Embed Size (px)
Citation preview
GERM CELL TUMOURS AS SEEN AT AHMADU BELLO
UNIVERSITY TEACHING HOSPITAL ZARIA: A TEN YEAR
HISTOPATHOLOGICAL REVIEW (2004-2013).
BEING A DISSERTATION FOR THE PART TWO (FINAL)
EXAMINATION IN PARTIAL FULFILMENT OF THE REQUIREMENT
FOR THE FELLOWSHIP OF THE NATIONAL POSTGRADUATE
MEDICAL COLLEGE OF NIGERIA IN PATHOLOGY (FMC Path)
BY
DR ABUBAKAR SIRAJO
AF/008/12/003/919
NOVEMBER, 2015
i
DECLARATION
I hereby declare that this Dissertation titled: GERM CELL TUMOURS AS SEEN AT
AHMADU BELLO UNIVERSITY TEACHING HOSPITAL ZARIA: A TEN YEAR
HISTOPATHOLOGICAL REVIEW (2004-2013) is an original dissertation developed by me.
It has not been presented to any college for fellowship neither has it been submitted elsewhere
for publication.
SIGNATURE …………………………… DATE …………
DR. ABUBAKAR SIRAJO

ii
CERTIFICATION
This study titled “Germ cell tumours as seen at Ahmadu Bello University Teaching Hospital
Zaria: A ten year histopathological review (2004-2013)” was carried out by Dr. Abubakar Sirajo
in the Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria under our
supervision.
1. Dr. Y. Iliyasu. MBBS, FMCPath, FICS, MIAC, IFCAP, FCPath (ECSA).
Consultant Pathologist and Associate Professor,
Department of Pathology,
Ahmadu Bello University Teaching Hospital,
Zaria, Nigeria.
Signature and Date…………………………………………………………………….
2. Dr. S.A. Ahmed. MBBS, MPH, FMCPath, FICS, IFCAP.
Consultant Pathologist and Associate Professor,
Department of Pathology,
Ahmadu Bello University Teaching Hospital,
Zaria, Nigeria.
Signature and Date……………………………………………………………………….

iii
ATTESTATION
This is to attest that Dr Abubakar Sirajo has developed this dissertation in partial fulfillment of
the requirements of the Part II FMCPath (Pathology) Examination.
……………………………… Date………………….
Dr S.A. Ahmed (MBBS, MPH, FMCPath, FICS, IFCAP).
Consultant Pathologist and Associate Professor.
Head of Department,
Department of Pathology,
Ahmad Bello University Teaching Hospital,
Shika-Zaria.
iv
DEDICATION
This work has being dedicated to my parents for their assistance and tender care they showed
me.
v
ACKNOWLEGDEMENT
All thanks be to Allah the almighty for making this dissertation to come to a meaningful
conclusive end.
I would like to show my gratitude to especially my supervisors, Dr. Yawale Iliyasu and Dr. Saad
A. Ahmed who helped and seen to the success of this work selflessly.
I also give thanks to those who helped me in one way or the other, they include Prof.
Abdulmumin H. Rafindadi, Prof. M.S Shehu, Dr. M.O.A. Samaila. Dr. Mayun, Dr. Almustapha
A. Liman, Dr. Garba D. Waziri and Dr. Umar Mohammed.
Most of all I also thank my family who endured and supported me through the whole endeavor.
I must thank my fellow residents like Dr. Fatima Y. Abdulqadir, Dr. Sulaiman Dauda for their
assistance. May God reward you abundantly.
vi
TABLE OF CONTENTS
DECLARATION……………………………………………………………………………....i
CERTIFICATION……………………………………………………………………………..ii
ATTESTATION…………………………………………………………………………… ..iii
DEDICATION…………………………………………………………………………………iv
ACKNOWLEGDEMENT……………………………………………………………… …v
TABLE OF CONTENTS………………………………………………………………… ..vi
LIST OF TABLES………………………………………………………………………..…..ix
LIST OF FIGURES……………………………………………………………………………x
ABBREVIATIONS AND THEIR MEANINGS……………………………………………..xi
ABSTRACT…………………………………………………………………………………xii
CHAPTER ONE
Introduction……………………………………………………………………………1
Rationale/Justification for the study………………………………………………...…3
Aims and Objectives……………………………………………………….…………..3
CHAPTER TWO
Literature Review…………………………………………………………………….………4
Epidemiology of Germ Cell Tumours………………………………………………………….4
Aetiology/Risk factors for development of Germ Cell Tumours………………………....….…9
Histiogenesis of Germ CellTumours…………………………………….……………….…….11
Cytogenetics and Molecular Pathology of Germ Cell Tumours…………….………….….…..12
Classification of Germ Cell Tumours……………………………………..…………….…..…14

vii
Review of some Morphological types of Germ Cell Tumours………………………..14
Dysgerminoma………………………………………………...……………………....14
Yolk Sac Tumours……………………………………………………………………..15
Embryonal Carcinoma…………………………………………………………………16
Polyembryoma………………………………………………………...………...……..17
Non Gestational Choriocarcinoma……………………………..……….……………...17
Mixed Malignant Germ Cell Tumours…………………………………………………18
Biphasic or TriphasicTeratoma…………………………………...……………………18
Immature Teratoma…………………………………………………………………….18
Mature Teratoma…………………………………………………………..……….…..19
MonodermalTeratoma…………………………………………...……………………..20
Seminomas………………………………………………………………………….….20
Diagnosis of Germ Cell Tumours…………………………………………..………….21
Immunohistochemistry of Germ cell Tumours………………………………………..21
Tumour Makers of Germ cell Tumours…………….…………………...……………..22
Pattern of Spread and Metastasis…………………………………..………………….23
Prognosis of Germ cell Tumours……………………………….……………………..24
Malignant Transformation of Germ Cell Tumours…………………...…………….…26
CHAPTER THREE
Materials and Methods……………………………………………………..………….27
Exclusion Criteria…………………………………………….………….……………27
Limitations………………………………………………………….…………….……28
CHAPTER FOUR
Results………………………………………………………………...……………….29
viii
CHAPTER FIVE
Discussion……………………………………………………………………………....41
Conclusion……………………………………………………………………….………..44
REFERENCES………………………………………………………………..……..……45
APPENDICES.
APPENDIX I………………………………………………………..…………….…...….49
APPENDIX II………………………………………………………………..……………52
APPENDIX III………………………………………………………..……………………54
APPENDIX IV……………………………………………………………………………..55
APPENDIX V…………………………………………………...……………………….…56.
ix
LIST OF TABLES
1.Table I: Age distribution of the germ cell tumours……………………………..…Page 34.
2.Table II: Sex distribution of the germ cell tumours………………………………...Page 34.
3.Table III: Anatomical sites distribution of the germ cell tumours………………….Page 35.

x
LIST OF FIGURES
1. Figure 1: Photomicrograph of mature ovarian teratoma from a 28years old female
showing keratinized stratified squamous epithelium overlying a fibrocollagenous ovarian
stroma……………………………………………………………(H&E X100)…..Page 36.
2. Figure 2: Photomicrograph of immature ovarian teratoma from an 18 years old female
showing numerous neuroepithelial rosettes and immature cartilage embedded in a
fibrocollageneous ovarian stroma……………………………. (H&E X100)….…Page 37.
3. Figure 3: Photomicrograph of an ovarian dysgerminoma from a 15 years old female
showing uniform cells with pale cytoplasm with fairly uniform nuclei separated by
fibrous septae infilterated by lymphocytes. (H&E X100)….………………...…...Page 38.
4. Figure 4: A.Photomicrograph of a testicular classical seminoma from a 22 years old male
showing uniform cells separated by thin fibrous bands. (H&E
X100)………...………………………………………………………………….....Page 39.
B. Immunohistochemical stain of figure 4A showing strong membraneous
staining of tumour cells. (C-Kit X 400)……………………………………………...….39.
5. Figure 5: A:Photomicrograph of yolk sac tumour from a sacrococcygeal region of a 3
years old female showing loose meshwork of communicating spaces lined by primitive
tumor cells. (H&E X100)…………………………………………………….……Page 40.
B: Immunohistochemical stain of figure 5A showing strong cytoplasmic
staining of tumour cells and luminal secretions. ( α-fetoprotein.X400)…………...……40.
xi
ABBREVIATIONS AND THEIR MEANINGS
1. DNA — Deoxy- Ribonucleic Acid.
2. FISH — Fluorescent in situ hybridization.
3. PLAP — Placental-Like Alkaline Phosphatase.
4. CEA — Carcinoembryonic antigen.
5. αFP — Alpha Fetoprotein.
6. hCG — Human Chorionic Gonadotrophin.
7. hpL — Human placental lactogen.
8. CA — Carbohydrate Antigen.
9. SPSS — Statistical Program for Social Sciences.
10. H&E __ Haematoxylin and Eosin.
11. ABUTH — Ahmadu Bello University Teaching Hospital.
12. WHO — World Health Organisation.
13. WSP — World Standard Population.
14. CGH — Comparative Genomic Hybridization
xii
ABSTRACT
Background: Germ cell tumours are uncommon neoplasms that generally arise in the gonads,
although several cases have being reported in the extragonadal sites. This study describes the
histopathological features of cases seen over a ten year period in a tertiary institution in Nigeria.
Aim and Objectives: The aim of this study was to determine the histopathologic pattern of germ
cell tumours as seen at Ahmadu Bello University Teaching Hospital Zaria, Nigeria. The
objectives of this study are: to determine the prevalence, age and sex distribution and
anatomical sites distribution of germ cell tumours.
Materials and Methods: This is a retrospective study of cases of Germ Cell Tumours diagnosed
histologically at the Department of Pathology, Ahmadu Bello University Teaching Hospital
(ABUTH) Zaria between January 2004-December 2013. The data was analyzed with respect to
age, sex, anatomical sites and histopathological pattern. The Haematoxylin and Eosin stained
slides were reviewed and where necessary, the paraffin blocks were recut and stained. The 2004
World Health Organization (WHO) Histopathological Classification of germ cell tumours was
used in this study for testicular and ovarian germ cell tumours.
Results: Germ Cell Tumours comprised of 160 cases which constituted 0.59% of all surgical
specimens seen within the study period. There were 18 (11.2%) males and 142 (88.8%) females
giving a male to female ratio of 1:7.9. The age range was 5 days to 79 years. Gonadal germ cell
tumours constituted 131 (81.9%) and extragonadal germ cell tumours 29 (18.1%) cases. Benign
neoplasms accounted for 132 (82.5%) while malignant neoplasms accounted for 28 (17.5%)
cases. Ovarian germ cell tumours accounted for 125 (78.1%) and testicular germ cell tumours 6
(3.8%) cases. One hundred and forty nine (93.1%) cases were teratomas, 6 (3.8%) were
xiii
seminomas, 4 (2.5%) were dysgerminomas and 1 (0.6%) was yolk sac tumour. The common
sites were the ovary (78.1%), sacrococcygeal region (11.3%) and neck (5.0%).
Conclusion: This study shows that germ cell tumours are infrequent in our environment and
affect all age groups. They are predominantly seen in females and the most common type is
teratoma. The most common sites are the ovary and sacrococcygeal region for the gonadal and
extragonal germ cell tumours respectively.
Keywords: Germ cell tumours, Extragonadal, Pathology, Zaria.
1
CHAPTER ONE
INTRODUCTION
The term germ cell tumours refers to a heterogenous group of neoplasms that originate from cells
belonging to the germ cell lineage.1 They can be divided into gonadal and extragonadal types.2
Their site of distribution has been explained by the route of migration of primordial germ cells
from the yolk sac to the genital ridge.1Although the gonad being the final destination of germ
cells is the most frequent anatomical location of germ cell tumours, they often display an axial
distribution pattern, such as brain, head and neck, mediastinum, retroperitoneum, vagina,
sacrococcygeal region and occasionally in other organs not in the midline of the body.2
The clinical behavior of germ cell tumours depends upon the age and sex of the patient, and the
anatomical localization and histological composition of the tumour. The benign ones known as
mature teratoma are found mainly in the ovary (dermoid cyst) and in extragonadal sites such as
head and neck and the sacrococcygeal region.1 The malignant germ cell tumours predominantly
found in males, are mainly located in the adult testis and occasionally in the anterior
mediastinum and hypothalamus-pineal gland region.1 These tumours may contain the neoplastic
counterparts of early germ cells known as seminomas in the testis and the anterior mediastinum,
germinoma in the midline of the brain and dysgerminoma in the ovary .1
Germ cell tumours are uncommon conditions as only about 2.4 children in one million will
develop one of these tumours in a given year.3 The malignant germ cell tumours account for
about 4% of all cancers in children and adolescents under the age of 20 years. 3
The cause of germ cell tumours is not completely understood. A number of inherited defects
have been associated with an increased risk of developing germ cell tumours including central
2
nervous system and genitourinary tract malformations as well as major malformations of the
lower spine.4 Specifically, males with cryptorchidism have an increased risk to develop testicular
germ cell tumours.5,6 So also patients with a past or current testicular germ cell tumour are at
definite increase risk for a contralateral testicular germ cell tumour.5
Germ cell tumours account for approximately 30% of primary ovarian tumours. Over ninety five
percent of which are mature cystic teratomas, while the remaining germ cell tumours are
malignant and represent approximately 3% of all ovarian cancers in Western countries.7
Malignant germ cell tumours are the most common ovarian cancer among children and
adolescent females. Approximately 60% of ovarian tumours occurring in women under the age
of 21 are of germ cell type, and up to one-third of them may be malignant.8
The incidence of testicular germ cell tumours shows a remarkable geographical variation. The
highest levels of incidence, around 8-10 per 100,000 world standard population (WSP) are found
in Denmark, Switzerland, Norway, Hungary and Germany. In populations in Africa, the
Caribbean and Asia the level of incidence is typically less than 2 per 100,000 WSP. 9 ,10,11
In Nigeria, Akang et al12 in a study found that teratomas accounted for 3.4 cases per 1000
surgical biopsies received in the Pathology Department of University College Hospital Ibadan.
The commonest site of teratomas was in the ovaries which accounted for 83.2% of the cases,
followed by the sacrococcygeal region which accounted for 6.3%. Other sites of occurrence
included the neck, testes, mediastinum, abdominal cavity and buccal cavity in descending order
of frequency.12
This study is a retrospective histopathological review of germ cell tumours seen over a ten year
period (2004 - 2013) at the Ahmadu Bello University Teaching Hospital (ABUTH), Shika, Zaria.
3
RATIONALE/ JUSTIFICATION FOR THE STUDY
Malignant germ cell tumours account for about 4% of all cancers and commonly affect children
and adolescents though any age group can be involved.3 In Zaria where this study has been
carried out, there are limited number of studies done on germ cell tumors.13,14 Thus this study
was the first; that studied both gonadal and extragonadal germ cell tumours in Zaria. The study
documents their histopathologic pattern and frequency distribution in Zaria and serves as a base
line for future studies.
AIM AND OBJECTIVES:
The aim of this study was to do a histopathological review of germ cell tumours as seen in
Ahmadu Bello University Teaching Hospital Zaria between 2004 – 2013.
The objectives are:
1. To determine the prevalence of germ cell tumours.
2. To determine the age and sex distribution of germ cell tumours.
3. To determine the anatomical sites of germ cell tumours.
4. To determine the histopathologic pattern of germ cell tumours.

4
CHAPTER TWO
LITERATURE REVIEW
EPIDEMIOLOGY OF GERM CELL TUMOURS
Germ cell tumours in general are uncommon, but their incidence varies depending on the site of
presentation. Germ cell tumours of the ovary account for 20-30% of primary ovarian tumours.8,15
Most of them are seen in children and young adults.16,17 Approximately 95% of these tumours
are benign cystic teratomas.8,15 The remaining germ cell tumours are malignant and represent
approximately 3% of all ovarian cancers in Western countries, and have been reported to
represent up to 20% of ovarian tumours in Japanese women.18 Malignant germ cell tumours are
the most common ovarian cancer among children and adolescent females.19,20,21,22
Approximately 60% of ovarian tumours occurring in women under the age of 21 are of germ cell
type, and up to one-third of them may be malignant.8
In Asia, a study conducted by Jha23 in Nepal of one hundred and sixty one ovarian tumours
found that 83.9% (135 cases) were benign and 16.1% (26 cases) were malignant. Surface
epithelial tumours were the most common 52.2% followed by germ cell tumours 42.2%; and
mature cystic teratoma was the commonest benign ovarian tumour (48.2%). Germ cell tumours
were seen more commonly in patients within the first two decades of life.23 Thanikasalam24 from
Kuala Lumpur, Malaysia in a study of pattern of ovarian tumours among Malaysian women,
reviewed a total of 280 cases out of which 193 were benign and 81 were malignant and 6 cases
were border line malignancy. Teratomas were the commonest benign tumours.24 In addition,
from this study mature cystic teratomas tend to predominate over the other germ cell tumours

5
and are commonly seen in younger age groups. These findings are similar to those obtained in
Western countries.8,15
Lancaster25 from South Africa, conducted a study of 512 cases of ovarian tumours; which
showed that germ cell tumours constituted 47.8% of all cases; 67% (341 cases) were benign and
33% (171 cases) were malignant.25
From Nigeria, studies conducted by Junaid26 in Ibadan, south western Nigeria, in 169 patients
less than 20 years of age showed that the germ cell tumours is the second most common ovarian
neoplasm and accounted for 30.2% (51 cases) of 169 cases.26 Also, Onyiaorah et al27 conducted
a study in Lagos state between 1991 to 2000 showed that germ cell tumours of ovary accounted
for 52.7% (107 cases) out of 203 specimens of true ovarian neoplasms, and mature teratoma was
the commonest benign tumour accounting for 60.1% (98 cases) of benign ovarian tumours,
showing a wide age of occurrence, with peak age between 20 and 29 years. Germ cell tumours
were the commonest ovarian neoplasm followed by surface epithelial tumours.27
Nggada28 in Maiduguri, North Eastern Nigeria studied 66 germ cell tumours seen from 1990 to
2001 which revealed that 87.9% (58 cases) were benign and 12.1% (8 cases) were malignant,
with ovary being the commonest organ involved. There was broad peak age of presentation from
2nd to 4th decade of life which accounted for 69.7% of all cases.28
Mohammed et al19 in Zaria, North Western Nigeria, studied ovarian tumours in children below
15 years of age between January, 1981 and December,2005. The study showed that germ cell
tumours accounted for 58% of neoplastic enlargement of the ovary with mature cystic teratoma
being the most common.19 From these studies done in Nigeria, it was showed that the
percentages of ovarian germ cell tumours were a little bit higher than those obtained in Western
6
countries ( i.e. 52.7% and 58% from Lagos27and Zaria19 respectively as compared to 20-30% in
western literature.8,15) Mature cystic teratoma is also found to be the commonest benign ovarian
germ cell tumour in Nigeria and Western countries where it accounted for 60%27 and 95%15
respectively. However, the value is lower in Asia, with 48.2% in Nepal.23
Testicular germ cell tumours comprise 95-98% of all testicular malignancies and are the most
common type of malignancy in American men aged 15-34 years.29,30,31 They occur mainly in the
third and fourth decades of life. To date, the incidence of testicular germ cell tumours is between
6 and 11 per 100,000, and is increasing.1 The incidence of testicular cancer rises dramatically
around puberty, peaks between 25 and 35 years of age, and slowly declines to a relative nadir
near the age of 60 years.5 There is circumstantial epidemiological evidence that the steep
increase in new cases is associated with the western life style, characterized by high caloric diet
and lack of physical exercise.11
The incidence of testicular germ cell tumours is over five- fold greater among men in the United
States of European ancestry compared with men in the United States of African ancestry, and it
has been increasing among European Americans since 1940.29 A similar increase in incidence
has been reported among other populations of European ancestry in Australia, New Zealand and
Canada.29 Among these populations, it has been reported consistently that risk is affected more
significantly by birth cohort rather than by calendar-period.29
A study done by Opotet al9 from Nairobi showed that out of 162,768 surgical admissions over a
15 year period (1983-1997) only 39 cases of testicular cancer were recorded representing only
0.02%. The age range was 3-70 years with a mean of 34.8 years and a peak incidence in the 30-
44 year age group. Histologically, 89.8% of the cancers were of germ cell origin. Seminoma
7
accounted for 67.35% (33 patients), teratoma for 12.24% (6 patients), embryonal carcinoma for
8.16% (4 patients), rhabdomyosarcoma of testicular adnexae for 6.12% (3 patients) and
malignant germ cell tumour, orchioblastoma and dysgerminoma accounted for 2.04% (1 patient)
each.9
Another, study conducted in Ilorin, Nigeria by Izegbu et al32of 8 cases of testicular malignancies
seen within span of thirteen years (1990-2003) out of 5,870 male specimen, showed that
testicular tumours account for 0.14% of the male biopsy. The germ cell tumours constituted
50% of all the malignant testicular neoplasms and the mean age of presentation was 18.25±
6.45.32
Furthermore Salako et al33 from Ife Ijesha, South Western Nigeria, conducted a study of
testicular and paratesticular tumours between 1989 and 2005 (17 years) got 26 cases of testicular
and paratesticular tumours with an average incidence of 1.5 cases per year, with an incidence of
0.55 per 100,000 population. Seminomas comprised 50% of the germ cell tumours and 15.4% of
all testicular tumours in this series.33 The median age of presentation was 20 years with a mean
of 26.8± 3.6 years and more than 65% of cases occurred in the 2nd and 3rd decades of life.33
Obafunwa et al from Lagos, South Western Nigeria, also conducted a study of testicular and
paratesticular tumours over a ten year period, found only ten cases of testicular tumours with a
rate of 1 case per year. Germ cell tumours constitute 70% about half of these are seminomas
whilst paratesticular tumours account for the remaining 30%.34 From the above studies we can
see that the incidence of testicular germ cell tumours are higher in Western countries with
incidence of 6 to 11 per 100,000 1 compared to that seen in African populace of about 0.55 per
100,000 in Ife Ijesha Nigeria.33 The age at presentation of testicular germ cell tumours is found
8
to be a decade lower in Nigerian studies than the data obtained from the Western literature, as
most of the patients fall within 2nd to 3rd decade of life32,33 compared to 3rd to 4th decade of life
seen in Western countries.1 However, studies from Nairobi9 showed their own age at
presentation to be within 3rd to 4th decade of life similar to that obtains in Western countries.1 It
has also been shown that testicular germ cell tumours are the most common testicular
malignancies in young adult both in Western and African countries where it was found to be up
to 89.8% in Nairobi9 similar to 95-98% seen in Western countries, like Denmark.29,30,31 In
Nigerian studies the percentage is lower being about 50% in Ilorin32 and Ife Ijesha.33
EXTRAGONADAL GERM CELL TUMOURS
Extragonadal germ cell tumours are rare and often display an axial distribution pattern such as
brain, neck, mediastinum, retroperitoneum, vagina and sacrococcygeal region.2,35-
41Extragonadalteratoma is the most common congenital tumour comprising 37% to 52% of
congenital neoplasms and having a yearly incidence of approximately 1 in 40,000 live
births.14Sacrococcygeal teratoma although generally a rare condition, is said to be the most
common tumour in the newborn period, with a reported incidence of approximately one in
35,000- 40,000 live births.36-38,42,43 It is rare in adult, with less than a hundred cases of
saccrococcygeal teratoma in adult been documented.42
David et al44 from Boston, Massachusetts studied 254 teratomas from 245 patients from 1928 to
1982 (54 years) which showed that the tumours arose in the following anatomical sites:
sacrococcygeal 102 patients (40%), ovary 94 patients (37%), head and neck 14 patients (5.5%),
retroperitoneum 12 patients (5%), mediastinum 11patients (4%), brain/spinal cord 9
patients(3.5%), testis 8 patients (3%), liver 2 patients (1%), abdominal wall, paraumblical 1 and
9
scapular (back) 1.44 In Ibadan Akang et al12 from their study of teratoma over 26 years period
1960-1985 of 411 patients showed that the commonest site of teratomas was in the ovaries
which accounted for 83.2% (342) of the cases, followed by the sacrococcygeal region which
accounted for 6.3% (26 cases).12Edegbe et al45 also from Ibadan studied 39 cases of paediatric
germ cell tumours over a 20 year period (1988-2007) and found out that the most common site of
these tumours are the ovary (33.3%), sacrococcygeal region (20.5%) and neck (10.3%)
respectively.45
Mabogunje et al13 from Zaria studied 132 teratomas over a six year period (1972 -1977) and
found that twenty seven of these cases comprising most of extragonadal tumours were seen in
infants and children.13 Mohammed et al14 also from Zaria conducted a study of extragonadal
teratoma between January 2001 to December 2010 a total number of 39 cases were seen in the
10 year period. The most frequent anatomical sites were the sacrococcygeal region 43.6% (17
patients) and cervical region 12.8% (5 patients).14
The above mentioned studies of teratomas have shown that the most common site of
extragonadal teratoma is the sacrococcygeal region.14,36,44,45
AETIOLOGY/RISK FACTORS FOR DEVELOPMENT OF GERM CELL TUMOURS
The aetiology of ovarian germ cell tumours is unknown,8 however research for the causes of
testicular germ cell tumours has been guided by the hypothesis that the disease process starts in
fetal life and consists of the abnormal differentiation of the fetal population of primordial germ
cells.11There are several strong indications that testicular germ cell tumour is associated with
abnormal conditions in fetal life.5
10
1. Associations with congenital malformations of the male genitalia: Cryptorchidism is
consistently associated with an increased risk of testicular germ cell tumours.46 The
incidence is about 3-5 fold increased in men with a history of cryptorchidism.5In those with
unilateral cryptorchidism, both the undescended testicle and the normal, contralateral testicle
have increased risk of testicular cancer.9 The incidence of testicular cancer is possibly
increased in men with hypospadias and in men with inguinal hernia, but the evidence is less
strong than for cryptorchidism. Atrophy in maldescent and the normal, contralateral testicle
has an increased risk of testicular cancer.11
2. Prenatal risk factors: Case control studies have shown consistent associations of testicular
cancer with low birth weight and with being born small for gestational age, indicating a
possible role of intrauterine growth retardation.10
3. Bilateral testicular germ cell tumours: Patients with a past or current testicular germ cell
tumour are at definite increased risk for a contralateral testicular germ cell tumour.5In two
large series the frequency of simultaneous or subsequent testicular cancer was 1.9% and
2.7% respectively. Such frequencies correspond to an elevated risk calculated to be more
than 20 times higher than that of the general population. This risk is even greater if the
second testis is cryptorchid or atrophic.5
4. Familial testicular cancer: Familial testicular germ cell tumours of adolescents and adults
account for 1.5-2% of all germ cell tumours of adults. There is 6-10-fold increase in risk for
the development of a testicular germ cell tumour for the first-degree male relative of an
affected individual.46
5. Inter sex syndromes: There are several intersex syndromes associated with an increased risk
for a germ cell tumour; certain forms of gonadal dysgenesis, true hermaphroditism, and male

11
pseudohermaphroditism due to androgen insensitivity syndrome.5 Persons with 46,XY or
45,X/46XY gonadal dysgenesis are at very high risk of gonadal germ cell tumour. The
absolute risk is reported to be as high as 10-50%.11
6. Male infertility: Subfertile and infertile men are at increased risk of developing testicular
cancer. It has been hypothesized that common causal factors may exist which operate
prenatally and lead to both infertility and testicular neoplasia.10
7. Exposures in adulthood: There are no strong and consistent risk factors for testicular cancer
in adulthood. Possible aetiological clues, however, include a low level of physical activity
and high socioeconomic class. There is no consistent evidence linking testicular cancer to
particular occupational exposures.11
Trauma, inutero exposure to oestrogen, and non-specific mumps associated testicular atrophy
have also been implicated as risk factors for testicular germ cell tumours but there is very little
data to support this.9,10.
HISTIOGENESIS OF GERM CELL TUMOURS
The observations of Skakkebaek and the evolution of the concept of intratubular germ cell
neoplasia indicate that most, but not all germ cell tumours of the testis evolve from a common
neoplastic precursor lesion, intratubular germ cell neoplasia of the unclassified type.1,5 In past
schemes, two divergent pathways were theorized, one giving rise to seminoma and the second to
embryonal carcinoma. While seminoma is considered incapable of further differentiation,
embryonal carcinoma is capable of giving rise to other forms of germ cell tumours such as yolk
sac tumour, teratoma and choriocarcinoma.5 While Ovarian germ cell tumours are believed to be
12
from the primordial germ cells that migrate into the gonadal ridge at 6 weeks of embryonic life, a
small proportion may also arise from non-germ sterm cells present in the adult female genital
tract.8
CYTOGENETICS AND MOLECULAR PATHOLOGY OF GERM CELL TUMOURS
All testicular germ cell tumours, including their precursor, intratubular germ cell neoplasia
unclassified are aneuploid. Seminoma and intratubular germ cell neoplasia unclassified cells are
hypertripliod, while the tumour cells of non-seminomatous cancer irrespective of their
histological type are hypotriploid.1 This suggests that polyploidization is the initial event, leading
to a tetraploid intratubular germ cell neoplasia unclassified, followed by net loss of chromosomal
material.11 Aneuploidy of testicular germ cell tumours has been related to the presence of
centrosome amplification. Karyotyping, FISH and CGH also showed strikingly similar patterns
of over- and under-representation of (parts of) chromosomes in seminomas and non-seminomas.1
Parts of chromosomes 4,5,11,13,18 and Y are underrepresented, while (parts of) chromosomes
7,8,12,21 and X are over represented.47 Seminomas have significantly more copies of the
chromosomes 7,15,17,19 and 22 explaining their higher DNA content.11
The only consistent structural aberration in invasive testicular germ cell tumours is gain of 12p-
sequences, most often as isochromosome of the short arm of chromosome 12 {i(12p)}47 This
anomaly was first decribed by Atkin and Baker in 1982 and about 50% of the seminoma and
80% of the non seminomas show atleast one i(12p).1 Molecular analysis showed that the i(12p) is
of uniparental origin indicating that its mechanism is doubling of the p-arm of one chromosome,
and loss of the q-arm, instead of non sister chromatin exchange.11 Interestingly, i(12p) is not
13
restricted to the seminomas and non-seminomas of the testis, but is also detected in these types
of tumours in the ovary, anterior mediastinum and midline of the brain.11
Several candidate genes have been proposed to explain the gain of 12p in testicular germ cell
tumours. These included KRAS2, which is rarely mutated and sometimes overexpressed in
testicular germ cell tumours and cyclin D2.1,46 The latter might be involved via a deregulated
G1-S check point.46 A more focused approach to the identification of candidate genes was
initiated by the finding of a metastatic seminoma with a high level of amplification of a restricted
region of 12p, cytogenetically identified as 12p11.2-p12.1. Subsequently, primary testicular
germ cell tumours have been found with such amplification. The 12p-amplification occurs in
about 8-10% of primary seminomas, particularly in those lacking an i(12p) and it is much rarer
in non-seminomas. This suggests the existence of two pathways leading to overrepresentation of
certain genes on 12p, either via isochromosome formation, or an alternative mechanism, possibly
followed by high level amplification. The seminomas with amplification have a reduced
sensitivity to apoptosis for which DAD-R is a promising candidate. Probably more genes on 12p,
in particular in the amplification, help the tumour cells to overcome apoptosis.11
Immunohistochemistry demonstrates a high level of wild type TP53 protein in testicular germ
cell tumours. However, inactivating mutations are hardly found. This led to the view that high
levels of wild type TP53 might explain the exquisite chemosensitivity of testicular germ cell
tumours.47However, it has been shown that this is an oversimplification and that inactivation of
TP53 explains only a minority of treatment resistant testicular germ cell tumours. In fact, the
overall sensitivity of testicular germ cell tumours might be related to their embryonic origin, in
contrast to the majority of solid cancers.11

14
CLASSIFICATION OF GERM CELL TUMOURS
Germ cell tumours can be classified into gonadal and extragonadal germ cell tumours. Gonadal
germ cell tumours can be ovarian or testicular. For ovarian germ cell tumours comprehensive
classification was formulated by the World Health Organization (WHO) and the International
Society of Gynaecological Pathologist (ISGYP).7 While for the testicular germ cell tumours
there is a lack of uniformity in the classification, with two major systems currently in widespread
use, one formulated by the WHO and the other proposed by the British Testicular Tumour Panel
(BTTP).5 The classification of the germ cell tumours is essentially based on morphology. Two
main systems of classification exist: WHO and ISGYP schemes and WHO and BTTP schemes
for ovarian and testicular germ cell tumours respectively (Appendix I and II respectively)5,7
REVIEW OF SOME MORPHOLOGICAL TYPES OF GERM CELL TUMOURS
1. DYSGERMINOMA
Dysgerminoma is a tumour composed of a monotonous proliferation of primitive germ cells
associated with connective tissue septa containing varying amount of lymphocytes and
macrophages. This tumour is identical to testicular seminoma.8 It constitutes less than 1% of all
ovarian tumours, for 5% to 10% of ovarian cancers in patients in the first two decades and for
20% - 30% of ovarian cancers encountered during pregnancy.15 Approximately, 80% of
dysgerminomas occur in patients in the second and third decades.7 Most of the patients present
with signs and symptoms related to an abdominal mass.7Dysgerminoma is somewhat more
common on the right side and is bilateral in 15% of cases.15

15
Grossly, dysgerminomas are typically well encapsulated, with a smooth, often bosselated
surface. The cut surface is solid and gray; but foci of haemorrhage and necrosis can occur.
Microscopically the tumour is composed of uniform cells resembling primordial germ cell in
diffuse, trabecular and cord like patterns.15 The composing cells are polygonal having abundant
pale cytoplasm and fairly uniform nuclei. The stroma consists of thin to broad fibrous bands that
almost invariably contain mature T- lymphocytes and macrophages,8 The mitotic rate is variable
and some tumours show anisokaryosis.8
2. YOLK SAC TUMOURS
Yolk sac tumours are also referred to as endodermal sinus tumours. They are morphologically
heterogenous, primitive teratoid neoplasms differentiating into multiple endodermal structures,
ranging from the primitive gut to its derivatives of extraembryonal and embryonal somatic type,
e.g. intestine and liver.8 Yolk sac tumours account for approximately 20% of primitive germ cell
tumours, and are almost as common as dysgerminomas in the first two decades.7 These tumors
are most common in patients in the second and third decades with median age between 16 and 19
years.15 Although they are rare over the age of 40 years, exceptional examples have been
reported in elderly women.7
Grossly, the tumours are usually well encapsulated with an average diameter of 15cm. The
section of the tumour is soft and grey-yellow with frequent areas of necrosis, haemorrhage and
liquefaction.8 Yolk sac tumours exhibit a wide variety of microscopic patterns, but most tumours
have at least focally, a reticular pattern. It is characterized by a loose meshwork of
communicating spaces lined by primitive tumour cells with cytoplasm that is typically clear,
16
containing glycogen and occasional lipid. The hyperchromatic, irregular, large nuclei have
prominent nucleoli, mitotic figures are usually numerous. Reticular areas frequently merge with
microcystic or macrocystic areas. The presence of Schiller-Duval bodies is a characteristic
feature of yolk sac tumours.7Less common histologic variants of yolk sac tumours include
polyvesicularvitelline stumour, solid yolk sac tumours, parietal yolk sac tumour, glandular types
of yolk sac tumours and hepatoid yolk sac tumours.8
3. EMBRYONAL CARCINOMA
This rare germ cell tumour is characterized by large primitive cells resembling those of the
embryonic germ disc and growing in solid, papillary and glandular patterns.8 This tumour
account for only about 3% of primitive ovarian germ cell tumours; they are one fifth to one tenth
as common as yolk sac tumours.7 The patients range in age from 4 to 28 years with a median age
of 15 years.15
Grossly, the tumours are typically large (median diameter 17cm) with smooth external surfaces
in occasional cases, preoperative rupture occurs. Their cut surfaces are predominantly solid and
variegated, with extensive areas of necrosis and haemorrhage. Microscopically, this tumour has a
similar appearance to the embryonal carcinoma of the adult testis. As such, it is composed of
solid sheets and nests of large primitive cells, occasionally forming papillae and abortive
glandular structures.15These primitive cells have amphophilic or sometimes clear cytoplasm and
well-defined cell membranes; with nuclei that are round and vesicular with coarse, irregular
membrane and one or more prominent nucleoli. Mitotic figures including atypical forms are
usually numerous.7
17
4. POLYEMBRYOMA
This tumour is characterized by an exclusive or preponderant content of embryoid bodies, which
resemble normal early embryos in various stages of development. Ovarian polyembryomas are
exceedingly rare, with less than 10 cases reported during the last four decades. The patients are
typically children or young women who presented with manifestations related to the presence of
a pelvic mass.7
On gross examination, polyembryomas are usually bulky tumours with sectioned surfaces that
are typically spongy or microcystic, soft, reddish brown and focally haemorrhagic. Microscopic
examination reveals myriads of small structures resembling perfect or imperfect early embryos
containing germ discs, amniotic cavities, yolk sacs, chorionic elements including
syncytiotrophoblastic giant cells and extraembryonic mesenchyme scattered in a fibrous or
oedematous stoma.7
5. NON-GESTATIONAL CHORIOCARCINOMA
This tumour is composed of an intimate admixture of either cytotrophoblast, intermediate
trophoblast, or both and syncytiotrophoblast.8 Most choriocarcinomas involving the ovary
represent metastases from uterine tumours.15 Pure nongestational choriocarcinomas account for
less than 1% of primitive germ cell tumours of the ovary.7 Ovarian choriocarcinomas typically
occur in children and young adults.7 On gross examination, the pure choriocarcinoma is typically
solid, haemorrhagic and friable. Bilateral involvement is rare. Microscopically, they show the
typical admixture of syncytial and cytotrophoblastic elements in a necrotic and haemorrhagic
background.15
18
6. MIXED MALIGNANT GERM CELL TUMOURS
These tumours are composed of at least two different germ cell elements of which at least one is
primitive.8 They account for 8 to 10% of malignant primitive germ cell tumours of the
ovary.7Histologically, the most common combination of neoplastic germ cell elements found in
ovarian mixed germ cell tumours is dysgerminoma and yolk sac tumours. Additional neoplastic
germ cell elements, including immature or mature teratoma, embryonal carcinoma,
polyembryoma and/or choriocarcinoma may also be present. All components of a mixed germ
cell tumours and their approximate proportions should be mentioned in the diagnosis.8
7. BIPHASIC OR TRIPHASIC TERATOMAS
These are tumours composed of derivatives of two or three primary germ layers (ectoderm,
mesoderm, endoderm).7,8
(a) Immature teratoma: This is a malignant ovarian teratoma seen usually in children and
adolescents and composed of a mixture of embryonal and adult tissues derived from three
germ layers, regardless of its gross appearance.15 It represents 3% of teratomas, 1% of all
ovarian cancers and 20% of malignant ovarian germ cell tumours and is found either in
pure form or as a component of a mixed germ cell tumour.7
Macroscopically, immature teratoma is typically unilateral, large variegated,
predominantly solid, fleshy, and grey tan and may be cystic with haemorrhage and
necrosis.8 Microscopically it is composed of variable amounts of immature embryonal
type tissues, mostly in the form of neuroectodermal rosettes and tubules, admixed with
mature tissues. Immature mesenchyme in the form of loose, myxoidstroma with focal

19
differentiation into immature cartilage, fat, osteiod and rhabdomyoblast is often present
as well. Based on the quantity of the immature neuroepithelial component, primary and
metastatic ovarian immature teratomas are separatedly graded from 1 to 3. More recently
the possibility of using a two-tiered (low grade and high grade) grading system was
suggested.8
(b) Mature Teratoma: This tumour is solid or predominantly cystic and is composed
exclusively of mature adult tissues.7 A cyst lined by mature tissue resembling the
epidermis with its appendages is clinically designated as” dermoid cyst”. Homunculus or
Fetiformteratoma is a rare type of mature, solid teratoma containing highly organized
structures resembling a malformed fetus.8Although most mature cystic teratomas occur
during the reproductive years, they have a wide age distribution, from 2-80 years, and 5%
occur in postmenopausal women. Mature solid teratoma occurs mainly in the first two
decades of life. Mature cystic teratoma accounts for 20-44% of all ovarian tumours and
up to 58% of the benign tumours.8
Macroscopically, dermoid cyst is an ovoid, occasionally bilateral (8-15% of cases), cystic
mass of 0.5-40cm (average 15cm) with a smooth external surface and is filled with
sebaceous material and hair. A module composed of fat tissue with teeth or bone
protrudes into the cyst and is termed a Rokitansky protuberance. Mature solid teratoma
is a large, solid mass with multiple cysts of varying sizes, composed of keratin, sebum
and hairs.15 Microscopically, mature teratomas are composed of adult type tissue derived
from two or three embryonic layers.15
20
8. MONODERMAL TERATOMAS
They are teratomas composed exclusively or predominantly of a single type of tissue derived
from one embryonic layer (ectoderm or endoderm) and adult-type tumours derived from a
dermoid cyst. Example of this type of teratoma is the struma ovarii.8
Struma ovarii the most common type of monodermal teratoma, accounts for 2.7% of all ovarian
teratomas.8Thetumour is unilateral and varies from 0.5-10cm in diameter. Microscopically, is
composed of normal or hyperplastic thyroid- type tissue with patterns seen in thyroid adenoma
such as microfollicular, macrofollicular, trabecular and solid.7
9. SEMINOMAS
Seminomas make up 30% to 40% of all testicular tumours. They are divided into two major
categories: classic and spermatocytic, the former including several variants.48
Classic seminoma, which comprises approximately 93% of the cases of seminoma, has a
characteristic gross appearance. It is usually of moderate size, solid, homogeneous, and light
yellow, and it may contain sharply circumscribed zones of necrosis. Microscopically, the
individual tumour cells are uniform, with abundant clear cytoplasm, sharply outlined cell
membranes, a large centrally located nucleus with prominent amphophilic nucleolus. The tumour
cells are typically arranged in nests outlined by fibrous bands; in 80% of the cases, these bands
are infiltrated by lymphocytes, plasma cells and histiocytes. A granulomatous reaction
containing Langhans-type multinucleated giant cells and epithelioid cells may also be present.5

21
Spermatocytic seminoma, this comprises 4% to7% of all seminomas and occur in older age
group. Grossly, it has a soft, gelatinous appearance. Microscopically, it is composed of cells with
perfectly round nuclei and prominent variation in size. Bizarre giant forms are common, together
with small cells with a lymphocytic-like appearance. Mitoses may be numerous. The tumour
lacks cytoplasmic glycogen and is rarely associated with a lymphocytic infilterate or
granulomatous reaction, in contrast to typical seminoma.5,48
DIAGNOSIS OF GERM CELL TUMOURS
The diagnosis of germ cell tumours is based on morphological appearances following routine
paraffin embedded tissue sections and staining with haematoxylin and eosin (H&E). Other
ancillary investigative measures that can be used include:
IMMUNOHISTOCHEMISTRY: Dysgerminomas are consistently reactive for placental-like
alkaline phosphatase (PLAP) and CD117, variably for keratin, and sometimes for desmin, glial
fibrilary acidic protein but not for CD30.15 A more recent and promising marker is OCT4, which
stains the germ cell component of gonadoblstoma.15 SALL4, another germ cell tumour marker,
is also positive in dysgerminoma.15 C-kit gene product (CD117) is also present in seminoma,
further supporting the similarity to its ovarian counterpart.5 Seminomas too show positivity for
vimentin, and placental-like alkaline phosphatase.48 Alpha-feto protein (α-FP) is the
characteristic marker of the epithelial component of yolk sac tumours. The cytoplasm of the
tumour cells is almost always immunoreactive for AFP, alpha-1-antitrypsin and cytokeratin, but
not epithelial membrane antigen.49The usual positivity for cytokeratins may differentiate solid
yolk sac tumour from dysgerminoma.8 Embryonal carcinoma shows immunoreactivity for pan
22
keratin, CD30, OCT4 and SALL4 and variable focal staining for alpha fetoprotein.7,15 The
syncytiotrophoblastic cells of choriocarcinoma are typically immunoreactive for cytokeratin,
human chorionic gonadotrophin (hCG), human placental lactogen (hpL) and pregnancy-specific
beta-1 glycoprotein (SP1), while the cytotrophoblast is typically immunoreactive for cytokeratin,
and the intermediate trophoblast is usually immunoreactive for cytokeratin, hpL and SP1.15
Immunoreactivity for placental-like alkaline phosphatase, epithelial membrane antigen, neuron-
specific enolase, alpha-1-antitrypsin, and carcinoembryonic antigen may be present as well.7 In
teratomas, the neuroectodermal tissues are variably immunoreactive for one or more of a variety
of neural markers, including glial fibrillary acidic protein, neuron-specific enolase, S-100
protein, neurofilament protein, synaptophysin, nerve growth factor receptor, glial filament
protein, myelin basic protein and polysialic acid.7 Alpha-fetoprotein immunoreactivity in
immature teratoma is typically confined to hepatic tissue, yolk sac-like vesicles, and intestinal
type epithelium.7
TUMOUR MARKERS
Patients with yolk sac tumours have elevated serum level of alpha fetoprotein (α-FP).49Non
specific markers that may be found in the sera of patients with yolk sac tumours include CA125
and Carcinoembryonic antigen which are elevated in 100% and 10% of the patients
respectively.7 So also serum hCG and α-FP levels have been elevated in patients with embryonal
carcinoma and some patients with polyembryoma; while serum hCG levels are elevated in cases
of choriocarcinomas.15 Sixty five percent of the patients with immature teratoma have an
elevated serum level of alpha-feto protein at presentation, although the levels are only rarely as

23
high as those encountered in patients with yolk sac tumours.7 Other serum markers that may be
elevated include hCG, neuron-specific enolase, CA125, CA19-9 and carcinoembryonic antigen
CEA .7
PATTERN OF SPREAD AND METASTASES
It has been generally assumed that the first manifestation of local spread of testicular germ cell
tumours is in the tunica albuginea, but invasion of the testicular hilum is actually a much more
common event.48 Most testicular neoplasms extend into the paratesticular structures by way of
the mediastinum testis, but even this is seen uncommonly with only 10% to 15% of malignant
testicular tumours involving either the epididymis or spermatic cord.5 Extension into the rete
testis is, however, common, being seen in about 80% of seminomas in one series.7 Involvement
of scrotal skin is an unusual and late event.5
Metastases occur via either lymphatic or haematogenous routes. Seminoma tends to spread by
lymphatics, with haematogenous metastases usually occurring late in the clinical
course.5Choriocarcinoma on the other hand, has a proclivity for early dissemination through
blood borne routes, although nodal metastases also occur. The other nonseminomatous germ cell
tumours may show both lymphatic and haematogenous pattern of dissemination, with early
cases tending to have mainly lymphatic-based metastases, although recent studies suggest that
childhood yolk sac tumour is an exception, with a proclivity for haematogenous metastases.5
In terms of lymph-borne metastases, testicular tumours spread first to periaortic and iliac lymph
nodes and latter to mediastinal and left supraclavicular nodes.48 Retroperitoneal lymph node
metastases are on the side of the tumour in about 80% to 86% of cases and bilateral in about 13%
24
to 20%. The presence of contralateral metastases in the absence of ipsilateral metastases is rare.48
Blood- borne metastases occur most frequently in lungs, liver, brain and bone.5 In an autopsy
study of patients with testicular germ cell tumours, 89% had pulmonary involvement, 73% had
liver metastases, 31% had brain metastases and 30% had bone metastases.5 There is a high
incidence of brain metastases in choriocarcinoma and of bone metastases in
seminoma.5Embryonal carcinoma frequently metastasizes early, and choriocarcinoma almost
always has widespread metastases by the time the tumour is diagnosed.48 The microscopic
appearance of the metastases may differ from that of the primary tumour. Teratocarcinoma often
metastasizes as embryonal carcinoma, and the reverse also occurs.48In general, classic seminoma
metastasizes as classic seminoma, but it may also spread as embryonal carcinoma or
choriocarcinoma. Mixed germ cell tumours with focal choriocarcinoma tend to metastasizes as
pure choricarcinomas.48
PROGNOSIS
At present over 90% of patients with newly diagnosed germ cell tumours of the testis are
cured.48The prognosis varies widely according to the clinical stage and tumour type. It is
excellent for classic seminoma over 95% of the patients with disease clinically limited to the
testis (stage1) or to sub-diaphragmatic lymph nodes (stage 11) can be cured. It is even better for
spermatocytic seminoma which practically never metastasizes.48Dysgerminomas respond to
chemotherapy or radiotherapy. The clinical stage of the tumour is probably the only significant
prognostic factor.8The survival rate of pure dysgerminoma is 95%.15 The initial treatment of
unilateral dysgerminoma is oophorectomy. Until recently, radiation therapy was also
25
recommended, since dysgerminoma is an extremely radiosensitive neoplasm.15 At present,
multidrug chemotherapy is regarded as the method of choice for this tumour following its
conservative (unilateral) surgical removal.15 For yolk sac tumour because numerous patterns of
differentiation may coexist in the same neoplasm, their behavior, with some exceptions, is not
conditioned by specific tumour morphology but shows a generally favourable response to
chemotherapy.8 Although the histological appearance bears little prognostic implications, mature
or well differentiated glandular forms may have an indolent course even when treated by
surgery alone.8 While for immature teratoma both the stage and grade of the primary tumour and
that of its metastases are important predictive factors. Prior to the chemotherapy era, the overall
survival rate of patients with grade 1,2 and 3 neoplasms was 82%,63% and 30% respectively.8
The use of cisplatin-based combination chemotherapy has dramatically improved the survival
rate of patients, 90-100% of those receiving this regimen remain disease-free. The tumour grade
is a crucial feature that determine behavior and type of therapy. Patients with grade 1 tumours
that are stage 1A and those with mature (grade 0) implants do not require adjuvant
chemotherapy. Those with grade 2 or 3 tumours, including stage 1A, as well as those with
immature implants require combination chemotherapy.8 A recent report from the Paediatric
Oncology Group concluded that surgery alone is curative in children and adolescents with
immature teratoma of any grade, reserving chemotheraphy for cases with relapse.8
Patients with extragonadal nonseminomas should receive chemotherapy at diagnosis and
standard therapy would generally be considered to be four courses of BEP ( bleomycin,
etoposide, and cisplatin).50 The prognosis of retroperitoneal nonseminoma is reasonably good
and, similar to the situation with nodal metastasis from a testicular primary.50
26
MALIGNANT TRANSFORMATION OF GERM CELL TUMOURS
Germ cell tumours may develop somatic-type malignancies either within the primary tumour or
within a metastases.51 These somatic-type components should be histologically recognized and
diagnosed because they are often resistant to the chemotherapy used for the treatment of germ
cell tumours.52 The somatic malignancies arising in the germ cell tumours may be epithelial or
sarcomatous, with the sarcomatous malignancies tending to be more common.51 Malignant
transformation of germ cell tumours into somatic malignancy is uncommon and occurs in only
2.2% to 4.1% of germ cell tumours.52 Among sarcomatous malignancies, the most common is
rhabdomyosarcoma, followed by leiomyosarcoma, myxoidliposarcoma, chondrosarcoma,
angiosarcoma, glioblastoma, epithelioid haemangioendothelioma, malignant pheripheral nerve
sheath tumour, malignant triton tumour and undifferentiated sarcoma.53 Primitive
neuroectodermal tumour, meningioma, haematological malignancies and nephroblastoma also
have been reported.53 Adenocarcinoma and squamous cell carcinomas are rare but are the most
frequent epithelial malignancies arising in germ cell tumours.52

27
CHAPTER THREE
MATERIALS AND METHOD
This review was based on all histopathologically confirmed germ cell tumours (both gonadal and
extragonadal) cases obtained from specimens submitted to the Pathology Department of Ahmadu
Bello University Teaching Hospital (ABUTH) Zaria for histopathololgical examination in the
period, 1st January, 2004 to 31st December, 2013 (10 years). The hospital is a referral centre for
the North-West region of the country, serving neighbouring states which include Zamfara,
Katsina and Niger.
All cases diagnosed as germ cell tumours were extracted from the surgical pathology records.
The patient’s request cards filled by the requesting physicians and records or case folder where
necessary, together with all the relevant histology slides stained with routine Haematoxylin and
Eosin (H&E) were retrieved. Patients bio-data including age and type of specimen was extracted
from the accompanying case cards. Immunohistochemical stains such as c-kit (CD 117) for
seminoma and dysgerminoma, and alpha-fetoprotein (α-FP) for yolk sac tumour were done using
the protocol in Appendix iii and iv (Leica Novolink,R Newcastle UK). In cases of broken or
missing slides, fresh sections were made from stored tissue blocks. All the slides were reviewed
with the supervising consultants and the cases were classified using the 2004 World Health
Organisation (WHO) classification of germ cell tumours.11 Analysis of the collected data was
carried out using Statistical Program for Social Sciences (SPSS) version 20.0, and data was
presented in frequency distribution tables and figures.
EXCLUSION CRITERIA
Cases in which both slides and tissue blocks are missing were excluded from the study.
28
CONFIDENTIALITY
Ethical clearance for the study was obtained from the Ethics and Scientific Committee of the
Ahmadu Bello University Teaching Hospital,Shika- Zaria (Appendix v).
The data was accessible to the investigators only. All information was coded by numbers and no
names were recorded. All published articles arising from this research will have no information
that will reveal the identity of any patient.
LIMITATIONS
The study was hospital based and may not be representative of the total population.
29
CHAPTER FOUR
RESULTS
During the ten years period of this study the Department of Pathology Ahmad Bello University
Teaching Hospital Zaria received a total number of 27,109 specimens, out of these there were
160 germ cell tumours constituting 0.59% of all specimens. There were 18 (11.2%) males and
142 (88.8%) females giving a male to female ratio of 1:7.9. The age range was 5 days to 79
years. (Table I). Gonadal germ cell tumours constituted 131 (81.9%) cases and extragonadal
germ cell tumours 29 (18.1%) cases. Benign neoplasms accounted for 132 (82.5%) and
malignant neoplasms accounted for 28 (17.5%) cases. (Table II). Ovarian germ cell tumours
accounted for 125 (78.1%) and testicular germ cell tumours 6 (3.8%) cases. One hundred and
forty nine (93.1%) cases were teratomas, 6 (3.8%) were seminoma, 4 (2.5%) were
dysgerminoma and 1 (0.6%) was yolk sac tumour. (Table II). The commonest sites for gonadal
germ cell tumours was in the ovary 125 (78.1%) cases while for the extragonadal germ cell
tumours were sacrococcygeal region 18 (11.3%) and neck 8 (5.0%) cases. ( Table III).
AGE DISTRIBUTION
The patients’ ages ranged from 5 days to 79 years with a mean of 24.8 ± 15.7 yrs. The peak age
distribution of immature teratoma and mature teratoma were 1st and 4th decades respectively,
while for dysgerminoma and seminoma were the 2nd and 4th decades respectively. For yolk sac
tumour the peak age distribution is in the 1st decade of life. (Table I).
30
SEX DISTRIBUTION
There were 18 males and 142 females with a M:F ratio of 1:7.9. The most common histological
variant among both sexes is mature teratoma which accounted for 9 (5.6%) cases and 123
(76.9%) cases in males and females respectively. Immature teratoma was the second commonest
in both sexes with 3 and 14 cases accounting for 1.9% and 8.7% in males and females
respectively. Followed by seminoma of 6 (3.8%) cases in males only, dysgerminoma 4 (2.5%)
cases in females only and finally yolk sac tumour with 1 (0.6%) case in female only. (Table
II).
ANATOMICAL DISTRIBUTION FOR GERM CELL TUMOURS
The most common site of mature teratoma, immature teratoma and dysgerminoma were in the
ovary accounting for 112 (70%) cases, 9 (5.6%) cases and 4 (2.5%) cases respectively. The
second most common site is sacrococcygeal region in which there were 11 (6.9%) cases of
mature teratoma and 6 (3.8%) cases of immature teratoma and 1 (0.6%) case of yolk sac tumour
respectively. This followed by neck (cervical region) which has 6 (3.8%) cases of mature
teratoma and 2 (1.2%) cases of immature teratoma respectively. All the 6 (3.8%) cases of
seminoma occur in testis. Other sites are oral, sternum and retroperitoneum with 1(0.6%) case
each of mature teratoma respectively. (Table III).
TUMOUR TYPES
There are 131 (81.9%) cases of gonadal germ cell tumours and 29 (18.1%) cases of extragonadal
germ cell tumours. There are 125 (78.1%) cases of ovarian germ cell tumours and 6 (3.8%) cases

31
of testicular germ cell tumours. One hundred and thirty two cases (82.5%) were mature teratoma,
17 cases (10.6%) were immature teratoma, 4 cases (2.5%) were dysgerminoma, 6 cases (3.8%)
were seminomas and 1 case (1.6%) was yolk sac tumour. (Table III).
OVARIAN GERM CELL TUMOURS
There were 312 cases of ovarian neoplasms seen over this ten years period of study, out of these
there were 125 cases of ovarian germ cell tumours which accounted for 40.1% of all ovarian
neoplasms.
1.Teratomas.
a) Mature teratoma: 112 cases out of 125 cases of ovarian germ cell tumours are mature
teratoma and this accounted for 90% of cases. The highest frequency of this tumour
occurred in 4th decade of life. There is only one case of solid teratoma and 111 cases of
cystic teratoma. (Table I,II, III and Figure 1).
b) Immature teratoma: There were 9 (5.6%) cases of immature teratoma and the highest
frequency of this tumour occurred in those within the 1st decade of life. (Table I, III and
Figure 2).
2.Dysgerminoma: 4 cases of ovarian dysgerminoma were recorded and this accounted for 2.5%
and highest frequency occurred in those within 2nd decade of life (adolescents). (Tables I, III and
Figure 3).
32
TESTICULAR GERM CELL TUMOURS
There were 6 cases of testicular germ cell tumours seen and were all classical seminomas.
1.Seminoma: 6 cases of testicular classical seminoma were recorded and this accounted for 3.8%
and the highest incidence is in the 4th decade of life. (Table I, III and Figure 4).
EXTRAGONADAL GERM CELL TUMOURS
There were 29 cases of extragonadal germ cell tumours. (Table III)
1.TERATOMAS.
a. Mature teratomas: There were 20 cases of extragonadal mature teratomas which accounted for
69% of all extragonadal germ cell tumours. The commonest site was the sacrococcygeal region
with 11 (38%) cases followed by neck (cervical) region with 6 (20.6%) cases, and the highest
frequency occurred in 1st decade of life. (Table I and III).
b. Immature teratoma: There were 8 cases of extragonadal immature teratoma which accounted
for 27.6% of all extragonadal germ cell tumours. The commonest site was the sacrococcygeal
region with 6 (20.6%) cases, followed by neck with 2 (6.9%) cases; and the highest frequency
occurred in the 1st decade of life. (Table I and III).
2. YOLK SAC TUMOUR:
There was only 1 case of extragonadal yolk sac tumour and this accounted for 3.4% of all
extragonadal germ cell tumours and this occurred in sacrococcygeal region. (Table III and Figure
5).

33
IMMUNOHISTOCHEMISTRY
Two immunohistochemical stains were used in this study- they are CD-117 (c-kit) for seminoma
and dysgerminoma and alpha fetoprotein for yolk sac tumours.
There were 6 seminomas out of which 4 were CD 117 positive, thus accounted for 66.7% of the
cases.(Figure 4).
There were 4 cases of dysgerminomas out of which 2 were CD117 positive, this accounted for
50% of the cases.
There was 1 case of yolk sac tumours and is positive for alpha fetoprotein accounting for
100%.(Figure 5).
34
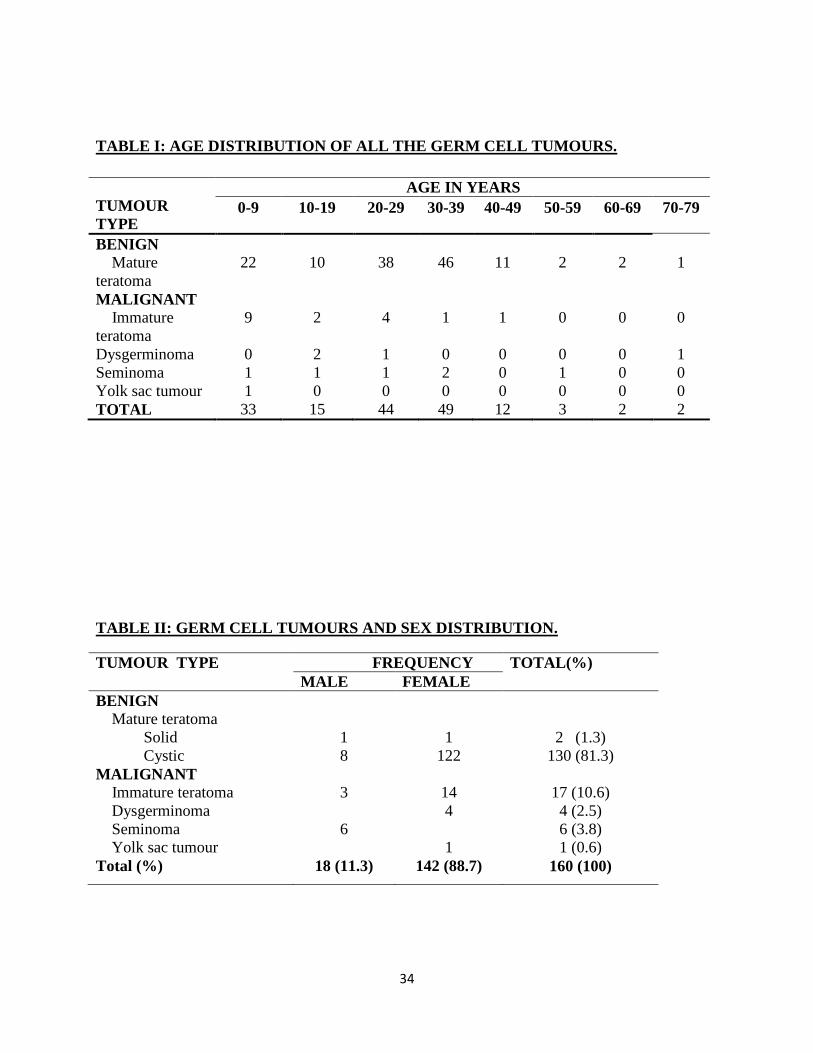
TABLE I: AGE DISTRIBUTION OF ALL THE GERM CELL TUMOURS.
TUMOUR
TYPE
AGE IN YEARS
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79
BENIGN
Mature
teratoma
22 10 38 46 11 2 2 1
MALIGNANT
Immature
teratoma
9 2 4 1 1 0 0 0
Dysgerminoma 0 2 1 0 0 0 0 1
Seminoma 1 1 1 2 0 1 0 0
Yolk sac tumour 1 0 0 0 0 0 0 0
TOTAL 33 15 44 49 12 3 2 2
TABLE II: GERM CELL TUMOURS AND SEX DISTRIBUTION.
TUMOUR TYPE FREQUENCY TOTAL(%)
MALE FEMALE
BENIGN
Mature teratoma
Solid 1 1 2 (1.3)
Cystic 8 122 130 (81.3)
MALIGNANT
Immature teratoma 3 14 17 (10.6)
Dysgerminoma 4 4 (2.5)
Seminoma 6 6 (3.8)
Yolk sac tumour 1 1 (0.6)
Total (%) 18 (11.3) 142 (88.7) 160 (100)

35
TABLE III: GERM CELL TUMOURS AND ANATOMICAL SITES DISTRIBUTION.
ANATOMICAL
SITES
TUMOUR TYPES
Mature
teratoma
Immature
teratoma
Seminoma Dysgerminoma Yolk sac
tumour
Total (%)
GONADAL
Ovary 112 9 0 4 0 125 (78)
Testis 0 0 6 0 0 6 (3.8)
EXTRAGONADAL
Oral 1 0 0 0 0 1(0.6)
Neck 6 2 0 0 0 8(5.0)
Sternum 1 0 0 0 0 1(0.6)
Retroperitoneum 1 0 0 0 0 1(0.6)
Sacrococcygeal 11 6 0 0 1 18(11.3)
Total (%) 132(82.5) 17(10.6) 6(3.8) 4(2.5) 1(0.6) 160( 100)

36
Figure 1: Photomicrograph of mature ovarian teratoma from a 28 years old female showing
keratinized stratified squamous epithelium overlying fibrocollagenous ovarian stroma ( H&E
X100).

37
Figure 2: Photomicrograph of immature ovarian teratoma from an 18 years old female
showing numerous neuroepithelial rosettes and immature cartilage embedded in a
fibrocollageneous ovarian stroma.( (H&E X100).

38
Figure 3: Photomicrograph of an ovarian dysgerminoma from a 15 years old female showing
uniform cells with pale cytoplasm with fairly uniform nuclei separated by fibrous septae
infilterated by lymphocytes. ( H&E X100).

39
Figure 4: A. Photomicrograph of a testicular classical seminoma from a 22 years old male
showing uniform cells separated by thin fibrous bands ( H&E X100).
B.Immunohistochemical stain of Figure 4A showing strong membraneous staining of tumour
cells.( C-Kit X400).
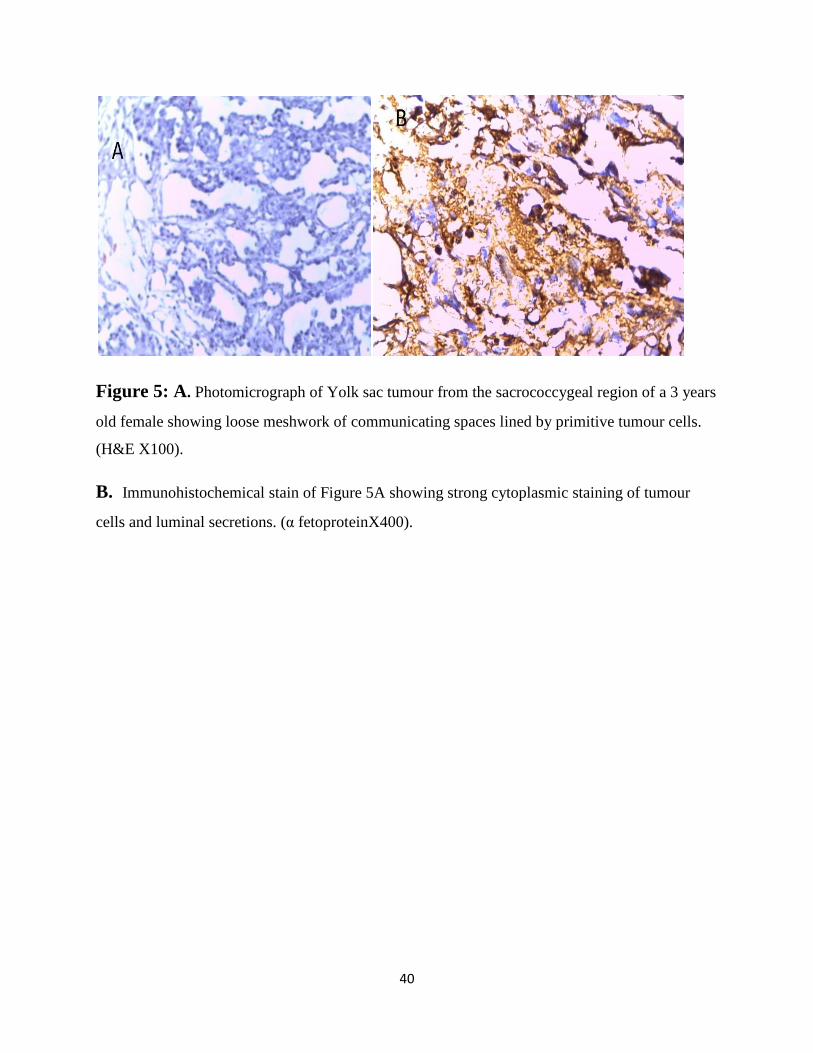
40
Figure 5: A. Photomicrograph of Yolk sac tumour from the sacrococcygeal region of a 3 years
old female showing loose meshwork of communicating spaces lined by primitive tumour cells.
(H&E X100).
B. Immunohistochemical stain of Figure 5A showing strong cytoplasmic staining of tumour
cells and luminal secretions. (α fetoproteinX400).
41
CHAPTER FIVE
DISCUSSION
Over a period of ten years 160 cases of germ cell tumours were recorded which accounted for
0.59% of all surgical biopsies received in our center. This finding is in support of the observation
of Edegbe45 from Ibadan that germ cell tumours are infrequent.
The germ cell tumours were more common in females than males in this study with a male to
female ratio of 1:7.9. The female predominance observed in this study is consistent with 1:15.5
male to female ratio reported by Nggada28 from Maiduguri. Teratomas show female
predominance with a male to female ratio of 1:13.6 in this study, this is in agreement with the
finding of male to female ratio of 1:18 in a study conducted by Akang12 from Ibadan.
Germ cell tumours comprise distinct entities with different peak age of presentation. The peak
age of occurrence of ovarian teratomas in this study was in the 4th decade of life, this is in
consonance with previous findings by Jha23 from Nepal which showed peak age occurrences of
21-40 years.
Malignant germ cell tumours such as immature teratomas, dysgerminoma and yolk sac tumours
in this study were more common in children and adolescents, (Table I) this conforms with the
findings of Samaila17, Mohammed19 and Junaid.26 The peak age of presentation of seminomas
was in the 4th decade of life from our study, which is similar to what Opot9 reported from
Nairobi. This figure is however, a decade higher than those obtained by other Nigerian studies
from Ilorin and Ile-Ife .32,33
The most common germ cell tumours encountered in this study were teratomas which accounted
for 93.2%. The ovaries are the most common site of teratomas followed by sacrococcygeal

42
region which accounted for 121( 75.6%) cases and 17( 10.7%) cases respectively. This is similar
to the findings by Akang12 who found out that the most common site of teratomas was in the
ovaries which accounted for 83.2% of the cases, followed by the sacrococcygeal region which
accounted for 6.3%. The majority 88.6% of teratomas were mature (benign) teratomas, while
11.4% were immature (malignant).
There were 125 cases of ovarian germ cell tumours seen over the period under study, with
mature teratomas accounting for 90% of all the ovarian germ cell tumours. This is in keeping
with Western literature8,15 which recorded 95%, this is higher than the figures reported by
Onyiaorah27 and Jha23 in Nigeria and Nepal respectively. The immature ovarian teratomas were
seen commonly in adolescent, similar to the findings by Mohammed19 and Junaid26.
There were 6 (3.8%) cases of testicular seminoma seen over this period of study, confirming the
rarity of testicular germ cell tumours in blacks.9,32,33
Extragonadal germ cell tumours are rare and often display an axial distribution pattern such as
brain, neck, mediastinum, retroperitoneum, vagina and sacrococcygeal region.35-41Extragonadal
teratoma is the most common congenital tumour and often occur in infancy and childhood.14
There were 29 (18.1%) cases of extragonadal germ cell tumors seen during this period of study.
The most common site of extragonadal germ cell tumours as recorded in this study was the
sacrococcygeal region 18(11.3%) cases followed by neck (cervical) region with 8(5%) cases.
Other rare sites are oral, sternum and retroperitoneum with 1(0.6%) case each. The majority of
the cases were in infants and children with only three cases seen in adults. This is in keeping
with previous findings of David et al44 from Boston who found out that sacrococcygeal region
was the most common site accounting for 40% followed by head and neck with
43
5.5%.Edegbe45from Ibadan also found out that the most frequent anatomical sites were the
sacrococcygeal region (20.5%) and neck (10.3%). The majority of their cases were infants and
children as was found in this study.
The most common extragonadal germ cell tumour encountered during this study was the mature
teratoma which accounted for 12.5% (20 cases) this is followed by immature teratoma which
accounted for 5.0% (8 cases) and were seen more commonly in sacrococcygeal and cervical
regions; and the majority of the patients are females. This corroborates with earlier study done by
Mohammed et al14 where they found that mature and immature teratoma accounted for 82% and
18% respectively.
Germ cell tumours such as seminomas and dysgerminomas are CD117 (c-kit) positive. CD117
expression is present in >85% of all dysgerminomas and seminomas.54 The staining pattern is
usually membraneous. CD117 encoded by the c-kit gene, is a transmembrane tyrosine kinase
growth factor receptor that is overexpressed in a variety of tumours, most notably gastro
intestinal stromal tumours (GIST’s). CD117 immunohistochemical expression by dysgerminoma
does not necessarily indicate an underlying c-kit gene mutation. About one-quarter of
dysgerminomas harbor a mutation, but these do not involve exon 11 as observed in GIST, and
therefore the therapeutic significance remains to be determined.54 The results of CD 117 obtained
from this study is relatively low (66.7% for seminoma and 50% for dysgerminomas) this may be
due to poor fixation of the tissues as this affects the sensitivity of the tumours to CD117.
Alpha fetoprotein is expressed in a majority of yolk sac tumour and the staining pattern is
cytoplasmic. The antibodies for alpha fetoprotein may also stain hyaline globules or luminal
44
secretions in yolk sac tumour. The case of yolk sac tumour in this study is positive for alpha
fetoprotein.
CONCLUSION
This study shows that germ cell tumours are infrequent in our environment and affect all age
groups. They are predominantly seen in females and the most common type is teratoma. The
most common sites are the ovary and sacrococcygeal region for the gonadal and extragonadal
germ cell tumours respectively.
45
REFERENCES
1. Looijenga LHJ, Oosterhuis JW. Pathogenesis of testicular germ cell tumours. Rev of
Reprod 1999;4: 90–100.
2. Wang J, Zheng Z, Qiu Y, Tou J, Liu W, Xiong Q et al. Primary mixed germ cell tumor
arising in the pancreatic head. J Pediatr Surg 2013;48:E21-E24.
3. Samaila MO, Maitama HY, Abdullahi K, Waziri GD. Yolk sac tumour of the penile
shaft:A rare primary extra-gonadal presentation. Afr J Paediatr Surg 2011;8(2):241-243.
4. Stewart BW, Kleihues P. World cancer report.World Health Organization 2003,
Lyon:IARC press.p.208-222.
5. Ulbright TM, Amin MB, Young RH. Atlas of tumor pathology: tumors of the testis,
adnexa, spermatic cord, and scrotum. 3rd series. Washington, D.C: Armed forces institute
of pathology; 1997. p.1-184.
6. Ogunbiyi JO, Shittu OB, Aghadiuno PU, Lawani J. Seminoma arising in cryptorchid testes
in Nigerian males. East Afr Med J 1996;73(2):129-32.
7. Scully RE, Young RH, Clement PB. Atlas of pathology: tumors of the ovary, maldeveloped
gonads, fallopian tube, and broad ligament. 3rd series. Washington D.C: Armed forces
institution of pathology; 1996. p. 239-306.
8. Nogales F, Talerman A, Kubik-Huch RA, Tavassoli FA, Devouassoux-Shisheboran M.
Germ cell tumours; Pathology and genetics of tumours of the breast and female genital
organs. World Health Organization Classification of tumours. 2004 Lyon: IARC Press.
p.163-175.
9. Opot EN, Magoha GAO. Testicular cancer at Kenyatta national hospital Nairobi. East Afr
Med J 2000;77:80-85.
10. Sonneveld DJA, Schaapveld M, Sleijfer DTh, Meerman GJ Te, van der Graaf WTA,
Sijmons RH et al. Geographic clustering of testicular cancer incidence in the northern part
of the Netherlands. British J Cancer 1999;81(7):1262-1267.
11. Woodward PJ, Heidenreich A, Looijenga LHJ, Oosterhuis JW, Mcleod DG, Moller H et
al.Germ cell tumours; Pathology and genetics of tumours of the urinary system and male
genital organs. World Health Organization classification of tumours.2004 Lyon:IARC
press p221-249.
12. Akang EEU, Odunfa AO, Aghadiuno PU. A review of teratomas in Ibadan. Afr J Med
1994; 23:53-60.

46
13. Mobogunje OA, Nirodi NS, Harrison KA, Edington GM. Teratomas in adult Nigerians.
Afr J Med sci 1980;151-158.
14. Mohammed U, Ahmed SA, Shehu MS, Mohammed A. Extragonadal teratoma in zaria,
Nigeria. Arc Int Surg 2013;3(1):11-13.
15. Rosai J. editor. Female reproductive system; ovary- germ cell tumour In: Ackerman's
surgical pathology 10th ed. St. Louis: Mosby; 2011. Vol 2. p.1583-1592.
16. Agboola AOJ, Adekanbi FA, Musa AA, Sotimehin AS, Deji-Agboola AM, Shonubi AMO
et al. Pattern of childhood malignant tumours in a teaching hospital in south-western
Nigeria. Med J Aust 2009;190(1):12-14.
17. Samaila MO. Malignant tumours of childhood in Zaria. Afr J Paedtr Surg 2009;6:19-23.
18. Koshy M, Vijayananthan A, Vadiveloo V. Malignant ovarian mixed germ cell tumour: a
rare combination. Biomed Imaging Interv J 2005;1(2):e10.
19. Mohammed A, Malami SA, Calvin B, Abdullahi K. A histopathological study of ovarian
neoplasms in children in a tertiary hospital of northern Nigeria. Afr J of Paediatr Surg
2010;7(2):75-77.
20. Tanko NM, Echejoh GO, Manasseh NA, Mandong MB, Uba AF. Paediatric solid
tumours in Nigerian children: A changing pattern?. Afr J Paediatr Surg 2009:6:7-10.
21. Shah SH, Pervez S, Hassan SH. Frequency of malignant solid tumors in children. JPMA
2000;Mar:1-3.
22. Iyoke CA, Ifeadike CO, Nnebue CC, Nkwo PO, Ezugwu EC, Edosuyi L Et al. A ten year
review of ovarian cancer in Enugu, south east Nigeria. Afrimedic J 2011;2(1):8-12.
23. Jha R, Karki S. Histological pattern of ovarian tumours and their age distribution. Nepal
Med Coll J 2008;10(2):81-85.
24. Thanikasalam K, Ho CM, Adeed N, Shahidan MN, Azizah WK. Pattern of ovarian
tumours among Malaysian women at general hospital, Kuala Lumpur. Med J Malaysia
1992;47(2):139-146.
25. Lancaster EJ, Muthuphei MN. Ovarian tumours in Africans: a study of 512 cases. Cent
Afr J Med 1995;41(8):245-8.
26. Junaid TA. Ovarian neoplasms in children and adolescents in Ibadan, Nigeria. Cancer
1981;47:610-614.
47
27. Onyiaorah IV, Anunobi CC, Banjo AA, Abdulkarem FA, Nwankwo KC.
Histopathological patterns of ovarian tumours seen in Lagos University Teaching
Hospital: a ten year retrospective study. Nig Q J Hosp Med 2011(2):114-8.
28. Nggada HA, Khalil MIA. Histopathological study of 66 germ cell tumours in Maiduguri,
north eastern, Nigeria. Sahel Med J 2003;6(1):10-13.
29. McGlynn KA, Devesa SS, Sigurdson AJ, Brown LM, Tsao L, Tarone RE. Trends in the
incidence of testicular germ cell tumors in the United States. Cancer 2003 Jan 1;97(1):63-
70.
30. Ogwumba FO, Aghaji AE. Testicular cancer: management challenges in an African
developing country. S Afr Med J 2010; 100:452-455.
31. Gilligan TD, Seidenfeld J, Basch EM, Einhorn LH, Fancher T, Smith DC et al. American
society of clinical oncology clinical practice guideline on uses of serum tumor markers in
adult males with germ cell tumors. J Clin Oncol 2010;28:3388-3404.
32. Izegbu MC, Ojo MO, Shittu LAJ. Clinico-pathological patterns of testicular malignancies
in Ilorin, Nigeria- a report of 8 cases. J Cancer Reseach and Therap 2005;1(4):229-231.
33. Salako AA, Onakpoya UU, Osasan SA, Omoniyi-Esan GO. Testicular and para-testicular
tumours in south western Nigeria. Afr Health Sci 2010;10(1):14-17.
34. Obafunwa JO, Elesha SO, Odunjo EO. Tumours of the testes in Lagos, Nigeria. Nig Med
Practitioner 1990; 19(4):50-52.
35. Samaila MOA. Immature neck teratoma in infants. Intern J of Path 2011;451-455.
36. Gonzalez-Crussi F. Extragonadal teratomas. Washington, D.C: Armed forces institute of
pathology; 1982:1-199.
37. Legbo JN, Opara WEK, Legbo JE. mature sacrococcygeal teratoma:case report. Afr
Health Sci 2008:8(1):54-57.
38. Ibekwe TS, Kokong DD, Ngwu BA, Akinyemi OA, Nwaorgu OG, Akang EE. Nasal
septal teratoma in a child. World J Surg Oncol 2007;5:58.
39. Chirdan LB, Uba AF, Pam SD, Edino ST, Mandong BM, Chirdan OO. Sacrococcygeal
teratoma:clinical characteristics and long-term outcome in Nigerian children. Ann Afr
Med 2009;8:105-109.
40. Ogun OA, Ogun GA, Brown BJ, Mosuro AL, Ashaye AO. Congenital orbital teratoma: a
case report and challenges of its management in a resource limited setting. Pan Afr Med
J 2012;12:3.
48
41. Benali HA, Lalya I, Allaoui M, Benmansour A, Elkhanoussi B, Benjelloun S et al.
Extragonadal mixed germ cell tumor of the right arm: description of the first case in the
literature. World J of Surg Onco 2012;10:69.
42. Afuwape OO, Ogundoyin OO, Ogunlana DI, Adeleye AO. Adult sacrococcygeal
teratoma: a case report. Ghana Med J 2009;43(1):40-42.
43. Daubenton JD, Hartley PS, Rode H, Sinclair-smith CC. Sacrococcygeal germ-cell
tumours- the red cross war memorial children's hospital experience, 1980-1996. S Afr
Med J 1998;88:1592-1594.
44. Tapper D, Lack EE. Teratomas in infancy and childhood. A 54-year experience at the
children's hospital medical center. Ann Surg 1983:398-409.
45. Edegbe FO, Okani CO, Ogun GO, Akang EE. Germ cell tumours in children: A twenty-
year retrospective study (January 1988- December 2007) in Ibadan, South-West Nigeria.
AFRIMEDIC Journal 2014;5(1):8-16.
46. Chaganti RSK, Houldsworth J. Genetics and biology of adult human male germ cell
umors. Cancer Res 2000;60:1475-1482.
47. Nayernia K, Mahmazi S. Genetics of testicular germ cell tumors. J of Rep and Infert
2000;1(1):44-51.
48. Rosai J. editor. Male reproductive system; Testis- germ cell tumor in: Ackerman's
surgical pathology. 10th ed. St. Louis: Mosby; 2011. vol.1 p 1338-1355.
49. Talerman A, Haije WG. Alpha-fetoprotein and germ cell tumors: a possible role of yolk
sac tumor in production of alpha-fetoprotein. Cancer 1974;34:1722-1726.
50. National Cancer Institute: PDQ Extragonadal Germ Cell Tumours Treatment. Bethesda,
MD: National Cancer Institute. Date last modified 02/28/2014.
51. Asakura K, Izumi Y, Ikeda T, Kimura Y, Horinouchi H, Hayashi Y et al. Mediastinal
germ cell tumor with somatic-type malignancy: report of 5 stage I/II cases. Ann Thorac
Surg 2010;90:1014-6.
52. Idrees MT, Kuhar M, Ulbright TM, Zhang S, Agaram N, Wang M et al. Clonal evidence
for the progression of a testicular germ cell tumor to angiosarcoma. Human Path
2010;4:139-144.
53. Ahmed T, Bosl GJ, Hajdu SI. Teratoma with malignant transformation in germ cell
tumors in men. Cancer 1985;56:860-863.
54. Rabban JT, Zaloudek CJ. A practical approach to immunohistochemical diagnosis of
ovarian germ cell tumours and sex cord-stromal tumours. Histopathology 2013; 62, 71-88

49
APPENDICES
APPENDIX I
World Health Organisation Histological Classification of Ovarian germ cell tumours.
Germ Cell Tumours:
PRIMITIVE GERM CELL TUMOURS
Dysgerminoma
Variant- with syncytiotrophoblatic cells
Yolk sac tumour (Endodermal sinus tumour)
Variants –polyvesicularvetillinetumour
-Hepatoid
-Glandular
Embryonal carcinoma
Polyembryoma
Non-gestational Choriocarcinoma
Teratomas
Immature
Mature
-Solid
-Cystic (dermoid cyst)
-Fetiformteratoma (homunculus)
Monodermalteratoma and somatic-type tumours associated with dermoid cysts

50
Thyroid tumour group
Struma ovarii
-Benign
-Malignant (specify)
Carcinoid group
Insular
Trabecular
Mucinous
Strumal carcinoid
Mixed
Neuroectodermaltumour group
Ependymoma
Primitive neuroectodermaltumour
Medulloepithelioma
Glioblastomamultiforme
Others
Carcinoma group
Squamous cell carcinoma
Adenocarcinoma
Others
Melanocytic group

51
Malignant melanoma
Melanocytic naevus
Sarcoma group (specify type)
Sebaceous tumour group
Pituitary-type tumour group
Retinal anlage tumour group
Others
52
APPENDIX II
WHO HISTOLOGICAL CLASSIFICATION OF TESTIS TUMOURS.
GERM CELL TUMOURS:
Intratubular germ cell neoplasia unclassified.
Other types
Tumours of one histological type (pure forms).
Seminoma
Seminoma with syncytiotrophoblastic cells
Spermatocytic seminoma
Spermatocytic seminoma with sarcoma
Embryonal carcinoma
Yolk sac tumours
Trophoblastic tumours
Choriocarcinoma
Trophoblastic neoplasms other than choriocarcinoma
Monophasic choriocarcinoma
Placental site trophoblastic tumour
Teratoma
Dermoid cyst
Monodermalteratoma
Teratomawith somatic type malignancies.

53
Tumours of more than one histological type (mixed forms)
Mixed embryonal carcinoma and teratoma
Mixed teratoma and seminoma
Choriocarcinoma and teratoma/embyonal carcinoma
Others

54
APPENDIX III
LEICA BIOSYSTEMS IMMUNOHISTOCHEMICAL PROTOCOL ADAPTED IN THIS
STUDY.
1. Cut and mount sections on slides coated with a suitable tissue adhesive.
2. De-paraffinize sections in xylene or xylene substitutes.
3. Re-hydrate through graded alcohols.
4. Wash slides in running tap water.
5. Perform antigen retrieval as required.
6. Wash slides in de-ionized water.
7. Neutralize endogenous peroxidase using peroxidase Block for 5 minutes.
8. Wash in TBS for 2 x 5 minutes.
9. Incubate with protein Block for 5 minutes.
10. Wash in TBS for 2 x 5 minutes.
11. Incubate with optimally diluted primary antibody
12. Wash in TBS for 2 x 5 minutes.
13. Incubate with post primary for 30 minutes.
14. Wash in TBS for 2 x 5 minutes.
15. Incubate with NovolinkTM polymer for 30 minutes.
16. Wash in TBS for 2 x 5 minutes with gentle rocking.
17. Develop peroxidase activity with DAB working solution for 5 minutes.
18. Rinse slides in water.
19. Counterstain with Haematoxylin.
20. Rinse slides in water for 5 minutes.
21. Dehydrate, clear and mount sections.
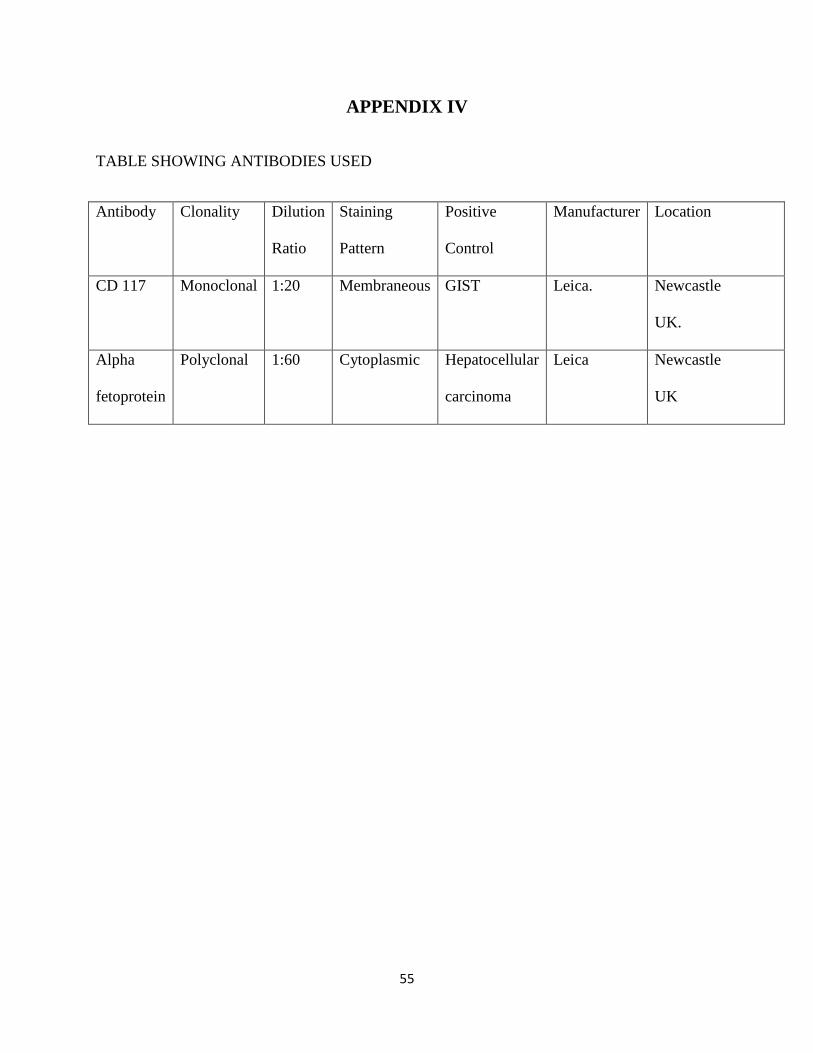
55
APPENDIX IV
TABLE SHOWING ANTIBODIES USED
Antibody Clonality Dilution
Ratio
Staining
Pattern
Positive
Control
Manufacturer Location
CD 117 Monoclonal 1:20 Membraneous GIST Leica. Newcastle
UK.
Alpha
fetoprotein
Polyclonal 1:60 Cytoplasmic Hepatocellular
carcinoma
Leica Newcastle
UK
56
APPENDIX V

57