Embed Size (px)
DESCRIPTION
Eosinophilic Esophagitis Presented by Sadudee boonmee, MD.
Citation preview

Eosinophilic Esophagitis : Diagnosis and Management
Sadudee Boonmee Klakayan, MD

Outline• Prevalence• Diagnosis• Clinical presentation • Endoscopic and Histologic finding• Allergic evaluation• Treatment
- Dietary- Pharmacotherapy- Esophageal dilatation

Prevalence
• Atopic male (male/female ratio 2:1 to 3:1) presents in childhood or during the third or fourth decades of life
• White, non-Hispanic• Prevalence is increasing with rate 6-30
cases/100,000 • EoE in the United States 52/100,000
LIACOURAS ET AL,J Allergy Clin Immunol 2011;128:3-20.

Pathogenesis
Current Opinion in Allergy and ClinicalImmunology 2010, 10:231–237

Definition
• A chronic, immune/ antigen-mediated esophageal disease characterized clinically by
- symptoms related to esophageal dysfunction
- histologically by eosinophil-predominant inflammation
LIACOURAS ET AL,J Allergy Clin Immunol 2011;128:3-20.

Diagnosis1. Symptoms related to esophageal dysfunction2. One or more esophageal biopsy specimens
show 15 Eo/hpf (peak value) (minimum threshold for a diagnosis of EoE)
3. Disease is isolated to the esophagus (other causes of esophageal eosinophilia should be excluded )
4. Disease remit with treatments of dietary exclusion, topical corticosteroids, or both

Eosinophil associated Esophagitis
( Rothenberg, J Allergy Clin Immunol 2004;113:11-28.)

LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

Most common clinical manifestration Age Clinical presentation
Infant and Toddlers feeding difficulties,feeding refusal or intolerance, irritability, vomiting,failure to thrive
School-aged children Abdominal pain, vomiting, GERD-like symptoms,difficulty swallowing, food aversion/self-limited diet, failure to thrive
Adolescents Dysphagia, esophageal food impactions, nausea,GERD-like symptoms, self-limited diet
Adult Dysphagia, esophageal food impactions
Mirna Chehade and Seema S. AcevesCurrent Opinion in Allergy and ClinicalImmunology 2010, 10:231–237

Clinical Manifestration
• Adult : Steriotypical symptom- Dysphagia- Chest pain - Food impaction - Upper abdominal pain
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

• Patients presenting with dysphagia in endoscopy units, EoE has prevalence up to 12% to 15%
• Food impaction is common in patients with histologic evidence consistent with EoE high as 40% at a median follow-up of 15 years
• Food impaction necessitating endoscopic bolus removal occurs in 33% to 54% of adults with EoE
Am J Gastroenterol 2007;102(12):2627–32.
J Allergy Clin Immunol 2011;128:132-8.
Gastrointest Endosc 2005;61:795-801

• Any pt with symptom suggestive of EoE should undergo careful history focus on eating and swallowing habits
• Children and adult with EoE often rapidly adapt eating habits to manage their impaired esophageal function
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

EoE vs GERD
( Rothenberg, J Allergy Clin Immunol 2004;113:11-28.)

LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20. LIACOURAS ET AL J Allergy Clin Immunol
2011;128:3-20.

Endoscopic Finding
• Esophageal endoscopy with biopsy reliable diagnostic test for EoE
• Appropriate clinical setting + any endoscopic finding supports but not establish the Dx of EoE
• 2 to 4 mucosal specimens of the proximal and distal esophagus should be obtain

Endoscopic Finding• Fixed esophageal rings (corrugated rings or
trachealization) • Transient esophageal rings (feline folds or
felinization), • Whitish exudates• Longitudinal furrows• Edema • Diffuse esophageal narrowing• Narrow-caliber esophagus• Esophageal lacerations by passage of the
endoscope
Can be predictive but not pathognomonic for EoE

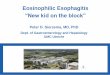
Normal Esophagous Esophageal furrowing
White mucosal plaques

Esophageal ring trachealization
Small-caliber esophagus with mucosal tearing after endoscopy

Radiography
• Not a recommended routinely • Helpful in selected cases
anatomic abnormalities difficult to endoscopeesophageal strictures (length and diameter)
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

Histologic Finding
• At least 15 Eo/HPF in the maximally affected esophageal tissue
• Histopathologic features of esophageal mucosal biopsy must be interpreted in with the patient’s clinical information
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

Histologic FindingMucosal eosinophilia
Eosinophil microabscess formation
Superficial layering of eosinophils
Extracellular eosinophil granules
Epithelial desquamation
Basal zone hyperplasia
Rete peg elongation
Dilated intercellular spaces
Subepithelial fibrosis/sclerosis–lamina propria fibrosis
Mastocytosis and mast cell degranulation
CD8+ lymphocytes and B cells
Typical finding associated with EoE > GERD

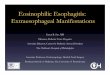
Normal esophagous EoE
Superficial layering of surface Eo Microabcess

Distinguishing Eosinophilic Esophagitis inPediatric Patients
• Retrospective case-control study• Children with esophageal eosinophilic inflammation who underwent esophageal biopsy ( EoE and non EoE)
J Clin Gastroenterol Volume 41, Number 3, March 2007
Eo > 20/hpf

Histologic Finding
• EoE might be focal and not be present in all biopsy specimens
• Peak number vs average number of Eo/hpf• Site and number of biopsy Affect Eo count
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

• Esophageal pH monitoring (and pH impedance ) useful diagnostic test to evaluate for GERD in patients with esophageal eosinophilia
• Peripheral eosinophil counts: patients EoE, 40% to 50% having increased numbers of circulating eosinophils (>300-350 per mm3)
• Total IgE : inadequate data to support the measuring the total IgE level as a surrogate disease in patients with EoE.

Allergic evaluation
• EoE is an antigen-driven allergic condition• EoE patient
- 28% to 86% of adults- 42% to 93% of pediatric
• 50% to 60% of patients with EoE have a prior history of atopy
• Major of patients have sensitization to food allergens, aeroallergens, or both (SPT or Specific IgE )
Have another allergicdisease
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

nejm 2004 351(9) 940-941

Evaluation of aeroallergen sensitization
• Aeroallergen-specific IgE44% to 86% of patients have serum IgE to outdoor, indoor, or both aeroallergens
• SPT to aeroallergen (pediatric and adult) - outdoor aeroallergens (grass, weeds, trees, and molds) 64% to 93%- indoor aeroallergens (dog, cat, cockroach, and dust mites) 16% to 69%
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

Studies Atopic disease
Evidence of IgE to Aeroallergen
Evidence of IgE to Food
Aceves et al,J Clin Gastroenterol Vol 41, No 3, March 2007
Asthma 47%AR 40 %Eczema 4%
+ aeroallergen RAST 44%
+ food RAST 60%
Collins et al,Clin Gastro and Hepato Vol. 6, No. 6
Asthma 52%AR 68 %Eczema 44%AC 56 %
+ SPT aeroallergen 71%
+ SPT food 76%
ROY–GHANTA et al,Clin Gastro and Hepato Vol. 6, No. 5
Asthma 26%AR 78%AD 4%
Specific IgE aeroallergen 86% ( Birch pollen ,Timothy ryegrass pollen Ragweed pollen , dust mite Pet dander )
Specific IgE for food 83%

Is There a Seasonal Variation in the Incidence orIntensity of Allergic Eosinophilic Esophagitis in
Newly Diagnosed Children?
Winter had significantly fewer newly diagnosed patientswith AEE when compared with Spring, Summer, and Fallindividually (P=0.0008, P=0.0001, P=0.0118,respectively)
Flint Y. J Clin Gastroenterol 2007;41:451–453

Seasonal Distribution in Newly Diagnosed Cases ofEosinophilic Esophagitis in Adults
signifi cant increase of EoE cases in spring and summer months ( n = 28) when compared with the fall and winter months ( n = 13) ( P = 0.019)
Am J Gastroenterol 2009; 104:828 – 833;

• Complete evaluation of patients with EoE for aeroallergen sensitization might alter clinical management.
LIACOURAS ET AL J Allergy Clin Immunol 2011;128:3-20.

Evaluation of Food sensitization
• Food - specific IgE- 50% of adult with EoE had positive at least 1 food, most common peanut 38%, egg 27%, and soy 23% Penfiel JD et al , J Clin
Gastroenterol 2010; 44:22-7

Atopic diseaseAeroallergen Specific IgE Food specific IgE
Aceves et alJ Clin Gastroenterol Vol 41, No 3, March 2007
Asthma 47%AR 40 %Eczema 4%
+ aeroallergen RAST 44% + food RAST 60%
COLLINS ET ALClin Gastro and Hepato Vol. 6, No. 6
Asthma 52%AR 68 %Eczema 44%AC 56 %
+ SPT aeroallergen 71% + SPT food 76%
ROY–GHANTA ET ALClin Gastro and Hepato Vol. 6, No. 5
Asthma 26%AR 78%AD 4%
Specific IgE aeroallergen 86% ( Birch pollen ,Timothy ryegrass pollen Ragweed pollen , dust mite Pet dander )
Specific IgE for food 83%

CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:531–535

Serum IgE measurement and detection of foodallergy in pediatric patients with eosinophilic
esophagitis• serum IgE measurement detected more positive results than did skin prick testing. Specific IgE to milk was most common (43%)
• low-titer IgE antibody may be useful in identifying relevant food sensitivities making a more directed approach to food avoidance possible
Ann Allergy Asthma Immunol. 2010;104:496 –502.

SPT vs APT
• mix of immunoglobulin E (IgE)-mediated and non-IgE (cell mediated) hypersensitivity responses
• Results from skin prick testing (SPT) and atopy patch testing (APT) may help to identify foods that contribute to the disease process, and removal of identified foods can be an effective treatment,

• High rates of food allergies in pt with EoE serum IgE and skin prick testing is warranted to identify comorbid food-induced allergic disease in patients with EoE
• SPTs, serum IgE, and food patch tests can use to identify foods that associated with EoE, but not sufficient to make the diagnosis of food allergy–driven EoE
SPT vs APT

Treatment
Diet therapy • Elemental diet : complete elimination of
dietary antigen and use amino acid formula

Patient Intervention Outcome
Markowitz et al. Am JGastroenterol Vol. 98, No. 4, 2003
51 with Dx EoE
(age 3-16 yr mean 8.3 yr )
•elemental diet (Neocate ) for 1 month •allowed to take water and one fruit (grape or apple)
• improve in vomiting, abd pain, & dysphagia •Esoeos/hpf 33.7 1.0 after thediet (p 0.01).
Chris A. Liacouras et al. Clin Gastroentrol Hepato 2005;3:1198–1206
10 yr study of 381 patients (66% male, age 9.1 + - 3.1 yr) Dx with EoE
• dietary restriction (if SPT of APT to food + )
• completedietary elimination (if can’t identified food allergy )
Neocate, Neocate EO28, Neocate 1, Elecare

esophageal eosinophils & No. of patients complaining of clinical symptoms before& 1 month after the initiation of dietary therapy
Chris A. Liacouras et al. Clin Gastroentrol Hepato 2005;3:1198–1206

Treatment
• Elimination diet • elimination of certain food allergens
Restrict most common food allergens VS
Restrict proteins based on allergy testing

Effect of Six-Food Elimination Diet on Clinical and Histologic Outcomes in Eosinophilic Esophagitis
• Retrospective observational study of children and adolescence were Dx EoE in 2 cohort study • 35 pt with SFED * 6 wk (SFED : CM,egg,soy,wheat,peanut/treenut,fish)• 25 pt with elemental diet (aminoacid formula * 6 wk )
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1097–1102

Effect of Six-Food Elimination Diet on Clinical and Histologic Outcomes in Eosinophilic Esophagitis
• SFED treatment associated with clinical & histologic improvement
• offers advantages of better acceptance, cost, and compliance than ELED and should be considered as an option in the initial management of children with EE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1097–1102

Predictive values for skin prick test and atopypatch test for eosinophilic esophagitis
Jonathan M. Sperge, Letters to Editor Jaci.2006.11.016

Predictive values for skin prick test and atopypatch test for eosinophilic esophagitis
Jonathan M. Sperge, Letters to Editor Jaci.2006.11.016

Predictive values for skin prick test and atopypatch test for eosinophilic esophagitis
• The combination of the 2 testing methods had an excellent NPV (88% to 100%) for all foods except milk, which was very low at 41%
• Combination of SPT and APT in designing a diet plan has a high success rate for food elimination or food reintroduction in EE with the exception of milk.
Jonathan M. Sperge, Letters to Editor Jaci.2006.11.016

Treatment Phamacological
• Oral corticosteroid - improve esophageal eosinophilia andsymptoms in patients with EoE- disease relapse within less than 6 mo after cessation & adverse effects of long-term treatment - used in severe cases,recommended dose 1-2 mg/kg of prednisone equivalent

Treatment
• Topical corticosteroid

Study Design & No. of Pt
Medication and Dosage
Outcome
Konikoff et al, 2006
RDBPCN = 36
Fluticasone propionate 2 puffs twice daily : All subjects received 220mcg/puff( total 880mcg/d) * 3 mo (Ages 3–16 y)
1 o outcome : Prox EsoEo 65.9 + - 25.3 vs 1.4 + -1.1 eos/hpf [P =0.03]:Dist EsoEo 84.6 + -19.7 vs 19.6 + - 12.9 eos/hpf [P=0.04 ]2o outcome :Resolution of vomiting FP vs placebo 67% vs 27%;[P =0 .04]:Improve endocopic finding (Furrow) [P=0.047]: reduce epithelial hyperplasia [ P= 0.01]:FP decreased the number ofCD8 & mast cells in proximaland distal esophagus (P=0 .05)

Study Design & No. of Pt
Medication and Dosage
Outcome
Dohil et al,2010
RDBPCN = 24
Oral viscous budesonide * 3 mo Subjects <5 ft tall: 1 mg dailySubjects >5 ft tall: 2 mg daily(Age 1–17 y mean 7.8 yr)
1 o outcome In OVB gr 87.6% responder Reduce peak EsoEo all esophagealLevels proximal (P=0.0024),mid (P =0 .0001), anddistal (P=0 .0001) when compared to baseline 2o outcome :Upper gastrointestinal endoscopy score reduced 4.6 1.5 [P=0.0005] :Symptom score decrease from 3.51.2 [p=0.0007]: Epithelial &Lamina propria Eosinophilia&Fibrosis reduced [P=0.0035]

Eosinophilic esophagitis: Updated consensusrecommendations for children and adults
(J Allergy Clin Immunol 2011;128:3-20.)

• After induction of clinicopathologic remission, topical corticosteroid therapy might need to be maintained
• long-term therapy must be individualized foreach patient
• When topical steroids used chronically : side effects, growth should be carefully monitoredin children
(J Allergy Clin Immunol 2011;128:3-20.)

Treatment
• 11 adult patients were randomized to mepolizumab (n = 5) or placebo (n = 6)
• Mepolizumab gr. decrease mean Eso Eo 54% vs placebo 5 %
• But no complete resolution in any suject, no significant in symptom improvement
Anti-interleukin-5 antibody treatment(mepolizumab) in active eosinophilic oesophagitis: a randomised, placebocontrolled,double-blind trial
Gut 2010 ;59(1):21-30

Treatment
• Treatment of EoE with cromolyn sodium, leukotriene receptor antagonists, and immunosuppressive agents (azathioprine or 6- MP) is not recommended
• Anti–tumor necrosis factor (TNF) : one case report
• Anti-IgE therapy (omalizumab) : no publish study, one case report

Treatment• Esophageal Dilation
- effective treatment of dysphagia, caused by strictures- significant symptomatic relief in up to 83% of patients for 20 month can be recurrence- chest pain, deep muscle tear, rare perforation

Summary
• Diagnosis of EoE should be made when symptoms of esophageal dysmotility + evidence of esophageal eosinophilia despite adequate acid suppression (adequate PPI Rx trial or normal esophageal pH).




Why 15 Eos/HPF ?
10 studies 15 eos/HPF based on peak count or mean number of fields
8 studies 20 eos/HPF based onPeak or mean number
2 studies 24 eos/HPF based on peak count or mean number
1 study 30 eos/HPF peak count GASTROENTEROLOGY 2007;133:1342–1363

Elemental Diet Is an Effective Treatmentfor Eosinophilic Esophagitis in Children
and Adolescents
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 98, No. 4, 2003