Embed Size (px)
Citation preview

HPB Surgery, 1997, Vol. 10, pp. 311-314Reprints available directly from the publisherPhotocopying permitted by license only
(C) 1997 OPA (Overseas Publishers Association)Amsterdam B.V. Published in The Netherlands
by Harwood Academic PublishersPrinted in India
Case Report
Hepatic Arterioportal Fistula: A Curable Causeof Portal Hypertension in InfancyJ.S. BILLING and N.V. JAMIESONb
aSenior House fficer, bConsultant Surgeon, Department of Surgery, Addenbrooke’s Hospital, Cambridge
(Received in final form 7 November 1996)
Hepatic arterioportal fistulae are a rare cause ofportal hypertension. The case is reported of a two-year old girl with a congenital arterioportal fistula,who presented with splenomegaly and ascites.Colour doppler ultrasound showed a large shuntbetween the left hepatic artery and a branch of theleft portal vein, producing a reversal of flow in themain portal vein. She was treated by a formal lefthemihepatectomy, which has been successful ineliminating the fistula and its consequent portalhypertension in the long term. The literatureregarding arterioportal fistulae and their treatmentis reviewed.
Keywords: Portal hypertension, arterioportal fistula, conge-nital, liver resection
INTRODUCTION
Fistulae between the hepatic artery and portalvein are an uncommon but potentially curablecause of portal hypertension. Shunting of hepa-tic arterial blood into the portal circulation mostcommonly occurs as a result of an acquiredarterioportal fistula [1]. Congenital arterioportal
fistulae are rare, with only a small number ofcase reports describing this entity in children[2-4]. We report here the sixth case of a con-
genital intrahepatic fistula between the hepaticartery and the portal vein in a child, and the firstsuch case to be successfully treated by hemi-
hepatectomy.
CASE REPORT
R. S. is a female child born spontaneously at termwho was noted to have the facies of Down’ssyndrome. Chromosomal analysis confirmed thepresence of trisomy 21 and she was followed upregularly in the Child Development Centre. The
only other abnormality apparent early in life wasa secundum atrial septal defect which did notcause any significant haemodynamic compro-mise. She was otherwise generally in good health.On review in the Child Development Centre
at 9 months of age she was noted to be pale, with
Correspondence to: N. V. Jamieson, Department of Surgery, Addenbrooke’s Hospital, Hills Road, Cambridge CB2 2QQ,U.K.
311

312 J.S. BILLING AND N. V. JAMIESON
an easily palpable spleen extending 4 cm belowthe costal margin. A reducable right inguinalhernia had also recently been noted by themother. Haematological examination showed ahaemoglobin of 9.3 g/dL, with a white cell countof 3.7 and a platelet count of 152. The blood filmrevealed variable red cell sizes with polychro-masia but no blasts. A planned hernia repair wascancelled because of the anaemia.When she was 15 months old, she presented
with a two week history of increasing abdominalgirth, and her inguinal hernia, which hadinitially been noted only intermittently, wasnow present continually. Clinical examinationrevealed the presence of ascites, with a fluidthrill evident. At this stage she was still anaemic,but her liver function tests were normal. Anascitic tap was performed, which showed cleartransudate fluid with no malignant cells, Ultra-sonography demonstrated marked ascites withsplenomegaly but a normal looking liver. Colourdoppler ultrasound revealed a large arteriove-nous shunt (2 cm in diameter) between the lefthepatic artery and the left branch of the portalvein, which was seen to produce an oscillatingreversal of flow in the main portal vein. Thisarteriovenous shunt was sufficiently large toexplain the observed portal hypertension, result-ing in splenomegaly and ascites.She was started on spironolactone therapy for
the ascites. Angiography was attempted in orderto investigate this arteriovenous malformation,but a radiologist skilled in paediatric interven-tional techniques found it impossible to cathe-terise either femoral artery. A decision wastherefore made a proceed to laparotomy.At operation a dilated arteriovenous malfor-
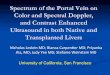
mation was identified in the left hemi liver(Fig. 1), just to the right of the falciform ligamentextending down into the umbilical fissure with-out a clear plane between the malformation andthe division of the left hepatic vessels into theirbranches to segments II, III and IV. An intra-
operative angiogram via the gastroduodenalartery confirmed that the right hepatic circulation
FIGURE Operative photograph showing the arterioportalfistula in the left lobe of the liver, immediately to the right ofthe falciform liagment. (See Color Plate III).
was normal with gross abnormality of the leftsided system in relation to the visible abnorm-ality in segment IV. A biopsy of the liver wastaken and confirmed normal histology. Localexcision was not felt to be possible given theextent and the site of arteriovenous malformationand a formal left hemihepatectomy was under-taken, the raw liver surface being sealed withfibrin glue and collagen. Bilateral inguinalhernias were closed from inside the abdomen.
Histological examination of the resected leftliver demonstrated dilated blood vessels nearthe resection margin, which were filled withfresh blood clot. The maximum diameter ofthe lumen was 1.5 cm. On microscopy this wasseen to be a large dilated vein with markedfibro-intimal thickening and features of anarteriovenous malformation, Post-operatively,

HEPATIC ARTERIOPORTAL FISTULA 313
ultrasound scans showed normal doppler tracesof the right hepatic artery, right portal vein andright hepatic vein. In particular, the arterialisa-tion and reversal of flow in the portal veinobserved preoperatively was no longer present.The early postoperative course was compli-
cated by a bile leak from the ligated stump of theleft hepatic duct. This was dealt with a secondlaparotomy eight days after the hemihepatect-omy, when a T-tube was inserted into the residualduct. The subsequent postoperative course wasuneventful and the T-tube was removed afterthree months, following a satisfactory T-tubecholangiogram. Ultrasonography six monthsafter her surgery showed that the right hemi liverhad hypertrophied and the spleen had decreasedin size. There was no ascites and normal portalvein and hepatic artery traces were identifiedwith doppler. It is now over four years since herliver resection and there has been no evidence ofrecurrence of her portal hypertension.
DISCUSSION
There are a number of reported causes ofarterioportal fistulae, which may be either intra-or extra-hepatic. Blunt and penetrating livertrauma, including iatrogenic injury, are the mostcommon [1]. There are a number of reports ofsuch fistulae occurring as a result of percutaneousliver biopsy [1,5]. Intrahepatic arterioportal fis-tulae were found in as many as five out of 65consecutive cases of blunt hepatic trauma [6], butmost of these were small peripheral fistulae withlow flow and closed spontaneously. In Tanaka’sseries only one case (a central fistula) persistedand required embolisation [6]. Erosion ofsplanchnic artery aneurysms into the portalcirculation is another relatively common causeof fistulae [7] and many of these will occur inextrahepatic locations. Other causes of arterio-portal fistulae are rare, and include liver tur-mours [8], hepatic amyloidosis [9] and much lesscommonly congenital cases.
Congenital shunts between the hepatic arteryand portal vein are rare lesions, as evidenced bythe small number of cases previously reported.Routh et al. could find only three previous caseswhen they reviewed the literature in 1992 [3],and there has been only one subsequent casereported from Berlin [4]. The case reported hereis also remarkable in that surgical treatment hasbeen successful in eliminating the source ofportal hypertension in the long term.The presentation of hepatic arterioportal fis-
tulae depends particularly on the flow throughthe shunt and thereby its haemodynamic con-sequences. Those with small shunts may presentas incidental findings at surgery for otherreasons, as a chance finding at post mortemexamination, or they may be detected in asymp-tomatic patients when a bruit and thrill arenoted over the liver. When there is a clinicalpresentation it is most commonly characterisedby the development of ascites or haemorrhagefrom oesophageal varices, as a result of portalhypertension [3, 8-10]. An unusual manifesta-tion of portal hypertension with which some ofthese fistulae have presented is mesentericvascular congestion, resulting in symptoms ofabdominal pain and diarrhoea [1,11].
It is of note that fistulae between the hepaticartery and portal vein tend not to produce heartfailure. This is in marked contrast to systemicarteriovenous shunts, which are a well recog-nised cause of high output cardiac failure. Foleyhas artributed this difference to the presence ofthe hepatic sinusoids lying between the vascularlesion and the right heart, which impose asignificant restriction on flow [12]. An alterna-tive explanation is that fistulae between thehepatic artery and portal vein present earlier intheir natural history due to the adverse effectsof portal hypertension, even when the flowthrough the fistula is still relatively modest.The rationale behind treatment of arterioportal
fistulae is either to overcome existing portalhypertension or to prevent its development. Ithas been demonstrated that some small arterio-

314 J.S. BILLING AND N. V. JAMIESON
portal fistulae can regress spontaneously [12].However, those shunts which are producingportal hypertension tend to persist and requiretreatment. The most direct form of treatment isformal suture ligation of the fistula itself: but thistends to be restricted to extrahepatic lesions. Analternative is to ligate the vessel or vessels feedingthe fistula [2, 3], although this has not always leftthe patient free from recurrence of portal hyper-tension as collateral vessel develop and allow thefistula to enlarge once more. A far less invasive
approach has been transcatheter arterial emboli-sation of these arterioportal fistulae [3, 5, 6] whichhas been used successfully in some cases.
For those intrahepatic arterioportal fistulaeconfined to one hemi liver or segment of theliver, hepatic resection offers a more definitiveform of treatment [10,13]. Liver resection is arather more extensive procedure than the otherapproaches discussed, with greater risk ofattendant morbidity, but it does avoid theproblem of recurrent portal hypertension whichhas been encountered when less radical techni-ques which have been employed. It also pro-vides a valuable second line of treatment when aless aggressive approach has been unsuccessful.We believe the case reported here to the firstexample of portal hypertension in a child causedby a hepatic arterioportal fistula to be success-fully treated by hemihepatectomy.
References[1] Strodel, W. E., Eckhauser, F. E., Lemmer, J. H.,
Whitehouse, W. M. and Williams, D. M. (1987).
Presentation and perioperative management of arter-ioportal fistulas. Archives of Surgery, 122, 563-71.
[2] Helikson, M. A., Shapiro, D. L. and Seashore, J. H.(1977). Hepatoportal arteriovenous fistula and portalhypertension in an infant. Paediatrics, 60, 921-4.
[3] Routh, W. D., Keller, F. S., Cain, W. S. and Royal, S. A.(1992). Transcatheter embolization of a high-flowcongenital intrahepatic arterial-portal Venous malfor-mation in an infant. Journal of Paediatric Surgery, 27,511-4.
[4] Gorenflo, M., Waldschmidt, J., Bein, G., Flocken, W.and Vogel, M. (1993). Arterioportal fistula in’infancy.Journal of Paediatric Gastroenterology and Nutrition, 16,87-9.
[5] Isik, F. F., Greenfield, A. J., Guben, J., Birkett, D. andMenzoian, J. O. (1989). latrogenic arterioportal fistulae:diagnosis and management. Annals of Vascular Surgery,3, 52- 5.
[6] Tanaka, H., Iwai, A., Sugimoto, H., Yoshioka, T. andSugimoto, T. (1991). Intrahepatic arterioportal .fistulaafter blunt hepatic trauma: case reports. Journal ofTrauma, 31, 143-6.
[7] Vanway, C. W., Crane, J. M., Riddell, D. H. and Foster,J. H. (1971). Arteriovenous fistula in the portalcirculation. Surgery, 70, 876-90.
[8] Granov, A. M., Tarazov,’P. G. and Ryzhkov, V. K.(1992). Arterioportal fistulas in liver tumors: prognosisin relation to treatment. HPB Surgery, 5, 87-94.
[9] Aramaki, T., Terada, H., Okumura, H., Tsutsui, H.,Fujita, S., Tajiri, T., Ohya, T. and Tajima, H. (1989).Portal hypertension secondary to intrahepatic arterio-portal shunt in primary amyloidosis: a case report.Gastroenterology of Japan, 24, 4103.
[10] OishiA. J., NagorneyD. M. and CherryK. J. (1993).Portal hypertension, variceal bleeding and high outputcardiac failure secondary to an intrahepatic arteriopor-tal fistula. HPB Surgery, 7, 53-9.
[11] Gryboski, J. D. and Clemett, A. (1967). Congenitalhepatic artery aneurysm with superior mesentericartery insuciency: a steal syndrome. Paediatrics, 39,344.
[12] Foley, W. J., Turcotte, J. G., Hoskins, P. A., Brant, R. L.and Ause, R. G. (1971). Intrahepatic arteriovenousfistulas between the hepatic artery and portal vein.Annals of Surgery, 174, 849-55.
[13] Shumacker, H. B. and Waldhausen, J. A. (1961).Intrahepatic arteriovenous fistula of hepatic arteryand portal vein. Surgery. Gynecology and Obstetrics,112, 497-501.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com