-
Growth hormone prevents the development ofautoimmune
diabetesRicardo Villaresa,1, Dimitri Kakabadsea,1, Yasmina
Juarranzb, Rosa P. Gomarizb, Carlos Martínez-Aa,and Mario
Melladoa,2
aDepartment of Immunology and Oncology, Centro Nacional de
Biotecnología, Consejo Superior de Investigaciones Científicas,
E-28049 Madrid, Spain;and bDepartment of Cell Biology, Faculty of
Biology, Complutense University of Madrid, E-28040 Madrid,
Spain
Edited by Tak W. Mak, The Campbell Family Institute for Breast
Cancer Research, Ontario Cancer Institute at Princess Margaret
Hospital, University HealthNetwork, Toronto, ON, Canada, and
approved October 18, 2013 (received for review August 9, 2013)
Evidence supports a relationship between the neuroendocrine
andthe immune systems. Data from mice that overexpress or
aredeficient in growth hormone (GH) indicate that GH stimulates
Tand B-cell proliferation and Ig synthesis, and enhances
maturationof myeloid progenitor cells. The effect of GH on
autoimmunepathologies has nonetheless been little studied. Using a
murinemodel of type 1 diabetes, a T-cell–mediated autoimmune
diseasecharacterized by immune cell infiltration of pancreatic
islets anddestruction of insulin-producing β-cells, we observed
that sus-tained GH expression reduced prodromal disease symptoms
andeliminated progression to overt diabetes. The effect involves
sev-eral GH-mediated mechanisms; GH altered the cytokine
environ-ment, triggered anti-inflammatory macrophage (M2)
polarization,maintained activity of the suppressor T-cell
population, and lim-ited Th17 cell plasticity. In addition, GH
reduced apoptosis and/orincreased the proliferative rate of
β-cells. These results supporta role for GH in immune response
regulation and identify a uniquetarget for therapeutic intervention
in type 1 diabetes.
beta cells | Tregs
Growth hormone (GH) is a pleiotropic hormone that affectsa broad
spectrum of physiological functions, from carbohy-drate and lipid
metabolism to the immune response (1). Severalstudies have linked
GH with autoimmune diseases, although itseffects on the immune
system are still debated. Whereas somereports using GH-deficient
mice indicate that it does not affectimmune competence (2), others
suggest that GH is necessary forcorrect immune system development
(1, 3). The GH receptor(GHR) is expressed by several lymphocyte
subpopulations (4).GH stimulates in vitro T and B-cell
proliferation (5) and Igsynthesis (6); enhances human myeloid
progenitor cell matura-tion (7); and modulates in vivo Th1/Th2 (8)
and humoral im-mune responses (1). In addition, therapeutic
activation of theGH/STAT5B axis is postulated as a target for
restoring mucosaltolerance in Crohn disease (9, 10). A single point
mutation inSTAT5B limits its DNA binding activity as well as
maintenanceof FOXP3 expression by Treg cells in nonobese diabetic
(NOD)mice (11). These mice develop type 1 diabetes, which is
char-acterized by autoimmune destruction of pancreatic β-cells due
tothe effect of environmental factors on genetically
predisposedindividuals (12, 13). Although this murine model does
notcompletely mimic the human disease, most steps in the
patho-genesis, including prodromal and clinical symptoms, are
closelycomparable (14).Despite the interdependence of GH and
insulin regulation
and the known effects of GH and insulin-like growth factor
1(IGF1) on pancreatic β-cell survival, proliferation and
neo-genesis (15, 16), hormone influences have not been described
intype 1 diabetes; no specific studies have addressed the
con-sequences of long-term GH replacement therapy in this
disease.Here we show the effects of long-term GH supplementation
asa tool to modulate autoimmune attack on pancreatic β-cells.NOD
mice transgenic for bovine GH (NOD-Tg bGH) do not
develop type 1 diabetes, and show normal glycemia
throughouttheir lives. Our histological analyses indicated that
these micedevelop periinsulitis, but show little or no islet
infiltration orβ-cell destruction. The mechanism involved specific
GH-medi-ated effects on β-cells, where it influenced proliferation
andapoptosis, and others that modulate the immune system.
GHaffected Th17/Th1 plasticity, M1/M2 macrophage differentia-tion,
and Treg cell function. Our findings show an unanticipatedGH effect
on tolerization mechanisms that reduce type 1 di-abetes
development, and underline the importance of neuroen-docrine
regulation of the immune system.
ResultsSustained GH Expression Precludes Development of Overt
Diabetes inNOD Mice. In our animal facility, >85% of virgin
female NODmice develop overt diabetes before 40 wk of age (Fig.
1A). Tostudy the effects of sustained high levels of circulating
GH, weobtained a mouse strain transgenic for bGH under the control
ofthe rat phosphoenolpyruvate carboxykinase (PEPCK) promoter(17),
on the NOD background. In this strain, as in the parentalC57BL/6-Tg
bGH strain, circulating GH levels are constant(∼5 μg/mL). Our mice
were healthy and showed no external signsof other autoimmune
diseases or tumor development throughouttheir lives. Histological
examination showed mild sialitis. Wemonitored glycemia in female
NOD-Tg bGH mice and controllittermates for 60 wk, and found that
the transgenic mice were
Significance
Although the relationship between endocrine and immunesystems is
well documented, few studies have been performedon autoimmune
disorders other than those that are sex hor-mone-related. We
studied a murine model of autoimmunediabetes, showing that growth
hormone (GH) modifies theimmune response to render diabetic mice
resistant to diseasedevelopment. The mechanism involves a
GH-mediated effecton β-cell survival and/or proliferation and a
direct effect onimmune cells. GH triggers a cytokine environment
that pro-motes anti-inflammatory macrophage polarization,
maintainsthe activity of the suppressor T cells, and limits Th17
cell plas-ticity. This study provides evidence of the importance of
endo-crine control of immune functions and indicates that
therapiesbased on GH analogs should be considered for treatment
ofautoimmune diabetes.
Author contributions: R.V., C.M.-A., and M.M. designed research;
R.V., D.K., Y.J., andR.P.G. performed research; R.V., D.K., Y.J.,
R.P.G., and M.M. analyzed data; and R.V. andM.M. wrote the
paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.1R.V. and D.K.
contributed equally to this work.2To whom correspondence should be
addressed. E-mail: [email protected].
This article contains supporting information online at
www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1314985110 PNAS | Published
online November 11, 2013 | E4619–E4627
IMMUNOLO
GY
PNASPL
US
Dow
nloa
ded
by g
uest
on
June
21,
202
1
mailto:[email protected]://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplementalhttp://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplementalwww.pnas.org/cgi/doi/10.1073/pnas.1314985110
-
almost completely resistant to diabetes development (Fig. 1A),as
reflected by their higher survival rate compared with NODmice (Fig.
1A). The results indicated significant lowering of cir-culating
glucose levels in the transgenic mice with age (Fig. 1B),resulting
in relative hypoglycemia. This observation contrastswith the
susceptibility of C57BL/6-Tg bGH mice to type 2 di-abetes in a
high-fat diet study (18). In histological analyses,NOD-Tg bGH mice
showed giant islets with anomalous mor-phology and a periinsular
mononuclear cell infiltrate that char-acterizes the initial stages
of diabetes (Fig. 1 C–F). The irregularislet morphology suggests
β-cell hyperproliferation and islet co-alescence (Fig. 1D), in
agreement with the β-cell hyperpro-liferation observed in the
presence of placental lactogen (19).Although the results were not
statistically significant, the numberof apoptotic β-cells was
reduced and Ki-67+ cells were increasedin NOD Tg-bGH pancreas (Fig.
S1). These data suggest a role
for GH in protection of β-cells from apoptosis and stimulation
oftheir proliferative capacity.
NOD-Tg bGH Mice Have Normal Delayed Type
HypersensitivityResponses. Some reports indicate a role for GH as
an immuneresponse activator (5, 20); we thus characterized immune
cellpopulations in blood, spleen, and peripheral lymph nodes ofNOD
and NOD-Tg bGH mice. Flow cytometry analysis showedsimilar immune
cell populations in both mouse lines (Table S1).No differences were
observed in activation markers (CD25,CD69, CD44, and CD62L) in CD3+
cells isolated from NODand NOD Tg-bGH lymph nodes (Fig. S2).To
obtain an overview of immune function in NOD-Tg bGH
mice, we evaluated T-cell responses in a delayed type
hyper-sensitivity (DTH) assay of sensitization and challenge with
allo-geneic splenocytes. NOD-Tg bGH mice and control
littermateswere sensitized by i.v. injection of C57BL/6 splenocytes
andchallenged 6 d later by inoculating splenocytes into the right
hindfootpad. Inflammation was measured every 24 h until remissionby
comparing thickness of the inoculated to the
contralateral,vehicle-inoculated footpad. Both mouse groups reacted
similarly,with no significant differences in inflammation grade or
resolu-tion time, with only a slight remission delay in the
transgenicmice (Fig. 2A).
NOD-Tg bGH Mice Have Altered Serum Cytokine Levels. In type
1diabetes, a Th1-to-Th2 shift in the immune response is postu-lated
to be protective for pancreatic islets (21). Indeed, theconversion
of Th17 to Th1 is necessary to induce diabetes effi-ciently (22).
To determine whether the GH-protective effectis associated with
changes in circulating cytokines, we used aLuminex assay and
detected higher peripheral blood levels ofIFN-γ, IL-4, IL-13,
IL-17A, and TNF-α in sera from NOD-TgbGH mice than from NOD
littermates (Fig. 2B). The Th2/Th1and Th17/Th1 cytokine ratios
suggested a GH-mediated biasagainst a Th1 response in the
transgenic mice (Fig. 2C).
Preclinical Type 1 Diabetes Symptoms in NOD-Tg bGH Mice. Early
intype 1 diabetes progression, an inflammatory environment
isestablished around the islets of Langerhans, usually
interpretedas a result of anomalous macrophage activity during
postnatalremodeling of the endocrine pancreas (23). Mononuclear
cellsare recruited into the pancreas and situate around the
pancreaticislets shortly after weaning. The insular parenchyma is
invadedprogressively by immune cells, which destroy
insulin-producingβ-cells. On serial pancreas sections from NOD-Tg
bGH, NODlittermates, and control C57BL/6 mice at different ages, we
usedH&E staining to evaluate islet size as well as insular and
peri-insular infiltration (Fig. 1 C–F). In NOD-Tg bGH mice,
insularinfiltration was delayed and most β-cells were conserved
overtime (Fig. 3A). The islet-cell mass thus diminished
progressivelyin NOD mice, as predicted, whereas it increased
continuouslyin NOD-Tg bGH mice (Fig. 3B). These data concur with
thereported GHR-dependent islet hyperplasia (24) and the
com-pensatory hyperinsulinemia mechanism associated with
GH-dependent insulin resistance (25).Using immunohistochemistry and
flow cytometry, we analyzed
infiltrate composition in pancreata from 3- to 5-mo-old
mice.Snap-frozen organs were sectioned and stained with
anti-CD4,-CD8, -F4/80, -CD11c, and -B220 antibodies. Although
in-dividual variation was broad, the inflammation grade in
NOD-TgbGH mouse pancreas was lower than that of NOD mice (Fig.3A).
Infiltrate composition was nonetheless grossly similar, witha
predominance of T cells, mainly CD4+ (Fig. S3). We observedno
immune cell infiltration in NOD-Tg bGH islet parenchyma,even in
older mice in which infiltration was massive, but alwaysrestricted
to the islet periphery (Fig. 3C). This inflammationcoincides with
no apparent degradation of the periinsular laminin
Age (weeks)
Gly
cem
ia (m
g/dl
)
A
C D
E F
B
0
100
200
300
400
500
10 20 30 40 50 60
NODNOD-TgbGH
500 m 500 m
100 m100 m
600
20
40
60
80
100
0.0
0.2
0.4
0.6
0.8
1.0
0 10 20 30 40 50
Sur
viva
l rat
e (%
)
Diab
etes
incid
ence
Age (weeks)
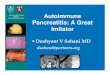
Fig. 1. NOD-Tg bGH mice are protected against type 1 diabetes
de-velopment. (A) Cumulative diabetes incidence in female NOD
(continuousred line, n = 90) and NOD-Tg bGH mice (continuous green
line, n = 89). Micewere maintained and glucose levels determined as
described in Materialsand Methods. The survival rate of transgenic
mice after 60 wk in the absenceof diabetes was 76% (dotted green
line). The NOD mouse survival curve(dotted red line) reflects mouse
sacrifice at disease onset. (B) Tendency tolower blood glucose
levels with age in NOD-Tg bGH mice (green line; n = 10mice per
group, Pearson’s correlation coefficient, r = −0.61, P < 0.01).
Eachglucose measurement is plotted (twice monthly per mouse). Red,
NOD mice;green, NOD-Tg bGH mice. (C–F) Immunohistochemistry of
pancreas from 12-wk-old NOD (C and E) and NOD-Tg bGH (D and F) mice
stained for lamininand counterstained with hematoxylin. (C and D)
Low-magnification images(6×) showing mononuclear infiltrates
(arrows) surrounding islets. (Scale bar:500 μm.) (E and F)
High-magnification (40×) images showing damage in-duced in the NOD
mouse in the laminin sheet (arrows) surrounding islets andcompared
with its preservation in NOD-Tg bGH mice. (Scale bar: 100 μm.)
E4620 | www.pnas.org/cgi/doi/10.1073/pnas.1314985110 Villares et
al.
Dow
nloa
ded
by g
uest
on
June
21,
202
1
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=SF1http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=ST1http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=SF2http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=SF3www.pnas.org/cgi/doi/10.1073/pnas.1314985110
-
layer, which defines the basal lamina of the sheet of
Schwanncells thought to be the first target of autoimmune attack
(26)(Fig. 1 E and F). In some cases, we found intrainsular foci in
maturemice (Fig. 3 C and D), although they must be considered
peri-vascular, because they are surrounded by an intact laminin
sheet.Because type 1 diabetes is also characterized by
development
of a humoral response to islet antigens, we evaluated
antiinsulinantibodies in prediabetic NOD-Tg bGH and control
prediabeticNOD mice. Whereas NOD mice had high antiinsulin
antibodytiters, indicative that insulin is the primary antigen for
type 1diabetes in these mice (27), as it is in humans (28), NOD-Tg
bGHmice had much lower titers (barely detectable even at 12 wk;Fig.
3E). Spleen B cells from NOD and NOD Tg-bGH mice wereactivated in
vitro with anti-mouse IgM antibody (10 μg/mL, 180–360min, 37 °C)
alone or with exogenous GH (5 μg/mL); activation wassimilar, as
demonstrated by flow cytometry using anti-CD69 andanti-CD86
antibodies (Fig. S4). These findings rule out B-cell ac-tivation
defects in NOD Tg-bGH mice.In addition to the maintenance of normal
glycemia, the lack of
antiinsulin antibodies and the absence of islet-infiltrating,
puta-tive antigen-specific CD4+ T cells in NOD-Tg bGH mice
sug-gests that GH modulates the adaptive immune response in type1
diabetes.
Circulating GH Levels Are Responsible for the Protective
Phenotype.For detailed characterization of the role of the adaptive
immuneresponse in NOD-Tg bGH mice, we evaluated diabetogenic
cellpopulations and suppressor cell activity. We transferred
totalsplenocytes from NOD-Tg bGH or NOD mice into untreatedor
sublethally (7 Gy) irradiated NOD or NOD-Tg bGH mice.Splenocytes
from NOD-Tg bGH mice did not protect untreated
NOD mice from disease development (Fig. 4A), suggesting
thatNOD-Tg bGH regulatory cells had insufficient suppressive
ca-pacity in NOD mice. In addition, cells from the transgenic
micedid not accelerate diabetes in sublethally irradiated NOD
mice(Fig. 4B), indicating a lack of diabetogenic effector cells in
theNOD-Tg bGH splenocyte population.Radiomimetic drugs trigger type
1 diabetes in NOD mice by
targeting the CD4+CD25+FoxP3+ T-cell population and impair-ing
their recovery in pancreas infiltrates (29). To determine therole
of Treg cells in our model, we transferred splenocytes (2 ×107)
from a pool of three overtly diabetic 6-mo-old NOD miceinto
6-wk-old sublethally (7 Gy) irradiated NOD-Tg bGH mice.Diabetes did
not develop in the recipients (Fig. 4C), whereas di-abetes was
accelerated in irradiated control NOD littermates.These data
suggest a resistant suppressive mechanism in irradiatedNOD-Tg bGH
mice that blocked NOD effector cells.Because Treg cells are
reported to be relatively radioresistant
(30), we transplanted diabetogenic splenocytes into lethally
ir-radiated (12 Gy) NOD and NOD-Tg bGH recipients for a
3-wkradioprotection/accelerated diabetes assay. Recipient mice
wererescued from lethality and, though NOD mice became
hyper-glycemic within 7–10 d, transgenic mice remained
normoglyce-mic throughout the experiment (Fig. 4D). Untransferred
mice ofboth genotypes, used as a lethality control, died during the
firstweek. The results imply a suppressive mechanism for
diabetogeniccells in NOD-Tg bGH mice, which are resistant even to a
highdose of full-body irradiation. The relative radioresistance of
Tregcells and monocytes might account for this suppression.We
tested whether transgenic splenocytes protect mice in an
accelerated diabetes model. Two groups of 12-wk-old
NOD/SCID(severe combined immunodeficiency) mice were inoculated
i.v.
95 100 105 110 115 120 125 130 135 140
24 48 72 96 Hours post challenge
Foot
pad
swel
ling
(%)
A C
0 1 2 IL17/IFN-
IL17/TNF-
IL4/IFN-
IL4/TNF-
IL13/IFN-
IL13/TNF-
Relative ratio
Cyt
okin
es
** **
**
**
B
0
2
4
6
8
NOD Tg
IL4
NOD Tg0
100
200
300
400IL13
0
75
150
225
300
NOD Tg
IL17
NOD Tg NOD Tg0
250
500
750
1000TNF-
0
15
30
45
60IFN-
pg/ml
*** *** *** * *
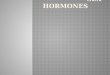
Fig. 2. T-cell response in NOD-Tg bGH mice. (A) NOD-Tg bGH mice
show standard DTH responses. Footpad swelling at several times
postchallenge in NOD-TgbGH (dark gray, n = 6) and NOD mice (light
gray, n = 6). Swelling was calculated as the percentage of footpad
thickness compared with the baseline at t = 0.Values shown are mean
± SD. Student t test showed no significant differences at any time.
(B) Circulating cytokine levels in 4-mo-old NOD (n = 12) and NOD-Tg
bGH (Tg) (n = 11) mice. Individual and mean values are shown.
Student t test, *P < 0.05, ***P < 0.001. (C) Ratios between
Th2/Th1 and Th17/Th1 profiles,assessed by circulating cytokines
quantification, in NOD (light gray bars, n = 12) and NOD-Tg bGH
(dark gray, n = 11) mice. Values have been normalized toNOD mice
data. Student t test, **P < 0.01.
Villares et al. PNAS | Published online November 11, 2013 |
E4621
IMMUNOLO
GY
PNASPL
US
Dow
nloa
ded
by g
uest
on
June
21,
202
1
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=SF4
-
with 2 × 107 splenocytes from a pool of two 5-mo-old diabeticNOD
mice. One group also received 2 × 107 splenocytes froma pool of two
5-mo-old transgenic mice (Fig. 4E). All mice thatreceived NOD
splenocytes alone developed hyperglycemia by4 wk posttransfer. The
group inoculated with splenocytes fromNOD + NOD-Tg bGH mice showed
a slight, nonsignificantdelay in hyperglycemia (log-rank test P =
0.094), suggesting lossof a hypothetical protective mechanism in
the absence of circu-lating GH.
Suppressive Potential in NOD-Tg bGH Mice. Although Treg cells
arebroadly implicated in type 1 diabetes development, their
precise
function during the prediabetic stage is not well understood
(31–34). CD4+CD25+ Treg cells control disease progression
throughvarious potential mechanisms, inhibiting activation,
proliferation,and/or migration of islet-specific T cells in lymph
nodes and inpancreas (35). Because Treg cell suppressive potential
is associ-ated with FoxP3 levels (36), we used flow cytometry to
determineFoxP3 expression on CD4+CD25+ peripheral blood
lymphocytesfrom C57BL/6, NOD, and NOD-Tg bGH mice at 2 mo of
age,before hyperglycemia was detected (Fig. 5A), and at 5 mo,
whenNOD mice were hyperglycemic (Fig. 5B). We found no differ-ences
in FoxP3 expression in any 2-mo-old mice (Fig. 5 A and C),whereas
CD4+CD25+ lymphocytes from 5-mo-old NOD miceshowed a clear
reduction in FoxP3 levels compared with thosefrom B6 mice; this
down-regulation was not observed for NOD-Tg bGH CD4+CD25+ Treg
cells (Fig. 5 B and C). The resultssuggest a GH effect on the
maintenance of Treg cell activity.In 2-mo-old mice, the percentage
of CD4+CD25+FoxP3+
cells was higher in C57BL/6 than in NOD-Tg bGH mice or NOD
Fig. 3. Type 1 diabetes symptoms are largely suppressed in
NOD-Tg bGHmice. (A) Severity of insulitis and destructive lesions
in NOD, NOD-Tg bGH,and C57BL/6 (control) mice. After H&E
staining, ∼50–100 random islets perpancreas were evaluated. Three
mice were analyzed for each genotype andage group (13, 20, and 24
wk). The degree of mononuclear cell infiltrationwas graded
independently by two observers as follows: 0, normal (white);
1,mild periinsulitis (light gray); 2, severe periinsulitis (dark
gray); or 3, insulitis(black; see Materials and Methods for
details). (B) Islet mass estimated frompercentage of endocrine area
(relative to total pancreas surface) asa function of age for NOD
(gray), NOD-Tg bGH (black), and C57BL/6 mice(white; n = 3 for each
age group). (C and D) Late infiltration in islets fromNOD-Tg bGH
mice. Frozen pancreas sections of 7-mo-old NOD-Tg bGH mice.Islets
(I) and infiltrates (M) are labeled. (Scale bar, 100 μm.) (C)
Mergedimage of H&E staining showing giant coalescent islets.
Original magnifi-cation, 6×. (D) Section stained with antilaminin
antibody to identify thebasal layer of pancreatic acini, blood
vessels, and periinsular sheet ofSchwann cells. Hematoxylin
counterstain shows perivascular and isletinfiltrates. Mononuclear
infiltrates were surrounded by this laminin sheetand hence did not
invade the islet parenchyma. Original magnification,10×. (E )
Evaluation of prodromal antiinsulin antibodies (NOD-Tg bGH, n =
5;NOD, n = 7; C57BL/6 control, n = 3) at 10 (light gray), 12 (dark
gray), and 14wk (black). ELISA for human insulin did not detect
autoantibodies in NOD-Tg bGH mice. Background optical density was
subtracted. Student t test,**P < 0.01.
D
0 10 20 30 40
0 10 20 30 40
100
80
60
40
20
0
B100
80
60
40
20
0
A
0 10 20 30 40
100
80
60
40
20
0
E
0 10 20 30 40
100
80
60
40
20
0
C100
80
60
40
20
0
0 2 4 6 8 10 12 14Cum
ulat
ive
surv
ival
(%)
Age (weeks)
NS
NS
Fig. 4. Kaplan–Meyer analysis for adoptive transfer protocols.
(A) Seven-week-old NOD mice (continuous line, n = 4) were
inoculated with 2 × 107
NOD-Tg bGH mouse splenocytes; inoculated NOD-Tg bGH mice were
used ascontrols (dashed line). No delay in hyperglycemia was
observed comparedwith the normal behavior of NOD mice. (B)
Seven-week-old NOD mice(continuous line, n = 6) were sublethally
irradiated and inoculated with 2 ×107 NOD-Tg bGH mouse splenocytes.
No delay was observed in manifesta-tion of overt diabetes compared
with untreated NOD control mice (dashedline). (C) Six-week-old
NOD-Tg bGH mice (dashed line, n = 5) were sub-lethally irradiated
and inoculated with 2 × 107 diabetic NOD mouse sple-nocytes.
Irradiated NOD littermates (continuous line, n = 4) were used
ascontrols. Accelerated diabetes development was observed in NOD
controls,whereas NOD-Tg bGH mice remained fully resistant. (D) The
experiment in Cwas repeated using lethally irradiated NOD-Tg bGH
mice (dashed line, n = 4).NOD mice (n = 2) were used as controls
for accelerated diabetes development,and uninoculated mice (NOD, n
= 2; NOD-Tg bGH, n = 2) as controls of lethality;all four
untransferred mice died within 2 wk of irradiation. (E) NOD/SCID
mousesensitivity to diabetes development after splenocyte transfer
(NOD, continuousline; NOD + NOD-Tg bGH, dashed line; 12 wk old, n =
4 for both groups). Log-rank test P < 0.05 was considered
significant. NS, not significant.
E4622 | www.pnas.org/cgi/doi/10.1073/pnas.1314985110 Villares et
al.
Dow
nloa
ded
by g
uest
on
June
21,
202
1
www.pnas.org/cgi/doi/10.1073/pnas.1314985110
-
littermates, with no difference between the last two groups.
Thepercentage of CD4+CD25+FoxP3+ cells was higher in 5-mo-oldNOD-Tg
bGH mice than in NOD littermates, although in bothcases it was
lower than that in C57BL/6 mice (Fig. 5D), whichsuggests higher
suppressive T-cell activity in NOD-Tg bGH thanin NOD mice.
We used an in vitro suppression assay to test for a
correlationbetween reduced FoxP3 expression on CD4+CD25+
lympho-cytes and a reduction in their suppressive capacity.
Coculture ofCD4+CD25−NODT cells with varying proportions of
CD4+CD25+
T cells from 5-mo-old NOD or NOD-Tg bGH mice led to slightbut
significantly higher suppressive activity by NOD-Tg bGH-derived
cells (Fig. 5E).These results indicate that GH participates in
maintenance of
the suppressive potency of Treg cells as well as of the
relativelyhigh FoxP3 levels in CD4+CD25+ cells. This effect might
bepotentiated in vivo, because NOD-Tg bGH cells are continu-ously
exposed to high levels of circulating GH. Treg cells in vivomight
also be activated locally by antigen-presenting cells
(37)specifically charged with islet antigens, which were absent in
ourin vitro experiments.
GH Effect on Macrophage Polarization. Macrophages have a keyrole
in pancreas remodeling (23) and are also present in pan-creas
infiltrate in NOD and NOD-Tg bGH mice. There are twomain macrophage
types: M1 or inflammatory macrophages,characterized by high NOS2
(inducible nitric oxide synthase)expression, and M2 or
anti-inflammatory macrophages charac-terized by arginase-1
expression. We used quantitative real-timePCR to quantify M1/M2
macrophage markers in pancreaticlymph nodes from 3-mo-old NOD and
NOD-Tg bGH mice. Wefound lower NOS2 and higher arginase-1 RNA
levels in nodesfrom NOD-Tg bGH than from NOD mice (Fig. 5F). These
datawere confirmed by immunohistochemical identification of
argi-nase-1–producing cells in NOD and NOD-Tg bGH mouse pan-creas
(Fig. 5 G and H). The results indicate a GH effect onmacrophage
polarization toward the M2 phenotype in NOD-TgbGH mice.
GHModulates Th17 Cell Plasticity.Diabetes development is
reportedto be associated with acquisition of a Th1-like phenotype
by Th17cells (38), which then express T-bet and secrete IFN-γ. We
testedthe GH effect on Th17/Th1 plasticity using RT-PCR to
determineIL-17, IFN-γ, IL-2, IL-22, and GM-CSF mRNA levels in
totalpancreas of age-matched NOD-Tg bGH and prediabetic NODmice, as
well as of ROR-γT and T-bet transcription factors asspecific
markers of Th17 and Th1 polarization, respectively (Fig.6A). To
avoid interference due to different numbers of infiltratingcells in
the pancreas, we compared the ratio for messages char-acteristic of
Th17 and Th1 cells, which is more indicative of therelative
abundance of nonpathogenic Th17 cells than are in-dividual Th17 or
Th1 values (39). The results showed a higherRORC/Tbx21 (Fig. 6B)
and IL-17/IFN-γ (Fig. 6C) ratios inNOD-Tg bGH mouse pancreas. In
addition, we detected higherIFN-γ, IL-2, IL-22, and GM-CSF mRNA
levels in NOD mousepancreas (Fig. 6A). These data indicate a
significant reduction ofpathogenic Th17 cells infiltration and
their plasticity to Th1 inNOD-Tg bGH mouse pancreas.
DiscussionType 1 diabetes is a multifactorial disease caused by
the con-currence of genetic and environmental factors that include
in-fectious agents, diet, and illness (40). Endocrinopathies
charac-terized by chronic overproduction of hormones whose
actionopposes that of insulin, such as epinephrine, glucagon,
cortisol, orGH, generally cause diabetes by triggering insulin
resistance (41);nonetheless, very little is known of their
potential to influenceautoimmune diabetes. Here we observed that a
transgenic mousestrain on the NOD background that expresses bGH
under thecontrol of the rat PEPCK promoter (NOD-Tg bGH) did
notdevelop type 1 diabetes. The pancreatic inflammatory
phenotypecharacteristic of the NOD background was severely reduced
inthe presence of GH. These mice also showed almost
completesuppression of the adaptive immune response. We detected
no
A B
FoxP3
C D
FE
0
1
2
HG
3
ARG1 iNOSRel
ativ
e ex
pres
sion
(2-
Ct )
2:1 4:1 8:1 C
*
*
*0
2
4
6
8
cpm
(x 1
04)
2 m 5 m
FoxP
3+ in
CD
4+ (%
)
0 100 200 300 400 500 600 700
2 m 5 m
FoxP
3 M
FI
NOD NOD-Tg bGH C57BL/6
I I
****
16
12
8
4
0
Fig. 5. Bias toward a regulatory phenotype in NOD-Tg bGH mice.
Down-regulation of FoxP3 in NOD Treg cells. Blood samples from
2-mo-old (A) and5-mo-old mice (B) of C57BL/6, NOD, and NOD-Tg bGH
genotypes were la-beled for CD4, CD25, and FoxP3; Treg cells were
gated by light-scatterproperties (forward scatter and side
scatter), CD25 and CD4. One represen-tative sample of nine is
shown. C57BL/6, black line; NOD, red line; NOD-TgbGH, green line.
(C) FoxP3 expression in CD4+CD25+ cells assessed by flowcytometry.
FoxP3 mean fluorescence intensity in blood samples from 2-
and5-mo-old mice. (D) Relative abundance of FoxP3+ cells in the
blood CD4+
population, assessed by flow cytometry, at 2 and 5 mo. (C and D)
NOD (lightgray), NOD-Tg bGH (dark gray), and C57BL/6 (white) mice
mean values + SDfor four experiments (total n = 9 for each mouse
group). Student t test, *P <0.5; **P < 0.1. (E) Suppressive
activity of CD4+CD25+ splenocytes from NOD(light gray) and NOD-Tg
bGH (dark gray) mice at various ratios of CD4+CD25−
effector cells (letter C indicates no suppressor cells added).
[3H]thymidineincorporation after coculture is shown as a percentage
of the value forcultured pure effector cells. (F) M1 and M2
macrophage marker expression.Quantitative RT-PCR was used to
quantify relative levels of NOS2 and arginase-1 mRNA in pancreatic
lymph nodes from 3-mo-old mice. Values (2−ΔΔCt) arerelative to the
mean level of each message in samples from NOD mice. (G andH)
Immunohistochemistry showing arginase-1 expression within the
peri-insular infiltrate in young mice (8 wk). Anti–arginase-1
antibody was visualizedwith horseradish peroxidase and
diaminobenzidine (arrows); hematoxylin wasused as counterstain (G,
NOD; H, NOD-Tg bGH). Original magnification, 20×.
Villares et al. PNAS | Published online November 11, 2013 |
E4623
IMMUNOLO
GY
PNASPL
US
Dow
nloa
ded
by g
uest
on
June
21,
202
1
-
prodromal antiislet antibody production or diabetogenic cell
ex-pansion; hence, there was no islet destruction in these
mice.There is considerable evidence for distinct GH effects on
pancreatic β-cells (16), some direct and others through its
mainmediator, IGF1 (42). Exogenous GH in rat islet cultures
thusstimulates DNA synthesis and insulin production (43); IGF1
andGH signaling have mitogenic effects on INS-1 cells (44).
Wedetected a large β-cell mass in NOD-Tg bGH mice that corre-lated
with the higher proliferation rate and lower apoptotic
β-cellnumbers detected in the pancreas of these mice, which
couldexplain in part the lack of hyperglycemia in these mice. By
ac-tivating the JAK/STAT pathway, GH can also stimulate
β-cellsurvival. The JAK/STAT-activated suppressors of cytokine
sig-naling block damage triggered by cytokines such as IFN-γ
orTNF-α (45), and expression of a constitutively active form
ofSTAT5b has a protective effect on β-cells in a model of
strep-tozotocin-induced diabetes (46).NOD-Tg bGH mice showed
periinsulitis, although we found
no sign of degradation of the periinsular laminin layer, and
noantiinsulin antibodies in serum. The results confirm a GH
effecton the immune system in addition to its effect on
β-cells.Although differences in immune cell activity are
associated
with high levels of circulating GH (47), we detected no
majordifferences in any of the circulating cell populations in
eithermouse type; B220+, CD3+, CD4+, CD8+, CD11b+, or Gr1+
cellnumbers were similar, as were the lymph node T-cell
activationmarkers (CD25, CD69, CD44, and CD62L). This
observationconcurs with the similar response in a DTH assay of NOD
andNOD-Tg bGH mice to immunization with allogeneic
splenocytes,ruling out general defects in the T-cell response
and/or antigenpresentation. It is nonetheless postulated that APC,
antigen pre-senting cell, defects are responsible for the lack of
adequate reg-ulatory potential in NOD mice (48). It could be argued
that thehalt observed at the periinsulitis checkpoint is due to a
reduced
Th2 response and Ig production in NOD-Tg bGH mice.
Over-expression of bGH in C57BL/6 mice alters the humoral
responseto egg albumin by reducing Th2 cytokine production (1).
Wedid not observe such Th2 defects on the NOD background,
asassessed by measurement of circulating cytokine levels. In
anycase, antiislet antibodies are not directly linked to β-cell
de-struction, and the role of β-cells appears to be restricted to
theirantigen-presenting activity (49). β-cells from NOD and
NOD-TgbGH mice showed no defects in their in vitro activation by
anti-IgM antibodies. We previously observed that after
stimulationwith conventional antigens, the antigen response is
reduced in TgbGH mice, with a IgG1 to IgG2 isotype shift (1). These
findingsimplicate GH in altering T-cell function.Transferred NOD-Tg
bGH splenocytes did not protect NOD
mice from diabetes, and NOD splenocytes did not promote
di-abetes when transferred into NOD-Tg bGH mice, suggestingthat
control of T-cell responses in NOD-Tg bGH mice is de-pendent on
circulating GH levels.At 5 mo of age, with a well-developed
inflammatory environ-
ment, CD4+CD25+ Treg cell numbers are maintained at stablelow
levels in NOD mice, whereas they rise in NOD-Tg bGHmice. In NOD-Tg
bGH mice, we did not observe the down-regulation of FoxP3
expression found in hyperglycemic NODmice. Because FoxP3 expression
is directly linked to the regu-latory action of Treg cells (50), it
is thus possible that GH reg-ulates FoxP3 activation via STAT5b or
STAT3. A single pointmutation in STAT5b, which encodes a
transcription factor in-volved in GH signaling (51), limits FoxP3
expression by Tregcells (11). Sustained activation of STAT3
(another transcriptionfactor involved in signaling through the GHR)
is needed to main-tain FoxP3 expression by Treg cells (52). Through
STAT5B orSTAT3 activation, GH might thus increase FoxP3 levels,
regu-lating Treg cell activity.In the adoptive transfer
experiments, sublethal and even lethal
irradiation did not alter the protective effect of GH expression
inNOD-Tg bGH mice. GH promotes radioprotection in a varietyof cell
types, and radiation sensitivity differs in some immunesystem
niches. For example, GH and IGF1 enhance hemato-poietic stem cell
radioresistance and proliferation (53). Theseresistance mechanisms
nonetheless appear to be insufficient forthe rapid expansion of
suppressive cells that would be needed tocontrol disease in an
accelerated diabetes model. It is more likelythat GH increases the
radioresistance of the Treg cell pop-ulation; lethally irradiated
wild-type hosts transferred with scurfybone marrow cells did not
develop autoimmune disease, due tosuppression of sf-derived T cells
by radioresistant host FoxP3+
Treg cells (30).We tested the in vitro suppressive capacity of
Treg cells from
NOD and NOD-Tg bGH mice and found slight but
significantdifferences. These differences might be considered
insufficient toexplain complete resistance to diabetes development;
nonethe-less, T-cell differentiation and activity are dependent on
antigen-presenting cell type and the microenvironment in which
pre-sentation occurs, and Treg cells might be induced only locally
byM2 macrophages (37). Macrophages have two distinct pheno-types
(54): inflammatory (M1) macrophages participate in anti-gen
recognition and secretion of inflammatory cytokines,
andnoninflammatory (M2) macrophages are involved in tissue
repairand remodeling (55). M1 polarization is induced by IFN-γ
andcharacterized by high NOS2 expression and by secretion
ofproinflammatory cytokines IL-1 and IL-12, whereas M2 are in-duced
by IL-4 and IL-13 and are characterized by high
arginase-1expression and by IL-10 secretion. Our data for
pancreatic lymphnodes and pancreata from prediabetic NOD mice
showed thepresence of M1 macrophages (arginase-1lowNOS2high),
whereasage-matched NOD-Tg bGH mouse macrophages had an M2
phe-notype (arginase-1highNOS2low). This difference might be the
result
RORC/Tbx21
0
50
100
150
200
250
**
mR
NA
RO
Rt
/mR
NA
T-b e
t
IL-17/IFN-
0
10
20
30
40*
mR
NA
IL-1
7/m
RN
AI F
N-
)B
A
C
* *** * *** *** * NS *
0% 20% 40% 60% 80% 100% 120%
RORC Tbx21 IL22 IL2 IFNG GM-CSF IL17 IL10
Relative expression
Fig. 6. Cytokine expression in the pancreas of NOD prediabetic
and NOD-TgbGH diabetes-resistant mice. RNA from 13-wk-old mouse
whole pancreaswas quantified by quantitative RT-PCR. Student t test
(n = 6); *P < 0.05; **P <0.01; ***P < 0.001. (A) Relative
expression (2−ΔΔCt) of characteristic Th1 andTh17 transcription
factors and cytokines in NOD and NOD-Tg bGH micepancreas, relative
to mean values in NOD. The ratios between mRNA expressionof
RORC/Tbx21 (B) and IL-17/IFN-γ (C) in NOD (light gray) and NOD-Tg
bGH (darkgray) mice are shown.
E4624 | www.pnas.org/cgi/doi/10.1073/pnas.1314985110 Villares et
al.
Dow
nloa
ded
by g
uest
on
June
21,
202
1
www.pnas.org/cgi/doi/10.1073/pnas.1314985110
-
of the high circulating levels of IL-17 (56), and could also
influenceincreased local Treg cell activity.Autoimmune diabetes is
a well-characterized Th1 pathology.
We detected high IFN-γ and IL-2 mRNA levels in NOD
mousepancreas, which were lower in NOD-Tg bGH pancreas. Bothmouse
models also had high IL-17 mRNA levels, suggestingTh17 cell
involvement in type 1 diabetes. Th17 cells are found insome
autoimmune diseases such as experimental
autoimmuneencephalomyelitis (57) and rheumatoid arthritis (58);
NODand NOD-Tg bGH mouse pancreas also showed high ROR-γTmRNA
levels.Recent evidence suggests that depending on the
microenvi-
ronment, Th17 cells can alter their differentiation program
toinduce protective or proinflammatory responses (59, 60). Wefound
a significant reduction in mRNA levels of IFN-γ, IL-2, andGM-CSF,
characteristic mediators for Th17 pathogenic cells(59), in NOD-Tg
bGH pancreas compared with that of NODmice. Although, increasing
evidences points to the role of Th17cells in NOD mice, it seems
that the conversion of this cell subsetinto Th1 is more important
(22, 38). How the inflammatorymicroenvironment modulates this Th17
differentiation is notcompletely understood, although our results
suggest that GHmaintains a nonpathogenic profile of Th17 cells and
reducestheir Th1 potential in the pancreas.We cannot rule out that
GH might also contribute to trans-
genic islet resistance to immune attack via STAT3
activation.STAT3 activation in Treg cells, associated with type 1
diabetesresistance in NOD mice (61), controls the macrophage
IL-10–mediated anti-inflammatory response (62) and is an
importantsurvival factor in β-cells (63, 64). Our data show that
GH-mediated interference in type 1 diabetes development involvesan
increase in β-cell mass, protection of the periinsular
lamininlayer, and a direct effect on immune cells—mainly
macrophages,Th17, and possibly Treg cells. These results
demonstrate theimportance of endocrine control of immune functions,
and in-dicate that therapies based on GH analogs and/or their
signalingcascades should be considered for treatment of
autoimmunediabetes.
Materials and MethodsMice.Mice transgenic for bGH under the
control of the phosphoenolpyruvatecarboxykinase promoter on a
C57BL/6J × C3H/J hybrid background (65) werecrossed on the NOD
background until NOD polymorphic alleles were stabi-lized (F0;
NOD-Tg PEPCK-bGH/Ccnb), as assessed by the length of single
se-quence repeats (66). The transgenic strain was maintained by
continuousbackcrosses on NOD females. Experimental results were
obtained from F5onward, always using strict littermates. Mice were
fed a standard laboratoryrodent diet (Global Diet 2918, Harlan
Iberica; 18.5% protein, 5.5% oils andfat) and tap water ad libitum.
The mice were monitored twice a week withAccutrend kits (Roche
Diagnostics) for development of hyperglycemia, anddeclared diabetic
when glucose was >200 mg/dL in two consecutive mea-surements.
Overtly diabetic mice were killed. Mice were handled accordingto
national and European Union guidelines, and experiments were
ap-proved by the Comité Ético de Experimentación Animal, Centro
Nacional deBiotecnología.
Immunohistochemistry. Pancreata were embedded in optimal cutting
tem-perature freezing medium (Sakura) and snap-frozen in cooled
isopentane.Sections (7 μm) were cut, air-dried, and fixed in cold
acetone. When storedat −80 °C, sections were postfixed in
ethanol/acetone (1:3) before staining.Primary antibodies were
guinea pig anti-porcine insulin antibody (Dako), anti–arginase-1
(BD Biosciences), rabbit anti-laminin (Sigma), and rabbit
anti-Ki67(Novocastra antibodies); immunodetected with the tyramide
signal amplifica-tion indirect staining kit (Perkin-Elmer); and
visualized with diaminobenzidine.Hematoxylin was used for
counterstaining.
β-Cell Mass Determination and Infiltration Level Count.
Pancreata frommice ofdifferent ages (three per group) were
extracted, weighed, formaldehyde-fixed, and paraffin-embedded. For
quantification, one 5-μm section wasanalyzed every 100 μm. Sections
were H&E stained and photographed at 10×
magnification. Composite images were generated with the
photomergefunction of Adobe Photoshop CS5. On merged images, a grid
was super-imposed and β-cell mass calculated from the ratio of
intersections in endo-crine vs. total pancreas and pancreas weight
(67). Separation between gridlines was 50 μm. The same slides were
used to determine infiltration level inislets. Insulitis was scored
by the following criteria: insulitis (grade 3), in-filtration in
the islet parenchyma; severe periinsulitis (grade 2), three ormore
rows of mononuclear cell infiltrate surrounding the islet; mild
peri-insulitis (grade 1), less than three rows of periinsular
infiltrating cells, and noinsulitis (grade 0), absence of cell
infiltration. Apparent intraislet area wassometimes counted as
periinsular when the insular parenchyma was notinvaded, as
determined by the integrity of Schwann cell basal lamina.
Delayed Type Hypersensitivity. C57BL/6J splenocytes were
isolated by me-chanical disaggregation and erythrocyte lysis with
NH4Cl, washed once withPBS + 0.1% BSA and twice with PBS. The
6-wk-old mice were sensitized byi.v. injection of 2 × 105 C57BL/6J
splenocytes, and challenged on day 6 in theright footpad with 1.5 ×
107 cells in 50 μL PBS. Control left footpads received50 μL PBS.
Footpad thickness was measured with a vernier caliper
(MitutoyoJapan) at 24, 48, and 72 h after challenge. Results of
footpad swelling werecalculated as the difference between
challenged vs. prechallenged footpad,expressed as a percentage.
Student t test P values >0.05 were considerednonsignificant.
Adoptive Transfer. Donor spleens were processed as above. The
indicatednumber of splenocytes was injected i.v. into the tail of
recipient mice. Whenindicated, host mice were previously irradiated
lethally (12 Gy) or sublethally(7 Gy) with a single full-body dose
from a 137Cs source. SPSS Statistics softwarewas used for
statistical analyses.
Cytokine Measurement. Circulating cytokines were quantified in
serum witha Bio-Plex kit and analyzer (BioRad). Serum samples were
stored at −80 °Cuntil use. Antiinsulin and total antibodies in
serum were measured bystandard ELISA at 495 nm. Plates were coated
with 100 μL per well withhuman insulin (20 μg/mL; Novo-Nordisk) or
goat anti-mouse Ig kappa chain(50 μg/mL) in PBS. Plates were
incubated (overnight, 4 °C), washed with PBS,0.1% Tween 20, and
blocked with 1% BSA, 0.05% Tween-20 in PBS [1 h,room temperature
(RT)]. Serial serum dilutions were added to washed platesand
incubated (2 h, RT); after washing, peroxidase-conjugated
anti-Ig(1:2,000; Dako) was added. Plates were incubated (1 h, RT),
washed, and 100μL orthophenylenediamine substrate solution (Sigma)
was added. The re-action was terminated after 20 min and
measured.
Cell Purification and Flow Cytometry. To prepare single-cell
suspensions,spleens and lymph nodes were harvested and minced on a
40-μm nylon meshin RPMI medium 1640 (Lonza) supplemented with 10%
FBS, 2 mM L-gluta-mine, and 50 μg/mL penicillin/streptomycin. For
APC preparations, spleenswere predigested with collagenase A and
DNase I. CD11c+, CD4+CD25+, andCD4+CD25− cell populations were
enriched by CD11c Microbeads Mouse(Miltenyi Biotech), Dynabeads
Flow Comp Mouse CD4+CD25+ Treg Cells Kit(Invitrogen), and an
AutoMACS Cell Sorter (Miltenyi Biotech). When re-quired, murine B
cells were purified using mouse pan-T Dynabeads (Invi-trogen) and T
cells with mouse T-cell negative isolation kit (Dynal). Purity
ofall cell preparations was routinely >95%. Blood samples were
lysed withVersaLyse (Beckman Coulter).
Single-cell suspensions of lymphoid organs or blood leukocytes
wereprepared and blocked with anti-CD16/32 (BD Pharmingen) to
impede Fc-mediated nonspecific antibody binding. Samples were
stained with antibodyconjugates by a standard procedure, using FITC
anti-CD25, FITC anti-CD11b,and SPRD anti-Gr1 (Pharmingen); SPRD
anti-CD4 (eBiosciences); FITC anti-CD3, FITC anti-CD8, PE
anti-CD44, FITC anti-CD69, FITC anti-CD45, and APCanti-B220
(Beckman Coulter); PE anti-CD86 (BioLegend); and PE
anti-CD62L(Southern). FoxP3 expression was determined after
permeabilization andintracellular staining with a PE-labeled
antibody (FoxP3 staining set; eBio-sciences). When necessary, naïve
B cells (92–95% pure) were first activatedwith 10 μg/mL goat
anti-mouse IgM Ab (Jackson ImmunoResearch; 3 or 6 h,37 °C), alone
or with exogenous human GH (5 μg/mL, Genotonorm; Pfizer).Stained
samples were analyzed on a flow cytometer (Cytomics FC 500;
Beck-man Coulter). FACS data were analyzed with FlowJo and CytoSpec
software.
In Vitro Suppression Assay. CD4+CD25− NOD splenocytes (5 × 104)
werecocultured with variable ratios of CD4+CD25+ cells (2:1, 4:1,
and 8:1) and withNOD spleen CD11c+ cells (5 × 104; previously
γ-irradiated, 15 Gy) in the pres-ence of anti-CD3 (1 μg/mL).
Cultures were prepared in triplicate in U-bottom96-well plates
(Nunclon Surface) with RPMI-1640 medium supplemented with
Villares et al. PNAS | Published online November 11, 2013 |
E4625
IMMUNOLO
GY
PNASPL
US
Dow
nloa
ded
by g
uest
on
June
21,
202
1
-
10% FBS, 2 mM L-glutamine, 1 mM pyruvate, and 50 μM
β-mercaptoethanol(72 h, 37 °C), and cells were pulsed (16 h) with 1
μCi [3H]thymidine (Perkin-Elmer) per well. The 3H incorporation was
measured by liquid scintillationspectrometry using CytoScint
mixture (MP Biomedical) and a 1450 MicroBetacounter
(Perkin-Elmer).
Semiquantitative Real Time PCR. cDNA sequences were obtained
from theGenBank database. PCR primers were designed from the cDNA
sequencesusing Primer-BLAST (68) (Table S2). RNA (5 μg) was used
for reverse tran-scription. cDNA was obtained by SuperScript II
reverse transcriptase (Invi-trogen). Then cDNA was amplified by PCR
analysis, using Power SYBR GreenPCR Master Mix (Applied
Biosystems), 0.3 μM of primers, and three serialdilutions of RT
products. Triplicate samples were quantified using the ABI
Prism HT7900 sequence detection system (Applied Biosystems). For
relativequantification, we used the equation 2−ΔΔCt. We normalized
each samplewith β-actin (ΔCt), and ΔΔCt represents the difference
between the Ct fromeach gene expression of NOD at 13 wk and each
datum.
ACKNOWLEDGMENTS. We are grateful for the gift of Genotonorm
(PfizerEspaña). We thank R. Barroso and G. Cascio for technical
support, L. Gómez foranimal handling, C. Bastos for secretarial
assistance, and C. Mark for editorialassistance. Support for this
work was provided by Comunidad de MadridContract S2011/BMD-2502 (to
R.V.); a La Caixa Fellowship (to D.K.); SpanishMinistry of Science
and Innovation Grant SAF 2011-27370; European UnionFP7-integrated
project Masterswitch 223404; Fondo de Investigación
Sanitaria,Instituto de Salud Carlos III RD12/009/009 and
RD12/009/002; and the Comunidadde Madrid S2010/BMD-2350.
1. Gonzalo JA, et al. (1996) Enterotoxin septic shock protection
and deficient T helper2 cytokine production in growth hormone
transgenic mice. J Immunol 157(8):3298–3304.
2. Cross RJ, Bryson JS, Roszman TL (1992) Immunologic disparity
in the hypopituitarydwarf mouse. J Immunol 148(5):1347–1352.
3. Murphy WJ, Durum SK, Anver MR, Longo DL (1992) Immunologic
and hematologiceffects of neuroendocrine hormones. Studies on DW/J
dwarf mice. J Immunol 148(12):3799–3805.
4. Dardenne M, Mello-Coelho V, Gagnerault MC, Postel-Vinay MC
(1998) Growth hor-mone receptors and immunocompetent cells. Ann N Y
Acad Sci 840:510–517.
5. Postel-Vinay MC, de Mello Coelho V, Gagnerault MC, Dardenne M
(1997) Growthhormone stimulates the proliferation of activated
mouse T lymphocytes. Endocri-nology 138(5):1816–1820.
6. Yoshida A, Ishioka C, Kimata H, Mikawa H (1992) Recombinant
human growth hor-mone stimulates B cell immunoglobulin synthesis
and proliferation in serum-freemedium. Acta Endocrinol (Copenh)
126(6):524–529.
7. Merchav S, Tatarsky I, Hochberg Z (1988) Enhancement of human
granulopoiesis invitro by biosynthetic insulin-like growth factor
I/somatomedin C and human growthhormone. J Clin Invest
81(3):791–797.
8. Takagi K, Suzuki F, Barrow RE, Wolf SE, Herndon DN (1998)
Recombinant humangrowth hormone modulates Th1 and Th2 cytokine
response in burned mice. Ann Surg228(1):106–111.
9. DiFedele LM, et al. (2005) Tumor necrosis factor alpha
blockade restores growthhormone signaling in murine colitis.
Gastroenterology 128(5):1278–1291.
10. Han X, et al. (2007) Tumour necrosis factor alpha blockade
induces an anti-inflammatory growth hormone signalling pathway in
experimental colitis. Gut 56(1):73–81.
11. Murawski MR, Litherland SA, Clare-Salzler MJ,
Davoodi-Semiromi A (2006) Upregu-lation of Foxp3 expression in
mouse and human Treg is IL-2/STAT5 dependent: Im-plications for the
NOD STAT5B mutation in diabetes pathogenesis. Ann N Y Acad
Sci1079:198–204.
12. King C, Sarvetnick N (2011) The incidence of type-1 diabetes
in NOD mice is modu-lated by restricted flora not germ-free
conditions. PLoS ONE 6(2):e17049.
13. Pollard KM (2012) Gender differences in autoimmunity
associated with exposure toenvironmental factors. J Autoimmun
38(2-3):J177–J186.
14. Driver JP, Serreze DV, Chen Y-G (2011) Mouse models for the
study of autoimmunetype 1 diabetes: A NOD to similarities and
differences to human disease. Semin Im-munopathol 33(1):67–87.
15. Heit JJ, Karnik SK, Kim SK (2006) Intrinsic regulators of
pancreatic beta-cell pro-liferation. Annu Rev Cell Dev Biol
22:311–338.
16. Nielsen JH, Svensson C, Galsgaard ED, Møldrup A, Billestrup
N (1999) Beta cell pro-liferation and growth factors. J Mol Med
(Berl) 77(1):62–66.
17. McGrane MM, et al. (1990) Developmental regulation and
tissue-specific expressionof a chimaeric phosphoenolpyruvate
carboxykinase/bovine growth hormone gene intransgenic animals. J
Reprod Fertil Suppl 41:17–23.
18. Olsson B, et al. (2005) Bovine growth hormone transgenic
mice are resistant to diet-induced obesity but develop hyperphagia,
dyslipidemia, and diabetes on a high-fatdiet. Endocrinology
146(2):920–930.
19. Vasavada RC, et al. (2000) Targeted expression of placental
lactogen in the beta cellsof transgenic mice results in beta cell
proliferation, islet mass augmentation, andhypoglycemia. J Biol
Chem 275(20):15399–15406.
20. Smaniotto S, et al. (2005) Growth hormone modulates
thymocyte development invivo through a combined action of laminin
and CXC chemokine ligand 12. Endocri-nology 146(7):3005–3017.
21. Lin MS, et al. (2011) A multivalent vaccine for type 1
diabetes skews T cell subsets toTh2 phenotype in NOD mice. Immunol
Res 50(2-3):213–220.
22. Martin-Orozco N, et al. (2009) T helper 17 cells promote
cytotoxic T cell activation intumor immunity. Immunity
31(5):787–798.
23. Charré S, et al. (2002) Abnormalities in dendritic cell and
macrophage accumulation inthe pancreas of nonobese diabetic (NOD)
mice during the early neonatal period.Histol Histopathol
17(2):393–401.
24. Wu Y, et al. (2011) Growth hormone receptor regulates β cell
hyperplasia and glu-cose-stimulated insulin secretion in obese
mice. J Clin Invest 121(6):2422–2426.
25. Valera A, et al. (1993) Glucose metabolism in transgenic
mice containing a chimeric P-enolpyruvate carboxykinase/bovine
growth hormone gene. FASEB J 7(9):791–800.
26. Winer S, et al. (2003) Autoimmune islet destruction in
spontaneous type 1 diabetes isnot beta-cell exclusive. Nat Med
9(2):198–205.
27. Nakayama M, et al. (2005) Prime role for an insulin epitope
in the development oftype 1 diabetes in NOD mice. Nature
435(7039):220–223.
28. Kent SC, et al. (2005) Expanded T cells from pancreatic
lymph nodes of type 1 diabeticsubjects recognize an insulin
epitope. Nature 435(7039):224–228.
29. Brode S, Raine T, Zaccone P, Cooke A (2006)
Cyclophosphamide-induced type-1diabetes in the NOD mouse is
associated with a reduction of CD4+CD25+Foxp3+regulatory T cells. J
Immunol 177(10):6603–6612.
30. Komatsu N, Hori S (2007) Full restoration of peripheral
Foxp3+ regulatory T cell poolby radioresistant host cells in scurfy
bone marrow chimeras. Proc Natl Acad Sci USA104(21):8959–8964.
31. D’Alise AM, et al. (2008) The defect in T-cell regulation in
NODmice is an effect on theT-cell effectors. Proc Natl Acad Sci USA
105(50):19857–19862.
32. Gregori S, Giarratana N, Smiroldo S, Adorini L (2003)
Dynamics of pathogenic andsuppressor T cells in autoimmune diabetes
development. J Immunol 171(8):4040–4047.
33. Kim D-H, et al. (2011) Inhibition of autoimmune diabetes by
TLR2 tolerance.J Immunol 187(10):5211–5220.
34. Tarbell KV, Yamazaki S, Steinman RM (2006) The interactions
of dendritic cells withantigen-specific, regulatory T cells that
suppress autoimmunity. Semin Immunol 18(2):93–102.
35. You S, et al. (2008) Immunoregulatory pathways controlling
progression of autoim-munity in NOD mice. Ann N Y Acad Sci
1150:300–310.
36. Manirarora JN, Kosiewicz MM, Parnell SA, Alard P (2008) APC
activation restoresfunctional CD4(+)CD25(+) regulatory T cells in
NOD mice that can prevent diabetesdevelopment. PLoS ONE
3(11):e3739.
37. Savage NDL, et al. (2008) Human anti-inflammatory
macrophages induce Foxp3+ GITR+CD25+ regulatory T cells, which
suppress via membrane-bound TGFbeta-1. J
Immunol181(3):2220–2226.
38. Bending D, et al. (2009) Highly purified Th17 cells from
BDC2.5NOD mice convert intoTh1-like cells in NOD/SCID recipient
mice. J Clin Invest 119(3):565–572.
39. McGeachy MJ, et al. (2007) TGF-beta and IL-6 drive the
production of IL-17 and IL-10by T cells and restrain T(H)-17
cell-mediated pathology. Nat Immunol 8(12):1390–1397.
40. Peng H, Hagopian W (2006) Environmental factors in the
development of Type 1diabetes. Rev Endocr Metab Disord
7(3):149–162.
41. Yuen KC, Chong LE, Riddle MC (2013) Influence of
glucocorticoids and growth hor-mone on insulin sensitivity in
humans. Diabet Med 30(6):651–663.
42. Hill DJ, Petrik J, Arany E, McDonald TJ, Delovitch TL (1999)
Insulin-like growth factorsprevent cytokine-mediated cell death in
isolated islets of Langerhans from pre-diabetic non-obese diabetic
mice. J Endocrinol 161(1):153–165.
43. Whittaker PG, Taylor KW (1980) Direct effects of rat growth
hormone in rat islets oflangerhans in tissues culture. Diabetologia
18(4):323–328.
44. Rhodes CJ (2000) IGF-I and GH post-receptor signaling
mechanisms for pancreaticbeta-cell replication. J Mol Endocrinol
24(3):303–311.
45. Flodström-Tullberg M, et al. (2003) Target cell expression
of suppressor of cytokinesignaling-1 prevents diabetes in the NOD
mouse. Diabetes 52(11):2696–2700.
46. Jackerott M, et al. (2006) STAT5 activity in pancreatic
beta-cells influences the severityof diabetes in animal models of
type 1 and 2 diabetes. Diabetes 55(10):2705–2712.
47. Clark R (1997) The somatogenic hormones and insulin-like
growth factor-1: Stim-ulators of lymphopoiesis and immune function.
Endocr Rev 18(2):157–179.
48. Alard P, et al. (2006) Deficiency in NOD antigen-presenting
cell function may be re-sponsible for suboptimal CD4+CD25+
T-cell-mediated regulation and type 1 diabetesdevelopment in NOD
mice. Diabetes 55(7):2098–2105.
49. Serreze DV, et al. (1998) B lymphocytes are critical
antigen-presenting cells forthe initiation of T cell-mediated
autoimmune diabetes in nonobese diabetic mice.J Immunol
161(8):3912–3918.
50. Wan YY, Flavell RA (2007) Regulatory T-cell functions are
subverted and convertedowing to attenuated Foxp3 expression. Nature
445(7129):766–770.
51. Gebert CA, Park SH, Waxman DJ (1997) Regulation of signal
transducer and activatorof transcription (STAT) 5b activation by
the temporal pattern of growth hormonestimulation. Mol Endocrinol
11(4):400–414.
52. Pallandre J-R, et al. (2007) Role of STAT3 in
CD4+CD25+FOXP3+ regulatory lympho-cyte generation: Implications in
graft-versus-host disease and antitumor immunity.J Immunol
179(11):7593–7604.
53. Chen BJ, et al. (2010) Growth hormone mitigates against
lethal irradiation and en-hances hematologic and immune recovery in
mice and nonhuman primates. PLoSONE 5(6):e11056.
E4626 | www.pnas.org/cgi/doi/10.1073/pnas.1314985110 Villares et
al.
Dow
nloa
ded
by g
uest
on
June
21,
202
1
http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.1314985110/-/DCSupplemental/pnas.201314985SI.pdf?targetid=nameddest=ST2www.pnas.org/cgi/doi/10.1073/pnas.1314985110
-
54. Martinez FO, Sica A, Mantovani A, Locati M (2008) Macrophage
activation and po-larization. Front Biosci 13:453–461.
55. Gordon S (2003) Alternative activation of macrophages. Nat
Rev Immunol 3(1):23–35.56. Zizzo G, Cohen PL (2013) IL-17
stimulates differentiation of human anti-inflammatory
macrophages and phagocytosis of apoptotic neutrophils in
response to IL-10 andglucocorticoids. J Immunol
190(10):5237–5246.
57. Komiyama Y, et al. (2006) IL-17 plays an important role in
the development of ex-perimental autoimmune encephalomyelitis. J
Immunol 177(1):566–573.
58. Hirota K, et al. (2007) Preferential recruitment of
CCR6-expressing Th17 cells toinflamed joints via CCL20 in
rheumatoid arthritis and its animal model. J Exp
Med204(12):2803–2812.
59. Ghoreschi K, Laurence A, Yang XP, Hirahara K, O’Shea JJ
(2011) T helper 17 cellheterogeneity and pathogenicity in
autoimmune disease. Trends Immunol 32(9):395–401.
60. Marwaha AK, Leung NJ, McMurchy AN, Levings MK (2012) TH17
Cells in Autoim-munity and Immunodeficiency: Protective or
pathogenic? Front Immunol 3:129.
61. Wang R, et al. (2007) The role of STAT3 in antigen-IgG
inducing regulatoryCD4(+)Foxp3(+)T cells. Cell Immunol
246(2):103–109.
62. Gaba A, et al. (2012) Cutting edge: IL-10-mediated
tristetraprolin induction is part ofa feedback loop that controls
macrophage STAT3 activation and cytokine production.J Immunol
189(5):2089–2093.
63. Hoang PT, et al. (2010) The neurosurvival factor Humanin
inhibits beta-cell apoptosisvia signal transducer and activator of
transcription 3 activation and delays andameliorates diabetes in
nonobese diabetic mice. Metabolism 59(3):343–349.
64. Mori H, et al. (2007) Suppression of SOCS3 expression in the
pancreatic beta-cell leadsto resistance to type 1 diabetes. Biochem
Biophys Res Commun 359(4):952–958.
65. Cecim M, Kerr J, Bartke A (1995) Effects of bovine growth
hormone (bGH) transgeneexpression or bGH treatment on reproductive
functions in female mice. Biol Reprod52(5):1144–1148.
66. Dietrich WF, et al. (1996) A comprehensive genetic map of
the mouse genome. Na-ture 380(6570):149–152.
67. Montanya E, Téllez N (2009) Pancreatic remodeling: Beta-cell
apoptosis, proliferationand neogenesis, and the measurement of
beta-cell mass and of individual beta-cellsize. Methods Mol Biol
560:137–158.
68. Ye J, et al. (2012) Primer-BLAST: A tool to design
target-specific primers for poly-merase chain reaction. BMC
Bioinformatics 13:134.
Villares et al. PNAS | Published online November 11, 2013 |
E4627
IMMUNOLO
GY
PNASPL
US
Dow
nloa
ded
by g
uest
on
June
21,
202
1