Embed Size (px)
Citation preview

TABLE OF CONTENTS
Executive Summary ...........................................................................................................................................................1
Introduction ......................................................................................................................................................................... 5
Background .................................................................................................................................................................. 5
Significantadditionalinvestmentsareneededfrombothdomesticand internationalresourcestoclosethefundinggap ....................................................................................... 6
Financingarrangementsundermineequitableandsustainedprogressas countriestransitionfromlow-tomiddle-incomestatus ........................................................................ 9
TheefficiencyofRMNCAHinvestmentsissuboptimal ..........................................................................10
Poorstateofcivilregistrationandvitalstatistics(CRVS)systems .................................................. 11
Inadequateprovisionofglobalpublicgoods .............................................................................................. 12
Fragmentedfinancingandgovernancecausehightransactioncosts, hinderingprogressatthecountrylevel ......................................................................................................... 12
Goals,PrinciplesandObjectivesforaGlobalFinancingfacility ............................................................... 13
Objective1:FinancenationalRMNCAHscale-upplansandmeasureresults .............................. 15
Objective2:Supportcountriesinthetransitiontowardsustainabledomestic financingofRMNCAH ..............................................................................................................................................16
Objective3:Financethestrengtheningofcivilregistrationandvitalstatisticssystems ...... 17
Objective4:Financethedevelopmentanddeploymentofglobalpublic goodsessentialtoscaleup .................................................................................................................................. 18
Objective5:Contributetoabetter-coordinatedandstreamlinedRMNCAH financingarchitecture ............................................................................................................................................ 18
CountrySelection ............................................................................................................................................................19
CountryAccesstoFinancing ................................................................................................................................... 20
GFFCountryFinancingScenarios ........................................................................................................................... 21
GovernanceandInstitutionalArrangements ....................................................................................................23
Governanceprinciples ..........................................................................................................................................24
Institutionalarrangements ...................................................................................................................................24
CoreGFFcapabilities .............................................................................................................................................25
NextStepsandTimeline .............................................................................................................................................26
Annex1:GFFWorkingGroupMembership .......................................................................................................27
Annex2:The75CountdownCountries ...............................................................................................................29
Annex3:MethodologyforEstimatingHealthImpactsandResourceGaps ......................................31
Annex4:ConceptualFramework ...........................................................................................................................34
Annex5:RoleofthePrivateSector ......................................................................................................................35
Annex6:PartnershipforBetterMaternalandChildHealthResultsinDRC .....................................36
Annex7:RMNCAHFinancialRoadmaps ...........................................................................................................38
Annex8:LeveragingIDAThroughtheHealthResultsInnovationTrustFund ...............................40
ACRONYMS AND ABBREVIATIONS
AIDS acquiredimmunodeficiencysyndrome
CRVS civilregistrationandvitalstatistics
CSO civilsocietyorganization
DFID DepartmentforInternationalDevelopment
DRC DemocraticRepublicofCongo
EPMCD endingpreventablematernalandchilddeaths
EWEC EveryWomanEveryChild
GFATM TheGlobalFundtoFightAIDS,TuberculosisandMalaria
GFF GlobalFinancingFacility
HIV humanimmunodeficiencyvirus
HRITF HealthResultsInnovationTrustFund
IBRD Int’l.BankforReconstructionandDevelopment
IDA InternationalDevelopmentAssociation
iERG IndependentExpertReviewGroup
IHP+ InternationalHealthPartnership
IMCI integratedmanagementofchildhoodillness
LIC low-incomecountry
LMIC lower-middle-incomecountry
MDG MillenniumDevelopmentGoals
MDSR maternaldeathsurveillanceandresponse
MIC middle-incomecountry
MNCH maternal,newbornandchildhealth
NGO non-governmentalorganization
P4H ProvidingforHealth-SocialHealthProtectionNetwork
PMNCH PartnershiponMaternal,NewbornandChildHealth
PMNCH PartnershipforMaternal,NewbornandChildHealth
RBF results-basedfinancing
RMNCAH reproductive,maternal,newborn,childandadolescenthealth
SDG SustainableDevelopmentGoals
TB tuberculosis
UMIC upper-middle-incomecountry
UN UnitedNations
UNFPA UnitedNationsPopulationFund
UNICEF UnitedNationsChildren’sFund
USAID U.S.AgencyforInternationalDevelopment
WBG WorldBankGroup
WHO WorldHealthOrganization
1
EXECUTIVE SUMMARYAstheworldapproachesthe2015deadlinefortheMillenniumDevelopmentGoals(MDGs),theenormousprogressthathasbeenmadeinimprovingmaternalandchildhealthisbecomingevident.However,despitetheprogress,itisequallyclearthatmoreremainstobedone:fartoomanynewborns,children,adolescentsandwomendieofpreventableconditionseveryyear,andfartoofewhavereliableaccesstoqualityhealthservices.
ThereisnowanunprecedentedglobalmomentumtofurtheraccelerateimprovementsinReproductive,Maternal,Newborn,ChildandAdolescentHealth(RMNCAH).ThroughkeyglobalpartnershipssuchasthePartnershiponMaternal,NewbornandChildHealth(PMNCH),theG8MuskokaInitiative,CommittingtoChildSurvival:APromiseRenewedandtheUnitedNationsSecretary-General’sEveryWomanEveryChild(EWEC)movement,theimportanceofwomen’sandchildren’shealthhavebeenputatthecenterofglobaldevelopmentefforts.Buildingonthismomentum,thereisnowstrongsupportfortheconceptof“convergence”:acceleratingprogressinimprovingthehealthandqualityoflifeofwomen,children,andadolescentssothatallcountriesachievethelevelsreachedbythebest-performingmiddle-incomecountries.TheglobalinterestinRMNCAHisanopportunitytomakeafinalpushontheMDGsandensureasolidfoundationforthepost-2015work.Totakeadvantageofthisopportunityandensuremorerapidaccelerationtowardthe2030convergencetargets,thesefollowingchallengeswillneedtobeaddressed:
• SignificantadditionalinvestmentsareneededfrombothdomesticandinternationalresourcestoclosethefundinggapofUS$5.24percapitain74high-burdencountriesin2015;
• Financingarrangementsundermineequitableandsustainedprogressascountriestransitionfromlow-tomiddle-incomestatus;
• Thestateofcivilregistrationandvitalstatisticssystemsremainspoor;
• Globalpublicgoodsareinadequatelyfinanced;
• Fragmentedfinancingandgovernancecausehightransactioncosts,hinderingprogressatthecountrylevel.
ThisConceptNotearguesthataGlobalFinancingFacility(GFF)insupportofEveryWomanEveryChildcanhelpdrivethetransformativechangeneededtopreparethe
1
2
roadtoconvergenceonRMNCAH.TheoverallgoaloftheGFFwillbetocontributetotheglobaleffortstoendpreventablematernal,newborn,childandadolescentdeathsandimprovethehealthandqualityoflifeofwomen,adolescentsandchildren.Itisestimatedthatcomparedwithcurrenttrends,anacceleratedinvestmentscenariowouldhelppreventatotalof4millionmaternaldeaths,107millionchilddeaths,and22millionstillbirthsbetween2015and2030in74high-burdencountries.1
TheGFFwillmobilizeandchanneladditionalinternationalanddomesticresourcesrequiredtoscaleupandsustainefficientandequitabledeliveryofqualityRMNCAHservices.Additionally,theGFFwillsupportthetransitiontolong-termsustainabledomesticfinancingforRMNCAH.AspecialfocusareafortheGFFwillbetosupportthescaleupofcivilregistrationandvitalstatistics(CRVS)systemstocontributetouniversalregistrationby2030.
TheGFFhasfiveobjectives:
1. FinancenationalRMNCAHscale-upplansandmeasureresults;
2. SupportcountriesinthetransitiontowardsustainabledomesticfinancingofRMNCAH;
3. Financethestrengtheningofcivilregistrationandvitalstatisticssystems;
4. Financethedevelopmentanddeploymentofglobalpublicgoodsessentialtoscaleup;
5. Contributetoabetter-coordinatedandstreamlinedRMNCAHfinancingarchitecture.
TheGFFwillfacilitateaclearstrategyforfully-scaledandsmartfinancingofRMNCAHservicesindifferentcountries.Thisstrategywillbearticulatedinafinancingroadmapinformedbyarights-based,results-focused,fullycostedRMNCAHnationalplanlinkedtonationalstrategiesforhealthandothersectors.Theroadmapwillprovideacomprehensivepictureofacountry’simmediateandlonger-termRMNCAHresourceneedsandwilloutlinestrategiestomobilizetherequisitedomestic(publicandprivate)andinternational(bilateralandmultilateral)fundingovertime.TheaimistoharmonizefundingforRMNCAHplansthroughacommoncountryfinancingframeworkwhichislinkedtoclearresultsandbackedbycommonaccountabilityandreportingmechanisms.Thefinancingroadmapswillbelinkedtolonger-termplanningthatstrengthensdomesticresourcemobilizationanddiversifiesmodalitiesofdevelopmentassistanceinlinewithacountry’srateofeconomicgrowth.
1SouthSudanwasexcludedfromtheanalysisduetolackofdata.
3
TheGFFwillalsopositionitselfasamajorinvestorinthefinancialroadmapthroughmobilizationofdevelopmentassistance.Specifically,itwillbuildontheexistingHealthResultsInnovationTrustFund(HRITF)attheWorldBankthatoffersexcellentleverageofInternationalDevelopmentAssociation(IDA)andInternationalBankforReconstructionandDevelopment(IBRD)resources,goodvalue-for-moneyintermsofachievingRMNCAHresultsandlowadministrativecosts.Inaddition,throughadedicatedfinancingwindow,theGFFwillsupportthestrengtheningandscaling-upofCRVSplanscontributingtotheuniversalregistrationofeverypregnancy,everybirthandeverydeathby2030.Otherfinancingwindowsarealsoenvisagedfor“multi-sectoral”,“multi-lateral”and“market-shaping”investments.
ThreediscretegovernancecapabilitiesneedtobeputinplaceforthefurtherdevelopmentoftheGFF.Onerelatestotheneedforeffectiveconveningaroundthedevelopmentandimplementationofthecountryfinancingroadmaps.AsecondrelatestotheoperationsandfurtherdevelopmentoftheGFFwindows.Andathirdrelatestotheneedforanumbrellastewardshipthatconvenesstakeholders,forgesconsensusamongstdomesticandinternationalfinanciers,reviewsprogress,andrecommendsactionstoacceleratetheachievementofresults.WithanagreementontheobjectivesandfunctionsoftheGFF,acollaborativebusinessplanningprocessisanticipatedinthecomingmonths.TheWorldBankwillplayaconveningrolefortheGFF,workingwithpartnerstofurtherdesignandoperationalizetheGFFinthelead-uptoaformallaunchinmid-2015.

4
5
INTRODUCTIONThisConceptNotelaysoutthehigh-levelrationale for and objectives of a proposed Global Financing Facility (GFF) for reproductive, maternal, newborn, child and adolescent health (RMNCAH) in support of Every Woman Every Child.Itdescribessuggestedfinancingprioritiesofthefacility,proposedcountrygroupingstobenefitfromsupport,andhowthefacilitywillcollaboratewithpartnerstosimplifyRMNCAHfinancingatthecountrylevel.Finally,itprovideskeyprinciplestoguideGFF governance,asequencedapproachfordefiningGFFgovernanceandinstitutional arrangementsandoutlineshowthesewillinteractwithandhelpstreamlinetheexistingRMNCAHfinancingarchitecture.
TheConceptNotewasdevelopedundertheguidanceoftheGFFWorkingGroup,whichincludedabroadrangeofpartnersandwaschairedbytheGovernmentofNorway,theUnitedStatesAgencyforInternationalDevelopment(USAID)andtheWorldBank(seeAnnex1formembership).Itmarksthebeginningofandprovidesthefoundationforaconsultativeprocessoverthecomingmonthstodevelopinmoredetailthestrategicapproach,operationaldesignandgovernancefortheGFF.ThesewillbesummarizedinaGFFbusinessplan,withtheaimoflaunchingafullyoperationalGFFbySeptember2015.
Background Astheworldapproachesthe2015deadlinefortheMillenniumDevelopmentGoals(MDGs),theenormousprogressthathasbeenmadeinimprovingreproductive,maternalandchildhealthisbecomingevident.Theunder-fivemortalityrateandmaternalmortalityratio–keyindicatorsforMDGs4and5–havebothdroppeddramatically,from90deathsper1,000livebirthsin1990to46in2013andfrom380deathsper100,000livebirthsin1990to210in2013.2Thissuccessmakesitconceivablethatpreventabledeathscanbeavertedandthehealthandqualityoflifeofwomenandchildrenimprovedwithinageneration.
However,despitethisprogress,itisequallyclearthatmoreremainstobedone.Fartoofewwomen,newborns,children,andadolescentshavereliableaccesstoqualityhealthservicesandtoomanydieofpreventablecauseseveryyear.Annually,6.6millionchildrenstilldiebeforetheageof5,ofwhich2.9millionarenewbornbabiesinthefirstmonthoflife.Manychildrenstilldiefromeasilypreventablediseases,suchasmalnutrition(theunderlyingcauseof45percentofallunder-fivedeaths),pneumoniaanddiarrhea.Forthosechildrenwhosurvive,malnutritioncanjeopardizetheir
2WHO,UNICEF,UNFPA,UNPOPandtheWorldBank(jointpublication).(2014). TrendsinMaternalMortality:1990to2013.
5
6
potentialforoptimalgrowthanddevelopment,withsignificantconsequenceslaterinlife.Malaria,HIVandAIDSfurthercausesignificantdeathsinhigh-burdencountries.
Theleadingcausesofmaternalmortality—heavybleeding,highbloodpressure,infectionsandunsafeabortion—are,toalargeextent,preventable.Ensuringtheavailabilityofcertainservices—suchasfamilyplanning,prenatalcare,skilledcareatbirth,reproductivehealthcareafterdeliveryandarangeofservicesforadolescents—iskeytopreventingmaternaldeathsandimprovingthequalityoflifeforwomanandchildren.Some11percentofallbirthsworldwidearetogirlsaged15to19years,andthevastmajorityofthesebirthsareinlow-andmiddle-incomecountries.Complicationslinkedtopregnancyandchildbirtharethesecondmostcommoncauseofdeathfor15-19-year-oldgirlsglobally.Accesstoservicesforcontraception,preventionandmanagementofsexuallytransmitteddiseasesandcareinpregnancyarekeytobetterhealthandqualityoflifeforadolescents.However,coverageformanyoftheseinterventionsremainslowinmanycountries.Further,coverageformanyhigh-impactessentialhealthservicesisunevenlydistributedacrosstheworld,withsub-SaharanAfricaandSouthAsialagginginparticular.
Within-countrydistributionalsoremainsuneven,withinsufficientprogressonequitydimensionssuchaswealth,gender,age,maternaleducation,ethnicity,andurban/ruralresidence.Achievingmeaningfulprogressinreproductive,maternal,newborn,childandadolescenthealthrequiresdeliveringessentialhealthservicestoallpopulationgroups.Further,asmoremotherschoosetocometohealthfacilitiestogivebirth,theyneedtobetreatedwithrespectanddignity,andgivenhighqualitycare.Otherwise,evenadvancesincoveragemaynottranslateintogoodhealthoutcomes.
ThegrowingglobalinterestinRMNCAHisanopportunitytomakeafinalpushontheMDGsandensureasolidfoundationforpost-2015work.Inordertotakeadvantageofthisopportunity,anumberofchallengeswillneedtobeaddressedtoensuremorerapidaccelerationtowardthe2030convergencetargets.
Significant additional investments are needed from both domestic and international resources to close the funding gapInternationaldonorfinancingforRMNCAHhasincreasedsignificantlyoverthepastdecade.Bilateralandmultilateraldisbursementstothe75highest-burdencountries(Annex2)reachedanestimatedUS$9-9.5billionin2011,anincreaseofmorethan70percentcomparedwith2006.Between2009and2012anestimatedtotalofUS$38billionwasdisbursedtothesecountries.Ofthisamount,66percentwaschanneledviabilateralprogramsand34percentviamultilateralinstruments.Inaddition,theBill&MelindaGatesFoundationprovidedUS$3billioninprivategrantsforRMNCAHtothe75highest-burdencountries.
DataondomesticfinancingforRMNCAHaremuchpoorerthanthoseforinternational
7
financing,butitisestimatedthatnearlyUS$60billionofdomesticgovernmentresourceswasspentonRMNCAHin2012intheCountdownto2015countries.3 Despitetheseincreasesinbothinternationalanddomesticfinancing,asignificantfinancinggapremainsforthefinancingoftheGlobalStrategy.
The Global Investment Framework for Women’s and Children’s Health4andtheLancet Commission on Investing in Health5havebothshownthatfinancingwillneedtoincreasesignificantlyoverthecoming15yearstoachievethelevelsofcoverageandimprovementsinthehealthstatusofwomenandchildrenreflectiveoflevelscurrentlyreachedbythebest-performingcountries.Bothreportsarguethatinvestmentsintheso-called“grand convergence”willyieldhigheconomicreturnsandsocietalgainssuchasenhancedpoliticalandsocialcapital.
Bybuildingonandcombiningkeyelementsofthesetwoefforts,furthermodelingwasundertakenforthisConceptNote.Theaimwastoestimatetheresourcesneededtoscaleuptoahigh-coveragescenario,thepotentialcontributionsfromdomesticfinancing,andtheremainingresourcegapforthe75high-burdencountriescurrentlybeingtrackedundertheCountdownto2015initiative.6ResourceneedsestimatesfromtheGlobalInvestmentFrameworkwereadjustedforanumberofadditionalfactorsincludinginflationandthepurchaseandscale-upofnewtechnologies,basedonmethodsusedbytheCommissiononInvestinginHealth.DomesticfinancingflowswereestimatedusingasimilarapproachtothattakenbytheCommissiononInvestinginHealth.Allestimateswereprojectedthrough2030.ThemethodologyisdescribedinAnnex3.
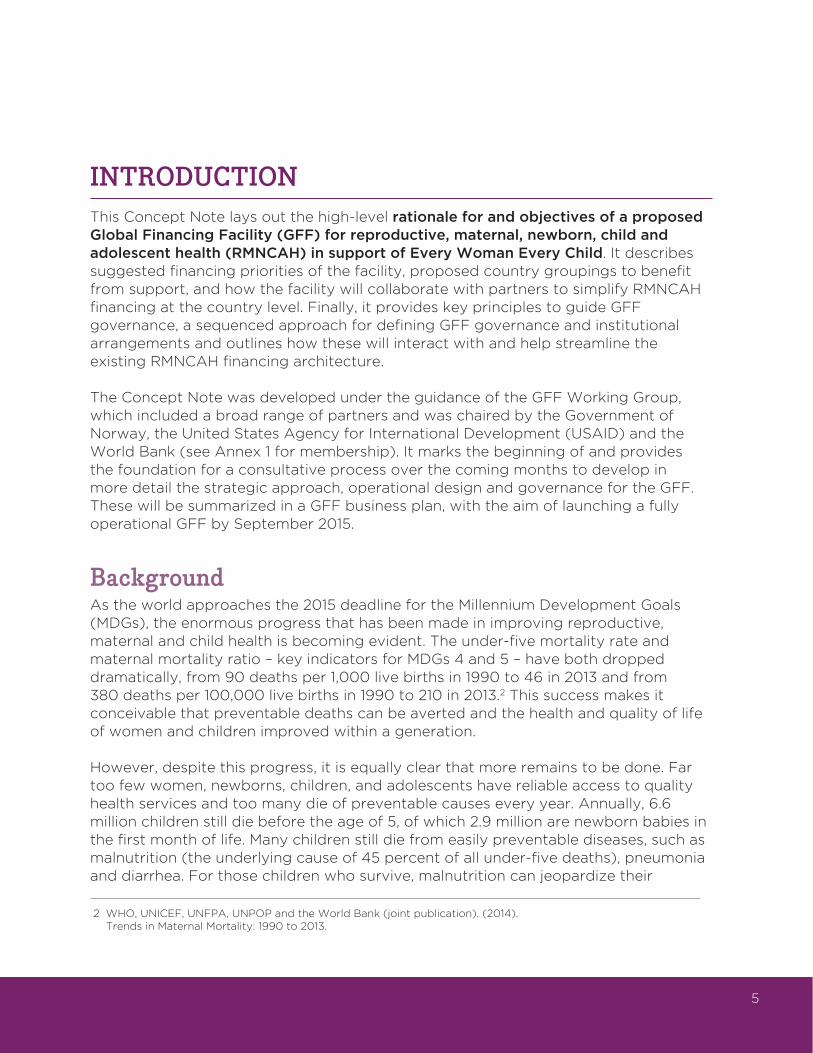
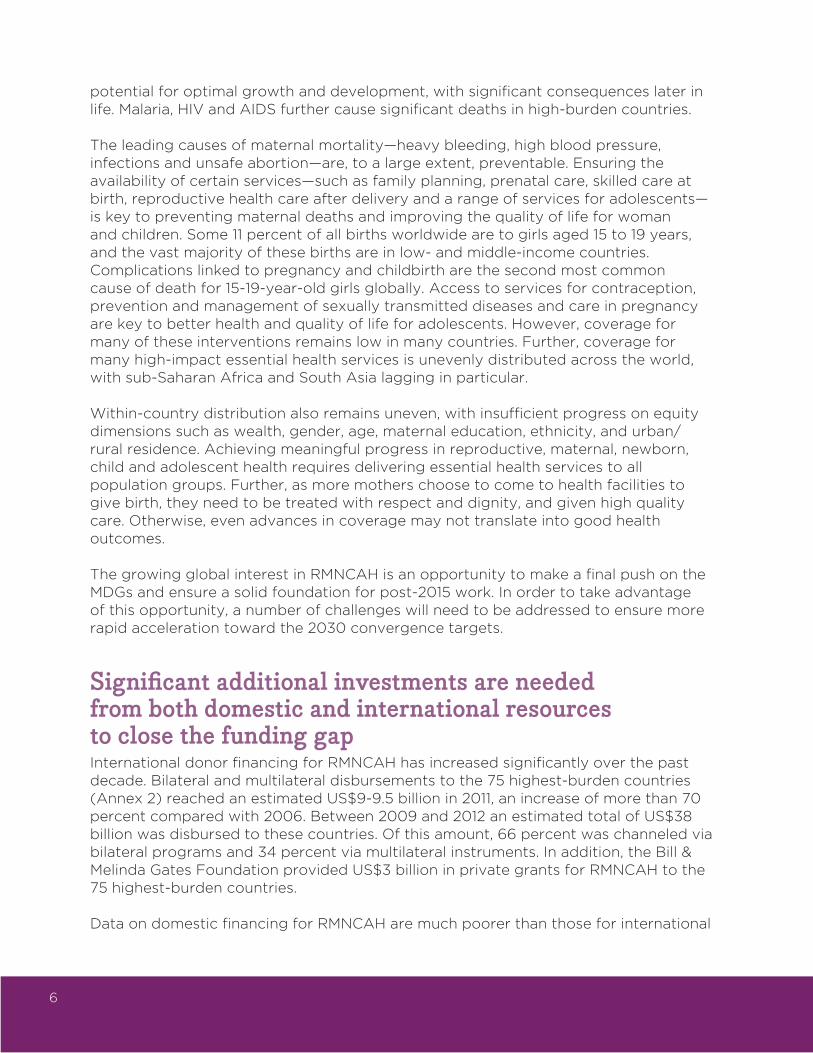
Theprojectedresourcegapspeakearlyintheperiod,whenanestimatedUS$28-30billionofadditionalfinancingisneeded,inlargepartduetoup-fronthealthsystemsstrengtheninginvestments(particularlyinlow-incomecountries)thatarethenecessaryfoundationforconvergence.By2030,thetotaladditionalfinancinggapisprojectedtofallconsiderablytoaboutUS$8billion,orUS$1.23perperson(downfromUS$5.24perpersonin2015),duetoacombinationofincreaseddomesticfinancingandreducedhealthsystemsstrengtheningcosts,asshowninFigure1.
Nearlytheentireresourcegapoccursinthe63Countdowncountriesclassifiedaslow-income(LIC)andlower-middle-income(LMIC).In2015,theprojectedresourcegapforthesecountriesisUS$27.2billion,fallingtoUS$7.2billionby2030.Inper-capitaterms,thistranslatesintoaresourcegapofUS$7.68perpersonin2015andUS$1.69in2030.ResourcegapsremainparticularlylargeinLICs,whereonlyabouthalfoftheUS$11billionneededin2030isprojectedtobemetbydomesticgovernmentexpenditures,leavingagapofUS$5.4billion,orUS$4.60perperson.
3PartnershipforMaternal,Newborn,andChildHealth.(2014).PMNCHAccountabilityReport2014.
4Stenberg,K.etal.(2014).Advancingsocialandeconomicdevelopmentbyinvestinginwomen’sandchildren’shealth:anewGlobalInvestmentFramework.The Lancet,383:1333-54.
5Jamison,D.T.etal.(2013).Globalhealth2035:aworldconvergingwithinageneration.The Lancet,382:1898-955.
6http://countdown2015mnch.org/.SouthSudanisaCountdowncountrybuthasnotbeenincludedbecauseofinsufficientdata.
8
Figure1highlightsanimportantconsiderationininterpretingthesenumbers:thedomesticfinancingestimatesaresensitivetotheshareofdomestichealthfinancingallocatedtoRMNCAH.Inthebasecase,thisshareistakenas25percent,whichisanestimatedevelopedfromtheCountdownto2015processandusedbytheGlobalStrategy.Ifthisincreasesto50percent–asharethatmaybemoreappropriateformanycountriesgiventhehighburdenofdiseaserelatedtoRMNCAH–thefinancinggapdropstounderUS$3.5billionin2030.
60
50
40
30
20
10
02015 2020 2025 2030
All Coundown Countries
50%of domestic health expenditures to RMNCH
Resource Gaps
Figure 1: Resource needs to reach convergence and the role of domestic financing in the closing gap
Billio
ns
US
$
18
16
14
12
10
8
6
4
2
-
30
25
20
15
10
5
-2015 2020 2025 2030 2015 2020 2025 2030
Billio
ns
US
$
Figure 2: Resource needs to reach convergence and the role of domestic financing in the closing gap
25%of domestichealth expendituresto RMNCH
50%of domestic health expendituresto RMNCH
ResourceGaps
25%of domestichealth expendituresto RMNCH
50%of domestic health expendituresto RMNCH
ResourceGaps
Low-Income Countries Lower-Middle-Income Countries
25%of domestic health expenditures to RMNCH
Peak gap of US$28-30 billion per year, of which US$11 billion is covered by current international financing
US$3 billion gap if 50% ofdomestic health spendingtoward RMNCH
US$8 billion gapif 25% of domestic
health spending
60
50
40
30
20
10
02015 2020 2025 2030
All Coundown Countries
50%of domestic health expenditures to RMNCH
Resource Gaps
Figure 1: Resource needs to reach convergence and the role of domestic financing in the closing gap
Billio
ns
US
$
18
16
14
12
10
8
6
4
2
-
30
25
20
15
10
5
-2015 2020 2025 2030 2015 2020 2025 2030
Billio
ns
US
$
Figure 2: Resource needs to reach convergence and the role of domestic financing in the closing gap
25%of domestichealth expendituresto RMNCH
50%of domestic health expendituresto RMNCH
ResourceGaps
25%of domestichealth expendituresto RMNCH
50%of domestic health expendituresto RMNCH
ResourceGaps
Low-Income Countries Lower-Middle-Income Countries
25%of domestic health expenditures to RMNCH
Peak gap of US$28-30 billion per year, of which US$11 billion is covered by current international financing
US$3 billion gap if 50% ofdomestic health spendingtoward RMNCH
US$8 billion gapif 25% of domestic
health spending
9
Figure2showsthatthefinancinggapvariesconsiderablybyincomelevel,withmiddle-incomecountries(MICs)betterpositionedtoassumeprogressivelylargersharesofRMNCAHfinancing.Forthe63low-andlower-middle-incomecountriesoverall,theresourcegapisestimatedatjustoverUS$7billionby2030(downfromUS$27billionin2015).Shouldahigherproportion(50percent)ofgovernmenthealthexpendituresbeallocatedtoRMNCAH,theresourcegapwillclosefurther,toUS$2.6billionforLICsandUS$0.8billionforLMICs.
Itshouldbenotedthattheseestimatesarehighlysensitivetoeconomicgrowth.DomesticfinancingestimatesarebasedonprojectionsofcontinuedhighgrowthinmostLICsandMICs.Shouldtherecenttrendofrapideconomicgrowthinlow-andmiddle-incomecountriesbegintoslow,domesticfinancingflowscoulddropconsiderably.
Theseprojectionshighlightthefactthatwithoutasignificantincreaseinfinancingfrombothinternationalanddomesticsources,thegoalofconvergencewillremainoutofreach.Thescaleofthechallengesuggeststhatnewapproachesareneeded,asincrementalincreasesinexistingmechanismswillbeinsufficienttoclosethegap.
Financing arrangements undermine equitable and sustained progress as countries transition from low- to middle-income statusMostcountriesintheworldareexperiencingatransitioninhealthfinancingcharacterizedbyanincreaseinhealthexpendituresandarisingshareofgovernmentspendingduetoacombinationofeconomicgrowthandchangingpoliticalpriorities.Thehealthfinancingtransition,however,isoftennotasteadyprocessbutratheranunevenonewithparticularchallengesforeconomiesundergoingthetransitionfromlow-incometomiddle-incomestatus.AsRMNCAHconstitutesalargeshareofhealthexpendituresinlow-andlower-middle-incomecountries,thesegeneralhealthfinancingchallengesimpedeprogressandjeopardizeearlygainsmadetowardthe2030goals.
Attheonsetofthistransition–whenstillclassifiedaslow-income–countriestendtorelyheavilyoninternationalsupport.Thisassistance,however,oftenreducesdomesticfundingforhealth—onaverage,eachadditionaldollarofdevelopment assistanceforhealthdiminishesdomesticfinancingbyapproximately50cents.7 Thispatternleavescountriesunpreparedforthechallengestheyfaceaseconomicgrowthpropelsthemintolower-middle-incomestatus.Mostimportantly,duringthistransition,thelinkbetweenincomegrowthandincreasesintotalandgovernmentexpenditureonhealthisweakestwhenthecountriesattainlower-middle-incomestatus.Forexample,whileeverypercentagepointincreaseineconomicgrowth
7Lu,C.,Schneider,MT.,Gubbins,Petal.(2010).Publicfinancingofhealthindevelopingcountries: across-sectionalsystematicanalysis.The Lancet,375(9723):1375-1387. -Farag,M.,Nandakumar,A.K.,Wallack,S.S.,Gaumer,G.,Hodgkin,D.(2009).Doesfundingfromdonorsdisplacegovernmentspendingforhealthindevelopingcountries?Health Affairs,28:1045–1055.
10
translatesintoa1.18percentagepointincreaseingovernmentexpenditureonhealthinLICsand0.54percentagepointsinuppermiddle-incomecountries(UMIC),itisonly0.37percentagepointsinLMICs.ItisthereforelikelythatgovernmentsofLMICsfailtoeffectivelycompensateforpotentialdecreasesindevelopmentassistance.Asaconsequence,out-of-pocketspendingincreasesandhouseholdsbearalargeshareofthefinancingburden.Inbothlower-andupper-middle-incomecountries,unprecedentedlevelsoftotalandgovernmentexpendituresonhealthmaskdrasticdifferencesinspendingacrosspopulationgroups.Theseinequalitiesinspendingimplysignificantdifferencesinaccesstoservicesandfinancialprotection,tothedetrimentofthepoor.
The efficiency of RMNCAH investments is suboptimalMuchattentioninrecentyearshasfocusedonmakingRMNCAHresourcesgofurtherandmaximizingvalueformoney.8SignificantprogresshasbeenmadeindevelopingaconsensusontheessentialRMNCAHinterventionpackagesthatshouldbeprioritizedincountryplanning,andtechnicalpartnersareworkingwithcountriestoensurethisisreflectedinnationalplans.Despitethisprogress,manyRMNCAHplanshavesuboptimaltargetingandinsufficientprioritizationofevidence-based,high-impactinterventions.9Further,someaspectsofthecontinuumofcareandsomepopulationshavereceivedinadequateinvestment.Reproductive,newbornandadolescenthealthhavebeennotablyunder-prioritizedcomparedtotheirrelativeburdenandpotentialforimpact.RMNCAHinterventionsarefrequentlyhamperedbybottlenecksinthehealthsystem,suchasinsufficienthumanresourcesforhealth.10TheimplementationofRMNCAHprogramscanbeenhancedbyimprovingefficiencyinthedeliveryofservicesthroughinnovativemechanismsincludingresults-basedfinancing.11Finally,inequitybetweenrichandpoorpopulationsismorepronouncedwithregardtoRMNCAHservicesthanwithanyotherhealtharea.Althoughincreasesinhealthservicescoveragehavebeeningeneralpro-poor12,thishasnotalwaystranslatedintobetterhealthoutcomesforpoorpeople,possiblypointingtoapoor/richdivideinthequalityofhealthservicesprovided.EffortstoimproveRMNCAHwillneedtoaddressthis,andmeasurementofprogressbysocioeconomicstatuswillbeessential.ImprovingthehealthimpactofexistingresourcesisanimportantmeasuretobeconsideredalongsidefurtherincreasesinfinancingforRMNCAH.
8TheWorldBank.(2013).UsingResults-BasedFinancingtoAchieveMaternalandChildHealth:ProgressReport2013.Availablefromhttp://rbfhealth.org/progressreport2013
9Bhutta,Z.A.etal.(2014).Canavailableinterventionsendpreventabledeathsinmothers,newbornbabies,andstillbirths,andatwhatcost?The Lancet,384(9940):347-370.
10Dickson,K.E.,etal.(2014).Everynewborn:health-systemsbottlenecksandstrategiestoacceleratescale-upincountries.The Lancet,384(9941):438-454.
11Basinga,P.etal.(2011).EffectonmaternalandchildhealthservicesinRwandaofpaymenttoprimaryhealth-careprovidersforperformance:animpactevaluation.The Lancet,377(9775):1421-1428.
–Gertler,P.,Giovagnoli,P.,&Martinez,S.(2014).Rewardingproviderperformancetoenableahealthystarttolive:EvidencefromArgentina’sPlanNacer.TheWorldBank,PolicyResearchWorkingPaper6884.
12Wagstaff,A.,Bredenkamp,C.,&Buisman,L.R.(August2014).ProgressonGlobalHealthGoals:arethePoorBeingLeftBehind?World Bank Research Observer.
11
Poor state of civil registration and vital statistics (CRVS) systemsCivilregistrationandvitalstatistics(CRVS)systemsareacknowledgedasacriticalplatformforpromotingwomenandchildren’shealth.13StrongCRVSsystemsarecriticalforsafeguardingpeople’srightsandthoseoftheirchildren.Theyarecrucialfordevelopmentandaccountability,particularlyinhealth,aswellasforgeneratinginformationonvitalevents(births,deathsandcauseofdeath),populationtrendsandtheoverallwell-beingofthepopulation,especiallymaternalandchildhealth.CRVSsystemsarealsoimportantforeffectivepolicymakingandlong-termnationalplanning,efficientresourceallocationandaccurateevaluationandmonitoring.ThesesystemswillbeanimportantsupporttoacceleratingRMNCAHimprovementsandinvestments.
Yetover100developingcountrieslackwell-functioningCRVSsystems.Aroundtheworld,almost230millionchildrenundertheageoffivearenotregistered.14
Despitethecriticalneedforinformationaboutmortality,progresswithdeathregistrationhasbeenslowglobally,withupto80percentofdeathsthatoccuroutsideofhealthfacilitiesandtwo-thirdsofalldeathsgloballynotcounted.15 Bothdemand-sideandsupply-sidechallengesexplainthecurrentpoorstateofCRVSsystems.ThesechallengesincludepoorcoordinationamongvariousministriesanddevelopmentpartnersresponsibleforCRVSanddevelopmentpartners,lackofneededinfrastructureandcapacityatthecountrylevel,absenceofnecessarylegalframeworksandlimitedawarenessamongpeopleontheimportanceofregistration.
YetthetransformativepotentialofeffectiveCRVSsystemshasbeenrecognizedbymanypartnersandfora,suchastheUNCommissiononInformationandAccountabilityforWomen’sandChildren’sHealth.Themulti-stakeholderworkplantoimplementtheCommission’srecommendationshasidentifiedstrengtheningCRVSandmaternaldeathsurveillanceandresponse(MDSR)aspriorityareasin75countries.Recentglobalmomentumhasbeenachievedthroughregionalandglobalpartnerships,aswellascriticalcountrypartnerships.ThehealthsectorisacknowledgedasagoodentrypointforthedevelopmentandstrengtheningofCRVSsystems,withRMNCAHsystemsacknowledgedasbothabeneficiaryofandcontributortostrengthening.16Healthprovidesamajorentrypointforscalingupbirthanddeathregistrationthroughinnovativeapproaches(e.g.linkingbirthregistrationandMNCHtrackingandimmunization,mortalityreportingthroughcommunityhealth
13CommissiononInformationandAccountabilityforWomenandChildren’sHealth(2011)KeepingPromises,MeasuringResults.http://www.everywomaneverychild.org/images/content/files/accountability_commission/final_report/Final_EN_Web.pdf
14UNICEF.(2013).UnitedNationsChildren’sFund.APassporttoProtection:Aguidetobirthregistration programming.
15WorldBank-WHO(2014)GlobalCivilRegistrationandVitalStatisticsScalingupInvestmentPlan2015–2024.http://www.worldbank.org/en/topic/health/publication/global-civil-registration-vital-statistics-scaling-up-investment
16WHO2013StrengtheningCRVSthroughInnovativePracticesintheHealthSector:GuidingPrinciplesandGoodPractices,http://www.who.int/healthinfo/civil_registration/crvs_meeting_dec2013_report.pdf?ua=1
12
workers).Itcanbethesectorresponsibleforbirthnotificationandcauseofdeathinformationanditisoneofthemaininvestorsinandusersofvitalstatistics.
Inadequate provision of global public goodsGlobalpublicgoodssuchasresearchanddevelopment,marketshaping,diseasesurveillance,andinternationalnormsandstandardsettingarecomponentscriticaltomakinghealthsystemswork,but,inthewordsoftheCommissiononInvestinginHealth,“theseriousunderfundingofglobalpublicgoods…hasnowreachedacrisispoint.”17Twoexamplesaremeasurementandaccesstocommodities.TheCommissiononInformationandAccountabilityforWomen’sandChildren’sHealthandtheUNCommissiononLife-SavingCommoditiesforWomen’sandChildren’sHealthdevelopedasetofrecommendationsintheseareas.Mostoftheserecommendationsstillneedtobeimplemented.
Fragmented financing and governance cause high transaction costs, hindering progress at the country levelSincethelaunchoftheUNSecretary-General’s“GlobalStrategyforWomen’sandChildren’sHealth”andtheG8MuskokaInitiativeonMaternal,NewbornandChildHealth,bothin2010,morethan300stakeholdershavemadeabroadrangeoffinancialandnon-financialcommitmentstosupporttheGlobalStrategy.Somebringanin-depthfocustospecificelementsoftheRMNCAHContinuumofCare(suchastheChildSurvivalCalltoAction–APromiseRenewed;theGlobalActionPlanforNewborns;theGlobalActionPlanforPneumoniaandDiarrhoea).OthersaddresskeyelementsoftheunderlyingRMNCAHarchitectureincross-cuttingways,suchastheUNCommissiononInformationandAccountabilityandtheRMNCHSteeringCommittee.ThePartnershipforMaternal,NewbornandChildHealth(PMNCH),establishedin2005,bringstogethermorethan600memberstocatalyzecollectiveactionforRMNCAH.
TherecentreviewoftheEveryWomanEveryChild(EWEC)accountabilitywork(August2014)listedamultitudeofdifferentfinancingmechanismsforRMNCAH,includingFamilyPlanning2020,theH4+Partnership,theHealthResultsInnovationTrustFund,theThematicTrustFundforMaternalHealth,theGlobalProgramtoEnhanceReproductiveHealthCommoditySecurity,theUSFundforUNICEF,theBridgeFund,thePledgeGuaranteeforHealthandtheRMNCHTrustFund.
RecentyearshaveseenanincreasedfocusonbettercoordinationofthemultitudeofinitiativesintheRMNCAHecosystemandincreasedtransparency,especiallyrelatingtofinancingflowstocountries.In2011and2012,PMNCHproposedoptions
17Jamison,D.T.etal.(2013).Globalhealth2035:aworldconvergingwithinageneration.The Lancet,382:1910.
13
forstrengtheningtheglobalfinancingarchitectureandthenledamulti-stakeholderprocessthatincludedin-depththinkingaroundapooledfinancingfacilityforRMNCAH.In2013,theRMNCHSteeringCommittee,supportedbytheRMNCHStrategyandCoordinationTeam,wascreatedasaplatformtobetterharmonizeandcoordinateinternationalfinancingandreporting,andstrengthenalignmentwithcountryplans,workingcloselywiththeH4+.
However,despitetherecenteffortstostrengthencoordination,themultitudeoffinancinginitiativesstillcausesfragmentationinfinancingstreamsatthecountrylevel.NationalgovernmentsroutinelydevoteconsiderableresourcestomanagingmultipleparallelinitiativesandtheassociatedplanningandreportingneedsofthemultiplepartnerssupportingRMNCAHservices.Additionally,itremainshardtotrackdonorfinancingtoRMNCAHandtodriveaccountabilityforcommitmentsmade.Fragmentationalsoleadstosuboptimaldistributionofresourcesglobally.Somecountriesreceivedisproportionatelyhighlevelsofsupportwhileothersare“donororphans”.
GOALS, PRINCIPLES AND OBJECTIVES FOR A GLOBAL FINANCING FACILITYTheunprecedentedlevelofglobalsupportforRMNCAHprovidesanopportunitytostepupeffortsandachievetheambitiousbutrealizablegoalof“convergence”by2030.Ifthisgoalistobeattained,decisiveactionisneedednowtoovercomethechallengesoutlinedabove.Simplystrengthening,expandingorcoordinatingcurrentinitiativesisunlikelytobringthetransformativeimpactrequiredtoreachtheconvergencegoal.
ThisConceptNoteoutlinesaproposalforaGlobalFinancingFacilityforRMNCAHtohelpdrivethetransformativechangeneededtopreparetheroadtoconvergence.TheoverallgoaloftheGFFwillbetocontributetotheglobaleffortstoendpreventablematernal,newborn,childandadolescentdeathsandimprovethehealthandqualityoflifeofwomen,adolescentsandchildren.Itisestimatedthatcomparedwithcurrenttrends,anacceleratedinvestmentscenariowouldhelppreventatotalof4millionmaternaldeaths,107millionchilddeaths,and22millionstillbirthsbetween2015and2030intheCountdownto2015countries(excludingSouthSudan).Intermsofeconomicbenefits,theGlobalInvestmentFrameworkestimatesthatscalingupinterventioncoveragewouldyieldhighratesofreturn,producinguptoninetimestheeconomicandsocialbenefitby2035.18Italsoemphasizesthathealthgainscanleadtowidersocietalgainsinareassuchaseducation,environment,genderequalityandhumanrights,andthatthesecan,inturn,leadtohealthbenefits.
18Stenberg,K.etal.(2014).Advancingsocialandeconomicdevelopmentbyinvestinginwomen’sandchildren’shealth:anewGlobalInvestmentFramework.The Lancet,383:1333-54..
14
Toreachthetargetsset,investmentsareneededinkeyinterventionsaswellasinkey
enablerssuchaslawsandpolicies,improvedhealthsystemsperformance,community
engagementandinnovations.Inaddition,investmentsarerequiredincross-sectoral
issuessuchasgender,equityandhumanrights.Theconceptualframeworkdeveloped
fortheGlobalInvestmentFrameworkoutlinesthekeyenablersandinterventions
leadingtolivessavedandhealthylives19andisattachedinAnnex4.
ConsistentwiththerecommendationsoftheGlobalInvestmentFrameworkand
theCommissiononInvestinginHealth,theGFFwillmobilizeandchanneladditional
internationalanddomesticresourcesrequiredtoscale-upandsustainefficientand
equitabledeliveryofqualityRMNCAHservices.Additionally,theGFFwillsupportthe
transitiontolong-termsustainabledomesticfinancingforRMNCAH.Aspecialfocus
areafortheGFFwillbetosupportthescale-upofCRVStocontributetotheuniversal
registrationofeverybirth,deathandcauseofdeathasaplatformforaccelerating
improvementsinRMNCAHby2030.
TheprinciplesoftheGFFarebasedonexistingagreementsonprinciplesofcooperation
amongkeyRMNCAHstakeholders(suchasthoseadoptedbythePMNCHBoard20):
• Country leadership and ownership,basedontheInternationalHealthPartnership(IHP+)principlesandalignedwithnational
healthsectorstrategiesandRMNCAHplans,andtheirbudget
processesandcycles;
• Efficiency focus throughscaling-upthehighestimpact,evidence-basedinterventionpackages;
• Equity focusprioritizingthedisadvantagedandmostvulnerable;
• Results focus andprioritizationofhigh-impactcountries,populationsandapproaches;
• Simplicity, alignment, and complementaritythatbuildsonthesuccessesofexistingmechanisms.
TheGFFwillconcentrateonfiveobjectives:
1. FinancenationalRMNCAHscale-upplansandmeasureresults;
19Stenberg,K.etal.(2014).Advancingsocialandeconomicdevelopmentbyinvestinginwomen’sandchildren’shealth:anewGlobalInvestmentFramework.The Lancet,383:1333-54.
20http://www.who.int/pmnch/about/governance/board/members/en/
15
2. SupportcountriesinthetransitiontowardsustainabledomesticfinancingofRMNCAH;
3. Financethestrengtheningofcivilregistrationandvitalstatisticssystems;
4. Financethedevelopmentanddeploymentofglobalpublicgoodsessentialtoscaleup;
5. ContributetoabettercoordinatedandstreamlinedRMNCAHfinancingarchitecture.
Therearemanyotherneedsrelatedtothescale-upofRMNCAHservicesthattheGFFwillnotattempttoaddress.Instead,theGFFwillworkcloselywithexistingstakeholderswhoareactivelyworkingontheseissues.Forexample,theGFFwillnotplayanormativerolewithregardtotechnicalmattersassociatedwiththedeliveryofRMNCAHservices.ThetechnicalassistanceneededtodevelopandimplementhighqualityRMNCAHplanswillmostlybeprovidedthroughpartnerswithin-countrypresenceandexistingcapacityinthisarea.
Thefacilitywillbetime-limitedandfocusedonachievingconvergencetargetsby2030;thisreinforcesasenseofurgencytoachieveresultsandtheprospectofanexitstrategyfordevelopmentpartners.
Objective 1: Finance national RMNCAH scale-up plans and measure resultsThefirstobjectiveoftheGFFistofacilitateaclearstrategyforfully-scaledandsmartfinancingofRMNCAHservicesineachcountry.Thisstrategywillbearticulatedina“financingroadmap”informedbyarights-based,results-focused,fully-costedRMNCAHnationalplanlinkedtostrategiesforhealthandothersectors21andalignedwithcountryplanningcycles.Theprocessofarticulatingtheseroadmapswillbefullyinclusive–comprisingthegovernment,privatesector22,civilsociety,anddevelopmentpartners–withastrongfocusontheneedsofvulnerablepopulations.Theroadmapswillbeguidedbyarobustfinancingframeworkthatincludescorefinancingfunctionsrelatedtoresourcemobilization,allocation,purchasing,paymentandaccountabilitywiththeaimofachievinguniversalandequitableaccesstoqualityserviceswithoutfinancialbarriersorcompromisetousers.
Thefinancingroadmapswillplaceapriorityondomesticresourcemobilizationfrompublicandprivatesourcesandexplicitlylookatneworinnovativeapproaches.
21GiventhealreadysignificantmobilizationoftheRMNCAHandhealthpartnersatthecountrylevel,theGFFwillalignwiththeseeffortsandprovidesupportwhereappropriatetostrengthennationalplanningeffortsaroundRMNCAH.
22FormoreinformationontheroleoftheprivatesectorrefertoAnnex5.
16
DevelopmentassistancethatcontributestothefullfinancingofRMNCAHstrategies23willalsobeaccountedforintheseroadmaps,irrespectiveofwhetheritisdirectedthroughdirectcontributionsincountriesbybilateralaidagencies(USAID,DFIDetc.)ormultilateralchannels(GFATM,Gavi,WorldBank).Thetotalresourcestobemobilizedwillbebasedoncosted,evidence-based,“best-buy”interventionpackagescoveringthefullcontinuumofhealthservices,andwillbeinclusiveofthecostsofthenecessaryhealthsysteminputssuchasinfrastructureandhumanresources.RecognizingthatsectorsbeyondhealthsuchaseducationandsocialprotectionarecriticalareasforinvestmenttoachieveRMNCAHgoals,theGFFwilladvocateforandfacilitate“multi-sectoral”financingopportunities.Insofarastherearesub-nationaldistributions,thesewillreflectdifferentialRMNCAHneeds.Purchasingarrangementsofserviceswilldrawongrowingevidenceofthebettervalue-for-moneythatisbeingachievedthroughresults-basedfinancing,payingforresults,vouchers,cashtransfersandothermechanisms.Strengthenedinstitutionalmechanismsandcountryplatformsrelatedtoprocurement,financialmanagement,reportingandaccountabilitywillfigurecentrallyintheplans.
Objective 2: Support countries in the transition toward sustainable domestic financing of RMNCAHAsecondobjectiveoftheGFFistosupportcountriesinanticipatingandpreparingforthetransitiontowardsustainabledomesticfinancingofRMNCAH.Inthe15-yeartimeframe(2015-2030)oftheSustainableDevelopmentGoals(SDG),manycountrieswillmovefromlow-tolower-middle-incomestatusandperhapseventoupper-middle-incomestatus.BuildingonthefinancingroadmapsdescribedinObjective1,theworkunderthisobjectivewillextendtheseroadmapsforwardtoprojectfinancingneeds,costs(accountingforfactorssuchaspopulationgrowth)andrevenuesourcesoverthe15-yearSDGperiod.Guidedbytheseprojections,anexplicitstrategytostrengthendomesticresourcemobilizationforRMNCAHwillbearticulated.Thiswillinvolveanalysesoffiscalspace,publicexpenditurereviews,andinstitutionalcapacityassessmentsthatinformtheopportunitiesandconstraintsofpublicfinanceaswellasidentificationanddevelopmentofinnovativeprivatefinancingarrangements.ExternalfundingfromdevelopmentpartnerswillseektocontributetostrengtheningandacceleratingthetransitionbylinkingexternalfinancingtodomesticresourcemobilizationtargetsandtransitioningdevelopmentassistancefromthecurrentpredominanceofgrantstowardIDAcreditsandIBRDloans.Grantswillbere-structuredtocreateincentivesforborrowing(e.g.buy-downs).Thetransitionalfinancingstrategieswillalsoincludeotherinternationalfinancingopportunitiessuchassocialimpactbonds,advancedmarketcommitmentsandpooledprocurementarrangements(seeObjective4).Thistransitionalfinancingagendawillbeexplicitlylinkedwiththebroader“financingfordevelopment”agendafortheSDGsforwhichtheWorldBankGroup(WBG)istakingaleadershiprole.
23Thealignmentofexternalfundingfromkeypartners,includingGavi,theGlobalFund,othermultilaterals(UNICEF,UNFPA),andbilaterals,canlearnfromthepositiveexperiencesinforexampleEthiopia,Rwanda,BeninandBurundiwheredevelopmentpartnershavejointlyfinancedcountrystrategieswithcommonindicatorsandaccountabilitymechanisms.
17
Objective 3: Finance the strengthening of civil registration and vital statistics systemsAvailabilityofaccurate,timely,andconsistentcauseofdeathandvitalstatisticsdatageneratedbyCRVSsystemsatthenationalandsub-nationallevelsiscrucialforcountriestobeabletoeffectivelymanagetheirhealthsystems,allocateresourcesaccordingtoneedand,importantly,ensureaccountabilityfordeliveringonRMNCAHcommitments.ThereisgrowingrecognitionthattheseCRVSsystemsrequiredeliberateanddedicatedstrategiesandinvestmentstobestrengthened.TheworkofboththeIndependentExpertReviewGroup(iERG)andtheUNCommissiononInformationandAccountabilityhighlightedthecriticalneedtoimprovecoverageandqualityofinformationsystems.Alongsidethisconsensus,the“leap-frog”opportunitiesinherentine-andm-healthapplicationstostrengthenCRVSsystemsandinformationforbothprovidersandusersofRMNCAHserviceshavebeenrecognized.24TheGFFwillfinancecoordinatedinvestmentsinstrengtheningthecapacitiesrequiredatalllevelsofthehealthsystemtoregisterbirthsanddeathsandcausesofdeath,andgenerateandusethesevitalstatistics.
CRVSsystemsareanespeciallyimportantinformationplatformforcountingthelivesanddeathsofeverywomanandeverychild.ThepoorstateofCRVSsystemsinmanycountries,coupledwiththeopportunitiesemergingfrominnovativeapplicationofinformationandcommunicationstechnologies(ICTs)andacknowledgedpoliticalcommitmentatthecountryandregionallevels,hasledtheRMNCAHcommunity,throughtheiERG,toadvocateforstrongerandscaled-upCRVSinallcountries.AstrongCRVSthatcoversanentirecountryoffersanunprecedentedopportunityforareal-timescorecardthatcantrackprogresstowardthe2030targetsofendingpreventablematernalandchilddeaths.Thisopportunityisalsorecognizedinastrategyandinvestmentplantostrengthenandscale-upCRVSrecentlypublishedbytheWorldHealthOrganization(WHO)andtheWorldBank.
BuildingontheworkoftheGovernmentofCanada,theWorldBankandWHO,andusingadedicatedwindow,theGFFwillsupportthisCRVSscale-upsuchthatby2030therewillbeuniversalregistrationofeverybirthanddeath(includingcauseofdeath).25 AchievingthisobjectiveentailsworkingwithabroadersetofstakeholdersandsectorsthanwouldnormallybeidentifiedaspartoftheRMNCAHcommunitytoarticulatemulti-sectoralCRVSinvestmentplans.TheGFFwillfacilitatetheproductionoftheseplanswithinputsfromallpartners,andwillfocusonmobilizingtherightmixofdomesticandinternationalresourcesrequiredtoaccelerateimprovementsandsustainCRVSsystemsby2030(asperObjective2above).ItwillalsosupportaCenterofExcellenceforCRVSthatarticulatesbestpracticesandshareslessonsonimplementation.
24WorldHealthOrganization.(2013).StrengtheningCRVSthroughInnovativePracticesintheHealthSector:GuidingPrinciplesandGoodPractices,http://www.who.int/healthinfo/civil_registration/crvs_meeting_dec2013_report.pdf?ua=1
25WorldBank-WHO(2014)GlobalCivilRegistrationandVitalStatisticsScalingupInvestmentPlan2015–2024.http://www.worldbank.org/en/topic/health/publication/global-civil-registration-vital-statistics-scaling-up-investment
18
Objective 4: Finance the development and deployment of global public goods essential to scale upGlobalpublicgoodscanhelptoacceleratetheaffordabilityandaccessibilityofRMNCAHservicesbybreakingthroughknowledge,know-how,priceandtechnologybarriersandbottlenecks.TheGFFwillworkwithpartnerstoidentifypromisingareasforthedevelopmentanddeploymentofglobalpublicgoods.Investmentareasmayincludemarketshapingtoensuresustainableaccesstokeycommodities,technologicaldevelopmentsthatsimplifydelivery,innovationsinthedeliveryofservicessuchastask-shiftingandimpactassessmentsthatinformwaysofovercomingbottleneckstoimplementation.Agoodexampleofapromisinginvestmentistotranslateglobalinteragencyeffortstoalignsupplychainmanagementintoappropriateandeffectivecountry-levelresponsesfordeliveringcommoditiesto“lastmile”facilities.TheGFFfinancingcansupplementavailablefinancingfromothersourceswhereneeded.Thiswillmostlybedonethroughimplementingpartnerswhowillbeselectedbasedonthenatureofthespecificactivity.
Objective 5: Contribute to a better-coordinated and streamlined RMNCAH financing architecture Beyonditsspecificfinancingobjectives,theGFFaimstocontributetoabetter-coordinatedandstreamlinedRMNCAHfinancingarchitectureatthecountryandgloballevelbyprovidingaplatformforcoordinationaroundfinancingofRMNCAHandbyfacilitatingtheconvergenceandconsolidationoffragmentedRMNCAHfinancingstreams.Whileacentralaimoftheseeffortsistoreduceunreasonablyhightransactioncostsforcountriesaswellasotherpartners,greateralignmentaroundtheroadmapswillimproveleverageprospectsforindividualinvestorsaswellasgreaterefficiencyandeffectivenessofthoseinvestments.Evidenceontheleverageratiosandvalue-for-moneyofinvestmentsareincreasinglyimportantcriteriaforsustainingtheresourcecommitmentsofdevelopmentpartners.
Aspartoftheplanningprocessforthelongtermfinancialroadmaps,theGFFwillfacilitatemoreefficientandcompletefinancingofRMNCAHplansatthecountrylevelbydevelopinglong-termstrategiesforfinancingandworkingwithpartnerstobetteralign,andwherepossiblepool,fundingforefficientimplementationoftheplans.MoredetailonthecoordinationandconsolidationobjectiveoftheGFFisincludedinthegovernancesectionofthisConceptNote.
19
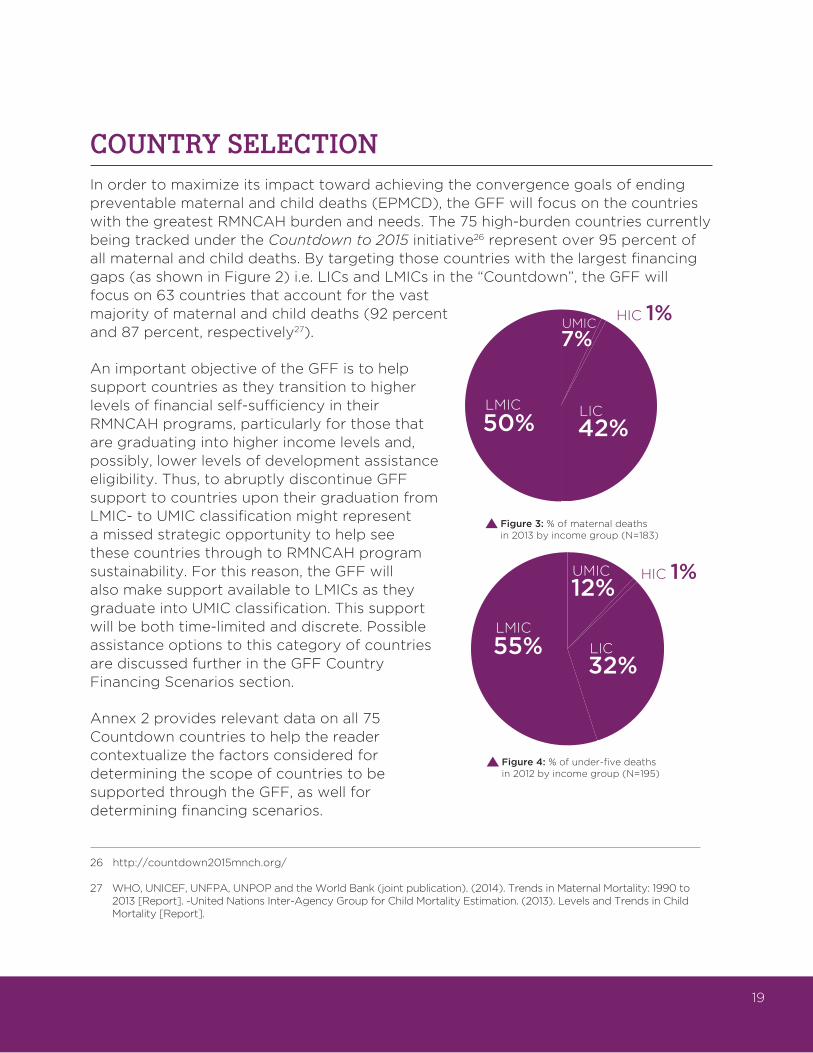
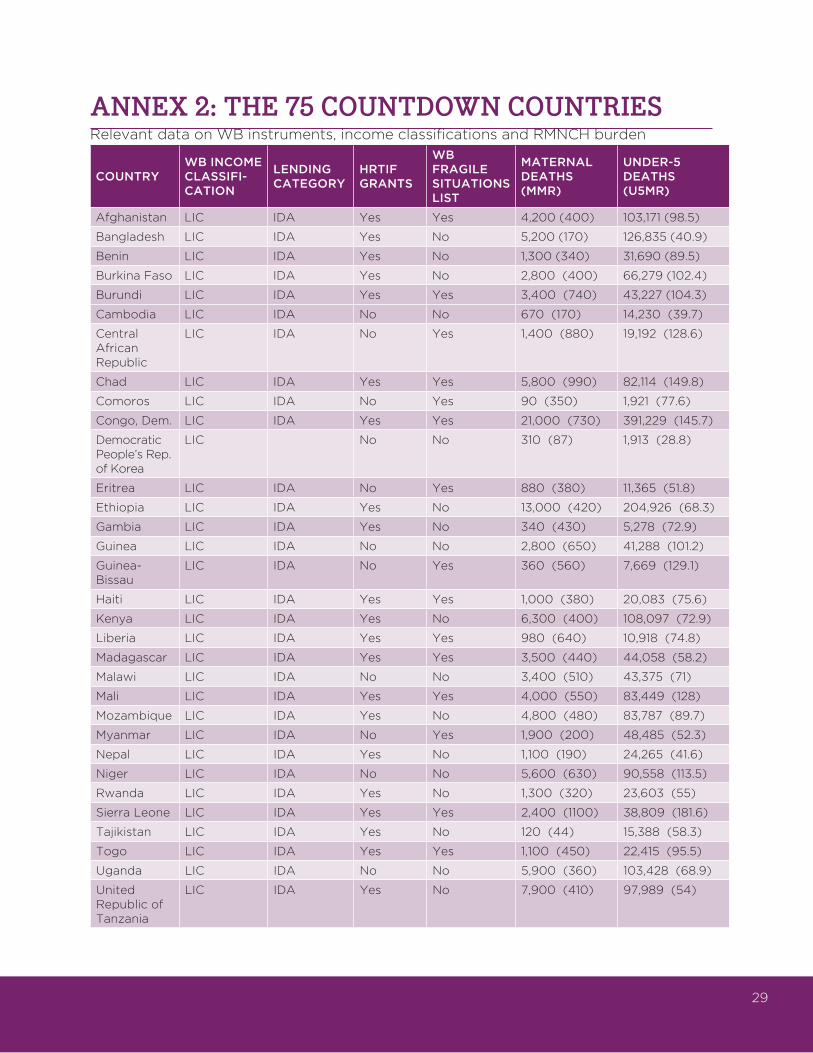
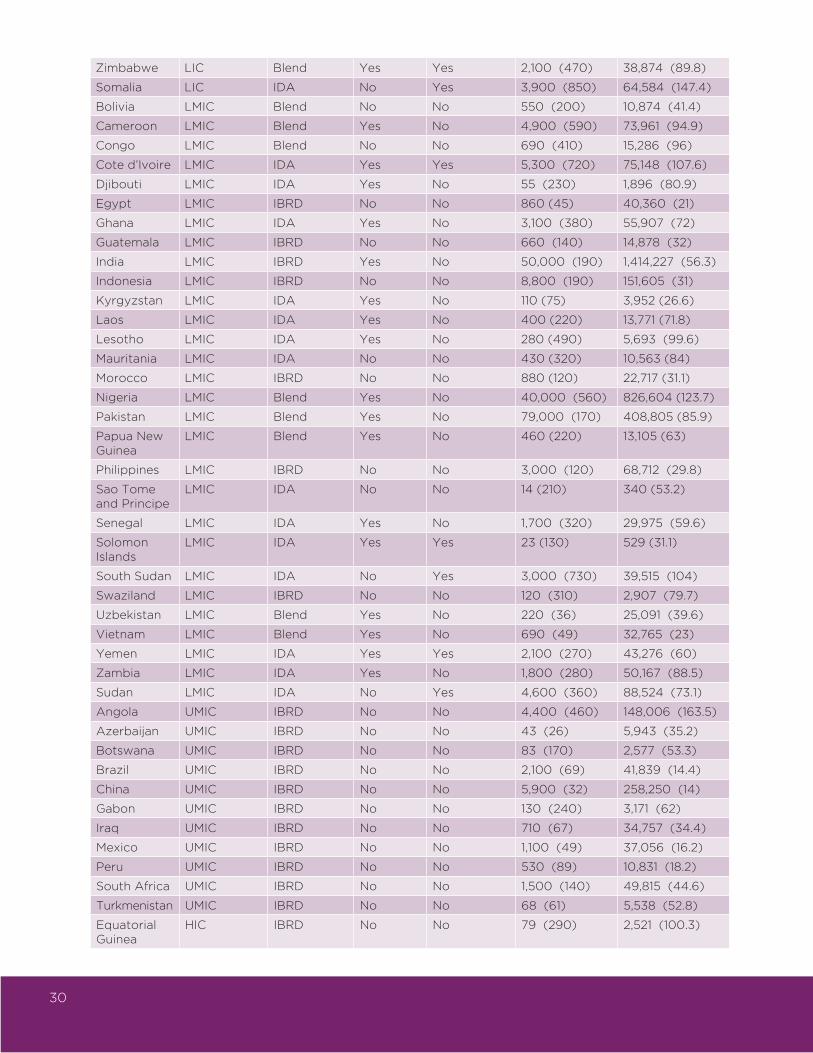
COUNTRY SELECTIONInordertomaximizeitsimpacttowardachievingtheconvergencegoalsofendingpreventablematernalandchilddeaths(EPMCD),theGFFwillfocusonthecountrieswiththegreatestRMNCAHburdenandneeds.The75high-burdencountriescurrentlybeingtrackedundertheCountdown to 2015 initiative26representover95percentofallmaternalandchilddeaths.Bytargetingthosecountrieswiththelargestfinancinggaps(asshowninFigure2)i.e.LICsandLMICsinthe“Countdown”,theGFFwillfocuson63countriesthataccountforthevastmajorityofmaternalandchilddeaths(92percentand87percent,respectively27).
AnimportantobjectiveoftheGFFistohelpsupportcountriesastheytransitiontohigherlevelsoffinancialself-sufficiencyintheirRMNCAHprograms,particularlyforthosethataregraduatingintohigherincomelevelsand,possibly,lowerlevelsofdevelopmentassistanceeligibility.Thus,toabruptlydiscontinueGFFsupporttocountriesupontheirgraduationfromLMIC-toUMICclassificationmightrepresentamissedstrategicopportunitytohelpseethesecountriesthroughtoRMNCAHprogramsustainability.Forthisreason,theGFFwillalsomakesupportavailabletoLMICsastheygraduateintoUMICclassification.Thissupportwillbebothtime-limitedanddiscrete.PossibleassistanceoptionstothiscategoryofcountriesarediscussedfurtherintheGFFCountryFinancingScenariossection.
Annex2providesrelevantdataonall75CountdowncountriestohelpthereadercontextualizethefactorsconsideredfordeterminingthescopeofcountriestobesupportedthroughtheGFF,aswellfordeterminingfinancingscenarios.
Figure 3: % of maternal deathsin 2013 by income group (N=183)
Figure 4: % of under-five deathsin 2012 by income group (N=195)
32%
12%
55%LMIC
UMIC
LIC
HIC 1%
42%
7%
50%LMIC
UMIC
LIC
HIC 1%
26http://countdown2015mnch.org/
27WHO,UNICEF,UNFPA,UNPOPandtheWorldBank(jointpublication).(2014).TrendsinMaternalMortality:1990to2013[Report].-UnitedNationsInter-AgencyGroupforChildMortalityEstimation.(2013).LevelsandTrendsinChildMortality[Report].
20
COUNTRY ACCESS TO FINANCINGApre-requisiteforreachingthepost-2015targetsofendingpreventablematernalandchilddeathswillbetheimplementationofcountry-specificplanswithcleartargets,prioritysettingofkeyinterventionsandarticulationoftheirdeliverystrategies.Furthermore,theplansneedtolinktothenationalhealthplansandothersectoralplansthatbearonthehealthofwomenandchildren,andtonationaldevelopmentplans.Inaddition,theymustrespondtothecountryspecificcontextandbebasedonthebestavailableevidence.Countryownershipwillbeakeyoperatingprincipleinallaspectsofthework,withgovernments,ministriesofhealthandotherrelevantactorsplayingacentralleadershiproleinplanning,coordinationandoversight,andensuringcoherenceintheimplementation,monitoringandreportingofstrongnationalRMNCAHplans.TheprocessofarticulatingtheseplanswillbuilduponexistingcoordinatingmechanismssuchasIHP+.RecognizingthecriticalroleoftheH4+inthearticulationandimplementationoftheseplans,theGFFwilladvocateforfullfinancingofH4+andothertechnicalpartnersincarryingouttheseessentialfunctions.
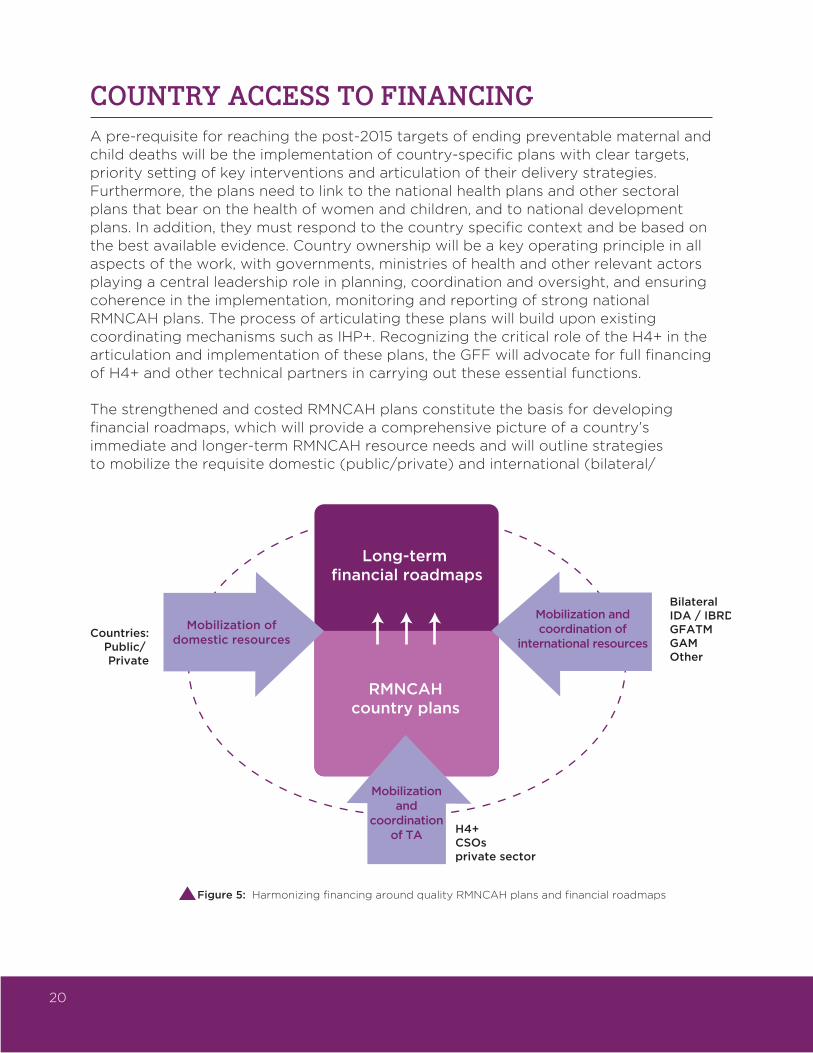
ThestrengthenedandcostedRMNCAHplansconstitutethebasisfordevelopingfinancialroadmaps,whichwillprovideacomprehensivepictureofacountry’simmediateandlonger-termRMNCAHresourceneedsandwilloutlinestrategiestomobilizetherequisitedomestic(public/private)andinternational(bilateral/
Long-term financial roadmaps
RMNCAHcountry plans
Mobilization ofdomestic resources
Mobilization andcoordination of
international resources
Mobilizationand
coordinationof TA
BilateralIDA / IBRDGFATMGAMOther
Countries:Public/ Private
H4+CSOsprivate sector
Figure 5: Harmonizing financing around quality RMNCAH plans and financial roadmaps
21
multilateral/private)fundingovertime.Theroadmapwillreflectthebroaderpictureofeconomicgrowth,nationalhealthpriorities,andtheoverallbudget-andfiscalspaceforthehealthsector.Theprocessfordevelopingfinancialroadmapswillinvolvestrongcountry-basedanalyticalworkthatlinkswithnationalplanningaswellasbudgetingmechanisms,cyclesandprocesses.
Together,theRMNCAHplansandfinancialroadmapswillbethebasisfortheharmonizationofthevariousstreamsoffinancing–bothdomestic(public/private)andinternational(bilateral/multilateral/private)–aroundtheoverallplan,therebymaximizingtheimpactandprogrammaticcoherenceofallpartners’in-countryRMNCAHsupport.TheaimistoharmonizefundingforRMNCAHplansthroughpoolingresourcesaroundacommoncountryfinancingframeworklinkedtoclearresultsandbacked-upbycommonaccountabilityandreportingmechanisms.TheGFFwillhavetheflexibilitytoadaptbasedoncountryspecificanddonorfinancingrequirements.AnexampleofaninnovativepartnershiptoimproveRMNCAHoutcomesfromtheDemocraticRepublicofCongo(DRC)canbefoundinAnnex6.
GFF COUNTRY FINANCING SCENARIOSTheGFFfinancingroadmapswillbedesignedtocatalyzeandsustainprogresstowardnationalRMNCAHobjectives.Morespecifically,theyaimto:(i)mobilizedomesticresourcesacrossthepublicandprivatesectors;ii)scaleinternationalfinancingtocomplementdomesticresourcesandprovideastrongleveragerationaleforindividualinvestors;(iii)improvetheefficiencyofinvestmentswithrespecttoachievingresults;and(iv)makethelonger-termsustainabilityoffinancingforRMNCAHanexplicitandfeasiblestrategy.Tofulfilltheseaims,theGFFanditspartnerswilldrawuponamenuofavailablefinancingoptionsrangingfrommoretraditionalinstrumentssuchastaxes,grants,credits,loansandguarantees,tomoreinnovativeapproachessuchasimpactbonds,buy-downsandhealthtransformationfunds.LeveragingpartnerfinancingtoolsandresourceswillprovidetheopportunityformoreharmonizedfinancingforRMNCAHacrossdomesticandinternationalpartners.Drivenbythespecificcontextofeachcountry,theGFFroadmaps,forexample,willleadtoavarietyoftangiblefinancingresultssuchas:ensuringthatallinternationalfinancingforRMNCAHisonbudgetandadditional,earmarkingspecificbudgetallocationtargetsforRMNCAHunderreduceddebtserviceobligations,linkingfinancetoattainmentofRMNCAHresultsacrossthesystemthroughPayforResultsapproaches,andacceleratingpolicyandinstitutionalreformstoscaleupandmakedomesticRMNCAHfinancingmoresustainable(e.g.throughDevelopmentPolicyCredits/Loans).
GFFfinancingofroadmapsandinstrumentswillbetailoredtospecificcountryneeds.Whilefinaleligibilitycriteriahaveyettobeagreedupon,fourcountrygroupscanbe
22
envisaged,allfacinghighRMNCAHburdens28butdifferentfinancingchallengesduetotheireligibilityforexternalfundingandincomelevels.Theseinclude:(1)LICsnotexpectedtotransitiontoLMICstatusintheforeseeablefuture;(2)LICstransitioningtoLMICstatus;(3)LMICs;and(4)LMICstransitioningtoUMICstatus.29
TheGFFwillsupportacountry’stransitionalfinancingthroughmultiplesetsofinstrumentsandapproaches.MoredetailsonthefinancialroadmapsforRMNCAHcanbefoundinAnnex7.
Low-income countries: ThisgroupwillincludethepoorestcountrieswithhighRMNCAHburdens,noneofwhichareexpectedtotransitiontolowermiddle-incomestatusintheforeseeablefuture.CountryexamplesincludeBurundiandtheDemocraticRepublicofCongo.GFFgrantswillfocusoncomplementingexistingresourcestoreduceout-of-pocketexpendituresandachievehighercoverageofkeyRMNCAHinterventions.WithdisbursementslinkedtoRMNCAHresults,suchgrantswillalsoencouragecountriestoseekadditionalgrantfundingand/orconcessionalloans(forexampleIDAgrantsandcredits)aswellascommitlocalresourcestoaccelerateprogress.GFFgrant-financedtechnicalassistancewillfocusonlayingthefoundationsofgoodpublicfinancialmanagementtoensurethatfundsactuallybenefitmothersandchildren.InLICsexperiencingpoliticalinstabilityandconflict,suchastheCentralAfricanRepublic,publicfinancinganddeliverysystemsmayproveunfitforthispurposeandGFFgrantswillusealternativefinancingroutestoensureaccesstobasicRMNCAHservices,includingdirectfinancingofnon-governmentalorganizations(e.g.civilsocietyandinternationalorganizations)orevenhumanitarianinterventions.
Low-income countries in the transition to lower-middle-income status:Thisgroupwillincludehigh-burdenLICstransitioningintoLMICstatussuchasUgandaandKenya.GFFgrantswillaimtoincreasecoverageofkeyRMNCAHinterventions,butwouldadoptdesignsthatfacilitatedomesticresourcemobilizationtosustainthegrowthinRMNCAHfinancingwhenoverallexternalassistancedeclines.GFFgrantswillfinancebuy-downsofinterest,principleofcreditsorloans,oranycombinationoftheseitems(e.g.WBIDAcreditsandIBRDloans),encouragingcountriesnotonlytoborrowforRMNCAH,butalsotocommittospecificbudgetallocationtargetsforRMNCAH.Suchgrants,creditsandloanswillbedisbursedagainsttheattainmentofRMNCAHresults(e.g.throughPayforResultsapproaches)aswellastheimplementationofpolicyandinstitutionalactionsthatscale-upandmakedomesticRMNCAHfinancingmoresustainable(e.g.throughDevelopmentPolicyCredits/Loans).GFFgrantswillalsofinancetechnicalassistancetosupportsuchpolicyandinstitutionalactions.Thisincludes,forexample,stepsthatbuildonearlierpublicfinancialmanagementreformstoimproveprocurement,financialandhuman
28“Highburden”referstoacountry’sdesignationasoneofthehigh-burden,priorityRMNCAHcountriesundertheCountdowninitiative,asdescribedearlierinthisnote.
29Theinstrumentsandtoolsdescribedinthefollowingparagraphsareindicativeandnotnecessarilyavailabletoallwithineachgrouping,norunavailabletoothergroupings.Eligibilityforeachinstrumentortoolisbasedonanumberoffactors,andnotstrictlyonincomeclassification.
23
resourcemanagementaswellastheintroductionofmoreadvancedproviderpaymentsmechanisms(particularlypayforperformancearrangements)withthepotentialtoenhancethequalityandefficiencyofRMNCAHservices.Moreover,technicalassistancewillsupportinnovationstobroadenthedomesticrevenuebaseforRMNCAHby,forexample,emulatingreformsprovensuccessfulinupper-middleandhigh-incomecountriessuchassintaxes.Incountrieswithrapideconomicgrowth,supportwillfocusoninnovationstostrengthentheoftenweaklinkbetweeneconomicgrowthandspendingonRMNCAHby,forexample,capturingrevenuesfromextractiveindustriesandinvestingtheminRMNCAH.
Lower-middle-income countries: Thisgroupwillincludesomelargecountrieswiththehighestnumbersofmaternal-andchilddeaths,suchasIndia,NigeriaandPakistan.Inthesecountries,markedimprovementsinthecoverageandqualityofRMNCAHinterventionswouldhaveasignificantimpactontheglobalRMNCAHburden.SimilartofinancingmodalitiesincountriestransitioningtoLMICstatus,GFFgrantswillleverageloanswithdisbursementslinkedtoRMNCAHresultsandpolicyandinstitutionalreformsoffinancingarrangementsforRMNCAH.Suchgrantsandloans,however,willbecontingentuponsignificantincreasesinRMNCAHfinancingfromgeneraltaxrevenue.GFFgrantswillalsofinancetechnicalassistancetodeepenreformsofpublicfinancialmanagement,paymentandrevenuesystems.Inaddition,theywillhelpcountriestacklethegrowinginequalitiesinRMNCAHfinancingandservicedeliverytypicalforthisstageoftheeconomictransitionbytargetingpublicresourcestothepoorandequalizinggeographicalandfiscalimbalances.Oftenthisisdoneinthecontextofdecentralizingpowerandfunctionstolowerlevelsofgovernment.
Lower-middle-income countries in the transition to upper-middle-income country status: ThisgroupwillincludecountriesthatreceivedGFFsupportasLMICs,which–upontheirgraduationtoUMICstatus–wouldbenefitfromcontinuedsupporttoexpandRMNCAHgainswhileachievingfinancialsustainability.Thesupportwillbelimitedintime(e.g.3yearsaftergraduationtoUMICstatus)andscope(e.g.grantsfinancingtechnicalassistancetodeepen,completeandassessreformsanddevelopconsecutivephasesoffinancingroadmaps).Atthesametime,thisgroupofcountrieswillremaineligibleforIBRDlendingandtheWorldBankGroupwillencouragethemtodrawupontheseloanstodeepencoverageandimprovethequalityofRMNCAHservices.
GOVERNANCE AND INSTITUTIONAL ARRANGEMENTSThissectionoftheConceptNoteoutlinestheinstitutionalandgovernancearrangementsfortheGFF.Itdescribestheguidinggovernanceprinciples,therationalefortheWorldBankhostingtheGFFandthreegovernancecapabilitiestheGFFneedstosecure.
24
Governance principles TheroleofGFFgovernanceistoprovidetheoversight,strategicguidanceandwell-coordinateddecision-makingrequiredfordeliveringonthecorefunctionsoftheGFF.Inordertodoso,GFFgovernancearrangementswillbeguidedbythefollowingkeyprinciples:
• Country-driven: Forgeviablefinancingroadmaps,alignitselfandworkeffectivelywiththepolicyandplanningcyclesanddevelopmentpartnercoordinationmechanismsrelatedtoRMNCAH,healthandothersectorsthatarespecifictoeachcountry.
• Inclusive and streamlined: Engageallmajorfinancialpartners–domestic/international,public/private–supportingRMNCAH, withtheaimofstreamliningthefinancialarchitectureforRMNCAH.
• Responsive and accountable: Deliverfinancialservicesthataretailoredtocountryneedsinatimelyandcost-efficientway.
• Scale and leverage:InfluencesignificantflowsofinternationaldevelopmentassistanceforRMNCAHthatofferleverageincentivestoRMNCAHinvestors.
• Aligned and synergistic:Workwithandpromotetheconsensusstrategies,publicgoodsandtechnicalassistanceservicesofferedbydiversepartners–multilateral,bilateral,privatesectorandCSOs–undertheEWECumbrella.
Institutional arrangementsWhilethereare,inprinciple,anumberofinstitutionalandhostingoptionsfortheGFF,itisproposedthattheGFFbelocatedattheWorldBankforthefollowingreasons:
• Credibility and mandate: TheWorldBankGroupisplayingaleadingroleinarticulatingthefinancingneedsandarchitectureforthepost-2015developmentgoalsandwillplayanimportantroleinfinancingforthenewgoals.
• Proven leverage: AshasbeenseenoverthelastfiveyearsoftheHRITF,channellinggrantfinancingthroughtheWorldBankcreatesanopportunitytounlockfarlargerinvestmentsintheformofcreditsandloansfromIDAandIBRDthatareanchoredinthefiscalaccountsofcountries.
• Multi-sectorality: ManyofthecriticalinterventionsnecessarytoachieveacceleratedRMNCAHresultslieoutsidethehealthsector.
24
25
TheWorldBank,byvirtueofitsoverarchingdevelopmentfocus,canmobilizeco-investmentsinsectorssuchaseducation,socialprotection,waterandsanitationandmacro-fiscalpolicy,amongothers.Inaddition,theprivatesectorarmoftheWorldBank–theInternationalFinanceCorporation–canbetappedtoengageprivatesectorpartnersmoresystematically.
• Hit the ground running: GiventhattheHRITFanditssecretariathousedattheWorldBankarealreadyupandrunning,theGFFwillbeabletomoveforwardswiftlyandefficientlywiththeworkontheground.
• Expertise on financing: TheWorldBankhasthedepthandbreadthofexpertiserelatedtothefullrangeoffinancingchallengesthatwillfigureprominentlyinthefinancingroadmapsoftheGFF.Thesechallengesincludepurchasingandprocurementandfinancialmanagementandaccountability.Further,theBank’scloseworkingrelationshipwithministriesoffinancewillhelptoforgenecessarylinkageswiththebroaderandlonger-termfinancingpoliciesforhealth.
Core GFF capabilitiesTheGFFrequiresatleastthreedifferentgovernancecapabilitiesinordertoachieveitsobjectives.Thefirst capabilityrelatestosupportingcountry-basedmechanismsthatwillpermitthearticulationandimplementationofthefinancingroadmapsthrougheffectiveconveningandbuildingalliancesamongallmajorstakeholders,whichGFFgovernanceshouldfacilitate.Developinghigh-qualityfinancingroadmapsinvolvesbothcontentandprocessdimensions.ThecontentrelatestothecostingofRMNCAHplans,identifyingdomesticandinternationalsourcesoffinancing,specifyingprocurementandpurchasingarrangementsaswellasfinancialmanagementandprojectionsrelatedtosustainability.Theprocessrelatestothealignmentwithplanningcycles,theengagementofkeystakeholdersintheRMNCAHcommunity–bothdomestic(public/private)andinternational(bilateral/multilateral/private)–andgeneratingconsensuson,orbuy-in,toplans.Achievingthiswillrequireeffectiveconveningandbuildingalliancesamongallmajorstakeholders,whichGFFgovernanceshouldfacilitate.
A second governance capabilityoftheGFFrelatestoitsabilitytoberecognizedasamajorsourceofinternationalfinancingfortheRMNCAHagendathroughdedicatedfinancingwindows.Inthisregard,theGFFgovernancestructurewillbuildontheexistingHRITFattheWorldBankinordertoallowforarapidaccelerationofinvestmentsinRMNCAHthatoffergoodleverage,highvalue-for-moneyandlowadministrativecosts.MoreinformationontheHRITFisinAnnex8.ThescopeoftheexistingHRITFwillbeexpandedfromitscurrentfocusonservicedeliverytothefinancingofcomprehensiveRMNCAHplanswiththepossibilityofalsofundingacrosssectors.Assuch,thecountryplatformdevelopedthroughtheHRITFwillfacilitatetheconveninganddevelopmentoffinancingroadmaps.TheGFFplatformwillalsofacilitatethedevelopmentofadedicatedmulti-sectoralwindowforthefinancing
26
ofCRVSandanotherwindowwillfinanceglobalpublicgoodsandnormativeandtechnicalassistancefunctionscriticalforRMNCAHscaleup.ThiscanincludefinancingforUNtechnicalagencies,NGOsandtheprivatesector.Theoperationaldetailsforthesefinancingwindows,criteriaforcountryeligibility,financinganddecision-makingwillbespecifiedinthedevelopmentofthebusinessplan.
A third governance capabilityfortheGFFrelatestoglobalconvening,coordinationandcommunicationamongstkeystakeholders.TheGFFneedstoconveneafullrangeofpartnersincludingclientcountries,thepublic,privateandnongovernmentalsectors,andbilateralandmultilateralagencies.TogethertheGFFpartnersmustpromoteeffectiveandefficientconvergenceonthestrategiesandopportunitiestoachievetheobjectivesoffullyscaled,smartandsustainablefinancingoftheRMNCAHagenda.
Further,theremustbeacapacitytomonitorandreviewprogressagainstanagreedsetoffinancingtargetsthatreflecttheoverallaimsandobjectivesoftheGFF.Finally,theGFFmustbeabletoissue,advocateandactonrecommendationstoimproveperformance.ItisrecognizedthatthisgovernancecapabilityoftheGFFneedstoalignwith,orbepartofaconsolidationof,existingsteeringandcoordinatingmechanismsthatcurrentlypopulatetheRMNCAHgloballandscape.
NEXT STEPS AND TIMELINEFollowingthedevelopmentoftheConceptNoteandtheinitialcommitmentsattheUNGeneralAssembly2014,thefocuswillbeonkeepingthemomentumforimplementationandscaleupofsuccessfulprogramsunderthecurrentportfolio.Therewillbeastrongemphasisonexpandingexistingpackagesofservicestoincorporateagreed-uponpriorityareasincludingnewborncareandadolescenthealth,aswellasincreasesingeographicalscopeandequityfocustoachievemaximumimpact,particularlyforpoorandvulnerablegroups.
ThesecondphaseoftheplanningprocesswillfocusonthedevelopmentoftheBusinessPlanfortheGFF.DuringbusinessplanningthefulloperatingmodelincludingthefinancingwindowforCRVSwillbedeveloped.Thebusinessplanwillalsobeinformedbythecurrentmobilizationofpartnersaroundregions(inthecaseofCRVS)andspecificcountries,suchastheDRC.Bybuildingonexistingin-countrymomentumthereisanopportunitytoacceleratetheachievementofresultsundertheGFF.
Morein-depthanalysiswilltakeplaceonthestructureandcontentofthefinancingroadmap,includingthedevelopmentofcountryexamples.Theworkonthebusinessplanwillbeinformedbyin-depthconsultationswithcountries,donorsandotherpartners.
UponcompletionofthebusinessplanbyMay2015thefulloperationalizationoftheGFFwillbegin.ThegoalisfortheGFFtobefullyoperationalaroundthetimeoftheUNGeneralAssemblyin2015.

27
ANNEX 1: GFF WORKING GROUP MEMBERSHIP
NAME TITLE
MinisterKesetebirhanAdmasu MinisterofHealth,Ethiopia
MichaelAnderson CEO,Children’sInvestmentFundFoundation
SuprotikBasu CEO,UNSecretaryGeneral’sSpecialEnvoyforFinancing theHealthMDGsandforMalaria
PascalBijleveld RMNCHStrategyandCoordinationTeam,UNICEF
Dr.FlaviaBustreo AssistantDirector-General,Family,Women’sand Children’sHealth,WorldHealthOrganization
KathyCalvin President&CEO,UnitedNationsFoundation
JoanneCarter ExecutiveDirector,Results
Dr.MickeyChopra ChiefofHealth,UNICEF
Dr.MariamClaeson Director,MaternalNewbornandChildHealth, TheGatesFoundation
KateDodson VPofGlobalHealth,UnitedNationsFoundation
Dr.JaneEdmondson GroupHead,HumanDevelopment,DFID
Dr.TimEvans SeniorDirectorofHealth,Nutrition,Population, TheWorldBankGroup
Dr.ToreGodal SpecialAdvisoronGlobalHealth,Officeofthe PrimeMinisterofNorway
DianeJacovella AssistantDeputyMinister,ForeignAffairs,Trade andDevelopment,Canada
JosianeKamikazi TechnicalAdviser,MinisterofFinance,Burundi
HindKhatib-Othman ManagingDirector,Gavi,theVaccineAlliance
MichaelKlosson VicePresident,Policy&HumanitarianResponse, SavetheChildren

28
AlexiaLatortue DeputyAssistantSecretaryforInternationalDevelopment &Debt,USDepartmentoftheTreasury
Dr.ChristopherMacLennan DirectorGeneral,DepartmentofForeignAffairs, Trade&Development,Canada
JacquelineMahon SeniorPolicyAdviser,GlobalHealth&HealthSystems, UNFPA
JoanneManrique President,CenterforGlobalHealthandDiplomacy
Dr.AndersNordstrom AmbassadorforGlobalHealth,Ministryfor ForeignAffairs,Sweden
Dr.ArielPablosMendez AssistantAdministratorforGlobalHealth,USAID
Dr.CarolePresern ExecutiveDirector,PartnershipforMaternal, Newborn&ChildHealth
AnnStarrs President&CEO,GuttmacherInstitute
NanaTaonaKuo Sr.Manager,EveryWomanEveryChild,UnitedNations
Dr.AlbertWeloKalema Délégué,DemocraticRepublicoftheCongo
MarijkeWijnroks ChiefofStaff,GFATM
29
ANNEX 2: THE 75 COUNTDOWN COUNTRIESRelevantdataonWBinstruments,incomeclassificationsandRMNCHburden
COUNTRYWB INCOME CLASSIFI-CATION
LENDING CATEGORY
HRTIF GRANTS
WB FRAGILE SITUATIONS LIST
MATERNAL DEATHS (MMR)
UNDER-5 DEATHS (U5MR)
Afghanistan LIC IDA Yes Yes 4,200(400) 103,171(98.5)
Bangladesh LIC IDA Yes No 5,200(170) 126,835(40.9)
Benin LIC IDA Yes No 1,300(340) 31,690(89.5)
BurkinaFaso LIC IDA Yes No 2,800(400) 66,279(102.4)
Burundi LIC IDA Yes Yes 3,400(740) 43,227(104.3)
Cambodia LIC IDA No No 670(170) 14,230(39.7)
CentralAfricanRepublic
LIC IDA No Yes 1,400(880) 19,192(128.6)
Chad LIC IDA Yes Yes 5,800(990) 82,114(149.8)
Comoros LIC IDA No Yes 90(350) 1,921(77.6)
Congo,Dem. LIC IDA Yes Yes 21,000(730) 391,229(145.7)
DemocraticPeople’sRep.ofKorea
LIC No No 310(87) 1,913(28.8)
Eritrea LIC IDA No Yes 880(380) 11,365(51.8)
Ethiopia LIC IDA Yes No 13,000(420) 204,926(68.3)
Gambia LIC IDA Yes No 340(430) 5,278(72.9)
Guinea LIC IDA No No 2,800(650) 41,288(101.2)
Guinea- Bissau
LIC IDA No Yes 360(560) 7,669(129.1)
Haiti LIC IDA Yes Yes 1,000(380) 20,083(75.6)
Kenya LIC IDA Yes No 6,300(400) 108,097(72.9)
Liberia LIC IDA Yes Yes 980(640) 10,918(74.8)
Madagascar LIC IDA Yes Yes 3,500(440) 44,058(58.2)
Malawi LIC IDA No No 3,400(510) 43,375(71)
Mali LIC IDA Yes Yes 4,000(550) 83,449(128)
Mozambique LIC IDA Yes No 4,800(480) 83,787(89.7)
Myanmar LIC IDA No Yes 1,900(200) 48,485(52.3)
Nepal LIC IDA Yes No 1,100(190) 24,265(41.6)
Niger LIC IDA No No 5,600(630) 90,558(113.5)
Rwanda LIC IDA Yes No 1,300(320) 23,603(55)
SierraLeone LIC IDA Yes Yes 2,400(1100) 38,809(181.6)
Tajikistan LIC IDA Yes No 120(44) 15,388(58.3)
Togo LIC IDA Yes Yes 1,100(450) 22,415(95.5)
Uganda LIC IDA No No 5,900(360) 103,428(68.9)
United RepublicofTanzania
LIC IDA Yes No 7,900(410) 97,989(54)
30
Zimbabwe LIC Blend Yes Yes 2,100(470) 38,874(89.8)
Somalia LIC IDA No Yes 3,900(850) 64,584(147.4)
Bolivia LMIC Blend No No 550(200) 10,874(41.4)
Cameroon LMIC Blend Yes No 4,900(590) 73,961(94.9)
Congo LMIC Blend No No 690(410) 15,286(96)
Coted’Ivoire LMIC IDA Yes Yes 5,300(720) 75,148(107.6)
Djibouti LMIC IDA Yes No 55(230) 1,896(80.9)
Egypt LMIC IBRD No No 860(45) 40,360(21)
Ghana LMIC IDA Yes No 3,100(380) 55,907(72)
Guatemala LMIC IBRD No No 660(140) 14,878(32)
India LMIC IBRD Yes No 50,000(190) 1,414,227(56.3)
Indonesia LMIC IBRD No No 8,800(190) 151,605(31)
Kyrgyzstan LMIC IDA Yes No 110(75) 3,952(26.6)
Laos LMIC IDA Yes No 400(220) 13,771(71.8)
Lesotho LMIC IDA Yes No 280(490) 5,693(99.6)
Mauritania LMIC IDA No No 430(320) 10,563(84)
Morocco LMIC IBRD No No 880(120) 22,717(31.1)
Nigeria LMIC Blend Yes No 40,000(560) 826,604(123.7)
Pakistan LMIC Blend Yes No 79,000(170) 408,805(85.9)
PapuaNewGuinea
LMIC Blend Yes No 460(220) 13,105(63)
Philippines LMIC IBRD No No 3,000(120) 68,712(29.8)
Sao Tome andPrincipe
LMIC IDA No No 14(210) 340(53.2)
Senegal LMIC IDA Yes No 1,700(320) 29,975(59.6)
SolomonIslands
LMIC IDA Yes Yes 23(130) 529(31.1)
SouthSudan LMIC IDA No Yes 3,000(730) 39,515(104)
Swaziland LMIC IBRD No No 120(310) 2,907(79.7)
Uzbekistan LMIC Blend Yes No 220(36) 25,091(39.6)
Vietnam LMIC Blend Yes No 690(49) 32,765(23)
Yemen LMIC IDA Yes Yes 2,100(270) 43,276(60)
Zambia LMIC IDA Yes No 1,800(280) 50,167(88.5)
Sudan LMIC IDA No Yes 4,600(360) 88,524(73.1)
Angola UMIC IBRD No No 4,400(460) 148,006(163.5)
Azerbaijan UMIC IBRD No No 43(26) 5,943(35.2)
Botswana UMIC IBRD No No 83(170) 2,577(53.3)
Brazil UMIC IBRD No No 2,100(69) 41,839(14.4)
China UMIC IBRD No No 5,900(32) 258,250(14)
Gabon UMIC IBRD No No 130(240) 3,171(62)
Iraq UMIC IBRD No No 710(67) 34,757(34.4)
Mexico UMIC IBRD No No 1,100(49) 37,056(16.2)
Peru UMIC IBRD No No 530(89) 10,831(18.2)
SouthAfrica UMIC IBRD No No 1,500(140) 49,815(44.6)
Turkmenistan UMIC IBRD No No 68(61) 5,538(52.8)
EquatorialGuinea
HIC IBRD No No 79(290) 2,521(100.3)
31
ANNEX 3: METHODOLOGY FOR ESTIMATING HEALTH IMPACTS AND RESOURCE GAPSTheapproachtomodelinghealthimpacts,resourceneedsestimates,thefinancingflowsfromdomesticsourcesandtheresultingfinancinggapforthisConceptNoteisbasedheavilyonusingexistingestimatesandmethodologies.Tworecentmodelingeffortshaveassessedkeyelementsoftheresourceneeds,financingflowsandprojectedhealthoutcomesofscaling-upcoverageforRMNCH(bothofwhichbuiltonearlierefforts,includingthoseoftheGlobalStrategy,theCommissiononMacroeconomicsandHealth,andtheCommoditiesCommission).
TheGlobalInvestmentFrameworkforWomen’sandChildren’sHealth,ledbyWHO,presentedan“investmentcase”in2014thatcomparedthehealthimpactsandincrementalcostsofthreescenariosfortheperioduntil2035:(i)maintainingthepresentcoveragebutscalingupcostsaccordingtoanticipatedpopulationgrowth(lowscenario),(ii)graduallyincreasingcoveragebasedonhistoricaltrends(mediumscenario),and(iii)acceleratingthescale-uptothepaceachievedbytop-performinglowandmiddle-incomecountries(highscenario).Thisworkwasundertakenfor74ofthe75countrieshighlightedintheCountdownto2015initiative;SouthSudanwasomittedfromtheanalysisbecauseoftheabsenceofdata.
TheLancetCommissiononInvestinginHealth(CIH)builtonthisinvestmentcaseandaddedsomenewapproaches(e.g.,factoringintheadoptionofnewtoolsandtechnologiesoverthecourseoftheperiod)andsomenewdiseasesandpopulations(e.g.,HIVandmalariainadults,tuberculosis,neglectedtropicaldiseases)inthecourseofmodelingthehealthimpactsandincrementalcostsoftwoscenarios(currentcoverageand“convergence”,oracceleratedscale-up).TheCIHalsoexaminedthelikelyexpansionofdomesticfinancingforRMNCHinlightofeconomicgrowthandincreasedallocationofgovernmentbudgetstohealth(whichhastypicallybeenthecaseascountriesexperienceeconomicgrowth).
Boththeseeffortswerepeer-reviewedandpublishedtheirresultsandmethodologiesinTheLancet.
Estimating resource needsForthepurposeofthisConceptNote,thestartingpointfortheestimatesoftheresourceneedswastheGlobalInvestmentFramework.Inparticular,needswerecalculatedfortheincrementalcostsofscalingupcoveragetoboththehighandthemediumscenarios.Country-leveldatafromtheGlobalInvestmentFrameworkwasadjustedfrom2011to2013constantUSdollarsusingIMFcountry-levelGDPdeflators.Arealinflationfactorof2percentwasappliedtoprojectedcoststoaccountforexpectedincreasesinthecostofscalingupservicesanddelivery.
Toreflecttheimpactoftherolloutofanticipatedfutureresearchanddevelopment,themethodologyemployedbytheCommissiononInvestinginHealthwasusedtofactorinthecostsofpurchasingandscalingupnewtechnologies.Anincremental
32
reductionof2percentwasappliedtothenumberofstillbirths,whiledeclinesinthematernalmortalityratioandunder-5mortalityrateswereacceleratedby2percent.
Thecostperdeathavertedbetweenthehigh-andlow-coveragescenarioswasthenmultipliedbytheincrementalnumberoflivessavedfromnewtechnologiestoestimatethecostofpurchasingandscalingupnewtechnologies.Costsofnewtechnologyscale-upwerecalculatedattheincomegrouplevel(low-income,lower-middle-income,andupper-middleandhighincome),withtheper-countrycostsallocatedbasedoncountries’relativeshareofresourceneedsintheirincomegroup.Thecostsforbasicinvestmentsinresearchanddevelopmentwerenotincluded.
Estimating domestic financing flowsToestimatedomesticfinancing,theapproachemployedbytheCommissiononInvestinginHealthwasused.Thefirstcomponentofthisiscapturethepotentialincreaseindomesticfinancingthatrelatestoeconomicgrowth.IMFprojectionsofrealGDPgrowthratesforeachcountrywereusedthrough2019,afterwhichthesimpleaverageofprojectedgrowthratesfor2014-2019wasappliedto2020-2024.
Between2025and2027,allprojectedgrowthratesabove5percentweredroppedto5percent,whilefor2028-2030,allgrowthratesabove3percentweredroppedto3percent.Shouldtherecenttrendofrapideconomicgrowthinlow-andmiddle-incomecountriesbegintoslow,thepotentialdomesticfinancingflowscoulddropconsiderably.
TheshareofGDPdirectedtowardgeneralgovernmentexpendituresonhealth(GGHE)wasthenassessedunderthreescenarios:
• Countriesmaintainexisting(2012)proportionsofGGHE,whicharegenerally2-3percentofGDP;
• GGHEsteadilyclimbsto3percentofGDPby2030forlow-andlower-middle-incomecountries,whileremainingstableatthehistoricalaverageof3.24percentforupper-middleandhigh-incomecountries;
• GGHEsteadilyclimbsto4percentofGDPforallincomegroupsby2030.
Countriesallocatelessthan100percentoftotalGGHEtoRMNCAH,soarangeofproportionsforthesharegoingtoRMNCAHwasthenassessed.
Incrementaldomesticfinancingestimateswerethencalculatedrelativetoa2013baselinelevel.ThemaximumfinancingavailableforRMNCAHwascappedatacountry’stotalresourceneedsforthatyear,undertheassumptionsthatcountrieswouldnotrationallyspendmorethantheirtotalneedsforRMNCAH,andthatdomesticfinancingisnon-transferablebetweencountries.SeveraloftheCountdowncountriescouldnotbeincludedbecauseofdataunavailability:Comoros,DemocraticPeople’sRepublicofKorea,Myanmar,Somalia,andZimbabwe.
33
Estimating overall resource gapsToestimatethegapbetweenoveralldomesticfinancingflowsandresourceneeds,thefollowingparameterswereusedforthebasecase:
• Resourceneedscomparedtheincrementalamountsbetweenthelowandhighcoveragescenarios;
• Themiddlescenarioofcountriesallocating3percentofGDPtohealthwasused(basedonthehistoricalexperiencethatGGHEincreasesascountriesexperienceeconomicgrowth);
• TheshareoftotaldomesticfinancingallocatedtoRMNCAHwas25percent,anestimatethatwasdevelopedintheCountdownto2015processandemployedbytheGlobalStrategyforWomen’sandChildren’sHealth.
AnadditionalscenarioinwhichtheshareofdomesticfinancingforRMNCAHincreasesto50percentwasalsoincludedintheConceptNote.
Estimating health impactsAswithestimatingtheresourceneeds,projectionsfromtheGlobalInvestmentFrameworkforWomen’sandChildren’sHealthwereadaptedtocalculatetheprojectedhealthimpactofscaling-uptoahighcoveragescenario.
TheGlobalInvestmentFrameworkestimatedthetotalnumberofdeathspreventedusingtwoapproaches:Livessavedfromthescale-upofhealthinterventions,anddeathsavertedduetothescale-upoffamilyplanning.
Deathsavertedcapturesthefallindeathsattributabletoareductioninunwantedpregnanciesandsubsequentreductioninthenumberofbirths,whilelivessavedcapturesthefallindeathsthatoccursasaresultofhealthtechnologyscale-upandsubsequentdecreasesinmortalityrates.Deathspreventedwerethenestimatedasthesumoflivessavedanddeathsaverted.
Toreflecttheanticipatedhealthgainsofadoptingandscalingupfuturetechnologicalinnovations,livessavedestimatesfromtheGlobalInvestmentFrameworkweremodifiedbasedonasimilarmethodtotheresourceneedsestimates.
Theannualreductionsinunder-5mortalityratesandmaternalmortalityratioswereacceleratedbyafurther2percentperyear.Stillbirthswereincrementallyreducedby2percentperyear.Nootheradjustmentsweremadetotheestimatesofstillbirthspreventedorunder-fiveandmaternallivessaved.
AdjustedlivessavedestimateswerethenaddedtotheGlobalInvestmentFramework’sestimatesofdeathsavertedduetoscalingupoffamilyplanningtocalculatethetotalnumberofdeathspreventedfromscalingupRMNCAHinterventions.
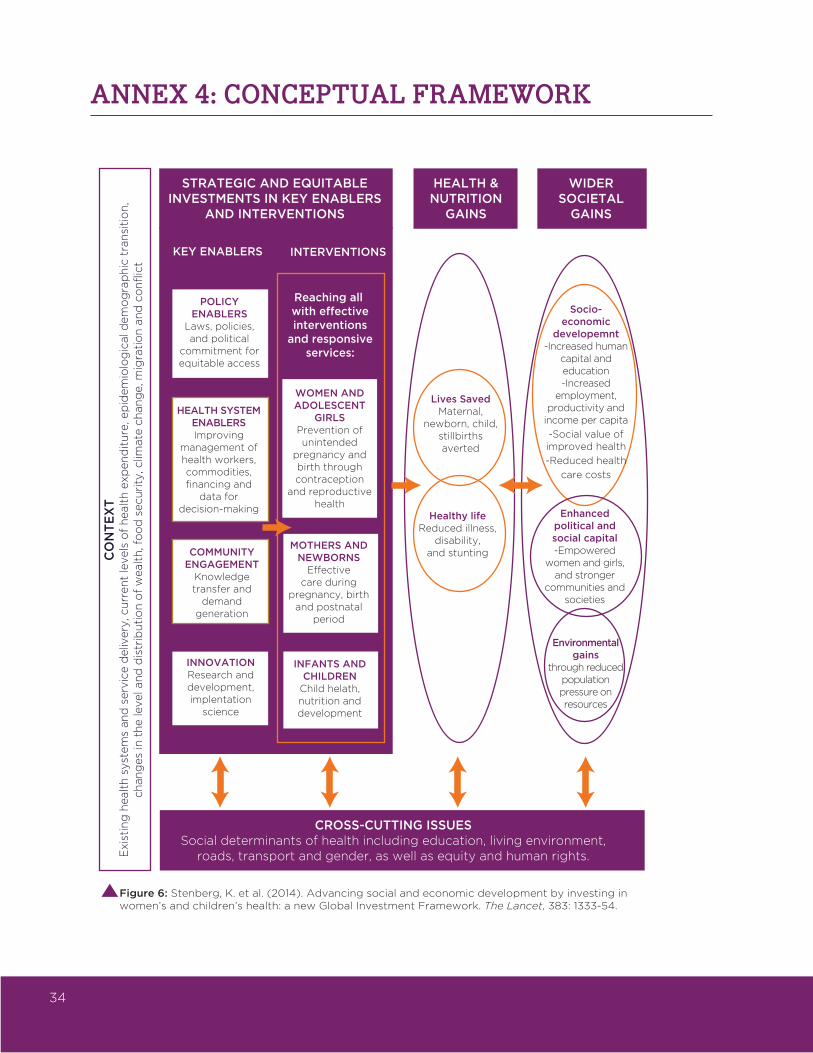
34
ANNEX 4: CONCEPTUAL FRAMEWORK
STRATEGIC AND EQUITABLEINVESTMENTS IN KEY ENABLERS
AND INTERVENTIONS
HEALTH &NUTRITION
GAINS
WIDERSOCIETAL
GAINS
KEY ENABLERS INTERVENTIONS
POLICY ENABLERS
Laws, policies, and political
commitment for equitable access
HEALTH SYSTEM ENABLERSImproving
management of health workers, commodities, financing and
data for decision-making
COMMUNITY ENGAGEMENT
Knowledge transfer and
demand generation
INNOVATIONResearch and development, implentation
science
WOMEN AND ADOLESCENT
GIRLSPrevention of unintended
pregnancy and birth through contraception
and reproductive health
MOTHERS AND NEWBORNS
Effective care during
pregnancy, birth and postnatal
period
INFANTS AND CHILDREN
Child helath, nutrition and development
Reaching all with effectiveinterventions
and responsiveservices:
Lives SavedMaternal,
newborn, child,stillbirths averted
Healthy lifeReduced illness,
disability,and stunting
Socio-economic
developemnt-Increased human
capital and education-Increased
employment, productivity and
income per capita
-Social value of improved health
-Reduced health
care costs
Enhanced political and social capital-Empowered
women and girls, and stronger
communities and societies
Environmentalgains
through reduced population pressure on resources
CROSS-CUTTING ISSUESSocial determinants of health including education, living environment,
roads, transport and gender, as well as equity and human rights.
CO
NT
EX
TE
xist
ing
heal
th s
yst
em
s an
d s
erv
ice d
eliv
ery
, cu
rren
t le
vels
of
heal
th e
xpen
dit
ure
, ep
idem
iolo
gic
al d
em
og
rap
hic
tra
nsi
tio
n,
chan
ges
in t
he le
vel a
nd
dis
trib
uti
on
of
weal
th, f
oo
d s
ecu
rity
, clim
ate c
han
ge, m
igra
tio
n a
nd
co
nfl
ict
Figure 6: Stenberg, K. et al. (2014). Advancing social and economic development by investing inwomen’s and children’s health: a new Global Investment Framework. The Lancet, 383: 1333-54.
35
ANNEX 5: ROLE OF THE PRIVATE SECTORToimproveRMNCAHoutcomes,weneedanintegratedhealthsystemapproachthatlooksforthebestsolutions,regardlessofwhethertheyareprovidedbythepublic,privatesectorsorbothinmeaningfulcollaborationwitheachother.AccordingtoDHSdata,inAfrica,SouthAsiaandEastAsiaPacific,where92percentofthepoorlive,50-80percentofgeneraloutpatientpediatriccarevisitsbythepoorestquintileweretoprivateproviders(seefigure);maternaldeliveriesinprivateclinicsincreasedfrom8percentin1990toapproximately22percentin2008.Therefore,thereisaclearopportunityforgovernmentstoexpandeffectivecoverageofRMNCAHservicestothepoorbyleveragingprivatesectorcapacity.
Healthsystemsneedtobebetterregulated,lessfragmented,andmoreefficienttoofferbasicandessentialhealthcaretomothersandchildrenataffordableprices.ThiscanbedoneforexamplebystrengtheningtheroleofthegovernmentasastrategicpurchaserofRMNCAHservicesfromthebestproviderregardlessofpublic/privateownership.Inordertoachievethis,countriesanddonorsneedsupporttoidentifyanddevelopfinancingmechanismsthataresustainableandappropriatetothelocalcontext.
TheGFFcansupportscalingupeffortsofmainstreamingmixedhealthsystems approachesinRMNCAHatthecountry,regionalandgloballevelsby:
• Analysisandstrategicthinkingtomatchtherightinstrument(performance-basedcontracts,vouchers,insurance,etc.)tothespecificobjective;
• Experimentationwithdifferentapproachestocostingandpricingofservicesthatprovideincentivesforhighqualityservices;
• Reformoflicensingandregistrationregimesthatpushprivateproviderstooperateinformallyorseekworkoutsidethehealthsector;
• Strengtheningofthegovernment’scapacitytosuperviseandimprovepatientsafetyandqualityofcare;
• Privatesectorengagementthroughprivateproviderassociationsandthecreationofpublicprivatedialogueplatforms;
• Adviceonaddressinginefficienciesinsupplychainsofessentialmedicinesandcommodities,improvedpriceregulationsandprocurementpractices;
• Facilitationofregulatoryharmonizationbetweencountriestoreduceunnecessarybarrierstomarketentryforessentialmedicinesandtechnology.
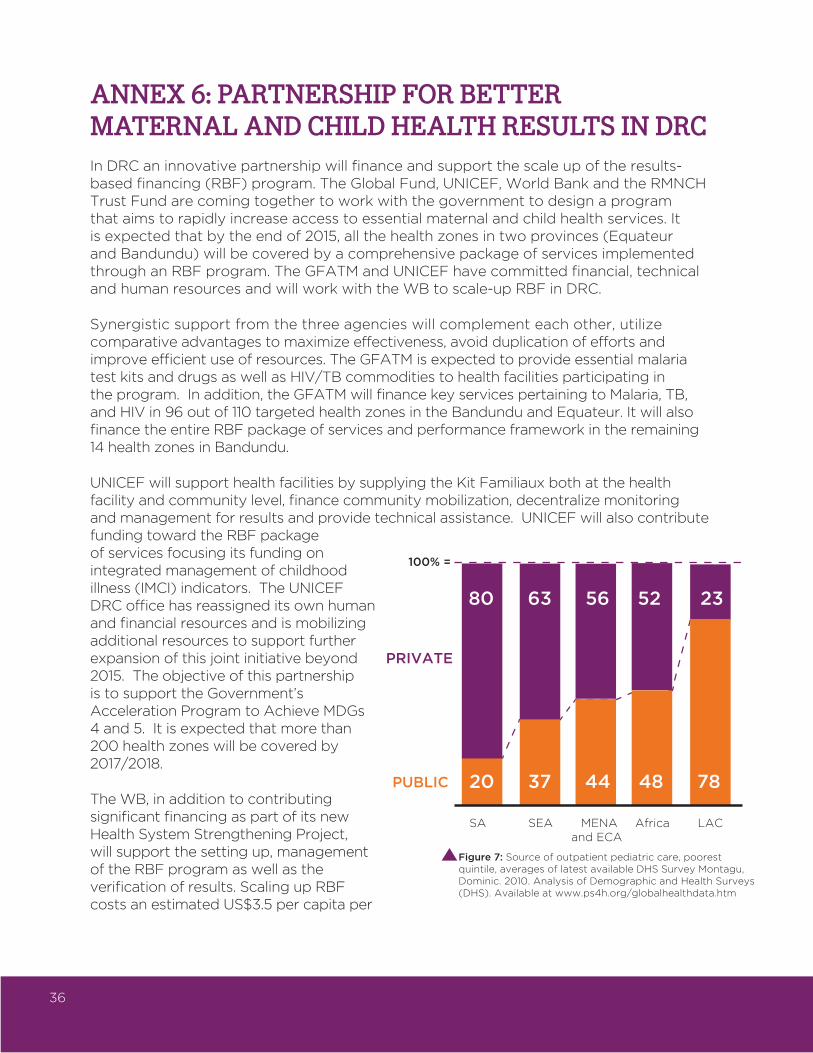
36
ANNEX 6: PARTNERSHIP FOR BETTER MATERNAL AND CHILD HEALTH RESULTS IN DRCInDRCaninnovativepartnershipwillfinanceandsupportthescaleupoftheresults-basedfinancing(RBF)program.TheGlobalFund,UNICEF,WorldBankandtheRMNCHTrustFundarecomingtogethertoworkwiththegovernmenttodesignaprogramthataimstorapidlyincreaseaccesstoessentialmaternalandchildhealthservices.Itisexpectedthatbytheendof2015,allthehealthzonesintwoprovinces(EquateurandBandundu)willbecoveredbyacomprehensivepackageofservicesimplementedthroughanRBFprogram.TheGFATMandUNICEFhavecommittedfinancial,technicalandhumanresourcesandwillworkwiththeWBtoscale-upRBFinDRC.
Synergisticsupportfromthethreeagencieswillcomplementeachother,utilizecomparativeadvantagestomaximizeeffectiveness,avoidduplicationofeffortsandimproveefficientuseofresources.TheGFATMisexpectedtoprovideessentialmalariatestkitsanddrugsaswellasHIV/TBcommoditiestohealthfacilitiesparticipatingintheprogram.Inaddition,theGFATMwillfinancekeyservicespertainingtoMalaria,TB,andHIVin96outof110targetedhealthzonesintheBandunduandEquateur.ItwillalsofinancetheentireRBFpackageofservicesandperformanceframeworkintheremaining14healthzonesinBandundu.
UNICEFwillsupporthealthfacilitiesbysupplyingtheKitFamiliauxbothatthehealthfacilityandcommunitylevel,financecommunitymobilization,decentralizemonitoringandmanagementforresultsandprovidetechnicalassistance.UNICEFwillalsocontributefundingtowardtheRBFpackageofservicesfocusingitsfundingonintegratedmanagementofchildhoodillness(IMCI)indicators.TheUNICEFDRCofficehasreassigneditsownhumanandfinancialresourcesandismobilizingadditionalresourcestosupportfurtherexpansionofthisjointinitiativebeyond2015.TheobjectiveofthispartnershipistosupporttheGovernment’sAccelerationProgramtoAchieveMDGs4and5.Itisexpectedthatmorethan200healthzoneswillbecoveredby2017/2018.
TheWB,inadditiontocontributingsignificantfinancingaspartofitsnewHealthSystemStrengtheningProject,willsupportthesettingup,managementoftheRBFprogramaswellastheverificationofresults.ScalingupRBFcostsanestimatedUS$3.5percapitaper
100% =
Figure 7: Source of outpatient pediatric care, poorest quintile, averages of latest available DHS Survey Montagu, Dominic. 2010. Analysis of Demographic and Health Surveys (DHS). Available at www.ps4h.org/globalhealthdata.htm
SA SEA MENA Africa LAC and ECA
80 63 56 52 23
20 37 44 48 78
PRIVATE
PUBLIC
37
yearwhichincludestheoutputbudgetandtheoverheadcostsofRBF,butexcludesthedrugs,donatedkitsandmanagementcostsofthevariousagencies.
Thiscollaborativeapproachwillcontributetowardtheprovisionofanintegratedpackageofservices,offeredtoalargerportionofthepopulation.Itisexpectedthatsuchalignmentofdevelopmentpartnerswillcontributetonotonlystrengtheningthehealthsystem(efficient,effectiveandbettergoverned)bothfromaservicedeliveryandstewardshipaspectbutwillalsoachievetheintendedresultsintermsofimprovingutilizationandqualityofcareaswellasachievingtheintendedmaternalandchildhealthresults.Finally,thisalignmentisverymuchinlinewiththeMinistryofPublicHealthobjectivestoreducepartners’fragmentationandensureharmonization.DiscussionsforfuturealignmentwithGAVI,USAID,UNFPAandtheGatesFoundationareongoing.
38
ANNEX 7: RMNCAH FINANCIAL ROADMAPSTheGFFaimstosupportcountriesintheirhealthfinancingtransition,especiallyastheymovefromlow-tolower-middle-incomestatus.Thehealthfinancingtransitionischaracterizedbyanincreaseinhealthexpendituresandarisingshareofgovernmentspendingduetoacombinationofeconomicandpoliticaltrends.However,thistransitionisoftennotasteadybutratherabumpyprocesswithparticularchallengesforeconomieswhentheyadvancefromlow-incometomiddle-incomestatus.Attheonsetofthistransition,countriestendtorelyheavilyondevelopmentassistance.Thisassistancedecreasesdomesticfinancingandcommonlyflowsthroughmechanismsdevelopedoutsideweakpublicfinancialmanagementsystems.Ascountriesattainlower-middle-incomecountrystatus,thelinkbetweeneconomicgrowthandincreasesingovernmenthealthexpenditureoftenweakens.Governmentsthenfailtocompensateforshortfallsindevelopmentassistance,withpeoplefacingincreasingpressurestomeettheirhealthcareneedsbypayingout-of-pocketandmakingthemvulnerabletocatastrophicexpendituresandimpoverishment.Duringthetransitionfromlowtomiddle-incomecountrystatus,countriesincreasinglyfacethechallengeofdistributingthegrowinglevelsofgovernmentexpenditureequitably,withoftenrapidlygrowingdifferencesinhealthspendingacrosspopulationgroups.
TheGFFwillsupportcountriesindevelopingfinancialroadmapsthatwillhelpthemmakethehealthfinancingtransitionmoreequitableandsustainableandleadthemtowarduniversalaccesstoqualityRMNCAHservicesby2030.TheRMNCAHfinancialroadmapsareintegratedfinancingstrategiesthathelpcountriesmeettheirRMNCAHgoals.Theyprovideestimatesofmediumandlong-termRMNCAHresourceneedsinlinewithnationalRMNCAHobjectives.Theytranslatetheseestimatesandobjectivesintomedium-termbudgetaryandperformanceframeworks,takingintoaccountothernationalhealthpriorities,fiscalpolicyframeworksandeconomictrends.TheRMNCAHfinancialroadmapsalsosetforthfully-funded,medium-termactionframeworkstostrengthenlocalRMNCAHandhealthfinancingsystems.
Medium-termbudgetaryandperformanceframeworkssetforththefinancialcommitmentsofagovernmentanditsdevelopmentpartnersforRMNCAHoveraperiodof3to5years.TheyharmonizethevariousstreamsoffinancingaroundnationalRMNCAHplans,therebyreducingtheadministrativeburdenforcountriesandmaximizingtheimpactofallpartners’RMNCAHsupport.Moreover,theycombinefinancinginstrumentsacrosssourcestofacilitatethetransitiontowarddomesticfinancingandencourageprogresstowardRMNCAHgoals.
Forexample,grantsmaybecombinedwithcreditsandloanstofinancebuy-downsofinterestandprincipletoencouragenotonlyborrowingforRMNCAH,butalsocountrycommitmentstospecificbudgetallocationtargetsforRMNCAHunderreduceddebtserviceobligations.Grants,creditsandloansmayalsobedisbursedagainsttheimplementationofpoliciesandinstitutionalactionsthatscale-upandsustaindomesticRMNCAHfinancing(e.g.throughDevelopmentPolicyCredits/Loans)aswellasagainstRMNCAHresults(e.g.throughPayforResultsapproaches).TheframeworksguidetheannualhealthsectorbudgetingprocessesforRMNCAH.
3939
Medium-termRMNCAHandhealthfinancingactionframeworksestablishactivities-includingtheresponsibilitiesforfinancingandimplementation–thatarecriticaltosupportacountry’stransitiontogreaterself-sufficiencyinfinancingbothRMNCAHandhealthmoregenerally.Theactionframeworksensuretheprogrammaticcoherenceandimpactoftechnicalassistance.Theyaimtostrengthenpublicfinancialmanagement,includingtheintroductionofmoreadvancedproviderpaymentsystems,toallowforgreateruseofcountrysystemsandenhancethereturnstoinvestmentsinRMNCAH.TheyalsoaimtoenhancedomesticresourcemobilizationandallocationtomakeRMNCAHgainsmoresustainableandequitable.FrameworkssupporturgentlyneededinnovationstostrengthentheoftenweaklinkbetweeneconomicgrowthandspendingonRMNCAH,forexample,bycapturingrevenuesfromextractiveindustriesandearmarkingsharesofthemforinvestmentsinRMNCAHincountrieswithrapid,naturalresourcedrivengrowth.
ThedevelopmentoffinancialroadmapsbuildsonIHP+,P4Handotherwell-establishedcoordinationmechanismsatthecountrylevel.TheprocessprovidestheplatformtoengagewithministriesoffinancetoplanforincreasedlevelsofspendingonRMNCAH.Itstartswithanin-depthassessmentoftheRMNCAHandnationalhealthfinancingsystem,thepublicfinancingarchitecture,andthefiscalandmacrocontext.Thein-depthassessmentoftheRMNCAHandnationalhealthfinancingsystemcombinesvariousinstruments,suchaspublicexpenditurereviews,fiscalspaceanalysis,andcapacityandinstitutionalassessments.Theroadmapsarereviewedannuallyand,asneeded,adjusted.Lessonsarecapturedandsharedacrosscountries.Reviewsmaytriggerupdatesofthein-depthassessmentoftheRMNCAHandnationalhealthfinancingsystems.

40
ANNEX 8: LEVERAGING IDA THROUGH THE HEALTH RESULTS INNOVATION TRUST FUNDSince2007,theHealthResultsInnovationTrustFund(HRITF)hassupportedresults-basedfinancing(RBF)approachestohelpresource-constrainedcountriesaccelerateprogresstowardthehealth-relatedMillenniumDevelopmentGoals(MDGs),focusingparticularlyonMDGs1c(nutrition),4(childmortality),and5(maternalhealth).
HRITFissupportedbythegovernmentsofNorwayandtheUnitedKingdom,withatotalcommitmentofUS$537million,andmanagedbytheWorldBankasamulti-donortrustfund.CountryimplementationgrantsfromthetrustfundarelinkedtoprojectfinancingfromIDA.30
ThecombinedIDAandHRITFfinancingjointlyfinancesthein-countryprogram,significantlyincreasingtheoverallresourceenvelopeforRMNCAH.EachdollarfromthetrustfundgeneratesonaveragefivedollarsfromIDA.Theoverallportfoliocurrentlyconsistsof32countryprogramswithUS$420millioningrantfundingleveragingUS$2.4billioninIDAfunding.BylinkingthegrantfundingtoWorldBankoperations,thetrustfundhasaverylowoverheadoflessthan2percent.
CountryprogramsfinancetheimplementationofcomprehensivematernalandchildhealthserviceswithanaimtoimprovethevolumeandqualityofRMNCAHservices.Manyprogramssupportadditionalcommunityanddemand-sideinterventionstoincreasetheutilizationofessentialservices.AcrosstheportfoliotherearemanydifferentwaysinwhichRBFprogramsimproveequity.Anindependentlyverifiableinformationsystemforreal-timetrackingofservicedeliveryperformanceprovidesaccountabilityandensurescarefulmonitoringofimplementationprogress.
Asaresult,theprojectsfundedachieveanaveragefive-foldreturnoninvestment,witha4percentadditionalinvestmentinRMNCAHservicesyieldinga20percentgaininperformance.Theimpactevaluationsaccompanyingtheprogramsaremeasuringtheimpactonservicecoverage,qualityandhealthoutcomes.InArgentina,theprogramresultedina74percentdecreaseinneonatalmortality31inNigeria,themoderncontraceptiveprevalenceratedoubledincomparisontonon-RBFareas,from10to21.5percent;andinZimbabweinstitutionaldeliveriesincreasedfrom33percentto67percentininterventiondistricts.
ThereareanincreasingnumberofcountrieswheredevelopmentpartnersjointlysupportthefinancingandimplementationofRBFprogramsatthecountrylevel.Forexample,inDRC,GAVI,theGlobalFund,UNICEFandUSAIDareworkingtogethertoscaleupservices
30IDA-InternationalDevelopmentAssociation,theWorldBank’sfundforthepoorestcountries.
31Gertler,P.,Giovagnoli,P.,&Martinez,S.(2014).Rewardingproviderperformancetoenableahealthystarttolive:EvidencefromArgentina’sPlanNacer.TheWorldBank,PolicyResearchWorkingPaper6884.
40

41
andharmonizingfinancingaroundacomprehensivepackageofservices.InBenin,theGlobalFund,GAVIandtheWorldBankarecoveringthecostofacomprehensivepackageofmaternalandchildhealthservicesindifferentgeographicalareas,contractingthesameimplementingagency.32
32Vergeer,P.,&McCuneS.(2013).HowGovernmentsandDevelopmentPartnersWorkTogethertoScaleUpSuccessfulResults-BasedFinancingPrograms.Availablefrom:http://www.rbfhealth.org/resource/how-govern-ments-and-development-partners-work-together-scale-successful-results-based#sthash.f2zmYs53.dpuf.
41

42