Embed Size (px)
Citation preview
GERD: An Update
S Nasseri-Moghaddam MD, MPH
Associate Professor of Medicine
DDRI, TUMS, IAGH meeting
World Digestive Health Week, 2012 (1391)
Shariati Hospital, Tehran
In the Name of God
GERD is a common disease
• Various studies have shown this • Up to 40% in western reports • Several Iranian studies:
• Up to 18% (If minor symptoms included up to 27%)
• Many never refer • Prevalence has increased significantly • Why? No one clear answer, maybe:
• Life style • Better hygiene less HP • Nitrates
GERD: Diagnosis
• No “Gold standard” for Dx • Mostly relied on symptoms: HB/AR (also dysphagia,
chest pain and some minors) • Sensitivity of HB/AR: 30-75% • Specificity of HB/AR: 62-96%
• The point is that w/o having a “gold standard” these figures are also shaky
• Endoscopy: Distal esophageal erosions seen in 30-50% of cases
• pH-metry, Multi-channel Intraluminal Impedance (MII): Left for difficult cases, refractory cases, and surgery candidates
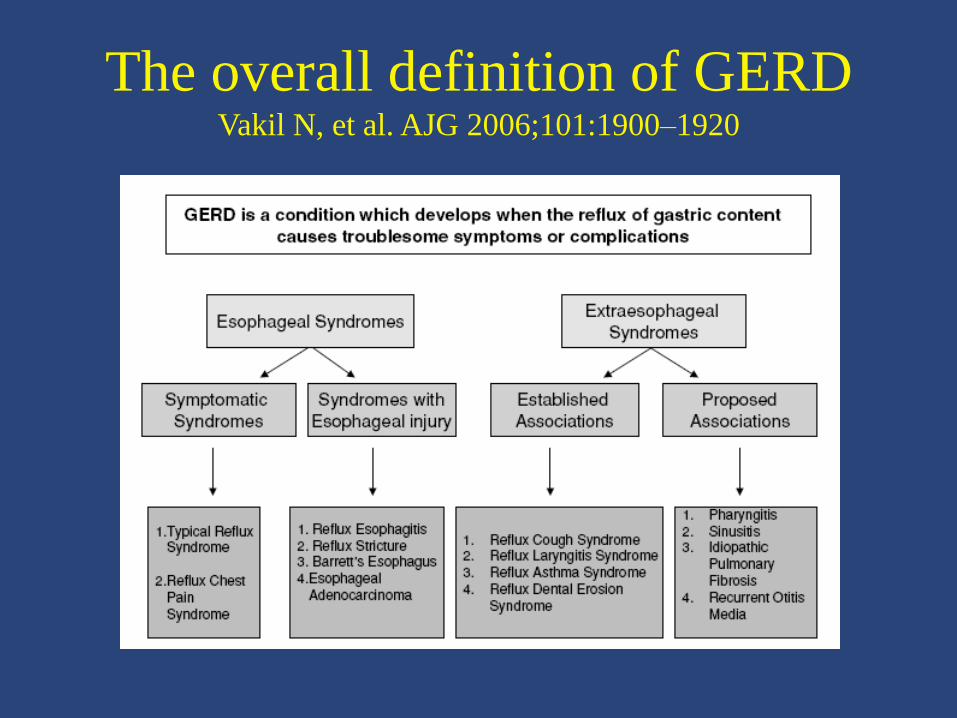
The overall definition of GERD Vakil N, et al. AJG 2006;101:1900–1920
GERD: Some definitions (Rome III criteria)
• Erosive GERD: Definite mucosal breaks in the distal esophagus • May have normal or abnormal acid exposure
• NERD: typical symptoms, Normal endoscopy, excessive acid exposure on MII/pH
• Hypersensitive esophagus: Typical symptoms, reflux on MII, normal acid exposure
• Functional heartburn: Typical symptoms, No reflux on MII, normal acid exposure
GERD: Pathophysiology
• Many reflux episodes are not associated w symptoms
• Many symptom episodes are not associated w GER
• Pathophysiology is largely unknown
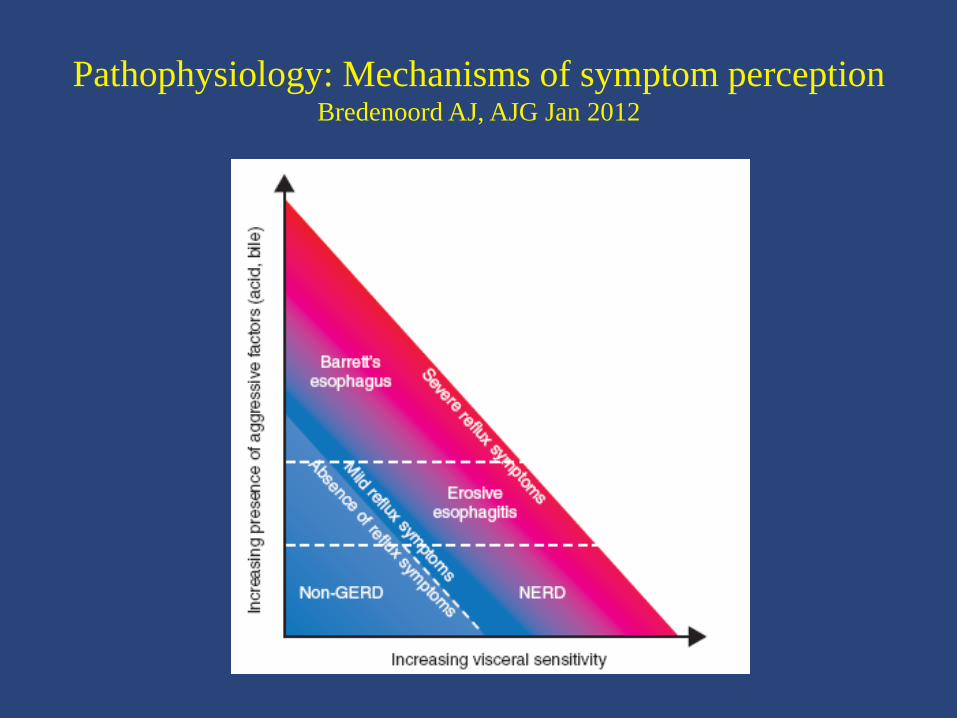
Pathophysiology: Mechanisms of symptom perception Bredenoord AJ, AJG Jan 2012
Symptom perception in GERD
• NERD pts • fewer acid reflux episodes and less esophageal acid
exposure than patients with reflux esophagitis but,
• perceive less intense stimuli because of greater esophageal sensitivity
• Factors contributing to greater esophageal sensitivity: • impaired mucosal barrier function,
• peripherally mediated esophageal sensitivity (enhanced esophageal receptor signaling), and
• centrally mediated esophageal sensitivity (physiological stressors, sensitization of spinal sensory neurons)

Other contributing factors to symptom
perception
• Reflux characteristics other than acidity, e.g.
• the presence of bile, pepsin, liquid, or gas in reflux, and
• the proximal extent or volume of reflux
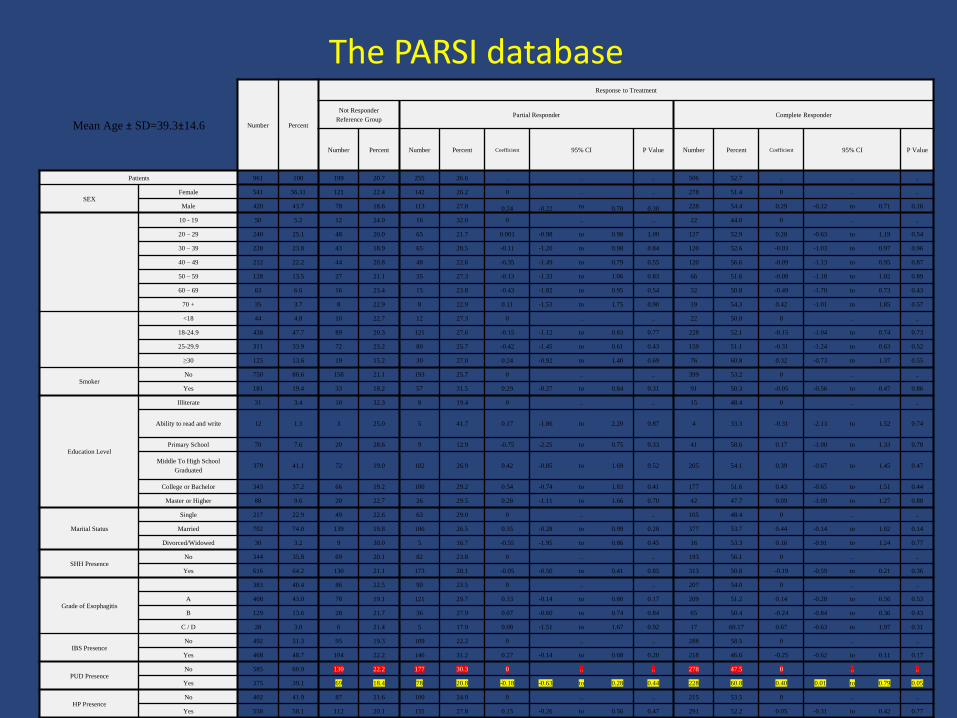
Mean Age ± SD=39.3±14.6 Number Percent
Response to Treatment
Not Responder
Reference Group Partial Responder Complete Responder
Number Percent Number Percent Coefficient 95% CI P Value Number Percent Coefficient 95% CI P Value
Patients 961 100 199 20.7 255 26.6 .. .. .. 506 52.7 .. .. ..
SEX Female 541 56.31 121 22.4 142 26.2 0 .. .. 278 51.4 0 .. ..
Male 420 43.7 78 18.6 113 27.0 0.24 -0.22 to 0.70 0.30 228 54.4 0.29 -0.12 to 0.71 0.16
10 - 19 50 5.2 12 24.0 16 32.0 0 .. ... 22 44.0 0 .. ..
20 – 29 240 25.1 48 20.0 65 21.7 0.001 -0.98 to 0.98 1.00 127 52.9 0.28 -0.63 to 1.19 0.54
30 – 39 228 23.8 43 18.9 65 28.5 -0.11 -1.20 to 0.98 0.84 120 52.6 -0.03 -1.03 to 0.97 0.96
40 – 49 212 22.2 44 20.8 48 22.6 -0.35 -1.49 to 0.79 0.55 120 56.6 -0.09 -1.13 to 0.95 0.87
50 – 59 128 13.5 27 21.1 35 27.3 -0.13 -1.33 to 1.06 0.83 66 51.6 -0.08 -1.18 to 1.02 0.89
60 – 69 63 6.6 16 25.4 15 23.8 -0.43 -1.82 to 0.95 0.54 32 50.8 -0.49 -1.70 to 0.73 0.43
70 + 35 3.7 8 22.9 8 22.9 0.11 -1.53 to 1.75 0.90 19 54.3 0.42 -1.01 to 1.85 0.57
<18 44 4.8 10 22.7 12 27.3 0 .. .. 22 50.0 0 .. ..
18-24.9 438 47.7 89 20.3 121 27.6 -0.15 -1.12 to 0.83 0.77 228 52.1 -0.15 -1.04 to 0.74 0.73
25-29.9 311 33.9 72 23.2 80 25.7 -0.42 -1.45 to 0.61 0.43 159 51.1 -0.31 -1.24 to 0.63 0.52
≥30 125 13.6 19 15.2 30 27.0 0.24 -0.92 to 1.40 0.69 76 60.8 0.32 -0.73 to 1.37 0.55
Smoker No 750 80.6 158 21.1 193 25.7 0 .. .. 399 53.2 0 .. ..
Yes 181 19.4 33 18.2 57 31.5 0.29 -0.27 to 0.84 0.31 91 50.3 -0.05 -0.56 to 0.47 0.86
Education Level
Illiterate 31 3.4 10 32.3 8 19.4 0 .. .. 15 48.4 0 .. ..
Ability to read and write 12 1.3 3 25.0 5 41.7 0.17 -1.86 to 2.20 0.87 4 33.3 -0.31 -2.13 to 1.52 0.74
Primary School 70 7.6 20 28.6 9 12.9 -0.75 -2.25 to 0.75 0.33 41 58.6 0.17 -1.00 to 1.33 0.78
Middle To High School
Graduated 379 41.1 72 19.0 102 26.9 0.42 -0.85 to 1.69 0.52 205 54.1 0.39 -0.67 to 1.45 0.47
College or Bachelor 343 37.2 66 19.2 100 29.2 0.54 -0.74 to 1.83 0.41 177 51.6 0.43 -0.65 to 1.51 0.44
Master or Higher 88 9.6 20 22.7 26 29.5 0.28 -1.11 to 1.66 0.70 42 47.7 0.09 -1.09 to 1.27 0.88
Marital Status
Single 217 22.9 49 22.6 63 29.0 0 .. .. 105 48.4 0 .. ..
Married 702 74.0 139 19.8 186 26.5 0.35 -0.28 to 0.99 0.28 377 53.7 0.44 -0.14 to 1.02 0.14
Divorced/Widowed 30 3.2 9 30.0 5 16.7 -0.55 -1.95 to 0.86 0.45 16 53.3 0.16 -0.91 to 1.24 0.77
SHH Presence No 344 35.8 69 20.1 82 23.8 0 .. .. 193 56.1 0 .. ..
Yes 616 64.2 130 21.1 173 28.1 -0.05 -0.50 to 0.41 0.85 313 50.8 -0.19 -0.59 to 0.21 0.36
Grade of Esophagitis
383 40.4 86 22.5 90 23.5 0 .. .. 207 54.0 0 .. ..
A 408 43.0 78 19.1 121 29.7 0.33 -0.14 to 0.80 0.17 209 51.2 0.14 -0.28 to 0.56 0.53
B 129 13.6 28 21.7 36 27.9 0.07 -0.60 to 0.74 0.84 65 50.4 -0.24 -0.84 to 0.36 0.43
C / D 28 3.0 6 21.4 5 17.9 0.08 -1.51 to 1.67 0.92 17 60.17 0.67 -0.63 to 1.97 0.31
IBS Presence No 492 51.3 95 19.3 109 22.2 0 .. .. 288 58.5 0 .. ..
Yes 468 48.7 104 22.2 146 31.2 0.27 -0.14 to 0.68 0.20 218 46.6 -0.25 -0.62 to 0.11 0.17
PUD Presence No 585 60.9 130 22.2 177 30.3 0 .. .. 278 47.5 0 .. ..
Yes 375 39.1 69 18.4 78 20.8 -0.18 -0.63 to 0.28 0.44 228 60.8 0.40 0.01 to 0.79 0.05
HP Presence No 402 41.9 87 21.6 100 24.9 0 .. .. 215 53.5 0 .. ..
Yes 558 58.1 112 20.1 155 27.8 0.15 -0.26 to 0.56 0.47 291 52.2 0.05 -0.31 to 0.42 0.77
The PARSI database
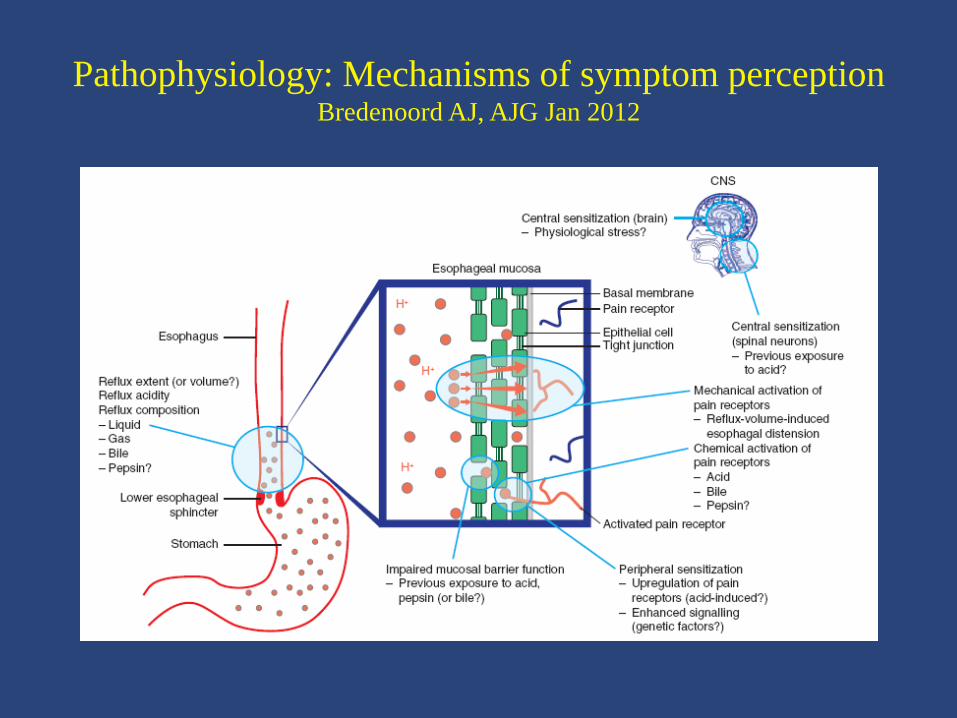
Pathophysiology: Mechanisms of symptom perception Bredenoord AJ, AJG Jan 2012
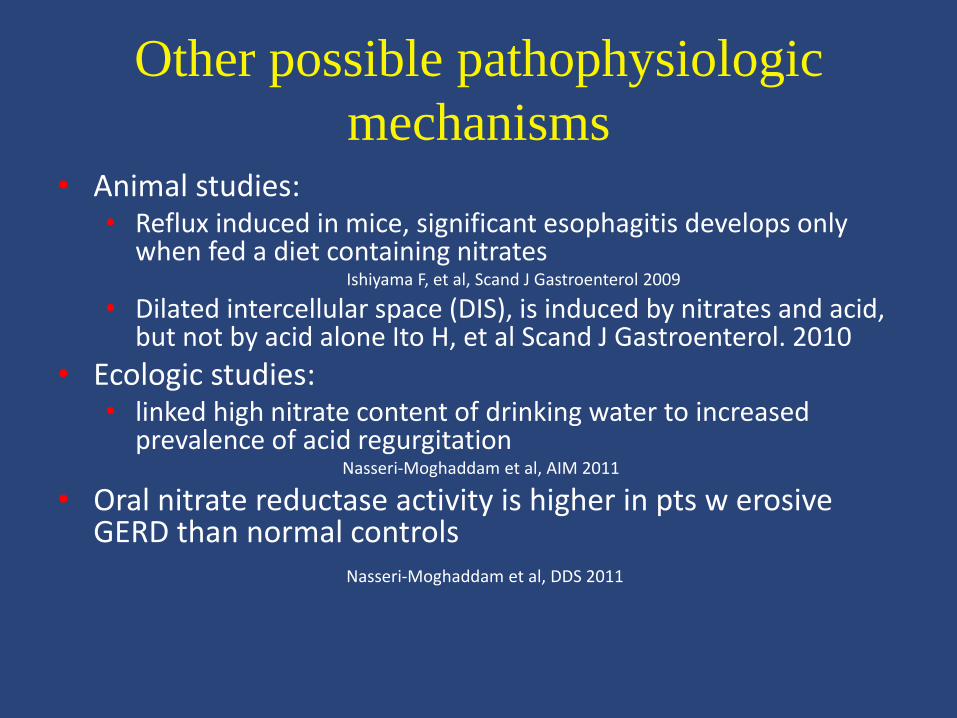
Other possible pathophysiologic
mechanisms • Animal studies:
• Reflux induced in mice, significant esophagitis develops only when fed a diet containing nitrates
Ishiyama F, et al, Scand J Gastroenterol 2009
• Dilated intercellular space (DIS), is induced by nitrates and acid, but not by acid alone Ito H, et al Scand J Gastroenterol. 2010
• Ecologic studies: • linked high nitrate content of drinking water to increased
prevalence of acid regurgitation Nasseri-Moghaddam et al, AIM 2011
• Oral nitrate reductase activity is higher in pts w erosive GERD than normal controls
Nasseri-Moghaddam et al, DDS 2011
GERD: Investigations
• History
• Significant number of symptoms considered as atypical e.g. nausea, eructaion, chest pain, etc
• Significant overlap w IBS
• Significant overlap w PUD
• Endoscopy
• MII-pH
GERD: Treatment
• Life style modification
• Diet
• Stress
• Habits
• Medications:
• H2 blockers
• PPIs
• Newer drugs
Facts about PPIs as mainstay of Rx
• Are PPIs safe over long term? • Yes, no malignancy reported in humans up to 15 years of
use (uncontrolled studies) • Recent SR of controlled trials: no malignancy up to 7 years • Osteoporosis: very low risk,
• older people, • high dose • Long term
• Infections • Maybe in older people, not a big burden
• Renal problems: • Hypomagnesemia/renal injury • Interstitial nephritis

Facts about PPIs as mainstay of Rx
• Are PPIs safe during pregnancy?
• Yes, all even in the first trimester
• Omeprazole may be better in the pre-conception period
Facts about PPIs as mainstay of Rx • Several PPIs available: Omeprazole, Pantoprazole,
Lansoprazole, Rabeprazole, Esomeprazole and a couple of long-acting variants
• In most instances (80%) all have equal efficay and clinical profile • Therefore the cheapest will do
• In some subgroups one may be better • Some refractory cases are CYP 2C19 related PPIs not
metabolized by this pathway (e.g. Rabeprazole/Pariet) preferrable
• Sometimes switching to another PPI may help (not CYP 2C19 related)
• Acute cases need rapid onset of action (Rabeprazole/Pariet) • Pts on multiple drugs may be better off on Pantoprazole or
Rabeprazole (almost no interaction with other drugs) • Drug resistant HP: Rabeprazole may add a small benefit
• Overall different PPIs have similar efficacy and safety profile
Facts about PPIs as mainstay of Rx
• Do PPIs decrease the anti-platelet effects of Clopidogrel? • In vitro studies: Yes
• In vivo studies: No consistent effect, most probably no significant clinical interaction
• Do we need to select a special PPI to minimize this possible effect? • No consistent data, most probably NO
• Some propose PPIs w less interaction (e.g. Pantoprazole, Rabeprazole/Pariet)
How should PPIs be administered?
• Step up vs step down therapy
• Single vs double dose administration
• Before meals
• Continue long term
• Taper before D/C
• Maintain at the lowest dose
Refractory GERD
• GERD pts unresponsive to PPIs after 4-8 weeks
• Differential diagnoses: • True refractory
• Achalasia
• Eosinophilic esophagitis
• Malignancy
• Lichen Planus and related disorders
• Hypersensitive esophagus
• Functional heartburn
Refractory GERD
• Review pt hx (attention to symptoms, concomitant IBS)
• UGIE + 4 quadrant upper and lower esophageal bx
• Ba swallow
• Manometry (high resolution)
• pH-metry/MII
Refractory GERD
• Abnormal acid-reflux causes symptoms • Normal acid reflux causes symptoms
(hypersensitive esophagus) • Non-acid reflux causes symptoms Esophageal pH/Impedance monitoring • Non-GERD esophageal disorders cause symptoms UGIE/esophageal Manometry/Ba swallo • Extra-esophageal disorders cause symptoms Test for heart/biliary/other disorders • Symptoms are functional
Thank you for your attention





























