Embed Size (px)
Citation preview
George Boulton
Topics Covered What is quality?
Quality myths
Financing to achieve policy aims
Linking quality to a capitation system
Joined-up implementation issues
04/19/23 Quality Conference 2008 2
Quality in Health Care
“It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm” – Florence Nightingale (1859)
“Conformance to requirements” - TQM definition – Philip Crosby ‘Quality Without Tears (1984)
“Doing the right things, right” - J. A. Muir Gray ‘Evidence-based Healthcare’ (1997)
Donabedian (1966) advocated the assessment of quality through 3 approaches: Structure, process and outcome
04/19/23 Quality Conference 2008 3
Defining Quality in Health Care Robert Maxwell Kings Fund, London (1984)
identified 6 dimensions of quality:
ACCESS: Geographical convenience, waiting time for appointment, hours of business, transport etc?
EQUITY: Opportunity of access for equal need regardless racial, cultural and social factors
RELEVANCE TO NEED: Over provision, gaps in services etc.
SOCIAL ACCEPTABILITY: Is the way in which the service is provided acceptable to the population
served?
EFFICIENCY: Are the services delivered as efficiently as possible within the resources available?
EFFECTIVENESS: Do the services provided attain the intended benefits in for the heath of the population served?
04/19/23 Quality Conference 2008 4
Quality Myths Quality is separate from efficiency. Not so, quality is
inextricably linked to efficiency e.g. TQM and DIRFT Patients don’t understand quality. Not so, access to
knowledge changing the doctor/patient relationship – the ‘intelligent’ patient
Quality is a `soft`, subjective issue. Not so, quality is as measurable as finance or activity
Quality is a system. Not so, it is a corporate culture, a mind set, a sub-routine as driving a car
Quality in health care is `accreditation`, `TQM`, `EBM`, `ISO 9001`, medical audit etc. Not so, these systems and approaches help develop and sustain a ‘quality’ culture.
04/19/23 Quality Conference 2008 5
Quality Conference 2008 6
Quality Sustaining Systems Law and regulation Accreditation Visiting and inspection Licensing & re-licensing of professionals Professional codes and standards TQM (based on prevention and DIRFT) CQI/Quality Assurance Evidence-based health care Medical Practice variation (MPV) Contracting Care pathways, clinical guidelines, clinical protocols,
clinical algorithms Patient surveys Complaints systems
04/19/23
Quality Conference 2008 7
Quality Sustaining Systems Research and development Health Technology Assessment (HTA) Clinical governance Clinical /medical/organizational audit Patient-centered planning Performance indicator systems Risk management systems ISO 9000, 9001,9002 etc. Benchmarking League tables Star ratings – linked to accreditation Continuous professional education and
development Contracting Resource allocation and reward systems
04/19/23
Policy Outcomes for Primary Health Care?
Improved community/population health status Reduced avoidable (amenable) mortality Improved quality of life for the chronically ill
and disabled Morbidity compression related to the elderly Higher volume and levels of cases resolved in
primary health care High levels of uptake (population-based) of
PHC and preventive services Increased patient satisfaction
04/19/23 Quality Conference 2008 8
Quality and its Link to Resource Allocation & Reward Systems
Capitation – a fixed sum per person paid in advance (usually 1 year) to a health care entity (e.g. DZ) for the provision of contracted health care services to an eligible person.
Capitation should be ‘risk adjusted’ for:- Population age structure- Gender structure- Health need differences (crude or standardised mortality
rates- Poverty/social deprivation
04/19/23 Quality Conference 2008 9
Capitation Reimbursement Systems
Capitation can operate at two levels:
As a resource allocation formula to communities, hospitals or to PHC facilities
As part of the reward system to individual physicians and teams
04/19/23 Quality Conference 2008 10
Capitation Weaknesses Capitation alone can produce low efficiency and
effectiveness
It is often used in conjunction with complimentary and inter related financing streams:
- Incentives for high quality or good practice- Rewards for high levels of performance
A typical resource allocation/reimbursement mechanism using capitation will often involve :Capitation + Incentive + Performance (85:15, 75:25, 60:40)
04/19/23 Quality Conference 2008 11
Joined-up Quality Strategy How to link quality initiatives, approaches and
systems to the resource allocation system?
A major quality initiative in Serbia is the Book of Rules on Health Care Quality Indictors
Linkage can be achieved through:- Developments in the contracting process to
include quality systems, processes and targets
- Use of the incentive and performance components of the resource allocation system
- Use of the reward system
04/19/23 Quality Conference 2008 12
What Should the Financing System Support?
The development of the ‘Gatekeeper’ role
The integration of care (referral systems, care pathways, clinical networks, clinical protocols, care algorithms etc.)
Increased focus on health promotion and primary and secondary prevention systems
Emphasis on early identification, management and control of chronic disease and illness
Continuous quality improvement and innovation
04/19/23 Quality Conference 2008 13
What Should the Financing System Support?
Increased focus on health maintenance and quality of life issues for the long term chronically sick
Evidence-based practice (appropriate antibiotic use, call and recall screening etc.) Compliance with best practice guidelines/protocols
Increased levels of community/patient satisfaction with PHC
Efficiency and effectiveness in service delivery
04/19/23 Quality Conference 2008 14
Finance-linked Performance Examples
New Zealand is currently in the process of implementing capitation payment system and divides the incentive and performance components into:
― Clinical performance issues― Process/capacity performance issues― Financial performance issues
04/19/23 Quality Conference 2008 15
Examples : Clinical Proportion of children fully vaccinated by x age
from target population Proportion of cervical smears in accordance
with protocol from target population Breast screening undertaken in accordance
with protocol from target population Inhaled corticosteroids – average inhaled doses Ratio of metformin to sulphonylurea
prescriptions Investigation of thyroid function (TSH v T4) Ratio ESR to CRP test ordering Flu vaccinations for +65 from target population
04/19/23 Quality Conference 2008 16
Examples : Process/capacity Number/proportion of patients registered from
catchment Number/proportion of cases resolved in PHC Emergency admissions to hospital for chronic
conditions Number of new patients attending for a new episode
of treatment Waiting times for treatment and in facilities against
targets Rate of blood pressure checking for over 40s
compared to target population Patient satisfaction (as measured by survey) Introduction of audit systems
04/19/23 Quality Conference 2008 17
Examples : Financial Performance Compliance of activities, outputs to planned Compliance of expenditure to budget Pharmaceutical expenditure in comparison
with benchmarks Laboratory expenditure in comparison with
benchmarks Antibiotic prescribing patterns (1st gen/3rd
gen) Proportion of prescriptions expressed on a
generic basis
04/19/23 Quality Conference 2008 18
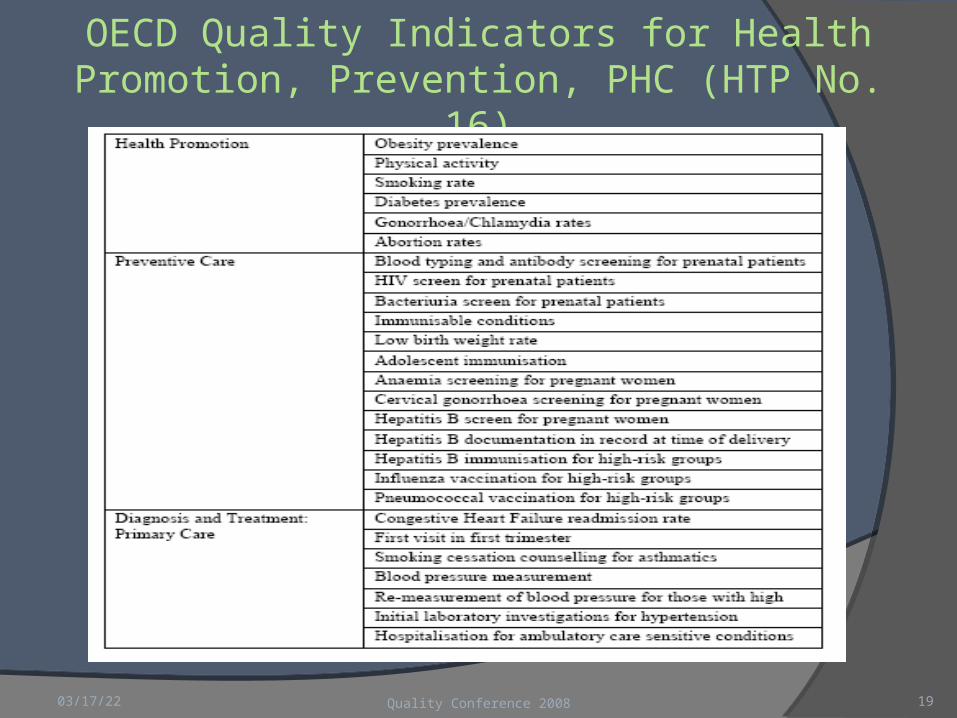
OECD Quality Indicators for Health Promotion, Prevention, PHC (HTP No. 16)
04/19/23 19Quality Conference 2008
Practical Implementation Issues The urgent need for a population data base (registration) at
DZ level to help shift from a curative to a preventive service
How to link existing quality assurance system (book of rules of Health Care Quality Indicators) to the financing system to avoid duplication of effort?
Convert averages to targets (top 25 percentile performance), rates of screening to target populations etc.
Beware over complicated, non-transparent formulae and incentive arrangements that can be self-defeating
Need for financial flexibility and incentives at DZ level to promote and stimulate innovation and continuous quality improvement?
04/19/23 Quality Conference 2008 20











![ACOs, GLOBAL PAYMENTS AND CAPITATION REIMBURSEMENT · PDF file1 Chapter 17 ACOs, GLOBAL PAYMENTS AND CAPITATION REIMBURSEMENT [Eliminating Fee-For-Service Physician Compensation] David](https://img.pdfslide.us/doc/110x75/5aa95fd37f8b9a72188ccbbd/acos-global-payments-and-capitation-reimbursement-chapter-17-acos-global-payments.jpg)

















