Embed Size (px)
Citation preview

10/21/2015
1
Stephen Duckett
@stephenjduckett
Presentation to
Tasmanian Economic Forum
October 2015
Improving efficiency in
hospital care
2
What are we trying to achieve?
Cost/outcome
Cost/output
Outcome/output
3
0
5
10
15
20
25
30
35
40
45Real growth
Growth if spending
a constant
proportion of GDP
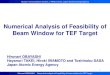
Change in Australian governments’ expenditure 2003-2013
$ bn relative to CPI
Health expenditure is the fastest growing
segment of government expenditure
Welfare Health Education Defence Infra-
structure
Ageing,
comm &
disability
services
Govern-
ment
Other
4
Hospitals are the fastest growing segment of
health expenditure
-5
0
5
10
15
20
25
Hospitals Primarycare andmedicalservices
Other Pharmac-euticals
Privatehealth
insurance
Notfurther
specified
Real growth
Growth if spending
a constant
proportion of GDP
Change in Australian governments’ health expenditure 2003-2013
$ bn relative to CPI

10/21/2015
2
5
-$2,000
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
Most of the spending increases is a result of
more services per person of a given age
Other
Health inflation
(beyond CPI)
Ageing
Population growth
Sources: AIHW; ABS; DOHA
Change in Australian governments’ health expenditure 2004-2011
2011$ m
Public
hospitals Medical
services
Medication
Private
hospitals
Research
Community
health
Dental
Other
6
Growth in spending is evenly balanced across
ages
Older population
$172
$108
$181
$250
$231
$187
$246
$246
$186
$438
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
0s 10s 20s 30s 40s 50s 60s 70s 80splus
Ageing (more elderly
people)
More services (to people of the same age)
Why are we spending more per person? Contribution to increase in per-person costs, 1989 to 2010
Note: Less reliance ought to be placed on figures for 80+, as sample sizes are small and data categories change across surveys
Source: ABS Fiscal Incidence Studies (various years); ABS Cat. 3101.0 Table 59; Grattan analysis
Age group
7
Projected Commonwealth government grants for
public hospitals to states have been cut substantially
(sort of)
Source: 2014-15 Budget Overview p7 http://budget.gov.au/2014-15/content/overview/download/Budget_Overview.pdf
Grattan Health
Program on
hospital waste

10/21/2015
3
9
Waste abounds in hospitals: proportion of
beds with identified waste at audit
Note: Only one type of waste was recorded for each bed.
Resar, R. K., et al. (2011) Hospital inpatient waste identification tool, Institute
for Healthcare Improvement 10
There is significant within-state variation in
public hospital costs (2010-11 data)
Note: Some small hospitals (total admissions < 4,000 p.a.) not shown
$0 $500 $1,000 $1,500 $2,000 $2,500 $3,000
NSW
VIC
QLD
WA
SA
TAS
ACT
NT
Unexplained costs above the lowest level in each state ($ per admission) Hospitals with the lowest unexplained cost in each state = 0
Hospitals
Average level of unexplained costs
Avoidable costs unexplained costs above the average level
11
Avoidable costs add up to $1 billion a
year
$0
$50
$100
$150
$200
$250
$300
ACTNTTASSAWAVICNSWQLD
Avoidable cost by state, 2010-11
$ million
12
$2,000 $4,000 $6,000 $8,000 $10,000
ACT
TAS
QLD
WA
SA
NSW
VIC
Range Median
There is huge variation in the cost of
treatments, e.g. gall bladder removal …
Cost of laproscopic colecystectomy (gall bladder removal), unadjusted, 2010-11
$2,000 $4,000 $6,000 $8,000 $10,000
Note: H08B, the less complicated DRG category for the procedure

10/21/2015
4
13
$0 $10,000 $20,000 $30,000 $40,000
ACT
TAS
QLD
SA
WA
VIC
NSW
Range Median
Cost of hip replacement, unadjusted, 2010-11
$0 $10,000 $20,000 $30,000 $40,000
Note: I03B, the less complicated DRG category for the procedure
… and hip replacements
14
4,128
4,478
6,029
6,106
7,934
$0 $5,000 $10,000 $15,000
Admissions
Median cost
High volume hospitals
A
E
D
C
B
Costs aren’t driven by scale Cost of gall bladder removal, unadjusted, five high-volume hospitals, 2010-11
Note: H08B, the less complicated DRG category for the procedure
15
There are three steps to remove avoidable
costs, starting with setting the right price
Arbitrary
Pay for
costs caused
by patient
factors
Don’t pay for
avoidable
costs
Pay for care that works
Adjust for
adverse
events
Adjust for
readmissions
Pay for
pathways
Adjust for
outcomes
Their own
pervious
standard
What care
does cost More
research &
better data
needed Average cost
Current
system
Grattan
proposal
Below-
average cost
What care
should cost
What costs are funded?
What
standard
should
hospitals
reach?
16
Medical workforce supply and demand – three
scenarios
80,000
85,000
90,000
95,000
100,000
105,000
110,000
115,000
Comparison Productivity gain Low demand
Supply Demand
Number of doctors 2025

10/21/2015
5
17
Job satisfaction improved with more complex
roles
Hospital specialists' overall job satisfaction by responses to the statement "I often undertake tasks that could be done by somebody less qualified
than me"
0%
20%
40%
60%
80%
100%
Strongly
disagree
(n=137)
Disagree
(n=811)
Neutral
(n=487)
Agree
(n=1040)
Strongly
agree
(n=427)
Satisfaction:
Very dissatisfied
Not sure
Moderately
satisfied
Very satisfied
Moderately
dissatisfied
18
There was very strong agreement with a wide range of
substitution options
Respondents were asked to what extent they agreed that the following shifts of workload would
reduce the cost without reducing quality and safety
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Interns to ENs
ENs to cleaners
Residents to clerical workers
ENs to clerical workers
RNs to personal care assistants
Specialists to RNs
RNs to clerical workers
Specialists to physician assistants
Residents to physician assistants
Residents to RNs
Interns to nurse practitioners
Interns to RNs
RNs to ENs
Residents to nurse practitioners
ENs to personal care assistants
Specialists to nurse practitioners
Occupational therapists to allied health assistants
Physiotherapists to physiotherapy assistants
Strongly agree Agree Neither Disagree Strongly disagree
5
19
Pharmacy staff mix and automation,
European hospitals, 2010
0
5
10
15
20
0
1
2
1–49 50–99 100–199 200–299 300–399 400–599 600–799 800–999 1000–1499 1500–2000 >2000
Hospital size (beds)
Pharmacists
Staff / 100 beds
Assistants
Per cent hospitals with stock dispensing robots (dots)
Frontini, R., Miharija-Gala, T. and Sykora, J. (2012) 'EAHP survey 2010 on hospital pharmacy in Europe: Part 1. General frame and staffing', European Journal of Hospital Pharmacy: Science and
Practice, 19(4), p 385-387 (and Part 2)
20
Substitution opportunities reported in
Victoria
0%
20%
40%
60%
80%
Nutrition OT Orthotics Physio Podiatry Social work
Speech path
Acute
Sub-acute
Percentage of time that allied health practitioners spend completing assistant-attributable tasks.

10/21/2015
6
21
Different barriers as a proportion of all responses (top barrier)
Professional culture and industrial relations were seen
as the biggest barriers to substitution across all fields …
7
0% 10% 20% 30% 40%
Blank
Implementation or transition costs
Substitute workforce availability
Management capacity
Other
Substitute workforce capacity/quality
Tradition
Registration restrictions
Industrial relations
Professional culture
22
Opportunity 1: Nursing assistants
• Identify roles currently
performed by registered
nurses that can be
performed by nursing
assistants
• Nurse assistants are
away of recruiting from a
different pool (non-school
leavers, returning to
workforce)
Registered nurses
Nursing assistants
23
Opportunity 2: Specialist roles for nurses
• International and Australian
evidence show that nurses can do
low-risk, high-volume procedures
well and safely
• We propose specialist nurse
endoscopy and nurse sedationist
roles
• Nurse endoscopists would only
provide less-complex endoscopies
(no biopsies or other interventions)
• Nurse sedationists would only work
in low-risk age groups and cases
Registered nurses
RN advanced roles
24
Opportunity 3: Allied health assistants
Physio, OT
Allied health assistants
(Physio, OT)
0% 20% 40% 60% 80%100%
Interns to ENs
ENs to cleaners
Residents to clerical…
ENs to clerical workers
RNs to personal care…
Specialists to RNs
RNs to clerical workers
Specialists to…
Residents to…
Residents to RNs
Interns to nurse…
Interns to RNs
RNs to ENs
Residents to nurse…
ENs to personal care…
Specialists to nurse…
Occupational…
Physiotherapists to…
Strongly agree

10/21/2015
7
25
GP
Practice
nurse
Physician
assistant
Opportunity 4: Physician assistants
Narrow scope
of practice
Wide scope
of practice
Autonomy
Delegation
GP or other medical practitioner
Physician assistant
26
Transition grants to facilitate change
1. Hospitals sign up to
• embed new roles in their workforce
• agree to a target ratio of existing
and new (not simply adding)
2. Hospitals get a time-limited grant to
fund a proportion of the cost of
introducing new workforce. It tapers
over time.
3. At mid-point, hospitals must prove they
are halfway to meeting the final staffing
ratio. The second half of the grant is
conditional upon demonstrating
progress.
4. The transition grant finishes at end of
workforce introduction period, by which
time new workforce roles embedded.
5. Savings will be passed back to the
system by a fall in the cost of care (and
prices).
Temporary subsidy for new roles
Change in workforce mix
Phase out subsidy with
system savings
27
What are we trying to achieve?
Cost/outcome
Cost/output
Outcome/output
28
Most variation analyses look at geographic
variation and find large disparities …
-125% -100% -75% -50% -25% 0% 25% 50% 75% 100% 125% 150%
MLA procedure rate: difference from national average
Cholecystectomy
Colectomy
Hip replacement
Lumpectomy
Mastectomy
Knee replacement
CABG
Open prostatectomy
Closed prostatectomy
Tonsillectomy
Appendectomy
Hysterectomy
Source: Grattan Institute

10/21/2015
8
29
… but that doesn’t tell you much
Procedure
rates
Highest
Lowest
… is it due to different case-mix?
… is it due to severity of condition?
… is it due to patient preferences?
… is it due to lack of certainty about effectiveness?
… what does regional analysis mean anyway?
High could be bad but …
Low could be bad but…
There’s little clarity about when variation is legitimate
That’s made it difficult to develop effective policy
30
Increasing certainty that variation can
identify inappropriate care
Variation in rates suggests inappropriate care
31
Increasing certainty that variation can
identify inappropriate care
Variation in rates suggests inappropriate care
On average this treatment should not be provided routinely for this class of patient
32
Increasing certainty that variation can
identify inappropriate care
Variation in rates suggests inappropriate care
On average this treatment should not be provided routinely for this class of patient
High level evidence that on average this treatment should not be provided for this class of patient

10/21/2015
9
33
Increasing certainty that variation can
identify inappropriate care
Variation in rates suggests inappropriate care
On average this treatment should not be provided routinely for this class of patient
High level evidence that on average this treatment should not be provided for this class of patient
Definitive advice that this treatment should not be provided in this patient
34
We analyse 5 ‘do-not-dos’ and 3 ‘do-not-do
routinely’ treatments from NICE, MSAC and Prasad
Do-not-dos:
• Vertebroplasty for osteoporotic vertebral fractures
• Arthroscopic lavage or debridement for OA of the
knee
• Laparoscopic uterine nerve ablation for chronic pelvic pain
• Removing healthy ovaries during a hysterectomy
• HBOT for a range of conditions (inc.
osteomyelitis, cancer, and non-diabetic wounds
and ulcers)
Do-not-do routinely:
• Fundoplication for gastro-intestinal reflux
• Episiotomy for spontaneous vaginal births
• Amniotomy to augment a normal delivery
Patients with ‘legitimating’ diagnoses are excluded
35
79
302
813
4659
0 1000 2000 3000 4000 5000
Nerve ablation
Ovary removal
Vertebroplasty
Knee arthroscopy
Hyperbaric oxygen
Do-not-do procedures, Australia, 2010-11
35
A large proportion of relevant patients have
do-not-dos
0% 10% 20% 30% 40% 50% 60%
Ovary removal
Hyperbaric oxygen
Vertebroplasty
Knee arthroscopy
Nerve ablation
36
-
20
40
60
80
100
120
-
1
2
3
4
5
NSW VIC QLD WA SA TAS NT
-
5
10
15
20
NSW VIC QLD WA SA TAS NT
Hyperbaric oxygen
chamber for various
conditions
Vertebroplasty for
compression fractures
Knee arthroscopy for
osteoarthritis
Removal of healthy ovaries
during hysterectomy
Nerve ablation
for pelvic pain
Rate
pe
r 1
00
0
‘DN
D’ p
atie
nts
Rate
pe
r 1
00
0
‘DN
D’ p
atie
nts
0
10
20
30
40
50
60
NSW VIC QLD WA SA TAS NT
0
20
40
60
80
100
120
NSW VIC QLD WA SA TAS NT
Rates of do-not-dos vary across states

10/21/2015
10
37
0%
20%
40%
60%
80%
Hospital
Average
Hyp
erb
aric
Art
hro
scop
y
Vert
eb
rop
lasty
Ova
ry r
em
ova
l
Nerv
e a
bla
tion
0%
10%
20%
30%
40%
50%
Amniotomy Episiotomy Fundoplication
Proportion of relevant patients getting do-not-do procedure Proportion of relevant patients getting do-not-do routlinely procedure
There are outliers with troubling patterns of
care
38
Information gap 1:
What not to do
0% 10% 20% 30% 40%
Consumer involvement documented
Setting identified
Users identified
Endorsed by other agencies
Replicable description of review
Recommendations linked to evidence
Professionals involved identified
Development process described
Quality indicators for Australian clinical practice guidelines, 2005-2013
Source: National Health and Medical Research
Council
0
0.2
0.4
0.6
0.8
1
1.2
1994199920042009
0
2
4
6
8
10
1994199920042009
Articles (million)
Articles (thousand)
• There is a huge volume of evidence
• Guidance focuses on what to do, is of variable quality, is
inconsistent & hard to use
• 50+ organisations work on disinvestment and their
approaches are largely uncoordinated and inconsistent
All
Systematic reviews
PubMed artices, 1994-2013
39
Information gap 2:
Who’s doing what
0%
20%
40%
60%
80%
Worse About the same Better or much better
Overall quality of health care Safe and skilled workforce
Responding to health care incidents
Proportion of board members Victorian LHNs, views on own network relative to average Victorian network
Notes: n = 233, 70% response rate, 96% of networks included
Source: Bismark et al (2013)
40
Hospital Name – 2010-11
Multiples of
national
rate DND/Rs
Relevant
patient
group Do-not-dos
HBOT DNDs - - - - - -
Removal of healthy ovaries 13.0 8 183
Vertebroplasty for CFs 0.0 0 31
Knee arthroscopy for OA 0.5 2 95
Nerve ablation for pelvic pain 0.6 1 75
Do-not-do routinely
Fundoplication for GORD 0.6 3 366
Episiotomy 2.9 211 1507
Amniotomy 0.4 26 1912
- - not in comparator group
Over benchmark
Less than 10% under benchmark
Recommendation 2:
ACSQHC report to all providers & funders

10/21/2015
11
41
Accountability gap
Recommendation 3: clinical reviews with
consequences
Identify outliers
Inform outliers that they are being
closely monitored
No further action State to initiate
external clinical review
Are they still
outliers after one
year?
Yes No
Does clinical
review support
practices? No further action Set clear targets for
improvement
No Yes
Are targets met?
No further action
No Yes
Financial and/or
governance sanctions
42
Recommendation 4:
Improve variation measurement
• Find more do-not-dos elsewhere (e.g.
Cochrane) and add more do-not-do
routinely treatments
• Link patient separations to
• analyse treatments that should not
be given first-line
• adjust for readmissions
• allow better adjustments for
morbidity
00%
10%
20%
30%
40%
50%
Linked imaging and pathology results
MBS and PBS diagnosis data
Linked records from MBS, PBS, hospitals
Hospital records (used in this report)
Measurable with:
Many more NICE do-not-dos can be measured with data we already collect
• Link to PBS and MBS data to acute data to allow measurement of more do-not-dos
(e.g. primary care do-not-dos, polypharmacy, patients not getting routine first-line
drug therapies)
• Pilot morbidity database for GP care in a few PHNs – collect data as part of MBS
billing
43
Some of our choices
• How much ‘benefit of doubt’ to give?
oIs a ‘Do Not Do’ a ‘Never Do’?
• Who should initiate investigation for potentially
inappropriate care?
• Is it OK for private hospital to be the focus (vs
surgeon)
• When should private insurers be able to deny
payment?
oWhen ACSQHC makes a determination?
oWhen clinical review makes a determination?
oWhen hospital fails to respond to external review?
44
What hospitals might do:
Table the Grattan report for discussion with the relevant
clinical governance group:
• Are any of the DNDs or DNDRs are an issue in the hospital?
• There are other issues we didn’t look at which are prominent in the
public debate (e.g. diagnostic test use). Are they relevant?
• How robust are your clinical governance processes?
• Is appropriateness of care being systematically monitored?
• What are the accountability mechanisms for clinical
choices?
• NB: I don’t think there are big savings for hospitals here
• NB: I do think this will be an increasing clinical governance
issue

10/21/2015
12
45
What Tasmania could do:
• Initiate clinical reviews where appropriate
for both the Do Not Dos and the Do Not Do
Routinelys
• Ask ACSQHC to develop a guideline
program about clinically ineffective care
• Ask ACSQHC to use link other data sets to
investigate other DNDs which can't be
identified with the Hospital Morbidity data
set
• Maybe start looking at cost-ineffective
care?
46
Some suggestions
• Drive (technical) efficiency through
• benchmarking
• tight(er) pricing (change range)
• workforce reform (change mean)
• Drive allocative efficiency through
• benchmarking
• P4P/nP4nP
• accountability for ineffective care























![Seed system of tef [Eragrostis tef (Zucc.) Trotter] In East Gojjam Zone](https://img.pdfslide.us/doc/110x75/589eca691a28ab384d8b4f63/seed-system-of-tef-eragrostis-tef-zucc-trotter-in-east-gojjam-zone-.jpg)



