Embed Size (px)
Citation preview

Avi Levine, HMS IIIGillian Lieberman, MD August 2008
Avi Levine, HMS IIIGillian Lieberman, MD
Genitourinary Tuberculosis

Patient SO: HistoryPatient SO: History
60 year old female60 year old femaleHPI: Single episode of painless HPI: Single episode of painless hematuriahematuria
No associated symptomsNo associated symptoms
PMH: PMH: Hypothyroidism, hypertension, Hypothyroidism, hypertension, hypercholesterolemia, depressionhypercholesterolemia, depression
Family History: Family History: Mother Mother -- Renal cell carcinomaRenal cell carcinoma
Social History: 45 pack year smoking historySocial History: 45 pack year smoking history

Imaging Menu of Tests for Imaging Menu of Tests for HematuriaHematuria
Intravenous Intravenous PyelographyPyelography (IVP)(IVP)UltrasoundUltrasoundMRIMRICTCT
Initial imaging modality of choice for patients with Initial imaging modality of choice for patients with unexplained unexplained hematuriahematuria

Our Patient: NonOur Patient: Non--Contrast CT Contrast CT –– Complicated Cystic LesionComplicated Cystic Lesion
Calcification
Area of inhomogeneityw/ disruption of normal
kidney contour
PACS, BIDMC
Axial C-
CT

Our Patient: Contrast CT Our Patient: Contrast CT –– Complicated Cystic LesionComplicated Cystic Lesion
Area of inhomogeneityw/ disruption of normal
kidney contour+
peripheral enhancement
Complicated cystic lesion w/ calcification
PACS, BIDMC
Axial C+ CT
Calcification

Definitions: Cysts and Cystic LesionsDefinitions: Cysts and Cystic Lesions
Cyst Cyst –– fluid filled lesionfluid filled lesionSimple cysts can be complicated with hemorrhage, infection, Simple cysts can be complicated with hemorrhage, infection, inflammation, or ischemiainflammation, or ischemiaFluid filled renal mass is considered a complicated cyst when itFluid filled renal mass is considered a complicated cyst when ithas one of the following features:has one of the following features:
CalcificationCalcificationHigh attenuation (>20 HU)High attenuation (>20 HU)SeptationsSeptationsMultiple Multiple loculesloculesEnhancementEnhancementWall thickeningWall thickeningNodularityNodularity

Our Patient: Differential DiagnosisOur Patient: Differential Diagnosis
Renal Cell CarcinomaRenal Cell CarcinomaTransitional Cell CarcinomaTransitional Cell CarcinomaMetastasesMetastasesInfectious diseaseInfectious disease
TuberculosisTuberculosis
OncocytomaOncocytomaMultilocularMultilocular Cystic Cystic NephromaNephroma
Benign renal dysplasiaBenign renal dysplasia

Menu of Tests for Imaging a Cystic Menu of Tests for Imaging a Cystic Renal MassRenal Mass
IVPIVPSensitivity for small renal masses is limitedSensitivity for small renal masses is limited
UltrasoundUltrasoundStrength: reliable identification of simple renal cystsStrength: reliable identification of simple renal cysts
CTCTGold standard for renal mass evaluationGold standard for renal mass evaluation
MRIMRINo significant advantage over CTNo significant advantage over CTGood for patients with contrast allergy or elevated blood Good for patients with contrast allergy or elevated blood creatininecreatinine levellevel

BosniakBosniak
Classification SystemClassification System
CategoryCategory DescriptionDescription
II Benign simple cyst with hairline thin wall that does not containBenign simple cyst with hairline thin wall that does not contain
septa septa calcifications, or solid components.calcifications, or solid components.
IIII Benign cyst that may contain a few hairline thin septa in which Benign cyst that may contain a few hairline thin septa in which perceived perceived enhancement may be present. Does not require further evaluation.enhancement may be present. Does not require further evaluation.
IIFIIF Cysts that contain multiple hairline thin septa or minimal smootCysts that contain multiple hairline thin septa or minimal smooth thickening of h thickening of wall or septa. Wall or septa may contain calcification that may wall or septa. Wall or septa may contain calcification that may be thick and be thick and
nodular.nodular.
IIIIII Indeterminate cystic masses with thickened irregular or smooth wIndeterminate cystic masses with thickened irregular or smooth walls or septa in alls or septa in which measurable enhancement is present.which measurable enhancement is present.
IVIV Clearly malignant cystic masses that can have all the criteria oClearly malignant cystic masses that can have all the criteria of category III but f category III but also contain enhancing softalso contain enhancing soft--tissue components adjacent to the wall or septum.tissue components adjacent to the wall or septum.

Management of Renal CystsManagement of Renal Cysts
For renal cysts in categories IIF and III, such as For renal cysts in categories IIF and III, such as our patient, optimal approach is uncertainour patient, optimal approach is uncertainMRI can be used as an additional modalityMRI can be used as an additional modality
Useful to characterize internal contents of cystsUseful to characterize internal contents of cystsMore sensitive at showing enhancement of internal More sensitive at showing enhancement of internal septationsseptations
Our patient underwent MRI for further Our patient underwent MRI for further evaluation of the lesionevaluation of the lesion

Our Patient: T2Our Patient: T2--Weighted Contrast Enhanced Weighted Contrast Enhanced MRI MRI ––
Complicated Cystic LesionComplicated Cystic Lesion
Multi-cystic lesion with areas of low signal
Multiple internalseptations
with
enhancementPACS, BIDMC
Axial C+ MRI

Our Patient: T2Our Patient: T2--Weighted Contrast Enhanced Weighted Contrast Enhanced MRI MRI ––
Complicated Cystic LesionComplicated Cystic Lesion
• Multi-cystic lesion
• Disruption of normal kidney contour
• Enhancement of internal septations
PACS, BIDMCCoronal C+ MRI

Our Patient: Clinical CourseOur Patient: Clinical Course
Due to high suspicion of RCC or TCC, our Due to high suspicion of RCC or TCC, our patient underwent a laparoscopic radical patient underwent a laparoscopic radical nephrectomynephrectomy
Pathology report revealed necrotizing Pathology report revealed necrotizing granulomasgranulomas and active inflammation, likely and active inflammation, likely renal tuberculosisrenal tuberculosis

Our Patient: More Detailed Family HistoryOur Patient: More Detailed Family History
Father hospitalized many years ago for “severe” Father hospitalized many years ago for “severe” pulmonary TBpulmonary TB18 month old brother died from 18 month old brother died from tuberculoustuberculousmeningitismeningitisSurviving brother developed TB and was Surviving brother developed TB and was hospitalized for one yearhospitalized for one yearS.O. and sister told they “could never have a S.O. and sister told they “could never have a PPD”PPD”

ExtraExtra--Pulmonary TuberculosisPulmonary Tuberculosis
Aside from Aside from lymphadenopathylymphadenopathy, the genitourinary , the genitourinary system is the most common site of involvement system is the most common site of involvement by extraby extra--pulmonary TBpulmonary TB
Accounts for 15% Accounts for 15% -- 20% of infections outside the 20% of infections outside the lunglungOnly 25% of patients have a known history of prior Only 25% of patients have a known history of prior pulmonary TBpulmonary TBAdditional 25% Additional 25% -- 50% of patients will have 50% of patients will have radiographic evidence of prior subradiographic evidence of prior sub--clinical clinical pulmonary infectionpulmonary infection

Our Patient: PreOur Patient: Pre--Op CXROp CXR
Initially read by radiologist as normal
PACS, BIDMC
Chest: Frontal P-A Plain Film
However, upon closerexamination…

Our Patient: Evidence of Prior TB Infection Our Patient: Evidence of Prior TB Infection on Preon Pre--Op CXROp CXR
Granulomas+
Fibrosis
PACS, BIDMCChest: Frontal P-A Plain Film, Magnified
Ghon
Focus

Pathogenesis of Renal TBPathogenesis of Renal TB
Small Small granulomasgranulomas form in renal cortexform in renal cortexCapillary rupture results in delivery of organisms Capillary rupture results in delivery of organisms to proximal tubules and loops of to proximal tubules and loops of HenleHenle and and eventually papillary necrosiseventually papillary necrosisHost response includes fibrosis, calcium Host response includes fibrosis, calcium deposition, and stricture formationdeposition, and stricture formation

Renal AnatomyRenal Anatomy
http://www.nlm.nih.gov/MEDLINEPLUS/ency/images/ency/fullsize/110http://www.nlm.nih.gov/MEDLINEPLUS/ency/images/ency/fullsize/1101.jpg1.jpg

Companion Patient #1: MothCompanion Patient #1: Moth--Eaten Eaten Calyx on IVUCalyx on IVU
Abnormal calyx with some loss of renal substanceAbnormal calyx with some loss of renal substance
Eastwood, J. Tuberculosis Eastwood, J. Tuberculosis and the kidney. and the kidney. Journal of the Journal of the
American Society of American Society of NephrologyNephrology. 12:1307. 12:1307--1314, 1314,
20012001
Abdomen: C+ Frontal Plain Film

Companion Patient #1: Calcification on Companion Patient #1: Calcification on Plain FilmPlain Film
Calcification in lower pole of kidneyCalcification in lower pole of kidneyPresent in 24% Present in 24% -- 44% of patients with renal TB44% of patients with renal TB
Eastwood, J. Tuberculosis Eastwood, J. Tuberculosis and the kidney. and the kidney. Journal of the Journal of the
American Society of American Society of NephrologyNephrology. 12:1307. 12:1307--1314, 1314,
20012001
Abdomen: Frontal Plain Film
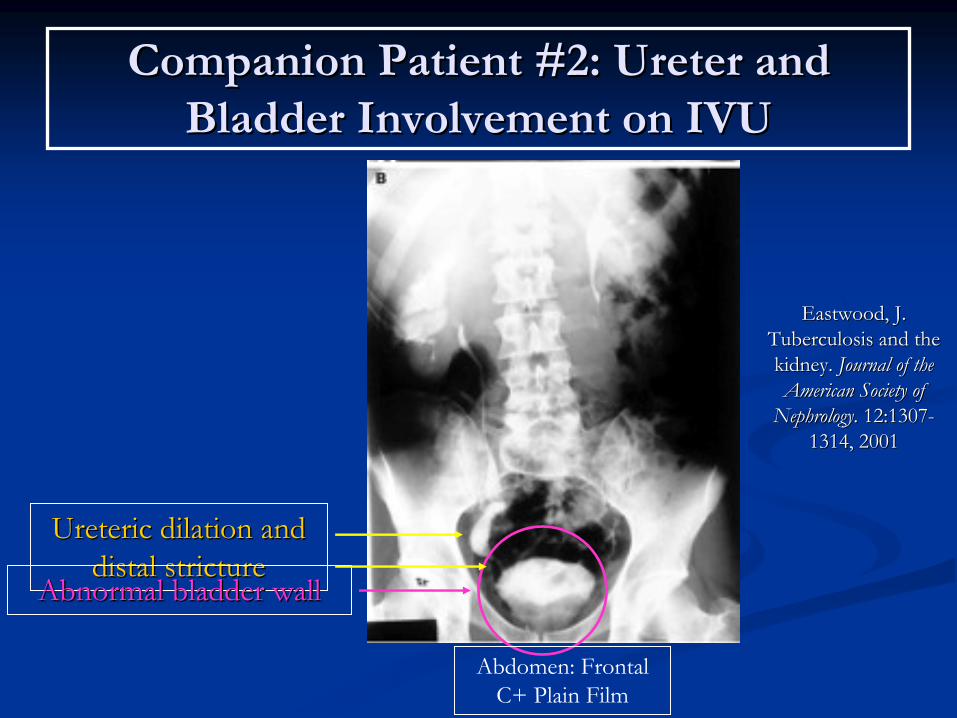
Companion Patient #2: Companion Patient #2: UreterUreter
and and Bladder Involvement on IVUBladder Involvement on IVU
UretericUreteric
dilation and dilation and distal stricturedistal stricture
Abnormal bladder wallAbnormal bladder wall
Eastwood, J. Eastwood, J. Tuberculosis and the Tuberculosis and the kidney. kidney. Journal of the Journal of the American Society of American Society of
NephrologyNephrology. 12:1307. 12:1307--
1314, 20011314, 2001
Abdomen: Frontal C+ Plain Film

Genital TuberculosisGenital Tuberculosis
Genital TB is usually associated with renal TBGenital TB is usually associated with renal TBMale genital TB involves the prostate, seminal Male genital TB involves the prostate, seminal vesicles, vesicles, epididymisepididymis, and testes, and testesFemale genital TB can spread to the peritoneum, Female genital TB can spread to the peritoneum, endometriumendometrium, ovaries, cervix, and vagina, ovaries, cervix, and vagina

Companion Patient #3: Testicular TB on Companion Patient #3: Testicular TB on CTCT
Large, irregular left sided Large, irregular left sided testicular masstesticular mass
Golden, M. Golden, M. ExtrapulmonaryExtrapulmonary
tuberculosis: an overview. tuberculosis: an overview. American American Family PhysicianFamily Physician. 72(9): 1761. 72(9): 1761--1768, November 2005.1768, November 2005.
Axial C-
CT

Our Patient: Clinical CourseOur Patient: Clinical Course
Currently being treated with a multiCurrently being treated with a multi--drug drug regimen for 12 months:regimen for 12 months:
IsoniazidIsoniazidRifampinRifampinEthambutolEthambutolPyrazinamidePyrazinamide

ConclusionsConclusions
Tuberculosis is not limited to just the pulmonary Tuberculosis is not limited to just the pulmonary systemsystemEven without prior known pulmonary TB Even without prior known pulmonary TB infection, TB must be kept on the differential infection, TB must be kept on the differential diagnosis for many lesions and pathologies of diagnosis for many lesions and pathologies of the genitourinary systemthe genitourinary system

AcknowledgmentsAcknowledgments
Dr. Sanjay Dr. Sanjay ShettyShettyDr. Frank BradleyDr. Frank BradleyDr. David YaoDr. David YaoDr. Gillian LiebermanDr. Gillian LiebermanMaria Maria LevantakisLevantakis
ReferencesReferences
Eastwood, J. Tuberculosis and the kidney. Eastwood, J. Tuberculosis and the kidney. Journal of the American Society Journal of the American Society of of NephrologyNephrology. 12:1307. 12:1307--1314, 2001.1314, 2001.EnginEngin, G. Imaging of , G. Imaging of extrapulmonaryextrapulmonary tuberculosis. tuberculosis. RadiographicsRadiographics. 2000; . 2000;
20:47120:471--488.488.Gibson, M. Renal tuberculosis. Gibson, M. Renal tuberculosis. RadiographicsRadiographics. 2004; 24:251. 2004; 24:251--256.256.Golden, M. Golden, M. ExtrapulmonaryExtrapulmonary tuberculosis: an overview. tuberculosis: an overview. American Family American Family
PhysicianPhysician. 72(9): 1761. 72(9): 1761--1768, November 2005.1768, November 2005.Hartman, D. A practical approach to the cystic renal mass. Hartman, D. A practical approach to the cystic renal mass. RadiographicsRadiographics. . 2004; 24:S1012004; 24:S101--S115.S115.Israel, G. An update of the Israel, G. An update of the BosniakBosniak renal cyst classification system. renal cyst classification system. UrologyUrology. . 66:48466:484--488, 2005.488, 2005.Wolf Jr., J. Evaluation and management of solid and cystic renalWolf Jr., J. Evaluation and management of solid and cystic renal masses. masses.
The Journal of UrologyThe Journal of Urology. 159: 1120. 159: 1120--1133, April 1998.1133, April 1998.