Embed Size (px)
Citation preview

COMPUTED TOMOGRAPHY EVALUATION OF HEPATIC PERFUSION DISORDERS
I MARZOUK MOUSSA, F KSONTINI, L BEN FARHAT, A MANAMANI, N DALI, L HENDAOUI
MEDICAL IMAGING AND INTERVENTIONNAL DEPARTEMENT, MONGI SLIM HOSPITAL, LA
MARSA TUNISIA
GI12
Introduction The liver has a dual blood supply , which
comes from the hepatic artery ( 25% of vascularization) and the portal vein ( 75% of vascularization).
There are several communications between both systems including hepatic sinusoids and peribiliary plexus .
when vascular compromise of hepatic blood supply or venous drainage occurs ,control systems intervene inducing in imaging abnormalities of parenchymal enhancement time varying.
These hepatic perfusion disorders (HPD) can be detected with multiphases computed tomography imaging through the study of the parenchymal enhacement kinetic.
HPD are commonly associated with changes in arterial , portal or venous flow and sometimes have mixed origin .
Material and Methods
A retrospective study including seven patients with hepatic perfusion disorders :
hepatic abscess Rendu-Osler disease Pancreatic head cancer with an hepatic hilar
lymph node compressing the hepatic artery Budd Chiari syndrome Superior vena cava thrombosis Hepatic cirrhosis Thrombosis of the left portal branch.
Results Arterial origin
Arterial occlusion : It rarely induces hepatic perfusion
disorders in imaging except in case of:
*Thrombosis of hepatic artery in transplantation
*An associeted venous occlusion (figure 3 ) .
CT findings : a triangular segmentary or lobar
hypodensity persisting in different phases of Iodin contrast injection with hilar somet and peripheral base .
Intrahepatic bile ducts are sensitive to arterial ischemia and may necrose giving biliar false cyst.
Arterial origin
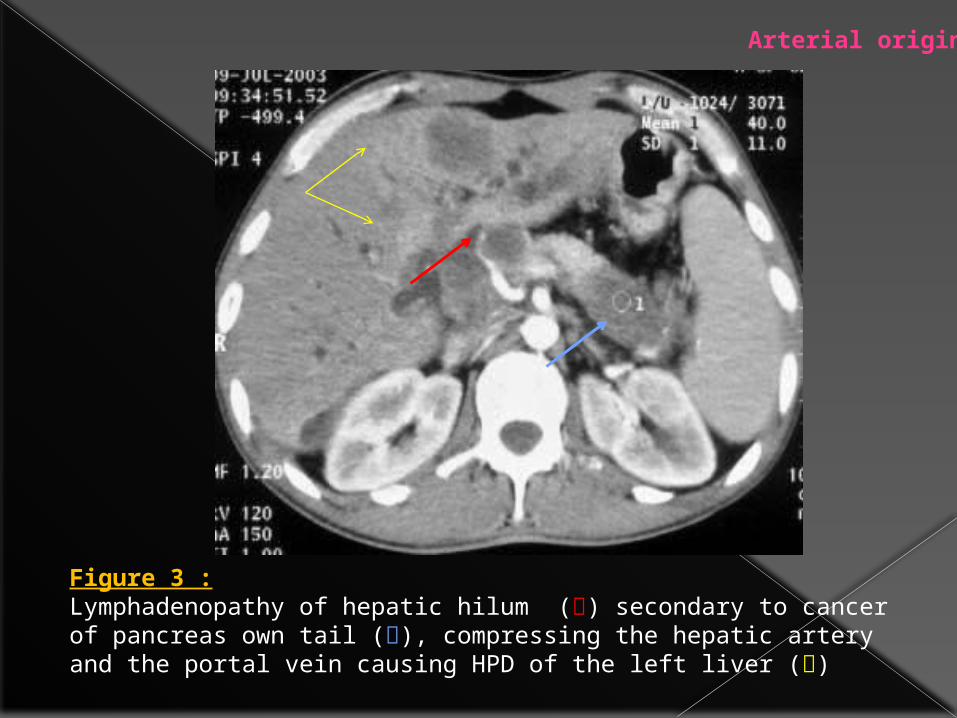
Figure 3 :Lymphadenopathy of hepatic hilum () secondary to cancer of pancreas own tail (), compressing the hepatic artery and the portal vein causing HPD of the left liver ()
Arterial origin
Arterial flow increase :
Hypervascular tumor . Intense inflammatory reaction ( figure 1) . Hereditary Hemorrhagic Telangiectasia
(HHT) called Disease of Rendu_Osler (figure 2) .
Arterial origin
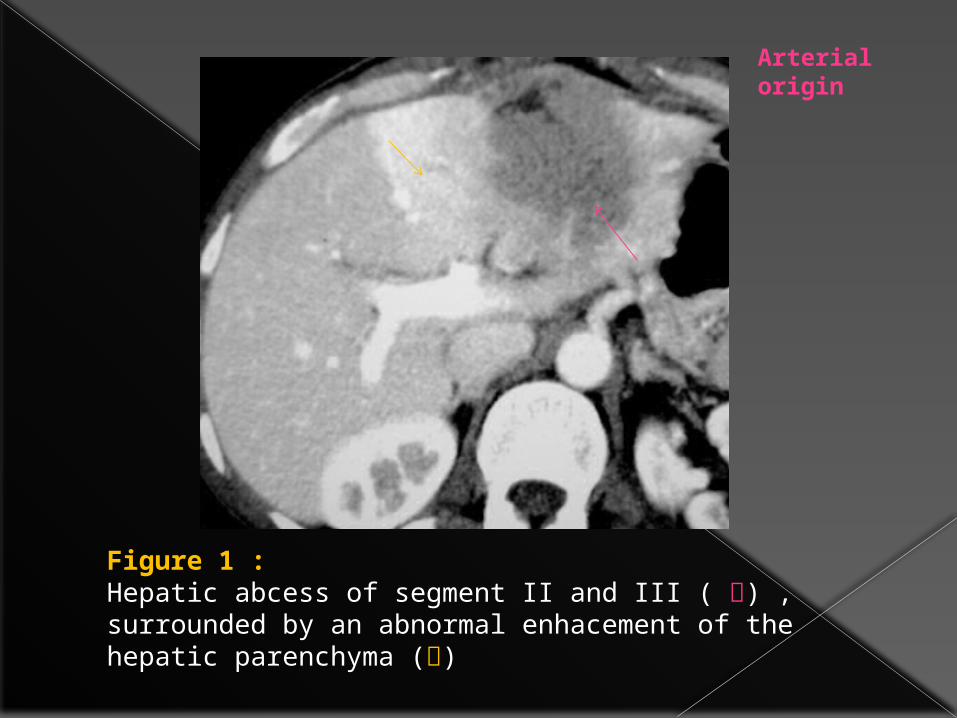
Figure 1 :Hepatic abcess of segment II and III ( ) , surrounded by an abnormal enhacement of the hepatic parenchyma ()
Arterial origin

HHT is a vascular disease with autosomal dominant transmission characterized by multiple telangiectases.
It affects mucocutaneous tissue most frequently, but any part of the body can be affected including the liver traduced by numerous arteriovenous shunts between hepatic artery branches and branches of the hepatic or portal veins.
Arterial origin
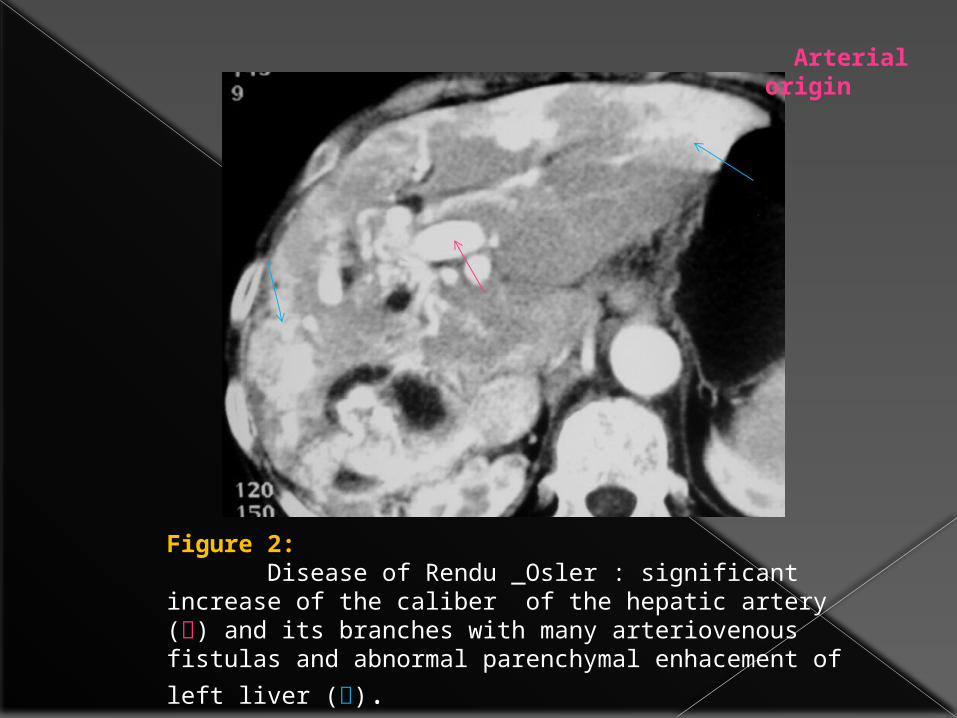
Figure 2: Disease of Rendu _Osler : significant increase of the caliber of the hepatic artery () and its branches with many arteriovenous fistulas and abnormal parenchymal
enhacement of left liver ().
Arterial origin
Portal origin
HPD are often caused by venous inflow obstruction due to portal vein thrombosis , tumor invasion ,compression or surgical ligation .
The causes of portal vein thrombosis include neoplasm that invades or compresses the portal system , infection process , embolisation , hypercoagulative states and myeloproliferative disorders.
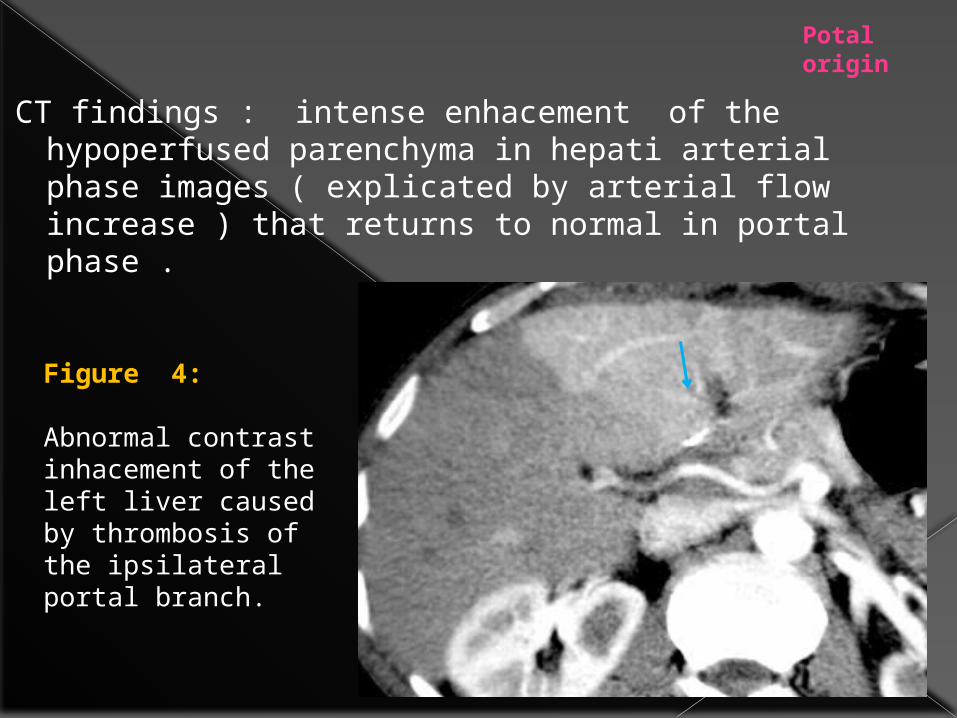
CT findings : intense enhacement of the hypoperfused parenchyma in hepati arterial phase images ( explicated by arterial flow increase ) that returns to normal in portal phase .
Figure 4:
Abnormal contrast inhacement of the left liver caused by thrombosis of the ipsilateral portal branch.
Potal origin
Venous origin
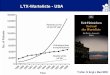
Cardiac liver . Budd Chiari syndrome ( figure 5).
CT findings : hypoperfusion of peripheral parenchyma
contrasting with a normal perfusion of the central parenchyma .
Budd-Chiari syndrome is defined as lobar or segmental hepatic venous outflow obstruction at the level of the hepatic veins or inferior vena cava (IVC) and may be primary or secondary .
This Hepatic venous outflow obstruction leads to elevation of sinusoidal pressure and diminished portal venous flow, which culminates in centrilobular congestion followed by necrosis and atrophy.
Venous origin
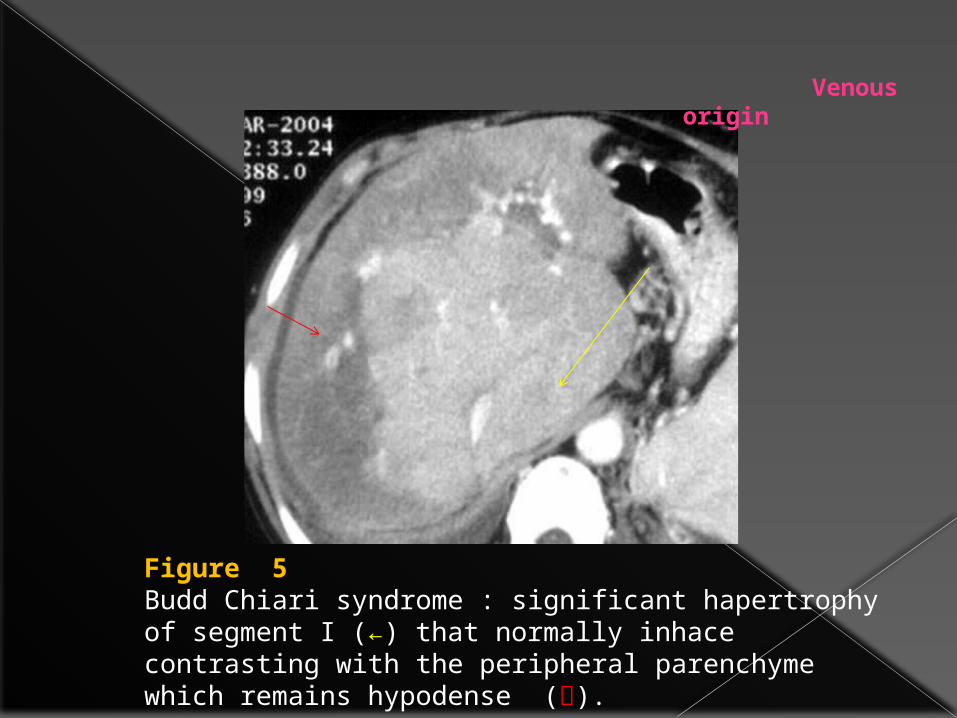
Figure 5 Budd Chiari syndrome : significant hapertrophy of segment I (←) that normally inhace contrasting with the peripheral parenchyme which remains hypodense ().
Venous origin
Mixed origin
Arterio portal fistula (APF) : An APF is an organic or a functionnal
communication between an arterial hepatic branch and the portal venous system , resulting in redistribution of arterial flow into a focal region of portal venous flow .
The causes of APF include : liver cirrhosis (figure 6) , hepato cellular carcinoma , iatrogenic fistulae after liver biopsy ,traumatic or spontaneous fistulae .
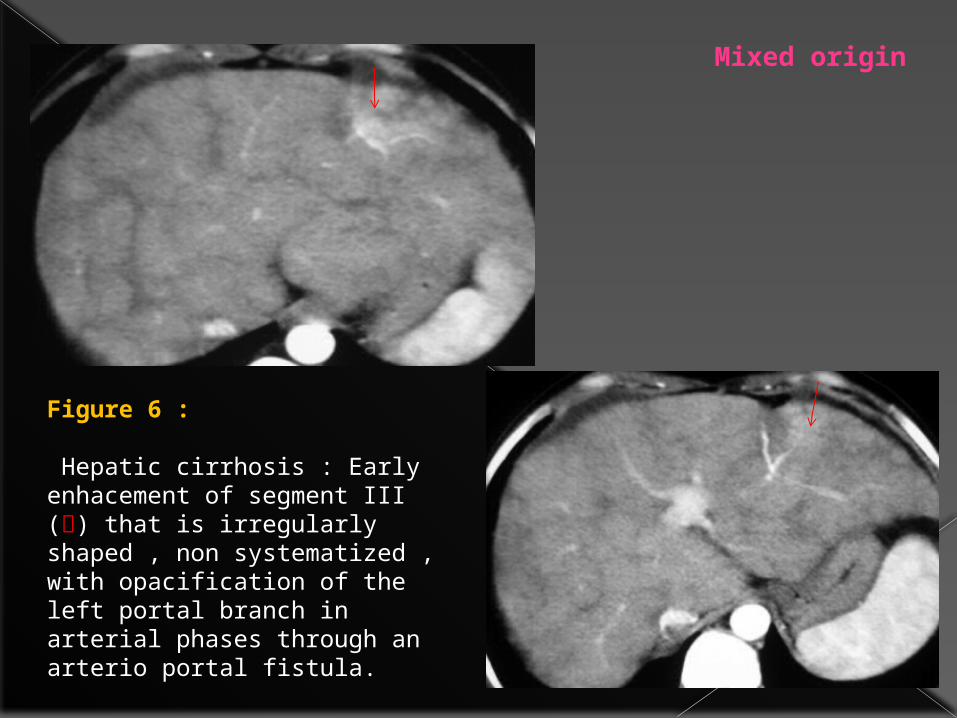
Figure 6 :
Hepatic cirrhosis : Early enhacement of segment III () that is irregularly shaped , non systematized , with opacification of the left portal branch in arterial phases through an arterio portal fistula.
Mixed origin
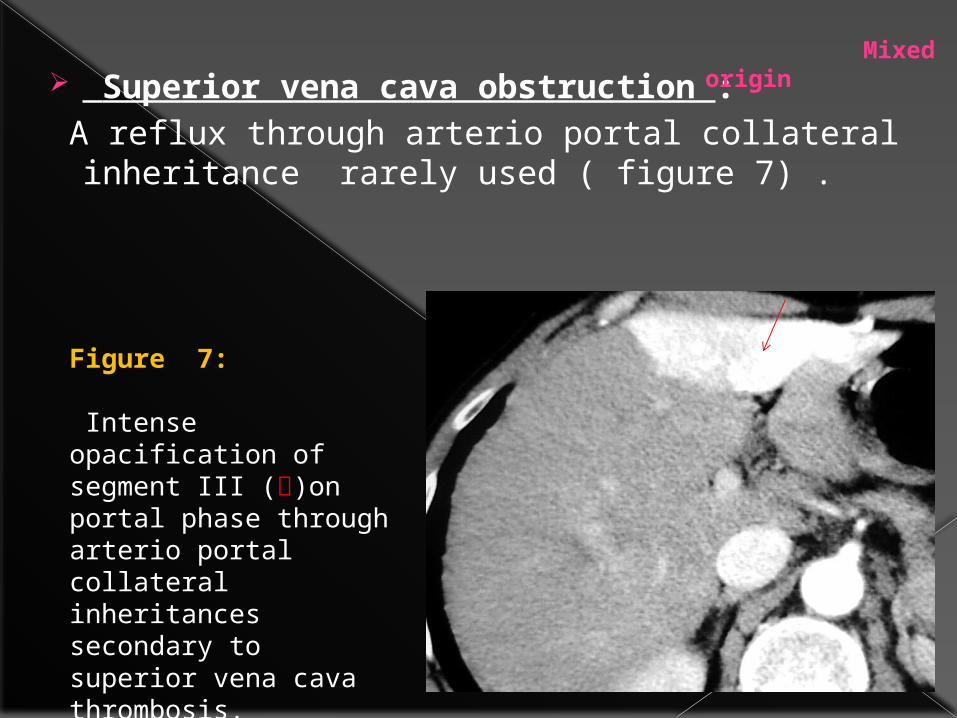
Superior vena cava obstruction : A reflux through arterio portal collateral
inheritance rarely used ( figure 7) .
Figure 7:
Intense opacification of segment III ()on portal phase through arterio portal collateral inheritances secondary to superior vena cava thrombosis.
Mixed origin
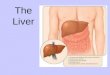
Discussion Hepatic diffuse diseases ,benign conditions
and malignant tumors are commonly
associeted with changes in arterial , portal
or hepatic venous flow, detected in imaging
by abnormal parenchymal enhacement after
iodin contrast injection ; which can be
inerpreted as false positives and negatives
in tumor detect and staging.
The mechanism can be obstruction , fistulae
or compression .
Such images are very common :
thrombosis of the portal branch induces
an early parenchymal enhancement
disappearing in portal phase. Arterial
obstruction induces segmentary or lobar
hypodensity persisting in different phases
of iodin contrast injection .
Arterio_portal fistulae can be mistaken with
hypervascular tumors or intense
inflammatory reaction.
Cardiac liver and Budd Chiari syndrome
induces a normal enhancement of the
central parenchyma contrasting with a
low enhancement in the peripheral tissue.
Conclusion
The study of different aspects of hepatic
perfusion disorders which are sometimes
misleading allows to not confuse them
with organic hepatic lesion.