Embed Size (px)
Citation preview

Nefrologia pediatrica tra aggiornamento e linee guida
Sabato 14 novembre 2015
Università degli Studi di Milano-Bicocca, Monza
Citopatia mitocondriale con coinvolgimento renale:
nuove prospettive fisiopatologiche e terapeutiche
Giovanni Montini
Milano, [email protected]
CLINICA PEDIATRICA
Direttore : Prof Andrea Biondi


Characteristics of mitochondrial genetics
Mutant and wild type mtDNA molecules segregate randomly in
daughter cells during each cell division
Random drift
A mutation must affect a critical proportion (usually >70~%) of
the total mtDNA molecules within a cell or tissue to cause a
biochemical effect resulting in a clinical phenotype
Threshold effect
Wild type and mutant mtDNA molecules can coexist in different
proportions within cells of the same tissue or in different
tissues of the same individual
Heteroplasmy
Both genders might be affected by mtDNA mutations, but only
females transmit mutations to their children
Maternal
inheritance
F Emma, G Montini, SM Parikh, L Salviati
Nature Reviews in Nephrology in press

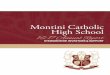
Interplay of mitochondrial and nuclear genes in
the biogenesis of the respiratory chain
F Emma, G Montini, SM Parikh, L Salviati
Nature Reviews in Nephrology in press
Mitochondrial DNA
encodes for 13 structural
subunits of the RC, and
for the 2 rRNA and 22
tRNA required for
mitochondrial protein
synthesis.
Nuclear DNA encodes for
all other structural
subunits of the RC
complexes, cytochrome c,
and their assembly
factors and for the
enzymes required for
CoQ10 biosynthesis.
F Emma, G Montini, SM Parikh, L Salviati
Nature Reviews in Nephrology in press

Citopatie mitocondriali e rene
• Malattie tubulari (più frequenti)
• Malattie glomerulari (secondarie a mutazioni della
via metabolica della biosintesi del coenzima Q10 o
mutazioni m.3243 A>G mutation in the
tRNALeu(UUR) gene)
• Il malfunzionamento mitocondriale concorre alla
fisiopatologia del danno tessutale


Podocytes
• Podocytes are highly differentiated cells with limited replicative capacity. Their functions are:
– they are major component of the glomerular filtration barrier,
– they support the other capillary components in counteracting endocapillary pressure
– they synthesize major cytoskeletal proteins and extracellular matrix components
– they have several immunological roles.
• Podocytes are particularly dependent on energy and are rich in mitochondria. Impairment of oxidative phosphorylation in podocytes results in
– excessive generation of ROS
– disruption of the glomerular filtration barrier
– proteinuria and ultimately the development of glomerular sclerotic lesions.

� Coenzyme Q10, Ubiquinone, ubidecarenone, Coenzyme Q, CoQ10, CoQ or Q10
� It is a 1,4-benzoquinone chemical compound, where Q refers to the redox active benzoquinone chemical group and 10 refers to the number of isoprenyl chemical subunits in its tail.
Coenzyme Q10 (1)

Coenzyme Q10 (2)
• Vitamin like substance, lipophilic
• First isolated in 1957 in beef heart
mitochondria (Crane FL et al., Isolation of a quinone
from beef heart mitochondria. Biochimica et Biophysica Acta,
1957)
• Highest concentrations in tissues
with high energy turnover (heart,
brain, liver, kidney)
• Humans and rodents mainly CoQ10
and CoQ9

PDSS1 and PDSS2 (COQ1)

Coenzyme Q10(3)
Co Q10 functionsElectron transporter in the mitochondrial respiratory chain
P. Mitchell
Nobel Prize for Chemistry 1978

Di Mauro S et al JCI 07

Coenzyme Q10(3)
Co Q10 functionsElectron transporter in the mitochondrial respiratory chain
Cofactor for dehydrogenases
Electron transporter outside the mitochondria
It is implicated in the inhibition of apoptosis
Regulates mitochondrial transmembranepermeability
It is required for pyrimidine nucleoside biosynthesis
Anti oxidant
P. Mitchell
Nobel Prize for Chemistry 1978

CoQ10 may be of benefit as an ingredient for topical cosmetic products.
CoQ10 has the beneficial effect of preventing photoaging. We were
able to demonstrate that CoQ10 reduce the level of oxidation.
Furthermore a reduction in wrinkle depth following CoQ10 application
was shown. CoQ10 was determined to be effective against UVA
mediated oxidative stress in human keratinocytes.

(100 single or combination-ingredient products. In 2002 200m $ sales in USA)

Accessed August 2014

Two sisters (14 and 12 yo) presented with encephalomyopathies.
Blood tests: Elevated lactic acid and creatine kinase
Muscle histology: ragged-red fibers and excessive lipid
Muscle biochemistry: Decreased
activities of mitochondrial respiratory chain complexes I+III and II+III.
Low CoQ10 (~5% of normal)

• 3 siblings with a complex clinical syndrome: progressive encephalopathy and SRNS.
• 2 developed ESRF and were transplanted at 8 and 9 years of age
• 1 died at 8 years of age after rapid neurologic deterioration

• Male, b 02.12.2000; Parents first cousins
• At 2 months nystagmus
• At 12 months NS
• Renal biopsy: FSGS
• Mutation analyses of nephrin and podocin negative.
• Treatment with steroids, diuretics, and cyclosporine ineffective

SL, male, b. 02.12.00
• Neurologic deterioration with progressive psychomotor
regression and loss of the ability to walk and stand.
Funduscopic examination showed optic atrophy.
• Brain MRI showed diffuse cerebral atrophy
• 18 mo ESRF PD Tx
• Low CoQ10 levels and complex II+III in the fibroblasts
• CoQ10 was initiated with neurologic improvement
Neurology 2005;65:606-608

NL, b. 10.10.02
� Female sibling with a preclinical diagnosis of CoQ10 deficiency at 12 months of age
� At 12 months of age Nephrotic Syndrome: urinary protein excretion: 55 g per square meter of bs per day, hypoalbuminemia (13.5 g/L of albumin), and severe generalized edema.
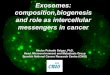
� Renal biopsy: mild focal segmental glomerulosclerosis; at EM : podocytes particularly rich in mitochondria.

2 podocytes with the cytoplasm completely occupied by mitochondria and hyperplasia of the podocyte villae. For the richness of mitochondria these cells appear similar to "oncocytes".
Detailed view of the mitochondria showing a reduced number of crests

After 8 yrs no neurological symptoms.
Normal renal function
Regression of NS
30 mg/Kg

� Visual acuity: 1/10
� Visual field restricted (rode cone dystrophy)
� Deafness; hearing aid
� Kidney transplantation
� Severe neurologic sequelae of encephalopathy, seizures, and hemiplegia
� Visual acuity: 8/10
� Normal visual field
� Normal hearing
� Normal kidney function; modest proteinuria
� Normal neurologic examination
SL CoQ10 late Tx NL CoQ10 early Tx
NL and SL long-term effects of CoQ10 Tx
ML 3 year old, normal boy: prental diagnosis, no mutation

c. 890 A>G Y297C
Homozygous missense mutation in COQ2
Am J Hum Genet 2006; 78: 345-349
CoQ10 Deficiency: Genetics
The A G transition at nucleotide 890 changes a highly conserved tyrosine tocysteine at amino acid 297 within a predicted transmembrane domain
Quinizii C et al

Yeast Model
Δ
COQ2
Transformation with WT or Mut
(human or yeast) Gene
Does not grow onnon-fermentable
media


(150)
(151)
(152)
(153)
(154)
Tubulopathy
Tubulopathy
Tubulopathy
Tubulopathy*
Tubulopathy*
RRM2BTWINKLEMPV17SUCLA2DGUOK
Defects in genes involved in mtDNA
maintenance
(147)
(148)
(149)
Tubulopathy
Tubulopathy
Tubulopathy
MRPS22YARS2SARS2
Defects in genes Involved in mtDNA Translation
(142)
(143)
(144)
(145)
(146)
Tubulopathy
Tubulopathy*
Tubulopathy
Tubulopathy
Tubulopathy*
COX10SURF1BCS1LUQCC2TMEM70
Defects of assembly factors
(90)
(89)
(88)
(85)
(86)
(63)
SRNS
SRNS
SRNS
SRNS
SRNS
Tubulopathy
PDSS1PDSS2COQ2COQ6ADCK4COQ9
Defects of electron carriers (including CoQ
biosynthesis)
ReferenceRenal phenotypeGeneCategory
Defects in nuclear genes that affect the
biogenesis of the respiratory chain and present
with a renal phenotype
F Emma, G Montini, SM Parikh, L Salviati
Nature Reviews in Nephrology in press


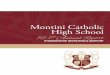
Copyright ©2008 American Physiological Society
Saiki, R. et al. Am J Physiol Renal Physiol 295: F1535-F1544 2008;doi:10.1152/ajprenal.90445.2008
Fig. 8. Hematoxylin- and eosin-stained sections of kidneys from Q10-treated and untreated B6
Normal kidney in a Q10 treated162-day-old B6.Pdss2 mice. Urine albumin: 3.7 mg/24 h
Severe IN in an untreated
128-day-old B6.Pdss2 mice. Urine albumin: 57.34 mg/24 h
Note the severe interstitial
inflammation, tubular dilatation, and glomerular crescents

• Rare autosomal recessive trait (ca 60 patients have been reported), first described in 1989
• Clinically heterogeneous disorder of the respiratory chain
• Four major phenotypes
• Encephalomyopatic form
• Multisystemic infantile variant with renal disease
• Myopathic form
• Ataxic form
CoQ10 Deficiency: Clinical Presentations
Multisystemic Form
• Developmental delay, ataxia, pyramidal signs, mental retardation
• Nephrotic syndrome, renal failure, tubulopathy; FSGS, collapsing glomerulopathy, severe extracapillaryproliferation
• Cardiomyopathy
• Frequent visual and hearing involvement
• Early onset: from birth up to 2nd year of life
• Onset symptoms: nystagmus, severe myopia, deafness, delayed motor development, poor feeding, nephrotic syndrome
CoQ10 Deficiency: Clinical Presentations

• Blood lactate levels
• Decreased combined activity of complex II+III in muscle
biopsies toghether with normal both complex II and III
• Biochemical study of CoQ10 in both muscle and fibroblasts
seems advisable to demonstrate the deficiency in all patients
• CoQ10 concentration in peripheral blood mononuclear cells?
• Plasma concentration is inadequate as it is influenced by
diet.
• Screening using NGS and specific gene panels is becoming a
valuable diagnostic approach
CoQ10 Deficiency: Diagnosis

• Dietary contribution (3-5 mg per day) is minimal. The body relies on endogenous synthesis: supplementation is essential
in the treatment of CoQ10 deficiency
• Importance of CoQ formulation: soluble
formulations are better. Our patients both worsened their
symptoms when switched from vials to tablets (bioavailability of the
crystalline form is low and inconsistent, because of the poor solubility
and high molecular weight of this form)
• Now capsules containing oily formulation (absorption is enhanced in the presence of lipids)
• Remarkable safety profile (very few side effects).Safe at intakes of up 3000 mg/day
CoQ10 Deficiency: Treatment

� Coenzyme Q10 nephropathy should be considered when mitochondrial abnormalities in podocytes are present on EM, in familial cases of NS or in association with a multisystemic disease .
� Renal cortex, and cultured skin fibroblasts should be analysed for coenzyme Q10 content.
� If coenzyme Q10 deficiency is present, genetic studies should be performed.
� It is important that ubiquinone deficiency be recognized because this form of mitochondrion dysfunction respond well to oral coenzyme Q10
supplementation.
CoQ10 Deficiency: conclusions