Embed Size (px)
Citation preview

( … B U T I S I T R E A L LY B E N I G N ? )
BENIGN EARLY REPOLARIZATION

WHO GETS IT?
• 2-5% of the general population (Wellens, 2008)• Usually the young and physically fit• Generally disappears with advancing age
• Don’t forget clinical context, a 45yr old with <2mm STE in a BER morphology w/o sxs concerning for ACS can still be BER

WHAT IS IT?
• The truth of the matter is…we aren’t too sure!• Nerdy answer: • Experimental data shows pts with BER to have
heterogeneous repolarization physiology with myocytes containing a larger concentration of transient outward current, inducing a voltage gradient during the ST segment (Kusumoto, Cardiovascular Pathophysiology, 2006)
• What to tell your patient:• This is a normal, benign variation that we see in a lot of
patients that has no clinical significance

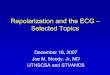
WHAT DOES IT LOOK LIKE?
Red arrows: concave up ST-segment elevation anteriorly Blue arrows: hyperdynamic, symmetrical, concordant T-waves

CLASSIC FINDINGS
1. J-point “notching”
2. Concave-up ST segment (smiley face)
3. ST segment elevation from baseline in V2-V5, typically <3mm
4. Large, symmetrically concordant T-waves in leads with STE

CAN WE TEASE IT OUT?
• The degree of ST segment elevation is thought to be indirectly proportional to the degree of sympathetic tone
• In other words, the more relaxed the patient, the more pronounced the ST segment elevation (and vice versa)
• If you truly want to test your patient, get their heart rate up and look at the ST segment

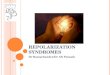
14yo M w/ palpitations
HR: 64

1. Notched J-point
2. Concave down ST elevation in precordial leads

Same patient after asking him to do 2min of jumping jacks in the room to try and get his heart rate up…
HR 83 (up 20bpm from previous)

HR 64 HR 83
The ST segment is NOT fixed in pts w/ BER and changes from EKG to EKG and with the degree of sympathetic strain
On the right, note the complete resolution of the ST elevation but maintenance of the J-point notching in V4

TO BER, OR NOT TO BER…THAT IS THE QUESTION!
• New studies are suggesting BER is not always so benign…• http://www.nejm.org/doi/full/10.1056/NEJMoa071968#t= article• http://www.nejm.org/doi/full/10.1056/ NEJMoa0907589
• But before you go working up every case of BER because of these papers, know this…• These are far from conclusive papers! • One is a retrospective review of 206 patients after an episode
of VF (Haissaguerre, et al)• The other suggests repolarization in the inferior leads in middle
aged people was associated with increased risk of cardiac death in the long-term, with only a relative risk of <3! (Tikkanen, et al)

IN CONCLUSION
• BER should be a diagnosis of exclusion and should ALWAYS be placed in clinical context!!!
• The above was taken in a patient with difficulty breathing and chest pain…and is an AMI, NOT BER!!!• Note the hyperacute T-waves (disproportionately larger than
the QRS complex, developing q-waves, and lack of J-point notching)