option is to deposit a small amount apically, fol-lowed by compaction to ensure an apical seal (see Fig. 12-14, D). Additional material is then placed in the canal with the delivery device to complete the obturation (Fig. 12-15). With ALL techniques of canal preparation and choice of injection techniques and compaction:
than the size of the instrument. In these cases, selection of a nonstandardized cone may be indicated. Nonstandardized cones can be cut to fit more accurately into the apically prepared space using a metallic standardized gauge (see Fig. 12-6).
• The cone must fit to the appropriate length with snugness of fit or tugback.
• Pluggers (compactors) must be prefit to within 3 to 5 mm from the working length without binding.
• Sufficient space must exist for the plugger to move apically to the desired depth without binding between the dentin walls during compaction.
Thermoplasticized Injection TechniquesGutta-percha may be softened and delivered to the prepared canal using a variety of instruments designed for injection that permits compaction (Calamus Flow, Calamus Dual 3D obturation system [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]; BeeFill 2in1 [VDW, Munich, Germany]; Ele-ments Obturation Unit [SybronEndo, Orange, CA, USA]; E&Q Master [Meta Dental Co., Elmhurst, NY, USA]).15,46
A B C D
E F G
FIGURE 12-12 A, The master cone is fitted for vertical compaction. B, Heated instrument is used to sever the coronal portion of the canal and add heat to the cone. C, Initial compaction. D, Segments are removed with a heated instrument, followed by compaction. E, Once the apical extent of compaction is reached (F), heated segments are placed in the canal and compacted (G).

226 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
depending on the canal shape and size. Needles are usually available in 20, 23, and 25 gauges, depending on the unit chosen.
• Delivery needles or tips must not bind in the canal. The tip is placed to the point of binding and retracted
• Tapers above a .04 using NiTi rotary instruments are recommended because the taper produced is essential for the flow and compaction of the softened material.
• Delivery needles or tips must reach to within 3 to 5 mm of the prepared apical terminus of the canal,
A B C D
FIGURE 12-14 A, Injection needle is fitted for the thermoplasticized gutta-percha. B, The process for injecting the gutta-percha can stop with an apical plug, followed by compaction (C), or the entire canal can be filled, followed by compaction (D).
A B
C D
FIGURE 12-13 A to D, Examples of well-shaped and well-obturated canals that were achieved by using NiTi rotary instruments to ensure proper enlarging and shaping. Note the tapers and shapes of the canals. Excessive removal of root dentin was not necessary to achieve these goals.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 227
Intracanal vertical compaction of the softened material around the core is recommended. Once complete, the core is cut off with a bur at the orifice (see Fig. 12-16, D). Labora-tory evaluations of these techniques demonstrate well-filled canals with three-dimensional adaptation of the gutta-percha to the intricacies of the canal (Fig. 12-17).
Modifications and combinations of these techniques yield numerous possible ways to obturate the prepared root canal space. For example, recent attempts to enhance the adapta-tion of the gutta-percha delivered in the thermoplasticized state to the intricacies of the canal walls have shown an intimate adaptation and penetration into the dentinal tubules when the smear layer is removed (Fig. 12-18, A-D). This technique has shown excellent adaptation, especially in complex canal systems (oval canals, C-shaped canals), but additional compaction may be a necessary part of the filling technique in demanding situations (see Fig. 12-18, E and F ).30
A concern on the part of many clinicians is the potential need for removal of this core material for post space or if there is a treatment failure (see Chapters 5 and 14). Fortu-nately, many techniques provide for simple, efficacious removal. To address this issue, Dentsply, the prime manu-facturer of the core-carrier product and technique will intro-duce a new product with a complete gutta-percha core: Gutta-Core (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA). The availability of this new delivery device and its achievements will surpass those of previous core-carrier mate-rials in ease of usage, adaptation to the properly prepared canal, and elimination of any concerns for post space prepara-tion or canal revision, inasmuch as the material is easily removed (Fig. 12-19).
1 mm. This placement creates a space for flow of the material apically while allowing trapped air to escape coronally. The material is injected without pressure on the needle or attached apparatus. When the material is felt to push coronally on the needle, the needle is allowed to be moved passively or lifted from the canal coronally by the movement of the softened filling material. As an alternative, injection can be stopped at any point with subsequent compaction, followed by the injection of additional segments of filling material. Many clinicians who use this technology are referred to as “squirters,” and often incremental applications are chosen to ensure thorough compaction of the filling material at every position in the canal.
Thermoplasticized Core- Carrier TechniquesGutta-percha that has been previously coated on a metallic or plastic core (carrier), corresponding to standardized instru-ment sizes, is heated in a preset system or oven.15,46 (Note: The vast majority of core carriers today are plastic: Therma-Fil, GT, and ProTaper & Vortex gutta-percha carriers [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]; Soft Core [CMS Dental ApS, Copenhagen, Denmark].) After proper softening in a standardized heating oven, the coated gutta-percha core is placed to the working length, with the harder central core used as a compactor to carry the softened material apically and laterally (Fig. 12-16, A-C). Root canal sealer is an intimate and essential part of this system.
BA
FIGURE 12-15 A, Maxillary premolar obturated only with the injection method. The canal shape is essential for this achievement. B, Mandibular molar obturated with the injection technique.

228 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
CA
CCLC
B
CCLC
FIGURE 12-17 A and B, Two examples of the mesial roots of mandibular molars are turned to view them proximally. The canals are filled using either lateral compaction with gutta-percha or the thermoplasticized core-carrier technique. Teeth are placed in India ink dye then demineralized and cleared to be able to see the canal anatomy and adaptation of the filling material with both techniques. Each specimen is labeled as to lateral compaction (LC) or core carrier (CC). The core-carrier technique provides better movement of both gutta-percha and sealer into the canal irregularities than does the lateral compaction technique. A, Distinguishing which canal is filled with which technique is difficult, emphasizing the importance of canal cleaning and shaping. C, Clinical case is filled with the core-carrier technique.
A B C D
FIGURE 12-16 A, Heated core carrier is carried to the cleaned and shaped canal and delivered slowly (B and C), avoiding any coronal movement or rotation of the carrier. D, Carrier is stabilized and cut off with a bur or instrument designed for this purpose.

A B
C
D E
F
FIGURE 12-18 A, Fields of gutta-percha plugs penetrate the dentinal tubules after the smear layer is removed (see Chapter 11) (scanning electron micrograph [SEM] ×66). B, Gutta-percha plugs are placed in the tubules with sealer, giving them a carpeted or matted appearance (SEM ×720). C, Tips of the gutta-percha plugs display sealer particles (SEM ×2000). D, Cleared tooth specimen shows the penetration of both sealer and gutta-percha plugs into the tubules. E, After placing a core carrier, a lateral or vertical compacting instrument can be used to compact, followed by additional gutta-percha placement via cones and small gutta-percha segments or injection. F, After placement of a core carrier with gutta-percha, four additional cones are placed (arrows) and compacted. This technique works well in irregularly shaped canals (canals that are wide buccal lingually and C-shaped canals) when multiple core carriers cannot be used.
BA
FIGURE 12-19 A, New Gutta-Core core carriers that do not contain plastic or metal. B, Example on extracted tooth of the appearance and quality of canals filled with this technique.

230 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
being used.20,38-41 Fourth, while these same, previous concerns apply to the Activ GP monocone obturation, there are no evidenced-based data that support single-cone obura-tion,9,26,27 regardless of the sealer and manufacturer claims.
Even with the advent of these newer materials, the obtura-tion process itself has not really changed, and any of the techniques of canal filling can be used. This is especially important when the canal anatomy prior to enlarging and shaping and subsequent to this process is taken into consid-eration. The technique must use methods or variations that will ensure movement of the filling materials into all aspects of the prepared root canal anatomy.30
Conceptually, however, a resin-bonded root canal filling material would be the ideal future of obturation in endodon-tics. Presently, many clinicians have adopted these new tech-nologies with empirical claims of success being made globally (Fig. 12-20)4 (www.resilonresearch.com). However, great care must enter into the development and evaluation of these types of materials before and during widespread patient use.39 In this light, the operative term is evidence-based, that is, the need for long-term, prospective, randomized clinical trials to ensure that years from now, the dental clinician will be faced with tooth retention in symptom-free function and not with the ravages of periapical periodontitis and the need for treat-ment revision.
Guiding Principles for All Obturation Techniques
1. The success of any root canal obturation technique depends largely on the care exercised in canal preparation. Presently, with the newer NiTi rotary canal enlarging and shaping techniques, the final shape will enhance obturation no matter what technique is chosen.
2. Canals should be prepared with a definite apical matrix (seat, stop, or constriction in sound dentin) to retain
Resin-Bonded Obturation Techniques
The development of resin-bonded adhesive root canal filling materials naturally evolved from the need to more effectively seal the root canal apically and coronally. Successes with resin-bonded materials in the coronal portion of the tooth inspired this obturation innovation.42,44 Important in this respect were the needs for a material that (1) would be fully biocompatible, (2) would not deteriorate over time, (3) would seal all communications against the commonly found organisms in the root canal and oral cavity, and (4) could be easily placed into the canal and create a bond with the organic and inorganic components of dentin.
Multiple systems with this approach have appeared: Epiphany Soft Resin and Epiphany SE Self-Etching, in both cones and pellets for obturation (Pentron Technologies LLC, Wallingford, CT, USA); RealSeal, RealSeal 1 Bonded Obtu-rator, and RealSeal Sealer (SybronEndo, Orange, CA, USA); Activ GP Monobloc Obturation and Activ GP Glass Ionomer Sealer (Brasseler USA, Savannah, GA).
These systems require the use of smear layer removal agents, such as 15% to 17% ethylenediamine tetraacetic acid (EDTA), to enable movement of the primer and sealer into the dentinal tubules (see Chapter 11). The materials are highly radiopaque and compact well into the prepared root canal, using cold lateral or warm vertical compaction. The availability of self-etching is claimed to enhance the product and process. Chemically, the main component is a polyester (polycaprolactone) that contains embedded bioactive glass and calcium hydroxide. The Activ points (which do not contain polycaprolactone) actually have the glass ionomer embedded on the points and in the sealer. If the polycapro-lactone undergoes degradation, the manufacturer claims the bioactive glass component initiates an inductive response for bone or cementum formation.
This new technology’s major claims focus on its ability to produce a monoblock (and therefore a better seal of the root canal)35,42 and its ability to strengthen the root.43 In light of these claims, some very important observations must be made in a problem-solving format. First, for monoblock to be achievable, root dentin must be completely free of debris and bacteria.38 To date, this level of cleaning and disinfection is not achievable on a predictable basis, although technologic advances are reaching for this goal (see Chapter 11). Second, strengthening the root system has had serious challenges,8,11,18,47 because if monoblock is not achieved, strengthening cannot be achieved. Some have claimed greater strengthening compared to gutta-percha and sealer, but this may merely be a measure of the adherence of the sealer used with the gutta-percha.36 In fact, there are sealer/gutta-percha combinations that appear stronger than Resilon45 and positive long-term findings when it comes to leakage.48 Additional concerns center on the potential shrinkage polym-erization that may occur in the root.2,24 Third, there are substantial claims as to the degradation of the materials
FIGURE 12-20 Mandibular molar obturated with resin-bonded root filling materials.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 231
the canal short of the full working length, three issues are potentially at work and must be considered:
• The shape of the canal is improper for the cone chosen.
• The wrong cone is chosen.• Debris is packed in the canal.
To problem solve these issues, the following steps are recommended:
1. Cone size and shape should be checked and compared with the master apical file.
2. Recapitulation should be performed with the last K-file or size verified in the case of a core-carrier. All files should be curved as appropriate for the canal shape.
3. Radiographs should be obtained to verify that the working length is correct and that no ledges, blockages, or false canals have been created. However, these errors should have been seen much earlier by the cognizant, problem-solving clinician.
4. If necessary, the same-sized Hedström file as the master apical file or the final rotary NiTi should be used, and the canal walls should be carefully shaved in a step-back circumferential fashion. This step may permit selective shaping in specific canal areas. The goal is not to enlarge but shape.
5. Copious irrigation should be used to enhance instrumentation and dentin chip removal.
6. After reestablishing length with the file and drying the canal with paper points, recapitulation should be performed once more to remove any dry-packed chips from the apical dentin matrix (Fig. 12-21).
the filling material within the canal space. This is key from both a biological and clinical perspective.14
3. Regardless of the type of gutta-percha filling or the nature of the resin material that is chosen, compaction to some degree is indicated. This enables the clinician to address the significant and widespread nature of root canal irregularities.
4. A complete and appropriate armamentarium to accomplish the chosen technique must be readily available. Clinicians must be prepared to learn the techniques well and have necessary instruments to manage the specific canal anatomy of each tooth (e.g., large canals, curved canals, C-shaped canals, canals with resorptive defects, etc.).
5. Obturation techniques may have to be modified to meet the needs of an individual case. Multiple techniques are often required to properly obturate a single canal because anatomic challenges dictate the need to practice problem solving during this phase of treatment. Most important may be the fact that no one technique can manage all cases.
Problems Preparing to Obturate the Canal
The main problems encountered when preparing to obturate are a blocked or ledged canal, debris present apically, or a separated instrument in the canal. When NiTi instruments are applied properly, along with the advocated irrigation techniques, these problems do not occur. Should they occur, this area of concern tends to show itself when trying to fit a master cone for any technique. When a master cone binds in
A B C
FIGURE 12-21 A, Master cone fits short of working length on a model because of canal blockage with dentin chips. B and C, After recapitulation, chip removal, and confirmation of working length, the master cone is fitted to the correct length.

232 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
A B
FIGURE 12-22 A, Gutta-percha is cut with a sharp scalpel to avoid irregularities. B, Gutta-percha master cones are cut with a scalpel (left) and scissors (right). Flanges are noted on right cone.
A B
FIGURE 12-23 A, A gutta-percha solvent used for 1 to 3 seconds softens the surface of the cone without distorting the strength of the cone in its long axis, which is needed for firm placement into the canal. B, Upon placement, the cone will become adapted to the walls of the canal to enhance the fit (arrows). This process can be repeated until the cone reaches the desired depth and snugness of fit.
7. If the master cone does not snugly fit to the appropriate length, a different-sized cone can be chosen and adapted by cutting the cone based on the taper and the final instrument size. For example, enlarging with NiTi rotary instruments often produces a canal that is larger than the instrument. If the size were a No. 30, .06, the master cone would be a matching size. If it goes all the way to the working length, but is loose, by cutting off (Fig. 12-22) a half millimeter, the cone will be a No. 33. If the No. 33 does not go all the way, a 1- to 3-second apical chloroform dip (Fig. 12-23, A) will permit good adaptation to the apical portion of the canal. Another example: Presume the canal is prepared to an F3 ProTaper instrument (No. 30, .09), but the cone does not go all the way to the working length. Consider taking an F2 cone (No.
25, .08) and cutting off half a millimeter, which prepares a cone to an approximate size 29. Additional cutting or molding with chloroform in a creative and knowledgeable manner will enable custom preparation with any gutta-percha or resin-based cone. The gauge seen in Fig. 12-6 is most helpful for this process.
Problems During Canal Obturation
The main problems encountered during obturation focus on the inability to place the compacting instrument to the desired length, or pulling the material out of the canal with the compactor. Failure to place the compacting instru-ment occurs mainly because of lack of proper canal shape

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 233
• Is the compactor clean? Is there tacky sealer on the instrument before reinserting?
• Is the integrity of the compactor compromised by having bends, hooks, or irregularities at its tip?
• Is there moisture in the canal (blood, pus, or saliva)?• Was the master cone too small?• Was the compactor loosened before withdrawal from
the canal?• Was the compactor, if precurved, rotated in a curve
canal?• Was a separating medium, such as alcohol, used on
the compactor?
Answers to these questions can only be provided when the clinician reassesses all aspects of a specific case. The following general guidelines may help in problem solving these queries. As previously discussed, a customized cone adapted to the apical 1 to 3 mm by means of a solvent or heat may be neces-sary if the walls are too divergent. This will create a better snugness of fit that will resist displacement during compac-tion. The moderate use of sealer is always recommended to provide a seal between the interface of gutta-percha and dentin. All compaction techniques when done properly in an ideally shaped canal will move the sealer laterally and apically into a thin layer along the dentin and into the dentinal tubules when the smear layer has been removed. To achieve good compaction with a spreader, it must be clean each time it is introduced into the canal. Often the clinician will have the assistant wipe the spreader, but if it is wiped in a straight motion, sealer will remain; wiping in a circular motion will remove the sealer thoroughly. Furthermore, there can be no irregularities in the shape of the spreader—that is, no flanges, hooks, or severe kinks in the instrument (Fig. 12-24). Too often these instruments are used for tasks for which they were not intended (e.g., searching for canals, trying to remove old filling materials), and they get these irregularities.
Root canals must always be dry before compaction. It may be necessary to dehydrate the root canal before obturation. Sterile paper points are the best devices for moisture removal. If necessary, the canal may be irrigated with 2 to 3 mL of either 70% or 95% isopropyl alcohol. The alcohol should be allowed
and taper, use of inappropriate (too large) compacting instruments, or use of a straight, inflexible compacting instrument in a curved canal.
These problems can all be prevented by fitting the com-pacting instruments in the canal before obturation to deter-mine their degree of adaptation. NiTi compacting instruments are also available for curved canals if necessary,3 although most compactors can be curved if carefully bent with a pair of hemostats.
Instruments that have a taper similar to that of the pre-pared canal should always be used. For example, not all D-11T spreaders have the same thickness and tapered shape because differences exist among the various manufacturers. In smaller-prepared canals, such as a size 25 to 35 at the apical extent, a D-11TS spreader is appropriate. In larger canals, a D-11T will work. In long canals (i.e., greater than 23 mm), these spreaders will not work. In these cases a GP-3 is used. Finger spreaders and hand spreaders are also available in NiTi alloy.3 Compared with stainless steel spreaders, these highly flexible compactors can more easily negotiate properly shaped curved canals; this negotiation is essential for ade-quate apical compaction. In addition, no precurving is neces-sary, and recent research suggests that decreased stress on root structure when compacting with NiTi finger spreaders exists, thus potentially decreasing the chance of vertical root frac-ture. Potential disadvantages of using these compactors include buckling the instrument during compaction and a limited accessibility to some canals because the spreader cannot be precurved. Present findings indicate that the flex-ible NiTi finger spreaders should be used to compact the gutta-percha in the apical third, followed by stiffer stainless steel finger spreaders to compact the gutta-percha in the remaining coronal two-thirds. Using stainless steel finger spreaders in the more flared portion of the canal may com-pensate for the buckling that would occur if NiTi compactors were used for the entire obturation procedure.
Compactors (pluggers) also vary in shape and taper, and they should be selected based on their adaptation within the tapered canal preparation. They are available to fit the specifi-cally tapered root canal files. When a canal is obturated with the injectable thermoplasticized gutta-percha techniques, similar solutions as previously mentioned are recommended. However, vertical compactors do not have to fit to within 1 to 2 mm from the apical dentin matrix. Compactors are loosely fit only to within 3 to 5 mm from the apical dentin matrix or constriction. Similarly, the shape and flow of the canal in this area must be a smooth, continuously tapering funnel. With core-carrier techniques, seating the core to the depth of the prepared canal is very important.
If the compacting instrument, spreader, or plugger is pulling the master cone or accessory cones out of the canal, the following problem-solving questions should be considered.
• Is there too much canal wall divergence and lack of a snugly fitted master gutta-percha master cone?
• Has too much sealer been used? Is the sealer mix too thin?
FIGURE 12-24 Various spreaders are shown with less than ideal tips. Placement of these into canals is a recipe for problems.

234 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
filling material extrudes beyond the confines of the canal (Fig. 12-26). However, an overextended root filling is solely limited to the vertical dimension of the root canal filling material, relative to the apical foramen. An overextended fill does not imply that the root canal has been three-dimension-ally obturated. Rather, the implication is that the filling mate-rial has been placed beyond the confines of the canal but has not necessarily sealed the apical foramen (Fig. 12-27). Addi-tionally, if placed in areas where vital structures are located, such as the inferior alveolar canal or mental foramen, there is a greater potential for serious complications.12
An additional problem that may arise with core-carrier filling is the stripping of the gutta-percha from the core. This may be seen on a posttreatment radiograph and is usually due to improper canal shaping, as seen in Fig. 12-28. Note the core is exposed in the middle to apical third (arrows) because the shape of the canal narrows too rapidly, and there is no gradual and continuous funnel shape to the canal.
Major causes of placing the root canal filling material beyond the apical constriction in either overfilling or overex-tending when lateral or vertical compaction techniques are used are due to the following errors:
• Excessive instrumentation beyond the apical constriction, resulting in the lack of an apical dentin matrix
• Unanticipated communicating resorptive defects anywhere in the canal system
• Defects incorporated into the canal system during cleaning and shaping, such as zips, perforations, and strips (see Chapter 10)
• Excessive compaction force or excessive amounts of sealer; often occurs with the core-carrier technique when placed too rapidly and with too much pressure
• Use of a too-small master cone that allows for excessive penetration of the compacting instrument
• Any combination of these errors
The intentional placement of gutta-percha beyond the confines of the root canal system is not considered an accept-able technique because no long-term prospective or retro-spective studies exist to justify this approach to canal obturation. Many techniques used in canal obturation are predisposed to this possibility, and their use should be modi-fied to produce predictable control of the obturating material when possible. In fact, going beyond the apical foramen, other than to establish apical drainage,10 may not be war-ranted; pushing materials past may only hinder periapical healing5,25,37 and create problems for the patient that may not be immediately evident.
Although proper techniques have been followed, occasion-ally gutta-percha, resin-bonded filling materials, or root canal sealer may be unintentionally pushed beyond the confines of the root canal system. However, the periradicular tissues generally tolerate these materials. Although sealers may provoke an initial inflammatory response to a greater or lesser degree over a short period, the macrophage scavenger system eliminates the excessive material from the periradicular
to remain in the canal for 3 to 4 minutes and then dried with sterile paper points. Rarely is this technique indicated.
In some cases, a larger or more appropriately tapered master cone must be selected before compaction. Properly fit master cones will penetrate to within 0.5 mm of the working length, and space is found on either side of the cone from the junction of the apical and middle thirds to the coronal orifice. When placing the compacting instrument, it should be rotated in a 180-degree curve until it becomes loose within the canal (Fig. 12-25). A retracting force can be gradually applied during this movement to allow the spreader to pas-sively “walk” out of the canal without dislodging the com-pacted gutta-percha. However, if the canal is curved and the spreader is curved, then rotation will have to be limited to approximately 90 degrees while the clinician exerts a continu-ous coronal retracting force.
If the core-carrier technique is being used and a problem arises, the issue that may need to be addressed is:
• During the cutting of the core (metallic carrier with a bur or plastic carrier with a bur or a controlled heat source), was the handle of the core stabilized to prevent removal of the core (carrier)? (See Fig. 12-16, D). Even if not removed, failure to stabilize the top of the core may significantly disrupt the previously placed gutta-percha.
All the problems encountered during canal obturation can be prevented with careful attention to detail in canal preparation and during obturation. The operative word is prevention.
Problems Identified After Obturation
The major problems identified after obturation include over-filling, overextension, underfilling or lack of apical density, and voids in the filling.12 Overfilling implies that a root canal system has been filled in three dimensions, and a surplus of
A B
FIGURE 12-25 A, Rotating the spreader in a 180-degree arc will loosen the instrument in the canal without dislodging the filling material. B, During rotation, force is gradually exerted in a coronal direction to allow passive removal of the spreader.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 235
BB
A
C
FIGURE 12-26 A, Maxillary lateral incisor with lesion many clinicians would claim is a cyst. Invariably, teeth with lesions have some degree of apical root resorption. B, Overfilled root canal. Material extends as much as 2 to 3 mm beyond the apical foramen, which is not at the end of the root (arrow indicates probable foramen, and red line indicates possible extent of overfill). C, Twelve-month reexamination shows excellent healing. (Case courtesy Dr. Paul Buxt.)
FIGURE 12-27 Significant filling material is pushed past the end of the root. In many such cases, a long-term chronic inflammatory problem occurs, so the case must be periodically reassessed.
FIGURE 12-28 Canals are filled with the core-carrier technique. Although obturation appears good, improper canal shaping has resulted in stripping of the gutta-percha from the core (arrows).

236 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
vertical compaction or an injectable thermoplasticized gutta-percha technique, retraction of the filling material through the apical foramen is impossible. Although some authors may cite this situation as an indication for periradicular surgery, the routine and immediate use of surgical intervention is neither indicated nor justified (see Fig. 12-26). In most cases, the periradicular tissues will heal, and the patient will be symptom free. If, however, the patient exhibits signs or symp-toms of periradicular inflammation, surgery may be indi-cated. In cases of thermoplastic core-carrier overextension, removing the core from its overextended position is neces-sary. Concomitantly, retrieving small amounts of gutta-per-cha from beyond the confines of the apical matrix may be possible if they remain attached to the core.
Failure to achieve adequate apical density is a common problem in root canal obturation that only too often goes unnoticed by the undiscerning clinician (Fig. 12-29). In
tissues. In any case, the mere placement of filling material outside the canal system is not a major cause for alarm if the canal space is three-dimensionally obturated. If excessive amounts of materials are extruded, the patient should be informed, and periodic reexaminations are indicated. In cases of overextension with the lateral compaction technique, the filling material can often be teased back through the foramen, provided the sealer has not hardened. If the sealer has hard-ened, it may still be possible to retrieve the gutta-percha, provided it is an intact cone. The gutta-percha is softened with one of the previously mentioned solvents in the apical third of the canal. While the gutta-percha is soft, a Hedström file is inserted into the softened mass, and excess solvent is flushed from the root canal. In a few minutes, the gutta-percha will harden around the Hedström file. The file is carefully teased out of the canal as parallel as possible to the long axis of the canal. In cases of overextension with the
A B
C D
FIGURE 12-29 A, Apical half of these canals is insufficiently shaped to allow for thorough compaction of filling material. Excessive use of Gates-Glidden burs is noted in the coronal portion of the root canal. B, These canals are obturated with a single-cone filling in the apical half of the canal, whereas the coronal half is weakened by excessive removal of dentin with Gates-Glidden burs. C and D, Two cases of obviously less-than-ideal compaction are visualized as lack of apical density in root canal fillings. Each of these scenarios is preventable. In all four cases, apical lesions are present, and to be retained, teeth will require treatment revision.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 237
essence, the apical third of the canal is filled with a sea of root canal cement and a single uncompacted master cone or a poorly condensed mass of previously softened gutta-percha. Radiographically, the apical third of the canal appears less radiodense (Fig. 12-30). An ill-defined outline to the canal wall is evident, along with obvious gaps or voids in the filling material or its adaptation to the confines of the canal. This problem is more evident when minimally radiodense sealers are used. Some clinicians avoid this perception by using highly radiodense sealers. Similarly, resin-bonded filling materials, both core and sealer, are highly radiodense; this problem may be evident with their use. Contributing factors to this problem include:
• Lack of canal patency inside the root and sufficient taper to allow for spreader penetration to the apical seat in the lateral-compaction technique, plugger penetration in the vertical compaction technique, and the flow of gutta-percha in thermoplasticized gutta-percha injection and core-carrier techniques (In particular, this lack of proper shape and taper will
accentuate the wiping or removal of the gutta-percha from the carriers in the thermoplasticized core-carrier techniques [see Fig. 12-28].)
• Failure to coat the accessory cones with a thin layer of root canal sealer (lateral compaction)
• Failure to insert accessory cones to the full length of spreader penetration (lateral compaction)
• Use of accessory cones with very fine tips that curl up or kink on placement during lateral compaction
• Use of a too-large spreader (lateral compaction) or plugger (vertical compaction, thermoplasticized gutta-percha injection techniques)
• Too much root canal sealer (all techniques)• Use of a rapidly setting root canal sealer or an
improperly mixed sealer that may set up too fast (all techniques)
• Failure to achieve depth of compaction and flow of softened gutta-percha (vertical compaction, all thermoplasticized gutta-percha techniques)
• Failure to soften the apical segment of the gutta-percha before compaction (vertical compaction)
A BB
C D
FIGURE 12-30 A, Root canal treatment that appears acceptable, but note the apical third of the canals are poorly filled and probably poorly enlarged, shaped, and cleaned, because the patient is symptomatic. B, Revision with enhanced shaping, cleaning, and obturation; symptoms have abated. C, Same scenario as previous case. Note the poor obturation that was accepted by the clinician as being to the standard of care, yet the patients are all symptomatic until proper enlarging, shaping, cleaning, and obturation are performed. D, 12-month reevaluation indicating complete healing of the apical lesion. The patient remained asymptomatic.

238 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
a problem-preventing approach—to root canal obturation. To obturate the prepared root canal system as densely as possible throughout its entire length, attention must be paid to canal preparation, proper fit of the master cone or injec-tion needle, and proper fit of compacting instruments. In addition, effective use of not only the root canal sealer but also the accessory gutta-percha cones or material segments, gutta-percha, or resin-bonded materials is a must to fill the prepared canal space.
Radiographic voids in the root canal filling can be viewed in a number of ways:
“So what, and why should I worry? They never fail.”“That doesn’t look good, but it will work.”“That’s my signature, and I can’t let the patient or any
other clinician see this radiographic film!”
• Excessive packing of dentin chips in the apical 1 to 3 mm (This should not occur when using NiTi rotary instruments and good irrigation, as these instruments are designed to bring debris out of the canal.)
• Failure to seat the core carrier to the apical seat or stripping of the core filler at its apical extent
• Inconsistent heating, too little or too much, with the core-carrier techniques (This inconsistency is easily prevented by using the manufacturer’s heating systems. The heating of the core filler over an open flame is subject to too many discrepancies and should be avoided.)
Each of these potential problems can be averted when using a cognizant, problem-solving approach—or better yet,
A B C
D
FIGURE 12-31 Tooth models that have been obturated and either sectioned (A) or cleared (B); voids are evident. C, Scanning electron micrograph of voids or gaps where the gutta-percha was not warmed sufficiently and compacted thoroughly. D, Obturation in the first molar is compared to that of the second molar. Compare the voids and lack of density in the second molar to the smooth contours and density of the canal shapes and fillings in the first molar.

chapter 12 | Problem-Solving Challenges in Root Canal Obturation 239
“It’s an antiseptic filling designed to heal the bone.”“I think I have to improve my technique to eliminate
these errors.”
There are few if any studies that have shown a correlation between voids and treatment failure (other than the poor apical density discussed earlier or the voids between intrara-dicular posts and the root canal filling28; see Chapters 5 and 21). In fact, rarely do we see all the voids we leave in the root canal obturation (Fig. 12-31).
Although classic studies have identified poor obturation as the major cause of failure of root canal treatment,7 these find-ings were based on cases in which cleaning and shaping were not performed as they are done today. Additionally, obtura-tion was performed with little compaction, using single gutta-percha or silver cones. Occlusal leakage may have also contributed to many of the failures, especially in the single gutta-percha cone fills or when silver cones were used, and corrosion products initiated adverse periradicular tissue responses. Modern approaches to root canal cleaning, shaping, and obturation minimize the likelihood of voids affecting success. In addition, if proper apical compaction is performed, voids are usually limited to the middle and coronal canal seg-ments and pose minimal to no threat to prognosis.
RefeRenCeS1. Allison DA, Weber CR, Walton RE: The influence of the method
of canal preparation on the quality of apical and coronal obtura-tion, J Endod 5:298-304, 1979.
2. Bergmans L, Moisiadis P, DeMunck J, et al: Effect of polymeriza-tion shrinkage on the sealing capacity of resins fillers for endodon-tic use, J Adhes Dent 7:321-329, 2005.
3. Berry KA, Loushine RJ, Primack PD, et al: Nickel-titanium versus stainless steel finger spreaders in curved canals, J Endod 24:752-754, 1998.
4. Connor DA, Caplan DJ, Teixeira FB, et al: Clinical outcome of teeth treated endodontically with a nonstandardized protocol and root filled with Resilon, J Endod 33:1290-1292, 2007.
5. Dahl JE: Toxicity of endodontic filling materials, Endod Topics 12:39-43, 2005.
6. De Deus GR, Gurgel-Filho ED, Maniglia-Ferreira C, et al: The influence of filling technique on depth of tubule penetration by root canal sealer: a study using light microscopy and digital image processing, Aust Endod J 30:23-28, 2004.
7. Dow PR, Ingle JI: Isotope determination of root canal failure, Oral Surg Oral Med Oral Pathol 8:1100-1104, 1955.
8. Fisher MA, Berzins DW, Bahcall JK: An in vitro comparison of bond strength of various obturation materials to root canal dentin using push-out test design, J Endod 33:856-858, 2007.
9. Franzen JN, He J, Glickman GN, et al: Comparative assessment of Activ GP/glass ionomer sealer, Resilon/Epiphany, and gutta-percha/AH plus obturation: a bacterial leakage study, J Endod 34:725-727, 2008.
10. Gesi A, Bergenholtz G: Pulpectomy—studies on outcome, Endod Topics 5:57-70, 2003.
11. Gesi A, Raffaelli O, Goracci C, et al: Interfacial strength of Resilon and gutta-percha to intraradicular dentin, J Endod 31:809-813, 2005.
12. Gluskin AH: Mishaps and serious complications in endodontic obturation, Endod Topics 12:52-70, 2005.
13. Gutmann JL: Adaptation of thermoplasticized gutta-percha in the absence of the dentinal smear layer, Int Endod J 26:87-92, 1993.
14. Gutmann JL: Biologic perspective to support clinical choices in root canal treatment, Australian Endod J 31:9-13, 2005.
15. Gutmann JL, Witherspoon DE: Obturation of the cleaned and shaped root canal system. In Cohen S, Burns RE, editors: Pathways of the pulp, ed 7, St Louis, 2002, Mosby.
16. Grossman LI: Root canal therapy, ed 2, Philadelphia, 1946, Lea & Febiger.
17. Hatton EH: Changes produced by disease in the pulp and periapi-cal regions and their relationship to pulp-canal treatment and systemic disease, Dent Cosmos 66:1183-1189, 1924.
18. Hemalatha H, Sandeep M, Kulkarni S, et al: Evaluation of fracture resistance in simulated immature teeth using Resilon and Ribbond as root reinforcements—an in vitro study, Dent Traumatol 25:433-438, 2009.
19. Hill A: Hill’s stopping, Am J Dent Sci 9(1st Series): 82-85, 1848.20. Hiraishi N, Yau JY, Loushine RJ, et al: Susceptibility of a polycap-
rolactone-based root canal filling material to degradation. III. Tur-bidimetric evaluation of enzymatic hydrolysis, J Endod 33:952-956, 2007.
21. Jasper EA: Root-canal therapy in modern dentistry, Dent Cosmos 75:823-829, 1933.
22. Johnson WB: A new gutta-percha technique, J Endod 4:184-188, 1978.
23. Kokkas AB, Boutsioukis ACh, Vassiliadis LP, et al: The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: an in vitro study, J Endod 30:100-102, 2004.
24. Lawson MS, Loushine B, Mai S, et al: Resistance of a 4-meta-containing, methacrylate-based sealer to dislocation in root canals, J Endod 34:833-877, 2008.
25. Love RM, Firth N: Histopathological profile of surgically removed persistent periapical radiolucent lesions of endodontic origin, Int Endod J 42:198-202, 2009.
26. Monticelli F, Sadek FT, Schuster GS, et al: Efficacy of two con-temporary single-cone filling techniques in preventing bacterial leakage, J Endod 33:310-313, 2007.
27. Monticelli F, Sword J, Martin RL, et al: Sealing properties of two contemporary single-cone obturation systems, Int Endod J 40:374-385, 2007.
28. Moshonov J, Slutzky-Goldberg I, Gottlieb A, et al: The effect of the distance between post and residual gutta-percha on the clinical outcome of endodontic treatment, J Endod 31:177-179, 2005.
29. Ørstavik D: Materials used for root canal obturation: technical, biological and clinical testing, Endod Topics 12:25-38, 2005.
30. Ozawa T, Taha N, Messer HH: A comparison of techniques for obturating oval-shaped root canals, Dent Mater J 28:290-294, 2009.
31. Patterson SS, Newton CW: Preparation of root canals and filling by lateral condensation techniques. In Gerstein H, editor: Tech-niques in clinical endodontics, Philadelphia, 1983. Saunders.
32. Pitts DL, Matheny HE, Nicholls JI: An in vitro study of spreader loads required to cause vertical root fracture during lateral conden-sation, J Endod 9:544-550, 1983.
33. Postman N: Technopoly: the surrender of culture to technology, New York, 1993, Vintage Books.
34. Rucucci D, Siqueira JF, Jr: Anatomic and microbiologic challenges to achieving success with endodontic treatment: a case report, J Endod 34:1249-1254, 2008.

240 chapter 12 | Problem-Solving Challenges in Root Canal Obturation
44. Teixeira FB, Trope M: Gutta-percha-the end of an era? Alpha Omegan 97(4):16-22, 2004.
45. Ungor M, Onay EO, Orucoglu H: Push-out bond strengths: the Epiphany-Resilon endodontic obturation system compared with different pairings of Epiphany, Resilon, AH Plus and gutta-percha, Int Endod J 39:643-647, 2006.
46. Whitworth J: Methods of filling root canals: principles and prac-tice, Endod Topics 12:2-24, 2005.
47. Wilkinson KL, Beeson TJ, Kirkpatrick TC: Fracture resistance of simulated immature teeth filled with Resilon, gutta-percha, or composite, J Endod 33:480-483, 2007.
48. Wu MK, van der Sluis LW, Wesselink PR: A 1-year follow-up study on leakage of single-cone filling with RoekoRSA sealer, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:662-667, 2006.
ReCommended AddITIonAL ReAdIngBenenati F: Obturation of the radicular space. In Ingle JI, Bakland LK,
Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker.
Johnson JD: Root canal filling materials. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontics 6, Hamilton, Ontario, 2008, BC Decker.
Kim YK, Gandini S, Ames JM, et al: Critical review on methylacrylate resin-based root canal sealers, J Endod 36:383-399, 2010.
Wesselink PR: Root filling techniques. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
35. Shipper G, Ørstavik D, Texeira FB, et al: An evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymer-based root canal filling material (Resilon), J Endod 30: 342-347, 2004.
36. Skidmore LJ, Berzins DW, Bachall JK: An in vitro comparison of the intraradicular dentin bond strength of Resilon and gutta- percha, J Endod 32:963-966, 2006.
37. Spångberg LSW, Haapasalo M: Rationale and efficacy of root canal medicaments and root filling materials with emphasis on treatment outcomes, Endod Topics 2:35-58, 2002.
38. Tay FR, Pashley DH: Monoblocks in root canals—a hypothetical or a tangible goal, J Endod 33:391-398, 2007.
39. Tay FR, Pashley DH, Loushine RJ, et al: Susceptibility of a poly-caprolactone-based root canal filling material to degradation. Evi-dence of biodegradation from a simulated field test, Am J Dent 20:365-369, 2007.
40. Tay FR, Pashley DH, Williams MC, et al: Susceptibility of a polycaprolactone-based root canal filling material to degradation. I. Alkaline hydrolysis, J Endod 31:593-598, 2005.
41. Tay FR, Pashley DH, Yiu CK, et al: Susceptibility of a polycap-rolactone-based root canal filling material to degradation. II. Grav-imetric evaluation of enzymatic hydrolysis, J Endod 31:737-741, 2005.
42. Teixeira FB, Teixeira EC, Thompson JY, et al: Dentinal bonding reaches the root canal system, J Esthet Restor Dent 16:348-354, 2004.
43. Teixeira FB, Teixeira EC, Thompson JY, et al: Fracture resistance of roots endodontically treated with a new resin filling material, J Am Dent Assoc 2004; 135:646-652, 2004. Erratum in J Am Dent Assoc 135:868, 2004.

241
Chapter 13
Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
Problem-Solving ListProblem-solving challenges and dilemmas in the total management of compromised roots and root canal systems and anatomic deviations addressed in this chapter are:
Problem-Solving Challenges in the Tooth With a Necrotic Pulp and Immature Apical Development: Apexification
Problem-Solving Challenges in the Tooth With Fine and Calcified Canals
Problem-Solving Challenges in the Tooth With Resorptive Defects
Internal resorption
External resorption
Cervical resorption
Problem-Solving Challenges in the Tooth With a C-Shaped Canal
Problem-Solving Challenges in the Tooth With Moderate-to-Severe Canal Curvature
Problem-Solving Challenges in the Tooth With an S-Shaped Canal
Problem-Solving Challenges in Anatomic Deviations
It is seldom that we see canals in buccal roots of superior molars, or in roots of lower molars, in which a drill can be used. . . . There are canals that are constricted just at the chamber, sometimes so much so that they can scarcely be found. . . . There are canals in curved roots and canals obstructed by osseous growths that, if not properly opened, would most likely cause trouble. It is with this difficult class of root-canals that I wish to deal at this time.9
J.R. Callahan, 1894
Problem-Solving Challenges in the Tooth With a Necrotic Pulp and Immature Apical Development: Apexification
Historically, when a dental pulp had undergone demise before full root formation, an apexification procedure was indicated and still is the treatment of choice.29,55 However,
I have seen resorption of apical cementum progressing with such attending conditions, while on the opposite surface of the same root there was a marked hyperplasia of cementum. In fact, it seems quite common to find these processes going on at the same time.8
J.R. Blayney, 1927
This chapter will focus exclusively on the total management of difficult or challenging root canal anatomies, such as immature root development and a necrotic pulp; teeth that have been altered due to caries (irritational dentin and calci-fication) or resorptive processes both internal and external; teeth with accentuated curvatures; and unusual root and pulp space development in C-shaped canals. The reader is encour-aged to seek additional and supportive information from the other chapters in this text; however, the challenges addressed in this chapter seemed to warrant individual attention using the problem-solving format.

242 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
odontoblasts rarely if ever survive pulpal necrosis (Fig. 13-1). This important concept, while understood in the context of traditional apexification, has not necessarily been elucidated or addressed in the purported revascularization or regenera-tive techniques that will be discussed later. The tissue response in the traditional technique has been shown to be a gnarled osteocementum type of material30 (Fig. 13-2). It is often porous, and its formation, thickness, and location are often irregular in nature. It is a valid procedure for both anterior and posterior teeth. Figs. 13-3 and 13-4 offer detailed descrip-tions of traditional apexification using Ca(OH)2 technique in anterior and posterior teeth.
From a contemporary standpoint, Ca(OH)2 is still used for bacterial control,69,76 but its presence over a long period may weaken the dentin.2,3,15,48,58 A major problem inherent in the tooth with immature root formation is the structural weakness of root walls (root wall thickness) (Fig. 13-5).1,12,68 If the impact of Ca(OH)2 is added to this weakness, the chance for long-term retention of these teeth would be doubtful. Often over time, these teeth—even with apical closure—may be unable to withstand not only the occlusal and functional stresses but also the impact of the wide range of restorative procedures that have been used to main-tain these teeth. Furthermore, the use of preformed, intrara-dicular metallic posts in the tooth are not indicated; even if used, they would not likely strengthen the root structure (see Chapter 20). A bonded, carbon fiber post may be a
multiple directions in the management of this clinical chal-lenge have emerged that differ from the traditional calcium hydroxide apexification procedure.23 The details of the tradi-tional technique will be discussed briefly, as it has withstood the test of time. This will be followed by alternatives that are currently being advocated78,79 that include the use of mineral trioxide aggregate (ProRoot MTA [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA])62 and a technique that is referred to by some as revascularization and by others as regeneration within the pulpal space.10
The traditional apexification procedure requires complete canal cleaning, shaping, removal of smear layer, and disinfec-tion (see Chapters 10 and 11) before the placement of calcium hydroxide (Ca[OH]2) to promote the formation of osteocementum or apical bridge formation. This technique is often referred to as the Frank technique.23 The calcium hydroxide kills bacteria, dissolves tissue, and creates an envi-ronment conducive to hard-tissue formation.69,75,80 The material is left in place or changed every 3 months, with intervals as long as 12 months in later stages to enhance the tissue response.29 The mean time to barrier formation in incisor teeth has been shown to be 34.2 weeks (range 13 to 67 weeks),22 but data on posterior teeth is unavailable. Recently this technique of changing the Ca(OH)2 has been shown to be counterproductive to the formation of hard tissue, although it did seem to lessen inflammatory response.20 The hard tissue that ultimately forms is not dentin, because
C
A B
FIGURe 13-1 a, Developing root apex showing the Hertwig epithelial root sheath (arrows). B, Note how the sheath invaginates into the mesenchymal tissues (dental sac) on its way to root development. Once this sheath dies, the chance for normal root development ceases. C, View of tooth root that has not closed; perimeter of the opening represents the area of the root sheath.

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 243
The use of MTA in one-visit apexification treatment has received some significant attention,42,65,79 with outcomes favoring this approach as opposed to the use of Ca(OH)2 followed by MTA (Fig. 13-7, A-E ).* However, what is defined as a one-visit treatment may be ambiguous47 insofar as many clinicians access, enlarge, shape, and clean, then place Ca(OH)2 for 7 to 14 days. Instead of waiting for a lengthy period, the canal is filled with MTA within 2 weeks or less (Fig. 13-8). If everything could be done in one visit, it would also negate the potential for leakage that has been identified when MTA has been placed following the use of Ca(OH)2.66 In some cases, it may be wise to use MTA in a one-visit placement surgically to manage an open apex in light of other complications (Fig. 13-9).47
Following placement of MTA in the canal, some options are available to the clinician for restoring the tooth, depend-ing on whether only apical plugs were placed or the entire canal was filled.50 First, a glass ionomer can be placed on top of the MTA, followed by a bonded composite or bonded post.16 Second, bonded materials can be placed directly against the MTA after allowing the MTA to set for a minimum of 2 to 4 hours; some clinicians bring the patient back the following day for this procedure. Bonding the canal walls in these cases is a wise choice to prevent fracture.36,43 As mentioned, the use of metallic posts is contraindicated, but the newer resin-bonded obturation materials may be a choice because the strength of the root may be enhanced.68 Clinical evidence of this effect is unavailable, but what is known is that MTA itself may enhance the strength of the root struc-ture by an interesting mechanism in which it induces the expression of tissue inhibitors of metalloproteinases (TIMPs), thereby preventing destruction of the collagen matrix.34 In adhesive restorations, one major problem is hybrid layer deg-radation. At present, this deterioration is explained by the activation of endogenous matrix metalloproteinases (MMPs) present in dentin owing to the acidic property of adhesive systems. Even mild self-etching adhesives activate latent MMPs without denaturing these enzymes and may adversely affect the longevity of bonded root canal fillings and posts.70 In this regard, the use of chlorhexidine (CHX) has been advocated to prevent the release of MMPs,35 and it is possible that CHX should also be advocated in place of Ca(OH)2 for bacterial control in teeth with immature root development and a necrotic pulp. The concept of inducing TIMPs and preventing the release of MMPs is essential in achieving bonding in the root canal system with products such as Epiphany/Resilon (Pentron Technologies Inc., Wallingford, CT, USA).
The most contemporary approach to the management of teeth with immature root formation and either irreversible pulpitis and periapical periodontitis5,10,11,39,40 or necrotic infected pulps41,71 has been promulgated as revasculariza-tion,56 or even regeneration.10,32,73 In their infancy, these tech-niques claimed to be taking advantage of the pluripotential
consideration, although little is known about its ability to enhance treatment outcome.1 Therefore, exit Ca(OH)2 and enter MTA62,78,79 as the contemporary material of choice for apexification techniques, even to the point of citing this approach as being “regenerative” in nature.10 This material has been shown to be inductive for hard-tissue formation,26,57 in particular in its use in apexification.* Moreover, its sealing properties in the root have been shown to be acceptable with or without the use of an accelerator that would enhance its physical properties for placement.37
MTA, while effective in most cases in securing a positive tissue response and healing when used in a variety of applica-tions,47,57 has been difficult to manipulate in its present form. To meet these challenges, a number of techniques have been advocated for its placement and retention. For example, pellets of the material can be mixed to a workable consistency and then measured in length to determine the amount to be placed into the canal. The MTA can be placed in this form and compacted with measured pluggers or a custom fit gutta-percha cone.67 This procedure seems to work well (Fig. 13-6). A second option would be to use an appropriately sized amalgam carrier or any one of a number of devices designed for this purpose (see Chapter 16 for further details). Pres-ently, many studies have attempted to alter the physical prop-erties of MTA to enhance its clinical management.6,44
FIGURe 13-2 Apical closure of a primate’s tooth during apexification with calcium hydroxide, showing a gnarled-type of hard tissue has formed over the root canal. There is no root lengthening or root wall strengthening.
*References 18, 21, 30, 31, 53, 60, 62, 78, and 79. *References 18, 21, 28, 33, 53, and 60.

244 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
cells in the dental papilla and/or periodontal ligament, induc-ing them to form hard tissue into the root canal or to somehow continue the development of Hertwig’s epithelial root sheath (HERS; see Fig. 13-1 and Chapter 7).40
Preliminary technique: The technique to achieve this goal consists of an access to the canal, drainage as necessary, rinsing the canal with sodium hypochlorite (NaOCl) and CHX, drying the canal, and placement of a mixture of ciprofloxacin, metronidazole, and minocycline with a lentulo spiral.5,38,41,59 Placement to the working length or extent of the root apically does not appear to be important, and there is no compaction of the antibiotic paste. If successful, this is followed by the ingrowth of soft tissue (revascularization) and the presence of hard tissue building up along the internal walls of the root to varying degrees of thickness. In some cases this thickness is uniform, in others it may only occur in the apical portion of the root canal. In essence, what is being achieved is possibly a revitalization to some extent that encourages the apexogenesis process, as described in Chapter 7.
C D
BA
FIGURe 13-3 a, Two traumatized maxillary central incisors with immature root formation and necrotic pulps. B, Calcium hydroxide was placed. The patient is symptom free, and the teeth are functional. C, Removal of the calcium hydroxide at 1 year and verification of apical bridge formation. D, Both canals filled with gutta-percha and sealer. Note the porosity of the apical bridging.
This initiative has even developed some of its own nomen-clature in its claims, such as bioroot engineering, pulp revascu-larization, regenerative endodontic treatment or regenerative therapies, and stem cells from the apical papilla (SCAP).39,40 While only supported by diverse case reports at this moment, there is a significant research initiative to pursue this model, calling it “the hidden treasure in apical papilla.”40 The trea-sure refers to the uniqueness of the SCAP relative to cellular types and their potential for differentiation and expression of their genetic potential—that is, cells with the phenotypic capability of becoming new odontoblasts. In combination with the genetic capabilities of cells from the periodontal ligament (periodontal ligament stem cells [PDLSCs]), they offer the promise of truly regenerating lost or damaged tissues.
It is not the intent of this text to espouse these theories or clinical innovations, but rather to raise some challenging problem-solving questions relative to the thought and direc-tion behind them. The concept of stem cell identification and their potential applications is laudable, exciting, and should

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 245
A B
C
FIGURe 13-4 a, This 10-year-old male has significant decay and delayed root development on the mandibular first molar. Apical and furcation bone loss is evident, and the tooth is scheduled for extraction. B, The pulp chamber and canals are cleaned and shaped, and calcium hydroxide is placed. The open apices and slight extrusion of the material is noted. C, Six-month assessment shows great healing and the beginning formation of apical bridging. The roots are filled with gutta-percha and sealer. Slight porosity of the apical bridge is noted, but the healing response is excellent. A space maintainer is placed on the tooth.
BA
FIGURe 13-5 a, Maxillary central incisor that has undergone apexification and canal filling. B, Four months later, the patient had not had the tooth restored and complained of soreness in his gingival tissues. Radiograph shows a horizontal root fracture on the central incisor.

246 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
A
D
B
C
FIGURe 13-6 a, Maxillary lateral incisor with an open apex, thin root walls, and a large periapical lesion. The tooth was opened by her general dentist 2 months subsequent to a coronal fracture in which the pulp was exposed. B, The root canal was cleaned and a plugger (compactor) fitted into the canal for both length and width assessment. C, Mineral trioxide aggregate (MTA) is placed and compacted using the plugger. D, Canal is completely filled and a 6-month evaluation shows good bony response. Healing is not complete but is progressing.
be pursued. However, there are issues that need distillation and clarification before these concepts and potential tech-niques can become meaningful and sought after by the clinician:
• If the pulp is necrotic, how can “regeneration” in the truest sense be achieved in a predictable manner? Where do the stem cells for “odontoblasts” come from in a necrotic environment, especially if there is a long-standing periapical lesion?
• The tissue, both soft and hard, that is claimed to grow into the root during “revascularization”: Is it pulp? Dentin? Cementum? Osteocementum? Bone?
• What purpose will it serve to have this tissue grow into the pulpal space if in time the tooth suffers from the ravages of caries or trauma?
• Is there any difference in tissue response when the pulp is necrotic or just irreversibly inflamed?
• How can the extent of tissue damage be determined clinically?
• How do we know the extent of the inflammation, and where do we stop our treatment procedures in the tooth?
• Will the use of antibiotics in the pulp canal have a systemic impact on the patient over time?
• Will bacterial species adapt and reengineer themselves around the capability of these antibiotic mixtures in time?
• How can we know that these procedures will provide predictable outcomes for the patient?
• If the procedure fails, how do we know we can revert to a traditional or MTA apexification process?

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 247
D
B
C
E
A
FIGURe 13-7 a, A 13-year-old male with a large periapical lesion on a mandibular second premolar. B, Calcium hydroxide was placed. C, Within 3 months, the apex appears to be closing. D, Entire canal filled with MTA. Note slight amount of material that is past the foramen, probably calcium hydroxide. e, Three months later, the tooth and periapical tissues are stable.
C
A B
FIGURe 13-8 a, Mandibular molar with significant decay, periapical lesions, and open apices. B, Decay was excavated, and calcium hydroxide was placed. Four months later, the root apices appear to be closing. C, Mineral trioxide aggregate (MTA) was placed in the canal, and the tooth was restored.

248 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
Problem-Solving Challenges in the Tooth With Fine and Calcified Canals
The problem of calcification was introduced in Chapter 8 in reference to access preparation and location of the canal orifices. Calcification in the root canal system is also a fre-quently encountered problem in root canal treatment.14,63 Radiographs often indicate an apparent complete obliteration of the pulp chamber and the canal spaces (Fig. 13-10). The process of calcification appears to be a linear phenomenon
beginning in the crown and progressing apically in most cases. Therefore, the failure to locate a canal orifice during a non-surgical access procedure, even if it is extended quite deep, does not rule out the possibility that canal space exists more apical than can be reached.
In these types of cases, the eventual development of peri-apical pathosis has been observed by the authors to be uncommon. It is also fortunate that only a small percentage of cases that radiographically exhibit fine or unidentifiable canals prove to be unmanageable using nonsurgical root canal techniques (Fig. 13-12). However, when patent canal space is present, successful negotiation of this type of canal to its apical extent is extremely diffcult.64 Of the numerous
A B C
FIGURe 13-9 a, Maxillary lateral incisor with a dens in dente, open, immature apex, periapical lesion, and no response to sensibility testing. The dens in dente was intact, and surgery was chosen. B, Apical fill with mineral trioxide aggregate (MTA). C, 19-Month reevaluation healing is excellent.
CLINICAL PROBLEMProblem: A 71-year-old female sought dental consultation because the porcelain fused to metal crown on her left maxillary lateral incisor fractured off at the gingival margin. There were no symptoms and the tooth had no clinical or radiographic signs of pathosis. A root canal space is evident on the examination film (Fig. 13-11, A). Intraradicular root canal treatment was initiated with the object of providing space for a post. Following careful excavation with a No. 2 surgical length round bur deep into the root, no canal could be identified. A control radiograph was made with an endodontic explorer in the excavation to assess the direc-tion of excavation (see Fig. 13-11, B). The direction of excavation appeared to be accurate in the mesial-distal orientation and clini-cally, the excavation appeared centered in the buccal-lingual ori-entation. Further excavation was no longer considered prudent due to the limited ability to assess the buccal-lingual orientation
of the bur angulation. What is the best course of treatment at this point?
Solution: In the absence of symptoms or signs of pathosis, conversion of the excavation to a preparation for an intraradicu-lar post is indicated. The tooth was subsequently restored with a resin-fiber type of post, followed by a new full crown. Two years later, the patient developed symptoms of periapical inflamma-tion. A radiograph revealed an apical lesion(see Fig. 13-11, C). Periapical surgery was the appropriate remedial treatment. At surgery, an ultrasonically energized endodontic file was used for the root-end preparation (see chapter 16). The file followed the existing canal space to the point of calcified occlusion at which point the apical canal space was enlarged and filled with MTA (see Fig. 13-11, D).

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 249
Before file insertion, a small curve is placed in its apical 1 mm. This can also be done with the C+ file. The precurved instrument must be directed along the pathway the canal is most likely to follow (see Fig. 13-13, D). Consequently, knowing the direction in which the curve in the instrument is pointed is vitally important. Observing the rubber stop on the instrument shaft of the directional type makes this deter-mination easy. Penetrate slowly, using a slight 90-degree back-and-forth rotation to assess for patency. If patent, proceed apically until resistance is met, but do not try to just push the file apically in a linear fashion. The operative word is tease; teasing the file will allow it to find its way through the milieu of tissue debris and calcified matter.
During penetration, the chamber must be filled with NaOCl . A chelating agent can be used, but this will not dissolve loose debris, and it will negate the action of NaOCl. The calcified canal should never be negotiated without irrig-ant. This approach only serves to pack debris or calcifications into the canal and risks complete blockage. As the file is teased into the canal, try to establish a “sense of the patency” as this will provide a guideline for subsequent instrument use. Obtaining radiographs to verify the file position is exceedingly important64 (Fig. 13-14). Once a few millimeters of penetration have been achieved, the file should be used in a circumferential manner, opening the orifice. This is followed by removing the file, irrigating, and replacing the file to the previous depth. The file should fit loosely; if not, the first step should be repeated with a No. 10 or possibly a No. 15 K-file, or C+ file. As the irrigant penetrates into this small opening, the instruments loosen debris and begin to create a coronal pathway to the middle portion of the canal.
techniques available to locate and negotiate these canals, those procedures known to be most effective in clinical prac-tice and used by the authors are considered here. Success in negotiating small or calcified canals is predicated on a proper access opening and identifying the canal orifice or orifices as discussed in Chapter 8. Typically, the canal is ready for pen-etration with an endodontic file when the endodontic explorer firmly “sticks” when forcibly inserted into the orifice. If avail-able, it is often helpful to use the ultrasonic instrument with a probe type of tip (see Fig. 14-4) to both enlarge the orfice and circumferentially remove some of the calcified material.
This discussion will assume that the orifices have been located. Each tooth group will be somewhat different, but the concept and technique of gaining access to these canals are the same.
A 21-mm No. 8 K-file can be used initially to negotiate the calcified canal (Fig. 13-13). This file is flexible enough to negotiate around curvatures and calcifications. If the flexibil-ity is too great, then instruments such as the C+ file or ProFinder files (Dentsply Maillefer, Ballaigues, Switzerland) will serve. The C+ file is possibly better in some canals; the instrument shaft provides as much as a 300% increase in resistance to a buckling force during penetration. If chosen, a 21-mm No. 6 C+ file will work nicely for canal penetration, because even though it is smaller than the No. 8 file, it has a stiffer shaft. If the canal is longer than 21 mm, changing to a 25-mm instrument once 21 mm of penetration has been achieved is simple. A No. 10 K-file is usually too large and a No. 6 K-file is too weak to apply any firm apical pressure, particularly if precurved. Nickel-titanium (NiTi) files are contraindicated for this purpose because of their lack of tor-sional strength.
A B
FIGURe 13-10 a, Maxillary molar with significant calcification present. B Histologic variations that may be noted in these types of calcified canals (H&E stain ×40).

250 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
AB
CD
FIGURe 13-11 a, Complete crown fracture on a maxillary lateral incisor with extensive calcification. B, Unsuccessful attempt to negotiate canal. C, Two-year reevaluation following restoration with resin-fiber post retained crown. Apical pathosis is evident. Note: Conversion of access excavation into post space. D, Post operative radiograph. Apical surgery was indicated to clean and seal remaining canal space at the apex.
Once the file reaches the coronal to middle portion of the canal, a No. 10 or 8 K-file may be used to penetrate deeper into the middle third. If successful, the orifice should be irrigated and the file used to loosen debris. Excessive apical pressures should be avoided during all efforts at penetration; however, greater amounts of pressure can be applied with the C+ files. The last two steps may have to be repeated multiple times to gain access to the canal.
Once the middle portion of the canal is reached, a NiTi rotary instrument can be used to enhance the flare of the coronal portion of the canal if desired. This will establish a more patent pathway and will improve the tactile sensitivity as canal negotiation and enlargement continues. As an alternate, a small Hedström file may be used. Continue to use copious irrigation during this process.

A B
FIGURe 13-12 a, Mandibular premolar with apparent complete calcification of the entire root canal system.B, Successful negotiation of the canal with a .08 file in combination with a solution containing EDTA.
A CB
D E
FIGURe 13-13 a, 38-year-old male presented with a history of tooth trauma to his mandibular anterior teeth. His chief complaint was periodic pain to pressure in the left lateral incisor. The tooth was nonresponsive to sensibility tests, with a slightly abnormal response to palpation and percussion. A radiograph showed significant pulp chamber and coronal canal calcification. B, Initial penetration of the pulpal space shows a mesial deviation of the file in the root and how the dental dam clamp can block direct vision of the file penetration. C, After failing to penetrate the canal, a temporary filling was placed and a radiograph was exposed without the dental dam in place to determine the angle of the access relative to the residual canal position. D, Reorientation and penetration with a small apically curved file. e, the canal was located, and penetration was achieved to the apex.

252 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
CBA
FIGURe 13-14 a, 66-year-old male presents with periodic pain in the maxillary right lateral incisor. The tooth has a long history of decay and restorations. The tooth is very tender to percussion and palpation. Thermal sensibility tests are negative for response. The canal space is quite calcified, and the root is curved in the apical third. B, Deep penetration has been achieved without the canal being located; note the serious deviation in a distal (and clinically) buccal direction. C, Reorientation of bur penetration and use of a pathfinder instrument enabled the initial penetration into the true canal space. Liberal use of irrigant and liquid ethylenediamine tetraacetic acid (EDTA) was essential to slowly and carefully penetrate the partially calcified space to its apical extent.
When the middle portion of the canal is opened, the apical portion can be approached in a similar manner as described. The philosophy of this approach is based on two concepts: (1) using the crown-down canal technique and (2) limiting the application to only small segments of the canal instead of trying to gain full penetration immediately. This tech-nique should be used to open all orifices and canals before determining working length (see Chapter 7).
During penetration into the apical portion of the canal, a stainless steel file (No. 10 or 15) with a slight apical curve should be used to penetrate beyond the middle third of the canal. A probing and very gentle stem-winding movement should advance the instrument another 1 to 2 mm into the canal. The middle portion and junction of the middle- to-apical portion of the canal can have highly variable ana-tomic challenges, such as rapid narrowings, canal deviations, and canal junctions.
The newly penetrated space is filed until the instrument freely slides to the next desired level in the canal. Remember that the entire canal does not have to be negotiated immedi-ately. This technique continues with alternating irrigation and advancement in 1- to 2-mm increments. In extremely narrow or tight canals, a No. 8 K-file should be immediately exchanged for a No. 6 K-file or switched for a C+ file. However, forcing these small files too vigorously may lead to ledge formation or blockage.
Frequent inspection of the apical curvature of the files is performed to identify any defects. Any instrument that shows evidence of fatigue or irregularity of the spiral flutes should be replaced (Fig. 13-15, see Figs. 14-39 and 14-40).
Once the estimated working length of the tooth has been reached, the No. 8 K-file should be used in a filing-only motion until a No. 10 K-file can be passed freely to within 1 mm of the length. Retain the instrument in the canal at that point for radiographic verification of the working length.
In the attempted management of calcified canals, finding a total occlusion of the canal space at any level is common. Histologic studies reveal that these calcifications are seldom complete to the apex (Fig. 13-16, A). Consequently, the prognosis of the root canal treatment depends on the con-tinued health of the pulp or the periradicular tissues on the apical side of the blockage. In the absence of symptoms or evidence of periapical pathosis, it is clinically reasonable and acceptable to instrument and fill the canal to the level negotiated and evaluate the tooth periodically (see Fig. 13-16, C ).
The previous directives addressed canals that had calcifica-tions but could ultimately be negotiated. In the case of canals with extensive calcifications, consider the following guidelines:

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 253
FIGURe 13-15 All files should be inspected frequently for irregularities in the flutes that indicate weakness and potential fracture.
• Irrigate copiously throughout the process; 3% to 6% NaOCl enhances dissolution of organic debris, lubricates the canal, and keeps dentin chips and pieces of calcified material in solution.
• Advance instruments slowly.• Clean and inspect instruments upon withdrawal, and
do not reinsert if the integrity of the instrument is questionable.
• Obtain a radiograph or use an electronic apex locater when a fine instrument has reached the approximate canal length; it should not be removed until this is done. The only difficulty may be when using digital radiography, as smaller files are difficult to see. When trying to remove this instrument after securing the length information, tease it out with slight rotational force. Do not try to pull it straight out, because separation can occur.
• Acids (hydrochloric acid) or alkalis (sodium hydroxide) should not be used to aid in canal penetration. Chelating pastes or solutions should be used to assist in canal penetration (see Chapter 11).
• Ultrasonic instruments should be used in the pulp chamber to loosen calcifications and debris in the
C
A
B
FIGURe 13-16 a, Calcification in the dental pulp routinely occurs from the coronal to the apical root anatomy. B, Maxillary molar requiring revision due to severe pain and swelling. C, Revision is complete, but further length could not be obtained in the distal buccal root (arrows). Patient is to be observed for any signs or symptoms. Apical surgery would be indicated if pathosis were to develop.

254 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
BA
FIGURe 13-17 Radiographic characteristics of external (a) and internal (B) resorption. Note the irregularity of external resorption versus the smooth, symmetric outline of internal resorption.
FIGURe 13-18 a, Maxillary lateral incisor with radiolucency in the middle of the root that resembles internal resorption. A closer look reveals a small canal that runs the length of the root. This is an external or extracanal invasive resorptive defect.
canal orifices (ProUltra tips or Start X instruments [Dentsply Maillefer, Ballaigues, Switzerland]).
• Flare and enlarge any negotiated canal space to improve tactile perception and create the necessary pathway or glidepath for continued canal penetration.
• NiTi rotary orifice-penetrating instruments used with gentle pressure until resistance is met will assist in canal enlargement and shaping.
Problem-Solving Challenges in the Tooth With Resorptive Defects
Resorption can occur in any tooth and has multiple etiolo-gies, of which bacteria, inflammation, pressure, and trauma are probably the most common. Chemical and mechanical injury also are key factors.25 Treatment or management is usually related to the stimulating factors and their removal. For example, intrapulpal infection from bacteria is the stimulation factor for internal and external resorptive defects. This requires appropriate root canal procedures. This same stimulation factor via the gingival sulcus can cause cervical resorption, as can chemicals used in internal tooth bleaching.46,54,77 In these cases, management may include periodontal therapy, root canal procedures, restor-ative procedures, and surgical procedures. Orthodontic pres-sures during tooth movement can cause resorption both longitudinally, which usually undergoes some type of repair, and apically, which does not repair and results in loss of tooth length and sometimes tooth vitality. Two additional stimulation factors that affect tooth resorption are impacted teeth and ankylosis. Management of an impacted tooth usually implies a surgical extraction and subsequent treat-ment modalities on any retained resorbed teeth if possible. Ankylosis has no known factor and therefore the manage-ment thereof is unknown.25
Most clinicians tend to place resorption into two broad categories of resorption: internal resorption (IR; Fig. 13-17, A) and external resorption (ER; see Fig. 13-21). However, from a diagnostic standpoint, the clinician should also be knowledgeable about the wide range of potential resorptive processes that can occur. If necessary, management support can be secured from dental specialists with expertise in treat-ing teeth with more specific types of resorptive processes. In some situations, no treatment is indicated, whereas in others (especially when symptoms are present), rapid, thorough, expeditious management is required. From an endodontic standpoint, the resorptive process, not the pulpal inflamma-tion and need for root canal treatment, limits the long-term prognosis of the teeth to be treated and causes nonfunctional-ity and premature loss. For example, the maxillary lateral incisor seen in Fig. 13-18 appears to have an internal resorp-tive defect. However, a careful examination of the midroot radiolucency shows the canal is intact; the radiolucency must
be due to external invasive or extracanal invasive resorption.24 The prognosis with this resorptive defect is much worse than if it were IR. For additional examples of resorptive lesions see Chapter 3.
Internal ResorptionInternal resorption is defined as a process by which a cell within the pulp can differentiate into a clastic type of cell (Fig. 13-19, A) that resorbs dentin in the pulp chamber (see Fig. 13-19, B), within the root canal system, or both. It can

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 255
A
B
FIGURe 13-20 a, Example of a severe internal resorptive defect in the middle third of the distal root. Chronic inflammation due to caries was the most likely etiology. B, Internal resorptive defect beginning at the orifice of the distal root canal.
occur anywhere along the root canal wall (Fig. 13-20). Bac-teria and chronic inflammation of pulpal tissue have also been implicated as causes of IR.25 Unfortunately, no adequate animal models have been discovered that allow researchers to study this phenomenon adequately. The IR process is not self-limiting; without expedient and appropriate treatment, the resorption will continue until communication occurs from the root canal system to the periodontium, at which time the prognosis for the tooth becomes guarded.
The simple placement of radiopaque Ca(OH)2 in the canal, followed by a radiograph, will assist in the determina-tion of a perforative defect.17 In addition, the IR can begin in the pulp chamber and spread aggressively so that the entire crown of the tooth becomes nothing but a shell of enamel, making it unable to withstand the normal forces of occlusion and thereby severely compromising the strength of the crown (Fig. 13-21). Fortunately, IR is rarely a sequela to traumatic injuries such as luxated or avulsed teeth because of the patho-genesis of pulpal necrosis. Luxated teeth either heal rapidly or quickly become necrotic, and chronic inflammation plays no role in the healing process. Avulsed teeth routinely become necrotic, which prevents chronic pulpal inflammation from occurring, thereby eliminating the possibility of IR.
When the clinician identifies what appears to be IR, chances are that root canal treatment will be the main
A
B
FIGURe 13-19 a, Scanning electron micrograph (×2000) of an isolated multinucleated odontoclast that is present on the root surface. Note the surface of the root and the numerous lacunae. B, Clastic cell resorbing hard tissue.
FIGURe 13-21 Large internal resorptive defect that threatens the strength of the tooth subsequent to orthodontic tooth movement.

256 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
A B C
FIGURe 13-22 a, Root canal treatment of a small internal resorptive defect on the mandibular incisor. B, Large internal resorptive defect on a maxillary lateral incisor. C, Twelve-month reexamination. No symptoms. Note the density of the compacted root filling material in the resorptive defect.
treatment modality If IR is diagnosed and the pulp responds to vitality tests, the ideal treatment is to remove the pulpal tissue as soon as possible. A vital pulp will continue the resorption process until either the pulp becomes necrotic (which is not necessarily the typical sequela) or until the pulp is removed during root canal treatment. If, on the other hand, there is evidence of pulp necrosis or there is apical pathosis, the resorptive process may be presumed to be arrested. Prevention is the operative word from many stand-points: prevention of symptoms and prevention of further destruction of tooth structure, including root weakening and the possibility of a resorptive perforation. It is a particular challenge to clean and seal the irregularities in tooth structure caused by the resorption. Small defects such as the one seen in Fig. 13-22, A are treated with little variation from a routine endodontic case. Large defects require more generous coronal canal enlargement though the access cavity itself should not be excessive. Large Gates-Glidden drills (5 or 6) can be used to enlarge the lingual aspect of the coronal canal from the access opening to the enlarged defect. The defect itself is much too large for standard endodontic files to be effective for cleaning. Alternative and sometimes improvisational debridement techniques are indicated. Long endodontic curettes, periodontal curettes and the ultrasonic instrument have all been effective depending on the location of the defect. Generous rinses and soaks with sodium hypochlorite are always indicated. It is wise to leave the sodium hypochlo-rite and the solution should be left in the defect for a few minutes if possible.
Typically, the canal space apical to the defect is treated in a standard manner. It can be filled by either the lateral or vertical compaction techniques. If warm, vertical compaction is used, the defect can be filled at the same time. It is very
difficult to achieve dense compaction with lateral compac-tion. Furthermore, the lateral pressures on such a weakened root invite vertical or horizontal fracture. An excellent alter-native is to fill the defect with MTA after sealing the apical canal space with gutta-percha and sealer or a resin-based material (see Fig. 13-22, B and C ).
External ResorptionExternal resorption is quite common in long-standing peri-apical lesions, abnormal pressures (e.g., tumors or impac-tions), avulsion injuries, and orthodontic tooth movement. It is also seen routinely in intrusive luxation cases (Fig. 13-23). Most concussion, subluxation, lateral, and extrusive luxation injuries do not demonstrate ER as a typical sequela; however, it is possible in these forms of trauma (see Chapter 19). The two external resorptive defects that must be dis-cussed with the patient are inflammatory resorption (Fig. 13-24, A and B) and inflammatory replacement resorption (IRR; see Fig. 13-24, C ). Occasionally a form of extracanal invasive resorption is identified, but it usually does not involve the dental pulp24 (Fig. 13-25, A). If it should pene-trate the pulp and manifest as symptoms or signs of pulpal pathosis, extraction or root canal treatment can be antici-pated (see Fig. 13-25, A-C ).
Inflammatory resorption is rapid and extremely destruc-tive, but for the most part it can be prevented or minimized by proper cleaning and shaping of the root canal system. This resorption is characterized radiographically by moderate to large “scooped out” radiolucent areas on the root of the traumatized tooth (Fig. 13-26). These areas cannot be treated, but removing the necrotic and bacteria-infested pulpal tissue within the root canal system can prevent additional damage.

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 257
FIGURe 13-23 Clinical appearance of extensive destructive external resorption. The radiographic image of this lesion is Fig. 3-22, B.
A B
C
FIGURe 13-24 a, Mandibular molar that responded normally to sensibility testing (as did all the teeth in this arch), yet the patient was experiencing vague discomfort. B, Patient returned 4 weeks later with swelling and severe pain; note the extensive inflammatory resorption in just 4 weeks. C, Inflammatory replacement resorption on the distal of the second molar.
Studies suggest the use of long-term Ca(OH)2 (6 to 12 months) as a therapeutic agent to prevent resorption13; however, recently this treatment has been shown to decrease the fracture resistance of dentin2,3,12,15 and the ability of healing periodontal ligament cells to proliferate,49 thereby causing an increase in replacement resorption.
Inflammatory resorption is also seen in intrusive luxation injuries and will eventually cause loss of the tooth. The process occurs over several months to years before it becomes critical and the tooth is subsequently lost. The patient should be made aware of this type of sequela, and its ramifications should be included in the long-term treatment plan. Avulsion injuries will also demonstrate replacement resorption, but this can take months to years before it becomes apparent. The process is not self-limiting, and no known treatment prevents its occurrence or its spread throughout the root.
When inflammatory resorption occurs apically, it creates a challenge in the cleaning, shaping, disinfection, and obtura-tion of the root canal system. The natural apical foramen and general apical constriction of the canal is lost creating large irregular apical canal openings through which filling materi-als are easily displaced (Fig. 13-27).

A B
C D
FIGURe 13-25 a, Extracanal resorption; tooth responds normally to sensibility testing. B, Extracanal resorption; tooth had symptoms. C, Pulp removed and calcium hydroxide placed. D, The canals were filled with mineral trioxide aggregate (MTA). Six-month reexamination; patient was symptom free. (Case courtesy Dr. Paul Buxt.)
FIGURe 13-26 Histologic appearance of inflammatory root resorption. Multinucleated giant cells are present in the resorption lacunae that are deep into the dentin. No tissue replacement is evident (H&E stain ×10).

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 259
defect was not adequately accessible from a surgical stand-point, and the patient and clinician elected to watch the progression of the resorption over a 10-year period.
Although systemic conditions may play a role in the cause of this form of resorption, most research fails to identify any relationship with systemic medical conditions. However, one recent finding has determined a mild association of idiopathic external resorption to calciuria and a history of nephrolithiasis.
Other authors suggest that the cause may be correlated with injury, irritation, or both to the periodontal ligament. Proposed etiologies are excessive pressure from tooth erup-tion, normal and abnormal orthodontic forces, nonvital bleaching, bacteria, and treatment of periodontal diseases. Treatment of idiopathic resorption is a function of its sever-ity, the location, whether the defect has perforated into the root canal system, and the restorative integrity of the tooth. If the defect is accessible surgically, removal of granulation tissue and repair with a biocompatible restorative material is indicated. Smaller lesions are sometimes confused with cervi-cal caries and an attempt is made to restore the defect. Lesions of this type do not often develop pulpal symptoms. Cervical
During canal shaping, it is wise to choose a termination point that is 1 to 2 mm shorter than would be appropriate for a routine case in order to create an apical stop. Often the use of MTA, custom-fit gutta-percha cones (Fig. 13-28), or apical barriers are necessary. Inflammatory resorption will also have an impact on the working length of the tooth (see Chapter 9).
Cervical ResorptionWhen inflammatory resorption occurs at the cemental-enamel junction, it is referred to as cervical resorption (CR) or sometimes idiopathic resorption; the etiologies and process are sometimes vague and elusive. CR can result from a dental procedure or inappropriate technique causing destruction of the external surface of the root, usually (but not always) beginning at the cemental-enamel junction. The resorptive process can be self-limiting, but more often it is not; if left untreated, it can destroy significant amounts of tooth struc-ture. Fig. 13-29 presents examples of idiopathic root resorp-tion that began at the cementoenamel junction of the maxillary left central and lateral incisors. In this case, the
A B
C D
FIGURe 13-27 a, Apical root resorption with the eating away of the root laterally. Note the canal is visible; the resorptive process is only attacking the highly mineralized peritubular and intratubular dentin but not the poorly mineralized predentin. B, Histologic depiction of apical root resorption (H&E stain ×4). C, Maxillary premolar with apical resorption. D, Canal filled with gutta-percha and sealer. Six-month examination shows some evidence of healing. Note the excellent control of the filling material and the extrusion of sealer through the porosity of the resorbed distal wall.

260 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
A B C
D E F
FIGURe 13-28 a, This 15-year-old male’s central incisor was traumatized and is now discolored. The apex of the left central shows evidence of resorption (arrow). B, Three months after placement of calcium hydroxide, the patient is symptom free. C, Custom-fit gutta-percha cone. D, Radiograph showing the fit of the cone near the resorptive defect. e, Sealer was placed, the cone was seated and then removed; note the contact on the walls of the gutta-percha cone when it is custom fitted prior to obturation. F, Vertical compaction of the cone.

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 261
A
B
FIGURe 13-29 a, Initial presentation of cervical or idiopathic resorption of the maxillary left central and left lateral incisors. Note the vast amount of tooth resorption at the cemental-enamel junction. No known systemic medical or other health-related dental conditions were discovered to aide in diagnosing the etiology of this condition. B, Radiographic presentation of the same patient 10 years after initial presentation. Root canal therapy was performed with surgery to remove the granulation tissue within the defects in a futile attempt to improve the prognosis.
G
G, One-year reevaluation. Patient is symptom free.FIGURe 13-28, cont’d
resorption is usually discovered on routine radiographic examinations or after the overlying gingival develops chronic inflammation. Despite the lack of a specific etiology or pathogenesis, smaller lesions are amenable to treatment with excellent long-term results (Fig. 13-30). See Chapter 17 for additional information on the treatment of cervical resorp-tion defects.
In all cases, the clinician must initially assess the restor-ability of the tooth. The surgical accessibility of the defect and the depth of extension below crestal bone are important, since periodontal surgery is virtually always required. The effect of bone recontouring on the adjacent teeth must be weighed against the desire to place the bony crest 2 or more millimeters below the margin of the resorption defect. Finally, there is always the possibility of recurrence. Therefore the patient should be informed that the prognosis of managing any idiopathic resorption defect is guarded.
Root canal therapy is only indicated if the defect has per-forated into the canal system or for restorative purposes. Root canal treatment in and of itself will not in any way minimize or inhibit the continued clastic activity of the granulation tissues within the defects created by the resorptive processes. Clearly, the management of this type of root resorption requires a multifaceted approach, oftentimes involving many procedures in dentistry ranging from the placement of simple restorative materials to complex surgical intervention. The root canal treatment is usually delayed until the resorption defect has been repaired. It is difficult to provide quality root
canal treatment when the pulp is in contact with the hemor-rhagic granulation tissue that is present with the resorptive process. The challenge in the repair process is to maintain the patency of the canal during the placement of the repair filling material. Calcium hydroxide is a good choice due to the ease of removal. See Chapter 17 for additional informa-tion. Because the teeth involved with this resorptive process are often anterior teeth, the clinician is urged to consider the additional esthetic complications of this treatment approach when planning treatment.

262 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
A B
C D
EF
FIGURe 13-30 a, Cervical resorption on a mandibular premolar that was mistaken for a carious lesion and restored with composite resin. Eventually, the gingival over the defect became chronically inflamed. B, Surgical exposure of the defect with the composite removed. Note the extension below crestal bone. C, After osseous recontouring and exposure of the gingival margin of the defect. D, Restoration with composite resin. Root canal treatment was subsequently completed. e and F, One year posttreatment. Patient is asymptomatic and the tooth is fully functional, with no signs of recurrent pathosis.
Problem-Solving Challenges in the Tooth With a C-Shaped Canal
Although the prevalence of C-shaped canals is low in many parts of the world, other countries have a high incidence of these diagnostic and treatment challenges (Fig. 13-31, A). Some C-shaped canals are difficult to interpret on radio-graphs and are not often identified until an endodontic access is made. These anatomic variations primarily occur in
mandibular second molars and maxillary first molars.81 When roots in these teeth appear very close or fused, a C-shaped canal anatomy should be anticipated (see Fig. 13-31, B).
The key problems encountered during cleaning and shaping C-shaped canals include difficulty removing pulp tissue and necrotic debris, excessive hemorrhage, and persis-tent discomfort during instrumentation. Because of the large volumetric capacity of the C-shaped canal system housing transverse anastomoses and irregularities, continuous circum-ferential filing along the periphery of the C-shaped root walls with copious amounts of 3% to 6% NaOCl is often necessary to ensure maximum tissue removal and cessation of bleeding.

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 263
shaped, often includes the mesial buccal and distal canals, and may include the mesial lingual canal. Canal orifices may be found within the C-shaped trough, or the C shape may be continuous throughout the length of the canal (see Fig. 13-31, E and Fig. 13-35). In maxillary molars, the C-shaped canal can encompass the mesial buccal and palatal canals or the distal buccal and palatal canals.
• Multiple concavities along the external surfaces of the root should be anticipated to prevent a strip perforation.
• An unrestricted approach to the complex canal system should be created, and the canals should be initially soaked with NaOCl.
Once the canals have been properly cleaned and shaped, a cold or warm gutta-percha or a thermoplasticized gutta- percha obturation technique should be used to manage the complex three-dimensional nature of the C-shaped system (Figs. 13-33 and 13-34). Core-carrier obturations such as ThermaFil, ProTaper, and GT X series or Vortex™ (Dent-sply Tulsa Dental Specialties, Tulsa, OK, USA) are especially effective in obturating the C-shaped canal system (Fig. 13-35).
A B
C
DE
FIGURe 13-31 a-C, Photographs of mandibular molars with C-shaped orifices. D, Apical view of one of these molars that verifies the C-shaped configuration. e, Root resection verifies the C-shaped configuration.
Hedström files are especially effective for efficient tissue removal. If bleeding persists, then ultrasonic removal of tissue or placement of Ca(OH)2 may be used between appoint-ments to enhance tissue dissolution and removal and control hemorrhage.82 Further ultrasonic instrumentation should be considered to remove tissue and debris in inaccessible areas.
Overpreparation of C-shaped canals should be particularly avoided because only minimal amounts of dentin are between the external root surface and the canal system in these teeth. In some cases, even with adequate local anesthesia, pain persists during canal enlarging and cleaning. Frequent admin-istration of intrapulpal anesthesia may be necessary to keep the patient comfortable until all remnants of pulp tissue have been removed. Ca(OH)2 may be used as an intracanal medi-cament to both neutralize bacteria and dissolve remaining tissue remnants.
Before commencing management of a C-shaped canal, the nature of the challenges in treating these teeth should be foremost in the clinician’s mind:
• The three-dimensional nature of the C-shaped canal must be visualized (Fig. 13-32). It is usually ribbon

A B
DC
FIGURe 13-32 a, Radiograph of mandibular molar with C-shaped canal. B, Microcomputed tomography scan of cross-section of a. C, Longitudinal section of a showing shape of the pulpal space within dentin. D, Shape of pulpal space only. (Sections and photo courtesy Dr. Fan Bing.)
B CA
FIGURe 13-33 a, Mandibular molar in need of endodontic revision. B, Resin model of a C-shaped canal system similar to the tooth being treated. Note the flanges and wide canal configuration. C, Six-month reexamination of completed revision with tooth restored. Patient is symptom free. (Case courtesy Dr. Faisal Amir.)

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 265
FIGURe 13-35 Obturationof C-shaped canals with gutta-percha on thermoplastic core carriers. Note the thorough adaptation of the obturation material despite the variations seen in this type of canal anatomy. (Courtesy Dr. Mary Soo.)
Problem-Solving Challenges in the Tooth With Moderate-to-Severe Canal Curvature
Clinicians who perform root canal treatment deal with root canal curvatures on a regular basis. The level of case difficulty increases with increasing degrees of root curvature. The basic principle of canal shaping has already been discussed in Chapters 8, 9, and 10, with the ultimate shape of the canal at the point of obturation resulting in a continuum of access design, orifice enlargement, length determination, and intra-canal mechanics. In this section, ideas to enhance the prepa-ration of canals of increased curature will be described. Essentially, there is no simple solution to this problem and the management of curved canals improves with experience. Even experienced endodontic specialists face a major chal-lenge with severe canal curvature (Fig. 13-36). Fortunately, the incidence of teeth with severe root curvatures requiring root canal treatment is low.
This discussion will focus on canals with moderate curva-ture such as the one depicted in Fig. 13-37, A. The canal or canals of greatest difficulty will be in the mesial-buccal root. Management begins with the extension of the access cavity. It is not necessary or helpful to make the access cavity exces-sively large overall but it is very helpful to extend the mesial wall of the opening 1 to 2 mm closer to the mesial marginal ridge (see Fig. 13-37, B). The enlargement of the orifices begins with hand files and copious irrigation. Once patency has been established, the hand filing should be especially vigorous toward the mesial and mesial buccal. The intention is to straighten the curvature in the coronal third of the canal. Hand files are followed by Gates-Glidden drills or nickel-titanium orifice wideners. Pressure on the rotary instruments should be mainly to the mesial and mesial buccal. Penetration into the canal should be 2 to 4 mm at the beginning with Gates-Glidden drills and perhaps a bit more with tapered orifice wideners. A ledge is likely to be created or the instru-ment may fracture if it is extended deep into the canal. Recapitulate with hand files often and maintain patency around the curvature.
Once the orifice has been sufficiently enlarged and the coronal third of the canal has been straightened, the preparation of the apical canal space can be done. By elimi-nating some of the coronal curvature, the completion of treatment will be more or less routine for most canals. On mandibular molars the identical approach is effective (see Fig. 13-37, C ). Many useful ideas for canal cleaning and shaping of these canals can be adapted from the next section.
A
B
FIGURe 13-34 a and B, Variations in radiographic anatomy of root treated mandibular molars with C-shaped canals. (Cases courtesy Dr. Faisal Amir.)

266 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
A B
FIGURe 13-36 a, Severe curvature on the mesial-buccal root of a maxillary first molar. B, Posttreatment radiograph indicating obturation 2 mm short of radiographic apex. Treatment was done by an experienced endodontist.
C
A
B
FIGURe 13-37 a, Posttreatment of maxillary molar with moderate curvature in the mesial-buccal root. B, Access cavity placed more mesially for roots with significant curvature. C, Mandibular molar treated in same manner as described for the maxillary molar.

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 267
Zip Ledge Strip
FIGURe 13-38 Diagram depicting key problem areas in S-shaped canal systems. Notice that stripping can occur in areas where external root concavities exist.
BA
FIGURe 13-39 a, Maxillary second premolar with S-shaped root canal system. B, Two mandibular second molars; the mesial roots have S-shaped root canal systems.
Problem-Solving Challenges in the Tooth With an S-Shaped Canal
S-shaped, or bayonet-shaped, canals can be troublesome and challenging because they involve at least two curves, with the apical curve being the most vulnerable to deviations in anatomy, loss of working length, and potential for instru-ment separation (Fig. 13-38). These double-curved canals (in two dimensions) that often have an additional curve (three dimensions) are usually identified radiographically when they traverse in a mesial distal direction. If they also traverse in a buccal lingual direction, they may be identified with multi-ple-angled radiographs or when the initial apical file is removed from the canal and it simulates multiple curves. In these situations, the use of cone-beam computed tomography (CBCT) may be of assistance (see Chapter 2). S-shaped canals are found in maxillary lateral incisors, maxillary
canines, maxillary premolars (primarily second premolars), and mandibular molars (primarily second molars) (Fig. 13-39).
To manage these canal systems, the clinician must approach them with knowledge of the anatomic challenges, experience in the use of both contemporary and traditional instruments, and a thorough assessment of the case at hand. Using a traditional approach with hand stainless steel instru-ments, the following guidelines are set forth. First, the three-dimensional nature of the S-shaped canal must be visualized mentally, using the radiographic evidence available (see Fig. 13-39, A). Second, multiple concavities along the external surfaces of the root and the approximate positions of both the curves and concavities must be anticipated to prevent a strip perforation. Third, the clinician must create an unre-stricted approach to the first curve by skewing the access preparation if necessary. Fourth, shape the coronal curve passively, as the coronal curve is first to facilitate the cleaning and shaping of the apical curve. Irrigate frequently and reca-pitulate as necessary with small files. Fifth, it is usually neces-sary to overcurve the apical 3 mm of the stainless steel file to maintain the curvature of the apical portion of the canal (or use NiTi hand or rotary instruments). In this process, the master apical file should be in the smaller size range (20 to 25), and smaller file sizes are used in this mid-to-apical region with short-amplitude strokes to effectively manage the ana-tomic challenges and prevent stripping and ledging in the apical curve. Anticurvature or reverse filing in the coronal curve is used, with primary pressure placed away from the curve of the coronal curvature to prevent stripping. Each case will vary depending on the nature of the curvatures, position of the tooth, and skill/experience of the clinician.
If the loss of working length or deviations in anatomy are identified during enlarging and shaping, the same principles of error management apply as those with a straightforward canal system (see Chapter 10). However, focusing on a problem that has occurred in the apical curvature can easily produce an additional problem in the coronal curvature. The

268 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
B
9–12 mm
C
D
A
FIGURe 13-40 a, Attention is paid to skewing the access to minimize entry into the curvatures. B, Determination of the position of the curves and the approximate length over the entire canal from the orifice to the apex. C, Instruments are used around the first curve to open the pathway for deeper penetration. D, Use of various instruments at various depths to ensure a smooth transition in the canal’s pathway.
astute clinician must render careful clinical judgment when managing problems in the apical curve. Once enlarging, shaping, and cleaning have been completed, finger compac-tors are used with either a cold or warm gutta-percha tech-nique to obturate these delicate canal systems. Here also, the core carriers would be ideal.
The use of hand or rotary NiTi instruments has enhanced the ability to manage S-shaped canals (Fig. 13-40). The attributes of these types of NiTi instruments have enabled the clinician to maintain the canal anatomy while cleaning and shaping with a minimum of errors. First, the three-dimensional nature of the S-shaped canal must be visualized mentally, using the radiographic evidence available. Second, multiple concavities along the external surfaces of the root must be anticipated to prevent a strip perforation. Third, the clinician must create an unrestricted approach to the first curve by skewing the access preparation if necessary. Rinse the canal extensively with NaOCl to begin tissue dis-solution. Fourth, create a pathway or glidepath by using
small K-files (No. 8, 10, and 15 minimum) in the canal to loosen debris and create an accessible shape in the multiple curves. PathFiles (Dentsply Maillefer, Ballaigues, Switzer-land) can be used effectively for this purpose. Rinse often and use hand instruments circumferentially, but do not penetrate the apical segment during this initial cleaning and shaping. Apply all NiTi rotary instruments with minimal pressure, allowing the instruments to move through the pathway that has been created and providing a tapered shape to the coronal portion of the canal first. Fifth, develop the shape of the apical portion of the canal after the coronal portion is opened, tapered, and patent. Use irrigants fre-quently and recapitulate as necessary. In the process of enlarging and shaping, maintain a small apical preparation—approximately 20 to 25—with the progressively or continu-ously tapered instruments. Taper the canal from 4% to 8% in the apical portion, thereby creating both a clean canal and one that is sufficiently tapered for good obturation using any technique (Fig. 13-41).

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 269
*References 4, 7, 19, 27, 45, 72, and 74.
B
A
FIGURe 13-42 Various anatomic challenges in root anatomy that require the attention of a specialist. Premolar with three roots (a) and germination with an open apical segment (B).
A
B
FIGURe 13-41 a, Completed root canal treatment on a maxillary premolar with S-curvature. B, completed treatment on a mandibular second molar with S-curvature. Note the change in apical curvature in the canal relative to the root shape.
REfEREnCES1. Al Ansary MAD, Day PF, Duggal MS, et al: Interventions for
treating traumatized necrotic immature permanent anterior teeth: inducing a calcific barrier and root strengthening, Dent Traumatol 25:367-379, 2009.
2. Andreasen JO, Farik B, Munksgaard EC: Long-term calcium hydroxide as a root canal dressing may increase the risk of root fracture, Dent Traumatol 18:134-137, 2002.
3. Andreasen JO, Munksgaard EC, Bakland LK: Comparison of frac-ture resistance in root canals of immature shape after filling with calcium hydroxide or MTA, Dent Traumatol 22:154-156, 2006.
4. Arslan A, Ozel E, Altuyndal H: Various root abnormalities. Report of three cases, N Y State Dent J 74(3):41-43, 2008.
5. Banchs F, Trope M: Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 30:196-200, 2004.
6. Ber BS, Hatton JF, Stewart GP: Chemical modification of ProRoot MTA to improve handling characteristics and decrease setting time, J Endod 33:1231-1234, 2007.
Problem-Solving Challenges in Anatomic Deviations
Most anatomic deviations are the result of genetic altera-tions in tooth development, changes in development of the Hertwig epithelial root sheath as it penetrates into the cancellous bone during root development, or trauma to the developing tooth. These deviations may include extra canals, extra roots (such as the radix entomolaris), dilacera-tions, defalcations, twinning, concrescence, dens invaginatus, dens evaginatus, talon cusps, and combinations of any of the above* (Fig. 13-42). Most of these abnormalities or deviations are rare, with the exception of having multiple root canals or roots on mandibular incisors, premolars, and molars.74 The most important aspect of these devia-tions is the recognition of such by the general clinician and referral to a specialist for treatment planning and management.

270 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
7. Biggs JT, Sabala C: Endodontic implications of anatomical varia-tions and developmental anomalies in maxillary and mandibular anterior teeth, J Okla Dent Assoc 85(2):24-28, 1994.
8. Blayney JR: The biological aspects of root canal therapy, Dent Item Int 49:681-708, 1927.
9. Callahan JR: Sulfuric acid for opening root-canals, Dent Cosmos 36:329-331, 1894.
10. Chueh LH, Ho YC, Kuo TC, et al: Regenerative endodontic treat-ment for necrotic immature permanent teeth, J Endod 35:160-164, 2009.
11. Shueh L-H, Huang GTJ: Immature teeth with periradicular peri-odontitis or abscess undergoing apexogenesis: a paradigm shift, J Endod 32:1205-1213, 2006.
12. Cvek M: Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha: a retrospective clinical study, Endod Dent Traumatol 8:45-55, 1992.
13. de Souza RS, de Souza V, Holland R, et al: Effect of calcium hydroxide-based material on periapical tissue healing and orth-odontic root resorption of endodontically treated teeth in dogs, Dent Traumatol 25:213-218, 2009.
14. Dodds RN, Holcomb JB, McVicker DW: Endodontic manage-ment of teeth with calcific metamorphosis, Compend Cont Educ Dent 6:515-520, 1985.
15. Doyon GE, Dumsha T, von Fraunhofer JA: Fracture resistance of human root dentin exposed to intracanal calcium hydroxide, J Endod 31:895-897, 2005.
16. Duprez JP, Bouvier D, Bittar E: Infected immature teeth treated with surgical endodontic treatment and root-reinforcing technique with glass ionomer cement, Dent Traumatol 20:233-240, 2004.
17. England MC: Diagnostic procedure for confirmation of a sus-pected resorptive defect of the root, J Endod 3:157-159, 1977.
18. Erdem AP, Sepet E: Mineral trioxide aggregate for obturation of maxillary central incisors with necrotic pulp and open apices, Dent Traumatol 24:e38-e41, 2008.
19. Ezoddini AF, Sheikhha MH, Ahmadi H: Prevalence of dental developmental anomalies: a radiographic study, Community Dent Health 24:140-144, 2007.
20. Felippe WT, Felippe MC, Marques MM, et al: The effect of renewal of mineral trioxide aggregate on the apexification and periapical healing of teeth with incomplete root formation, Int Endod J 38:436-442, 2005.
21. Felippe WT, Felippe MC, Rocha MJ: The effect of mineral trioxide aggregate on the apexification and periapical healing of teeth with incomplete root formation, Int Endod J 39:2-9, 2006.
22. Finucane D, Kinirons MJ: Non-vital immature permanent inci-sors: factors that may influence treatment outcome, Endod Dent Traumatol 15:273-277, 1999.
23. Frank AL: Therapy for the divergent pulpless tooth by continued apical formation, J Am Dent Assoc 72:87-93, 1966.
24. Frank AL: Extracanal invasive resorption: an update, Compend Contin Educ Dent 16:250, 252, 254, 256, 259, 260, 262, 1995.
25. Fuss Z, Tsesis I, Lin S: Root resorption—diagnosis, classification and treatment choices based on stimulation factors, Dent Trauma-tol 19:175-182, 2003.
26. Gaitonde P, Bishop K: Apexification with mineral trioxide aggre-gate: an overview of the material and technique, Eur J Prosthodont Restor Dent 15:41-45, 2007.
27. Grover PS, Lorton L: Gemination and twinning in the permanent dentition, Oral Surg Oral Med Oral Pathol 59:313-318, 1985.
28. Guiliani V, Baccetti T, Pace R, et al: The use of MTA in teeth with necrotic pulps and open apices, Dent Traumatol 18: 217-221, 2002.
29. Gutmann JL, Heaton JF: Management of the open (immature) apex, 2, Non-vital teeth, Int Endod J Sep;14(3):173-178, 1981.
30. Ham JW, Patterson SS, Mitchell DF: Induced apical closure of immature pulpless teeth in monkeys, Oral Surg Oral Med Oral Pathol 33:438-449, 1972.
31. Ham KA, Witherspoon DE, Gutmann JL, et al: Preliminary evalu-ation of BMP-2 expression and histological characteristics during apexification with calcium hydroxide and mineral trioxide aggre-gate, J Endod 31:275-279, 2005.
32. Hargreaves KM, Geisler T, Henry M, et al: Regeneration potential of the young permanent tooth: what does the future hold? Pediatr Dent 30:253-260, 2008.
33. Hatibovic-Kofman S, Raimundo L, Chong L, et al: Mineral triox-ide aggregate in endodontic treatment for immature teeth, Conf Pro IEEE Eng Med Biol Soc 1:2094-2097, 2006.
34. Hatibovic-Kofman S, Raimundo L, Zheng L, et al: Fracture resis-tance and histological findings of immature teeth treated with mineral trioxide aggregate, Dent Traumatol 24:272-276, 2008.
35. Hebling J, Pashley DH, Tjäderhane L, et al: Chlorhexidine arrests subclinical degradation of dentin hybrid layers in vivo, J Dent Res 84:741-746, 2005.
36. Hemalatha H, Sandeep M, Kulkarni S, et al: Evaluation of fracture resistance in simulated immature teeth using Resilon and Ribbond as root reinforcements—an in vitro study, Dent Traumatol 25:433-438, 2009.
37. Hong ST, Bae KS, Baek SH, et al: Microleakage of accelerated mineral trioxide aggregate and Portland cement in an in vitro apexification model, J Endod 34:56-58, 2008.
38. Hoshino E, Kurihara-Ando N, Saito I, et al: In vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline, Int Endod J 29:125-130, 1996.
39. Huang GT: A paradigm shift in endodontic management of imma-ture teeth: conservation of stem cells for regeneration, J Dent 36:379-386, 2008.
40. Huang GT, Sonoyama W, Liu Y, et al: The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering, J Endod 34:645-651, 2008.
41. Iwaya S, Ikawa M, Kubota M: Revascularization of an immature permanent tooth with apical periodontitis and sinus tract, Dent Traumatol 17:185-187, 2001.
42. Juriga S, Marretta SM, Niederberger V: Mineral trioxide aggregate (MTA) for apexification of non-vital immature permanent teeth, J Vet Dent 24:274-277, 2007.
43. Katebzadeh N, Dalton BC, Trope M: Strengthening immature teeth during and after apexification, J Endod 24:256-259, 1998.
44. Kogan P, He J, Glickman GN, et al: The effects of various additives on setting properties of MTA, J Endod 32:569-572, 2006.
45. Kremeier K, Pontius O, Klaiber B, et al: Nonsurgical endodontic management of a double tooth: a case report, Int Endod J 40:908-915, 2007.
46. Loulaouzidou E, Lambrianidis T, Beltes P, et al: Role of cementoe-namel junction on the radicular penetration of 30% hydrogen peroxide during intracoronal bleaching in vitro, Endod Dent Traumatol 12:146-150, 1996.
47. Kratchman SI: Perforation repair and on-step apexification proce-dures, Dent Clin North Am 48:291-307, 2004.
48. Marending M, Stark WJ, Brunner TJ, et al: Comparative assess-ment of time-related bioactive glass and calcium hydroxide effects

chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations 271
on mechanical properties of human root dentin, Dent Traumatol 25:126-129, 2009.
49. Lengheden A, Jansson L. pH effects on experimental wound healing of human fibroblasts in vitro, Eur J Oral Sci 103:148-155, 1995.
50. Martin RL, Monticelli F, Bracket WW, et al: Sealing properties of mineral trioxide aggregate orthograde apical plugs and root fill-ings in an in vitro apexification model, J Endod 33:272-275, 2007.
51. Mjör IA: Pulp-dentin biology in restorative dentistry, Chicago, Quintessence Publishing, 2002.
52. Moss-Salaentijn L, Hendricks-Klyvert M: Calcified structures in human dental pulps, J Endod 14:184-189, 1988.
53. Oliveira TM, Sakai VT, Silva TC, et al: Mineral trioxide aggregate as an alternative treatment for intruded permanent teeth with root resorption and incomplete apex formation, Dent Traumatol 24:565-568, 2008.
54. Patel S, Kanagasingam S, Pitt Ford TR: External cervical resorp-tion: a review, J Endod 35:616-625.
55. Rafter M: Apexification: a review, Dent Traumatol 21:1-8, 2005.56. Reynolds K, Johnson JD, Cohenca N: Pulp revascularization of
necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: a case report, Int Endod J 42:84-92, 2009.
57. Roberts HW, Toth JM, Berzins DW, et al: Mineral trioxide aggre-gate material use in endodontic treatment: a review of the litera-ture, Dent Mater 24:149-164, 2008.
58. Rosenberg B, Murray PE, Namerow K: The effect of calcium hydroxide root filling on dentin fracture strength, Dent Traumatol 23:26-29, 2007.
59. Rule DC, Winter GB: Root growth and apical repair subsequent to pulpal necrosis in children, Br Dent J 120:586-590, 1966.
60. Sarris S, Tahmassebi JF, Duggal MS, et al: A clinical evaluation of mineral trioxide aggregate for root-end closure of non-vital imma-ture permanent incisors in children—a pilot study, Dent Trauma-tol 24:79-85, 2008.
61. Schindler WG, Gullickson DC: Rationale for the management of calcific metamorphosis secondary to traumatic injuries, J Endod 14:408-412, 1988.
62. Shabahang S, Torabinejad M: Treatment of teeth with open apices using mineral trioxide aggregate, Pract Proced Aesthet Dent 12:315-320, 322, 2000.
63. Selden HS: Radiographic pulpal calcifications: normal or abnormal—a paradox, J Endod 17:34-37, 1991.
64. Serene TP: Technique for the location and length determination of calcified canals, J Calif Dent Assoc 4:62-65, 1976.
65. Simon S, Rilliard F, Berdal A, et al: The use of mineral trioxide aggregate in one-visit apexification treatment: a prospective study, Int Endod J 40:186-197, 2007.
66. Stefopoulos S, Tsatsas DV, Kerezoudis NP, et al: Comparative in vitro study of the sealing efficiency of white vs grey ProRoot mineral trioxide aggregate formulas as apical barriers, Dent Trau-matol 24:207-213, 2008.
67. Steinig TH, Regan JD, Gutmann JL: The use and predictable placement of mineral trioxide aggregate in on-visit apexification cases, Aust Endod J 29:34-42, 2003.
68. Tait CM, Ricketts DN, Higgins AJ: Weakened anterior roots–intraradicular rehabilitation, Br Dent J 28;198:609-617, 2005.
69. Tanomaru JM, Leonardo MR, Tanomaru Filho M, et al: Effect of different irrigation solution and calcium hydroxide on bacterial LPS, Int Endod J 36:733-739, 2003.
70. Tay FR, Pashley DH, Loushine RJ, et al: Self-etching adhesives increase collagenolytic activity in radicular dentin, J Endod 32:862-868, 2006.
71. Thibodeau B, Trope M: Pulp revascularization of a necrotic infected immature permanent tooth: case report and review of the literature, Pediatr Dent 29:47-50, 2007.
72. Tsesis I, Steinbock N, Rosenberg E, et al: Endodontic treatment of developmental anomalies in posterior teeth: treatment of gemi-nated/fused teeth—report of two cases, Int Endod J 36:372-379, 2003.
73. Tziafas D: The future role of a molecular approach to pulp- dentinal regeneration, Caries Res 38:314-320, 2004.
74. Vertucci FJ, Haddix JE, Britto LR: Tooth morphology and access cavity preparation. In Cohn S, Hargreaves KM, editors: Pathways of the pulp, ed 9, Mosby Elsevier, 2006.
75. Wadachi R, Araki K, Suda H: Effect of calcium hydroxide on the dissolution of soft tissue on the root canal wall, J Endod 24:326-330, 1998.
76. Wesselink P, Bergenholtz G: Treatment of the necrotic pulp. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
77. Weiger R, Kuhn A, Löst C: Radicular penetration of hydrogen peroxide during intra-coronal bleaching with various forms of sodium perborate, Int Endod J 27:313-317, 1994.
78. Witherspoon DE, Ham K: One-visit apexification: technique for inducing root-end barrier formation in apical closures, Pract Proced Aesthet Dent 13:455-460, 462, 2001.
79. Witherspoon DE, Small JC, Regan JD, et al: Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate, J Endod 34:1171-1176, 2008.
80. Yang SF, Rivera EM, Baumgardner KR, et al: Anaerobic tissue-dissolving abilities of calcium hydroxide and sodium hypochlorite, J Endod 21:613-616, 1995.
81. Yilmaz A, Tuncel B, Serper A, et al: C-shaped root canal in a maxillary first molar: a case report, Int Endod J 39:162-266, 2006.
82. Zehnder M, Grawehr M, Hasselgren G, et al: Tissue- dissolution capacity and dentin-disinfecting potential of calcium hydroxide mixed with irrigating solutions, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:608-613, 2003.
RECommEnd AddItIonAl REAdIngFan B, Cheung GS, Fan M, et al: C-shaped canal system in mandibular
second molars: Part I—anatomical features, J Endod 30:899-903, 2004.
Fan B, Cheung GS, Fan M, et al: C-shaped canal system in mandibular second molars: Part II—radiographic features, J Endod 30:904-908, 2004.
Fan B, Gao Y, Fan W, et al: Identification of C-shaped canal in mandibular second molars, Part II: the effect of bone image super-imposition and intraradicular contrast medium on radiograph inter-pretation, J Endod 34:160-165, 2008.
Fan B, Min Y, Lu G, et al: Negotiation of C-shaped canal systems in mandibular second molars, J Endod 35:1003-1008, 2009.
Fan B, Yang J, Gutmann JL, et al: Root canal systems in mandibular first premolars with C-shaped root configurations, Part I: micro-computed tomography mapping of the radicular groove and associ-ated root canal cross-sections, J Endod 34:1337-1341, 2008.
Fan W, Fan B, Gutmann JL, et al: Identification of C-shaped canal in mandibular second molars, Part I: radiographic and anatomical features revealed by intraradicular contrast medium, J Endod 33:806-810, 2007.

272 chapter 13 | Problem-Solving Challenges in Compromised Roots, Root Canal Systems, and Anatomic Deviations
Fan W, Fan B, Gutmann JL, et al: Identification of C-shaped canal in mandibular second molars, Part III: anatomic features revealed by digital subtraction radiography, J Endod 34:1187-1190, 2008.
Gao Y, Fan B, Cheung GS, et al: C-shaped canal system in mandibular second molars, Part IV: 3-D morphological analysis and transverse measurement, J Endod 32:1062-1065, 2006.
Gutmann JL, Dumsha TC, Lovdahl PE: Problem solving in endodon-tics, ed 4, St Louis, 2006, Mosby.
Min Y, Fan B, Cheung GS, et al: C-shaped canal system in man-dibular second molars, Part III: the morphology of the pulp chamber floor, J Endod 32:1155–1159, 2006.
Ordinola-Zapata R, Bramante CM, de Moraes IG, et al: Analysis of the gutta-percha filled area in C-shaped mandibular molars obtu-rated with a modified MicroSeal technique, Int Endod J 42:186-197, 2009.
Wang X, Thibodeau B, Trope M, et al: Histologic characterization of regenerated tissues in canal space after the revitalization/revascular-ization procedure of immature dog teeth with apical periodontitis, J Endod 36:56-63, 2010.

273
Whenever a pulp is removed and the canal treated and filled in a manner that is compatible with or favorable to a physiologic reaction, we may expect a satisfactory percentage of success. Also, whenever treatment is carried on in such a way as to antagonize biologic processes of repair, we will continue to have many failures.4
J.R. Blayney, 1928
Chapter 14
Problem-Solving Techniques for Revision of Previous Root Canal Procedures
Problem-Solving ListProblem-solving issues and challenges in the revision of previous root canal procedures addressed in this chapter are:
Recommendations for Removal of Existing Restorations
Removal of Restorative Materials from the Pulp Chamber
Techniques for removing intraradicular posts
Removal of Soft Root Canal Filling Materials
Techniques for removing gutta-percha
Techniques for removing paste root canal filling materials
Techniques for removing plastic core carriers
Removal of Metallic Objects from the Root Canal
The ultrasonic instrument
Hedström files
Specialized forceps
Masserann kit
Techniques for removing metallic core-carrier obturators
Removal of Silver Cones from the Root Canal
Prevention of Metallic Instrument Separation During Root Canal Procedures
Removal of Separated Instruments from the Root Canal
Gates-Glidden bur heads, Peeso bur heads, and large metallic fragments
Separated endodontic instruments
Unfortunately, the need for revision of previous nonsurgical (and surgical) root canal procedures is quite common in today’s practice of endodontics. The number of these cases can be largely reduced, however, if adherence to the princi-ples of technical excellence provided in this book is a priority during the initial treatment.1 Sadly, the origin of the majority of recurrent pathosis can be attributed to diagnostic and
If by accident, the instrument used should break—and this is an accident careful handling should make very rare—it will sometimes be found difficult, and it may be impossible, to remove. If not jammed in the fang so as to be immovable, it may, in many cases, be withdrawn by rendering a small instrument magnetic, and passing gently up till it comes into contact with the fragment to be removed. The use of a magnetized instrument was suggested some time ago by the late Dr. John Harris, for a similar purpose. Once or twice during my practice I have found it impossible to remove the broken fragment of the instrument from the fang, and was obliged to fill without regard to it. I have observed no unfavorable results in these cases which I could attribute to this cause.2
R. aRthuR, 1852

274 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
Recommendations for Removal of Existing Restorations
Root canal treatment in general, whether initial treatment or revision, does not usually require the removal of existing crowns. It is in the best interests of the patient to preserve satisfactory restorations, but if by doing so, the ability to revise the previous root canal treatment is compromised, it behooves the clinician to treatment plan the dismantling of the restoration. Similarly, while it is wise to make access cavi-ties as conservative as possible, the access cavity should not be so small as to compromise access to the root canal system and perhaps the quality of the revision. Excessively large access cavities, on the other hand, undermine the retention of existing and usually satisfactory fixed prostheses. In most cases, the size of the access cavity should be the same as one would make for initial treatment.
Revision of root canal treatment can sometimes be accom-plished while preserving existing posts and cores as well. Knowledge of internal tooth anatomy will provide avenues of success without the necessity of post removal. Anatomi-cally wide canals such as the distal canals of mandibular molars or the canals of maxillary second premolars typically have a morphology a preformed stainless steel post will not completely obliterate (Fig. 14-1, A). This fact leads to two clinically useful approaches to revision. The first approach concerns the root that has only one canal. If the post is round
technical inadequacies in the treatment previously provided by others or by the examining clinician. This set of circum-stances is being used by many professionals in other dental disciplines to condemn all endodontic or root canal interven-tions as “an implant in waiting.” The label of root canal or endodontic failure is not the basis for the wholesale extraction of many teeth in favor of implants. In the vast majority of cases, the issue is in reality a dentist failure, or endodontist failure. It is difficult to admit one has failed and proceed to revise the treatment at no cost to the patient or refer the patient to a capable, experienced specialist. It is much easier to condemn the tooth and reap the impending financial rewards of implants than to commit to performing all aspects of endodontic treatment at a higher level. Further-more, there are many cases where a wait-and-watch approach may be warranted, especially when the patient is symptom free and any radiolucency is stable or appears to be reduced.11,19,26
The purpose of this chapter is to provide guidance in the techniques for successful revision of failed nonsurgical treat-ment.12 These cases are more difficult and usually involve compromised circumstances. Also, teeth requiring revision usually have undergone extensive restorations, requiring spe-cialized access techniques not commonly needed for initial treatment. The diagnosis of treatment failure was discussed at length in Chapter 5. This chapter will focus on techniques for removal of restorative and root canal filling materials. Following removal, it is assumed the reader will follow the principles referred to in this text for cleaning, reshaping, disinfecting, and reobturating the canals.
B CA
FIGuRe 14-1 a, Cross-section of a typical maxillary premolar showing unprepared canal space that might be available to bypass an existing post during revision. B, Symptomatic maxillary premolar with inadequate root canal treatment. C, Revision in progress without removal of existing restoration.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 275
distal-buccal root, which had no radiographic signs of patho-sis. Without removing the post and the coronal restoration, access was made through the crown and core, and revision was completed.
Crown or restoration removal becomes a necessity when recurrent caries is found to extend well under the crown margins and is often in fact the etiology of periapical patho-sis. A simple method for removing a full crown is seen in Fig. 14-3, A to D. If the crown is metallic, a fissure bur, long carbide finishing bur or transmetal bur can be used to cut through the crown to the depth of the tooth
and the canal is ovoid, it is possible to negotiate past the post and revise the canal treatment without removing the post or restoration (see Figs. 14-1, B and C ).
Second, in a multicanal tooth, the canal in which the post was placed may not need revision. Again, it may be possible to access a canal with recurrent pathosis or a canal that was previously uncleaned without removing the entire restora-tion. Fig. 14-2 illustrates a case in which a root canal treatment failure was encountered in a mandibular molar with four canals, a large cast post core, and satisfactory crown restoration. Fortunately the post was placed in the
A B
FIGuRe 14-2 a, Inadequate root canal treatment and recurrent apical pathosis in mandibular first molar. Note the post is in the distal buccal root, which has no apical lesion. B, Completed revision of three canals without removal of the cast post-core.
B
C D
A
FIGuRe 14-3 a, Crown indicated for removal due to recurrent caries under margin. B, Beginning at the buccal gingival margin, the crown is cut up the buccal surface and across the occlusal-lingual aspect. Note the underlying tooth structure is not cut. C, Large, flat instrument such as an operative chisel or surgical elevator is used to pry the crown away from the tooth. D, Crown removed.

276 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
CLINICAL PROBLEMProblem: A 43-year-old male presented with symptoms that focused on the maxillary left second premolar area. He stated that the tooth had had root canal treatment and a post and crown, and he could not understand why he was now having a problem. The tissues were slightly swollen in the midroot region of this tooth. Radiographically, there was evidence of root canal treatment with a post and the presence of a large lateral lesion (Fig. 14-6, A). One of two possibilities might explain the cause of the lesion: a post perforation (which did not seem plausible) or a lateral canal. These aberrant canal structures cannot possibly be cleaned and obturated thor-oughly.24 Failure was probably due to the internal exposure of the lateral canal during post preparation. The crown was aes-thetic and worth preserving. Moreover, surgical revision would be extremely difficult, with the location of the lateral canal interproximally on the distal surface of the root.
Solution: Through a routine occlusal access opening, the composite resin surrounding the post was carefully removed, and the post was subjected to ultrasonic vibration with the probe type of tip described above. Revision was completed, and a 7-month reexamination of the patient indicated that the tooth was in full function; radiographically, healing of the lesion was apparent (see Fig. 14-6, B). This problem-solving case points to the importance of approaching each case based on its unique circumstances and assessing all factors before making a plan of treatment.
structure (see Fig. 14-3, B) To preserve as much of the internal structure as possible, the cut should not extend into dentin but may extend into underlying buildup mate-rial. Cut completely from the gingival margin on the buccal vertically and across the occlusal surface onto the lingual surface. The crown is then expanded with any flat-bladed instrument and removed. If the crown is metalloceramic, a diamond bur used for crown preparation will remove the veneer prior to cutting the underlying metal coping with a carbide bur.
Removal of Restorative Materials from the Pulp Chamber
Although standard round and fissure burs are typically used for this procedure as the access preparation extends into the pulp chamber, there is an inherent risk of cutting excessive tooth structure and weakening the tooth. If the pulp chamber is restored with amalgam or composite resin, there is no alternative but to carefully dissect this material with high-speed burs. If, on the other hand, the pulp chamber is found to be filled with a cement such as Cavit (3M ESPE Cavit Temporary Filling Material, St. Paul, MN, USA), zinc oxyphosphate, or zinc oxide eugenol, an ultrasonic handpiece will efficiently remove the restorative material with little effect on the dentinal walls. The ultrasonic tip of choice is usually a prophylaxis tip or a probe shaped tip (Fig. 14-4) used on a moderate to maximum power setting with copious water irrigation. The ProUltra (Dentsply Tulsa Dental Specialties, Tulsa, OK) without water or Start-X (Dentsply Maillefer, Ballaigues, Switzerland) ultra-sonic tips—with or without water—are effective alterna-tives. Gutta-percha is one of the easiest materials to remove by this technique.
The ultrasonic technique is especially useful if the root filling material has a core carrier or is composed of metal. A bur will cut these materials and eliminate the potential to retrieve them using a forceps-type instrument. The removal of zinc phosphate cement from the pulp chamber with the ultrasonic instrument is seen in Fig. 14-5. The entire pulp chamber was cleaned in 3 minutes.
Techniques for Removing Intraradicular PostsIntraradicular posts are used routinely in restoring severely carious or fractured teeth (see Chapter 20). It is not unusual to find a post in a root in which root canal treatment has failed; to revise the treatment nonsurgically, the post must be removed.5 The presence of a post, the difficulty of removing it, and the possible adverse restorative consequences of removal are considered an accepted indication for surgical repair.3 Nevertheless, nonsurgical revision is the treatment of choice in most but not all instances.
FIGuRe 14-4 Probe-type ultrasonic tip.
Although it is possible to remove almost any post with the current technology, the tooth may become so mutilated in the process, prognosis is questionable. For example, after post removal, a short root with thin walls has little hope for a long-term viable restoration (Fig. 14-7). The potential for

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 277
A
B
FIGuRe 14-5 a, Demonstration case: silver cones embedded in zinc phosphate cement. B, Removal of zinc phosphate was done with the probe-type ultrasonic tip. The cement was removed completely in 3 minutes without damage to silver cones.
A
B
FIGuRe 14-6 a, Lateral lesion on a maxillary premolar due to a lateral canal communicating with unsealed canal space prepared for the post. B, Reevaluation of revised root canal treatment after 7 months, showing complete resolution of the lesion.
BA
FIGuRe 14-7 a, Inadequate root canal treatment in a maxillary lateral incisor with a fractured post. B, Successful removal of the post, but a very weak tooth remains. Treatment planning may warrant the consideration of an implant.

278 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
C
B
A
FIGuRe 14-8 a, Fractured post in a maxillary second premolar. Note the inadequate root canal treatment and periapical pathosis. B, Successful removal of the post fragment and revision of the root canal treatment. C, Reevaluation after 30 months, indicating healing of the apical lesion.
retention of a new post is compromised, and the risk of verti-cal root fracture increases. The following case illustrates the problem of the fractured intraradicular post, which can occur with and without concomitant failure of the root canal treat-ment. Unfortunately, this occurrence is labeled incorrectly by many clinicians as an endodontic failure.
Fractures of intraradicular posts are typically observed to occur at or just below the cavosurface margin of the post preparation. They appear to be the result of metal fatigue, not unlike continuous bending of a piece of wire (like a coat hanger) that breaks eventually. In almost all cases of post facture, it is also observed that there was minimal extension of the crown margin past the post/core buildup onto tooth structure. This is often referred to as lack of a ferrule. Several examples are illustrated in Chapter 20. Ini-tially after placement, a crown restoration under function has support from the core cement bond to the surface of the tooth and the post. Eventually, the cement bond between the core and the tooth surface will fail, and the post becomes the sole support for the crown. This will be undetectable clinically until the post fatigues and breaks, and the crown falls out. Prevention of post failure focuses on preservation of as much tooth structure as possible in the initial carious excavation. If there is minimal tooth structure remaining, crown lengthening (see Chapter 17) is an excellent solution.
CLINICAL PROBLEMProblem: A 55-year-old male presented with a fractured post in the maxillary right second premolar. In addition, the root canal treatment was less than acceptable, resulting in recurrent periapical pathosis (Fig. 14-8, A). The patient was having no pain but faced the dilemma of either having the tooth removed and an implant placed or trying to have the post removed and the entire treatment revised. Problem- solving considerations must include a full explanation of the treatment possibilities and outcomes, including the potential for implant failure. The clinician can give guidance to aid the patient in making the choice but should not make the choice of treatment for the patient.
Solution: Following a thorough discussion of the treatment options and potential outcomes, the patient opted to retain the tooth. The post was removed using ultrasonic techniques, and the root canal treatment was revised. The root canal was filled slightly short of the divergent apical canal walls using a custom-fit gutta-percha cone and a root canal sealer that included mineral trioxide aggregate (MTA) powder (see Fig. 14-8, B). The patient returned for reexamination at 12 months. He was symptom free, and the tooth was restored to function with a post and crown. At the 30-month reexamination, healing was almost complete, and the patient was still symptom free (see Fig. 14-8, C). This case illustrates that a conservative choice of treatment usually has a positive outcome and points to the importance of approaching each case based on its unique circumstances.
With the availability of ultrasonic devices, removal of intraradicular posts has become much easier, and there is less risk of physical damage to the root compared with levering types of post removers or pullers. In addition, specialized tips are available designed to apply energy to the post.
Posts can be removed successfully from the inside of full crowns in molar teeth, as illustrated in Fig. 14-9.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 279
C
BA
FIGuRe 14-9 a, Mandibular first molar bridge abutment with inadequate root canal treatment. Clinically, a drainage tract had been present for months. B, Following removal of two posts and renegotiation of the canals. C, Reevaluation after 1 year, indicating complete periapical healing.
Through a traditional access opening, the coronal restorative material was dissected from the post circumferentially with surgical length half-round burs. It was necessary to remove the surrounding material to the level of the orifice at least on the mesial, buccal, and lingual surfaces. The post mate-rial extending into the pulp chamber was freed from the restorative material prior to use of the ultrasonic device. Sometimes it is advantageous to apply lateral pressure on the post with a hand instrument inside the access cavity to observe even slight movement. This will break the bond with any remaining restorative material. Using the ultrasonic tips previously mentioned, more often than not the post can be loosened using midrange to high energy levels, depending on the ultrasonic unit. A conventional heavy-gauge scaler tip will also suffice. If the cement luting the post has also degraded from coronal or apical leakage, ultra-sonic vibration will often loosen the remaining portion of the post in a few seconds.
If the post cannot be removed with ultrasonic application only, a Masserann trephining bur (MicroMega SA, Besançon, France)28 is selected that has a diameter slightly larger than the post. The Masserann kit will be described later in the section on removal of metal fragments from the canal, but at this point, the trephine, which is a tubular drill, will effectively prepare a narrow space around a post sufficient to allow the ultrasonic instrument to vibrate it loose (Fig. 14-10). Since the trephines are made of stainless steel, they
will not be effective if composite resins, amalgam, or glass ionomer cements remain around the base of the post. The ultrasonic device is useful for the removal of fragments of these materials if they have been reduced sufficiently with burs. After removing the restorative material in the center of the pulp chamber, often it is helpful to bend the post to remove additional restorative materials behind it. For example, if the post is in the distal root and surrounded by composite filling material, bend it to the anterior after remov-ing the composite from the more accessible mesial side. This will enable further removal of composite on the distal side with surgical-length small round burs.
In the case of fractured posts, access is no problem, but the margins of the fractured end of the post must be troughed with a half-round bur or the ultrasonic instrument in advance of the trephine. With copious irrigation, frequent pauses to clean the bur, and slow penetration, a space is created around the post fragment to a depth of approximately half the post length. During use, it is important to inspect the bur for flaring and to resharpen it. Since the post is metal, there is no danger of cutting into it or of straying from it into the root. The drilling normally will take between 5 and 10 minutes.
Once the space has been created around the post, the ultrasonic device is used on the maximum setting with a vibrating tip against the exposed end of the post.8,15 Ultra-sonic vibration of the post may take from 30 seconds to 10

280 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
C D
A B
FIGuRe 14-10 a, Masserann trephining bur. B, Fractured post in a maxillary lateral incisor. C, Use of the trephine to create space around the post prior to application of ultrasonic instrument. Approximately half the post length must be exposed for successful removal. D, Post removed.
minutes before mobility is detected. The post fragment can then be teased out of the canal. If there is no mobility after 10 minutes of continuous vibration, the Masserann bur should be used to deepen the space around the post another few millimeters, after which the ultrasonic probe is applied again in the same manner.
Occasionally the most difficult part of post removal is getting the loose post fragment out of the canal because of the very limited space around it and the lack of post material
above the occlusal surface on which to grasp with an instru-ment. The usual approach is continued ultrasonic vibra-tion.18,29 Other aids that have worked successfully are the ultrasonically energized endodontic file in the space along-side the post, or a tightly fitting Masserann extractor that can effect removal by friction. If available, any section of stainless steel tubing, such as a section of a very large-gauge hypodermic needle, can be attached with cyanoacrylate cement.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 281
the maxillary central in Fig. 14-12, this is a very effective and rapid approach to gutta-percha removal.
• Establish access to the entire pulp chamber, eliminating dentinal overhangs or constrictions around the access opening.
• Enlarge the coronal 5 mm of the palatal or lingual aspect of the canal using a No. 5 or No. 6 Gates-Glidden (GG) drill to provide a more straight-line path of removal for the filling material. This operation is done even if this involves removal of some of the root filling material itself, which will present no difficulty for the bur.
• Screw a large-size Hedström or K-file (No. 45 or greater) into the gutta-percha material, and pull the file out (see Fig. 14-12, B). If the file proves too difficult to withdraw by hand, a surgical needle holder (preferably with carbide jaws to reduce slippage) can be used to lever the file against the occlusal or incisal edge of the tooth in the manner shown in Fig. 14-12, C. If the instrument pulls out leaving the gutta-percha filling material, a larger-sized instrument is then inserted, and the procedure is repeated. In most cases where removal is successful, the gutta-percha will come out in one piece after the first or second attempt (see Fig. 14-12, D).
• If this approach fails, the coronal canal space is already prepared for the use of rotary instruments (see Fig. 14-12, E). The technique will be the same as described later for small canals. This method will seldom completely remove the material in large canals, but it will quickly reduce the amount remaining in the canal, after which the remainder in the apical third can be removed with hand files.
Small CanalsThe Hedström file technique is also viable for small canals but is unlikely to remove the entire filling in one piece, and the smaller-diameter files required are more prone to fracture if they are screwed into the gutta-percha. To devise a plan for removing gutta-percha from small canals, no one hand-instrument technique is effective or recommended to clear the entire canal. It is helpful to consider which techniques are more useful in the coronal half of the canal and which are more appropriate for the apical half, especially in the presence of curves.
Gutta-Percha Removal in the Coronal Half of Small CanalsRotary Nickel-Titanium Technique Nickel-titanium (NiTi) files normally used for canal preparation can be used for gutta-percha removal as well.23 The instruments can remove gutta-percha at normal preparation speeds for shaping the root canal (250 to 400 rpm) but are more effec-tive at higher speeds (500 to 700 rpm) owing to thermoplas-ticization (Fig. 14-13). ProFile and ProTaper instruments (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA; Dentsply
Another option that can be used with fractured threaded posts is a combination of ultrasonic vibration and cutting a slot across the top of the post to serve as purchase for a small screwdriver. The slot can be made with a No. 1
2 to 1 round bur or 331
2 inverted cone. A small jeweler’s screwdriver is placed in the groove, followed by application of ultrasonic vibration. Pressure is applied in a counterclockwise fashion on the screwdriver during vibration (Fig. 14-11, A and B). This approach is very useful when the fractured post has no place for lateral purchase and troughing would be dangerous owing to root configuration.
Removal of Soft Root Canal Filling Materials
Techniques for Removing Gutta-PerchaLarge CanalsHedström File TechniqueWhen the need for treatment revision is identified in the case of a poorly obturated, relatively large diameter canal, such as
B
A
FIGuRe 14-11 a, Fractured post in a maxillary lateral incisor. B, Removal with a jeweler’s screwdriver.

282 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
A B C
D
E2
E1
E3
FIGuRe 14-12 a, Inadequate root canal treatment in a maxillary right central incisor. B, Removal of gutta-percha in one piece with a large Hedström file. C, File retrieval assisted with a surgical needle holder. D, Hedström file with removed gutta-percha. Note the fluting of the file is ideally designed to engage the filling material on withdrawal. e, Nickel-titanium rotary instruments for gutta-percha and paste removal. (e courtesy Dentsply Tulsa Dental Specialties, Tulsa, OK, USA.)
B CA
FIGuRe 14-13 a, Rotary nickel-titanium file for removal of gutta-percha. B, Instrument is rotated at 500 to 700 rpm to soften the material. C, Gutta-percha adhering to the instrument.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 283
• The instrument can be a plugger or spreader made of metal designed to be heated (if not, the instrument will be unusable for its intended purpose after just a few heatings) or a specific heat-transfer instrument. It is heated until it is cherry red and then plunged into the gutta-percha.
• The instrument is left in the softened gutta-percha for no more than 1 to 2 seconds. Usually the gutta-percha will have an ideal consistency for removal.
• The process is repeated, and gutta-percha is sequentially removed as the technique is continued into the canal.
• The disadvantage of this approach is that it is relatively ineffective for old gutta-percha that has lost its plasticity with age.
Ultrasonic Technique Currently available ultrasonic units designed for endodontic use possess enhanced energy to soften even old, hardened gutta-percha material (Fig. 14-15).
• Using a probe-type tip or even a standard prophylaxis tip, the machine is set on moderate to maximum power. If the ultrasonic instrument has been used to remove materials from the pulp chamber, it is easy and uncomplicated to extend the tip into the orifices of the canals at the same time. This will also help to locate the canals and clarify the internal anatomy.
Maillefer, Ballaigues, Switzerland) have been advocated for removal of gutta-percha in the coronal half of the canal. One of the newest and most consistent techniques uses NiTi rotary retreatment instruments. In particular, the D-series revision instruments have been designed with descending tapers (.09→.08→.07) to permit removal of the bulk of gutta-percha from the coronal portion of the canal, opening a pathway to the apical half of the canal (D-files [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]; see Fig. 14-12, E). These instruments rotate between 500 and 700 rpm and soften and remove the gutta-percha by creating frictional heat in addition to their mechanical activity in the canal. They are designed to be used in a crown-down manner, reaching depths up to 22 mm and moving around curves without deviation or destruction of root walls. The first instrument has a cutting tip and is limited to a depth of 16 mm, which is ideal to remove the coronal half to two-thirds of the material in most canals. The remaining two instruments have modified tips to prevent gouging into the root walls. Depending on the length of the canal, removal in the apical few millimeters may require the use of a hand instrument.7,9,13
Heat Technique Heated instruments have been recom-mended to remove the gutta-percha from the orifices and coronal third to half of the canal space (Fig. 14-14).
A B C
FIGuRe 14-14 a, Heated endodontic plugger used for gutta-percha removal. B, The heated instrument is plunged into the canal. C, Melted gutta-percha adhering to the plugger.
B CA
FIGuRe 14-15 a, Ultrasonic instrument used for gutta-percha removal. B, Probe tip is used on a high power setting. C, Gutta-percha material adhering to the ultrasonic tip.

284 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
Gutta-Percha Removal in the Apical Half of Small Canals
Rotary Nickel-Titanium Technique Once again, with NiTi rotary instruments, thermal softening of the gutta-percha by frictional heat is the goal. This is the reason for higher speeds, but it is not the intention at this point to begin reshaping the canal. Therefore, the taper and the file diameter must always be smaller than the canal size to prevent binding and instrument fracture.
Possible techniques favored by the authors for removing the gutta-percha filling at this point include the following. (Note: all techniques must be tailored to the challenges of each case and are dependent on the clinician’s experience and expertise.)
Technique A
• Use a .06 No. 25 ProFile run at speeds of 500 to 700 rpm, depending on canal anatomy.
• Proceed carefully while the material is plasticized.• Use a sequential plunge-and-withdrawal technique
to go deeper into the canal.• Use copious irrigation throughout the procedure.• Use the solvent to remove the remainder of the
gutta-percha along with the instrument segment, if an instrument should separate.
B C
D E F
A
FIGuRe 14-16 a, Gates-Glidden drill used for gutta-percha removal. B, Instrument is used at high rpm and will follow canal. C, Thermoplasticized material adhering to the drill. D, Peeso reamer used for gutta-percha removal. e, The instrument is used in a manner identical to the Gates-Glidden drill. F, Removed gutta-percha.
Caution:Do not use a Peeso bur in a curved canal.
Caution:When in contact with the walls of the access in the metalloceramic or full-ceramic crown, the ultrasonic probe may cause delamination or fracture of any porcelain veneer material around the access cavity opening.
• With copious irrigation, the tip is inserted into each canal orifice. The gutta-percha will soften immediately and come out of the canal.
• Depth of penetration into the canal will be limited by the length of the tip.
Gates-Glidden or Peeso Bur Technique These burs are in common use for orifice widening. They can be used in canals filled with gutta-percha as well (Fig. 14-16). The material will not alter the effectiveness of the burs to both enlarge the orifice and remove the gutta-percha simultane-ously. If larger instruments are used, they may do some unwanted cutting on the dentin walls and must be used carefully in canals that anatomically deviate rapidly in the coronal third.
• The basic approach is “crown down” using a No. 4 GG bur or a No. 2 Peeso bur to open the orifice to a depth of 2 to 3 mm.
• A No. 3 GG bur is used to extend another 2 mm.• Finally, a No. 2 GG bur extends the preparation and the
gutta-percha removal another 2 to 3 mm to complete this first phase of removal.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 285
may be uninstrumented or difficult to access. It is usually better to use this method after the bulk of material has been removed by other techniques. (Solvent may also cause movement of the old filling material into the dentinal tubules, thereby preventing access for medicaments to reach potentially embedded bacteria.)
• Removal of some root canal sealers may be enhanced through the use of EDTA (ethylenediamine tetraacetic acid) and NaOCl (sodium hypochlorite).17
Techniques for Removing Paste Root Canal Filling MaterialsThe presence of paste filling materials in the root canal is usually easy to detect on a radiograph. Paste materials typi-cally have “bubbles” or air voids because a lentulo spiral instrument was used to augur the unset material into the canal during filling. The density of the material often varies radiographically within the same tooth. Sometimes the mate-rial will appear to be gutta-percha, and the paste is discovered only after access is made into the tooth. Visually it may appear as gray, white, or reddish.
On opening into a canal filled with a paste, the material usually looks and feels as though it had never set, or as though it had been dissolved by the action of the tissue fluid that has diffused through the unsealed apical foramen. It is usually soft, even mushy to the explorer. Any hand file or rotary file may be used to remove most of the remainder of the material, after which routine cleaning and shaping of the canal may begin.
Fig. 14-18, A illustrates a typical case of a failing paste-filled root canal. The treatment had been done approximately 7 years prior to the onset of pain to biting. The discomfort was confirmed during the oral examination. The paste filling material does not extend to the radiographic apex in the mesial root, and there is no apparent treatment of the distal root. The canal spaces apical to the filling material appear calcified or not negotiated. Following access to the pulp chamber, the paste filling material was removed easily, and fortunately all three canals proved to be negotiable The
Technique B
• Choose a ProTaper finishing instrument that is slightly smaller than the root canal filling as estimated from the radiograph. (Note: ProTaper finishing instruments have the same sizing as ProTaper D retreatment/revision instruments, only in reverse; that is, the D1 has a taper of .09, whereas the F3 has a taper of .09, and so on.)
• Place a small amount of solvent in the chamber.• Using speeds of 300 to 500 rpm, allow the instrument
to move gradually but steadily into the gutta-percha material to approximately two-thirds to three-fourths the length of the canal; further, safe penetration can be achieved using the ProTaper hand instrument of the same size.
• Withdraw the instrument frequently to wipe the material from the cutting edges and flutes of the file.
• Use copious irrigation throughout the procedure.• ProTaper retreatment/revision instruments are also
effective when applied at speeds of 500 to 700 rpm (see Fig. 14-12, E ).
Solvent Technique A long-used method of removing gutta-percha and sealer from a root canal is softening the gutta-percha with a solvent such as methylchloroform, rectified white turpentine, or eucalyptol (Fig. 14-17).13 Solvent is especially useful in canals with ledges or other obstructions which limit the use of rotary files. This would also be the method of choice if during the use of the rotary technique, a section of NiTi file separated in the gutta-percha material.
• Once the orifice of the canal has been uncovered, fill the access cavity with solvent. The solvent must not be allowed to run onto the dental dam because it will denature both natural rubber and vinyl, and a large hole will quickly result.
• After 1 or 2 minutes, the solvent in the pulp chamber will dissolve the gutta-percha to the extent that a No. 15 or 20 K-file will easily negotiate the canal.
• Begin reshaping and cleaning of the canal.• Solvents make thorough removal difficult; dissolved
gutta-percha tends to flow into areas of the canal that
CBA
FIGuRe 14-17 a, Removal of gutta-percha with solvent. Solvent should fill the pulp chamber. B, After 2 or 3 minutes, the dissolved gutta-percha is removed with hand files. C, Dissolved material wiped on a cotton roll.

286 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
CA B
FIGuRe 14-19 a, Paste filler in a maxillary central incisor. B, Following post removal. C, Completed revision.
symptoms resolved shortly after the initial débridement, and the treatment was completed without complications (see Fig. 14-18, B).
The unsuccessful use of paste fills can be found in both posterior and anterior teeth. In Fig. 14-19, A the coronal restoration is aesthetic and worth preserving. The adjacent central incisor was diagnosed as having a necrotic pulp and also in need of a primary root canal procedure. Through a routine access opening, the post was retrieved by careful removal of the surrounding composite resin and ultrasonic vibration. The disintegrated paste filler was easily removed with a hand file and irrigation (see Fig. 14-19, B). Root canal treatment for the left central incisor was completed simultaneously with the revision of the right central (see Fig. 14-19, C ).
Although most paste filling materials are largely zinc oxide eugenol in composition and are soluble in solvents, the ultra-sonic instrument is much more effective in removing set material. Rotary NiTi instruments are equally effective for
this procedure. If a case is encountered in which the material appears hard set deep into the canal orifice, solvents may help after removing as much of the paste as possible with the ultrasonic instrument. Usually the remaining material is soft enough to be penetrated with either hand or rotary instru-ments, but the exceptional case may benefit from the use of a solvent. In some cases, the paste will be impenetrable, or a calcified dentinal bridge will block further access into the uncleaned apical canal space. Periapical surgery may be the only recourse if pathosis exists in the periapical tissues (see Chapter 16).
Techniques for Removing Plastic Core CarriersUnfortunately, identification of a plastic core carrier on the preoperative radiograph may be difficult insofar as it may not be distinct from the gutta-percha material that surrounds it.
A B
FIGuRe 14-18 a, Paste filler used in a mandibular first molar. B, Completed revision. The paste is usually easy to remove.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 287
flared, gutta-percha adaptation to the walls may exhibit voids or gaps in the fill, especially in the proximal dimension. This gives the clinician a false sense of the quality of the obturation.
Proper access openings are also necessary when core- carrier techniques are used (Fig. 14-21, A). If the access is improperly shaped or insufficiently large, the softened gutta-percha will be stripped from the core carrier as it is placed into the canal. Because core carriers are flexible, they can lodge under ledges of the pulp chamber in anterior teeth or pulp chamber roofs or horns in posterior teeth. This creates significant problems when attempting to gain access to the chamber during revision while protecting the coronal exten-sion of the core carrier.
It may be impossible to preoperatively associate the cause of failure with the problems of this filling technique (Fig. 14-20). To understand the problems encountered in remov-ing the plastic core carriers, the major reasons for the need for revision when using this method of obturation must be discussed.10 First, the canal preparation must be a continu-ously tapered funnel (see Chapter 10). It is commonly observed that canals intended to be obturated with core car-riers are underprepared. The lack of taper may allow the core carrier to reach the prepared apical seat, but the movement of the gutta-percha is impeded. The result is a stripping of the gutta-percha from the core due to frictional binding and a consequent lack of gutta-percha at the apex to provide the necessary seal. Conversely, if the canal is too large or too
BA
FIGuRe 14-20 a, This diagnostic radiograph includes a sinus tract exploration with a gutta-percha point. B, One-year reevaluation after complete revision indicates excellent resolution of the apical pathosis. (Case courtesy Dr. Erick Menegazzo.)
CBA
FIGuRe 14-21 a, Access cavity for revision should be approximately the same as routine root canal treatment. B, Removal of filling materials in the pulp chamber should be done with care to avoid cutting core carriers. C, Gutta-percha can now be removed from the pulp chamber with the ultrasonic instrument.

288 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
The technique for removal of plastic core carriers must begin with the removal of all restorative materials, endodon-tic cements, and excess gutta-percha from the pulp chamber (see Fig.14-21, B). If the pulp chamber contains only cement-based materials, Cavit, gutta-percha, or root canal sealers, an endodontic ultrasonic instrument with the probe tip on a high setting for débridement is used on the pulp chamber floor, in the same manner as described for gutta-percha and paste removal. The ultrasonic probe will not degrade the core material so long as contact is brief. As with removal of any root filling material, if the pulp chamber is restored with any of the permanent materials such as composite, glass ionomer, or amalgam, extreme care must be taken during their removal with the high-speed bur to avoid cutting the core-carrier material. Once the pulp chamber is prepared and the plastic core carriers are free from surrounding materials (see Fig. 14-21, C), the following techniques and considerations may be incorporated into the revision approach:
• Use a grasping instrument or small forceps if the plastic core carrier is long enough and reachable. The Stieglitz forceps or the Peet splinter forceps, among others, are suitable for this purpose (Fig. 14-22).
• Use the Hedström file technique without solvent.27 Screwing one or more Hedström files (No. 25 to 35) into the coronal canal space will engage the plastic core material in the flutes. It is often necessary to use a surgical needle holder for leverage because the Hedström file will be very resistant to retrieval. The plastic core will be retrieved completely in many cases without additional steps (Fig. 14-23). Most often the gutta-percha material will remain in the canal and must then be removed by one of the methods described earlier for gutta-percha.
• Flood the pulp chamber with chloroform. After a couple of minutes, the gutta-percha surrounding the plastic core carriers becomes softened, enabling a Hedström file to become easily engaged in its surface.14
• Solvents can be reintroduced into the canal if only a portion of the plastic core comes out. The remainder of the core is “instrumented” away slowly. Other solvents such as xylene, eucalyptol, and halothane do not soften the gutta-percha as readily as chloroform.
• Use a NiTi rotary file at high speed (1400 rpm), as with the removal of gutta-percha. The core material will become softened by friction and will either spin out of the canal space or will be removable by further filing. Alternatively, use a ProTaper retreatment file (D1-D3) or finishing file (F1-F3) that will macerate the plastic core as it cuts apically in the canal, or in some cases may result in removal in toto.
If extensive canal irregularities are present (e.g., fins, webs, culs-de-sac), the softened gutta-percha may lock the carrier into its position. Removal with a grasping instrument may be difficult, even after softening with a solvent. Likewise, if a file is being used with solvent to remove the gutta-percha
A B
FIGuRe 14-22 a, Specialized forceps for removal of plastic and metallic core carriers. B, Removed plastic core carriers.
A
C
B
FIGuRe 14-23 a, Braided Hedström files used to remove a plastic core carrier. B, Retrieval of the Hedström files aided by a surgical needle holder levering against a cusp. C, Core carrier retrieved.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 289
along the length of the carrier, the carrier may be severed, thinned, or pushed into the canal irregularities, especially with the smaller, more flexible carriers. If this occurs, it may give the impression that the canal is being cleaned, when in actuality the carrier is being slowly cut by the filing action. Radiographic checks during removal attempts will provide evidence that a portion of the carrier is still present, yet the canal may feel “smooth and clean” to the clinician. A curved or bent Hedström file can be used to engage the adherent section of the plastic carrier for removal. This approach also favors canal cleaning and shaping. Although the majority of plastic core carriers can be routinely retrieved—even those extending beyond the apical foramen—apical surgery cannot be excluded as a possibility for some of these cases.
Removal of Metallic Objects from the Root Canal
Various specialized strategies have been developed for instru-ments that can be used routinely for the revision of treat-ment, and some instruments are designed specifically for this purpose.
The Ultrasonic InstrumentThe use of the ultrasonic instrument has already been dis-cussed with respect to the removal of cements and debris from the pulp chamber surrounding plastic core carriers. This technique uses a prophylaxis or probe-type tip (see Fig. 14-4). The same technique will also apply to the removal of metallic carriers, with the added advantage that there is no effect from the ultrasonic tip on the stainless steel core, so the device can be used on a higher or even maximum power setting, depend-ing on the unit without fear of weakening the carrier.
• Using the probe tip will often remove any calcified tooth structure in the orifice area that was not removed initially.
• The probe tip can apply ultrasonic energy directly to the metallic core with the object of loosening it. If corrosion and loss of sealer has occurred, the probe tip may loosen a failing silver cone and cause it to come out completely. This will rarely if ever happen with a metallic core carrier. If used directly on a segment of NiTi file, the file will usually break off.
• The probe tip will excavate dentinal tooth structure around an embedded fragment, similar to its use in exploring for a calcified canal. It will also excavate dentin circumferentially in the orifice area and longitudinally parallel to a metallic fragment in some roots (Fig. 14-24).
• An endodontic file can be attached to the ultrasonic instrument (Fig. 14-25), which can débride the canal of cements and paste filling materials.
• An ultrasonically energized endodontic file can enlarge root canal spaces alongside embedded metallic fragments.
A B
FIGuRe 14-24 a, Trenching around metallic fragment by ultrasonic instrument. B, Removal of the fragment with a specialized forceps.
B
A
FIGuRe 14-25 a, Ultrasonic mounting for an endodontic file. B, Application of the ultrasonic file to enlarge space around a metallic fragment.
In this application, it will usually be necessary to create a pathway by hand instrumentation prior to introducing the ultrasonic instrument. Occasionally, this strategy also may also loosen the object and remove it.
Hedström Files• Hedström files are generally useful to enlarge a space in
the canal adjacent to a silver cone, fractured instrument segment, or plastic core carrier. The use of rotary files against metal objects increases the risk of breakage,

290 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
Specialized ForcepsAs mentioned earlier, several specialized forceps are available for removing metallic objects. All have narrow beaks that will extend into a reasonably conservative access opening (see Fig. 14-22, A). The Steiglitz (right) forceps is a grooved, needle-nosed pliers that is often too bulky to use in small access openings. The Peet splinter forceps (left) are generally more useful because the taper on the beaks is more gradual, allow-ing freedom for beak separation and grasping the metallic object in deep access openings. Equally useful alternatives are Perry gold foil pliers and Hartman 31
2-inch curved mosquito forceps (Miltex, Inc, York, PA, USA). Any of these instru-ments is useful for removing a loosened silver cone, a loose separated endodontic file fragment, or the shaft of a GG drill from the pulp chamber (see Fig. 14-24, B).
Masserann KitA useful and versatile system for retrieving metallic objects from canals is the Masserann kit (Fig. 14-27, A). This kit contains a series of tubular trephining drills, the largest of which were discussed earlier in the removal of endodontic posts. In addition, there are two sizes of tubular extractors (1.2 and 1.5 mm) (see Fig. 14-27, B). If a significant portion of the metallic object extends into the pulp chamber, only the extractor may be needed to remove it. The tubular extrac-tor is placed over the object, and the plunger is screwed until tight. This will lock the object against a knurled ring in the
which compounds the difficulty. Initial negotiation usually begins with Nos. 6, 8, and 10 K-type files. Once these files have opened a pathway, the Hedström file can rapidly enlarge the space for either bypassing an embedded file or using the ultrasonic instrument to dislodge it.
• If there is a space into which a No. 25 to 35 or larger Hedström file can be partially inserted, it can be further “screwed” into a deeper position, taking care not to stress it to the point of breakage. The metallic object may be dislodged and may come out as the file is withdrawn directly from the canal.
• In a larger canal with ample space surrounding the metallic object, multiple files can be placed alongside a silver cone (similar to the previous approach) and are withdrawn simultaneously. This is known as the file-braiding technique (Fig. 14-26).8
• Hedström files will not secure a purchase on other stainless steel files, and the technique will generally not work on metallic core carriers, broken files, lentulo spirals, or GG drills unless the canal shape permits an easy bypass.
• The one exception is the possibility of getting a purchase in the fluting of another file, metal-core gutta-percha carrier, or around the flutes when there is larger spacing in the fluting, such as a Peeso bur. Much time and effort can be spent trying to achieve retrieval without the desired result. This would rarely be the initial technique of choice in these cases.
BA C
FIGuRe 14-26 a, Failed silver cone root canal treatment. B, File-braiding technique to remove the silver cone. C, Silver cone enmeshed in braided Hedström files.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 291
Nevertheless, it may become necessary to revise a case that was obturated in this manner, either because of treatment failure or the restorative need for an intraradicular post.
Whereas plastic core carriers are difficult to distinguish radiographically, metal core carriers typically have the famil-iar spiral appearance of endodontic files (Fig. 14-29). Unlike the previous case (see Fig. 14-28) where the file shape is obvious, the metallic core carrier is surrounded by gutta-percha and can be somewhat disguised, especially with small-diameter carriers. A frequent clue to the presence of metal core carriers is the increased radiodensity of the filling mate-rial in canals that might appear to be underinstrumented. In addition to the mesial buccal root canal in Fig. 14-29, the gutta-percha was stripped from the carrier during placement in the palatal canal, leaving the apical 3 mm of the core carrier denuded.
Revision will begin with access through the existing restoration. If the pulp chamber is filled with Cavit or other softer cements, the ultrasonic instrument will suffice. If the pulp chamber is filled with composite resin or glass ionomer cement, it will be necessary to dissect these mate-rials with the high-speed bur or ultrasonic. Upon removing the restorative material from the pulp chamber, it is espe-cially important to avoid contact between the bur and the metal carrier, as even a small cut or notch will be a weak point at which the metal may break off during the attempt to loosen or remove it. The ultrasonic instrument is highly effective for both removing the surrounding endodontic filling materials in the coronal canal space and loosening the metal core carrier, at least in the coronal third to half of the canal. Since the stainless steel is unaffected by ultrasonic vibration, the device can be used at maximum power, which will help loosen the carrier and remove
tube wall. This mechanism provides adequate retention for removal of most silver cones, metallic core carriers, and some separated endodontic instruments.
If the metallic instrument is cut off at a level preventing use of the extractor, the smaller tubular trephining drills can create enough space in both length and width for eventual placement of the extractor. Once the extractor device is secured to the end of the metallic object, the technique for removal is a gentle pull combined with a slight counterclock-wise rotation. The general idea is to “unscrew” a separated instrument rather than attempt to pull it out directly.
Techniques for Removing Metallic Core-Carrier ObturatorsAlthough never advocated in formal institutions of dental education, some practitioners once embraced the use of end-odontic files for permanent obturation of the canals (Fig. 14-28, A). This is a perfect example of “clinician failure” through the use of inappropriate materials and techniques for root canal treatment. Due to the inherently inadequate seal, the treatment failed and revision was indicated. Following removal of the zinc phosphate cement surrounding the ends of the files protruding into the pulp chamber, the Masserann extractor was used to remove the instruments (see Fig. 14-28, B). Routine root canal procedures were used to complete the revision (see Fig. 14-28).
This case illustrates a removal technique that applies directly to metal core-carrier obturators, since the concept of the core carrier for gutta-percha obturation is derived from a K-type endodontic file coated with gutta-percha. Metallic core carriers have mostly been replaced with plastic.
BA
FIGuRe 14-27 a, Masserann kit. B, Large and small Masserann extractors.

292 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
(e.g., amalgam compactor) can be applied to the carrier two or three times for 5 to 10 seconds each (Fig. 14-30).
• In canals that are wide buccal lingually, a hand or rotary instruments can be used to soften and remove gutta-percha filling material around the core. Sometimes the canal size may allow removal as far as the apical third. This will allow the core greater mobility in the canal space. Ultrasonic vibration may complete the retrieval.
• The specialized forceps technique is very fast and works well if the metal core is fairly loose and long enough to be accessible. Fig. 14-31 documents the revision of a mandibular molar in which the metal core carriers were removed with a Peet forceps. The file-braiding technique might work if the core is very loose but too short to grasp with the forceps.
• A Masserann extractor is especially effective if the metal core has great retention. In the same manner as shown in
surrounding gutta-percha. It is rarely possible to loosen a metal core carrier to the point of removal with ultrasonic vibration alone.
Once ultrasonic vibration is done and the coronal exten-sion of the core is mobile, there are a number of useful ways to proceed to removal:
• As described with removal of plastic cores, additional gutta-percha in the midroot area can be removed by flooding the pulp chamber with solvent and using a small instrument to attempt to bypass the core as far as possible both vertically and circumferentially.
• Heat applied directly to the metallic core, using a Touch ’N Heat or System B (both from SybronEndo, Orange, CA, USA) BeeFill 2in1 (VDW, Munich, Germany); or Calamus® Dual (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), can be helpful to soften the gutta-percha that surrounds the metal carrier deeper in the canal space. In lieu of this, a heated large instrument
A B
FIGuRe 14-28 a, Maxillary premolar with K-type endodontic files as root fillings. B, File retrieval with Masserann extractor.
FIGuRe 14-29 Maxillary molar with grossly inadequate root canal treatment completed with metal core-carrier obturation. Note the stripping of the gutta-percha from the carrier in the palatal root.
FIGuRe 14-30 The apical gutta-percha is softened by placing a heated endodontic plugger against the carrier.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 293
through the coronal buildup and is in contact with a metal-lic restoration or a full crown, either all metal or porcelain with a metal coping. The metal core carrier will often act as a thermistor in the conduction of temperature changes to the vital periapical tissues. In these cases, patients report significant discomfort to heat in a root canal–treated tooth. This problem is especially acute when the core carrier is beyond the root apex or has been stripped of its gutta-percha in the apical third of the canal. A positive response to a heat test on such a tooth would be convincing evidence for revision.
Fig. 14-28, B, the extractor is secured tightly over the end of the metal core, which is virtually the same as an endodontic file. Simultaneously the extractor is both pulled and rotated counterclockwise, thereby “unscrewing” it from the canal space. Pulling directly on the metal core does not usually result in retrieval; friction of the metal against the canal wall or adhesion to the gutta-percha in which it is embedded inhibit withdrawal. The Masserann extractors can be used to expose more of the length of the core to affix the extractor. When the core extends into the pulp chamber, the trephine will easily follow its long axis.
• Carriers that are surrounded by amalgam in the pulp chamber are difficult to distinguish and could be cut off at or below the canal orifice. Some cases present for revision with the obturators already cut off at the level of pulp chamber floor. These circumstances pose a different set of problems in revision because it is impossible to grasp the core remaining in the canal space. Furthermore, passage of a small instrument alongside the metal core may be a technical challenge even with the aid of a solvent. The trephining technique is indicated.
• The technique for loosening would begin with an ultrasonic tip followed by the Masserann trephining burs that would cut a widened space around the metal carrier in the canal orifice. Initially, it is usually more difficult to center the trephine over the metal core owing to the lack of core material in the pulp chamber to follow. This is where the ultrasonic comes in by helping to not only loosen but expose more of the coronal end of the object. Ultimately the goal is to attach the Masserann extractor or instrument retrieval system (IRS) extractor in a stable position and remove in the manner described earlier. This may prove to be difficult and time consuming.
An interesting clinical finding with metal core gutta-percha carriers sometimes occurs if the metal core extends
A B
FIGuRe 14-31 a, Recurrent apical pathosis on a mandibular molar treated with metal core carrier endodontic obturators. B, Retrieval of the metal cores with a Peet splinter forceps after removal of coronal gutta-percha by ultrasonic instrumentation.
CLINICAL PROBLEMProblem: A 26-year-old male with symptoms of acute prolonged sensitivity to cold and spontaneous pain in the mandibular right quadrant was seen for emergency consulta-tion. He could not bite on the first molar without excru-ciating pain. Root canal treatment had been completed 3 days earlier using a metallic core-carrier obturation technique (Fig. 14-32). When cold was applied to the teeth in ques-tion, the main source of the discomfort was the second molar. However, pain to percussion was most intense on the first molar.
Solution: A diagnosis of irreversible pulpitis and normal periapical tissues was made for the second molar and acute apical periodontitis for the first molar. Root canal treatment was initiated on the second molar, and the occlusion was adjusted on the first molar. Percussion pain continued on the first molar for 1 week after occlusal adjustment. After comple-tion of the root canal treatment on the second molar, using gutta-percha and sealer, treatment on the first molar was revised (see Fig. 14-32, B). All symptoms subsided within 2 weeks, and the first molar was obturated with gutta-percha and sealer using lateral compaction (see Fig. 14-32, C).

294 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
irrigation and drying will allow the earliest detection of the silver cone in the surrounding filling material (Fig. 14-34). Once again, if the material filling the pulp chamber is relatively soft, it can be removed entirely with the ultrasonic unit, as was shown in Fig. 14-5. If the filling material is hard and requires removal with a high-speed bur, avoidance of contact between the bur
Removal of Silver Cones from the Root Canal
The use of silver cone root canal fillings has diminished steadily over the past 30 years as research has provided both experimental support and improved techniques for the place-ment of gutta-percha. Nevertheless, cases of treatment failure with this technique continue to appear in practice. Silver cones are distinguished radiographically by a radiodensity consistent with metal materials and uniform, slightly tapering shape (Fig. 14-33).
As a general consideration, the techniques for removing metallic cores will also apply to the removal of silver cones, with some additional cautions and recommendations. As with the other filing materials, careful removal of the pulp chamber restoration material is the first step in this tedious and demanding process.
• Preservation of any extension of the cones into the pulp chamber is critical.
• After the occlusal surface of the final restoration has been penetrated with the high-speed bur, frequent pauses for
C
BA
FIGuRe 14-32 a, Amalgam packed deep into the pulp chamber and canal orifices around metal core carriers. B, Dissection of metal cores in amalgam is difficult. Trephines were used to expose cores in canal orifices that permitted retrieval with the Masserann extractor. C, Completed revision.
FIGuRe 14-33 Silver cone obturation in a mandibular molar.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 295
Masserann extractor is an effective device for silver cone retrieval. Like the retrieval of a metal-core gutta-percha carrier or an endodontic file, the extractor is attached to the silver cone and withdrawn (Fig. 14-36). Caution: No rotational force should be used with silver cone removal. Significant force can be applied, although the surgical needle holder strategy is not recommended because it will collapse and ruin the extractor (even though the removal may be successful!).
• In the absence of a set of Masserann instruments, a similar effect may be improvised with a section of stainless steel tubing, as might be obtained from a large-diameter hypodermic needle. The tubing is placed over the exposed end of the silver cone. A Hedström file is selected by trial and error and “screwed” into the space between the silver cone and the wall of the tubing, locking it in place. The Hedström file and tubing are then withdrawn simultaneously with the silver cone (Fig. 14-37). Like the Masserann extractor, this technique is suited to removing silver cones that are relatively inaccessible by the other methods.
and the silver cone is even more critical than with the removal of a metallic core because of the relatively soft nature of the silver. If the handpiece does contact the silver cone, the cone is weakened and will probably break off at this point later in the removal.
• If a silver cone is loose and accessible, the simplest method of removal is the specialized forceps (Fig. 14-35).
• Single Hedström file: Assuming all filling material has been removed from the pulp chamber, use the ultrasonic probe tip to vibrate in the orifice areas of all canals. This will remove some of the coronal sealer and loosen the coronal extension of the silver cones. If a space can be negotiated alongside the silver cone with small K-type files, the goal would be to enlarge this space by hand instrumentation until a No. 25 to 35 or larger Hedström file can be inserted and “screwed” to a deeper position. Silver is relatively soft, and the Hedström file will gain a purchase in the side of the cone. The file is then withdrawn directly as described previously for the removal of plastic core carriers. Once again, a surgical needle holder may be of use to increase the leverage to effect withdrawal.
• Multiple Hedström files: If one Hedström file does not provide removal and there is sufficient space to accommodate additional files, the file-braiding technique may be applied. The technique is illustrated in Fig. 14-26. In this variation, two or three smaller files (in the No. 20 to 35 range) are placed beside the silver cone as far apically as possible and screwed into position until tight. The Hedström files are then twisted together and are simultaneously pulled out by hand, or again, clamped together with a surgical needle holder and levered out against the incisal or occlusal edge. This technique is especially useful when access is limited or the silver cone does not extend out of the orifice. Even “twist-off ” or sectional silver cones can be removed.
• Occasionally the silver cone will have too much retention for either of the methods described. Once again, the
FIGuRe 14-35 Removal of the silver cone with the Peet instrument.
BA
FIGuRe 14-34 a, Access preparation for revision of a failed silver cone root canal treatment. Note that the access preparation extends only deep enough to visualize the ends of the silver cones. B, Further dissection of surrounding cement should be done with the ultrasonic device as described in Fig. 14-5. NOTE: If the pulp chamber was restored with composite, amalgam, or glass ionomer cements, dissection must be done with high-speed burs or the use of the Start-X ultrasonic system (Dentsply Maillefer, Ballaigues, Switzerland.). Every effort should be made to avoid cutting into the silver. This can be done by cutting as close as possible and using the endodontic explorer to pry the silver cone loose, breaking away any remaining restorative material.

296 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
• Very large-diameter silver cones can be very resistant to removal. There may be no lateral space to negotiate and insufficient silver cone extension into the pulp chamber to engage with instruments (Fig. 14-38, A). Some silver cone cases were treated with a sectional silver cone called the twist-off technique to leave post space. Retrieval of the apical section is sometimes impossible. The only recourse in either case may be apical surgery (see Fig. 14-38, B and C). The surgical procedure is also complicated by the presence of metallic filling material in the apical canal space. Preparation for a retrograde seal can be a technical challenge.
FIGuRe 14-36 Silver cone removal with the Masserann extractor.
FIGuRe 14-37 Silver cone removal with an improvised extractor consisting of a short section of stainless steel tubing from a large-gauge syringe needle and a Hedström file.
A CB
FIGuRe 14-38 a, Irretrievable silver cone. B, Irretrievable sectional silver cone. C, Postapical surgery. Apical preparation with metal in the canal is a challenge.
Prevention of Metallic Instrument Separation During Root Canal Procedures
Prior to a discussion of the removal of fractured or separated instruments, from a problem-solving standpoint, it is appro-priate to consider how this complication might be prevented. Most breakages of metallic instruments in the root canal system can be prevented by knowing how the instruments are manufactured, how they are to be used, and what limita-tions should be placed upon them. In general, all types of

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 297
and maintain canal curvatures has been most beneficial. However, these instruments require a different tactile sensa-tion during working motions. Movements such as aggressive, rapid penetration of the canal, forcing an instrument to an arbitrary length, or forcing an instrument around a curve have led to numerous fractures of these instruments without warning. This also occurs with both rotary and hand instru-ments of all manufacturers. Most of these instruments do not have the standard tapers found in traditional hand instru-ments and therefore lack the same tactile sensations an expe-rienced operator may expect. The best way to deal with the increased possibility of breakage is to practice extensively with these instruments, learning their nuances and develop-ing an acute tactile sensation. Prevention is the operative word in their successful usage. If they should fracture, the techniques for removal identified in this chapter will apply.
Before GG drills or orifice shapers/openers are used to countersink the coronal portion of the canal (some refer to this as preflaring),21,25 a pathway should be established with a hand instrument first. With some systems like the ProTaper, the pathway then allows for an immediate application of the first shaping instrument that in essence eliminates the need for GGs. In fact it is the pathway or glidepath that is devel-oped initially that makes the use of NiTi instruments both effective and safe in their applications in the root canal system. If the GGs are used, short advances of the rotary instrument followed by complete withdrawal will allow the shavings to escape and prevent binding of the bur head in the canal orifice. Copious irrigation is also necessary. The smaller-size burs will almost invariably bind and break if forced. When GGs are used to flare the canal after the use of files, all cutting should be done passively as the drill is withdrawn from the canal. If the orifice-shaping instruments that come with the new NiTi systems are used in sequence during cleaning and shaping root canals, the use of GGs is unnecessary.
root canal instruments are too often used beyond their useful-ness, in a manner for which they were not designed, or with excessive amounts of force (see Chapter 10).
To avoid problems, basic guidelines for using and evaluat-ing intracanal instruments are:
1. Inspect all instruments for irregular windings or evidence of fatigue on stainless steel hand files, NiTi files, and NiTi rotary files.
2. Pass the instrument through a bright light and check for irregularities in the symmetry of the fluting (Fig. 14-39, or shiny spots that indicate unwinding of the instrument. Small stainless steel files will become fatigued but often without visual evidence, so it is wise to test each file by intentionally placing a small curve in the apical 2 to 3 mm before use and recurving it during use.
3. Even good stainless steel instruments separate with only gentle curving. Smaller-sized instruments (Nos. 8 to 20) should be used minimally and replaced automatically if bent or kinked during use.
4. NiTi instruments should never be precurved and should be discarded if one should appear slightly curved after use.
5. Inspect NiTi instruments for irregularities in the fluting, and discard any file that shows even slight deformation (Fig. 14-40).
6. There is a worldwide movement to encourage or even mandate the single use of all root canal instruments, particularly in light of the transmission of diseases. In some countries, single use is mandatory, and the future of endodontics may very well be one that embraces this concept.16,18,20,22
The advent of Ni-Ti hand instruments has had both a positive and a negative effect on the delivery of quality root canal treatment (see Chapter 10). The ability to negotiate
FIGuRe 14-39 Deformity in the fluting of a file indicates metal fatigue. Instrument separation is imminent.
FIGuRe 14-40 Deformities in nickel-titanium files. These instruments should be discarded.

298 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
treatments. Fig. 14-44 shows a case of failure in which a small-sized Hedström file separated in the coronal third of the canal. The file fragment extends approximately 2 mm through the apical foramen. The remainder of the canal was obturated with gutta-percha. Removal of the instrument fragment was accomplished with an IRS extractor after removal of as much gutta-percha as possible with the ultra-sonic probe tip.
For the removal of instrument fragments in the coronal third to midroot level, the available techniques are reasonably reliable and successful. As previously noted, the NiTi instru-ments now commonly in use are more prone to fracture in the canal than conventional stainless steel instruments. Unfortunately, their susceptibility to fracture is often a func-tion of incorrect and inappropriate application, not necessar-ily a shortcoming of the instruments themselves. However, the techniques for removal are quite different, due mainly to the limited effectiveness of ultrasonic instrumentation on nickel-titanium metal. With stainless steel, ultrasonic vibra-tion can be used for trenching surrounding tooth structure and vibrating directly against the metal. In contrast, prolonged vibration against a NiTi file will usually result in fracture of the exposed length of instrument. If ultrasonic vibration is considered, it should be used mainly for precise excavation around or parallel to the fragment, avoiding continuous contact. If the ultrasonic device is used with the intention of vibrating the fragment loose, the fragment should be well dissected from the surrounding dentin to increase the chance of removal. At the same time, the device should be used on a low power setting and only for short time frames.
Removal of Separated Instruments from the Root Canal
For these procedures, the operating microscope has proven to be indispensable. In the absence of a microscope, high-power loupes with a good light source are strongly recommended.
Gates-Glidden Bur Heads, Peeso Bur Heads, and Large Metallic FragmentsFor instruments fractured at the midroot level, including GG bur heads, Peeso reamer heads, explorer tips, and files, the best approach is ultrasonic instrumentation. The first step is to enlarge the canal space coronal to the fractured segment with a series of GG burs or Peeso reamers in a step-back manner. The purpose of this approach is to remove any dentinal barrier to the coronal passage of the fragment after it is loosened. Next, it is absolutely essential that if possible, the fractured segment be bypassed using small hand instrumentation. This space must be carefully enlarged so that a No. 20 Hedström file will pass easily by the obstruction. At this point, a new No. 15 file in the standard ultrasonic endodontic tip is placed in the canal and energized at normal settings (usually a low setting) for instrumentation.
• Fig. 14-41 illustrates successful bypass and removal of a separated Peeso bur head at the midroot level of a maxillary lateral incisor, using a Hedström file.
• Fig. 14-42 demonstrates the case of a fractured-off endodontic explorer tip that prevented completion of the root canal treatment in the mesial buccal root of the maxillary first molar. The treatment was done 8 years prior to the onset of symptoms. The ultrasonic technique was used to remove the fragment, and the revision was completed.
• Fig. 14-43 documents the unusual case of two sewing-needle tips fractured by the patient in the root canal of the maxillary canine in the effort to relieve an acute abscess months after the tooth had been opened for routine root canal treatment. The patient had neglected to have the treatment completed. The ultrasonic technique was used to remove the needle fragments, and the root treatment was completed.
Separated Endodontic Instruments
The least difficult challenges in removing endodontic instru-ment fragments are when the fragments are long, located near the access openings, and are in large canal spaces. Unfortu-nately, these factors tend to be found in the minority of failed
A B
FIGuRe 14-41 a, Successful bypassing of the Peeso bur head with a Hedström file. B, Revison in progress following removal of the instrument segment.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 299
application will remove it rapidly; or a small trephining drill may be used to create space for the extractor or choice of forceps. If the instrument is stainless steel, there is no danger of cutting or weakening it with the trephining drill. The procedure would be the same as that for the retrieval of a metal-core gutta-percha carrier or silver cone cut off at this level. Typically the trephining drill will follow the instrument very easily whether it is stainless steel or NiTi. Once the shaft of the instrument is exposed at least 2 mm, the extractor is used with the appropriate caution. The 1.2-mm extractor will be adequate for instruments up to size 40. Because of the spiral shape of endodontic instruments, a gentle counter-clockwise rotational pressure is exerted during instrument withdrawal.
Previous authors have diagrammatically described the removal of instrument fragments deep in the canal by pen-etration with the Masserann trephines.6 In clinical practice, however, trephining into the apical third of the root can be extremely hazardous and is not recommended even in large,
If a stainless steel instrument fragment is in the coronal half of the canal, use of the Masserann or IRS extractor has no limitations other than it is expensive and does not have the versatility an ultrasonic unit may have. Therefore most clinicians will have access to an ultrasonic unit of some type. What is of benefit with the extractor devices is the locking mechanism. The grip is effective, and on stainless steel, the device can be tightened with considerable force. However, care must be exercised when locking onto a segment of NiTi file because breakage of the exposed portion of the file is possible. Note the locking mechanism shown in Fig. 14-44, B.
On the positive side, NiTi hand files (see Chapter 10) often separate in shorter segments than stainless steel files and owing to the difference in flute design are not as tightly locked into the tooth structure. Light vibrations from an ultrasonic or a light rotation with a Masserann extractor will often “pop” a NiTi file loose. If the end of a broken end-odontic instrument is near the orifice of the canal, ultrasonic
A B
FIGuRe 14-42 a, Fractured endodontic explorer tip in the orifice of the mesial buccal canal of a maxillary second molar. B, Following successful removal with the ultrasonic handpiece.
B CA
FIGuRe 14-43 a, A maxillary canine with two sewing-needle tips fractured in the canal. B, The sewing needles after removal with an endodontic file in the ultrasonic device. C, Completed revision.

300 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
• When removing fractured instruments in multirooted teeth, there is the potential problem of the fractured segment floating out of one canal and finding its way into one of the other orifices. To prevent this, it is wise to place cotton into the other orifices or complete the
straight roots with generous use of large GG burs to enlarge the coronal access. In most attempts, the trephining drill will approach a lateral perforation as the root tapers anatomically toward the apex. Fig. 14-45 documents an unsuccessful retrieval of an instrument fragment located in the apical third. Although generous coronal canal widening with GG drills was done prior to the use of the Masserann technique, the trephines failed to reach the fragment. In addition, the smallest trephine nearly caused a lateral perforation.
The removal of very deep instrument fragments is possible with the ultrasonic technique if the fragment can be bypassed. Fig. 14-46 shows routine removal of a deep instrument frag-ment in the buccal canal of a maxillary premolar. Fortu-nately, the canal shape permitted small files to bypass the instrument fragment. It was ultimately removed by the ultra-sonic handpiece with an endodontic file. Subsequently, the canal treatment was successfully revised. Unfortunately, if an instrument fractures in a canal smaller in diameter than the instrument, it will rarely be bypassed. Excessive rotational pressure is more likely a cause of instrument fracture than manufacturing defects (see Chapter 10).
• File separation can be a significant problem with ultrasonic instrumentation itself, especially in the smaller file sizes. It is important to stay within the recommended power settings. Usually the fragment will loosen and flow out of the access cavity undetected, along with the irrigant. The same result is achievable when using specifically designed abrasive ultrasonic tips. There would be no difference in technique for the NiTi file fragment if it can be bypassed. This frequently occurs in the first minute of ultrasonic usage.
A B C
FIGuRe 14-44 a, Separated small-diameter Hedström file protruding through the apex of a maxillary canine. B, Instrument removed with a Masserann extractor, and the detail of the locking mechanism. NOTE: nickel-titanium (NiTi) files cannot be bent in this manner. Locking of an extractor on nickel-titanium should be very light. C, Completed revision.
FIGuRe 14-45 A failed attempt to use the Masserann trephines to penetrate to the apical third of a maxillary premolar. Separated file could not be removed.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 301
no apical pathosis and the tooth is asymptomatic, cleaning, shaping, and obturation of the coronal portion are indicated. The prognosis is generally favorable. Reevaluation is indi-cated at various time intervals. Surgical revision would be the treatment of choice in the event of failure.
When choosing nonsurgical revision of previous root canal procedures, careful assessment and treatment planning with each case are the cornerstones to success. Keen aware-ness of the options, skill in the techniques advocated for revision, appreciation for the support provided by adjunctive technologies, and understanding the potential hazards encountered in revision will allow the astute practitioner to enjoy a significant level of success in this approach to the prevention, identification, and management of these end-odontic challenges.
obturation on the other canals, so long as there is no communication with the canal containing the obstruction.
The application of techniques to remove small fragments in the apical third or around significant canal curvature is not only difficult but fraught with risks of severe thinning of the root wall if not outright perforation. Removal of instrument fragments that cannot be bypassed is problematic. New tech-niques using ultrasonic excavation under magnification and without irrigation have shown success in exposing a portion of the buried file fragment without breaking it off.
Excavation deep into the root parallel to an instrument fragment requires consideration of the root anatomy. To avoid potential perforation, it is safest to excavate in the thickest area of the root. For the mesial buccal root of a maxillary molar, the safest area to excavate would be palatal to the mesial buccal canal in which the fractured instrument is located; however, very small-diameter ultrasonic tips are required (Fig. 14-47).
Fig. 14-48 illustrates a technical procedure to remove a fractured instrument. The strategy is to excavate a space parallel to the instrument fragment. The fragment is then loosened laterally into the space sufficiently to negotiate past it with a small file. Once this is accomplished, the space is gradually enlarged until a No.15 file in the ultrasonic instru-ment can vibrate the fragment loose. In some cases, the Masserann extractor or the smaller-sized extractor, the IRS, would have application as well if the instrument fragment is exposed sufficiently.
Many file fragments cannot be removed. Attempts to do so usually are both unproductive and destructive. If there is
A B
FIGuRe 14-46 a, Separated instrument in apical canal space of the buccal root of a maxillary premolar. B, Completed revision. The instrument was bypassed by hand instrumentation and removed with an endodontic file in the ultrasonic handpiece.
FIGuRe 14-47 A selection of extra-small ultrasonic tips for excavation around separated metallic fragments.

302 chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures
7. Giuliani V, Cocchetti R, Pagavino G: Efficacy of ProTaper univer-sal retreatment files in removing material during root canal retreat-ment, J Endod 34:1381-1384, 2008.
8. Glick DH, Frank AL: Removal of silver points and fractured posts by ultrasonics, J Prosthet Dent 55:212-215, 1986.
9. Gu LS, Ling JQ, Wei X, et al: Efficacy of ProTaper universal rotary retreatment system for gutta-percha removal from root canals, Int Endod J 41:288-295, 2008.
10. Gutmann JL, Battrum DE: Challenges in retreatment of Thermafil obturated root canals, Lebanese Dent J 33(2):57-66, 1994.
11. Halse A, Molven O, Fristad I: Diagnosing periapical lesions— disagreement and borderline cases, Int Endod J 35:703-709, 2002.
12. Helfer A: To revise or retreat—your choice, J Endod 12:799, 2002.13. Hülsmann M, Bluhm V: Efficacy, cleaning ability and safety of
different rotary NiTi instruments in root canal retreatment, Int Endod J 37:468-476, 2004.
REFERENCES1. Abou-Rass M: Evaluation and clinical management of previous
endodontic therapy, J Prosthet Dent 47:528-534, 1982.2. Arthur R: Treatment of dental caries. Complications with affec-
tions of the pulp and peridental membrane (extirpation of the pulp), Am J Dent Sci 2(2nd series):505-531, 1852.
3. Bergeron BE, Murchison DF, Schindler WG, et al: Effect of ultra-sonic vibration and various sealer cement combinations on tita-nium post removal, J Endod 27:13-17, 2001.
4. Blayney JR: What teeth should be extracted: a report based upon further studies of root-canal therapy, J Am Dent Assoc 15:1217-1221, 1928.
5. Chalfin H, Weseley P, Solomon C: Removal of restorative posts for the purpose of nonsurgical endodontic retreatment: report of cases, J Am Dent Assoc 120:169-172, 1990.
6. Feldman G, Solomon C, Notaro P, et al: Retrieving broken end-odontic instruments, J Am Dent Assoc 88:588-591, 1974.
A B C
D E F
FIGuRe 14-48 a, Demonstration case showing fractured nickel-titanium file in the mesial buccal canal of a maxillary first molar. B, Excavation with small ultrasonic tip. Prolonged contact with the separated instrument should be avoided. C, View through the operating microscope showing exposure of the end of the instrument. Excavation is primarily in the thick dentin just palatal to the canal. Additional dentin can be excavated from the instrument with an endodontic explorer. D, Bypassing the instrument with a No. 6 file. e and F, The instrument is ultimately dislodged after progressive enlargement of the bypass space.

chapter 14 | Problem-Solving Techniques for Revision of Previous Root Canal Procedures 303
24. Rucucci D, Siqueira JF, Jr: Anatomic and microbiologic challenges to achieving success with endodontic treatment: a case report, J Endod 34:1249-1254, 2008.
25. Stabholz A, Rotstein I, Torabinejad M: Effect of preflaring on tactile detection of the apical constriction, J Endod 21:92-94, 1995.
26. Van Nieuwenhuysen JP, Aouar M, D’Hoore W: Retreatment or radiographic monitoring in endodontics, Int Endod J 27:75-81, 1994.
27. Wilcox LR: Thermafil retreatment with and without chloroform solvent, J Endod 19:563-566, 1993.
28. Williams VD, Bjorndal AM: The Masserann technique for the removal of fractured posts in endodontically treated teeth, J Pros-thet Dent 49:46-48, 1983.
29. Yoshida T, Gomyo S, Itoh T, et al: An experimental study of the removal of cemented dowel-retained cast cores by ultrasonic vibra-tion, J Endod 23:239-241, 1997.
RECOMMENdEd AddITIONAL REAdINGFriedman S, Stabholz A: Endodontic retreatment—case selection and
technique. Part 1: criteria for case selection, J Endod 12:28-33, 1986.
Friedman S, Stabholz A, Tamse A: Endodontic retreatment—case selection and technique. Part 3: retreatment techniques, J Endod 6:543-549, 1990.
Stabholz A, Friedman S: Endodontic retreatment—case selection and technique. Part 2: treatment planning for retreatment, J Endod 14:607-614, 1988.
14. Ibarrola JL, Knowles KI, Ludlow MO: Retrievability of Thermafil plastic cores using organic solvents, J Endod 19:417-418, 1993.
15. Johnson WT, Leary JM, Boyer DB: Effect of ultrasonic vibration on post removal in extracted human premolar teeth, J Endod 22:487-488, 1996.
16. Kazemi RB, Stenman E, Spångberg LS: The endodontic file is a disposable instrument, J Endod 21:451-455, 1995.
17. Keles A, Köseoglu M: Dissolution of root canal sealers in EDTA and NaOCl solutions, J Am Dent Assoc 140:74-79, 2009.
18. Krell KV, Jordan RD, Madison S, et al: Using ultrasonic scalers to remove fractured root posts, J Prosthet Dent 55:46-49, 1986.
18a. Messer H, Parashos P, Moule A, Australian and New Zealand Academy of Endodontists: Should endodontic files be single-use only? A position paper from the Australian and New Zealand Academy of Endodontists, Aust Endod J 29(3):143-145, 2003.
19. Molven O, Halse A, Fristad I, et al: Periapical changes following root-canal treatment observed 20-27 years postoperatively, Int Endod J 35:784-790, 2002.
20. Morrison A, Conrod S: Dental burs and endodontic files: are routine sterilization procedures effective? J Can Dent Assoc 75:39, 2009.
21. Pecora JD, Capelli A, Guerisoli DM, et al: Influence of cervical preflaring on apical file size determination, Int Endod J 38:430-435, 2005.
22. Puttaiah R, Cederberg R, Youngblood D: A pragmatic approach towards single-use-disposable devices in dentistry, Bull Group Int Rech Sci Stomatol Odontol 47:18-26, 2006.
23. Ring J, Murray PE, Namerow KN, et al: Removing root canal obturation materials: a comparison of rotary file systems and retreatment agents, J Am Dent Assoc 140:680-688, 2009.

304
Chapter 15
Problem Solving in the Management of Painful Tooth Emergencies
Problem-Solving ListProblem-solving challenges and dilemmas in the management of painful tooth emergencies addressed in this chapter are:
Patients Presenting With Complaints of Hypersensitive Teeth
Patients Presenting With Signs/Symptoms of Reversible Pulpitis
Patients Presenting With Signs/Symptoms of Irreversible Pulpitis
Procedures to Manage Teeth With Irreversible Pulpitis
Single-rooted and single-canal teeth
Multicanal teeth
Procedures to Manage Teeth With Necrotic Pulps
Incision and drainage
Apical and Surgical Trephination
Analgesics and Antibiotics
Anesthesia for Painful Teeth
To cure the Tooth-ache, Take a new Nail, and make the Gum bleed with it, then drive it into an Oak. This did Cure William Neal, Sir William Neal’s Son, a very stout Gentleman. When he was almost Mad with the Pain, and had a mind to have Pistoll’d himself.1
J. Aubrey, 1972
The most important aspects of treating the endodontic emer-gency patient are accurate and expedient diagnosis of the problem and the ability to relieve the patient’s pain. Diagno-ses must be based on the patient’s signs and symptoms, and because pain is always variable and subjective at times, filter-ing appropriate information during the subjective assessment is essential for all clinicians. Chief complaints are extremely valuable and offer a wide range of potential diagnoses, from mere hypersensitivity to irreversible pulpitis to potential peri-apical abscess:
“I get an occasional short shooting sensation in my tooth when I drink my morning tea.”
“My teeth are really sensitive when I brush at night.”
“This one tooth will not let me eat ice cream unless I move it to the other side of my mouth.”
“I had to take some pain medicine, but the pain went away in 20 minutes, and that’s the only time it hurt.”
“The pain has kept me up all night.”“I cannot chew on my tooth because it feels as though
it’s sticking up in my mouth, and it’s the first tooth I hit even when I just try to close my teeth together.”
Chief complaints also give the clinician clues as to the level of tissue damage if any in the pulp or periapical areas.
Many patients also believe they know which tooth is causing the problem, and here the clinician must be able to selectively filter useful information from information so sub-jective it should be discarded, such as “The pain hurts me in these three teeth.” It is highly unlikely that there are three problem teeth causing the patient’s symptoms, but in the case of hypersensitivity due to gingival recession, it is possible. The same is true when the patient indicates that a tooth hurts terribly when they drink something cold, and the clinician’s records and radiographs indicate there is a well-done root canal procedure on that particular tooth. The operative words in dealing with a patient’s painful situations are listen-ing, understanding, integrating, analyzing, and synthesizing. Without this problem-solving approach, the clinician may very often jump to invalid conclusions and miss the real diagnosis.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 305
determine whether this is an actual “painful” tooth emer-gency or merely an accentuated hypersensitivity that was not dealt with previously in a timely manner. The reader is referred to Chapter 7 for a more in-depth discussion of tooth hypersensitivity; this diagnosis and its treatment parameters fall within the realm of vital pulp therapy. Needless to say, some prolonged cases of hypersensitivity will fall in the diag-nostic range of either a reversible pulpitis or an irreversible pulpitis. Invariably the patient will comment, “I should have come to see you months ago when this first started bothering me, but it was only slight, and I thought it would go away, and I’ve been very busy and could not come in, but now it has my attention.”
Patients Presenting With Signs/Symptoms of Reversible Pulpitis
In this pulpal condition, patients will have transient pain of mild to occasionally moderate nature (see Chapter 1). There is often a history of recent restorative dental procedures, periodontal therapy, or possibly a history of minor dental trauma, such as a concussion or subluxation injury (see Chapter 19). Rarely do these patients complain about the pain keeping them up at night or being awakened by the pain in the middle of the night.
The symptoms of thermal sensitivity do not prevent the patient from eating or drinking normally, although in more severe cases, there may be a history of avoidance of tempera-ture extremes in specific areas of the mouth. In these situa-tions, and in particular when thermal sensitivity is the patient’s chief complaint, the clinician must be able to dis-tinguish between sensitivity and true pain. The interpretation of either by the patient and clinician may vary considerably. Too many cases of root canal treatment are done in the pres-ence of an annoying sensitivity as opposed to a true pain that indicates the need for pulp removal, and too many patients are being overtreated for a minor inflammatory situation that may be handled in a much less aggressive way. The only way to manage these situations properly is to attempt to identify the etiology and remove it. If successful, the transient sensi-tivity will subside, and the patient will not only be comfort-able but grateful to the clinician for the professional expertise in managing the problem.
If an etiology such as caries, exposed cervical margins of dentin, a fractured cusp, or a fractured restoration is dis-covered, the majority of cases will resolve by appropriate restorative treatment (Fig. 15-1). Tincture of time will also improve some patients’ symptoms. In most cases, the revers-ible pulpitis was the result of some restorative procedure that caused transient inflammation within the pulpal tissues (Fig. 15-2). In no case does the inflammation spread into the periapical tissues, and therefore no periapical changes are seen as one might find when an irreversible pulpitis is diagnosed.
The clinician must decipher from the patient’s own words approximately where the problem is located and how severe the problem has become (see Chapter 1). The final diagnosis is a combination of the patient’s description of the problem, which represents the subjective data, and the objective data elicited from the various sensibility and manipulative tests.10 As a rule of good clinical judgment, no tooth should ever be destined for root canal treatment unless the clinician is approximately 90% or better assured that the correct diag-nosis has been made and the correct tooth has been identi-fied. At times, from the history and description of the symptoms, the clinician will sometimes know root canal treatment is indicated but not be able to identify the offend-ing tooth upon clinical examination. This is especially common in quadrants of teeth in which all have had exten-sive coronal restorations and sensibility testing is limited. For example, all the data may point to an irreversible pulpitis, but identification of the tooth is elusive. Although contrary to the desire to provide pain relief for the patient, it may often be better to send the patient home with palliative support rather than risk treatment of the wrong tooth. It is especially difficult to send the patient away when the diag-nosis cannot be made in the case of moderate to severe pain.11,30 The clinician fears that the patient will lose confi-dence in his or her diagnostic ability.
In reality, however, if the clinician has conducted a thor-ough examination and has presented the diagnostic dilemma in a compassionate manner, the patient will understand that the symptoms will localize in time to a specific tooth. It will then be possible to diagnose the problem accurately and provide definitive treatment. The solution to difficult diag-nostic problems in endodontics is never found by guesswork. It is entirely inappropriate to initiate a root canal procedure with the attitude of “Let’s try this and see if it works.” This is especially true when one considers the many possible sources of nonodontogenic pain (see Chapter 6). Whereas Chapter 1 dealt in depth with diagnosing odontogenic pain, this chapter’s focus will be on problem solving painful tooth emergencies.
Patients Presenting With Complaints of Hypersensitive Teeth
A perceived reason to see the dentist for a painful tooth can be anything from an occasional shooting sensation to a tin-gling or sensitivity when ingesting certain foods or drink to discomfort during tooth brushing or flossing. If the clinician is seen immediately upon the onset of the symptoms, more often than not there is no pulpal pathosis that requires sig-nificant intervention. However, if the patient does not seek help immediately and the problem continues or accentuates, often they are referred to a specialist for an in-depth evalua-tion or even root canal treatment. It is in these scenarios that a true differential diagnosis must be made—especially to

306 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
Patients in pain should be made aware that any type of restorative procedure, whether the removal of an existing amalgam, the removal of caries, or preparation of a crown prep or a class II inlay, has the potential to cause pulpal inflammation that may linger for various time periods. In most cases, the inflammation of the pulp is “reversible,” but the pulp is only able to withstand a given amount of insults or irritations before the inflammatory state becomes irrevers-ible. This is a concept not always considered by the restor-ative dentist prior to extensive restorative procedures. Obvious changes may have occurred in the tooth: a narrowed pulp chamber, the presence of pulp stones or linear calcification in the root canal, hidden caries beneath an old restoration, the presence of various degrees of condensing osteitis, the presence of minor areas of root resorption, obvious crack lines on the margin ridges, and so forth (Fig. 15-3). Such
On occasion, the patient might experience continued mild pulpal pain from a minimal restorative procedure (class I amalgam or class III composite restoration). However, this will not usually degenerate into an irreversible problem unless the pulp was already in a degenerative state prior to the restorative procedure. In these recalcitrant situations, if the pain does not subside after 2 weeks or so, removal of the restoration and placement of a base or sedative dressing may be helpful in alleviating the patient’s symptoms. However, in pursuing this approach, the clinician must remember that at some time the sedative restoration will have to be removed, and in the process all restorative procedures may add addi-tional insult to the dental pulp. If all efforts have been made to maintain the dental pulp in a healthy state and symptoms continue or get progressively worse, a root canal procedure is indicated.
BA
FIGure 15-1 A, This 20-year-old female with slight sensitivity to temperature changes was sent for root canal treatment on the mandibular second molar. All tests were normal, and there were no radiographic changes. b, After caries excavation, a sedative restoration was placed. At the 2-week reassessment, the patient was symptom free.
BA
FIGure 15-2 A, This 45-year-old patient complained of significant pain to cold on a tooth with a newly placed crown and was sent for root canal treatment. She used her finger to point to the palatal aspect of the first molar as her source of discomfort. b, Clinical examination revealed an exposed dentinal margin on the palatal, where the crown was short of the prepared tooth structure (arrows). The patient was advised to have the crown replaced without having root canal treatment.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 307
tissue cannot respond favorably to any type of palliative treatment and must be removed, or the tooth must be removed (see Chapter 1). If the patient or clinician can localize the source of the pain to a particular tooth, the diagnosis can usually be made within a few minutes of taking the patient history and performing a few clinical tests as necessary (see Chapter 1). If the patient complains about any of the following symptoms, the likelihood of an irre-versible pulpitis is high. These symptoms include (but are not limited to) pain that lasts several minutes to hours, pain that throbs or is sufficiently intense to awaken the patient at night, pain that is spontaneous throughout the day or evening hours, pain that is severe when hot or cold foods come into contact with a specific tooth, pain to biting on the tooth, or pain so severe the patient completely avoids eating on that side of the mouth.
These findings are all valid indicators of an irreversible pulpitis and in some cases will indicate that the inflamma-tory response has already progressed through the apical
changes may not bode well for a tooth that is treatment planned for extensive restorative procedures. The tooth may exhibit no symptoms, and sensibility tests may give the impression that the pulp is vital or a subtle reversible pulpitis is identified, but this does not mean the pulp is healthy and can withstand further insult without succumbing to an irre-versible pulpitis. These issues are key for the restorative dentist to understand to prevent problems for the patient, and these considerations in treatment planning must be com-municated fully to the patient.
Patients Presenting With Signs/Symptoms of Irreversible Pulpitis
The diagnosis of irreversible pulpitis implies that there are sufficient signs and symptoms to indicate that the pulp
A B
C
D
FIGure 15-3 A, Mandibular first molar with significantly reduced pulp chamber, pulp stones, and condensing osteitis. Changes reflect degenerative pulpitis. No symptoms. b, Mandibular first molar showing a pulp chamber that is almost occluded with calcification and canals that also show the same. While teeth like this may register as “vital,” the pulps are not healthy, and this is where the diagnostic dilemma lies when it is difficult to determine the source of the patient’s distress. C, Occlusal surface that depicts questionable restorative margins and the presence of significant fractures on the distal margin (arrows). Patient was suffering from vague pain in the maxillary left quadrant. D, Crack in tooth dentin showing invasion of bacteria even into the dentinal tubules. In the presence of long-term defects of this nature, dental pulps can easily undergo degeneration and be symptomatic.

308 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
apical neural elements. Thoroughness is the operative word in managing this emergency situation. Upon completion of the emergency procedure, a medicament such as calcium hydrox-ide can be placed (see Chapter 11).
Some clinicians choose to do a pulpotomy because the procedure is virtually the same with respect to the amount of time required. It is more appropriate to perform a
foramen and affected the periapical tissues. This information can be obtained from a thorough history of the patient’s symptoms, and a definitive diagnosis can usually be made regarding the patient’s need for a root canal procedure. However, the true histopathologic status of the tissues cannot be ascertained at this point, so clinical tests must be per-formed to obtain a pulpal and periradicular diagnosis. The patient’s responses have only informed the clinician of an “irreversible situation” that is occurring but not whether the pulp is inflamed or necrotic. The use of thermal tests may provide a definitive but not entirely accurate diagnosis of the pulpal status.
Procedures to Manage Teeth With Irreversible Pulpitis
Once the diagnosis of irreversible pulpitis has been estab-lished, concise treatment will usually provide the patient with immediate relief. However, there are specific treatment modalities with respect to irreversible pulpitis that minimize the patient’s postoperative discomfort and enhance confi-dence in the treating clinician. The approach to treatment will depend upon two factors. The first is whether the irre-versible inflammation is in a single-rooted/single-canal tooth or a multicanal tooth. The second factor is whether the tooth demonstrates sensitivity or pain to percussion. Once these two factors are known, the treatment can be rendered expedi-ently and accurately with a high degree of success and minimal postoperative sequelae. While these two determinants for treatment are not “cast in concrete,” they will guide the clini-cian in the rapid problem-solving management of these painful situations.
Single-Rooted and Single- Canal TeethWhen a single-rooted or single-canal tooth has been diag-nosed with irreversible pulpitis, the ideal treatment is to remove the pulp in its entirety (pulpectomy; Fig. 15-4). A pulpectomy means complete removal of the pulp from its root canal. To be effective, however, this implies more than just placing a file or broach into the root canal at some undeter-mined level for a few seconds. Once profound anesthesia is obtained, it takes but a few minutes to access the tooth, obtain a working length (see Chapter 9), and clean and shape the canal sufficiently to remove the dental pulp and any residual remnants. While a properly sized broach or two may work to remove the pulp on occasion, this process is most effective when using rotary nickel-titanium (NiTi) instru-ments and 6% sodium hypochlorite (NaOCl) to perform a pulpectomy (Fig. 15-5). If the problem is to be solved expedi-tiously in the patient’s best interest, the procedures used must favor the complete removal of the inflamed tissue. Hand instruments (K-files and broaches) will often just shred the tissue, leaving remnants that may still be connected to the
B
FIGure 15-4 Pulp extirpation with a broach.
FIGure 15-5 Use of a rotary nickel-titanium instrument to remove the dental pulp intact.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 309
Fortunately, in most emergency situations, symptomatic relief can be achieved without removal of all of the pulp to the apices even though this would be preferable. It is impor-tant to note the approximate length of the roots and pene-trate at least into the apical third in each canal.
On the other hand, it is extremely important to remove pulp tissue from all canals. Patients who seek relief of acute thermal sensitivity can sometimes experience the same symp-toms after emergency treatment if vital, acutely inflamed pulp remains intact in one of the canals. Persistent signs and symptoms of an acute apical abscess can also be due to failure to clean a root canal of its inflamed tissue (see Fig. 15-6). If time permits, the approach is similar to that discussed for anterior teeth, with access, working length, cleaning, and shaping to a size sufficient to remove the tissue to the desired length (usually a minimum of No. 25 K-file and larger if possible). This procedure is indicated because it is difficult to ascertain which root or roots may be causing the periapical inflammation. In many cases, the root canal systems are narrowed or quite small in diameter, but if there is sufficient time to manage the emergency, the original dictate applies. If there is insufficient time to manage this problem ideally, then a pulpotomy should be performed and the occlusion reduced, or it may be possible to perform a pulpectomy on the largest root canal (distal root in mandibular molars, palatal root in maxillary molars and premolars). Upon completion of the emergency pro-cedure, a medicament such as calcium hydroxide can be placed (see Chapter 11).
Patients with irreversible pulpitis usually present with a history of severe pain, either spontaneous in nature or stimulated by cold foods or liquids. At times the patient may identify a particular tooth they feel is causing the problem, but the clinician is unable to reproduce the symp-toms, even with extensive and rigorous testing. Likewise, the
pulpectomy than a pulpotomy, however; the latter can leave a significant amount of inflamed pulpal tissue in the root canal system, and symptoms will continue. If the patient exhibits pain to percussion, pulpectomy is the preferred treat-ment. When the patient demonstrates periradicular inflam-mation, all of the pulpal tissue should be removed throughout the root canal system.
Multicanal TeethMost posterior teeth with irreversible pulpitis will require either a pulpotomy or pulpectomy for immediate pain relief 33
(Fig. 15-6). If no mastication sensitivity is reported, a pulp-otomy is usually sufficient as an emergency treatment. When the tooth demonstrates percussion sensitivity or pain, it is important to adjust the occlusion or remove the tooth from occlusion, or the patient may not have adequate relief from their symptoms.
The treatment of posterior teeth is not much different than that of anterior teeth. The canals of posterior teeth are significantly smaller than those of anterior teeth, and emer-gency procedures may require modification. Only the largest of canals in posterior teeth permit the use of broaches and one seldom sees the pulp as an intact tissue after removal. The removal of the pulp in typical small canals is virtually a by-product of the mechanical enlargement of the canal with rotary or hand files. Patients who are seeking treatment for acute problems on an emergency basis are often seen by dentists who do not have full appointment times immediately available. An emergency visit may be scheduled after normal hours or “squeezed” into an improvised time period during the day. For single canal teeth described above, thorough canal débridement is possible even in an abbreviated time period. For multi-canal teeth, the time commitment for com-plete preparation to the apices may not be available.
A B
FIGure 15-6 A, Mandibular molar with vague symptoms. The radiograph shows chronic focal sclerosing osteitis on the distal root end, indicative of a chronic degenerating pulp. When testing with cold, the tooth exhibited no response at first then gave a throbbing ache that lingered. b, Mandibular molars with probable carious exposures. Both were painful to percussion and varying degrees of thermal stimulation.

310 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
radiographic presentation is often completely normal or at least thought to be normal. There are no signs of abnormal periapical changes, the lamina dura and periodontal ligament space all seem to be within normal limits, several teeth have large restorations or crowns present, but the clinician cannot elicit any pain to percussion or abnormal response to cold from the tooth the patient is convinced is the source of pain. Unfortunately, there is often a disparity between the symp-tomatic status of a tooth and the histologic picture of its pulp, which may explain the difficulties of diagnosis (Fig. 15-7).
Procedures to Manage Teeth With Necrotic Pulps
Under the diagnosis of necrotic pulp, there are several situa-tions that must be considered. These include whether the necrotic pulp is in an anterior or posterior tooth, whether or not the tooth has developed a sinus tract and whether or not there is swelling.
B
C
CI
PN
AI
LN
NP
A
FIGure 15-7 A, Mandibular molar that exhibits narrowed chamber and canals and the presence of condensing osteitis, indicative of a degenerating pulp. Symptoms are minimal, and tests could not reproduce the patient’s discomfort and chief complaint. b and C may very well provide an explanation of the changes and why it is difficult at times to make a diagnosis. b, Mandibular molar that was symptom free, and the patient had no recollection of any pain or discomfort to function. All tests were normal but because of the depth of the caries, she was advised that root canal treatment was likely to be needed along with a crown to maintain the tooth. Because of cost factors, she opted to have the tooth extracted. C, Histologic section of the coronal pulp. Note the wide variety of histologic findings in a tooth that was symptom free and had normal responses to cold, percussion, palpation, and electric pulp testing. (NP, Normal pulp; AI, acute inflammation; CI, chronic inflammation; PN, partial necrosis; LN, liquefaction necrosis (B&B stain ×4; no bacteria evident).
First, single-root/single-canal teeth will be much easier to manage than multicanal teeth. Second, if a sinus tract is present, treatment will be much easier because more often than not the patient’s symptoms are minimal. Third, if a swelling is present, the type of swelling, such as a localized swelling or nonlocalized (cellulitis) must be determined. There are appropriate treatment approaches for each situa-tion, and these will be dealt with separately.
The tooth with a necrotic pulp will usually give no response to cold or other thermal tests and will not respond to an electric pulp test (EPT) (Fig. 15-8). The tooth may be sensitive to mastication or percussion, but this is not relevant to the diagnosis and only becomes significant when consider-ing the need for occlusal reduction.
When the diagnosis of a necrotic pulp has been established in an single-rooted or single-canaled tooth and no swelling is present, the tissue must be removed completely from the canal system in order to alleviate the symptoms (Fig. 15-9). The clinician may use the same technique as in the anterior teeth with an irreversible pulpitis to remove the necrotic

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 311
FIGure 15-8 Diagnosis of a necrotic pulp on the maxillary lateral incisor.
CLINICAL CHALLENGEClinical Challenge #1: In these not-so-rare instances, the clinician must not act based upon the patient’s insistence that a particular tooth is painful and the source of their problems, but rather must rely on the objective findings produced at the time of the emergency visit. If clinical findings are confusing and do not lend themselves to a rapid or logical diagnosis, it may be wise to not act upon meaningless data but wait until valid data can be obtained and an accurate diagnosis established.
In most cases, the symptoms will recur within a short time and the patient can be reexamined. It is always inappropriate for the clinician to begin root canal treatment without having a reasonable diagnosis. Patients have sometimes been sub-jected to treatment on multiple teeth in the hope of relieving pain only to discover, ultimately, that the pain was of non-dental origin. See Chapter 6.
Clinical Challenge #2: It may be necessary to examine clinical findings more comprehensively: How extensive are the restorations that are present? How long have they been there? Are there marginal discrepancies that may be contributing to bacterial leakage? Are there fracture or significant craze lines? Are there changes in the size of the pulp canal spaces and chamber compared to other teeth? Are there pulp stones present? Is condensing osteitis present? Are there subtle changes in the root apex compared to others that may indi-cate some evidence of a low-grade resorptive process? These questions may or may not be helpful, but they provide a better assessment of the data available and help the clinician make interpretive judgments (see Fig. 15-7). One result could easily be that the patient is sent immediately to a specialist for an in-depth evaluation.
Clinical Challenge #3: In securing the subjective data, important questions must be asked, and these are detailed in Chapter 1 (“Listen to the patient, they are giving you the diagnosis!”—Sir William Osler, 1867). Often, thermal tests do not lend themselves to a diagnosis and are in fact within normal limits, as is frequently the case when an acute irrevers-ible pulpitis becomes chronic and pulp responses become identical to noninflamed teeth (see Fig. 15-7). Radiographic signs are the only definitive method for obtaining a diagnosis. However, it is common for the radiographic presentation to be normal; or is it truly normal? This is especially true in cases of early irreversible pulpitis or in posterior mandibular teeth in which the cortical plate is extremely dense and changes in the bone may not become obvious until significant destruc-tion has taken place, usually in the last stages of irreversible pulpitis.
tissue from the canal system. The use of NiTi rotary instru-ments in a crown-down fashion favors a thorough cleaning. The nature of the instruments and their application result in auguring debris out of the canal in addition to developing ideal canal shapes for rinsing residual materials from the canal. A significant amount of NaOCl (see Chapter 11) should be used, especially because of the need to remove the necrotic tissue and kill the bacteria in the root canal system. Large, single-rooted anterior teeth and premolars with large,
single canals should be treated identically. If a working length cannot be established (the ideal method before instrumenting the canal in an emergency visit), an estimated working length should be obtained based on the initial radiographic film. This can also be achieved with an electronic apex locator (see Chapter 9). The operative word in this clinical situation is débridement, which includes the effective use of NaOCl. Upon completion of the emergency procedure, a medica-ment can be placed (e.g., calcium hydroxide mixed with 2% chlorhexidine [see Chapter 11]).
If the necrotic pulp is in a multicanaled tooth, the treat-ment is similar to that of a single-rooted/single-canaled tooth, but there are different approaches. The purpose of any tech-nique is to establish the most rapid method to remove a majority of the necrotic tissue within the root canal system. In molars, this can be challenging because of the difficulty in removing the necrotic tissue from very small, curved, and narrow canals.
The first approach can be similar to that used for posterior teeth with irreversible pulpitis. When possible, a hand or rotary instrument can be used to remove the pulpal debris. This may not be accomplished routinely in the canals of posterior teeth (buccal canals of maxillary teeth and mesial canals of mandibular teeth) inasmuch as these canals require smaller files initially for easy penetration. A pathway for the larger instruments must be made, and at the same time, débridement is achieved. Here again the crown-down tech-nique must be used. Initially a small K-file, such as a No. 08 or 10, is used to establish coronal patency. Next, a rotary PathFile (Taper .02 at diameters of 0.13, 0.16, and 0.19 [Dentsply Maillefer, Ballaigues, Switzerland]) can be used to enhance access to the apical portion of the canal. Once the canal is opened coronally, it can be débrided gradually and safely, increasing to a size No. 25 or comparable rotary file

312 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
A B C
FIGure 15-10 A, Necrotic pulp causing symptoms in a mandibular premolar. b, Drainage and working length established. C, One-year reevaluation indicates excellent healing.
BA
FIGure 15-9 A, Débridement of the canal system reveals complete putrefaction of the dental pulp. b, In some cases, the necrotic pulp will come out intact.
to the estimated working length. Copious amounts of irrigant (NaOCl- 3% to 6%) must be used during the débridement process. Care must be exercised with this technique to prevent necrotic debris from being forced out the apical foramen and into the periradicular tissues, thereby causing additional dis-comfort for the patient. Here again, the use of crown-down instrument techniques will be beneficial to prevent this potential postoperative sequela.36
In the second approach, the first step is to establish a working length for all canals. This is easily accomplished in canals that are patent (Fig. 15-10, B). After obtaining a working length, the canals are instrumented to a size No. 25 or comparable rotary file using copious amounts of NaOCl. The larger distal or palatal canals are instrumented routinely to a larger size (approximately Nos. 30 to 40) during this procedure. An intracanal medicament of calcium hydroxide is placed, and a cotton pellet is placed over the exposed canal orifices, followed by an appropriate temporary with adequate
depth (a minimum of 3 to 4 mm) to prevent occlusal leakage.The patient who presents with a necrotic pulp and a draining sinus tract usually has little to no symptoms. There is often a history of pain associated with a specific tooth or a history of a bad taste in the patient’s mouth, but rarely does the patient recall severe pain associated with a tooth. It does, however, occur on occasion and this is usually a result of the abscess within the cortical bony plates eroding the last couple of millimeters of cortical bone, causing pressure on the peri-osteum. This pressure, immediately before the sinus tract is established, is the cause of the severe pain the patient may have experienced. Clinically, the patient is diagnosed with a necrotic tooth, and a soft-tissue lesion is present in the form of a small orifice or “pimple-like” lesion on the attached gingiva or in the mucosa. It may have many different appear-ances from a swelling to being pedunculated to merely a reddish area on the gingiva. A sinus tract should always be traced to verify the diagnosis that is made based upon clinical

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 313
antibiotic therapy in these cases; however, appropriate follow-up care is essential.
Patients with necrotic pulps will present periodically with a localized swelling. Often these patients are symptomatic and sensitive to palpation over and around the soft-tissue swelling. The lesion is generally directly over the apices of the offending root, but it must be recognized that penetration through the bone and periosteum of an inflammatory process usually occurs at the site of least resistance. Therefore in some cases, the soft-tissue swelling will not be directly over the root or necrotic tooth causing the lesion but manifest adjacent to the offending tooth, and one or two teeth will appear to be contributing to this swelling (Fig. 15-12).
The treatment of a necrotic pulp with localized swelling is not an indication for antibiotic therapy. However, it is imperative that the necrotic tissue be completely removed from the pulp chamber and root canal system. The patient should always be made aware before treatment is rendered that regardless of the clinical diagnosis, most root canal treat-ment results in additional periapical inflammation with subsequent symptoms. In all probability, the patient will experience additional discomfort and in some cases, an increase in localized swelling. Most interventions such as instrumentation, obturation with sealer, and pulpectomy/
tests and patient symptoms (Fig. 15-11). This is accom-plished by using a size 25 to 40 gutta-percha point that is placed into the sinus tract and slowly traced to the source of the problem. By threading the gutta-percha slowly into the sinus tract, the clinician can determine more accurately which tooth is the source of the problem. If the gutta-percha is introduced into the sinus tract slowly, it will warm up to body temperature and not cause any undue pain or discom-fort while it is being inserted. Using too small a gutta-percha point will sometimes prevent the point from reaching its true endpoint because it will bend prematurely. Too large a point will be prevented from tracing the tract the entire distance because of the morphology of the sinus tract and its lack of flexibility. In a majority of cases, gutta-percha points between sizes 25 and 40 should achieve the objective.
Because of the lack of true “emergency-type” symptoms in these cases, routine root canal procedures are indicated. Should the patient be in that rare instance when they are experiencing acute pain, the most appropriate emergency procedure would be complete débridement of the root canal system.
Postoperative instructions should indicate that the prob-ability of any painful sequelae is rare, and only over-the-counter analgesics are indicated. There are no indications for
A B
C
FIGure 15-11 A, A typical tract stoma (opening). b, Clinical photo of tracing of a tract with a gutta-percha cone. C, Radiograph of a sinus tract tracing with a gutta percha cone.

314 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
can be minimal (Fig. 15-13, A) or profuse and in some cases may continue for minutes, exhibiting a pulsating type of flow. This usually starts as purulent only (see Fig. 15-13, B) and culminates with both purulence and blood (sero-purulent; see Fig.15-13, C ). The canal is cleaned and shaped, and a medicament and temporary filling is placed. If the tissue is fluctuant, an incision and drainage can be per-formed, especially if the tissue is still turgid (Fig. 15-14), but since drainage was obtained through the tooth, most of the time this procedure is optional. Additional anesthetic solution should be introduced around but not into the area of the localized swelling. If a small gauge needle is available, the tip can be inserted into (not through) the thin mucosa in the area of intended incision and a couple of drops can be deposited to blanch the tissue.
Fluctuancy: No Drainage Through the ToothIn these cases, the pulp chamber is opened, but no drain-age is obtained from the canal or canals. Cleaning and shaping are completed, calcium hydroxide is inserted along with a cotton pellet, and a temporary filling is placed. Anesthetic solutions are delivered on either or both sides of the swelling, providing the patient with sufficient time for anesthesia to become profound. Do not inject directly into the swollen tissue. It will only cause the patient sig-nificant pain and potentially disseminate undesired inflam-matory products and bacteria deeper into the tissues. A No. 12 or 15 scalpel blade is placed into the fluctuant mass and pressed firmly down onto the bony plate through the swelling (Fig. 15-15). This incision can be made hori-zontally at the base of the swelling or vertically but pref-erably between the roots of the teeth. In posterior teeth, the purulence in the tissues may not be as localized and can spread laterally both buccally and lingually/palatally (Fig. 15-16). In these cases, drainage may not occur immediately and must be encouraged if necessary by opening and closing a hemostat within the incised fluctu-ant area. The abscess “pocket” must be opened, releasing the purulence and achieving additional drainage (Fig. 15-17). Drains are not indicated in most instances; the incision will remain open long enough to achieve the desired result. Warm saline rinses are suggested for approxi-mately 24 to 48 hours after the incision and drainage procedure.
No Fluctuance: Drainage Through the ToothAfter the access opening is established, cleaning and shaping of the canals are completed. During this procedure, drainage is obtained through the canal(s). Because the tissues are nonfluctuant, meaning they are usually quite firm, there is no indication to incise and drain the soft tissue inasmuch as this procedure would be nonproductive. Warm saline “holds” as opposed to rinses may be suggested in an attempt to pool the purulence into a localized area for later incision and drainage. Although the amount of purulence and necrotic debris that exits though the root canals of teeth is nominal, it usually is adequate to provide relief for the patient in acute discomfort.
pulpotomy procedures result in additional periapical irrita-tion and inflammation. This results in tissue changes that manifest as pain in the periapical area, which the patient perceives as pain in the tooth or discomfort in the mandible or maxilla when the tooth is moved or palpated.
In no cases should a tooth with an inflamed, vital, or necrotic pulp be left open to drain, either if drainage has been established from within the tooth or if no drainage was obtained.36 Leaving a tooth open for drainage will only lead to additional bacteria and salivary contaminants being intro-duced into the root canal system the clinician is attempting to “sterilize” as well as possible, although some studies refute this impact clinically.37 There is clinical evidence that the longer a tooth is left open for drainage, the longer it will take (additional postop appointments required to close the tooth) to manage the closure of the tooth. This can be attributed to colonization of the root canal spaces with bacterial species that are able to protect themselves through mechanisms of biofilm formation.37,38,44
Incision and DrainageIf a swelling is present adjacent to a tooth or teeth, the clini-cian must determine whether the swelling is fluctuant or nonfluctuant. This determination must be made so the appropriate treatment can be provided for the patient. Should an incorrect assessment be made, inappropriate treatment may result in additional discomfort for the patient, and a longer period of healing will be required.
There are four scenarios to consider, each requiring proper management to alleviate patient symptoms and provide the appropriate periapical environment for healing to ensue. In all these cases, the pulp has been diagnosed as necrotic, and periapical symptoms range from mild to severe.26
Fluctuancy: Drainage Through the ToothOnce the tooth is opened for treatment, drainage is obtained from the canal(s) through the access opening. The drainage
FIGure 15-12 Localized swelling is centered above the maxillary lateral incisor but extends laterally to include the roots of the central and the canine.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 315
A B
C
FIGure 15-13 A, Seropurulent drainage from a small canal in a mandibular molar. b, Initial purulent drainage from a maxillary lateral incisor with a necrotic pulp and localized swelling. C, As the drainage continues, it becomes more seropurulent. Drainage of these types occurs often just upon access to the pulp chamber. In some other cases, apical trephination may be warranted.
FIGure 15-14 Incision and effective drainage from the swelling above a maxillary lateral incisor.
No Fluctuance: No Drainage Through the ToothIf an access opening is made but no drainage is obtained, the canals are cleaned, shaped, medicated, and closed. Because the tissue is nonfluctuant, incision and drainage is
contraindicated. The patient should be placed on hot saline rinses that will soothe the tissues and may promote either a reduction in overall symptoms or encourage more rapid movement of the inflammatory response through the bone into the soft tissues; at this point the incision and drainage can be attempted. These clinical scenarios present difficult challenges. The patient must be treated expediently and appropriately, but cleaning and shaping of the canal system is the only treatment that can be performed in an attempt to alleviate the symptoms. Although some clinicians advocate the routine use of patency filing in all cases, this may not be the time to consider a technique that has no clinical or scientific basis (see Chapter 9). If used aggres-sively, especially without cleaning the canal thoroughly prior to going past the apical constriction, it may inoculate the periapical tissues with undesirable bacterial species, thereby creating an even worse clinical situation.38 Likewise, while studies have shown that drainage may not achieve the level of desired pain relief,32 a systematic review of the literature (done to identify evidence-based directives) found that drain-age is indicated to lessen the patient’s problem.26 However, if there is a reasonable possibility drainage could not be obtained by going past the apex, apical trephination can be considered.

316 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
BA
FIGure 15-16 A, Drainage could not be obtained through the tooth in a maxillary molar. Note the swelling. b, Incision with drainage readily achieved. (Case courtesy Dr. Rob Roda.)
A BB
FIGure 15-15 A, Incision and drainage of a localized swelling. The area has been anesthetized, but the anesthetic solution is not placed directly into the swelling. Placement of a No. 11 scalpel blade for the incision. b, Deep incision releases the contents of the tissue swelling.
Apical and Surgical Trephination
A trephination procedure can be of tremendous help when indicated for relieving a patient’s excruciating pain. Apical trephination is indicated when a diagnosis of acute alveolar abscess can be made with reasonable assuredness, there is no swelling, and there is every reason to believe that going beyond the apical foramen with a small file will result in drainage. The procedure is accomplished by aggressively placing a No. 15 to 25 K-file 2 to 3 mm beyond the confines
FIGure 15-17 Opening the incision with a hemostat to enhance drainage.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 317
of the apex. In most cases, this will establish drainage. Each case should have radiographic verification of the file position beyond the apex. This procedure can introduce some treat-ment problems, such as destruction of the natural apical constriction or zipping of the canal at the apex in curved canals if the clinician is too aggressive. Remember also that in cases of acute pain and acute infection, obtaining profound anesthesia for surgical intervention can be difficult. However, the benefits of the procedure far outweigh the potential problems.
Surgical trephination is rarely needed to manage pain if good principles of diagnosis and treatment are followed. Although studies have not supported its efficacy,21,28 when chosen selectively it is a reliable procedure to manage intrac-table pain when all other methods have failed. In all likeli-hood, the severe pain is caused by a significant increase in intracortical pressure in the periradicular tissues, which can only be relieved through a surgical opening when apical trephination has failed or cannot be performed, as in the case of a previous root canal procedure in which the canal cannot be accessed at that moment or the canal is blocked apically. Surgical trephination involves a soft-tissue incision, cortical penetration with a rotary instrument, and creation of a pathway for drainage from the periradicular tissues.12 Three approaches may be considered:
Treatment Option 1:
1. Proper anesthesia is obtained.2. A No. 15 scalpel blade is used to make a small
(5 mm) horizontal or vertical incision in the mucosa apical and usually superior or lateral to the root apex. This positioning is critical to avoid penetration into tooth structures.
3. Retract the mucosa with a tissue retractor, periosteal elevator, or the wide end of a sterile No. 7 wax spatula (Fig. 15-18, A).
4. A No. 6 or 8 round bur is used to penetrate the cortical plate at an angle designed to reach the periradicular tissues or lesioning, avoiding contact with the root (see Fig. 15-18, B). This approach works well when a large periradicular lesion is present.
5. Immediate drainage for relief of intracortical pressure is usually obtained.
6. The patient is advised to use warm to hot saline rinses for at least 24 hr; longer is desirable.
Treatment Option 2:
1. Proper anesthesia is obtained.2. A No. 15 scalpel is used to make a small (5 mm)
vertical incision adjacent to the root of the tooth in question.
3. Retract the mucosa with a tissue retractor or wide end of a sterile No. 7 wax spatula (see Fig. 15-18, A).
4. A No. 6 or 8 round bur is used to penetrate the cortical plate only (see Fig. 15-18, B).
5. A large K-file (No. 40 minimum) (see Fig. 15-18, C ) or spoon curette is used to bore a path through the cancellous bone to the periradicular tissues or lesion, avoiding contact with the root apex (Fig. 15-19).
6. Immediate drainage or relief of intracortical pressure is usually obtained.
7. The patient is advised to use warm to hot saline rinses for at least 24 hr; longer is desirable.
More often, option 2 is a safer approach, especially if vital structures are adjacent to the tooth in question, if roots are closely approximated, or if the vestibule is shallow (Fig. 15-20). Failure to adhere to these principles can result in destruction of the root structure and periodontal ligament, with the potential for subsequent external root resorption. An alternative to either of the previous options is to use a large endodontic spreader to penetrate the cortical plate6:
Treatment Option 3:
1. After the penetration site has been anesthetized, a No. 3 spreader is placed parallel to the root surface, with a silicon stop as a reference point.
2. The spreader is then rotated to a point nearly perpendicular to the root apex.
3. Apical pressure is applied as the spreader pierces the alveolar mucosa, periosteum, and cortical bone into the periradicular lesion.
The value in this approach is that no incision or surgical flap is necessary, and the chance of damage to the root structure is minimized. However, entry to the lesion may be very dif-ficult in the presence of thick cortical bone.
If a patient presents with a necrotic pulp and an extensive extraoral swelling or cellulitis, accurate and aggressive treat-ment is essential. In these cases, the patient should be placed on antibiotics immediately upon completion of the root canal treatment—or before if the clinician is unable to treat the patient in a timely fashion (Fig. 15-21). Antibiotics of choice are penicillin or amoxicillin 500 mg every 6 hours for 5 to 7 days. Clindamycin has become very popular as a sub-stitute for penicillin and cephalosporin, but there is little evidence-based support for other antibiotics over penicillin at this point in time. Because of the potential for this condi-tion to worsen quickly without any indications of its rapidly deteriorating state, removal of all necrotic tissue within the root canal system is recommended. This type of root canal infection requires immediate and aggressive action on the part of the clinician. Mistakes are costly and can result in serious sequelae.
If the patient is febrile and has lymphadenopathy in com-bination with a cellulitis, it is advisable to prescribe a loading dose of antibiotic. Usually, in the case of penicillin, a loading dose of 2 g is indicated and adequate to control a fulminating infection. Unless the patient is allergic to penicillin, antibiot-ics should not be substituted without adequate clinical judg-ment. One-appointment root canal treatment in these cases is not contraindicated based on any physiologic or biological

318 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
BA
C
FIGure 15-18 A, Preparation for a surgical trephination; a small vertical incision was made and the tissue was retracted slightly with a small periosteal retractor. b, While the tissue is retracted, a bur is used to begin cortical penetration. C, Once most if not all of the cortical bone is penetrated, a large file can be used to create a drainage pathway from the desire site.
A B
FIGure 15-19 A, This 27-year-old female was referred for treatment; maxillary lateral incisor was opened and left open for drainage, but no drainage occurred. b, After an incision was made, a curette was used to establish a pathway for drainage, which was profuse. However, the patient became swollen and was sent to an oral surgeon, who opened the area and did a biopsy; report indicated rhabdomyosarcoma.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 319
taking antiinflammatories, but they may not be taking suf-ficient doses to have an impact on the problem at hand. Because most pain of tooth origin is inflammatory in nature, there are few medications the clinician can prescribe that are superior to over-the-counter (OTC) NSAIDs. The OTC market is redundant with aspirin and acetaminophen sub-stitutes that are both analgesics and antiinflammatories. In fact, recent data support the combined used of ibuprofen (600 mg) and acetaminophen (1000 mg) to achieve anal-gesia and pain relief equivalent to that of a narcotic without the side effects.14,27 Despite such findings, no correlating decrease in purchases of prescription analgesics has been documented.
If analgesics and/or antibiotics are being prescribed on a regular basis to manage endodontic emergencies, there is likely a problem with accurate diagnosis and treatment tech-niques. Pain is not an indication for antibiotic treatment.19
basis. However, most clinicians would agree that because the patient is in a potentially labile state that could become unstable and serious very rapidly, one-appointment treat-ment is unadvisable. The patient should be reassessed every few days. Because cleaning, shaping, and obturation can cause additional irritation to periapical tissues, the clinician should wait for signs and symptoms to subside before treat-ment completion. If lymphadenopathy is present, the enlarged nodes should be responding to the antibiotic treat-ment before additional root canal procedures. Once resolved, treatment can be completed.
Analgesics and AntibioticsWith the advent of nonsteroidal antiinflammatory drugs (NSAIDs), many patients present to the dental office already
A B
FIGure 15-20 A, This patient was in severe pain, and the referring dentist could not find the root canal to begin revision. For pain relief, trephination was indicated on the mandibular first premolar. The mental foramen did not appear to preclude this approach to pain relief. b, Use of a curette to establish direct and immediate drainage.
BA
FIGure 15-21 A, Buccal cellulitis in the right mandible. Place the patient on antibiotics, and wait for a reduction in the swelling or if fluctuant, incise and drain. b, Facial cellulitis in the canine space; arrows indicate extent of swelling.

320 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
improvement in the first 24 to 48 hours, and the fact that the cellulitis has not increased during this latency period should be ample support for the clinician that the antibiotic is working appropriately. Switching antibiotics within the 24- to 48-hour time frame at the behest of a patient who has not seen improvement occurs too often via a phone call. The clinician should see the patient and make a proper objective evaluation of the patient’s condition.
For the benefit of the patient, first and foremost the clini-cian should be cognizant of the following considerations:
• The reduction or disappearance of pain is an excellent indicator of the effectiveness of the treatment, even if some residual swelling remains.
• When a patient presents with a definite indication for antibiotic use, the clinician should not consider the patient’s remaining status quo for the first 2 to 3 days of therapy indicative of antibiotic failure if prescribed properly.
• A loading dose is recommended when the patient presents with a fever, lymphadenopathy, or moderate cellulitis.
• Most antibiotics will not produce significant clinical changes or effects within the first 24 to 48 hours.
• The clinician should not consider switching antibiotics within the first 24 to 72 hours after the initial dose unless the patient is demonstrating rapid and significant clinical signs/symptoms of deterioration. At this point, referral to a specialist is probably indicated.
Anesthesia for Painful TeethOne of the greatest problems in managing pain of tooth origin is inability to provide adequate anesthesia for the patient in distress.13 With the advent of newer anesthetic devices, much if not all of the discomfort can be eliminated. Problem solving painful tooth emergencies mandates an understanding of the inflammatory processes involved,3 a knowledge of the osseous and neural variations of the area to be anesthetized, knowledge of the action of anesthetic solu-tions, skill in administering solution to the target area, and an appreciation for the psychologic makeup of the patient.
The normal pulp has a relatively high blood flow that is minimally influenced by vasodilator substances (irritational products). This results in only minor increases in localized blood flow during irritation and inflammation.20 In this inflamed environment, capillary permeability appears then to be more significant than blood flow with regard to the inflammatory response of the pulp. This rules out the concept of generalized pulpal edema, despite the low-compliance environment within the tooth. The localized inflamed tissues experience an increase in tissue pressure that results in a focal vascular stasis, ischemia, and tissue necrosis. These focal areas of necrosis serve as additional insults within the pulp, and the subsequent cyclic episodes of inflammation and cellular death result in the incremental circumferential spread of tissue destruction.40
Pain before or after an emergency appointment does not necessarily indicate an infection or the need for antibiotic coverage. Mild pain and occasionally moderate pain are normal consequences of treatment intervention. Not every patient will be completely pain free immediately afterward, but the majority will be improved significantly or completely within 1 to 3 days following any type of emergency manage-ment. If this is not the case, reevaluation of clinical proce-dures and diagnostic techniques is in order. When endodontic treatment procedures are managed properly, the incidence of a painful response requiring emergency treatment is docu-mented at only 3% to 5%.42
Overuse of antibiotics became a significant problem in the late 20th century.15,16 Clinicians prescribed antibiotics for everything from routine problems such as pain after instru-mentation to “covering” a potential infection when a diag-nosis could not be determined and the practitioner felt obligated to “do something” for the patient. This blatant misuse of antibiotics resulted in the development of antibiotic-resistant bacteria, but increasing awareness of such harmful consequences has fortunately led to more judi-cious prescribing practices.
When antibiotics are prescribed because a patient is febrile, the effect of this medicament will not manifest for several days. The fact that the patient’s temperature is not continu-ing to rise is usually indicative that the antibiotic is working appropriately and that additional antibiotics or switching antibiotics is not indicated (Fig. 15-22). Patients often need education in this regard if they expect antibiotic treatment to have immediate results.
The same is true for a patient who presents with a cellu-litis. If placed on an antibiotic, there will be minimal
FIGure 15-22 In febrile patients, periodic assessment is necessary to monitor the situation, and referral is often indicated for possible extraoral incision and drainage.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 321
but affect the entire neuron cell membrane in every involved fiber. The nature of these changes is such that the reduction in ion flow and in action potential created by local anesthetic agents is not sufficient to prevent impulse transmission for the reason that the lowered excitability threshold allows transmission even under conditions of anesthesia.3,41 As sug-gested by some investigators, an increase in anesthetic con-centration (not necessarily volume) is required to lower the neural action potential when attempting to achieve complete anesthesia in the presence of inflamed tissues.42 An alternative approach would be to administer the local anesthetic remote from the area of inflammation, such as the use of a regional nerve block whenever possible, especially in the case of exten-sive cellulitis.7
Variations in the osseous anatomy surrounding tooth roots and aberrant neural structures have received renewed attention as potential impediments to administering success-ful anesthesia.8,42 The common variations encountered are discussed relative to the maxilla and mandible, along with the suggested sequence for achieving profound anesthesia in each jaw.
Generally the outer cortical plate of the maxillary bone is thin and sufficiently porous in the adult to make infiltration anesthesia effective. However, in facial or buccal areas of the zygomatic alveolar crest, penetration of the anesthetic solu-tion to the middle superior alveolar nerve may be restricted, especially in children. Likewise, the absence of this neural branch has been reported, requiring more extensive place-ment of the anesthetic solution to manage the first molar and premolars.
Anteriorly, the prominence of the anterior nasal spine and prominent floor of the piriform aperture may preclude approximation of the root apices of the incisor teeth. In the premolar and molar region, the position of the palatal roots relative to the buccal cortical plate may by necessity require placement of palatal infiltration anesthesia.
Providing adequate anesthesia in the maxillary arch is not difficult. Most often the inability to do so cannot be attrib-uted to the presence of infection but rather to error in tech-nique and placement of the anesthetic solution. For the patient in pain, maxillary infiltration in the buccal or labial vestibule of one carpule (1.8 mL) is usually sufficient for anterior teeth; however, some maxillary anterior teeth are palatally inclined (lateral incisors, some central incisors, canines), whereas others have palatal roots that must also be anesthetized. These roots are often overlooked after the buccal infiltration, and the patient experiences needless discomfort.
Infiltration on the facial or buccal side should vary from the standard approach of depositing the solution near the apex with the needle parallel to the long axis of the root. Rather, an angulated approach directed at the root apex will usually provide a more rapid and accurate diffusion through the bone.
Palatal infiltration should be used routinely, especially when the patient is already somewhat hypersensitive.25 Knowledge of the exact location of the palatal apex with
The periodic irregular inflammation and destruction of localized tissue components coupled with bacterial invasion can only partially explain the clinical experience of episodic pain. Further explanation may include neural fluctuations, with cycles of increased nerve-fiber and peptide cytochemical alteration followed by decreases, perhaps associated with cycles of intrapulpal abscess expansion and pulpal attempts at repair.3 Interestingly in this respect, the sprouting of new nerve fibers and alterations in neuropeptides associated with a painful carious attack have been identified. Likewise, sus-tained severe pain might be interpreted as multiple areas of tissue simultaneously undergoing demise. In many patients, episodes of severe pain are often followed by the absence of symptoms, indicating pulpal necrosis or that an effective avenue of drainage from the inflammatory process has been obtained.
The inflammatory process of pulpal disease and degenera-tion is basically the same as elsewhere in the body’s connec-tive tissue. When coupled with endodontic procedures, coronal leakage of bacteria and their products from inferior dental restorations, or toxic root canal filling materials, the periradicular tissues will appear variable with regard to inflammation and repair. Histologically, the lesion consists predominantly of granulation tissue, exhibiting significant angioblastic activity, many fibroblasts, connective-tissue fibers, an inflammatory infiltrate, and often connective-tissue encapsulation. The inflammatory infiltrate consists of plasma cells, lymphocytes, mononuclear phagocytes, and neutro-phils. Occasionally cholesterol clefting is seen along with foreign-body giant cells. If, in addition, adjacent strands of epithelium or rests of Malassez have been stimulated by the inflammatory response to form a stratified squamous epithelium–lined cavity filled with fluid or semisolid mate-rial, a cyst will be present.
As long as there is an egress of tissue irritants and bacteria from the root canal system, or there is a failure of the phago-cytic macrophage system to control this irritation, the histo-logic pattern of the periradicular lesion will be one of concomitant repair and destruction. Often this variable tissue response is subjected to superimposed inflammatory, infec-tive, or immunologic processes, and patient signs and symp-toms will reflect these changes, moving from a chronic clinical state of minimal to no symptoms to an acute state with the complete litany of painful characteristics.
The inflammation that accompanies pulpal and periapical degenerative/infective changes results in a reduced tissue pH over variable areas, depending on the extent and acuteness of the process. This has been suggested as the explanation for the difficulty in achieving quality anesthesia, because the ability of the weak anesthetic base (pKa 7.5 to 9) to dissociate is significantly affected. Others have suggested that inflam-mation alters peripheral sensory nerve activity, possibly because of neurodegenerative changes along the inflamed neural element distal from the inflammatory site. Research data suggests that nerves located in inflamed tissue have altered resting potentials and excitability thresholds and that these changes are not restricted to the inflamed pulp itself

322 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
accessory innervation has received the most attention.5 These range from the presence of well-defined foramina in the retromolar fossa (Fig. 15-24),17 to extension to and innerva-tion of both posterior and anterior teeth by branches of the mylohyoid nerve,9,23 to the presence of median symphyseal crossover from branches of the incisive nerve. Finally, the existence of a transverse cervical cutaneous nerve that may intermingle with fibers of the mental nerve has been sug-gested to enter the mental foramen and course posteriorly, innervating the premolars or molar teeth.35,36
The mandibular posterior teeth are perhaps the most dif-ficult to anesthetize adequately. The reasons are multiple and include accessory nerve innervation, inadequately adminis-tered mandibular blocks, and lower pain thresholds for inflamed teeth.29,41-43 However, a few basic principles can aid in achieving profound anesthesia:
• Do not infiltrate for the purpose of anesthetizing accessory innervation until the mandibular block has been given and lip signs indicate profound anesthesia.
• Infiltrate one-third carpule of anesthetic solution around the affected tooth.
• Use a mental block and/or mylohyoid infiltration with mandibular molars.
• Do not attempt root canal treatment until the tooth can undergo percussion (if originally sensitive) or until the stimulus of pain (cold, heat) can be placed on the tooth without discomfort.
Too often the clinician fails to wait an adequate amount of time before initiating emergency treatment, and the cold water or air from the turbine causes severe pain for the patient. This lessens the patient’s confidence in the practitio-ner and decreases the patient’s pain threshold. If after these basic principles have been followed, adequate anesthesia still has not been achieved, intraligamental injection (Fig. 15-25) or intraosseous injections (Stabident [Fairfax Dental Inc., Miami, FL, USA]; X-tip [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]) may be considered.24 However, with mul-tirooted teeth, intraligamental and intraosseous injections should be placed beside or near each root for complete anes-thesia. This is especially true in molar teeth, where in some
respect to the palatal vault is critical for proper placement of the anesthetic solution and elimination of any painful response. Block anesthesia, such as an infraorbital block, posterior superior alveolar block,22 or injection into the greater palatine foramen, is considered very good for achiev-ing maximum anesthesia, especially in cases where the patient has minimal discomfort.
The mandibular foramen is the primary target for deposi-tion of anesthetic solution for profound anesthesia of the mandibular teeth. Although the position of the foramen is variable, it is usually found anterior to the midpoint of the ramus of the mandible when the anterior border of the man-dible is defined as the internal oblique ridge (Fig. 15-23).17,31 Studies have identified this position as slightly above the occlusal level of the molar teeth.18 The importance in this variability cannot be overemphasized for the clinician, because the angle and level of needle penetration will have to be reassessed and altered accordingly in many cases in which profound anesthesia is not readily achieved with a standard approach. Although rare, the potential for extreme variability in the coursing of the mandibular canal has been identified, even to the extent of bifidity. Conventional attempts at mandibular blocks in these cases may lead to failure. Examination of panoramic views of the mandible is extremely helpful to anticipate variations of this nature, at least two-dimensionally.
Of all the variables that create controversy in achieving profound anesthesia in the mandible, the presence of
AF
FIGure 15-23 Note the position of the entry of the mandibular nerve into the lingual surface of the ramus of the mandible (arrow). Also note the excessive foramina and their positions on the ramus wall. Many of these foramina are located well above the occlusal plane, which may influence positioning the needle for mandibular anesthesia.
FIGure 15-24 Note the vast number of foramina on the retromolar pad in this mandibular cadaver specimen.

chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies 323
chamber, with the anesthetic agent injected during penetra-tion. Often only a few drops of solution are necessary to anesthetize the pulp tissue. The intrapulpal technique may anesthetize only the coronal pulpal tissue. Often the vital tissue in the canals has not been properly anesthetized, and a pulpectomy should not be attempted. In some cases, total pulpal anesthesia can be achieved, and the pulp can be removed in its entirety. After complicated crown fractures (see Chapter 19), especially in the presence of soft-tissue swelling, injections can be given directly into the site of the pulp exposure. Rapid anesthesia is achieved with minimal patient discomfort.
ReFeReNCeS1. Aubrey J: In Foley GH, editor: Foley’s footnotes, Wallingford, PA.,
1972, Washington Square East.2. Birchfield J, Rosenberg PA: Role of anesthetic solution in
intrapulpal anesthesia, J Endod 1:26-27, 1975.3. Byers MR, Taylor PE, Khayat BG, et al: Effects of injury and
inflammation on pulpal and periapical nerves, J Endod 16:85-91, 1990.
4. Carter RB, Keen EN: The intramandibular course of the inferior alveolar nerve, J Anat 108:433-440, 1971.
5. Chapnick L: Nerve supply to the mandibular dentition: a review, J Can Dent Assoc 46:446-448, 1980.
6. Elliott JA, Holcomb JB: Evaluation of a minimally traumatic alveo-lar trephination procedure to avoid pain, J Endod 14:405-407, 1988.
7. Evers H, Haegerstam G: Introduction to dental local anesthesia, Fribourg, 1990, Mediglobe, SA, p 91.
8. Fragouli E: Anaesthesia in endodontics, ENDO (Lond Engl) 2:171-184, 2008.
9. Frommer J, Mele FA, Monroe CW: The possible role of the mylo-hyoid nerve in mandibular posterior tooth sensation, J Am Dent Assoc 85:113-117, 1972.
10. Gutmann JL: A clinical repair—predictive/treatment approach to pulpal diagnosis, BCDS Forum 2(2):9-10, 1982.
cases the distal root is separated from the mesial root by a considerable distance.
If all other techniques fail to provide proper anesthesia, or if the area into which the anesthetic solution is placed may be compromised (swelling, trauma), intrapulpal anes-thesia can be used (Fig. 15-26).8 This technique may initially evoke pain until the pulp has been penetrated.2 Therefore, attention to proper technique is mandatory. To gain entrance to the pulp chamber with the least amount of patient dis-comfort, a No. 1 or 2 round bur is used in short incremental strokes. The bur is used to cut into the center of what would normally be the outline of the access opening prepa-ration, or it is directed to the highest pulp horn. If the bur penetrates only a few tenths of a millimeter at a time into the tooth, severe discomfort is minimized, and access to the pulp is achieved (Fig. 15-27). A 30-gauge needle is passed into the small opening in the roof of the pulp
FIGure 15-26 Use of the intrapulpal injection technique using a 30-gauge needle in a patient who has suffered facial trauma and has significant swelling.
FIGure 15-25 Use of a periodontal ligament injection can be beneficial in many cases of pain in mandibular teeth.
FIGure 15-27 The pulp is barely exposed but sufficient for a 30-gauge needle to penetrate for the delivery of intrapulpal anesthetic solution. Upon insertion, immediate and forceful pressure on the syringe should be applied to anesthetize the dental pulp.

324 chapter 15 | Problem Solving in the Management of Painful Tooth Emergencies
30. Natkin E: Treatment of endodontic emergencies, Dent Clin North Am 18:243-255, 1974.
31. Nicholson ML: A study of the position of the mandibular foramen in the adult human mandible, Anat Rec 212:110-112, 1985.
32. Nusstein JM, Reader A, Beck M: Effect of drainage upon access on postoperative endodontic pain and swelling in symptomatic necrotic teeth, J Endod 28:584-588, 2002.
33. Oguntebi BR, DeSchepper EJ, Taylor TS, et al: Postoperative pain incidence related to the type of emergency treatment of symptom-atic pulpitis, Oral Surg Oral Med Oral Pathol 73:479-483, 1992.
34. Roda RS, Blanton PL: The anatomy of local anesthesia, Quintes-sence Int 25:27-38, 1994.
35. Rood JP: The analgesia and innervations of mandibular teeth, Br Dent J 140:237-239, 1976.
36. Rood JP: Some anatomical and physiological causes of failure to achieve mandibular analgesia, Br J Oral Surg 15:75-82, 1977-1978.
37. Siqueira JF, Jr: Aetiology of root canal treatment failure: why well-treated teeth can fail, Int Endod J 34:1-10, 2001.
38. Siqueira JF, Jr: Microbial causes of endodontic flare-ups, Int Endod J 36:453-463, 2003.
39. Tjäderhane LS, Pajari UH, Ahola RH, et al: Leaving the pulp chamber open for drainage has no effect on the complications of root canal therapy, Int Endod J 28:82-85, 1995.
40. Van Hassel HJ: Physiology of the human dental pulp, Oral Surg Oral Med Oral Pathol 32:126-134, 1971.
41. Wallace JA, Michanowicz AE, Mundell RD, et al: A pilot study of the clinical problem of regionally anesthetizing the pulp of an acutely inflamed mandibular molar, Oral Surg Oral Med Oral Pathol 59:517-521, 1985.
42. Walton RE, Torabinejad M: Managing local anesthesia problems in the endodontic patient, J Am Dent Assoc 123:97-102, 1992.
43. Wong MKS, Jacobsen PL: Reasons for local anesthesia failures, J Am Dent Assoc 123:69-73, 1992.
44. Wu MK, Dummer PM, Wesselink PR: Consequences of and strategies to deal with residual post-treatment root canal infection, Int Endod 39:343-356, 2006.
ReCoMMeNDeD ADDITIoNAl ReADINgCohen LA, Bonito AJ, Akin DR, et al: Toothache pain: a comparison
of visits to physicians, emergency departments and dentists, J Am Dent Assoc 139:1205-1217, 2008.
Colleagues for Excellence: Taking the pain out of restorative dentistry and endodontics: current thoughts and treatment options to help patients achieve profound anesthesia, Chicago, 2009, Am Assoc Endodontists, Winter.
Happonen R-P, Bergenholtz G: Apical periodontitis. In Bergenholtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodontol-ogy, Oxford, 2003, Blackwell Munksgaard.
Little JW, Falace DA, Miller CS, et al: Antibiotic prophylaxis in den-tistry: an update, Gen Dent 56:20-28 2008.
Skaug N: Systemic complications of endodontic infections. In Bergen-holtz G, Hørsted-Bindslev P, Reit C, editors: Textbook of endodon-tology, Oxford, 2003, Blackwell Munksgaard.
11. Gutmann JL: Endodontic emergency treatment, J Calif Dent Inst Contin Educ 42:3-48, 1992.
12. Gutmann JL, Harrison JW: Surgical endodontics, St Louis, 1991, IEA [Ishiyaku EuroAmerica] Publishers Inc.
13. Gutmann JL: Problems attaining local anesthesia with endodontic emergencies, Anesth Pain Control Dent 2:133-139, 1993.
14. Hargreaves KM, Keiser K: New advances in the management of endodontic pain emergencies, J Calif Dent Assoc 32:469-473, 2004.
15. Harrison JW, Svec TA: The beginning of the end of the antibiotic era? Part I. The problem: abuse of the “miracle drugs”, Quintes-sence Int 29:151-162, 1998.
16. Harrison JW, Svec TA: The beginning of the end of the antibiotic era? Part II. Proposed solutions to antibiotic abuse, Quintessence Int 29:223-229, 1998.
17. Haveman CW, Tebo HG: Posterior accessory foramina of the human mandible, J Prosthet Dent 35:462-468, 1976.
18. Heaseman PA: Variation in the position of the inferior dental canal and its significance to restorative dentistry, J Dent 16:36-39, 1988.
19. Henry M, Reader A, Beck M: Effect of penicillin on postoperative endodontic pain and swelling in symptomatic necrotic teeth, J Endod 27:117-123, 2001.
20. Heyeraas KJT: Vascular reactions in the dental pulp during inflam-mation, Acta Odontol Scand 4:247-256, 1983.
21. Houck V, Reader A, Beck M, et al: Effect of trephination on post-operative pain and swelling in symptomatic necrotic teeth, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90: 507-513, 2000.
22. Loetscher CA, Melton DC, Walton RE: Injection regimen for anesthesia of the maxillary first molar, J Am Dent Assoc 117:337-340, 1988.
23. Madeira MC, Percinoto C, Silva MGM: Clinical significance of supplementary innervation of the lower incisor teeth: a dissection study of the mylohyoid nerve, Oral Surg Oral Med Oral Pathol 46:608-614, 1978.
24. Malamed SF: The periodontal ligament (PDL) injection: an alter-native to the inferior alveolar block, Oral Surg Oral Med Oral Pathol 53:117-121, 1982.
25. Malamed SF: The management of pain and anxiety. In Cohen S, Burns R, editors: Pathways of the pulp, ed 6, St Louis, 1994, Mosby.
26. Matthews DC, Sutherland S, Basrani B: Emergency management of acute apical abscesses in the permanent dentition: a systematic review of the literature, J Can Dent Assoc 69:660, 660a-660i, 2003.
27. Menhinick KA, Gutmann JL, Regan JD, et al: The efficacy of pain control following nonsurgical root canal treatment using ibuprofen or a combination of ibuprofen and acetaminophen in a random-ized, double-blind, placebo-controlled study, Int Endod J 37:531-541, 2004.
28. Moos HL, Bramwell JD, Roahen JO: A comparison of pulpectomy alone versus pulpectomy with trephination for the relief of pain, J Endod 22:422-425, 1996.
29. Najjar TA: Why can’t you achieve adequate regional anesthesia in the presence of infection? Oral Surg Oral Med Oral Pathol 44:7-13, 1977.

325
part 3 Problem-Solving Treatment Procedures in Surgical Procedures
Chapter 16
Problem-Solving Challenges in Periapical Surgery
Problem-Solving ListProblem-solving challenges encountered in periapical surgical considerations addressed in this chapter are:
Rationale for Surgical Endodontic Treatment
Indications for Apical Surgery
Failure of nonsurgical root canal treatment or persistent apical radiolucencies
Reaction to Foreign Bodies in the Periapical Tissues
Root Canal Anatomy That Is Impossible to Manage Nonsurgically
Anatomic obstructions
Iatrogenic obstructions
Failure of previous periapical surgery
Surgical Access and Manipulative Techniques: In Vitro Directives
Surgical Access and Manipulative Techniques: In Vivo Directives
Surgical anatomy
Anesthesia and hemostasis
Soft-tissue considerations: flap design
Curettage and enucleation of the soft-tissue lesion when the lesion penetrates the bone
Root apex exposure in the absence of a periapical lesion
Root-end resection and identifying the root canal space
Root-end cavity preparation
Root-end fillings: materials and placement
Tissue repositioning and stabilization
Postsurgical Care and Potential Complications
Complications
Probably the first requisite for a successful operation is that the operator should be thoroughly familiar with the anatomy of the region.2
J.R. Blayney, 1932
Rationale for Surgical Endodontic Treatment
There are multiple treatment planning options for root-treated teeth that develop recurrent periapical pathosis or have periapical lesions that fail to heal following adequate root canal treatment. While nonsurgical revision is usually the clinical treatment of choice,3 many teeth are unsuitable for revision owing to irreversible changes in the tooth or to the nature of the periapical pathosis.5 Furthermore, there are very few studies that reflect high levels of evidence relative to the success or failure of nonsurgical revision.44 Periapical surgery is not only appropriate for these cases10 but also for the occasional case in which nonsurgical revision is possible but may result in excessive destruction of either the tooth or restoration. In fact, data show that the success rate for surgical intervention may be higher than that for nonsurgical revi-sion* and should be considered in the treatment-planning
process when teeth are compromised with failure of previous root treatment.1 The choice of periapical surgery is a valid alternative to tooth extraction17 and should always be considered. At the same time, there may be unique cir-cumstances that indicate extraction would be the treatment
Pulpless teeth, no matter how well filled, with the slightest previous history of functional or periodontal disturbance which showed any evidence of apical denudation (as indicated by variation in the lamina dura and trabeculae and periodontal width, when compared with adjacent normal teeth) should be root resected.12
C.F. Fawn, 1927
*References 10, 11, 32, 43, 56, and 60.

326 chapter 16 | Problem-Solving Challenges in Periapical Surgery
Indications for Apical SurgeryFailure of Nonsurgical Root Canal Treatment or Persistent Apical RadiolucenciesSeveral etiologies have been identified for persistent periapi-cal pathosis following nonsurgical root canal treatment.* Of all factors identified, the only one for which nonsurgical revi-sion would have a predictably high chance for success is the case of inadequate initial root canal treatment in which there are no iatrogenic alterations of the canal morphology8,19 (Fig. 16-1). If the apical 2 to 3 mm of canal space was cleaned and shaped minimally in the original treatment or left completely uncleaned, the procedures of revision would not differ sig-nificantly from routine root canal treatment of any similar tooth.3 The prognosis for healing would be correspondingly very good (Fig. 16-2).
Inadequate nonsurgical root canal treatment in teeth with significant alteration of the root canal morphology is not unusual in cases with recurrent or persistent apical pathosis (Fig. 16-3). A poor healing response would be expected after nonsurgical revision owing to the increased difficulty or impossibility of cleaning, disinfecting, and obturating the altered apical canal anatomy. While the level of success with nonsurgical revision is below that of initial treatment,32,74,75 nonsurgical revision is still indicated in most cases as the
of choice. Even in these situations, the option for intentional replantation73 may exist, and an informed clinician will usually take into account all options before condemning a tooth to removal.
It may appear that no treatment and a watchful waiting period is an additional option, but in reality, this approach only delays the decision to choose one of the other viable treatment plans. Furthermore, a significant delay in treat-ment may result in irreversible bone loss and limit the ulti-mate choice of treatment to extraction.
The theory and treatment planning behind the choice of periapical surgery has not varied much from the earliest citations in the endodontic literature.24 The objectives are to eliminate any periapical reactive tissues when present and to clean and seal all communications from the root canal space through a surgical approach to the apex. His-torically, however, it was not uncommon to perform a surgical curettage with the belief that the patient’s problem resided in the inflamed/infected tissue around the end of the root.24 More often than not, the source of the problem was failure to clean, disinfect, and fill the root canal space, or to seal the canal space coronally, permitting leakage into a poorly managed root canal system. Ironically, both of these issues would ultimately doom the tooth to extraction following the surgical procedure because of the recurrence of pathosis. Substantial changes in understanding the causes of the disease processes, improvements in surgical techniques, and enhanced choices for root-end materials, supported by a wealth of excellent research,21 have made surgical end-odontics a reasonable and predictable choice in tooth retention.13,38,58,77
BA
FIGURe 16-1 a, Maxillary lateral incisor with inadequate root canal treatment. Note that the apical canal anatomy has not been altered during the root canal. B, Mandibular molar with inadequate root canal treatment and persistent apical pathosis. There has been no alteration of the apical canal morphology, owing to complete lack of apical preparation.
*References 4, 41, 42, 47-49, 74, and 75.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 327
BA
FIGURe 16-2 a, Persistent periapical pathosis on a tooth with inadequate root canal treatment. B, Following removal of the crown and post, routine root canal procedures were used in revision. Reevaluation at 8 months indicating normal healing.
primary approach, since healing may be possible despite the diminished prognosis (Fig. 16-4). After a suitable period of healing time, usually 6 to 12 months, apical surgery would become the treatment of choice for those that fail to heal. In all cases of nonsurgical revision, the patient should be informed that healing may be delayed and surgical revision may yet be necessary.
Four causes of persistent periapical pathosis that are unlikely to be identified or differentiated by clinical or radiographic means41,42,74,75 are infection located in inaccessible spaces in
the root canal system16,30,47-49,71 (Figs. 16-5 and 16-6), infec-tion located outside the root canal in the apical lesion itself 47-49 (Fig. 16-7), true cysts or tumors (Fig. 16-8), and vertical root fracture (see Fig. 4-12, B). The chief clinical presentation is a nonhealing periapical lesion after acceptable root canal treat-ment. The specific etiology is usually not identifiable pre-operatively and is confirmed either at the time of surgery by direct observation or later by histologic examination.41,42
Residual bacteria located in inaccessible parts of the root canal system have been the subject of considerable research.
B CA
FIGURe 16-3 a, Inadequate root canal treatment with significant alteration of the canal morphology. It appears that the apical foramen was grossly enlarged. B, Inadequate root canal treatment with perforation of the apical foramen. C, Inadequate root canal treatment with alteration of the canal morphology. Periapical surgery would be required to treat all three of these cases.

328 chapter 16 | Problem-Solving Challenges in Periapical Surgery
A B
C
FIGURe 16-4 a, Recurrent periapical pathosis on a mandibular molar with inadequate root canal treatment. B, Working length measurement radiograph indicating significant alteration of the apical canal morphology from the original treatment. C, Reevaluation at 8 months indicating excellent periapical and furcation healing.
FIGURe 16-5 Demineralized tooth demonstrating inaccessible canal spaces at the apex along with the presence of silver cone corrosion product that contributed to persistent periapical pathosis.
Histologic studies of resected root tips and microbiologic studies of bacteria sampled from root canals have identified that the majority of root canal treated teeth with asymptom-atic periapical periodontitis harbored persistent bacteria in the apical portion of the complex root canal system.42,48,49,71,74 From a clinical standpoint, there is no available method to
detect such spaces, but knowledge of their possible presence should serve to increase the thoroughness of canal prepara-tion during routine treatment (Fig. 16-9).
Cases of persistent periapical infection caused by bacteria that persist after adequate root canal treatment are not common. In some cases, these pathogens have established a

chapter 16 | Problem-Solving Challenges in Periapical Surgery 329
A B
FIGURe 16-6 a, 6-month reevaluation after root canal treatment of a mandibular left central incisor indicating the lesion had failed to heal. B, Postsurgical treatment radiograph. During surgery, multiple accessory canals were observed as the apical bevel was prepared. The canal had been well filled.
BA
FIGURe 16-7 a, Large radiolucency around maxillary right incisors. Root canal treatment had no impact on the course of the acute infection. Infection gradually involved the bone of adjacent vital teeth. B, Surgical exposure and curettage 1 week after root canal treatment. The infection continued. The central and lateral incisors were ultimately extracted, after which healing progressed uneventfully.
BA
FIGURe 16-8 a, Large radiolucency associated with a failed root canal with silver cones. B, Reevaluation after 6 months indicating radiographic resolution of the lesion. Histologic examination confirmed a true cyst.

330 chapter 16 | Problem-Solving Challenges in Periapical Surgery
during periapical surgery, a fracture line is observed to origi-nate at the apex and extend coronally. If there is no extension through the attachment, the fracture line may be repaired as part of the root-end filling (Fig. 16-10).
Reaction to Foreign Bodies in the Periapical Tissues
At times gutta-percha filling material may be inadvertently extruded through the apical foramen or lateral foramina during obturation.37,54,76 The appearance of a small amount of filling material at the apex or at a lateral canal site is not
A
EP
B
FIGURe 16-9 a, Histologic section of a resected root apex from the mesial buccal root of a maxillary first molar. Note the canal with the arrow was cleaned, shaped, and obturated, but the canal configurations in the rest of the root were not touched during root canal procedures. Tissue debris is still present, and at the end of the root, there is a cyst forming (EP, epithelium). B, Resected root apex from a maxillary lateral incisor demonstrating multiple canal openings and irregularities. Thorough cleaning and disinfecting of these aberrations is all but impossible and may hold the irritants that result in persistent periapical pathosis.
A B
FIGURe 16-10 a, Vertical root fracture extending coronally from the apex. It did not extend through the attachment. B, Repair of the fracture with mineral trioxide aggregate as part of the periapical filling.
recalcitrant extraradicular infection that requires surgery.61-63 The identification of pathogens implicated in this process is usually based on postsurgical histologic examination of the resected tissues.15,61,62 Like true cysts or periapical pocket cysts (bay cysts),41,42,53 the clinical diagnosis is usually a nonhealing periapical lesion of indeterminate cause.61,62
The diagnosis of vertical root fractures was discussed in Chapter 4. Most of these defects will be found to extend through the gingival sulcus, exhibiting a unique periodontal defect that can be probed. In the context of etiology for persistent periapical pathosis, some vertical fractures may not probe or be detectable by radiographic means, such as the case presented in Chapter 18, Fig. 18-17. Occasionally

chapter 16 | Problem-Solving Challenges in Periapical Surgery 331
CLINICAL PROBLEMProblem: Root canal treatment was completed 1 month pre-viously on the maxillary right first molar. The postoperative radiograph indicated an acceptable and unremarkable result. The patient continued to complain that since the day of treat-ment, there has been a small lump over the apex in the vesti-bule that remains tender to touch. Clinical examination confirms the small nodule that is locally inflamed and sore to palpation.
Solution: The apices of many maxillary premolar and molar buccal roots are very superficial relative to the surface of the bone (fenestration) (Fig. 16-13).24 If gutta-percha filling material/sealer are extruded through such a root, it will some-times extend laterally into the periosteal tissues. The radio-graph may not look unusual, since the extruded material is often angled toward the x-ray beam. Periapical surgery will be necessary to remove the extruded material and resect the root end into the bony housing. This will usually resolve the problem (Fig. 16-14). Rarely, a bone graft and membrane may need to be considered.68
A B
FIGURe 16-11 a, Obturated mandibular molar with extrusion of filling materials out of a large lateral canal in the mesial root and the apical foramen of the distal root. Note the extent bone destruction in the furcation. B, Healing in progress 6 months later.
BA
FIGURe 16-12 a, Inadvertent extrusion of gutta percha through the apical foramen during routine obturation. B, Six-month reevaluation indicating normal healing despite the presence of the extruded material.
unusual and is even considered desirable or “esthetic” by some practitioners. Rarely do these materials present a prog-nostic problem (Fig. 16-11).
Occasionally, excessive material may be extruded, which clearly does not look “esthetic” on the postoperative radio-graph. Nevertheless, if the apical foramen is clean and well sealed, lesions will heal around the extruded material. Assum-ing the patient is comfortable, the best postoperative course is reevaluation in 6 to 12 months (Fig. 16-12). If symptoms or signs of pathosis either persist or recur, surgery might be indicated before a 6-month reevaluation. Even if the patient has been comfortable, apical surgery would also be indicated if the lesion showed no radiographic signs of resolution at the time of reevaluation.
Paste-type root filling materials are largely uncontrollable when placed with a lentulo spiral. If the apical foramen is naturally large or has been enlarged during canal cleaning and shaping, the paste material can be forced through the apex into apical bone, the sinus, or the mandibular canal. Exces-sive extrusion of these materials can result in persistent periapical pathosis. Surgery is indicated to both remove the

332 chapter 16 | Problem-Solving Challenges in Periapical Surgery
FIGURe 16-13 Cadaver specimen of the right maxilla illustrating the superficial relationship of the buccal roots to the surface of bone.
FIGURe 16-14 Clinical photograph of gutta-percha that had been extruded into the submucosal tissues. Periapical surgery was required for removal.
B
C
A
FIGURe 16-15 a, Radiograph illustrating extrusion of paste filling material into the maxillary sinus. B, Radiograph demonstrating gross extrusion of paste filling material into the periapical bone of the maxillary right lateral incisor, causing acute periapical periodontitis. C, Clinical photograph depicting removal of the extruded material during periapical surgery.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 333
FIGURe 16-16 Radiograph of a mandibular premolar with severe apical curvature in the canal that proved to be nonnegotiable to the apex. Surgery was indicated to resolve the persistent apical periodontitis.
excess and ensure the canal is filled properly at its terminus (Fig. 16-15).
Root Canal Anatomy That Is Impossible to Manage Nonsurgically
Some teeth have root shapes that prove impossible to treat nonsurgically. Severe curvature combined with calcifications can prevent negotiation to the terminus of the root canal (Fig. 16-16).
Anatomic ObstructionsThe standard of care for treatment of teeth with open apices centers around techniques and materials that result in the formation of a calcified apical barrier. Apical surgery would be indicated in cases that fail to develop the barrier or in which the canal anatomy prevents using the technique. Fig. 16-17 illustrates a case in which an early radiograph indicated the formation of a dens in dente in a maxillary lateral incisor.
Five years later, the patient developed an acute apical abscess, and the periapical film at the time of emergency treatment confirmed that the apex had not developed. It was judged that nonsurgical access through the dens in dente would be destructive and would in itself diminish the long-term prognosis of the tooth. Apical surgery in this case was the most effective and least invasive option.
One of the most common complications in routine root canal treatment is the presence of calcified material in the root canal space. Chapters 8 and 13 discussed the various techniques for successfully locating and penetrating canals that appear radiographically to be partially or completely closed. Nevertheless, some of these teeth are in reality calci-fied to the extent that penetration to the apex is not possible
B
C
A
FIGURe 16-17 a, Dens in dente formation in developing lateral incisor. B, Five-year reevaluation indicating an apical lesion and incomplete apex formation. The patient presented on emergency with an acute apical abscess. C, A 19-month postsurgical reevaluation indicating excellent healing.

334 chapter 16 | Problem-Solving Challenges in Periapical Surgery
in the canal space that prevent the use of nonsurgical revision techniques (see Chapter 14). The placement of these materi-als could have been intentional, as in the case of posts, or accidental, as in the case of instrument separation. Chapter 14 describes the usual techniques for removing these materi-als or obstacles, but at times this is impossible, especially when the blockage is in the apical third or located in a curved canal. Periapical surgery is the only effective method to resolve the periapical pathosis and retain the tooth.
One technique which is particularly difficult to revise nonsurgically is the sectional silver cone that was placed to allow space for an intraradicular post. Fortunately, the use of silver cones is obsolete, but a legacy of cases remain. In the event the silver cone section is not removable nonsurgically, apical surgery is indicated. Fortunately in many cases, it is possible to remove the entire piece of silver cone from the apical direction because many will be found to be loose in
(Fig. 16-18). Apical surgery is indicated for any of these teeth with apical lesions or persistent symptoms, since root canal procedures terminating far short of the apical foramen are not likely to have any effect. The difficulty of penetrating calcified canals can lead to aberrant canal preparations that are often observed in cases with persistent periapical pathosis. It is rarely possible to successfully renegotiate the uncleaned canal spaces in these cases (Fig. 16-19).
It is almost always appropriate to make a traditional access to the canal space and attempt to locate the canal. Ultimately, if the canal cannot be negotiated, the attempt should be terminated before excessive destruction of coronal tooth structure or a perforation occurs. Subsequently the tooth should be restored and periapical surgery treatment planned (Fig. 16-20).
Iatrogenic ObstructionsThe term iatrogenic refers to adverse complications caused by previous treatment. In the case of obstructions, it would be the presence of irretrievable dental materials or instruments
FIGURe 16-18 Calcification made negotiation to the apex impossible in any canal in this maxillary first molar. Surgery is indicated if symptoms persist or an apical lesion develops in the future.
FIGURe 16-19 Mandibular molar with persistent periapical pathosis. The attempt to negotiate the mesial canals was unsuccessful. Periapical surgery was indicated.
FIGURe 16-20 a, Severely calcified maxillary left central incisor with periapical pathosis. B, After a nonsurgical attempt to locate the canal, the access was permanently restored and surgery was completed.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 335
BA
FIGURe 16-21 a, Root canal completed with a sectional silver cone. A symptomatic lesion is present. B, After an unsuccessful attempt at removal, surgery was completed.
the canal following resection. If the silver cone can be removed, apical preparation can proceed in the usual manner without complication.
If the silver cone cannot be removed, the apical prepara-tion (described later in this chapter) becomes much more complicated. The metal will have to be cut back with a very small bur or diamond-coated ultrasonic tip to create a cavity preparation for the root-end filling material (Fig. 16-21). The same problem may be encountered with some paste filling materials that set to a hard consistency.
When separated instrument fragments cannot be removed, surgery is indicated to clean and fill the apical portion of the root canal. If the instrument fragment does not extend to the apex, it is not necessary to remove it. In fact, the attempt to remove it may excessively destroy root structure. Instrument
fragments at the apex or protruding through the apex can frequently be removed during surgery, which greatly facili-tates apical preparation and placement of a root-end filling (Fig. 16-22).
Intraradicular posts can be problematic in three ways rela-tive to periapical surgery. Like other iatrogenic obstructions, they impede the use of nonsurgical revision techniques. For-tunately, modern technology makes it possible to remove most posts, but it is not always advantageous to do so. On occasion, the remaining tooth structure may be severely weakened, which will diminish the prognosis of the restored tooth even if the revision is successful (Fig. 16-23). Often, periapical surgery is the more conservative approach.
Secondly, although removal of the post is usually the treat-ment of choice, it is seldom possible to determine the extent
A B
FIGURe 16-22 a, Root-treated mandibular first molar with periapical pathosis. Note the separated instrument extending through the apex of the distal root. B, Immediate postsurgical radiograph indicating removal of the instrument fragment before placing the root-end filling. (Courtesy Dr. Ryan Wynne.)

336 chapter 16 | Problem-Solving Challenges in Periapical Surgery
BA
FIGURe 16-23 a, Fractured post in a short root: a treatment planning dilemma. B, Post removal completed. Although necessary for restoration, removal resulted in a very large post preparation and thin dentinal walls.
BA
FIGURe 16-24 a, Mandibular canine with inadequate root canal and recurrent apical pathosis. The tooth is an abutment for a functional and esthetic fixed prosthesis. B, Although the post appears easily removable, periapical surgery was elected to avoid possible loosening of the crown.
to which a post may be essential to the retention of a restora-tion. Treatment planning for periapical surgery is sometimes based on the conservation of satisfactory functional or esthetic restorations even if the post could be removed (Fig. 16-24).
A third consideration concerns post placement within the canal. If the post preparation is overextended, or if a post is placed in a short root, the apical portion of the root fill may be compromised, resulting in the development of a periapical
lesion. During surgery, insufficient canal space may remain for ideal surgical filling of the apical portion of the canal (Fig. 16-25). Occasionally the apical portion of the canal can be prepared by cutting the post itself. This procedure is more difficult than that described for silver cones. Contemporary metal post materials such as stainless steel and titanium are extremely difficult to cut with small burs, and the burs tend to be difficult to control.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 337
A B
FIGURe 16-25 a, Very short maxillary central incisors restored with overextended intraradicular posts; periapical pathosis on both teeth. B, Postsurgical radiograph. Lack of available canal space for a root-end filling made surgery on the right central impossible.
Resin and ceramic post materials cannot be cut with burs and must be prepared with diamond-coated ultrasonic tips, a technique that is very slow if effective at all. The resulting preparations can become excessively large and shallow, and the prognosis for healing may be compromised. Successful surgical management of cases requiring preparation into post materials requires a high level of skill and experience. Never-theless, the result can be satisfactory (Fig. 16-26).
Prevention of potential surgical complications due to post placement involves excellence of both endodontic and restor-ative treatment. The restoration of root canal treated teeth with posts is discussed further in Chapter 21.
Failure of Previous Periapical SurgeryThe causes of failure of previous periapical surgery have been identified by many authors.51,52 Often indicted is failure to properly clean and shape the root canal system, which implies that either the apical portion of the root canal was not filled during surgery, not filled properly, or filled with an unaccept-able material. Second, a major factor identified for failure following surgery is advancing marginal periodontitis. One of three possibilities will support this claim: (1) periodontal disease was present at the time of periapical surgery and ignored by the clinician; (2) periodontal disease has devel-oped since the surgical procedure; or (3) the reflected tissue at the time of surgery was not repositioned and stabilized properly, which resulted in a downgrowth of epithelium and communication with the periapical surgical site. Additional causes of failure cited include coronal leakage through faulty restorations of teeth that have had surgery, anatomic
aberrations that were not addressed during surgery, iatrogenic damage to the tooth, and iatrogenic damage to the support-ing periodontium.52
Amalgam was in common use as a root-end filling material for the first 90 years of the 20th century.24 At the time, there appeared to be no viable alternatives, even though amalgam was not considered biocompatible52 and failures occurred. Eventually, studies confirmed that the long-term prognosis for amalgam retrofills was poor,14 despite the observation that many cases remained functional for decades.24 Although amalgam is considered obsolete in this application, the legacy of cases completed in this manner is significant and repre-sents possibly the most common type of surgical failure. Unfortunately its use continues today in many parts of the world.39
Nonsurgical revision alone is never an option in cases of surgical failure unless the previous surgery has completely missed the apex, which is rare (Fig. 16-27). In virtually all cases, there is the need to remove the existing root-end filling material. Secondly, previous apical surgery has irreversibly altered the apical canal shape that cannot be corrected by nonsurgical revision. Third, bacteria in the preparation sur-rounding the existing root-end filling will be impossible to eliminate. And fourth, when amalgam is present as the root-end filling, the apical preparation is usually contaminated with corrosion products. Fortunately, surgical revision of previous apical surgery is a reasonable and effective treatment if the causative factors can be eliminated (Fig. 16-28).52
There are a few differences in surgical techniques used with surgical revision as compared to cases without previous surgery. First is the necessity of removing previously placed root-end fillings. Fortunately, the techniques for apical prep-aration prior to the advent of ultrasonic instruments were not

338 chapter 16 | Problem-Solving Challenges in Periapical Surgery
bur can penetrate. Often the only solution is to create more extensive apical bevel than would typically be desired. Another solution is to use ultrasonic diamond-coated tips, but they may not possess the necessary length to remove the entire filling, and their aggressive ability to cut dentin relative to the amalgam can create excessive enlargement. The operator must avoid high power levels with the use of ultrasonic tips, especially in a narrow, fragile root tip. Cracks in the root can result.46,55
able to penetrate very far into the canal. At surgery, prepara-tion of a new apical bevel will sometimes eliminate most or all of the old retrofilling and sometimes the preparation as well if it is shallow.
If the root-end filling extends well into the canal space, removal can be a challenge if the material is hard, like amalgam. Amalgam can only be removed with a high-speed bur. Similar to the problems with silver cones described earlier, access and angulation limit the depth to which the
B CA
D E F
G H
FIGURe 16-26 a, Maxillary premolar with a post and broken instrument in the apical few millimeters. A draining sinus tract is traced to the pontic area of the fixed prosthesis. Surgery is necessary. B, The bony window has been cut, and just the tip of the broken instrument is becoming visible (arrow). C, An apical preparation has been initially cut, and both the broken instrument and post are visible. D, An ultrasonic instrument was used to remove the broken segment. e, A bur is used to cut into the root and the end of the post. F, Apical cavity is prepared. G, Intermediate restorative material (IRM) is placed. H, Radiograph showing the final root-end fill. (Case courtesy Dr. Fasial Amir.)

chapter 16 | Problem-Solving Challenges in Periapical Surgery 339
It is beyond the scope of this text to present all the varia-tions of surgical anatomy, issues of access to apices, and the techniques to accomplish root-end filling of canals in the posterior teeth. Subsequent discussions will focus on problem-solving techniques designed to prevent problems when performing periapical surgery on the anterior teeth, which for the novice are the best experiences for developing skills and experience.
Prior to considering a clinical application, the techniques for root-end cavity preparation and root-end filling of an anterior tooth will be illustrated in vitro. Preparation of the root apex consists of two operations, the first being root-end resection with an apical bevel that is made primarily to visual-ize the terminus of the root canal. Historically, the bevel was usually made at an angle of 45 to 60 degrees from the long
Surgical Access and Manipulative Techniques: In Vitro Directives
From the examples presented in the previous section, it can be seen that endodontic surgery is applicable to almost all roots of all teeth. It is also true that the objective of periapi-cal surgery is invariably the same for all applications: the cleaning and proper filling of the apical portion of the root canal at the level of the resected root face. From a practical standpoint, however, the more posterior the tooth, the more difficult the actual procedures become, owing to complexity of tooth anatomy and the anatomy of the alveolar arches.
BA
FIGURe 16-27 a, Case of apparent surgical failure on a maxillary central incisor. B, Canal negotiated. Note that the amalgam root-end filling is not in contact with the canal or the apical radiolucency.
BA
FIGURe 16-28 a, Maxillary second premolar presenting with tenderness to percussion and palpation. Surgical treatment completed with an amalgam root-end fill approximately 10 years previously. B, Six-month reevaluation radiograph indicating excellent postsurgical healing. The patient was asymptomatic, and the tooth was functional. The apex is filled with MTA.

340 chapter 16 | Problem-Solving Challenges in Periapical Surgery
B
C
A
FIGURe 16-30 Manufactured surgical ultrasonic tip with 3 mm effective cutting depth.
FIGURe 16-29 a, Apical bevel made with a surgical-length fissure bur. B, Diamond bur (right) for making the apical bevel, and ultrafine diamond bur (left) to refine the bevel. C, Completed apical bevel. Note the canal is in the center of the cut surface.
axis of the canal (Fig. 16-29).24 This angle may open many bacteria-laden dentinal tubules in cases of persistent periapi-cal pathosis.34 When the root is resected at any bevel, the canal orifice should be near the center of the beveled surface. With modern ultrasonic preparation techniques and the impact of magnification, the bevel can be made at right angles to the canal if visualization and access permit.55
The second step is enlargement and cleaning of the apical portion of the root canal to permit placement of a root-end filling.55 Studies have focused on the direction and permeability of the dentinal tubules.59,67 The diameter of the tubules is sufficient to permit leakage of fluid and could permit ingress of bacteria into the root canal. In the midroot region, the dentinal tubules are roughly perpendicular to the root surface and pulp chamber. In the apical region, however, the dentinal tubules angle coronally from the root surface to the pulp chamber. With an apical bevel of 0 degrees (per-pendicular to the long axis of the tooth), the angulation of the dentinal tubules would require canal preparation to a
depth of 1 mm to adequately seal the dentinal tubules.18 If the bevel was cut at an angle of 45 degrees, the depth of preparation would need to be increased to 2.5 mm. For this reason, many if not most ultrasonic tips manufactured for apical surgery are designed with an effective cutting length of 3 mm (Fig. 16-30).

chapter 16 | Problem-Solving Challenges in Periapical Surgery 341
FIGURe 16-31 Ultrasonic preparation of the apical canal space with ultrasonic tip.
FIGURe 16-33 Three ultrasonic tips with different angles and tip sizes. The arrow indicates the largest tip that should not be used in narrow resected root ends.
Preparation of the apical canal space has two objectives: (1) removing necrotic debris, bacteria, and any previous filling materials and (2) enlarging the space sufficiently to permit compaction of a dental material to fill the preparation. Currently, the apical preparation is usually performed with an ultrasonic instrument. Manufactured tips are available in various angle configurations, either plain or diamond coated. They can be used to prepare an adequate apical preparation for root-end filling in most anterior teeth (Fig. 16-31). A particular advantage of manufactured diamond-coated tips is their ability to cut metal such as silver cones, posts, and previ-ous amalgam fillings. In practice, this may be a laborious and time-consuming approach, but in combination with high-speed burs, the diamond ultrasonic tip is a valuable surgical aid for removal of metallic materials.
Manufactured ultrasonic tips may also have some distinct disadvantages in certain cases. Due to their relatively large diameter and rigid construction, they do not necessarily follow the pathway of a prepared canal (Fig. 16-32). However, smaller, narrower diamond-tipped instruments are available (Fig. 16-33). This issue also involves visibility, surgical access, and clinician experience in the application of these tips. Diamond ultrasonic tips can be quite aggressive at higher energy levels, may cut in any direction (Fig. 16-34), and may create fractures on the resected root face.7,57 Caution must be exercised in maintaining a diamond tip in the long axis of the canal; short bursts of activation in applying the tip are suggested.
Another potential disadvantage is limitation to a 3-mm preparation depth (Fig. 16-35). Often it is desirable to clean the canal to a greater depth, especially if there is unclean space (Fig. 16-36). This situation may very well occur in the mesial buccal root of maxillary first molars.9 Fortunately, an alterna-tive approach to apical canal preparation is possible with an ultrasonically energized K-file. The file will follow the pathway of the canal, and small, previously uncleaned canals can be negotiated (Fig. 16-37). Gutta-percha/sealer and paste filling materials are removed easily (Fig. 16-38), while the
FIGURe 16-32 a, Preoperative surgery case without previous preparation of the canals at the apices. B, Postoperative radiograph indicating aberrant preparation of the apical foramina with ultrasonic diamond-tipped instrument.
depth of preparation can be much greater than 3 mm, limited only by the space available in the lesion to place the instru-ment in the canal (Fig. 16-39).
The chief disadvantages of the ultrasonic file technique are the need to curve the file by hand and the potential for

342 chapter 16 | Problem-Solving Challenges in Periapical Surgery
A B
FIGURe 16-36 a, Large post core restorations in two maxillary central incisors without previous root canal. Surgery is indicated. Ideally, penetration of the apical canal space should be to the level of the posts. B, Postoperative image of surgery on an open-apex lateral incisor. Note penetration and placement of filling material adjacent to the post.
BA
FIGURe 16-35 a, Preoperative radiograph of a previously treated lateral incisor. The tooth has a deeply seated intraradicular post, and patient is symptomatic. B, Postoperative image of the apical surgery completed with a manufactured ultrasonic tip. Depth of penetration is limited to 3 mm or less. It would have been desirable to remove all of the gutta-percha to the level of the post.
BA
FIGURe 16-34 a, Demonstration of the cutting efficiency of an ultrasonic diamond-coated tip. There is no defect or canal on the lateral surface of the extracted tooth. B, Hole prepared in the root surface in less than 1 minute. At the apex, there is a risk of overpreparation and failure to remain centered in the canal.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 343
C
D
BA
FIGURe 16-37 a, Demonstration of apical preparation of a previously unprepared canal using an ultrasonically energized endodontic file. B, The No. 15 K-file penetrates and follows the canal. C, Preoperative image of a maxillary central incisor with periapical pathosis. The canal appears to be completely calcified. D, Postoperative image shows completed root-end fill. Preparation was completed with an endodontic file in the ultrasonic device.
BA
FIGURe 16-38 a, Demonstration of apical preparation in a canal filled with gutta-percha. B, Larger-sized endodontic file used in the ultrasonic unit on a high setting only long enough to remove the gutta-percha. The power is reduced to complete the preparation.

344 chapter 16 | Problem-Solving Challenges in Periapical Surgery
A B
FIGURe 16-39 a, Maxillary central incisor indicated for apical surgery. B, Postoperative image indicating removal of the gutta-percha and filling the canal to the level of the intraradicular post.
FIGURe 16-42 Completed apical preparation.
FIGURe 16-41 Ultrasonic unit set at a low power potential for apical instrumentation.
FIGURe 16-40 Precurving the file using a surgical needle holder; avoid sharp angle bends that will cause rapid instrument breakage when used ultrasonically.
instrument breakage during use. The curve can be made with a surgical needle holder or hemostat (Fig. 16-40). To mini-mize instrument breakage, care should be taken to avoid a sharp angle bend, and the ultrasonic device should be kept on a lower setting, which will vary depending on the unit (Fig. 16-41).
The completed preparation should be sufficiently large to permit compaction of the root-end filling material (Fig. 16-42). Contemporarily, the most commonly used root-end material may be mineral trioxide aggregate (MTA), but inter-mediate restorative material (IRM) is also favored by many clinicians. In randomized, prospective clinical studies, both

chapter 16 | Problem-Solving Challenges in Periapical Surgery 345
more recent approach is the formation of small columns of MTA in a block which are carried to the preparation on a half Hollenbeck carver (Lee MTA Forming Block [G. Hartzell & Son, Concord, CA, USA])33 (Fig. 16-44). The material is then compacted with small pluggers available commercially or can be handmade from dental instruments such as endodontic or operative dentistry explorers (Fig. 16-45). Following compaction, the excess is removed with slightly moistened cotton pellets (Fig. 16-46).
BA
FIGURe 16-43 a, Syringe-type carrier for the placement of mineral trioxide aggregate (MTA) at the apex (MAP system). B, Amalgam miniature carrier used for placement of MTA.
FIGURe 16-44 Lee MTA Block for the formation of small columns of mineral trioxide aggregate. The material is carried to the apical preparation with a half Hollenbeck carver.
FIGURe 16-45 Compaction of filling material with miniature pluggers. Pluggers are available commercially or custom made from endodontic explorers, periodontal probes, or other restorative hand instruments that can be fashioned into a plugger-shaped instrument.
materials have shown equivalent healing responses over time as evaluated radiographically.6,35
Both materials can be carried to the apical preparation in a number of ways. There are commercially available minia-ture carriers of various designs originally designed for amalgam (retrofill amalgam carrier [Miltex, York, PA, USA]) or newly developed systems (MAP system [Roydent Dental Products, Johnson City, TN, USA]; Dovgan MTA carriers [Quality Aspirators, Duncanville, TX, USA]) (Fig. 16-43). A

346 chapter 16 | Problem-Solving Challenges in Periapical Surgery
BA
FIGURe 16-46 a, Excess filling material is removed with a cotton ball. B, Completed root-end filling.
For larger lesions in the maxilla, palatal anesthesia should always be administered. It is also occasionally necessary to supplement the local anesthesia with direct infiltration of the tissue lining the apical lesion.
Soft-Tissue Considerations: Flap DesignThere are four tissue-flap designs suitable for anterior apical surgery. The most convenient to elevate and close is the tri-angular flap, which consists of one vertical incision and an intrasulcular incision24,65 (Fig. 16-47). The vertical incision is usually placed at least one tooth width mesial to the tooth being operated and should include the papilla. The sulcular, or horizontal, incision usually extends at least one tooth width distal to the operated tooth. This design will provide adequate exposure of the apical area in almost all cases. If insufficient exposure is obtained with one vertical incision, a second vertical incision can be made at the distal end of the flap, creating a rectangular flap24,65 (Fig. 16-48). Again, the papilla should be included, and the incisions should be angled to make the base of the flap wider than the margin. This is to ensure a generous vascular supply to the flap.
A third type of tissue flap design is the submarginal flap.24,65 This design is appropriate for preserving the gingival margin level around esthetic restorations when there is a suf-ficient width of attached gingiva that covers the entire planned surgical site. The flap consists of two vertical inci-sions which do not extend to the gingival sulcus, but rather are connected by a horizontal incision placed approximately 2 mm coronal to the mucogingival line (Fig. 16-49). The result is a horizontal flap margin of keratinized tissue that is more substantial than mucosal tissue for suturing.
The final type is the papilla-base flap.64 This tissue flap has been suggested to prevent recession of the papilla. It
Surgical Access and Manipulative Techniques: In Vivo Directives
Surgical AnatomyIn both the maxillary and the mandibular arches, there are no anatomic complications to routine surgery on any of the six anterior teeth. There are no major blood vessels, nerve canals, sinus cavities, or excessively thick bone structures, with the possible exception of the anterior nasal spine. In some cases, surgical access to the apex may be restricted by a very shallow vestibule or unusually long roots, in particular with both mandibular and maxillary canines. Excessive ante-rior protrusion of the tooth will angle the apex deeper into the alveolus, making the canal less accessible as well.
Anesthesia and HemostasisPeriapical surgery is well suited to routine local anesthesia techniques, and the same anesthetic solutions can be used as for operative dentistry.26 Once anesthesia is established, hemostasis in the soft tissues can be enhanced by infiltration with anesthetic solutions containing vasoconstrictors in con-centrations of 1:50,000.23 In some areas of the world, only concentrations of 1:80,000 are available. These solutions are not recommended for mandibular blocks.
Articaine (Septocaine [Septodont USA, New Castle DE, USA]) may be advantageous because of an increased ability to penetrate bone. In the mandibular anterior area, it is often possible to complete apical surgery with infiltration alone. Because of the long duration of effect, bupivacaine (Marcaine [Hospira Inc., Lake Forest, IL, USA]) is effective not only for the operation itself but also for pain control in the post-operative period.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 347
FIGURe 16-48 Rectangular flap. A second vertical incision is helpful to enhance tissue reflection and apical exposure. It is very important to design flap with base wider than the free margin.
A B
C D
FIGURe 16-47 a, Location of vertical incision for triangular flap. The vertical incision is placed at least one tooth width distal to the operated tooth. B, Incision made firmly to bone, reducing the possibility of tearing elevation. C, Incision terminates as shown, leaving the papilla. The same incision can also terminate so as to include the papilla, as suturing is somewhat easier if the papilla is included. D, Completion of flap with intrasulcular incision, again to crestal bone.
the gingival margin. In the second step, the scalpel retraces the base of the previously created incision while inclined vertically towards the crestal bone margin. The second inci-sion results in a split-thickness flap in the apical third of the base of the papilla. From this point on, moving apically, a full-thickness mucoperiosteal flap is elevated. While the papilla-base flap can result in predictable healing results, this technique is challenging to perform and is not recommended for the neophyte. However, knowledge of this approach is especially helpful in treatment planning surgery in the pres-ence of soft-tissue or esthetic concerns in the anterior portion
consists of two releasing vertical incisions connected by the papilla-base incision and intrasulcular incision in the cervical area of the tooth. A microsurgical blade should be used that does not exceed 2.5 mm in width, because intricate, minute movement of the surgical blade within the small dimensions of the interproximal space is crucial.
Two different incisions are made at the base of the papilla. A first shallow incision severs the epithelium and connective tissue to the depth of 1.5 mm from the surface of the gingiva. The path is a curved line connecting one side of the papilla to the other. The incision begins and ends perpendicular to
FIGURe 16-49 Submarginal flap preserving the position of the free gingival margin.

348 chapter 16 | Problem-Solving Challenges in Periapical Surgery
FIGURe 16-51 No perforation of labial plate. The bone must be dissected with a No. 4 (1.4 mm) or No. 6 (1.8 mm) surgical-length round bur. Dissect using a shaving motion and copious water irrigation.
FIGURe 16-50 Elevation of tissue with a sharp periosteal elevator.
of the mouth. When considered, cases can then be referred to someone more experienced in using this surgical approach.
Atraumatic handling of the soft tissues with the papilla-base flap is of utmost importance in order to obtain rapid healing through primary intention. The epithelium of the partial thickness flap has to be supported by underlying con-nective tissue; otherwise, it will necrose and lead to scar formation. On the other hand, excessive thickness of the connective-tissue layer of the split flap portion could com-promise the survival of the buccal papilla left in place.
Incisions are always made firmly to bone so the perios-teum can be elevated with the flap and to prevent the tearing of the tissue. Sharp periosteal elevators will ensure a uniform exposure of the alveolar bone (Fig. 16-50). The vertical and horizontal incisions can always be extended if the tissue cannot be elevated or is not relaxed over the intended apical portion of the surgical site.
Curettage and Enucleation of the Soft-Tissue Lesion When the Lesion Penetrates the BoneFrequently the apical lesion will have perforated the labial plate of bone.28 The lesion will be plainly visible after the tissue is retracted. If there is a draining sinus tract, a portion of the lesion will be attached to the inferior surface of the tissue flap and will require extra care in tissue elevation and retraction. In these cases, it is wise to identify the circumfer-ential margin of the lesion on bone before attempting to separate all of the attachment between the lesion and the flap. Once the margins have been located, the soft tissues may be cut carefully with a scalpel. This approach will avoid cutting the tissue so as to perforate it or make it excessively thin. The tissue within the apical lesion may then be curetted to expose the apex of the tooth.
Root Apex Exposure in the Absence of a Periapical LesionIf there is no visual sign of the soft-tissue lesion after retrac-tion of the flap, which routinely occurs in cases of small apical
lesions, the buccal plate must be penetrated to gain access to the lesion. Initially, the bone should be probed, looking for a possible defect or an area in which the bone has been thinned out over the root. Subsequently, the bone is removed using a surgical-length round bur with a shaving action under copious irrigation28 (Fig. 16-51). Periodically explore the bone with a periodontal curette or an explorer as the opening in the buccal plate is being made. The walls of the lesion and the tooth itself can be palpated, and the opening can be reoriented so it is centered over the apex. Ideally, for purposes of healing, keeping the opening of the bony window to a minimum in a mesial-distal dimension is recommended.69 If the patient has any painful sensation when this exploration is performed, anesthetics should be injected into the tissue of the lesion at this time. The tissue within the apical lesion may then be curetted free from the bone, exposing the root apex (Fig. 16-52).
CLINICAL PROBLEMProblem: A 49-year-old patient presented with acute sensi-tivity over the apex of the maxillary right central incisor. The periapical film indicated that previous root canal treatment was performed with an apparently overextended intraradicu-lar post, leaving barely 1 mm of gutta-percha root filling mate-rial (Fig. 16-53, A). Only a small radiolucency was present on the x-ray, but palpation over the apex indicated a distinct localized swelling. How could an acute lesion develop with minimal radiographic evidence of pathosis?
Solution: Periapical surgery was indicated. After elevation of a submarginal flap, it was apparent that the apex was ana-tomically superficial relative to the labial plate. In this case, the infection and associated swelling that extended easily into the overlying soft tissues did not cause sufficient bone loss to create a radiographic lesion (see Fig. 16-53, B).

chapter 16 | Problem-Solving Challenges in Periapical Surgery 349
FIGURe 16-52 Apex exposure after bone removal with the round bur and curettage of the tissue within the lesion. Note the interruption of the crestal bone from the sulcular drainage tract. It is important to inspect the area for a vertical root fracture. In this case, no fracture is present. To ensure postoperative reattachment, it is vitally important to avoid curettage of the root surface in this area.
A B
FIGURe 16-53 a, Radiograph of the maxillary right central incisor with minimal evidence of periapical pathosis. Clinically, there was an acute local swelling. B, Elevation of the tissue indicates that the apex is located superficially relative to the labial plate of bone. The infection involved the overlying periosteum and mucosal tissues.
Root-End Resection and Identifying the Root Canal SpaceOnce the apex is exposed, the apical bevel is prepared so that the canal is plainly visible, centered in the beveled surface as was described previously (Fig. 16-54, A). Because 98% of apical canal anomalies and 93% of lateral canals exist in the apical 3 mm, it is important to resect at least 3 mm of the root end.24,28,55 An ideal bevel would be close to perpendicular to the long axis of the root, but often various angles of
resection must be used for both visual and surgical access without sacrificing tooth structure. If the bevel is too great, there is a spatial disorientation that is difficult to overcome, and the root-end preparation and filling may fall short of ideal. When considering the angle of the bevel, each and every case will be different. For anterior teeth, the smallest bevel possible should be considered. For posterior teeth, the considerations change significantly because of the root anatomy. Once the root end has been resected, it should be carefully examined for cracks or fractures as well as extensions and irregularities such as isthmuses, anastomoses, and the like.25,29,55 These anatomic variations will then dictate the procedures to follow, such as a further extension of the resec-tion or extention of the root-end cavity.
Root-End Cavity PreparationThe apical portion of the root canal is prepared with the ultrasonic instrument as described in vitro (see Fig. 16-54, B). Miniature surgical mirrors can enhance visualization of the canal preparation and insure the cleaning of all areas of the preparation wall55 (see Fig. 16-54, C ). In preparation for the placement of the root-end filling, dry cotton balls may be placed into the bony cavity surrounding the apex to prevent scatter of any excess filling material (see Fig. 16-54, D and E ). If there is bleeding emanating from within the bony walls following curettement, cotton pellets impreg-nated with racemic epinephrine can be substituted (Racellet [Pascal Co., Bellevue, WA]); or cotton pellets with Vicostat (Ultradent Inc., South Jordan, Utah, USA)26 (see Fig. 16-54, F ). Other hemostatic products based primarily on collagen72 have also been recommended (e.g., Colla-Cote [Integra LifeSciences Corp., Plainsboro, NJ, USA]). These can even have drops of 2.25% racemic epinephrine (Nephron Phar-maceutical Corp., Orlando, FL, USA) added to enhance hemostasis.70

350 chapter 16 | Problem-Solving Challenges in Periapical Surgery
D EF
B CA
FIGURe 16-54 a, Surgical exposure of the apex in a routine periapical surgery. Note the black stain around the gutta-percha, indicating leakage. B, Ultrasonic preparation. C, Miniature mirrors for surgery. D, Placement of cotton around the prepared apex. e, Apex ready for placement of a root-end filling. F, Epinephrine-impregnated (1 : 1000) cotton pellets can be placed if bleeding continues in the bony crypt around the root end.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 351
A B
C
FIGURe 16-55 a, Exposure of a root apex that exhibits a small vertical fracture line extending coronally on the labial. B, Preparation of the apical canal space and the crack line. The apex canal was prepared in the usual manner with an endodontic file. The crack line was enlarged with a half-round (0.5 mm) bur. C, Mineral trioxide aggregate filling the apex and fracture line.
In a rare occurrence, a vertical root fracture may be dis-covered in the apical portion of the root, moving in a coronal direction. If the fracture line does not extend through the attachment, it can be prepared with a half-round (0.5 mm) bur and filled with MTA as a part of the root-end filling (Fig. 16-55).
CLINICAL PROBLEMProblem: A 37-year-old male presented with a moderate, localized swelling over the root apex of the maxillary left central incisor. The tissues were tender to palpation, and the tooth was tender to percussion. The tooth had a post core and crown and very poor root canal filling that appeared to be of a paste nature. There was a large apical radiolu-cency (Fig. 16-56, A). Based on the data available and the clinical circumstances, periapical surgery was treatment planned.
Solution: Once the tissue was reflected and the soft tissue curetted, a small portion of the root was resected at almost 90 degrees to the long axis of the root. This was followed by cleaning the canal down to the extent of the post with a K-file attached to the ultrasonic handpiece (see Fig. 16-56, B). Subsequently the canal was filled with MTA (see Fig. 16-56, C).
Root-End Fillings: Materials and PlacementMTA is the current material of choice for the root-end filling, although IRM has also shown favorable results. In its present formulation, MTA is a difficult material to manage, but for apical applications, it is often effective to leave the canal wet and place the material in a relatively dry mix. As the material becomes hydrated during compaction, excess moisture can be absorbed with additional dry cotton pellets. After the material completely fills the cavity preparation, the apical bevel is wiped with a dry or lightly moistened cotton pellet to remove any excess (Fig. 16-57). This procedure is quite easy with IRM.
If MTA is mixed wet on a slab, avoid compaction and tease or lightly pat the material into the cavity prepa-ration. This is followed by placing the compactor in contact with the MTA in the preparation and gently touching the nonworking end of the instrument with an activated ultrasonic tip. The material will flow into the preparation as the trapped air is released. This is referred to as ultra-sonic densification.31,55
The cotton pellets surrounding the apex should then be removed along with any excess material. A careful accounting of the pellets should be done. Leaving a cotton pellet in the lesion will result in an acute foreign body reaction.

352 chapter 16 | Problem-Solving Challenges in Periapical Surgery
FIGURe 16-57 Apex of a routine surgical case filled with gray mineral trioxide aggregate.
Tissue Repositioning and StabilizationPrior to wound closure, the surgical site should be irrigated with saline solution to remove debris, and the tissue edges are approximated in their correct position to promote healing by primary intention.45 Compressing the repositioned tissue with a saline-moistened piece of gauze will reduce the coagu-lum to a thin fibrin layer between the repositioned tissue and cortical bone (Fig. 16-58).22,24 This will enhance tissue
B CA
FIGURe 16-56 a, Maxillary central incisor with a radiolucency around the root apex. An intraradicular post is present, root canal treatment is incomplete, and patient is symptomatic. Treatment done in Cambodia 20 years previously. B, After tissue reflection, apical curettage, and root-end resection, the root canal is cleaned and prepared to the level of the post. When soft tissue was removed, there were clumps of yellowish material mixed in with the granulomatous tissue. C, Canal filled with mineral trioxide aggregate. Biopsy of lesion identified as granuloma with islands of actinomycoses dispersed throughout.
C
B
T
FIGURe 16-58 a, Compression of the repositioned tissue with a moist gauze for 3 to 5 minutes before suturing. B, Note the minimized coagulum (C) adjacent to the bone (B) following good tissue compression; repositioned tissue (T). This minimizes swelling while enhancing early tissue healing.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 353
stabilization and reduce bleeding and swelling. The tissue is now stabilized with monofilament sutures, which are the best to eliminate wicking of bacteria and their byproducts into the wound site. Smaller-gauge sutures, 4-0 and 5-0, are indi-cated because sutures are tissue irritants, and the smallest possible size for adequate wound support is preferred.66 In papilla-base incisions, sutures as small as 6-0 and 7-0 are indicated. Likewise, nonresorbable sutures are recommended, since the tissue irritation terminates as soon as the sutures are removed. Suture removal can take place as early as 48 hours but not later than 4 to 5 days.27 For a triangular flap design, a sling-type suture will secure the papillae, and a single simple suture will often close the vertical incision. For a submarginal type of flap, a continuous mattress suture is efficient, but interrupted simple sutures will function just as well. If the suture material is resorbable, a return visit for suture removal can be eliminated.
Postsurgical Care and Potential Complications
Postoperatively, swelling can be reduced by immediate appli-cation of an ice pack, which should be used for the rest of the day of operation. The typical pattern of ice application is 20 minutes in place alternating with a 20-minute interval of rest. This is followed by the use of moist heat the day fol-lowing the surgical procedure.22
It is wise to have the patient take an analgesic prior to the surgical procedure or at least while the area is still anes-thetized. A highly effective analgesic without the effects of a narcotic is 600 mg ibuprofen plus 1000 mg of acetamino-phen.40 These over-the-counter medications are not only readily available but are frequently already possessed by the patient. If not taken prior to surgery, an effective regimen is to recommend the ibuprofen-acetaminophen combination as the first postoperative analgesic. This combination can be taken every 4 to 5 hours as needed. For the potential of more intense pain, a traditional narcotic analgesic can be prescribed (e.g., 5 to 10 mg hydrocodone in combination with 500 mg acetaminophen). If the patient starts with over-the-counter analgesics, a prescription for hydrocodone can also be given. Once the anesthesia wears off, the narcotic prescription can be filled for further pain relief if ibuprofen/acetaminophen is insufficient. More often than not, if the patient requires the narcotic medication, one dose is usually sufficient.
Postsurgical use of a chlorhexidine rinse (0.12%) for 1 to 2 days is recommended to control bacterial populations and inhibit plaque formation.20,50 Many clinicians will also rec-ommend these rinses at least 1 day presurgery. The use of antibiotics presurgically has been questioned, and contro-versy may exist78; however, rarely will this be indicated for localized issues (as opposed to systemic indications), because no value has been shown in the reduction of postoperative infections, which are minimal.36
ComplicationsFortunately there are few complications to apical surgery. The most common is postoperative infection under the tissue flap. Infection is characterized by local swelling and increas-ing pain, typically developing 2 to 3 days after the procedure. A prescription for amoxicillin 500 mg to be taken 4 times daily will usually resolve the infection. There is no alteration of outcome or prognosis with this approach.
Occasionally the margin of the flap may necrose and slough. No treatment is required. The outcome of eventual healing may be root or crown margin exposure, for which there are few simple options as remedies. The most effective would be orthodontic extrusion and replacement of the crown.
REFERENCES1. Abramovitz I, Better H, Shacham A, et al: Case selection for apical
surgery: a retrospective evaluation of associated factors and ratio-nal, J Endod 28:527-530, 2002.
2. Blayney JR: Fundamentals governing pulp-canal therapy, Dent Cosmos 74:635-653, 1932.
3. Caliskan MK: Nonsurgical retreatment of teeth with periapical lesions previously managed by either endodontic or surgical inter-vention, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100:242-248, 2005.
4. Chavez de Paz LE: Redefining the persistent infection in root canals: possible role of biofilm communities, J Endod 33:652-662, 2007.
5. Cheung GS: Endodontic failure—changing the approach, Int Dent J 46(3):131-148, 1996.
6. Chong BS, Pitt Ford TR, Hudson MB: A prospective clinical study of mineral trioxide aggregate and IRM when used as root-end filling materials in endodontic surgery, Int Endod J 36:520-526, 2003.
7. De Bruyne MA, De Moor RJ: SEM analysis of the integrity of resected root apices of cadaver and extracted teeth after ultrasonic root-end preparation at different intensities, Int Endod J 38:310-319, 2005.
8. de Chevigny C, Dao TT, Basrani BR, et al: Treatment outcome in endodontics: the Toronto study—phases 3 and 4: orthograde retreatment, J Endod 34:131-137, 2008.
9. Degerness R, Bowles W: Anatomic determination of the mesiobuc-cal root resection level in maxillary molars, J Endod 34:1182-1186, 2008.
10. Del Fabbro M, Taschieri S: A systematic review on the outcomes of surgical vs non-surgical procedures for the retreatment of peri-apical lesions, Minerva Stomatol 56:621-632, 2007.
11. Del Fabbro M, Taschieri S, Testori Tm, et al: Surgical versus nonsurgical endodontic re-treatment for periradicular lesions, Cochrane Database Syst Rev 18(3):CD005511, 2007.
12. Fawn CF: Root amputation, Br Dent J 48:1029-1032, 1927.13. Forbes G: Apical microsurgery for failed endodontics, Atlas Oral
Maxillofac Surg Clin North Am 8:1-25, 2000.14. Frank AL, Glick DH, Patterson SS, et al: Long-term evaluation of
surgically placed amalgam fillings, J Endod 18:391-398, 1992.15. Fukushima H, Yaamamoto K, Kirohata K, et al: Localization and
identification of root canal bacteria in clinically asymptomatic periapical pathosis, J Endod 16:534-538, 1990.

354 chapter 16 | Problem-Solving Challenges in Periapical Surgery
16. Furusawa M, Asai Y: SEM observations of resected root canal end following apicoectomy, Bull Tokyo Dent Coll 43:7-12, 2002.
17. Gagliani MM, Gorni FG, Strohmenger L: Periapical resurgery versus periapical surgery: a 5-year longitudinal comparison, Int Endod J 38:320-327, 2005.
18. Gilheany PA, Figdor D, Tyas MJ: Apical dentin permeability and microleakage associated with root end resection and retrograde filling, J Endod 20:22–26, 1994.
19. Gorni FG, Gagliani MM: The outcome of endodontic retreat-ment: a 2-yr follow-up, J Endod 30:1-4, 2004.
20. Greenstein G, Berman C, Jaffin R: Chlorhexidine: an adjunct to periodontal therapy, J Periodontol 57:370-376, 1986.
21. Gutmann JL (ed): Endodontic apical surgery: a delineation of contemporary concepts, Endod Topics 11:1-262, 2005.
22. Gutmann JL: Surgical endodontics: post-surgical care, Endod Topics 11:196-205, 2005.
23. Gutmann JL: Parameters of achieving quality anesthesia and hemostasis in surgical endodontics, Anesth Pain Control Dent 2:223-226, 1993.
24. Gutmann JL, Harrison JW: Surgical endodontics. Boston, 1991, Blackwell Publishing Co.
25. Gutmann JL, Pitt Ford TR: Management of the resected root end: a clinical review, Int Endod J 26:273-283, 1993.
26. Hargreaves KM, Kahn A: Surgical preparation: anesthesia & hemostasis, Endod Topics 11:32-55, 2005.
27. Harrison JW, Jurosky KA: Wound healing in the tissues of the periodontium following periradicular surgery, J Endod 17:425-435, 1991.
28. Hoskinson AE: Hard tissue management: osseous access, curettage, biopsy and root isolation, Endod Topics 11:98-113, 2005.
29. Hsu YY, Kim S: The resected root surface. The issue of canal isthmuses, Dent Clin North Am 41:529-540, 1997.
30. Ida RD, Gutmann JL: Importance of anatomic variables in end-odontic treatment outcomes: case report, Endod Dent Traumatol 11(4):199-203, 1995.
31. Jou Y, Pertl C: Is there a best retrograde filling material? Dent Clin North Am 41:555-561, 1997.
32. Kvist T: Endodontic retreatment. Aspects of decision making and clinical outcome, Swed Dent J Suppl 144:1-57, 2001.
33. Lee ES: A new mineral trioxide aggregate root-end filling tech-nique, J Endod 26:764-765, 2000.
34. Lin S, Platner O, Metzger Z, et al: Residual bacteria in root apices removed by a diagonal root-end resection: a histopathological evaluation, Int Endod J 41:469-475, 2008.
35. Lindeboom JA, Frenken JW, Kroon FH, et al: A comparative prospective randomized clinical study of MTA and IRM as root-end filling materials in single-rooted teeth in endodontic surgery, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100:495-500, 2005.
36. Lindeboom JA, Frenken JW, Valkenburg P, et al: The role of pre-operative prophylactic antibiotic administration in periapical end-odontic surgery: a randomized, prospective double-blind placebo-controlled study, Int Endod J 38:877-881, 2005.
37. Love RM, Firth N: Histopathological profile of surgically removed persistent periapical radiolucent lesions of endodontic origin, Int Endod J 42:198-202, 2009.
38. Maddalone M, Gagliani M: Periapical endodontic surgery: a 3-year follow-up study, Int Endod J 36:193-198, 2003.
39. Martí Bowen E, Peñarrocha Diago M, García Mira B: Periapical surgery using the ultrasound technique and silver amalgam retro-grade fillings. A study of 71 teeth in 100 canals, Med Oral Patol Oral Cir Bucal 10:67-73, 2005.
40. Menhinick KA, Gutmann JL, Regan JD, et al: The efficacy of pain control following nonsurgical root canal treatment using ibuprofen or a combination of ibuprofen and acetaminophen in a random-ized, double-blind, placebo-controlled study, Int Endod J 37:531-541, 2004.
41. Nair PN: On the causes of persistent apical periodontitis, Int Endod J 39:249-281, 2006.
42. Nair PNR: Pathobiology of primary apical periodontitis. In Cohen S, Hargreaves KM editors: Pathways of the pulp, ed 9, St. Louis, 2006, Mosby Elsevier.
43. Ng YL, Mann V, Gulabivala K: Outcome of secondary root canal treatment: a systematic review of the literature, Int Endod J 41: 1026-1046, 2008.
44. Paik S, Sechrist C, Torabinejad M: Levels of evidence for the outcome of endodontic treatment, J Endod 30:745-750, 2004.
45. Peters LB, Wesselink PR: Soft tissue management in endodontic surgery, Dent Clin North Am 41:513-528, 1997.
46. Rainwater A, Jeansonne BG, Sarkar N: Effects of ultrasonic root-end preparation on microcrack formation and leakage, J Endod 26:72-75, 2000.
47. Ricucci D, Martorano M, Bate AL, et al: Calculus-like deposit on the apical external root surface of teeth with post-treatment apical periodontitis: report of two cases, Int Endod J 38:262-271, 2005.
48. Ricucci D, Siqueira JF, Jr: Anatomic and microbiologic challenges to achieving success with endodontic treatment: a case report, J Endod 34:1249-1254, 2008.
49. Ricucci D, Siqueira JF, Jr, Bate AL, et al: Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients, J Endod 35:493-502, 2009.
50. Rölla G, Melsen B: On the mechanism of plaque inhibition by chlorhexidine, J Dent Res 54:57-62, 1975.
51. Rud J, Andreasen JO, Möller Jensen JE: A multivariate analysis of the influence of various factors upon healing after endodontic surgery, Int J Oral Surg 1:258-271, 1972.
52. Saunders WP: Considerations in the revision of previous surgical procedures, Endod Topics 11:206-218, 2005.
53. Simon JHS: Incidence of periapical cysts in relation to the root canal, J Endod 6:845-848, 1980.
54. Spångberg LSW, Haapasalo M: Rational and efficacy of root canal medicaments and root filling materials with emphasis on treatment outcomes, Endod Topics 2:35-58 2002.
55. Stropko JJ, Doyon GE, Gutmann JL: Root-end management: resection, cavity preparation, and material placement, Endod Topics 11:131-151, 2005.
56. Taschieri S, Del Fabbro M, Testori T, et al: Endodontic surgery using two different magnification devices: preliminary results of a randomized controlled study, J Oral Maxillofac Surg 64:235-242, 2006.
57. Taschieri S, Testori T, Francetti L, et al: Effects of ultrasonic root end preparation on resected root surfaces: SEM evaluation, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98:611-618, 2004.
58. Tesis I, Rosen E, Schwartz-Arad D, et al: Retrospective evaluation of surgical endodontic treatment: traditional versus modern tech-nique, J Endod 32:412-416, 2006.
59. Tidmarsh BG, Arrowsmith MG: Dentinal tubules at the root ends of apisected teeth: a scanning electron microscopic study, Int Endod J 22:184-189, 1989.
60. Torabinejad M, Corr R, Handysides R, et al: Outcomes of non-surgical retreatment and endodontic surgery: a systematic review, J Endod 35:930-937, 2009.

chapter 16 | Problem-Solving Challenges in Periapical Surgery 355
61. Tronstad L, Barnett F, Cervone F: Periapical bacterial plaque in teeth refractory to endodontic treatment, Endod Dent Traumatol 6:73-77, 1990.
62. Tronstad L, Barnett F, Riso K, et al: Extraradicular endodontic infections, Endod Dent Traumatol 3:86-90, 1987.
63. Tronstad L, Kreshtool D, B Arnett F: Microbiological monitoring and results of treatment of extraradicular endodontic infections, Endod Dent Traumatol 6:129-136, 1990.
64. Velvart P, Ebner-Zimmermann U, Ebner JP: Comparison of long-term papilla healing following sulcular full thickness flap and papilla base flap in endodontic surgery, Int Endod 37:687-893, 2004.
65. Velvart P, Peters CI, Peters OA: Soft tissue management: flap design, incision tissue elevation and tissue retraction, Endod Topics 11:78-97, 2005.
66. Velvart P, Peters CI, Peters OA: Soft tissue management: suturing and wound closure, Endod Topics 11:179-195, 2005.
67. Vertucci FJ, Beatty RG: Apical leakage associated with retrofilling techniques: a dye study, J Endod 12:331-336, 1986.
68. von Arx T, Cochran DL: Rationale for the application of the GTR principle using a barrier membrane in endodontic surgery: a pro-posal of classification and literature review, Int J Periodontics Restorative Dent 21:127-139, 2001.
69. von Arx T, Hänni S, Jensen SS: Correlation of bone defect dimen-sions with healing outcome one year after apical surgery, J Endod 33:1044-1048, 2007.
70. Vy CH, Baumgartner JC, Marshall JG: Cardiovascular effects and efficacy of a hemostatic agent in periradicular surgery, J Endod 30:379-383, 2004.
71. Wada M, Takase T, Nakanuma K, et al: Clinical study of refrac-tory apical periodontitis treated by apicectomy. Part 1. Root canal morphology of resected apex, Int Endod J 31:53-56, 1998.
72. Witherspoon DE, Gutmann JL: Haemostasis in periradicular surgery, Int Endo J 29:135-149, 1996.
73. Wolcott J, Rossman LE: Intentional replantation of endodontically treated teeth: an update, Compend Contin Educ Dent 24:68-72, 74, 2003.
74. Wu MK, Dummer PM, Wesselink PR: Consequences of and strat-egies to deal with residual post-treatment root canal infection, Int Endod J 39:343-356, 2006.
75. Wu K, Wesselink P: Timeliness and effectiveness in the surgical management of persistent post-treatment periapical pathosis, Endod Topics 11:25-31, 2005.
76. Yusuf H: The significance of the presence of foreign material periapically as a cause of failure of root treatment, Oral Surg 54:566-574, 1982.
77. Zesis A, Lin S, Fuss Z: Endodontic surgery (apicoectomy)— success rate of more than 90% using dental operating microscope and ultrasonic tips (In Hebrew), Refuat Hapeh Vehashinayim 22:33-41, 86, 2005.
78. Zuolo ML, Ferreira MO, Gutmann JL: Prognosis in periradicular surgery: a clinical prospective study, Int Endod J 33:91-98, 2000.
RECOMMENDED ADDITIONAL READINgKim S, Pecora G, Rubinstein RA, et al: Color atlas of microsurgery in
endodontics, Philadelphia, 2000, W.B. Saunders Co.Merino EM: Endodontic microsurgery, London, 2009, Quintessence
Publishing Co. Ltd.von Arx T, Salvi GE, Janner S, et al: Gingival recession following apical
surgery in the aesthetic zone: a clinical study with 70 cases, ENDO (Lond Engl) 4:255-268, 2009.

356
Chapter 17
Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins Including Radicular Defects
Problem-Solving ListProblem-solving issues and challenges in managing compromises in sound tooth margins and radicular defects addressed in this chapter are:Normal Periodontium in Relation to Surgical Treatment PlanningIndications for Crown Lengthening
Convenience of tooth isolationEstablishing increased clinical crown for the “ferrule effect”Preventing restorative failureAvoiding marginal problems with restorationsManaging deep fracturesLocation of obscure root canal orificesFollowing orthodontic extrusion of teeth or roots
Potential Contraindications for Crown LengtheningMedical statusEsthetic zoneMinimal vertical dimension of the root trunk
Surgical Techniques for Crown LengtheningSurgical proceduresEnvelope tissue flapThinning or undermining the tissueRecontour of alveolar boneTissue closurePeriodontal surgical dressingHealingComplications with surgical crown lengthening
Application of Crown Lengthening Techniques to Other Endodontic Problems
Iatrogenic perforations in the marginal periodontiumResorption defects in the marginal periodontiumVertical root fracture repair
Once the biologic width of the supporting periodontal attachment apparatus has been severely violated, more extensive procedures are often necessary to manage compromised root structure and supporting bone.20
J.L. Gutmann, 1991
Preserving the natural dentition in symptom-free clinical function is a major goal of dentistry and its specific disci-plines. Prosthetic dentistry has provided fixed and removable substitutes for teeth that have been lost, and the advent of implant dentistry has brought about a new concept, replace-ment of the natural dentition. While the development of implantology has been a marvelous addition to the practice of dentistry and has enhanced patient well-being,9,35,42 the enthusiasm for this option has in some cases clouded the process of sound treatment planning.8,43 However, many teeth that could be preserved in normal function through reasonable and adjunctive procedures (nonsurgical endodon-tic revision, surgical endodontic revision, crown lengthening, orthodontic root extrusion, root resection, etc.) are removed in favor of replacement with implants. Data do not support the superiority of implants over these other procedures when treatment planned and executed properly.24,25 In many respects, implant dentistry is not an option for a great many people, and tooth retention is not only possible but in the patient’s best interest and the best choice.
In this chapter, surgical procedures will be presented that can be used effectively to retain teeth with a variety of com-plications in addition to pulpal disease. The most common problems encountered are clinical crowns with subgingival

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 357
A discussion of average sulcus depth was included at the beginning of Chapter 4. The essential anatomic relationships between the tooth, bone, and soft tissues of the average healthy periodontal sulcus are depicted in Fig. 17-1. These dimensions have been described as the biologic width,* defined as the physiologic dimension of the junctional epithelium and connective tissue attachment.16,33
The width of the attached gingiva varies from 1 to 9 mm,6 with an average of 3.7 mm in the anterior areas, 3.8 mm in the premolar regions, and 4.2 mm in the molar37 (Fig. 17-2). However, at least 5 mm of attached gingiva are recom-mended for restorative dentistry.32 Ideally, areas of attached gingiva with less than 5 mm should be considered for aug-mentation procedures if restorative margins are to be placed in the sulcus.4 The healthy gingival sulcus has been shown to have an average depth of 0.69 mm.33
carious or fractured margins and insufficient tooth structure to retain a restoration. In many of these cases, crown length-ening is an ideal solution. Exposure of sound tooth structure can make restoring certain types of compromised teeth a routine procedure, enhancing not only the restoration of the tooth but the biologic widths of the supporting periodon-tium. The basic techniques of this surgical intervention can be extended to the management of other endodontic prob-lems such as resorption and perforation defects.
Normal Periodontium in Relation to Surgical Treatment Planning
Prior to considering periodontal surgical procedures, a review of the normal anatomy of these tissues is essential.
B
0.5 mmsulcus
A
1 mmepithelial attachment
1 mmfibrous attachment
FIGuRE 17-1 a, Normal periodontium. B, Histologic section through normal periodontium (H&E stain ×10).
*References 10, 27, 28, 32, 33, 36, and 37.
A B
FIGuRE 17-2 a, Attached gingiva of normal, ample width. B, Width of attached gingiva in this maxillary right premolar area is 1 mm or less.

358 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
The contours of the normal alveolar bone are also of great significance. Most often, surgical crown lengthening cannot be achieved without removing some crestal bone. Postopera-tively, the measure of success is not only increased clinical crown length but also restoration of a normal periodontium circumferentially. In recontouring bone, the clinician should reproduce or create the contours of normal periodontium. Except in the mandibular second and third molar areas, the
A B
FIGuRE 17-3 a, Labial plate of bone is normally thin. B, Cross-section of maxilla in the first molar area, showing buccal and palatal plates of bone.
BA
FIGuRE 17-4 a, Excessive width of buccal plate of bone. B, Recontoured buccal plate during periapical surgery procedure.
buccal and lingual plates are usually fairly thin throughout the dentition (Fig. 17-3). If the buccal plate appears exces-sively thick with a shelflike contour, it can be reduced (Fig. 17-4). Occasionally, a dehiscence or fenestration will be found after the flap is elevated (Fig. 17-5). The only signifi-cance of this finding is that the exposed areas of the root should be left untouched. Reattachment will invariably occur, providing that these root surfaces are not curetted.
CLINICAL PROBLEMProblem: Can the interproximal bone throughout the mouth be recontoured using a standardized technique?
Solution: No, because there is a significant difference between the interproximal contours of the bone between the posterior teeth and the contours found between the anterior teeth. The normal contour between posterior teeth is flat buccolingually (Fig. 17-6). Crown lengthening will require an apical relocation of the bone while maintaining the identical form. Frequently, bony defects from chronic periodontitis are found interproximally,
leaving intact ridges of the buccal and lingual or palatal plates. These ridges are normally reduced to restore as flat a buccal lingual contour as possible (Fig. 17-7). Conversely, in the anterior dentition, there is an interproximal crest (Fig. 17-8). In crown lengthening, the reproduction of these contours is necessary for optimal periodontal healing and also esthetics (Fig. 17-9). The interdental papillae are supported and shaped by the underlying bone. If the supporting bone is either lost by periodontal disease or failure to recreate the proper contour during surgery, the papilla will collapse (Fig. 17-10).

FIGuRE 17-6 Normal interproximal anatomy of bone is flat in posterior dentition.
FIGuRE 17-5 Dehiscence of root surfaces after flap elevation. These areas should not be curetted.
FIGuRE 17-8 Normal interproximal anatomy of bone in the anterior dentition is characterized as a crest.
A
B
FIGuRE 17-9 a, Crown lengthening on fractured maxillary central incisors. B, Restoration of interproximal bony crests which will support the papillae.
A
B
FIGuRE 17-7 a, Periodontal surgery for severe chronic periodontitis. B, Following osseous recontouring and pocket elimination. Note ramping of buccal plate into interproximal spaces. (Courtesy Dr. Curtis Wade.)
FIGuRE 17-10 Loss of the interproximal crest of bone results in collapse of the interdental papilla and an unesthetic “black triangle.”

360 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
FIGuRE 17-11 Placing dental dam clamp directly on gingival margin does not address subgingival caries or restorability following root canal treatment.
FIGuRE 17-12 Dental dam sealers are effective, but restorability of the deep fracture in this case remains a problem.
FIGuRE 17-13 Temporary restorations often leak.
FIGuRE 17-14 Complete permanent restorations are effective in achieving tooth isolation. The access cavity could weaken the structural support if this restoration were included in a crown preparation.
Indications for Crown Lengthening
There are multiple considerations in which crown lengthen-ing can and should be considered in the treatment planning for tooth retention.
Convenience of Tooth IsolationBefore arriving at crown lengthening as the treatment of choice, a discussion of common alternatives is indicated. Most teeth with significant carious lesions can be isolated without crown lengthening. One simple solution is to place the dental dam clamp directly on the gingiva and complete the root canal treatment (Fig. 17-11). The difficulty of this approach is that it merely postpones the problem of treatment planning the final restoration. A second method of isolation is caulking the gaps around the dental dam with temporary filling materials or a specialized putty (Fig. 17-12). Once again, root canal treatment can usually be completed without leakage, but the restorability issues remain. Temporary filling materials can be used to seal large excavations within the tooth as well (Fig. 17-13). Unless the caries is thoroughly removed and a high quality restoration is placed, leakage can be a problem, especially if the root canal treatment requires multiple visits. Leakage between appoint-ments is a very common cause of reinfection.
Many clinicians favor complete restoration of the end-odontically involved tooth. Access is then made through the new restoration (Fig. 17-14), which helps prevent leakage. After the root canal treatment is completed, however, the restoration often does not provide sufficient structural integ-rity to support a full crown.30,31 Crown lengthening satisfies all the endodontic and restorative needs. Isolation is excel-lent, while access and visibility are unimpeded. Issues of restorability can be determined early, and the final restora-tion can take advantage of the treated canals for retention if necessary (Fig. 17-15).
Establishing Increased Clinical Crown for the “Ferrule Effect”This key restorative goal is discussed in detail in Chapter 20. Full crown restorations require retention on sound tooth structure as well as any restorative foundation that is

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 361
A B
C
FIGuRE 17-15 a, Mandibular molar with severe caries extending subgingivally on the distal. B, Clinical view of same tooth. Restorability appears to be questionable. C, Following crown lengthening; restorability is confirmed and isolation for root canal treatment is excellent.
constructed.2,33 This also provides an additional barrier to marginal leakage that may adversely affect the prognosis of the root canal treatment (see Fig. 17-15, C ).
Preventing Restorative FailureLack of a ferrule also can focus excessive occlusal forces on the post and core and eventually cause the post to loosen or fracture17 (Fig. 17-16).
Avoiding Marginal Problems With RestorationsExcavation of caries below the free gingival margin or a frac-ture requires subgingival margin placement, or impressions and restorations will be faulty (Fig. 17-17). Exposure of all margins will ensure the chance for an excellent restorative result.
Managing Deep FracturesMany deep subgingival fractures cannot be restored adequately, and over time the tooth may develop peri-odontal complications. Crown lengthening addresses such
FIGuRE 17-16 Lack of “ferrule effect” in previous crown preparation led to post fracture.

362 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
FIGuRE 17-17 Failure to include entire tooth circumference in crown preparation, owing to lack of visibility of mesial aspect of tooth. Marginal leakage is also a result. Crown lengthening might have been the means to avoid this outcome.
A
B
FIGuRE 17-18 a, Fractured palatal cusp on a maxillary first premolar. This would be a restorative challenge and a long-term periodontal liability. B, After crown lengthening, the periodontium is in a normal relationship, and the restoration will be routine.
A
B
FIGuRE 17-19 a, A fractured maxillary lateral incisor with a calcified canal and hyperplastic gingiva covering part of the remaining tooth surface. B, Locating the canal is much easier after crown lengthening.
complications prior to restoration, resulting in a routine procedure with an excellent, uncomplicated prognosis (Fig. 17-18).
Location of Obscure Root Canal OrificesA specific endodontic indication is the case in which a coronal fracture has resulted in hyperplasia of the marginal gingiva, obscuring the location of a canal orifice. Often, if these frac-tures were present as mere cracks for any length of time, narrowing and calcification of adjacent root canal orifices occurred secondary to long-term bacterial ingress and pulp tissue irritation. After crown lengthening, orientation is greatly improved, enhancing access preparation and canal orifice location (Fig. 17-19).
Following Orthodontic Extrusion of Teeth or RootsThe techniques for orthodontic extrusion are discussed in previous editions of this text and in the orthodontic

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 363
literature. The periodontal consequence of extrusion is coronal movement of the attachment.5 Crown lengthening will usually be necessary to reposition the gingival margin apically for both esthetics and restorability (Fig. 17-20).
Potential Contraindications for Crown Lengthening
There are both general and local considerations in which crown lengthening may not be considered in the treatment planning for tooth retention.
Medical StatusGenerally, the medical status and current medications pre-scribed for the patient are reviewed for the same conditions that would contraindicate any surgical procedure. The reader is referred to other texts on oral surgery for a discussion of these issues.
Esthetic ZoneLoss of a clinical crown through fracture is a common indica-tion for crown lengthening. In the esthetic zone, however,
A
B
FIGuRE 17-20 a, The attachment follows the tooth in orthodontic extrusion. B, Crown lengthening is indicated to reposition the gingival attachment apically for both restorative and esthetic purposes.
FIGuRE 17-22 A severely carious molar with less than 4 mm of root trunk. Crown lengthening cannot be accomplished without exposure of the furcation.
FIGuRE 17-21 Crown lengthening alone on fractured teeth leads to unesthetically long crowns. Orthodontic extrusion should be considered first.
apical repositioning of the gingival margin may be unaccept-able esthetically,33 particularly in a patient with a prominent “gingival smile.” Even though the restorative results may be technically excellent, the crown may be unacceptably long (Fig. 17-21).
Minimal Vertical Dimension of the Root TrunkOn molar teeth, the root trunk is defined as the distance from the furcation to the level of crestal bone. If the trunk distance is less than 4 mm, crown lengthening cannot establish the 4 mm of tooth exposure without extending past and into the furcation11 (Fig. 17-22).
Surgical Techniques for Crown Lengthening
Surgical crown lengthening does not require an extensive list of instruments or supplies. Generally the procedure will

364 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
FIGuRE 17-23 Surgical-length round burs.
A B
FIGuRE 17-24 a, Brasseler end-cutting bur. B, Enlarged photo showing smooth sides and cutting flutes on ends only.
include a standard oral surgery setup to incise, elevate, reflect, reposition, and suture tissue. In addition, a set of periodontal curettes, a small chisel, and a series of surgical-length round burs will be sufficient to complete most procedures. If the clinician is already equipped to perform periapical surgery, few additions to the instrument list will be necessary. A sug-gested instrument list is provided in Table 17-1; all instru-ments listed have functional substitutes.
Surgical ProceduresThe objective of the surgical procedure is to place a sound dentinal margin at least 2 mm above the free gingival margin. Since the average sulcular depth of the normal periodontium is greater than 2 mm, the dentin margin will have to be at least 4 mm above the crestal bone. At the very least, in areas with minimal attached gingiva, horizontal surgical incisions
taBLE 17-1 Suggested Instruments for Crown Lengthening Procedures
Instrument Suggested Choice
Scalpel Bard-Parker No. 15
Periosteal elevator No. 7 Spatula or Woodson No. 1*
Periosteal retractor Seldin No. 23 or Minnesota*
Periodontal curettes Gracey 1-2, 11-12, 13-15, and 15-16*
Surgical-length burs Round (USA) No. 2, 4, 6, 8; ISO 1.0, 1.4 1.8, and 2.3 mm (Fig. 17-23)
End-cutting bur Brasseler (USA) 958C WDEPTH† (Fig. 17-24)
Chisel Wedelstadt 1-2‡
Needle holder Mayo-Hegar 140 mm, preferably with tungsten carbide†
Suture 4-0 Resorbable
* Hu-Friedy Co., Chicago, Illinois, USA.†Brassler USA, Savannah, GA, USA.‡CK Dental Industries, Orange, CA, USA.
should be placed in the sulcus to preserve all available gingival tissue. On the other hand, in areas of attached gingiva that measure over 5 mm, including the entire palate, the surgical plan may include resection of gingival tissue from the margin to effect crown lengthening. Following crown lengthening, biologic width will be restored and stable at 6 months from the date of surgery.28 At 1 year, the gain in exposed tooth structure has been observed to diminish as gingival tissue appears to rebound.38 For purposes of discussion, the step-by-step labial or buccal approach will be described in an uncomplicated case with a healthy, normal preoperative periodontium.
Envelope Tissue FlapAn envelope flap is the design of choice for crown lengthen-ing, because the keratinized gingival tissues are much easier to elevate, retract, and suture.20 Postoperatively, the course of healing is more rapid and less uncomfortable than flap designs with a vertical incision into the mucosa.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 365
Under appropriate local anesthesia, a reverse-bevel sul-cular incision (Fig. 17-25) is made to the crestal bone, beginning in the mesial labial aspect of the tooth immedi-ately anterior to the tooth that requires crown lengthening, continuing through the mesial and distal papillae, and ending distal labial to the tooth immediately posterior. The incision line should be scalloped to recreate the papillary form (Fig. 17-26, A-C ). If there is more than 5 mm of attached gingiva, the incision can be placed submarginally so as to leave 5 mm of gingiva. Removal of the excised, marginal tissue will effect crown lengthening in this area. If there is insuf-ficient relaxation for the tissue, a vertical incision is indicated. It should be located anterior to the tooth being treated and should include the papilla (see Fig. 17-26). This often occurs in the canine area where the flap is covering a convex bony anatomy.
If crown lengthening is to be circumferential, the identi-cal tissue incision and reflection would be done on the palatal or lingual aspects. Procedures on the lingual aspect of mandibular teeth are always done with envelope flaps. Since it is very difficult to obtain vertical mobility of a
A B
FIGuRE 17-25 a, Diagram of a maxillary premolar with a subgingival fracture of the buccal cusp. B, Clinical photo of fractured maxillary first premolar.
B
A
C
FIGuRE 17-26 a, Preoperative diagram of a fractured maxillary second premolar with incision line for full mucoperiosteal envelope flap (broken line). B, Clinical photograph of completed incision with curettage of marginal tissue. C, Diagram of same incision line with addition of vertical relief incision (broken line).
lingual flap, a submarginal incision is indicated to create a more apical flap margin. The palatal soft tissues are com-pletely keratinized, which allows for apical placement of the incision line at any desired level (Fig. 17-27). All tissue excised from the margins of the flap are removed with peri-odontal curettes.
FIGuRE 17-27 A palatal incision can be placed at any level. Note the inclusion of papillary form.

366 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
FIGuRE 17-28 Diagram of the undermining incision.
FIGuRE 17-29 Photograph of the connective tissue severed from the papilla areas of the flap with the undermining incision. This tissue is removed with periodontal curettes together with all interproximal soft tissue.
A
B
C
D
FIGuRE 17-30 a, Elevated palatal flap after the undermining incision. B, Following curettage of the connective tissue. C, The mobile flap margin can be drawn to the tooth with sutures. D, Three-week reevaluation photograph indicating normal healing. Note that crown lengthening was accomplished with soft-tissue reduction only.
Thinning or Undermining the TissueUsing the scalpel, a second “undermining” incision to the bone is made parallel to the surface of the gingiva through the papillae to produce a uniform flap thickness of approxi-mately 2 mm (Fig. 17-28). The connective tissue severed from the papilla is continuous with the interproximal tissue (Fig. 17-29). All of this connective tissue is now removed with periodontal curettes. If crown lengthening is limited to either the buccal or lingual, the interproximal tissue must be severed from the papillae on the opposite side prior to curettage.
Undermining of the entire tissue flap is frequently required on palatal surgeries to achieve mobility of the flap margin. The excised connective tissue is then removed with periodon-tal curettes. Mobility will allow the tissue to be drawn against the tooth during suturing. Often, palatal crown lengthening can be accomplished by soft-tissue reduction alone (Fig. 17-30).
Recontour of Alveolar BoneThe tissue is now retracted, and the distance between crestal bone and the tooth margin is measured. A minimum of 4 mm of exposed root structure is required.2,10 If the patient

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 367
has lost supporting bone due to chronic periodontitis, the entire crown lengthening operation may be completed by repositioning of the soft tissues alone. In most cases, however, the crest of alveolar bone will be less than 4 mm from the margin of the tooth, and osseous recontouring will be necessary.
The No. 6 (1.8 mm) or 8 (2.3 mm) round bur is used to thin the alveolar crest of bone surrounding the tooth. The recontouring should include ramping into interproximal areas and should not leave sharp ridges or grooves (Fig. 17-31). Recalling the normal anatomy of these areas in the anterior region, the interproximal crest form should be pre-served or recreated, and in posterior areas, the interproximal contour should be flat buccal lingually. The smaller No. 2 (1 mm) and No. 4 (1.4 mm) round burs are used to reduce bone when more narrow interproximal areas are present. As the tooth surfaces are approached, the bone is made as thin as possible while avoiding contact with the tooth surface. Subsequently, the Wedelstadt chisel (CK Dental Industries, Orange, CA, USA) and periodontal curettes are used to remove the remaining bone up to the root surface at right angles (Fig. 17-32).
The Brasseler end-cutting bur (Brasseler USA, Savannah, GA, USA) may also be of use at this point if the interproximal space is accessible vertically—that is, there is no coronal tooth structure in contact with the adjacent tooth. The advantage of the end-cutting bur is that the interproximal surface of the bone is left in a flat plane, requiring less use of the Wedelstadt
chisel, and there are no cutting surfaces on the lateral surface of the bur, which protects the proximal root surfaces from unintended injury.
To assess the sufficiency of bone recontouring, it is useful to release the tissue and allow it to lie passively along the tooth. If it must be forced into the desired position, more bone should be removed. Ultimately, with the tissue flap passively in place, 2 mm or more of tooth structure should be visible above the tissue margin.
Tissue ClosureThe tissue is now repositioned and stabilized with sutures apical to its original position (Fig. 17-33, A-C ), owing prin-cipally to the recontouring of the underlying bone. Two simple sutures or a sling suture from the mesial papilla to the distal papilla around the palatal surface of the tooth are usually sufficient to secure the flap. Generally, 4-0 suture material with a small curved needle will be the easiest to manipulate, but any type of suture material can be used. If the suture material is resorbable, an additional appointment for suture removal will not be required. Plain gut and chromic gut resorbable suture materials should be hydrated before use to reduce breakage when the knots are tied. The easiest method is to open the sterilized packet and drop the suture on its cardboard mount into a cup of water before beginning the procedure, but this retains some of the bends in the suture and may not eliminate all the alcohol used as a preservative.
A B
C
FIGuRE 17-31 a, Diagram of the osseous recontouring technique with a round bur. B, Recontouring is continued circumferentially, with smaller burs used interproximally. C, Photograph of osseous recontouring with a surgical-length round bur. Note the slight ramping of the facial surface of bone toward the interproximal spaces.

368 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
C
A B
FIGuRE 17-32 a, Diagram of proper use of the Wedelstadt chisel to remove the thin bone remaining on root surface. The chisel is shown in a horizontal position elevating the thin remaining bone over the root surface to expose 3 to 4 mm of root surface. B, The chisel is now shown removing bone in the vertical position. C, Photograph of the chisel finishing the crestal bone at right angles to the root surface. This procedure is continued through the interproximal spaces. If necessary, this procedure can extend around the palatal (or lingual) surfaces as well.
A
B
C
2.0 mm
FIGuRE 17-33 a, Diagram of postoperative result. B, Photograph of completed crown lengthening. C, Cross-sectional diagram of postoperative result, showing desired restoration of biologic width and 2 mm exposure of tooth structure.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 369
Ideally, the suture material should be completely removed from the stint and placed in 100 mL of sterile water, where it will unwind in a jerky, undulating fashion and become hydrated.39 After 3 or 4 minutes, the suture material will have absorbed the maximum amount of water. Upon removal, the hydrated gut material will be smooth, devoid of residual knots, and pliable, with manipulative properties similar to silk suture.39
Periodontal Surgical DressingIn most cases, a periodontal dressing will not be necessary. The tissue flap should remain passively in its position on the bone. If, however, the suture tends to draw the margin of the flap over the tooth, a periodontal dressing will hold it in the desired position. Occasionally, an oversized tempo-rary crown is useful to contain the pack material (Fig. 17-34). For patient comfort, a dressing might also be considered if the area of surgery includes multiple teeth or there is exposed bone not covered by the flap. The dressing should be left in place for no more than 2 to 3 days, because a bacterial biofilm will gradually form on the inferior surface adjacent to the tissues, impeding the process of healing, although some authors have recommended that it be left on for at least 1 week.27 Often, with instructions, the pack can be removed by the patient, which eliminates the inconvenience of a return visit.
HealingThe usual healing period after crown lengthening is about 3 to 4 weeks (Fig. 17-35). This may vary from patient to patient and is dependent on the quality of dental hygiene during the healing phase. The accumulation of plaque pro-motes inflammation and delays healing. This can be a problem if the patient is reluctant to disturb the area because it is sore and apt to bleed with normal brushing. Nevertheless, light brushing should be encouraged; softening the bristles
FIGuRE 17-34 A periodontal dressing retained by an oversized temporary crown. FIGuRE 17-35 Three-week postoperative reevaluation.
of the toothbrush in hot water may lessen trauma on newly healing tissues. Alternatively, a cotton-tipped applicator with 3% hydrogen peroxide or 0.12% chlorhexidine 2 or 3 times a day can be recommended. Most often, within 7 days the area can be brushed as normal.19
CLINICAL PROBLEMProblem: A 36-year-old male was referred for extraction of the mandibular second premolar. The treatment plan was to then construct a fixed partial denture from the first premolar to the first molar. The second premolar had carious margins below the free gingival margin (Fig. 17-36, A). The patient pre-ferred to retain and restore the premolar if possible.
Solution: Crown lengthening was proposed as a possible solution for the problem of restorability. Assessing the depth of caries was difficult preoperatively, so the patient agreed that surgical crown lengthening would be the treatment of choice. The option of extraction remained if the caries proved to be too deep. In such cases, removal of excessive alveolar bone would compromise the periodontal support for the adja-cent teeth.
A reverse-bevel, mucoperiosteal flap with an anterior verti-cal releasing incision was reflected from the distal of the canine to the distal of the first molar on the buccal. On the lingual, an envelope flap was elevated. Using a high-speed No. 6 (1.8 mm) round bur, the bone was carefully removed and contoured to expose sufficient tooth structure on both the buccal and lingual surfaces. Interproximally, a No. 2 (1.0 mm) round bur was used to apically reposition the crest of the interproximal bone. The Wedelstadt chisel was used to remove the remaining interproximal bone on the root surfaces. At the same time, the new osseous contours were blended with con-tours of the bone around the adjacent teeth. The root canal treatment can be completed at any time, including immedi-ately following the surgery while anesthesia is in effect. Four weeks later there was excellent postoperative healing with supragingival exposure of 2 mm of sound tooth structure (see Fig. 17-36, B and C). The tooth is ready for the completion of restorative treatment with a post, core buildup, and crown.

370 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
Complications With Surgical Crown LengtheningThere are few complications to crown lengthening, and some problems are only complications as treatment planning con-cerns. These issues should be discussed with the patient before treatment is initiated. For example, an adjacent third
A B
FIGuRE 17-37 a, The distal caries on the second molar would be difficult to expose with crown lengthening alone. B, Removal of the third molar greatly improves the crown lengthening result.
C
BA
FIGuRE 17-36 a, Severely carious mandibular right premolar. B, Four-week reevaluation after crown lengthening indicating complete healing. C, Lingual view of the haled tissue.
The mucosal extensions of vertical incisions will heal slower than incisions in the keratinized tissues. While the soreness of these mucosal areas is a common postoperative complaint, there is usually no treatment indicated, and ulti-mately the wound will heal normally. This occurrence is another argument for use of the envelope flap design as much as possible.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 371
molar is occasionally an impediment to adequate crown lengthening exposure. Extraction of the third molar should be considered as a part of the crown lengthening procedure (Fig. 17-37). In the same way, the restorability of some teeth may be difficult to assess preoperatively. If during the proce-dure, the tooth appears unrestorable, extraction would be indicated (Fig. 17-38).
Generally, patients will not have significant discomfort following the procedure unless a great deal of bone recon-touring was necessary. Mandibular posterior surgeries tend to cause more discomfort than other areas. The most common postoperative complication is the formation of granulation tissue during the immediate postoperative healing period. This tissue is very tender to touch and bleeds easily; patients are reluctant to brush, which promotes further granulation tissue formation. This will sometimes occur if a temporary restoration is placed and makes postoperative hygiene more difficult (Fig. 17-39). Granulation tissue is easily removed under anesthesia with a periodontal curette. If the restoration appears to be a contributing factor, it should be reshaped or removed for the remainder of the healing phase.
A second complication is sloughing of the tissue margins. One contributing factor is making the flap too thin with the
BA
CD
FIGuRE 17-38 a, Radiograph of a mandibular right first molar with buccal caries under the crown margin. Note the radiolucency in the furcation. B, Following crown removal, surgical exposure and excavation. The furcation is extensively involved and unrestorable. C, The furcation is sectioned completely through to the lingual aspect. D, The roots are removed separately, preserving the ridge for an implant.
FIGuRE 17-39 Postoperative granulation tissue formation.
undermining incision. The flap margin should be no thinner than 2 mm. A more serious contributing factor is smoking. Heavy smoking has a very detrimental effect on healing of oral tissues.3,15,26,42 There is no treatment other than pallia-tive. It will gradually heal, but it may be a slow and painful

372 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
treatable nonsurgically (see Chapter 8 for discussion of these perforations).
Crown lengthening techniques will be of use in managing perforations that have occurred at the level of the marginal periodontium and have resulted in a periodontal lesion. Often the chief complaint is chronic gingival soreness. Inflammation related to the defect in the root and the physi-cal damage to the tissues will result in a periodontal defect that can be probed. Typically these perforations result from misdirected high-speed burs during endodontic access or during preparation for an endodontic post.
A B
FIGuRE 17-40 a, Necrosis of a surgical flap margin due to heavy smoking. B, Healing of the slough after 8 months.
process (Fig. 17-40). Patients should be encouraged to cease smoking for at least 1 week following the surgery, if not forever!
Application of Crown Lengthening Techniques to Other Endodontic Problems
Iatrogenic Perforation in the Marginal PeriodontiumIatrogenic perforations are found at every level of the root. Radiographic interpretation and diagnosis of lesions associ-ated with perforations were discussed in Chapters 3 and 4. This section will focus on treatment approaches for those that occur in the marginal periodontium. Perforations can occur during a search for a calcified canal or in the attempt to penetrate one to the apex. As discussed in Chapter 8, most perforations that occur in this way are small. If it is fresh and the pulp chamber did not contain necrotic tissue, it will be uninfected, and the healing response will be good.44 Immedi-ate internal repair with MTA (mineral trioxide aggregate; Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) is the treatment of choice.7 The repair of very small perforations is likely to be successful whether they are above the attachment or below.
Perforations that occur well below the level of periodontal attachment, such as stripping perforations or lateral perfora-tions from misdirected post preparations, are generally larger, more irregular, and difficult to repair internally. In these cases, the prognosis may be questionable.44 It is still worth-while to attempt an internal repair with MTA if the perfora-tion has just occurred. Chapter 18 will discuss surgical repair of perforation defects that are located well below the level of the gingival attachment and have caused lateral lesions to develop in the periodontium. A distinction should be made between perforations located well below the level of the attachment and those exposed to the oral environment. Per-forations that occur in the marginal periodontium are rarely
CLINICAL PROBLEMProblem: A 39-year-old patient presented with a perfora-tion that was made during access for root canal treatment in a mandibular second molar (Fig. 17-41, A). Note the two sections of a lentulo spiral that are embedded in the adjacent periodontal tissues. The chief complaint of the patient was chronic soreness of the gingival papilla between the first and second molars (see Fig. 17-41, B). Probings indicated periodontal bone loss only in the area adjacent to the per-foration site.
Solution: Surgery was performed only in the mesial papilla area, not circumferentially. An envelope flap was elevated in the same manner as for crown lengthening. The lentulo spiral fragments were removed, and the bone was recontoured so the tissue could be repositioned apically. The biologic width was restored below the perforation site (see Fig. 17-41, C). Healing was uneventful, and the root canal treatment was revised.
In the preoperative evaluation of perforation defects, peri-odontal probings will give an accurate assessment of the potential for successful pocket elimination. There is virtually no potential for regaining normal attachment over a peri-odontal pocket caused by a perforation. The basic approach of surgical crown lengthening is pocket elimination. If the pocket is too deep for successful elimination, extraction should be considered (Fig. 17-42).

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 373
A B
C
FIGuRE 17-41 a, Radiograph of a mandibular second molar with a repaired perforation to the mesial buccal. Note the two segments of lentulo spirals which are external to the root canal system. B, Clinical view of one segment of the lentulo spiral protruding into the gingival attachment (arrow). C, With flap reflected. The lentulo spiral segments are removed, and crestal bone is recontoured as with crown lengthening to restore biologic width.
A B
FIGuRE 17-42 a, Radiograph of a maxillary second premolar with a deep periodontal defect on the mesial secondary to an access perforation. B, Surgical exposure of the osseous defect. The probe indicates a depth of 6 mm from crestal bone level. Extraction is indicated.

374 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
E
A
BC
D
FIGuRE 17-43 a to E, Illustrations showing the repair of a labial perforation.
CLINICAL PROBLEMProblem: A 48-year-old patient presented with a perfora-tion in the marginal periodontium (Fig. 17-43). The chief com-plaint was chronic gingival soreness for at least 7 years (see Fig. 17-43, A). The defect could be felt with an explorer in the sulcus. The periapical radiograph indicated the perforation undoubtedly occurred in an unsuccessful attempt to locate an obscure or calcified canal (see Fig. 17-43, B).
Solution: The area was exposed with a typical envelope flap, revealing a large perforation on the midlabial surface of the root, with approximately 2 mm of crestal bone loss (see Fig. 17-43, C). The defect was repaired with routine restorative techniques and composite filling material (see Fig. 17-43, D). The tissue was repositioned to the preoperative level, but inevitably 1 to 2 mm of recession will occur (see Fig. 17-43, E). The patient was advised and was not concerned. No attempt was made to locate the canal; the apex was well healed from the apical surgery performed at the time of the original attempt at nonsurgical root canal treatment failed.
In the esthetic zone, a 1- or 2-mm loss of crestal bone will usually not pose an esthetic postoperative problem.
Deeper lesions as a result of a perforation ultimately turn into periodontal pockets. Pocket reduction or elimination may resolve the periodontal lesion but leave an unacceptable esthetic result. Repositioning the tissue flap apically would leave margins exposed (Fig. 17-44) or require an unaccept-ably long coronal anatomy (see Fig. 17-21). One solution to this problem may involve orthodontic extrusion. Extrusion could level the attachment and elevate the repair to a point where it can be covered by a crown margin (Fig. 17-45). Crown lengthening will still be necessary.
Fig. 17-46, A illustrates a second case in which the nonsurgical repair of a furcation perforation has failed. Since the attachment was lost and there was a bony defect in the furcation already, the result of any treatment will be a compromise to the periodontium. Nevertheless, the progno-sis was fairly good, and such a compromise is common in the long-term maintenance of periodontally involved teeth. Under local anesthetic, an envelope tissue flap was elevated,

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 375
FIGuRE 17-44 Crown lengthening in the esthetic zone can leave unacceptable gingival contours and root exposure.
FIGuRE 17-45 Orthodontic extrusion can eliminate periodontal defects caused by perforations into the marginal periodontium.
A
B
C
D
FIGuRE 17-46 a, Failure of an internal repair of a perforation. B, Envelope flap reflected and furcation granulomatous tissue removed. Probe demonstrates near through-and-through lesion. C, Recontoured interproximal bone, furcation bone, and furcation. D, Six-month reevaluation indicating stable periodontal status.
and granulomatous tissue was curetted from the furcation area (see Fig. 17-46, B). Using the same techniques as in crown lengthening, the bone was reduced in the interproxi-mal areas to the level found in the furcation. The bone in the furcation was recontoured inferiorly (see Fig. 17-46, C ). Finally, the furcation itself was enlarged superiorly and later-ally to facilitate oral hygiene. A 6-month recall indicated excellent healing and good maintenance (see Fig. 17-46, D).
Resorption Defects in the Marginal PeriodontiumRadiographic interpretation and diagnosis of lesions of inter-nal and external resorption were discussed in Chapters 3 and 4. This section will focus on the treatment of resorption defects that occur in the marginal periodontium.18 It is
possible for internal resorption to perforate the dentinal and cemental wall and cause a periodontal defect in the marginal periodontium (Fig. 17-47). Because the relative occurrence of internal resorption as opposed to external resorption is infrequent, this is a rare occurrence.34

376 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
The majority of resorptive lesions are found to originate in the periodontium, approximately at the level of the attach-ment.34 Sometimes this pathologic process is also referred to as cervical resorption or invasive cervical resorption.21-23 A variant has been described as invasive extracanal resorption, distinguished by the fact that radiographically and at surgery, the resorption process does not involve the pulp.14 Con-firmed etiologies for these resorptive defects are often inter-twined with orthodontic treatment (the most common sole factor),22 trauma,23 and a history of internal bleaching using
A B
C
FIGuRE 17-47 a, Photograph of a drainage tract originating from perforation from internal resorption on the second molar. The defect could be detected in the sulcus with a No. 17 explorer. B, Radiograph illustrating extensive internal resorption. C, Surgical exposure of the small perforation using an envelope tissue flap. The defect was repaired and root canal treatment followed.
the heated technique as the prime etiologies. Young female patients appear to be predisposed to this pathologic process.29 Because the lesions usually originate in the mar-ginal periodontium, the surgical techniques used for crown lengthening are easily adapted for the repair of resorptive defects (see Chapter 13).
Most lesions of external resorption are more extensive than the case presented in Fig. 17-48. Since the process appears to originate at the level of the attachment, most resorptive lesions involve crestal bone as well.
CLINICAL PROBLEMProblem: A 28-year-old female was evaluated on referral for a presumptive diagnosis of internal resorption (Fig. 17-48). Angled radiographs demonstrated an external location, fortunately on the labial surface.
Solution: A mucoperiosteal flap was elevated from the position of a sulcular incision, and a vertical incision was included because of the lack of sufficient exposure with an envelope design. Gener-ally, vertical incisions are necessary when the flap extends around a curved area of the dental arch (see Fig. 17-48, C). The defect was repaired with composite resin (see Fig. 17-48, D), and the tissue he was repositioned apically to avoid closure over the repair material, which would likely have resulted in a periodontal pocket.
However, in these types of cases it may be possible to use a resin-composite (Geristore; Den-Mat®, Santa Maria, CA, USA), since human gingival fibroblasts have shown preferential attachment to this product, with minimal cytotoxicity.1 This material is a dual-cure, hydrophilic, nonaqueous, polyacid-modified composite resin. Its advantages are being insoluble in oral fluids and having increased adherence to tooth structure, low cure shrinkage, low coefficient of thermal expansion, radiopacity, fluoride release, and biocompatibility.12,13 Geristore has been used to repair mechanical root perforations.40 MTA (ProRoot MTA; Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) has also been used in combined endodontic-periodontic problems due to cervical resorption.18

B
A C
D E
FIGuRE 17-48 a, Referral radiograph indicating midroot radiolucency. B, Clinical view of mandibular right canine with no clinical evidence of pathosis. C, Surgical exposure of the lesion (arrows) with a triangular flap (one vertical incision). Note there is no pulpal involvement. D, Repair of the defect with composite resin. E, Closure with tissue apically repositioned.
CLINICAL PROBLEMProblem: A 44-year-old patient was seen following nonsurgical and surgical root canal treatment of a lesion found in a mandibu-lar canine (Fig. 17-49, A). The first premolar also had extensive resorption well below the level of the attachment and on the lingual surface. Repair was not possible, and it was treatment planned for extraction.
Solution: Under local anesthesia, a mucoperiosteal envelope tissue flap was elevated in the same manner as for crown length-ening. In the area of the resorption, the tissue in the resorptive defect was severed from the lining of the tissue flap, leaving the tissue with adequate thickness (approximately 2 mm). Next, the defect was curetted to eliminate the soft tissue. Commonly, the gingival and lateral margins of the resorption defect can be indis-tinguishable from the surrounding bone (see Fig. 17-49, B), but in some cases, bone will extend into the resorptive defect. Using the same approach as in crown lengthening, the bone surrounding the lesion was removed to expose the margins of the resorptive defect (see Fig. 17-49, C). The bone was contoured interproximally
with the intent of repositioning the tissue apically to a level below the resorptive repair. After healing, normal probings were expected in all areas. Next, the margins of the defect were refined for a Class I composite or compomer restoration (see Fig. 17-49, D). Glass ionomer restorations are not recommended, owing to their tendency to degrade subgingivally and because they are cytotoxic, so the use of a resin ionomer may be indicated. To maintain root canal patency during placement of the restoration, calcium hydroxide was placed into the exposed canal and packed densely with dry cotton pellets (see Fig. 17-49, E). Routine restor-ative procedures were used to place the resin filling. With the densely packed calcium hydroxide in place, the cavity can be etched and dried (see Fig. 17-49, F). The resin restoration was placed (see Fig. 17-49, G). Following the restoration, the tissue was repositioned and stabilized with sutures—in this case, after extraction of the premolar (see Fig. 17-49, H). Routine root canal procedures can be performed immediately or on a subsequent visit (see Fig. 17-49, I). Reevaluation at 5 years (see Fig. 17-49, J) indicated excellent healing. Recurrence is possible but is fortu-nately uncommon with this approach.

378 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
A
B
C
D
E
F
G
FIGuRE 17-49 a to J, Illustrations of a routine repair of a cervical resorptive defect.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 379
The basic concepts of surgical crown lengthening are also useful for exploratory purposes. For resorption defects, explo-ration may be required to determine if the problem can be treated. Some defects may extend well below crestal bone into inaccessible interproximal surfaces or into the furcation. Even if repairable, the prognosis for periodontal maintenance may be poor (Fig. 17-50). In some cases, efforts have been made to consider intentional replantation, which allows for repair in these isolated, difficult-to-get-to defects.41
Vertical Root Fracture RepairAlthough the periodontal probing pattern of most vertical root fractures is virtually diagnostic in itself, some fractures
H
I
J
FIGuRE 17-49, cont’d
may be atypically located, may not probe in the usual vertical manner, or may present as a lesion of periodontal origin. The true diagnosis may not be known without surgical explor-atory exposure. The flap designs for surgical access would be the same as those used in surgical crown lengthening. In most cases, the presence of a vertical root fracture to the apex requires either extraction of the tooth, or in the case of some multirooted teeth, removal of the individual fractured root (Fig. 17-51). Root resection and hemisection techniques will be discussed in the following chapter. A rare case of a suc-cessful treatment of a vertical root fracture is presented in Fig. 17-52.

380 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
A B
C
D
FIGuRE 17-50 a, Sinus tract near the maxillary left first molar is the chief complaint. B, Radiograph indicates extensive resorption. C, Exploratory surgery reveals furcation defect with poor prognosis. D, Extracted tooth reveals an extensive furcation defect.
FIGuRE 17-51 Elevation of mucoperiosteal flap for diagnosis of a vertical root fracture (arrow). Flap technique is the same as for crown lengthening.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 381
A B
C D
EF
G
FIGuRE 17-52 a to G, Illustrations of a successful vertical root fracture repair with mineral trioxide aggregate. The repair was performed in February of 2006. The reevaluation radiograph and photos were made in September 2007. Probings were 4 mm in the site of the repair.

382 chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins
REFEREnCES1. Al-Sabek F, Shostad S, Kirkwood KL: Preferential attachment of
human gingival fibroblasts to the resin ionomer Geristore, J Endod 28:291-294, 2005.
2. Assif D, Pilo R, Marshak B: Restoring teeth following crown lengthening procedures, J Prosthet Dent 65:62-64, 1991.
3. Balaji SM: Tobacco smoking and surgical healing of oral tissues: a review, Indian J Dent Res 19:344-348, 2008.
4. Becker W, Ochsenbein C, Becker B: Crown lengthening: the peri-odontal restorative connection, Compend Contin Educ Dent 19:239-254, 1998.
5. Biggerstaff RH, Sinks JH, Carazola JL: Orthodontic extrusion and biologic width realignment procedures: methods for reclaiming nonrestorable teeth, J Am Dent Assoc 112:345-348, 1986.
6. Bowers GM: A study of the width of attached gingival, J Peri-odontol 34:2012-2019, 1963.
7. Clauder T, Shin S-J: Repair of perforations with MTA: clinical applications and mechanisms of action, Endod Topics 15:32-55, 2009.
8. Cohn SA: Treatment choices for negative outcomes with non-surgical root canal treatment: nonsurgical retreatment vs. surgical retreatment vs. implants, Endod Topics 11:4-24, 2005.
9. Curtis DA, Sharma AB, Finzen FC: The use of dental implants to improve quality of life for edentulous patients, J Calif Dent Assoc 36:275-280, 2008.
10. Deas DE, Moritz AJ, McDonnell HT, et al: Osseous surgery for crown lengthening: a 6-month clinical study, J Periodontol 75:1288-1294, 2004.
11. Dibart S, Capri D, Kachouh I, et al: Crown lengthening in man-dibular molars: a 5-year retrospective radiographic analysis, J Peri-odontol 74: 815-821, 2003.
12. Dragoo MR: Resin-ionomer and hybrid-ionomer cements: part I. Comparison of three materials for the treatment of subgingival root lesions, Int J Periodontics Restorative Dent 16:594-601, 1996.
13. Dragoo MR: Resin-ionomer and hybrid-ionomer cements. part II. Human clinical and histologic wound healing responses in specific periodontal lesions, Int J Periodontics Restorative Dent 17:75-87, 1997.
14. Frank AL: Extracanal invasive resorption: an update, Compend Contin Educ Dent 16:250-260, 1995.
15. García B, Larrazabal C, Peñarrocha M, et al: Pain and swelling in periapical surgery, Med Oral Patol Oral Cir Bucal 13(11):E726-E729, 2008.
16. Gargiulo A, Krajewski J, Gargiulo M: Defining biologic width in crown lengthening, CDS Rev 88:20-23, 1995.
17. Gegauff AG: Effect of crown lengthening and ferrule placement on static load failure of cemented cast post-cores and crowns, J Prosthet Dent 84:169-179, 2000.
18. Gonzales JR, Rodekirchen H: Endodontic and periodontal treat-ment of an external cervical resorption, Oral Surg Oral Med Oral Pathol Oral Radio Endod 104:e70-e77, 2007.
19. Gutmann JL: Surgical endodontics: post-surgical care, Endod Topics 11:196-205, 2005.
20. Gutmann JL, Harrison JW: Surgical endodontics. Boston, 1991, Blackwell Scientific Publications.
21. Heithersay GS: Clinical, radiologic, and histopathologic features of invasive cervical resorption, Quintessence Int 30:27-37, 1999.
22. Heithersay GS: Invasive cervical resorption: an analysis of potential predisposing factors, Quintessence Int 30:83-95, 1999.
23. Heithersay GS: Invasive cervical resorption following trauma, Aust Endod J 25(2):79-85, 1999.
24. Iqbal MK, Kim S: For teeth requiring endodontic treatment, what are the differences in outcomes of restored endodontically treated teeth compared to implant-supported restorations? Int J Oral Max-illofac Implants 22(Suppl):96-116, 2007.
25. Iqbal MK, Kim S: A review of factors influencing treatment plan-ning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy, J Endod 34:519-529, 2008.
26. Kaldahl WB, Johnson GK, Patil KD, et al: Levels of cigarette consumption and response to periodontal therapy, J Periodontol 67:675-681, 1996.
27. Klokkevold PR, Takei HH, Carranza A: General principles of periodontal surgery. In Newman MG, Takei HH, Klokkevold PR, Carranza A, editors: Carranza’s clinical periodontology, ed 10, St. Louis, 2006, Saunders Elsevier.
CLINICAL PROBLEMProblem: A 46-year-old woman reported chronic soreness in the buccal gingiva adjacent to the mandibular right second molar. A periapical film indicated the tooth had previous root canal treatment that appeared technically excellent, and there was no evidence of pathosis (see Fig. 17-52, A). Clinically, however, prob-ings revealed a narrow defect on the buccal surface over the distal root, consistent with a vertical root fracture (see Fig. 17-52, B). However, unlike the majority of root fractures that probe to the apex, the probing depth was only 6.5 mm. Exploratory surgery was recommended.
Solution: An envelope tissue flap was elevated on the buccal side as in crown lengthening (see Fig. 17-52, C). The exposure revealed a vertical fracture line extending apically from the crown to a level about 4 mm below crestal bone. The generally poor long-term prognosis was discussed with the patient, but due to
the minimal depth of the fracture line, the decision was made to attempt a repair. The fracture line was enlarged with a No. 2 (1 mm) round bur and filled with the white formulation of MTA (see Fig. 17-52, D and E). MTA is not reported to be successful in repair of defects in contact with oral fluids but has been success-ful in the repair of a variety of defects below the level of the attachment, which will be discussed in the next chapter. The patient returned for reevaluation 7 months after the procedure, reporting no symptoms. Probing indicated a 4.5-mm attachment level in the surgical area (see Fig. 17-52, F), and the gingival margin was approximately at the same level as it was preoperatively. No crown lengthening was included in the original procedure. The radiograph made at reevaluation indicated healing of the post-surgical radiolucency (see Fig. 17-52, G). This case appears to offer hope that continued research in the area of surgical repair will provide materials capable of producing this result routinely on fractures of any depth.

chapter 17 | Problem Solving in the Management of Teeth With Subgingival Carious and Fractured Margins 383
28. Lanning SK, Waldrop TC, Gunsolley JC, et al: Surgical crown lengthening: evaluation of the biological width, J Periodontol 4:468-474, 2003.
29. Liang H, Burkes EJ, Frederiksen NL: Multiple idiopathic cervical root resorption: systematic review and report of four cases, Dentomaxillofac Radiol 32:150-155, 2003.
30. Lovdahl PE: Periodontal management and root extrusion of trau-matized teeth, Dent Clin North Am 39:169-179, 1995.
31. Lovdahl PE, Gutmann JL: Periodontal and restorative consider-ations prior to endodontic therapy, Gen Dent 28(4):38-45, 1980.
32. Maynard G, Wilson RD: Physiologic dimensions of the periodon-tium significant to the restorative dentist, J Periodontol 50:170-174, 1979.
33. Melnick P: Preparation of the periodontium for restorative den-tistry. In Newman MG, Takei HH, Klokkevold PR, Carranza A, editors: Carranza’s clinical periodontology, ed 10, St. Louis, 2006, Saunders Elsevier.
34. Ne RF, Witherspoon DE, Gutmann JL: Tooth resorption, Quin-tessence Int 30:9-25, 1999.
35. Nickenig HJ, Wichmann M, Andreas SK, et al: Oral health-related quality of life in partially edentulous patients: assessments before and after implant therapy, J Craniomaxillofac Surg 36:477-480, 2008.
36. Novak JM, Albather HM, Close JM: Redefining the biologic width in severe, generalized, chronic periodontitis: implications for Therapy, J Periodontol 79:1864-1869, 2008.
37. Perez JR, Smukler H, Nunn ME: Clinical dimensions of the supra-osseous gingivae in healthy periodontium, J Periodontol 79: 2267-2272, 2008.
38. Pontoriero R, Carnevale G: Surgical crown lengthening: a 12-month clinical wound healing study, J Periodontol 72:841-848, 2001.
39. Rakusin H, Harrison JW, Marker V: Alteration of the manipulative properties of plain gut suture material by hydration, J Endod 14:121-124, 1988.
40. Resillez-Urioste F, Sanandajt K, Davidson RM: Use of a resin-ionomer in the treatment of mechanical root perforation: report of a case, Quintessence Int 29:115-118, 1998.
41. Shuman IE: Repair of a root perforation with a resin-ionomer using an intentional replantation technique, Gen Dent 47:392-395, 1999.
42. Silverstein P: Smoking and wound healing, Am J Med 93(1A):22S-24S, 1992.
43. Torabinejad M, Goodacre CJ: Endodontic or dental implant therapy: the factors affecting treatment planning, J Am Dent Assoc 137:973-977, 2006.
44. Tsesis I, Fuss Z: Diagnosis and treatment of accidental root perfo-rations, Endod Topics 13:95-107, 2006.
RECOMMEnDED ADDITIOnAL READIngDibart S: Practical advanced periodontal surgery, Oxford, 2007, Black-
well Munksgaard.Fugazzotto P: Decision making: the furcated molar, J Implant Adv Clin
Dent 2:63-87, 2010.Merino EM: Endodontic microsurgery, London, 2009, Quintessence
Publishing Co. Ltd.

384
Chapter 18
Problem-Solving Challenges That Require Periradicular Surgical Intervention
Problem-Solving ListProblem-solving challenges requiring periradicular surgical considerations addressed in this chapter are:
Surgical Management of Problems Associated With Lateral Canals
Surgical Repair of Root Perforations Below the Attachment
Surgical Repair of Problems Associated With Some Root Fractures
Surgical Techniques for Resection of Roots and Teeth
General considerations
Case selection criteria
Endodontic considerations prior to root resection
Periodontal considerations prior to root resection
Restorative considerations before and after root resection
Surgical techniques for root resection
Basic recommendations for all root resections
Surgical techniques for tooth resection (hemisection)
Basic recommendations for all tooth resections
Outcomes Assessment for Teeth With Root or Tooth Resection
Maxillary molar roots
Mandibular molar roots
The successful management of perforative defects is dependent not only on the etiology of the perforation, but also on the early diagnosis of the defect, choice of treatment, materials used, host response and practitioner expertise.
J.L. Gutmann, 1991
Periapical surgery (see Chapter 16) and surgical management of defects in the marginal periodontium (see Chapter 17) address many of the problems encountered in tooth reten-tion. However, other challenges to tooth retention also exist on root surfaces below the level of periodontal attachment, and for the most part do not involve the marginal periodon-tium or the root apices. Often these issues are not considered in treatment planning in favor of tooth extraction and implant placement.14 Furthermore, many of these issues are
never explained to the patient relative to the treatment options and the potential outcomes.
There are two general approaches to problem solving the treatment of lesions or defects on root surfaces below the attachment. The first is aimed at the repair of defects on the root surfaces, with the nature of the defect and its location being of major importance. The surgical techniques advocated are modifications of the periapical surgical proce-dures discussed in Chapter 16. The second approach is to consider surgical techniques that result in complete root removal. These surgical concepts apply to a wide variety of clinical problems that can be addressed in a positive manner and result in a good prognosis for tooth retention, docu-mented levels of positive outcomes, enhanced patient satis-faction, and economic feasibility for a wide range of patients.
Surgical Management of Problems Associated With Lateral Canals
The clinical incidence of problems associated with natural lateral canals does not rise to the statistical percentage of roots that actually have anatomically demonstrable lateral canals.15,48 Additionally, the incidence of lateral canals in the middle and coronal thirds of roots is statistically rare. Most bony lesions that arise from necrotic debris in a nonvital tooth heal with routine nonsurgical treatment (Fig. 18-1). In

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 385
In the preoperative evaluation, determining the location of the lateral canal is a diagnostic challenge. Lateral canals can occur on any surface of the root and are rarely visible radiographically.48 Perhaps the easiest to locate are those that have clinical signs of a draining tract but no radiographic changes. These canals will usually be found on the labial aspect of the root (Fig. 18-4).
The presence of most lateral canals is inferred by the pres-ence of a lateral radiolucency, which is only a two-dimen-sional representation of a dynamic three-dimensional process (Fig. 18-5). Since lesions tend to develop symmetrically from the source of infection, the approximate location of the lateral canal, if present, can be identified vertically—that is, the midpoint between the coronal and apical limits of the lesion.
the case of a previously treated tooth, most lateral lesions resolve with revision, as demonstrated in Chapter 14, Fig. 14-6. This is all the more amazing because although many clinicians take personal pride in being able to extrude sealer, gutta-percha, or both through these canal spaces (Fig. 18-2), there are no proven techniques to actually clean and disinfect these aberrant channels. Furthermore, the empirical concept that pushing filling materials through these canals will débride this small space of its irritants is faulty.39
There are relatively few teeth with lateral lesions that fail to heal after root canal treatment. Even fewer are those which develop lateral lesions after root canal treatment.48 Unfilled or poorly obturated canal spaces can be a predisposing factor to the development of a lateral lesion, especially spaces between a gutta-percha filling and an intraradicular post (Fig. 18-3; see Chapter 20). Nonsurgical revision is usually the treatment of choice but not always feasible. Lesions that fail to heal, as well as those associated with teeth that cannot be revised, generally require surgical intervention.
A B
FIGuRE 18-1 a, Preoperative radiograph of an endodontically treated mandibular premolar with a lateral canal lesion. B, One-year reevaluation radiograph showing resolution of the lateral lesion. (Courtesy Dr. Ryan Wynne.)
FIGuRE 18-2 Postoperative image showing extrusion of the filling materials and/or sealer through the lateral canal.
FIGuRE 18-3 Amalgam repair of a lateral canal communicating with an unfilled canal space between the root canal filling material and the post. Case was treated in 1976.

386 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
The greatest difficulty is determining the location in a hori-zontal orientation. Lesions often extend circumferentially from their sources. What is observed radiographically as a lesion on the mesial or distal surface of the root may in reality originate from a lateral canal on either the palatal or labial
C
A
B
FIGuRE 18-4 a, Clinical view of a sinus tract found on the labial aspect of the maxillary left lateral incisor. B, No radiolucency is visible in this area. C, Surgical exploration reveals a midroot lateral canal on the labial surface.
aspect of the root. Palatally or lingually located lateral canals will generally not be accessible to surgical repair.
A second anatomic problem is the surgical accessibility of the canal in interproximal or interradicular spaces. Lateral canals occurring in fluting of molar roots can be impossible to see at surgery, although some may be large enough to locate tactilely with an explorer. Even if they can be located, space limitations can prevent successful completion of the repair. The only avenue for possible resolution of these dilemmas is surgical exploration. Preoperatively, the patient should be informed that if the lateral canal is not accessible, the root may have to be removed in its entirety or the tooth may have to be extracted (Fig. 18-6).
The essential elements of the surgical procedure are the same as for periapical surgery, which is described in detail in Chapter 16. The lateral communication is located, cleaned, enlarged, and filled exactly as one would surgically fill the prepared apical foramen on the resected root surface.44 A small ultrasonic tip or No. 15 or 20 K-file in the ultrasonic handpiece will usually follow the course of a lateral canal and enlarge it to the point at which a larger file or a diamond tip could follow the initial pathway. As with apical preparations, the size of the preparation must be sufficient for the place-ment of the filling (preferably mineral trioxide aggregate [MTA]).
FIGuRE 18-5 Messal bony lesion associated with a lateral canal presumably due to coronal leakage from recurrent caries.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 387
A B
C
FIGuRE 18-6 a, Lateral canal lesion located on the distal aspect of the mesial root of the mandibular right first molar. B, Extracted mesial root. Surgical repair was attempted, but it was not possible to visualize the lateral canal, owing to deep fluting of root surface. Note lateral canal (arrow). C, A radiograph of the root. Note the distance of the lateral canal (yellow dot) from the treated canals. Revision would have had no effect on this problem.
A B
FIGuRE 18-7 a, Preoperative radiograph of maxillary right central. Lesion associated with lateral canal extends from midroot level to alveolar crest in the midline. B, Reevaluation at 9 years, 3 months, demonstrating excellent healing.
CLINICAL PROBLEMProblem: A 47-year-old male presented with a draining sinus tract on the midline of the labial papilla adjacent to the maxillary right central incisor. The lesion was difficult to discern radio-graphically (Fig. 18-7, A). A periodontal probe indicated normal sulcular probings but probed through the draining tract to the side of the root.
Solution: Because of the presence of a post in the root and the absence of any periapical pathosis, the midroot area was exposed surgically, and the presence of a lateral canal was confirmed and repaired. A 9-year, 3-month reevaluation radiograph indicated excellent healing with restoration of the periodontal ligament space and lamina dura in the surgical site (see Fig. 18-7, B).

388 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
C
A B
FIGuRE 18-8 a, Furcal bone loss associated with an access perforation through the floor of the furcation. B, Calcium hydroxide used as a temporary seal during completion of the endodontic treatment. C, Reevaluation after 1 year. The perforation was permanently sealed with mineral trioxide aggregate. Note the restoration of normal bone architecture in the furcation.
As described for apical surgery in Chapter 16, some diamond-coated or metal ultrasonic instruments may be too large to begin the preparation, so a smaller-tipped instrument or a small endodontic file must be selected. Low to medium power is indicated to prevent aggressive and indiscriminate cutting of root structure.44 Instruments with ideally angled tips for access to these aberrant canals should be considered (see Figs. 16-33 and 16-34).
Surgical Repair of Root Perforations Below the Attachment
Most perforations during access opening occur in the mar-ginal periodontium (see Chapters 8 and 16). The only common exception to this observation is the case where the access perforation occurs in the furcation. If the attachment tissues are not disturbed, small furcation perforations have a good chance of long-term stability with an internal repair using MTA47 (Fig. 18-8).
Larger perforations in the furcation can be problematic. If significant portions of the floor of the pulp chamber have
been removed, the chance of successful repair is poor (Fig. 18-9).47 Similarly, cases that have been repaired with materials other than MTA may have poor long-term out-comes, especially if the material is forced through the defect into the periodontal tissues.45 It is almost impossible to remove the excess nonsurgically, and attempts are likely to make the perforation larger. In this regard, even surgical repairs with MTA of larger perforations of the roots in the furcation can have mixed results. Fig. 18-10 illustrates a case in which a perforation was initially repaired internally with MTA. After 61
2 years, a furcation radiolucency lesion had developed, and a surgical repair was attempted. One year later, the bone had not healed completely. Although the patient was symptom free and the tooth functional, the prog-nosis was guarded.
Lateral strip perforations can occur during root canal cleaning and shaping, generally with hand instruments or excessive use of large nickel-titanium instruments (see Chapter 10). Often the anatomy of the root plays a role (Fig. 18-11); deep flutes or invaginations of the proximal root surfaces cannot be discerned radiographically. Although anti-curvature filing (see Chapter 10), skewed positions of the access cavity, and other techniques are effective in reducing this problem, it cannot be avoided completely.

FIGuRE 18-9 Extrusion of cement repair material through a furcation perforation. Chronic drainage through the gingival sulcus was apparent at the time of examination. Extraction was recommended.
A B
CD
E
FIGuRE 18-10 a, Referral radiograph of mandibular left first molar. The furcation was perforated in the access procedure and was temporarily repaired with calcium hydroxide (arrows). B, Root canal treatment completed and perforation filled with mineral trioxide aggregate. It was a challenge to pack the material and not have extrusion. C, Reevaluation radiograph after 6 1
2 years. Probings were normal but tooth was symptomatic, and the tooth had a sinus tract on the buccal mucosa. D, Surgical repair in progress. Note the intact crestal bone over the furcation. E, Fifteen-month reevaluation. Patient was asymptomatic, sinus tract had not reappeared, but prognosis was guarded.

390 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
C
A
B
D
FIGuRE 18-12 a, Lateral lesion associated with a strip perforation. Probings are normal. B, Radiograph of repair with mineral trioxide aggregate. C, One-year reevaluation film showing restoration of normal periodontium on the buccal. Probings were normal. D, One-year reevaluation radiograph indicating bone healing in the furcation.
FIGuRE 18-11 Routine access and orifice-widening procedures on extracted tooth with a deeply fluted mesial root. A strip perforation quickly occurred that appeared to be unavoidable in a clinical case.
As with lesions adjacent to lateral canals, accessibility to the defect can be a major problem for repair, but these defects are usually larger and much easier to locate. If the defect is visible, the repair can be made in the same manner as with the repair of defects from lateral canals. Often the preparation must be longer vertically because of the thin dentin above and below the perforation itself (Fig. 18-12).
Strip perforations can also occur from excessive enlarge-ment of the canal during post space preparation.36 This is seen most often in roots with thin mesial-distal widths and roots with fluted anatomy on the proximal surfaces. If accessible, the techniques for placing an MTA filling are effective (Fig. 18-13). Many strip perforations resulting from post preparations are particularly difficult to repair because very thin dentin remains around the perforation defect. The greater the post diameter, the thinner the tooth structure will be. Cutting into the metal of the post requires a high-speed handpiece and good access. Some creative, specialized approaches may be considered to repair these defects, but they are beyond the scope of this text. It is usually better to remove the post if pos-sible (Fig. 18-14).
Perforations with endodontic instruments can occur deep in the root from failure to negotiate curves, attempting to bypass blockages, or failing to consider the normal anatomy of the tooth during cleaning and shaping procedures. If dis-covered early, internal repairs may effectively resolve the per-foration problem; if not possible, then surgery will probably be necessary.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 391
A B
FIGuRE 18-13 a, Lateral lesion associated with a stripping perforation due to overenlargement of the canal for post preparation. B, Five-month reevaluation indicating healing of the lesion.
A B
FIGuRE 18-14 a, Intraradicular post protruding through a perforation. B, Removal of the post is preferred, rather than attempting to cut the post back into the root prior to repairing the perforation.
CLINICAL PROBLEMProblem: A 38-year-old female presented with what was con-sidered to be a failing root canal procedure on a maxillary right central incisor (Fig. 18-15, A). The tooth had been root treated approximately 6 years previously. At the time of examination, the symptoms were palpation tenderness, dull aching, and per-cussion tenderness. The periapical film indicated a well-filled root canal, but a large periapical radiolucency was present, and non-surgical revision of the previous treatment was recommended.
Solution: The tooth was reopened, and while the existing filling material was being removed, the patient felt pain at
a level well short of the estimated tooth length. An instru-ment was placed, and a radiograph was made. A labial per-foration was revealed that proved to be the etiology of all the current pathosis (Fig. 18-15, B). Reparative surgery was performed, and the perforation was repaired with MTA. A 1-year reexamination indicated excellent healing of the original lesion without revision of the root canal treatment in the apical half of the canal. A porcelain veneer crown had been placed by another dentist in the interim, but unfortunately, the post space that had been prepared for the final restora-tion was not properly used.

392 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
Surgical Repair of Problems Associated With Some Root Fractures
The etiology of partial root fractures on the lateral root surface of some teeth is unknown. Clinical findings are typical of lesions associated with lateral canals or strip perfo-rations along with normal periodontal probings. Often the signs of acute or chronic inflammation/infection (midroot swelling, sinus tracts, etc.) are present.
A CB
FIGuRE 18-15 a, Root-treated maxillary right central incisor with a large apical lesion. B, Instrument in perforation. The perforation was repaired with mineral trioxide aggregate. C, One-year reevaluation. Note that the post space was not used in placement of crown. This presents a long-term liability for continued success of the repair.
A B
FIGuRE 18-16 a, Preoperative radiograph of a large radiolucent lesion assumed to be associated with a lateral canal on the treated second premolar. B, Fracture line (arrows) located on palatal surface. Tooth was extracted due to inaccessibility.
Radiographic findings are similarly nonspecific. The radiolucency is characterized by an apical and a coronal border. In these cases, the apex is usually not involved (see Fig. 18-16, A). Consequently, it is not possible to make the specific preoperative diagnosis of partial vertical root fracture. In all cases, they are discovered at surgery. The clinical appearance is a vertical fracture line located in the midroot area on the palatal surface (see Fig. 18-16, B).
If the fracture line is in a position where repair is possible, the techniques for lateral repairs will be effective. The most significant and difficult modification is the preparation that

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 393
A
C D
B
FIGuRE 18-17 a, Preoperative radiograph of a lateral radiolucency assumed to be associated with a lateral canal on the treated first premolar. B, Surgical exposure reveals a vertical midroot fracture line (arrows). C, Repair of the fracture line with MTA. D, Four-year reevaluation radiograph indicating excellent healing.
must follow the crack line to its full extent. The result is a narrow slot preparation similar to the preparation of an isthmus between two canal orifices in periapical surgery.
If straight-line access is possible, a quarter-round (0.5 mm) bur is ideal. For maximum control, the straight, low-speed
handpiece, held in the pencil grip, works well. If straight-line access is not possible, the ultrasonic instrument can be used with either a small, angled apical surgery tip or an endodontic file that has been shortened to increase stiffness and placed in a special ultrasonic adaptor.
Surgical Techniques for Resection of Roots and Teeth
General ConsiderationsRoot resection, or root amputation, involves removing the root and either leaving the crown intact (Fig. 18-18) or additionally removing the portion of the crown that overlies the removed root.26,27,49 In the treatment of maxillary molars, this procedure is also known as trisection.20,24 This concept also applies to the removal of a single-rooted tooth from a multiabutment fixed bridge or splint.25
Tooth resection, or hemisection, is a technique in which a tooth is “cut in half.”27 As with root resection, multiple techniques can be used: cutting the tooth in half and retain-ing both segments, known as bicuspidization19 (Fig. 18-19),
CLINICAL PROBLEMProblem: A 40-year-old patient presented with a swelling in the midroot area of the mandibular left second premolar. The tooth had a previous root canal procedure and was restored with a post and crown. Radiographically, a large midroot radiolucency was present, and a large uncleaned lateral canal was suspected (Fig. 18-17, A).
Solution: Nonsurgical revision was not considered and the defect was exposed surgically. Following curettage, a midroot fracture line was observed on the distal buccal aspect (see Fig. 18-17, B arrows). Because of accessibility, the fracture line was prepared with a quarter-round (0.5 mm) bur and an ultrasonic tip. The preparation was filled with gray MTA (see Fig. 18-17, C). A reevaluation radiograph made 4 years later demonstrates excellent healing with restoration of a normal periodontal ligament space and lamina dura (see Fig. 18-17, D).

394 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
or cutting the tooth in half with the intent of retaining only one of the segments.1,5,35 (see Fig. 18-21). This type of resec-tion is seldom indicated due to the difficulty of restoring and maintaining the former furcation area. This procedure may also result in unfavorable soft and hard tissue relationships. Two areas of the mouth in which the resection procedure is reasonably successful are on on mandibular molars with sepa-rated roots and in some maxillary molars, with the removal of the palatal root.
Performing root/tooth resections to allow retention of compromised teeth has been all but abandoned owing to the success of contemporary implants.7,26,27 However, resective procedures are viable treatment considerations in preserving natural tooth structure and can provide the patient with a reasonable alternative in many critical clinical situations. When done properly and the patient practices good oral hygiene, success rates can be quite high and comparable to other treatment choices.12
Multiple published studies in the periodontal literature have supported root resection as a successful long-term treat-ment.* Success with this treatment modality is generally defined as tooth retention with probing depths of less than 4 mm, no bleeding on probing, no exudation, and no evi-dence of root caries or fracture. The success rates overall for resected molars in these studies can be judged comparable to the success rates of implants in the same locations.
Case Selection CriteriaRoot resection (root amputation) and tooth resection (hemi-section) procedures are useful solutions for a variety of clini-cal problems. From a periodontal standpoint, the most common indication is significant periodontal bone loss local-ized to one root, with adequate bone support for the adjacent roots. Additional periodontal indications are grade II or III horizontal furcation involvement, dehiscence/fenestration, invasive resorption, and adverse root proximity.26,31,42 Although it is not within the scope of this text to provide a comprehensive discussion of periodontal diagnosis or surgical procedures, there are many clinical problems that require knowledge of both endodontic and periodontal disciplines to
*References 6, 8-13, 18, 21, 28, 31, 33, 37, and 46.
A
B
FIGuRE 18-18 a, Maxillary first molar with a vertical fracture in the mesial-buccal root. B, Following root amputation of the fractured root.
FIGuRE 18-19 Hemisected mandibular first molar restored with splinted crowns (bicuspidization).
CLINICAL PROBLEMProblem: A 58-year-old male presented for examination with palpation tenderness and dull pain in the area of the maxillary left first molar. A periapical radiograph indicated a large radiolucency over the apex of the mesial buccal root, suggesting periapical pathosis of pulpal origin, specifically associated with a necrotic pulp (Fig. 18-20, A). Pulp sensibility test responses, however, were normal, and periodontal probing indicated a loss of periodontal attachment over the mesial buccal root (see Fig. 18-20, B). Calculus was observed on the exposed root surface and could be felt with the peri-odontal probe subgingivally on the root surface.
Solution: Surgical exploration of the lesion confirmed bone loss of periodontal etiology (see Fig. 18-20, C). The mesial buccal root had no remaining bone support, and it was quite simple to resect (see Fig. 18-20, D). When vital root amputa-tions are dictated by the findings at surgery, a pulpectomy should be performed on the remaining roots immediately after the tissue is repositioned and sutured or as soon as pos-sible postoperatively.50

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 395
FIGuRE 18-20 a, Maxillary left first molar with a periapical lesion presumed to be of pulpal etiology. Sensibility tests indicated normal vitality. B, Probings confirmed a periodontal etiology. C, Surgical exposure showed complete bone loss around the mesial buccal root. D, Vital root resection. Pulpectomy followed immediately after completion of the surgery.
A B
FIGuRE 18-21 a, Mandibular first molar with a vertical fracture in the distal root. B, Post root resection. This is one of the most common endodontic indications for tooth resection.
arrive at the correct diagnosis and treatment plan. For example, it is not uncommon to identify a tooth with peri-radicular pathosis presumed to be of pulpal origin, only to identify instead that the lesion is of periodontal etiology and that the pulp is normally responsive to sensibility tests.
From an endodontic standpoint, problems for which root or tooth resection are options include: vertical root fractures (Fig. 18-21), coronal fractures (Fig. 18-22), furcation perfo-rations (Fig. 18-23), post perforations (Fig. 18-24), irrepa-rable strip perforations (Fig. 18-25), nonnegotiable root canals (Fig. 18-26), irretrievable separated instruments (Fig.
18-27), irremovable canal filling materials (Fig. 18-28), cervi-cal resorptions (Fig. 18-29), extensive caries (Fig. 18-30), and periodontal defects (Fig. 18-31). With creative endodontic treatment planning, retention of teeth and prostheses is both reasonable and feasible.
Endodontic Considerations Prior to Root ResectionWhile it is generally thought that root canal treatment is always indicated because of the pulp exposure at the
A B
C D

396 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
FIGuRE 18-23 Post perforation into furcation in a mandibular second molar. Note the periodontal defect in the furcation. The furcation had chronic purulent drainage. Removal of the mesial root would eliminate the furcation and prolong retention of the bridge.
A
B
FIGuRE 18-22 a, Significant coronal fracture of the palatal cusp of a maxillary first molar due to intense bruxism. B, Preoperative radiograph. Case is continued in Fig. 18-46.
A
B
FIGuRE 18-24 a, Distal lateral lesion associated with perforation from aberrant intraradicular post. The tooth was hemisected. B, Reevaluation radiograph of the restored mesial root after 3 years.
are necessary for healing and maintenance. Despite the results of these studies, complete root canal treatment still appears preferable on teeth with resected roots.
As described in the case presented in Fig. 18-20, the deci-sion to resect a root may not always be anticipated preopera-tively. In most cases, however, root or tooth resection can be treatment planned well in advance of the actual surgery. If the tooth requiring root removal does not have root canal treatment, it is usually more convenient do the treatment before surgery, for two important reasons. First, it is much more difficult to complete root canal treatment on the retained root postsurgically. Tooth isolation and canal man-agement are much easier with an intact crown. Second, the difficulty of root canal treatment cannot be determined pre-operatively in some cases. If treatment is done before the surgery and the canals prove to be difficult to penetrate, or if a procedural accident compromises the anticipated result, the treatment plan can be altered to extraction.
Although complete root canal treatment is not necessary in the root that will be removed, it is wise to seal the orifice permanently through the access cavity. The orifice should be enlarged more than would be necessary for routine cleaning and shaping procedures so that a permanent restorative mate-rial can be compacted past the point of amputation (Fig. 18-32). This procedure eliminates the need to place a
amputation site,43 some studies have reported successes without performing root canal treatment, or at most a pulp-capping procedure on the resected pulp stump.29,30 However, following any vital exposure, the prognosis for continued pulpal vitality is questionable to poor at best in mature per-manent teeth. Furthermore, exposed vital pulp in the surgical area can be a strong deterrent to oral hygiene measures that

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 397
A B
FIGuRE 18-26 a, Periapical and periodontal pathosis on a mandibular molar due to inadequate root canal treatment. Revision was initiated but the mesial canals proved impossible to renegotiate to the apical foramina. B, Hemisection retained the distal root as a terminal abutment for a removable partial denture. Treatment revision of this root was uncomplicated.
A B
C
FIGuRE 18-25 a, Maxillary first molar with a lesion associated with strip perforation on the buccal surface of the palatal root. B, Post hemisection radiograph. C, Photograph of the resected root showing the strip perforation.
A B
FIGuRE 18-27 a, Mandibular second molar with a separated instrument in one of two distal roots. B, The instrument was irretrievable; the root was resected, preserving the tooth in function.

A
C
B
FIGuRE 18-28 a, Symptomatic mandibular second molar requiring revision. The silver cones in the mesial canals proved to be irretrievable. B, The mesial root was resected. C, Reevaluation radiograph at 14 years, 7 months; the distal root continued to function as the distal abutment for a fixed bridge.
A
B
C
FIGuRE 18-29 a, Acute palatal abscess–associated cervical resorption. B, Surgical exposure. Lesion found to extend into the furcation on the mesial. C, Postoperative photograph of hemisection.
A B
FIGuRE 18-30 a, Distal caries to the furcation in a mandibular first molar. B, Resection of the distal root. Mesial root retained to be restored as a functional premolar, similar to Fig. 18-24, B.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 399
A B
FIGuRE 18-31 a, Mandibular central incisor with a periapical lesion suspected to be of pulpal origin. Probings revealed bone loss consistent with chronic periodontitis. B, Root was resected, preserving the fixed splint in function.
A B
FIGuRE 18-32 a, Completed root canal treatment of maxillary second molar. Note deep placement of amalgam in distal buccal root (arrow). B, Postoperative radiograph indicating root resection for periodontal reasons and preestablished amalgam seal of the orifice.
A B
FIGuRE 18-33 a, Immediately post root resection, indicating exposure of the orifice of the mesial buccal canal. B, Amalgam restoration of the exposed orifice to prevent coronal leakage.

400 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
FIGuRE 18-34 Furcation level at crestal bone.
FIGuRE 18-35 Furcation level above crestal bone.
FIGuRE 18-36 Furcation level well below crestal bone. Arrows indicate posthealing bone levels if mesial root were to be resected.
restoration in the external orifice at the time of resection (Fig. 18-33). These procedures are important to prevent coronal leakage into the retained roots.
If teeth indicated for root resection have already been root treated, preoperative evaluation of the root fillings in the roots to be retained is essential. Revision of previous root canal treatment should be done if there is any concern with the quality of the obturation or if there is evidence of periapi-cal or lateral pathosis. Furthermore, presurgical revision of the root canal treatment should be done in any roots with metal-core gutta-percha fillings or silver cone fillings because of the likely need for post space.
Periodontal Considerations Prior to Root ResectionThe level of supporting bone is of primary importance in assessing the periodontal condition of the root to be retained.2,17 Even with splinting, a root with only 5 mm of supporting bone must be considered unsuitable. A safe minimum would be 50% bone loss; that is, a crestal bone height no lower than half the distance from the cemental-enamel junction to the apex. There must also be a relatively uniform crestal bone height around the root and no localized deep periodontal defects.
Of equal significance is the level of the furcation bone relative to the level of crestal bone on both the mesial and distal aspects of the tooth.2,16 A favorable relationship would be a furcation height at the level of interproximal bone height (Fig. 18-34). Occasionally the furcation may even be above this level, as might be found in a tooth with bone loss from chronic periodontitis (Fig. 18-35).
Teeth with long root trunks and furcations 2 mm or more below the crestal bone are less suitable for resection. The bone level on the furcation side of the retained root can heal no higher than the furcation itself (Fig. 18-36). Root resec-tion would result in periodontal pocket formation postopera-tively on the furcation side of the root. For example, if the furcation level is 3 mm below crestal bone, the sulcus depth on the untreated surface of the retained root would be 2 mm. On the furcation surface, it would be 5 mm, which is clearly undesirable and difficult to maintain. This problem may be avoided in some cases with sufficient root length or by recon-touring the crestal bone circumferentially to make it level with the furcation. This approach should generally be limited to resection of teeth without immediate neighbors. Routine removal of large amounts of alveolar bone supporting adja-cent teeth is seldom indicated. Extrusion is another alterna-tive if the root is long enough (see Chapter 20).
Teeth with fused roots or roots with a C-shaped configura-tion (primarily mandibular second molars)27 are not suitable for resection (see Chapter 13). Although fusion of roots in maxillary molars does occur, it cannot be seen radiographi-cally,27 nor can the level of the furcation between the palatal root and the buccal roots be determined in this manner (Fig. 18-37). In cases where this problem is suspected, the patient

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 401
A
C
B
FIGuRE 18-37 a, Clinical photograph of a maxillary molar considered for resection of the palatal root. B, Radiograph suggesting a possible fused root anatomy. During surgery, the fusion of the distal buccal root with the palatal root was confirmed. The tooth was extracted. C, Lateral view of an extracted maxillary molar showing fusion of distal buccal and palatal roots. This tooth is not a candidate for either palatal or distal buccal root resection.
should be advised that extraction may be necessary if this anatomic variation is encountered. If the reason for resection is bone loss from a root perforation in a tooth with fused roots, an intentional replantation along with a root repair may be considered.41,47
FIGuRE 18-38 Drawing illustrating the little advantage of retaining a molar root if there are good bridge abutments adjacent to the problem tooth.
Restorative Considerations Before and After Root ResectionDuring the treatment planning process, the clinician must determine whether the resected tooth or root will be restor-able. In cases of minimal clinical crown height, crown length-ening at the time of root removal should be considered, and the adjacent teeth should also be considered in the treatment plan. It must be decided at the outset whether tooth resection would be superior to extraction of the involved tooth (Fig. 18-38). There is seldom an advantage to retaining a molar root if both adjacent teeth are suitable abutments for a fixed bridge or if an implant would be indicated. Although the remaining root could be retained, the additional choices of hemisection and root canal procedures add complexity, cost, and time to the treatment plan. The simplicity of extraction of the whole tooth and placement of a fixed bridge or implant must be considered and discussed with the patient. After resection, the final restoration of the root-resected tooth will depend significantly on the nature of the resection, the amount of remaining tooth structure, and the patient’s occlu-sion and periodontal status.1,3,4
Surgical Techniques for Root ResectionThe basic surgical procedure will be similar to crown length-ening in flap design, osseous contouring, closure, and post-operative periodontal objectives. However, in many cases a vertical releasing incision may be indicated.27 The surgical instruments are essentially the same as for the crown- lengthening procedure (see Chapter 20). Fig. 18-39 depicts the removal of the mesial buccal root from a maxillary first molar.
Initially, a horizontal sulcular incision is made both buc-cally and lingually (or palatally) at least one complete tooth width mesial and distal to the tooth that is to have a root removed (see Fig. 18-39, B). If the root intended to be ampu-tated is very short, it may be possible to use an envelope flap. If a vertical releasing incision is used, it should be placed to align with the interproximal space one tooth anterior to the

402 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
A B
C
F
G
I
E
D
H
FIGuRE 18-39 a, Maxillary right first molar with a vertical fracture in the mesial buccal root. B, Elevation of the flap. C, Reduction of exostosis. D, Removal of the buccal plate for eventual removal of the root. E, Sectioning of the root. F, Root removed. G, Radiograph to confirm complete resection. H, Recontouring of the crestal bone for optimal periodontal result. I, Flap closure.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 403
• Use a brush stroke with sufficient coolant when cutting root and bone.
• Identify the anatomy of the root junction in the furcation to protect the retained roots and furcation anatomy.
• Reduce occlusal tables prior to resection to better distribute the functional forces; if necessary, further refinement can be done after resection.
• Whenever in doubt, a surgical incision and tissue reflection permitting direct inspection will always enhance the procedure, especially in cases resected for perforative, resorptive, or carious damage in the furcation region.
• Surgical-length burs are essential; surgical handpieces with angled heads are desirable.
• Restore the pulp chamber with a bonded restoration (composite or core material) prior to resection if possible.
• Resect roots at the expense of the root to be removed, and avoid gouging the segments to be retained.
• Establish sufficient dentin and bone clearance as necessary for root removal.
• Use a splint if mobility of the retained segments is an issue.
Surgical Techniques for Tooth Resection (Hemisection)In mandibular molars, multiple approaches to tooth resection are available and are often dependent on the retention or removal of the resected segments. A vertical cut can be made continuously from the buccal to lingual. If there is through-and-through furcal bone loss, a silver cone or wire can be inserted to mark the furcation path. Movement of the metal-lic marker will indicate the depth of penetration. Cuts can also be made starting at the buccal to the tooth center and joined with a cut from the lingual furcation inward. A pre-contouring technique can also be used in which the segment(s) to be retained are prepared for restorative purposes with the internal proximal cut carried through the furcation (Fig. 18-40, A).22,34 This approach has the added advantage of reducing the amount of debris that may enter into the adja-cent root socket if a segment is prepared for a retainer prior to the removal of the other segments,27 and creates a prepara-tion for the immediate fabrication of a temporary prosthesis (see Fig. 18-40, C to E ).
The need for provisional splinting following tooth resec-tion must be determined for each case and is dependent on root position, occlusal function, and whether or not segments sectioned are retained or removed. Splinting after tooth resec-tion is more common than after root resection alone. Provi-sional splints can be constructed from wire and acrylic resin, wire and amalgam, orthodontic bands, acrylic resin, or the use of preexisting restorations.5,40 Centric occlusion contacts which prevent supra-eruption should be maintained, but lateral interferences should be eliminated.4 The final restora-tion of resected posterior teeth will often be in the form of single crowns or copings with telescopic crowns resembling premolars.32 Pontics are easily used in cases where a resected portion has been extracted. If proper adjunctive osseous
operated tooth and should include the papilla (see Fig. 18-39, B). Subsequently, the interproximal tissue is curetted, remov-ing any connective-tissue tags and identifying the precise location of the furcation. Using a surgical-length round bur, any exostosis or excessive thickness of the buccal plate is reduced (see Fig. 18-39, C ), and the buccal plate is removed over the root to be extracted (see Fig.18-39, D).
Using a surgical-length straight fissure or similar bur, begin the section on the root to be removed. Do not begin in the furcation, where danger of cutting into the surface of the retained tooth is great. It is always easier to remove more tooth structure after the bulk of the root has been resected and anatomic landmarks are clear (see Fig. 18-39, E ). Once the root has been completely severed from the retained tooth structure (verified radiographically and clinically), the segment to be removed is carefully extracted through the prepared opening in the buccal plate without elevating against the retained tooth (see Fig. 18-39, F ). If necessary, cut a trench in the bone mesial and distal to the root, using fine burs; stay as close as possible to the resected root to avoid cutting into the adjacent roots. Diamond burs, carbide fin-ishing burs, and polishing points can be used to shape the surface of the cut crown so that a smooth transition exists from the crown surface to the root surface. Verify radio-graphically that no fluting or overhanging spurs of furcation tooth structure are left protruding into the furcation (see Fig. 18-39, G ). If not already completed as a preoperative proce-dure, repair the canal opening at the site of the amputated root with a permanent filling as discussed earlier (see Fig. 18-33). Then compare the level of bone on the furcation side with the level of bone on the opposite side of the root. If there is a discrepancy in height, use a combination of a round bur, an end-cutting bur and the Wedelstadt chisel to level the bone height, as in the crown-lengthening technique. Interproximal bone on the buccal and lingual is ramped toward the interproximal space (see Fig. 18-39, H ). Wound closure and dressing are the same as described for the crown-lengthening procedure (see Fig. 18-39, I ).
For purposes of simplicity, only this one technique of resection will be presented. This approach is used primarily for maxillary molars, but it can be used in selective cases for mandibular molars. (See the case presentation in Fig. 18-51; in-depth details on this approach are available in other publications.)26,27
Basic Recommendations for All Root ResectionsWith all root resections, using any of the techniques to be described, there are some basic principles that will prevent problems both during and subsequent to the resective proce-dures. However, not all these concerns will apply to each and every clinical situation for which resective procedures are treatment planned.
• Use transillumination before and after resection to examine for crazes, cracks, or fractures.

404 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
in the access opening to the position of a line drawn from the buccal to lingual furcation. Zinc oxide eugenol (ZOE) is placed in the other half of the access opening. During sec-tioning, the coronal cut can be made along the amalgam/ZOE interface, always favoring the segment to be retained. Improper angulation of the handpiece or an excessive deep cut during sectioning may lead to gouging of the optimal root segment and ultimate loss of the entire tooth.27
The vertical cut technique has many advantages: direct visualization during resection, removal of potential occlusal problems when the root is to be removed, precise sectioning based on the tooth anatomy, and excellent access for the smoothing of resected tooth margins.49
In cases where both resected segments are to be retained (bicuspidization),19 the vertical cut technique allows for the creation of proper embrasures and, if necessary, orthodontic separation of the segments.1,3,22,23,40 This approach to reten-tion of all segments would be indicated in periodontal furca-tion management and in cases of furcation perforation where the horizontal osseous level is high and the furcation is
contouring and soft-tissue adaptation and healing have occurred, resected tooth margins are easily prepared for fixed prostheses. Many singular resected root segments can serve as viable abutments or as support for overdentures.1,38
The process and completeness of tooth resection in man-dibular molars should be verified radiographically and clini-cally. This is especially true with teeth exhibiting roots angled from the crown. However, radiographs must be exposed in the direct line of the cut to be diagnostic (Fig. 18-41, A to C ). If an elevator is used to determine segment freedom or mobility prior to radiographic demonstration of complete sectioning, fractures of valuable tooth structure to be retained may occur, compromising the ultimate restor-ative treatment.
In addition to the use of a silver cone or wire, a periodon-tal probe can be used to identify the path of tooth resection through the furcation, or placing different restorative materi-als in the endodontic access opening can provide a guide during the coronal cut (see Fig. 18-41, D).27 For example, on the half of the tooth to be retained, an amalgam is placed
A
CD
E
B
FIGuRE 18-40 a, Precontouring method of resection, with a bur cutting into the furcation area on the buccal and lingual to provide a guide for full resection. B, Two mandibular molars requiring hemisections due to furcation bone loss. C, Teeth have been resected. Segments to be retained are prepared for crown coverage prior to extraction of the other segments to prevent debris from going into the extraction sockets. D, Segments have been extracted. E, Immediate preparation and placement of temporary coronal restorations.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 405
coronally placed in the tooth. Initial root proximity must also be considered as well as root curvature.
Basic Recommendations for All Tooth ResectionsWith all root resections using any of the techniques to be described, there are some basic principles that will prevent problems both during and subsequent to the resective proce-dures. However, not all of these concerns will apply to each and every clinical situation for which resective procedures are treatment planned.
• Use transillumination before and after resection to examine for crazes, cracks, or fractures.
• Surgical tissue reflection may be necessary, therefore plan for such.
• Root curvatures may require bone removal.• Good visibility is essential at all times.• Expose radiographs in mandibular resections to
determine the thoroughness of the cut (see Fig. 18-41, A to C ).
• Ensure the resection is complete prior to root elevation and extraction.
• Use periodontal probes to ensure complete resection.• Verify furcation pathways with probes, wires, and
so forth (periodontal probes, endodontic files, or silver cones if available [see Fig. 18-41, D].
• Recontour and adjust occlusion prior to removal of the unwanted segment.
A
D
B
C
FIGuRE 18-41 a, Mandibular molar with significant bone loss on the mesial root is indicated for hemisection. The distal root is root treated and the orifice is filled with amalgam. B, Resection of the mesial root with preservation of bone on the mesial of the distal root. When cutting the tooth, avoid cutting the furcation bone and develop a smooth cut surface on the retained portion of the crown for proper restoration. C, Retained distal half of tooth with intact furcation bone. D, Use of silver cone to trace the pathway of the resective cut.
CLINICAL PROBLEMProblem: A 39-year-old female sought care for a draining sinus tract in the area of the mandibular right first molar. She had root canal treatment and a crown 1 year previously, and the sinus tract has been present for about 3 months. Clinical examination confirmed a draining tract that probes into the furcation of the first molar (Fig. 18-42, A). A radiograph (see Fig. 18-42, B) supported the differential diagnosis of a possible lateral canal or strip perforation.
Solution: The decision was made to attempt a surgical repair, but if the area was not accessible, to resect the tooth. The crown was removed and a full mucoperiosteal tissue flap, using a vertical releasing incision, was elevated on both buccal and lingual sides of the tooth. The location of the furcation was clear because of the drainage tract (see Fig. 18-42, C), but repair of the defect was not possible. Sectioning began over the distal root to avoid cutting into the distal side of the mesial root (see Fig. 18-42, D). The distal root had a strip per-foration resulting from a post preparation (see Fig. 18-42, E). Following removal of the distal root, the distal surface of the mesial root was recontoured vertically to the crest of the furcation, and the tissue was repositioned and stabilized with sutures (see Fig. 18-42, F). The mesial root was then restored with a premolar-sized crown. Fig. 18-42, G illustrates the restored mesial root in normal function after 1 year.

406 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
B
C D
F
G
E
A
FIGuRE 18-42 a, Sinus tract on the buccal of the mandibular first molar probing into the furcation. B, Radiograph demonstrating a furcation lesion. C, After flap elevation on both sides and curettage of the granulomatous tissue in the furcation, the location of the furcation and distal aspect of the mesial root are determined. D, Section is made through the crown over the distal root, avoiding the distal surface of the mesial root. E, Resected root showing the strip perforation. F, Flap closure. G, One-year reevaluation with crown restoration.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 407
Outcomes Assessment for Teeth With Root or Tooth Resection
Most root-resected teeth are able to function normally but are susceptible to the same influences that can negatively affect any root-treated tooth. Chapter 5 explored the param-eters of negative or questionable outcomes for nonsurgical root canal treatment. The quality of root canal treatment provided for teeth with resections is crucial to their long-term outcomes. In many cases, because of the unusual shape of the tooth and with cut margins positioned differently than those found with normal restorations, poor restorations will result in coronal leakage. The evaluation and alteration of the occlusal table and functional contacts, as already stressed earlier, are essential to prevent aberrantly placed forces on the altered tooth with the possibility of a resultant vertical frac-ture (see Chapter 6). The following discussion will assume that tooth anatomy and levels of furcation and crestal bone are suitable for resection. Although it is possible to remove roots from any multirooted tooth, practical experience has shown that case selection is critical to long-term success.
Maxillary Molar RootsMesial Buccal RootThe mesial buccal root may be the most frequently vertical-fractured root in maxillary molars. Following resection, peri-odontal maintenance may be more challenging because of the wide and deep interproximal space. Long-term prognosis is good, however, with careful attention to oral hygiene prac-tices (Fig. 18-43).
Distal Buccal RootPerhaps the most successful outcome for root resection is the removal of this root. Following resection, periodontal main-tenance is not typically a problem. This is especially true if the tooth is the last member of the arch (Fig. 18-44). The occlusion should be altered to ensure the repositioning of occlusal forces primarily over the palatal root; often the remaining mesial buccal root may be narrow and unable to withstand significant functional stresses.
Palatal RootA critical factor in evaluating the outcome of this treatment option is the sulcus depth on the palatal surface. The ana-tomic relationship of the palatal furcation to the level of surrounding bone usually cannot be determined preopera-tively. If a long root trunk should be discovered at surgery, the choice must be made between an unfavorable periodontal result or extraction. If the furcation is near crestal bone, the periodontal result will be optimal with a normal biologic width on the palatal surface (Fig. 18-45).
Resection of the palatal root, leaving the crown intact is indicated in but a few situations, one of which is economy
of treatment cost due to the retention of the existing crown. If chosen, there must be a significant altering of the occlusal table, with forces directed buccally (see Fig. 18-45, D). Con-tinued heavy occlusion on the palatal cusp in the long term tends to cause mobility and possible fracture.
Hemisection with removal of the palatal half is more preferable than palatal root resection. Fig. 18-46 documents the treatment of a maxillary first molar with palatal cusp fracture. The fracture depth made restoration impossible without removal of the palatal root. The furcation was at a level favorable for an optimal periodontal outcome. This approach has a more favorable long-term prognosis. The occlusal forces can be better managed with a narrower crown (Fig. 18-47).
Maxillary Premolars With Resection of the Buccal RootBecause of the relatively long root trunk, resections from crestal bone level are rarely if ever possible. Consequently, there are few indications for root resection on a premolar. Vertical fractures, periodontal defects, perforations, and resorption tend to involve the root trunk or both roots. One valid indication is to gain access to the furcation or to the palatal root. A postoperative radiograph of a maxillary first premolar with two roots is seen in Fig. 18-48, A. Root canal treatment was satisfactory but the patient returned 2 years later, and there was a lateral lesion present in the apical third
B
A
FIGuRE 18-43 a, A maxillary right first molar with a vertical fracture in the mesial buccal root. B, Fifteen-year reevaluation radiograph of the same molar continuing in normal function.

408 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
and removal of gutta-percha from one canal (see Fig. 18-48, B). The buccal root was resected, giving access to the palatal root (see Fig. 18-48, C ). The postsurgical radiograph is seen (see Fig. 18-48, D ) with two MTA root-end fillings.
Mandibular Molar RootsThere are two general applications for root/tooth resection in mandibular molars: the retention of existing prostheses
A B
C D
FIGuRE 18-44 a, Maxillary first molar with severe periodontal bone loss around the distal buccal root. B, Following root canal treatment. C, One-year reevaluation radiograph of the tooth after distal buccal root resection and restoration. D, Clinical photograph of the restoration. Note the crown is contoured to reflect the shape of a two-rooted tooth.
CLINICAL PROBLEMProblem: A 48-year-old female presented for evaluation of the maxillary left first premolar. She was experiencing local pain to palpation and dull, continuous pain. A diagnostic radiograph indi-cated that the tooth had root canal treatment and a porcelain veneer crown supported by a post and core (Fig. 18-49, A). On the distal, there was a 3- to 4-mm spherical radiolucency in the inter-proximal bone at the midroot level. Periodontal probings were normal. The diagnosis of lateral abscess of indeterminate origin was made.
Solution: Since the etiology of this lesion was unclear, explor-atory periradicular surgery was recommended. After the lesion was enucleated and the defect explored, it was clear that the etiology of the lesion originated from the furcation.
The presumptive diagnosis was furcation perforation from the intraradicular post space preparation. In order to access the fur-cation, the buccal root was resected. A perforation was observed on the buccal aspect of the palatal root at the level of the furca-tion. The defect was prepared and filled with MTA (see Fig. 18-49, B). One year later, the patient returned for reevaluation. The tooth had been comfortable and functional for the entire year until recently, when it became slightly mobile and tender to occlusal pressure. The reevaluation radiograph revealed a midroot fracture (see Fig. 18-49, C). The tooth was extracted. Although this is a rare case, it is reasonable to expect that a tooth with more robust root structure would have had a better long-term prognosis.
and the use of individual resected roots as abutments or as functional premolars. Root resection can be a compara-tively inexpensive approach to problem solving in the case of existing fixed bridges. Fig. 18-50 illustrates a case of severe periodontal bone loss around the distal root of the mandibular first molar. The long-term prognosis for the bridge appears poor, but the 1-year reevaluation indicates excellent healing and satisfactory function of the remaining mesial root.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 409
A
C
B1
E
D
B2
FIGuRE 18-45 a, Radiograph of a large resorption defect on the palatal surface of a maxillary first molar (arrow). B, Resection of the palatal root leaving the crown intact. This approach was chosen chiefly for economic reasons. C, Occlusal contact on the palatal cusp should be eliminated. D, One-year reexamination radiograph. Note the amalgam repair of the palatal canal orifice. E, Clinical photograph indicating excellent healing of the surgical site.
The most common indication for root resection in end-odontics is vertical root fracture (Fig. 18-51). Occlusal loading appears to be a major factor in their development. Once again, removal of the fractured root can preserve a bridge (Fig. 18-52), but the remaining root can be sus-ceptible to the same occlusal forces. It is vitally important to reduce the occlusion on any tooth with root resection, especially if there are signs of bruxism, such as large wear facets. Even with extensive occlusal modification at the time of resection, intense bruxism can ultimately cause fracture of the remaining root as well (see Fig. 18-52, C ). The prognosis for prostheses in which there has been root fracture is guarded, but here again, force distribution
is essential, along with proper maintenance of the periodontium.
Root resection on unsplinted mandibular molars may not be as successful as with maxillary molars, although this should not be a major deterrent in considering this option during treatment planning (Fig. 18-53). This is a relatively inexpen-sive approach to tooth retention and has a reasonably good prognosis if the tooth opposes a full denture or the occlusion is otherwise very light. If occlusal forces are heavy, especially on the unsupported half of the crown, fracture of the remain-ing root is likely (Fig. 18-54).
Hemisection is a much more predictable treatment plan for retention of an unsplinted molar. Generally, the value

410 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
A
E
B
C D
FIGuRE 18-46 a, Maxillary first molar with significant fracture of the palatal cusp due to bruxism. B, After palatal root resection. The midpalatal furcation level should be nearly equal to the level of interproximal crestal bone for optimal postoperative biological width. C, Three weeks posttreatment. D, Posttreatment radiograph of the same molar after palatal root resectional (see Fig. 18-22, B, which is the preoperative radiograph of this tooth). E, One-year reevaluation photograph of the molar, indicating normal palatal sulcus depth.
FIGuRE 18-47 Full crown on a resected maxillary first molar with the palatal root removed is narrower buccal lingually than a normal molar crown.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 411
A B
DC
FIGuRE 18-48 a, Postoperative radiograph indicating satisfactory root canal treatment. B, Two-year reevaluation radiograph indicating lateral lesion in the apical third and removal of gutta-percha from one canal. C, Resection of buccal root for access to palatal root. D, Postoperative surgical result with mineral trioxide aggregate root-end fillings.
B
C
A
FIGuRE 18-49 a, Preoperative radiograph of maxillary first premolar with lateral lesion due to furcation perforation from post preparation. B, Postoperative radiograph indicating resection of buccal root and repair of perforation with mineral trioxide aggregate. C, One-year reevaluation indicating root fracture that occurred under normal function. The tooth was extracted.

A B
C
FIGuRE 18-51 a, Vertical fracture of the mesial root of the mandibular first molar was confirmed by surgical exploration. This is unusual in a tooth without previous root canal treatment. B, Completed treatment in the distal root; note the two canals. C, Reexamination radiograph 9 months. Patient is symptom free, and tooth/bridge is functional.
BA
C
FIGuRE 18-50 a, Surgical exposure of a mandibular first molar with severe periodontal bone loss around the entire distal root. B, Immediate postoperative radiograph indicating resection of distal root. Prognosis is guarded for tooth and prosthesis because of minimal bone support. C, One-year posttreatment reevaluation indicating complete healing of original lesion. The bridge is in normal function, and the prognosis is greatly improved.

A B
C
FIGuRE 18-52 a, Mandibular left first molar with vertical fracture of the distal root. The entire bridge was in heavy occlusion. Occlusal reduction of wear facets was done at the time of surgery. B, One-year post root resection, radiograph shows complete healing of the operative site. The bridge was in normal function. C, Three-year reevaluation radiograph shows vertical fracture of the mesial root. The tooth and pontic were extracted.
A B
FIGuRE 18-53 a, Resection of a mesial root of a mandibular molar. B, Tooth was not splinted, but occlusal forces were minimal on the mesial of the tooth. Reexamination at 12 months indicates complete healing. The tooth was in normal, if light, function.
FIGuRE 18-54 a, Immediate postoperative radiograph of root resection of the distal root of a mandibular second molar due to vertical root fracture. B, Reevaluation radiograph at 1 12 years shows vertical fracture of the mesial root; the tooth was extracted. Hemisection would have been a better original solution.
A B

414 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
CLINICAL PROBLEMProblem: An 82-year-old male presented with extensive caries under the distal half of a full gold crown on the man-dibular left first molar (see Fig. 18-56, A). Cost of treatment was a major concern. He had no plans to have bridges placed in several areas with missing teeth. It was noted that the molar in question occluded only with the maxillary second premolar (see Fig. 18-56, B). The crown was removed, and the caries was excavated, confirming that the caries extended into the furca-tion, and the tooth was unrestorable (see Fig. 18-56, C).
Solution: Noting that the mesial half of the tooth was in excellent condition and that it occluded directly with the second premolar, hemisection was completed, removing the distal root (see Fig. 18-56, D). Root canal treatment was done on the mesial root during the same visit (see Fig. 18-56, E). Following a period of healing, the mesial root was restored as a functional premolar. This plan preserved the tooth in the same function as it had preoperatively at a far lower cost than any prosthetic alternative.
of retaining of either root of a mandibular molar is ques-tionable if there are potential bridge abutments on both sides (see Fig. 18-38), but there can be exceptions. Possibly the most useful application of hemisection in mandibular molars is for terminal teeth in the arch. A mesial root of either the first or second molar in contact with the neighbor can function quite well as a third premolar, as depicted in Fig. 18-55. Fig. 18-56 documents a very useful conversion of a molar tooth with extensive caries into a functional premolar.
Retention of the distal root will require splinting or a small bridge to the adjacent tooth. This treatment plan will serve
the patient well, with a retained functional tooth having a very good prognosis (Fig. 18-57).
With the techniques described to manage problems encountered in osseous and root defects below the attach-ment of the periodontal ligament, many but not all teeth with various problems can be successfully retained in full function and without patient symptoms.26,27 Further-more, prostheses that are in place and functional can be maintained as opposed to dismantling and rebuilding when not necessary.25
Recent retrospective studies attempt to dispute the value of mandibular molar resections in favor of implants.51 The level of evidence for this claim is less than ideal (non- prospective, non-randomized, retrospective, mixed data on the causes for failure with 12 patients out of 56 having non-resective failures [21%], small “n” size study) versus a con-temporary prospective study with a large “n” size, a highly controlled population, and a 10-year reexamination period that showed in excess of 93% success with the resective treat-ments (site-specific differences on the two studies).12 It is obviously difficult in these situations to make claims of supe-riority with one technique or the other unless careful treat-ment planning and treatment execution are at their highest levels.
The major challenges are to recognize these alternative possibilities during the treatment-planning phase and to either have the expertise to manage these challenges or refer the patient to someone who can. These approaches to tooth retention are reasonable, cost effective, and successful and will provide an excellent service for many patients who cannot afford or who do not desire tooth removal and replacement with fixed prostheses. Success rates for root/tooth resection are quite high based on the studies, but do also require commitment on the part of the patient to prac-tice excellent home oral physiotherapy daily.
FIGuRE 18-55 a, Radiograph of mandibular molar that has had mesial roots treated; the distal root was not treated fully, since it will be resected (tooth hemisection) due to the large bony defect and evidence of a fracture. This approach to treatment is generally intended to be a short-term solution. B, Reevaluation radiograph at 2 1
2 years, indicating complete healing of the surgical site. The tooth was in normal function against natural teeth.
BA

E
A
C
B
D
FIGuRE 18-56 a, Mandibular first molar with extensive caries in the distal half of the clinical crown. B, Occlusal relationship with opposing second premolar. C, After excavation, indicating unrestorability of the distal half. D, Posttreatment radiograph indicating resection of distal root and root canal treatment of mesial root. E, Functional relationship of retained mesial half with the opposing premolar.
A B
C
FIGuRE 18-57 a, Mandibular second molar bridge abutment with advanced chronic periodontitis. The osseous defect on the mesial root is not amenable to pocket elimination surgery. Hemisection was elected as the treatment of choice. B, Completed hemisection and root canal treatment. C, A reevaluation radiograph made 24 years later. The bridge is in normal function against natural teeth.

416 chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention
REfEREnCES1. Abrams L, Trachtenberg DI: Hemisection—technique and restora-
tion, Dent Clin North Am 18:415-444, 1974.2. Ammons WF, Jr, Harrington GW: Furcation: involvement and
treatment. In Carranza’s clinical periodontology, ed 10, St. Louis, 2006, Saunders-Elsevier, pp 991-1004.
3. Appleton IE: Restoration of root-resected teeth, J Prosthet Dent 44:150-153, 1980.
4. Baima RF: Considerations for furcation treatment. Part III. Restor-ative therapy, J Prosthet Dent 58:145-147, 1987.
5. Basaraba N: Root amputation and tooth hemisection, Dent Clin North Am 13:121-132, 1969.
6. Basten CH, Ammons WF, Persson R: Long-term evaluation of root-resected molars: a retrospective study, Int J Periodontics Restorative Dent 16:206-219, 1996.
7. Bergenholtz A: Radectomy of multirooted teeth, J Am Dent Assoc 85:870-875, 1972.
8. Blomlöf L, Jansson L, Appelgren R, et al: Prognosis and mortality of root resected molars, Int J Periodontics Restorative Dent 17(2):190-201, 1997.
9. Borio PS, Pessoli M, Mina M: L’uso di elementi rizectomizzati come pilastri di protesi. Considerazioni su 40 casi, Minerva Sto-matol 33:495-502, 1984.
10. Bühler H: Survival rates of hemisected teeth: an attempt to compare them with survival rates of alloplastic implants, Int J Periodontics Restorative Dent 14(6):536-543, 1994.
11. Carnevale G, DiFebo G, Tonelli MP, et al: A retrospective analysis of the periodontal-prosthetic treatment of molars with interradicu-lar lesions, Int J Periodontics Restorative Dent 11(3):189-205, 1991.
12. Carnevale G, Pontoriero R, diFebo G: Long-term effects of root-resective therapy in furcation-involved molars. A 10-year longitu-dinal study, J Clin Periodontol 25:209-214, 1998.
13. Carnevale G, Pontoriero R, Hürzeler MB: Management of furca-tion involvement, Periodontol 2000 9:69-89, 1995.
14. Cohn SA: Treatment choices for negative outcomes with non-surgical root canal treatment: non-surgical retreatment vs. surgical retreatment vs. implants, Endod Topics 11:4-24, 2005.
15. DeDeus QD: Frequency, location and direction of the lateral, secondary and accessory canals, J Endod 1:361-366, 1975.
16. DeSanctis M, Murphy KG: The role of resective periodontal surgery in the treatment of furcation defects, Periodontol 2000 22:154-168, 2000.
17. Eastman JR, Backmeyer J: A review of the periodontal, endodon-tic, and prosthetic considerations in odontogenous resection pro-cedures, Int J Periodontol Rest Dent 6(2):34-57, 1986.
18. Erpenstein H: A 3-year study of hemisected molars, J Clin Peri-odontol 10:1-10, 1983.
19. Farley JR: Hemisection and bicuspidization of molars, Tex Dent J 92(6):4-5, 1974.
20. Fournier DF: Odontic trisection: an alternative therapy, J Prosthet Dent 57:397-400, 1987.
21. Fugassotto PA: A comparison of the success of root resected molars and molar position implants in function in a private prac-tice: results of up to 15-plus years, J Periodontol 72:1113-1123, 2001.
22. Gerstein H: Surgical endodontics. In Laskin DN, editor: Oral and maxillofacial surgery, Volume II, St. Louis, 1985, The CV Mosby Co.
23. Grant DA, Stern IB, Listgarten MA: Periodontics in the tradition of Gottlieb and Orban, St. Louis, 1988, The CV Mosby Co.
24. Greenstein G, Caton J, Polson A: Trisection of maxillary molars: a clinical technique, Compend Contin Educ Dent 5:624-626, 631-632, 1984.
25. Gutmann JL: Treatment planning & management of fixed pros-theses supported by vertically fractured roots, Roots 3(3):30-36, 2007.
26. Gutmann JL: Perspectives on the use of root/tooth resections in the retention of teeth, ENDO (Lond Engl) 1:239-255, 2007.
27. Gutmann JL, Harrison JW: Surgical endodontics, Boston, 1991, Blackwell Scientific Publications, pp 420-439.
28. Hamp S-E, Nyman S, Lindhe J: Periodontal treatment of multi-rooted teeth. Results after 5 years, J Clin Periodontol 2:126-135, 1975.
29. Haskell EW: Vital root resection, Oral Surg Oral Med Oral Pathol 27:266-274, 1969.
30. Haskell EW, Stanley HR: A review of vital root resection, Int J Periodontics Restorative Dent 2:29-49, 1982.
31. Hempton T, Leone C: A review of root resective therapy as a treatment potion for maxillary molars, J Am Dent Assoc 128:449-455, 1997.
32. Hou GL, Tsai CC, Weisgold AS: Treatment of molar furcation involvement using root separation and a crown and sleeve-coping telescopic denture. A longitudinal study, J Periodontol 70:1098-1109, 1999.
33. Klavan B: Clinical observations following root amputation in max-illary molar teeth, J Periodontol 46:1-5, 1975.
34. Kirchoff DA, Gerstein H: Presurgical crown contouring for root amputation procedures, Oral Surg 27:379-384, 1969.
35. Kurtzman GM, Silverstein LH, Shatz PC: Hemisection as an alter-native treatment for vertically fractured mandibular molars, Compend Contin Educ Dent 27:126-129, 2006.
36. Kuttler S, McLean A, Dorn S, et al: The impact of post space preparation with Gates-Glidden drills on residual dentin thickness in distal roots of mandibular molars, J Am Dent Assoc 135:903-909, 2004.
37. Langer B, Stein SD, Wagenberg B: An evaluation of root resec-tions: a ten-year study, J Periodontol 52:719-722, 1981.
38. Richard GE, Sarka RJ, Arnold REM, et al: Hemisected molars for additional overdenture support, J Prosthet Dent 38:16-21, 1977
39. Ricucci D, Langeland K: Apical limit of root canal instrumentation and obturation, part 2. A histological study, Int Endod J 31:394-409, 1998.
40. Rosen H, Gitnick PJ: Separation and splinting of the roots of multirooted teeth, J Prosthet Dent; 21:34-38, 1969.
41. Shuman IE: Repair of a root perforation with a resin-ionomer using an intentional replantation technique, Gen Dent 47:392-395, 1999.
42. Smidt A, Nuni E, Keinan D: Invasive cervical root resorption: treatment rationale with an interdisciplinary approach, J Endod 33:1383-1387, 2007.
43. Smukler H, Tagger M: Vital root amputation. A clinical and his-tological study, J Periodontol 47:324-330, 1976.
44. Stropko JJ, Doyon GE, Gutmann JL: Root-end management: resection, cavity preparation, and material placement, Endod Topics 11:131-151, 2005.
45. Spångberg LSW, Haapasalo M: Rationale and efficacy of root canal medicaments and root filling materials with emphasis on treatment outcome, Endod Topics 2:35-58, 2002.
46. Svärdström G, Wennström JL: Periodontal treatment decisions for molars: an analysis of influencing factors and long-term outcome, J Periodontol 71:579-585, 2000.

chapter 18 | Problem-Solving Challenges That Require Periradicular Surgical Intervention 417
47. Tsesis I, Fuss Z: Diagnosis and treatment of accidental root perfo-rations, Endod Topics 13:95-107, 2006.
48. Weine FS: The enigma of the lateral canal, Dent Clin North Am 28:833-852, 1984.
49. Weine FS: Endodontic therapy, ed 4, St Louis, 1989, The CV Mosby Co.
50. Weine FS, Hoag PM, Healey HJ: Endodontic emergency treat-ment following root amputation in periodontally involved teeth, J Periodontol 41:391-393, 1970.
51. Zafiropoulos G-G, Hoffmann O, Kasaj A, et al: Mandibular molar resection versus implant therapy: a retrospective nonrandomized study, J Oral Implantol 35(2): 52-62, 2009.
RECoMMEnDED ADDiTionAl READinGBergenholtz G (Guest Editor): Interactions between pulpal and perio-
dontal disease conditions, Endod Topics 13:1-122, 2006.Dibart S: Practical advanced periodontal surgery, Oxford, 2007, Black-
well Munksgaard.Fugazzotto P: Decision making: the furcated molar, J Implant Advan
Clin Dent 2:63-87, 2010.Merino EM: Endodontic Microsurgery, London, 2009, Quintessence
Publishing Co. Ltd.

418
part 4 Problem-Solving Issues in Adjunctive Dental Procedures
Chapter 19
Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
Problem-Solving ListProblem-solving issues and challenges in the management of traumatic tooth injuries addressed in this chapter are:
Tooth Crazes, Cracks, and Fractures
Traumatic Tooth Injuries
Concussion
Subluxation
Extrusive luxation
Lateral luxation
Intrusive luxation
Sequelae to Luxation Injuries
Pulp canal obliteration
Marginal bone loss
Coronal discoloration
Transient apical breakdown
Pulpal necrosis
Avulsion Injuries
Resorption Associated With Traumatic Tooth Injuries
Inflammatory replacement resorption and ankylosis
Horizontal Root Fractures
Apical-third fractures
Middle-third fractures
Coronal-third fractures
Healing Responses to Horizontally Fractured Teeth
Calcified union between the segments
Bone and connective-tissue healing
Connective-tissue or soft-tissue union
Failure of fracture to heal
Splinting of Traumatized Teeth
When a Tooth is loosened by violence, but not moved out its socket, ligature alone, and astringent washes to brace the gums, are sufficient for the cure. In this case the pain ceases with the looseness of the Teeth; but if it be violent in the beginning, sedatives must be applied.11
T.G. Berdmore, 1768
Tooth Crazes, Cracks, and Fractures
The diagnosis and management of structural defects in teeth other than those caused by accidental trauma pose a unique challenge for the clinician. These defects involve posterior teeth and are usually slow to develop and manifest themselves within a variety of intertwined variables. They can be on the surface and stable, or they can migrate into the tooth, result-ing in significant structural defects and clinical challenges. All defects may involve the crown, root, or both, in addition to being horizontal, vertical, or angulated.
The types of alterations in tooth structure include crazes, cracks, and fractures. Diagnosis, management, and preven-tion of these alterations is dependent on thorough patient assessment, identification of those factors that contribute to these defects, management of those factors when possible by the clinician, and creative measures in the overall prevention of these problems. Fractures that are the result of accidental trauma and that occur primarily in the anterior teeth are addressed in the next section of this chapter.
For purposes of clarification and clinical differentiation, the following descriptions are provided. Crazes are areas of

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 419
A B
C
D
FIGUre 19-2 A, Image shows a symptomatic molar that was excavated and stained with methylene blue on the cavity floor. Note the mesial-to-distal fracture. B, Evidence of a fracture on the distal marginal ridge often results from weakened tooth structure in that area. C, Extracted tooth shows the crack (arrows) running apically down the root in a diagonal manner. Also the periodontal ligament forms a tract as the crack is propagated. Note the lack of divergence in the occlusal preparation that is necessary for seating inlays. This was probably the contributing factor in this tooth’s demise. d, After access opening, the distal fracture line can be seen to run down the distal wall. The tooth was extracted.
weakness in the tooth structure where further propagation may result in a crack or facture. These are not visible radiographically but can be seen with fiberoptic transil-lumination. Cracks are definite breaks in the continuity of the tooth structure beginning in the enamel or cementum. No separation is evident clinically, and these are visible
BA
FIGUre 19-1 A, Mandibular molar with crack lines on the mesial and marginal ridges (arrows). B, Mandibular molar with a crack running parallel to the buccal developmental groove (arrows).
with fiberoptic transillumination in which light transmission is impeded across the crack line. They may often be stained due to patient diet. Fractures exhibit definite separation of the tooth structure into two or more distinct segments and are visible clinically and sometimes radiographically. They also may exhibit stain when located coronally.

420 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
Many factors that predispose to these tooth defects cannot be altered or controlled by the clinician. These include masticatory accidents, bruxism, and thermal cycling.31,34 Clinical detection of these defects can be exceedingly dif-ficult, especially in their initial stages of development or beneath extensive restorations. Additionally, radiographs are of little value in these initial stages. In some cases, surgical intervention may actually be necessary for fracture identi-fication. Patient symptoms may mimic many other possible diagnoses, such as temporomandibular disease, sinus prob-lems, vague headaches, and ear pain. Efficacious management of fractured teeth is highly dependent on a complete set of variables that are often not controllable by the practitioner, such as extent and size of the defect, tooth and root anatomy,
position of fracture, masticatory function, and previous dental intervention.
There is a paucity of new information regarding these types of tooth defects, and therefore the reader is referred to previous editions of this text and other supportive references that will detail the challenges of the clinician faces with these types of problems.14-16,26,28,31,35 However, in the series of figures (Figs. 19-1 to 19-5), the main concepts will be high-lighted for reader reference and clinical recognition. This will help differentiate these defects from those found with acci-dental trauma. The reader is referred to early chapters in this text that discuss many aspects of these structural defects rela-tive to identification and management (see Chapters 1 to 5, 15, and 18).
A B
C
D
FIGUre 19-3 Open anterior bites (A) and cross bites (B) contribute to excessive occlusal forces on the posterior teeth. C, Placement of multiple pins in a tooth for retention may lead to fractures. Note the fractures at the base of this pin (scanning electron microscopy photo). d, Traceable sinus tract to the midroot of this premolar. Note the size and shape of the intraradicular post. The tooth was fractured vertically.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 421
FIGUre 19-5 Proximal view of the extracted tooth; note the oblique fracture line. Clinical view in Fig. 19-4, A.
The first and most important step in understanding how to treat these injuries is to determine the nature of trauma.16 This chapter will provide fundamental concepts in diagnos-ing and treating traumatic injuries of the more severe nature in the permanent dentition. It will also address the more common sequelae of traumatic injuries and the most appro-priate methods to manage them effectively for the best outcome. Trauma ranging from luxation injuries and avul-sions to horizontal root fractures will be covered in a clinically relevant manner.
Active prevention of coronal fractures in normal day-to-day living is unrealistic and a moot point. Prevention during hazardous activities such as job-related activities (e.g., during sports), however, may occur in the form of mouth protection and on-the-job training to avoid circumstances that may pre-dispose to traumatic incidents.25 Although such incidents are uncommon, the major result of these types of fractures is dental trauma, whether direct or indirect; accidental injuries remain the predominant type reported. This implies that management of the crown fracture will usually fall into the category of a dental emergency, and principles cited in Chap-ters 1, 4, and 15—diagnosis, treatment planning, anesthesia, analgesics, and antibiotics—should be integrated into the total case management.
In cases in which an acute trauma accident has resulted in a crown fracture (Fig. 19-6), pulpal preservation is crucial when root formation is incomplete (see Chapter 7). Teeth with coronal and coronal-root fractures and completed root development can and should be retained, even if adjunctive treatment is indicated. The range of management may be limited to dentin protection and a bonded restoration to a root canal procedure and, in some cases, root extrusion, crown lengthening, a post, a core buildup, or acid-etched bonded core and crown (Figs. 19-7 and 19-8).
Traumatic Tooth InjuriesThe management of traumatic injuries is a constant source of difficulty for the clinician because of the complexity in diagnosing and treating these injuries properly.4 The most important concept of managing dental trauma is to feel con-fident in the diagnosis. By knowing the type of damage that has occurred to the dentition and supporting tissues, the clinician will be better suited to treat the affected tooth or teeth and the sequelae of these types of injuries. In the present litigious society, every clinician should know the proper guidelines for treatment of traumatized teeth to avoid the potential risk of litigation.2-4,23,24
A B C
FIGUre 19-4 A, Placement of a fiberoptic on a symptomatic maxillary premolar. Note that the light does not pass the fracture line. Transillumination can be more dramatic without the overhead light. B, Clinically deep probing in a narrow channel. C, Tissue reflection allows for visualization of the fracture (arrows).

422 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
FIGUre 19-6 Enamel-dentin fractures, with the right central incisor having an angled fracture into the coronal portion of the root.
B
A
FIGUre 19-7 A, Complicated coronal fractures that are deep into the dentin with an exposed pulp. B, Clinical view.
FIGUre 19-8 Complete coronal fracture that lends itself to immediate and complete root canal treatment and appropriate restorative procedures. However, because the patient is young, a prefabricated metallic post may not be indicated, but rather a bonded type of carbon fiber post may be better.
Luxation injuries present a greater demand for the clini-cian in their management, as they must be diagnosed accu-rately.2-4,17,22,23 The following are the more commonly accepted definitions of luxation injuries, arranged (in order of damage to the tooth and surrounding tissues) from the least severe to the most destructive type. A luxation is defined as a disloca-tion of the tooth from its normal physiologic position in the socket. However, as will be seen in the specific descriptions of these injuries, a large variety of luxation injuries exist, so a number of different classifications have been suggested.4
ConcussionA concussion injury is defined as a relatively minor blow to the tooth in which the affected tooth is not damaged, but the periodontium becomes inflamed. Typically, patients experience mastication sensitivity or pain on brushing or pressure on the tooth. No splinting is required in these types of luxation, and only palliative treatment is required. In most instances, reducing the occlusion is all that is required. Patients should be reevaluated within the first 2 weeks after the injury to ensure that no further treatment is required. In the vast majority of cases, root canal therapy is not indicated, because only a small percentage of these injuries become necrotic. Monitoring pulpal status for 1 year is recommended (Fig. 19-9).23
SubluxationA subluxation is slightly more severe than a concussion of the tooth, because increased mobility exists that is comparable with a periodontally involved tooth (mobility +1 to +2).4,23 Although the tooth is more mobile than it was before the injury, it is at the discretion of the clinician to determine whether splinting is required. In most instances, no splint is required unless additional trauma to the tooth or the area is

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 423
A
B
FIGUre 19-10 A, Subluxated tooth with the typical clinical presentation of a bleeding epithelial attachment apparatus. B, 30 months after a subluxation injury, radiograph shows ankylosis in the midroot portion. The patient is symptom free.
FIGUre 19-11 An extrusively luxated central incisor. Note that the tooth is dislocated along its long axis.
anticipated (e.g., young patient involved in multiple sports). If splinted, stabilization up to 2 weeks is usually indicated.23 Pulp sensibility responses are usually variable and should be monitored until a definite pulpal diagnosis can be made.
Reduction of the occlusal forces on the tooth will aid in the healing process and minimize the patient’s symptoms. Subluxations account for the most frequent type of luxation injury, although the probability of pulpal necrosis zis very small with subluxation injuries.4 Clinically it is common to see hemorrhage around the epithelial attach-ment (Fig. 19-10).
Extrusive LuxationIn extrusive luxation injuries, the tooth is dislocated along its long axis and can be displaced almost entirely out of the socket (Fig. 19-11). These injuries are significantly more severe than either concussion or subluxation injuries. Radio-graphically there may be an increased periodontal ligament space apically. Extrusive luxation injuries account for only 1% of total traumatic dental injuries. Although the use of anesthesia is not always required when dealing with younger patients, it is strongly recommended.
Initially the soft-tissue damage must be assessed and managed properly. The tooth is carefully and accurately repo-sitioned in the socket. This procedure may be performed manually with gauze or with forceps (if significant dislocation has occurred) to replace the tooth gently into its original position. Keep in mind that teeth will usually realign into their original position in the socket without significant forces being required. However, the greater the post-trauma time period before treatment, the higher the likelihood of coagula-tion in the socket; therefore additional force may be required to accomplish the repositioning.
Sensibility testing is used initially, with variable or no responses expected, and again on reexamination to determine the pulpal status. This is especially important in teeth with
FIGUre 19-9 History of a concussion injury on the right central incisor with no signs or symptoms at the time of injury. Six-month reexamination shows a darkened tooth that does not respond to sensibility testing.
immature root formation. If there is no response in the tooth with a fully formed apex, necrosis can be assumed to have occurred.22,23
In extrusive luxation injuries, the neurovascular bundle is usually disrupted, and therefore the blood supply is lost to the tooth. In adult patients and in young patients with

424 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
Because of the nature of the damage with lateral luxation injuries, the probability of pulpal damage and subsequent endodontic therapy is high.4,18,22,32 As with all luxation inju-ries, the older the patient (i.e., the smaller the diameter of the apical foramen), the less likely the tooth will regain its vascular supply; therefore a root canal procedure will be necessary. With both lateral and extrusive luxation injuries, external resorption (ER) or internal resorption (IR) is not a typical sequela; the patient should be informed that the long-term prognosis of these teeth is excellent.
Intrusive LuxationIntrusive luxation injuries are the most severe type of luxation injury and therefore have the poorest prognosis.2-4,7-9,30,33 With intrusive luxation injuries, the tooth is dislocated api-cally into the alveolar socket. The tooth is sometimes dis-placed so far apically that the clinician may not be able to visualize the incisal edge. There is seldom any observable mobility because of its new position deep within the alveolar bone. These injuries cause severe damage to the neurovascu-lar bundle, pulp, and periodontium.18 The blood supply and neurovascular tissues are crushed completely. In teeth with partially to completely closed apices, the pulpal prognosis is extremely poor, with almost a 100% probability of pulpal necrosis. Because of the severe damage to the periodontium,
closed apices, the likelihood of revascularization is extremely low and should not be considered a likely consequence of the healing process. Because the majority of these cases become necrotic, the patient should be notified that a root canal procedure will be necessary within a couple of weeks of the trauma or earlier at the time of splint removal. In all cases of extrusive luxation injuries, the teeth must be splinted.12
All luxation injuries require splints, using one nontrau-matized tooth on either side of the traumatized tooth. For example, if only one tooth is luxated, then one healthy tooth on either side of the traumatized tooth should be included in the splint. If two teeth are luxated, then a total of six teeth should be included in the splint (two teeth on either side of the two teeth that are traumatized for a total of six). The type of splint (physiologic, rigid, or passive) is incon-sequential to the healing process. However, in most instances, a nonrigid splint is easier to place and will avoid the possibil-ity of exerting excessive pressure on the damaged periodontal ligament.37
The splint should be placed for up to 2 weeks. During this period, the periodontium will stabilize the tooth sufficiently, and minor to normal mobility will be noted fol-lowing splint removal. Should the tooth be excessively mobile compared with a nontraumatized contralateral tooth, the splint may remain in place until normal mobility is noted. The use of a physiologic passive or flexible splint is indicated for any type of luxation injury.4,37 Most clinicians can use a composite-based splint, because it is the most convenient to use and place on the traumatized teeth. Should the splint remain in place for longer periods of time, no negative sequelae will result. Non-rigid splinting does not cause damage to the supporting tissues or to the tooth.
Lateral LuxationLateral luxation injuries are defined as a dislocation of the tooth in a mesial, distal, facial, or lingual (palatal) direction, with comminution or fracture of the bony alveolar socket. It is rare for a patient to have a pure lateral luxation. Most cases will have both a lateral and an extrusive component (Fig. 19-12). Lateral luxation injuries are considered more severe than extrusive luxation injuries because of the associated frac-ture or splintering of the bone in the alveolar socket.22
The assessment phase is similar to that for extrusive inju-ries. In these instances, a blunt instrument should be inserted gently into the alveolar socket to move the fractured bony segment back to its original position before the tooth can be properly repositioned.4,23 Care should be exercised to prevent damage to the healthy periodontium remaining in the socket or on the tooth. Once the tooth is repositioned, a splint should be placed to hold the traumatized tooth (or teeth) in position for 10 to 14 days. If bony fracture is noted, the splint should remain in place for 6 to 8 weeks to allow proper healing of the alveolar socket. Whenever bone is fractured, a more rigid splint should be placed in lieu of a flexible or physiologic splint.
B
A
FIGUre 19-12 A, Lateral luxation injury. Note the lateral and extrusive component to the injury. B, Significant lateral extrusion of the mandibular incisors. Note the radiographic view and the movement in the alveolar socket.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 425
A B
FIGUre 19-13 A, Radiographic appearance of an intrusively luxated tooth. B, During reeruption, resorption is evident.
the probability of ER is extremely high in these injuries; therefore the patient should be warned that the prognosis of an intrusively luxated tooth is guarded.
Clinically, the tooth is usually immobile and gives a high metallic sound similar to what would be found in ankylosis. Sensibility tests will probably be negative. In teeth with immature root formation, pulpal revascularization may occur (see Chapter 13).
Unfortunately, the proper treatment of intrusive luxation injuries remains a mystery, because numerous clinical research articles with various treatment protocols have led to conflict-ing results. Current philosophy of management includes the following. Teeth with incomplete root formation should be allowed to reposition spontaneously. If no movement is noted within 3 weeks, rapid orthodontic extrusion is recom-mended.7-9,23 Teeth with complete root formation should be repositioned as soon as possible. The pulp will probably be necrotic and root canal procedures indicated using calcium hydroxide (Ca[OH]2) as a temporary dressing. Appropriate treatment regimens are based on severity of the injury, age of the patient, status of the root development, and time subse-quent to injury.7-9 Patients should be informed in a compas-sionate manner of the extremely poor prognosis associated with these injuries.
In some cases, the ideal treatment is to allow the teeth to erupt passively on their own. This treatment modality appears to be better suited for patients who are young with minimal intrusion. Teeth that are actively repositioned with forceps, without the use of a surgical flap, have also been successful. However, several authors suggest that the ideal treatment for
intrusively luxated teeth is a function of the degree of damage and the age of the patient.
If the teeth do not or are not allowed to re-erupt into their normal physiologic position in the arch (Fig. 19-13), then a high probability exists that the intruded teeth will undergo inflammatory replacement resorption (IRR). This type of resorption is also mistakenly called ankylosis; however, replace-ment resorption is the active process of tooth destruction, and replacement with bone ankylosis is the result of this process.
Because of the severe damage to the periodontium in an intrusive luxation injury, the traumatized tooth will often begin to resorb, although the process is chronic in nature, taking months or years to eventually destroy the affected tooth. The tooth is literally locked into position and cannot be moved orthodontically or manually with forceps. If an extraction is attempted, the bone surrounding the tooth will often be extracted along with the tooth. Unless the apices are wide open and the tooth spontaneously re-erupts, root canal treatment should commence as soon as possible after the tooth is stabilized.
Because the pulps in the vast majority of these teeth become necrotic shortly after the injury, root canal treatment is indicated in 100% of the cases if the apices are closed. The only exception is whether the tooth with an open apex remains vital during its spontaneous re-eruption to its origi-nal position in the arch. In these few selected cases, the pulp remains vital, and little or no resorption of the root surface occurs. These cases are the exception rather than the rule; in the vast majority of intrusively luxated teeth, the pulp will become necrotic, and the root surface will undergo IRR.

426 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
Marginal Bone LossThe probability of marginal bone loss is less than one in four patients and ranges between 5% and 24%. An extreme example of this type of bone loss is seen in Fig. 19-15, which demonstrates severe marginal bone loss after an extrusive luxation injury in a medically compromised patient.18 This bone loss occurred over a 6-week period and was likely the result of both the luxation injury and the medical condition of the patient. In most instances, little can be done to prevent marginal bone loss; however, palliative treatment should be
Sequelae to Luxation InjuriesLuxation injuries have numerous sequelae. The most typical will be presented here with the appropriate treatment, when indicated, and the probabilities of each so that the patient can be provided with the appropriate information regarding the long-term status of the luxated tooth. The most typical sequelae to luxation injuries1 are pulp canal obliteration (PCO), marginal bone loss, discoloration of the crown, tran-sient apical breakdown (TAB), pulpal necrosis, and resorp-tion of the root.
The patient should be advised of the sequelae that have the greatest probability relative to the nature of their trauma. This also implies that the patient must be told of the poten-tial for long-term treatment and follow-up of these injuries. On the other hand, a knowledgeable patient can aid the clini-cian in monitoring the typical sequelae to injury of both the tooth and its supporting structures.
Pulp Canal ObliterationPulp canal obliteration (PCO) is a typical sequela to many forms of trauma, in particular to luxation injuries.1 In the literature, PCO has been found clinically to range between 6% and 35%, averaging about one in five luxated teeth (20%). In these situations, the pulp chamber, the root canal system, or both becomes partially or completely calcified to the extent that the canal system may become undetectable on the radiograph (Fig. 19-14 [see Chapter 13]). The pres-ence of PCO is not an indication for a root canal procedure. In the majority of cases, PCO does not lead to pulpal necro-sis. In fact, the probability of pulpal necrosis after PCO is quite low, ranging from 1% to a high of 13%.
FIGUre 19-14 Central incisor that was subluxated; over the course of 24 months, the canal became calcified.
BA
FIGUre 19-15 A and B, Marginal bone loss in an extrusively luxated tooth. This amount of bone loss occurred over a 4- to 6-week period.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 427
FIGUre 19-17 Tooth avulsion with minimal tissue damage.
architecture is noted. This is an uncommon sequela to luxa-tion injuries, and less than 4% of all traumatized teeth will be affected by this condition.
Pulpal NecrosisPulpal necrosis is a common sequela after luxation injuries of the more severe type, but the age of the patient (i.e., maturity of the apex) and severity of the trauma play a role.2,22 The more severe the trauma, the more likely a pulp will become necrotic. In younger patients, the maturity of the apical foramen will play a significant role in revascularization of the tooth. Revascularization is not a common sequela to luxation injuries and is always the exception rather than the rule. When all forms of luxation injuries are grouped together, the probability of pulpal necrosis ranges from a low of 15% to a high of 98%. Again, pulpal necrosis in luxated teeth is a function of the maturity of the root and, more specifically, the type of luxation injury.
Avulsion InjuriesAvulsion injuries are defined as a complete dislocation of the tooth from its alveolar socket (Fig. 19-17). Regardless of the extraoral period or the age of the patient, these injuries always have a guarded prognosis. Even under controlled conditions when a tooth is intentionally extracted and replanted within its socket, the prognosis is guarded because the likelihood of IRR is high (Fig. 19-18); therefore this sequela should be discussed with the patient. Avulsion injuries must be treated aggressively and competently for the patient to maintain the avulsed tooth for a reasonable period of time (Fig. 19-19).
The ideal treatment for the avulsed tooth is to replace it into the socket as soon as possible after the injury. If the patient or someone at the scene of the trauma can replant the tooth, a better prognosis will be obtained versus placing the tooth in a storage medium. If replantation is not possible, then placing the tooth in milk is the next best treatment option. To date, no studies have demonstrated that any sub-stance other than milk is a better storage medium within the first couple of hours after the avulsion injury. Once the patient has arrived at the dental office, the tooth should be
instituted (e.g., 0.12% chlorhexidine rinses and oral hygiene instruction) when appropriate.
Coronal DiscolorationA typical sequela to trauma is a discoloration of the crown of the traumatized tooth. Color changes are not an automatic indication for root canal treatment. Fundamentally, two types of discoloration are seen in traumatized teeth. The first type of change in color that can occur as a result of trauma is that of a deep yellow coloring of the crown. These teeth are typically vital and are discolored because of severe calci-fication of the crown and root canal system. These teeth may or may not respond to the electric pulp tester (EPT) or thermal tests. Regardless of the results of sensibility testing, root canal treatment is indicated only when the patient has symptoms of irreversible pulpitis or pulpal necrosis. A calci-fied tooth typically gives no response to either the EPT or a cold test. However, without radiographic evidence of periapi-cal pathosis, no root canal procedure is indicated. The pulps in these teeth often remain vital and do not become necrotic.
If teeth display a grayish, pinkish, or reddish hue, and an intense light source will not pass through the tooth (fiberop-tic), the pulp is usually necrotic or damaged significantly, and a root canal procedure is indicated (Fig. 19-16; see Fig. 19-8).
Transient Apical BreakdownThe term transient apical breakdown (TAB) refers to a persis-tent radiolucency associated with a luxated tooth2,4; however, sensibility tests indicate a normal pulp. The radiolucency may persist for upwards of 1 year before a normal bony
FIGUre 19-16 Hemorrhage and pinkish to red discoloration in the crown of a central incisor following trauma.

A B C
FIGUre 19-18 A, This 24-year-old female presented with an irregular tooth margin on her central incisor that was irritating her gingival tissues. The tooth had been avulsed 10 years previously, and no treatment other than replantation was performed at that time. B, Radiographic image shows extensive inflammatory root resorption. C, The extracted crown shows the moth-eaten nature of the process.
A B
CD
FIGUre 19-19 A, Avulsed right central incisor out of the socket less than 1 hour. Replanted and splinted. B, Within a few weeks, significant inflammatory replacement resorption is present. C, Placement of calcium hydroxide at various intervals. d, Advanced replacement resorption at 12 months, yet the lamina dura has reformed over the resorbed root end.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 429
A B
FIGUre 19-21 A, Extensive external resorption following replanted central incisors. Calcium hydroxide was placed. B, Histologic appearance of inflammatory external resorption. Note how the multinucleated cells invade the dentin (H&E stain ×100).
FIGUre 19-20 Traumatic avulsion with adjacent soft tissue damage.
briefly rinsed in saline and replanted. Determine whether the traumatic injury was a clean or dirty wound.
If a high probability exists that a foreign body (e.g., stone, metallic object, or dirt) may have entered the alveolar socket, a radiograph of the empty socket should be taken before replantation. If the radiograph reveals any foreign body inside the alveolar socket, it should be rinsed aggressively to eliminate the object. After the socket is clean of any foreign object or objects, the tooth should be replanted as quickly as possible. The only exception to this rule is whether the tooth has been extraoral and dry for more than 60 minutes. Root canal treatment may then be performed before replantation, because a few extra minutes will not affect the prognosis negatively.
If the avulsed tooth has a closed apex and has already been replanted or has been kept in a special storage medium (e.g., milk, saline, Hank’s Balanced Salt Solution)4,29,36 and the extraoral dry time for the periodontal ligament and its cells is less than 60 minutes, adhere to the following guidelines24:
• Clean the area and replant the tooth as soon as possible if not already done (Fig. 19-20). Suture any lacerations. The possibility of revascularization is higher than in any other situation, but the probability is nevertheless quite low.
• Administer systemic antibiotics: doxycycline 200 mg immediately and 100 mg twice daily for 7 days. Consider age of the patient for possible discoloration; if necessary switch to penicillin V. Consider tetanus depending on case circumstances.
• Root canal treatment within 7 to 10 days; place Ca(OH)2.
• Splint the tooth for 10 to 14 days with composite, wire, or a combination of flexible methods.
• Reevaluate the patient every 2 weeks for the first 3 months.
Under the same circumstances, if the tooth extraoral dry time is greater than 60 minutes, the prognosis is poor. Remember that if a closed-apex tooth has been avulsed and dry for more than 1 hour, the prognosis is poor. Because the probability of IRR is extremely high (Fig. 19-21), inform the patient that the long-term prognosis will be a function of how rapidly replacement resorption may occur. Nonetheless, because teeth that have been extraoral and dry for up to 48 hours have been shown to be functional for 7 years, keep in mind that few contraindications prevent the practitioner

430 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
splint interproximally is discouraged because significant soft-tissue damage usually occurs (Fig. 19-22).
• Any evidence of resorption or lack of development of the traumatized tooth noted radiographically warrants root canal treatment (Fig. 19-23) with apexification procedures (see Chapter 13). Teeth with open apices typically have extremely large canals and pulp chambers. Should the revascularization procedure fail, a large quantity of necrotic pulpal tissue and bacteria will induce a rapid and extremely destructive resorption of the root. This can result in loss of the tooth in less than 2 to 3 months.
If the avulsed tooth has an open apex and the extraoral drying time is more than 60 minutes, consider the following guidelines:
from replanting an avulsed tooth regardless of the extraoral time period. The tooth is splinted for 10 to 14 days and root canal procedures started within 7 to 10 days after replanta-tion. Ca(OH)2 is also indicated in these cases until the root canal is obturated.
Unlike most other cases of healing, an older patient has a better prognosis than a young patient with respect to avulsed teeth. In the adult patient, the root canal system and pulp chamber has become more calcified and is usually smaller in volume than it is in the young patient. In addition, the den-tinal tubules are more calcified and smaller in volume. This prevents the spread of inflammatory resorption and provides the older patient with a more favorable prognosis with respect to avulsed teeth.
Should the tooth begin to demonstrate IRR, over time, the patient will lose the tooth. However, IRR is chronic, and the process takes months to years before the tooth is com-pletely resorbed.32 The advantage of allowing the tooth to resorb is that the alveolar socket will gradually fill in with bone. Additionally, the patient will not have an esthetic defect such as is the case if the tooth were not replanted or extracted prematurely and the socket had to fill in with bone. By letting the tooth resorb, the entire root will be eventually replaced with bone, and the alveolar socket will completely fill in with healthy bone that can be used for an implant or an esthetic bridge.
If the avulsed tooth has an open apex and the extraoral drying time is less than 60 minutes, consider the following guidelines:
• Replant the tooth as quickly as possible. The possibility of revascularization is higher than in any other situation, but the probability of revascularization is nevertheless quite low.
• Recall the patient for evaluation every 2 weeks for the first 3 months to determine whether the revascularization process is occurring. In all cases where revascularization is attempted, both the patient and the clinician should know that the prognosis is guarded; without proper follow-up treatment, the tooth can be lost in as little as 5 weeks. If possible, include the contralateral tooth in the follow-up radiograph to compare the development of the avulsed tooth with the nontraumatized contralateral tooth.
• Splint the tooth for 10 to 14 days with a flexible device if possible. The type of splint, rigidity, or length of time the splint is in place are not critical to the success of the replantation; however, the splint should be secured to stabilize the tooth for the time period. Fig. 19-22 shows wire and composite splints. A bonded composite is ideal for traumatic injuries and the tooth can be checked for stabilization without ruining the splint. Should additional time be required for stabilization of the tooth, replace the wire with rubber bands, and the splint will again be functional. The use of wires to
FIGUre 19-22 Following removal of interdental wire splints, significant tissue damage is evident.
FIGUre 19-23 A replanted mature central incisor being almost completely resorbed in 6 months.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 431
A B
FIGUre 19-25 A, The central incisor was avulsed and left out of the mouth for over 48 hours. Root treatment was then done, and the tooth was replanted and splinted. B, One year later, there is evidence of healing following a small amount of resorption on the mesial surface (arrow). The tooth is stable and functional.
These areas cannot be treated; however, removing the necrotic and bacteria-infested pulpal tissue within the root canal system can prevent additional damage. Studies suggest the long-term use of Ca(OH)2 (6 to 12 months) as a thera-peutic agent to prevent resorption, but this treatment has recently been shown to decrease the fracture resistance of dentin and the ability of healing periodontal ligament cells to proliferate, thereby causing an increase in IRR (Fig. 19-26).10,13,21
This resorptive process is seen in intrusive luxation injuries and will eventually cause loss of the tooth. The process occurs
• Little chance exists that revascularization will take place under these circumstances.
• The ideal treatment for these cases is to replant the tooth after performing root canal therapy extraorally and placing root-end filling.
• In all cases of an avulsed tooth with open apex and more than 1 hour of extraoral dry time, the prognosis is very poor; eventual loss of the tooth should be considered in the long-term treatment plan. If so, the tooth can be decoronated at a later time with a tissue flap covering the root to preserve the alveolar ridge.
• If replanted before root canal procedures, access the tooth, place Ca(OH)2 and perform root canal treatment within 7 to 10 days.
Resorption Associated With Traumatic Tooth Injuries
Resorption can and does play a significant role as a more severe sequela to traumatic injuries. The basic concepts in resorption are discussed in Chapter 13. The process as it relates to the unique challenges faced in managing traumatic injuries will be discussed here, focusing primarily on external inflammatory resorption (Fig. 19-24).
Inflammatory resorption that occurs externally is rapid and extremely destructive, but for the most part it can be prevented or minimized by proper cleaning and shaping of the root canal system. This resorption is characterized radio-graphically by moderate to large “scooped-out” radiolucent areas on the root of the traumatized tooth (Fig. 19-25).
FIGUre 19-24 Excessive drying and treatment mismanagement prior to replantation resulted in significant resorption.

432 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
A B C
FIGUre 19-26 A, Both central incisors were avulsed and replanted within 2 hours. B, The root canal treatment was done within 1 month. C, Three years later, the resorptive process is present in both teeth and more advanced in the left central incisor.
over several months to years before it becomes critical and the tooth is subsequently lost. The patient should be made aware of this type of sequela, and its ramifications should be included in the long-term treatment plan of the patient. Avulsion injuries will also demonstrate IRR, but this can take months to years before it becomes apparent. The process is not self-limiting, and no known treatment prevents its occur-rence or spread throughout the root.
Inflammatory Replacement Resorption and AnkylosisAs noted earlier, IRR is commonly and mistakenly called ankylosis. Inflammatory replacement resorption is the term used to designate the actual process of root resorption and its replacement with hard tissue. Ankylosis is the result of this process by which the tooth (specifically the periodontium and radicular structures) becomes locked in the cancellous bone (Fig. 19-27). As defined in the medical literature, it is a solid fixation of a tooth resulting from fusion of the cemen-tum and alveolar bone. As IRR destroys the cementum and dentin, bone is deposited directly and contiguously within the resorbed tooth structure. The PDL is lost, and bone is adjacent to cementum and dentin. No soft tissue or PDL exists between the bone and tooth, and because the resorptive process is irregular and quite invasive, the tooth becomes locked into the cancellous bone, resulting in no mobility of the affected tooth.
The currently accepted cause of IRR is severe damage or complete loss of the PDL, usually associated with an avulsion injury or intrusion of a tooth into its socket. It is also seen in the elderly and occasionally in younger patients. There seems to be virtually no correlation of IRR with bacteria or
necrotic pulpal tissue, because it can and does occur in avulsed teeth with previous root canal therapy. In addition, patients who have avulsed a tooth and have no occurrence of IRR will still demonstrate inflammatory resorption in the affected tooth. Once initiated, inflammatory resorption can and usually does continue until the entire tooth is lost.
Two types of IRR should be noted. The first type is tran-sient RR in which the tooth undergoes IRR, but the damage to the PDL is minor and the ligament is able to heal, which prevents the continuation of the resorptive process. The other type that is more common is progressive IRR in which the resorptive process continues and eventually destroys the entire root structure, thereby causing premature loss of the tooth. IRR is chronic in nature and therefore usually a very slow process that occurs over several months to years. The resorption is always initiated on the external root surface where the PDL was damaged, usually by trauma (i.e., avul-sion or intrusive luxation). Similar to inflammatory resorp-tion, IRR is not self-limiting and therefore will continue until the entire tooth is lost.
The radiographic characteristics of IRR are completely unlike those of inflammatory resorption. Because the etiology is entirely different from inflammatory resorption, the radio-graphic presentation is also unique. IRR results in destruction of the root; however, this destruction is rapidly replaced with bone, and therefore the radiographic characteristic is that of a radiopacity and not a radiolucency, as is the case with IRR. Similar to inflammatory resorption, the defects are usually irregular and asymmetric, presenting initially on the mesial or distal root surface. Younger patients will have a more rapid course of RR, whereas older patients have the best prognosis because of the chronicity of this very destructive process.
The onset of IRR is insidious and difficult to see unless specifically looking for signs of IRR and minor changes in

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 433
comparison to an elderly patient in whom the destructive process usually occurs over many years.13
Inflammatory resorption and IRR are similar in their clini-cal presentation. Neither is associated with symptoms or soft-tissue changes. Because of their insidious onset, the diag-nosis is often made during review of routine radiographs. These types of resorptive defects should be anticipated when-ever a history of trauma exists (i.e., avulsion or luxation injury) or attempts have been made to treat the traumatic injury. Sinus tracts or other soft-tissue manifestations are rarely associated with either of these resorptive processes.
Treating IRR by removing the infected pulpal tissue is of little value, unlike with inflammatory resorption. In fact, no current techniques or medicaments have demonstrated reli-able and valid therapeutic advantages for the prevention or inhibition of IRR. Enamel matrix proteins have been recom-mended as a medicament to inhibit inflammatory resorption, IRR, or both in animal models. However, investigators have
the PDL. Fig. 19-28 demonstrates this phenomenon in which avulsed left central incisors are beginning to show signs of IRR at the junction of the middle and apical third on the mesial surface of the root. These changes occurred within 2 months after the tooth was replanted. Without knowledge of what to expect radiographically as classical early IRR, the clinician might easily overlook this defect, considering it to be an artifact. This radiographic presentation is in stark con-trast to Fig. 19-19, which demonstrates classical inflamma-tory resorption that has taken 12 months to develop in an adolescent patient. The reader should note that the root is approximately 40% to 50% resorbed and progressing chroni-cally. In a futile attempt to prevent or inhibit the RR, Ca(OH)2 was used over a 21
2-year period. The result was likely to be the same regardless of the use of an intracanal medicament. Although stabilized at 12 months, the tooth was eventually lost after 3 years of Ca(OH)2 therapy. In this case, the inflammatory resorption proceeded rapidly in
A
B C
FIGUre 19-27 A, Histologic picture of inflammatory replacement resorption. Note how the bone cells have invaded the resorptive lacunae in the dentin. Bone matrix appears to be developing rapidly (H&E stain ×100). B, Ankylosis; note the invasion of the dentin (left) with bony Haversian systems (H&E stain ×10). C, Thick section (70 µ) of dentin and bone photographed with a filter to enhance the ankylosis. Note the penetration into the dentin of the bone and the “locked-in” appearance.

434 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
repositioned if displaced, and an additional radiograph should be exposed to verify correct repositioning of the two segments. Splinting is indicated if the coronal segment is mobile (usually 6 to 8 weeks or longer); however, because most HRF occur in anterior maxillary teeth, the roots are stable because of the amount of supporting bone. In horizon-tal fractures, two teeth on either side of the traumatized tooth should be splinted because of the need for rigid splinting of the segments.
Root canal treatment is not indicated in most instances, because only 20% to 44% of the pulps become nonvital.20 When treatment is indicated, only the coronal segment should be treated. The apical segment will maintain its vital-ity and usually undergoes significant calcification of the canal system. Sensibility tests should not be considered until at least 4 to 6 weeks after the trauma, because these tests are usually invalid immediately after the trauma.
Middle-Third FracturesAs is the case with apical-third fractures, all middle-third HRF should be radiographed to determine the extent of damage to the root and surrounding tissues. Repositioning of the tooth should be completed with forceps or 2 × 2 gauze, and the splint should remain in place for at least 6 to 8 weeks (Fig. 19-30). If a root canal procedure is indicated from radiographs, patient symptoms, or clinical tests, it should be completed as soon as the diagnosis of necrotic pulp is estab-lished. As with apical-third fractures, the apical segment will remain vital, and this segment will not need treatment unless radiographic signs indicate pathologic changes.
Coronal-Third FracturesCoronal root fractures are the most difficult cases to treat because of their location and the possibility for extreme
failed to substantiate these recommendations, and it is likely that until the cause of IRR has been discovered, a suitable treatment to prevent or inhibit its occurrence will not be available. When IRR is identified, the patient must be informed of the extremely destructive nature of this process and advised to consider the long-term consequences of loss of the affected tooth.
Horizontal Root FracturesHorizontal root fractures (HRF) are classified into one of three categories: apical-, middle-, or coronal-third fractures.5,6 Most apical and many middle-third fractures may require splinting; however, because these teeth should be immobi-lized for at least 6 to 8 weeks, some type of stabilization is strongly recommended depending on the individual case cir-cumstances. Most of these patients are young and often extremely active. During the healing period, fractured teeth, although not necessarily mobile from the trauma, must be splinted to prevent additional damage during the 6 to 8 weeks in which healing takes place. Unlike luxation and avul-sion injuries, rigid splinting of HRF teeth is mandatory in all cases to obtain successful healing and prevent undesired sequelae.
Apical-Third FracturesApical-third HRF, as the name implies, occur in the apical third of the root through cementum, dentin, and pulpal tissue. A radiograph should always be exposed before the tooth is repositioned to determine the extent of the fracture.
Apical-third fractures, especially in the central incisors, typically do not require splinting because of the amount of bone surrounding the coronal segment of the root that has been displaced (Fig. 19-29). The tooth should be
FIGUre 19-28 Extensive and almost complete IRR on the left central incisor. The process is active on the right central.
FIGUre 19-29 Apical-third horizontal root fracture.

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 435
FIGUre 19-31 Coronal-third fracture of a central incisor. Note how easy communication with the gingival sulcus can be and how the prognosis of these fractures is highly guarded.
mobility of the fractured coronal root segment (Fig. 19-31).19 Depending on the location of the fracture, immediate stabi-lization is required, and the need for root canal treatment is more probable than in the other two situations. If the clini-cian can probe periodontally to the fracture site, then the coronal segment should be removed, and a treatment plan for the apical segment must be determined. In these cases, salivary contamination will have occurred and the two
FIGUre 19-30 Repositioning and splinting of a middle-third fractured tooth.
segments will not heal properly. In these circumstances, once the coronal segment is removed, the apical segment can be orthodontically moved coronally27 and a post, core, and crown can be fabricated to save the apical segment of the tooth. However, depending on the length of the tooth and the shape of the root, this is not always feasible; in these cases the tooth must be extracted.
Healing Responses to Horizontally Fractured Teeth
Four types of healing or tissue responses typically occur with horizontally fractured teeth: calcified union between the seg-ments, bone and connective-tissue healing, connective-tissue or soft-tissue union, and failure to heal. The first three rep-resent an adequate healing response from proper stabiliza-tion, but a calcific union is the desired ideal result.
Calcified Union Between the SegmentsThis type of healing occurs when rigid stabilization of the two segments has been maintained. In this case, a calcific union occurs between the two segments, and radiographi-cally little or no radiolucent line is seen from the original fractured segment (Fig. 19-32). The mobility of the tooth is within normal limits, and the pulp maintains its respon-siveness to sensibility testing. The patient remains symptom free and is able to function normally on the tooth. This healing usually takes at least 8 to 12 weeks to occur. If the tooth should darken coronally and healing of the hori-zontal fracture is evident, then a root canal procedure is indicated (Fig. 19-33).
FIGUre 19-32 Calcific union between two fractured segments of a horizontally fractured tooth.

436 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
FIGUre 19-33 Even when calcific healing occurs, the coronal segment may darken, and a root canal procedure in the coronal third is indicated.
normally on the previously fractured segment. The pulp maintains its vitality in both segments, and no additional follow-up is required. However, in those cases in which the pulp has not retained its vitality and root canal treatment is indicated, mineral trioxide aggregate (MTA) can be used (see Fig. 19-34, B ). In this case, the segments were not closely approximated, and the apical portion was filled with gutta-percha and sealer. Then there was an unsuccessful attempt to orthodontically reposition the coronal segment. The coronal portion was filled with MTA and over time actually separated even more with an ingrowth of bone and connec-tive tissue between the segments—8 years following the origi-nal trauma.
Connective-Tissue or Soft-Tissue UnionThese cases heal with a normal periodontal ligament between the two segments that are in close approximation to each other (Fig. 19-35). Radiographically a normal periodontal ligament is noted between the two segments, and mobility is within normal limits. Both segments maintain their vitality, and no additional treatment is indicated.
Failure of Fracture to HealIn cases in which a union of the two segments is not achieved, the patient may become symptomatic during the splinting period, or radiographic signs of failure to heal will be apparent. The classical presentation is a semilunar radio-lucency at the fractured segment on both sides of the fracture, and often a sinus tract develops that can be traced to the fractured area (Fig. 19-36). Depending on whether a peri-odontal probing to the fractured area can be determined,
A B
FIGUre 19-34 A, Bone and connective-tissue healing in two horizontally fractured central incisors. B, Eight-year reexamination of the central incisor that had a coronal fracture in which the segments were separated. The segments were orthodontically repositioned, the root canal treatment done on the apical portion, and the coronal was filled with mineral trioxide aggregate. Over time, the segments separated; however, note the nature of the bone and periodontal ligament healing between the segments. (B, Courtesy Dr. Sonia Ferreyra.)
Bone and Connective-Tissue HealingThis type of healing usually occurs in young patients in whom the maxillary bone is still developing (Fig. 19-34). The two segments become separated over time (usually months), with normal periodontal ligament surrounding each segment. There may be several millimeters between the two segments, which are separated by normal bone. Addi-tional treatment is not needed, and the patient can function

chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries 437
FIGUre 19-35 Connective-tissue healing of the two segments in horizontally fractured roots and various levels.
the prognosis is guarded to poor in most cases. Whenever the periodontal probe can be placed to the fracture site, the prognosis is poor, and the tooth will not heal properly. In most instances, the coronal segment must be removed and a determination made regarding saving the apical segment. These cases involve complex treatment plans, and usually integrated (periodontal, restorative, and endodontic) treatment is required. The clinician must determine whether an implant versus an extensive and complex treatment plan to save the tooth is warranted. If the periodontal probings
A B
FIGUre 19-36 A and B, Examples of horizontal root–fractured teeth that failed to heal properly. Note the semilunar radiolucencies on either side of the fracture line in A. A sinus tract can be traced to the fracture line in A, while resorption of the coronal segment is beginning in B.
of the coronal segment are within normal limits, then sta-bilization of the coronal segment, root canal treatment of that segment, and appropriate restorative treatment can be used to save the fractured tooth. The determining factor in these cases is always whether the coronal segment can be stabilized adequately. Significant mobility of the coronal segment always contraindicates any additional treatment of this segment.
Splinting of Traumatized Teeth
Over the years, there has been an interesting evolution on whether or not to splint, when to splint, the type of splint, and the length of splinting times. The previous discussion provided indications for each trauma type, but as a summary, the concise information provided in Table 19-1 should guide the clinician in splinting times for traumatized teeth.23
TABLe 19-1 Splinting Times
Type of Injury Splinting Time
Subluxation 2 weeks
Extrusive luxation 2 weeks
Avulsion 2 weeks
Lateral luxation 4 weeks
Root fracture (middle third) 4 weeks
Alveolar fracture 4 weeks
Root fracture (coronal third) 4 months

438 chapter 19 | Problem Solving in the Management of Tooth Fractures and Traumatic Tooth Injuries
19. Cvek M, Mejare I, Andreasen JO: Healing and prognosis of teeth with intra-alveolar fractures involving the cervical part of the root, Dent Traumatol 18:57-65, 2002.
20. Cvek M, Mejare I, Andreasen JO: Conservative endodontic treat-ment of teeth fractured in the middle or apical part of the root, Dent Traumatol 20:261-269, 2004.
21. Doyon GE, Dumsha TC, von Fraunhofer JA: Fracture resistance of human root dentin exposed to intracanal calcium hydroxide, J Endod 31:895-897, 2005.
22. Dumsha TC, Hovland EJ: Pulpal prognosis following extrusive luxation injuries in permanent teeth with closed apexes, J Endod 8:410-412, 1982.
23. Flores MT, Andersson L, Andreason JO, et al: Guidelines for the management of traumatic dental injuries. I. Fractures and luxa-tions of permanent teeth, Dent Traumatol 23:66-71, 2007.
24. Flores MT, Andersson L, Andreason JO, et al: Guidelines for the management of traumatic dental injuries. II. Avulsion of perma-nent teeth, Dent Traumatol 23:130-136, 2007.
25. Geary JL, Clifford TJ, Kinirons MJ: Occlusal accommodation and mouthguards for prevention of orofacial trauma, Oral Health Prev Dent 7:55-59, 2009.
26. Gutmann JL, Rakusin H: Endodontic and restorative management of incompletely fractured molar teeth, Int Endod J 27:343-348, 1994.
27. Heithersay GS: Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest, Oral Surg Oral Med Oral Pathol 36:404-415, 1973.
28. Hiatt WH: Incomplete crown-root fracture in pulpal-periodontal disease, J Periodontol 44:369-379, 1073.
29. Hiltz J, Trope M: Vitality of human lip fibroblasts in milk, HBSS, and Viaspan storage media, Endod Dent Traumatol 7:69-72, 1991.
30. Lin S, Zuckerman O, Fuss Z, et al: New emphasis in the treatment of dental trauma: avulsion and luxation, Dent Traumatol 23:297-303, 2007.
31. Maxwell EH, Braly BV: Incomplete tooth fracture—prediction and prevention, Calif Dent Assoc J 5(10):51-55, 1977.
32. Oikarinen K, Gundlach KK, Pfeifer G: Late complication of luxa-tion injuries to teeth, Endod Dent Traumatol 3:296-303, 1987.
33. Oulis C, Vadiakas G, Siskos G: Management of intrusive luxation injuries, Endod Dent Traumatol 12:113-119, 1996.
34. Schweitzer JL, Gutmann JL, Bliss RQ: Odontiatrogenic tooth fracture, Int Endod J 22:64-74, 1989.
35. Silvestri AR: The undiagnosed split-root syndrome, J Am Dent Assoc 92:930-935, 1976.
36. Trope M, Yesilsoy C, Koren L, et al: Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teeth, J Endod 18:492-496, 1992.
37. von Arx T: Splinting of traumatized teeth with focus on adhesive techniques, J Calif Dent Assoc 33:409-414, 2005.
RECOMMENDED ADDITIONAL READINgAndreasen JO, Andreasen FM: Essentials of traumatic injuries to the
teeth. A step-by-step treatment guide, ed 2, Copenhagen, 2000, Munksgaard.
Bakland L (Guest Editor): Update on traumatic dental injuries, Endod Topics 14:1-118, 2006.
Berman LH, Blanco L, Cohen S: A clinical guide to dental traumatol-ogy, St Louis, 2007, Mosby Elsevier.
Bornstein MM, Wölner-Hanssen AB, Senid P, et al: Comparison of intraoral radiography and limited cone beam computed tomogra-phy for the assessment of root-fractured permanent teeth, Dent Traumatol 25:571-577, 2009.
REFERENCES1. Andreasen FM: Pulp healing flowing acute dental trauma: clinical
and radiographic review, Prac Proced Aesthet Dent 14:315-322, 2001.
2. Andreasen FM, Vestergaard Pedersen B: Prognosis of luxated per-manent teeth—the development of pulp necrosis, Endod Dent Traumatol 1:207-220, 1985.
3. Andreasen FM, Zhijie Y, Thomsen BL, et al: Occurrence of pulp canal obliteration after luxation injuries in the permanent denti-tion, Endod Dent Traumatol 3:103-115, 1987.
4. Andreasen JO, Andreasen F, Andersson L: Textbook and color atlas of traumatic injuries to the teeth, ed 4, Oxford, 2007, Blackwell Munksgaard.
5. Andreasen JO, Andreasen FM, Mejàre I, et al: Healing of 400 intra-alveolar root fractures. I. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation, Dent Traumatol 20:192-202, 2004.
6. Andreasen JO, Andreasen FM, Mejàre I, et al: Healing of 400 intra-alveolar root fractures. II. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and anti-biotics, Dent Traumatol 20:203-211, 2004.
7. Andreasen JO, Bakland LK, Matras RC, et al: Traumatic intru-sion of permanent teeth Part 1. An epidemiological study of 216 intruded permanent teeth, Dent Traumatol 22:83-89, 2006.
8. Andreasen JO, Bakland LK, Andreasen FM: Traumatic intrusion of permanent teeth Part 2. A clinical study of the effect of preinjury and injury factors, such as sex, age, stage of root development, tooth location, and extent of injury including number of intruded teeth on 140 intruded permanent teeth, Dent Traumatol 22:90-98, 2006.
9. Andreasen JO, Bakland LK, Andreasen FM: Traumatic intrusion of permanent teeth Part 3. A clinical study of the effect of treat-ment variables such as treatment delay, method of repositioning, type of splint, length of splinting and antibiotics on 140 teeth, Dent Traumatol 22:99-111, 2006.
10. Andreasen JO, Farik B, Munksgaard EC: Long-term calcium hydroxide as a root canal dressing may increase the risk of root fracture, Dent Traumatol 18:134-137, 2002.
11. Berdmore TG: A Treatise on the disorders and deformities of the Teeth and Gums, London, 1768, B White, J Dodsley, T Becket and PA de Hondt.
12. Berude JA, Hicks ML, Sauber JJ, et al: Resorption after physiologi-cal and rigid splinting of replanted permanent incisors in monkeys, J Endod 14:592-600, 1988.
13. Blömlof L, Lengheden A, Lindskög S: Endodontic infection and calcium hydroxide-treatment. Effects on periodontal healing in mature and immature replanted monkey teeth, J Clin Periodontol 19:652-658, 1992.
14. Cameron CE: Cracked-tooth syndrome, J Am Dent Assoc 68:405-411, 1964.
15. Cameron CE: The cracked-tooth syndrome: additional findings, J Am Dent Assoc 93:971-975, 1976.
16. Cohen S, Blanco L, Berman L: Vertical root fractures: clinical and radiographic diagnosis, J Am Dent Assoc 134:434-441, 2003.
17. Crona-Larsson G, Noren JG: Luxation injuries to permanent teeth—a retrospective study of etiological factors, Endod Dent Traumatol 5:176-179, 1989.
18. Cunha RF, Pavarini A, Percinoto C, et al: Pulpal and periodontal reactions of immature permanent teeth in the dog to intrusive trauma, Endod Dent Traumatol 11:100-104, 1995.

439
Chapter 20
Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
Problem-Solving ListProblem-solving issues and challenges in the restoration of endodontically treated teeth addressed in this chapter are:
Postendodontic and Intertreatment Temporary Restorations
Restoring Access Openings
Problem-Solving Key Factors That Influence Restorative Choices in Anterior and Posterior Teeth
Restoration of anterior teeth
Restoration of posterior teeth
Intraradicular posts
Exposed and Contaminated Root Fillings Due to Coronal Leakage
I have made a diligent search to find whether or not teeth from which the pulp had been removed, and the canals and pulp chamber filled without admitting the fluids of the mouth, were subject to a similar deterioration of strength. It is now well known that teeth treated in this way retain their color almost perfectly; and from my observation of the relation of color to strength of the teeth I am prepared to entertain the suppositions that they retain their strength also. Only one tooth came into my hands with a root filling. It was a central incisor, and had not sufficient tissue for me to obtain a block; but it showed no undue percentage of water, and the color was good. Up to the present time I have been unable to obtain the history of the filling of this root.21
G.V. Black, 1885
The concept of restoring endodontically treated teeth usually evokes challenging images of teeth with significant coronal tooth loss. In reality it may be the simple closure of an access cavity in a satisfactory coronal restoration to the total recon-struction of a tooth with no clinical crown due to the ravages of caries, faulty restorations or traumatic episodes, both short and long term (e.g., accidents, occlusal wear, abnormal func-tion, etc.). Regardless of the clinical situation, the two primary objectives are to preserve the integrity of the root canal filling and rebuild the tooth into a symptom-free, func-tional, stable contributor in the patient’s dentition.29,47,51,90
In the last 25 to 30 years, a plethora of scientific studies, clinical-technique articles, and the introduction of new mate-rials have addressed the enigmatic issue of restoring an
endodontically treated tooth.49,93 During this same period, however, the significance of coronal leakage relative to end-odontic failure has been highlighted, although this problem was identified over 90 years ago.33 The application of the principles of problem solving must now include, through careful and deliberate diagnostic assessments, the elements of identification and prevention as well as the need to manage these issues using either evidence-based or the best evidence directives. Although scientific insights and technologic improvements have provided a clearer understanding of this issue, sound clinical judgment and experience must still enter into the decision-making process in the restoration of these teeth. This includes the choice and placement of interim restorations before and during root canal treatment as well.
In Chapter 8, the importance of removing questionable restorative materials and all caries, along with proper tooth isolation, was stressed in conjunction with (1) the assessment of the restorability of the tooth, (2) identification of defects in the tooth structure, and (3) the development of a func-tional endodontic access opening in the tooth to be treated. To enhance this important phase of treatment, the use of

440 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
in the pulp chamber prior to permanent restoration, may become entrapped in the materials along the cavity wall and provide an avenue for leakage.95,145 A well-placed temporary restoration can be expected to protect against bacterial leakage no longer than 1 month.14
While all materials leak to some extent,7,17,105,132,154 zinc oxide eugenol cements have long been regarded as possessing the best sealing properties of all cement materials because of their antimicrobial properties.28,146 However, zinc oxide/calcium sulfate materials such as Cavit tend to be more resis-tant to leakage than zinc oxide eugenol materials.146 The combined use of both materials may minimize leakage,12 but in either case, a minimum of 3 mm of thickness is essen-tial.16,68,99,146 Resin-based materials can be used, but they have a tendency to shrink and result in leakage.26
The placement of a temporary post and core creates a different set of circumstances, especially as it relates to an impervious seal.34,43 In these circumstances, a barrier40,82 using a self-curing material may need to be placed over the coronal, intracanal termination of the root canal filling material.
A better consideration for a temporary filling, if the tooth is not to be restored permanently in the immediate future, would be placement of a temporary material to the pulpal chamber floor without the use of a cotton pellet.116 The seal may be enhanced by thickness (usually greater than 3 mm). If a cotton pellet is to be used, however, orifice barriers are recommended. First, countersink the orifice with a small round bur, followed by a thorough cleaning with alcohol or a detergent to remove excess cement and debris. Second, if possible use air abrasion to free the dentin from films and debris. Third, place a temporary or permanent restoration in the orifices and over the floor of the chamber. In this regard, bonded materials or glass ionomers are favored.19,20,45,148,149 Mineral trioxide aggregate (MTA) may also be considered,4,77 but a clear material would assist the restoring clinician in identifying the orifice(s).
If temporary materials are used to fill the entire chamber in lieu of an orifice barrier, they may create a problem for the restoring clinician for two reasons. Firstly, careful removal of the material at the time of restoration is essential to prevent gouging the pulp chamber floor or walls or removing excess tooth structure in the cervical area. Secondly, weakening of the tooth in this area is a potential problem relative to future tooth fracture. Retention of sound dentin, especially in the cervical portion of the tooth, is very important. Thirdly, if eugenol-based materials have been used, future bonding in the chamber may be affected.
None of the laboratory studies that have investigated the efficacy of many of the temporary filling materials has included perhaps one of the most devastating of complica-tions, namely the forces of occlusion on a temporary filling over time. Under clinical conditions and involving access cavities in the occlusal surfaces of teeth in function, the ability of any temporary restoration to maintain a seal is questionable. This is especially true in occlusional relation-ships with deep plunging cusps that can destroy the
magnification and a caries detector is usually beneficial, but the latter may also stain sound dentin that has decreased mineral content. Recent advances in the development of caries-detecting agents may have eliminated this problem.59 In many cases requiring root canal treatment, two or more treatment visits may be indicated, and this requires that a proper interim temporary restoration be placed. The same dictate applies to each tooth upon completion of the root canal treatment if a permanent restoration is not going to be placed immediately. However, the effectiveness of temporary cements can vary,10,99 so the importance of these temporary restorations cannot be overemphasized relative to the prog-nosis for positive treatment outomes.56,74
Postendodontic and Intertreatment Temporary Restorations
With the initial access opening preparation, all caries, under-mined tooth structure, and areas that are questionable relative to their integrity are to be removed or investigated (cracks, stained lines, etc.) so the tooth can be assessed for restorability prior to the actual root canal procedures. Some clinicians choose not to do these procedures, claiming there might be leakage if a wall were removed or if all the caries under a crown were eliminated. The claim is also made that the tooth cannot be isolated properly if specific tooth structure is removed. In essence, these approaches destroy the problem-solving concept and actually create environments conducive for problems. For example, salivary and bacterial leakage through carious dentin or poorly placed temporary materials can cause interappointment flare-ups and the opportunity for bacteria and their biofilms and byproducts to gain a foothold into an open canal or even one that has been obturated (see Chapter 5).*
As a basic principle in restorative dentistry, restorations usually leak in time, and no materials are perfect. When con-sidering temporary restorative materials for endodontic access openings, everything will leak sooner rather than later.68,116 Even in well-done root canal procedures, coronal leakage can result in reinfection of the apical tissues in as little as 19 days,69,135 with relative certainty within 3 months.76 There-fore prevention is essential in these cases by first considering immediate, permanent restoration following root canal treat-ment. If not possible, preventive techniques are necessary to minimize the possibility of this devastating occurrence.
Many premixed preparations have enjoyed popularity as interim or post root-treatment temporary filling materials, such as Cavit (3M ESPE, St. Paul, MN, USA) or IRM (Dentsply Caulk, Milford, DE, USA). Laboratory studies indicate, however, that their ability to prevent the ingress of bacteria over time is poor.12-14,71 A second complication arises in that cotton, which is commonly used to maintain space
*References 1, 7, 11, 13, 14, and 16.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 441
are the most durable.116 They might be the best materials to use with eugenol-contaminated surfaces.100,102,148 Secondly, dentin bonding agents will lose bond strength as early as 3 months, followed by the potential for leakage over time.23 Finally, self-etching materials may not fare well with intact enamel rods around the margins; therefore, the margins must be beveled.
Postoperatively, the very best solution is to restore the tooth immediately and avoid temporization completely. If this approach is not possible, the treatment plan should seek to accomplish as much permanent closure of the root canal system as possible. The pulp chamber should be permanently restored immediately if a post is not required. If the tooth requires a post and core, it would be best to proceed to these procedures immediately on completion of the root canal treatment. The crown could be completed at a later time. An alternative would be temporary closure of the pulp chamber and immediate crown preparation so that the integrity of the root canal procedures and the internal anatomy could be further protected with a temporary crown. The important goal is the preservation of all the efforts made to clean, dis-infect, and obturate the root canal system.
Restoring Access OpeningsRoot canal procedures are commonly required for teeth that have satisfactory existing restorations, primarily crowns that have good margins and no evidence or deterioration (if metalloceramic no obvious craze lines or fractures). In doing so, potential weakening of the restoration or the tooth struc-ture supporting the restoration is a valid concern.9 A number of studies have addressed the clinical scenario.54,92,136-139,151 For this reason, conservative access cavities are always prefer-able to generous and often excessive preparations. Keep in mind, however, that when crowns have been placed on rotated teeth or roots and canals exit the coronal part of the tooth at unusual angles, access openings may have to be enlarged or altered in shape significantly in order to find the entire canal system (see Chapter 8).
The crowns of many teeth are frequently reconstructed entirely of amalgam or composite resin filling materials. Fol-lowing root canal treatment, it is common to repair the access cavities with restorations of the same material. Nevertheless, research has demonstrated that routine access through large, multiple surface amalgam restorations significantly compro-mises the fracture strength of the repaired restoration post-operatively.54 For this reason, the placement of a full crown is worthy of consideration because the prognosis of this type of restoration will enhance tooth retention.5 The effect of access preparations through coronal reconstructions with composite resin is an unknown entity, and good restorative principles must be applied based on individual case demands. If any area of exposed enamel exists during the access opening preparation, beveling of the enamel margin followed by a self-etching adhesive system would be favored38 to protect the weaker dentin bonding beneath the surface.36
temporary, resulting in coronal leakage or in tooth fracture. These potential problems have been identified by some as a rationale for one-visit root canal treatment for all teeth; however, it does not consider those patients who delay the ultimate restorative process.
For interappointment temporary fillings, the most reason-able approach to prevent bacterial ingress would be to use calcium hydroxide as an intracanal medicament or, as some studies have pointed out, the combination of chlorhexidine and calcium hydroxide (see Chapter 11). This material or combination is not only antibacterial but also provides a physical barrier at the orifice. Secondly, if desiccated, it will not compress when the temporary filling material is placed. This would also be the method of choice in the case of a tooth with prepared post space, in which the post could not be permanently cemented immediately. The choice of tem-porary materials could still include a zinc oxide eugenol cement if the interval between appointments will be short. If the interval will be extended, or if the tooth is under heavy occlusal loading, composite resins or amalgam would provide better sealing under function. In the experience of the authors, glass ionomer cements have not been durable under occlusion, especially when placed in the access opening that has been made in a metalloceramic crown.
A second complication that may arise with the use of temporary filling materials over long periods of time is the presence of unrestored post space.11,34,91 If coronal leakage occurs, the significantly shorter gutta-percha fillings have been shown to leak much more rapidly than fully filled canals.1,2,86,87 In these situations, the use of a calcium hydrox-ide/2% chlorhexidine dressing in the post space would seem to be advantageous.100 At the time of restoration, removal of the dressing and rinsing of the post space with additional antimicrobial solutions such as 2% chlorhexidine would be of benefit.117
Regarding the use of intermediate restorative material (IRM, Dentsply Caulk, York, PA, USA) as a temporary material, the issue of a eugenol-based material is controversial relative to the ultimate use of a bonded restoration, com-posite, or core material for the final restoration.42,150 Since dentinal tubules account for only ±15% of the material retention,53 the dentinal surface, in particular the collagen matrix in the intertubular dentin, will influence the bulk of the ultimate retention.101,129,130 Eugenol-contaminated dentin will lessen the adhesiveness of the bonded restora-tions, whether by stopping the polymerization reaction or interfering with the actual bonding mechanism,96 and there-fore the surfaces must be etched and rinsed to regain full bonding capability.102,148 Various approaches have been advo-cated to achieve this goal, such as air abrasion techniques (EtchMaster [Gorman Dental, Ann Arbor, MI, USA]) and etch-and-rinse management.
There are other problem-solving concepts that must be addressed when using composites to restore access openings in root-treated teeth. First, while there are multiple genera-tion bonding systems available for this purpose, the three-step adhesives (fourth generation) seem to work the best and

442 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
BOX 20-1 Case Study Highlighting the Problems Encountered With Failure to Restore Endodontically Treated Teeth in a Timely and Appropriate Manner
Case Study:A 49-year-old female was referred for evaluation of the mandibular right posterior teeth. She had a recent history of spontaneous pain episodes in the area and was now experiencing prolonged pain to heat. Clinical examination revealed a large carious lesion on the distal surface below the margin of the full gold crown of the mandibular right first molar (Fig. 20-1, A). Pulp sensibility testing indicated tooth number 30 was abnormally responsive to heat stimulation. The crown was removed, the caries was excavated, and complete root canal treatment was performed. The distal root was prepared for an intraradicular post, and the tooth was temporized with IRM. The patient was dismissed with the expectation that the tooth would be restored as soon as possible.
Two months later, the patient called with the complaint that the temporary filling had come out. Upon examination, the IRM was found to be intact over the mesial orifices, but the distal canal was exposed to saliva (see Fig. 20-1, B). The distal canal was immediately recleaned and reobturated, again leaving space for a post. The patient was urged to have the tooth restored immediately.
Seventeen months later, the patient was referred for evaluation of a draining sinus tract lateral to the mandibular right first molar. The tooth was now restored, and a radiograph indicated that a post had been placed in the distal canal. A large periapical lesion was identified on the same root (see Fig. 20-1, C), but there was no apparent pathosis associated with the mesial root apices. The patient recalled that again there had been a delay of several weeks before she was able to get an appointment for the restoration. Periapical surgery was performed on the distal root only (see Fig. 20-1, D), which upon
8-month reexamination appeared to have healed completely (see Fig. 20-1, E).
Nearly 9 years after the original treatment, the patient was referred again for reevaluation of the mandibular right first molar, as the referring dentist had discovered another draining tract in the buccal vestibule. The radiograph indicated that there was a periapical lesion at the apex of the mesial root which extended coronally to the furcation (see Fig. 20-1, F). Clinically, the restoration was in excellent condition without evidence of caries or marginal leakage. The mesial canals were revised nonsurgically through the existing restoration (see Fig. 20-1, G) and on reexamination 9 months later, the lesion on the mesial root appeared to be healing normally (see Fig. 20-1, H).
Problem-Solving Analysis:In retrospect, the most obvious etiology for the multiple postoperative problems was coronal leakage that occurred before the final restoration of the tooth initially. This could be attributed to an inadequate temporary restoration and prolonged delays before permanent placement of the post and crown. Leakage into the prepared post space most likely accelerated the failure of the root canal treatment in the distal root. The most reasonable explanation for the eventual failure of the root treatment of the mesial canals was residual bacteria in the pulp chamber from the original leakage problem. If the tooth had been restored immediately and periods of temporization had been avoided, none of the subsequent problems would likely have occurred. These problems are identified daily in private practice and can be prevented with a cognizant approach to the protection of all root-treated teeth with immediate attention to proper restoration.
For onlays and full crown restorations, the structural integrity of the underlying tooth structure and restorative materials is more of a concern than the structure of the crown itself. Therefore, the clinician should use a caries detector upon entry to ensure that there are no hidden carious pathways that have undermined the restoration.84,116 This examination is also enhanced with magnification (i.e., loupes or microscope). Access openings made through an existing restoration result in loss of retention92,151 and strength.54 When the access opening is restored, loss of reten-tion is reversed,92,151 and if a post is added, additional reten-tion can be gained.151
The most significant structural consideration in making access though full crowns is the presence of ceramic material. As discussed in Chapter 8, access cavities can be safely made through metalloceramic and full ceramic crowns without serious risk of fracture, although craze lines have been noted.139 Once the root canal procedures have been com-pleted, the restoration of the access cavity must be completed. Bonding to dentin deeper in the access opening is not as
effective as bonding to enamel.36 In these cases, however, there is a metalloceramic or ceramic margin. Etched ceramic materials can form a strong and durable bond with resin.67 A micromechanical bond can be obtained by roughening the porcelain with a bur, air abrasion, or etching with hydroflu-oric acid,128 but acid etching appears to be the most effective method.3,89,124,133 This acid is provided in a 10% concentra-tion in a syringe, and adherence to the manufacturer’s instructions is essential to prevent problems.8 Adhesion between a resin and porcelain may be enhanced by the use of a silane coupling agent.120 Some systems can bond well to both composites and amalgams, thereby reducing leakage with either material.31 This could provide direction for restor-ing a root-treated tooth that is not in a load-bearing area or has little contact in function, such as opposing a removable denture or partially edentulous space.
The metallic ring in the metalloceramic crowns is usually not significant when restoring an access opening. However, if the occlusal boundaries of the access opening are all metal, then some type of mechanical adhesion is necessary.89 The

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 443
A B
C
D
E
G
H
F
FIGURE 20-1 a, Preoperative radiographic image of mandibular molars. Note carious defect on distal margin of crown on the first molar. B, Two months posttreatment with degraded temporary restoration. c, A 17-month reexamination radiograph indicating lesion on distal apex. D, Immediate postsurgical radiograph. E, Eight-month postsurgical radiograph indicating healing of the surgical site. F, Nine years after the surgery, a reexamination radiograph indicates failure of the root canal treatment in the mesial canals. G, Radiograph following nonsurgical revision of mesial canals. H, Nine-month reevaluation indicating healing of the lesion on the mesial apex.

444 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
A B
D
E
C
F
G
H
FIGURE 20-2 a, Access cavity to be restored following routine root canal treatment. Sealer has been thoroughly removed with solvent. B, Acid etch. c, Placement of the bonding system. D, Light curing of bonding system. E, Placement of compomer in 1-mm increments. Each increment is light cured, creating an intracoronal barrier. F, Remainder of cavity is restored with composite resin. G, Resin restoration cured. H, Completed restoration.
resin, compomer, or MTA.* Following placement of the intracoronal barrier, the remainder of the access cavity may be restored as discussed earlier, depending on the nature of the coronal material. The technique for composite repair of the access cavity made through a gold three-quarter crown is seen in Fig. 20-2. The intracoronal barrier would be
use of burs or air-abrasion techniques is indicated; chemical adhesion is also possible with metals that form an oxide layer, but silane has no effect on bonding to metal.142
Traditionally it has been common in restorative dentistry to place a cement base for deeper preparations. A more con-temporary evolution of this concept is the intracoronal barrier as discussed above. Research has recently shown the effective-ness of sealing the canal orifices against coronal leakage with a 3-mm layer of glass ionomer cement, flowable composite *References 4, 14, 45, 63, 78, 141, 148, and 152.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 445
indicated even if the final restoration of the occlusal surface were amalgam or gold.
Problem-Solving Key Factors That Influence Restorative Choices in Anterior and Posterior Teeth
Multiple factors that must be considered in choosing the final restoration include:
• Amount of remaining sound tooth structure• Occlusal function and the use of cuspal coverage in
posterior teeth• Nature of the opposing dentition• Position of the tooth in the arch• Length, width, and curvature of the roots• Alterations in the tooth architecture caused by removal
of the roof of the pulp chamber and the loss of cusps and marginal ridges
• Changes that occur in the dentin of endodontically treated teeth, and the ability of the tooth to function under stress
• The need for crown lengthening (see Chapter 17)• The need for a ferrule to retain and stabilize the
restoration• Preservation of cervical tooth structure• Use of agents (eugenol-based) that impact on bonding
posts in the root canal55,85 and on coronal tooth structure25,27
Alterations in the tooth that result in the potential for structural weakness are not attributable to changes in moisture content,51,98 but rather these changes are attributable to architectural changes in the remaining compromised dentin, both on a macroscopic and microscopic basis.51,108 Studies in the biomechanical properties of root-treated teeth and their contralateral vital pairs indicate that teeth do not become brittle after root canal treatment, as was previously thought.118 However, the strongest tooth will always be the one in which sound dentin and enamel can be retained and used to rebuild the tooth.29,62,94,117 Multiple restorative options are available to best serve the patient’s needs; these options must be chosen carefully for each particular situation.
Restoration of Anterior TeethThe use of a composite resin in combination with dentinal bonding systems is the restorative material of choice in teeth that have intact marginal ridges, cingulum, and incisal edges.121-123,136-139 Additionally, prevention of coronal leakage is a primary concern. When restorations are placed without sufficient adherence to restorative protocols, failure is likely to result (Fig. 20-3). Because most anterior teeth experience fewer functional forces than posterior teeth do, the routine
removal of sound tooth structure in favor of extensive post-core restorations is rarely warranted.52,58,140 In this regard, many root-treated and discolored teeth may be bleached to an esthetically acceptable color by use of a chemical or “walking bleach” technique without placement of a veneer or ceramic crown.
Some root-treated anterior teeth require complete coronal coverage. The most common indications are loss of tooth structure in the incisal half of the crown from trauma or from fracture associated with large or multiple restorations. Such heavily restored teeth often become unaesthetic as well through staining and wear. Full coverage is both aesthetic and durable and should be considered routinely in these situations.
The retention of a sound cingulum in anterior teeth also appears to be a major consideration, especially as it relates to the “ferrule effect” to be discussed later in this chapter.117 Often, removal or undermining of the cingulum has been encouraged in anterior teeth that have the propensity to have two canals, such as mandibular anterior teeth. The lingual canal is usually located beneath the cingulum, and failure to find it has led to many failures in these teeth. Ironically, the destruction of the cingulum in an attempt to find the canals may adversely affect the ultimate retention of an artificial crown on these teeth. Of greater importance, however, may be the concerns that come with treatment planning the reten-tion of these teeth in the presence of significant lingual decay or, more frequently seen, lingual resorption that destroys the integrity of the cingulum.
Restoration of Posterior TeethPrimarily because of the loss of structural integrity and the amount of occlusal force during function, these teeth have a different set of restorative needs.47,115 Contemporary thought in research, clinical practice, and outcomes studies supports the placement of a restoration with full cuspal protection.5,29 Restorations of this nature are essential to prevent fracture when occlusal forces from the opposing cusps tend to wedge and separate cusp tips during function. Retrospective evalu-ation of endodontically treated teeth up to 8 years has shown that 85% of the teeth that are lost were not protected with full-coverage restorations.123 Furthermore, studies have shown that endodontically treated posterior teeth that do not receive full, protective coverage fail as much as six times more than those restored with full coverage.5 In cases of posterior teeth opposing a partial or complete denture, the forces of mastication and cuspal interdigitation may be reduced sig-nificantly, and tooth restoration with complete coronal cov-erage may or may not be warranted.
Of initial restorative concern is the seal of the pulp chamber. A separate intracoronal barrier should be placed before the construction of the final restoration begins. During core construction, care must be taken to insure that areas of deep excavation or fracture near the future crown margins are well sealed to prevent possible marginal leakage. When there is substantial remaining coronal tooth structure, any

446 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
FIGURE 20-4 Root-treated molar indicated for core build up.
restorative material can be used for the core as the support for the crown is derived principally from dentin. However, if the coronal preparation would eliminate or reduce the remaining dentin thickness to where it is of no value, then a bonded composite or core paste-type material is indicated. If the final preparation will be in sound dentin, even a glass ionomer would be appropriate as a core buildup mate-rial, however, it lacks sufficient strength as a free-standing restoration.46
Bonded composite resin cores, sometimes supported by intraradicular posts, are indicated in cases with loss of up to half of the clinical crown (Fig. 20-4).89 In cases missing more than half of the clinical crown, the physical properties of the core material become crucial to long-term survival.72 For maximum strength, bonded amalgams, composites, and core paste materials are preferred.46,60,72,103,104 Again, glass iono-mers are not considered strong enough for this purpose. From the endodontic perspective, however, direct core
A
B
C
D
FIGURE 20-3 a, Mandibular incisor with failed access restoration. B, Periapical lesion resulting from treatment failure. c, Completed revision with satisfactory intracoronal barrier and final restoration. D, Clinical view of restoration.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 447
the level of the furcation. Consider the example depicted in Fig. 20-7. To provide a restorable clinical crown and facilitate a “ferrule effect” for such (see below), a minimum of 2 mm of crown exposure above the free gingival margin would be required. On the mesial, there is only 1 mm of tooth struc-ture remaining above crestal bone. Resecting another milli-meter of crestal bone would immediately infringe on the furcation, but that is not all. Crown lengthening requires the restoration of biologic width (see Chapter 17). Biologic width is the normal physiologic distance from the gingival attach-ment to the margin of the free gingival. This would require an additional 2.5 mm of crestal bone reduction, which for this tooth is entirely unfeasible. A third consideration is rela-tively short root length. There would be a compromise between the root canal seal and post length. The treatment plan for this tooth would favor extraction (Fig. 20-7).
Although the majority of structurally compromised teeth are restored with an intraradicular post, this philosophy and clinical approach does not necessarily reinforce teeth as was once widely believed.47,48,52,121,149 In the short term, posts may be of benefit,117 with bonded posts having an impact on root strengthening initially.80 Over time, their value may be lost because of the loss of adhesion due to thermal, chemical, and mechanical stresses from the oral cavity.116,117 The routine use of posts is now believed to have a negative impact over time on the retention of teeth. Therefore, there is no value in placing posts in otherwise intact root-treated teeth that do not need core retention (Fig. 20-8).
The principal function of the post is retention of the core. There are a number of considerations in determining the indications for a post, the choice of a post, and the technique for its placement. These considerations fall into two catego-ries, restorative and endodontic.
Restorative Considerations for Post PlacementPosts should be selected or designed to preserve as much coronal tooth structure as possible. Therefore, the prepara-tion in the canal should remove as little dentin as possible. Cast posts by their very nature cannot be given a specific design because they represent the shape of the prepared root
construction without posts should be confined to the pulp chamber; occasionally, careful extension into the coronal 2 to 3 mm of the canal space may be indicated. Overzealous enlargement and extension into the canal spaces, however, can result in weakening, fracture, or perforation of the root (Fig. 20-5).
In treatment planning the restoration of posterior teeth with significant loss of coronal tooth structure, it is important to consider the amount of crown preparation that will be required once the core is placed. Although the tooth may have a satisfactory core buildup, there may be insufficient tooth structure after preparation to retain it. The result is frequently a complete fracture of the crown at the level of the gingival margin. Neither dentinal bonding nor retentive pins appear to be a solution for the retention of large cores in teeth with minimal coronal dentin (Fig. 20-6).
Intraradicular PostsBoth anterior and posterior teeth that lack sufficient remain-ing coronal dentin to place a direct core must be evaluated carefully for restorability. Crown lengthening and orthodon-tic extrusion (see Chapter 17) are useful adjuncts for many compromised teeth, but some limitations exist. For example, crown lengthening cannot be effectively carried out below
FIGURE 20-5 Amalgam core overzealously extended into canal orifices, resulting in weakening of tooth structure and fracture of the distal root.
A B C
FIGURE 20-6 a, A prosthetic crown fractured off due to insufficient remaining tooth structure. B, The addition of retentive pins fails to compensate for lack of coronal tooth structure. c, Fracture of thin palatal tooth structure led to failure of entire crown.

448 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
The choice of a post system can also be greatly influenced by the installation stresses. Cement viscosity, cement type, the option of intracanal bonding, canal cleanliness, and general fit of the post must be considered in treatment plan-ning the final restoration (see Table 20-1). The parallel-threaded post systems have relatively low installation and functional stresses compared with the tapered, self-threading systems. Other systems have similar characteristics depending on their use.
Bonded carbon fiber (no longer black), glass fiber, quartz fiber, and silicon fiber posts have also been advocated. The chief benefit is that they are white and do not detract from the esthetics of full ceramic crowns. The purported structural benefit of these post types is a modulus of elasticity that is similar to dentin. However, long-term randomized clinical trials assessing the efficacy and outcomes of using these types of posts are lacking, as the use of fiber posts in endodontically treated teeth with full crowns has been studied primarily in vitro.
canal in conjunction with a core buildup. They tend to be the most conservative type of post, respecting the remaining tooth structure.89 Because of the tapered shape, they are less retentive and may induce wedging forces, depending on cement viscosity. Retention is highly dependent on the cementing media or irregularities incorporated into the post design to enhance stability,64 but at least one study indicates that clinically there were no problems with custom posts of adequate length.147
Threaded posts are the most retentive (Table 20-1). Although highly retentive, some threaded posts may predis-pose to root fracture (Fig. 20-9 [see Chapter 4]). Parallel-sided serrated posts are also highly retentive64 but have the disadvantage that apically, the preparation may become too large for a narrow tapering root. Tapered posts have also been successful in selected cases but are the least retentive and rely heavily on the integrity and strength of the cementing medium. Factors such as roughening or notching the post may increase retention.
FIGURE 20-7 A molar tooth with anatomically short roots. There is insufficient coronal tooth structure for the ferrule effect and to retain a core. There is insufficient root length for both post retention and adequate root canal filling. The patient was advised to have the tooth extracted.
FIGURE 20-8 Root-treated maxillary incisor with an intact crown. The post is redundant and not indicated.
TaBlE 20-1 Characteristics of Generic Post Systems
Type Retention Installation Stresses Functional Stresses
Tapered smooth Low Little or none Wedging effect
Parallel serrated Higher Little or none Uniformly distributed through the cement layer
Tapered self-threaded Intermediate; affected by high installation stresses
Very high; wedging stresses High stresses; accentuates installation wedging
Parallel threaded Highest Low after counter-rotation Relatively low; transmitted through individual threads
Parallel serrated tapered end Similar to parallel serrated Little or none Wedging effect at apex
Cast post Less retentive than parallel Little or none Wedging effect

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 449
would result in post lengths of 7.5 to 10 mm. Ratios of half, two-thirds, or three-quarters the length of the root have also been advocated.47 If the average root lengths were considered within these ratios, it would provide a post length similar to the two-thirds ratio recommendation.
A number of studies have confirmed the relationship between post length and retention. A sampling of four of these studies indicates that by increasing post length from 5 mm to 8 mm, retention increased by 33% to 47%.* There-fore post lengths around 9 to 10 mm for anterior teeth and 8 mm for posterior teeth would appear to be adequate and effective when a post is needed to restore the tooth (Fig. 20-10).
Fracture resistance was shown to be improved, and the fractured tooth was judged to be restorable more often in teeth with fiber posts.111 On the other hand, the value of flexibility is questionable with respect to cement or bonding seals at the interface of dentin and core material.32 As with all methods of restoring root-treated teeth, preservation of as much coronal tooth structure as possible would be an impor-tant adjunct to the success of these posts. When removal is necessary, the ultrasonic instrument has been found to be effective.37,117
Zirconium and ceramic posts are also available. Although similar in esthetic application to fiber posts, these materials have less tensile strength; consequently, more bulk is required. They are also weaker than metal posts, so along with an increase in diameter comes more removal of sound dentin in the root than a corresponding metal or fiber design. A second disadvantage is that they are extremely difficult to remove if a fracture occurs. The posts cannot be etched and therefore cannot be bonded, which may impact negatively on core retention.24 While it might be possible to grind the remaining ceramic material from the canal, at very best, the post prepa-ration will inevitably become larger as a result. Zirconium is virtually impossible to grind. A fractured zirconium post would most likely result in extraction of the tooth.
From a restorative viewpoint, recommendations for post length were empirically derived from clinical experience. While numerous clinicians believed that the post should roughly equal the length of the crown,* there are abundant guidelines for post length, each having its own research or empirical support.47 In an effort to arrive at a consensus, a table of average measurements of crowns and roots was devised almost 30 years ago.115 Crowns of maxillary anterior teeth are around 10 mm, while the mandibular teeth mea-sured around 9 mm. The posterior teeth have crowns averag-ing around 7.5 mm. If these measurements were used, this
A B
FIGURE 20-9 a, Kurer anchor. B, Threaded posts providing active retention are associated with increased incidence of root fracture.
*References 9, 15, 35, 50, 57, 109, 112, 114, 115, 119, 131, and 134. *References 26, 30, 70, 73, 110, 125, and 126.
FIGURE 20-10 Maxillary right lateral incisor restored with an intraradicular post of appropriate length and a composite core.

450 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
FIGURE 20-12 A grossly undersized post fails to provide retention.
roots,66,113 and prevent coronal leakage.6 However, this tech-nique requires extra steps in cleaning and preconditioning of the dentinal wall. Failure of the pretreatment agents to reach all areas of the preparation or contamination of either the post or the canal will prevent bonding. Self-curing resins would be preferred over light-cured varieties because of the lack of light penetration.41 There is also the question of the durability of the bond. Additionally, degradation over time may characterize intracanal bonding procedures.144 The dis-advantages of this approach may defeat the theoretical benefits.
The eugenol-containing cements used for root canal obtu-ration are thought to inhibit polymerization of resin cements that are used to cement posts, and for that matter seal an access opening. Therefore the walls of the canal and coronal portion of the tooth must be cleaned.22,79,80,83,148 The use of chlorhexidine to rinse the canal space prior to post and core placement will assist in bacterial control117 and enhance the bonding that is desired. Chlorhexidine may leave some surface debris, but it does not appear to effect the shear bond strength.100
Clinically, the adaptation of the post to the canal wall is important. Grossly undersized posts cannot possibly provide retention for the core (Fig. 20-12). In large canals, there may be no effective way to place a post (Fig. 20-13). This is espe-cially true in mandibular second molars that exhibit a C-shaped canal system or any molar that has ribbon-shaped canals (see Chapter 13). When the attempt is made to place a post in a very large canal, it often occurs that the post is cemented to gutta-percha and nothing else. There is no
Clinical experience indicates that short posts tend to become easily dislodged (Fig. 20-11). Moreover, there is evidence to conclude that a short post may contribute to vertical root fracture during the period of loosening and dislodgement.61,126 The often insurmountable problem is the anatomically short tooth and how to restore it based on remaining tooth structure and patient function. Again, pres-ervation of coronal tooth structure is one important strategy. Less stress would be put on the post core if crown retention depended on the remaining dentin of the clinical crown. Therefore, teeth with roots need to be assessed fully during treatment planning, and in this case extraction may be in the patient’s best interest.
In vitro studies on the luting of posts do not present a clear preference for a cement type, although any of the cements can be used if the proper principles are followed.117 Zinc phosphate and glass ionomer cements have been used for many years with a good deal of clinical success; one caution, however, with glass ionomer cement is the setting time, which may take days for a complete set.81 Continued buildup and preparation on the day of cementation may permanently weaken the cement.
Presently there appears to be a trend toward the use of resin-modified glass ionomer and resin cements.88,97 These materials provide initial increased retention and tend to leak less than other cements,6,80,107 but they are more technique sensitive, requiring extra steps in the preparation of the canal walls and efficiency in placement and cementation. While it is thought that eugenol-based root canal sealers would inhibit resin polymerization, intracanal dentinal bonding may actually increase retention,41,65,143 strengthen
FIGURE 20-11 Maxillary canine restored with a post of inadequate length.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 451
increased with crown margins placed on ferrules of 1 to 2 mm in width.101,121,127,153 As discussed in the earlier section on core buildups without posts, the coronal tooth structure must be assessed before placing the post and core to envision how much will remain after crown preparation. Although the crown preparation may appear to have the desired ferrule effect, in actuality, the observed dentin may now be very thin and weak, contributing very little to the structural integrity of the completed restoration. Post failures are common once the dentin fractures (Fig. 20-16).
The ferrule also protects against coronal leakage. In teeth restored without a ferrule, occlusal loading will cause failure of the cement seal between the core and the dentinal wall. Experimentally, this has been found to be visually undetect-able and results in coronal leakage into the post space over time.44 These cases are usually discovered clinically, when the entire post-core-crown becomes loose (Fig. 20-17; see Fig. 20-16, A and B) or there is a root fracture (Fig. 20-18). A second disastrous form of failure is metal fatigue and fracture of the post itself (Fig. 20-19). A common denominator in examining the core inside the crown is the lack of adequate extension over tooth structure identical to the failures of cores alone (see Fig. 20-6) and post cores (see Figs. 20-16 and 20-17). Fortunately, most post fragments can be removed, but unless more tooth structure can be included under the next restoration, a recurrence of post fracture is likely. In cases where there is little remaining clinical crown, surgical crown lengthening is recommended. The restoration could also include the use of multiple posts (Fig. 20-20) if appropriate to support the large core that is needed.
Endodontic Considerations for Post PlacementAlthough many teeth cannot be restored by any means other than the use of an intraradicular post, there are a number of significant risks and prognostic concerns even with their use, although the restorative requirements are satisfied. The key
evidence to suggest that this provides any more support for the core-crown than the grossly undersized post seen in Fig. 20-12. In addition, placing a post in gutta-percha can lead to a catastrophic failure of the treatment rendered (Fig. 20-14).
The ferrule is a dentinal portion of a crown preparation immediately above the finish line (Fig. 20-15). According to studies, the minimum width of the ferrule should be 1.5 to 2 mm from the margin of the core to the finish line of the preparation.75 In the case of a tooth with a post-core build up, studies have shown that fracture resistance is dramatically
FIGURE 20-13 Developing post retention in large-diameter canal spaces is difficult.
FIGURE 20-14 There is no evidence to support placement of a small-diameter post into gutta-percha.
FIGURE 20-15 Ferrule is adequate to provide support for the crown and ensure a seal of the core-dentin interface.

FIGURE 20-18 Radiograph that verifies the nature of the fracture abutment, again on a mandibular premolar bridge abutment. Multiple issues are involved with these occurrences: namely, length of bridge span, lack of ferrule, poor root length, improper occlusal forces (especially during function), improper use of posts, and failure to consider double abutments.
FIGURE 20-19 A fractured intraradicular post in a maxillary left lateral incisor. The restoration had no ferrule.
B
C
A
FIGURE 20-17 a, Right mandibular first molar restored with a post, core, and full gold crown. B, Marginal leakage extended to the post space causing failure of the luting cement. c, Examination of crown and the post core indicates the lack of sufficient ferrule circumferentially.
A B
FIGURE 20-16 a, Failed post core restoration. An intraradicular post cannot compensate for lack of sufficient coronal tooth structure. B, Loss of bridge abutment due to fracture of dentin (arrow) below the crown that caused the posts to loosen in the tooth.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 453
A B
C D
FE
FIGURE 20-20 a, Mandibular left second molar which was an abutment for a failed bridge. B, Note the lack of coronal tooth structure in the clinical crown. c, Postoperative photograph of the molar following surgical crown lengthening. D, It is possible to use two posts in this case. E, Completed coronal reconstruction and crown preparation. Note the dentinal portion of the preparation for the ferrule. F, Radiograph of the same tooth depicted in E. Note the sufficient post lengths.
problem-solving concept in this area is prevention. Most of the problems described in this section will seriously affect prognosis or require immediate extraction of the tooth.
The discussion of coronal leakage in the section on tem-porary fillings applies to permanent restorations as well. Timely if not immediate restoration of any prepared post space is one of the best ways to prevent coronal leakage, the effects of which may not appear for a considerable time after treatment. In the same manner, any avenue of leakage that might remain or develop postoperatively will result in failure of the root canal procedures, with predictable evidence for persistent of or a new periapical pathosis. Likewise, coronal leakage to the site of a lateral canal must always be suspected when a lesion develops laterally at the level of the terminus
of a post, and this finding may be misdiagnosed as being due to a post perforation or a periodontal pocket (Fig. 20-21).
The amount of filling in the root canal that is left after post space preparation is critical to the prognosis of treat-ment. Most authors have concluded that 4 to 5 mm of root filling material is sufficient to maintain the apical seal (Fig. 20-22).62 Every effort must be made to resist the temptation to extend the post preparation beyond a radiographically predetermined level as the seal of the root canal filling may be compromised (Fig. 20-23). In these cases, if the root canal treatment fails, revision is difficult and demanding. There are only two options, nonsurgical or surgical revision. When a post is present, removal is difficult, and many cases either require or result in the removal of a satisfactory restoration

454 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
FIGURE 20-21 A radiolucency associated with a lateral canal is likely communicating with unfilled canal space.
FIGURE 20-22 A completed post core restoration with appropriate post length and preservation of root canal fillings.
just to remove the post. Periapical surgery, on the other hand, is compromised because of the difficulty in preparing the apex for a root-end filling (Fig. 20-24).
In the anatomically short-rooted tooth, a conflict arises between adequacy of post length for core retention and ade-quacy of root canal filling to ensure the integrity of the seal. The root canal seal cannot be compromised, and therefore if there are no alternatives for core retention or exposure of more clinical crown, extraction should be considered as was discussed with Fig. 20-7.
A B
FIGURE 20-23 a and B, Overzealous extension of the post that resulted in perforation of the apex. Note complete displacement of the minimal apical gutta-percha in the maxillary left lateral incisor. Apical surgery complicated by the difficulty of removing the metallic post material to reseal the apical foramina. (B, Courtesy Dr. Rachel Hogan.)
A recent clinical study has confirmed what many clinicians have observed empirically. Unfilled root canal space that might be left between the post and the residual gutta-percha filling material may negatively affect the long-term prognosis of the tooth.91 In this study, 94 root-treated teeth were restored with post and cores and followed for 5 years. Teeth with no gap were found to be 83% successful. Teeth with a gap of over 2 mm were found to be 29% successful. Although the cause of failure was not the object of this study, a number of causes can be identified or at least suspected. The first is leakage into the canal. As was discussed earlier in the section on temporary fillings, studies indicate that canals with less gutta-percha filling materials, such as those prepared for intraradicular posts, are more susceptible to leakage.1,86
Secondly, lateral canals are not uncommon at the midroot levels of teeth. This is usually about the level that

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 455
BA
FIGURE 20-24 a, Inadequate apical filling due to overextended post. B, Postoperative radiograph documenting the difficulty of placing the root-end filling.
intraradicular post preparations terminate (Fig. 20-25). Occasional lateral abscesses are found to be caused by the bacteria and tissue debris that emanates from lateral canals that communicate with unfilled and probably contaminated spaces in the main canal (Fig. 20-26).
A study of the timing of post space preparation relative to completion of the root canal treatment indicates that immediate preparation has no effect on the newly created
apical filling and its seal.39 This supports the treatment plan of immediate restoration and avoids any period of tem-porization that could invite coronal leakage. Prior to initiat-ing any treatment, an accurate radiograph of the tooth should be measured to determine an approximate depth to which the post should extend. Any root curvature should be noted so that the preparation will stop before exiting the canal space. Similarly, the general anatomy of the root should be noted to look for possible indications of lateral fluting, lateral canals, or generally thin root structure.50,51 These factors
FIGURE 20-25 Lateral canals at the level of the termination of the post.
FIGURE 20-26 A lateral radiolucency presumed to be associated with a lateral canal communicating with unfilled canal space between the post and the root filling material.

456 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
A B C
FIGURE 20-27 a, A lateral perforation to the mesial of molar root. The operator failed to negotiate the root curvature. B, A lateral perforation in a maxillary incisor due to the use of an excessively large-diameter post for the root. c, A furcation perforation in the mesial root of a mandibular molar. Note the thin mesial-distal width and the curvature of the root. Post placement should have been confined to the distal root alone.
would suggest a smaller-diameter post than might otherwise be indicated.
Removing the gutta-percha prior to the use of rotary instruments to enlarge the canal space has always been a safe approach to creating post space. The various techniques described in Chapter 14 for the removal of root filling mate-rials in the process of treatment revision will apply to prepa-ration for posts as well. A hot endodontic plugger or heating device (System B or Touch ’N Heat [SybronKerr, Orange, CA, USA]; BeeFill 2in1 [VDS, Munich, Germany]; Cala-musDual 3D Obturation System [Dentsply Tulsa Dental Specialties, Tulsa, OK, USA]) are ideal for this purpose. This can be followed by Gates-Glidden burs, Peeso burs, and solvents, depending on the root shape and canal size. Once the canal space is free from most of the filling materi-als, larger burs that come with the prefabricated post kits or drills that can be used safely will follow the prepared space with much less risk of perforation. Before their use, make sure the canal is clean and dry and the drill will be centered in the canal. The gutta-percha should remain visible and centered at the base of the preparation throughout the process.
Unfortunately, perforation of the root during post space preparation occurs and is a disastrous event that diminishes the prognosis for tooth retention. Posts and post preparations will not follow curvatures in the root, so preoperative assess-ments should prevent continued penetration past the point where straight-line enlargement is possible (Fig. 20-27). For example, in the palatal canal of maxillary molars, it is not possible to appreciate buccal-palatal curvature radio-graphically. As a consequence, it is extremely important to remove the gutta-percha filling and either visualize the
direction of the canal or use an endodontic file to explore the curvature before beginning post preparation. Perforations will usually occur on the furcation side of the palatal root (Fig. 20-28), which will not be evident on a film (Fig. 20-29, A). These lesions generally drain to the palatal surface around the mesial or distal aspect of the root (see Fig. 20-29, B), and probing will often identify the tract (see Fig. 20-29, C ).
FIGURE 20-28 A post perforation to the buccal surface of the palatal root of a maxillary molar.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 457
A
C
B
FIGURE 20-29 a, A clinical case of a perforated palatal root. The etiology is difficult to discern on the radiograph. B, Clinically there is usually a sinus tract. c, Narrow probings into the furcation space on the mesial palatal or distal palatal line angles.
FIGURE 20-30 Occasionally, a palatal post perforation can be suspected by the divergence of the post from the filled canal.
FIGURE 20-31 Perforation of the palatal root is suspected from loss of furcation bone. There is no indication of advanced periodontal disease.
Radiographically, if the post space perforation is on the furca-tion or the palatal side of the root, it may not deviate with an angled film. If the perforation tends to go either to the distal or mesial, the post may appear to deviate from the direction of the canal (Fig. 20-30). Another possible clue to a furcation perforation of the palatal root is bone loss in the clinical absence of periodontal disease (Fig. 20-31).
Perforations can occur as a result of unanticipated ana-tomic variation, such as deep fluting on the mesial or distal surfaces of posterior teeth (Fig. 20-32). Strip perforations
can also occur during an attempt to place a post that is too large for the root (Fig. 20-33). It is also possible to perforate into the furcation of maxillary premolars, because the anatomy of that area cannot be visualized radiographically (Fig. 20-34).
Small perforations detected early can often be repaired with MTA in the base of post preparation. However, the prognosis diminishes rapidly with increasing size of the

458 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
FIGURE 20-33 Grossly oversized post in the distal root of the left mandibular first molar, resulting in a strip perforation.
FIGURE 20-32 Extrusion of luting cement through a stripping perforation. The post diameter is too large for the root size.
FIGURE 20-35 Post perforation in the marginal periodontium. It is often possible to treat the problem with a combination of crown lengthening and placement of a longer crown. An alternative approach would be orthodontic extrusion.
FIGURE 20-34 Post perforation into the furcation of a maxillary first premolar.
perforation. Irritating medicaments in the canal or coronal leakage resulting in infection of the adjacent periodontal tissues will also reduce the probability of successful repair.
Unfortunately, the majority of perforations occur through misalignment of post drills or beginning a post preparation without prior removal of the gutta-percha filling. If the resultant perforation is above or at crestal bone level, repair will generally be possible without a serious effect on the prognosis (Fig. 20-35). Deeper perforations that do not affect the marginal or sulcular attachment can also be repaired with an excellent long-term prognosis if the defect is small and accessible (Fig. 20-36). The techniques for repair of these types of defects are beyond the scope of this book, but other examples106 of this type of surgery can be found in Chapter 18.
Regardless of size, perforations into the furcation do not bode well for a positive outcome (Fig. 20-37). If small and repaired immediately, the prognosis may be good. Attempts
at internal repair of older perforations that have become infected are not usually successful, most likely due to the difficulty of adequate cleaning and disinfection of the perfo-ration site internally.
Similarly, surgical repair is difficult due to the inaccessibil-ity of the defect and the destruction of the attachment in the process (see Chapter 8).
Occasionally, gross perforations are encountered for which extraction is the only option. Typically, at the point of discovery, irreversible destruction of the periodontium adja-cent to the perforation has taken place, resulting in a perma-nent periodontal defect. Repair of the perforation at this point is futile (Fig. 20-38).

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 459
B
CA
FIGURE 20-36 a, A midroot perforation to the labial. B, Probings are normal, indicating the perforation is located below the level of the marginal attachment. Repair with mineral trioxide aggregate (MTA) would have an excellent prognosis for healing. c, One-year reevaluation after perforation repair with MTA. The lesion has completely resolved clinically.
FIGURE 20-37 Perforations into the furcation are difficult to repair. With a post protruding through a perforation, repair is virtually impossible.

460 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
FIGURE 20-39 An asymptomatic root-treated tooth with gutta-percha that is exposed to saliva.
A
B
FIGURE 20-38 a, Some perforations cannot be explained. B, Extraction is the only remedy for large perforations.
Exposed and Contaminated Root Fillings Due to Coronal Leakage
Occasionally, fractured or carious teeth that have had previ-ous root canal treatment require reconstruction. There may be no symptoms, and the radiograph may give no evidence of apical pathosis, but the gutta-percha filling material has been exposed to saliva and bacteria, often for unknown time periods (Fig. 20-39). The dilemma is whether or not such a tooth can be restored without nonsurgical root canal revision (see Chapter 5). Even if the crown had come off the same day as the examination, it is entirely unknown
if the tooth had been cracked or if the tooth-restorative margins had been leaking. Usually, most teeth will have clinical and radiographic signs of failure within months of a crown failure, but even this finding does not always occur (Fig. 20-40).
The weight of scientific evidence cited earlier concerning coronal leakage leaves little doubt that the case in question is in the process of failing. Placement of an intraradicular post
A
B
FIGURE 20-40 a, Periapical lesion resulting from coronal leakage. B, Swelling of sinus tract stoma (arrow) at gingival margin.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 461
19. Belli S, Zhang Y, Pereira PN, et al: Regional bond strengths of adhesive resins to pulp chamber dentin, J Endod 27:527-532, 2001.
20. Belli S, Zhang Y, Pereira PN, et al: Adhesive sealing of the pulp chamber, J Endod 27:520-526, 2001.
21. Black GV: An investigation of the physical characteristics of the human teeth in relation to their diseases, and to practical dental operations, together with the physical characters of filling- materials, Dent Cosmos 37:353-421, 1885.
22. Boone KJ, Murchison DF, Schindler WG, et al: Post retention: the effect of sequence of post-space preparation, cementation time, and different sealers, J Endod 27:768-771, 2001.
23. Breschi L, Mazzonie A, Ruggeri A, et al: Dental adhesion review: aging and stability of the bonded interface, Dent Mater 24:90-101, 2008.
24. Butz F, Lennon AM, Heydecke G, et al: Survival rate and fracture strength of endodontically treated maxillary incisors with moderate defects restored with different post-and-core systems: an in vitro study, Int J Prosthodont 14:58-64, 2001.
25. Campos EA, Correr GM, Leonardi DP, et al: Chlorhexidine diminishes the loss of bond strength over time under simulated pulpal pressure and thermo-mechanical stressing, J Dent 37:108-114, 2009.
26. Carvalho CN, de Oliveira Bauer JR, Loquercio AD, et al: Effect of ZOE temporary restoration on resin-dentin bond strength using different adhesive strategies, J Esthet Restor Dent 19(3):144-153, 2007.
27. Chaiyabutr Y, Lois JC: The effects of tooth preparation cleansing protocols on the bond strength of self-adhesive resin luting cement to contaminated dentin, Oper Dent 33:556-563, 2008.
28. Chandler NP, Heling I: Efficacy of three cavity liners in eliminat-ing bacteria from infected dentinal tubules, Quintessence Int 26:655-659, 1995.
29. Cheung GS, Chan TK: Long-term survival of primary root canal treatment carried out in a dental teaching hospital, Int Endod J 36:117-128, 2003.
30. Colley IT, Hampson EL, Lehman ML: Retention of post crowns: an assessment of the relative efficiency of posts of difficult shapes and sizes, Brit Dent J 124:63-69, 1968.
31. Cooley RL, Tseng EY, Barkmeier WW: Dentinal bond strength and micro leakage of a 4-meta adhesive to amalgam and compos-ite resin, Quintessence Int 22:979-983, 1991.
32. Cury AH, Goracci C, de Lima Navarro MF, et al: Effect of hygroscopic expansion on the push-out resistance of glass iono-mer-based cements used for the luting of glass fiber posts, J Endod 32:537-540, 2006.
33. Dahlgren BE: The root canal problem. Asepsis and sterilization, Aust J Dent 21:79-84, 1917.
34. Demarchi MG, Sato EF: Leakage of interim post and cores used during laboratory fabrication of custom posts, J Endod 28:328-329, 2002.
35. Demas NC: Direct impression for cast Richmond crown using acetate crown forms, Dent Dig 63:258-259, 1957.
36. De Munck J, Van Meerbeek B, Yoshida Y, et al: Four-year water degradation of total-etch adhesives bonded to dentin, J Dent Res 82:136-140, 2003.
37. de Rijk WG: Removal of fiber posts from endodontically treated teeth, Am J Dent 13(Spec No):19B-21B, 2000.
38. Fabianelli A, Kugel G, Ferrari M: Efficacy of self-etching primer on sealing margins of Class II restorations, Am J Dent 16:37-41, 2003.
would greatly complicate the eventual need for revision. Most likely, the treatment plan would be apical surgery. At the time of diagnosis, revision would be relatively simple, perhaps not even requiring anesthesia.
REfEREnCEs1. Abramovitz I, Lev R, Fuss Z, et al: The unpredictability of seal
after post space preparation: a fluid transport study, J Endod 27:292-295, 2001.
2. Abramovitz I, Tagger M, Tamse A, et al: The effect of immediate vs. delayed post space preparation on the apical seal of a root canal filling: a study in an increased-sensitivity pressure-driven system, J Endod 26:435-439, 2000.
3. Aida M, Hayakawa T, Mizukawa K: Adhesion of composite to porcelain with various surface conditions, J Prosthet 73:464-470, 1995.
4. Al-Hezaimi K, Naghshbandi J, Oglesby S, et al: Human saliva penetration of root canals obturated with two types of mineral trioxide aggregate cements, J Endod 31:453-456, 2005.
5. Aquilino SA, Caplan DJ: Relationship between crown placement and the survival of endodontically treated teeth, J Prosthet Dent 87:256-263, 2002.
6. Bachicha WS, DiFiore PM, Miller DA, et al: Microleakage of endodontically treated teeth restored with posts, J Endod 24:703-708, 1998.
7. Balto H: An assessment of microbial coronal leakage of temporary filling materials in endodontically treated teeth, J Endod 28:762-764, 2002.
8. Barghi N: To silanate or not silanate: making a clinical decision, Compend Contin Educ Dent 21:659-662, 664, 2000.
9. Barker BCW: Restoration on non-vital teeth with crowns, Aust Dent J 8:191-200, 1963.
10. Barkhordar RA, Kempler D: Microleakage of endodontic access cavities restored with composites, J Calif Dent Assoc 25(3):215-218, 1997.
11. Barrieshi KM, Walton RE, Johnson WT, et al: Coronal leakage of mixed anaerobic bacteria after obturation and post space prepa-ration, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 84:310-314, 1997.
12. Barthel CR, Strobach A, Briedigkeit H, et al: Leakage in root coronally sealed with different temporary fillings, J Endod 25:731-734, 1999.
13. Barthel CR, Zaritzki FF, Raab WH, et al: Bacterial leakage in roots filled with different medicaments and sealed with cavit, J Endod 32:127-129, 2006.
14. Barthel CR, Zimmer S, Wussogk R, et al: Long-term bacterial leakage along obturated roots restored with temporary and adhe-sive fillings, J Endod 27:559-562, 2001.
15. Baumhammers A: Simplified technique for a one-unit cast dowel crown, Dent Dig 68:468-472, 1962.
16. Beach CW, Calhoun JC, Branwell JD, et al: Clinical evaluation of bacterial leakage of endodontic temporary filling materials, J Endod 22:459-462, 1996.
17. Baldissara P, Comin G, Martone F, et al: Comparative study of the marginal microleakage of six cements in fixed provisional crowns, J Prosthet Dent 80:417-422, 1998.
18. Bayindir R, Akyil MS, Bayindir YZ: Effect of eugenol and non-eugenol containing temporary cement on permanent cement retention and microhardness of cured composite resin, Dent Mater J 22:592-599, 2003.

462 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
60. Howdle MD, Fox K, Youngson CC: An in vitro study of coronal microleakage around bonded amalgam coronal-radicular cores in endodontically treated molar teeth, Quintessence Int 33:22-29, 2002.
61. Hunter AL, Feiglin B, Williams JF: Effects of post placement on endodontically treated teeth, J Prosthet Dent 62:166-172, 1989.
62. Isidor F, Brondum K, Ravnholt G: The influence of post length and crown ferrule length on the resistance to cyclic loading of bovine teeth with prefabricated titanium posts, Int J Prosthodont 12:78-82, 1999.
63. John AD, Webb TD, Imamura G, et al: Fluid flow evaluation of Fuji triage and gray and white ProRoot mineral trioxide aggregate intraorifice barriers, J Endod 34:830-832, 2008.
64. Johnson JK, Sakumura JS. Dowel form and tensile force, J Pros-thet Dent 40:645-649, 1978.
65. Junge T, Nicholls JI, Phillips KM, et al: Load fatigue of compro-mised teeth: a comparison of 3 luting cements, Int J Prosthodont 11:558-564, 1998.
66. Katebzadeh N, Dalton BC, Trope M: Strengthening immature teeth during and after apexification, J Endod 24:256-259, 1998.
67. Kato H, Matsumura H, Tanaka T, et al: Bond strength and dura-bility of porcelain bonding systems, J Prosthet Dent 75:163-168, 1996.
68. Kazemi RB, Safavi K, Spangberg LS: Assessment of marginal stability and permeability of an interim restorative endodontic material, Oral Surg Oral Med Oral Pathol 78:788-796, 1994.
69. Khayat A, Lee SJ, Torabinejad M: Human saliva penetration of coronally unsealed obturated root canals, J Endod 19:458-461, 1993.
70. Knight JS, Sneed WD, Wilson MC: Strengths of composite bonded to base metal alloy using dentin bonding agents, J Pros-thet Dent 84:149-153, 2000.
71. Koagel SO, Mines P, Apicella M, et al: In vitro study to compare the coronal microleakage of Tempit Ultra-F, Tempit, IRM, and Cavit by using the fluid transport model, J Endod 34:442-444, 2008.
72. Kovarik RE, Breeding LC, Caughman WF: Fatigue life of three core materials under simulated chewing conditions, J Prosthet Dent 68:584-590, 1992.
73. Krupp JD, Caputo AA, Trabert KC, et al: Dowel retention with glass ionomer cement, J Prosthet Dent 41:163-166, 1979.
74. Lee Y-C, Yang S-F, Hwang Y-F, et al: Microleakage of endodontic temporary restorative materials, J Endod 19:516-520, 1993.
75. Libman WJ, Nicholls JI: Load fatigue of teeth restored with cast posts and cores and complete crowns, Int J Prosthodont 1:155-161, 1995.
76. Magura ME, Kafrawy AH, Brown CE, Jr, et al: Human saliva coronal microleakage in obturated root canals: an in vitro study, J Endod 17:324-331, 1991.
77. Mah T, Basrani B, Santos JM, et al: Periapical inflammation affecting coronally inoculated dog teeth with root fillings aug-mented by white MTA orifice plugs, J Endod 29:442-446, 2003.
78. Maloney SM, McClanahan SB, Goodell GG: The effect of thermocycling on a colored glass ionomer intracoronal barrier, J Endod 31:526-528, 2005.
79. Mannocci F, Ferrari M, Watson TF: Intermittent loading of teeth restored using quartz fiber, carbon-quartz fiber, and zirconium dioxide ceramic root canal posts, J Adhes Dent 1:153-158, 1999.
80. Mannocci F, Ferrari M, Watson TF: Microleakage of endodonti-cally treated teeth restored with fiber posts and composite cores after cyclic loading: a confocal microscopic study, J Prosthet Dent 85:284-291, 2001.
39. Fan B, Wu MK, Wesselink PR: Coronal leakage along apical root fillings after immediate and delayed post spaces preparation, Endod Dent Traumatol 15:124-127, 1999.
40. Fathi B, Bahcall J, Maki JS: An in vitro comparison of bacterial leakage of three common restorative materials used as an intra-coronal barrier, J Endod 33:872-874, 2007.
41. Ferrari M, Vichi A, Grandini S: Efficacy of different adhesive techniques on bonding to root canal walls: an SEM investigation, Dent Mater 17:422-429, 2001.
42. Fonseca RB, Martins LR, Quagliatto PS, et al: Influence of pro-visional cements on ultimate bond strength of indirect composite restorations to dentin, J Adhes Dent 7(3):225-230, 2005.
43. Fox K, Gutteridge DL: An in vitro study of coronal microleakage in root canal treated teeth restored by the post and core tech-nique, Int Endod J 30:361-368, 1997.
44. Freeman MA, Nicholls JI, Kydd WL, et al: Leakage associated with load fatigue-induced preliminary failure of full crowns placed over three different post and core systems, J Endod 24:26-32, 1998.
45. Galvan RR, Jr, West LA, Liewehr FR, et al: Coronal microleakage of five materials used to create an intracoronal seal in endodonti-cally treated teeth, J Endod 28:59-61, 2002.
46. Gateau P, Sabek M, Dailey B: In vitro fatigue resistance of glass ionomer cements used in post and core applications, J Prosthet Dent 2001;86:149-155.
47. Goodacre CJ, Baba NZ: Restoration of endodontically treated teeth. In Ingle JI, Bakland LK, Baumgartner JC, editors: Ingle’s endodontic 6, Hamilton, Ontario, 2008, BC Decker Inc.
48. Goodacre CJ, Bernal G, Rungcharassaeng K, et al: Clinical com-plications in fixed prosthodontics, J Prosthet Dent 90:31-41, 2003.
49. Goto Y, Ceyhan J, Chu SJ: Restorations of endodontically treated teeth: new concepts, material, and aesthetics, Pract Proced Aesthet Dent 21(2):81-89, 2009.
50. Gutmann JL: Preparation of endodontically treated teeth to receive a post-core restoration, J Prosthet Dent 38:413-419, 1977.
51. Gutmann JL: The dentin-root complex: anatomical and biologic considerations in restoring endodontically treated teeth, J Pros-thet Dent 67:458-467, 1992.
52. Guzy GE, Nichols JI: In vitro comparison of intact endodonti-cally treated teeth with and without endo-post reinforcement, J Prosthet Dent 42:39-44, 1979.
53. Gwinnett JA, Tay FR, Pang KM, et al: Comparison of three methods of critical evaluation of microleakage along restorative interfaces, J Prosthet Dent 74575-74585, 1995.
54. Hachmeister KA, Dunn WJ, Murchison DF, et al: Fracture strength of amalgam crowns with repaired endodontic access, Oper Dent 27:254-258, 2002.
55. Hagge MS, Wong RD, Lindemuth JS: Effect of three root canal sealers on the retentive strength of endodontic posts luted with a resin cement, Int Endod J 35:372-378, 2002.
56. Hansen SR, Montgomery S: Effect of restoration thickness on the sealing ability of TERM, J Endod 19:448-452, 1993.
57. Healey HJ: Coronal restoration of the treated pulpless tooth, Dent Clin N Amer 1:885-896, 1957.
58. Heydecke G, Butz F, Strub JR: Fracture rate and survival rate of endodontically treatment maxillary incisors with approximal cavities after restoration with different post and core systems: an in-vitro study, J Dent 29:427-433, 2001.
59. Hosoya Y, Taguchi T, Tay FR: Evaluation of a new caries detecting dye for primary and permanent dentin, J Dent 35:137-143, 2007.

chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth 463
81. Matsuya S, Maeda T, Ohta M: IR and NMR analyses of harden-ing and maturation of glass-ionomer cement, J Dent Res 75:1920-1927, 1996.
82. Mavec JC, McClanahan SB, Minah GE, et al: Effects of an intra-canal glass ionomer barrier on coronal microleakage in teeth with post space, J Endod 32:120-122, 2006.
83. Mayhew JT, Windchy AM, Goldsmith LJ, et al: Effect of root canal sealers and irrigation agents on retention of preformed posts luted with a resin cement, J Endod 26:341-344, 2000.
84. McComb D: Caries-detector dyes—how accurate and useful are they? J Can Dent Assoc 66(4):195-198, 2000.
85. Menezes MS, Queiroz EC, Campos RE, et al: Influence of end-odontic sealer cement on fiberglass post bond strength to root dentine, Int Endod J 41:476-484, 2008.
86. Metzger Z, Abramovitz R, Abramovitz I, et al: Correlation between remaining length of root canal fillings after immediate post space preparation and coronal leakage, J Endod 26:724-728, 2000.
87. Metzger Z, Schaham G, Abramovitz I, et al: Improving the seal of amalgam cores with cemented dowels: a comparative in vitro radioactive tracer study, J Endod 27:288-291, 2001.
88. Mezzomo E, Massa F, Libera SD: Fracture resistance of teeth restored with two different post and core designs cemented with two different cements: an in vitro study. Part 1, Quintessence Int 34:301-306, 2003.
89. Morgano SM, Milot P: Clinical success of cast metal posts and cores, J Prosthet Dent 70:11-16, 1993.
90. Morgano SM, Rodrigues AHC, Sabrosa CE: Restoration of end-odontically treated teeth, Dent Clin N Am 48:397-416, 2004.
91. Moshonov J, Slutzky-Goldberg I, Gottlieb A, et al: The effect of the distance between post and residual gutta-percha on the clini-cal outcome of endodontic treatment, J Endod 31:177-179, 2005.
92. Mulvay PG, Abbott PV: The effect of endodontic access cavity preparation and subsequent restorative procedures on molar crown retention, Aust Dent J 41:134-139, 1996.
93. Nandini VV, Venkatesh V: Current concepts in the restoration of endodontically treated teeth, J Indian Prosthodont Soc 6:63-67, 2006.
94. Nayyar A: Amalgam coronal-radicular dowel and core technique for endodontically treated posterior teeth, J Prosth Dent 43:511-515, 1988.
95. Newcomb BE, Clark SJ, Eleazer PD: Degradation of the sealing properties of a zinc oxide-calcium sulfate-based temporary filling material by entrapped cotton fibers, J Endod 27:789-790, 2001.
96. Ngoh EC, Pashley DH, Loushine RJ, et al: Effects of eugenol on resin bond strengths to root canal dentin, J Endod 27:411-414, 2001.
97. Nissan J, Dmitry Y, Assif D: The use of reinforced composite resin cement as compensation for reduced post length, J Prosthet Dent 86:304-308, 2001.
98. Papa J, Cain C, Messer HH: Moisture content of vital vs. end-odontically treated teeth, Endod Dent Traumatol 10:91-93, 1994.
99. Pashley EL, Tao L, Pashley DH: The sealing properties of tem-porary filling materials, J Prosthet Dent 60:292-297, 1998.
100. Perdigão J, Deheny GE, Swift EJ, Jr: Effects of chlorhexidine on dentin surfaces and shear bond strengths, Am J Dent 7:81-84, 1994.
101. Pereira JR, de Ornelas F, Conti PC, et al: Effect of a crown ferrule on the fracture resistance of endodontically treated teeth restored with prefabricated posts, J Prosthet Dent 95:50-54, 2006.
102. Peutzfeldt A, Asmussen E: Influence of eugenol-containing tem-porary cement in efficacy of dentin-bonding systems, Eur J Oral Sci 107:65-69, 1999.
103. Pilo R, Cardash HS, Levin E, et al: Effect of core stiffness on the in vitro fracture of crowned endodontically treated teeth, J Prosthet Dent 88:302-306, 2002.
104. Rafeek RN, Smith WA, Lalla A: Assessment of coronal microle-akage of three materials used in endodontically treated teeth, Eur J Prosthodont Restor Dent 12:39-45, 2004.
105. Ravanshad S, Ghoreeshi N: An in vitro study of coronal micro-leakage in endodontically treated teeth restored with posts, Aust Endod J 29:128-133, 2003.
106. Regan JD, Witherspoon DE, Foyle D: Surgical repair of root and tooth perforations, Endod Topics 11:152-178, 2005.
107. Reid LC, Kazemi RB, Meiers JC: Effect of fatigue testing on core integrity and post microleakage of teeth restored with different post systems, J Endod 29:125-131, 2003.
108. Rivera EM, Yamauchi M, Chandler G, et al: Dentin collagen cross-links of root-filled and normal teeth, J Endod 14:195, 1988.
109. Rosen H: Operative procedures on mutilated endodontically treated teeth, J Prosthet Dent 11:973-986, 1961.
110. Ruemping DR, Lung MR, Schnell RJ: Retention of dowels sub-jected to tension and torsional forces, J Prosthet Dent 41:159-162, 1979.
111. Salameh Z, Sorrentino R, Papacchini F, et al: Fracture resistance and failure patterns of endodontically treated mandibular molars restored using resin composite with or without translucent glass fiber posts, J Endod 32:752-755, 2006.
112. Sapone J, Lorencki SF: An endodontic-prosthodontic approach to internal tooth reinforcement, J Prosthet Dent 45:164-174, 1981.
113. Saupe WA, Gluskin AH, Radke RA: A comparative study of fracture resistance between morphologic dowel and cores and a resin-reinforced dowel system in the intraradicular restoration of structurally compromised roots, Quintessence Int 27:483-491, 1996.
114. Schillingburg HT, Fisher DW, Dewhirst RB: Restoration of end-odontically treated posterior teeth, J Prosthet Dent 24:401-409, 1970.
115. Schillingburg HT, Kessler JG: Restoration of the endodontically treated teeth, Chicago, 1982, Quintessence Publishing Co.
116. Schwartz RS, Fransman R: Adhesive dentistry and endodontics: materials, clinical strategies and procedures for restoration of access cavities: a review, J Endod 31:151-165, 2005.
117. Schwartz RS, Robins JW: Post placement and restoration of end-odontically treated teeth: a literature review, J Endod 30:289-301, 2004.
118. Sedgley CM, Messer HH: Are endodontically treated teeth more brittle? J Endod 18:332-335, 1992.
119. Segat L: Restoration of non-vital teeth, J Mich St Dent Assoc 44:254-259, 1962.
120. Shen C, Oh WS, Williams JR: Effect of post-silanization drying on the bond strength of composite to ceramic, J Prosthet Dent 91:453-458, 2002.
121. Sorenson JA, Engleman MJ: Ferrule design and fracture resistance of endodontically treated teeth, J Prosthet Dent 63:529-536, 1990.
122. Sorenson JA, Martinoff JT: Clinically significant factors in dowel design, J Prosthet Dent 52:28-35, 1984.
123. Sorenson JA, Martinoff JT: Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth, J Prosthet Dent 51:780-784, 1984.

464 chapter 20 | Problem Solving the Challenges Faced in the Restoration of Endodontically Treated Teeth
124. Stacey GD: A shear stress analysis of the bonding of porcelain veneers to enamel, J Prosthet Dent 70:395-402, 1993.
125. Standlee JP, Caputo AA, Hanson EC: Retention of endodontic dowels: effects of cement, dowel length, diameter, and design, J Prosthet Dent 39:401-405, 1978.
126. Standlee JP, Caputo AA: The retentive and stress distributing properties of split threaded endodontic dowels, J Prosthet Dent 69:436-442, 1992.
127. Stankiewicz NR, Wilson PR: The ferrule effect: a literature review, Int Endod J 35:575-581, 2002.
128. Stewart GP, Jain P, Hodges J: Shear bond strengths of resin cements to both ceramic and dentin, J Prosthet Dent 88:277- 284, 2002.
129. Tagami J, Tao L, Pashley DH: Correlation among dentin depth, permeability, and bond strength of adhesive resins, Dent Mater 6:45-50, 1990.
130. Tao L, Pashley DH: Shear bond strengths to dentin: effects of surface treatments, depth and position, Dent Mater 4:371-378, 1988.
131. Taylor AG: Dowel abutment crown, R Can Dent Corps Quart 4:1-4, 1963.
132. Tewari S, Tewari S: Assessment of coronal microleakage in inter-mediately restored endodontic access cavities, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93:716-719, 2002.
133. Thurmond JW, Barkmeier WW, Wilwerding TM: Effect of por-celain surface treatment on bond strengths of composite resin bonded to porcelain, J Prosthet Dent 72:355-359, 1994.
134. Tidmarsh BG: Restoration of endodontically treated posterior teeth, J Endod 2:374-375, 1976.
135. Torabinejad M, Ung B, Kettering JD: In vitro bacterial penetra-tion of coronally unsealed endodontically treated teeth, J Endod 16:566-569, 1990.
136. Trautmann G, Gutmann JL, Nunn ME, et al: Restoring teeth endodontically treated through existing crowns. Part I. Survey of pulpal status upon access, Quintessence Int 31:713-718, 2000.
137. Trautmann G, Gutmann JL, Nunn ME, et al: Restoring teeth endodontically treated through existing crowns. Part II. Survey of restorative materials commonly used, Quintessence Int 31:719-728, 2000.
138. Trautmann G, Gutmann JL, Nunn ME, et al: Restoring teeth endodontically treated through existing crowns. Part III. Material usage and prevention of bacterial leakage, Quintessence Int 32:27-32, 2001.
139. Trautmann G, Gutmann JL, Nunn ME, et al: Restoring teeth endodontically treated through existing crowns. Part IV. Material usage and prevention of dye leakage, Quintessence Int 32:33-41, 2001.
140. Trope M, Maltz DO, Tronstad L: Resistance to fracture of restored endodontically treated teeth, Endod Dent Traumatol 1:108-111, 1985.
141. Tselnik M, Baumgartner JC, Marshall G: Bacterial leakage with mineral trioxide or a resin-modified glass ionomer used as a coronal barrier, J Endod 30:782-784, 2004.
142. Umemoto K, Kurata S: Effects of mixed silane coupling agent on porcelain tooth material and various dental alloys, Dent Mater J 14:135-142, 1995.
143. Varela SG, Rabade LB, Lombardero PR, et al: In vitro study of endodontic post cementation protocols that use resin cements, J Prosthet Dent 89:146-153, 2003.
144. Vichi A, Grandini S, Davidson CL, et al: An SEM evaluation of several adhesive systems used for bonding fiber posts under clini-cal conditions, Dent Mater 18:495-502, 2002.
145. Watanabe EK, Yamashita A, Imai M, et al: Temporary cement remnants as adhesion inhibiting factors in the interface between resin cements and bovine dentin, Int J Prosthodont 10:440-452, 1997.
146. Webber RT, del Rio CE, Brady JM, et al: Sealing quality of a temporary filling material, Oral Surg Oral Med Oral Pathol 46:123-130, 1978.
147. Weine FS, Wax AH, Wenkus CS: A retrospective study of tapered, smooth post systems in place for 10 years or more, J Endod 17:293-297, 1991.
148. Wolanek GA, Loushine RJ, Weller RN, et al: In vitro bacterial penetration of endodontically treated teeth coronally sealed with a dentin bonding agent, J Endod 27:354-577, 2001.
149. Wolcott JF, Hicks ML, Himel VT: Evaluation of pigmented intra-orifice barriers in endodontically treated teeth, J Endod 25:589-592, 1999.
150. Woody TL, Davis RD: The effect of eugenol-containing and eugenol-free temporary cements on microleakage in resin bonded restorations, Oper Dent 17:175-180, 1992.
151. Yu YC, Abbott PV: The effect of endodontic access cavity prepa-ration and subsequent restorative procedures on incisor crown retention, Aust Dent J 39:247-251, 1994.
152. Zakizadeh P, Marshall SJ, Hoover CI, et al: A novel approach in assessment of coronal leakage of intraorifice barriers: a saliva leakage and microcomputed tomographic evaluation, J Endod 34:871-875, 2008.
153. Zhi-Yue L, Yu-Xing Z: Effects of post-core design and ferrule on fracture resistance of endodontically treated maxillary central incisors, J Prosthet Dent 89:368-373, 2003.
154. Zmener O, Banegas G, Pameijer CH: Coronal microleakage of three temporary restorative materials: an in vitro study, J Endod 30:582-584, 2004.
RECommEndEd AddITIonAl REAdIngKostka E, Roulet J-F: The root filled tooth in prosthodontic reconstruc-
tion. In Bergenholtz G, Hørsted-Bindslev, Reit C: Textbook of endodontology, Oxford, 2003, Blackwell Munksgaard.
Saunders WP: Restoration of root filled teeth. In Ørstavik D, Pitt Ford TR: Essential endodontology, Oxford, 1998, Blackwell Science.

Index 465
465
Index
AAbscesses, acute periapical
acute periodontal abscess vs., 8-9, 73-74, 73f
differential diagnosis of, 72f, 82mobility testing for, 9-10periodontal probing of, 8, 8fradiographic interpretation of, 11swelling from, 5fvisual inspection of soft tissue, 4
Access openings. see also orifice locations, identifying
anterior teeth considerations, 158, 159fcaries excavation for, 153-156, 154b,
154f-155fclinical considerations, 167-168, 168fclinical problem examples for, 151b,
154b, 155f, 156bcrown or large restoration considerations,
166-167, 166f-167fdeviations in canals, 157-158, 157fmagnification for, 158f, 163f-164f, 164other than lingual or occlusal, 150-151,
151fperforation prevention and management
of, 158, 158f, 160, 164-166, 164f-166f
posterior teeth considerations, 160-162, 160f-162f
pulp chamber calcifications, 162, 163fpulp horn considerations, 158-162,
158f-159frestoration of, 441-445, 444frestoration removal, 156, 156b, 156ftooth isolation advantages in, 152-153,
152f-153funsupported tooth structure removal,
156, 156fworking length determination during,
182-183Accidents, dental. see coronal fractures;
tooth fractures; traumatic tooth injuries
Acid etching, 442Aerodontalgia, 19
Aggregatibacter actinomycetemcomitans (Actinobacillus), 77
Aggressive periodontitis, lesions of, 77-78, 78f
Alveolar bone contoursclinical problem examples of, 358b, 359fcrown lengthening for recontouring,
366-367, 367f-368fsurgical treatment planning of, 358,
358f-359fAmoxicillin
prescribing loading dose of, 317-319for surgical trephination, 317
Analgesics, for painful tooth emergencies, 319-320, 320f
Anatomic deviations, teeth, 269Anatomy
apical root. see apical root anatomyobstructions requiring surgery, 333-334,
333f-334fsurgical, in vivo, 346tooth. see tooth anatomy
Anesthesiapainful tooth emergencies using,
320-323, 322f-323fperiapical surgery using, 346surgical trephination options, 317
Anesthetic carpules, making ice sticks with, 12, 12f
Anesthetic test, in pulpal diagnosis, 14-15Angulation. see anterior-posterior
angulation; beam angulationAngulation, incorrect image
anterior-posterior, 33-36effect on images, 32-36elongation, 32-33foreshortening, 32
Ankylosisdefined, 425inflammatory replacement resorption
and, 432-434, 433f-434fAnterior teeth. see also incisors
access openings through, 158, 159f-160f, 160
cementoma on, 65, 66f
electric pulp test on, 14, 16fnecrotic pulp treatment for, 310-315,
311f-315fperforations into periodontal attachment
of, 85, 87fpermanent restoration factors for, 445,
446fpulp exposure from traumatic fracture of,
144-145radiographs of, 25, 25b, 26f-27f, 31,
31f-32f, 49, 49fworking length determination in, 182,
187fAnterior zygomatic arch, diagnosing TMD,
124-125, 124fAnterior-posterior angulation, 33-36,
34f-36fAntibiotics
avulsion injury guidelines, 429painful tooth emergencies using,
319-320, 320fprescribing loading dose of, 317-319surgical trephination using, 317
Apexificationcalcium hydroxide weakening tooth in,
242-243, 245ffailed nonsurgical management of
open-apex tooth indicating, 107-108, 107f
indications for, 241-242MTA techniques for, 243, 246f-248frevascularization or regeneration
techniques for, 243-246traditional procedure of, 242, 242f-245ftreating revulsed tooth with, 430, 430f
Apical bevelpreparing root apex for surgery with,
339-340, 340f, 349, 350fsurgical revision with, 337-338
Apical constrictionestablishing working length short of, 204losing after excessive instrumentation,
200-201managing, 201
Anterior teeth (Continued)
Note: Page numbers followed by “f” refer to illustrations; page numbers followed by “t” refer to tables; page numbers followed by “b” refer to boxes.

466 Index
placing filling material beyond, 234preventing, 201
Apical delta, 179f-180f, 180-181Apical density, after obturation, 236-238,
236f-237fApical root anatomy
CDJ in periodontal disease, 182fclinical problem, 183b, 184fevaluating with silicon stop, 184finvasive apical resorption, 183-184, 183fnecrotic pulp and immature. see
apexificationoverview of, 181-189straight-line access to canal orifice, 182,
183fApical seal, inadequate, 107-109, 107f-
108f, 108bApical surgery. see periapical surgeryApical trephination, for tooth emergencies,
316-319, 318f-319fApical-third horizontal root fractures, 434,
434fArch bars, in radiographic interpretation,
58, 59fArticaine (Septocaine), 346Articulating paper
diagnosing occlusal discrepancies with, 120b, 120f, 122b
diagnosing TMD with, 127, 127fAvulsion injuries
aggressive treatment for, 428fcleaning and replanting, 429, 429fdefined, 427minimal tissue damage in some, 427foverview of, 427-431probability of IRR in, 428ftrauma as cause of, 429f-430f
BBayonet-shaped canals. see S-shaped canalsBeam angulation
evaluating image quality, 28-29, 28fradiographs taken with incorrect, 25-28,
27f-28fBicuspidization
defined, 393-394, 394fsurgical techniques, 404-405
Biologic width, crown lengthening determination, 357, 357f, 448f
BioPure MTAD, 211-212Bioroot engineering, 244Bite pressure test, 7, 8fBitewing radiographs, 166Bleaching root-treated and discolored teeth,
445Block anesthesia, 321-322Bonded carbon fiber posts, 448Bone and connective-tissue, in horizontal
root fractures, 436, 436fBone loss, from luxated tooth, 426-427,
426f
Bony defects, from pulpal/periodontal pathosis
acute periapical abscess, 72f, 82acute periodontal abscess, 73-74, 73fcemental tears, 78-80, 80fchronic periodontitis. see chronic
periodontitischronic sinus tracts of pulpal origin.
see sinus drainage tracts of pulpal origin
deep coronal fractures, 87-89, 88f-90fdevelopmental lingual groove on
maxillary lateral incisors, 92-93, 94fdisease interactions, 71external root resorption, 78, 79ffurcation/lateral lesions without loss of
attachment, 80-82, 81flesions of aggressive forms of
periodontitis, 77-78, 78flesions of periodontium not from
periodontal/pulpal pathosis, 87-95periodontal lesions involving furcation,
75-77, 78fperiodontal vs. pulpally induced lesions,
73-85, 73f, 81froot perforations. see root perforations,
response of periodontium tovertical root fractures. see vertical root
fracturesBrasseler end-cutting bur
alveolar bone recontours with, 367crown lengthening with, 364t, 373f
Bruxismdeveloping TMD from, 123-124sensitivity to percussion from, 7
Buccal object rule, working length determination, 186-187, 188f
Bupivacaine (Marcaine), 346Burs
access opening through crowns, 167accessing anterior teeth, 129f, 160accessing posterior teeth, 124-125, 130fBrasseler end-cutting, 364t, 367, 373fGates-Glidden. see Gates-Glidden (GG)
drillsMasserann. see Masserann kitTMD management with, 127, 128f
CC+ file
negotiating calcified canal, 249pathfinding using, 205
Calcified canalsaccess openings affected by, 162, 163faccessing apical portion of, 252, 253faccessing initially, 249, 251f-252faccessing middle portion of, 249, 252guidelines for extensive calcifications,
253-254irrigation of, 249, 252locating orifices of, 163f, 168-171,
168f-170f
nonsurgical management of, 248-249, 251f
problem case demonstrating, 248, 250fradiograph of, 248, 249freaching estimated working length, 252
Calcified union, in healed horizontal root fracture, 435, 435f-436f
Calcium hydroxide, Ca(OH)2
apexification use of, 242, 244f-245fapical constriction treatment with, 201C-shaped canals using, 262-263disinfection using, 215indirect pulp capping using, 139inflammatory resorption treated with,
428f-429f, 431-433, 432finternal resorption determined with, 255intrusive luxation injury treated with,
140MTA vs. use of, 242-243, 245freplacement resorption increased by use
of, 256-257temporary restorations using, 441vital pulp therapy with, 137, 138f
Canal. see calcified canalsCanines
access through rotated mandibular, 150-151, 151f
coronal fracture of, 71, 88felongation in radiographs of maxillary,
32-33evaluating tooth anatomy of, 43, 44fmultiple canals in, 157, 157fnonremoval of post in, 335-336, 336forifice identification in mandibular,
172-173perforation of, 85b, 86f, 167-168, 168fresorption in maxillary, 183b, 184fswelling from necrotic pulp extending to,
313, 314fvertical root fracture of, 91, 93fworking length determination in, 178f,
186Ca(OH)2. see calcium hydroxide,
Ca(OH)2
Carbon dioxide spray, 12, 12f-13fCardiogenic pain, 130Caries. see also direct pulp caps, carious
exposure inaccess openings, and removing, 153-154,
154f-155faccess openings, restoring using detectors,
442clinical problem example of, 47b, 48finadequate coronal seal caused by,
109-110, 109fpulpal pathosis indications in, 46, 46fradiographs of, 46-47radiographs of lesions, 46-47, 46f-47fradiographs of restorations, 47, 48fresection criteria for extensive, 398fvisual inspection of, 3, 3f
Apical constriction (Continued) Calcified canals (Continued)

Index 467
vital pulp therapy indications, 47, 47f-48f, 135, 144, 144f
Carriers, MTA, 345, 345fCast posts, 447-448, 448tCavit
minimizing leakage with, 440removing from pulp chamber, 276, 287f,
288, 291-292temporary restorations using, 440
CBCT (cone-beam computed tomography)as digital radiography, 37-39, 40fevaluating tooth anatomy, 43, 44f
Cement types, intraradicular posts, 450-451, 450f-451f
Cemental tears, diagnosing, 78-80, 80b, 80fCementin-dentin junction (CDJ)
apical root anatomy impacting working length in, 178-189, 182f-183f
definition of, 178-180, 180fCementoma
clinical problem example of, 66b, 67fradiographic changes of, 65, 66f
Cemento-osseous dysplasia. see cementomaCeramic posts, 449Cervical resorption (CR)
cause of, 254defined, 52indications for, 259-261, 261f-262f
Chelating agents, purpose and rationale of, 212, 213f-214f
Chlorhexidine (CHX)disinfection with, 215final rinsing with, 211-212irrigation with, 215-216preventing release of MMPs with, 243pulpal vitality preserved by, 134revascularization or regeneration using,
244temporary restorations using, 441
Chronic periodontitisclinical problem examples of, 74b-75b,
76f-77fendodontic perspective on, 71-72, 72ffailure of root-treated tooth vs., 106lesions of, 74, 74f-77f
Clindamycinprescribing loading dose of, 317-319for surgical trephination, 317
Clinical examinations, 3-10bite pressure testing, 7mobility testing, 9-10palpation testing, 6percussion testing, 6-7periodontal probing, 8-9use of explorer, 5-6visual inspection, 3-5
Cluster headaches, causing facial pain, 130Cold tests
applying dental dam for, 14overview of, 12-13pulpal diagnosis using, 12f-14f
Compaction. see obturationConcussion injury, diagnosing/treating/
prognosis of, 422, 423fCondensing osteitis, radiograph of, 59, 60fCone cuts, 25-28, 28fCone-beam computed tomography
(CBCT)as digital radiography, 40fevaluating tooth anatomy, 43, 44foverview of, 37-39
Connective-tissue/bone union, in horizontal root fractures, 436, 436f
Connective-tissue/soft-tissue union, in horizontal root fractures, 436, 437f
Core-carriers. see also thermoplasticized core-carrier, gutta-percha
removing metal obturators, 291-293, 292f-293f
removing plastic, 286-289, 287f-288fCoronal discoloration, luxated tooth
causing, 427, 427fCoronal fractures
active prevention of, 421clinical problem, 89b, 90fcomplete cusp, 4fendodontic complications from, 125,
126fetiology of deep, 87-89, 88f-90fon intact marginal ridges, 4fon interproximal surface, 4fpreserving teeth with, 421, 422fradiographic changes in, 49, 49f-50froot or tooth resection criteria, 396ftenderness to percussion of, 7TMD often cause of deep, 125visual inspection of, 4
Coronal leakageexposed/contaminated root fillings
caused by, 460-461, 460fperiradicular pathosis/persistence due to,
109-110, 109f-111frestoration of anterior teeth with, 445,
446fsealing canal orifices against, 444-445,
444ftemporary restoration risks of, 440,
442b, 443fCoronal perforations, managing, 164-166,
164f-166fCoronal-third horizontal root fractures,
434, 435fCR. see cervical resorption (CR)Cracks, tooth, 418-420Crazes, tooth, 418-420, 419f, 442Crestal bone
managing resorption in, 261perforations damaging, 71, 85probing location of, 72, 72f
Crown lengthening, 352fclinical problem examples of, 358b, 359f,
372b, 373f-374f, 374b, 376b-377b, 377f-379f
contraindications for, 363, 363f, 447, 448f
indications for, 360-363, 360f-362fnormal periodontium/surgical planning
for, 357-358, 357f-359foverview of, 356-357perforations indicating, 372-375, 373f,
375f, 380fresorption defects indicating, 375-379,
376b-377b, 376f-379fvertical root fracture indicating, 379,
381f, 382bCrown lengthening, surgical techniques
alveolar bone recontour, 366-367, 367f-368f
complications with, 370-372, 370f-372fenvelope tissue flap, 364-365, 364f-365fhealing period for, 369-370, 369f-370finstruments for, 364toverview of, 363-364periodontal surgical dressing, 369, 369fsurgical procedures, 364, 364fthinning or undermining tissue, 366,
366ftissue closure, 367-369, 368f
Crown-down techniqueenlarging and shaping canal, 205, 206fremoving gutta percha in coronal half of
small canals, 284, 284fremoving necrotic pulp, 310-312
Crowns. see also coronal fractures; coronal leakage
access openings through, 166-167, 166f-167f
cold tests on metalloceramic, 13, 14firreversible pulpitis diagnosis in, 19radiographic images of, 24-25, 27fremoving, 275-276, 275fremoving posts from inside of full,
278-279, 279fC-shaped canals
managing, 262-263, 263f-265froot resection not suitable for, 400-401
Curettage, of soft-tissue lesion penetrating bone, 348
Curvature of canalsC-shaped, 262-263, 263f-265f, 400-401moderate-to-severe, 265, 266fS-shaped, 393-394, 401f-402f, 404f-405f
Cvek partial pulpotomy, with MTA, 145, 146f-147f
DDebridement, removing necrotic pulp,
310-311Dental (rubber) dam
applying for thermal testing, 14crown lengthening using, 360,
360f-361fdisinfecting, 153, 153fheat tests using, 16f
Caries (Continued) Crown lengthening (Continued)

468 Index
retracting to view film position, 25-28, 28f
thermal pulp tests using, 14, 16ftooth isolation using, 152-153,
152f-153fDental history
diagnosing occlusal discrepancies from, 122b
diagnosing trigeminal neuralgia from, 123
patient description of pain in, 2Dental stopping
heat tests using, 13-14, 15focclusal pressure tests using, 125-127,
126f-127fDentin
excessive removal of root, 202failure to properly remove debris from,
204managing lost apical constriction with
chips of, 201sodium hypochlorite impacting, 211working length lost from packed,
197-198, 198fDentin hypersensitivity
defining, 133overview of, 132-133patient considerations, etiologies and
treatment issues, 132-133toothpastes or solutions for, 18using desensitization for, 133vital pulp therapy for. see vital pulp
therapyDevelopmental cysts
clinical problem example of, 66b, 67fradiographic changes in, 66, 66f
Developmental lingual groove, on maxillary lateral incisors, 92-93, 94f
Diamond-tipped ultrasonic instruments, 341, 341f-342f
Differential diagnosisbony defects. see bony defects, from
pulpal/periodontal pathosisoverview of, 11periodontal abscess using, 8-9
Digital radiography, 37, 37f-39fDigital sensors. see film/digital sensorsDirect pulp caps
calcium hydroxide used in, 137, 138fcarious exposure in, 140-142, 140b,
141f-143fiatrogenic exposure in, 142-144, 143f
Disease interactions, 71Disinfectants, 214-216Drainage. see incision and drainageD-series, rotary NiTi instruments, 281-284
EE. faecalis, residual infections from, 116EAL. see electronic apex locator (EAL)Edge-Ease cushions, film, 27f
EDTA (ethylenediamine tetraacetic acid)as chelating agent, 212, 213f-214fas final rinsing agent, 211-212removing root canal sealer with, 285resin-bonded obturation using, 230
Elbow, zipping with, 199, 201fElectric pulp test (EPT)
necrotic pulp diagnosis with, 310, 311fnormal teeth diagnosis with, 17pulpal diagnosis with, 14, 16f
Electronic apex locator (EAL)irrigation using, 211working length determination using, 58,
59f, 187-189Elongation
evaluating image quality, 28-29, 28fincorrect image angulation causing, 27f,
30f-31f, 32-33, 34fEmergencies. see necrotic pulp; painful
tooth emergencies; pulpitis; traumatic tooth injuries
Endo ice, 12, 12f-13fEndoActivator, 211Endodontic failure, radiographic changes
in, 64-65, 65fEndodontic lesions, healed, 66, 67fEndoVAC, 211Energized K-files
in canal filled with gutta-percha, 343foverview of, 341-344removal of gutta-percha, 344fremoving, 344fultrasonic unit setting for, 344funprepared canals using, 343f
Envelope flaps, crown lengthening, 364-365, 364f-365f
Environmental factors, film/digital sensors, 23
Epinephrine, coronal perforations using, 165
Epithelial cell rests of Malassez, 178fEPT. see electric pulp test (EPT)ER. see external resorption (ER)Ethyl chloride crystals, cold tests with, 12,
12fEthylenediamine tetraacetic acid. see EDTA
(ethylenediamine tetraacetic acid)Explorer, pulpal diagnosis using, 5-6Exposure, controlling radiographic, 23, 23fExternal invasive resorption, 52, 55fExternal resorption (ER)
inflammatory replacement resorption as, 256, 257f
inflammatory resorption as. see inflammatory resorption
internal resorption vs., 78, 78b, 79fradiographic tooth changes of, 52,
53f-55fExtracanal resorption, 256, 258fExtraction, gross perforations indicating,
458, 460fExtrusive luxation injury, 423-424, 423f
FFalse canals (root perforations), 199, 202fFenestration
clinical problem example of, 331b, 332fas normal anatomic finding, 6, 6fsurgical treatment planning and,
358, 359fFerric sulfate
coronal perforations and, 165effectiveness in pulpotomies, 144vital pulp therapy considerations, 134
Ferrule effectcrown lengthening contraindications,
448fcrown lengthening indications,
360-361restorative failure prevented with, 361,
361fretaining cingulum in anterior teeth
with, 445Ferrule width, for intraradicular posts,
451, 451f-453fFever
acute periodontal abscess with, 73loading dose of antibiotic for, 320
Fiber posts, 448-449Fibrous attachment, periodontal, 357fFile-EZE chelate, 212Files
energized K-files. see energized K-filesHedström. see Hedström fileK-files. see K-filesmaster apical file. see master apical file
(MAF)NiTi. see NiTi (nickel-titanium)
instrumentsrotary NiTi instruments. see NiTi
(nickel-titanium) instruments, rotary
Filling materials. see materialsFilm/digital sensors
inability to keep film deep in mouth, 24b, 26f
muscular tongue indications, 25b, 27fnarrow mandibular arch indications,
25b, 26f-27fpositioning, 23-25, 24f, 27fradiation beam angulation for, 25-28
Finger pressure, for image taking, 32, 35fFinger spreaders, in NiTi alloy, 233Flaps
crown lengthening with envelope, 364-365, 364f-365f
types used in periapical surgery, 346-348, 347f-348f
Flaring (canal shaping), 202, 204Fluctuancy. see incision and drainageForceps
metal object removal with, 289f, 290, 292
plastic core carrier removal with, 288, 288f
Dental (rubber) dam (Continued)

Index 469
Foreign bodies. see metallic object removalForeshortening, radiographic images
clinical problem example of, 32b, 33fincorrect image angulation causing,
31f-32f, 32quality evaluation, 28-29, 28f
Formaldehyde, not for use in root canal, 214
Formocresol, not for use in pulpotomy, 144
Fracturescoronal. see coronal fracturesNiTi instrument, 298post. see intraradicular posts, removing
fracturedroot. see root fracturestooth. see tooth fractures
Frank technique, 242Furcation
periodontal lesions involving, 75-77, 78froot resection considerations, 400, 400fwithout loss of attachment, 80-82, 81f
Furcation perforationscoronal, 165-166maxillary premolars with, 457, 458fperiradicular surgery indications,
388-390, 388f-391fprognosis for, 458, 459frepairing larger, surgically, 388, 389frepairing smaller, with MTA, 388, 388froot or tooth resection criteria, 396f
Fusion of roots, root resection not suitable for, 400-401
GGates-Glidden (GG) drills
moderate-to-severe canal curvature with, 265
removing gutta percha with, 281, 284, 284f
removing separated bur head from canal with, 298, 298f-299f
Gauze, for ice tests, 12, 12fGingival recession, dentin hypersensitivity
in, 133Glass fiber posts, 448Glass ionomer (GI), in coronal
perforations, 164-165Globulomaxillary cysts, 66Glyde file chelate, 212Gutta-Core core carriers, 227, 229fGutta-percha, 286-289Gutta-percha, removing
in apical half of small canals, 282f, 284-285, 285f
plastic core carriers, 286-289, 287f-288fprior to enlarging canal space, 456
Gutta-percha, removing in coronal half of small canals
Gates-Glidden or Peeso bur technique, 284, 284f
heat technique, 283, 283f
rotary NiTi technique, 281-284, 282fultrasonic technique, 283-284, 284b,
284fGutta-percha obturation techniques
clinical problem example of, 223bC-shaped canals using, 263, 264f-265fefficacy of, 218lateral compaction, 221-223, 222f-224foverview of, 221-227, 222fproblems identified after, 234-239,
235f-237fproblems preparing for, 231-232,
231f-232froot canal sealers for. see sealer, root
canalthermoplasticized core-carrier techniques,
227, 228f-229fthermoplasticized injection techniques,
225-227, 226f-227fvertical compaction, 224-225, 225f-226f
HHand spreaders, in NiTi alloy, 233Healing period. see also horizontal root
fractures (HRF)crown lengthening, 369-370, 369b,
369f-370fradiographs of endodontic lesions, 66,
67fHeat technique
removing gutta percha in small canals, 283, 283f
removing metallic core-carriers, 292Heat tests, pulpal diagnosis, 13-14, 15fHedström file
cleaning C-shaped canals with, 262-263managing loss of working length with,
198managing lost apical constriction with,
201removing gutta percha in canals with,
281, 282fremoving metallic objects, 289-290, 290fremoving plastic core carriers, 288-289,
288fremoving separated, 298, 300f
Hemisection. see tooth resection (hemisection)
Hemostatic agentscoronal perforations using, 165periapical surgery using, 346
Hemostats. see film/digital sensorsHertwig epithelial root sheath (HERS),
177-178, 178f-179fHorizontal root fractures (HRF)
apical-third, 434, 434fbone and connective-tissue healing of,
436, 436fcalcified union between segments healing
of, 435, 435f-436f
connective-tissue/soft-tissue union healing of, 436, 437f
coronal-third, 434, 435ffailure to heal, 436-437, 437fmiddle-third, 434, 435foverview of, 435
Hypersensitive teethdefining, 133desensitization for, 133patient considerations, etiologies and
treatment issues, 132-133patients presenting with, 305toothpastes or solutions for, 18vital pulp therapy for. see vital pulp
therapy
IIatrogenic obstructions requiring surgery
broken instruments, 338ffunctional or esthetic considerations,
336flack of available canal space, 337foverview of, 334-337perforations. see perforationsseparated instrument fragments, 335fsilver cone removal, 335fweakening tooth structure when
removing posts, 336fIce
cold testing with, 12making with anesthetic carpules, 12fprotecting adjacent teeth testing with,
12ftesting with ice stick, 12f
Idiopathic root resorption, 252, 259-261, 261f-262f
IKI (iodine potassium iodide), disinfecting with, 215
Immature teethanesthetic test on, 14-15, 17felectrical pulp test on, 14, 16f
Impacted teeth, radiographs of, 58, 58f-59fImplants
clinical problem example of, 58b, 60fradiographic interpretation of, 58, 59ftooth retention vs., 356
In vitro. see periapical surgery techniques, in vitro
In vivo. see periapical surgery techniques, in vivo
Incision and drainagefluctuancy with drainage through tooth,
314, 315ffluctuancy with no drainage through
tooth, 314, 316fnonfluctuancy with drainage through
tooth, 314nonfluctuancy with no drainage through
tooth, 315overview of, 314-315
Incisive canal cysts, 66, 66f
Gutta-percha, removing in coronal half of small canals (Continued)
Horizontal root fractures (HRF) (Continued)

470 Index
Incisorsanesthesia for, 321apexification with calcium hydroxide on,
242, 244fapical-third fractures of, 434, 434fcrown lengthening on fractured, 358b,
359fdentinal bridging in, 145, 147fdevelopmental lingual groove on lateral,
92-93, 94felectric pulp test on, 14, 16ffractured post removal in, 276-278healing horizontally fractured, 436, 436fidentifying orifice locations in
mandibular, 172-173, 173fidiopathic root resorption in, 259, 261fimaging mandibular, 28-29, 28fimaging maxillary teeth using, 24-25,
25f-26finflammatory replacement resorption of,
432-433, 434flateral luxation injury of, 424, 424flocating multiple canals in, 99-101, 102f,
157-160, 157f, 159f, 172-173, 173fnecrotic pulps on, 310, 311boverextended posts in, 336, 337fperiapical ossifying fibromas on, 65, 66fperiapical pathosis on, 61-62, 61f-62fresorption after traumatic injury to, 431,
432fresorption following implanted, 429-430,
429fS-shaped canals of maxillary, 267-268traumatic fracture with pulp exposure in,
134f, 144-145Indirect pulp caps, 134, 139Inflammatory replacement resorption (IRR)
ankylosis and, 432-434, 433f-434favulsion injuries creating, 428f-429f,
429-430illustration of, 257fintrusive luxation injuries creating, 425overview of, 256traumatic tooth injuries creating,
431-432Inflammatory resorption
apically occurring, 257, 259, 259fappearance of, 257f-258finflammatory replacement resorption vs.,
433overview of, 256-257radiographic tooth changes of, 52traumatic tooth injuries creating,
431-434, 431f-432fInstallation stresses, choosing post structure,
448, 448tInstrument separation. see separated
instrumentsInstruments. see also files; NiTi (nickel-
titanium) instruments; NiTi (nickel-titanium) instruments, rotary
crown lengthening, 364t
lubricating with irrigation, 209perforations with endodontic, 384, 390,
391b, 392fperiradicular surgical, 388, 399f-400f
Intermediate restorative material (IRM)case study, 442b, 443fas root-end filling material, 344-345, 351as temporary material, 440-441
Internal resorption (IR)canal space treatment for, 256, 256fchallenges of, 254, 254fdefined, 254-255, 255fdetermining, 255, 255fexternal resorption vs., 52, 53f, 78, 78b,
79fillustrations of, 52fradiographic tooth changes of, 52root canal treatment for, 255-256, 256f
Intertreatment temporary restorations, 440-441
Intraligamental injections, anesthesia, 322-323, 323f
Intraosseous injections, anesthesia, 322-323
Intrapulpal anesthesia, 323, 323fIntraradicular posts
cement types for, 450-451, 450f-451fcharacteristics of, 447-449, 448t, 449fclinical problem example of, 278b, 278fcontraindications for, 447, 448fcoronal leakage risk in, 453, 454fcrown lengthening for, 361, 361fferrule width and, 451, 451f-453flength of/preservation of fillings in,
453-455, 454f-455flength recommendations for, 449-450,
449f-450foverview of, 447-458, 448fperforation risk in, 390, 391f, 456-458,
456f-460fprotruding through perforations, 391fremoving, 276-281, 277f-281fremoving fractured, 278-279, 278b,
278f, 281, 281fremoving gutta-percha prior to enlarging
canal, 456temporary filling complications of, 441when to remove restorations, 274-275,
274f-275fIntrusive luxation injury
diagnosing/treating/prognosis of, 424-425, 425f
inflammatory resorption from, 257, 431-432
Iodine potassium iodide (IKI), disinfecting with, 215
IR. see internal resorption (IR)IRM. see intermediate restorative material
(IRM)IRR. see inflammatory replacement
resorption (IRR)
Irreversible pulpitisdiagnosis of, 18-19management of, 308-310multi-canal teeth with, 309-310,
309f-310fnot localized, 19revascularization or regeneration for,
243-246signs/symptoms of, 307-308single-root/single-canal teeth with,
308-309, 308fIrrigants
calcified canals negotiated with, 249-250enlarging/shaping canal with, 196, 204obturation and, 231role of, 209-212, 210f-212fsmear layer removed with, 209, 210fultrasonic devices for, 211working length lost through lack of, 196
IRS extractor, instrument fragments, 298-299
JJeweler’s screwdriver, 281, 281fJ-shaped lesions, vertical root fractures, 103,
103fJuvenile periodontitis, lesions of, 77-78, 78f
KK-files. see also energized K-files
apical trephination using, 316-317deviations in canal anatomy caused by,
199negotiating calcified canal with, 249removing gutta percha in large canals
with, 281, 282fremoving necrotic pulp with, 311-312
LLateral canals
clinical problem example of, 387b, 387fintraradicular posts and, 454-455, 455fnonsurgical revision example of, 276b,
277fperiradicular surgery indications,
384-388, 385f-387fLateral compaction, gutta-percha
clinical problem example of, 223bas filling material of choice, 218-219overview of, 221-223, 222f-224f
Lateral compaction, resin-bonded obturation, 230
Lateral lesions, in pulpal necrosis, 60bLateral luxation injury, diagnosing/treating/
prognosis of, 424, 424fLateral periodontal cyst, 67-68, 67fLeakage. see coronal leakageLedermix paste, as disinfectant, 215Ledges
instrument error resulting in, 199, 201floss of working length from, 196, 196f
Instruments (Continued)

Index 471
refining posterior access openings by removal of, 151f-152f, 160-162
removal of gutta percha with solvent in, 285, 285f
restricting canal enlarging and shaping, 204
results of failure to remove, 196stainless steel instruments
negotiating, 205uncovering extra canals after removing,
158-160, 159fverifying lack of before obturation, 231
Ligament injections, anesthesia, 322-323, 323f
Ligature wires, and radiographic interpretation, 58, 59f
Lingual surface, cold tests on, 13, 14fLoupes, telescopic
access preparation using, 163f-164f, 164identifying orifices using, 175inspecting excavation for calcifications
using, 162removing separated instruments with,
298restoring access openings using, 442
Luxation injuriesconcussion, 422, 423fcorrect diagnosis of, 422extrusive luxation, 423-424, 423fintrusive luxation, 424-425, 425flateral luxation, 424, 424fsubluxation, 422-423, 423f
Luxation injuries, sequelae tocoronal discoloration, 427, 427fmarginal bone loss, 426-427, 426foverview of, 426pulp canal obliteration (PCO), 426, 426fpulpal necrosis, 427transient apical breakdown (TAB), 427
MMagnification. see loupes, telescopic;
microscopesMandibular anterior teeth
cementoma occurring primarily in, 65, 66f
orifice identification in, 159f, 172-173, 173f
removing cingulum in multi-canaled, 445
taking radiographs of, 25b, 26f, 31, 31f-32f
Mandibular molarsanesthesia of, 322, 322fclinical problem example of, 29b, 30fC-shaped canals in. see C-shaped canalsinadequate root canal in, 99-101,
101f-102fmetal core carrier removal with forceps
in, 292, 293fobturation of, 221, 223f
orifice identification in, 173-175, 173f-174f
revising inadequate root canal in, 275, 275f
root or tooth resection outcomes of, 408-414, 412f-414f
silver cone obturation in, 294, 294ftaking radiographs of, 29, 29ftooth resection in, 404, 405f
Manufactured ultrasonic tip with 3mm cutting length, 340-341, 340f-342f
Marcaine (bupivacaine), 346Marginal periodontium
crown lengthening indications, 361, 362fperforation in. see perforation, marginal
periodontiumMasserann kit
instrument fragment removal with, 299-300, 300f
metallic object removal with, 290-293, 291f
post removal with, 279-280, 280fMaster apical file (MAF)
identifying loss of working length with, 196, 197f
identifying underprepared canals with, 204
lateral compaction with, 221, 222fproblem-solving canal preparation for
obturation, 231problem-solving S-shaped canals with,
267Master cones, gutta-percha
custom-fitting before obturation, 234, 259, 260f-261f
cutting to desired length, 232, 232ffailure to coat with root canal sealer, 237failure to insert to full length, 237as filling material of choice, 219solving when compactors pull out, 233
Materials. see also gutta-percha; MTA (mineral trioxide aggregate)
evolution of filling, 218-219for intertreatment temporary restorations,
440-441MTAD, 211-212resin-bonded, 230, 230f, 234-238for restoration of access openings,
441-445for restoration of posterior teeth,
445-447, 446f-447fvital pulp therapy, 137-139, 138f-139fworking with posts. see intraradicular
postsMatrix metalloproteinases (MMPs), 243Maxillary molars. see also C-shaped canals
deep coronal fractures in, 88-89, 90finadequate root canals in, 99, 99b,
100f-101f, 103b, 103fmetal fragment removal in root of,
301, 301f
orifice identification in, 162f, 172, 172fremoving metallic core-carrier obturators
in, 291, 292froot resection outcomes for, 407-408,
407f-411fMaxillary sinusitis, 129-130, 130fMaxillary teeth
clinical problem examples of, 408b, 411f
developmental lingual groove on lateral incisors, 92-93, 94f
imaging, 24-25, 27fimaging, elongation, 30f-31f, 32-33,
34f-35fimaging quality, 29, 30f-31forifice identification in, 171-172,
171f-172fradiolucency in, 56f-57fsigns of TMD in, 124-125, 124f
Measuring gauge, gutta-percha obturation, 221, 222f
Metallic object removal. see also separated instruments
core-carrier obturators, 291-293, 292f-294f, 293b
with Hedström files, 289-290, 290flarge fragments, 298, 298f-299fwith Masserann kit, 290-291, 291fsilver cones, 294-296, 294f-296fwith specialized forceps, 290with ultrasonic instruments, 289, 289f
Microscopesidentifying orifices with, 175inspecting excavation for calcification
with, 162removing separated instruments with,
298restoring access openings with, 442
Midroot fracturesdiagnostic radiographs for, 49, 50fmiddle-third horizontal root fractures,
434, 435fMineral trioxide aggregate. see MTA
(mineral trioxide aggregate)MMPs (matrix metalloproteinases), 243Mobility
pulpal diagnosis using, 9-10tests, for deep coronal fractures, 88
Molars. see also mandibular molars; maxillary molars; premolars
developmental lingual groove on, 92-93, 94f
electric pulp test on cusp of, 14, 16ffurcation of lateral lesions without
loss of attachment, 80-82, 81fperiodontal lesions involving furcation,
75-77, 78fMonoblock, in resin-bonded obturation,
230Mouth protection, preventing coronal
fracture, 421
Ledges (Continued) Mandibular molars (Continued) Maxillary molars (Continued)

472 Index
MTA (mineral trioxide aggregate)apexification using, 246f-248favailable versions of, 138-139coronal perforations treated with,
152-153, 165, 166fdiscoloration from, 145, 147ffurcation perforations repaired
with, 388, 388f-389f, 457-458indirect pulp capping replaced
by, 139lost apical constriction treated
with, 198mixing, 139, 139fpathosis from inadequate apical seal
treated with, 107-108pulp capping with, 137-138, 140-142,
141f-142fpulp exposure from traumatic
fracture treated with, 145, 146f
pulpotomies using, 138, 144root perforations treated with, 84as root-filling material, 344-345,
345f-346f, 351, 351b, 352ftemporary restorations using, 440
MTAD, BioPure, 211-212Mucosal surface, nodule or bump
on, 3Multicanaled teeth
managing, 154, 154f-155fmanaging necrotic pulps in, 311
Muscle symptoms, TMD, 123M-wire files, 204Myofascial pain, interpretation of, 3
NNaOCL. see sodium hypochlorite
(NaOCL)Nasopalatine duct cysts, 66, 66fNecrotic pulp. see also apexification
clinical challenge example of, 310f, 311b
clinical problem example of, 60b, 61fdiagnosis of, 19, 19felectric pulp test for, 16f, 310, 311fintrusive luxation injuries with, 425lateral radiographic changes of, 63-64,
63f-64f, 64bluxated tooth with, 426-427management of, 310-315, 312f-314fperiapical radiographical changes of,
60-63, 61f-63fremoving completely from canal,
310-311, 312fremoving during enlarging and shaping.
see root canal, enlarging and shaping
treating localized swelling of, 311f, 313-314
Neoplasm pain, 130Nickel-titanium instruments. see NiTi
(nickel-titanium) instruments
NiTi (nickel-titanium) instrumentsbeyond canal terminus, 200-202, 203fcanal deviations using, 199, 199f,
201f-203fcontemporary use of, 195, 204-205, 206fdelivering disinfectants with, 215-216failure to properly use, 202, 204loss of working length and. see working
length, loss ofpreventing separation of, 297, 297fproblems during obturation, 232-234removal of fragments from, 298-299susceptibility to fracture, 298
NiTi (nickel-titanium) instruments, rotarycrown-down technique with, 205, 206fdelivering disinfectants with, 215-216enlarging and shaping canal with, 205obturation with, 230-231preventing separation of, 297, 297fpulpectomies performed with, 308removing gutta percha with, 281-285,
282fremoving necrotic pulp with, 310-311removing paste fillings with, 286removing plastic core carriers with, 288S-shaped canals managed with, 268, 268fvertical compaction using, 224, 226f
Nocturnal clenching, and occlusal trauma, 7
Nonfluctuancywith drainage through tooth, 314with no drainage through tooth, 315
Nonnegotiable root canals, root or tooth resection for, 397f
Nonodontogenic pain diagnosisatypical face pain in, 123description of, 119-120maxillary sinusitis, 129-130, 130focclusal discrepancies causing. see occlusal
discrepanciesother etiologies in oral cavity and head
of, 130TMD. see TMD (temporomandibular
disorder)trigeminal neuralgia, 123
Nonsteroidal antiinflammatory drugs (NSAIDs), 319
Nonsurgical treatmentclinical problem examples of, 98b-99b,
99f-101f, 103b, 103fincomplete, 99-101, 101f-102fsuccess of, 97, 98f
Nonvital pulp, working length determination, 186, 187f
Normal teethcold tests first on, 12-13, 13fdiagnosis of, 17radiographic images of, 36, 36f
NSAIDs (nonsteroidal antiinflammatory drugs), 319
Number 17 explorer, pulpal diagnosis, 5-6, 6f
OObturation. see also gutta-percha obturation
techniquescompaction with pluggers during, 345,
345f-346fevolution of filling materials for,
218-219guiding principles for, 230-231inadequate, 101, 102finadequate apical seal during, 107-109,
107f-108f, 108bproblems during canal, 232-234,
233f-234fproblems identified after, 234-239,
235f-237fproblems preparing canal for, 231-232,
231f-232froot canal sealers in, 219, 219f-221fvertical root fractures during, 49-51, 51f
Occlusal discrepanciesclinical problem examples of, 121f-122f,
122bdiagnosing nonodontogenic pain as,
120-121problem solving example of, 120b,
120f-121fOcclusal pressure sensitivity, symptom of
TMD, 125-126, 126fOcclusal trauma
restoration of posterior teeth after, 445-447, 446f-447f
temporary fillings subject to, 440-441tenderness to percussion indicating, 7tooth mobility from, 9-10vertical root fracture caused by, 91vertical root fractures from, 51
One-visit apexification treatment, 243On-the-job training, preventing coronal
fracture, 421Operating microscopes. see microscopesOrifice locations, identifying
calcification of dental pulp/pulp canal space complicating, 163f, 168-171, 168f-170f
in mandibular incisors, canines, and premolars, 159f, 172-173
mandibular molars, 173-175, 174fmandibular molars indications, 173fmaxillary central and lateral incisors
and canines, 171, 171f-172fmaxillary molars, 162f, 172, 172fmaxillary premolars, 171-172, 172fpreventing/managing problems in, 154f,
175, 175fOrthodontic extrusion, crown lengthening
indications, 362-363Otitis media pain, 130Overexposure, radiographs, 23, 23fOverextended root filling, after
obturation, 234Overfilling, after obturation, 234Overpreparation of canals, 202, 263

Index 473
PPain
hearing patient describe chronic, 2-3nonodontogenic. see nonodontogenic
pain diagnosispulpal diagnosis of. see pulpal diagnosis,
after testingPainful tooth emergencies
analgesics and antibiotics for, 319-320, 320f
anesthesia for, 320-323, 322f-323fapical/surgical trephination for, 316-319,
318f-319fclinical challenge example of, 310f, 311bhypersensitive teeth complaints, 305incision and drainage for. see incision
and drainageirreversible pulpitis management in,
308-310, 308f-310firreversible pulpitis signs in, 307-308necrotic pulp management in, 310-315,
311f-314freversible pulpitis signs in, 305-307,
306f-307fsubjective assessment of, 304-305, 317
Palatal infiltration, of anesthesia, 321-322Palpation
pulpal diagnosis signs in, 6, 6fvertical root fractures signs in, 89-91
Paper points, in working length determination, 189
Papilla-base flap, 346-348, 347f-348fParallel-threaded posts, 448, 448tPaste fills
obturation using, 218-219occlusal leakage from, 239removing from root canal, 285-286,
286fPatency filing, managing loss of working
length, 201-202PathFile
managing S-shaped canals with, 268removing necrotic pulp using, 311-312treating loss of working length with,
198-199PCO (pulp canal obliteration), from
luxated tooth, 426, 426fPDLSCs (periodontal ligament stem
cells), 244Peeso bur
avoiding in curved canals, 284bremoving gutta-percha in small canals
with, 284, 284fremoving separated head with, 298,
298f-299fPeet splinter forceps, 288, 288f, 290Penicillin
prescribing loading dose of, 317-319for surgical trephination, 317
Percussionpulpal diagnosis using, 6-7, 7fvertical root fractures signs, 89-91
Perforations. see also furcation perforations; root perforations, response of periodontium to
access opening in restorations causing, 158, 158f
clinical problem examples of, 372b, 373f-374f, 374b
coronal, 164-166, 164f-166fendodontic instruments causing, 384,
390intraradicular posts causing, 456-458,
456f-460fmarginal periodontium, 372-375, 375f,
380froot or tooth resections for post, 396froot or tooth resections for strip, 397fstrip, 388, 390, 390f-391f
Periapical abscesses. see abscesses, acute periapical
Periapical ossifying fibroma. see cementomaPeriapical pathosis. see necrotic pulp;
treatment failurePeriapical periodontitis
pulpation detecting, 6revascularization or regeneration for,
243-246Periapical surgery
anatomic indications for, 333-334, 333f-334f
clinical problem examples of, 331b, 332f, 351b, 352f
failure of previous surgery indicating, 337-338, 339f
iatrogenic obstructions indicating, 334-337, 335f-338f
indications for, 326-330, 326f-330frationale for, 325-326reaction to foreign bodies from, 330-333,
331f-332fPeriapical surgery techniques, in vitro
apical bevel, 339-340, 340fcarriers for placement of MTA, 345,
345fcleaning canal to greater depth, 342fcompaction of fillings with pluggers, 345,
345f-346fcompleted apical preparation, 344-345,
344fmanufactured ultrasonic tip with 3mm
cutting length, 340-341, 340f-342foverview of, 339-345ultrasonic diamond-tipped instruments,
341, 341f-342fultrasonically energized K-files, 341-344,
343f-344fPeriapical surgery techniques, in vivo
anesthesia and hemostats, 346clinical problem examples of, 348b, 349f,
351b, 352fcomplications, 353curettage of soft-tissue lesion penetrating
bone, 348
postsurgical care, 353root apex exposure in absence of
periapical lesion, 348, 348f-349froot-end cavity preparation, 349-351,
350f-351froot-end fillings:material/placement, 351,
352froot-end resection, 349, 350fsoft tissue flap design, 346-348,
347f-348ftissue positioning and stabilization,
352-353, 352fPeriapical tissue. see necrotic pulpPericoronitis, 5, 5fPeriodontal abscess, acute
acute periapical abscess vs., 8-9, 73-74, 73f
bony lesions of pulpal origin vs., 73-74, 73f
Periodontal diseaseacute periodontal abscess in, 73-74, 73faggressive periodontitis in, 77-78, 78fcemental tears in, 78-80, 80fchronic periodontitis. see chronic
periodontitisexternal root resorption in, 78, 78b, 79flesions involving furcation in,
75-77, 78fmobility found in teeth with, 9-10probing in endodontic evaluation,
8-9, 9fpulpally induced lesions vs., 73-80,
73f, 81fradiographic changes in, 67-68,
67f-68froot or tooth resections for, 399f
Periodontal ligament (PDL)inflammatory replacement resorption
and, 432-433working length determination using,
178-180, 180fPeriodontal ligament stem cells (PDLSCs),
244Periodontal probes
checking periodontal attachment levels with, 71-72, 72f
diagnosing chronic periodontitis with, 72f
diagnosing periodontal vs. pulpally induced defects with, 75-77
pulpal diagnosis using, 8-9, 8f-9fsounding location of crestal bone
with, 72tooth resection with, 404, 405f
Periodontal surgical dressing, in crown lengthening, 369, 369f
Periodontitisadvanced, 68, 68faggressive, 77-78, 78fchronic. see chronic periodontitis
Periapical surgery techniques, in vivo (Continued)

474 Index
Periodontiumbony lesions not originating from
periodontal or pulpal pathosis in, 87-95
predictable dimensions of, 72root resection considerations, 400-401,
400f-401fsurgical management of defects in
marginal. see crown lengtheningPerio-endo lesions, 81-82Periradicular radiographs, working length
determination, 184-185, 185fPeriradicular surgery
clinical problem examples of, 387b, 387f, 391b, 392f-393f, 393b, 405b, 406f
furcation perforations indicating, 388-390, 388f-391f
lateral canals indicating, 384-388, 385f-387f
overview of, 384root fractures indicating, 392-393, 392froot resection technique. see root
resectiontooth resection recommendations for,
405, 405ftooth resection techniques for, 403-405,
404f-405fPeriradicular surgery, case selection criteria
cervical resorptions, 398fcoronal fractures, 396fextensive caries, 398ffurcation perforations, 396firremovable canal fillings, 398firreparable strip perforations, 397firretrievable separated instruments, 397fnonnegotiable root canals, 397foverview of, 394-395periodontal defects, 399fpost perforations, 396fvertical root fractures, 395f
Persistent idiopathic facial pain (PIFP), 123
Phenol, not for use in root canal, 214PiezoFlow Ultrasonic Irrigation Needles,
211PIFP (persistent idiopathic facial pain), 123Plastic core carriers, removing, 286-289,
287f-288fPluggers
compaction of filling material with, 345removing gutta-percha, 456
Polycaprolactone, in resin-bonded obturation, 230
Post herpetic pain, 130Postendodontic restorations, 440-441Posterior teeth
access openings through, 160-162, 160f-161f
electric pulp test on, 14, 16festablishing working length in, 182intraradicular posts for, 445managing multicanal, 154, 154f-155f
necrotic pulps in, 310-315, 311b, 312f-313f, 315f
permanent restoration of, 445-447, 446f-447f
preparing access opening in, 160-162, 160f-162f
radiographs of coronal fractures of, 49, 50f
Postman, Dr. Neil, 218-219Posts. see intraradicular postsPostsurgical care, periapical surgery, 353Posttreatment disease. see treatment failurePrematurities, treatment of, 128, 128f-129fPremolars
anesthesia placement for, 321-322finding S-shaped canals in maxillary,
267, 267flingual edge removal in multirooted,
105f, 110, 181locating canal orifices in, 171-173,
172f-173fmultiple canals in, 99-101, 102fnecrotic pulp management in, 310-311orifice identification in mandibular, 173fperforations into furcation of, 165, 457radiographic assessment of working
length of, 186, 188fradiographic diagnostics of, 37, 39fremoving existing restoration in
maxillary, 274f, 281resection of buccal root in maxillary,
407-408, 408b, 411fProfinder file, 205Prophylaxis cup, heat tests using, 13-14,
15fPro-Root MTA, 137-138, 138fProUltr PiezoFlow irrigation device, 211ProUltra PiezoFlow Ultrasonic Irrigation
Needles, 211ProUltra tips, 162, 163f, 253-254, 276Pulp canal obliteration (PCO), from
luxated tooth, 426, 426fPulp caps, use of MTA for, 137-138, 138fPulp chamber
calcifications in, 162, 163fpreventing coronal perforations,
164-166, 164f-166fpreventing coronal perforations in, 163fremoving restorative materials from,
276-281, 276fsealing when restoring posterior teeth,
445-446Pulp exposure from traumatic fracture,
144-145Pulp horns, access entry through, 158,
158f-159fPulp revascularization, 244Pulpal diagnosis, after testing
aerodontalgia/barodontalgia, 19final pulpal diagnosis, 20irreversible pulpitis, 18-19
irreversible pulpitis not localized, 19necrotic pulp, 19normal, 17reversible pulpitis, 17-18
Pulpal necrosis. see necrotic pulpPulpal pathosis. see also abscesses, acute
periapical; clinical examinations; testing techniques
accuracy problem in, 1aerodontalgia/barodontalgia in, 19chronic sinus tracts of. see sinus drainage
tracts of pulpal origincontroversies and highlight of disease
interactions, 71dental history indications in, 2diagnosing bony defects from. see bony
defects, from pulpal/periodontal pathosis
diagnosing in occlusal discrepancies, 120-121
differential diagnosis in, 11external root resorption vs., 78,
78b, 79ffurcation/lateral lesions without loss of
attachment in, 80-82, 81finterpreting historical data and
subjective findings, 2-3lesions confused with periodontal lesions,
80-85, 81fperiodontal lesions involving furcation
vs., 75-77, 78fpulpally induced vs. periodontal lesions,
80-85radiographs of, 10-11, 10b, 10fradiographs of caries in, 46, 46fsensibility (vitality) testing in, 11-12working length determination in,
190-193, 190b, 191f-192fPulpal vitality, preserving. see vital pulp
therapyPulpectomy
defined, 308managing irreversible pulpitis with,
308-309, 308fposterior teeth with irreversible pulpitis
requiring, 309Pulpitis. see irreversible pulpitis; reversible
pulpitisPulpotomy
calcium hydroxide used in, 137, 138fdefined, 144irreversible pulpitis requiring, 308-310,
309f-310fMTA used in, 137-138, 138fpulp exposure from caries indicating,
144, 144fpulp exposure from traumatic fracture
indicating, 144-145, 145f-147f
QQuartz fiber posts, 448
Posterior teeth (Continued) Pulpal diagnosis, after testing (Continued)

Index 475
RRadiographic images, creating
beam angulation directives, 25-28clinical directives for, 41correctly and accurately, 22, 29-31,
29f-31fdigital and cone-beam computed
tomography for, 37-39evaluating quality of, 28-31exposure control when, 23, 23fhandling film and sensors in, 23incorrect angulation effects, 32-36limitations of, 184-185normal structures in, 36, 36fpositioning film and sensors for, 24-25
Radiographic images, interpretingcementoma, 65, 66fclinical problem, 10b, 10fdental caries, 46-47, 46f-48fdevelopmental cysts, 66, 66f-67fdeviations from normality, 42endodontic failure, 64-65, 65ffunctions of, 42healed endodontic lesions, 66, 67fperiodontal lesions, 67-68, 67f-68fpulpal diagnosis and, 10-11, 10fpulpal necrosis in periapical tissues,
60-63, 61f-63fpulpal necrosis, lateral changes of, 63-64,
63f-64fradiolucent anatomic structures, 55-58,
56f-58fradiopaque structures, 58-59, 58f-60fresorption, 52, 52f-55ftooth anatomy, 43, 44f-45ftooth fractures, 49-51, 49f-51fvertical root fractures not visible in, 91,
93fRadiolucency
loss of bone in periapical area producing, 10f, 11
overexposed radiographs creating, 23radiographic interpretation influenced by,
55-58, 56f-58ftransient apical breakdown from luxated
tooth, 427Radiopaque structures
clinical problem example of, 58b, 60finfluencing radiographic interpretation,
58-59, 58f-60fRC-Prep chelate, 198, 212Recapitulation
loss of working length from failure to perform, 196, 197f
for problems when preparing to obturate, 231
Rectangular flap, soft tissue, 335, 347fRegeneration. see revascularization or
regenerationReplacement resorption, 52, 55fReplantation, criteria for intentional, 115,
115f
Resections. see tooth resection (hemisection)Resin-bonded obturation
illustration of, 230foverview of, 230problems identified after, 234-238
Resorption. see also external resorption (ER); inflammatory replacement resorption (IRR); inflammatory resorption; internal resorption (IR)
apical complex altered by, 178, 179f-180f
cervical, 259-261, 261f-262f, 398fcrown lengthening indications for,
375-379, 376b-377b, 376f-379fproblem solving of, 254, 255fradiographic tooth changes associated
with, 52Restorations. see also treatment failure
access opening problems in large, 166-167, 166f-167f
access opening problems in removal of, 156, 156b, 156f
clinical problem example of, 17b, 18fcrown lengthening for, 361, 361firreversible pulpitis in teeth with, 19marginal problems, avoiding in, 361,
362fpersistence/pathosis from coronal
leakage in, 109-110, 109f-111fpossible perforation of access
openings in, 158, 158fradiographs of recurrent decay in,
47, 48fremoval of, 274-276, 274f-275freversible pulpitis caused by, 17-18,
17b, 18f, 305-307, 306f-307froot resection considerations for, 401
Restorations, of endodontically treated teeth. see also intraradicular posts; treatment failure
anterior teeth factors in, 445, 446fcase study example of, 442b, 443fcontaminated root fillings due to coronal
leakage in, 460-461, 460ffactors influencing choices in, 445postendodontic and intertreatment
temporary restorations in, 440-441
posterior teeth factors in, 445-447, 446f-447f
problem-solving issues in, 439restoring access openings in, 441-445,
444fRevascularization or regeneration, 243-246Reversible pulpitis
clinical problem example of, 17b, 18fdiagnosis of, 17-18, 18fsigns/symptoms of, 305-307, 306f-307f
Rinn XCPpositioning film or sensor position,
24, 24fradiation beam angulation and, 25, 27f
Root apex exposure in absence of periapical lesion
clinical problem example of, 348b, 349foverview of, 348, 348f-349f
Root canal anatomies. see also calcified canals; ledges; resorption
C-shaped canals, 262-263, 263f-265f, 400-401
extra canals, 158-160, 159ffalse canals, 202fimmature root development/necrotic
pulp. see apexificationmoderate-to-severe curvature of, 265,
266foverview of, 195recognizing types of deviations, 269,
269fS-shaped, 267-268, 267f-269fstrip perforations, 202f-203fzips, 201f
Root canal, cleaning and disinfectingbest use of disinfectants, 214-216clinical problem, 210bas neglected phase of, 209purpose of chelator solutions, 212,
213f-214fpurpose of disinfectants, 214purpose of intracanal irrigants, 209-212,
210f-212frequired for success of obturation,
230-231Root canal, enlarging and shaping. see also
access openings; working length determination
beyond canal terminus, 200-202, 203fcontemporary techniques, 195, 204-205crown-down technique, 205, 206fdeviations, 199, 199f, 201f-203fexcessive removal of root dentin, 202failure to properly, 204key role of irrigants during, 196, 204,
209-212, 210f-212floss of working length. see working
length, loss ofin moderate-to-severe canal curvature,
265, 266foverview of, 195problems in C-shaped canals, 262-263traditional techniques, 195
Root canal obturation. see also gutta-percha obturation techniques
challenges of, 218-219clinical problem, 223bguiding principles of, 230-231problems during, 232-234, 233f-234fproblems identified after, 234-239,
235f-238fproblems preparing canal, 231-232,
231f-232fresin-bonded techniques, 230, 230froot canal sealers, 219, 219f-221fviewing radiographic voids after, 238-239

476 Index
Root canal sealers. see sealer, root canalRoot canal treatment. see also orifice
locations, identifying; treatment failure; working length determination
correct diagnosis for, 20furcation or lateral lesions without loss of
attachment indicating, 80-82, 81firreversible pulpitis indicating, 18-19radiographic interpretation for, 10-11reversible pulpitis not indicating, 18tooth anatomy evaluation for, 43,
44f-45fvertical root fracture caused by, 91vital treatment of pulp vs. indications
for, 134-137, 136b, 137fRoot canal treatment, revision of
clinical problems, 276b, 277f-278f, 278b, 293b, 294f
overview of, 273-274preventing instrument separation during
root canal procedures, 296-297, 297f
removal of restorative materials from pulp chamber, 277f
removing existing restorations, 274-276, 274f-275f
removing gutta-percha in large canals, 281, 282f
removing gutta-percha in small canals, 281-285
removing gutta-percha in small canals, apical half of, 282f, 284-285, 285f
removing gutta-percha in small canals, coronal half of. see gutta-percha, removing in coronal half of small canals
removing intraradicular posts, 276-281, 277f-281f
removing metallic core-carrier obturators, 291-293, 292f-293f
removing metallic objects with Hedström files, 289-290, 290f
removing metallic objects with Masserann kit, 290-291, 291f
removing metallic objects with specialized forceps, 290
removing metallic objects with ultrasonic instrument, 289, 289f
removing paste filling materials, 285-286, 286f
removing plastic core carriers, 286-289, 287f-288f
removing restorative materials from pulp chamber, 276-281, 276f
removing separated instruments. see separated instruments
removing silver cones, 294-296, 294f-296f
Root fracturesclinical problem example of, 393b, 393fmidroot, 49, 50fsurgically repairing problems from,
392-393, 392f
threaded posts at risk for, 448, 449fvertical root. see vertical root fractures
Root perforations, as false canals, 199Root perforations, response of
periodontium toclinical problem examples of, 85b,
86f-87ffurcation perforations, 86finfiltration of marginal periodontium,
87fmisdirected posts, 87foverview of, 84-85strip perforations, 86f-87f
Root resectionbasic recommendations for, 402fcase selection. see periradicular surgery,
case selection criteriaclinical problem examples of, 394b, 395f,
408b, 411f, 414b, 415fendodontic considerations prior to,
395-400, 399fgeneral considerations for, 393-394,
394fidentifying root canal space, 349, 350foutcomes assessment of mandibular
molars, 408-414, 412f-415foutcomes assessment of maxillary
molars, 407-408, 407f-411fperiodontal considerations prior to,
400-401, 400f-401frestorative considerations before/
after, 401surgical techniques for, 401-403, 402f
Rootscrown lengthening contraindications,
363, 363fdecreasing sensitivity in exposed, 18developmental lingual groove on,
92-93, 94felectrical pulp test on immature,
14, 16fmechanical perforation of. see root
perforations, response of periodontium to
radiographs capturing apices of, 24, 24fRotary NiTi instruments. see NiTi
(nickel-titanium) instruments, rotaryR-phase instruments, 204Rubber dam. see dental (rubber) damRubber polishing wheel, heat tests using,
13-14, 15f
SSCAP (stem cells from the apical papilla),
244Sealer, root canal
gutta-percha thermoplasticized core-carrier using, 227
problems identified after obturation, 234-236
removal of, 285role and use of, 219, 219f-221f
Sensibility (vitality) testing. see also pulpal diagnosis, after testing
acute periodontal abscess diagnosis with, 73-74
anesthetic test for, 14-15cold test for, 12-13electric pulp test for, 14heat test for, 13-14percussion findings after, 6-7periodontal abscess diagnosis using, 8-9pulpal diagnosis using, 11-12test cavity in, 17thermal pulp testing with rubber
dam for, 14using when radiographic assessment is
difficult, 58, 59fSeparated instruments
blockage/loss of working length from, 198-199, 199f-200f
bypassing removal of, 301, 301f, 397f
endodontic removal of, 298-301, 300f-302f
preventing, 296-297, 297fremoval of, 298-301removal with GG/Peeso bur heads,
298, 298f-299froot/tooth resections for irretrievable,
397ftreatment failure from, 112-115,
113f-115fSeptocaine (articaine), 346Sialolithiasis pain, 130Silicon fiber posts, 448Silicon stops, working length measurement,
184, 184fSilver cones
external resorption from, 104f, 107inadequate coronal seals from,
109-110, 110fobturation using, 218-219occlusal leakage from, 239removal from root canal of, 294-296,
294f-296f, 334-335, 335fremoval with Hedström file, 289-290,
290fSinus, and radiolucency, 55, 56fSinus drainage tracts, lesions of chronic
periodontitis and, 74Sinus drainage tracts of pulpal origin
chronic periodontitis vs. periapical lesions, 74
periapical abscess from, 9permanent periodontal attachment
loss from, 83-84, 83f-85f, 84b
through gingival sulcus, 82-83, 82f-83f, 83b
Sinusitis, maxillary, 129-130, 130fSLOB (same lingual, opposite buccal)
rule, working length determination, 186-187, 188f
Smart X Tips, 162
Root fractures (Continued)

Index 477
Smear layer removal, 215fapexification requiring, 242chelating agents for, 212, 213f-214fcrown-down technique for, 205disinfectants more effective after,
214-216, 215fgutta-percha plugs penetrating dentinal
tubules after, 227, 229fintracanal aspiration technique for, 211irrigants not useful for, 209, 211-212,
213f-214fresin-bonded obturation requiring, 230sealer penetrating dentinal tubules after,
219, 220fsodium hypochlorite not useful for, 212,
212fSodium hypochlorite (NaOCL)
as best intracanal irrigant, 212chelating agents alternating with, 212clinical problem, 210bdelivery of, 211, 211fenhancing efficacy of, 209-211enlarging and shaping canal with, 196,
204final rinsing agents for use after, 211-212impact on dentin, 211necrotic pulp removed by, 310-311pulpectomies using, 308root canal sealer removed by, 285
Soft-tissueenucleation of, 348flap design in periapical surgery,
346-348, 347f-348frepositioning/stabilizing before sutures,
352-353, 352fswelling from acute periapical abscess, 5funion with connective tissue in
horizontal root fractures, 436, 437fvisual inspection of, 4
Solvent techniqueremoving gutta percha with, 285, 285fremoving plastic core carriers with,
288-289Sounding, location of crestal bone, 72Splinting
avulsion injury guidelines, 429-430extrusive luxation injuries, 423-424lateral luxation injuries, 424after tooth resection, 403-404
S-shaped canals, 267-268, 267f-269fStafne’s defect, 58, 58fStainless steel instruments. see also K-files
NiTi instruments vs., 204pathfinding using, 205
Stem cells from the apical papilla (SCAP), 244
Stepwise excavation, for indirect pulp caps, 139
Sterile paper points, dehydrating root canal, 233-234
Stieglitz forcepsremoving metallic objects, 290removing plastic core carriers, 288, 288f
Stopping. see dental stoppingStops, instrument
malpositioned, 195, 197fpreventing enlarging beyond canal
terminus, 201Strip perforations, 390, 391f
anatomy of root causing, 388, 390finstrument error resulting in, 199,
202f-203f, 205, 206f, 388, 390f-391f
posts too large for roots causing, 457, 458f
root/tooth resections for irreparable, 397fSubjective findings, in pain diagnosis, 2-3Subluxation injuries, diagnosing/treating/
prognosis of, 422-423, 423fSubmarginal flap, soft tissue, 346, 347fSulcus depth
endodontic evaluations probing, 8, 8fperiapical abscess diagnosis using, 9
Surgical anatomy, in vivo, 346Surgical procedures. see also periapical
surgery; periradicular surgerycrown lengthening, 364, 364f, 364troot resections, 401-403, 402f
Surgical trephination, for painful teeth, 316-319, 318f-319f
Swelling, in periodontal /acute periapical abscesses, 73, 73f
Sybron Endo Vitality Scanner, 16f
TTAB (transient apical breakdown), from
luxated tooth, 427Tactile sensation, in working length
determination, 189, 189fTapered self-threaded posts, 448, 448tTemporary restorations, 440-441Temporomandibular disorder. see TMD
(temporomandibular disorder)Test cavity, pulpal diagnosis and, 17Testing techniques, 12-17
anesthetic test, 14-15cold test, 12-13dental dam for thermal pulp testing, 14electric pulp test, 14heat test, 13-14sensibility (vitality), 11-12test cavity, 17
Thermal testing. see also nonsurgical treatment, incomplete; pulpal diagnosis, after testing
anesthetic test as, 14-15applying dental dam for, 14cold test as, 12-17electric pulp test as, 14heat test as, 13-14incomplete nonsurgical treatment and,
99necrotic pulp diagnosis using, 310patient symptoms reproduced in,
11-12positive or negative aspect of, 11
qualitative aspect of, 11reversible pulpitis signs/symptoms in, 305
Thermoplasticized core-carrier, gutta-perchaillustrations, 228f-229finjection techniques, 225-227, 226f-227foverview of, 227problems after obturation, 234problems during obturation, 234
Threaded posts, 448, 448t, 449fTIMPs (tissue inhibitors of
metalloproteinases), bonding with, 243Tissue
closing in crown lengthening, 367-369, 368f
crown lengthening complications, 371-372, 371f-372f
periodontal surgical dressing indications, 369
position and stabilization in periapical surgery, 352-353, 352f
thinning or undermining in crown lengthening, 366, 366f
TMD (temporomandibular disorder), 129fdental signs of, 125, 125fdental symptoms of, 125-127, 126f-127fhot, moist compresses for, 129maxillary symptoms of, 124-125, 124fmuscle relaxant prescription for, 129NSAIDs for, 129occlusal adjustment for, 128, 128f-129foverview of, 123-127patient education about stress causing,
129stones and finishing burs for, 127, 128f
Tongue, positioning film around muscular, 25, 27f
Tooth anatomyapical root. see apical root anatomycanal deviations in, 199, 199f, 201f-203fclinical problem example of, 43b, 45fnecrotic pulp and immature. see
apexificationradiographic evaluation of, 43, 44fsurgical treatment planning and, 346,
357-358, 357f-359fTooth bleaching, creating hypersensitivity,
133Tooth fractures. see also coronal fractures;
root fractures; traumatic tooth injuries#17 explorer detecting, 5-6, 6fcrazes and cracks vs., 418-420, 419fcrown lengthening for deep, 361-362,
362fdefinition of, 419f-421fperiodontal probing indicating, 4f, 9pulp exposure in traumatic, 144-145
Tooth hypersensitivity. see dentin hypersensitivity
Tooth isolationcrown lengthening indications, 360,
360f-361fdental dam used for, 152-153, 152f-153f
Thermal testing (Continued)

478 Index
Tooth resection (hemisection)case selection. see periradicular surgery,
case selection criteriaclinical problem example of, 405b, 406fmandibular molar root outcomes after,
408-414, 412f-414fmaxillary molar root outcomes after,
407-408, 407f-411foverview of, 393-394, 394frecommendations for, 405, 405fsurgical techniques for, 403-405,
404f-405fTooth Slooth, 7, 125-126, 126fTooth structure
excessive removal of root dentin weakening, 202
immature root formation creating weakness in, 242-243
removing unsupported, 156Transient apical breakdown (TAB), from
luxated tooth, 427Transillumination, of fractured tooth,
87-88, 88fTraumatic tooth injuries
avulsion injuries, 427-431, 427f-430fconcussion, 422, 423felectrical pulp test results on, 14extrusive luxation, 423-424, 423fhorizontal root fractures, 434-435,
434f-435fhorizontally fractured teeth, healing
responses to, 435-437, 435f-437fintrusive luxation, 424-425, 425flateral luxation, 424, 424foverview of, 421-425, 422fresorption associated with, 431-434,
431f-434fsensibility testing of, 6-7sequelae to luxation injuries. see luxation
injuries, sequelae tosplinting times for, 437, 437tsubluxation, 422-423, 423f
Treatment failurecontaminated canal space causing, 107diagnoses confused with, 103-106,
103f-106f, 104b, 106bdiagnosing, 106-107, 116, 116finadequate apical seal causing, 107-109,
107f-108f, 108binadequate coronal seal causing, 109-110,
109f-111fincomplete nonsurgical treatment
causing, 99-101, 101f-103f, 103bnonnegotiable canals causing, 111-112,
112fnonsurgical treatment success vs., 97,
98f-99foverview of, 97separated instruments causing, 112-115,
113f-115fTreponema lecithinolyticum, 77Triangular flap, soft tissue, 335, 346
Trigeminal neuralgia, 123Trisection, 393Twisted Files, 204
UUltrasonic instruments
gutta percha in coronal half of small canals removed with, 283-284, 283f
instrument fragments removed with, 300-301, 301f
intraradicular posts removed with, 278-280
metal objects removed with, 283f, 289, 289f
paste filling materials removed with, 286restorative materials in pulp chamber
removed with, 276, 277fUltrasonic instruments, types of
diamond-tipped, 341, 341f-342fenergized K-files, 341-344, 343f-344ffile separation problem with, 300-301fracture around access opening causing,
284birrigation devices, 211manufactured tip with 3mm cutting
length, 340-341, 340f-342fUnderexposure, radiographic, 23, 23f
VVertical compaction
gutta-percha techniques for, 224-225, 225f-226f
gutta-percha thermoplasticized core-carrier using, 227
resin-bonded obturation using, 230Vertical root fractures
chronic sinus drainage tracts from, 103, 104f
clinical and radiological changes of, 103-106, 105f
clinical problem examples of, 91b, 92f, 104b, 105f-106f, 106b, 381f, 382b
crown lengthening indications in, 379, 381f, 382b
differential diagnosis of, 89-92, 91f, 93f-94f
periodontal probing in, 9, 103, 104fradiographic diagnosis of, 49-51, 51f,
103f, 105froot resection indications, 395f, 409,
412f-413fVisual inspection
clinical problem example of, 3b, 3fpulpal diagnosis using, 3-5
Vital pulp therapycontemporary dentistry using, 133-134direct pulp cap with carious exposure.
see direct pulp caps, carious exposure in
direct pulp cap with iatrogenic exposure, 142-144, 143f
indirect pulp capping for, 139
Vital pulp therapy (Continued)materials for, 137-139, 138f-139fpulpotomy procedures for. see pulpotomyroot canals instead of, 135-137, 137fviable options for, 134, 134f-136fwhen to use, 134-135
Vitality testing. see sensibility (vitality) testing
WWear patterns, sensitivity to percussion
from, 7Wedelstadt chisel, alveolar bone recontours,
367, 368fWeeping canals, 200-201Working length determination, 162
anatomic basis for challenges with, 177-181
apical foramen position in, 181, 181fapical portion of root canal system in,
180-181, 180fapical root anatomy. see apical root
anatomyclinical problem examples of, 183b, 184f,
190b, 191f-192f, 192bdeveloping root structure in, 177-178,
178f-179felectronic apex locator for, 187-189external apical root morphology in, 178,
179f-180finternal morphology at end of root canal
in, 178-180, 180fother clinical techniques for, 189, 189fposttreatment implications/outcomes
based on, 191f, 193pulpal/periapical status in, 190-193,
190b, 191f-192fradiographic techniques in, 184-187,
185f-188fremoving necrotic pulp by establishing,
312-313, 312f-313fWorking length, loss of, 196-199
creating new working length coronal to blockage for, 198, 198f
errors causing, 196, 196f-197fnewer NiTi instruments and, 199packed dentinal/tissue debris causing,
197-198, 198fpreparing to obturate, 231f-232fseparated or broken NiTi instruments
causing, 196-199, 199f-200fsurgical correction for, 198, 199f
ZZinc oxide eugenol (ZOE)
coronal perforations using, 164-165, 166f
minimizing leakage of, 440tooth resections using, 405f
Zips, canal, 199, 201fZirconium posts, 449Zygoma, and TMD, 124-125, 124f