Embed Size (px)
Citation preview
Turkish Neurosurgery 10: 36 - 42, 2000 Sayrak:Prolifemtive celliiuc/ear aiitigen aiid AgNOR method for preopemtive histological gradiiig of glitil h/mors
Cell Nuclear AntigenThe AgNOR Method For
Grading Of Glial Tumors
Value Of ProliferativeImmunohistochemistry AndPreoperative Histological
Glial Tümöderin Preoperatif Histolojik Derecelendirmesinde ProliferatifHücre Nükleer Antijeni Immünositokimyasi ve AgNOR Yönteminin Yeri
HAKAN SAYRAK, ÇiÇEK BA YINDIR
Istanbul Memorial Hospital, Pathology Department (HB), Istanbul University Faculty of Medicine,
Neuropathology Division of Department of Neurosurgery (ÇB), Istanbul
Received: 15.1.1998 Ç:> Accepted: 1.6.1999
Abstrart Extended short fomis again here - same in the key wordsso please modify according to your journa\'s style the aim of thisstudy was to determine whether or not assessing cell kinetics byargyrophilic nucleolar organizer region counting, and usingimmunohistochemistry to deted proliferative cell nuclear antigenare valuable methods for predieting the biological behavior of glialtumors. Specimens were obtained from 17patients with glial tumorsusing stereotactic procedures, and smears of the tissue were made.For each smear, we investigated for antibodies to proliferatiye cellnuclear antigen (PCLO,DAKO) using the streptavidine peroxidasemethod, and also counted the number of argyrophilic nucleolarorganizer region s using a specific staining technique to identifythese. Of the 17 tumors, 3 were grade i pilocytic astrocytomas, 3were grade II fibrillary astrocytomas, 1 was a grade IIoligodendroglioma,4 were grade III anaplastic astroeytomas, and6 were grade IV glioblastomas. We analyzed each case based onindependent assessment of the proliferatiye cell nuclear antigenlabeling index, argyrophilic nucleolar orga.nizer region count,histological type, and histological grade, and then compared theresults statistically. Although the proliferatiye cell nuclear antigenlabeling index and argyrophilic nucleolar organizer region countboth increased in parallel with histological grade, we found thatthe only statistical difference between low-grade (grades iand i!)and high-grade glial tumors (grades III and IV) was the groups'argyrophilic nucleolar organizer region counts. The findingsindicated that the proliferatiye cell nuclear antigen labeling indexis not a good prognostic indicator in the preoperative histologicalevaluation of glial tumors, and that argyrophilic nucleolar organizerregion counting can be used to differentiate benign tumors (gradesI-I!) from malignant ones (grades III-IV).Key Words: AgNOR method, glial tumors, proliferatiye cellnuclearantigen, immunohistochemistry, stereotactic biopsy
Özet: Bu çalismanin amaci, hücre kinetigini degerlendirmeyöntemlerinden biri olan AgNOR sayiminin ve proliferatifhücre nükleer antijeni (PCNA) immünositokimyasinin,glial tümörlerin biyolojik davranislarini öngörmede yeriolup olmadigini saptamaktir. Stereotaktik islem yoluylaglial tümörlü 17 hastadan materyelleri elde ettik vedokulardan yaymalar hazirladik. Her bir yaymayi,streptavidin-peroksidaz yöntemiyle antiproliferatif hücrenükleer antijeni (PClO, DAKO) ve AgNOR saymayöntemini uygulayarak, inceledik 17 tümörün, üçü derecei pilositik astrositoma, üçü derece II fibriler astrositoma,biri derece II oligodendroglioma, dördü derece IIIanaplastik astrositoma ve altisi derece Iv glioblastoma idi.Her bir vaka için, PCNA baglanma indeksi, AgNORsayimi, histolojik tip ve histolojik dereceyi ayri ayri analizettik ve sonuçlari istatistikselolarak kiyasladik. PCNAbaglanma oranlari ve AgNOR sayimlari histolojikdereceye paralel artis gösterse de, istatistikselolarakfarkliligi sadece, AgNOR sayimi açisindan, düsük dereceli(derece i ve II) ve yüksek dereceli (derece III ve Iv) glialtümör gruplari arasinda tespit ettik. Sonuç olarak, glialtümörlerin histolojik derecelendirmesinde PCNA oranininbir ölçüt olarak alinamayacagina, AgNOR metodunun iseselim tümörleri (derece I-II) malign (derece III-Iv)olanlardan ayirmakta kullanilabilecegi ne karar verdik.
Anahtar Kelimeler: AgNOR, glial tümörler, prliferatifhücre nükleer antijeni, immünositokimya, stereotaktik
biyopsi
36

Tiirkish Neiirosiirgery 10: 36 - 42, 2000 Saymk: Prolifemtive celliiiiclear aIitigeil and AgNOR metliod for preopemtive Iiistologicalgmdiiig of gliii/ tumors
INTRODUCTION
Many features are used to predict clinicalprognosis in patients with glial tumors, includinghistological type of tumor, histological grade,anatomic sites involved, tumor size, encroachmenton the ventricular system, extension across themidline and invasion of the contralateral cerebralhemisphere, extension to the contralateral side of thetentorium cerebelli, patient age, Karnovsky score andothers. Two main features used to predict thebiological behavior of glial tumors are histologicaltype and grade (16), but the behavior of a tumor doesnot always match its histological grade, alabel thatis based solely on morphology (9). Possibleexplanations for this include the remarkablehistological heterogeneity of glial tumors, the fact thatthe assigned histological grade (especially that ofsmall biopsy samples) may not represent the wholetumor, and the progression of tumor malignancy thatoccurs over time (32,31). In efforts to improve ourability to prognosticate and to overcome thelimitations of traditional histopathologicalevaIuation, research has focused on adaptingknowledge and advances in cell kinetics andmolecular genetics for use in diagnosticneuropathology (8).
Although an objective, cost-effective, easilyapplicable and reliable method has yet to bedeveloped, it has been suggested that of tumorproliferation rates can be used to determinehistological grade and prediet biological behavior(24,27,38).Options for measuring such rates includebromodeoxyuridine (BrdU), Ki-67 and proliferativecell nuclear antigen (PCNA) labelingo The use ofBrdU requires intraoperative injection of thishalogenated pyrimidine, whereas monoclonalantibodies Ki-67 and PCNA can be applied to frozensections and to paraffin-embedded tissue.
PCNA is a 36 kD nuclear protein that is anauxiliary protein of DNA polymerase delta, and takespart in DNA synthesis and repair (43). it is detectablein interphase, begins to rise in the middle of Gl phase,is threefold higher at the G1/S transition than ininterphase, and remains elevated during G2 phaseand mitosis (43,49). it follows that the proportion ofcells marked by anti-PCNA reflects the proliferationrate of a tumor (29).
Another means of assessing proliferatiyeactivity in tumors is the argyrophilic nucleolarorganizer region (AgNOR) method, which is a fairly
simple technique based on the detection of colloidalsilver. The process involves staining an acidiephosphoprotein of nonhistonic stmeture that existsin the nucleus together with DNA coils that carryRNA genes. The number and shapes of AgNORs canbe assessed under light microscopy, and the quantityof these figures rises in parallel with increasedproliferatiye and metabolic activity (13).
MATERIAL and METHOD
Material for histopathological evaluation wasobtained through image-guided stereotactic biopsy(Leksell stereotaetic system, Elekta AB, Stockholm,Sweden) of 17patients with glial tumorso Five to eightbiopsi es of each tumor were obtained, and smearsfrom these were prepared and stained withhematoxylin and eosin. Histopathological evaIuationwas done according to the World HealthOrganization's 1993 classification of tumors of thecentral nervous system. The series use d in the studyincluded three pilocytic astrocytomas (grade 1),threefibrillary astrocytomas and one oligodendroglioma(grade 11),four anaplastic astrocytomas (grade III)and six glioblastomas (grade IV).
For PCNA assessment, anti-PCNA (PCLO,DAKO) was applied to smears fixed in concentratedethyl alcohol using streptavidine peroxidase.Diaminobenzidine tetrahydrochloride was used asa chromogen, and Mayer's hematoxylin was used forcounterstaining.
For AgNOR staining, the first phase involvedsubmersing the slides in a solution of one part ethylakohol and two parts concentrated acetic acid for 3minutes. This was followed by a wash in deionizedwater. Next, the specimens were bathed in workingsolution and shielded from light for 20 minutes, afterwhich they were again washed with deionized water.The working solution was made up of two partssolution A and one part solution B, with solution Acontaining 50 g silver nitrate in 100 ml distilled waterand solution B containing 2 g of gelatin and 1 ml offormic acid in 100 ml distilled water. In the final
phase, the slides were placed in 5% sodiumthiosulphate, washed in distilled water for 1minute,dehydrated in absolute ethyl akoho!, cleared inxylene, and mounted with mounting medium(Canada balsam).
The nuclei that stained in the anti-PCNA and
AgNOR methods were counted under the lightmicroscope using 10x40 and 10x100 fields of
37
Tiirkis/i Neiirosiirgery 10: 36 - 42, 2000 Saynik:Prolifemtive cell nuctear antigen and AgNOR met1wdfor preoperative histological gmdiiig of glial h/mors
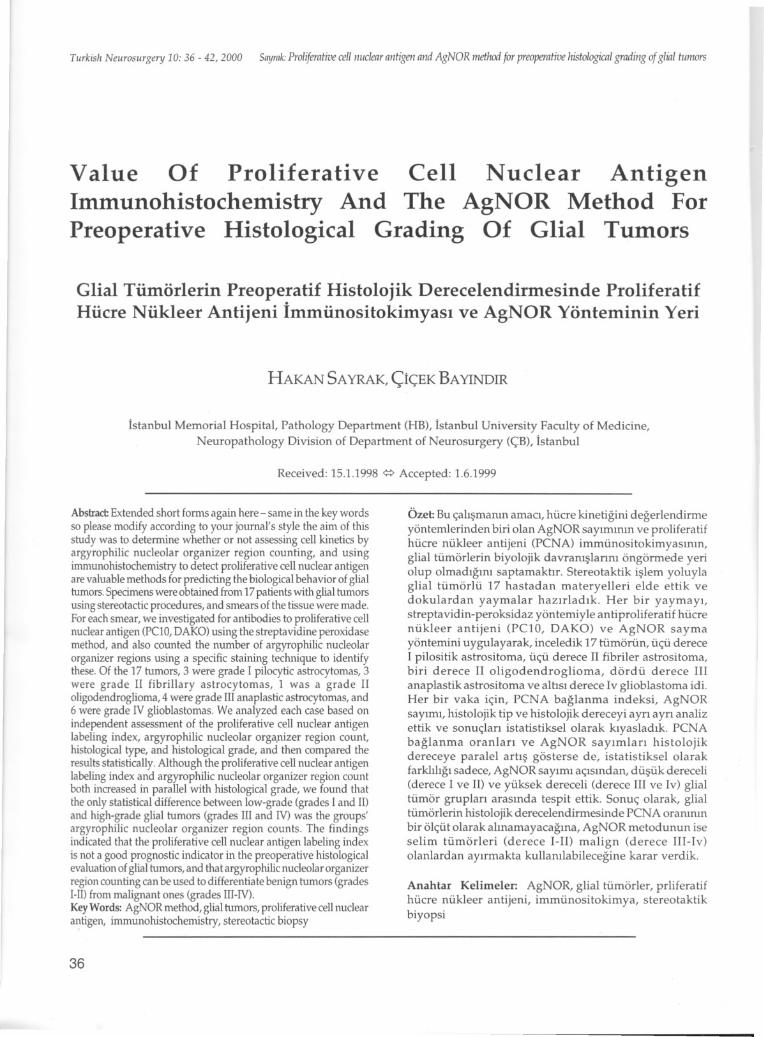
magnification, with 20 different sedions of the slidebeing counted for each case (approximately 2,000cells). The staining in all cells marked with antiPCNA was limited to the nudeus, was diffuse or
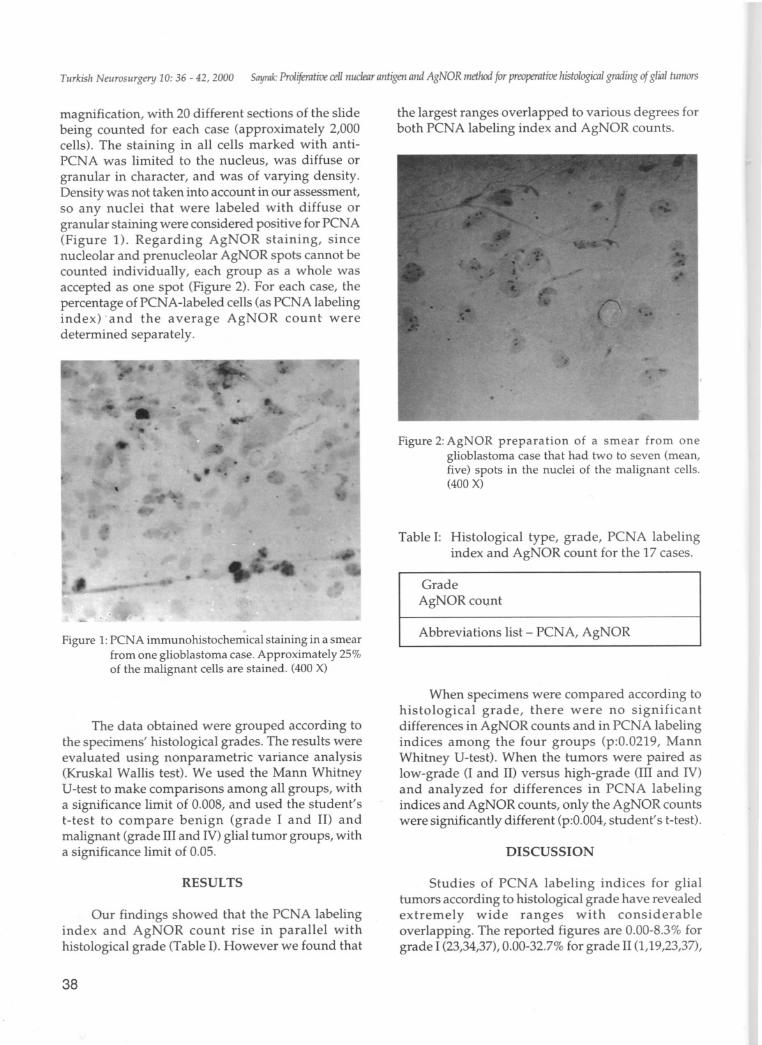
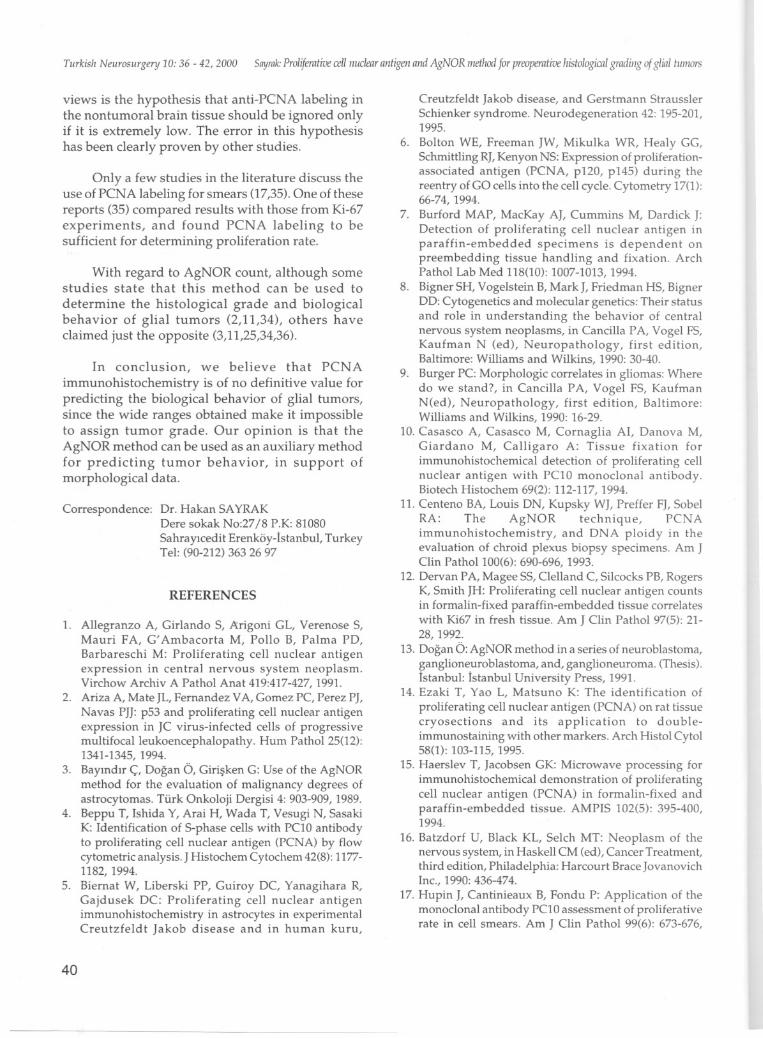
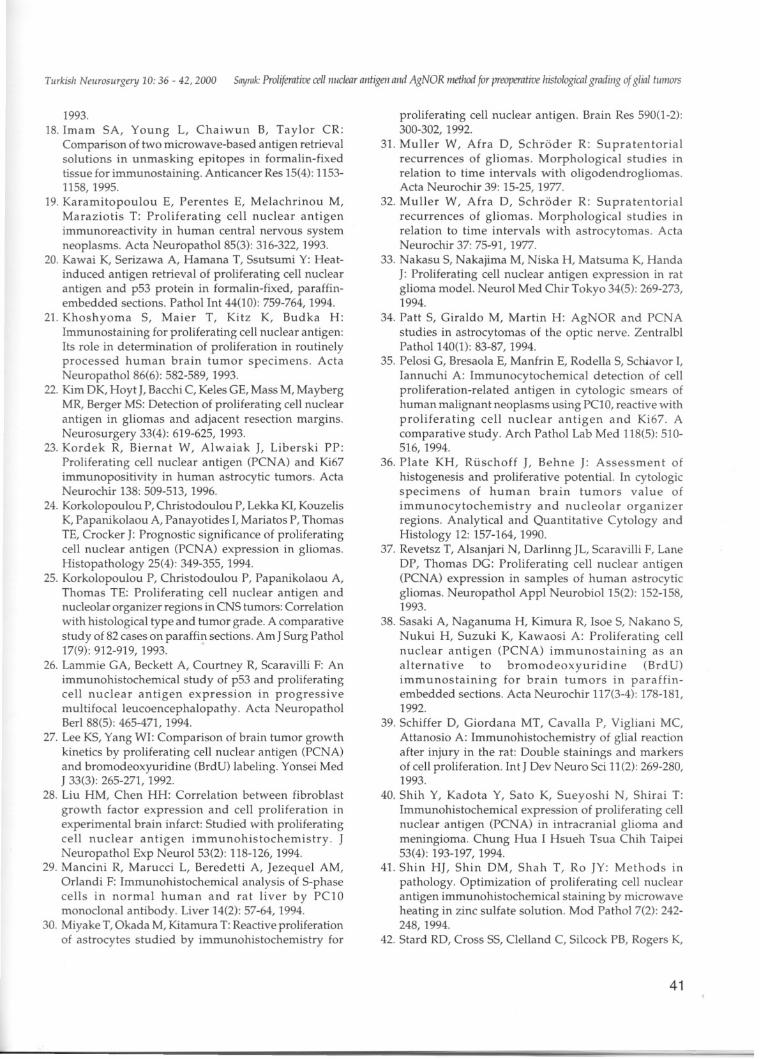
granular in charader, and was of varying density.Density was not taken into account in our assessment,so any nudei that were labeled with diffuse orgranular staining were considered positive for PCNA(Figure 1). Regarding AgNOR staining, sincenudeolar and prenudeolar AgNOR spots cannot becounted individually, each group as a whole wasaccepted as one spot (Figure 2). For each case, thepercentage of PCNA-Iabeled cells (as PCNA labelingindex) .and the average AgNOR count weredetermined separately.
Figure 1:peNA immunohistochemical staining in a smearfrom one glioblastoma case. Approximately 25%of the malignant cells are stained. (400 X)
The data obtained were grouped according tothe specimens' histological grades. The results wereevaluated using nonparametric variance analysis(Kruskal Wallis test). We used the Mann WhitneyU-test to make comparisons among all groups, witha significance limit of 0.008, and used the student'st-test to compare benign (grade i and II) andmalignant (grade III and IV) glial tumor groups, witha significance limit of 0.05.
RESULTS
Our findings showed that the PCNA labelingindex and AgNOR count rise in parallel withhistological grade (Table 1).However we found that
38
the largest ranges over lapp ed to various degrees forboth PCNA labeling index and AgNOR counts.
Figure 2: AgNOR prepara tion of a smear from oneglioblastoma case that had two to seven (rnean,five) spots in the nuclei of the malignant cells.(400 X)
Table I: Histological type, grade, PCNA labelingindex and AgNOR count for the 17 cases.
Grade
AgNORcount
Abbreviations list - PCNA, AgNOR
When specimens were compared according tohistological grade, there were no significantdifferences in AgNOR counts and in PCNA labelingindices among the four groups (p:0.0219, MannWhitney U-test). When the tumors were paired aslow-grade (i and II) versus high-grade (III and IV)and analyzed for differences in PC NA labelingindices and AgNOR counts, only the AgNOR countswere significantly different (p:0.004, student' st-test).
DISCUSSION
Studies of PCNA labeling indices for glialtumors according to histological grade have revealedextremely wide ranges with considerableoverlapping. The reported figures are 0.00-8.3% forgrade 1(23,34,37),0.00-32.7% for grade II (1,19,23,37),
Turkish Neurosurgery 10: 36 - 42, 2000 Sayrak:Proliferative cellii!lclear aiitigeii aiid AgNOR method for preoperative hist%gica/ gradillg of g/ia/ h/mors
0.04-86.3% for grade III 0,19,23,34,37,40) and 2.786.3%for grade LV(1,19,23,37,40).Similarly, the meanindices calculated for each histological grade bydifferent laboratories have varied widely. Theinconsistency of these PCNA results has made itimpossible to establish limits that separate cases intogwups that reflect histological grades or biologicalbehavior.
Another point of interest is that someresearchers have suggested that PCNA labelingindices for astrocytoma and glioblastoma far exceed50% (23,37,40). Although kinetic studies onglioblastomas have found the proliferation rate foralmost all these tumors to be below 50% (16), there isstill question as to what the reported high PCNAlabeling indices truly reflect.
There are also other questions surrounding theaccuracy of this index. Experimental investigationsinvolving rats with PCNA in their CHOK1 cell serieshave shown that up to 10% of the cells leaving thecell cycle and entering GO are positive for PCNA (6).This indicates that approximately 10% of the cellsthat stain for anti-PCNA at interphase, which, to date,have contributed to the proliferation rate figure,should actually be considered normaL.
A study that compared BrdU and PCNAfindings showed that the PCNA labeling index was2.2 times greater than the BrdU labeling index ± 0.8(27). Such high values for PCNA in this and manyother studies may reflect the differences between themethods which used, and may not represent the truecell proliferation rate. The authors of this particularstudy stated that the PCNA labeling index does notreflect histological grade and is not a reliable value.They focused on problems inherent in the techniqueinvestigators have used to derive this figure(19,21,46).
In order to eliminate problems associated withthis method, various groups have examined differenttypes of fixative, different fixation times, and theeffects that microwave rays have on tissue fixed withdifferent fixatives. Investigators have found thattissues fixed with 10% buffered formalin yieldsproliferation rate results closest to those obtainedwith Ki-67 (12,48). Some authors have suggested thatthe length of the fixation period does not affect results(42), while others have bracketed the mostappropriate fixation time between 6 and 30 hours(44). Casasco et aL.suggested that the structure ofPCNA in tissues fixed in formalin deteriorates at an
increasing rate after 3 hours, and stated that alcoholbased fixatives should be used (10). it has also beenproposed that a mixture of 4% paraformaldehydeand 5% glutaraldehyde is suitable fixative for PCNAimmunohistochemistry, that digestion beaccomplished using 0.001 % pepsin (14), thatmethanol beused for fixation (7,29), and that fixationbe accomplished with periodonateparaformaldehyde (33).
With regard to fixing specimens, the best resultshave been obtained using 15 minutes of acetonefixation followed by 15 minutes of methanol fixation(4). After optimal fixation has been achieved andbefore the immunohistochemical procedure, someauthors have proposed that tissue sections shouldbe irradiated in microwave oven (at 600 W tomaximum power). The various suggested ways ofaccomplishing this include irradiating in distilledwater for 2x5 minutes (15), in 0.05 M glycine-HClbu ffer (pH 3.6) containing 0.01 % EDTA for 2x5minutes (18), in 1% zinc sulphate for 7.5 minutes (41),and in citrate buffer solution (pH 6) for 10 minutes(20,45).
Clearly, the variety of methods listed for allthese steps shows there is still no standardizedtechnique for anti-PCNA labelingo StilI, despite theproblems associated with determining PCNAproperties, the literature discusses the merits andpossible applications of the technique.Korkolopoulou and colleagues suggested that thePCNA labeling index could be used separate fromhistological grade (24). Also, Vigliani et aL.proposedthat labeling indices of greater than 5% allow theidentification of subgroups of benign tumors that willbegin to exhibit anaplastic behavior but which, todate, have not been recognized in advance (47). Kimand associates daimed that recurrence can be
predicted for glioma groups of each grade by lookingat the PCNA labeling indices of tumor cells at theresection border (22). Miyake et aL.found that up to5% of the cells in the reparative tissue followed braininjury, were labeled with PCNA (30). Although thisrate was calculated on the third day of woundhealing, it is still significant because it indicates highlevels of PCNA positivity in areas of gliosis. Otherresearchers have reported similar findings (28,39).
Some studies have revealed that PC NA
immunopositivity rate of up to 4.5% in slow virusinfections of the central nervous system might occur(2,5,26). Thus, there is suspicion about the 5% PCNApositivity limit. The foundation of these authors'
39
Tiirkish Neiirosiirgenj 10: 36 - 42, 2000 Snyrnk:Prolifemtive cel/Ilucleiir antigen and AgNOR method for preaperative hist%gim/ gmdiiig of g/in/ tiiirlOrs
views is the hypothesis that anti-PCNA labeling inthe nanturnoral brain tissue should be ignored onlyif it is extremely low. The error in this hypothesishas been dearly proven by other studies.
Only a few studies in the literature discuss theuse of PCNA labeling for smears (17,35). One of thesereports (35) compared results with those from Ki-67experiments, and found PC NA labeling to besufficient for determining proliferation rate.
With regard to AgNOR count, although somestudies state that this method can be used to
determine the histological grade and biologicalbehavior of glial tumors (2,11,34), others havedaimed just the opposite (3,11,25,34,36).
In conclusion, we believe that PCNA
immunohistochemistry is of no definitive value forpredicting the biological behavior of glial tumors,since the wide ranges obtained make it impossibleto assign tumor grade. Our opinion is that theAgNOR method can be used as an auxiliary methodfor predieting tumor behavior, in support ofmorphological data.
Correspondence: Dr. Hakan SAYRAKDere sokak No:27/8 P.K: 81080Sahrayicedit Erenköy-Istanbul, TurkeyTel: (90-212) 363 26 97
REFERENCES
1. Allegranzo A, Girlando S, Arigoni GL, Verenose S,Mauri FA, G' Ambacorta M, Pollo B, Palma PD,Barbareschi M: Proliferating cell nudear antigenexpression in central nervous system neoplasm.Virchow Archiv A Pathol Anat 419:417-427, 1991.
2. Ariza A, Mate JL, Fernandez VA, Gomez PC, Perez PJ,Navas PJJ: p53 and proliferating cell nudear antigenexpression in JC virus-infected cells of progressivemultifocal leukoencephalopathy. Hum Pathol 25(12):1341-1345,1994.
3. Bayindir ç, Dogan Ö, Girisken G: Use of the AgNORmethod for the evaluation of malignancy degrees ofastrocytomas. Türk Onkoloji Dergisi 4: 903-909, 1989.
4. Beppu T, Ishida Y, Arai H, Wada T, Vesugi N, SasakiK: Identification of S-phase ceiis with PCLOantibodyto proliferating cell nuclear antigen (PCNA) by flowcytometric analysis. J Histochem Cytochem 42(8):11771182, 1994.
5. Biernat W, Liberski PP, Guiroy DC, Yanagihara R,Gajdusek OC: Proliferating ceii nudear antigenimmunohistochemistry in astrocytes in experimentalCreutzfeldt Jakob disease and in human kuru,
40
Creutzfeldt Jakob disease, and Gerstmann StrausslerSchienker syndrome. Neurodegeneration 42: 195-201,1995.
6. Bolton WE, Freeman JW, Mikulka WR, Healy GG,Schmittling RJ,Kenyon NS: Expression of proliferationassociated antigen (PCNA, p120, p145) during thereentry of GO cells into the cell cyde. Cytometry 17(1):66-74, 1994.
7. Burford MAP, MacKay AJ, Cummins M, Dardick J:Detection of proliferating cell nudear antigen inparaffin-embedded specimens is dependent onpreembedding tissue handling and fixation. ArchPathol Lab Med 118(10): 1007-1013, 1994.
8. Bigner SH, Vogelstein B, MarkJ, Friedman HS, BignerDD: Cytogenetics and molecular genetics: Their statusand role in understanding the behavior of centralnervous system neoplasms, in Caneilla PA, Vogel FS,Kaufman N (ed), Neuropathology, first edition,Baltimore: Williams and Wilkins, 1990: 30-40.
9. Burger PC: Morphologic correlates in gliomas: Wheredo we stand?, in Caneilla PA, Vogel FS, KaufmanN(ed), Neuropathology, first edition, Baltimore:Williams and Wilkins, 1990: 16-29.
10. Casasco A, Casasco M, Cornaglia AI, Danova M,Giardano M, Calligaro A: Tissue fixation forimmunohistochemical detection of proliferating ceiinudear antigen with PCI0 monodonal antibody.Biotech Histochem 69(2): 112-117, 1994.
11. Centeno BA, Louis ON, Kupsky WJ, Preffer FJ, SobelRA: The AgNOR technique, PC NAimmunohistochemistry, and DNA ploidy in theevaIuation of chroid plexus biopsy speeimens. Am JClin Path ol 100(6): 690-696, 1993.
12. Dervan PA, Magee SS, Cleiiand C, Silcocks PB, RogersK, Smith JH: Proliferating cell nudear antigen countsin formalin-fixed paraffin-embedded tissue correlateswith Ki67 in fresh tissue. Am J Clin Pathol 97(5): 2128, 1992.
13. Dogan Ö: AgNOR method in a series of neuroblastoma,panglione.uroblastoma, and, ganglioneuroma. (Thesis).Istanbul: Istanbul University Press, 1991.
14. Ezaki T, Yao L, Matsuno K: The identification ofproliferating cell nudear antigen (PCNA) on rat tissuecryosections and its application to doubleimmunostaining with other markers. Arch Histol Cytol58(1): 103-115, 1995.
15. Haerslev T, Jacobsen GK: Microwave processing forimmunohistochemical demonstration of proliferatingceii nudear antigen (PCNA) in formalin-fixed andparaffin-embedded tissue. AMPIS 102(5): 395-400,1994.
16. Batzdorf U, Black KL, Selch MT: Neoplasm of thenervous system, in Haskell CM (ed), Cancer Treatment,third edition, Philadelphia: Harcourt Brace JovanovichInc., 1990: 436-474.
17. Hupin J, Cantinieaux B, Fondu P: Application of themonodonal antibody PCI0 assessment of proliferativerate in cell smears. Am J Clin Pathol 99(6): 673-676,
Turkish Neurosurgery 10: 36 - 42, 2000 Saymk: Prolifemtive eell Hueletiraiitigen aiid AgNOR method for preoperative Jiistologicalgradiiig of glial tliiJlOrs
1993.
18. Imam SA, Young L, Chaiwun B, Taylor CR:Comparison of two microwave-based antigen retrievalsolutions in unmasking epitopes in formalin-fixedtissue for immunostaining. Antieaneer Res 15(4): 11531158,1995.
19. Karamitopoulou E, Perentes E, Melaehrinou M,Maraziotis T: Prolifera ting eel! nuclear antigenimmunoreaetivity in human central nervous systemneoplasms. Aeta NeuropathoI85(3): 316-322, 1993.
20. Kawai K, Serizawa A, Hamana T, Ssutsumi Y: Heatindueed antigen retrieval of proliferating een nuclearantigen and p53 protein in formalin-fixed, paraffinembedded sections. Pathol Int 44(10): 759-764, 1994.
21. Khoshyoma S, Maier T, Kitz K, Budka H:Immunostaining for proliferating een nuclear antigen:!ts role in determination of proliferation in routinelyproeessed human brain tumor specimens. AetaNeuropathoI86(6): 582-589, 1993.
22. Kim DK, Hoyt J, Baeehi C, Keles GE, Mass M, MaybergMR, Berger MS: Oeteetion of proliferating een nuclearantigen in gliomas and adjaeent reseetion margins.Neurosurgery 33(4): 619-625, 1993.
23. Kordek R, Biernat W, Alwaiak i, Liberski PP:Proliferating een nuclear antigen (PCNA) and Ki67immunopositivity in human astroeytie tumors. AetaNeuroehir 138: 509-513, 1996.
24. Korkolopoulou P, Christodoulou P, Lekka KI, KouzelisK, Papanikolaou A, Panayotides I, Mariatos P, ThomasTE, Croeker J: Prognostie signifieanee of proliferatingeen nuclear antigen (PCNA) expression in gliomas.Histopathology 25(4): 349-355, 1994.
25. Korkolopoulou P, Christodoulou P, Papanikolaou A,Thomas TE: Proliferating eel! nuclear antigen andnucleolar organizer regions in CNS tumors: Correlationwith histologieal type and tumor grade. A eomparativestudy of 82 eases on paraffin seetions. Am J Surg Pathol17(9): 912-919, 1993.
26. Lammie GA, Beekett A, Courtney R, Searavilli F: Animmunohistoehemieal study of p53 and proliferatingeel! nuclear antigen expression in progressivemultifoeal leueoeneephalopathy. Aeta NeuropatholBerI 88(5): 465-471, 1994.
27. Lee KS, Yang Wl: Comparison of brain tumor growthkineties by proliferating een nuclear antigen (PCNA)and bromodeoxyuridine (BrdU) labeling. Yonsei MedJ 33(3): 265-271, 1992.
28. Liu HM, Chen HH: Correlation between fibroblastgrowth faetor expression and eel! proliferation inexperimental brain infaret: Studied with proliferatingeel! nuclear antigen immunohistoehemistry. JNeuropathol Exp NeuroI53(2): 118-126, 1994.
29. Mancini R, Marueei L, Beredetti A, Jezequel AM,Orlandi F: Immunohistoehemieal analysis of S-phaseeells in normal human and rat liver by PC10monoclonal antibody. Liver 14(2): 57-64, 1994.
30. Miyake T, Okada M, Kitamura T: Reaetive proliferationof astroeytes studied by immunohistoehemistry for
proliferating een nuclear antigen. Brain Res 590(1-2):300-302, 1992.
31. Mul!er W, Afra D, Sehröder R: Supratentorialreeurrenees of gliomas. Morphologieal studies inrelation to time intervals with oligodendrogliomas.Aeta Neuroehir 39: 15-25, 1977.
32. Mul!er W, Afra D, Sehröder R: Supratentorialreeurrenees of gliomas. Morphologieal studies inrelation to time intervals with astroeytomas. AetaNeuroehir 37: 75-91, 1977.
33. Nakasu S, Nakajima M, Niska H, Matsuma K, HandaJ: Proliferating een nuclear antigen expression in ratglioma modeL. Neurol Med Chir Tokyo 34(5): 269-273,1994.
34. Patt S, Giraldo M, Martin H: AgNOR and PCNAstudies in astroeytomas of the optie nerve. ZentralblPathoI140(1): 83-87, 1994.
35. Pelosi G, Bresaola E, Manfrin E, Rodena S, Sehiavor I,Iannuehi A: Immunoeytoehemieal deteetion of eenproliferation-related antigen in eytologie smears ofhuman malignant neoplasms using PC10, reaetive withproliferating eel! nuclear antigen and Ki67. Aeomparative study. Areh Pathol Lab Med 118(5): 510516,1994.
36. Plate KH, Rüsehoff i, Behne J: Assessment ofhistogenesis and proliferatiye potential. In eytologicspeeimens of human brain tumors value ofimmunoeytoehemistry and nucleolar organizerregions. Analytieal and Quantitative Cytology andHistology 12: 157-164, 1990.
37. Revetsz T, AIsanjari N, Oarlinng JL, Searavilli F, LaneOP, Thomas OG: Proliferating een nuclear antigen(PCNA) expression in samples of human astroeytiegliomas. Neuropathol Appl NeurobioI15(2): 152-158,1993.
38. Sasaki A, Naganuma H, Kimura R, Isoe S, Nakano S,Nukui H, Suzuki K, Kawaosi A: Proliferating eel!nuclear antigen (PCNA) immunostaining as analternative to bromodeoxyuridine (BrdU)immunostaining for brain tumors in paraffinembedded seetions. Aeta Neuroehir 117(3-4): 178-181,1992.
39. Sehiffer D, Giordana MT, Caval!a P, Vigliani MC,Attanosio A: Immunohistoehemistry of glial reaetionafter injury in the rat: Oouble stainings and markersof eel! proliferation. Int J Dev Neuro Sci 11(2): 269-280,1993.
40. Shih Y, Kadota Y, Sato K, Sueyoshi N, Shirai T:Immunohistoehemical expression of proliferating eennuclear antigen (PCNA) in intraeranial glioma andmeningioma. Chung Hua I Hsueh Tsua Chih Taipei53(4): 193-197, 1994.
41. Shin HI, Shin DM, Shah T, Ro JY: Methods inpathology. Optimization of proliferating eel! nuclearantigen immunohistoehemieal staining by mierowaveheating in zine sulfate solution. Mod Pathol 7(2): 242248,1994.
42. Stard RO, Cross SS, Clel!and C, Silcoek PB, Rogers K,
41
Tiirkish Neiirosiirgery 10: 36 - 42, 2000 Snyrak:Proliferative cellmie/etlr antigen aiid AgNOR metliod for preoperative hist%gica/ gmdiiig of g/in/ tiimors
Smith JH: Delay in fixation does not affect theimmunoreactivity of proliferating cell nuclear antigen(PCNA). J PathoI168(2): 197-199, 1992.
43. Szepesi A, Gelfand EW, Lucas JJ: Association ofproliferating cell nuclear antigen with cyclindependent kinases and cyclins in normal andtransformed human T lymphocytes. Blood 84(10):34133421, 1994.
44. Tohan SR, Wei Y, Ling P, Bistrian BR: Influence ofFormalin fixation time and tissue processing methodon immunoreactivity of monoclonal antibody PClO forproliferating cell nuclear antigen. Mod PathoI8(2): 177182, 1995.
45. Taylor CR, Shi SR, Chaiwun B, Young L, Imam SA,Cote RJ: Strategies for improving theimmunohistochemical staining of various intranuclearprognostic markers in Formalin-paraffin sections:androgen receptor, estrogen receptor, progesterone
42
receptor, p53 protein, proliferating cell nuclear antigen,and Ki67 antigen revealed by antigen retrievaltechniques. Hum PathoI25(3): 263-270, 1994.
46. Theunissen PH, Blauw G: Proliferating cell nuclearantigen immunostaining and survival in cerebralastrocytomas. Histopathology 23(1): 75-79, 1993.
47. Vigliani MC, Chio A, Pezzulo T, Soffietti R, GiordanaMT, Schiffer D: Proliferating cell nuclear antigen(PCNA) in low-grade astrocytomas: !ts prognosticsignificance. Tumori 80(4): 295-300, 1994.
48. Yang XY: Preservation of PCNA in different fixatives,and demonstration of PCNA as well as membrane
antigen by double-labelling technique. Chung HuaPing Li Hsueh Tsa Chih 22(2): 74-76, 1993.
49. Zeng XR, Hao H, Jiang Y, Lee MY: Regulation ofhuman DNA polymerase delta during the cell cycle. JBiol Chem 269(39): 24027-24033, 1994.
















![PERFORMANS ÖLÇÜMÜ, YÖNETĠMĠ VE ...360 derece değerlendirme, vb. yaklaĢımlar kullanılmaktadır [SABUNCUOĞLU, s.166-169]. Bu çalıĢmada, yöneticilerce değerlendirilen](https://img.pdfslide.us/doc/110x75/5f78768d5d91b764e6372025/performans-loemoe-ynetm-ve-360-derece-deerlendirme-vb-yaklamlar.jpg)






![FA Equipment for Beginners(PLCs) TUR.ppt [互換モード] · (2) Olay/nesne slrasl alzlllm, Daglantm, aral¶K Olay derece slrasl, stra, stralanma (3) Olaylann/nesnelerin geçi$ :](https://img.pdfslide.us/doc/110x75/5e372327681de455053832b4/fa-equipment-for-beginnersplcs-turppt-fff-2-olaynesne-slrasl.jpg)