Embed Size (px)
Citation preview
Ghana-Denmark 1994-2016:
A Healthy Partnership An account of 22 years of life-saving cooperation in the health sector
1

The Ghanaian-Danish partnership in the health sector is unique for several reasons: It has lasted more
than 20 years; it has been characte- rized by open and frank dialogue; it has pioneered new and innovative ways of working together at both the level of policy and practical implementation. And most importantly: It has contributed to impressive results.
In short, the partnership has been a success: The Ghanaian government has been in the driver’s seat. Danida and other development partners have chipped in and provided financial and technical sup-port, and we can all be proud of having been part of this journey together.
We started in a completely different sit-uation in the mid-1990s when health con-ditions and the health system in Ghana were seriously challenged. Denmark, along with other development partners, came in to provide support at a very basic level and for capacity development of systems. Danida also provided technical advisors who took an active part in the day-to-day operations at the time.
22 years is a very long time. Ghana is no longer a low-income, but a lower middle-income country, and the Ghanaian
health system is in a much better condi-tion than when we started: Doctors and health staff are well trained, systems are working much better, and health indica-tors illustrate dramatic improvements: More children are surviving, people live longer, health services have improved, lives are saved.
We had to pull out at one stage, and the time is now. We constantly have to consider how we spend our development cooperation budget best, and we are convinced that things will work out in the Ghanaian health system without our active participation.
The phasing out of Danish support to Ghana’s health sector does not mean the end to the partnership. We are gradually moving from development cooperation and entering new forms of cooperation: Commercial, political, and cultural.
The new phase means a diversification of our relations, and the long-term part-nership in the health sector contributes to the solid foundation for the next phase of the Ghanaian-Danish partnership. We look forward to that.
Tove Degnbol
Ghana-Denmark 1994-2016:A Healthy Partnership December, 2015
Publisher: The Embassy of Denmark in Ghana67, Dr. Isert Road, North RidgeP.O. Box CT 596,Accra, Ghana
E-mail: [email protected]: www.ghana.um.dk
Design: Jørn RasmussenText: Jesper HeldgaardConsultant: Andreas BjerrumPhotos: Jesper HeldgaardExcept page 2 (Danida) and page 12-13 (private)
The publication can be downloaded from:www.danida-publikationer.dk
The text of this publication can be freely quoted
ISBN: 978-87-7087-898-2 (E-paper) 978-87-7087-899-9 (PDF) 978-87-7087-900-2 (HTML)
E-PAPER, REPORT AND FILMSThe experience from the Ghana-ian-Danish health partnership is worth documenting and learning from. The Danish Embassy in Ghana therefore commissioned health systems special-ist Andreas Bjerrum and freelance-jour-nalist Jesper Heldgaard to highlight some of the challenges, successes, beneficiaries and key players. Not in the form of a traditional review or evaluation, but through this e-paper, a technical report and five short films, which are all available on www.ghana.um.dk
The ambassador’s note:
A unique partnership
2 Ghana-Denmark 1994-2016 – A Healthy Partnership
ContentLeaving behind a healthier Ghana 4
6 The bad old days in Upper West
Champions of health insurance 8
10 Presbyterian AND governmental
Meet the Masters 12
14 Those were the happy days
Danida – a strong brand in Ghana 16
Ghana-Denmark 1994-2016 – A Healthy Partnership 3
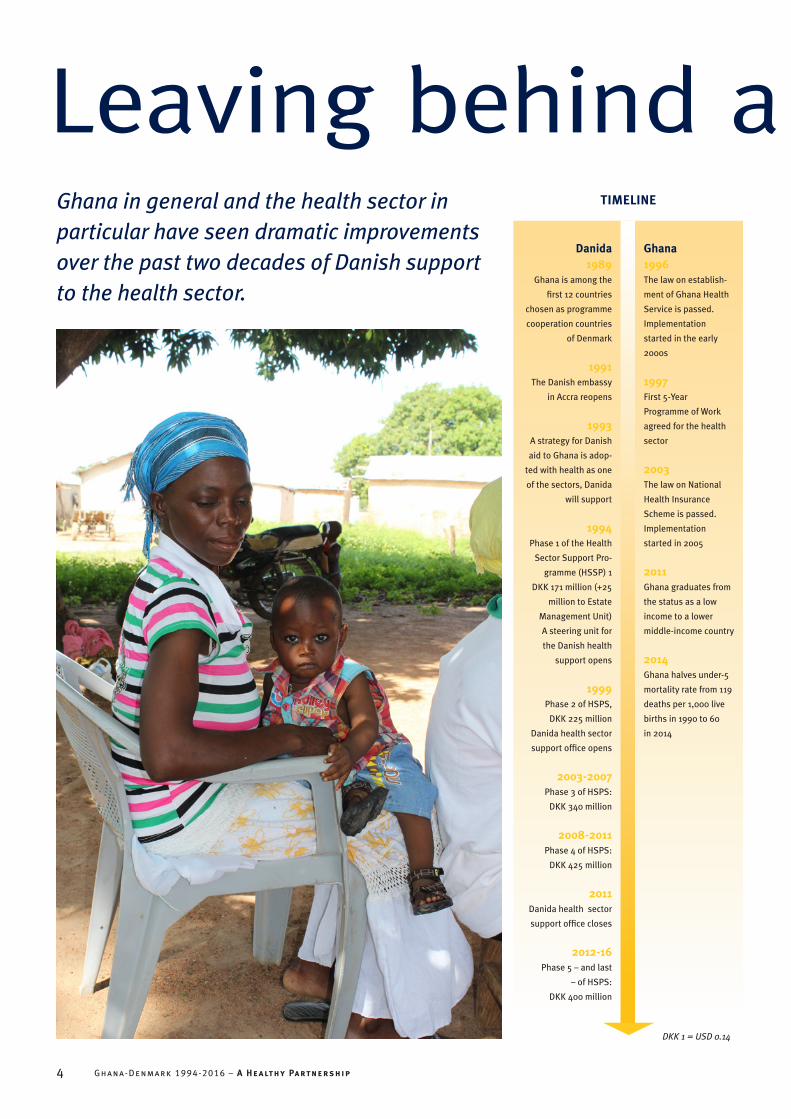
Ghana in general and the health sector in particular have seen dramatic improvements over the past two decades of Danish support to the health sector.
Leaving behind a healthier GhanaDanida
1989Ghana is among the
first 12 countries
chosen as programme
cooperation countries
of Denmark
1991The Danish embassy
in Accra reopens
1993A strategy for Danish
aid to Ghana is adop-
ted with health as one
of the sectors, Danida
will support
1994Phase 1 of the Health
Sector Support Pro-
gramme (HSSP) 1
DKK 171 million (+25
million to Estate
Management Unit)
A steering unit for
the Danish health
support opens
1999Phase 2 of HSPS,
DKK 225 million
Danida health sector
support office opens
2003-2007Phase 3 of HSPS:
DKK 340 million
2008-2011Phase 4 of HSPS:
DKK 425 million
2011 Danida health sector
support office closes
2012-16Phase 5 – and last
– of HSPS:
DKK 400 million
Ghana1996 The law on establish-
ment of Ghana Health
Service is passed.
Implementation
started in the early
2000s
1997 First 5-Year
Programme of Work
agreed for the health
sector
2003The law on National
Health Insurance
Scheme is passed.
Implementation
started in 2005
2011Ghana graduates from
the status as a low
income to a lower
middle-income country
2014Ghana halves under-5
mortality rate from 119
deaths per 1,000 live
births in 1990 to 60
in 2014
TIMELINE
DKK 1 = USD 0.14
4 Ghana-Denmark 1994-2016 – A Healthy Partnership
The contrast speaks volumes: When Ghana was an-
nounced a programme cooperation country of Danish aid in 1989, Ghana was a low-in-come country, suffering from political instability and a poor-performing health sector.
Today, Ghana has become a lower middle-income country with a vibrant, but stable democracy, and though growth has in recent years stagnated, Ghana boasts several years of impressive growth rates reaching a record 14% in 2011.
When it comes to health, achievements are as monumental: Under 5- and mater-nal mortality have been halved, health expenditure has increased dramatically, and the number of doctors has more than doubled. In short, Ghanaians have be-come healthier; they live longer and have access to better health care.
“Back in the 1990s, we were not dreaming that this could happen,” Ghana’s Deputy Minister of Health, Dr. Victor Asare Bampoe, says. “And I think that
the relative success of Ghana in health in
general can partially be attributed to Danida and to
Denmark.” “Danida has throughout been one
of what we call the core partners, who allowed Ghana to take the driver’s seat. And rather than earmarking its support, Danida put money in a basket to support the government’s policy and priorities. A recent example of this is the ebola threat. Here, Danida acted quickly and gave us funds to strengthen our ebola response. Though it was earmarked support, it was flexible and with no other strings attached than to use it most effectively. And as we speak now, Ghana has not had any case of ebola.”
GHANA FACTSPopulation and health
Mid-90s 2014
Total population 17 million 25.9 million
GDP per capita in current US dollars USD 403 USD 1,858
Share of poor of total population 51.7% (1998) 24.2%
Life expectancy at birth 56.8 years 61 years (2012)
Under 5 mortality per 1,000 119 60
Infant mortality rate per 1,000 66 41
Maternal mortality ratio (per 100,000 live births) 760 380
Immunization coverage, measles 64% 89%
Births attended by skilled staff 44% 74%
Health system and expenditure
Total expenditure on health per capita (public + private) in current US dollars
USD 19 USD 100 (2013)
Total expenditure on health (public + private) as % of GDP 3.1 5.4
Ghana government total expenditure on health USD 100 millionUSD 1,500 million
(2013)
Government health budget’s share of total government budget 7% 11%
Of this: Donors’ share 30% 10%
Number of doctors 1,115 (1999) 3,016
Number of nurses 16,000 (1999) 28,000
Sources: World Bank, Ghana Statistical Service, Demographic and Health Surveys
Leaving behind a healthier GhanaThe legacy of Danida according to Dr.
Victor Asare Bampoe also includes a con-sistent focus on geographical access to health as well as improving the financial access for the poor.
“Danida followed up on this with targeted support to the poorest regions of Ghana, to health infrastructure in remote areas and the inclusion of poor and vul-nerable in the National Health Insurance.”
While the ultimate goal of Ghana is to stand on its own feet without aid, Ghana is not quite there yet according to the Deputy Minister:
“We still have challenges, albeit differ-ent and not as dramatic as 20 years ago. We don’t have the financial resources to do what we want. Ghana’s new status as a lower middle-income country means that support from development partners – not only Danida – is dropping significantly. At the same time, we are facing a double disease burden: We still have work to do on the infectious diseases, but we in-creasingly – because of economic growth and life style changes – feel the burden of non-communicable diseases. I am grateful for Danida’s support, but I would have preferred Danida to stay on, so we could meet the new challenges together.” n
BRAIN DRAIN STOPPED, BUT AT A COST10-20 years ago, Ghana suffered from a dramatic ‘medical braindrain’. A survey in 2005 showed that 60% of the physicians trained in Ghana left the country. To reverse this trend, the go- vernment established the Ghana College of Physicians and Surgeons to educate specialists in medicine and surgery without sending doctors abroad. Moreover, Ghana decided to improve wages and working conditions of health staff. And this has worked: The number of doctors in Ghana has almost tripled since the mid-1990s.
This, though, has come at a cost: Salaries now make up almost 90% of Government of Ghana’s total health expenditure. One challenge has been replaced with a new one.
Ghana-Denmark 1994-2016 – A Healthy Partnership 5

Akuah Alandu stands out among the people queuing up at the Jeffisi Health Clinic in Sissala West
District in Upper West Region. For one, she is older than most of the others in the queue, who are mainly pregnant women and young mothers with their babies. She also has the aura of a person who has had her share of both joy, but even more tragedy in life. And indeed, she has:
“I have given birth to 12 children, but six of them passed away. When I was young, health services were poor. Most mothers gave birth at home without skilled birth attendants. Of course, this is very differ-ent now,” she says. Without bitterness.
Akuah Alandu is happy that health services and condi-tions have improved:
“These days, children start to walk even long before they are two years old. In the past, children could reach the age of three and still had not taken their first step. Health services are so much better now, patients come to the clinics and get the treatment and the medicine they need.”
The words of Akuah Alandu are echoed by many health staff in the Upper West Region. At Kulfuo Health Centre in Sissala
East District, midwife Luriwie K. H. Sala- matu on a busy Saturday morning with lots of mothers and babies attending the Child Welfare Clinic under a mango tree takes time to describe the change,
she has seen during her almost 10 years of service in the
region:“When I first came
here, I had to run out-reach services alone to 7 communities without roads. Now, staffing is much better. As you
see today, we are able to provide regular health
education and immunization to all. We don’t see measles any
more. Attendance has increased, and peo-ple have more faith in our services.”
Dr. Zakari Bukari is District Director of Health Services in Sissala West and Medi-cal Director of Tumu Hospital:
The bad, old days in Upper West
Ghana’s poorest region, Upper West, is where Danida’s health support has contributed to the most dramatic and visible improvements.
Child Welfare Clinic at Kulfuo Health Centre.
6 Ghana-Denmark 1994-2016 – A Healthy Partnership
“When I came to this hospital in Novem-ber 2006, I promised myself, I was leaving the following month because health ser-vice delivery was at the worst I have ever seen. The place was so deprived in terms of equipment and human resources. The patients that came had to pay, ‘cash and carry’, for services, but few could afford it. As a result, many malaria patients only showed up too late. 50% of the pregnant women were being delivered by tradi-tional birth attendants. So I thought there was no hope.”
Still, Dr. Zakari Bukari stayed on, and today he has no plans whatsoever of leaving:
“I have seen so much progress and I am keen to see more: Malaria fatality is down, ante-natal attendance is up. I could go on and on.”
More health clinics, more staff, and more equipment are all factors, which have contributed to the improved health system in the Upper West Region – and have been supported by Danida as part of the first two phases of the Danish health support: Danida-support to the Upper West Region amounted to DKK 65.2 million (USD 9.3 million) during phase 1 of the health support programme (1994-1998) and DKK 14.7 million (USD 2
million) in phase 2 (1999-2003). “This support went directly to the
beneficiaries and had a huge impact,” says Alex Bapula, Sissala East District
Health Director. “Unfortunately, Danida then decided to put its
money in a common pool, controlled by central go-
vernment, and that has created challenges for us at local level.”
Barriers removed“But as important is the
roll out of the National Health Insurance,” Dr.
Zakari Bukari stresses. “In the Upper West Region more than 85% of
women aged 15-49 years are covered by the insurance. This shows you that the in-surance has removed the most important barrier to health services for the poor and vulnerable, that is, the financial barrier. That is probably the main factor behind the drop in the malaria fatality rate, to give just one example. People now come for early treatment, because it is free.”
Dr. Zakari Bukari sees the fingerprint of Danida on most of the improvements in the region:
“Danida has for more than two decades been a staunch supporter of the Upper West Region and provided support to infrastructure, running costs, capacity building etc. Danida was also instrumen-
tal in the development of the National Health Insurance and pushed for the inclusion of the poor and vulnerable in the scheme. It is sad that Danida now phases out health support, but the capacity that Danida has helped build up in the region will stay on.” n
The bad, old days in Upper WestDANIDA’S FINGERPRINTThe Upper West Region is the poorest and most deprived region in Ghana and was from the onset of Danish aid to Ghana’s health sector a focus region for Danida. As early as 1993, Danida embarked on a 10-year programme of strengthening the health care deli- very system of the region. A starting point was improvement of the health infrastructure. In the first phase of the Danish programme, 41 health institu-tions in the region were constructed or renovated. In many cases this included staff accommodation to attract health staff to remote locations.
Danida-support also included motor-bikes to allow health staff to reach re-mote areas with poor roads. This alone resulted in a two-fold service coverage increase.
Support to radio communication also contributed to improving working con-ditions and connectivity of health staff.
The clinic funded by Danida in the 1990s is now
used for health staff accommodation in Jeffisi.
Ghana-Denmark 1994-2016 – A Healthy Partnership 7
“With the national health insurance, I can go to the hospital and get treatment
and medicine for free when I need to. Without it, I would have to pay every time and most likely end up paying far more than the premium,” 20 year-old Ramana Amina Kuyidu from Tumu in the Upper West Region explains. She has just paid the yearly premium of 20 Ghanaian Cedis (USD 5). A good bargain, as she puts it.
Ghana’s National Health Insurance Scheme (NHIS) is hailed as a model for other countries. It was established by law in 2003 with a vision to assure equitable access to health care for all residents without out-of-pocket payment.
And Danida took a very active part in the design and the roll out of the scheme with a particular focus on making sure that the poor were covered.
Putting an end to ‘Cash & Carry’After independence in 1957, health care in Ghana was financed entirely through tax revenue and provided to people for ‘free’ in public health facilities. But due to economic decline in Ghana, the standard of health care increasingly suffered and there were acute shortages of essential drugs. This in 1985 led to the introduction of user fees, known as ‘cash and carry’.
Over the years, exemptions of paying user fees were made for various diseases and categories of people. Efforts were also made at local level to set up insu- rance schemes to replace the unpopu-lar ‘cash and carry’-system with a fixed premium. In 2002, a survey found no less than 159 community-based health insu- rance schemes in Ghana.
Danida supported 35 of the local ‘bot-tom-up’ initiatives, which in many ways resembled local initiatives in Denmark in the late 19th century. Ghana’s gov-ernment, however, wanted to set up a national scheme, which should also serve the purpose of raising much needed extra funds for the health sector. There was open disagreement between Ghana and development partners, including Danida,
Champions of health insuranceGhana has – with the active support of Danida – developed an innovative model, which ensures free access to health services for the poorest and most vulnerable while also raising extra funds for the health system.
8 Ghana-Denmark 1994-2016 – A Healthy Partnership

as to how quickly to move from the bot-tom-up to a top-down approach. But in 2003, Ghana opted for the na-tional scheme and passed the 2003 legislation that paved the way for NHIS.
Danida’s support to local schemes, however, was not in vain, notes Nathanial Otoo, Acting Chief Executive Officer of the National Health Insurance Authority:
“The Danida-supported local schemes served as pilots and inspired the way NHIS was set up and developed. One im-portant example is that the pilots clearly documented that insurance schemes could not be financed through premiums only. Extra funding was needed, and that paved the way for the special financing model of NHIS including the 2.5% value added tax as the major income. Without that, NHIS would never have survived.”
to be met, meant that only 0.5% of Ghana’s population would be exempted as poor. A
survey in 1999, how-ever, categorised 27%
of Ghana’s population as ‘extremely poor’, while 40%
were categorised as poor.“So we continued making noise on
this issue. We took every opportunity to push government to make sure that the criteria for exemptions were changed so as to avoid excluding the poor from basic health services,” explains Finn Schlei-mann, Danida chief health advisor 1996 to 2007.
Even though Danida’s tough stand was not always welcome at the time, Nathani-al Otoo says that it did make an impact:
“Danida has throughout been a cham-pion for including the poor in NHIS, and Danida had a point. The initial criteria for being poor were too strict and rigid and have been abandoned. We now aim at exempting all Ghanaians living in core poverty, that is 8% of the population, and we are almost there with 1.5 million poor enrolled in the system.”
Back in Tumu in the Upper West Region, Abubakar Sulemana, NHIS-manager in Sissala East District, confirms that NHIS benefits the poor:
“NHIS affords everybody the opportu-nity to have access to quality health care. In this district, over 96 pct. of attendants at the health facilities are national health insurance subscribers – either because they pay or are exempted. It certainly tells you that the scheme has an impact in Sissala East District, one of the poorest in Ghana.” n
HOW DOES NHIS WORK?The National Health Insurance law was passed in 2003. Membership is indi-vidual, and all Ghanaian residents are supposed to be members. Members have a card which gives them access to free health care and medicine. NHIS is estimated to cover 95% of disease conditions reported in Ghana. All employers are obliged to ensure that employees are registered under NHIS, while adults aged 18-69 years in the informal sector pay an annual premi-um, which ranges between 15 and 48 Ghanaian Cedis (USD 4-12) per year, depending on the ability to pay.
WHO IS COVERED?In 2014 10.5 million out of some 27 million Ghanaians were covered by NHIS. Of these, 3.5 million paid premium while almost 7 million were exempted from paying. This group includes among others children less than 18 years of age, pregnant women and people, who are considered too poor to be able to pay the premium. People, who are not covered, have to pay for health services and medicine. More than half of the population has still not joined NHIS, though coverage has increased from 18% in 2006 to 38% in 2014.
HOW IS NHIS FINANCED?The income from premiums covers less than 4% of total NHIS revenue. The largest contribution – almost 75% - comes from a special 2.5% Value Added Tax imposed on all goods and services, which was part of the law passed in 2003 to finance NHIS. Some 20% come from a fixed salary deduc-tion for all formally employed persons.
Focus on the poorThe national health insurance scheme, however, did not remove barriers to health care for the poorest and most vulnerable, who could not afford paying the annual premium and would still have to pay – or simply stay away from hospitals and clinics.
NHIS did have provisions for exempting poor and other categories from paying the premium, but not provisions that satisfied Danida. The official term used to describe this group – ‘indigent’ – and the criteria
Ghana-Denmark 1994-2016 – A Healthy Partnership 9

The signboard at the entrance to Bawku Hospital in the furthest north-eastern corner of Ghana
leaves no doubt as to the affiliation of the hospital. ‘Presbyterian Church of Ghana’ is written in big letters on top of the signboard. And yes, the hospital is owned and run by the Presbyterian Church. At the same time, it is an integrated part of Ghana’s national health system.
The Presbyterian Church of Ghana is one of 21 Christian Church Denominations, which form the Christian Health Associa-tion of Ghana (CHAG). Together they run 183 health institutions including the hos-pital in Bawku, but also a lot of smaller health centres.
Actually, the busy Bawku Hospital was built as a government hospital in 1953 by the then colonial administration, but only three years later, in 1956, it was handed over to the church and was for the next decade run as an entirely private hospital under the church.
But in 1967, Christian health service providers and the government of Ghana took a first and cautious step towards a formalised cooperation, which has been developed and expanded ever since to become a model, which inspires other African countries. And also one, which is strongly supported by Fred Yeboah, Ge- neral Manager of Bawku Hospital:
“We enjoy the benefits of being a fully integrated part of the national health system. We work closely with govern-ment at local, regional and national level. Government pays salaries for our staff,
medical supplies etc. At the same time we are autonomous to a large extent: One example is that we appoint our own staff and thus are able to recruit locally.”
Peaceful and positive coexistenceAt the headquarters in Accra, Peter Yeboah, Executive Director of CHAG,
describes the formalized relationship as very special:
“We did not want to be swallowed by government, but opted for regulated cooperation, and we have developed a formal, legal framework, which makes the division of roles clear. We have a good dialogue at all levels and live in what I
Presbyterian AND governmentalThe close and formalized cooperation between Christian and government health service providers in Ghana is unique in Africa and a win-win that benefits the patients.
Olivia Kontomah brought her son
Bright to Martyr’s of Uganda Health
Centre in Sirigu for malaria treatment.
10 Ghana-Denmark 1994-2016 – A Healthy Partnership

DANIDA SUPPORT TO CHAGDanish support to CHAG started in the phase 2 of the Danish health sector support to Ghana 1998-2002. Here, DKK 10 million out of the total DKK 225 million was set aside to impro- ving public-private cooperation in Ghana’s health sector. This support was followed up and even increased in the following phases of Danida’s health support. In 2012, Danida covered almost 60% of CHAG’s running costs. The main purpose throughout has been to build the institutional capacity of the CHAG Secretariat.
WHAT IS CHAG?The Christian Health Association of Ghana (CHAG) is a faith-based network organisation founded in 1967. CHAG has grown from 25 health institutions in 1967 to 183 in 2015 and serves about 35-40% of the population including the most vulnerable and underprivileged population groups in the most remote areas of Ghana.
CHAG is a recognized, but autono-mous agency of the Ministry of Health. Since 1975, Government has paid the salaries of CHAG health staff. An exter-nal review of CHAG from 2007 showed that CHAG members got more support from government than is provided in any other country in Africa.
would describe as a peaceful and positive coexistence.”
Gilbert Buckle, Executive Director of CHAG until July 2014, is another strong supporter of the cooperation:
“What we do is very different from what happens in other African countries, where similar church institutions have to finance all their opera-tions themselves, and are not actively engaged in the dialogue on health with govern-ment and the various development part-ners. We cooperate on an equal footing. It is a win-win situation which also, and most importantly, benefits the patients. And other African countries come to learn about this relationship.”
Sam Adjei was deputy director of Ghana Health Services until his retirement in 2009. The close collaboration between Ghana Health Service and CHAG makes good sense, also from a government point of view:
“CHAG-facilities serve 35-40% of the population and cover many rural areas, which government facilities do not reach, so rather than competing, we preferred
cooperation and developed our own model of public-private partnership, using public resources to finance private health providers. It was quite an innovation, I would say.”
Danida in a key roleDanida has supported CHAG since the late 1990s:
“At that time the focus of Danida and most other donors had been very much on government-to-government cooperation and thus the public health sector. Still, the private health sector was a major player, but essentially focusing on service delivery only,” explains Kobina Bainson, Danida health advisor in Ghana 2000-2004. “At that time Ghana did not have a private sector policy in health, so one of the things Danida did was to support the dialogue between the public and the private sector.”
Gilbert Buckle praises the approach of Danida and its long-term, strategic
support to CHAG: “Danida very early recognized that the
church institutions can and actually do provide significant health services. They also recognized that
we have the potential to influence health
policy to promote equity and pro-poor consideration.
But we needed to develop our organisation to play a stronger policy and advocacy role. And Danida’s position was basically: We’ll support you to stand on your own. Danida has done so over many years, providing not only financial, but also technical support. This consistent support and dialogue has been key to the position, visibility and credibility, CHAG now enjoys – both with government and in the eyes of other development partners.”
Keeping each other on the toesWhile the aim is cooperation rather than competition between government and Christian health service providers, some competition remains, but now it is
competition on a level playing field, Fred Yeboah of Bawku Hospital in Northern Ghana stresses: “It helps us keeping each other on the toes.”
At the nearby Martyr’s of Uganda Health Centre in Sirigu, Tule Sebastian works as a physician as-sistant. He is well aware that government pays his salary. Still, it makes a difference to him to work at Christian health centre:
“My experience is that CHAG offers better health services than government facilities. The management at most of our facilities is very efficient and proactive because of the constant monitoring we receive from higher level,” Sebastian says and stresses that he does not want to criticize his colleagues at government health facilities, but only gives the reason why he chose to work at the Martyr’s of Uganda Health Centre. n
Presbyterian AND governmental
Ghana-Denmark 1994-2016 – A Healthy Partnership 11

From 1998 to 2013 The University of Copenhagen offered a Master of In-ternational Health (MIH) Course. Each
year around 25 students from a dozen different countries completed the course, which focused on challenges in health and health systems in low- and middle-income countries. An important element was a four weeks field trip to India, where the students were given the opportunity to test theories and methods in practice.
A total of 71 Ghanaians took the MIH-degree in Denmark, and most of them are now back in Ghana working in key positions all over the country. The following are excerpts of the feedback gathered from the Masters on the impact of their training in Denmark.
Bravo DanidaThe training in MIH has prepared me to take up an appointment as a District Director of Health Services.
My job description is to provide expert advice to the District Assembly on all matters on Health. Among other things, I lead in monitoring the implementation of Clinical and Public Health interventions including Communicable Disease Control and Surveillance, Reproductive, Ado-lescent and Child Health, Nutrition and Health Promotion.
I do appreciate the Danida scholarship for capacity building a lot. Most of my colleagues who benefited from the pro-gram are either District Directors of Health Service or Principals of Health Learning Institutions.
Bravo Danida!
Josephine Atusfe Ahorsu (MIH 2008)
A career makerI am currently doing a residency pro-gramme in public health with the Ghana College of Physicians and Surgeons. The MIH was a partial fulfilment of the re-quirements to enter the programme. I am also a medical superintendent and acting District Director of Health partly due to my MIH.
Abigail Codjoe (MIH 2013)
Inspiring IndiaThe course gave me the opportunity to go to India. I am not saying India has a perfect health system, but India inspired me as to how to properly do community health, how to get to the community and then mobilize the community to partici-pate in health. Then also team building, because the course also taught us how to build a team. You need to recognize that everybody has a role to play. It is not like you being the big man. People saying, yes sir! No, we need to work as a team and that is what I now apply in my position as District Health Director in Sissala East.
Alex Bapula (MIH 2008)
Meet the Masters
No less than 71 Ghanaian health personnel attended the 1 year Master of International Health course in Denmark from 1998 to 2013. A massive human resource capacity-building exercise.
12 Ghana-Denmark 1994-2016 – A Healthy Partnership
A life-changing experienceGetting a sponsorship and getting admitted into the MIH program has been the most life-changing experience to me! Studying at the University of Copenha-gen gave me a lot of opportunities. One was the opportunity to network with great minds around the globe on Global Health. In 2014, I was appointed a District Director of Health Service, becoming the youngest District Director of the Ghana Health Service. Later in 2014, I was given a consultancy job by the World Health Organization to support the South Sudan Government in the area of Childhood Immunization (EPI) and Surveillance.
Emmanuel K. Sanwuok (MIH 2012)
Punctiality!Today I am a District Director of Health Services in Ghana managing my district’s health system. Some lessons leant from Denmark: Punctuality; accurate docu-mentation; meeting timelines; effective planning: support for the less privileged.
Gertrude Yentumi (MIH 2010)
Useful in Ebola responseThe MIH program has indeed played an important role in my career path. With the experience gained I have effectively played key managerial roles in the Ghana Health Service. In 2014, I was deployed to Liberia during the Ebola outbreak and my knowledge of public health in low and middle income countries gained through the MIH was of great use during the period.
Gifty Sunkwa-Mills (MIH 2011)
International inspirationThere were students from other countries: East Africa, Denmark, Bhutan and also from Vietnam. So it was a very diverse group, and I learnt from each one of them.
Rufina Asuru (MIH 1999)
A word from the MIH-founderThe idea of offering the MIH-course was conceived by Dr. Ib Bygbjerg, professor at the University of Copenhagen. He also headed the course from the start. The feedback from former students to him confirms that the idea was right, even though it also carried some risks:
“When you train people from a country like Ghana, there is always a risk that they will use their degree to leave for greener pastures like Europe. But very few have done so. Most have gone back and now take up higher positions. Some have, of course, left their country of origin, but mainly to go to other African countries and use their new competences in the Ebola response, for example.
Another risk when you invite health staff from deprived areas like Northern Ghana to study in Denmark is that they may not have the qualifications to really benefit from the training. But again, this did not cause problems. The students, we had from Northern Ghana, were compe-tent, indeed, which also has to do with Ghana’s strong focus on public health.”
The MIH-course closed for uptake in 2013 and the last student is graduating soon, but the University of Copenhagen since 2013 offers a two years Master of Science (MSc) in Global Health course. It has also attracted Ghanaian students. n
Alex Bapula (2. from left) in the Danish snow with MIH fellow students.
Ghana-Denmark 1994-2016 – A Healthy Partnership 13
“It was a fantastic transformative process to be part of. We were pioneering new aid modalities,
making up with inefficient and rigid pro-ject support and replacing it with the new sector wide approach, where deve-
Those were the happy daysIn the 1990s Ghana and Danida pioneered the move from a donor-recipient relationship to a more equal partnership in the health sector. Though the visions proved right, they have not all stood the test of time.
lopment partners came together and put their money in a joint basket to support the priorities that had been defined by Ghana’s own government and agreed with the development partners.”
Dr. Victor Asare Bampoe is Ghana’s
Deputy Minister of Health, but in 1999 he joined the British aid agency’s, DfID, health support office, which was door to door with the health support office of Da-nida in Ghana. Danida, DfID and the World Bank were the dominant health develop-
14 Ghana-Denmark 1994-2016 – A Healthy Partnership

ment partners of Ghana at the time. Or as they were termed in the old-fashioned aid jargon, ‘donors’.
They had a strong presence in Ghana and a close dialogue with their Ghanaian counterparts which were key to pursuing the high-flying ambitions at the time.
Finn Schleimann, chief health advisor of Danida from 1996 to 2007, was part of the process and stresses that Danida and Ghana had a mutual interest in pushing the new aid agenda:
“Ghana was ready to take ownership of the health sector. The leadership was strong and competent and wanted to increase Ghana’s own allocation to the health sector which was at the time relatively low. On the Danish side, a new aid strategy, ‘Towards the year 2000’, had been adopted in 1994 and Ghana offered an ideal test ground for the new ideas. So even though there was some hesitance among my Danida colleagues, the Deve- lopment Minister at the time, Poul Nielson, enthusiastically backed what we tried out in Ghana.”
Sam Adjei, deputy director of Ghana Health Services until his retirement in 2009, also has fond memories of the time:
“We all spoke our minds very open-ly and though we had disagreements, government and development partners shared a sense of direction, and we managed to align the politicians behind the common goals. Danida right from the beginning supported the concept of pooling funds towards achieving the objectives, we had set up together, and implement-ing Ghana’s Programme of Work for the health sector. Also, we all bought into common mechanisms with a view to making sure that resources were allocated as much as possible to benefit people on the ground. That was new and a huge step forward.”
Sam Adjei stresses that the pooled funding did not make tracking of funds more difficult:
“We set up tracking systems which made sure we could track any penny spent of the joint baskets.”
Dr. Kobina Atta Bainson worked for Danida’s health support office in Accra 2000-2004:
“While most oth-er donors tended to focus on diseases like malaria and run specific programmes with earmarked support, Danida’s approach was: How do we support the whole system to deliver? As a consequence, most Danida support came in the form of budget support, less as earmarked support.”
What happened to the visions?The pioneers of the late 1990s and early 2000s all agree that while the transforma-tion, that they were an active part of, has made a lasting impact, the partnership is no longer as visionary as then, and that some of the achievements have to some extent been rolled back.
Why is that? The answer is not clear, but a combination of several factors accor- ding to key players, who all agree that the blame lies on both sides. Sam Adjei talks about a changed focus:
“Now there is an increased focus on quick results and value for money. Both government and donors want to see the
results of ‘their’ money, rather than being satisfied with contributing
towards achieving common goals. The trend is thus
towards reintroduction of ear-marked support and the development of si-los in the health sector. It has meant a rollback to a situation similar of
that prior to 1994 and a loss of the sense of joint
direction.”Others point to the fact that the
close dialogue in the health sector, that paved the way for the early changes, is no longer possible with the closure of
Those were the happy days the health support offices of Danida and
others. Still others stress that these trends do not apply to
Ghana’s health sector only, but to international aid in general. The Paris Declara-tion on Aid Effectiveness adopted in 2005, and based on the principles
that were tested in Ghana, can hardly be described as
the guiding principle for interna-tional development cooperation any
more. Moreover, international develop-ment cooperation – and the health sector in particular – has seen an upspring of huge vertical funds focusing on particular issues.
Dr. Victor Asare Bampoe, now Deputy Prime Min-ister of Ghana, but a former advisor at DfID’s health support office in Ghana, was out of Ghana for some years, but came back in 2014 and also found that some of the early gains in terms of partnerships had been eroded.
“I do miss the good old days, when the dialogue was tighter and the partnership was stronger. Going back to earmarked funding is not the best for us. We do, of course, have a say in what the funding should go to, but in practice, most deve- lopment partners have more or less made up their minds beforehand and tend to choose the more interesting bits of what should be done and then they do that. It takes away some of the power of the country to say want we want. So I wish we were back to the good, old days.” n
Ghana-Denmark 1994-2016 – A Healthy Partnership 15
In 1991, the Danish government in fact decided to abolish the term ‘Danida’ altogether, but it survived. The term
first appeared in 1963 and in 1971, Danida became the official name for the Danish International Development Agency. But in 1991, development assistance was incor-porated into Denmark’s Foreign Service. To mark that, it was decided to outright scrap the Danida name. The brand, however, had become so strong that it lived on. Consequently, it was officially reinterpreted as an abbreviation of Danish International Development Assistance. No longer an organisation, but an activity.
And in Ghana, and in the health sector in particular, the Danida name certainly lives on.
Danida – a strong brand in GhanaDenmark’s support to Ghana’s health sector is not only about money. It is also about a true partnership, which has earned Danida a strong brand in Ghana.
16 Ghana-Denmark 1994-2016 – A Healthy Partnership

Open and understanding“The Danida brand to me is one of being very open and understanding the Ghana-ian context and views. This does not mean that Danida-representatives would bend over and accept anything. But they would certainly be there to discuss, and you would have the feeling that they did understand and respect your point of view and as much as possible accommodate it in the programmes.”
Dr. Victor Asare Bampoe,
Deputy Minister of Health, former advisor
at the British aid agency’s, DfID, health
support office in Ghana
Focus on local capacity“Most other partners come in to ‘donate’ something. Here, Danida stands out clear-ly with its long-term focus on building local capacity, which remains here after Danida-support stops. The old saying of teaching a man to fish rather than giving him a fish certainly applies to the Dani-da-approach, we have seen.
Another key feature of Danida is super-vision and monitoring. Danida goes to the grassroots to make sure that whatever Danida has supported, continues to func-tion and benefit the people, whom it was put in place to help.”
Dr. Zakari Bukari, District Director
of Health Services in Sissala West and
Medical Director of Tumu Hospital
Interested in the partner“Danida is a partner interested in the partner. Danida was genuinely interest-ed in CHAG and encouraged CHAG to maximize its potential. For a development partner I think it is really unique. Danida does its home work, and it is open enough to say: This is what we think. What do you think? If Danida were a person, I’d say this is a very honest person, who is open about who he is, but also open to listening.”
Dr. Gilbert Buckle, Executive Director
of the Christian Health Association of
Ghana (CHAG) until July 2014
Small, but prominent“We know Denmark is a small country, but Danida has prominence in Ghana, and this is mainly due to the Danida-people who came to work with us. Danida was unique in that it was flexible. Danida-representa-tives understood the issues and the con-text, both technically and even politically. They were of a high caliber and created the Danida brand for us. We spoke our minds openly. Danida made preconditions known upfront, and did react, if we did not adhere to the preconditions. But then Danida would be flexible and open to take a dialogue on a plan B.”
Sam Adjei, deputy director, Ghana Health
Services, until retirement in 2009
Far ahead of others“Danida was far ahead of other donors with its focus on supporting systems rather than activities. Danida helped build capacity and supported innovation at all levels: Policy and implementation at both central and local level. Thus, Danida sup-port has made a lasting impact. Examples of that are several: Private sector players in health, like the Christian Health Associ-ation of Ghana, were not taken on board previously. Danida took it up, and gov-ernment developed a policy for it. Danida also influenced the design of the National Health Insurance to cater for the poor. Per-sonally, I have appreciated the long-term technical advisors of Danida in particular, because they had time to understand the culture and the policy.”
Dr. Kobina Atta Bainson, Danida’s health
support office in Accra 2000-2004
Customer-driven“Danida has been customer-driven – it does not come with a one size fits all pro-gramme, but is open to dialogue. We have had a very close and ongoing dialogue with many Danida-advisors.”
Nathaniel Otoo, acting Chief Executive,
National Health Insurance Authority
The Danida brand opens doors“Wherever you go in Ghana, the Dani-da-brand opens doors. The long and very good Danish-Ghanaian relationship that we have built through our development cooperation gives us access at high level in various ministries including the Ministry of Health. We are seen as a trust-worthy partner and we shall, of course, make use of that in the future. Also in our commer-cial cooperation. It would be completely different to fly in and try to start a com-mercial cooperation from scratch. The fact that we now know each other so well, and that Ghanaians have seen that we are not just pulling out, when things get difficult, provides a very good basis, also for other types of cooperation.”
Tove Degnbol,
Danish ambassador to Ghana
Ghana-Denmark 1994-2016 – A Healthy Partnership 17
Watch five short films:
Ghana-Denmark – a healthy partnership that saved lives http://webtv.um.dk/video/12592582/film-1eng-ghana-denmark-a-healthy
Denmark is phasing out support to Ghana’s health sector in 2016 after more than two decades, which have seen dramatic improvements in Ghana in general and in the poor Upper West Region in particular.
Access to health services – also for the poorest http://webtv.um.dk/video/12592643/film-2eng-access-to-health-services
Ghana has developed an innovative health insurance model, which ensures free access to health services for the poorest and most vulnerable while also raising extra funds for the health sector.
Keeping each other on the toes http://webtv.um.dk/video/12592491/film-3eng-keeping-each-other-on-the
A close and formalized cooperation between Christian and government health service providers in Ghana secures national coverage and leads to sound competition.
Meet the Masters http://webtv.um.dk/video/12592681/film-4eng-meet-the-masters
No less than 71 Ghanaian health personnel attended the 1 year Master of International Health course in Denmark from 1998 to 2013. Back in Ghana, 3 of them explain what they gained from the course.
Danida – a special brand in Ghana http://webtv.um.dk/video/12592720/film-5eng-danida-a-special-brand-in
More than two decades’ consistent health support to Ghana has earned Danida a special name in Ghana – not only due to the substantial financial support, but more to the very special Ghanaian-Danish partnership.
Isaac Kwesi Oduru Junior at work with his camera in Northern
Ghana documenting Danish support to the health sector on film.