Embed Size (px)
Citation preview

You are not alonePolymyalgia Rheumatica and Giant Cell Arteritis Newsletter Summer 2016
You are not aloneRegistered Charity No: 1138409
www.pmr-gca-northeast.org.uk 1
Our cover photo was taken at a Durham Park Run in April. Family and Friends went along to support. John Robson (bottom left) was taking part in his 100th Park Run.
Four of the eight runners, John, Emma, Gillian and Andrew, are also running in the Great North Run to raise funds for PMR&GCAUK North East Support. They pay their own entry fee and the only support we give is to provide the Running Vests. They refuse any other help.
To support them and, of course us, by making a donation, visit our website: www.pmr-gca-northeast.org.uk
and then click on: Donate or visit www.justgiving.com/Emma-Robson95 where Emma has set up a Team Page.
Why not support them? Go along on the day and cheer them on. Let‘s go our TEAM, let‘s go!
Support our RunnersGreat North Run 11September 2016 Team PMR&GCA
John Emma Andrew Gillian
New Video PMR&GCA North East Support group
now on YouTube:
youtu.be/_DQAgXzp8jc
Donatevia Just Giving

2www.pmr-gca-northeast.org.uk
Too many GPs miss symptoms of GCA says PMR&GCAuk Charity Patron Lord Wills but exciting progress is being madePMRGCAuk patron Lord Wills, formerly a health minister himself, has made a passionate call for improved diagnosis and treatment of GCA in a speech to rheumatologists who had gathered from across the world to attend a special symposium in Southend organised by our president Professor Bhaskar Dasgupta.
Lord Wills condemned the poor diagnosis and treatment, which mean that an estimated 3,000 patients a year suffer sight loss through GCA.
“Why are thousands of these avoidable tragedies happening every year?” he asked. “Far too often, GPs miss the symptoms. Far too often, patients are prescribed the wrong treatment and too late. You all know the devastation giant cell arteritis can cause – and how relatively easily it can be treated with the right diagnosis
GCA Guidelines
early enough – so why isn’t this happening and why isn’t the government more actively supporting action to promote such early diagnosis?”
Lord Wills said best clinical practice suggested that patients with suspected GCA should be started on high-dose steroids immediately without waiting for specialist review. They should then be referred quickly for a temporal artery biopsy or ultrasound to confirm diagnosis.
He said that a fast-track system launched for strokes had transformed treatment for that condition. “So, if the government can take such action on strokes, why isn’t it now taking similar action over GCA, which is in effect a stroke in the eye? Nevertheless, some progress has been made.” He welcomed the fact that new national guidelines were being drawn up and that a
Photographed at the special symposium organised in March 2016.

3 www.pmr-gca-northeast.org.uk
GCA Guidelinesfast-track pathway for swift diagnosis and treatment had been pioneered by Professor Dasgupta in Southend “with remarkable results”.
Lord Wills has helped PMRGCAuk lobby ministers and senior health officials over a period of five years. “After a series of parliamentary questions and several debates in the House of Lords and, most recently, with the support of the admirable Health Minister David Prior, NHS England has begun to engage with the need to address this issue more seriously. Two years ago, Sir Bruce Keogh, the Medical Director of NHS England, wrote to me that this fast-track pathway ‘represents a new way of doing things which is better and costs no more. We must learn from such innovative examples.’ “
“NHS England has now agreed to support the dissemination of best practice including the Southend Fast Track Pathway. And it has agreed to monitor on a regular basis the incidence of sight loss from GCA.” Currently, no national statistics are gathered on sight loss through GCA. The gathering of national statistics on other medical conditions, like lung cancer, has transformed diagnosis and treatment by showing up disparities in treatment in different parts of the country. Lord Wills also revealed that NHS England has agreed to publicise the fact that sight loss through GCA should be regarded by medical staff as what is formally known as ‘a serious untoward incident’. When a serious untoward incident is recorded, staff have to investigate within 28 days why the event took place and put systems in place to ensure it doesn’t happen again in future.
“As a means of consciousness raising, NHS England has agreed to publicise the fact that GCA-related sight loss is covered by the serious incident framework. This could be an important driver of progress, but the problem has been that this appears not to be widely known. As far as I have been able to discover, there is no known case of GCA-related sight loss being recorded as a serious incident. And so publicising this should help raise consciousness among clinicians.”
BSR AWARD FOR OUTSTANDING BEST PRACTICE: March 2015–16 Preventing blindness by fast-tracking suspected Giant Cell Arteritis patients to immediate treatment.
At the symposium Professor Dasgupta (founder member of PMRGCAuk and a Patron of PMR&GCAUK North East Support), who developed the fast-track pathway, said: “The pathway significantly reduces irreversible sight loss. This award means it’s now going to have national backing from the BSR for them to take it forward with commissioning authorities so that this pathway is rolled out across the country and perhaps at some point across the globe to benefit all patients. It is one of the main culminations of all the hard work and research that we have done.”
The fast-track pathway (FTP) at the Southend University Hospital NHS Trust has significantly reduced the number of patients suffering sight loss as an avoidable complication of giant cell arteritis (GCA). Furthermore, the service is cost-saving, results in an increased patient quality of life, and successfully reduces the time to diagnosis in line with clinical established guidelines.
(Extract from BSR Handout No 7 issued by the BSR at the Symposium held in March at Southend.)
Education is key ‘Time is Sight’

4www.pmr-gca-northeast.org.uk
Demystifying DIABETES In relation to Polymyalgia Rheumatica & Giant Cell Arteritis
My name is Karen Craggs. I was kindly invited by the North East support group for PMR&GCA, in my capacity as Lead Dietitian for Newcastle Diabetes Service, to talk about the link with PMR, GCA and how they link to Diabetes. But most importantly, how to support the self-management of blood glucose levels through diet and lifestyle, and the myriad of medications that can accompany this unwelcome diagnosis.
My main role as a Diabetes Specialist Dietitian for Newcastle Diabetes Service, is to support people to manage their condition on a daily basis through education about the vital link between food, blood glucose, insulin production, activity levels and any medications. This can be overwhelming for most; we help to make sense of all of the treatment information, and assist the person in identifying ways to incorporate this management into their daily lives, so that they are looking after their health.
So, what IS Diabetes? Diabetes is diagnosed when the body can no longer control glucose levels which occur after ingestion of certain foods. This is a problem because when left uncontrolled, constant high blood glucose levels can lead to long-term cardiovascular problems such as heart attack and stroke. Diabetes occurs when:
a) The body is no longer able to use its own insulin production effectively leaving blood glucose high, especially after a meal. This is known as Insulin Resistance. Insulin is the hormone responsible for transporting the glucose out of the bloodstream and into the cells where it will be used as energy.
As a result of blood glucose levels remaining constantly higher than desired, the pancreas responds by ‘working overtime’ making more insulin to keep up with the demand. This can be happening for up to 10 years, but eventually the pancreas will become unable to maintain this level of production and will ‘wear out’ leading eventually to:
b) A decline in the body’s ability to produce enough insulin in response to a meal
High glucose levels in the bloodstream over a long period of time weaken the walls of the blood vessels. Blood vessels are everywhere in the body, so this damage is what we are trying to avoid in daily diabetes management. Days add up to weeks, weeks add up to months, months add up to years of extra wear and tear on the blood vessels. So, the overall aim of diabetes management is about understanding how to keep blood glucose levels under control and protect those blood vessels from long-term damage.
We do this through a mixture of watching the type and amount of food we eat, taking any prescribed medication – at the time and dose prescribed, being active on a daily basis and aiming for, or keeping to, a healthy weight range.
Diabetes occurs in people with PMR often due to the high dose use of corticosteroids used to treat the symptoms of pain and reducing inflammation in the joints. Higher doses to alleviate pain taken for greater than three weeks can often lead to an increased risk of diabetes.
‘Mimic’ the body’s stress response to injury by asking your liver to release stored glucose, thus raising blood glucose levels – as if you have eaten some form of sugar! Because the drug is in your body constantly and sometimes in high doses to control pain, the effect on your blood glucose is as if you have been constantly eating some form of carbohydrate. This leads to the condition known as Insulin Resistance. Corticosteroids
9 inch plate
5 www.pmr-gca-northeast.org.uk
also can increase your appetite, which can lead to weight gain, and weight gain also leads to Insulin Resistance. This is where the risk of PMR and diabetes meet.
Not everyone with PMR will go on to get diabetes, but certain conditions aside from the use of corticosteroids, increase the risk independently: overweight, family history of diabetes, previous gestational diabetes, polycystic ovarian syndrome, over 40yrs old and Caucasian, over 25yrs old and South Asian, Afro-Caribbean or Middle Eastern ethnicity. As more of the above apply to you, the greater the risk of diabetes.
What are the symptoms of diabetes?Lethargy or extreme tiredness – especially noticeable after a meal, going to the toilet more often – especially at night, excessive thirst and dry mouth, occasional blurred vision, recurrent infections such as skin or thrush. These symptoms are all caused directly by high levels of glucose in the bloodstream.
At the end of the treatment course of corticosteroids blood glucose levels may return to normal levels. If you had pre-existing diabetes prior to corticosteroids, diabetes is likely to remain. If you were in the high risk of diabetes category prior to corticosteroids course, then diabetes may remain.
These symptoms can all be alleviated by reducing blood glucose levels. We can do that through our diet by controlling the amount of carbohydrate that we eat.
Carbohydrate – what exactly are carbohydrates I hear you say!Carbohydrates are a nutrient that the human body needs. It provides us with energy and plays a very important role in diabetes and glucose control.
Carbohydrates have two parts to their nutrient group; sugary carbohydrates and starchy carbohydrates. The sugary ones are easy to identify as they taste sweet: fruit
juice, cakes, biscuits, sweets, chocolate, sugary drinks.
Starchy carbohydrates don’t usually taste sweet I call them the ‘Big Five’ because no matter where you go in the world, these foods can be easily identified and enjoyed in various forms: bread, potato, pasta, rice and cereal grains. Now think laterally; everything made from or with the cereal grains (flour): crackers, crumpets, teacakes, scones, Yorkshire pudding, batter etc – the list goes on.
It is an important nutrient that is hugely prevalent in today’s diet and therefore influential on our blood glucose levels so we need to be able to identify it, consider how much of it we are going to have or have had, in order to control our blood glucose levels.
This is important because carbohydrate is broken down to glucose by the body, this is then the human body’s ‘fuel’. Carbohydrate is the nutrient that provides the body with potential energy. When we eat carbohydrates, which are then broken down to glucose, it is nature’s way of ‘filling our fuel tank’. However, it can only be used as fuel if insulin is released by the pancreas in similar amounts to the rise in glucose caused by eating the carbohydrates.
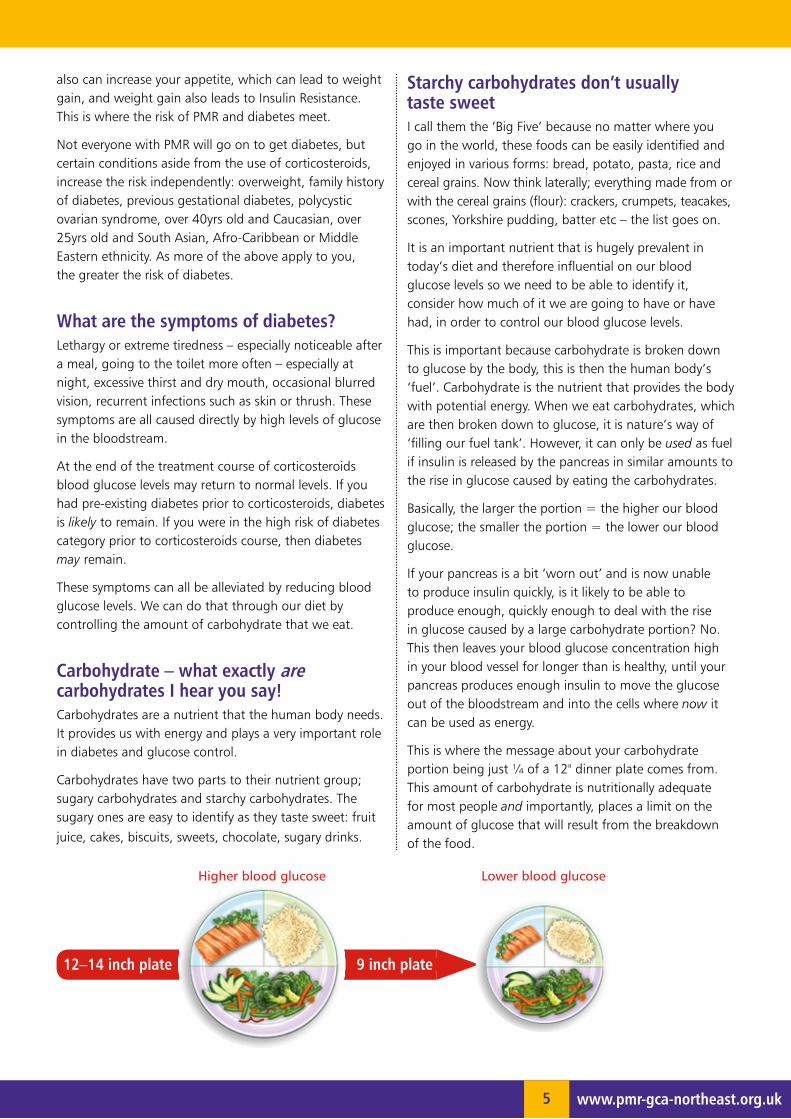
Basically, the larger the portion = the higher our blood glucose; the smaller the portion = the lower our blood glucose.
If your pancreas is a bit ‘worn out’ and is now unable to produce insulin quickly, is it likely to be able to produce enough, quickly enough to deal with the rise in glucose caused by a large carbohydrate portion? No. This then leaves your blood glucose concentration high in your blood vessel for longer than is healthy, until your pancreas produces enough insulin to move the glucose out of the bloodstream and into the cells where now it can be used as energy.
This is where the message about your carbohydrate portion being just ¼ of a 12" dinner plate comes from. This amount of carbohydrate is nutritionally adequate for most people and importantly, places a limit on the amount of glucose that will result from the breakdown of the food.
12–14 inch plate
Higher blood glucose Lower blood glucose

6www.pmr-gca-northeast.org.uk
Of course, we all know what eventually happens as a result of eating smaller portions – we lose weight! If you have any weight to lose, this will always remain a part of your treatment for diabetes, no matter the amount, no matter what medications you take for your diabetes. As you lose weight, the dose of diabetes medications will need to be monitored and reduced. Sometimes, stopped altogether.
In people with diabetes, body fat tends to settle around the torso, under the skin and around the organs. This can be thought of as an ‘obstacle course’ for your slowly produced insulin to have to work through. This is the condition known as Insulin Resistance as referred to above, when your insulin is unable to be used effectively.
This is the reason why.
As you lose weight, you are reducing the size of the ‘obstacle course’ that your insulin has to get through, thus allowing it to get where it needs to go quicker (to the glucose) resulting in lowered blood glucose in the bloodstream because the glucose has now been carried out of the bloodstream and into the cells of the body where it can now be used as energy. Because the glucose concentration is now at a level that your blood vessels are designed by nature to carry, your blood vessels are not being subjected to such aggressive ‘wear and tear’ by high levels of glucose.
So, ALL food affects our weight, but NOT ALL food affects our blood glucose…Let’s have a closer look at that statement:
4 FATS eg spreads, oils – have no immediate effect on our blood glucose levels, but in the longer term, affects our weight = increasing Insulin Resistance effect
4 PROTEINS eg meat, fish, eggs – have no effect on blood glucose levels, but may affect our weight = Insulin Resistance depending on our portions, if the meat is a fatty cut, if we cooked it without fat, if we removed visible fat
4 VEGETABLES eg carrots, broccoli – have no effect on weight and no effect on blood glucose
4 FRUIT eg bananas, apples – affects our blood glucose but not our weight
4 MILK & DAIRY eg milk, yogurt – affects blood glucose and may affect weight if full fat products used
4 CARBOHYDRATES eg bread, pasta, potatoes, rice, cereal grains – SUGARS & STARCHES – BOTH AFFECT WEIGHT & BLOOD GLUCOSE
Fill up on
veggies!

7 www.pmr-gca-northeast.org.uk
To summarise the dietary management of diabetes – whether linked to PMR or not:4 Aim for a healthy weight range [Reduces Insulin
Resistance]
4 Lose weight if you need to [Reduces Insulin Resistance, Increases Insulin production and efficiency]
4 Monitor and Limit carbohydrate portions to ¼ plate at each meal [Reduces glycaemic load, leads to weight loss]
4 Choose slower released carbohydrates – Low GI (wholegrain varieties) [Slow Insulin production has a chance to ‘keep up’ with glucose entering the bloodstream]
4 Fill up on vegetables [Weight loss/maintenance, Low GI addition]
4 Limit fruit to 3 portions per day [Controls glycaemic load]
4 Use less fats and oils and choose lower fat food choices [Reduces Insulin Resistance and weight]
4 Choose monounsaturated fats (olive and rapeseed) over polyunsaturated (sunflower and corn) or saturated (butter) [Cardiovascular protection, reduced Insulin Resistance]
4 Keep treats to occasional [maintains weight and blood glucose]
4 Eat fish twice a week, one of which is oily [Cardiovascular protection]
4 Be as active as you can manage – daily [Lowers/maintains blood glucose levels, expedites weight loss, improves cardiovascular protection]
Research in diabetesNewcastle upon Tyne’s Newcastle University is a centre of excellence for diabetes research.
Presently, the largest study ever funded by Diabetes UK is being carried out by some of the Professors of Endocrinology and research colleagues that I work with on a daily basis.
The study is at its third stage: tracking the glucose journey through the body and where and at what point does diabetes occur in some but not others; the exact role of the liver and pancreatic function in glucose metabolism and the effects of fat infiltration in these organs being linked to the onset of diabetes; the effects of significant weight loss on the potential reversal of Type 2 diabetes – the ‘magic number’ appears to be around 15kg weight loss; the duration of diabetes prior to significant weight loss occurring – does this still ‘reverse’ diabetes?
What a fascinating and complicated subject diabetes is – I can’t wait to hear the outcomes of the study as they emerge and to continue to be part of improving the health of the people of the North East of England.
Howay the Lads & Lasses!
Eat fish
twice a week!

8www.pmr-gca-northeast.org.uk
Fleur Anderson’s storyMy story begins late December 2015, after
suffering from what I thought was a pulled hamstring in both legs. I was treated by a
physiotherapist to solve the issue, but was puzzled that no amount of painkillers or treatment were successful. As time went on the pain seemed to move to my hips and neck and it was suggested that I had tests for arthritis and rheumatism – which proved negative. From then on I was determined to find out why I was in so much pain and no amount of NSAIDs, Tramadol etc could alleviate the intense pain I was in. It was becoming increasingly difficult to carry out day to day activities and looking after a 4-year-old and a husband was becoming more demanding as time went on.
At this point I sought the advice of a private rheumatologist where I had numerous tests and the results showed that not only were my ESR rates high but also my CRP, which reinforced that there was definite inflammation in my body. I had had a sore throat which had lasted over 6 weeks and on further investigation – a streptococcal virus was found to be present. This was cleared up by an intensive course of antibiotics, but from then I was still suffering with the constant ache and stiffness in the morning getting out of bed. I then turned to the Internet to try and find an explanation for my symptoms. It wasn’t until I came across the condition Polymyalgia Rheumatica that I immediately recognised the symptoms and the need for support and the necessary treatment.
With this in mind and my next appointment with the rheumatologist, I asked if he would give me a short course of prednisone, as I was sure that I had this condition/disease… He was reluctant at first, as I was young, 47, and this condition usually happens to those much older. He hadn’t had a patient under the age of 60 who had suffered these symptoms. So with 10 days supply... I really needed this to work. To my amazement 12 hours later, I actually got out of bed and performed my daily activities as a normal person. Wow, what an immediate relief!
I then began to realise what changes I would need to make. With further research on the Internet, I came across a website PMR&GCAUK North East Support… at first I thought this was an American site as all forums seemed to be American based. Not only was this in my town but one of the Charity Project Coordinators lived a mile away …. I joined immediately and within a day I was talking and meeting up with Margaret. The support I have received as a result has been so beneficial and valuable and I am very grateful.
Realising that this charity is small and usually age related, I decided to share my experiences with my students at school. I felt that it was important for them to understand that some days I have in school are good and other days can be more difficult. I wore one of the pansy badges one day and my tutor group were intrigued. This led me to want to further their understanding of the condition and we have at present raised £150 from the
selling of the badges. Within the next few weeks we hope to broadcast on local radio an interview with both myself and a representative from the charity to raise the awareness of this condition in order to enable those who are suffering to access effective support and guidance.
Self-diagnosis can be frowned upon but on this occasion proved accurate. Medical understanding of PMR is in its infancy, but with the right support and research, the Charity can provide a secure and understanding network.
Fleur Anderson – joined April 2016

9 www.pmr-gca-northeast.org.uk
Who is Eileen? I’ve been asked to talk about me! I am a wife of a scientist
(who fulfils every caricature of the vague professor!), mother of two daughters, one nurse-trained but working in social care and one who is a paramedic and studying for a Master’s degree. I have three grandchildren: the nurse daughter has a boy of 14 and girl of 16, and the paramedic has a 17-year-old stepson. I don’t think I am old enough for that – but I suppose I must be!
Originally I wanted to study medicine – but realised I didn’t want to starve for 6 years which is what it would have meant in those days! I left university and worked as a technologist in the NHS laboratories for several years, then went to St Andrews University to study physiology for an Honours degree before working in the college where technologists did their qualifications. My husband then moved to Germany and my own career was interrupted but I started translating medical and scientific texts for his University department and a medical market research company. I set up my own business which continued when we returned to the UK.
Before we moved to Germany, my husband had moved from physics to medical physics, obtaining a PhD, having developed an electrode to measure pH in skin. In Germany, he did a German postdoctoral Doctorate in physiology, developing an electrode which measures oxygen levels in skin. He continued with his research when we returned to the UK to work as a Clinical Scientist running a diagnostics department in the NHS, developing techniques for measuring oxygen levels in tissue, working on monitoring babies in the NICU, amputation level assessments, breast reconstruction after mastectomy and surgery to create stomas – nothing if not varied – and for some time I worked with him on some of the projects as a technologist until the grants came to an end. Some was done in Dundee, some in Durham.
PMR had raised its head but it wasn’t diagnosed for five years until shortly before my husband retired and we intended moving abroad to live again. I had a major flare – but had to find the answer myself and in doing so came across the patient info PMRGCA forum – where Mavis Smith of the PMR&GCAUK North East Support group posted regularly. One day she posted about the launch of the DVD, “You are not alone” – it so happened I was going to be “home” in the UK, in Durham, that day. I contacted her to ask if I could come to the event. I turned up at the Centre for Life in Newcastle to find a lady sitting outside the main door in a wheelchair – Mavis! She had arranged for me to remain for the lunch after the launch and that was when I met the people who had started
PMR&GCAUK North East Support. I went back to Italy, where I now lived, but became involved with the forum linked to the NE group when it started and then later with the HealthUnlocked forum. I have now had PMR for 12 years and have been on steroids for nearly 7 years.
Most of my involvement has been providing support on the forums, but a few years ago I was asked to advise the Leeds PMRGCA research group on a patient-related subject and that has resulted in me becoming a Patient Research Partner with them. My years of translation and medical background have taught me to “translate” medical-speak to patient-speak and this has made me passionate about communication as well as patients being able to share in their management to the best of their ability. Just a few weeks ago I was invited, together with 20-odd other patients, to a meeting of rheumatologists and other healthcare professionals where we, the patients, form an interface with the professionals, talking about our experiences of our illnesses and explaining what is important to us when living with a disease – by no means always the same things that the doctors think we are concerned about. Communication works two ways.
Doctors are notoriously poor at communication with their patients – they struggle to use language that the person in the street, who possibly has never studied a science subject, is able to relate to. Add to that the fact that when a patient is at an appointment they are probably still in a state of shock at a diagnosis that has come out of the blue which, while not life-threatening, is going to be life-changing and don’t process the words they hear whether it is in plain English or not, and something like “polymyalgia rheumatica” or “giant cell arteritis”– what’s that?
I try to do my best to shed light on the complexities of a patient’s journey and provide them with some basic knowledge about what their illness is. Patients are often scared or overawed by the white coats and the jargon, doctors haven’t time to explain. The result is that a patient is worried about the treatment and the drugs about which they have heard dreadful things and are often unwilling to take them – which means they may go home with a pack of drugs they won’t take. A patient who has some understanding is a patient who can work with their doctor to make the patient journey easier for both sides.
Not everyone can be an expert patient – but everyone can become an expert on their own illness and how it affects them.
Knowledge is power!

10www.pmr-gca-northeast.org.uk
I am very blessed here in Italy – I’d always been somewhat sceptical about “pain management” for chronic pain but was delighted to discover that here they send their anaesthetists off for pain control education. They don’t just hand out ever-increasing quantities and levels of drugs – they seek the cause and endeavour to do something about it.
In my case it was felt the PMR add-ons were primarily due to myofascial pain syndrome causing to the trigger points, the hard knots of muscle fibres identifiable in the middle of particular muscle groups. They in turn were irritating nearby nerves causing referred pain and spasmed muscles, which were adding to the typical PMR problems.
The doctor identified them and then worked on them for a few months using steroid injections and needling as well as manual mobilisation techniques to “break up” those hard knots. I also had some physio although the PMR did make that quite problematical.
Other than the injections I was never offered pain medications – the work was entirely on the cause rather than masking the pain.
I also had a wisdom tooth removed that was causing a bite problem – and since then the MPS is almost a thing of the past – there are twinges but they rarely progress.
Many of us have found that using Bowen therapy has helped a great deal to relieve MPS problems. It is unlikely to help with PMR itself and doesn’t help everyone, but by reducing the pain that comes with MPS or piriformis syndrome it can make the PMR problems easier to live with.
If it will work for YOU then you should see a difference in 3 sessions – the pain may take longer to go altogether and you may need several sessions or to have repeat sessions every few months to keep the improvement but if there is no change after 3, you can probably stop. On the other hand, many of us find there are other benefits with Bowen – it is relaxing and soothing to the spirit as well as the body. And every little helps.
www.pmr-gca-northeast.org.uk/assets/pmr_resource_61.pdf
www.bowen-therapy.co/Bowen/btpa-find-therapist.asp
Eileen Harrison BSc Hons, St Andrews University
❛ Maybe I can’t stop the downpour, but I will always, always join you for a walk in the rain.❜
Above: Eileen’s Mantra
Below: Eileen and Lorna O’Neill (PMR&GCA Scotland) attended the Omeract Conference held in Whistler as Patient Representatives.They were not sure whether the Totem Pole had PMR and/or GCA!
Whistler

11 www.pmr-gca-northeast.org.uk
Both myofascial pain syndrome (MPS) and piriformis syndrome (PS) are often found alongside PMR – I’ve written about it a lot on the forums in the past.
In both cases, they can trap or irritate the sciatic nerve – in some people it passes through the middle of a muscle group and if those muscles are in spasm the nerve is trapped.
Muscle problems – which don’t show on X-rays – are a very common cause of sciatic pain, but doctors are notoriously bad at identifying them. A local orthopaedic specialist I saw after a whiplash injury told me my back pain was due to wear and tear and I’d have to live with it. The pain doctor and the physiotherapist at the hospital saw what the problem was straight away when they examined my back, MPS – they expressed surprise at the doctor’s opinion and were able to solve the problem.
MPS is caused by the same cytokines that cause PMR – except they are often concentrated in trigger points which form hard knots of muscle fibres whereas in PMR they are all through the body or systemic. These trigger points may overlap with the ones they talk about in fibromyalgia but are a bit different – pred works on them! They are found in pairs
on either side of the spine in the shoulder muscles, about rib level and in the lower back, where the baby’s dimples are.
All of them can cause irritation of nerves which run close by – and that can lead to referred pain depending on which nerve it is. The pair in the shoulders can lead to shoulder, neck and upper arm pain. The middle pair may cause pain around the rib area and in the lower back it can lead to buttock and leg pain, into the thighs and as far down as the knees and even ankles. If the muscles in the lower back are affected and in spasm they can lead to sacroiliac pain by tightening the joints in the pelvis and this can irritate the surfaces of the joint. Sacroiliac pain is excruciating and you may be unable to move.
Piriformis syndrome is similar in the symptoms it causes. The piriformis muscle is at the bottom of your buttock, at the top of the back of your thigh, just where you sit on it. In about 20% of people the sciatic nerve passes through the middle of the muscle – and if it is tight, the nerve is pinched and irritated.
Typical symptoms may include tenderness or a dull ache in the buttocks and pain down the back of the thigh, calf and foot (sciatica). Walking up stairs or inclines may cause pain. The range of motion in your hip joint may be restricted and sitting for any length of time, walking or running often make it worse. It may feel better after lying down on your back. The pain can sometimes be mistaken for trochanteric bursitis – another add-on to PMR.
As you can see from the description of the symptoms of both MPS and PS, many of them are very like what you experience in PMR and many patients say that looking back they had noticed them even before the PMR appeared.
Often the higher doses of steroids will also relieve the pain after some time, although it may take a few months. It is quite likely that when you get that first miraculous relief of only some of the pain in PMR it is these that are what is left and seem stubborn.
Doctors who haven’t come across these problems before may just assume that perhaps it isn’t PMR – and in some ways they are correct.
This is a good article about a lot of aspects of MPS: www.mayoclinic.org/diseases-conditions/myofascial-pain-syndrome/basics/definition/con-20033195
Some Add-Ons to PMR: Myofascial Pain Syndrome and Piriformis Syndrome

12www.pmr-gca-northeast.org.uk
Group news from the North EastDates for your Diary
Members can attend meetings at either or both venues, so you could attend eight times a year.
Gateshead meetings 2016
Middlesbrough meeting 2016
forumup MIGRATION
Our forum: pmrandgcaforumup.co.uk
has a new address: pmrandgca.myfunforum.org
This has taken place over the past few weeks as the original server was replaced.
We hope that you will register on the new forum and continue to share information, fun and chat.
We have emailed all the current subscribers and they are taking part in this big migration.
Nearly one thousand people from all over the world are heading to a new link where they will meet up with old friends and make new ones.
Warm winter fleece hats for sale with the pansy logo for sale, ready for
the winter and perhaps as
Christmas presents…?
Add a Pansy Mug and you
get a free gift bag which will
hold both items!!!!
Gentle walkers, Hemlington lake, April 2016.
Pam Hildreth started up the Gentle Walking Group in the Middlesbrough area. Some of the participants are members and some are not.
The whole group decided that they would donate money to our Charity as Pam is a Trustee and Secretary. We thought you should meet the group who have raised and donated £550 to date.
Library, Prince Consort Road 1.30pm start Contact Margaret 0191 252 0627
Monday 26 SeptemberGuest Speaker: Northumberland Blood Bikers.
Marton Country Club. Contact Pam on 01287 623334
Wednesday 28 SeptemberGuest Speaker: TBA

Group news from the North East
Annual Bash in pictures!
Wendy, SRN, at Middlesbrough March meeting.
Treasurer Alan with Joyce who presented
cheque on behalf of Jim Aitkenhead.
The Workers at the Annual Bash.
Top left: Jackie Binding, a patron.
John presenting a cheque to Alan, Treasurer, on behalf of his son Jack who ran GNR Sept 2015.
Gordon and Gina Dyke playing at the Annual Bash.
March Annual Bash – Sing-a-long. Pianist Gordon, who has PMR, Violinist Gina, his wife, who does not have PMR.
13 www.pmr-gca-northeast.org.uk

14www.pmr-gca-northeast.org.uk
PMR-GCA Scotland (Registered Scottish Charity: SCo37780)
We were delighted to be invited to the Annual General Meeting on 19 April 2016.
Margaret Wright, Vice Chair, and Lynne Boyle, Membership Coordinator, travelled to Dundee. They left Newcastle at 6.30am and arrived back home at 10pm.
Guest speakers were Dr Neil Basu, Senior Lecturer of Rheumatology, presented ‘Unravelling Vasculitis related fatigue’ and Dr Vinod Kumar presented ‘GCA, its diagnosis and subsequent treatment’.
It was an excellent day.
Further information on the day and notes from the guest speakers can be found on www.pmrandgca.org.uk/about-pmr-gca-scotland
From left to right: Lynne Boyle; Jean Miller (founder of PMR-GCA) Scotland; Bea Nicholson, Chair; Margaret Wright; and Anne Chambers, Chair PMR-GCA North West.
Well, in between the colds, virus and stomach bugs, I actually managed to get some work done over the last month!!!
One of the highlights for me was attending the PMRGCA Northwest Support Group meeting at The Greyhound hotel. The event, run by Anne Chambers, founder and Chair of the Group, is
aimed at offering support to people who are dealing with conditions Polymyalgia Rheumatica (PMR) or Giant Cell Arthritis (GCA). PMR affects 4 in 10,000 people each year and the symptoms include pain and stiffness in the neck and shoulders. GCA, which is even rarer, causes soreness around the temples, jaw muscle pain and vision loss.
I attended the meeting to share ideas on stress management, in particular how relaxation can be used to not only relieve stress but also reduce physical discomfort.
We were fortunate to be able to conduct a simple relaxation session with many participants quickly achieving a pleasant level of relaxation and comfort.
Ian Guest HPD
News from a PMR GCA North West Support Group Guest Speaker
PMR&GCA UK North East Support
Donations&Gift AidWe wish to thank all the people who have donated monies to us over the past few months. We also wish to thank those taxpayers who filled in Gift Aid forms.
Gift Aid enables us to claim 25p for every £1 donated from HMRC. Once you fill in a Gift Aid form we can claim without you ever having to fill in another form.
Further information on our website: www.pmr-gca-northeast.org.uk

15 www.pmr-gca-northeast.org.uk
From: Symptomatrix Team<[email protected]> – Marijke Foundation
Dear Mavis,I hope and trust you are doing well these days.
Thank you very much for the Christmas Newsletter that just arrived.
A very nice piece of work!
I can only hope that one day a professional and convincing patient organisation like yours is founded in our country.
Considering the core ‘business’ of PMR&GCAUK North East, I was a little bit amazed to find an article about dark cocoa.
Very informative, though I knew about it from scientific articles in the seventies of the past century. At that time it was also published that the combination of dark chocolate / cocoa and red wine (!!) is very healthy for the brain and the brain functions (though I believe that a piece of dark chocolate and only one glass of wine will do the trick…; anyway, the combination is awful, I tried it once).
From our end there’s not really much to report.
The Symptomatrix is more frequently used worldwide than before. Its success keeps up with the increasing use of the Internet, in particular by people aged 45 years and over. Also the Symptomatrix seems to be accepted more and more in medical circles around the world.
What is remarkable is that we increasingly receive Symptomatrix forms from men, and moreover that in particular GCA increasingly hits younger women (in some cases even at the age of 27).
Furthermore, our statistics show that a combination of stress and severe flu seem to trigger both GCA and PMR.
Warm regards,
HanSecretary
Letter from the Netherlands
You are not aloneYou are not alonePolymyalgia Rheumatica and Giant Cell ArteritisNewsletter Winter 2015
Registered Charity No: 1138409

ATD At The Door
BFF Best Friend Fell
BTW Bring The Wheelchair
BYOT Bring Your Own Teeth
FWIW Forget Where I Was
GGPBL Gotta Go Pacemaker Battery Low
GHA Got Heartburn Again
LMDO Laughing My Denture Out
OMMR On My Massage Recliner
OMSG Oh My! Sorry, Gas
ROFLACGU Rolling On Floor Laughing And Can’t Get Up
TTYL Talk To You Louder
16www.pmr-gca-northeast.org.uk
Limericks!
A flea and a fly in a flu,
were imprisoned, so what could they do?
Said the fly, “Let us flee!”
“Let us fly, “said the flea,
and they flew through a flaw in the flue!
A young gourmet dining at Crewe
found a rather large mouse in his stew.
Said the waiter “Don’t shout
and wave it about,
Or the rest will be wanting one too”!
There was a young man from Devizes
Whose ears were two different sizes
The first was so small, it was no use at all
But the other won hundreds of prizes!
Supplied by Shirley Surrey Support Group.
Please get in touch: PMR&GCA UK North EastTel: 0191 411 1138Email: [email protected]
Want to join?
Need help?
Supported byPermission to reproduce contents, please email: [email protected]
Published by PMR&GCA UK North East SupportRegistered Charity No: 1138409
Designed by GDA (www.gda-design.co.uk) Printed by Statex Colour Print.
Senior Citizen Texting Codes