Embed Size (px)
Citation preview

Pathophysiologic mechanisms :Transient lower esophageal sphincter relaxations (tLESRs)A hypotensive lower esophageal sphincter (LES)Anatomic disruption of the gastro esophageal junction, often associated with a hiatal hernia


Heart burn and regurgitation are The most common symptoms
How the “Heartburn” recognised?

Gastro-esophageal Refluks Disease (GERD)
Esophageal syndromes Extra-Esophageal syndromes
Symptomaticsyndromes
ProposedAssociation
Syndromes with Esophageal injury
Established association
1. Typical reflukssyndrome
2. Refluks chestpain syndrome
1. Refluks esophagitis2. Refluks stricture3. Barret’s esophagus4. Esophageal
Adenocarcinoma
1. Refluks cough syndrome
2. Refluks laryngitis syndrome
3. Refluks astmasyndrome
4. Refluks dental erosion syndrome
1. Pharyngitis2. Sinusitis3. Idiopathic
Pulmonary fibrosis4. Recurrent otitis
media
(Vakil etal., Am J Gastroenterol 2006; 101:1900-1920)

Progressive dysphagiaOdynophagiaWeight loss (unintentional)Anemia (new onset)Hematemesis and/or melenaFamily history of gastric and/or esophageal cancerChronic non-steroid anti-inflammatory drug useAge >40 years in areas of a high prevalence of gastric cancer

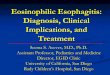
esofagitis esofagitis
normal
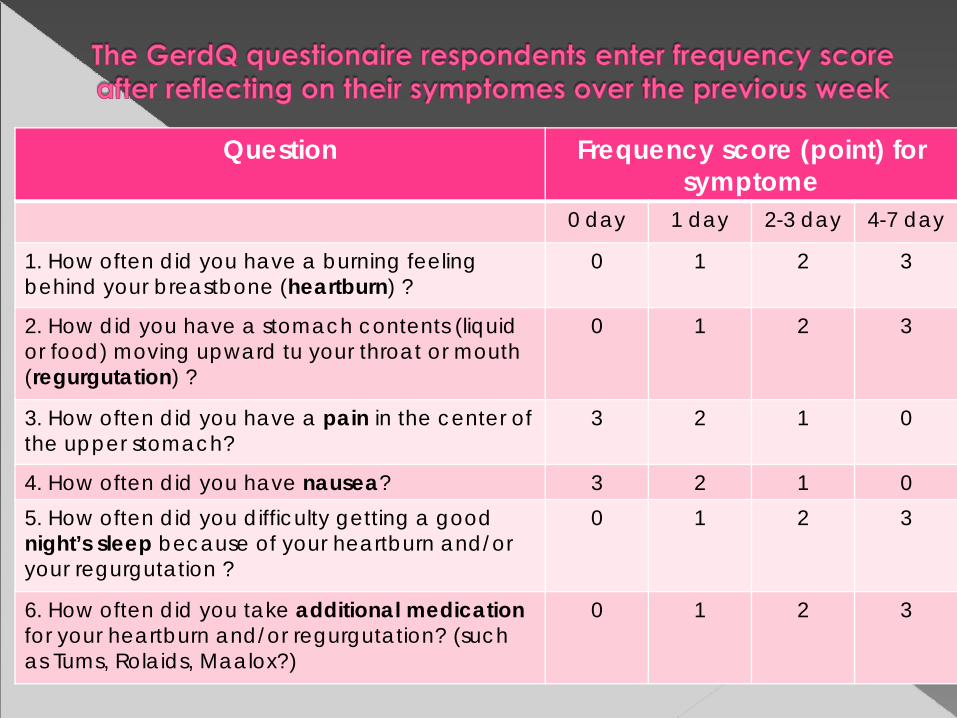
Question Frequency score (point) forsymptome
0 day 1 day 2-3 day 4-7 day
1. How often did you have a burning feeling behind your breastbone (heartburn) ?
0 1 2 3
2. How did you have a stomach contents (liquid or food) moving upward tu your throat or mouth (regurgutation) ?
0 1 2 3
3. How often did you have a pain in the center of the upper stomach?
3 2 1 0
4. How often did you have nausea? 3 2 1 05. How often did you difficulty getting a good night’s sleep because of your heartburn and/or your regurgutation ?
0 1 2 3
6. How often did you take additional medicationfor your heartburn and/or regurgutation? (such as Tums, Rolaids, Maalox?)
0 1 2 3

Alarm features
present
Alarm features
absent
PPI therapy 4 week andReview at 2 to 4 week
Symptomes persist
Symptomes respond
Trial forStop PPI
Relapse
RestartPPI
On-demand therapy
Frequent relapse, orAlarm features
Stop PPI atleast 1 week
REFER forEGD or
H.pylori test

... and “step down” dosing

Conclusion:-On-demand therapy is a useful option in GERD but needs to be limited to selectedpatients
-Severe Grade of esophagitis and Barret’s esophagus are best managed with continuous therapy
(Gjostedt et al. Aliment Pharmacol Ther 2005. 22: 183-91)


Patophysiologi of gastric-doodenal mucosa injury

Hp associated ulcer and cancer

NSAIDs associated ulcer and gastric erosion

Alterations in gastric mucosal barrier↓ Prostaglandin synthesis↓ Mucus and bicarbonate secretion↓ Submucosal blood flow↓ Mucosal ATP↓ Cell turnover↓ Platelet function (irreversible)
Ivey KJ. Am J Med. 1988;84:41-48.

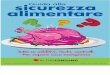
Ulkus antrum Ulkus duodenum
gastropathy

Singh G et al G. Epidemiology of NSAID-induced GI complications. J Rheumatol 1999;26:Sup 26:18-24.
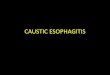
1997 US mortality data for seven selected disorders
0
5000
10,000
15,000
20,000
25,000Number of deaths
NS
AID
The ‘silent epidemic’
16500
Wolfe et al Gastrointestinal Toxicity of Nonsteroidal Antiinflammatory Drugs. NEJM 1999; 340: 1888-99.

male non-users
female users
male users
Hospitalisations/1000 person-years
20 30 40 50 60 70 80
20
15
10
5
0
25
female non-users
Age (years)
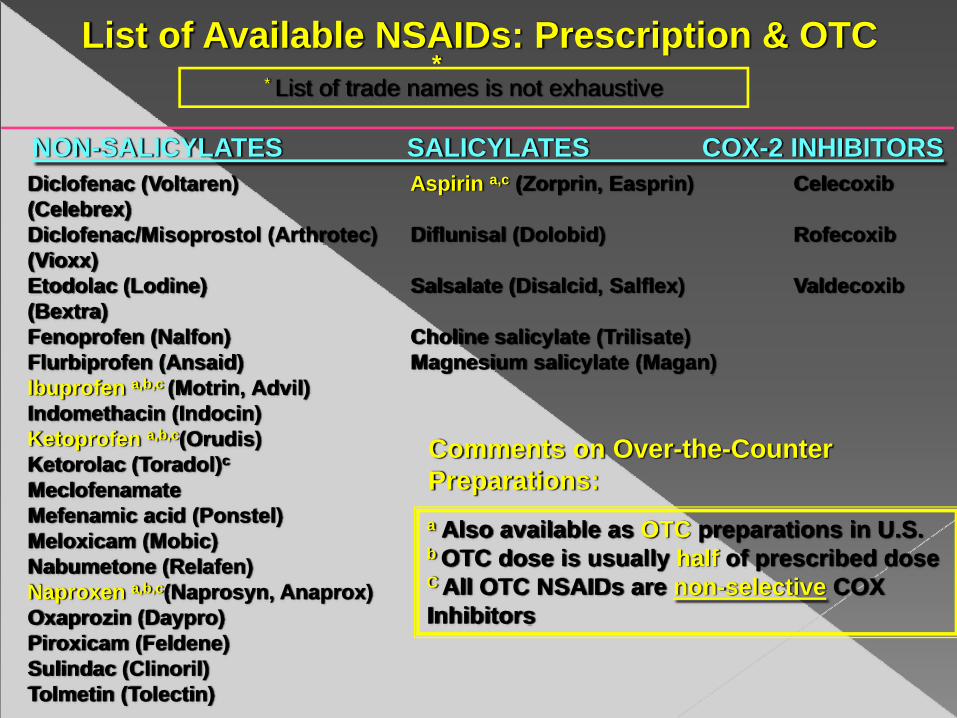
List of Available NSAIDs: Prescription & OTC *
NON-SALICYLATES SALICYLATES COX-2 INHIBITORSDiclofenac (Voltaren) Aspirin a,c (Zorprin, Easprin) Celecoxib(Celebrex)Diclofenac/Misoprostol (Arthrotec) Diflunisal (Dolobid) Rofecoxib(Vioxx)Etodolac (Lodine) Salsalate (Disalcid, Salflex) Valdecoxib(Bextra)Fenoprofen (Nalfon) Choline salicylate (Trilisate)Flurbiprofen (Ansaid) Magnesium salicylate (Magan)Ibuprofen a,b,c (Motrin, Advil) Indomethacin (Indocin)Ketoprofen a,b,c(Orudis) Ketorolac (Toradol)c
MeclofenamateMefenamic acid (Ponstel)Meloxicam (Mobic)Nabumetone (Relafen)Naproxen a,b,c(Naprosyn, Anaprox)Oxaprozin (Daypro)Piroxicam (Feldene)Sulindac (Clinoril)Tolmetin (Tolectin)
a Also available as OTC preparations in U.S.b OTC dose is usually half of prescribed doseC All OTC NSAIDs are non-selective COX Inhibitors
* List of trade names is not exhaustive
Comments on Over-the-Counter Preparations:

PPI (omeprazole 20-40mg 1x1/d) >PGE1, Misoprostol (cytotec 200 μg 1x3/d) >H2 receptor antagonist (famotidine 40mg 1x2/d or ranitidine 300 mg 1x2/d)
Misoprostol good for prevention of gastric ulcer but causes diarrhea

Algoritm of dyspepticpatients

• Diagnosis and outcome assessment by urea breath test (off PPIs) if endoscopy not required.
• Serology least sensitive and specific• Therapy should be according to best
practice, not ad hoc combinations• If first line failure, don’t retreat with the
same combination- use proven 2nd line Rx• Consider PPI prophylaxis selectively

1st line therapy in
Asia
Standard PPI – based triple therapy : 7-14 days› PPI, amoxicillin 1 g, clarithromycin 500 mg twice daily› PPI, metronidazole 400 mg, clarithromycin 500 mg
twice daily› PPI, amoxicillin 1 g, metronidazole 400 mg twice
dailyQuadriple therapy: 7–14 days› PPI twice daily, bismuth 240 mg twice daily,
metronidazole 400 mg twice daily or three times daily, tetracycline 500 mg four times daily
Levofloxacin-based triple therapy: 10 days› PPI, levofloxacin 250 mg (or 500 mg), amoxicillin 1 g
twice dailyRifabutin-based triple therapy: 7–10 days› PPI, rifabutin 150 mg, amoxicillin 1 g twice daily
Fock KM, et al. Journal of Gastroenterology and Hepatology 24 (2009) 1587–1600

Adapted from Fendrick. Am J Manag Care 2004; 10: 740-741 and Sung JGH 2010; 25: 229-33
H. pylori test and treat
LowNSAID gut risk
HighNSAID gut risk
Low CV risk(No aspirin)
High CV risk(On aspirin)
Consider non-NSAID therapy
Non-selective NSAID
Consider non-NSAID therapy orNon-selective NSAID + PPIorCOX-II NSAID (±PPI) or
Consider non-NSAID therapy
or
Non-selective NSAID + PPI
or
Avoid NSAIDs
Consider non-NSAID therapy
or
Non-selective NSAID
(naproxen)
± PPI

H.pylori : the Maastricht III Consensus Report
RecommendationsLevel of
evidenceGrade of
recommendationPU (active or inactive) including past bleeding: eradicate H pylori (includes prior to NSAID use)
In naïve users of NSAIDs (without prior PU), H pylorieradication may prevent peptic ulcer and or bleeding
Chronic NSAID users: H pylori eradication of value but is insufficient to prevent NSAID related ulcers completely
Long term NSAID users with PU and/or ulcer bleeding, PPI maintenance is better than H pylorieradication in preventing ulcer recurrence
1a
1b
1b
1b
A
A
A
A
Malfertheiner P et al. Gut 2007; 56: 772-78.

H. pylori infection should be tested for and eradicated:
• Prior to long-term aspirin or NSAID therapy in patients at high risk for ulcers and ulcer-related complications
• To reduce the risk of peptic ulcer and upper gastrointestinal bleeding in NSAID-naive users
Second Asia–Pacific Consensus Guidelines for Helicobacter pylori infection 2009
Fock KM, et al. Journal of Gastroenterology and Hepatology 24 (2009) 1587–1600



Feature of Gastric acid secretion