Embed Size (px)
Citation preview

Goodman et al. Chapter 16
Living with Race and Racism

Race and Health Disparities 1
• Epidemiology is the study of health patterns at the population level and is a subfield specialty of
demography (the study of people at the population level).
• There are many factors that affect one’s likelihood of becoming ill (the can be genetic, environmental
or social).
• It is with social epidemiology that we explore how social factors influence the patterns of health and
illness in populations.
• Race has real, and measurable, impact on disease (morbidity) and death (mortality), the two areas
studied by epidemiologists).
• While the race-as-biology concept is unreal, the concept that race and racism have biological
consequences is real.
• Racing and racism show effects prenatally. They may even go back further if the epigenetic data
is correct.
• The experiences of living with racism can negatively affect you.
• One such example is obvious. It was the Tuskegee Experiment.
• It was not until July of 1972 that Americans began to learn what had happened:
• Starting in 1932, 400 poor black Alabaman men were studied by the Public Health Service.
• The study consisted of leaving this men untreated and watching them die.
• Even after penicillin, the first known cure, was being used in 1947, they were left untreated.
• Many of the wives and children of these men were also infected.
• President Clinton apologized in 1973, the Office for Human Research Protections (OHRP)
was formed, as were Institutional Review Boards (IRBs)
• This case of medical abuse in not as isolated as we would wish to think, race becomes the basis for
the treatments which individuals receive, and it also affects what resources the person brings into
treatment.

Race and Health Disparities 2
• Health is patterned by race and class.
• We can explain the persistence of health disparities in the U.S. at least partially to race, but
also to class and even gender.
• This means that disease differs by both social disparity and economic disparity.
• Being poor means fewer health care opportunities, fewer changes for preventative
medicine.
• So it is not surprising that the poorest health statuses are found among poor women of color.
• The case for low birth weight
• Low birth weight is the number 1 predictor of perinatal (1st 28 days) and neonatal (1st year)
mortality.
• For decades, on average, African American babies have been 1 pound lighter than
EuroAmerican babies.
• Also, the number of low birth weight African American babies (<5 pounds, 8 ounces) is
double that of EuroAmerican babies.
• These birth weight differences are not genetic.
• These birth weight differences are due to inequality and racialized lives.
• The case for high birth weight
• Another health issue is high birth weight (> 8 pounds, 13 ounces).
• Among the factors that can increase birth weight are diabetes and high blood pressure (HBP).
• Minority populations exhibit greater numbers with diabetes.
• A higher percentage of African Americans suffer HBP and onset is earlier.


Race and Health Disparities 3
• Life expectancy: Death: The longer you live, the longer you live
• Life expectancy mostly increases as a population decreases child mortality.
• In America (in 2014, best year for life expectancy):
• Native Americans: 75.06 years; African Americans: 75.54 years; White Americans: 79.12 years;
Hispanic Americans: 82.89 years; Asian Americans: 86.67 years.
• By sex, women live longer than men in the U.S.
• Today, women outlive men in EVERY country, according to the WHO.
• In 1820, for both sexes, life expectancy was <40. Many lived longer; children were dying.
• In the U.S, life expectancy is down. [Drug overdoses and suicides up dramatically.] Globally we rank
33th.
• Race, discrimination and stress
• All organisms have mechanisms to respond to stress and to reestablish homeostasis.
• Stress, in a physiological context, is any factor that acts to disrupt homeostasis. The body’s response to
any factor that threatens its ability to maintain homeostasis.
• Homeostasis is a condition of balance, or stability, within a biological system, maintained by the
interaction of physiological mechanisms that compensate for changes (both external and internal).
• The stress response occurs the same way regardless of the type of stressor.
• Stress is a part of our daily lives and not a special set of responses. The generic nature of this set of
responses is called the general adaptation syndrome.
• The general adaptation syndrome is characterized by physiological activities that: 1) increase energy
availability; 2) inhibit long-term growth or maintenance of activities; 3) blunt pain; and 4) sharpen
memory.
• Overall, this set of responses is intended to maintain crucial functions.
• The stress response occurs the same way regardless of the type of stressor.


Race and Health Disparities 4
• Race, discrimination and stress (continued)
• The Whitehall studies are a classic example of how health is linked to stress and socioeconomic
status.
• Beginning in 1967, the Whitehall studies looked at civil servants because the British civil service is
highly stratified.
• They found that the highest classes had the highest levels of health. Overall, death rates were 4X
higher in the lower classes.
• Several hypotheses tried to explain these findings:
• Lower status persons had less access to health services [Nope all had universal access to health
care.]
• Lower status persons engage in riskier behaviors (smoking, drinking, eating fatty foods, not
exercising). [Explained less than 1/3 of the differences.]
• Those who are unhealthy are socially downwardly mobile, those healthier were upwardly
mobile. [Found to have a very small contribution to the explanation.]
• The poor are genetically predisposed to illness. [No such evidence was found.]
• The lived experience of inequality and the extent to which a country’s public policies elaborate
or attenuate social hierarchies. They include: One’s relative wealth and status; social cohesion
and social participation; and sources of social support.
• Krieger and Sidney, in 1996, developed a survey that documented racism in 7 situations.
• Their findings showed that 77% of black women and 84% of black men had experienced racism,
over ½ had experienced several of the situations.
• They then added in gender as a factor.
• They determined that when these factors compounded each other the result was chronic disease as a
constant struggle.

Race and Health Disparities 5
• Race, discrimination and stress (continued)
• There is a connection than between race, gender and
health status.
• Two examples include:
• African American women are more likely to suffer
from STDs (sexually transmitted diseases),
including AIDS.
• Also more likely to die from chronic diseases.
• Even though more white American women
contract breast cancer, black Americans are
more likely to die of this cancer.• Latinas have the lowest health status of all ethnic groups.
• Access to health care and to health insurance to a strong degree explains why this is occurring.
• Another factor for Latinos may be the language barrier.
• The working poor face other obstacles to health care:
• Taking time off of work can be impossible or financially too high a cost.
• Finding/paying for child care is an obstacle.
• Transportation is yet another factor.
• According to PolicyLink, in early 2020, 12 million Americans are among the working poor; They have jobs but
remain under the poverty line.
• According to ASPE, the poverty line is $12,490 for an individual and about $25,750 for a family of 4 in 2019.
• The number of working poor is increasing. The recovery from the Great Recession is, to a large part, into lower
paying jobs for man
• According to NPR: 1) A total of Americans were under the poverty line was 38.1 million in 2018; and 2)
those “… who did not have health insurance rose from 25.6 million people in 2017 to 27.5 million in
2018. That included 4.3 million children” (para. 3).
0.0
5.0
10.0
15.0
20.0
25.0
Under 18 18 to 64 65 and over
Perc
enta
ge
Age group (years)
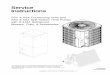
Figure 1: Percentage under poverty line by
gender and age group in 2011 (nf =
157,466,000; nm = 150,990,000)
Male
Female

Race and Health Disparities 6
• Black Americans who suffered the forced diaspora of the Middle Passage have high blood pressures
(hypertension, HBP); in fact they have among the highest globally.
• This is true even though the African populations from which they originated have among the lowest blood
pressures.
• One 1995 study of Africans from Nigeria and Cameroon with American and Caribbean blacks
demonstrated this.
• Even while they all shared a similar genetic history the numbers were very different.
• This strongly suggests the factor is not genetic, but cultural or physiological (stress).
• Why are there such differences between these populations?
• One explanation is labeled the slavery hypothesis.
• The argument is that Black Americans are more salt sensitive due to the effects of the Middle
Passage.
• The horrors of the Passage became a genetic bottleneck, causing by those less able to retain
water to die first from dehydration and diarrhea.
• There are problems with this idea:
• We know little about salt sensitivity in African populations.
• This explanation is not supported by data nor is it testable.
• But there is a link between hypertension and salt intake.
• The fits with the American diet, not just the Black American diet.
• Blacks do exhibit higher rates of hypertension, so salty diets may be more stressful.
• Others remind us that there are different types of hypertension.
• One part of the discussion is that many animals become hypertensive in the presence of high salt
diets.
• Thus the argument for hypertension levels in African Americans has to do with cultural practices.

Race and Health Disparities 7
• Race and hypertension: the cultural meaning of skin color
• The stresses of racism may also play a part in hypertension. There are several ways the cardiovascular
system is undermined by stress:
• Epinephrine causes spikes in BP that causes the heart to work harder and more pressure on the
blood vessels.
• Another way it interferes is through energy metabolism.
• Epinephrine stimulates glucose synthesis are maintained by a reduction in insulin.
• Increases blood glucose levels
• So fat levels are increased in the blood.
• Other cells are affected by the lowered insulin and become insulin resistant.
• These together heighten risks of diabetes and heart disease.
• Gravelee adds another component to the discussion: the color of one’s skin.
• He looked at this contribution to hypertension in Puerto Rico as it is linked to skin tone because:
• 1) The de facto explanation that skin color is a stand-in for African admixture.
• 2) Dark skin signifies lower status in PR.
• He measured skin color by use of a skin reflectance spectrophometry and by use of social
categories.
• Through ethnographic interviews he was able to identify a set of categories.
• Lighter categories: Blanco/a, Trigueño/a, Indio/a and darker categories: Jabao/a and Negro/a.
• These ascribed (status one is born with) colors are not linked to skin color; one’s SES was most
revealing SES (socioeconomic status) is one’s position in the social and economic hierarchy or level
of prestige. Occupation, education and/or income are most often used markers of one’s place.
• Being darker in low SES had little effect on HBP.
• Being darker in middle/higher SES means being black in a white world: high stress, high HBP.

Race and Health Disparities 8
• Environmental racism
• Exposure to pollutants and irritants obviously leads to poorer health and
is linked to environmental racism.
• Among the exposures are those linked to air quality, waste dumping,
and ground water contamination.
• According the 2007 report by the United Church of Christ Justice and
Witness Ministries (Toxic Wastes and Race 20):
• The single factor MOST predictor of where pollutants would be
located, in the United States, was one’s race.
• Hazardous-waste treatment and storage facilities more likely to be
found in minority neighborhoods
• People of color more likely to live in areas where the air pollution
levels to not meet the EPA standards.
• One’s race as a predictor was higher than household income, house
value, and the estimated amount of pollutants generated by the
industry.
• The Toxic Wastes and Race 20 report also reported that:
• Nine million Americans live within 1.8 miles of 413 commercial
hazardous facilities. Another 5.1 million people of color live in
neighborhoods with at least one commercial hazardous waste facility.
• Neighborhoods with higher clustering tend to be neighborhoods of
color and are areas of higher poverty (more disease risks).
Air pollution in China
Computers in Nigeria
Fracking in U.S.

Race and Health Disparities 9
• BiDil and race in medicine
• In 2005 the U. S. Food and Drug Administration (FDA) re-inscribed race as
a surrogate for genetic diversity.
• In the same year, FDA approved the first drug aimed at heart failure
treatment for African Americans: BiDil, produce by NitroMed of
Massachusetts.
• Some suggest this move was to get past the expiration date for the
drug by combining 2 drugs (isosorbide dinitrate & hydrochloride) and
‘repackaging’ as an exclusive use.
• The NitroMed stance was that this drug combo would enhance nitric
oxide levels and so increase vessel dilation (and so blood flow).
• But this combination of drugs was not tested to determine if it worked
better for blacks. In 2005 the U. S. Food and Drug Administration (FDA)
re-inscribed race as a surrogate for genetic diversity.
• an for other groups.
• At the FDA hearing the counterargument was that this drug was
targeting a very diverse group of Americans (being black is not a race).
• The FDA countered back and said that Blacks self-identified and so
represented a heterogeneous group of peoples but a real one.
• Assumes that there is some “Black biology’ or pathway that is
being targeted.
• Pushes the biology explanation rather than the social one,
‘naturalizing’ the explanation.
• This looks to be the start of ‘racial medicine’. It would be more useful to
do studies to see if there is a real difference or even if it is as effective in BiDil ad (note the tie)
BiDil bottle

Race and Health Disparities 10
• Should race be used in medical research?
• Many medical research studies are REQUIRED to collect data on race.
• The NIH (National Institutes of Health) as one of the largest funders of medical research
requires this data.
• The White House Office of Management and Budget (OMB) also require even as they admit
they are not scientific.
• Some reasons for using race make sense, and some do not.
• Research that looks for racial disparity in health has its uses.
• Research that looks at race these ways does not make sense as a substitute for social
environment, ancestry, or genetics
• Ancestry, not race, determines risks for genetic diseases.
• Sickle cell disease we discussed extensively in an earlier chapter.
• Cystic fibrosis (a disease of the mucus glands) is found most commonly in persons of northern
European ancestry. But one is white if ancestors are from southern Europe (and not the Middle
East).
• According to the Cystic Fibrosis Foundation website, “about 30,000 children and adults in the
United States (70,000 worldwide)” (para. 1).
• The survival rate is going up with new treatments, but life expectancy is the late-30s.
• Tay-Sachs disease is found in the general population the value is about 1 in 500,000 births, but
among Ashkenazi Jews of Eastern Europe it is 1 in 2,500 births• Tay-Sachs is a deadly disease caused by a lethal recessive allele that is associated with lipid
storage.• Death is usually in the first few years of life.

Race and Health Disparities 11
• Concepts of race, practices of racism (Susan Reverby)
• Reviews the stereotypes for what she calls the “black body” and further explores the “medical lust”
linked to this perception.
• She quotes an 1838 advertisement looking for American slaves that would be used in
experimentation (p. 224).
• She reminds us of the Tuskegee Experiments of the 1932-1972 and expands on the history.
• She reminds us that persons of lower SES are more likely to be willing to volunteer for
experiments and other studies.
• She states an “entire health industry now exists that has documented differences in kinds of
services, interventions, and care offered to patients that breaks down to racial lines” (p. 225).
• These differences are linked to overcrowding and poor housing, as well as access issues such
as health care resources and food deserts.
• Poor people are disadvantaged in their access to food and health care.
• Food deserts are places where access to healthy foods is limited.
• Many large supermarkets are uninterested in locating in low income areas so mom-and-
pop stores dominant (and so costs are higher)
• How mush money is spent on food differs by income.
• Our willingness to racialize medicine is evidenced by BiDil.