Embed Size (px)
Citation preview

Genetic Services Branch
Joan A. Scott, M.S., C.G.C.Department of Health and Human Services
Health Resources and Services AdministrationMaternal and Child Health Bureau
Division of Services for Children with Special Healthcare Needs
Chief, Genetics Services Branch
NEGC Annual MeetingApril 10, 2014

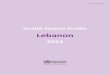
Roadmap of Federal Agencies Along the Translational Pathway
Clinical Trials
(Patients)
T1: from concept to
human studies
Clinical Practice
Guideline
T2: from studies to guidelines
Clinical Practice
T3: from guidelines to widespread
practice
HealthcareOutcomes
T4: from practice into true benefit
Basic Research
Ginsberg GM V 05.28.13
NIH
DOD/VADOD/VA
CDC
FDA/CMS AHRQ
PCORI
HRSA
Translating Genomics to Health

• Provides leadership to improve the physical and mental health, safety and well-being of the maternal and child health population which includes all of the nation’s women, infants, children, adolescents, and their families, including fathers and children with special health care needs.
Maternal and Child Health Bureau (MCHB)
• America’s healthcare safety net - HRSA is the primary Federal agency for improving access to health care services for people who are uninsured, isolated, or medically vulnerable.
Health Resources and Services Administration (HRSA)


GSBISB

Genetic Services BranchVision Genetic science is intrinsic to the understanding of health and well-being throughout the life course of an individual.Mission Provide national leadership to improve, expand, strengthen, and evaluate access to a system of genetic services and the quality of those services for children, youth, and adults across their life course.

• Title V of the Social Security Act, Section 502(a): Authorizing funds for Special Projects of Regional and National Significance (SPRANS) for
⁻ genetic disease testing, counseling, and information development and dissemination programs
⁻ comprehensive hemophilia diagnostic treatment centers without regard to age
⁻ the screening of newborns for sickle cell anemia, and other genetic disorders and follow-up services.
Legislative Authority

• Title XXVI of Children’s Health Act of 2000 “Screening for Heritable Disorders” enacted three sections of Public Health Service Act
– Grant programs to improve ability of States to provide newborn screening and to evaluate effectiveness of screening, counseling or health care services
– Established Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children (SACHDNC)
• Amended by Newborn Screening Saves Lives Act of 2008, 2014
– Clearinghouse of newborn screening– Program on laboratory quality– Interagency Coordinating Committee– National contingency plan for newborn screening– The Hunter Kelly newborn screening research program
Legislative Authority

Sickle Cell Disease Treatment Demonstration Program• Section 712(c) of the American Jobs
Creation Act of 2004, Public Law 108-357• Build a model of service deliver to improve
sickle cell care though;– Coordination of services– Genetic counseling and testing– Bundling of technical services– Training of health professional
Legislative Authority

HRSA’s National Inherited Blood Disorders Programs: Comprehensive Chronic Care Models• Sickle Cell Treatment Demonstration
Program• SPRANS
– Sickle Cell Newborn Screening Program– Thalassemia Program– The National Hemophilia Program
New
New

SCDTDP Regions
• North Atlantic
• Northeast
• Southeast
• Midwest
• Prairie
• Heartland
• Southwest
• pacific

Sickle Cell Treatment Demonstration Program • Goals
1. increase the number of providers treating sickle cell patients in the region;
2. increase the number of providers prescribing disease-modifying therapies, such as hydroxyurea; and
3. increase the number of sickle cell patient that are receiving care from providers with greater knowledge of how to treat sickle cell disease.


Sickle Cell Newborn Screening Program• Goal
1. Create a national effort to develop, implement, and maintain a strategy to identify and assess the care quality and outcomes of individuals with sickle cell disease;
2. Increase the use of sickle cell educator/counselors (e.g., community health workers); and
3. Increase the number of patients with care coordination, follow-up and referral to medical homes for sickle cell patients.
• Expected to work with SCDTDP
New

Thalassemia Program• Goal1. Create a national effort to identify and
assess the needs of individuals with thalassemia;
2. Propose a model protocol for improving the delivery of thalassemia care;
3. Implement strategies for increasing access to specialty providers; and
4. Implement strategies for ensuring that thalassemia patients have access to primary care providers who can address non-disease specific issues.
New

• Newborn Screening Saves Lives Act of 2008, reauthorized in 2014– Programs to support States– Advisory Committee– Clearinghouse of newborn screening and quality
improvement– Program on laboratory quality– Interagency Coordinating Committee– National contingency plan for newborn screening– The Hunter Kelly newborn screening research
program
Legislative Authority

• Programs to support States achieve timeliness• Advisory Committee
– Provide TA for those nominating conditions– Make recommendations regarding timeliness– Vote on conditions within 9 months– Secretary has 120 days to adopt or reject
• Reports– GAO report on timeliness in 2 years– Secretary report in one year, then every two years
• Research amendment– Research on NBS blood spots human subjects
research– Secretary 6 months for draft changes to Common
Rule, final in 2 yrs.
NBSSLA of 2014: New Activities

• Research amendment– Research on NBS blood spots human subjects
research– Secretary 6 months for draft changes to Common
Rule, final in 2 yrs.• March 9 meeting at NIH • March 24 SACHRP meeting voted on
recommendations to OHRP http://www.hhs.gov/ohrp/sachrp/
• May 11-12 DACHDNC meeting• Stay tuned for informational webinars for
State programs
NBSSLA of 2014: New Activities

Recommendations for timely NBS
A. To achieve the goals of timely diagnosis and treatment of screened conditions and to avoid associated disability, morbidity and mortality, the following time frames should be achieved by NBS programs:1. Presumptive positive results for time-critical conditions
should be communicated immediately to the newborn’s healthcare provider but no later than five days of life.
2. Presumptive positive results for all other conditions should be communicated to the newborn’s healthcare provider as soon as possible but no later than seven days of life.
3. All NBS tests should be completed within seven days of life.B. In order to achieve the above goals:
1. Initial NBS specimens should be collected in the appropriate time frame for the newborn’s condition but no later than 48 hours after birth, and
2. NBS specimens should be received at the laboratory as soon as possible; ideally within 24 hours of collection.

Additions to the Recommendations• The Committee encourages States to track their
progress in achieving each recommendation and support strategies that show progress in a transparent way.
• In order to support States with limited budgets, the Committee also encourages the Secretary to develop a grant program to further assist States in meeting the Committee’s recommendations.
• States are encouraged to have 95% or more of newborns meeting the timeliness goals by 2017 and to communicate their progress to a national data resource to be determined by DHHS.

Heritable Disorders Program: GSB Newborn Screening Activities• Staff the Discretionary Advisory Committee on
Heritable Disorders in Newborns and Children (DACHDNC)
• Establish grants – Support state newborn screening programs– Increase awareness and provide education for
broad range of stakeholders– Increase access to and coordinate services

Grant Programs to Support State NBS• Critical Congenital Heart Disease (CCHD)
Demonstration Program• Long-term Follow-up Program:
Demonstrate a plan for assessing the feasibility of establishing LTFU in a primary care setting
• Severe Combined Immunodeficiency (SCID) Newborn Screening Implementation Program

Grant Programs to Support State NBS• Timeliness of newborn screening
– ASTHO working State Health Officers– APHL CoIIN on timely NBS with 8 states
• HRSA-15-098 Improving Timeliness of Newborn Screening Diagnosis– Facilitate strategies and coordinate QI projects to
improve timeliness of newborn screening, diagnosis, and treatment in at least 20 state newborn screening programs.
– $1.8 M– 1 Cooperative agreement– Project period 9/1/2015 – 8/31/2018
New
New

Grant Programs
• Clearinghouse of Newborn Screening Information – Awarded Genetic AllianceAim: Increase awareness of newborn
screening• Newborn Screening Data Repository &
Technical Assistance Center – Awarded APHLAim: Measure performance of newborn
screening
Grant Programs to Support State NBS

NewSTEPs
NewSTEPs is the Newborn Screening Technical assistance and Evaluation Program
NewSTEPs is partnering with newborn screening programs throughout the U.S. to:
Provide technical assistance and resourcesCollate and summarize data in aggregate form Develop opportunities for quality improvement, locally, regionally, and nationally

National Data Repository for Newborn Screening
Purpose: Provide tools to state newborn screening systems to adequately evaluate, analyze, and benchmark the performance of their tests and the quality of their newborn screening programs

NewSTEPs Data Repository
• MOUs - 46% of NBS programs have fully ratified MOUs (or are close to ratifying) –
• Categories within repository– State Profiles (disorders screened,
policies, etc)– Quality Indicators (MOU required) – Case Level Data (MOU required)

Quality Indicator Data
• 8 Quality indicators developed vetted by the NBS community
• Track state progress over time• Upload tools available (many LIMS
vendors developing export queries for available data)

Purpose of the Newborn level data collected within NewSTEPs
“To provide an accurate characterization of the frequency of newborn screening disorders in the U.S., along with timing of screening and diagnostic activities”
Systematic definitions helpful at local AND national levels

Site Visit Reviews
• Part of the on-going technical assistance provided by NewSTEPs – at no cost to state
• Not regulatory• At the invitation of the state, a site visit is
scheduled and experts chosen depending on program needs
• Reviews all aspects of the newborn screening system—lab, follow up, expert care for infants diagnosed
• Two states visited to date: both made improvements in NBS program activities as result


• Title V of the Social Security Act, Section 502(a): Authorizing funds for Special Projects of Regional and National Significance (SPRANS) for
⁻ genetic disease testing, counseling, and information development and dissemination programs
⁻ comprehensive hemophilia diagnostic treatment centers without regard to age
⁻ the screening of newborns for sickle cell anemia, and other genetic disorders and follow-up services.
Legislative Authority

1. NEGC: New England Genetics Collaborative
2. NYMAC: New York-Mid-Atlantic Consortium
3. SERC: Southeast Regional Collaborative
4. Region 4: Region 4 Genetics Collaborative
5. Heartland: Heartland Regional Genetics and Newborn Screening Collaborative
6. MSGRCC: Mountain States Genetics Regional Collaborative
7. WSGSC: Western States Genetic Services Collaborative
Provide a regional infrastructure of public health genetics to improve, expand, and evaluate access to a system of genetic services and the quality of those services to improve health outcomes for children, youth and adults across their lifespan.
Regional Genetics Service Collaboratives (RCs)
National Coordinating Center - ACMG

National Genetics Education and Consumer Network (NGECN)
• Led by Genetic Alliance• Goal: Build a network of partnerships and
tools that improve consumers’ education about and access to genetic services, as well as improve the quality of those services
• Focus on consumer engagement in the RCs, supporting consumer-focused initiatives and groups, and public education

How do we evaluate what we’re doing?
• What are we doing?• How well are we doing it? • Is anyone better off because of it?

Going Forward• What are the gaps that a public health
approach can address? • What are the failures in the market
that HRSA can help address?• Who needs genetic services that
aren’t getting it?

Contact Information
Joan A. Scott, M.S., C.G.CChief, Genetics Services
Branch301-443-8860