Embed Size (px)
Citation preview

The Normal Knee JointThe knee is formed by the lowerend of the thigh bone (femur) resting on the upper end of theshin bone (tibia) with the kneecap (patella) at the front. To provide stability in all directions, ligaments join the bones, bothinside and outside the joint space.
The important ligaments thatstabilise the knee joint are: ■ the medial collateral ligament,which runs from the femur to thetibia on the inner side of the leg.■ the lateral collateral ligament,which runs from the lower femur tothe upper fibula on the outside of theleg; these collateral ligaments pre-vent sideways movement of the joint.■ the anterior cruciate ligament,
which extends from the under sur-face of the femur at the back andcrosses down to attach to the uppersurface of the tibia at the front.■ the posterior cruciate ligament,
which comes from the under sur-face of the femur at the front andcrosses down to attach to the uppersurface of the tibia at the back. ■ the medial and lateral menisci,which are C-shaped discs of carti-lage located on the upper surface ofthe tibia. The medial meniscusrests on the inner portion of theupper tibia and the lateral menis-cus on the outer portion. Actingas shock absorbers, they are
mobile and help to stabilise theknee.■ the patellar tendon, whichattaches the lower end of the patella to the front of the tibia. Thepatella is attached at its upper endby strong muscles on the front ofthe femur.
The load-bearing surfaces of thefemur, tibia and patella are coveredby articular cartilage. This is asmooth, tough tissue that acts as acushion, allowing the bones to glideeasily on each other.
A thin envelope of fibrous tissue,called a capsule, surrounds theknee joint. This is lined by a thinmembrane that produces lubricat-ing or “synovial” fluid to furtherreduce friction in the joint.
K nee arthroscopy is a common procedure thatorthopaedic surgeons use to examine and treatthe inside of the knee joint. An arthroscope, a
thin fibre-optic telescope about the width of a pencil, ispassed into the joint through a small incision at the outerside of the knee. This is done under an anaesthetic.
A camera is attached to the arthroscope, and a clearview of the inside of the joint can be seen on a video monitor. This allows your surgeon to examine all areasinside the joint. Usually a diagnosis can be made.Depending on the diagnosis, your surgeon may be able totreat a number of abnormalities during the same procedure.
Arthroscopic surgery has become a routine proce-dure. The incisions are much smaller, which assists fasterhealing and lowers the risk of complications.
Most arthroscopies can be done as a day procedure.This reduces the problems that can occur with prolonged bed rest and lack of mobility, such as bloodclots and chest infections.
Knee ArthroscopyA G U I D E F O R PAT I E N T S
Edition number: 3
Lateralmeniscus
Lateralcollateralligament
Patellarligament Fibula Tibia
Patella
Femur
Medial meniscus
Medial collateral ligament
Posterior cruciate ligament
Videomonitor
Arthroscope
Incision
Light
Femur
Articularcartilage
Surgicalinstrument
Anterior cruciate ligament
IMPORTANT: Fill in all details on the sticker below.
DEAR SURGEON: When you discuss this pamphlet with your patient, remove this sticker and put it on the patient's medical history or card. This will remind you and the patient that this pamphlet has beenprovided. Some surgeons ask their patients to sign the sticker to confirm receipt of the pamphlet.
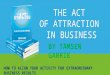
The arthroscope is inserted into the articular cavity.
Normal anatomy of the knee
AOA
A U S T R A L I A N O R T H O PA E D I C A S S O C I AT I O N
New Zealand Orthopaedic Association
Crest or
logo
Full colour anatomical
illustrations helpthe patient
understand theneed for surgical
treatment
Popular piggy-back stickerconfirms that the
patient did receivethe pamphlet
What’s in aname?...
authority andcredibility
Text and illustrationsextensivelyreviewed by
experts
“Hardcopy” pamphlet allows
patients to reviewtreatment informa-
tion after the consultation

A fter the anaesthesia is started, a tourniquet may beplaced around the thigh to stop blood flow through
the leg for a short period. This allows the surgeon to workin a virtually blood-free area, greatly improving visibility ofknee structures during the arthroscopic procedure.
The arthroscope is inserted through an incision on theouter side of the knee joint. Small operating instruments,ranging in width from three to five millimetres, are theninserted through one or two other incisions on the innerside of the knee.
The surgeon manipulates these instruments whilelooking at the video monitor. You may be able to watch theprocedure on the video monitor.
At this time, diagnosis, repair, reconstruction orremoval of damaged tissue can often be performed.Depending on the extent of the operation, the procedureusually takes from 45 minutes to two hours.
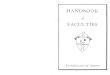
Repairs during ArthroscopyTears to the medial or lateral menisci: A tear tothe medial or lateral meniscus is usually caused by a twist-ing injury. Pain is felt on the inner or outer side of theknee, and there may be swelling of the joint with difficulty
moving it. Sometimes the joint will “lock” if the torn segment becomes caught between the bones. The tearshave a variety of names, based on their appearance.
Before Surgery
Y our surgeon needs to know yourmedical history, so it is important
to disclose all your health problemsand symptoms. Some health prob-lems may interfere with surgery,anaesthesia, sedation and care aftersurgery.
Tell your surgeon about:■ any allergy or bad reaction to
medication■ your smoking history; smoking
interferes with healing, so quit atleast two weeks before surgery
■ ALL medications you are taking,including insulin, warfarin orother blood thinning agents, orNSAIDs such as aspirin or ibupro-fen, among others
■ any history of a bleeding disorder,easy bruising, deep vein thrombo-
sis or pulmonary embolism■ recent illnesses, including recent
infections■ long-term illnesses and lung or
heart conditions.Your surgeon may advise you to
stop taking aspirin and other anti-inflammatory medication before surgery because they can increasethe risk of bleeding.
If required, paracetamol-basedpainkillers can be used. Continue totake your other medications unlessyour surgeon advises otherwise.
As the muscles of the knee jointare important to its function, yourrecovery after surgery is likely to beenhanced if these muscles are ingood shape. Exercises to helpstrengthen the thigh muscles beforeand after surgery are important.
Your surgeon will advise you aboutthe best exercises to prepare you forsurgery.
Also, on the day of surgery, youneed to fast (nothing to eat, drink orsmoke) for six hours before the oper-ation. Your surgeon may give youadditional instructions.
AnaesthesiaAn arthroscopy is performed:■ usually under a general anaes-
thetic (you are asleep)■ sometimes under a regional
anaesthetic (the whole leg is anaesthetised)
■ rarely under a local anaesthetic(only the knee is anaesthetised).Your anaesthetist can provide you
with more information about theanaesthesia best in your case.
The Injured Knee
T he knee joint can be easilyinjured, especially during sports
or work that requires twisting move-ments, sudden stopping and starting,changes in direction, and collisionswith other players. Osteoarthritis(wear-and-tear arthritis) is a commonsource of symptoms. As cartilagebecomes less supple with age, relatively minor trauma in older people may result in significant damage to the knee joint.
Common signs and symptoms ofan injured knee are swelling, persistent pain, catching or lockingduring certain movements, and “giving way” unexpectedly. If thesedo not improve with medical andphysiotherapy treatment, anarthroscopy is often recommended.
Physical examination of the kneejoint and X-ray examination are usu-ally performed before arthroscopyand may result in a diagnosis. Yoursurgeon may request an MRI or CT
scan prior to surgery if more information is needed. However, thesurgeon may not know beforehandwhether corrective surgery will bepossible at the time of arthroscopy.When the extent of the damage isseen through the arthroscope, thesurgeon can plan the most appropri-ate type of surgery.
Although not all types of kneeinjuries can be repaired duringarthroscopy, many conditions can betreated with arthroscopic surgery.
Procedures during Arthroscopic Surgery
Continued on page 3
Arthroscope
Light
Repair of medial meniscus tear
Operating instrument
Cross-section of arthroscopic surgery
Written in plainEnglish and easy to
discuss withpatients
Easy to ensurethat the patient
leaves the consultation with
treatment information
Printed in fullcolour on highquality paper
stock
High quality communications
enhance the doctor-patient relationship and
are the cornerstone of effective patient
educationHealth and
treatment informationfrom the web is oftenincomplete or wrong,
and may require a highlevel of education to
understand

Unless the tear is very small, it isunlikely to heal on its own. If untreat-ed, it will usually continue to catch inthe knee, resulting in long-term irritation and damage. This can leadto osteoarthritis over time.
Surgeons recommend removal ofthe torn piece to relieve pain andmechanical symptoms, and allow theknee to return to normal or near-normal function. The entire menis-cus is not removed, as this is morelikely to lead to early osteoarthritis.However all the damaged cartilagemust be removed or symptoms willpersist. In some younger people witha specific type of tear, the surgeonmay repair the damaged meniscus, ifpossible. After this procedure, thepatient must wait for three to sixmonths to allow enough time forhealing before returning to sports.
Damaged articular cartilageand the removal of loose fragments: Damage to the surface cartilage increases the friction in aknee joint and decreases its shock-absorption ability. If large pieces ofcartilage are floating inside the kneejoint, particularly if they are attachedto a bone fragment, the joint maylock. These “loose bodies” cause further damage to the joint surfacesand osteoarthritis, which will worsenwith time. The aim of surgery is to smoothen rough edges of thearticular cartilage and remove loosedebris.
Reconstruction of the anteriorcruciate ligament: A rupture of the anterior cruciate ligament (orless commonly, the posterior cruciate ligament) usually needs surgical reconstruction. An untreat-ed rupture makes the knee perma-nently unstable. See the AOA’spatient education pamphlet“Surgical repair of the anterior cruciateligament – a guide for patients”.
Treatment of the patella: Many patellar problems can be treatedwith physiotherapy and exercises.Surgery may be needed if these fail
to relieve symptoms. A conditioncalled mal-tracking may be treated byarthroscopic surgery. The “lateralrelease” procedure to correct mal-tracking often results in signifi-cant knee swelling and soreness,which can take about three monthsto settle.
Damage to the articular cartilageof the patella can be treated bysmoothing, but the surface cannotbe restored to normal.
Removal of inflamed joint membranes: Some inflammatory conditions, such as rheumatoidarthritis, result in an excess of synovial fluid being produced in thejoint due to inflammation of the finejoint lining. Removal of some of thistissue (synovectomy) can improvefunction and reduce pain. This operation normally requires a day ortwo in hospital because a small draintube is left temporarily in place tohelp drain the wound.
Washout of an infected kneejoint: A sterile solution is used to fill an infected knee joint and flush awaypus, infected fluid and other debris.
Cartilage grafts: Newer tech-niques that involve transplanting cartilage cells into areas of lost ordamaged tissue are being developed.These methods are currently beingused in younger people.
A technique called autologous chondrocyte grafting involves remov-ing cartilage cells from the damagedknee before sending them to a laboratory where they are grown inculture until they have multiplied intomany cells. The cell-culture mix isplaced into the area of damage,resulting in resurfacing by the cells;open surgery is usually used.
This second procedure requiresan arthrotomy (long incision) to gainentry to the joint and the site for graft-ing. It is only suitable if a defect needsto be filled. This treatment is usuallyconfined to patients less than 45 yearsold and can be expensive.
This pamphlet is intended to provide youwith information. It is not a substitute for
advice from your surgeon and does not con-tain all the known facts about arthroscopy.
It is important that you have enoughinformation about arthroscopy to enable youto compare the benefits and risks. If you arenot sure about the benefits, risks and
limitations of treatment, or the terms used inthis pamphlet, or anything else, ask your surgeon.
Be sure to read all the information in thispamphlet. Some technical terms are used thatmay require further explanation by your surgeon. Write down questions you want to
ask, and discuss them with your surgeon. Youare encouraged to fully discuss with your surgeon:■ the results you want■ the surgery to be done and why■ the outcome you can expect.
This pamphlet should be used only inconsultation with your surgeon.
Removal of cysts: A cyst is a fluid-filled sac. Cysts that arisebehind the knee are called Baker’scysts or popliteal cysts and may develop if menisci are torn or articular cartilage is worn. Oncethese conditions are repaired, thecyst usually disappears or reduces insize and does not need surgicalremoval itself. Usually cysts are notharmful. If they cause no symptoms,they typically do not require treatment.
Common types of injuries to menisci
Femur
“Parrot beak” tear
Flap Radial tear
“Bucket handle” tear
Calfmuscles
Poplitealcyst
Medialmeniscustear
Talk to Your Surgeon
A high quality medical
illustration may be crucial to
a patient’s understanding
Good communication
improves patients’realistic
expectations andcompliance
Full-colour medical illustrations
are more easily understood than grainy
black-and-white drawings and line
drawings
An educational pamphlet helps the
patients to rememberboth the good news and bad news about
diagnosis and treatment

This pamphlet, or portions of it, should not be photocopied and handed out, nor reproduced in any electronic format. ©
PossibleComplications ofKnee Arthroscopy
M odern arthroscopy is safe butdoes have risks. All surgical
procedures have some degree of risk.Despite the highest standards of surgical practice, complications arepossible.
It is not usual for a doctor to out-line every possible side effect or rare complication of a surgical procedure.However, it is important that you haveenough information about possibleside effects to fully weigh up the benefits and risks of surgery.
Most people having arthroscopywill not have complications, but if youhave concerns about possible sideeffects, discuss them with your surgeon. It may be helpful to preparea written list of issues and questions todiscuss with your surgeon.
The following possible complica-tions are listed to inform and not toalarm. There may be other possibleside effects that are not listed.
Some risks associated with thistype of surgery include:
■ Infection. If you develop a fever,chills, persistent or increasing pain orswelling in the knee, infection may bepresent. Infection can be a seriousorthopaedic emergency. Your sur-geon should be contacted at once,
and intervention will be undertaken.■ Uncommonly, persistent bleedingfrom the wound or bleeding into theknee or into the leg.
■ Blood clots in leg veins that cantravel to the lung. Any pain orswelling in the calves of the legs, orshortness of breath, or chest pain within 10 to 14 days of your surgeryshould be reported to your surgeon.
■ Stiffness. Follow your surgeon’sinstructions regarding exercising theknee to help prevent stiffness occurring.
■ Numbness of the skin near theincisions. This usually improves overtime. However, it may indicate damage to a nerve that may requirefurther treatment.
■ Injury to blood vessels and nervesis uncommon, but it may lead to achronic regional pain syndrome.
No surgeon can guarantee thatsurgical treatment during kneearthroscopy will always be successful.It may be that damage to the knee wasmore than was originally suspected,and surgery can only give partialrelief.
Arthroscopic surgery has limitedsuccess for knees with severeosteoarthritis or damage due to otherdiseases or injuries.
Recovery fromKnee Arthroscopy
A fter surgery, you are transferredto a recovery room before
returning to the ward. Most patientsare able to return home that day, butsome may have to stay in hospitalovernight for observation. You shouldnot drive and will need to be collected.
Some swelling in the knee is to beexpected and is best treated by elevat-ing your leg when seated for the firstfew days after surgery. An ice packapplied for 20 to 30 minutes every fewhours may help to reduce swelling.
A surgical dressing is used to coverthe incisions. The area should be keptclean and dry, so avoid soaking in abath or directing water at the incisions. A waterproof dressing isoften provided to allow for bathing.Showering is usually permitted if yoursurgeon agrees.
Weight bearing is usually possiblesoon after arthroscopic surgery.
Crutches or some form of weight support may be recommended byyour surgeon, depending on theoperation. Time on your feet is usual-ly restricted for the first two to threeweeks. If the knee keeps swelling, it isusually because you’re on your feettoo much.
Driving is possible once the kneefeels comfortable. This may be after24 hours or up to a week later,depending on the extent of surgery.
Exercises are important, as mostof the knee’s strength comes from themuscles surrounding it and not fromtendons or ligaments. You will notharm the knee by doing strengthen-ing exercises as recommended byyour surgeon or physiotherapist. Anexercise bike is often helpful duringrehabilitation.
If you are prescribed antibiotics,take the complete course as your surgeon advises. Painkillers may alsobe prescribed and should be taken asdirected.
Follow-up: Your surgeon will adviseyou about a follow-up visit andremoval of stitches. The length oftime off work depends on your levelof activity and should be discussedwith the surgeon. Usually, you canreturn to work once the knee feelscomfortable.
Most people are able to return tonormal daily activities in six to eightweeks. Any sport that involves signifi-cant weight-bearing stresses or twist-ing movements must be avoided untilapproved by your surgeon. Althoughcartilage and ligament repair oftenresults in a nearly normal knee, theknee does have an increased likeli-hood of developing arthritis in thelong term, so extreme weight-bearingactivities need to be modified.Exercises that have less impact onknees include swimming, cycling andwalking.
Maintaining a normal body weightand a healthy diet are also importantfor the long-term care of knees.
Your Surgeon
COSTS OF TREATMENT
Your surgeon can advise you about coverage by public or private health
insurance and out-of-pocket costs forarthroscopy. You may want to ask for an estimate that lists the likely costs. Thisincludes medical and surgical fees, and otheritems. Ask which costs can be claimed onpublic or private health insurance. You mayneed to contact the hospital or health fund.
As the actual treatment may differ fromthe proposed treatment, the final accountmay vary from the estimate. It is better todiscuss costs with your surgeon before treat-ment rather than afterwards.
Report to Your SurgeonTell your surgeon at once if you develop any of the following:■ temperature higher than 38˚C or
chills■ persistent bleeding from the
incisions■ severe pain, tenderness or
increased swelling in the knee■ nausea or vomiting■ any concerns you have regarding
your surgery.If your surgeon cannot be contact-
ed, attend your family doctor or nearest emergency department.
Editi
on n
umbe
r: 3
07D
ecem
ber2
010
Mi-t
ec M
edic
al P
ublis
hing
© T
elep
hone
: 613
988
8 62
62
Fac
sim
ile 6
13 9
888
6465
e
-mai
l: or
ders
@m
itec.
com
.au
w
eb o
rder
s: w
ww
.mite
c.co
m.a
u
These full-colour pamphlets have the
added security of the highest print quality,
which adds credibility,authority and reader
acceptance
In a Mi-tec survey of 400 surgeons,
five percent reported that a legal complaint or legalaction against them had been
abandoned because the patienteducation pamphlet clearly
outlined the risks and limitations
of the treatment
A pamphlet page can never go missing,unlike printouts from
laser printers
A list of the most relevant
possible complications
is crucial