Embed Size (px)
Citation preview

Grapefruit juice alters terfenadine pharmacokinetics, resulting in prolongation of repolarization on the electrocardiogram
Objectives: To establish whether the pharmacokinetics and electrocardiographic pharmacodynamics of terfenadine are affected by concomitant administration of grapefruit juice and to determine whether any effect of grapefruit juice is dependent on the timing of administration in relation to the dose of terfenadine. Methods: Twelve healthy volunteers were studied in a prospective randomized trial. The primary end points were QT prolongation on the surface electrocardiogram and the pharmacokinetic parameters: area under the concentration-time curve (AUC), maximum concentration, and time to maximum concentration of terfenadine and its acid metabolite terfenadine carboxylate. All subjects received 60 mg terfenadine twice a day with 240 ml water for 7 days. They were then randomized to drink 240 ml of double-strength grapefruit juice simultaneously with terfenadine (simultaneous group) for an additional 7 days or to drink the same dose of grapefruit juice 2 hours after terfenadine for 7 days (delayed group). Twelve timed electrocardiograms and plasma terfenadine and metabolite levels were measured on days 7 and 14. Results: None of the 12 subjects had quantifiable levels of terfenadine when the drug was administered with water. All six subjects who took terfenadine and drank grapefruit juice simultaneously had quanti- fiable terfenadine levels. Only two of six who drank grapefruit juice 2 hours after terfenadine had quantifiable levels. The AUC of the acid metabolite increased 55% (p < 0.05) in the simultaneous group and 22% (p = NS) in the delayed group. The mean QT interval increased from 420 to 434 msec (p < 0.05) in the simultaneous group and decreased from 408 to 407 msec (p = NS) in the delayed group. Conchssions: Administration of grapefruit juice concomitantly with terfenadine may lead to an increase in systemic terfenadine bioavailability and result in increases in QT interval. The clinical significance of an increase in QT interval of this magnitude is unclear. ( CLIN PHARMA COL THER 1996;59:383-8.)
Robert E. Benton, MD, Peter K Honig, MD, MPH, Kaveb Zamani, PhD, Louis R. Cantilena, MD, PhD, and Raymond L. Woosley, MD, PhD Washington, D. C., and Bethesda, Md.
From the Division of Clinical Pharmacology, Department of Inter- nal Medicine, Georgetown University Medical Center, Washing- ton, and the Division of Clinical Pharmacology of the Uniformed Services University of the Health Sciences, Bethesda.
Supported in part by Clinical Pharmacology Training grant T32- GM08386 from the National Institutes of Health, Bethesda, Md.
Presented in part at the annual meeting of the American Society for Clinical Pharmacology and Therapeutics, New Orleans, Louisiana, March 30-April 1, 1994.
The views expressed in this article are those of the authors and do not reflect the official policy of the Uniformed Services Uni- versity or the Department of Defense.
Received for publication June 26, 1995; accepted Oct. 17, 1995.
Reprint requests: Raymond L. Woosley, MD, PhD, Depart- ment of Pharmacology, Georgetown University College of Medicine, 3900 Reservoir Road, NW, Washington, DC 20007.
1311169994
Terfenadine is a second-generation selective Hi - receptor antagonist that has less central nervous system side effects than first-generation agents.’ It is rapidly and almost completely biotransformed by cytochrome P4503A4 (CYP3A4) into at least one metabolite that has antihistaminic properties.2 Un- changed terfenadine is usually undetectable in the plasma of patients who are taking recommended doses of the drug, unless they have liver disease or are taking other drugs that inhibit cytochrome P4503A4 activity.3 The cardiotoxic effect of terfena- dine when given concomitantly with drugs such as ketoconazole or erythromycin are well described.4 The parent compound of terfenadine has been shown to be a potent blocker of the delayed rectifier potassium current in feline ventricular myocytes.” Block of this channel in patients with elevated ter-
383

384 Benton et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
APIUL 1996
fenadine levels is the proposed mechanism for re- polarization abnormalities, which predisposes them to the development of torsades de pointes ventric- ular tachycardia.’
A novel food-drug interaction has been reported that involves the concomitant administration of grapefruit juice with highly cleared substrates of P4503A4 such as felodipine, nifedipine, nitrendi- pine, nisoldipine, and cyclosporine.6-9 It is presumed that a constituent of grapefruit juice inhibits the first-pass metabolism of these compounds. Candi- date substances are the bioflavonoids naringenin and quercetin, which in vitro have been shown to potently inhibit oxidation of nifedipine and felodi- pine.10s” Because naringenin or quercetin solutions did not have as potent an effect on dihydropyridine biotransformation as grapefruit juice that contained equivalent quantities of the bioflavonoids, other constituents of grapefruit juice may contribute to the effect in viva.”
Because the biotransformation of terfenadine is similar to that of the dihydropyridine calcium chan- nel blockers, we hypothesized there may be a rele- vant interaction between grapefruit juice and ter- fenadine that may result in accumulation of the parent compound and alterations in cardiac repo- larization.13 This study was conducted to determine whether systemic bioavailability of terfenadine is enhanced by grapefruit juice and whether the timing of administration of grapefruit juice relative to ter- fenadine is a factor in this interaction.
METHODS Study protocol. The study was a randomized par-
allel design in which all 12 subjects received the recommended dose of terfenadine (60 mg by mouth every 12 hours) at 8 AM and 8 PM for 6 days as outpatients. On day 6, the 8 PM dose was wit- nessed by the investigators to ensure correct tim- ing with regard to subsequent blood sampling. On day 7 the subjects reported to the Clinical Re- search Center at 7 AM after an overnight fast. An indwelling sterile catheter was inserted into a forearm vein of each subject to facilitate repeated blood sampling. Blood was collected with ethyl- enediaminetetraacetic acid as an anticoagulant. A predose blood sample was drawn and a 12-lead electrocardiogram (ECG) and simultaneous rhythm strip in orthogonal leads I, V2, and aV, was performed (25 and 50 mmisec paper speed). ECGs were performed with use of a MacVu ECG machine (Marquette Electronics, Milwaukee,
Wis.). The 8 AM dose of terfenadine was adminis- tered and blood samples were drawn at 1/2, 1, 2, 3, 4, 6, 8, 10, and 12 hours after administration. A standardized lunch was served 4 hours after ad- ministration. All subjects continued to take 60 mg terfenadine by mouth at 8 AM and 8 PM for another 7 days. Subjects were then randomized into two groups by means of a coin flip in blocks of 2. The subjects in the simultaneous group drank 240 ml grapefruit juice concomitantly with each terfena- dine dose, whereas the subjects in the delayed group drank grapefruit juice 2 hours after they took terfenadine. The grapefruit juice was pre- pared daily by diluting frozen concentrate (Giant Brand, Baltimore, Md.) 1: 1 with an equal volume of water. On study days 8 through 13 the subjects reported to the Clinical Research Center to re- ceive their 8 AM doses of terfenadine and grape- fruit juice and to have a predose ECG performed for safety reasons. On day 13 the 8 PM doses were again witnessed. On day 14 repeat pharmacoki- netic profiles and ECGs were performed except that the subjects in the simultaneous group re- ceived 240 ml grapefruit juice with terfenadine at 8 AM, whereas subjects in the delayed group drank grapefruit juice at 10 AM. The simultaneous group subjects drank 240 ml water at 10 AM, whereas the delayed group subjects drank 240 ml water with terfenadine at 8 AM.
Study site. This study was conducted at the Clinical Research Center of the Georgetown University Hospital (Washington, D.C.). Determination of plasma terfenadine and metabolite concentrations were performed at the Division of Clinical Pharma- cology, Uniformed Services University of the Health Sciences (Bethesda, Md.). Approval to conduct this study was obtained from the Institutional Review Board of Georgetown University.
Study population. Healthy volunteers between the ages of 21 and 65 years were eligible for this study. Twelve subjects (nine men and three women; age range, 22 to 33 years) were enrolled. The subjects showed normal physical findings, serum chemistries, complete blood counts, urine analyses, serum mag- nesium and calcium levels, and baseline resting ECG measurements (25 and 50 mmisec paper speed). All subjects were nonsmokers, and one sub- ject was African-American. They were asked to re- frain from ingesting alcohol- and caffeine-containing beverages and citrus products during the period of the study. Two of the three women (subjects 2 and 3) were taking oral contraceptives but followed the

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME SY. iWMRER4
same regimen throughout the 2-week period of the study. Subjects were prohibited from taking any other prescription or nonprescription drug product during the course of the study. A negative chorionic gonadotropin pregnancy test was required for all female subjects.
Terfenadine and acid metabolite assays. Plasma was separated from blood cells by centrifugation at 1000 G within 30 minutes of phlebotomy and stored fro- zen at -70” C. Solid-phase extraction was used to prepare the samples for quantification by automated HPLC with florescence detection. l4 The lower limit of quantification of the acid metabolite was 50 ngi ml. The lower limit of quantification was 5 rig/ml for terfenadine. The coefficients of variation were 4.9% for terfenadine and 9.8% for the acid metabolite at the lowest control point on the respective standard curves.
Analysis of ECG intervals. The ECG tracings were performed by the same individuals during the study to maintain uniformity of technique. All identifying information was removed, and the tracings were coded and randomized. QT interval determination and TU wave morphology was assessed blindly by one of the investigators (R.E.B.). Cycle length (RR interval) and QT interval were determined for each time point. The QT interval measurement was based on the method of Sale et a1.15 QT and RR interval determinations were performed using an Summa- sketch II electronic digitizing pad (Summagraphics, Seymour, Conn.). The QT interval was measured with use of orthogonal leads I, V,, and aV, by determination of the earliest onset of the QRS com- plex and latest return to baseline for 3 to 5 consec- utive complexes. Each rate-corrected QT interval (QT,) was calculated with use of the previous RR interval and Bazett’s formula.16 The mean of the 3 to 5 QT, intervals was used for each time point.
Pharmacokinetic analysis. The following parame- ters were determined from analysis of the data gen- erated by the sequential lo-point pharmacokinetic profiles of each subject: maximum concentration (C,,,), time to reach C,,, (tm,.J, and the area under the concentration-time curve (AUC). The trapezoi- dal rule was used to calculate the AUC to the last recorded time point in each profile.17 The elimina- tion rate constant (k,) for each subject during each phase of the study was calculated by regression of the terminal portion of the log-linear concentration- time curve.
Statistical analysis. Because a normal distribution of data could not be assumed or demonstrated, nonpara-
Benton et al. 385
Table I. Subject demographics Subject Age Weight He&h t
No. (yr) Gender Race (kg) (cm)
Simultaneous group * 1 30 Male White 82 185 2 30 Female White 51 163 3 34 Female White 61 172 4 22 Male Black 74 172 5 31 Male White 78 193 6 30 Male White 98 183
Mean ? SD 30 ? 4 74 2 16 178 t 11
Delayed group 7 7 27 Female White 5.5 161 8 25 Male White 67 172 9 33 Male White 70 167
10 26 Male White 82 167 11 25 Male White 107 183 12 30 Male White 88 183
Mean i- SD 28 5 3 78 ? 18 172 ? 9
“Grapefruit juice administered concomitantly with terfenadine iGrapefruit juice administered 2 hours after terfenadine.
metric statistical analysis (Wilcoxon signed-rank test) was used to compare the pharmacokinetic parameters. The mean QT, intervals while subjects were taking terfenadine alone and while they were taking terfena- dine with grapefruit juice were also compared with use of the Wilcoxon signed-rank test. Two-tailed hypoth- esis testing was used to calculate allp values.
RESULTS Subject demographics. Table I shows the charac-
teristics of the subjects in each group. No subjects were excluded during the screening and enrollment process. The mean ages and mean weights for the two groups were approximately equal. All subjects completed all phases of the study.
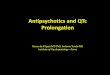
Pharmacokinetics. Fig. 1 shows the mean metabo- lite concentrations over the dosing interval for each of the two groups at steady state while subjects took terfenadine alone and while they took terfenadine with grapefruit juice (error bars are SEM, n = 6). Table II shows the C,,, of terfenadine and the AUC, Cmax, and t,, of the acid metabolite while subjects took terfenadine alone and after the addi- tion of grapefruit juice to the regimen. Terfenadine was unquantifiable in all subjects in both groups while the subjects took terfenadine alone at any time point; however, all six subjects in the simultaneous group had quantifiable levels after the addition of grapefruit juice at one or more time points. In the delayed group only two of six subjects had quantifi-

386 Benton et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
APRIL 1996
B Terfenadine + grapefruit juice
A 400 1 A Terfenadine + water
0 2 4 6 a
H Terfenadine + grapefruit juice
A 475
1 A Terfenadine + water
, I I I I 0 2 4 6 6 10 12
Time after dose (hours)
Fig. 1. Mean metabolite concentrations at indicated times after terfenadine administration. A, Simultaneous group: Grapefruit juice administered concomitantly with terfenadine. B, Delayed group: Grapefruit juice adminis- tered 2 hours after terfenadine.
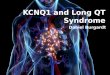
able concentrations while they were taking terfenadine Pharmacodyruzmics. There was no difference be- with grapefruit juice at one or more time points. Table tween the two groups in baseline screening QT, inter- II also contains the pharmacokinetic results for the vals (simultaneous group, 405 2 14 msec; delayed carboxylate metabolite. In the simultaneous group the group, 417 -+ 14 msec;p = NS). Fig. 2 shows the QT, metabolite AUC increased 55% (range, +26% to interval over the dosing interval for each of the two +112%, p < 0.05) after the addition of grapefruit groups at steady state while the subjects were taking juice, whereas in the delayed group the AUC in- terfenadine alone and with grapefruit juice (error bars creased only 22% (range, +11% to +88%,p = NS). are SEM; rz = 6). In the simultaneous group the mean In the simultaneous group, the metabolite t,, in- QT, is greater at every time point over the dosing creased from 2.8 t- 1.1 to 5.1 ? 1.1 hours (p < 0.05), interval. In the delayed group there was no significant and in the delayed group the t,, increased from 2.3 +- difference in QT, between terfenadine alone and 1.0 to 3.5 f 1.4 hours @ = NS). C,, did not increase grapefruit juice added to terfenadine. The results of significantly in either group. There was no significant the QT measurements are shown in Table II. In the difference in k, before and during the grapefruit juice simultaneous group the mean QT, increased signifi- phase of the study for either group. cantly: from 420 to 434 msec after the addition of
0 I I I I 8 I , 0 2 4 6 a 10 12
Time after dose (hours1
Fig. 2. Mean corrected QT interval (QT,) at indicated times after terfenadine administration. A, Simultaneous group: Grapefruit juice administered concomitantly with terfenadine. B, Delayed group: Grapefruit juice adminis- tered 2 hours after terfenadine.

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 59, NUMBER 4 Benton et al. 387
Table II. Pharmacokinetic and pharmacodynamic results
Terfeadine Metabolite Metabolite Metabolite Metabolite Mean C mar AUC t c max QTc
(ngiml) (ng * hrlml) $7 h&4 (h?‘) (~4 Subject
No. T+W T+GJ T+W T+GJ T-?-W T+GJ T+W T+GJ T+W T+GJ T+W T+GJ
Simultaneous group t 1 NQ 10 810 1160 1 4 145 163 0.26 0.16 406 426 2 NQ 5 1150 2440 3 4 419 368 0.20 0.19 439 450 3 NQ 11 1120 1570 4 6 172 198 0.13 0.17 412 451 4 NQ 6 370 510 4 4 51 73 0.30 0.18 410 411 5 NQ 5 920 1420 2 6 131 163 0.14 0.11 416 436 6 NQ 5 1180 1480 3 6 171 177 0.18 0.12 436 429
Mea&SD 7.Ok2.7 930+310 1430’-630* 2.821.1 5.0+1.1* 182’124 190?97 0.19~0.0 0.15+0.03 420214 434%15*
Delayed group $ 7 NQ 10 1220 2290 2 3 223 321 0.27 0.17 412 409 8 NQ NQ 2350 3122 1 2 608 484 0.20 0.17 436 441 9 NQ 6 2440 2360 4 3 333 351 0.13 0.12 399 393
10 NQ NQ 460 660 2 6 152 119 0.16 0.33 384 386 11 NQ NQ 1340 1660 2 4 184 216 0.17 0.15 401 388 12 NQ NQ 1660 1470 3 3 246 223 0.17 0.17 418 425
Mean-CSD 1580t750 1930?850 2.321.0 3.521.4 2912167 286~128 0X3+-0.05 0.19+0.07 408218 407222
C,,,, Maximum concentration; AUC, area under the concentration-time curve; t,,,, time to reach C,,,; k,, elimination rate constant; QT,, rate-corrected QT intenral; T, terfenadine; W, water; GJ, grapefruit juice; NQ, not quantifiable.
*p < 0.05 grapefruit juice versus water. tGrapefruit juice administered concomitantly with terfenadine. $Grapefruit juice administered 2 hours after terfenadine.
grapefruit juice to terfenadine (p < 0.05). In the de- layed group the mean QT, decreased from 408 to 407 (p = NS) There were no changes in T wave morphol- ogy in either group.
DISCUSSION In this study we demonstrate that concomitant
administration of grapefruit juice with terfenadine during steady-state conditions results in the accumu- lation of quantifiable terfenadine in some subjects. This pharmacokinetic interaction was accompanied by an increase in the QT, interval on the ECG. This raises the possibility that the coadministration of grapefruit juice with terfenadine may lead to accu- mulation of terfenadine and be a clinically relevant factor for potential cardiotoxicity.
ylate appears to be unchanged in both groups, which is consistent with the results of Rau et a1.i8 The implica- tions of these results are best viewed in the light of experience with other P4503A4 substrates. Ducharme et a1.19 showed that grapefruit juice had no effect on the metabolism of intravenous cyclosporine, but it in- creased the bioavailability of oral cyclosporine by 62%. The findings of our study with terfenadine appear to support the hypothesis that drug-grapefruit juice in- teractions are prehepatic and mechanistically based on inhibition of gut wall P4503A enzymes. The milder effect of grapefruit juice in the delayed group is prob- ably attributable to the rapid absorption of terfena- dine. Most of the prehepatic metabolism of the parent compound has occurred before the delayed dose of grapefruit juice reaches the small bowel.
The effect of grapefruit juice on terfenadine phar- The concentration-effect relationship between macokinetics appeared to be more pronounced when terfenadine plasma concentration and QT prolon- grapefruit juice and terfenadine were administered gation has not been systematically studied in the concomitantly, compared with a 2-hour delay in grape- absence of cytochrome P450 inhibitors. Although fruit administration. It is noteworthy that after admin- Honig et al.” observed a linear relationship be- istration of grapefruit juice, terfenadine was quantifi- tween terfenadine concentration and change in QT able in six of six subjects in the simultaneous group and interval, the effect was extremely variable at low in two of six subjects in the delayed group. Further- concentrations from 5 to 20 r&ml, such as those more, the terminal elimination of terfenadine carbox- seen in our study. It is doubtful that grapefruit juice

388 Beuton et al. CLINICALPHARMACOLOGY&THERAPEUTIcS
APRIL1996
alone caused any prolongation of QT interval or caused electrolyte abnormalities that would lead to such changes because there were no significant ECG changes observed in the delayed group.
In conclusion, concomitant administration of grapefruit juice increased the bioavailability of ter- fenadine and its acid metabolite. In subjects who had increased terfenadine concentrations, there was a statistically significant increase in the QT, interval. Although the magnitude of this QT interval differ- ence may not be large, given the high interindividual variability in cytochrome P4503A4 activity, there may be patients in whom grapefruit juice would cause elevated terfenadine levels and lead to devel- opment of arrhythmias. Clinicians should be aware of the potential for this interaction to occur and discourage patients from taking terfenadine with grapefruit juice.
References 1. Simons FE, Simons KJ. The pharmacology and use of
H,-receptor-antagonist drugs. N Engl J Med 1994: 330: 1663-70.
2. McTavish D, Goa KL, Ferrill M. Terfenadine: an updated review of its pharmacologic properties and therapeutic efficacy. Drugs 1990;39:552-74.
3. Kivisto KT, Pertti JN, Klotz U. Inhibition of terfenadine metabolism: pharmacokinetic and pharmacodynamic consequences. Clin Pharmacokinet 1994;27:1-5.
4. Monahan BP, Ferguson CL, Killeavy ES, Lloyd BK, Troy J, Cantilena LR Jr. Torsades de pointes occur- ring in association with terfenadine use. JAMA 1990; 264:2788-90.
5. Woosley RL, Chen Y, Freiman JP, Gillis RA. Mech- anism of the cardiotoxic actions of terfenadine. JAMA 1993;269:1532-6.
6. Bailey DG, Spence JD, Munoz C, Arnold JMO. In- teraction of citrus juices with felodipine and nifedi- pine. Lancet 1991;337:268-9.
7. Soons P, Vogels B, Roosemalen N, et al. Grapefruit juice and cimetidine inhibit stereoselective metabo- lism of nitrendipine in humans. CLIN PHARMACOL THER 1991;50:394-403.
8. Bailey DG, Arnold MO, Strong A, Munoz C, Spence JD. Effects of grapefruit juice and naringin on nisoldi- pine pharmacokinetics. CLIN PHARMACOL THER 1993;54: 589-94.
9. Ducharme MP, Provenzano R, Dehoorne-Smith M, Edwards DJ. Trough concentrations of cyclosporin in blood following administration with grapefruit juice. Br J Clin Pharmacol 1993;36:457-9.
10. Miniscalco A, Lunhahl J, Regardh CG, Edgar B, Eriksson UG. Inhibition of dihydropyridine metab- olism in rat and human liver microsomes by fla- vonoids found in grapefruit juice. J Pharmacol Exp Ther 1992;261:1195-9.
11. Guengerich FP, Kim DH. In vitro inhibition of dihy- dropyridine oxidation and aflatoxin B, activation in human liver microsomes by naringenin and other fla- vonoids. Carcinogenesis 1990;11:2275-9.
12. Bailey DG, Arnold MO, Munoz C, Spence JD. Grapefruit juice-felodipine interaction: mechanism, predictability, and effect of naringin. CLIN PHARMACOL
THER 1993;53:637-42. 13. Yun CH, Okerholm RA, Guengerich FP. Oxidation
of the antihistaminic drug terfenadine in human liver microsomes. Drug Metab Dispos 1993;21: 403-9.
14. Coutant JE, Westmark PA, Nardella PA, Walter SM, Okerholm RA. Determination of terfenadine and terfe- nadine acid metabolite in plasma using solid-phase ex- traction and high-performance liquid chromatography with florescence detection. J Chromatogr 1991;570:139- 48.
15. Sale ME, Barbey TJ, Woosley RL, et al. The electro- cardiographic effects of cetirizine in normal subjects. CLIN PHARMACOL THER 1994;56:295-301.
16. Bazett HC. Analysis of the times relations of electro- cardiograms. Heart 1920;7:353-70.
17. Gibaldi M. Biopharmaceutics and clinical pharmaco- kinetics. Philadelphia: Lea & Febiger, 1984.
18. Rau E, Bailey DG, Tran LT, Spence JD, Bend JR. Inhibition of terfenadine metabolism by co- administration of grapefruit juice in humans. In: Bell- ward GD, ed. Abstract book of the Tenth International Symposium on Microsomes and Drug Oxidations. To- ronto, Ontario, 1994:310.
19. Ducharme MP, Warbasse LH, Edwards DJ. Disposi- tion of intravenous and oral cyclosporine after admin- istration with grapefruit juice. CLIN PHARMACOL THER 1995;57:485-91.
20. Honig PK, Wortham DC, Zamani K, Conner DP, Mullin JC, Cantilena LR. Terfenadine-ketoconazole interaction: pharmacokinetic and electrocardio- graphic consequences. JAMA 1993;269:1513-8.


























![[Product Monograph Template - Standard] · erythromycin are co-administered with astemizole, cisapride, pimozide, or terfenadine resulting in cardiac arrhythmias (QT prolongation,](https://img.pdfslide.us/doc/110x75/5e16473e2fdf7450c26f66d7/product-monograph-template-standard-erythromycin-are-co-administered-with-astemizole.jpg)