-
8/13/2019 Glucagonoma Maligno
1/6
Glucagonomas are neuroendocrine tumours which
arise from -pancreatic cells and secrete glucagon andother
peptides. The annual incidence is extremely low,
only approximately 1 in 20 million, (1) and only 262cases have
been reported so far (2-5). Glucagonomas
are characterised by a slow growth rate even whenmalignant, and
have been reported in patients aged 19
to 72 years (6). The incidence is the same in males andfemales,
even though early reports suggested that they
predominantly occur in females (7). Approximately 60-80% of
glucagonomas are malignant and at least 50%
of them are metastatic at the time of diagnosis and
areconsequently associated with a poor prognosis. Metas-
tases occur primarily in the liver and in the peri-pan-creatic
lymph nodes. Most glucagonomas are sporadic,
but they can be associated with mutations in MEN1 or
familial adenomatous polyposis (8).
Glucagonoma diagnosis is based on positive clinicalfeatures with
biochemical findings of hyperglucago-
naemia and radiographic localisation of a pancreatic (orrarely
extrapancreatic) tumour. Abdominal computed
tomography (CT) and scintigraphic scan after intra-venous
administration of 111In-pentetreotide (Octre-
oscan
) are quite accurate and sensitive to detect andlocalize the
tumour and to identify hepatic metastases
(9-12). Surgery is the first treatment of choice and canbe
curative if the tumour is confined to the pancreas.
Cytoreductive surgery can also be used as palliativetreatment
when the tumour is disseminated (13,14).
Systemic chemotherapy is generally only met withlimited success
due to the unresponsiveness of this
tumour type (15). Somatostatin analogues are the first
J. Exp. Clin. Cancer Res., 25, 1, 2006 Case Report
135
Malignant Glucagonoma. New Options of Treatment
M. Appetecchia1, E. Ferretti1, M. Carducci2, F. Izzo3, L.
Carpanese4, F. Marandino5, E. Terzoli3.
Endocrinology Unit1, Department of Medical Oncology3, Department
of Radiology4 and Department of Pathology5; Regina Elena Cancer
Institute; Department of Dermatology2, San Gallicano Institute;
Rome - Italy
Few cases of malignant glucagonomas have been described in the
literature. In this paper we present a case of a77-year-old woman
with necrolytic migratory erythema and high plasma glucagon and
chromogranin A levelscaused by a neuroendocrine tumour. An
abdominal CT scan suggested a pancreatic lesion and two liver
metas-tases. The patient underwent pancreatic debulking and liver
metastasectomy. Histological and immunohisto-chemical
investigations revealed a well differentiated neuroendocrine tumour
with vascular invasion and scat-tered immunopositivity for
somatostatin receptors. The patient was treated with octreotide (20
mg i.m. every 28days) for three years without side effects. Three
months after surgery symptoms of disease recurred accompanied
by hyperglucagonaemia and newly diagnosed liver lesions. The
patient was treated with octreotide (30 mg i.m.every 28 days) and
interferon- (6 MU s.c. 3 times per week) plus three cycles of
hepatic chemoembolisation.Symptoms resolved after the first month
of therapy, hormone levels decreased compared to untreated levels
andmetastatic growth slowed as observed by radiographic evidence.
The patient is now asymptomatic with persis-
tent hepatic disease and normal serum glucagon levels forty
months after primary treatment. So far, only few
im-munohistochemical studies are reported on malignant glucagonoma
and combined treatment schedules. Wedemonstrated, for the first
time, a scattered immunopositivity for somatostatin receptors in a
malignantglucagonoma. For this reason, the somatostatin analogs
therapy was instituted. A combined antiproliferative med-ical
treatment and the hepatic chemoembolization have been able to
control tumor growth and disease symptomsfor a long time after
surgery.
Key Words: Glucagonoma, Immunohistochemistry, Somatostatin
analogues, Octreotide, Interferon-,Chemoembolisation
-
8/13/2019 Glucagonoma Maligno
2/6
choice for symptomatic treatment. Long-acting somato-statin
analogues result in disease stabilisation in 40% of
patients with metastatic gastroenteric endocrinetumours (16).
Interferon- has been shown to haveantineoplastic activity in 50-80%
of patients affected bycarcinoid tumours, due to its
anti-proliferative effect ontumour cells (17-21). Chemoembolisation
therapy for
metastatic neuroendocrine tumours has been demon-strated to
reduce tumour bulk and circulating hormonelevels, and to palliate
the symptoms of many patientswith liver-dominant metastases
(22,23).
In this report we describe a case of metastaticglucagonoma in
which the immunopositivity forsomatostatin receptors was clearly
demonstrated. The
patient was successfully treated with surgery followedby
combination therapy with somatostatin analoguesand interferon-, and
chemoembolisation of livermetastases.
Case Report
A 77-year-old woman presented with a desquamat-ing pruritic rash
in May 2001. She reported approxi-mately 10 kg of weight loss in
the past few months.Physical examination was suggestive of
necrolyticmigratory erythema and biochemical tests revealedhigh
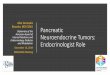
blood glucose levels. An abdominal CT scanrevealed a pancreatic
lesion and two liver metastases(Fig.1A). Two chest, abdomen and
pelvis single photonemission CT (SPECT) scans acquired at 24 and 48
hrs
and a whole-body scintigraphy scan using 111In-octreotide (111
MBq) showed abnormal uptake in asection of the pancreatic tail and
in two small areas inthe right lobe of the liver.
Endocrine work-up confirmed the suspected diagno-sis of
glucagonoma syndrome with high serum levels ofglucagon (566 pg/mL),
chromogranin A (460 U/L) andneuron specific enolase (59 ng/mL) at
diagnosis.
In July 2001, the patient underwent tumour debulk-ing and liver
metastasectomy. The cut section of the
pancreatic tail revealed two solid encapsulated lesions.The gall
bladder was also removed because of a non
specific nodular lesion. Histological examinationrevealed a
well-differentiated neuroendocrine tumourof the pancreas with
vascular invasion. The hepaticlesions showed the same features.
Chronic cholecystitiswith adenomyomatosis was found in the gall
bladder.
The histological sections were prepared forimmunohistochemistry
as follows. Tumour pancreaticand liver samples were routinely fixed
in formalin andembedded in paraffin. Serial 3 m sections were
cut
and mounted on protein-coated glass slides. The sec-tions were
immunostained with antibodies againstglucagon (rabbit polyclonal;
Dako), cytokeratin(MNF116; Dako), synaptophysin (SYN38;
Dako),chromogranin A (DAK-A3; Dako), neuron specific
enolase (rabbit polyclonal; Dako), somatostatin recep-tor
subtypes 2 (SSTR2) and 5 (SSTR5) (rabbit poly-clonal kindly
provided by Professor A. Spada from theUniversity of Milan, Italy),
using the streptavidin-
biotin-peroxidase complex technique.Glucagon and cytokeratin
were detected in the cyto-
plasm. Synaptophysin and neuron specific enolaseshowed a more
diffuse cytoplasmic distribution, andchromogranin A was not
detected. Scattered distribu-
M. Appetecchia et al.
136
Fig. 1 - CT scan of glucagonoma lesion at diagnosis
(A)demostrating the pancreatic localization, and the CT scan
images after three years of disease showing the livers
metastasis (B).
-
8/13/2019 Glucagonoma Maligno
3/6
tion of SSTR2 and SSTR5 expression was observed.The
immunostaining for glucagon (a), cytokeratin
(b), synaptophysin (c) and neuron specific enolase (d)are
reported in Fig.2.
After surgery, it was decided to treat the patient witha
slow-release somatostatin analogue octreotide (San-dostatin LAR;
Novartis), 20 mg intramuscularlyevery 28 days. After the first
injection, circulatingglucagon levels fell to 160 pg/mL, and after
the third
injection to 84 pg/mL. Three months later the patientnoticed
itchy cutaneous lesions in the legs and a 10kgweight loss. An
abdominal CT scan revealed twohypoechogenic lesions in the right
liver lobe (VII andVIII segment 2), one hyperechogenic nodule on
thesame side, one hyperechogenic nodule in the left lobe,and
microcalcifications in the VI segment. High bloodglucose levels
(130 mg/dL) were also reported. Serumglucagon levels were also
raised at 142 pg/mL. Circu-
lating chromogranin A and neuron specific enolasewere also high.
Alanine phosphatase was 319 U/L andcarcinoembryonic agent was in
the normal range (< 4.6ng/mL). Octreotide was then given at a
dose of 30 mgevery 28 days. Interferon- was introduced at the
doseof 6 MU subcutaneously 3 times per week. On treat-ment, a rapid
improvement in neoplastic symptoms wasobserved. Serum glucagon
levels decreased to 120
pg/mL. Four months later the patient again noticed
cutaneous lesions in the legs and biochemical analysisrevealed
high circulating levels of glucagon, neuronspecific enolase and
chromogranin A. Stable hepaticlesions were found on the abdominal
CT scan.Octreotide was initiated at a dose of 30 mg every
21days.
Nine months later, circulating glucagon, neuron spe-cific
enolase and chromogranin A levels were raisedagain and radiographic
scan revealed growing liver
Malignant Glucagonoma
137
Fig. 2 - Distribution of glucagon (a), cytokeratin (b),
synaptophysin (c) and neuron specific enolase (d) detected by
immunohistochem-
istry of glucagonoma tissue.
-
8/13/2019 Glucagonoma Maligno
4/6
metastases. Octreotide therapy was changed to 30 mgevery 15 days
and interferon- was continued with thesame schedule.
Chemoembolisation of the liver lesionswas started in order to help
provide disease control. The
patient underwent three cycles of hepatic
arterychemoembolisation from March 2003 to June 2004. Foreach
cycle, after an overnight fast, a catheter was insert-
ed into the hepatic artery and 50 mg superselectiveachiloblastin
with 10 mL lipidol ultrafluid 900-1200 mgspheres was
administered.
The patient continued the combination therapy at thesame dose
above described up to the present time. Shefeels good with a clear
improvement in quality of lifeand without any evidence of disease
progression.Serum glucagon levels were stable during the
follow-up
period.Stable hepatic lesions were found on the abdominal
CT scan as shown in Fig.1B.
Discussion
Immunohistochemical studies and single or com-bined treatment
schedules have only been described ina few cases of malignant
glucagonomas thus far (24).Several reports have described the
expression of thefive specific somatostatin receptors subtypes
(SSTRs)in normal and neoplastic neuroendocrine tissue (25).However,
data on protein expression of SSTRs are noteasily available due to
the lack of specific antibodiesthat can be used for
immunolocalisation. We had access
to polyclonal antibodies specifically targeted againstSSTR5 and
SSTR2 and were therefore able to localisethese two receptors in our
histological sections. Weshowed, for the first time, a scattered
distribution for
both receptor subtypes in the membrane and in thecytoplasm of
glucagonoma cells. This result was of par-ticular clinical interest
as the somatostatin receptors
bind not only the native peptide but exogenous somato-statin
analogues, a class of drugs commonly used forthe treatment of
neuroendocrine tumours. The somato-statin analogues are considered
the medical treatmentof choice for the symptoms of glucagonoma
(5,15,16,26-28), although their effects on tumourgrowth are
still matter of debate (15,16,26,29,30).
Chemotherapy has been used extensively in the pastfor the
management of neuroendocrine tumours and themost commonly used drug
is streptozotocin in mono-or combined chemotherapy with doxorubicin
or 5-fluo-rouracil without effects (24).
Neuroendocrine tumors are not chemosensitive, thisprobably is
due to their low rate of mitosis. Moreover,
these tumours show high expression of the multidrugresistance
gene and high levels of the antiapoptoticgene Bcl-2, which both
contribute to the resistance tochemotherapeutic agents (24).
Currently, chemotherapy may be beneficial forselected poorly
differentiated cases, while therapy withsomatostatin analogues
and/or with interferon- may
control the clinical symptoms when present and mayalso affect
tumor growth (19,31-33).
Because of the only modest success of current ther-apeutic
schedules, and since we obtained goodimmunopositivity for SSTRs, we
decided to treat our
patient with combination therapy consisting of thesomatostatin
analogue octreotide and interferon-. Thistreatment resulted in good
disease control for more thana year.
Radical resection of hepatic metastases, dependingon their
number and location, is recommended whenthey are present, as the
patient survival rate will
improve (2,34-36). Hepatic artery embolisation,
orchemoembolisation, has also been used and is associat-ed with
good control of glucagonoma symptoms in the
presence of disseminated liver disease, but without anyproven
survival advantage (15,22,23,30,37). In our casewe decided to carry
out chemoembolisation more thenone year after primary surgical
resection due to the radi-ological evidence of new hepatic
lesions.
The patient had a complete resolution of skin rash,normalisation
of plasma glucagon, chromogranin Aandneuron specific enolase
levels, and metastatic diseasestabilisation. The patient's quality
of life significantly
improved, and she is still alive 40 months after debulk-ing
surgery.
References
1. Wynick D., Williams S.J., Bloom S.R.: Symptomatic sec-
ondary hormone syndromes in patients with established malig-
nant pancreatic endocrine tumors. N. Engl. J. Med. 319 (10):
605-607, 1988.
2. Chu Q.D., Al-kasspooles M.F., Smith J.L., et al.: Is
glucagono-
ma of the pancreas a curable disease? Int. J. Pancreatol. 29
(3):
155-162, 2001.
3. Nishiguchi S., Shiomi S., Ishizu H., et al.: Acase of
glucagono-ma with high uptake on F-18 fluorodeoxyglucose
positron
emission tomography. Ann. Nucl. Med. 15 (3): 259-262, 2001.
4. Pech O., Lingenfelser T., Wunsch P.: Pancreatic
glucagonoma
as a rare cause of chronic obstructive pancreatitis.
Gastrointest.
Endosc. 52 (4): 562-564, 2000.
5. Bernstein M., Jahoor F., Townsend C.M. Jr., et al.: Amino
acid,
glucose, and lipid kinetics after palliative resection in a
patient
with glucagonoma syndrome. Metabolism 50 (6): 720-722,
2001.
M. Appetecchia et al.
138
-
8/13/2019 Glucagonoma Maligno
5/6
6. Grimelius L., Wilander E.: Silver stains in the study of
en-
docrine cells of the gut and pancreas. Invest. Cell. Pathol. 3
(1):
3-12 1980, .
7. Tomassetti P., Migliori M., Lalli S., et al.: Epidemiology,
clini-
cal features and diagnosis of gastroenteropancreatic
endocrine
tumours. Ann. Oncol. 12 Suppl 2: S95-99, 2001.
8. Chastain M.A.: The glucagonoma syndrome: a review of its
features and discussion of new perspectives. Am. J. Med. Sci.321
(5): 306-320, 2001.
9. Adams S., Baum R.P., Adams M., et al.: Clinical value of
so-
matostatin receptor scintigraphy. Studies of pre- and
intraoper-
ative localization of gastrointestinal and pancreatic
tumors.
Med. Klin. 92 (3): 138-143, 1997.
10. Jamar F., Fiasse R., Leners N., et al.: Somatostatin
receptor
imaging with indium-111-pentetreotide in gastroenteropancre-
atic neuroendocrine tumors: safety, efficacy and impact on
pa-
tient management. J. Nucl. Med. 36 (4): 542-549, 1995.
11. Nauck C., Ivancevic V., Emrich D., et al.:
111In-pentetreotide
(somatostatin analogue) scintigraphy as an imaging procedure
for endocrine gastro-entero-pancreatic tumors. Z. Gastroen-
terol. 32 (6): 323-327, 1994.
12. Kvols L.K.: Somatostatin-receptor imaging of human
malig-
nancies: a new era in the localization, staging, and treatment
of
tumors. Gastroenterology 105 (6): 1909-1911, 1993.
13. Jaffe B.M.: Surgery for gut hormone-producing tumors. Am.
J.
Med. 82 (5B): 68-76, 1987.
14. Casadei R., Tomassetti P., Rossi C., et al.: Treatment
of
metastatic glucagonoma to the liver: case report and
literature
review. Ital. J. Gastroenterol. Hepatol. 31 (4): 308-312,
1999.
15. Wermers R.A., Fatourechi .V, Wynne A.G., et al.: The
glucagonoma syndrome. Clinical and pathologic features in 21
patients. Medicine (Baltimore) 75 (2): 53-63, 1996.
16. Arnold R., Wied M., Behr T.H.: Somatostatin analogues in
the
treatment of endocrine tumors of the gastrointestinal tract.
Ex-
pert. Opin. Pharmacother. 3 (6): 643-656, 2002.17. Oberg K.:
Interferon-alpha versus somatostatin or the combi-
nation of both in gastro-enteropancreatic tumours. Digestion
57
Suppl 1: 81-83, 1996.
18. Taylor-Papadimitriou J., Shearer M., Rozengurt E.:
Inhibitory
effect of interferon on cellular DNA synthesis: modulation
by
pure mitogenic factors. J. Interferon Res. 1 (3): 401-409,
1981.
19. Arnold R.: Medical treatment of metastasizing carcinoid
tu-
mors. World J. Surg. 20 (2): 203-207, 1996.
20. Dirix L.Y., Vermeulen P.B., Fierens H., et al.: Long-term
results
of continuous treatment with recombinant interferon-alpha in
patients with metastatic carcinoid tumors. An antiangiogenic
effect? Anticancer Drugs 7 (2): 175-181, 1996.
21. Wilander E., Bengtsson A., Norheim I., et al.:
Interferon-in-duced nuclear DNA alterations in malignant carcinoid
tumors
in vivo. J. Natl. Cancer Inst. 76 (3): 429-433, 1986.
22. Venook A.P.: Embolization and chemoembolization therapy
for
neuroendocrine tumors. Curr. Opin. Oncol. 11 (1): 38-41,
1999.
23. Sutcliffe R., Maguire D., Ramage J., et al.: Management
of
neuroendocrine liver metastases. Am. J. Surg. 187 (1):
39-46,
2004.
24. Kaltsas G.A., Besser G.M., Grossman A.B.: The diagnosis
and
medical management of advanced neuroendocrine tumors. En-
docr. Rev. 25 (3): 458-511, 2004.
25. Benali N., Ferjoux G., Puente E., et al.: Somatostatin
receptors.
Digestion 62 Suppl. 1: 27-32, 2000.
26. Arnold R., Simon B., Wied M.: Treatment of
neuroendocrine
GEP tumours with somatostatin analogues: a review. Digestion
62 Suppl. 1: 84-91, 2000.
27. Eriksson B., Janson E.T., Bax N.D., et al.: The use of new
so-
matostatin analogues, lanreotide and octastatin, in
neuroen-docrine gastro-intestinal tumours. Digestion 57 Suppl 1:
77-
80, 1996.
28. Imam H., Eriksson B., Lukinius A., et al.: Induction of
apopto-
sis in neuroendocrine tumors of the digestive system during
treatment with somatostatin analogs. Acta Oncol. 36 (6):
607-
614, 1997.
29. Schott M., Scherbaum W.A., Feldkamp J.: Drug therapy of
en-
docrine neoplasms. Part II: Malignant gastrinomas, insulino-
mas, glucagonomas, carcinoids and other tumors. Med . Klin.
95 (2): 81-84, 2000.
30. Brentjens R., Saltz L.: Islet cell tumors of the pancreas:
the
medical oncologist's perspective. Surg. Clin. North Am. 81
(3):
527-542, 2001.
31. Oberg K.: State of the art and future prospects in the
manage-
ment of neuroendocrine tumors. Q. J. Nucl. Med. 44 (1):
3-12,
2000.
32. Frank M., Klose K.J., Wied M., et al.: Combination
therapy
with octreotide and alpha-interferon: effect on tumor growth
in
metastatic endocrine gastroenteropancreatic tumors. Am. J.
Gastroenterol. 94 (5): 1381-1387, 1999.
33. Faiss S., Pape U.F., Bohmig M., et al.: Prospective,
random-
ized, multicenter trial on the antiproliferative effect of
lan-
reotide, interferon alfa, and their combination for therapy
of
metastatic neuroendocrine gastroenteropancreatic tumors--the
International Lanreotide and Interferon Alfa Study Group. J.
Clin. Oncol. 21 (14): 2689-2696, 2003.
34. Hendry W.S., Munro A.: Pancreatic glucagonoma with lymphnode
metastases: disease-free survival six years after resection.
J. R. Coll. Surg. Edinb. 31 (2): 115-116, 1986.
35. Carty S.E., Jensen R.T., Norton J.A.: Prospective study of
ag-
gressive resection of metastatic pancreatic endocrine
tumors.
Surgery 112 (6): 1024-1031; discussion 1031-1032, 1992.
36. Azimuddin K., Chamberlain R.S.: The surgical management
of
pancreatic neuroendocrine tumors. Surg. Clin. North Am. 81
(3): 511-525, 2001.
37. Nesovic M., Ciric J., Radojkovic S., et al.: Improvement
of
metastatic endocrine tumors of the pancreas by hepatic
artery
chemoembolization. J. Endocrinol. Invest. 15 (7): 543-547,
1992.
Received: May 26, 2005
Accepted in revised form: October 25, 2005
M. Appetecchia, MD
Endocrinology Unit, Regina Elena Cancer Institute,
Via Elio Chianesi, 53 - 00144 Rome, Italy
Tel./Fax: +39 06 52666026
E-mail: [email protected]
Malignant Glucagonoma
139
-
8/13/2019 Glucagonoma Maligno
6/6
Finito di stampare nel mese di Marzo 2006
Stampa: LITOGRAF srl - Industria Grafica Editoriale - Todi
(PG)