Embed Size (px)
Citation preview

LEADERSHIP, MANAGEMENT & GOVERNANCE PROJECTInspired Leadership. Sound Management. Transparent Governance.
LEADERSHIP, MANAGEMENT & GOVERNANCE PROJECTInspired Leadership. Sound Management. Transparent Governance.
Inspired leadership, sound management, transparent governance
Governing for Better Health 2012 Survey
March 2012Prepared by the USAID Leadership, Management, and Governance Project
Tech
nica
l Brie
f

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 2
About the Leadership, Management, and Governance
Project (LMG)As the U.S. government enters a new era in international development through initiatives such as the Global Health Initiative and PEPFAR II, there is a strong emphasis on sustainability and country ownership within the health system strengthening framework. Development practitioners increasingly agree that improving the leadership, management and governance capacity of policy makers, health care providers, and program managers allows them to better implement quality health services, and meet local citizens’ health needs. Funded by USAID, the Leadership, Management and Governance Project (2011-2016) collaborates with health leaders at all levels to improve leadership, management and governance practices to create stronger health systems and improve health for all, including vul-nerable populations worldwide.
The LMG Project seeks to do the following:
■ Promote enhanced performance improvement processes driven by country leadership for individuals and teams through South-to-South dialogue and collaborative learning modules designed to increase organizational capacity
■ Develop senior leadership and governance capabilities using participatory processes and gender-aware approaches that enable health leaders and policy-makers to address their own challenges, and achieve results
■ Build and use evidence-based approaches by generating and disseminating evidence that shows how improved leadership, management, and governance contribute to health gains
Cover photo credit: A nurse and health leader in Bamyan Province, Afghanistan. Photo contributed by Management Sciences for Health
Management Sciences for Health784 Memorial DriveCambridge MA 02139
Suggested citation: Shukla, M., and Johnson Lassner, K. Governing for Better Health: 2012 Survey. Prepared for the U.S. Agency for International Development (USAID) by the USAID Leadership, Management and Governance Project. Arlington, VA: Management Sciences for Health, 2012.

3 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
AcknowledgmentsThis report was prepared for the United States Agency for International Development (USAID) by the Leadership, Management, and Governance (LMG) project. The LMG project team thanks the staff of the USAID Global Health Bureau, Office of Population and Reproductive Health for their generous support and technical guidance—in particular, Brenda Doe, the LMG project’s Agreement Officer’s Representative (AOR), for her constant encouragement and support.
Mahesh Shukla, MD, MPA, and Karen Johnson Lassner, MPH, MA, are the authors of this study. James A. Rice, PhD, reviewed the report, and Laura Lartigue, MIS, MA, edited the report. The authors wish to thank colleagues within the LMG project, as well as many staff members within the broader Management Sciences for Health (MSH) family- without their support the study and the report would not have been possible. Credit is also due to LMG partners: African Medical and Re-search Foundation (AMREF), International Planned Parenthood Federation (IPPF), Johns Hopkins University (JHU), MedicMobile, and the Yale Global Health Institute (GHLI) for their contributions at several stages of the study. Additionally, the authors appreciate the time and efforts of Dr. Sameen Siddiqi, MD, FCPS, MSc, Dr. Med, FFPH, Director of the Division of Health Systems and Services Development within the Eastern Mediterranean Regional Office of the World Health Organization in Cairo, Egypt, who reviewed the instruments and the final report as an external reviewer.
Finally, the LMG Project team thanks the 477 leaders, managers, and those who govern in the health sector and within health institutions in low- and middle-income countries, all of whom spent sub-stantial time in taking the 2012 survey that constitutes the foundation of this report. We wish them success in their efforts toward strengthening health systems in their respective countries, regions, and jurisdictions, and we hope that this report will be useful to them as well as to others charged with car-rying out similar responsibilities in resource-scarce and difficult-to-govern environments.

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 4
ContentsExecutive Summary ..................................................................................................................... 7
Introduction ................................................................................................................................ 9
Approach and Methods ............................................................................................................. 10
Research Questions ................................................................................................................... 11
Results ....................................................................................................................................... 11
Discussion ................................................................................................................................. 18
Limitations ................................................................................................................................ 20
Conclusion ................................................................................................................................ 21
Policy Implications .................................................................................................................... 23
AppendicesAppendix A: Charts and Tables ................................................................................................. 24
Appendix B: Subgroup Analysis ................................................................................................ 45
Appendix C: The Survey Instrument ......................................................................................... 52

5 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
List of FiguresFigure I: How Leadership, Management and Governance inter-relate and interact within a health system ....................................................................................................................................... 19
Figure II: Overlap between leading, governing and managing roles ........................................... 20
Figure 1: Sectors in which the respondents predominantly work ............................................... 25
Figure 2: Levels at which of the respondents work ..................................................................... 25
Figure 3: Foci of work of the respondents .................................................................................. 26
Figure 4: Whether the respondents govern, observe others govern, manage and lead ................. 26
Figure 5: Defining governing in practical terms ......................................................................... 27
Figure 6: Enablers of effective governance and their link to the improvements in the health service and health ................................................................................................................................. 28
Figure 7: Deterrents of effective governance .............................................................................. 29
Figure 8: Defining effective governance in the context of overall health ..................................... 30
Figure 9: Perception of the respondents on the linkage of effective governance in health sector with the quality of health service ............................................................................................... 30
Figure 10: Perception of the respondents on the linkage of effective governance in health sector with health gain by individuals and populations ........................................................................ 31
Figure 11: Perception of the respondents on the linkage of effective governance in sectors other than the health sector to the better health of individuals and populations .................................. 32
Figure 12: Perception of the respondents on the interaction of leadership, management, and gov-ernance ...................................................................................................................................... 33
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 6
List of TablesTable F (4) (i): Leadership, management and governance roles .................................................. 27
Table F (4) (ii): Overlap between leading, governing and managing at a practical level .............. 27
Table 1: Regions and countries represented (Number of respondents, country-wise) ................. 34
Table 2: Sector of workTable 3: Level of work ........................................................................... 35
Table 4: Focus of Work.............................................................................................................. 37
Table 5A: Defining governing in practical terms ........................................................................ 40
Table 5B: Defining ‘to include’ in practical terms ...................................................................... 41
Table 6: Enablers of effective governance ................................................................................... 42
Table 7: Deterrents of effective governance ................................................................................ 43
Table 8: Linkgae of effective governance in health sector with the health system outcomes ........ 44
Table 9: Wilcoxon Scores for variables classified by level of work .............................................. 47
Table 10: Wilcoxon Scores for variables classified by place of work (non-OECD countries versus OECD countries) ..................................................................................................................... 48
Table 11: Wilcoxon Scores for variables classified by geographical region (Asia, Africa, and Latin America and Caribbean) ........................................................................................................... 49
Table 12: Wilcoxon Scores for variables classified by the respondents who govern vs. respondents who manage but not govern ..................................................................................................... 50
Table 13: Wilcoxon Scores for variables classified by the respondents who govern vs. respondents who lead but not govern ............................................................................................................ 51
7 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Executive SummaryThis study, second of its kind to our knowledge, on governance in the sector of health in low- and middle-income countries, carried out in February-March 2012 by the USAID-funded Leadership, Management and Governance (LMG) project, surveyed 477 health leaders, managers, and those who govern in the health sector in 80 low- and middle-income countries to identify perceptions and opinions of the respondents on practices, impediments, and enablers of effective governance for health. These health practitioners were also asked about the outcomes of effective governance for health as well as their ideas concerning the relationship between leadership, management and governance in health.
Key findings from the survey included the following:
1. Respondents defined effective governance in the health sector in terms of improvements in both the health services and the health of individuals and populations.
2. Respondents identified both impediments and facilitators of effective governance.
3. Many respondents (more women than men) saw a clear link between governance in sectors other than health as having an effect upon the health of individuals and populations.
4. Respondents saw leadership, management, and governance as highly inter-related and mutually reinforcing constructs in the context of health.
5. Effective leadership was perceived by respondents as a prerequisite not only for effective governance but also effective management.
Leadership is largely viewed by respondents as being one of the most important enablers of effec-tive governance and management in health, and ineffective leadership the biggest impediment. Since many people lead while governing and managing on day-to-day basis, the findings support the idea that training and consulting support that is designed to strengthen governance practices should consider how leadership can enhance governing activities and management roles. It appears the effective integration and application of all three roles—leading, managing and governing—has a positive influence on the other building blocks of a health system (i.e., information, human resources, medicines, vaccines and technologies, financing and service delivery), enabling it to produce desired health outcomes.
In addition, a clear set of governing practices was defined for leaders who govern, who are said to do the following:

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 8
■ Include the governed in governing by communicating and engaging with them, engender trust, allow representation, provide information, promote dialogue, establish systematic feedback mechanisms, respond to the feedback, and resolve conflicts;
■ Collaborate across levels (local, state, national, and global) and across sectors (across public, private, and civil society sectors / and across health and other sectors), design and establish a process for such collaborations, establish alliances, networks and coalitions, adopt whole-of-government and whole-of-society approaches, and persuade actors across sectors and across levels for joint action
■ Steer i.e. decide a strategic direction, vision and mission, identify a policy problem, advocate policy, set policy agenda, and have a policy dialogue, analyze policy options, and make sound policies;
■ Regulate i.e. transform policies into legally enforceable instruments like laws, regulations, rules of procedure, protocols, standard operating procedures, or resolutions;
■ Allocate responsibility of policy implementation and the authority and resources to carry out that responsibility through legally enforceable instruments; and
■ Oversee the implementation of policies.
The respondents, who lead, govern and manage on daily basis, felt these practices or actions essen-tially constitute governing. Competent leaders performing these practices in conjunction with the en-ablers such as ethical and moral integrity, transparency, accountability, and participation were judged to make the governance effective in the context of health.
Sixty percent of the survey respondents were men and 40 percent were women, and gender played into differences in responses on a number of key points. Women leaders were more likely to perceive ‘to include’ and ‘to oversee’ as a significant part of governing. They were also more likely than male leaders to identify poor governance in sectors other than health as well as the political, historical, and cultural context as being significant impediments in governing for health. Consistent with this find-ing, women were more likely to perceive good governance in sectors other than health as an enabler in governing for health. In addition, women were more likely to see effective governance leading to shorter waiting times and equitable health service. They were also more likely to believe in power of effective governance in sectors other than health sector in leading to the better health of individuals and populations.
It should be mentioned that this study is a component of a four-part series focused on enhancing the potential contribution of improved governance for improved health in low- and middle-income countries. The series includes:

9 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
1. The Spring 2011 Global Survey on Health Sector Governance
2. A targeted literature Review on Governance for Health
3. Perspectives from the field: Interviews of 25 international health leaders
4. The Spring 2012 Global Survey on Governance for Health (this report)
The targeted literature review as well as discussions with experts in the field informed the survey instrument. It was extensively pilot-tested before administration.
The findings from this survey as well as the other governance studies mentioned above will help the LMG project test a conceptual model of governance for health that in turn will inform project interventions to enhance governance at the local, state, national, and institutional level as a means to achieve sustainable health outcomes, and ultimately better health for people living in low- and middle-income countries.
IntroductionDespite the massive increase in global health aid in the past decades, and the efforts made by govern-ments to improve the health of their citizens, progress toward meeting the health Millennium Devel-opment Goals (MDGs) is slow in many developing countries in Asia, Africa, Latin America, and the Caribbean. Successful health interventions oftentimes achieve results, however in many cases these results are not sustained over time. In addition, difficulties remain in scaling up successful interven-tions across larger geographical areas within countries and across regions.
Poor governance in the health sector in low- and middle-income countries has contributed to poor health outcomes. Conversely, effective governance in the health sector has the potential to enable sus-tainability of the effective health interventions as well as the ability to scale them up in order to reach many more people. As a result, the leadership, management, and governance of the health sector have become an important priority. Increasingly more attention is being given to assessing governance in the health sector and working to improve it. The Global Fund keeps track of how the country coordination mechanisms and principal recipients are governed to ensure efficient utilization of its resources. The World Health Organization (WHO) has also defined leadership and governance as one of the six key building blocks of any health system (WHO, 2007) . The World Bank (1999) believes that governance matters and annually measures governance in low- and middle-income countries. The health sector has been a focus of its public expenditure tracking surveys and public expenditure reviews for over a decade now.
In line with many of these initiatives, USAID has invested significant resources to improve the leader-ship and management of health systems of the low- and middle-income countries in the last 25 years. Management Sciences for Health (MSH), through a number of projects funded by USAID, has demystified core leadership and management concepts, functions and practices in the health sector, achieving enhanced results for health service delivery. Through its support of Leadership, Manage-
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 10
ment and Governance (LMG) project, USAID has added governance for health as a new dimension to its programming in order to achieve better health outcomes. Management Sciences for Health (MSH) is currently leading a consortium of partners in implementation of the LMG project, includ-ing the Johns Hopkins School of Public Health (JHSPH), the Yale Global Health Leadership Insti-tute (GHLI), the International Planned Parenthood Federation (IPPF), the African Medical Research Foundation (AMREF), and Medic Mobile.
MSH is a nonprofit international health organization with a 40-year history of saving lives and improving the health of the world’s poorest and most vulnerable people by closing the gap between knowledge and action in public health.
To begin to clarify what we mean by “governance for health,” which has not yet been so well-defined in the context of low and middle income countries, the LMG project team of MSH did a targeted litera-ture review on governance across various academic disciplines (most notably political science, public administration, public policy, comparative politics, international relations, sociology, management, and institutional economics). Based upon this literature review as well as and discussions with many health sector governance experts, the team created a conceptual model of governance for health. The global governance for health survey summarized within this report will help to further refine this model.
Approach and MethodsFrom February 20 to March 24, 2012, the Leadership, Management and Governance (LMG) project conducted this survey of health leaders, managers, and those who govern in the health sector in 80 low- and middle-income countries. The objective of the survey is to enable the LMG project to test a conceptual model of governance for health. This model is expected to inform LMG project interven-tions to improve national, state and local, and institutional governance in low- and middle-income countries as a means to achieve sustainable health outcomes.
The purpose of the survey, as alluded to earlier, was to identify the perceptions and opinions of the respondents on the following dimensions of governing for health:
■ Practices of governing for health
■ Impediments in effective governance for health
■ Enablers of effective governance for health
■ Outcomes of effective governance for health
■ Interaction of leadership, management and governance in health
The survey was administered to the members of two online communities of practice of health sector managers, leaders, and those who govern in the health sector. A link to the survey instrument was sent via e-mail to approximately 6,334 health leaders, managers, and those who govern in public,
private, and civil society sectors in primarily low- and middle-income countries.
11 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
The two communities of practice who took the survey are the LeaderNet and the Global Exchange Network for Reproductive Health. LeaderNet (http://leadernet.msh.org) is a global learning commu-nity of practice for managers who lead and leaders who govern in the health sector and in the health institutions. Launched by Management Science for Health (MSH) in November 2003, LeaderNet has grown to more than 5,000 members worldwide. USAID-funded AIDSTAR-Two project’s Ca-pacity Building Knowledge Exchange Network or CBKEN (http://www.aidstar-two.org/), a global resource for organizational capacity building, currently supports the LeaderNet community of prac-tice. The project encourages global interaction of its members as a way to help build a global health capacity-building community. The other community of practice, the Global Exchange Network for Reproductive Health, is also supported by MSH.
The survey instrument was created based upon the targeted literature review as well as discussions with experts in the field. It was extensively pilot-tested before administration. The survey was ad-ministered in English, Spanish, French and Portuguese depending upon the respondent’s language of preference. A total of 477 responses were received from respondents who completed the survey in the following languages: English (274), Spanish (122), French (66), and Portuguese (15).
Research QuestionsThe research questions guiding the survey were: What constitutes governance? What constitutes ef-fective governance? What constitutes effective governance in the context of health? What are enablers and deterrents of effective governance for health? How effective governance relates to health system outcomes and health outcomes? How governance, leadership and management interact in the context of health? The survey sought perceptions of the respondents on these questions.
ResultsRespondent profileA total of 477 leaders, managers and people who govern from 80 countries (See Appendix 1 Table 1) responded to the survey. Of the respondents, 60% were male and 40% were female. The vast majority of respondents (88%) lived and worked in non-OECD countries. By region, 48% of the respondents were from Africa, 35% from Latin America and the Caribbean, 11% from Asia, and 6% from the USA, Canada, and Europe.
When asked what sector they work in (See Appendix 1 Figure 1), 50% of the respondents said that they work in the public sector, 27% in civil society organizations, 15% in the private sector, and 8% in other sectors (See Table 2 for illustrative listing of other sectors). By level of the health system, 53% of the respondents work at the national level, 34% at the state level, and 41% at the local level.

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 12
Seventeen percent (17%) work regionally with groups of nations located within the same geographic region of the world. Less than 10% of the respondents indicated they work at the global level (See Appendix 1 Figure 2)1. Table 3 gives illustrative list of other levels that respondents have described.
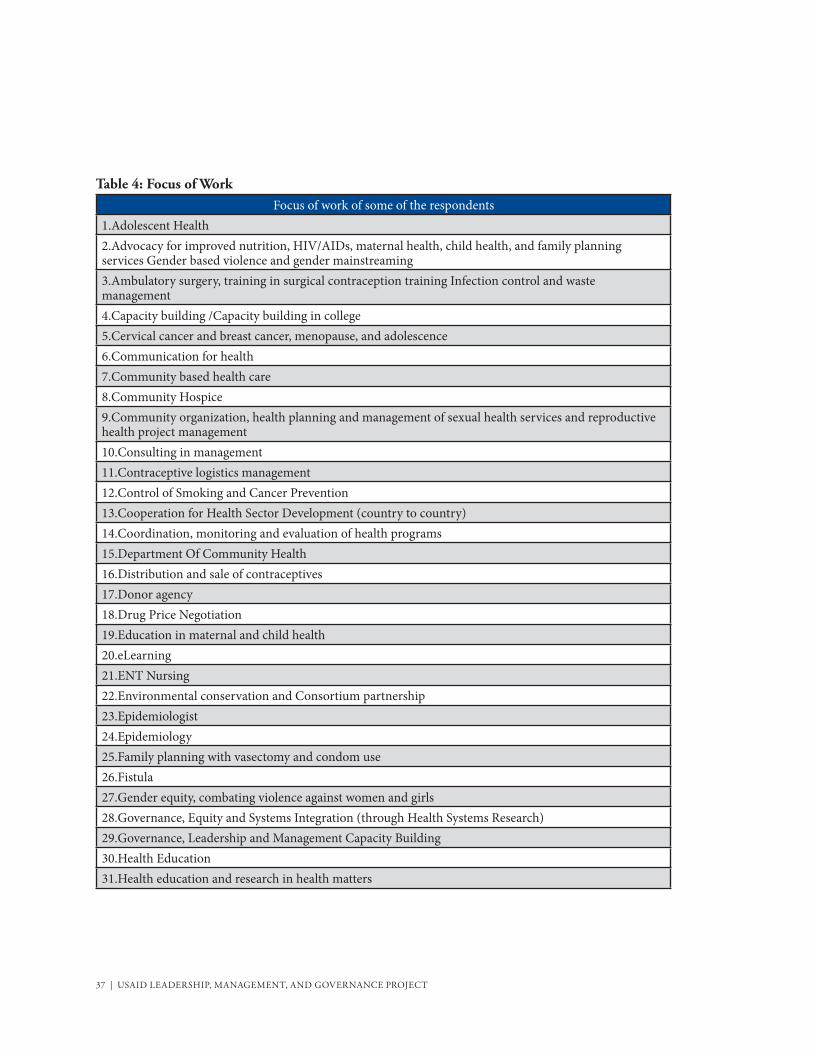
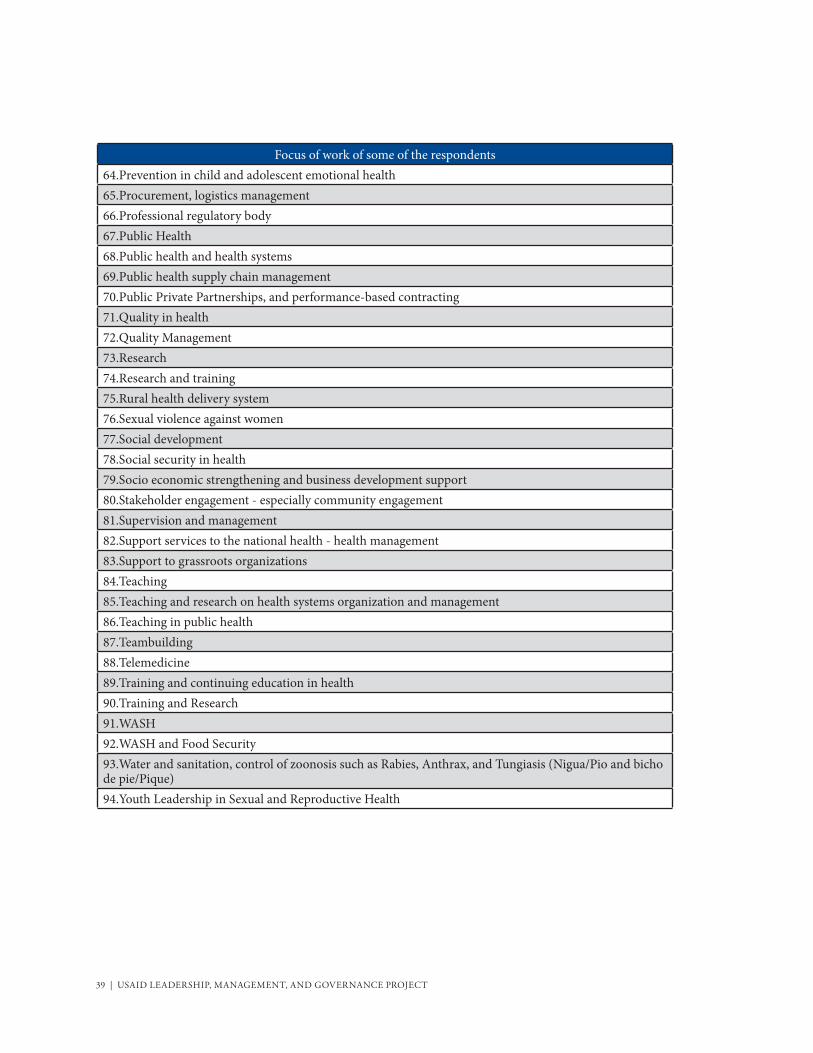
Viewed from the standpoint of the WHO building blocks of health systems,2 most respondents work within multiple health system building blocks with a focus on multiple service delivery areas (Figure 3). For example, a strong majority of respondents (83%) indicated that leadership and governance are the foci of their work. An almost equal proportion (81%) reported that health service delivery is also the focus of their work. Clearly, among these respondents there are service providers also lead, manage and/or govern, and vice-versa. In addition, 73% and 70% work with health information systems and human resources for health, respectively. Over half (52%) work with health systems financing and slightly over one-third (36%) work with medical products, vaccines and technologies. With regard to health focus, 75% or more work in at least one of the following areas: HIV & AIDS, family planning and reproductive health, maternal health, and child health. In addition, 58% and 57% work in ma-laria and/or tuberculosis respectively. The smallest percentage of respondents reported that they work with neglected tropical diseases (27%). Table 4 gives an illustrative listing of other foci of their work that the respondents indicated in their responses.
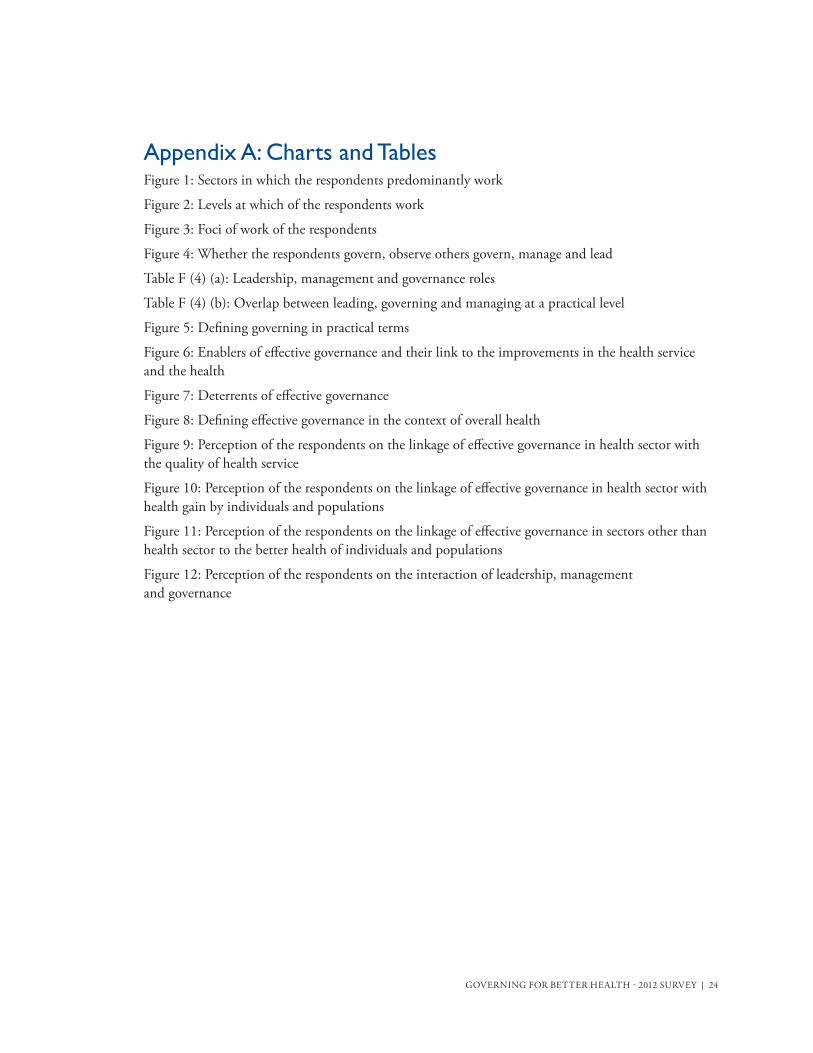
Each respondent was asked whether they lead, manage, govern, and/or observe others govern. Among this group of respondents, governing is not a common activity compared to leading and managing: 85% reported that they lead, and 85% say they manage, while only 32% reported that they govern. In addition, 85% stated that they observe others govern (See Figure 4). Much smaller percentages of the respondents (approximately 30%) reported that they lead and govern, or that they manage and gov-ern. In brief, more than 85% said they lead, 85% said they manage, and 85% said they observe closely those who govern. About one in every three respondents governs on a day-to- day basis. This indicates that there is a clear overlap among the roles of leading, managing, and governing. About 30% of the respondents also stated that they lead, manage, and govern. No respondent stated he or she governs but doesn´t manage or lead, indicating that when governance is exercised it is done while leading and/or managing. Respondents who govern also lead and manage. Respondents who manage also lead.
Elements or practices of governingThe survey sought to explore what governance means in practical terms for the respondents. In other words, what do people who govern do to govern? The respondents were asked the degree to which they consider each of the following practices (indicated by an action verb, such as “oversee”) and their corresponding activities as part of the governing process:
1 Note: the total adds up to more than 100% because the respondents could check multiple levels if they worked at multiple levels (See Appendix 1 Figure 2).
2 The six WHO health system building blocks are: health service delivery, health workforce, health information systems, essential medicines-vaccines-technologies, health financing, and leadership and governance.

13 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
■ To steer: To identify a policy problem, to advocate policy, to set policy agenda, to have a policy dialogue, to decide a strategic direction, to analyze policy options, to make sound policies, and use continual learning in refining and adapting policies for the future
■ To regulate: To formalize policies through laws, regulations, rules of procedure, protocols, standard operating procedures, or resolutions, etc.
■ To allocate: To allocate responsibility of policy implementation and also authority and resources to carry out that responsibility through any of the legally enforceable instruments stated above
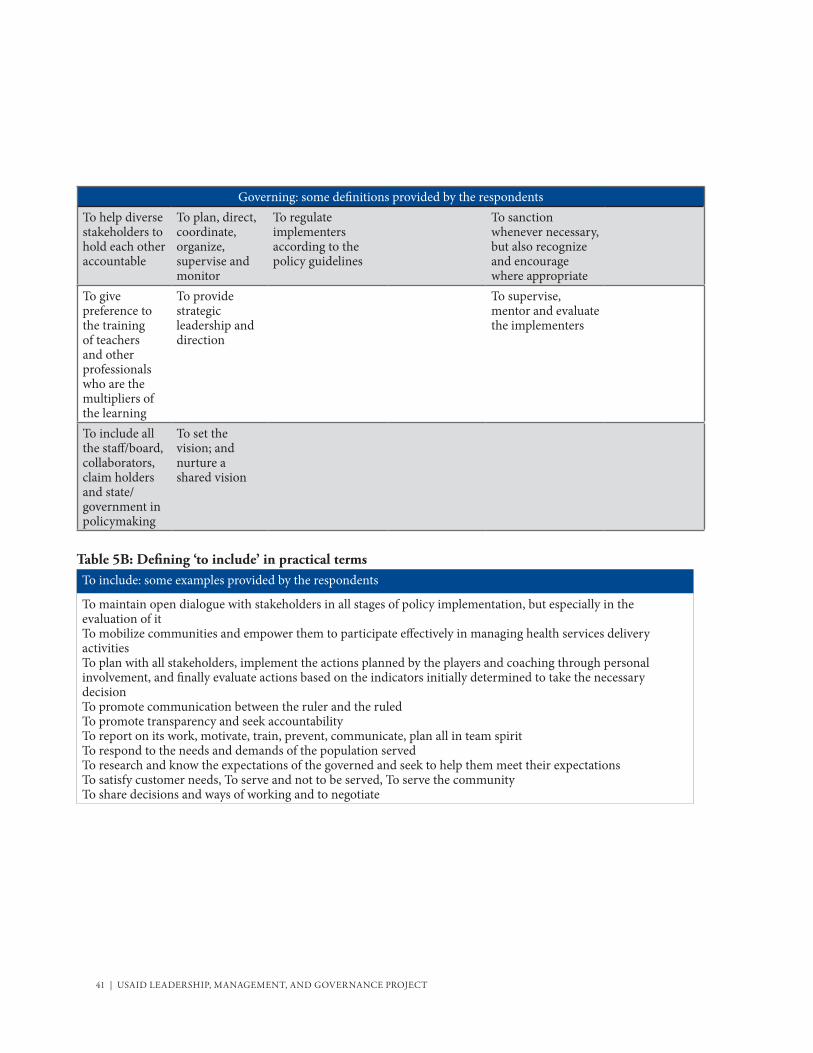
■ To include: To communicate and engage with the governed, to provide information, to promote dialogue, to engender trust, to allow representation, to establish systematic feedback mechanisms, to respond to the feedback received, to explain to the governed the changes made in response to their feedback, to enable openness, transparency, and accountability, and to resolve conflicts whenever they arise
■ To collaborate: To collaborate across levels (local, state or a province, national, regional and global) and across sectors (public, private, and civil society), to design and establish a process for such collaborations, to establish alliances, networks and coalitions, to adopt whole-of-government and whole-of-society approaches, and to persuade actors across sectors and across levels for joint action
■ To oversee: To communicate expectations to the policy implementers, watch and appraise the evaluation of implementation of policies, and use sanctions when necessary
There is strong agreement among these respondents that “include” and “steer” are two prominent governance practices (See Figure 5): fully 75% of the respondents stated that both “include” and “steer” are a highly significant part of the governing process.3 “Regulate,” “collaborate,” “oversee,” and “allocate” are also perceived as highly significant parts of the governing process by 67%, 63%, 60% and 58% of the respondents, respectively. The respondents in their optional comments have given a host of actions broadly similar to the six listed above (See Table 5 for similar elements and practices that constitute governance according to the survey respondents).
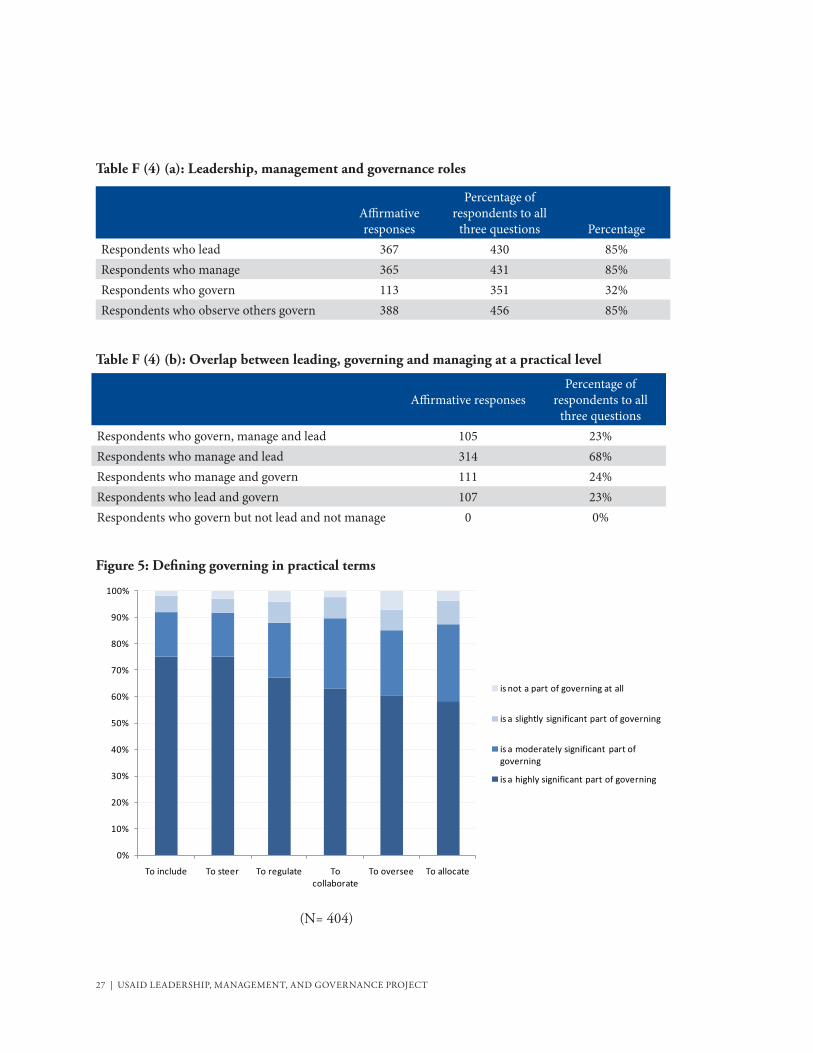
Enablers and impediments for effective governanceWhen queried about the enablers and impediments to effective governance for health, the respon-dents indicated that the top ten enablers are, in order of importance (See Figure 6):
1. Governing in health sector with ethical and moral integrity
2. Competent leaders governing in health sector
3. Governing in health sector with a definite policy on measurement, data gathering, analysis,
3 92% of the respondents indicated that both “include” and “steer” are highly or moderately significant parts of the governing process, while 89%, 88% 87% and 85% indicated the same for “collaborate”, “regulate”, “allocate” and “oversee”, respectively.
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 14
and use of information for policy making
4. Sound management of health sector
5. Adequate financial resources available for governing in health sector
6. Governing in health sector in open and transparent manner
7. Governing in health sector with client/community participation in decision making process
8. Governing in health sector with accountability to citizens/clients
9. Governing in health sector based on scientific evidence
10. Good Governance in sectors other than health
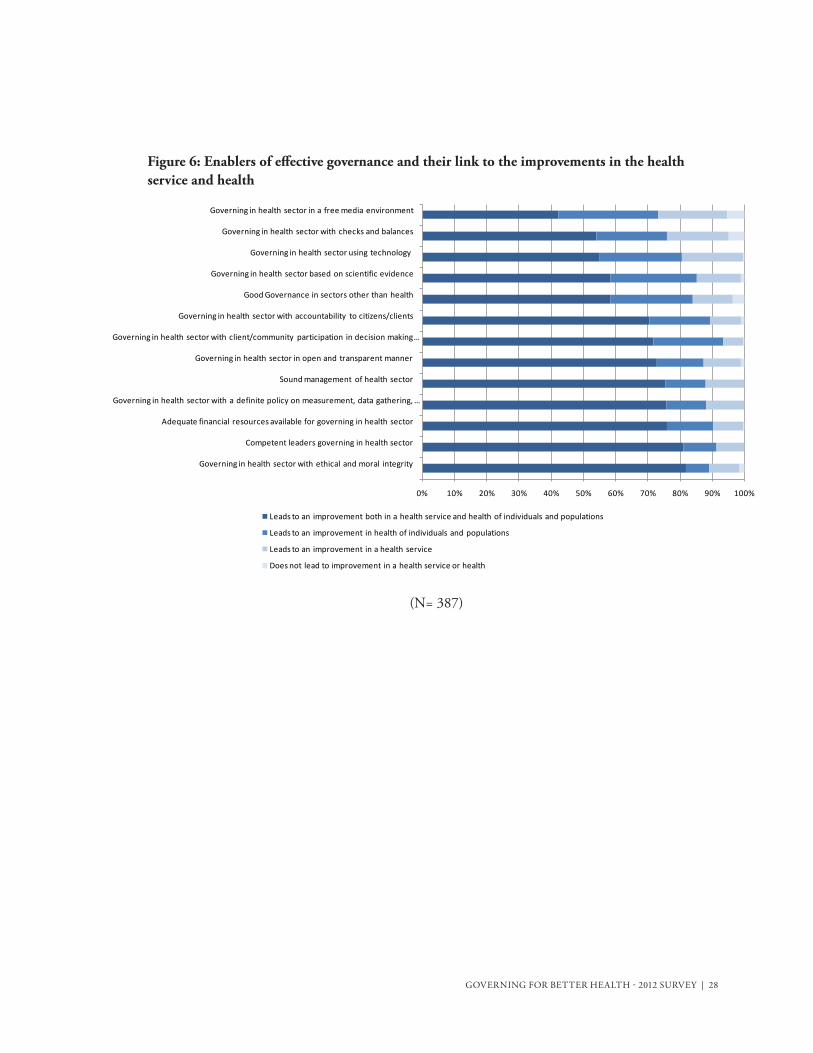
The top ten impediments to effective governance for health, according to the respondents, are (See Figure 7):
1. Ineffective leadership
2. Corruption
3. Ineffective management
4. Inadequate transparency
5. Inadequate accountability
6. Inadequate systems to collect, manage, analyze and use data
7. Inadequate participation of community/citizens/clients/consumers/patients
8. Political context
9. Inadequate checks and balances
10. Inadequate financial resources for governance
Of note is the central role that “ethical and moral integrity” and “leadership” play in effective gover-nance. Both are perceived as the most important facilitators. When they are absent, they are the most important impediments. According to the respondents, “governing with ethical and moral integrity” and “competent leaders governing in the health sector” are the two most important facilitators to effective governance while at the same time ineffective leadership and corruption are the two most important impediments.

15 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
The respondents were further asked whether governing with the enablers of effective health gov-ernance in place leads to improvements in health services and/or the health of individuals and the population. More than 70% of respondents said that governing with the following enablers of effec-tive governance (in order of importance) in place leads to both improvements in health services and in health:
1. Governing in the health sector with ethical and moral integrity
2. Competent leaders governing in health sector
3. Governing in health sector with a definite policy on measurement, data gathering, analysis, and use of information for policy making
4. Sound management of health sector
5. Adequate financial resources available for governing in health sector
6. Governing in health sector in open and transparent manner
7. Governing in health sector with client/community participation in decision making process
Respondents had an option to describe what they see as an enabler or an impediment to effective gov-ernance in the context of the health sector or a health institution. Tables 6 and 7 show an illustrative listing of the enablers and impediments according to the survey responses received.
Linkages between effective governance, improved health services, and improved health of individuals and the populationThe survey sought to understand how the respondents defined effective governance in the context of health (See Figure 8). Fully 75% of the respondents answered that effective governance in the context of health is the governance that leads to both an improvement in health services and the health of individuals and populations. Only 7% perceived effective governance as governance leading solely to improvement in health services, while 18% defined effective governance solely in terms of improve-ments in the health of individuals and populations.
The linkage between effective governance and improved health services The respondents were further asked to indicate the extent to which effective governance in the health sector leads to specific health service outcomes (See Figure 9). In order of importance, the respon-dents indicated that effective governance leads “to a large extent” to the following health service outcomes:4 services become effective (78%); access to and coverage of the service increase (77%);
4 Percentages of respondents indicating that effective governance leads “to a large extent” to the specific health service outcome are in parentheses.
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 16
clients are satisfied (77%); services become efficient (75%); and services become sustainable (75%). Of particular note is that these respondents do not perceive a strong relationship between effec-tive governance in the health sector and the safety of services: 65% stated that effective governance leads “slightly” to service safety and the remaining 35% indicated there is no relationship whatsoever between effective governance and service safety. Respondents perceive a very strong link, however, between effective governance and improvements in quality of health service. The respondents had an option of describing any other health system outcomes resulting from effective governance and they provided a host of health system outcomes; the link between effective governance and health systems outcomes was clearly identified (See Table 8).
The linkage between effective governance and improved health of individuals and the populationWhen asked to indicate the extent to which effective governance in the health sector leads to health gains by individuals and populations, 95% perceived that effective governance has either a large or moderate effect on health. Fully 94% indicated the same for client satisfaction (See Figure 10). The perception of effective governance leading to protection against financial risk was less prominent: 72% responded that it has a large or moderate effect while 28%% reported that it has a slight effect or no effect at all on financial risk protection.
The linkage between effective governance in sectors other than health and improved health of individuals and the populationRespondents also linked the health of individuals and populations to effective governance in other sectors. Approximately 93%% of the respondents stated that effective governance in sectors other than health leads to a large or moderate extent to better health of individuals and populations (See Figure 11).
Relationships between leadership, management, and governanceTo understand the relationships between leadership, management and governance, the respondents were asked to indicate the degree to which they agree with a series of statements. The influence of leadership on governance and management is clear. Leadership is pre-eminent among the three con-cepts and influences the other two. More than 90% of the respondents agreed or strongly agreed that: 1) leadership influences governance, 2) leadership influences management and 3) effective leadership is a pre-requisite for effective governance (See Figure 12).
Subgroup analysisA subgroup analysis across gender, sectors (public, private, civil society), levels (local, state, national and global), country where respondent works (non-OECD vs. OECD), geographical region (Asia vs. Africa vs. Latin America and Caribbean), those who govern vs. those who manage but don’t govern, and those

17 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
who govern vs. those who lead but don’t govern was performed to see if there are similarities and dif-ferences across these subgroups. A detailed discussion of these can be found in Appendix 2. The survey responses clearly had more similarities than differences on most of the aspects of governing.
Minor differences are nevertheless interesting to note. For example, female respondents were more likely to perceive ‘to include’ and ‘to oversee’ as a significant part of governing. There were no statistically significant differences in the way male and female respondents defined hindrances in effective governance for health, the exception being that women were more likely to identify poor governance outside the sector of health (i.e., the political, historical, and cultural context) as significant impediments to effectively governing for health. With regard to “enablers,” for the most part there were no statistically significant differences in the way men and women perceived enablers in effective governance for health, however there were two exceptions. One is that women were more likely to perceive good governance in sectors other than health as one of the enablers, a finding consistent with the preceding finding that women more likely to perceive poor gover-nance outside the sector of health as one of the impediments to effectively governing for health. In addition, female respondents were more likely to consider effective governance leading to shorter waiting times and equitable health service.
The male respondents were more likely than female respondents to believe in power of governance in the health sector to positively influence health outcomes, and promote financial risk protection as well as client satisfaction. On the other hand, the female respondents were more likely than male respondents to believe in power of effective governance in sectors other than the health sector leading to the better health of individuals and populations. The perceptions of female and male respondents were statistically similar in viewing the interaction and inter-relation of leadership, management, and governance in the context of health.
The perceptions of what constitutes governance as well as the identification of elements and prac-tices of governing are statistically similar across public sector, private sector and civil society, with the exception that respondents in the public sector as well as civil society were more likely to perceive “to allocate” as a significant part of governing than respondents in private sector. Based upon where they work, respondents working at the local level were more likely to perceive “to include” as a highly sig-nificant part of governing than those working at state level, who in turn were more likely to perceive it as highly significant than those working at national level. Along the same lines, those working at the national level were more likely to perceive this element of governing highly significant than those working at regional and global levels.
The respondents in the public sector were more likely to cite inadequate information as a constraint to decision-making than those working in civil society or the private sector. Consistent with this finding, public sector respondents were also more likely to cite a definite policy on measurement, data gathering, analysis, and use of information for decision-making as an enabler of effective governance. Similarly, the respondents in the public sector were more likely to perceive availability of adequate

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 18
financial resources for governing as an enabler of effective governance than those working in civil society or the private sector. The perceptions around and opinions on what impedes and what enables effective governance differed in a statistically significant manner based on the level at which the respondents worked (i.e., local, state, national, regional, or global level). Clearly, the facilitators and deterrents of effective governance are perceived with varying intensity at different levels.
DiscussionTo our knowledge, this is the second survey on perceptions of the people who lead, govern and manage within the heath sector and primarily within health institutions in low- and middle-income countries, the first being the 2011 MSH Survey on governance.5 The 2011 survey had a focus on governance in nonprofit institutions and institutions in the civil society sector. This 2012 survey, however, encompasses governance in all the three sectors (public, private and nonprofit), and at four levels: national, state, local, and institutional. The survey does not touch upon global governance for health or governance of global institutions in health. The survey attempts to distill common denomi-nators with regard to perceptions on the practices, facilitators, and outcomes of effective governance in the health sector at national and subnational levels in low- and middle-income countries.
The survey responses are of the people who lead, manage, and govern in the heath sector or the health institutions in the low- and middle-income countries. They have spoken clearly on several impor-tant dimensions of governing for health. Firstly, they define effective governance in health sectors in terms of the improvements in both the health services and the health of individuals and populations. Secondly, they see a clear link between the effective governance in the health sector and effective governance of the health institutions on one hand, and in health systems and health outcomes of individuals and populations. Third, many respondents, and women more than men, also see a clear link between governance in sectors other than health as well as the link between health outcomes of individuals and populations. Fourth, they identify what hinders effective governance in health sectors as well as identify what facilitates effective governance in the health sector, or within health institu-tions. Finally and perhaps most importantly, respondents clearly identify practices of governance and effective governance in the health context. These findings can also inform the design of interventions to enhance governance in these settings.
The constructs of leadership, management and governance have a theoretical and practical overlap. This survey provides insights into the interaction and interrelation between leadership, manage-ment, and governance in the context of health. This inter-relationship and interaction between the constructs as perceived by the respondents can be graphically depicted in a simple way (See figure (I) below). These three constructs influence the other levers or building blocks of a health system—infor-mation, human resources, medicines, vaccines and technologies, financing and service delivery—so that the health system is able to produce desired health outcomes.
5 Report of the Spring 2011 survey carried out by Management Sciences for Health is entitled, “Governing for Better Health: 2011 Survey.”

19 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Figure I: How Leadership, Management and Governance inter-relate and interact within a health system
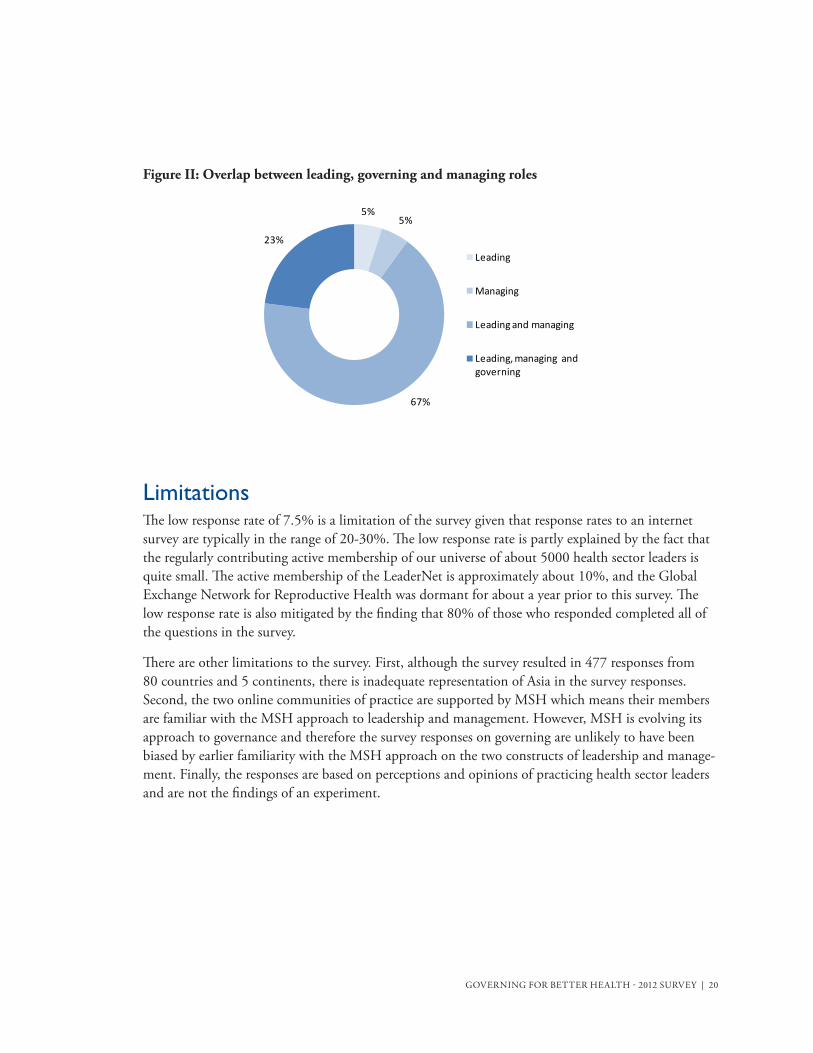
Among survey respondents, one in four respondents (23%) work in all three roles of leading, manag-ing and governing (they lead, manage and govern) on day-to-day basis; two in three (68%) respon-dents work in the two roles of leading and managing (they lead and manage) ; and only a very small minority of the respondents say they just lead or just manage. No respondents said they govern but do not lead or manage.
These findings have implications for the deployment of interventions to influence health sector gov-ernance policy and practice; any governance enhancement intervention has to consider the overlap between the leading, managing, and governing. This survey very clearly brings out two key findings: 1) Effective leadership is perceived by the target population as a prerequisite not only for effective governance, but also effective management. Effective leaders can enable and facilitate both the effec-tive governance and effective management. 2) Many people lead while governing and managing on day-to-day basis (See Figure (II) below). As a consequence, training and consulting support to en-hance governance should consider how leadership can enhance governing activities and management roles of these individuals.
Draft of LMG tools/resources category structure for web portal based on WHO six building blocks for Health Systems Strengthening. Note: their “leadership and Governance” block will need to be subsumed under our central L+M+G core in the diagram.
Health Information Systems
HumanResources Financing
Medicines, vaccines and technologies
Service delivery and demand
Leadership, Management
and Governance
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 20
Figure II: Overlap between leading, governing and managing roles
LimitationsThe low response rate of 7.5% is a limitation of the survey given that response rates to an internet survey are typically in the range of 20-30%. The low response rate is partly explained by the fact that the regularly contributing active membership of our universe of about 5000 health sector leaders is quite small. The active membership of the LeaderNet is approximately about 10%, and the Global Exchange Network for Reproductive Health was dormant for about a year prior to this survey. The low response rate is also mitigated by the finding that 80% of those who responded completed all of the questions in the survey.
There are other limitations to the survey. First, although the survey resulted in 477 responses from 80 countries and 5 continents, there is inadequate representation of Asia in the survey responses. Second, the two online communities of practice are supported by MSH which means their members are familiar with the MSH approach to leadership and management. However, MSH is evolving its approach to governance and therefore the survey responses on governing are unlikely to have been biased by earlier familiarity with the MSH approach on the two constructs of leadership and manage-ment. Finally, the responses are based on perceptions and opinions of practicing health sector leaders and are not the findings of an experiment.
5%5%
67%
23%
Leading
Managing
Leading and managing
Leading, managing and governing

21 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
ConclusionThe results of this survey provide ten important insights into effective gover-nance for health.
1. In considering the realms of leadership, management and governance, the influence of leadership on governance and management is clear. Leadership is pre-eminent among the three concepts and effective leadership is a prerequisite and an enabler of effective governance and effective management. Effective leaders are critical to the governing process. Ineffective
leadership is the largest impediment to effective governance.
2. Governing in the health sector with moral and ethical integrity is judged to be the most important enabler of effective governance. Lack of moral and ethical integrity in the form of
corruption is the second biggest impediment to effective governance.
3. Leaders who govern must master the following essential practices:
– Include the governed in governing by communicating and engaging with them, engender trust, allow representation, provide information, promote dialogue, establish systematic feedback mechanisms, respond to the feedback, and resolve conflicts;
– Collaborate across levels (local, state, national, and global) and across sectors (across public, private, and civil society sectors / and across health and other sectors), design and establish a process for such collaborations, establish alliances, networks and coalitions, adopt whole-of-government and whole-of-society approaches, and persuade actors across sectors and across levels for joint action
– Steer i.e. decide a strategic direction, vision and mission, identify a policy problem, advocate policy, set policy agenda, and have a policy dialogue, analyze policy options, and make sound policies;
– Regulate i.e. transform policies into legally enforceable instruments like laws, regulations, rules of procedure, protocols, standard operating procedures, or resolutions;
– Allocate responsibility of policy implementation and the authority and resources to carry out that responsibility through legally enforceable instruments; and
– Oversee the implementation of policies.
4. Effective governance is expected to result in improved health services, namely: improved effectiveness, client satisfaction, access, coverage, efficiency and sustainability; and reduced waiting times to obtain services.
5. Effective governance results in health gain for individuals and communities.

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 22
6. Effective governance for health must also consider multi-sectoral coordination beyond the realm of health and governance in the sectors other than health that affect health.
7. Several other factors are perceived by the health leaders to impede effective governance: ineffective leadership; corruption; ineffective management; inadequate transparency; inadequate accountability; inadequate systems to collect, manage, analyze and use data; inadequate participation of community, citizens and clients; the political context; inadequate checks and balances; inadequate financial resources for governance; poor governance in sectors other than health; policies not based on scientific evidence; the historical, social and cultural context; restricted media freedom; and inadequate use of technology for governance.
8. Factors that facilitate effective governance are: competent leaders governing with ethical and moral integrity, and make use of measurement as well as data collection, analysis, and use; sound management of the health sector; adequate financial resources available for governing; governing in an open and transparent manner; governing with client/community participation in decision-making, and being accountable to citizens/clients; governing based on scientific evidence; effective governance in sectors other than health; governing with checks and balances; governing using technology; and governing in a free media environment.
9. Certain differences in responses were linked to gender. For example, women leaders are more likely to perceive “to include” and “to oversee” as a significant part of governing. They are also more likely than male leaders to identify poor governance in sectors other than health, the political context, and the historical and cultural context as significant impediments in governing for health. Consistent with this finding, they are also more likely to perceive good governance in sectors other than health as one of the enablers. In addition, women are more likely to consider effective governance leading to shorter waiting times and equitable health service. Finally, they are more likely to believe in the power of effective governance in sectors other than the health sector leading to better health for individuals and populations.
10. There are far more similarities than differences in the perceptions and opinions arising out of the collective experience and wisdom of the 477 respondents on various dimensions of governing for health. There are more similarities than differences across different subgroups of the respondents i.e. across gender, sectors (public, private, civil society), levels (local, state, national and global), geographical regions (Asia, Africa, and Latin America and Caribbean), those who govern vs. those who manage but do not govern, and those who govern vs. those who lead but do not govern. The survey respondents have in effect identified common denominators with regard to what constitutes governing, effective governance, impediments and enablers of effective governance, and the outcomes of effective governance in the context of health.

23 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Policy ImplicationsOver the past decade, MSH has defined key practices for the effective leading and managing in the context of health . This framework defines leading as: 1) scanning (identifying client and stakeholder needs and priorities, recognizing trends, opportunities, and risks that affect the organization, looking for best practices, identifying staff capacities and constraints, and knowing yourself, your staff, and your organization—their values, strengths, and weaknesses); 2) focusing (articulating the organiza-tion’s mission and strategy, identifying critical challenges, linking goals with the overall organizational strategy, determining key priorities for action, and creating a common picture of desired results); 3) aligning/mobilizing (ensuring congruence of values, mission, strategy, structure, systems, and daily actions, facilitating teamwork, uniting key stakeholders around an inspiring vision, linking link goals with rewards and recognition, and enlisting stakeholders to commit resources); and 4) inspiring (matching deeds to words, demonstrating honesty in interactions, showing trust and confidence in staff, acknowledging the contributions of others, providing staff with challenges, feedback, and sup-
port, and being a model of creativity, innovation, and learning).
The framework similarly defines managing in the context of health in practical terms. This framework has informed the development of an MSH suite of interventions in the field of leadership and man-agement for health over the past ten years. The MSH Leadership Development Program (LDP) and Virtual Leadership Development Program (VLDP) are two examples of such successful MSH inter-ventions and have been implemented in over 70 countries around the world. The LDP has strength-ened health systems and has helped to achieve better health outcomes, and in a rigorous evaluation from its use in Kenya there is some early evidence of its sustainable impact on these outcomes . This survey now contributes to define governing in practical terms in the context of health, and will help to integrate governing into the framework of leading and managing for health.
There is an overlap between leadership, management and governance at both theoretical and practical levels. All interact to increase the probability of good health for those served by a health system. Each influences the other two. Effective leadership emerges as pre-eminent, and a prerequisite for effective governance and management. Often a single person fulfills multiple roles. A leadership, management or governance intervention that considers this overlap and inter-relationship is more likely to be effective.
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 24
Appendix A: Charts and TablesFigure 1: Sectors in which the respondents predominantly work
Figure 2: Levels at which of the respondents work
Figure 3: Foci of work of the respondents
Figure 4: Whether the respondents govern, observe others govern, manage and lead
Table F (4) (a): Leadership, management and governance roles
Table F (4) (b): Overlap between leading, governing and managing at a practical level
Figure 5: Defining governing in practical terms
Figure 6: Enablers of effective governance and their link to the improvements in the health service and the health
Figure 7: Deterrents of effective governance
Figure 8: Defining effective governance in the context of overall health
Figure 9: Perception of the respondents on the linkage of effective governance in health sector with the quality of health service
Figure 10: Perception of the respondents on the linkage of effective governance in health sector with health gain by individuals and populations
Figure 11: Perception of the respondents on the linkage of effective governance in sectors other than health sector to the better health of individuals and populations
Figure 12: Perception of the respondents on the interaction of leadership, management and governance

25 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Figure 1: Sectors in which the respondents predominantly work
50
27
15
8
0
10
20
30
40
50
60
Public Civil Society Private Others
(N=455)
Figure 2: Levels at which of the respondents work
41%
34%
53%
17%
9%
3%
0%
10%
20%
30%
40%
50%
60%
Local State National Regional Global Other

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 26
84%
83%
81%
79%
77%
76%
73%
70%
63%
58%
57%
52%
47%
47%
35%
27%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
HIV/AIDS
Leadership and governance
Health service delivery
Family planning and Reproductive health
Maternal health
Child health
Health information system
Human resources for health
Nutrition
Malaria
Tuberculosis
Health systems financing
Clinical and curative medicine
Chronic diseases
Medical products, vaccines and technologies
Neglected tropical diseases
(N= 477)
Figure 4: Whether the respondents govern, observe others govern, manage and lead
32%
85% 85% 85%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Do you govern? Do you observe others govern?
Do you manage? Do you lead?
Figure 3: Foci of work of the respondents
27 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Table F (4) (a): Leadership, management and governance roles
Affirmative responses
Percentage of respondents to all
three questions PercentageRespondents who lead 367 430 85%Respondents who manage 365 431 85%Respondents who govern 113 351 32%Respondents who observe others govern 388 456 85%
Table F (4) (b): Overlap between leading, governing and managing at a practical level
Affirmative responsesPercentage of
respondents to all three questions
Respondents who govern, manage and lead 105 23%Respondents who manage and lead 314 68%Respondents who manage and govern 111 24%Respondents who lead and govern 107 23%Respondents who govern but not lead and not manage 0 0%
Figure 5: Defining governing in practical terms
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
To include To steer To regulate To collaborate
To oversee To allocate
is not a part of governing at all
is a slightly significant part of governing
is a moderately significant part of governing
is a highly significant part of governing
(N= 404)
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 28
Figure 6: Enablers of effective governance and their link to the improvements in the health service and health
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Governing in health sector with ethical and moral integrity
Competent leaders governing in health sector
Adequate financial resources available for governing in health sector
Governing in health sector with a definite policy on measurement, data gathering, …
Sound management of health sector
Governing in health sector in open and transparent manner
Governing in health sector with client/community participation in decision making …
Governing in health sector with accountability to citizens/clients
Good Governance in sectors other than health
Governing in health sector based on scientific evidence
Governing in health sector using technology
Governing in health sector with checks and balances
Governing in health sector in a free media environment
Leads to an improvement both in a health service and health of individuals and populations
Leads to an improvement in health of individuals and populations
Leads to an improvement in a health service
Does not lead to improvement in a health service or health
(N= 387)
29 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Figure 7: Deterrents of effective governance
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Ineffective leadership
Corruption
Ineffective management
Inadequate transparency
Inadequate accountability
Inadequate systems to collect, manage, analyze and use …
Inadequate participation of community / citizens
Political context
Inadequate checks and balances
Inadequate financial resources for governance
Poor governance in sectors other than health
Policies not based on scientific evidence
Historical, social and cultural context
Restricted media freedom
Inadequate use of technology for governance
is one of the top impediments is a moderate impediment impedes slightly does not impede at all
(N= 387)

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 30
Figure 8: Defining effective governance in the context of overall health
75%
18%
7%
0%0%
10%
20%
30%
40%
50%
60%
70%
80%
Governance leading to improvements in both,
health service and health of the
individuals and the populations
Governance leading to improvement in health of the individuals and
the populations
Governance leading to improvement in health
service
None of the preceding
(N=408)
Figure 9: Perception of the respondents on the linkage of effective governance in health sector with the quality of health service
0% 20% 40% 60% 80% 100%
Service becomes effective
Clients are satisfied
Access to and coverage of the service increase
Service becomes sustainable
Service becomes efficient
Service becomes more equitable
Waiting times are reduced
Health care becomes safe
to a large extent moderate slight not at all

31 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Figure 10: Perception of the respondents on the linkage of effective governance in health sector with health gain by individuals and populations
59%
52%
36%36%
42%
36%
0%
10%
20%
30%
40%
50%
60%
70%
Better health Client satisfaction Financial risk protection
large moderate slight none
(N= 377)

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 32
Figure 11: Perception of the respondents on the linkage of effective governance in sectors other than the health sector to the better health of individuals and populations
1%
7%
31%
62%
0%
10%
20%
30%
40%
50%
60%
70%
There is no link at all
There is a slight link
There is a moderate link
There is a large link
(N= 379)

33 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Figure 12: Perception of the respondents on the interaction of leadership, management, and governance
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Leadership influences governance
Leadership influences management
Effective leadership is a prerequisite for effective governance
Effective leadership is a prerequisite for effective management
Governance influences management
Effective governance is a prerequisite for effective management
Governance influences leadership
Management influences governance
Effective management is a prerequisite for effective governance
Management influences leadership
Effective management is a prerequisite for effective leadership
Effective governance is a prerequisite for effective leadership
strongly agree agree neutral disagree strongly disagree
(N=379)

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 34
Table 1: Regions and countries represented (Number of respondents, country-wise)
Country # Country # Country # Country #Nigeria 43 Peru 37 Afghanistan 13 France 4Kenya 37 Bolivia 17 India 10 Spain 2Ethiopia 22 Haiti 15 Pakistan 6 Switzerland 2Burkina Faso 11 Brazil 13 Philippines 5 Albania 1Rwanda 10 Ecuador 11 Cambodia 3 Armenia 1Ghana 9 Guatemala 11 Bangladesh 2 Bosnia and
Herzegovina1
Uganda 9 Mexico 11 Fiji 1 Netherlands 1Côte d'Ivoire 8 Nicaragua 11 Israel 1 Poland 1United Republic of Tanzania
8 Dominican Republic
6 Japan 1 Ireland 1
Democratic Republic of the Congo
7 El Salvador 5 Democratic People’s Republic of Korea
1 Luxembourg 1
Sudan 6 Paraguay 4 Federated States of Micronesia
1 Australia 1
Botswana 4 Guyana 3 Nepal 1 Canada 2Mozambique 4 Honduras 3 Singapore 1 USA 13Niger 4 Trinidad and
Tobago3 Thailand 1
South Africa 4 Belize 2 Timor-Leste 1Namibia 3 Panama 2 United Arab
Emirates1
Senegal 3 Argentina 1 Yemen 1Sierra Leone 3 Colombia 1Burundi 2Cameroon 2Egypt 2Lesotho 2Malawi 2Mali 2Comoros 1Republic of the Congo
1
Guinea 1Madagascar 1Morocco 1Swaziland 1Togo 1Seychelles 1
215 156 50 31

35 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Table 2: Sector of workLevel of work of some of the respondents who reported levels other than local, state, national, regional or
global as a level of their work1.Academia2.Auxiliary to public authorities3.Bilateral aid worker4.Community-based5.Consultancy in Logistics6.Consultant in both private and public7.Cooperating Agency8.Development sector9.Donor Organization10.Faculty of Medicine at a government University 11.Faith-based organization12.Foundation13.Funder of health service delivery14.Health and Educational Institutions of Government15.Health Training institutions16.Implementing Agency17.International cooperation project18.International NGO19.International organization20.Local Non-Governmental Organization (NGO)21.Medical school and teaching hospital22.Medical universities23.National NGO24.NGO working with the public and private sectors25.Non-Governmental Organization26.Nonprofit Organization 27.Obstetric and gynecological28.Parastatal (A national referral, teaching and research institution)29.Parastatal / Quasi Government30.Project evaluation31.Public/private partnerships 32.Purchasing and Distribution 33.Red Cross34.Regional Health Directorate 35.Teaching institutions of higher learning36.Teambuilding for health-focused teams37.Technical and financial partner
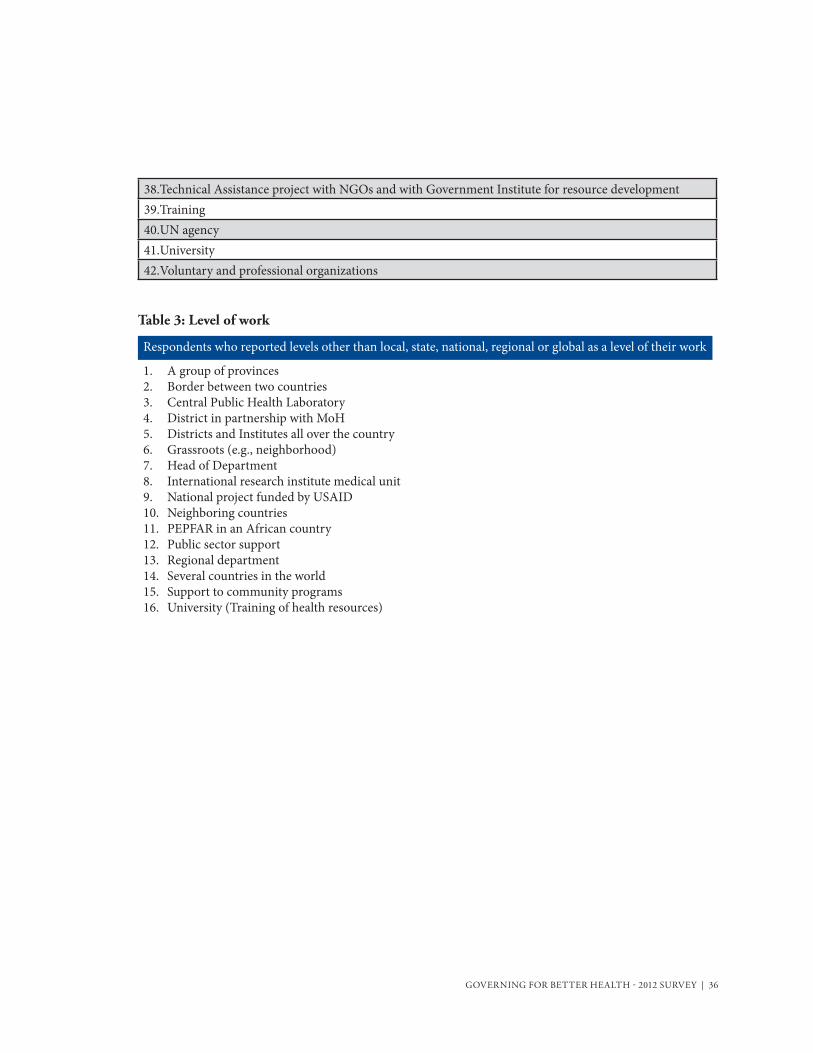
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 36
38.Technical Assistance project with NGOs and with Government Institute for resource development39.Training 40.UN agency41.University42.Voluntary and professional organizations
Table 3: Level of work
Respondents who reported levels other than local, state, national, regional or global as a level of their work
1. A group of provinces2. Border between two countries3. Central Public Health Laboratory 4. District in partnership with MoH5. Districts and Institutes all over the country6. Grassroots (e.g., neighborhood)7. Head of Department 8. International research institute medical unit9. National project funded by USAID10. Neighboring countries11. PEPFAR in an African country12. Public sector support13. Regional department14. Several countries in the world15. Support to community programs 16. University (Training of health resources)
37 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Table 4: Focus of WorkFocus of work of some of the respondents
1.Adolescent Health2.Advocacy for improved nutrition, HIV/AIDs, maternal health, child health, and family planning services Gender based violence and gender mainstreaming3.Ambulatory surgery, training in surgical contraception training Infection control and waste management4.Capacity building /Capacity building in college5.Cervical cancer and breast cancer, menopause, and adolescence6.Communication for health7.Community based health care8.Community Hospice9.Community organization, health planning and management of sexual health services and reproductive health project management 10.Consulting in management11.Contraceptive logistics management12.Control of Smoking and Cancer Prevention13.Cooperation for Health Sector Development (country to country)14.Coordination, monitoring and evaluation of health programs15.Department Of Community Health16.Distribution and sale of contraceptives17.Donor agency18.Drug Price Negotiation19.Education in maternal and child health20.eLearning21.ENT Nursing22.Environmental conservation and Consortium partnership 23.Epidemiologist 24.Epidemiology25.Family planning with vasectomy and condom use26.Fistula27.Gender equity, combating violence against women and girls28.Governance, Equity and Systems Integration (through Health Systems Research)29.Governance, Leadership and Management Capacity Building30.Health Education31.Health education and research in health matters

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 38
Focus of work of some of the respondents32.Health indicators33.Health Management and Administration34.Health policy and regulations35.Health Promotion36.Health promotion and development37.Health related NGO’s coordinator and Head of Planning, Monitoring and Evaluation in the Regional Health Bureau 38.Health system strengthening and capacity building39.Health system strengthening at provincial level40.Health systems training41.HIV/AIDS prevention, care and treatment as well as health system strengthening 42.Human rights for people with HIV43.Infections associated with health care44.Intervention design45.Local Health Management46.Logistics management47.Macro-organization of health48.Management49.Medical Education, HRH, Health Systems Research50.Medication inventory management51.Mental Health52.Monitoring and Evaluation53.Monitoring and evaluation of Health programs54.Municipal Health Management55.NGO health advice56.Organizational Development, First Aid services/products, Disaster Management, and International Humanitarian Law57.Organizational strengthening NGOs58.Palliative care and geriatric care59.Planning, monitoring and evaluation of policies, plans and social projects60.Political Dialogue61.Population, health and environment62.Prevention (Communication for Behavioral Change and Community Mobilization)63.Prevention and Health Promotion
39 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Focus of work of some of the respondents64.Prevention in child and adolescent emotional health65.Procurement, logistics management66.Professional regulatory body67.Public Health68.Public health and health systems69.Public health supply chain management70.Public Private Partnerships, and performance-based contracting71.Quality in health72.Quality Management73.Research74.Research and training75.Rural health delivery system76.Sexual violence against women77.Social development78.Social security in health79.Socio economic strengthening and business development support80.Stakeholder engagement - especially community engagement81.Supervision and management 82.Support services to the national health - health management83.Support to grassroots organizations84.Teaching85.Teaching and research on health systems organization and management86.Teaching in public health87.Teambuilding88.Telemedicine89.Training and continuing education in health90.Training and Research91.WASH92.WASH and Food Security93.Water and sanitation, control of zoonosis such as Rabies, Anthrax, and Tungiasis (Nigua/Pio and bicho de pie/Pique)94.Youth Leadership in Sexual and Reproductive Health

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 40
Governing: some definitions provided by the respondentsTo include To steer To regulate To collaborate To oversee To allocateNetworking and capacity building
To articulate policies, and plans and resources of key industry players and other social sectors
To encourage, promote, facilitate training of human resources and sufficient for efficient implementation strategies and health policies
To coordinate with national authorities to define policies for implementation
To create functional organizational structures to provide oversight
Stewardship
Partners’ and stakeholders’ coordination
To compile and use compelling evidence to instill urgency in global health to make it “a cause”
To enhance formal teamwork and accountability across all segments of the stakeholder communities to ensure best use of often-limited human and financial resources
To create strategic alliances with organizations involved in the health sector
To monitor the implementation of policies and strategies to improve governance and efficiency of policy implementation
To synchronize from top to bottom design, implementation of policies for health, with greater focus on reducing inequities in the allocation of resources: material, human and financial
To conceptualize, define and explain to those governing and those governed the boundaries between different players i.e. the leaders, the managers and people who govern
To demand and use data for policy decisions and program decision-making and ensuring that proper M&E procedures are in place
To ensure that the proper organizational structures are in place to ensure that responsibility and accountability are clearly articulated
To work with different organizations that work with health
To punish as appropriate and not award the leaders who did not contribute
To articulate resources of key industry players and other social sectors
To expect and receive feedback from the governed
To develop policy standards, utilization and revision after feedback for improvement
To implement ethical codes and behaviors in providers of health care
establishing strategic partnerships
To sanction
Table 5A: Defining governing in practical terms
41 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Governing: some definitions provided by the respondentsTo help diverse stakeholders to hold each other accountable
To plan, direct, coordinate, organize, supervise and monitor
To regulate implementers according to the policy guidelines
To sanction whenever necessary, but also recognize and encourage where appropriate
To give preference to the training of teachers and other professionals who are the multipliers of the learning
To provide strategic leadership and direction
To supervise, mentor and evaluate the implementers
To include all the staff/board, collaborators, claim holders and state/government in policymaking
To set the vision; and nurture a shared vision
Table 5B: Defining ‘to include’ in practical termsTo include: some examples provided by the respondents
To maintain open dialogue with stakeholders in all stages of policy implementation, but especially in the evaluation of itTo mobilize communities and empower them to participate effectively in managing health services delivery activitiesTo plan with all stakeholders, implement the actions planned by the players and coaching through personal involvement, and finally evaluate actions based on the indicators initially determined to take the necessary decisionTo promote communication between the ruler and the ruled To promote transparency and seek accountabilityTo report on its work, motivate, train, prevent, communicate, plan all in team spiritTo respond to the needs and demands of the population servedTo research and know the expectations of the governed and seek to help them meet their expectationsTo satisfy customer needs, To serve and not to be served, To serve the communityTo share decisions and ways of working and to negotiate
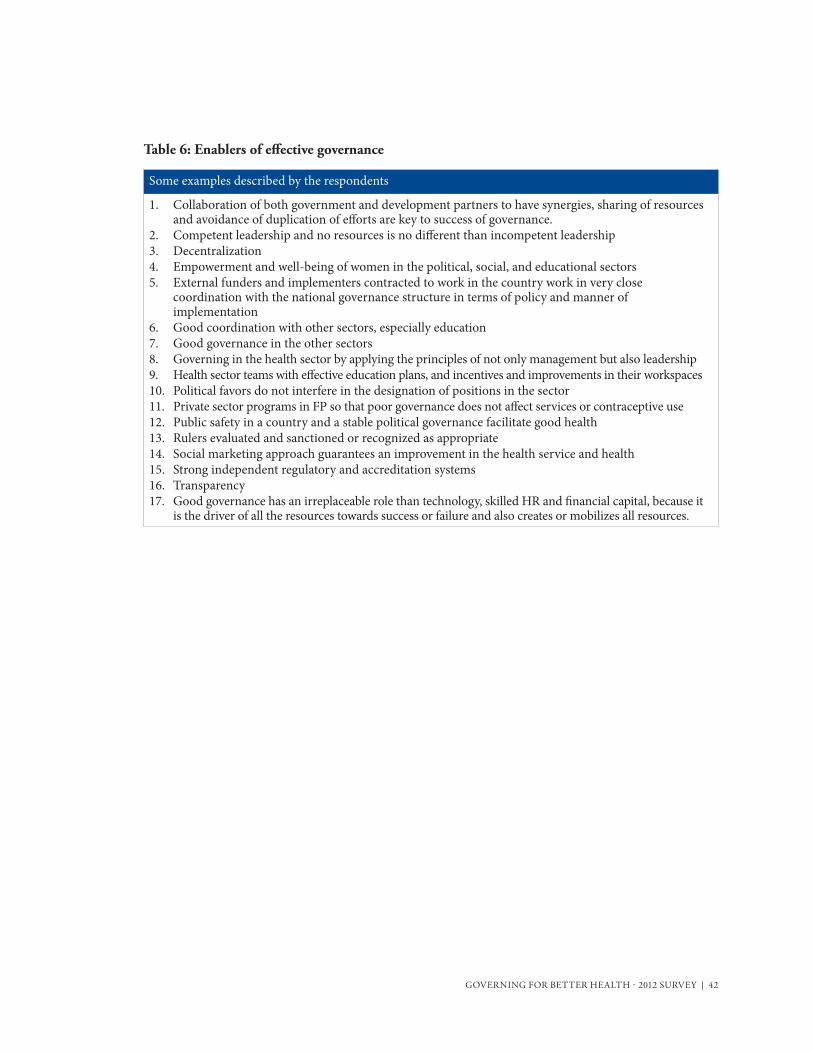
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 42
Some examples described by the respondents
1. Collaboration of both government and development partners to have synergies, sharing of resources and avoidance of duplication of efforts are key to success of governance.
2. Competent leadership and no resources is no different than incompetent leadership3. Decentralization4. Empowerment and well-being of women in the political, social, and educational sectors 5. External funders and implementers contracted to work in the country work in very close
coordination with the national governance structure in terms of policy and manner of implementation
6. Good coordination with other sectors, especially education7. Good governance in the other sectors 8. Governing in the health sector by applying the principles of not only management but also leadership9. Health sector teams with effective education plans, and incentives and improvements in their workspaces10. Political favors do not interfere in the designation of positions in the sector11. Private sector programs in FP so that poor governance does not affect services or contraceptive use12. Public safety in a country and a stable political governance facilitate good health13. Rulers evaluated and sanctioned or recognized as appropriate14. Social marketing approach guarantees an improvement in the health service and health15. Strong independent regulatory and accreditation systems16. Transparency17. Good governance has an irreplaceable role than technology, skilled HR and financial capital, because it
is the driver of all the resources towards success or failure and also creates or mobilizes all resources.
Table 6: Enablers of effective governance

43 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Table 7: Deterrents of effective governance
Some examples described by the respondents1.Context and situation dependent2.A focus on processes over outcomes3.Absence of leadership mindset (consistently striving to achieve results in spite of challenges)4.Bureaucracy 5.Capacity planning6.Commitment of Service Providers7.Context-specific 8.Election of heads for political reasons and no technical capacity9.Government commitment to involve all stake holders including NGOs and community based organizations in plan-ning, and M&E10.lliteracy11.mportation of models and ideas that are not context-specific12.Inadequate management and leadership resources for health service delivery13.Ineffective management 14.Insufficient budget for care15.Jurisdictional dispute with government health16.Lack of accountability and teamwork spirit17.Lack of clarity about the desired results18.Lack of commitment from government to separate political agenda and development activities19Lack of community involvement20Lack of consultation frameworks21.Lack of coordination among various actors in the same field22.Lack of or poor functionality of oversight structures23.Lack of or weak enforcement of policies and legislation 24.Lack of political will to promote health policies that confront cultural norms that discriminate against women - birth control, legal abortion, female literacy, female rights over their own bodies, females not being given priority in health issues25.Lack of resources relates to everything26.Lack of skilled professionals in the health services27.Lack of strong independent regulatory and accreditation systems28.Lack of supportive supervision and control 29.Lack of will power, motivation and too much fear of other factors30.Leadership that is not keen on follow-up (Why would drugs expire in the national medical stores if there was follow-up? Why would it take months for supplies to reach health facilities if there was keen governance follow-up? Keen follow-ups would instill a culture of responsibility in those down the line that stretches up to the health service beneficiary)31.Misuse of the financial resources (the hospitals have no medicines yet in stores the drugs expire or are later found in private clinics)32.Non-delegation
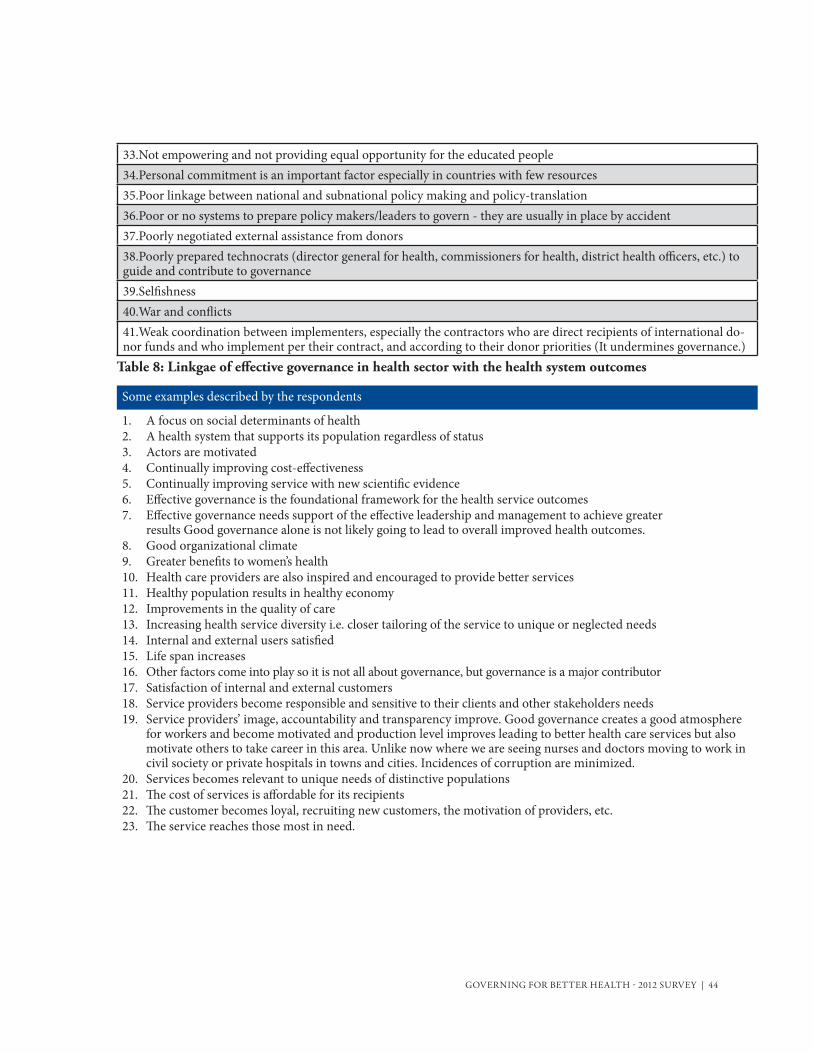
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 44
Some examples described by the respondents
1. A focus on social determinants of health2. A health system that supports its population regardless of status 3. Actors are motivated4. Continually improving cost-effectiveness 5. Continually improving service with new scientific evidence 6. Effective governance is the foundational framework for the health service outcomes7. Effective governance needs support of the effective leadership and management to achieve greater
results Good governance alone is not likely going to lead to overall improved health outcomes.8. Good organizational climate9. Greater benefits to women’s health10. Health care providers are also inspired and encouraged to provide better services11. Healthy population results in healthy economy12. Improvements in the quality of care13. Increasing health service diversity i.e. closer tailoring of the service to unique or neglected needs14. Internal and external users satisfied15. Life span increases16. Other factors come into play so it is not all about governance, but governance is a major contributor17. Satisfaction of internal and external customers18. Service providers become responsible and sensitive to their clients and other stakeholders needs19. Service providers’ image, accountability and transparency improve. Good governance creates a good atmosphere
for workers and become motivated and production level improves leading to better health care services but also motivate others to take career in this area. Unlike now where we are seeing nurses and doctors moving to work in civil society or private hospitals in towns and cities. Incidences of corruption are minimized.
20. Services becomes relevant to unique needs of distinctive populations21. The cost of services is affordable for its recipients22. The customer becomes loyal, recruiting new customers, the motivation of providers, etc.23. The service reaches those most in need.
Table 8: Linkgae of effective governance in health sector with the health system outcomes
33.Not empowering and not providing equal opportunity for the educated people34.Personal commitment is an important factor especially in countries with few resources35.Poor linkage between national and subnational policy making and policy-translation36.Poor or no systems to prepare policy makers/leaders to govern - they are usually in place by accident 37.Poorly negotiated external assistance from donors38.Poorly prepared technocrats (director general for health, commissioners for health, district health officers, etc.) to guide and contribute to governance 39.Selfishness40.War and conflicts41.Weak coordination between implementers, especially the contractors who are direct recipients of international do-nor funds and who implement per their contract, and according to their donor priorities (It undermines governance.)
45 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Appendix B: Subgroup AnalysisThis technical appendix describes the findings of subgroup analyses across gender, sectors (public, private, civil society), levels (local, state, national and global), country where respondent works (non-OECD vs. OECD), geographical region (Asia vs. Africa vs. Latin America and Caribbean), those who govern vs. those who manage but not govern, and those who govern vs. those who lead but not govern. There are more similarities than differences on most of the aspects of governing in the survey responses.
GenderThere is no statistically significant difference the way female and male respondents define governance and effective governance in the context of health. They were asked what governing means to them in practi-cal terms and to indicate the degree to which they consider to steer, to regulate, to allocate, to include, to collaborate, and to oversee are a part of the governing process. The responses of female and male respon-dents were statistically similar with regard to ‘to steer’ (exact test p-value = 0.8262), to regulate (p-value = 0.9122), to allocate (p-value = 0.2826), to include (p-value = 0.0697), to collaborate (p-value = 0.3128), and to oversee (p-value = 0.0827), at 95% confidence level. At 90% confidence level, female respondents were more likely to perceive to include and to oversee as significant part of governing.
Female and male respondents on average defined effective governance in the context of overall health as governance that leads to improvement in both a health service, and health of individuals and popu-lations. There were no statistically significant differences across gender at 95% confidence level (chisq p value= 0.0723). At 90% confidence level, on average women were more likely to define effective governance in terms of these improvements.
There were no statistically significant differences in the way men and women defined hindrances (all p-values >0.05) in effective governance for health except women were more likely to identify poor governance in sectors other than health (p-value = 0.0146), political context (p-value = 0.035) and historical and cultural context (p-value = 0.0231) as significant impediments in governing for health. Speaking of facilitators, there were no statistically significant differences in the way men and women defined facilitators (all p-values >0.05) in effective governance for health except women were more likely to perceive good governance in sectors other than health as one of the facilitators (p-value = 0.054). This finding is consistent with the earlier one recorded on women more likely to perceive poor governance in sectors other than health as one of the impediments to effective governing for health.
When asked to indicate the extent to which they considered effective governance in health sector leads health service outcomes, the female and male respondents gave statistically similar responses except at 90% confidence level female respondents were more likely to consider effective governance leading to shorter waiting times (p-value = 0.0607) and equitable health service (p-value = 0.0978).
The male respondents were more likely than female to believe in power of governance in health sector

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 46
to positively influence health outcomes (p-value < 0.001), financial risk protection (p-value = 0.0052) and client satisfaction (p-value < 0.001). On the other hand, the female respondents were more likely than male to believe in power of effective governance in sectors other than health sector leading to the better health of individuals and populations (p-value = 0.04860). The perceptions of female and male respondents were statistically similar in respect of interrelationships between leadership, management, and governance.
SectorsThe perceptions on what constitutes governance and what are the elements and practices of governing are statistically similar across public, private and civil society except the respondents in public sec-tor and civil society were more likely to perceive ‘to allocate’ as significant part of governing than the respondents in private sector (p-value = 0.0488).
The respondents in public sector were more likely to cite inadequate information as a constraint to decision making than those working in civil society or private sector (p-value = 0.0766). Consistent with this, they were more likely to cite a definite policy on measurement, data gathering, analysis, and use of information for decision making as an enabler of effective governance (p-value = 0.0846). Similarly, the respondents in public sector were more likely to perceive availability of adequate finan-cial resources for governing as an enabler of effective governance than those working in civil society or private sector (p-value = 0.0405).
LevelsBased on where they work, the respondents working at local level were more likely to perceive ‘to in-clude’ as a significant part of governing than those working at state level who in turn were more likely to so perceive than those working at national level (p-value = 0.0921). Those working at national level were more likely to perceive this element of governing as highly significant, than those working at regional and global levels.
The perceptions and opinions on what impedes and what enables effective governance differed in a statistically significant manner based on the level at which the respondents worked i.e. local, state, national, regional or global level. Clearly, the facilitators and deterrents of effective governance are perceived with varying intensity at different levels. On average, ineffective management, inadequate accountability, inadequate checks and balances, inadequate participation, inadequate financial resources for governing, inadequate use of technology were more likely to be perceived as highly significant deterrents. Similarly, reduced waiting time, increased client satisfaction, increased service effectiveness, and increased equity were perceived as highly significant health system outcomes at local level than other levels.
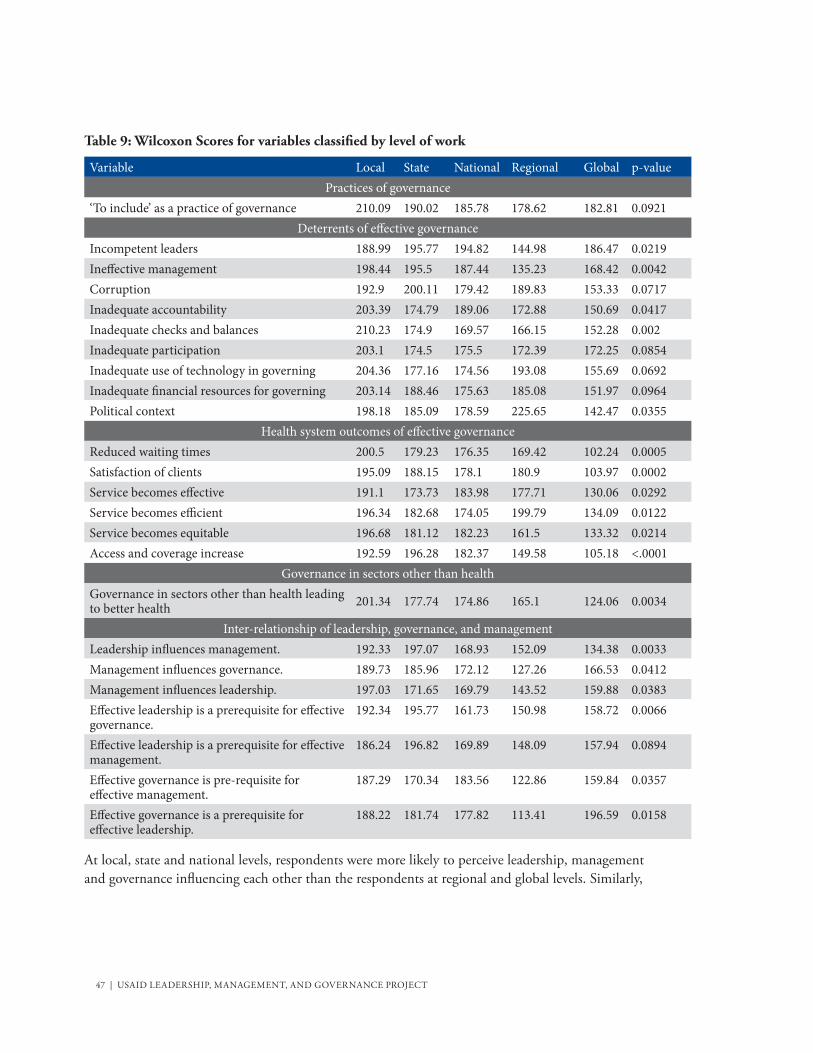
47 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Table 9: Wilcoxon Scores for variables classified by level of work
Variable Local State National Regional Global p-valuePractices of governance
‘To include’ as a practice of governance 210.09 190.02 185.78 178.62 182.81 0.0921Deterrents of effective governance
Incompetent leaders 188.99 195.77 194.82 144.98 186.47 0.0219Ineffective management 198.44 195.5 187.44 135.23 168.42 0.0042Corruption 192.9 200.11 179.42 189.83 153.33 0.0717Inadequate accountability 203.39 174.79 189.06 172.88 150.69 0.0417Inadequate checks and balances 210.23 174.9 169.57 166.15 152.28 0.002Inadequate participation 203.1 174.5 175.5 172.39 172.25 0.0854Inadequate use of technology in governing 204.36 177.16 174.56 193.08 155.69 0.0692Inadequate financial resources for governing 203.14 188.46 175.63 185.08 151.97 0.0964Political context 198.18 185.09 178.59 225.65 142.47 0.0355
Health system outcomes of effective governanceReduced waiting times 200.5 179.23 176.35 169.42 102.24 0.0005Satisfaction of clients 195.09 188.15 178.1 180.9 103.97 0.0002Service becomes effective 191.1 173.73 183.98 177.71 130.06 0.0292Service becomes efficient 196.34 182.68 174.05 199.79 134.09 0.0122Service becomes equitable 196.68 181.12 182.23 161.5 133.32 0.0214Access and coverage increase 192.59 196.28 182.37 149.58 105.18 <.0001
Governance in sectors other than healthGovernance in sectors other than health leading to better health 201.34 177.74 174.86 165.1 124.06 0.0034
Inter-relationship of leadership, governance, and managementLeadership influences management. 192.33 197.07 168.93 152.09 134.38 0.0033Management influences governance. 189.73 185.96 172.12 127.26 166.53 0.0412Management influences leadership. 197.03 171.65 169.79 143.52 159.88 0.0383Effective leadership is a prerequisite for effective governance.
192.34 195.77 161.73 150.98 158.72 0.0066
Effective leadership is a prerequisite for effective management.
186.24 196.82 169.89 148.09 157.94 0.0894
Effective governance is pre-requisite for effective management.
187.29 170.34 183.56 122.86 159.84 0.0357
Effective governance is a prerequisite for effective leadership.
188.22 181.74 177.82 113.41 196.59 0.0158
At local, state and national levels, respondents were more likely to perceive leadership, management and governance influencing each other than the respondents at regional and global levels. Similarly,
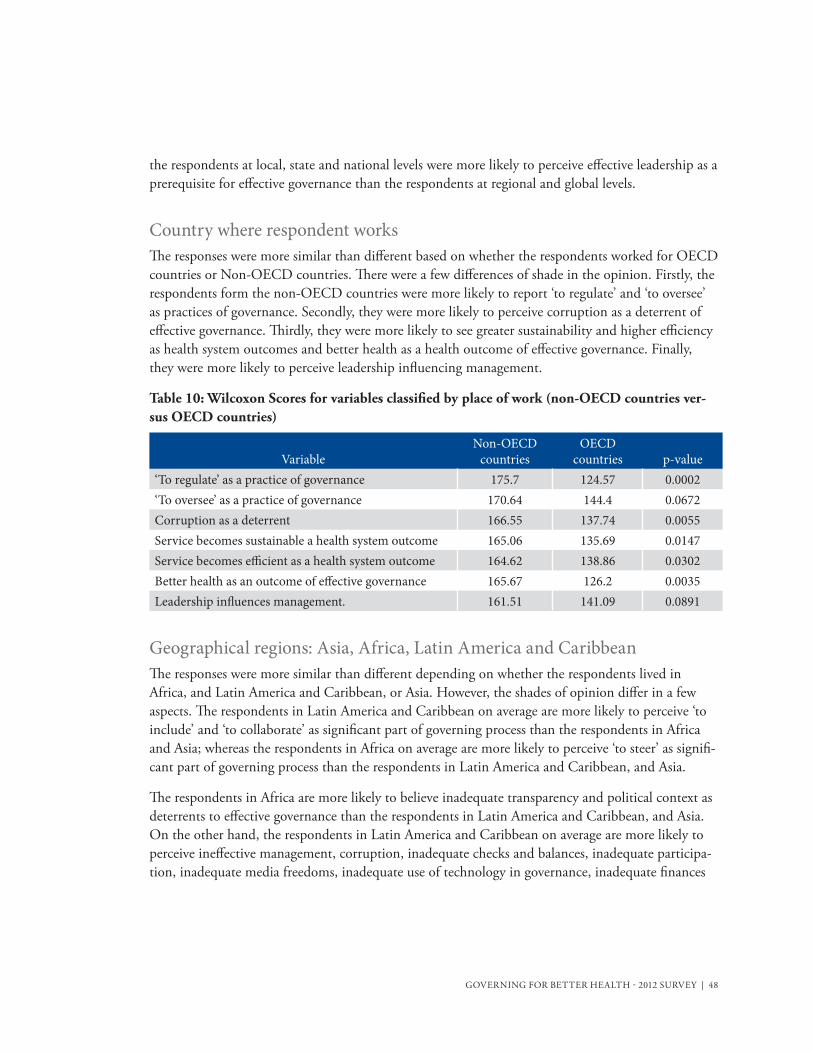
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 48
the respondents at local, state and national levels were more likely to perceive effective leadership as a prerequisite for effective governance than the respondents at regional and global levels.
Country where respondent worksThe responses were more similar than different based on whether the respondents worked for OECD countries or Non-OECD countries. There were a few differences of shade in the opinion. Firstly, the respondents form the non-OECD countries were more likely to report ‘to regulate’ and ‘to oversee’ as practices of governance. Secondly, they were more likely to perceive corruption as a deterrent of effective governance. Thirdly, they were more likely to see greater sustainability and higher efficiency as health system outcomes and better health as a health outcome of effective governance. Finally, they were more likely to perceive leadership influencing management.
Table 10: Wilcoxon Scores for variables classified by place of work (non-OECD countries ver-sus OECD countries)
VariableNon-OECD
countriesOECD
countries p-value‘To regulate’ as a practice of governance 175.7 124.57 0.0002‘To oversee’ as a practice of governance 170.64 144.4 0.0672Corruption as a deterrent 166.55 137.74 0.0055Service becomes sustainable a health system outcome 165.06 135.69 0.0147Service becomes efficient as a health system outcome 164.62 138.86 0.0302Better health as an outcome of effective governance 165.67 126.2 0.0035Leadership influences management. 161.51 141.09 0.0891
Geographical regions: Asia, Africa, Latin America and CaribbeanThe responses were more similar than different depending on whether the respondents lived in Africa, and Latin America and Caribbean, or Asia. However, the shades of opinion differ in a few aspects. The respondents in Latin America and Caribbean on average are more likely to perceive ‘to include’ and ‘to collaborate’ as significant part of governing process than the respondents in Africa and Asia; whereas the respondents in Africa on average are more likely to perceive ‘to steer’ as signifi-cant part of governing process than the respondents in Latin America and Caribbean, and Asia.
The respondents in Africa are more likely to believe inadequate transparency and political context as deterrents to effective governance than the respondents in Latin America and Caribbean, and Asia. On the other hand, the respondents in Latin America and Caribbean on average are more likely to perceive ineffective management, corruption, inadequate checks and balances, inadequate participa-tion, inadequate media freedoms, inadequate use of technology in governance, inadequate finances

49 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
for governance, poor governance in sectors other than health, and historical and cultural context as deterrents to effective governance than the respondents in Africa and Asia.
Talking of enablers of effective governance, the respondents in Africa are more likely to believe gov-erning with ethical and moral integrity, governing with openness and transparency, and governing with checks and balances as enablers of effective governance than the respondents in Latin America and Caribbean, and Asia. They are also more likely to believe improved safety of care, reduced wait-ing times, greater sustainability and increased efficiency of service as health system outcomes of effec-tive governance. Whereas the respondents in Latin America and Caribbean on average are more likely to perceive increased equity of service and improved access and coverage as health system outcomes of effective governance. The respondents in Africa and Asia are more likely to perceive better health, financial risk protection and client satisfaction as health outcomes of effective governance.
The respondents in Latin America and Caribbean on average are more likely to perceive management influencing governance, and management as a prerequisite of governance than the respondents in Africa and Asia. The respondents in Africa are likelier to believe governance influencing leadership.
Table 11: Wilcoxon Scores for variables classified by geographical region (Asia, Africa, and Latin America and Caribbean)
Variable Africa LAC Asia p-value‘To steer’ as a practice of governance 191.07 171.6 152.28 0.0051‘To include’ as a practice of governance 179.99 195.16 140.71 0.0006‘To collaborate’ as a practice of governance 176.63 199.64 145.77 0.002Ineffective management as a deterrent 172.67 185.02 151.73 0.0292Corruption as a deterrent 174.82 181.32 141.09 0.0017Inadequate transparency as a deterrent 178.71 175.58 142.99 0.031Inadequate checks and balances as a deterrent 175.27 179.34 133.26 0.0143Inadequate participation as a deterrent 174.37 180.98 134.68 0.0154Inadequate media freedoms as a deterrent 171.08 192.21 117.63 <.0001Inadequate use of technology as a deterrent 170.66 189.76 131.21 0.0023Inadequate finances for governance as a deterrent 169.44 189.45 147.38 0.0245Poor governance in sectors other than health 171.23 191.85 126.59 0.0005Political context 183.08 180.88 118.19 0.0002Historical and cultural context 165.27 191.69 149.13 0.0128Governing with ethical and moral integrity 178.59 175.02 145.62 0.0138Governing with openness and transparency 180.67 163.71 155.04 0.0566Governing with checks and balances as an enabler 180.82 160.2 150.4 0.0458Improved safety of care as a health system outcome 178.43 167.98 148.31 0.0915

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 50
Variable Africa LAC Asia p-valueReduced waiting times as a health system outcome 175.61 173.52 133.94 0.0154Client satisfaction as a health system outcome 212.62 111.78 182.62 <.0001Service becomes sustainable a health system outcome 179.74 165.01 157.33 0.0929Service becomes efficient as a health system outcome 177.03 170.78 149.5 0.0973Service becomes equitable as a health system outcome 169.42 184.77 140.18 0.0055Improved access and coverage as a health system outcome 167.67 180.47 148.86 0.0344Better health as an outcome of effective governance 215.97 108.59 185.93 <.0001Financial risk protection as an outcome of effective governance
200.12 122.01 189.32 <.0001
Governance influences leadership. 178.27 155.09 154.74 0.0505Management influences governance. 158.4 179.82 151.53 0.0661Effective management is a prerequisite for effective governance.
155.33 181.31 164.99 0.0422
Respondents who govern vs. respondents who manage but not governThose who said they govern but not manage are more likely to report inadequate transparency as a deterrent than those who said they manage and not govern. The former are likelier to report inad-equate checks and balances as a deterrent. Consistent with this, they are more likely to report govern-ing with checks and balances as an enabler of effective governance. The former are also more likely to report reduced waiting times and client satisfaction as health system outcomes, management influenc-ing leadership, and effective management as a prerequisite for effective leadership.
Table 12: Wilcoxon Scores for variables classified by the respondents who govern vs. respondents who manage but not govern
Variable Governors Managers p-valueInadequate transparency as a deterrent 125.96 112.4 0.0616Inadequate checks and balances as a deterrent 127.95 111 0.0375Governing with checks and balances as an enabler 131.37 106.37 0.0016Reduced waiting times as a health system outcome 125.91 111.65 0.0702Client satisfaction as a health system outcome 124.59 111.58 0.0994Management influences leadership. 124.53 108.25 0.0508
Effective management is a prerequisite for effective leadership.
124.36 108.48 0.0588

51 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Respondents who govern vs. respondents who lead but not governThose who said they govern but not lead are more likely to report inadequate transparency as a deterrent than those who said they lead and not govern. The former are likelier to report inadequate checks and balances as a deterrent. Again consistent with this, they are more likely to report gov-erning with ethical and moral integrity, competent leaders governing, and sound management as enablers of effective governance. The former are also more likely to report reduced client satisfaction as a health system outcome, management influencing leadership, and effective management and ef-fective as prerequisites for effective leadership.
Table 13: Wilcoxon Scores for variables classified by the respondents who govern vs. respon-dents who lead but not govern
Variable Governors Leaders p-valueInadequate transparency as a deterrent 129.62 116.07 0.0645Inadequate checks and balances as a deterrent 132.51 113.25 0.0199Governing with ethical and moral integrity 130.95 118.4 0.0566Governing with checks and balances as an enabler 136.01 107.82 0.0005
Competent leaders governing as an enabler 127.99 116.29 0.065Sound management as an enabler 127.49 115.92 0.0912Client satisfaction as a health system outcome 131.51 112.14 0.0173Management influences leadership. 130.51 108.61 0.0099Effective governance is a prerequisite for effective leadership.
128.03 110.3 0.0383
Effective management is a prerequisite for effective leadership.
128.22 110.3 0.0359
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 52
Appendix C: The Survey InstrumentThank you for your passionate work in public health and a special thank you to those of you who participated in the MSH 2011 survey on Governance for Health. We highly value the work you are doing to strengthen health systems in your jurisdiction.
Management Sciences for Health (MSH) commissioned the Leadership, Management and Gover-nance (LMG) Project on 26 September 2011. At MSH, we have a long history of 25 years of solid work in strengthening leadership and management for health. Now we are adding a new dimension of ‘governance’ to our existing model of leadership and management, to make the results of our work sustainable across time and scalable across geographical regions. The results of the MSH 2011 survey on governance for health have been a useful starting point. We solicit your inputs into the evolving conceptual model of governing for better health. Your inputs will make the model robust and we will then use it to inform our interventions to save lives and improve the health of the world’s poorest and most vulnerable people.
We value your insights and experiences and now ask you to help shape the model of ‘governing for health’. We are asking thought and practice leaders and managers in health sector and also those who govern for health worldwide to participate in a short, web-based survey about various elements of governing for health.
The questions are focused on various dimensions of governing for health:
■ Practices of governing for health
■ Impediments in effective governance for health
■ Facilitators of effective governance for health
■ Outcomes of effective governance for health
■ Interaction of Leadership, Management and Governance in health
Participation in this survey is completely voluntary. If you decide not to participate there will not be any negative consequences. Please be aware that if you decide to participate, you may stop participat-ing at any time and you may decide not to answer any specific question. If you would like to par-ticipate, your insights and comments will be confidential and reported in the aggregate. Your name or any other identifiable information will neither be collected nor be reported or published. There is a minimal risk in taking this interview. Discussion on governance in general, governance in health sector, and gender in governance is a sensitive discussion in many local contexts. Issues related to cor-ruption and poor governance may come up in your response which may not be viewed appropriately by your employer if these become known to the employer. In addition, you will spend 15 minutes in taking the survey which you could use otherwise.

53 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
You may not receive any direct benefit by responding to this survey. If you have any questions about this survey, feel free to contact Mahesh Shukla, Senior Technical Adviser, Leadership, Management, and Governance Project, Management Sciences for Health, 4301 N. Fairfax Drive, Suite 400, Arlington, VA 22203 United States (Telephone +1.703.310.3479 direct, +1.202.386.1164 mobile, fax +1.703.524.7898, email [email protected], skype mahesh.shukla8). The survey will take you about 15 minutes. To begin the survey, please continue to the next page.
Thank you again for your work to enhance health gains in nations and communities across the world.
Best Regards,
James A. Rice, Ph.D.Project DirectorLeadership, Management, and Governance ProjectInspired Leadership. Sound Management. Transparent Governance. Management Sciences for Health4301 N. Fairfax Drive, Suite 400Arlington, VA 22203United [email protected]: 1 612 703 4687Skype: jamesrice123Fax: +1.703.524.7898
1.Which of the following are foci of your work?
No YesClinical and curative medicineHIV/AIDSMalaria Tuberculosis
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 54
No YesMaternal healthChild health NutritionFamily planning and Reproductive health Neglected tropical diseasesChronic diseasesHealth service delivery Human resources for healthHealth information systemMedical products, vaccines and technologiesHealth systems financingLeadership and governance
Other (please specify) _____________________
2.What is your gender?
– Female
– Male
3.In which sector do you predominantly work?
– Public
– Private
– Civil society
– Other
4.At which of the following levels do you work? (check all that apply)
– Local
– State (or a province)
– National
– Regional (a group of nations)
– Global
– Other Other (please specify) _________________________________________
55 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
5.In which country do you live?Drop-down menu of the countries
6.For which country/countries do you predominantly work?OECD countries (Australia, Austria, Belgium, Canada, Chile, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Japan, Korea, Luxembourg, Mexico, Netherlands, New Zealand, Norway, Poland, Portugal, Slovak Republic, Slovenia, Spain, Sweden, Switzerland, Turkey, United Kingdom, and United States)
Non-OECD Countries
7.Please check all that apply
No YesDo you govern?Do you observe others govern?Do you manage?Do you lead?
Defining governance and effective governance in the context of health 8. This question seeks to find out what governing means to you in practical terms. Indicate the degree to which you consider each of the following is a part of the governing process?
Option is not
relevant
Is not a part of
governing at all
Is a slightly significant
part of governing
Is a moderately significant
part of governing
Is a highly significant
part of governing
To identify a policy problem, to advocate policy, to set policy agenda, to have a policy dialogue, to decide a strategic direction, to analyze policy options, to make sound policies, and use continual learning in refining and adapting policies for the future ('to steer')
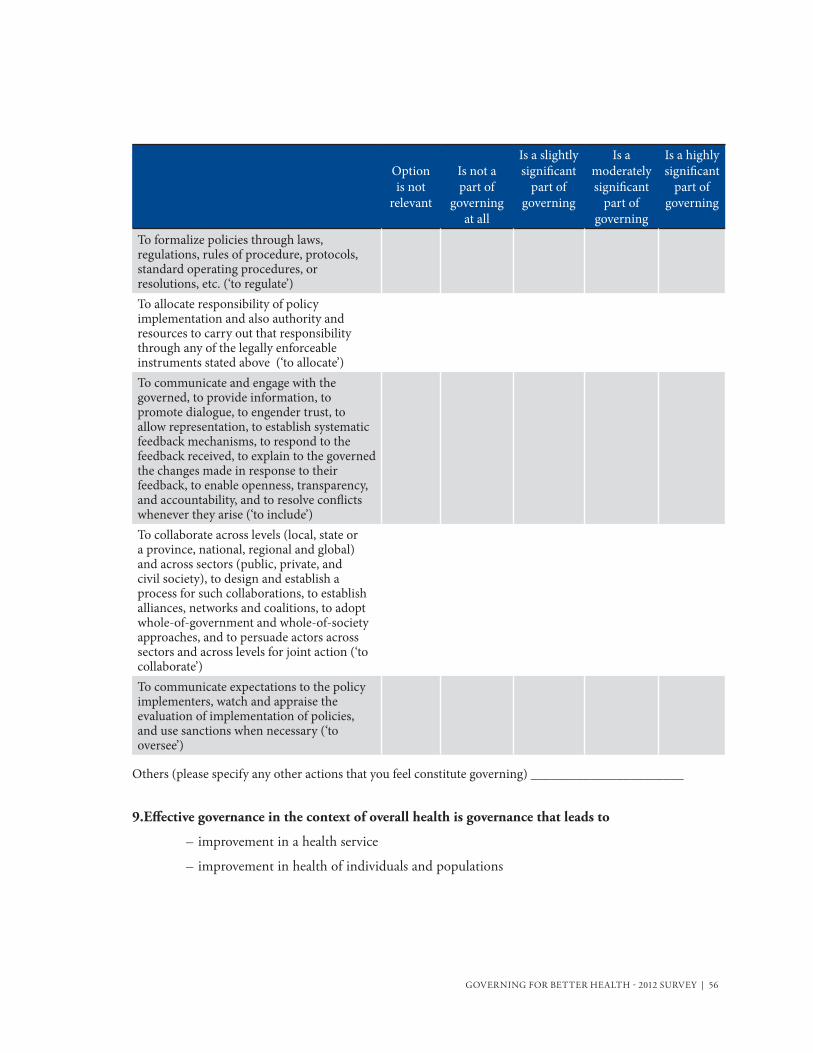
GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 56
Option is not
relevant
Is not a part of
governing at all
Is a slightly significant
part of governing
Is a moderately significant
part of governing
Is a highly significant
part of governing
To formalize policies through laws, regulations, rules of procedure, protocols, standard operating procedures, or resolutions, etc. (‘to regulate’) To allocate responsibility of policy implementation and also authority and resources to carry out that responsibility through any of the legally enforceable instruments stated above (‘to allocate’)To communicate and engage with the governed, to provide information, to promote dialogue, to engender trust, to allow representation, to establish systematic feedback mechanisms, to respond to the feedback received, to explain to the governed the changes made in response to their feedback, to enable openness, transparency, and accountability, and to resolve conflicts whenever they arise (‘to include’) To collaborate across levels (local, state or a province, national, regional and global) and across sectors (public, private, and civil society), to design and establish a process for such collaborations, to establish alliances, networks and coalitions, to adopt whole-of-government and whole-of-society approaches, and to persuade actors across sectors and across levels for joint action (‘to collaborate’) To communicate expectations to the policy implementers, watch and appraise the evaluation of implementation of policies, and use sanctions when necessary (‘to oversee’)
Others (please specify any other actions that you feel constitute governing) _______________________
9.Effective governance in the context of overall health is governance that leads to
– improvement in a health service
– improvement in health of individuals and populations
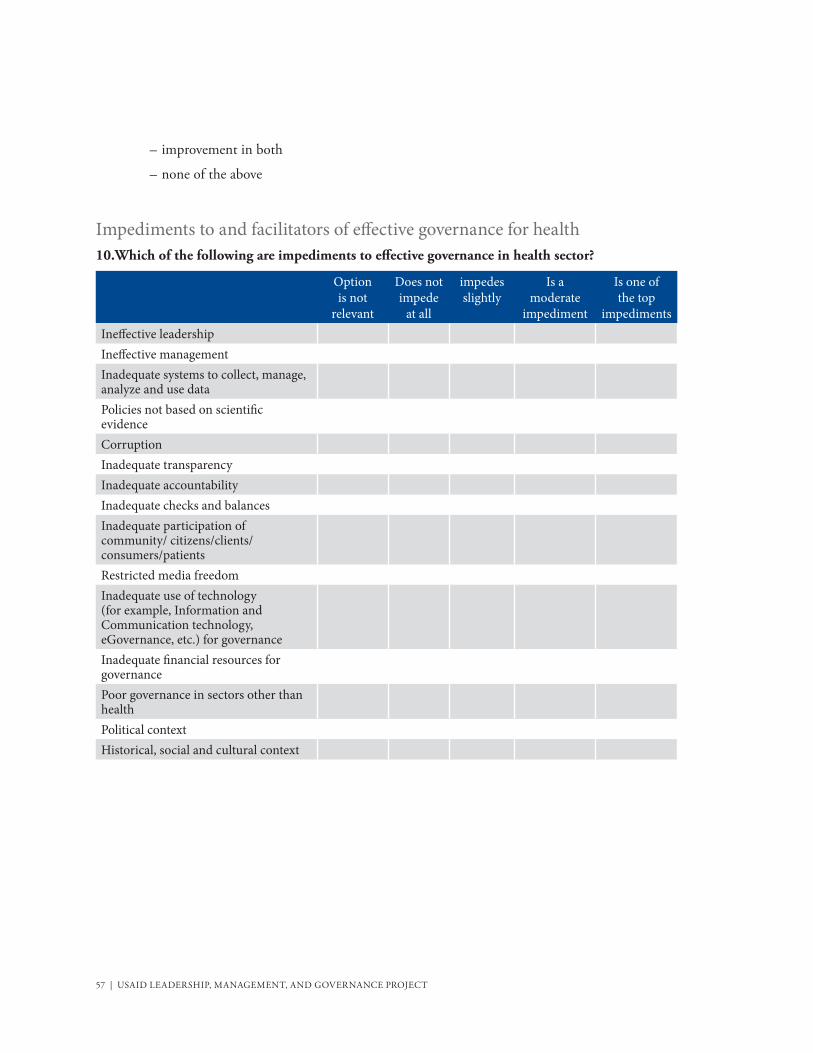
57 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
– improvement in both
– none of the above
Impediments to and facilitators of effective governance for health10.Which of the following are impediments to effective governance in health sector?
Option is not
relevant
Does not impede
at all
impedes slightly
Is a moderate
impediment
Is one of the top
impedimentsIneffective leadershipIneffective managementInadequate systems to collect, manage, analyze and use dataPolicies not based on scientific evidenceCorruptionInadequate transparency Inadequate accountabilityInadequate checks and balancesInadequate participation of community/ citizens/clients/consumers/patientsRestricted media freedomInadequate use of technology (for example, Information and Communication technology, eGovernance, etc.) for governanceInadequate financial resources for governancePoor governance in sectors other than healthPolitical contextHistorical, social and cultural context

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 58
Table 14: Indicate whether you believe each of the following leads to an improvement in a health service and health:
Does not lead to improvement
in a health service and
health of individuals and
populations
Leads to an improvement
in a health service
Leads to an improvement in health of individuals
and populations
Leads to an improvement
both in a health service and health of individuals
and populations
Governing in health sector with ethical and moral integrity
Governing in health sector with a definite policy on measurement, data gathering, analysis, and use of information for policy making
Governing in health sector based on scientific evidence
Governing in health sector in a free media environment
Governing in health sector in open and transparent manner
Governing in health sector with client/community participation in decision making process
Governing in health sector with accountability to citizens/clients
Governing in health sector with checks and balances
Competent leaders governing in health sector
Sound management of health sector
Governing in health sector using technology (for example, Information and Communication technology, eGovernance, etc.)
Adequate financial resources available for governing in health sector
Good Governance in sectors other than health
Other important outcomes (please specify):
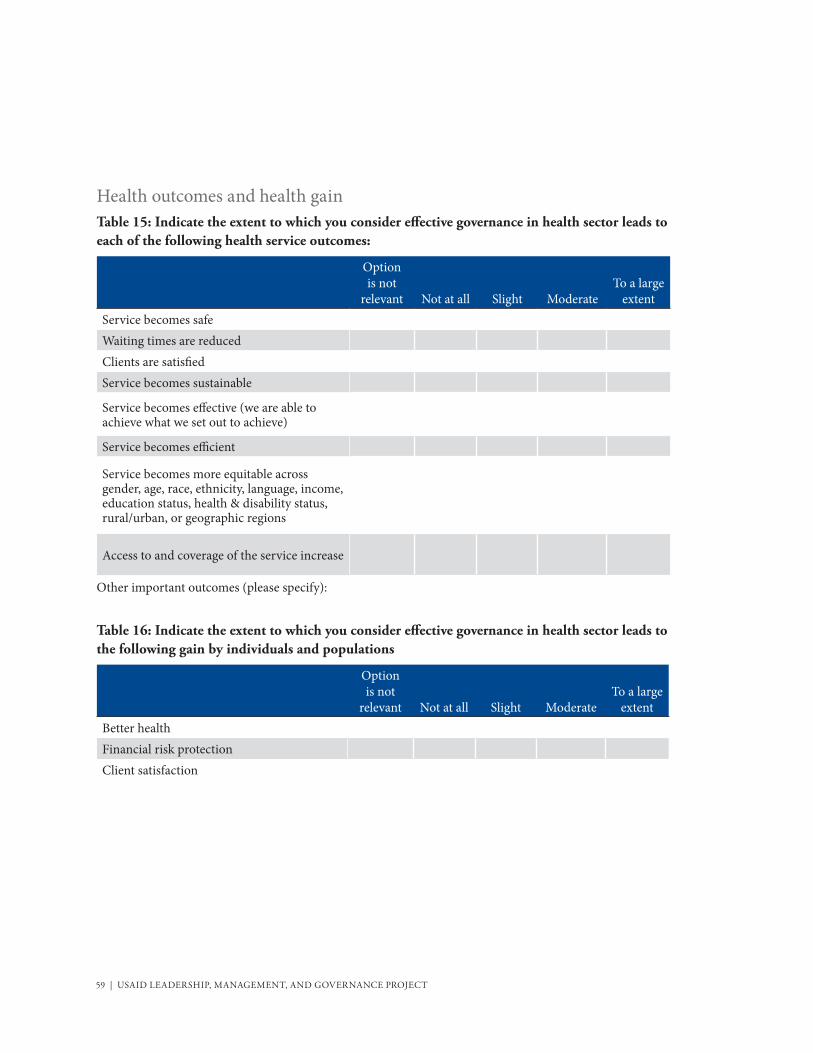
59 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT
Health outcomes and health gain Table 15: Indicate the extent to which you consider effective governance in health sector leads to each of the following health service outcomes:
Option is not
relevant Not at all Slight ModerateTo a large
extentService becomes safeWaiting times are reducedClients are satisfiedService becomes sustainable
Service becomes effective (we are able to achieve what we set out to achieve)
Service becomes efficient
Service becomes more equitable across gender, age, race, ethnicity, language, income, education status, health & disability status, rural/urban, or geographic regions
Access to and coverage of the service increase
Other important outcomes (please specify):
Table 16: Indicate the extent to which you consider effective governance in health sector leads to the following gain by individuals and populations
Option is not
relevant Not at all Slight ModerateTo a large
extentBetter healthFinancial risk protectionClient satisfaction

GOVERNING FOR BETTER HEALTH - 2012 SURVEY | 60
Table 17: Indicate the extent to which you consider effective governance in sectors other than health sector leads to the better health of individuals and populations.
Not at all Slight ModerateTo a large
extent
Table 18: Indicate whether you agree or disagree that each of the following statements is true:Strongly disagree Disagree Neutral Agree
Strongly agree
Leadership influences governance.Leadership influences management.Governance influences management.Governance influences leadership.Management influences governance.Management influences leadership.Effective leadership is a prerequisite for effective governance.
Effective leadership is a prerequisite for effective management.
Effective governance is a prerequisite for effective management.
Effective governance is a prerequisite for effective leadership.
Effective management is a prerequisite for effective governance.
Effective management is a prerequisite for effective leadership.

61 | USAID LEADERSHIP, MANAGEMENT, AND GOVERNANCE PROJECT

The USAID Leadership, Management, and Governance project is a five-year cooperative agreement with a funding ceiling of $200 million and is able to accept funding from all accounts. Missions and bureaus may access these state-of-the-art services and receive technical oversight and leadership from LMG through field support or sub-obligations on an annual or multi-year basis.
The LMG Consortium is also engaging with private sector partners to increase the impact of our activities and interventions, in particular to strengthen the capacity of our local partners to serve as stewards of the health systems and institutions they lead.
For further information, and to explore options for requests to address critical health leadership, management and governance challenges and needs in your country, please contact:
AOTR, Brenda Doe, GH/PRH/SDI202-712-1955, [email protected]
MSH Project Director Jim Rice612-703-4687, [email protected]