Embed Size (px)
Citation preview

GUIDOR ® easy-graft
100 % alloplastic bone graft system
Soft from the syringe
Mouldable in the Defect
In situ hardening

2 3
Simplifying bone regenera-tion techniques In their forward thinking 2003 arti-cle (1), Hammerle & Jung stated: “Developments in bone augmen-tation procedures can be related either to simplification of the clin-ical handling or to influencing of biological processes. To simplify clinical handling, new materials should comprise a matrix with optimal cell ingrowth capacities and good mechanical properties, providing space for tissue regen-eration. No membrane and no specific procedures for mechan-ical fixation should be necessary. This would reduce the technique sensitivity and increase the pre-dictability of bone augmentation. The use of synthetic (alloplastic) materials would result in lower surgical risks and lower morbidity
in augmentation procedures and would represent an important step forward in simplifying bone regeneration techniques.”…
Minimally invasive surgery and site-specific access flaps New tools to split the crest are now available, including bone expanders and the piezoelectric scalpel. With such tools, the idea of a reduced or flapless approach to implant dentistry, alleviating post treatment side effects, accel-erating healing and avoiding bone resorption caused by periosteal elevation becomes feasible… …with GUIDOR easy-graft ® and its stunningly easy handling such considerations become reality.
“Minimally invasive” and “Immedi-ate-delayed” implant protocols are ideal cases for mouldable bone graft materials with in-situ hardening.
GUIDOR easy-graft®: The Handling Advantage
GUIDOR easy-graft®: Trend-Setter
The GUIDOR easy-graft® principle:
1/4 million applications since 2007Launched in Switzerland following collaboration with Zurich University and then Internationally in 2007, GUIDOR easy-graft® has quickly established itself as a leading alloplastic material with over 250,000 applications. (1)
GUIDOR easy-graft® products are available in two resorption formats.
Both offer: • 100 % Alloplastic material
(no substances of animal or human origin)
• High porosity• Osteoconductivity• Syringe application• Mouldable, in situ hardening
Injectable granules Mouldable mass Stable scaffold
2 3

Zeit [Stunden]
0 1 2 3 4 50.5 1.5 2.5 3.5 5.54.5
100
80
60
40
20
0
Time [hours]
Rel
. N
MP
am
ount
in e
asy-
graf
t® [%
]
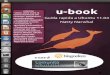
Stage 1) BioLinker® is extract-ed within hours.BioLinker® makes easy-graft®-
CLASSIC and easy-graft®CRYSTAL mouldable. In the defect, BioLink-er® is extracted by incoming blood, promoting rehardening of the ma-terial. More than 90 % of BioLinker® is removed from the bone graft substitute within three hours (1) and excreted through the urine within 1–3 days (2). BioLinker® contains NMP which is widely used in phar-maceutical and medical devices such as dental membranes, subcu-taneous drug-release systems etc.
Stage 2) The polylactide coating (PLGA) is resorbed over a few weeks.In parallel to the healing and regen-eration process the PLGA coating and adhesive connection between the granules gradually weakens (three to six weeks in vitro), expos-ing the osteoconductive scaffold.
PLGA polymers are widely used in devices such as membranes, screws and plates for maxillofacial surgery, suture anchors, and cages for spinal surgery. Resorption of PLGA releases small amounts of lactic and glycolic acid. Lactic acid is found naturally in the body and is degraded by metabolic processes. Glycolic acid is a fruit acid and can be degraded in the body or excret-ed with the urine.
GUIDOR easy-graft®: Mouldable from the Syringe, in-situ Hardening
GUIDOR easy-graft®: Resorption Process for BioLinker® and Polymer Coating
The resorption processes for BioLinker® and PLGA polymer coating takes place in two stages:
Resorption process for PLGA polymer coating
fig 1Each granule is factory pre-coated with a polylactide (PLGA) polymer to a depth of 10µm
fig 2The supplied BioLinker® is added to the syringe and allowed to thoroughly wet the granules softening the polylactide (PLGA) polymer coating creating a sticky easy-to-use graft.
fig 3Removal of BioLinker®
fig 4easy-graft® presents a homogenous mouldable mass, which is easy to apply directly from the syringe.
fig 5Compaction of the introduced easy-graft® combined with capillary action from the bone bed causes blood to permeate the porous material. In contact with blood, easy-graft® quickly hardens forming a scaffold of interconnected granules, which fit the defect morpholo-gy perfectly. In larger defects a second application can be applied immediately after the first.
fig 6GUIDOR easy-graft® products will not “set” or block the syringe. Unlike cements the hardening of easy-graft® is controlled and without heat generation. BioLinker® temporarily softens the PLGA coating which remains soft only until it is washed out.
Extraction of BioLinker® from easy-graft®
More than 90 % of BioLinker® is removed within three hours.
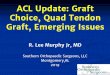
During resorptionColored electron microscope image of easy-graft®CRYSTAL during resorption. The resorption of the PLGA coating (blue) exposes the biphasic calcium phosphate (white).
Resorption of the PLGA coatingElectron microscope image from an in-vitro degradation experiment
4 5

6 7
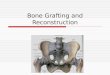
Handling (fig 1)Retracting the plunger makes wetting of the granules with BioLinker® easier.
Condensing in the defect (fig 2) If possible, GUIDOR easy-graft® products should be condensed in the defect for an intimate contact be tween the material and bone. The granules are pressure-stable and abrasion-resistant, which prevents potentially inflammatory debris from forming. When applied to large areas the material can be moulded and then compressed (aseptic conditions) with the finger using moist gauze.
Dispensing the material (fig 3) GUIDOR easy-graft® products can be dispensed on a sterile dry surface after mixing with a dry instrument (aseptic conditions) and placed in several small defects during a single surgical procedure. The material does not harden until in contact with body fluids, consequently, this meth-od can be used for filling multiple small bone defects in one patient with one single 0.4 ml application.
Flexible, porous shell (fig 4) After mixing, GUIDOR easy-graft® products can be (aseptically) shaped into a thin shell between two sterile, smooth and dry surfaces after ad-dition of a few drops of sterile water or sterile saline solution. The flexible, porous shell can, for example, be used for fixing and as resorption pro-tection for autogenous bone chips or as a cover in an external sinus lift.
Direct bone contactPLGA absorbs small amounts of water which creates a slight volume increase thus improving the graft to surrounding bone tissue contact. In some cases the patient may have a slight feeling of pressure in the first few days after application and should be advised accordingly. When filling the defect the material should be condensed and not overflow the margin of the bone defect.
Reentry (fig 5a, 5b)Depending upon time scale, vis-ualization of granules embedded on the surface of new bone will be observed.When undertaking flapless or mini-mally invasive (membrane-free) sur-gery excess granules can sometimes be seen in the soft tissue. Granules in the soft tissue can easily be removed at reentry if desired.
GUIDOR easy-graft®: Tips and Tricks
fig 1 fig 2 fig 3
fig 4 fig 5a fig 5b
easy-graft®CLASSIC Brand easy-graft®CRYSTAL
Phase-pure beta-tricalcium phosphate (ß-TCP)
Composition A compound of biphasic calcium phosphate (BCP) (60 % hydroxyapatite (HA) and 40 % ß-TCP)
Phase-pure ß-TCP has been used in oral surgery for more than 25 years and is one of the most widely researched biomaterials.
Provenance Biphasic calcium phosphates were developed for orthopedic surgery (13) and subsequently gained favour in oral surgery.
Offering complete resorption via physiological (1) and cell based (2) mechanisms in 5 to 15 months (3). In clinical practice resorption of phase-pure ß-TCP is observed after shorter healing periods (4).
Resorptionprofile
The ß-TCP component resorbs completely via physiological and cell based mechanisms. The interconnected hydroxyapatite remains embedded in the implantation site and forms an integrated long-term osteoconductive scaffold with new bone (18).
The resorption of phase-pure ß-TCP takes place in parallel to bone regeneration.
Regenerativeapplication
As newly regenerated bone replaces the ß-TCP component, it interconnects with the porous hydroxyapatite. Integrated hydroxyapatite contrib-utes to preservation of the hard-tissue volume in bone structures threatened by atrophy (12).
In addition to GBR (5) CLASSIC format materials are documented in:
(6) • Filling periodontal defects (7) • Defects after removal of bone cysts (8)
• Implantology (9) (simultaneous grafting and implant placement)
• Socket preservation
(10)
• For closure of oroantral communications (11)
Indications In addition to GBR, CRYSTAL format materials are documented in:
(14) • Filling periodontal defects (15) • Defects after removal of bone cysts (16)
• Implantology (14) (two stage grafting and implant placement)
• Socket preservation (17)
GUIDOR easy-graft®: Quick Summary
Product easy-graft®CLASSIC
Reference no. C11-012 C11-013 C11-072 C11-073 C11-002 C11-003
Units 3 x 0.15 ml 6 x 0.15 ml 3 x 0.25 ml 6 x 0.25 ml 3 x 0.4 ml 6 x 0.4 ml
Granule size 500 – 630 µm 500 – 630 µm 500 – 1000 µm 500 – 1000 µm 500 – 1000 µm 500 – 1000 µm Indications for use and material
descriptionMaterial Phase-pure ß-tricalcium phosphate (> 99 %)
Product easy-graft®CRYSTAL
Reference no. C15-012 C15-013 C15-072 C15-073 C15-002 C15-003
Units 3 x 0.15 ml 6 x 0.15 ml 3 x 0.25 ml 6 x 0.25 ml 3 x 0.4 ml 6 x 0.4 ml
Granule size 450 – 630 µm 450 – 630 µm 450 – 1000 µm 450 – 1000 µm 450 – 1000 µm 450 – 1000 µm Indications for use and material
descriptionMaterial Biphasic calcium phosphate (60 % hydroxyapatite / 40 % ß-TCP)

Distribution
Sunstar Deutschland GmbH · Aiterfeld 1 · 79677 SchönauTel.: +49 (0)7673 885 10855 · Fax: +49 (0)7673 885 10844E-Mail: [email protected]
Page 2
1. Hämmerle and Jung, Bone augmentation by means of barrier membranes Periodontology 2000 Volume 33, Issue 1, pages 36-53, Oct 03.
Page 3
1. Data on file, Sunstar Degradable Solutions, Wagistrasse 23 8952 Schlieren, Switzerland.
Page 5
1. Data on file: Degradable Solutions, Wagistrasse 23 8952 Schlieren, Switzerland.
2a) World Health Organization (2001). Concise International Chemical Assessment Document 35 N-Methyl-2-Pyrrolidone. Organization, W. H. Stuttgart, Wissenschaftliche Verlagsgesellschaft mbH: 32.
2b) Bader M., Keener S. A. and Wrbitzky R.: Dermal absorption and urinary elimination of N-methyl-2-pyrrolidone Int Arch Occup Environ Health (2005) 78(8): 673-6.
2c) Bader M., Wrbitzky R Blaszkewicz M. and van Thriel C.: Human experimental exposure study on the uptake and urinary elimination of N-methyl-2-pyrrolidone (NMP) during simula-ted workplace conditions Arch Toxicol (2007) 81(5):335-46.
2d) Bader M., Wrbitzky R., Blaszkewicz M., Schaper M. and van Thriel, C.: Human volunteer study on the inhalational and dermal absorption of N-methyl-2-pyrrolidone (NMP) from the vapor phase Arch Toxicol (2008) 82(1): 13-20.
Page 7
1a) Zerbo I. R, et al. Localisation of osteogenic and osteoclastic cells in porous beta-tricalcium phosphate particles used for human maxillary sinus floor elevation. Biomaterials (2005) 26(12): 1445-51.
1b) Knabe C., Koch C., Rack A. and Stiller M.: Effect of beta-tricalcium phosphate particles with varying porosity on osteogenesis after sinus floor augmentation in humans. Biomaterials (2008) 29(14): 2249-58.
2a) Kondo N. et al. Bone formation and resorption of highly purified beta-tricalcium phosphate in the rat femoral condyle Biomaterials (2005) 26(28): 5600-8.
2b) Nair P. N., Luder H. U., Maspero F A., Fischer J. H. and Schug J.: Biocompatibility of Beta-tri-calcium phosphate root replicas in porcine tooth extraction sockets – a correlative histological, ultrastructural, and X-ray microanalytical pilot study J Biomater Appl (2006) 20(4): 307-24.
2c) Chazono M., Tanaka T., Kitasato S., Kikuchi T. and Marumo K.: Electron microscopic study on bone formation and bioresorption after Implanta-tion of beta-tricalcium phosphate in rabbit models J Orthop Sci (2008) 13(6): 550-5.
2d) Lan Levengood S. K, et al. Multiscale osteo- integration as a new paradigm for the design of calcium phosphate scaffolds for bone regeneration Biomaterials (2010).
3. Wälivaara, D. A. et al. Evaluation of 4 different bone graft substitutes and autogenous bone grafting in root-end resection osteotomies after retrograde root-filling with Intermediate Restora-tive Material (IRM): An experimental study in dogs. Open Journal of Stomatology, 2013, 3, 203-208.
4. Bone Augmentation, Material Science and Clinical Manual, Ruffiex and Kohli pg: 76, 84,132 and 152.
5. Fugazzotto P. A., Shanaman R., Manos T. and Shectman R.: Guided bone regeneration around titanium implants: report of the treatment of 1503 sites with clinical reentries Int J Periodontics Restorative Dent (1997) 17(3):292, 293-9.
6a) Zerbo I. R., Zijderveld S. A., de Boer A., Bronckers A. L., de Lange G., ten Bruggenkate C. M. and Burger E. H.: Histomorphometry of human sinus floor augmentation using a porous beta- tricalcium phosphate: a prospective study Clin Oral Implants Res (2004) 15(6): 724-32.
6b) Zerbo I. R, et al. Localisation of osteogenic and osteoclastic cells in porous beta-tricalcium phosphate particles used for human maxillary sinus floor elevation. Biomaterials (2005) 26(12): 1445-51.
6c) Suba Z., Takacs D., Matusovits D., Barabas J., Fazekas A. and Szabo G.: Maxillary sinus floor grafting with beta-tricalcium phosphate in humans: density and microarchitecture of the newly formed bone. Clin Oral Implants Res (2006) 17(1): 102-8.
6d) Knabe C., Koch C., Rack A. and Stiller M.: Effect of beta-tricalcium phosphate particles with varying porosity on osteogenesis after sinus floor augmentation in humans Biomaterials (2008) 29(14): 2249-58.
7a) Stahl S. S. and Froum S.: Histological evalua-tion of human intraosseous healing responses to the placement of tricalcium phosphate ceramic implants. I. Three to eight months J Periodontol (1986) 57(4): 211-7.
7b) Froum S. and Stahl S. S.: Human intraos-seous healing responses to the placement of tricalcium phosphate ceramic implants. II. 13 to 18 months J Perio (1987) 58 (2):103-9.
7c) Yassibag-Berkman Z., Tuncer 0., Subasioglu T. and Kantarci A.: Combined use of platelet-rich plasma and bone grafting with or without guided tissue regeneration in the treatment of anterior interproximal defects J Periodontol (2000) 78(5): 801-9.
8. Zerbo I. R., Bronckers A. L., de Lange G. L., van Beek G. J. and Burger E. H.: Histology of human alveolar bone regeneration with a porous tricalcium phosphate. A report of two cases Clin Oral Implants Res (2001) 12(4): 379-84.
9a) Reinhardt C. and Kreusser S.: Der Einsatz von polylactid beschichtetem Beta-Tricalciumphos-phat zum Verschluss von Mund-Antrum-Verbin-dungen Die Quintessenz (2009) 60(8): 891-9.
11c) Thoma D. S., Halg G. A., Dard M. M., Seibl R., Hammerle C. H. and Jung R. E.: Evaluation of a new biodegradable membrane to prevent gingival
ingrowth into mandibular bone defects in mini-pigs. Clin Oral Implants Res (2009) 20(1): 7-16.
12. Zafiropoulos G. G., Hoffmann O., Kasaj A., Willershausen B., Weiss O. and Van Dyke T. E.: Treatment of intrabony defects using guided tis-sue regeneration and autogenous spongiosa alo-ne or combined with hydroxyapatite/betatricalci-um phosphate bone substitute or bovine-derived xenograft. J Periodontol (2007) 78(11): 2216-25.
13a) Passuti N., Daculsi G., Rogez J. M., Martin S. and Bainvel J. V.: Macroporous calcium phosphate ceramic performance in human spine fusion Clin Orthop Relat Res (1989) (248): 169-76.
13b) Delecrin J., Takahashi S., Gouin F and Passuti N.: A synthetic porous ceramic as a bone graft substitute in the surgical management of scoliosis: a prospective, randomized study Spine (2000) 25(5): 563-9.
13c) Xie Y., Chopin D., Morin C., Hardouin P., Zhu Z., Tang J. and Lu J.: Evaluation of the osteo-genesis and biodegradation of porous biphasic ceramic in the human spine Biomaterials (2006) 27(13): 2761-7.
14a) Cordaro L., Bosshardt D. D., Palattella P., Rao W., Serino G. and Chiapasco M.: Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: histomorphometric results from a ran-domized controlled multicenter clinical trial Clin Oral Implants Res (2008) 19 (8):796-803.
14b) Froum S. J., Wallace S. S., Cho S. C., Elian N. and Tarnow D. P.: Histomorphometric compa-rison of a biphasic bone ceramic to anorganic bo-vine bone for sinus augmentation: 6- to 8-month postsurgical assessment of vital bone formation. A pilot study Int J Periodontics Restorative Dent (2008) 28 (3): 273-81.
14c) Lee J. H., Jung U. W., Kim C. S., Choi S. H. and Cho K. S.: Histologic and clinical evaluation for maxillary sinus augmentation using macropo-rous biphasic calcium phosphate in human Clin Oral Implants Res (2008) 19(8): 767-71.
15. Sculean A., Windisch P., Szendroi-Kiss D., Horvath A., Rosta P., Becker J., Gera I. and Schwarz, F: Clinical and histologic evaluation of an enamel matrix derivative combined with a biphasic calcium phosphate for the treatment of human intrabony periodontal defects. J Perio-dontol (2008) 79 (10):1991-9.
16. Piattelli M., Favero G. A., Scarano A., Orsini G. and Piattelli A.: Bone reactions to anorganic bovine bone (Bio-Oss) used in sinus augmenta-tion procedures: a histologic long-term report of 20 cases in humans Int J Oral Maxillofac Implants (1999) 14(6): 835-40.
17. Weiss P., Layrolle P., Clergeau L. P., Enckel B., Pilet P., Amouriq Y., Daculsi G. and Giumelli B.: The safety and efficacy of an injectable bone sub-stitute in dental sockets demonstrated in a human clinical trial Biomaterials (2007) 28(22): 3295-305.
18. Lan Levengood S. K, et al.: Multiscale osteo- integration as a new paradigm for the design of calcium phosphate scaffolds for bone regenera- tion. Biomaterials (2010).
Cited Reference Listing
Art
. Nr.
T120
06/
2015