Embed Size (px)
Citation preview
GROUP 2: Martha Ingram, Megan Johnston, Chelsea Samson
MENTORS: Dr. Michael Holzman, Dr. William Beck, Dr. Benjamin Poulose
AN OPENING IN THE ABDOMEN,AN OPENING IN THE MARKET:
HERNIA TENSIOMETERS
Hernias and their repair
Background
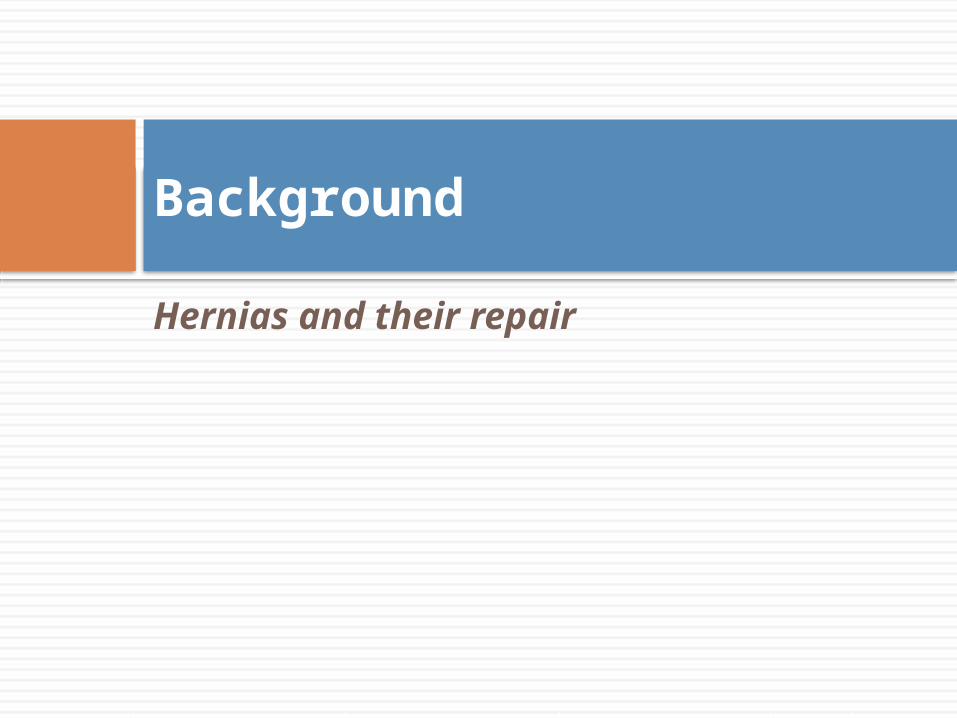
What is a hernia?
Protrusion of the abdominal contents through a hole in the musculature Affects 5 million
Americans every year Must surgically realign
the musculature and create a barrier, or circulatory and digestive complications may result
Repairing Hernias
Minimally-invasive laparoscopic surgery
Open hernia surgery performed for hernias greater than 25cm wide
Current solutions… …and complications
Tension from the abdominal muscles and fascia pulls sutures apart
Failure in over 40% of patients, despite “tension-free” repair method
Acceptable recurrence rate is 15%
“Making the Case for Hernia Research”Benjamin Poulose et al., 2011(Vanderbilt Medical Center)
Financial Impact of Decreasing Hernia Recurrence
Cost/Benefit Analysis
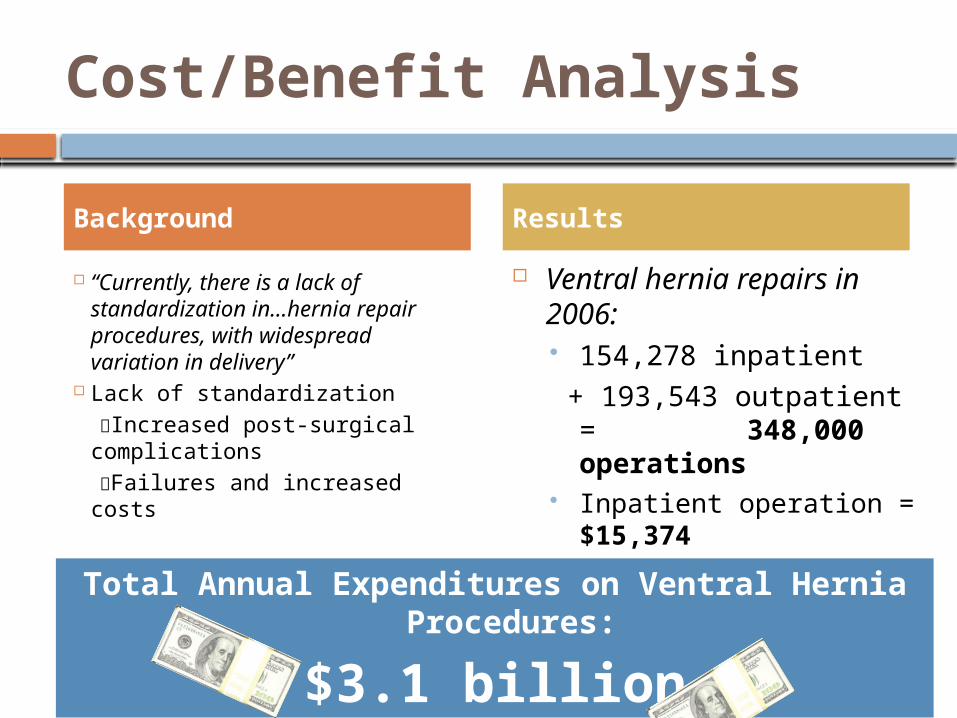
“Currently, there is a lack of standardization in…hernia repair procedures, with widespread variation in delivery”
Lack of standardization Increased post-surgical
complications Failures and increased costs
Ventral hernia repairs in 2006: 154,278 inpatient
+ 193,543 outpatient = 348,000 operations
Inpatient operation = $15,374
Outpatient operation = $3,745
Background Results
Total Annual Expenditures on Ventral Hernia Procedures:
$3.1 billion
40% recurrence 15% recurrence
= $775 million savedThe application of an intra-operative tension-
measuring device could increase understanding of and prevent hernia
recurrence, significantly decreasing costs.
Device requirements
Using Tension Measurements to Determine Recurrence Rates
Data Collection
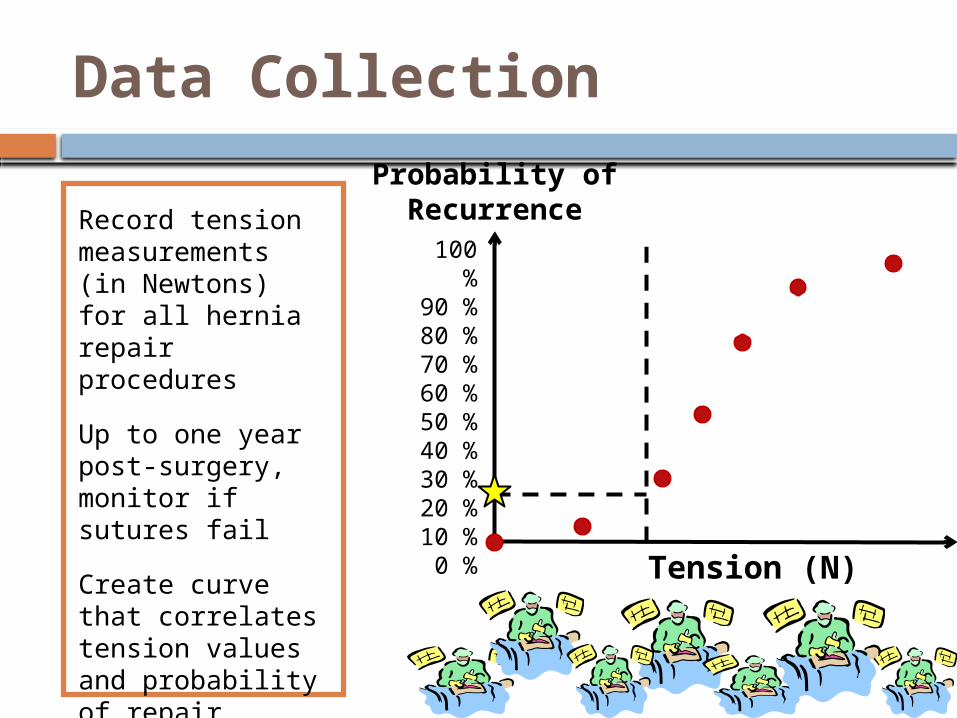
Record tension measurements (in Newtons) for all hernia repair procedures
Up to one year post-surgery, monitor if sutures fail
Create curve that correlates tension values and probability of repair failure
Determine tension at 15% recurrence
Tension (N)
100 %
90 %80 %70 %60 %50 %40 %30 %20 %10 %0 %
Probability of Recurrence
User Response
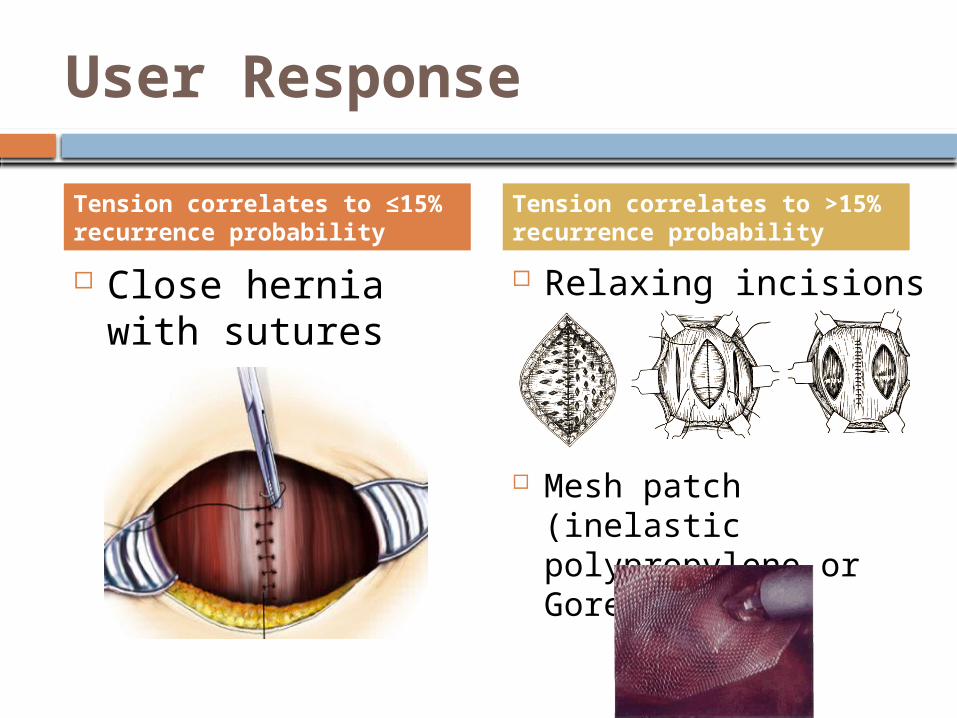
Close hernia with sutures
Relaxing incisions
Mesh patch (inelastic polypropylene or Gore-Tex)
Tension correlates to ≤15% recurrence probability
Tension correlates to >15% recurrence probability
Evolution of the device
Designing the Tensiometer
Device Functions and Qualities
Measure tension resisting closure at the central suture line, longitudinal to muscle alignment, after: dissection of the injury area separating fascia from muscle
Sterilizable, reusable, strong
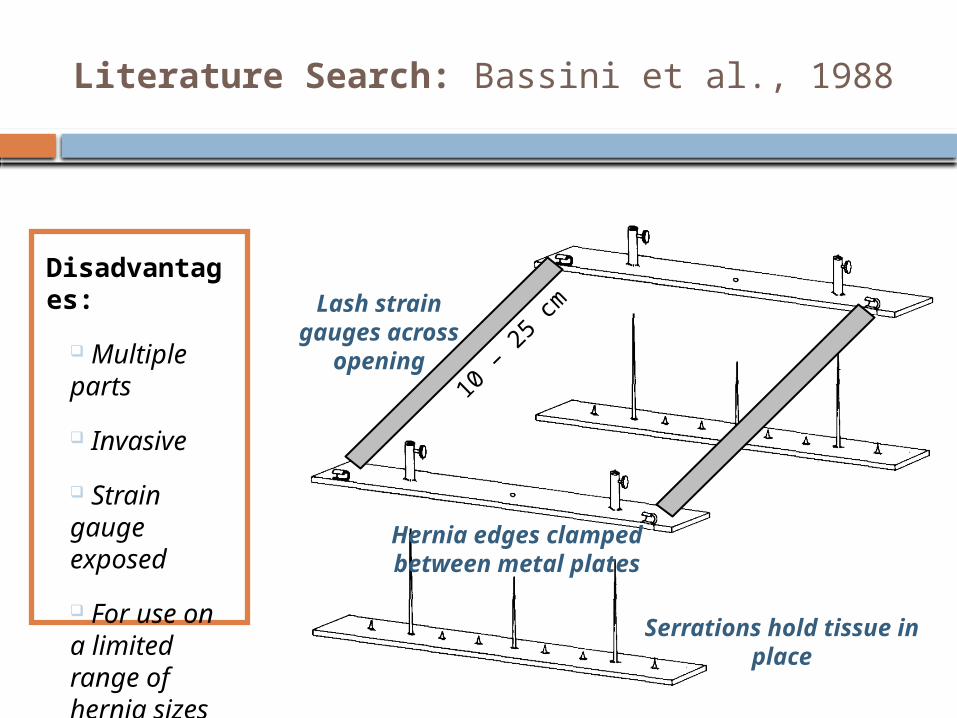
Literature Search: Bassini et al., 1988
Disadvantages:
Multiple parts
Invasive
Strain gauge exposed
For use on a limited range of hernia sizes
Hernia edges clamped between
metal plates
Serrations hold tissue in place
Lash strain gauges across
opening10
– 25
cm
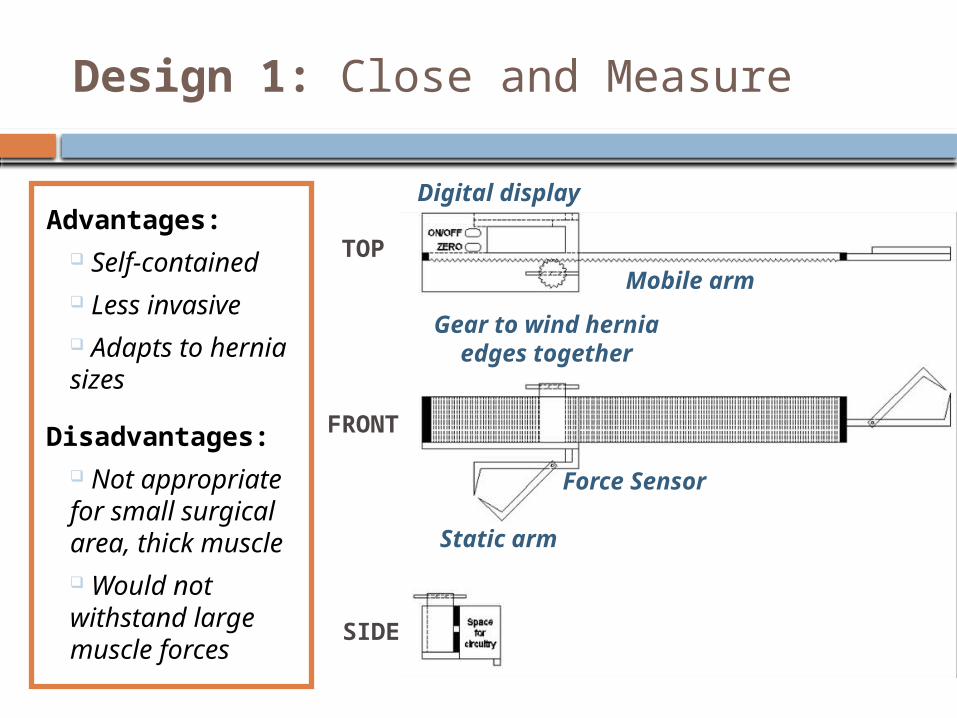
Design 1: Close and Measure
Advantages: Self-contained Less invasive Adapts to hernia sizes
Disadvantages: Not appropriate for small surgical area, thick muscle Would not withstand large muscle forces
FRONT
SIDE
TOP
Static arm
Mobile arm
Digital display
Gear to wind hernia edges
together
Force Sensor
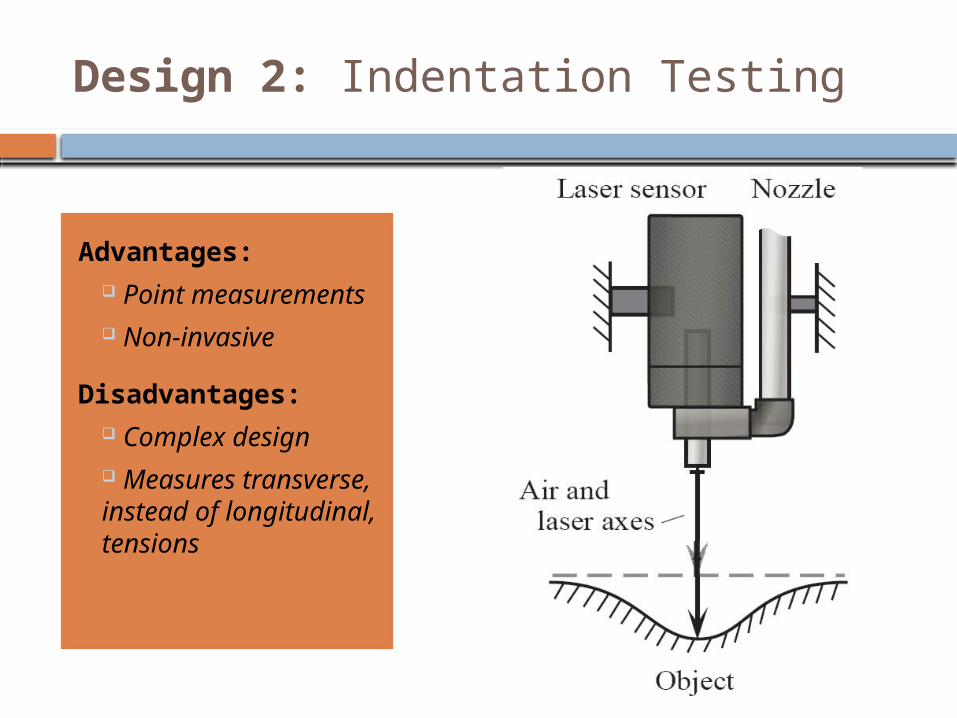
Design 2: Indentation Testing
Advantages: Point measurements Non-invasive
Disadvantages: Complex design Measures transverse, instead of longitudinal, tensions
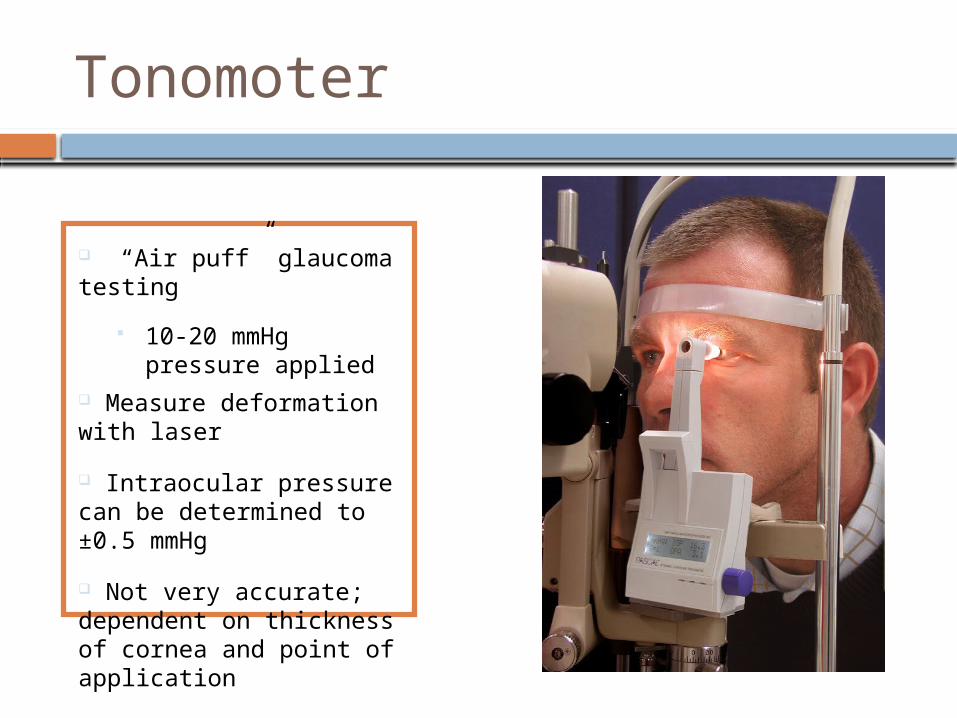
Tonomoter
“Air puff” glaucoma testing
10-20 mmHg pressure applied
Measure deformation with laser
Intraocular pressure can be determined to ±0.5 mmHg
Not very accurate; dependent on thickness of cornea and point of application
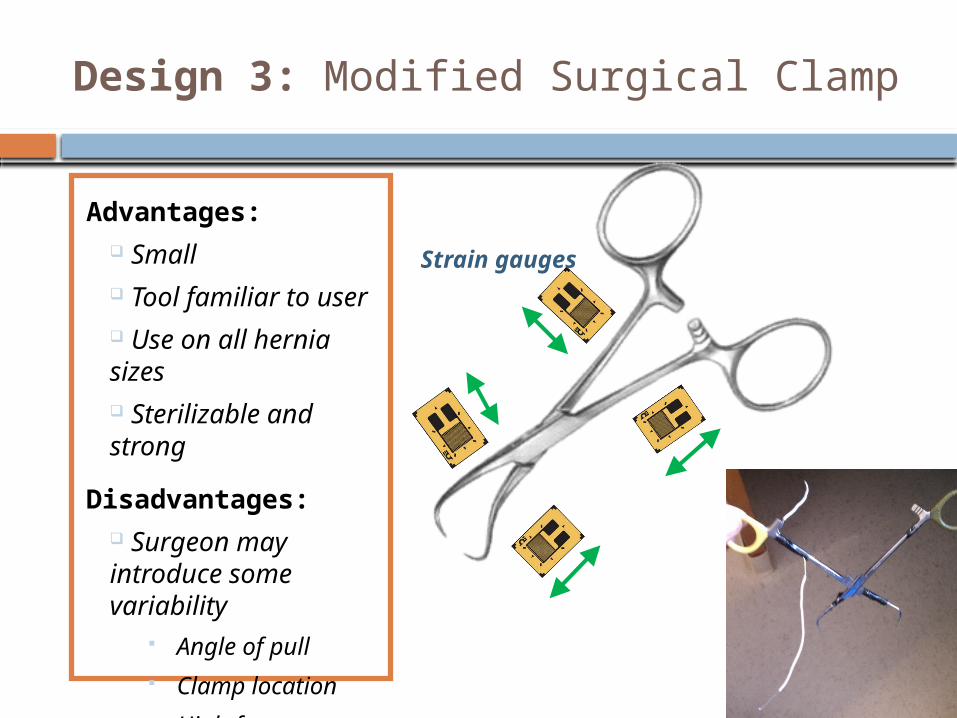
Design 3: Modified Surgical Clamp
Advantages: Small Tool familiar to user Use on all hernia sizes Sterilizable and strong
Disadvantages: Surgeon may introduce some variability
Angle of pull Clamp location High-frequency
noise
Strain gauges
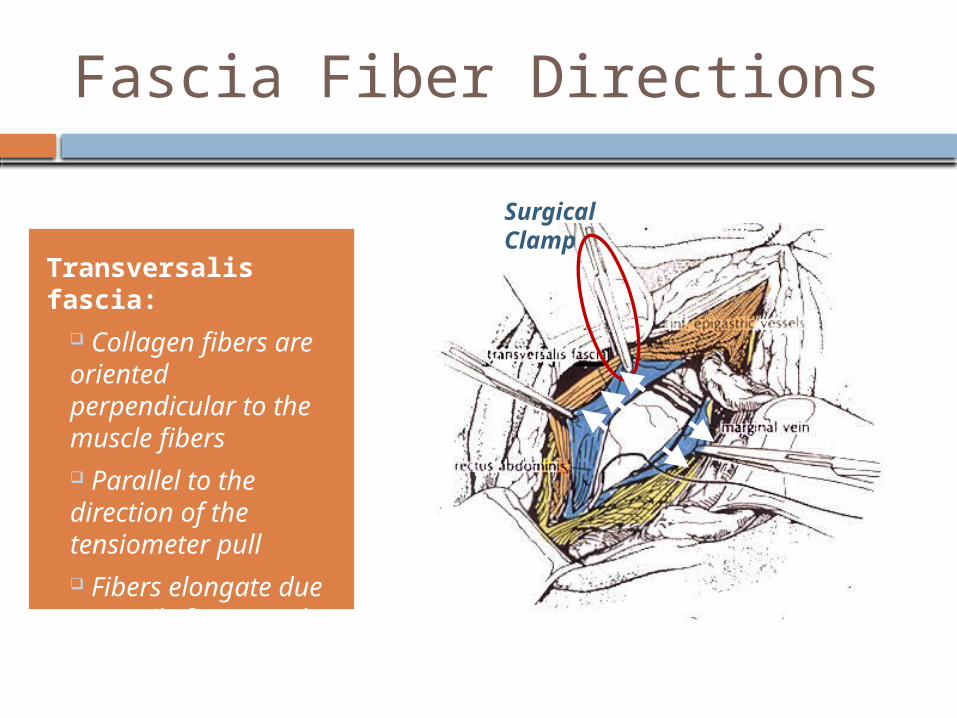
Fascia Fiber Directions
Transversalis fascia:
Collagen fibers are oriented perpendicular to the muscle fibers Parallel to the direction of the tensiometer pull Fibers elongate due to tensile forces and can rupture
Surgical Clamp
Proof of Concept
Strain gauge in Wheatstone Bridge Instrumentation
Amplifier [Low Pass Filter]Output Voltage
Resistance changes when clamp is pulled
Voltage changes when clamp is pulled
Clamp end
Handle end
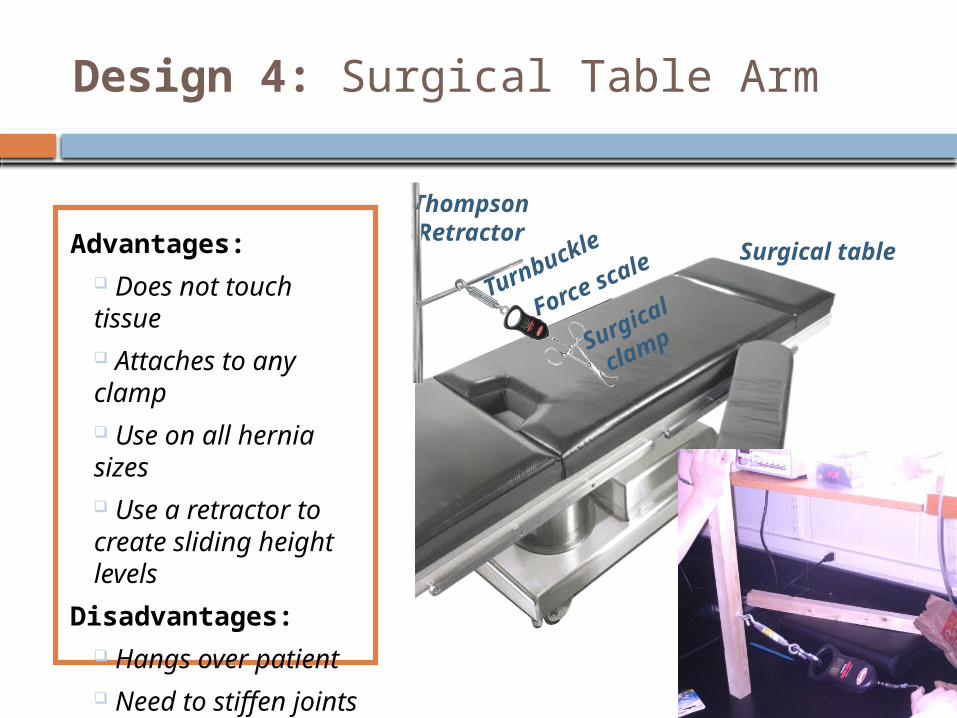
Design 4: Surgical Table Arm
Advantages: Does not touch tissue Attaches to any clamp Use on all hernia sizes Use a retractor to create sliding height levels
Disadvantages: Hangs over patient Need to stiffen joints (epoxy)
Thompson Retractor
Surgical table
Turnbuckle
Surgical
clampForce scale
Future Proof of Concept• Testing on porcine model the week of April 4th
• Clamp on one side of hernia; force scale on other• Determine tension values and standard deviations