Embed Size (px)
Citation preview
Geriatric Geriatric MedicineMedicine
Dr Stanley LipschitzDr Stanley Lipschitz
Specialist Physician & Specialist Physician & GeriatricianGeriatrician
““Growing old is not so Growing old is not so bad,bad,
when you consider thewhen you consider thealternativealternative ""
Woody Allen
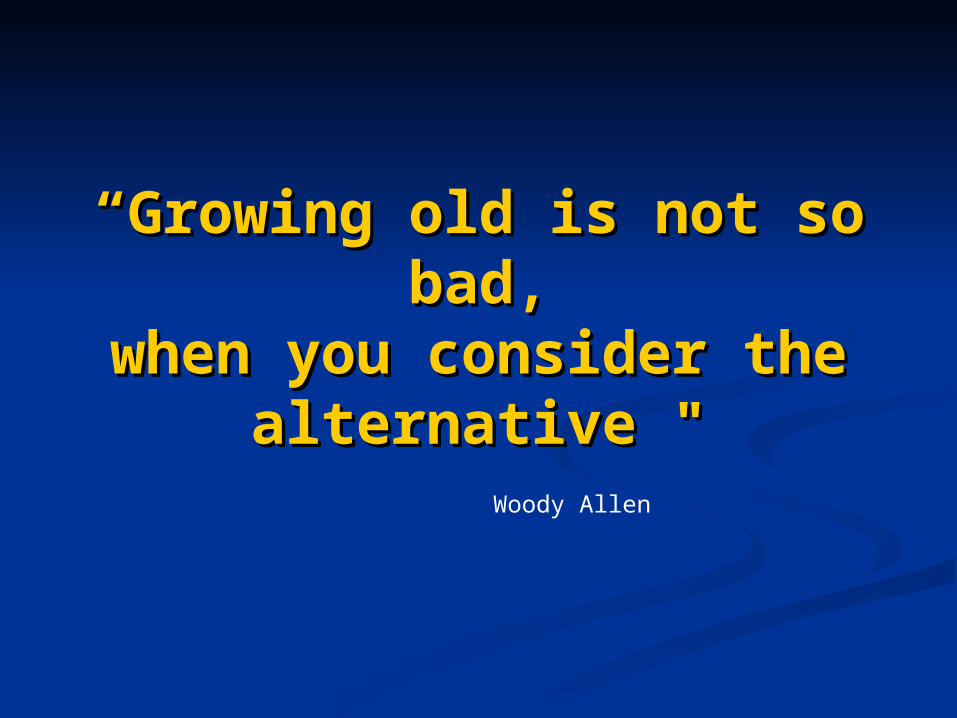
Relationship Between Age & Relationship Between Age & FunctionFunction
0
20
40
60
80
100
120
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Fu
nct
ion
%
Age ( Years )
Multiple ChronicDiseases
Loss of HomeostaticReserve
Vulnerability toInsults
+
IN THE ELDERLY
Biological Aging
+
Loss of Homeostatic Loss of Homeostatic FunctionFunction
Regulation of critical functions such as Regulation of critical functions such as body Temperature, energy metabolism, body Temperature, energy metabolism, heart rate and BP.heart rate and BP.
Adrenergic responsiveness declines with Adrenergic responsiveness declines with aging - may influence the regulation of aging - may influence the regulation of these bodily functions in the elderly.these bodily functions in the elderly.
Such Homeostatic losses mean that Such Homeostatic losses mean that Diagnostic and Therapeutic Diagnostic and Therapeutic undertakings, acute illness, flares of undertakings, acute illness, flares of chronic disease and traumatic insults chronic disease and traumatic insults will have the potential for greater than will have the potential for greater than usual ill effectusual ill effect
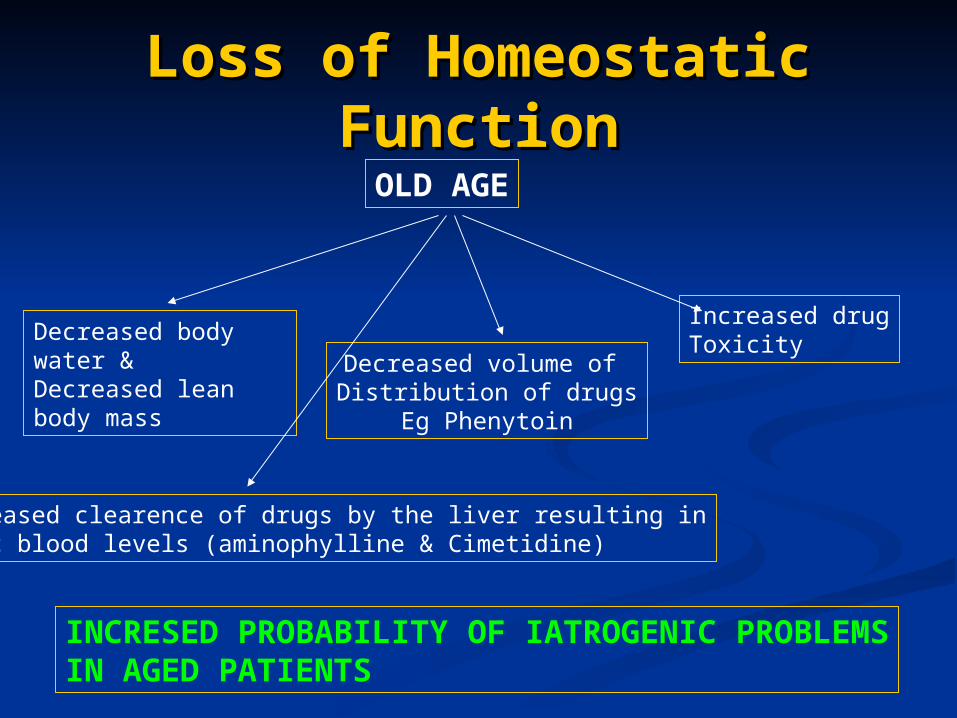
Loss of Homeostatic Loss of Homeostatic FunctionFunction
OLD AGE
Decreased body water &Decreased lean body mass
Decreased volume of Distribution of drugs
Eg Phenytoin
Increased drugToxicity
Decreased clearence of drugs by the liver resulting inToxic blood levels (aminophylline & Cimetidine)
INCRESED PROBABILITY OF IATROGENIC PROBLEMSIN AGED PATIENTS
Atypical Disease Atypical Disease PresentationPresentation
Loss of Homeostatic Function
Biological Aging,Multiple Chronic Diseases
& Disability
+
Modification of Host Response
Commonly acute Illness presents Atypically
‘‘GIANTS OF GIANTS OF GERIATRICS’GERIATRICS’
ATYPICAL PRESENTATION of ATYPICAL PRESENTATION of DISEASEDISEASE
DELIRIUMDELIRIUM FALLSFALLS LOSS OF MOBILITYLOSS OF MOBILITY INCONTINENCEINCONTINENCE LOSS of ADL ABILITYLOSS of ADL ABILITY
Atypical Disease Atypical Disease PresentationPresentation
UG Sepsis may cause Delirium UG Sepsis may cause Delirium without fever, polyuria or BOMwithout fever, polyuria or BOM
Pain response is often blunted – Pain response is often blunted – Delirium or breathlessness may be the Delirium or breathlessness may be the first response to AMIfirst response to AMI
Acute change in wellbeing or a decline Acute change in wellbeing or a decline in function or “something is different”, in function or “something is different”, may be the only indication of an acute may be the only indication of an acute Abdominal crisis in the ElderlyAbdominal crisis in the Elderly
Atypical Disease Atypical Disease PresentationPresentation
Such warnings of subtle changes, especially by Such warnings of subtle changes, especially by observers intimately and regularly involved, observers intimately and regularly involved, should be taken seriously by the Clinician and are should be taken seriously by the Clinician and are often the only indication of a Potentially often the only indication of a Potentially overwhelming event.overwhelming event.
Nonspecific change in status always warrants Nonspecific change in status always warrants careful and detailed assessment in particular careful and detailed assessment in particular looking for “occult illness” such as UG sepsis, looking for “occult illness” such as UG sepsis, silent MI, Pneumonia, Abdominal crises and Drug silent MI, Pneumonia, Abdominal crises and Drug Toxicity.Toxicity.
Even when nothing is found – ongoing surveillance Even when nothing is found – ongoing surveillance is required. TIME, may be the most important is required. TIME, may be the most important Diagnostic tool! Diagnostic tool! Diagnostic DifficultyDiagnostic Difficulty
Narrow window of Narrow window of Therapeutic and Therapeutic and
Diagnostic TolerenceDiagnostic Tolerence The challenge in Geriatric Medicine is the critical The challenge in Geriatric Medicine is the critical narrowing of the diagnostic and therapeutic window narrowing of the diagnostic and therapeutic window due to loss of homeostatic function, multiple diseases due to loss of homeostatic function, multiple diseases and disabilities and atypical disease presentationand disabilities and atypical disease presentation
There is much more room for mistakes in judgement There is much more room for mistakes in judgement when caring for the frail elderly when caring for the frail elderly
A diagnostic test for one problem may adversely A diagnostic test for one problem may adversely effect the overall function of the patient due to a effect the overall function of the patient due to a disease in another system e.g. Contrast medium & disease in another system e.g. Contrast medium & Renal dysfunctionRenal dysfunction
A therapeutic agent may have adverse effects e.g. A therapeutic agent may have adverse effects e.g. Cimetidine used for a DU may result in a decline in Cimetidine used for a DU may result in a decline in Cognitive functionCognitive function
The COMPREHENSIVE The COMPREHENSIVE GERIATRIC GERIATRIC
ASSESSMENTASSESSMENT Comprehensive assessment of the elderly Comprehensive assessment of the elderly
patient is critical for the provision of proper patient is critical for the provision of proper health carehealth care
Should be Standard – absolutely essential Should be Standard – absolutely essential when there has been an acute change in social when there has been an acute change in social circumstance, physical or mental status, or a circumstance, physical or mental status, or a confusing constellation of signs and symptoms, confusing constellation of signs and symptoms, when a patients living situation has changed when a patients living situation has changed often due to deteriorating health, in a patient often due to deteriorating health, in a patient with a new medical problemwith a new medical problem
Also as an integral part of decision making Also as an integral part of decision making regarding placement in any Care Facilityregarding placement in any Care Facility
The COMPREHENSIVE The COMPREHENSIVE GERIATRIC GERIATRIC
ASSESSMENTASSESSMENT To review in detail the Physical, To review in detail the Physical,
Mental and Social situation of the Mental and Social situation of the patientpatient
To correct any causes of Disability To correct any causes of Disability and to stabilise those that may be and to stabilise those that may be progressing unnecessarily progressing unnecessarily
The social and Physical environment The social and Physical environment may need to be modified to maximise may need to be modified to maximise independenceindependence
The COMPREHENSIVE The COMPREHENSIVE GERIATRIC GERIATRIC
ASSESSMENTASSESSMENT The search for specific Diagnoses and The search for specific Diagnoses and
cures is less often a Primary Goal, than cures is less often a Primary Goal, than is the formulation of a Practical Plan to is the formulation of a Practical Plan to preserve function, autonomy and preserve function, autonomy and DignityDignity
Hospitalization is a major risk to the Hospitalization is a major risk to the precarious homeostasis of the Elderly precarious homeostasis of the Elderly and should only be resorted to for the and should only be resorted to for the treatment of acute, severe or Life treatment of acute, severe or Life threatening illness.threatening illness.
The COMPREHENSIVE The COMPREHENSIVE GERIATRIC ASSESSMENT –GERIATRIC ASSESSMENT –
covers 5 categoriescovers 5 categories
Physical healthPhysical health Mental healthMental health Socioeconomic statusSocioeconomic status EnvironmentEnvironment Functional statusFunctional status
Detecting AD – who to Detecting AD – who to screenscreen
screen
New patients > 65 yrs Established patients > 65 yrs
Patients with early warning signs
Memory Loss Cognitive Deficits
Change in Personality or Behavior
AD making the AD making the DiagnosisDiagnosis
Careful HistoryCareful History Alternate sources – family, work, nursing staff, Alternate sources – family, work, nursing staff,
friends.friends. Onset and Progression – insidious/acute, Onset and Progression – insidious/acute,
smooth/stepwise.smooth/stepwise. Isolated Memory vs Multiple Cognitive deficitsIsolated Memory vs Multiple Cognitive deficits Similarities/Differences, Abstract Thought, Similarities/Differences, Abstract Thought,
ProverbsProverbs MMSEMMSE Physical and Neurological examinationPhysical and Neurological examination Laboratory tests and Brain ImagingLaboratory tests and Brain Imaging
AD making the AD making the Diagnosis:Diagnosis:The MMSEThe MMSE
Take a careful history of Cognitive Take a careful history of Cognitive function before doing the MMSEfunction before doing the MMSE
Interpret the MMSE in a patient Interpret the MMSE in a patient specific manner – Education, specific manner – Education, Language, MoodLanguage, Mood
Don’t be kind – score down!Don’t be kind – score down! It takes 10 minutes – do it when It takes 10 minutes – do it when
appropriate!appropriate!
DSM IV CRITERIA - DSM IV CRITERIA - DEMENTIADEMENTIA
MEMORY IMPAIRMENTMEMORY IMPAIRMENT DYSPHASIADYSPHASIA DYSPRAXIADYSPRAXIA AGNOSIAAGNOSIA EXECUTIVE FUNCTIONEXECUTIVE FUNCTION OCCUPATIONAL/SOCIAL FUNCTIONOCCUPATIONAL/SOCIAL FUNCTION DECLINE FROM FORMER LEVEL OF DECLINE FROM FORMER LEVEL OF
FUNCTIONINGFUNCTIONING
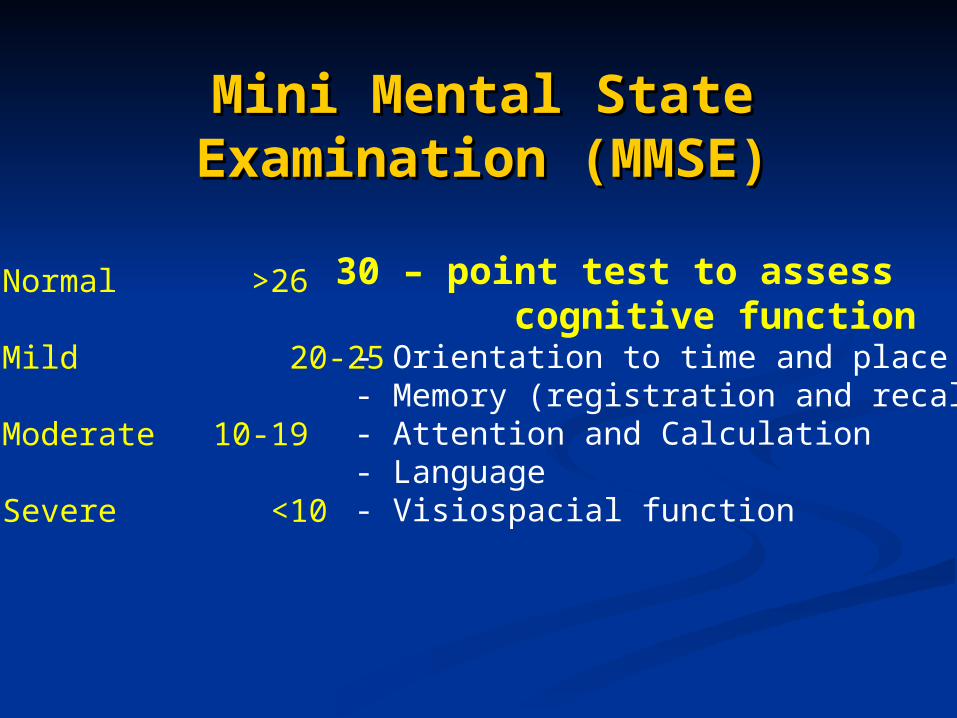
Mini Mental State Mini Mental State Examination (MMSE)Examination (MMSE)
30 – point test to assess cognitive function - Orientation to time and place - Memory (registration and recall) - Attention and Calculation - Language - Visiospacial function
Normal >26
Mild 20-25
Moderate 10-19
Severe <10
Value of (CGA) Value of (CGA) assessmentassessment
The Primary goal is preservation of the The Primary goal is preservation of the patient’s function and independencepatient’s function and independence
If reversible problems are not detected If reversible problems are not detected – goal is to identify support needs, – goal is to identify support needs, mobilize community and family mobilize community and family resources and maintain function and resources and maintain function and autonomyautonomy
A full knowledge of what Community A full knowledge of what Community resources are available is essential resources are available is essential
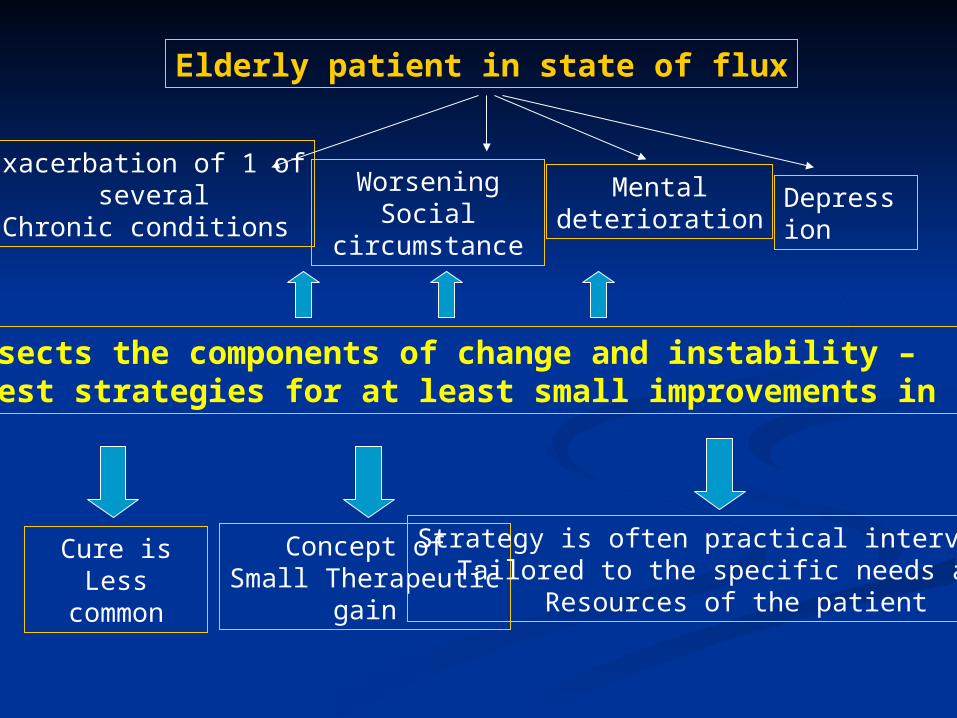
Elderly patient in state of flux
Exacerbation of 1 of several
Chronic conditions
WorseningSocial
circumstance
Mentaldeterioration
Depression
CGA dissects the components of change and instability – to suggest strategies for at least small improvements in Function
Cure isLess
common
Concept ofSmall Therapeutic
gain
Strategy is often practical interventionTailored to the specific needs and
Resources of the patient
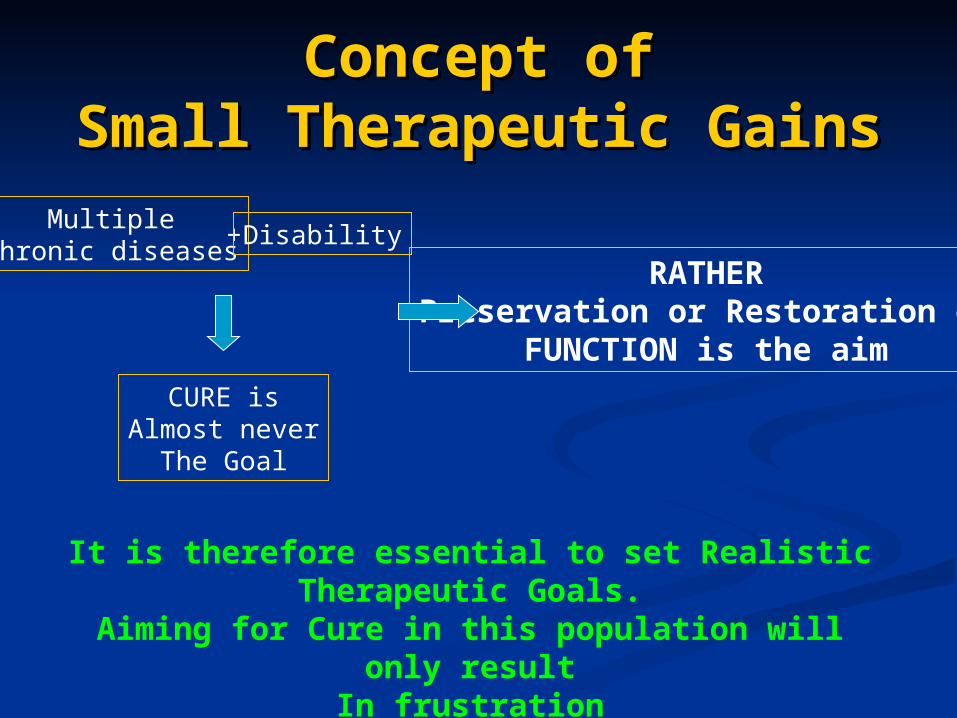
Concept ofConcept ofSmall Therapeutic GainsSmall Therapeutic Gains
MultipleChronic diseases
+ Disability
CURE isAlmost never
The Goal
RATHERPreservation or Restoration of
FUNCTION is the aim
It is therefore essential to set Realistic Therapeutic Goals.
Aiming for Cure in this population will only result
In frustration
PREVENTIONPREVENTION
Normal preventive medicine applies – glucose, Normal preventive medicine applies – glucose, BP, BMD, Lipids etcBP, BMD, Lipids etc
Identify SAFETY RISKS (home visit) – lighting, Identify SAFETY RISKS (home visit) – lighting, loose mats, handrails, stairs, showers/bath, loose mats, handrails, stairs, showers/bath, kitchen storagekitchen storage
Communication – telephone, alarmsCommunication – telephone, alarms Good Surveillance system – frequent visits from Good Surveillance system – frequent visits from
Dr, Community nurses, social workers etcDr, Community nurses, social workers etc NutritionNutrition PREVENTIVE REHABILITATION – for all PREVENTIVE REHABILITATION – for all
illnessillness
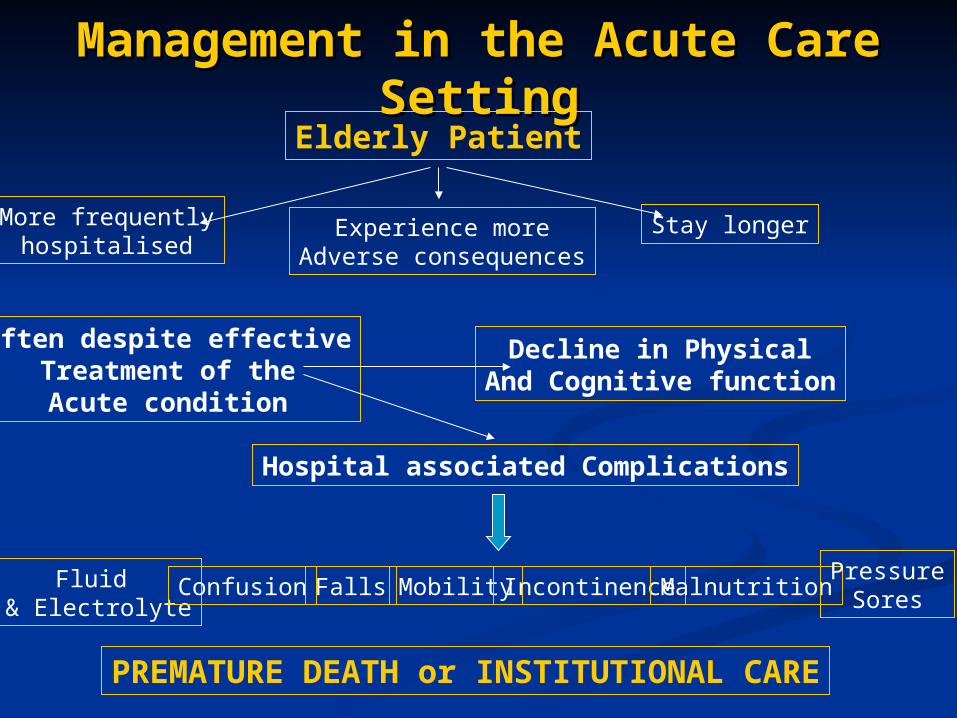
Management in the Acute Care Management in the Acute Care SettingSetting
Elderly Patient
More frequentlyhospitalised
Experience moreAdverse consequences
Stay longer
Often despite effectiveTreatment of theAcute condition
Decline in PhysicalAnd Cognitive function
Hospital associated Complications
Fluid & Electrolyte
Confusion Mobility IncontinenceMalnutritionPressure
Sores
PREMATURE DEATH or INSTITUTIONAL CARE
Falls
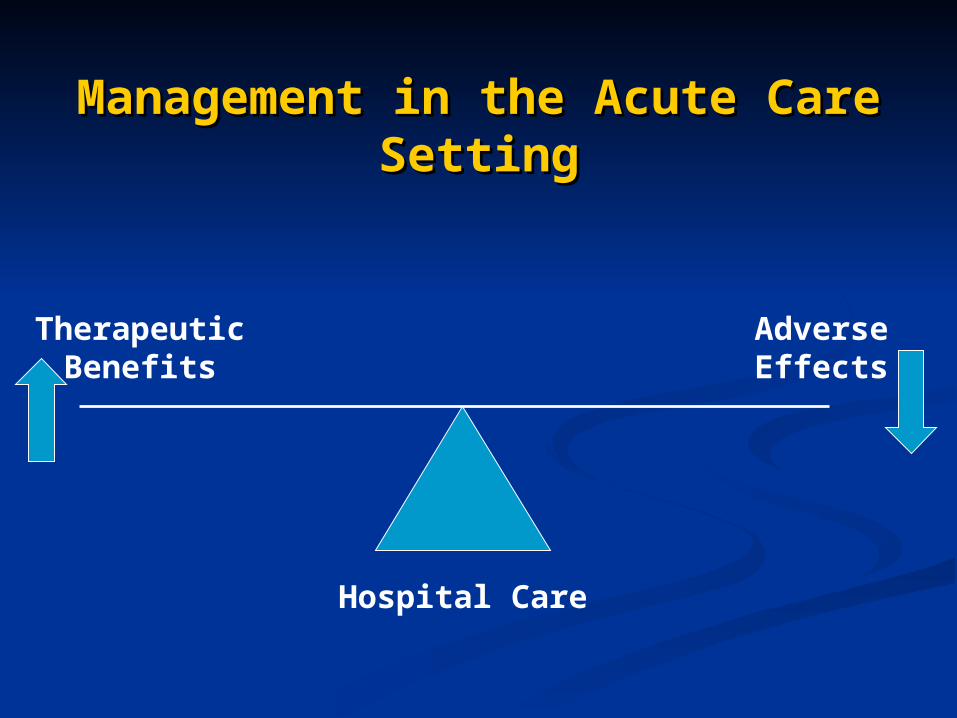
Management in the Acute Care Management in the Acute Care SettingSetting
TherapeuticBenefits
AdverseEffects
Hospital Care
Factors influencing Factors influencing ManagementManagement
in the Acute Care Settingin the Acute Care Setting
Those associated with AGINGThose associated with AGING Those associated with Those associated with
COEXISTENT DISEASECOEXISTENT DISEASE Those related to the PROCESS OF Those related to the PROCESS OF
CARE – Diagnostic and Treatment CARE – Diagnostic and Treatment relatedrelated
Factors influencing Factors influencing ManagementManagement
in the Acute Care Settingin the Acute Care SettingHOST AGINGHOST AGING
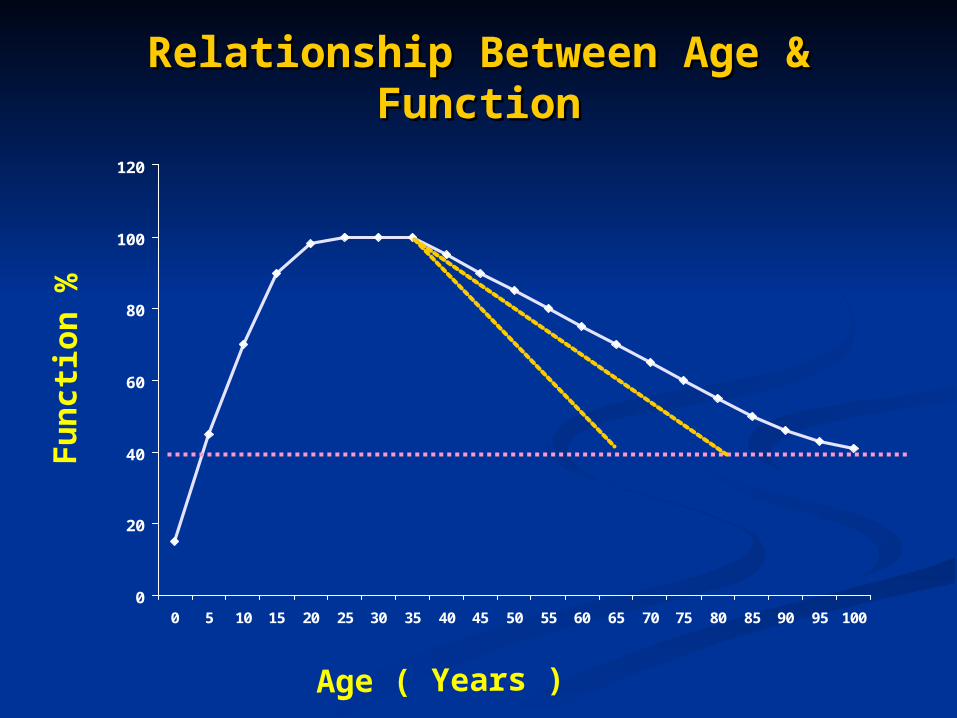
Gradual and variable decline in function over Gradual and variable decline in function over time – especially after 75 years, there is a time – especially after 75 years, there is a destinct loss of functional reserve (varies destinct loss of functional reserve (varies from organ to organ and person to person)from organ to organ and person to person)
This loss results in decreased ability to This loss results in decreased ability to handle stress (environmental or disease handle stress (environmental or disease related)related)
Impossible to focus on disease in one area, Impossible to focus on disease in one area, without being sensitive to changes in others without being sensitive to changes in others
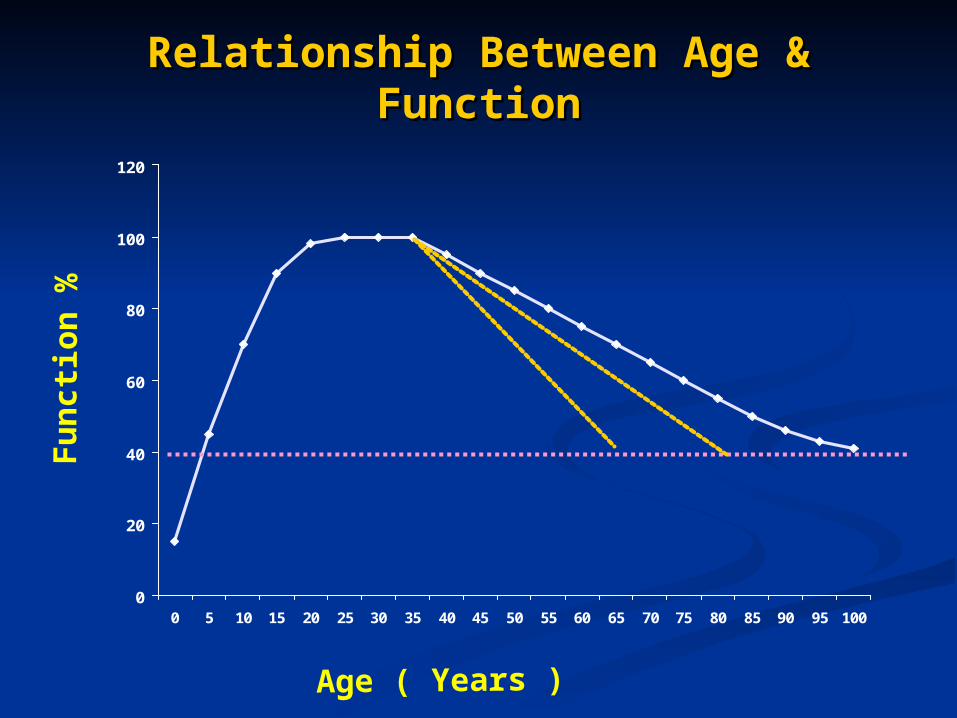
Relationship Between Age & Relationship Between Age & FunctionFunction
0
20
40
60
80
100
120
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Fu
nct
ion
%
Age ( Years )
Factors influencing Factors influencing ManagementManagement
in the Acute Care Settingin the Acute Care SettingHOST AGINGHOST AGING
The stress of illness usually manifests The stress of illness usually manifests itself first and prominantly in the itself first and prominantly in the organs with least functional reserve – organs with least functional reserve – usually the BRAINusually the BRAIN
Atypical presentation of disease (no Atypical presentation of disease (no fever/pain)fever/pain)
Physical variation/heterogeneity of the Physical variation/heterogeneity of the elderly patient – careful and elderly patient – careful and comprehensive individual assessmentcomprehensive individual assessment
‘‘GIANTS OF GIANTS OF GERIATRICS’GERIATRICS’
ATYPICAL PRESENTATION of ATYPICAL PRESENTATION of DISEASEDISEASE
DELIRIUMDELIRIUM FALLSFALLS LOSS OF MOBILITYLOSS OF MOBILITY INCONTINENCEINCONTINENCE LOSS of ADL ABILITYLOSS of ADL ABILITY
Factors influencing Factors influencing ManagementManagement
in the Acute Care Settingin the Acute Care SettingHOST DISEASEHOST DISEASE
Multiple illness/comorbidities are common – on Multiple illness/comorbidities are common – on average 3 per patientaverage 3 per patient
These interact with the changes of aging – further These interact with the changes of aging – further enhance vulnerability to stressenhance vulnerability to stress
Often comorbidities are subtle and nonspecific Often comorbidities are subtle and nonspecific (OA, BPH, Osteoporosis, Apathetic Thyrotoxicosis, (OA, BPH, Osteoporosis, Apathetic Thyrotoxicosis, etc) etc)
Careful delineation of all acute and chronic Careful delineation of all acute and chronic illnesses essentialillnesses essential
Identify the primary illness – place it accurately Identify the primary illness – place it accurately within the context of other illnesses and within the context of other illnesses and vulnerabilities – then investigate and treat vulnerabilities – then investigate and treat appropriatelyappropriately
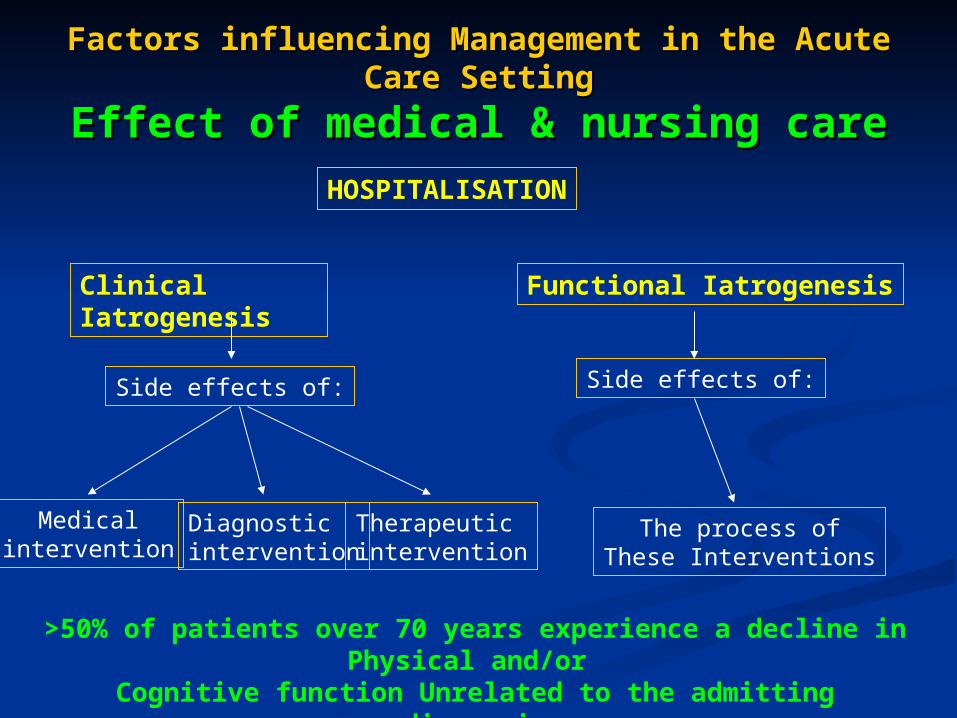
Factors influencing Management in the Acute Factors influencing Management in the Acute Care SettingCare Setting
Effect of medical & nursing careEffect of medical & nursing careHOSPITALISATION
Clinical Iatrogenesis
Functional Iatrogenesis
Side effects of:
Medicalintervention
Diagnostic intervention
Therapeuticintervention
Side effects of:
The process ofThese Interventions
>50% of patients over 70 years experience a decline in Physical and/or
Cognitive function Unrelated to the admitting diagnosis
ATYPICAL DISEASE ATYPICAL DISEASE PRESENTATIONPRESENTATION
MULTIPLE PATHOLOGYMULTIPLE PATHOLOGY
MULTIPLE AETIOLOGYMULTIPLE AETIOLOGY
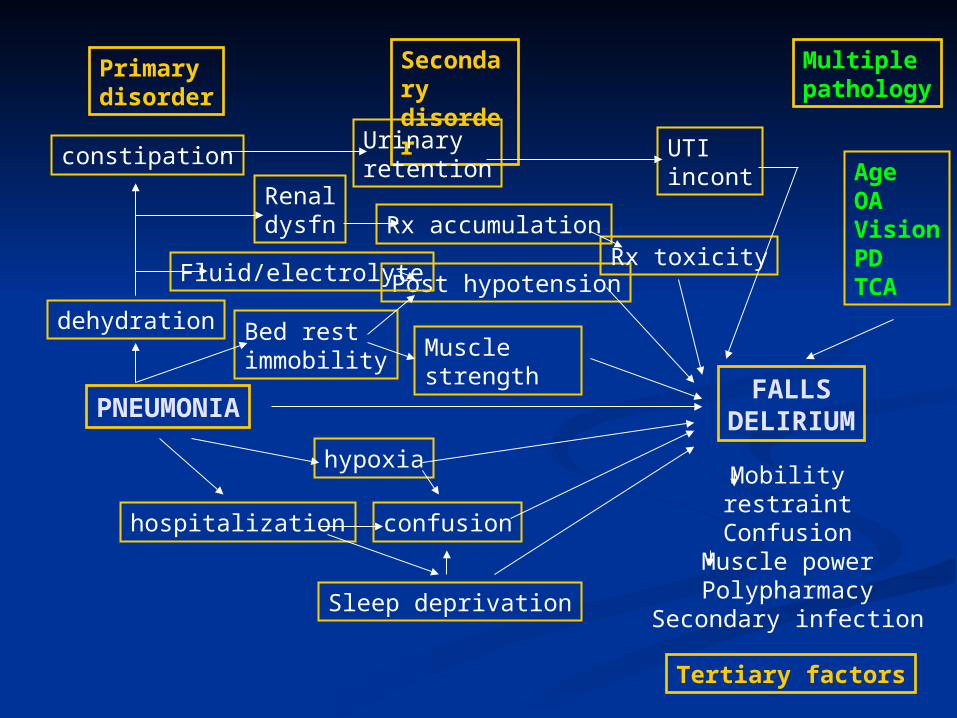
FALLSDELIRIUMPNEUMONIA
Multiplepathology
Primarydisorder
Secondarydisorder
Tertiary factors
Mobilityrestraint
ConfusionMuscle powerPolypharmacy
Secondary infection
Bed restimmobility Muscle
strength
Post hypotension
dehydration
constipationUrinaryretention
UTIincont
Renaldysfn
Fluid/electrolyte
Rx accumulationRx toxicity
hypoxia
hospitalization
Sleep deprivation
confusion
AgeOAVisionPDTCA
LESSONS LEARNEDLESSONS LEARNED
FAILURE TO LOOK BEYOND THE FAILURE TO LOOK BEYOND THE OBVIOUSOBVIOUS
AVALANCHE EFFECTAVALANCHE EFFECT SUPERMARKET EFFECTSUPERMARKET EFFECT
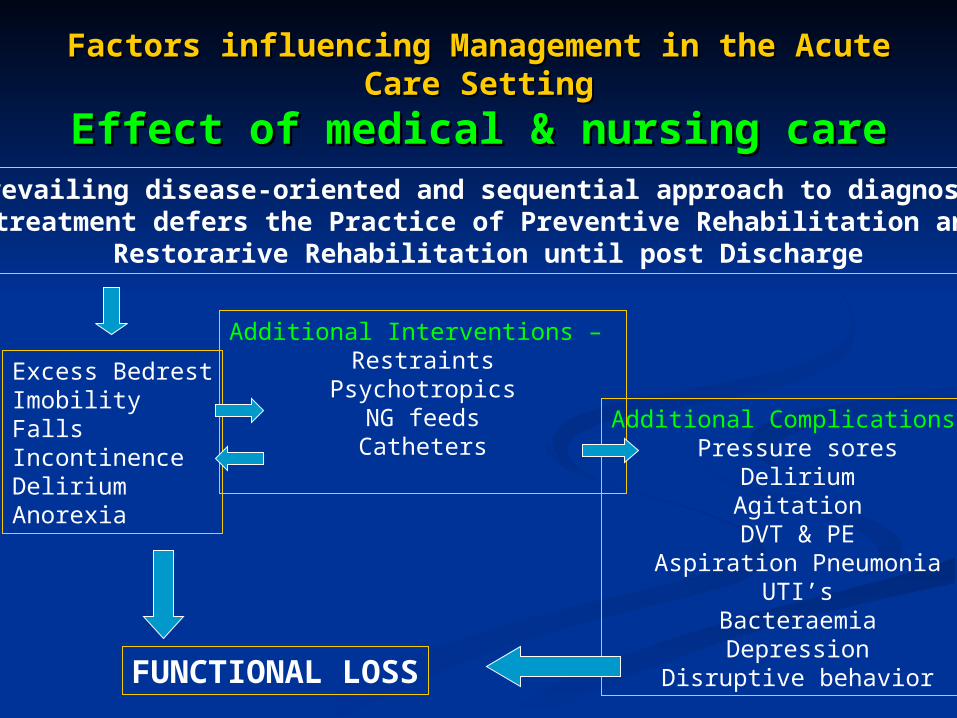
Factors influencing Management in the Acute Factors influencing Management in the Acute Care SettingCare Setting
Effect of medical & nursing careEffect of medical & nursing careThe prevailing disease-oriented and sequential approach to diagnosis and
treatment defers the Practice of Preventive Rehabilitation and Restorarive Rehabilitation until post Discharge
Excess BedrestImobilityFallsIncontinenceDeliriumAnorexia
Additional Complications -Pressure sores
DeliriumAgitationDVT & PE
Aspiration PneumoniaUTI’s
BacteraemiaDepression
Disruptive behavior
Additional Interventions – Restraints
PsychotropicsNG feedsCatheters
FUNCTIONAL LOSS
Acute Care Acute Care Assessment and Assessment and
ManagementManagement
Prehospital AssessmentPrehospital Assessment Admission AssessmentAdmission Assessment Acute Hospital CareAcute Hospital Care Discharge PlanningDischarge Planning
Acute Care – assessment and Acute Care – assessment and managementmanagement
Prehospital AssessmentPrehospital Assessment
Comprehensive Geriatric Assessment – detailed knowledge of:Coexistant medical problems
Nutritional statusPsychosocial strengths and vulnerabilities
Baseline Physical & Cognitive Function
Allows prediction of outcomes
Attempt to prevent unnecessary or inapproriate admissionsIt is possible to manage most illness as an outpatient!
You want my mother who has pneumonia to stay at home!!!
Is your medical insurance paid up?
Educate patient and carerCarer support and assistance
Appropriate and aggressive treatment for the acute illnessRegular follow up and reassessment
NutritionFluid and Electrolytes (subcutaneous fluids)
PREVENTIVE REHABILITATION
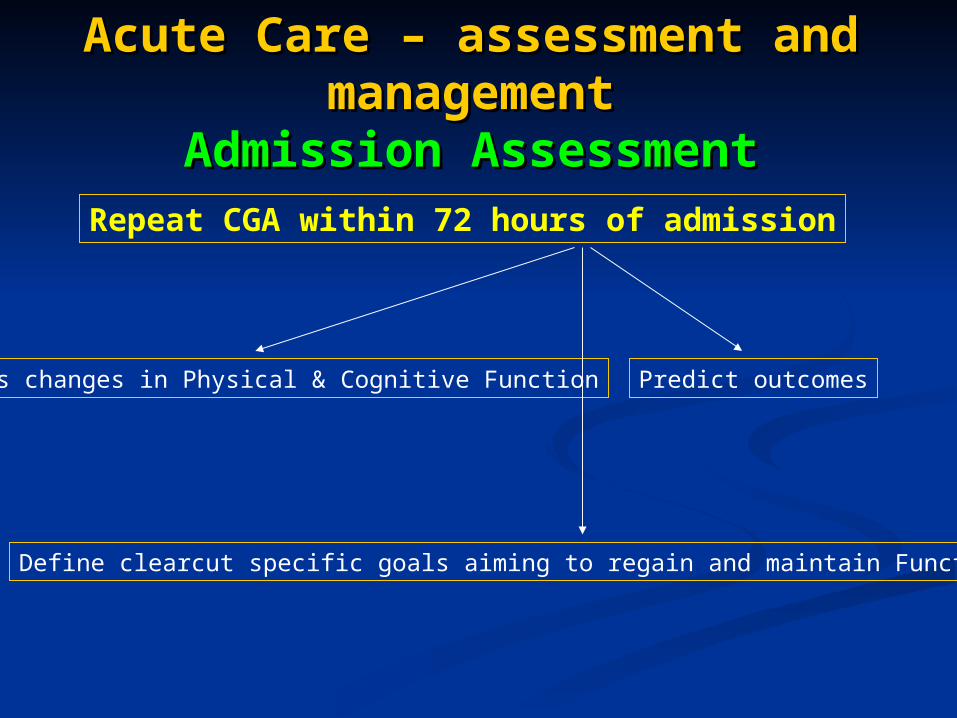
Acute Care – assessment and Acute Care – assessment and managementmanagement
Admission AssessmentAdmission AssessmentRepeat CGA within 72 hours of admission
Assess changes in Physical & Cognitive Function Predict outcomes
Define clearcut specific goals aiming to regain and maintain Function
Acute Care – assessment and Acute Care – assessment and managementmanagement
Acute Hospital CareAcute Hospital Care Identify acute event – accurately place this Identify acute event – accurately place this
within the context of other diseases and within the context of other diseases and disabilities…..then initiate appropriate disabilities…..then initiate appropriate investigations and interventionsinvestigations and interventions
Avoid the acute functional and cognitive decline Avoid the acute functional and cognitive decline associated with acute medical and nursing care.associated with acute medical and nursing care.
Close collaboration by the treating TEAM is Close collaboration by the treating TEAM is essentialessential
Allow the patient to retain maximal levels of self Allow the patient to retain maximal levels of self care, personal control, mobility, nutritioncare, personal control, mobility, nutrition
Retain basic daily functions while in hospital Retain basic daily functions while in hospital
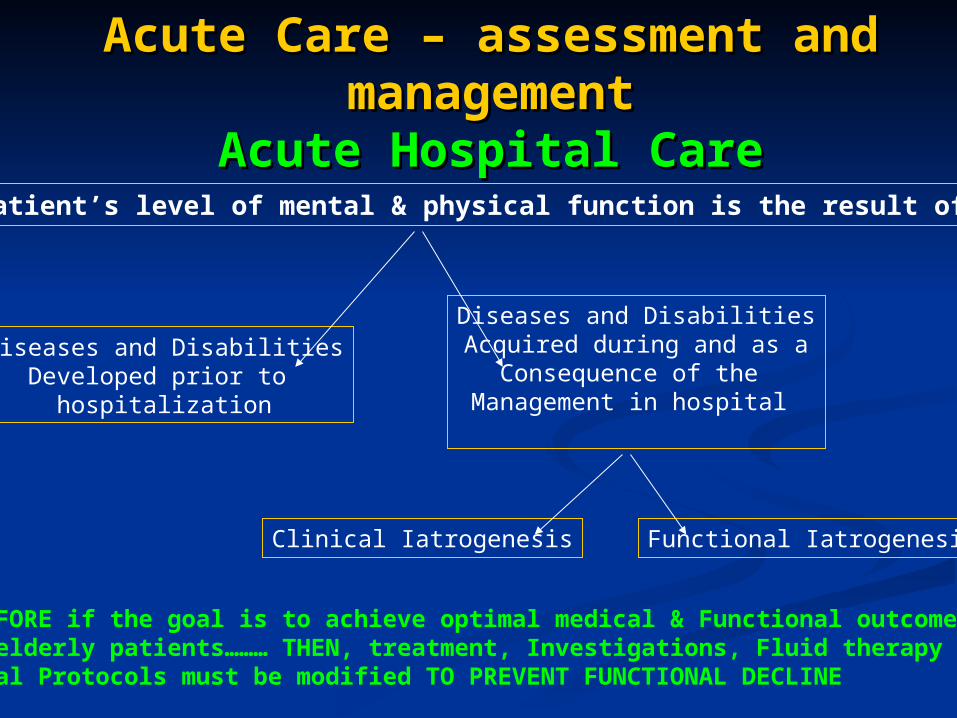
Acute Care – assessment and Acute Care – assessment and managementmanagement
Acute Hospital CareAcute Hospital CareA patient’s level of mental & physical function is the result of :
Diseases and DisabilitiesDeveloped prior to
hospitalization
Diseases and DisabilitiesAcquired during and as a
Consequence of the Management in hospital
Clinical Iatrogenesis Functional Iatrogenesis
THEREFORE if the goal is to achieve optimal medical & Functional outcomes for elderly patients……… THEN, treatment, Investigations, Fluid therapy and General Protocols must be modified TO PREVENT FUNCTIONAL DECLINE
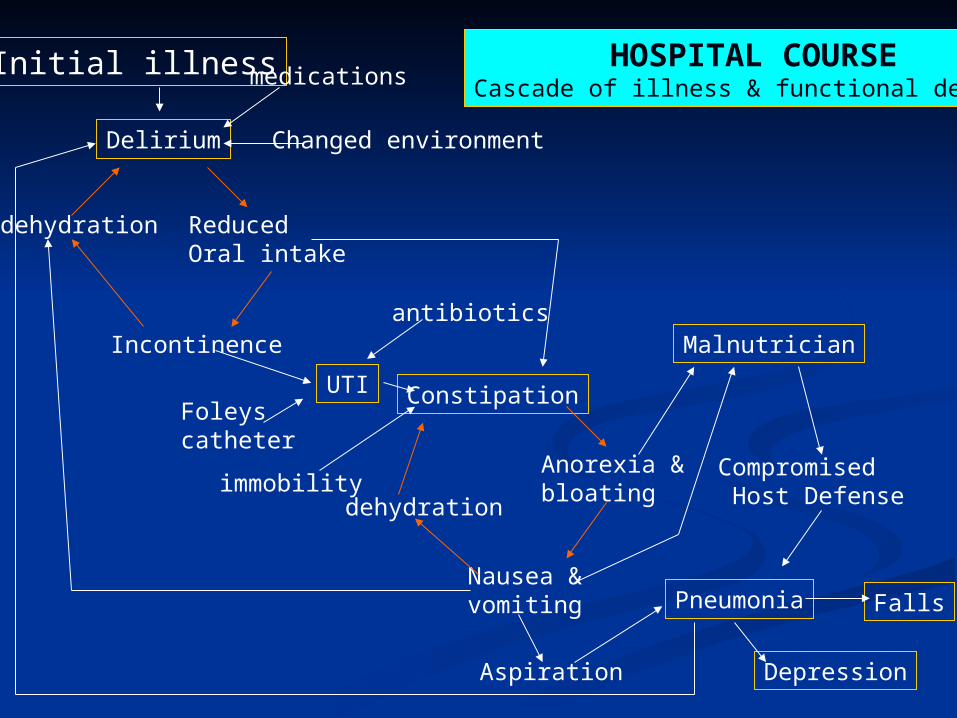
Initial illness
Delirium
medications
Changed environment
dehydration ReducedOral intake
Incontinence
UTIFoleyscatheter
antibiotics
Constipation
immobilitydehydration
Nausea &vomiting
Anorexia &bloating
Malnutrician
Compromised Host Defense
Pneumonia
DepressionAspiration
HOSPITAL COURSECascade of illness & functional decline
Falls
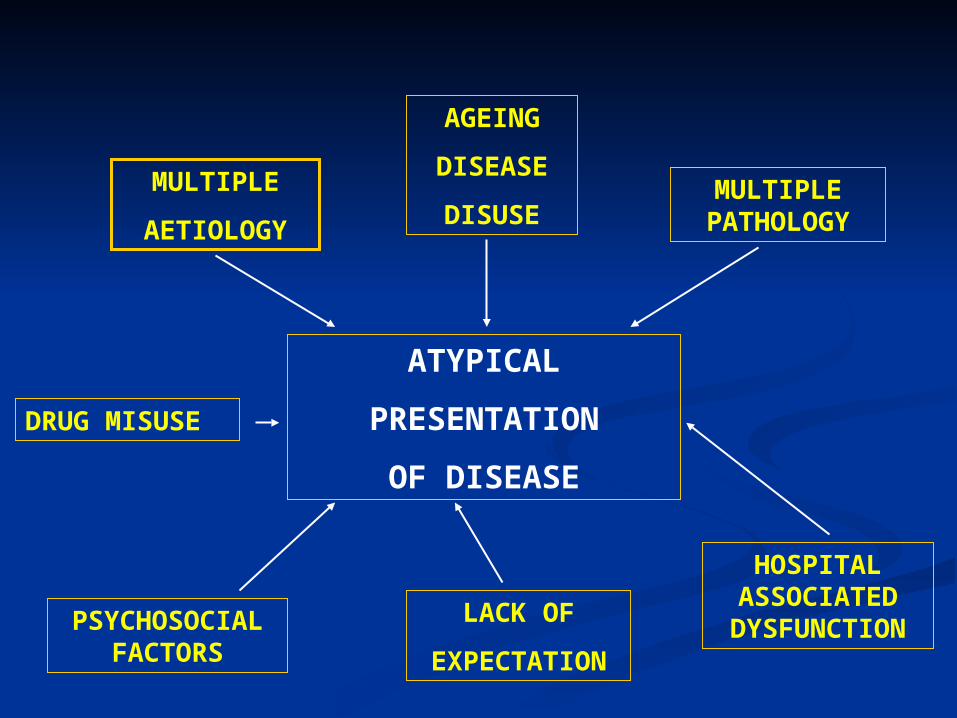
ATYPICAL
PRESENTATION
OF DISEASE
PSYCHOSOCIAL FACTORS
DRUG MISUSE
MULTIPLE
AETIOLOGY
MULTIPLE PATHOLOGY
AGEING
DISEASE
DISUSE
HOSPITAL ASSOCIATED
DYSFUNCTIONLACK OF
EXPECTATION
Acute Care – assessment and Acute Care – assessment and managementmanagement
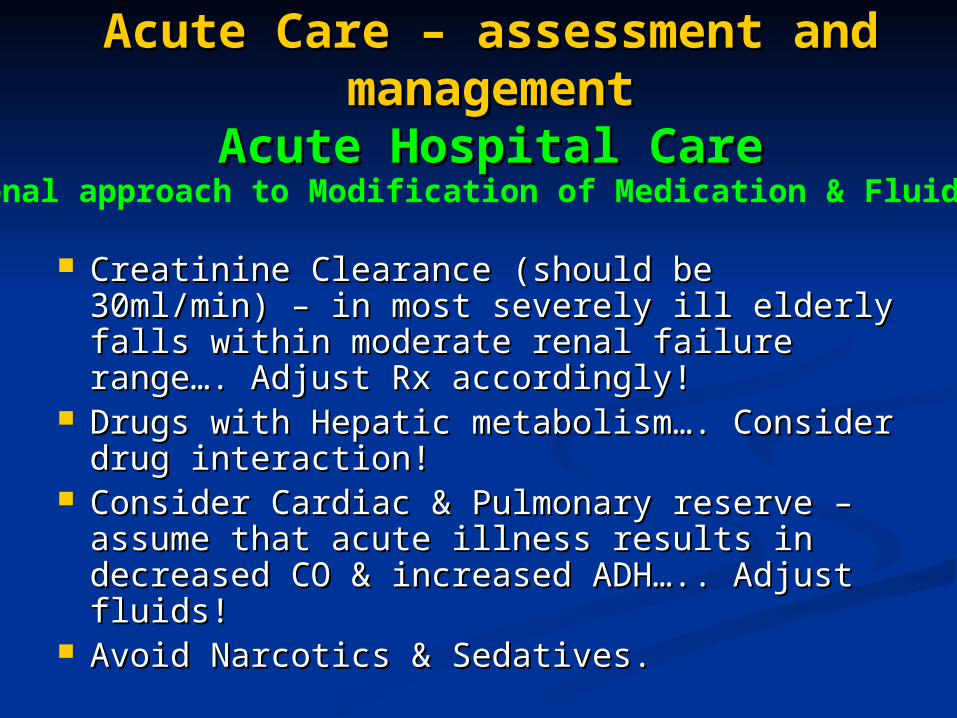
Acute Hospital CareAcute Hospital Care
Creatinine Clearance (should be 30ml/min) – Creatinine Clearance (should be 30ml/min) – in most severely ill elderly falls within in most severely ill elderly falls within moderate renal failure range…. Adjust Rx moderate renal failure range…. Adjust Rx accordingly!accordingly!
Drugs with Hepatic metabolism…. Consider Drugs with Hepatic metabolism…. Consider drug interaction!drug interaction!
Consider Cardiac & Pulmonary reserve – Consider Cardiac & Pulmonary reserve – assume that acute illness results in decreased assume that acute illness results in decreased CO & increased ADH….. Adjust fluids!CO & increased ADH….. Adjust fluids!
Avoid Narcotics & Sedatives.Avoid Narcotics & Sedatives.
Rational approach to Modification of Medication & Fluids
Acute Care – assessment and Acute Care – assessment and managementmanagement
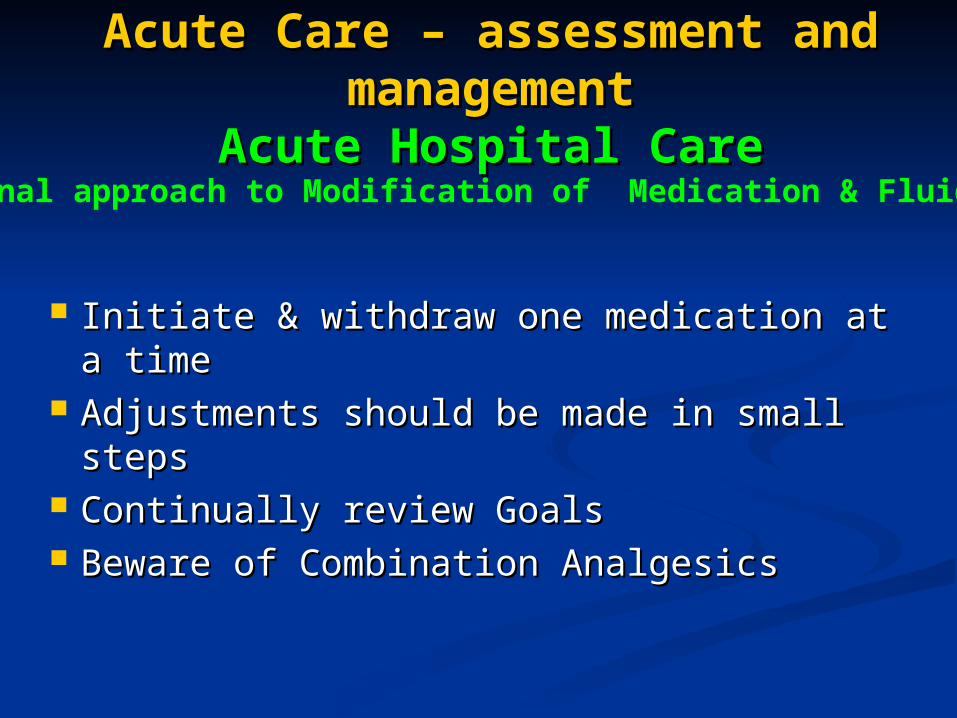
Acute Hospital CareAcute Hospital Care
Initiate & withdraw one medication at a Initiate & withdraw one medication at a timetime
Adjustments should be made in small Adjustments should be made in small stepssteps
Continually review GoalsContinually review Goals Beware of Combination AnalgesicsBeware of Combination Analgesics
Rational approach to Modification of Medication & Fluids
Acute Care – assessment and Acute Care – assessment and managementmanagement
DischargeDischarge DISCHARGE PLANNING begins at the DISCHARGE PLANNING begins at the
time of ADMISSION!time of ADMISSION! Regular TEAM MEETINGS – Doctor, Regular TEAM MEETINGS – Doctor,
Nurses, Social Worker, Physiotherapist, Nurses, Social Worker, Physiotherapist, Occupational Therapist, Community Occupational Therapist, Community Nurse etcNurse etc
At all times consider and avoid functional At all times consider and avoid functional and cognitive decline consequent to and cognitive decline consequent to hospitalizationhospitalization
Education of CAREGIVERS – Education of CAREGIVERS – DISCHARGE MEETINGSDISCHARGE MEETINGS
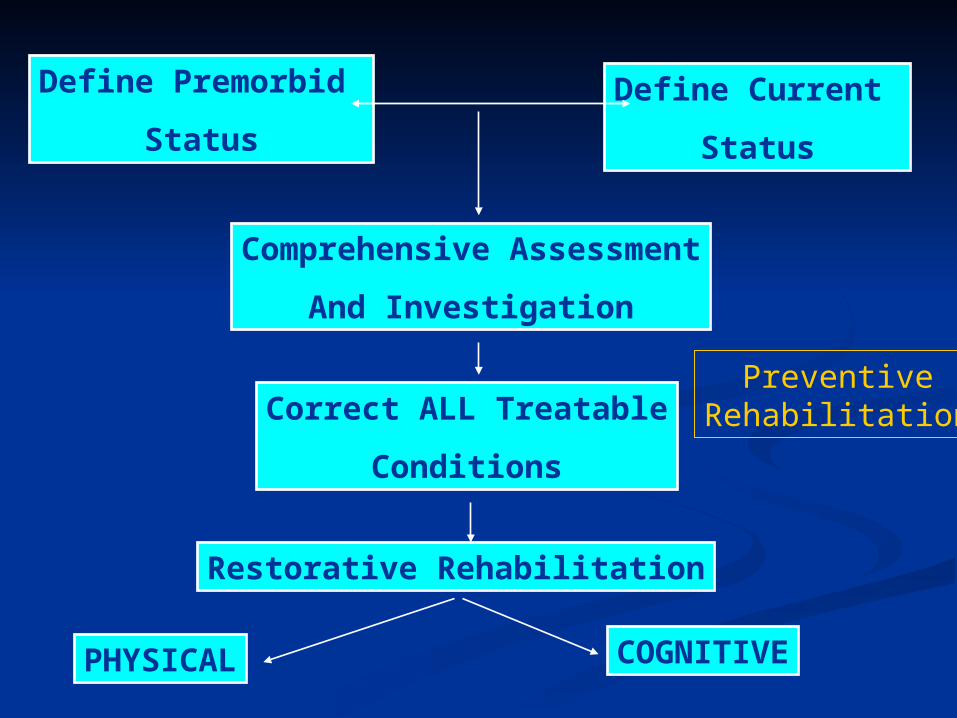
Define Premorbid
Status
Define Current
Status
Comprehensive Assessment
And Investigation
Correct ALL Treatable
Conditions
Restorative Rehabilitation
PHYSICAL COGNITIVE
PreventiveRehabilitation
Weeks 2 & 3Weeks 2 & 3Case StudiesCase StudiesHalf hour presentationsHalf hour presentations
At week 4At week 4
Case study and Treatment Case study and Treatment plan to be plan to be
Handed in for assessmentHanded in for assessment