Embed Size (px)
Citation preview
GastrointestinalDiseases
Test Kits for Research & Routine
1. Colorectal Cancer: prevention and early detection
2. Inflammatory bowel diseases
3. Exocrine pancreatic function
4. Food Intolerance
5. Infectious diseases
Content�
1. Colorectal Cancer: prevention and early detection ...............................3
2. Inflammatory bowel diseases .................................5
3. Exocrine pancreatic function ................................23
4. Food intolerances ............ 27
5. Infectious diseases .......... 36
Appendix: Stool sample preparation systems ............... 43
Albumin .........................................................................................................................................................................................6a1-Antitrypsin / a1-Antitrypsin Clearance..................................................................................................................7D-Arabinitol ..............................................................................................................................................................................41Calprotectin (PhiCal® Calprotectin) ................................................................................................................................9CRP (C-reactive Protein).....................................................................................................................................................12Chymotrypsin .........................................................................................................................................................................24b-Defensin 2 .............................................................................................................................................................................13Diamine Oxidase (DAO) ....................................................................................................................................................34EDN (EPX) ...................................................................................................................................................................................28Enterovirus ................................................................................................................................................................................39Ferritin ..........................................................................................................................................................................................14Gliadin ..........................................................................................................................................................................................29Gliadorphin (Gliadomorphin) ........................................................................................................................................31Hemoglobin ................................................................................................................................................................................4Hemoglobin-Haptoglobin-Complex ...........................................................................................................................4Helicobacter pylori ...............................................................................................................................................................37Histamin .....................................................................................................................................................................................35Lysozyme ...................................................................................................................................................................................15MutaGEL® Aldolase B .........................................................................................................................................................33MutaGEL® HLA-DQ 2+8 ....................................................................................................................................................30MutaGEL® Laktase (AS) .....................................................................................................................................................32Norovirus ...................................................................................................................................................................................38Myeloperoxidase (MPO) ...................................................................................................................................................16Pancreatic Amylase ..............................................................................................................................................................25Pancreatic Lipase ...................................................................................................................................................................26PMN-Elastase ...........................................................................................................................................................................17S100A8/A9 (MRP 8/14, Calprotectin) ........................................................................................................................10S100A12 (Calgranulin C, EN-RAGE) ............................................................................................................................11Salmonella sp. .........................................................................................................................................................................40Secretory IgA (sIgA) .............................................................................................................................................................18TNFa ............................................................................................................................................................................................19TNFa -Blocker Therapy Monitoring ...........................................................................................................................20Transglutaminase Antibodies .......................................................................................................................................29Zonulin ........................................................................................................................................................................................22
3
1. Colorectalcancer:preventionandearlydetection
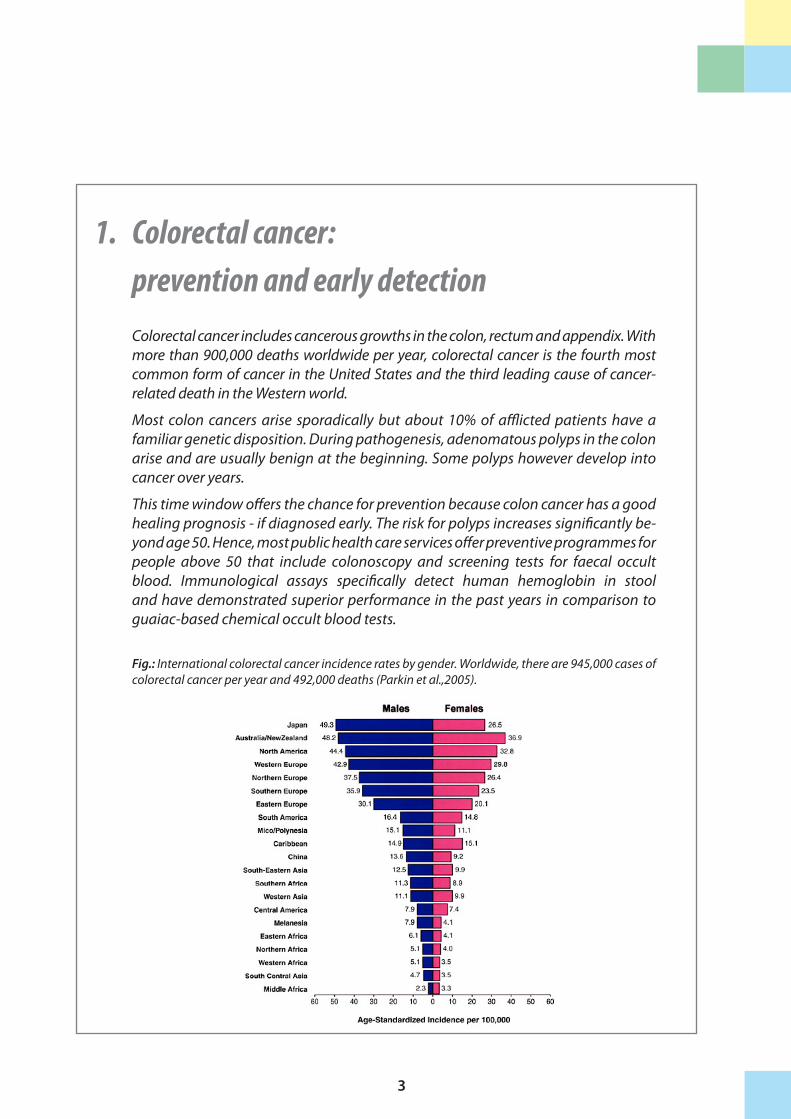
Colorectal cancer includes cancerous growths in the colon, rectum and appendix. With more than 900,000 deaths worldwide per year, colorectal cancer is the fourth most common form of cancer in the United States and the third leading cause of cancer-related death in the Western world.
Most colon cancers arise sporadically but about 10% of afflicted patients have a familiar genetic disposition. During pathogenesis, adenomatous polyps in the colon arise and are usually benign at the beginning. Some polyps however develop into cancer over years.
This time window offers the chance for prevention because colon cancer has a good healing prognosis - if diagnosed early. The risk for polyps increases significantly be-yond age 50. Hence, most public health care services offer preventive programmes for people above 50 that include colonoscopy and screening tests for faecal occult blood. Immunological assays specifically detect human hemoglobin in stool and have demonstrated superior performance in the past years in comparison to guaiac-based chemical occult blood tests.
Fig.: International colorectal cancer incidence rates by gender. Worldwide, there are 945,000 cases of colorectal cancer per year and 492,000 deaths (Parkin et al.,2005).

4
HemoglobinHemoglobin-Haptoglobin-ComplexIn contrast to commercially available rapid tests based on guaiac dye for the determination of hemoglobin, this hemoglobin ELISA does not require previous adherance to a diet (no raw meat etc.) and recognises human hemoglobin in 100-fold lower concentrations. This avoids false-negative results. Due to the choice of antibo-dies, false-positive results are practically absent.Recent data show that when determining the hemoglobin-haptoglobin- complexes (Hb-Hp complexes), the clinical specificity and sensitivity can be increased in cases of polyps and carcinoma.
Indications
• Occult blood in stool • Crohn’s disease, ulcerative colitis • Suspicion of colon carcinoma • Polyps in the colorectum
ReferencesHoepffner N et al. (2006) Aliment Pharmacol Ther 23:145-54Schirrmacher S et al. (2003) Abstract P4.54 of EUREGIO CCLM, 08.-10.10.2003, AachenTrojan J et al. (2002) Z Gastroenterol 40(11):921-24Sieg A et al. (1999) Int J Colorectal Dis 14 : 267-27Schmidt-Gayk H et al. (1994) Clin Lab 40:77-81
1.Colorectalcancer:preventionandearlydetection
Higher sensitivities in comparison to guaiac based occult blood tests
Detection of Hb-Hp complex increases detection rate of adeno-
mas in the upper intestinal tract
Highest sensitivity through combination of both parameters
(Sieg A et al. 1999 Int J Colorectal Dis 14:267-271;
Lüthgens K et al. 1988 Clin Lab 44:543-51)
New: both ELISAs easy to combineOne sample collection tube and one
dilution step for both parameters
1-Point-Calibration is possible for both assays (Cat. No. K 7836D, K 7837D)
Reference Values Hemoglobin
Stool: < 2 µg/ml
Hemoglobin-Haptoglobin-Complex (ELISA)
Sample volume 100 µlMatrix Stool Detection limit 0.081 µg/mlCalibrators 0.21 - 50 µg/gIncubation time 1 h; 1 h; 15 minTests 96 Cat. No. K 7817D
Hemoglobin (ELISA)
Sample volume 100 µlMatrix Stool Detection limit 0.447 µg/mlCalibrators 0.21 - 50 µg/gIncubation time 1 h; 1 h; 15 minTests 96 Cat. No. K 7816D
Reference Values Hemoglobin-Haptoglobin-Complex
Stool: < 2 µg/ml
5
2. Inflammatoryboweldiseases
Chronic diarrhea combined with gastrointestinal symptoms without infectious causes is indicative for a chronic, functional bowel disease.
In irritable bowel syndrome (IBS), digestion is impaired but the gut is not patholo-gically altered. The treatment of IBS differs individually and includes motility-modu-lating agents or even anti-depression therapy.
In contrast to IBS, inflammatory bowel diseases (IBD) like Morbus Crohn or Ulce-rative Colitis are caused by inflammatory pathologies of the gut mucosa and pose a severe health threat. IBD therapy therefore relies on inhibition of inflammation.
Since the symptoms for IBD and IBS overlap to a large degree, Immundiagnostik offers a broad portfolio of user-friendly ELISAs for the differential diagnosis of the diseases. Furthermore, we provide exclusive assays for monitoring and individual modulation of IBD-therapy which enable a comprehensive patient management.
The gut mucosa is an important immunocompetent system which performs local and systemic defense and control functions. To protect the organism, the mucosa establishes a powerful mechanic and immunological barrier - a complex system of immune and epithelial cells as well as a bacterial shield, the physiological intestinal flora.
Disruptions of the intestinal barrier, e.g. by mucosa irritations can increase the intestinal permeability and can lead to a "leaky gut syndrome", an overactivation of the immune system with elevated release of pro-inflammatory cytokines.
As a result, food intolerances, susceptibility to infections or nutrient deficiencies can occur. A pro-inflammatory alteration of the intestinal mucosa has also been obser-ved in IBD patients. The status of the intestinal barrier and of the intestinal immune system can be interpreted by an evaluation of marker proteins with the Immundia-gnostik ELISA portofolio.
Indications • Exclusion of intestinal infections• Differentiation of IBS and IBD• Diagnosis of Morbus Crohn, Colitis ulcerosa• Therapy monitoring of IBD patients• Integrity of the intestinal barrier• Analysis of the intestinal immune system
1.Colorectalcancer:preventionandearlydetection
6
Sandwich ELISA technology with two polyclonal
antibodies against human albumin
Short incubation time (2.5 hours)
High sensitivity
Designed to be suitable for processing small
amounts of specimen also
AlbuminChanges in the albumin concentration in plasma, urine und stool are mainly caused by distribution defects, rather than meatbolistic defects. In the case of nutrition with-drawal, the concentration of albumin falls below the lower reference range after one week at the earliest. In the case of protein deficient nutrition, the extent of edemas slightly correlates with the albumin concentration. Higher losses of albumin, e.g. nephrotic syndrome, leads to an increased synthesis.Increased albumin as well as increased haemoglobin concentrations in the stool are not only found in cases of colorectal carcinoma, but also in patients with polyps and chronic inflammatory bowel diseases (Crohn’s disease, ulcerative colitis).
Indications
• Detection of bleeding in the lower gastrointestinal tract • Identification of colorectal carcinomas • Crohn’s disease, ulcerative colitis • Examination of risk groups
ReferencesTrasch und Bloch (1993) Clin Lab 39: 479-484John et al. (1994) Clin Lab 40:77-81Berlet S, Armbruster FP, Aker I, Peters J, Schmidt-Gayk H (1986) J Clin Chem Biochem 24(10):771-772
2.Inflammatoryboweldiseases
Reference Values Albumin
Plasma, Serum 35 – 55 g/l
Urine 5 – 16 mg/l
Stool < 9,2 mg/l
Albumin (ELISA)
Sample volume 100 µlMatrix Urine
Stool (100 mg)Detection limit 12.5 µg/lCalibrators 12.5 - 800 µg/lIncubation time 1 h; 1 h; 15 minTests 96 Cat. No. K 6330

7
a1-Antitrypsin(Alpha-1-Proteinase-Inhibitor)
The a1-antitrypsin acts as a primary inhibitor of elastase from polymorphnuclear neutrophilic granulocytes (PMN) and is released during inflammatory processes in order to reduce the proteolytic activity of the PMN elastase in the inflammation region. In addition, it inhibits, via complex formation, a series of serin proteinase such as blood-clotting proteinases, trypsin, chymotrypsin, etc. Thus, the a1-antitrypsin plays an important regulatory as well as antiinflammatory role.
The a1-antitrypsin is a linear glycoprotein with a molecular weight of ca. 52 kDa (394 amino acid residues), a free cysteine residue and three carbohydrate side chains. It is predominantly synthesized in the liver but also by intestinal macrophages, mo-nocytes and epithelial cells. Although a1-antitrypsin is the main serine proteinase in-hibitor in human plasma, the proof of fecal a1-antitrypsin has become an important marker for intestinal protein loss and permeability as it is able to resist degradation in the gut due to its anti-proteolytic activity. It will, therefore, stay intact and it is pos-sible to detect it in the feces using an immunoassay.
Moreover, the measurement of fecal a1-antitrypsin concentration is used to eva-luate and monitor chronic inflammatory intestinal diseases. In the clinical routine, the a1-antitrypsin-clearence (ratio of the a1-antitrypsin-ELISA-values of stool and serum samples) has been established along with the sole determination of the 24h- a1-antitrypsin-secretion in stool. Thus, the group of J. S. Fordtran (Strygler et al. 1990) reports that the sole determination of the a1-antitrypsin-concentration in stool yielded false positive or false negative results in 21% of the patients compared to the a1-antitrypsin clearance measurements.
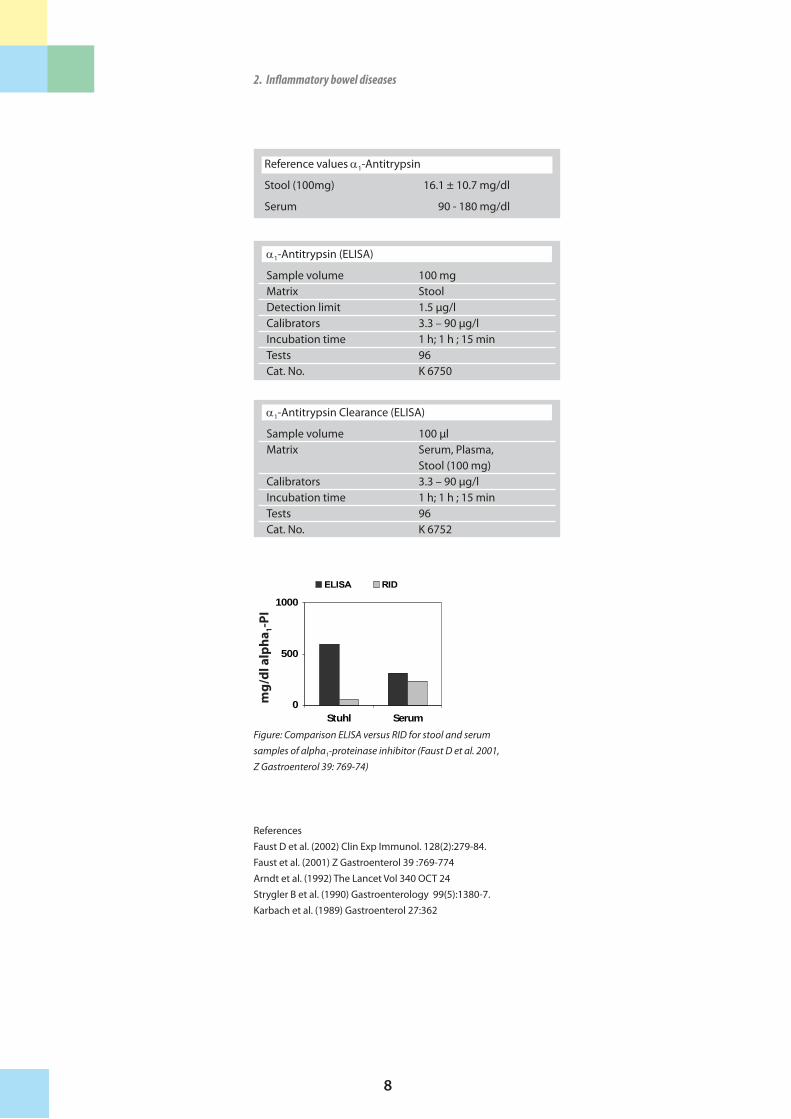
In a comparative study with the radial immune diffusion (RID), routinely used in the clinical diagnostics, the a1-antitrypsin-ELISA developed by Immundiagnostik demonstrated significant advantages in the analysis of serum, stool and Caco-2-cell culture supernatants (Faust et al. 2001):
• The a1-antitrypsin concentrations obtained by the ELISA were on average about 30 % higher than the corresponding values from the radial immuno- diffusion measurements. • Only the ELISA-system detected a1-antitrypsin in the cell culture superna- tants.
The results clearly demonstrate that our a1-antitrypsin-ELISA-test is more sensitive than other routinely used methods and that it recognizes the hepatic as well as the enteral a1-antitrypsin form. This newly developed test represents a promising alternative to the use of current clinical routine methods. It is superior to the radial immune diffusion especially in cases with extremely high protein loss through the intestine. The combination of two specific antibodies eliminates, to a large extent, the possibility of false negative results guaranteeing reliable diagnoses. This newly developed test is a non-invasive, simple test for the detection of protein loss through the intestine.
Indications
• Enteric protein loss and intestinal permeability • Morbus Crohn • Necrotic enterocolitis • Viral, bacterial or allergic inflammation
2.Inflammatoryboweldiseases
Sandwich ELISA It recognizes the a1-Antitrypsin form in stool.
Short incubation time (2 hours)
Designed to be suitable for small series of specimen also
2.Inflammatoryboweldiseases
ReferencesFaust D et al. (2002) Clin Exp Immunol. 128(2):279-84.Faust et al. (2001) Z Gastroenterol 39 :769-774Arndt et al. (1992) The Lancet Vol 340 OCT 24Strygler B et al. (1990) Gastroenterology 99(5):1380-7.Karbach et al. (1989) Gastroenterol 27:362
8
Figure: Comparison ELISA versus RID for stool and serum samples of alpha1-proteinase inhibitor (Faust D et al. 2001, Z Gastroenterol 39: 769-74)
0
500
1000
Stuhl Serum
ELISA RID
mg
/dl�a
lph
a 1-P
I
2.Inflammatoryboweldiseases
Reference values a1-Antitrypsin
Stool (100mg) 16.1 ± 10.7 mg/dl
Serum 90 - 180 mg/dl
a1-Antitrypsin (ELISA)
Sample volume 100 mgMatrix Stool Detection limit 1.5 µg/lCalibrators 3.3 – 90 µg/lIncubation time 1 h; 1 h ; 15 minTests 96 Cat. No. K 6750
a1-Antitrypsin Clearance (ELISA)
Sample volume 100 µlMatrix Serum, Plasma, Stool (100 mg)Calibrators 3.3 – 90 µg/lIncubation time 1 h; 1 h ; 15 minTests 96 Cat. No. K 6752
9
PhiCal® CalprotectinCalprotectin (MRP 8/14) is a heterodimer of two calcium-binding proteins present in the cytoplasm of neutrophils and expressed by the membranes of monocytes. It constitutes nearly 60% of the soluble cytosol proteins in neutrophils and plays a cen-tral role in neutrophil defense. Upon neutrophil activation or endothelial adhesion of monocytes, calprotectin is released and may be detected in serum, body fl uids or stool as a potentially useful clinical infl ammatory marker.
The acute phase protein shows a high stability in faeces (stable for one week at room temperature) and has been established as a faecal marker of infl ammatory bowel diseases (IBD). It allows a reliable diff erentiation between organic intestinal di-seases (e.g. chronic infl ammatory diseases, infectious diseases, polyps, colon cancer) and functional intestinal diseases (e.g. irritable bowel syndrome).
Calprotectin is ideal for monitoring disease activity (e.g. of M. Crohn or after polyp resection) and early detection of relapse. It shows high sensitivity in the detection of colorectal carcinoma (CC) and polyps (CRC: sensitivity 100%, polyps: sensitivity 88%).Due to the highly specifi c monoclonal�antibodies that the immunoassay is based on, the test detects only human calprotectin. The linear part of the calobration curve was optimised for easier diff erentiation between negative values, poorly increased values and high calprotectin values. This diff erentiation is important for excluding functional intestinal diseases (e.g. irritable bowel syndrome) and for the diagnosis and monitoring of organic intestinal diseases.
The better performance of the monoclonal� test� system in comparison to the polyclonal system has been shown in a study about prospective validation of faecal leucocyte markers in the diff erential diagnosis of chronic diarrhoea. There our mo-noclonal test system has proven to have a better performance than the polyclonal system which was used. Naumann et al. (2004) also found that of the investigated stool parameters (Calprotectin, MPO, Lactoferrin) only calprotectin was qualifi ed for discriminating between an organic diarrhoea and a functional diarrhoea.
Determination of faecal Calprotectin
• Chronic diarrhoea • Morbus Crohn, Colitis ulcerosa • Polyps
Calprotectin in faeces:
High stability in faeces
Ideal for monitoring disease acti-vity (e.g. of M. Crohn or after polyp resection) and early detection of relapse
For the discrimination between an organic and a functional diarrhoe
High sensitivity in detection of colorectal carcinoma (CC) and polyps
2.Infl ammatoryboweldiseases 2.Infl ammatoryboweldiseases
PhiCal® is a German trademark of Immundiagnostik AG, Bensheim
�Calprotectin��= MRP 8/14 = Calgranulin A/B = S100A8/A9
MRP� = Macrophage inhibitory factor-related protein
MRP�8/14�� = Heterodimer com-posed of light (MRP8) and heavy (MRP 14) chains (8 and 14 kDa)
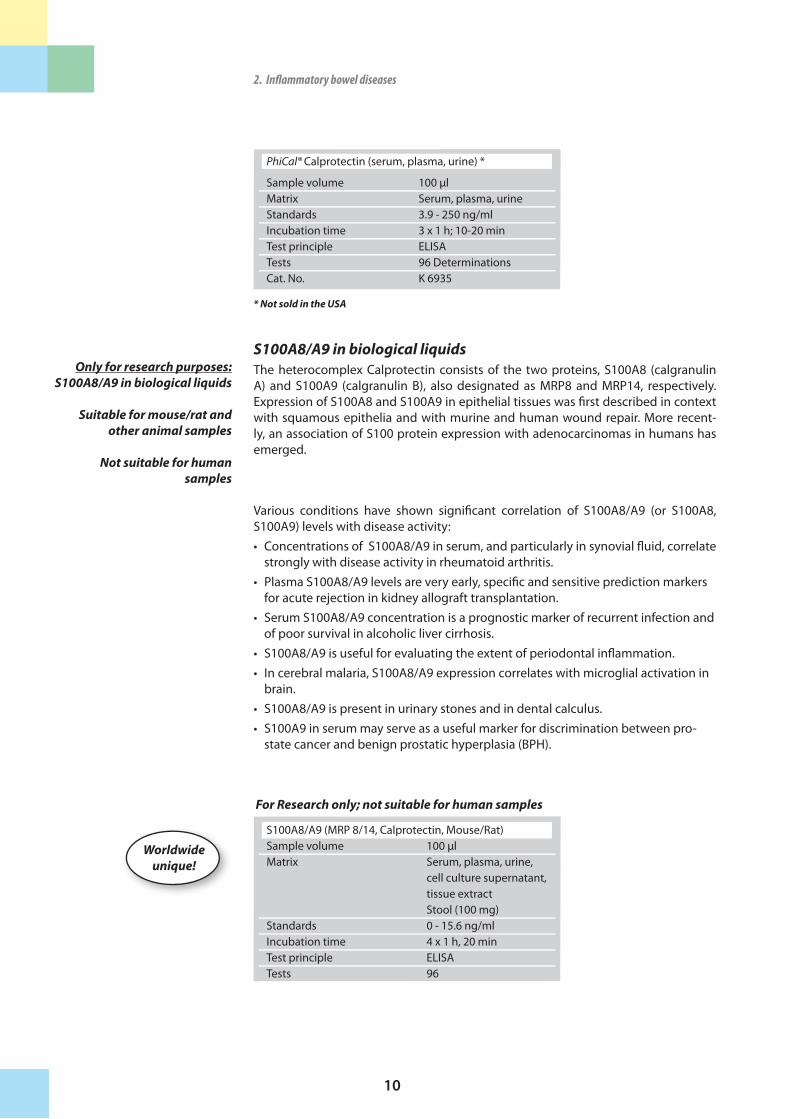
PhiCal® Calprotectin (Stool) (not sold in the USA)
Sample volume 100 mgMatrix StoolStandards 13 - 840 ng/mlIncubation time 1 h; 1 h; 10-20 minTest principle ELISATests 96 DeterminationsCat. No. K 6937 also available as 1-point-
calibration test (Cat. No. K 6947)
Reference Values Calprotectin
Stool: < 15 µg/g
Grey area: 15 - 50 µg/g
Cut off : 50 µg/g
PhiCal® Calprotectin (Stool) (not sold in the USA)
Sample volume 100 mgMatrix StoolIncubation time 2 x 30 minTest principle ELISATests 96 DeterminationsCat. No. K 6927
PhiCal®
NEW!
also available as 1-point-calibration test (Cat. No. K 6967)
also available as 1-point-
Incubation times only 2 x 30min
Ready-to-use conjugate
10
S100A8/A9 in biological liquidsThe heterocomplex Calprotectin consists of the two proteins, S100A8 (calgranulin A) and S100A9 (calgranulin B), also designated as MRP8 and MRP14, respectively. Expression of S100A8 and S100A9 in epithelial tissues was fi rst described in context with squamous epithelia and with murine and human wound repair. More recent-ly, an association of S100 protein expression with adenocarcinomas in humans has emerged.
Various conditions have shown signifi cant correlation of S100A8/A9 (or S100A8, S100A9) levels with disease activity: • Concentrations of S100A8/A9 in serum, and particularly in synovial fl uid, correlate
strongly with disease activity in rheumatoid arthritis. • Plasma S100A8/A9 levels are very early, specifi c and sensitive prediction markers
for acute rejection in kidney allograft transplantation. • Serum S100A8/A9 concentration is a prognostic marker of recurrent infection and
of poor survival in alcoholic liver cirrhosis. • S100A8/A9 is useful for evaluating the extent of periodontal infl ammation. • In cerebral malaria, S100A8/A9 expression correlates with microglial activation in
brain. • S100A8/A9 is present in urinary stones and in dental calculus. • S100A9 in serum may serve as a useful marker for discrimination between pro-
state cancer and benign prostatic hyperplasia (BPH).
Only for research purposes:S100A8/A9 in biological liquids
Suitable for mouse/rat and other animal samples
Not suitable for human samples
2.Infl ammatoryboweldiseases
Worldwide unique!
PhiCal® Calprotectin (serum, plasma, urine) *
Sample volume 100 µlMatrix Serum, plasma, urineStandards 3.9 - 250 ng/mlIncubation time 3 x 1 h; 10-20 minTest principle ELISATests 96 DeterminationsCat. No. K 6935
* Not sold in the USA
S100A8/A9 (MRP 8/14, Calprotectin, Mouse/Rat) Sample volume 100 µlMatrix Serum, plasma, urine,
cell culture supernatant, tissue extractStool (100 mg)
Standards 0 - 15.6 ng/mlIncubation time 4 x 1 h, 20 minTest principle ELISATests 96
For Research only; not suitable for human samples
11
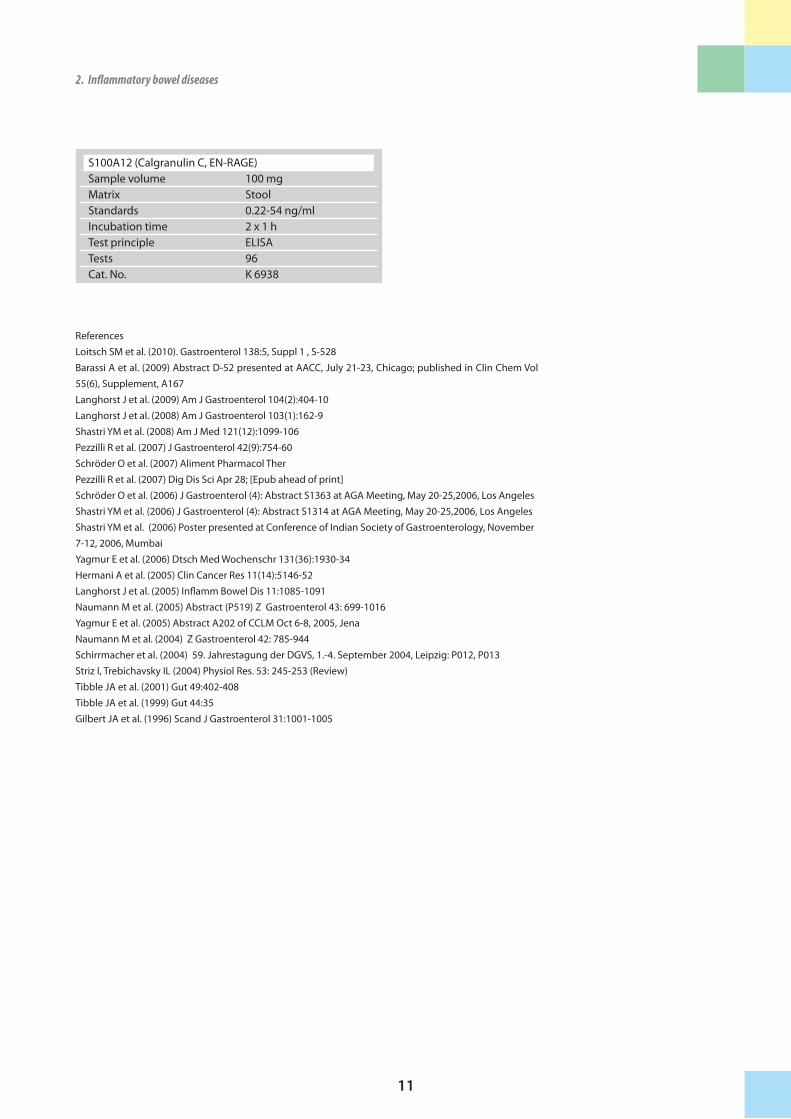
ReferencesLoitsch SM et al. (2010). Gastroenterol 138:5, Suppl 1 , S-528Barassi A et al. (2009) Abstract D-52 presented at AACC, July 21-23, Chicago; published in Clin Chem Vol 55(6), Supplement, A167Langhorst J et al. (2009) Am J Gastroenterol 104(2):404-10Langhorst J et al. (2008) Am J Gastroenterol 103(1):162-9Shastri YM et al. (2008) Am J Med 121(12):1099-106Pezzilli R et al. (2007) J Gastroenterol 42(9):754-60Schröder O et al. (2007) Aliment Pharmacol TherPezzilli R et al. (2007) Dig Dis Sci Apr 28; [Epub ahead of print]Schröder O et al. (2006) J Gastroenterol (4): Abstract S1363 at AGA Meeting, May 20-25,2006, Los AngelesShastri YM et al. (2006) J Gastroenterol (4): Abstract S1314 at AGA Meeting, May 20-25,2006, Los AngelesShastri YM et al. (2006) Poster presented at Conference of Indian Society of Gastroenterology, November 7-12, 2006, MumbaiYagmur E et al. (2006) Dtsch Med Wochenschr 131(36):1930-34Hermani A et al. (2005) Clin Cancer Res 11(14):5146-52Langhorst J et al. (2005) Inflamm Bowel Dis 11:1085-1091Naumann M et al. (2005) Abstract (P519) Z Gastroenterol 43: 699-1016 Yagmur E et al. (2005) Abstract A202 of CCLM Oct 6-8, 2005, JenaNaumann M et al. (2004) Z Gastroenterol 42: 785-944Schirrmacher et al. (2004) 59. Jahrestagung der DGVS, 1.-4. September 2004, Leipzig: P012, P013Striz I, Trebichavsky IL (2004) Physiol Res. 53: 245-253 (Review)Tibble JA et al. (2001) Gut 49:402-408Tibble JA et al. (1999) Gut 44:35 Gilbert JA et al. (1996) Scand J Gastroenterol 31:1001-1005
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
S100A12 (Calgranulin C, EN-RAGE) Sample volume 100 mgMatrix StoolStandards 0.22-54 ng/mlIncubation time 2 x 1 hTest principle ELISATests 96 Cat. No. K 6938
12
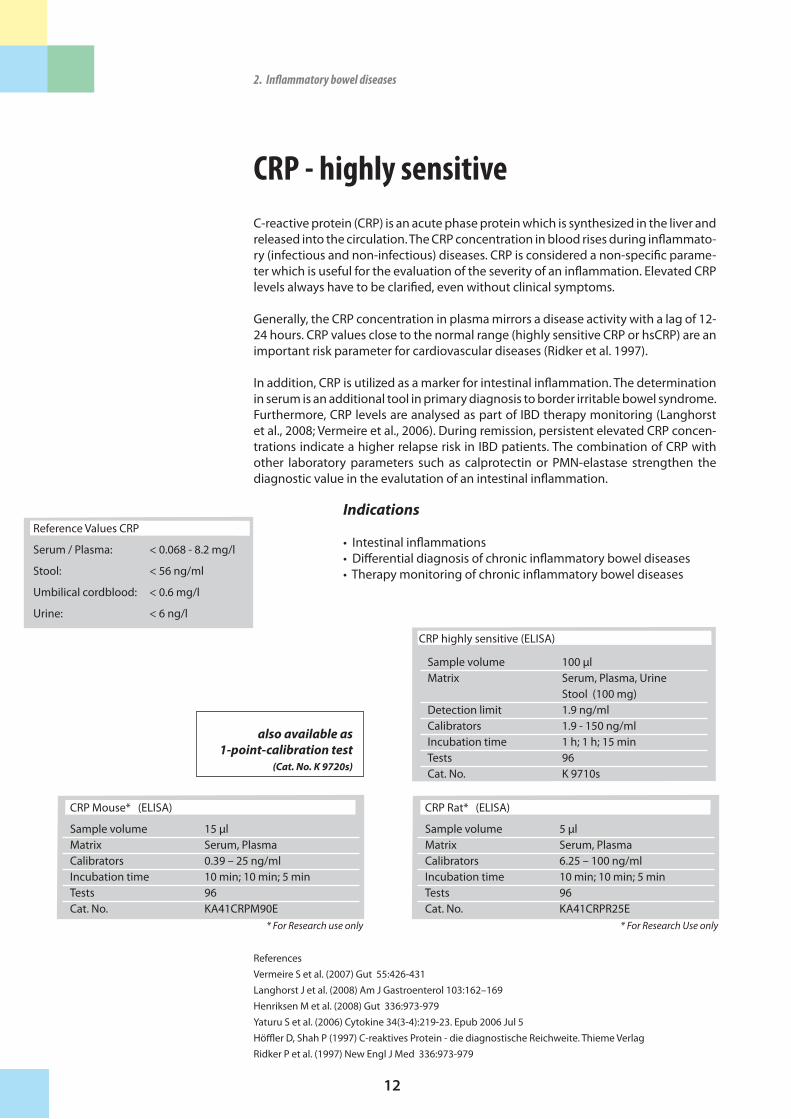
CRP - highly sensitiveC-reactive protein (CRP) is an acute phase protein which is synthesized in the liver and released into the circulation. The CRP concentration in blood rises during inflammato-ry (infectious and non-infectious) diseases. CRP is considered a non-specific parame-ter which is useful for the evaluation of the severity of an inflammation. Elevated CRP levels always have to be clarified, even without clinical symptoms.
Generally, the CRP concentration in plasma mirrors a disease activity with a lag of 12-24 hours. CRP values close to the normal range (highly sensitive CRP or hsCRP) are an important risk parameter for cardiovascular diseases (Ridker et al. 1997).
In addition, CRP is utilized as a marker for intestinal inflammation. The determination in serum is an additional tool in primary diagnosis to border irritable bowel syndrome. Furthermore, CRP levels are analysed as part of IBD therapy monitoring (Langhorst et al., 2008; Vermeire et al., 2006). During remission, persistent elevated CRP concen-trations indicate a higher relapse risk in IBD patients. The combination of CRP with other laboratory parameters such as calprotectin or PMN-elastase strengthen the diagnostic value in the evalutation of an intestinal inflammation.
Indications
• Intestinal inflammations• Differential diagnosis of chronic inflammatory bowel diseases• Therapy monitoring of chronic inflammatory bowel diseases
ReferencesVermeire S et al. (2007) Gut 55:426-431Langhorst J et al. (2008) Am J Gastroenterol 103:162–169Henriksen M et al. (2008) Gut 336:973-979 Yaturu S et al. (2006) Cytokine 34(3-4):219-23. Epub 2006 Jul 5Höffler D, Shah P (1997) C-reaktives Protein - die diagnostische Reichweite. Thieme VerlagRidker P et al. (1997) New Engl J Med 336:973-979
2.Inflammatoryboweldiseases
CRP Rat* (ELISA)
Sample volume 5 µlMatrix Serum, PlasmaCalibrators 6.25 – 100 ng/mlIncubation time 10 min; 10 min; 5 minTests 96Cat. No. KA41CRPR25E
* For Research Use only
CRP Mouse* (ELISA)
Sample volume 15 µlMatrix Serum, PlasmaCalibrators 0.39 – 25 ng/mlIncubation time 10 min; 10 min; 5 minTests 96Cat. No. KA41CRPM90E
* For Research use only
Reference Values CRP
Serum / Plasma: < 0.068 - 8.2 mg/l
Stool: < 56 ng/ml
Umbilical cordblood: < 0.6 mg/l
Urine: < 6 ng/l
Sample volume 100 µlMatrix Serum, Plasma, Urine
Stool (100 mg)Detection limit 1.9 ng/mlCalibrators 1.9 - 150 ng/mlIncubation time 1 h; 1 h; 15 minTests 96 Cat. No. K 9710s
CRP highly sensitive (ELISA)
also available as 1-point-calibration test
(Cat. No. K 9720s)

13
b-Defensin 2The b-defensins are an integral part of the congenital immune system and contribute with their antimicrobial effect to the barrier function of the intestinal epithelial cells. Defensins exert a variable degree of antimicrobial activity against bacteria, fungi, and some enveloped viruses. Vertebrate defensins are classified as a- or b-defensins, based on their pattern of disulfide bridges. Nine human defensins of epithelial origin have been found, three of them being b-defensins (HBD-1, -2 and -3).
The expression of b-Defensins are induced by the pro-inflammatory cytokines and also through microorganisms (e.g. E. coli, H. pylori or P. aeruginosa).
A reduced b-defensin 2 expression can, for example, be observed in the intestinal mucous of patients with Crohn’s disease. The defense system of the mucous memb-rane is therefore restricted and allows an increased invasion of bacteria, which could possibly lead to a typical infection in Crohn’s disease patients.
Whether the reduced b-defensin-2 expression could even play a role in the develop-ment of Crohn’s disease is currently being researched, as is the possibility that it is the probiotic bacterium which produces b-defensin.
Indications
• Inflammatory bowel diseases (IBD) • Research of intestinal barrier function
ReferencesKapel N et al.(2009) J Pediatr Gastroenterol Nutr 48(1):117-20Langhorst J et al. (2009) Am J Gastroenterol 104(2):404-10Soto E et al. (2007) J Matern Fetal Neonatal Med 20(1):15-22Langhorst J et al. (2007) Gut Apr 11, 2007 [Epub ahead of print]Langghorst J et al. (2006) Suppl 2 to J Gastroenterol (4):Abstract A205, S1340 vorgestellt bei 107th Annual Meeting of AGA, May 20-25, 2006, Los AngelesWehkamp J et al. (2003) J Clin Pathol 56: 352-357Schmid M et al. (2004) Z Gastro 42 : 333-338Harder J et al. (2001) J Biol Chem 276 : 5705-5713
Reduced b-defensin expression with Crohn’s disease (HBD-2)
Increased b-defensin expression with Colitis ulcerosa (HBD-2)
Also available for your research:
→ b-Defensin 5 ELISA and→ b-Defensin 6 ELISA
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
b-Defensin 2 (ELISA)Sample volume 100 mgMatrix Stool Standards 0.1 – 3 ng/mlIncubation time 3 x 1 h, 15 minTests 96 Cat. No. K 6500

14
FerritinIron deficit and the resulting anaemia are common disorders which can be caused e.g. by malnutrition, malabsorption or bleedings. The determination of iron and the binding capacity of total iron is therefore clinically relevant.Molecules like hemoglobin, hemosiderin, myoglobin and cytochromes act as iron reservoirs in the body. In most tissues however, ferritin is the prevalent iron storage. Human ferritin has a molecular weight of 450 kDa and consists of a protein shell co-vering an iron core - each ferritin molecule can carry up to 4000 Fe2+ atoms. Almost 20% of total iron in healthy individuals is stored in this way.The function of ferritin is the oxidation of Fe2+, the transport of Fe3+ into the core and its mobilisation. High ferritin concentrations can be detected mainly in liver, spleen and bone marrow.
The direct determination of iron in blood is not applicable for the detection of an iron deficit since these values are too inconsistent. Although the majority of ferritin mole-cules is intracellular, the ferritin concentration in serum is a meaningful parameter for the assessment of the total iron storage in the organism.
The analysis of the ferritin level is meanwhile routine in laboratory diagnostics and serves as a significant parameter in the diagnosis of anaemia and hemochromatosis.High ferritin concentrations indicate an iron overload which might be caused by hemochromatosis.Furthermore, ferritin status is used to monitor the iron supply in pregnant women, blood donors and dialysis patients. Ferritin serum concentrations also serve as an additional diagnostic parameter in inflammations, chronic liver diseases and tumors.
Indications
• Diagnosis of iron deficit / anaemia• Diagnosis and therapy monitoring of hemochromatosis• Iron status in pregnant women, blood donors and dialysis patients
For Research Use only
ReferencesWhite D et al. (1986) Am. J. Clin. Path. 72: 346Valberg L (1980) CMAJ. 122: 1240Forman D and Parker S (1980) Ann. Clin. Lab. Sci. 10: 345Hazard JT et al. (1977) J. Blood. 49: 139Smimes MA (1974) Blood. 43:581Clinical Guide to Laboratory Tests. Ed. Nw. Tietz, 3rd ED., W.B. Saunders Company, Philadelphia, PA 19106, 1995
Ferritin (ELISA)
Sample volume 20 µlMatrix SerumCalibrators 15 – 1000 ng/mlIncubation time 45 min; 20 minTests 96 determinationsCat.No. KD1872
2.Inflammatoryboweldiseases
15
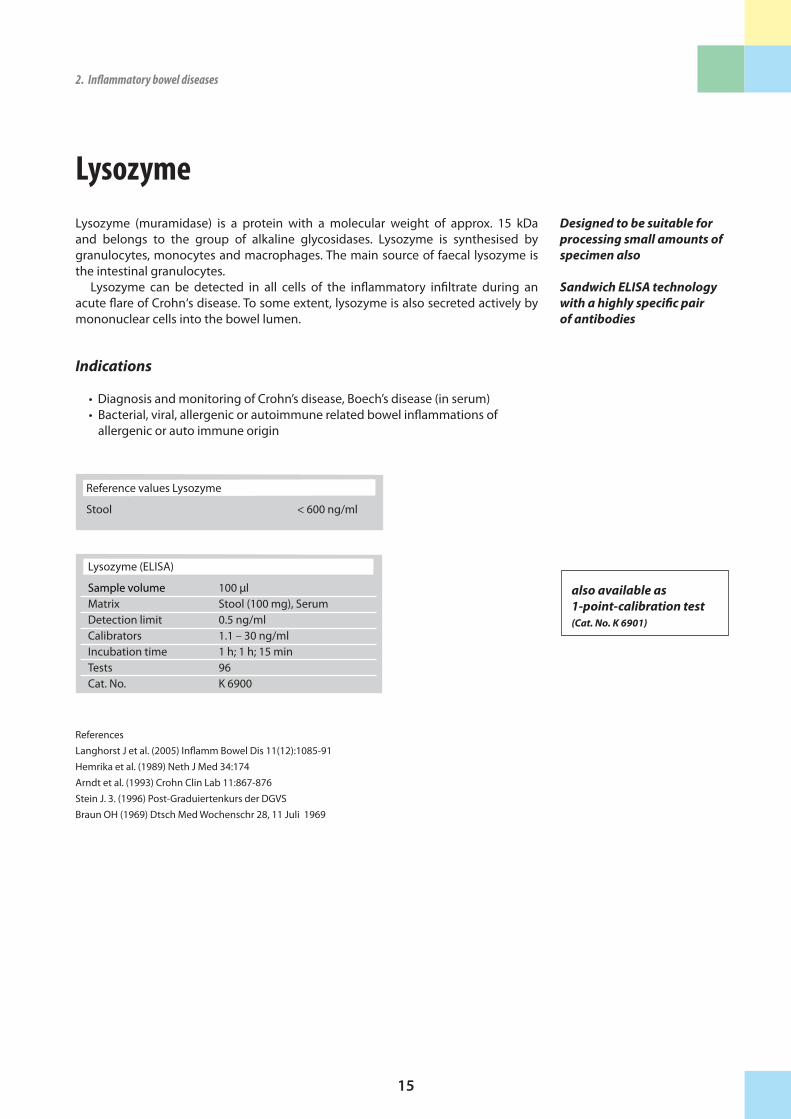
LysozymeLysozyme (muramidase) is a protein with a molecular weight of approx. 15 kDa and belongs to the group of alkaline glycosidases. Lysozyme is synthesised by granulocytes, monocytes and macrophages. The main source of faecal lysozyme is the intestinal granulocytes.
Lysozyme can be detected in all cells of the inflammatory infiltrate during an acute flare of Crohn‘s disease. To some extent, lysozyme is also secreted actively by mononuclear cells into the bowel lumen.
Indications
• Diagnosis and monitoring of Crohn’s disease, Boech’s disease (in serum) • Bacterial, viral, allergenic or autoimmune related bowel inflammations of allergenic or auto immune origin
ReferencesLanghorst J et al. (2005) Inflamm Bowel Dis 11(12):1085-91Hemrika et al. (1989) Neth J Med 34:174Arndt et al. (1993) Crohn Clin Lab 11:867-876Stein J. 3. (1996) Post-Graduiertenkurs der DGVSBraun OH (1969) Dtsch Med Wochenschr 28, 11 Juli 1969
Designed to be suitable for processing small amounts of specimen also
Sandwich ELISA technology with a highly specific pair of antibodies
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
Reference values Lysozyme
Stool < 600 ng/ml
Lysozyme (ELISA)
Sample volume 100 µlMatrix Stool (100 mg), SerumDetection limit 0.5 ng/mlCalibrators 1.1 – 30 ng/mlIncubation time 1 h; 1 h; 15 minTests 96 Cat. No. K 6900
also available as 1-point-calibration test (Cat. No. K 6901)
16
Myeloperoxidase (MPO)The granules of neutrophils (approx. 70 % of the white blood cells) contain a large number of different enzymes. Myeloperoxidase (MPO) catalyses the oxidation of substances via H2O2. The MPO H2O2 system has a toxic effect on many microorganisms such as bacteria, fungi, viruses and mycoplasma .
The efficiency of the bacteriocide myeloperoxidase H2O2 system is increased by PMN-Elastase. THE MPO determination in the stool reflects the inflammatory activity of Crohn’s disease or ulcerative colitis.
Indications
• Marker for inflammatory activities in the gastrointestinal tract • Renal transplant rejection
ReferencesSilberer H et al. (2005) Clin Lab 51(3-4):117-26Tomohisa et al. (1998) Kurume Medical Journal 45:69-73Kazunori et al. (1996) Am J Gastro, Vol 91(5)
Designed to be suitable for processing small
amounts of specimen also
Determination of MPO in different matrices
2.Inflammatoryboweldiseases
Reference Values Myeloperoxidase (MPO)
Stool < 2000 ng/ml
Serum mean value 340 ng/ml (SD 176.7)
EDTA-Plasma mean value 98.31ng/ml (SD 62.9)
MPO (ELISA)
Sample volume 100 µlMatrix Stool (100mg), UrineCalibrators 3.6 – 100 ng/mlIncubation time 1 h; 1 h; 1 h; 10-20 minTests 96 Cat. No. K 6630

17
PMN-ElastasePMN-Elastase from human polymorphonuclear granulocytes is a glycoprotein of 30 kDa and belongs to the group of serine proteases. Active PMN-Elastase is released from azurophil granula of neutrophil granulocytes after irritation or disintegration.The determination of the PMN-Elastase in stool is used to record inflammatory re-actions where neutrophil granulocytes are involved. Especially in Crohn’s disease the inflammatory processes go hand in hand with an increased phagocytic activity and the biological decay of these cells and thus leads to an increased release of PMN-Elastase and other lysosomal enzymes.
Indications
• Diagnosis of Crohn’s disease • Chronic arthropathy • Pancreatitis • Bacterial infection, sepsis
ReferencesEggert-Kruse W et al. (2008) Int J Androl, Jan 10. [Epub ahead of print] Langhorst J et al. (2008) Am J Gastroenterol 103(1):162-9Langhorst J et al. (2007) Z Gastroenterol 45: P261Langhorst J et al. (2005) Inflamm Bowel Dis 11(12):1085-91Silberer H et al. (2005) Clin Lab 51(3-4):117-26Heinichen et al. (1995) Clin Lab 41:539-545Oremek et al. (1995) MTA 10:273-278
Short incubation time (3 h)
Designed to be suitable for processing small amounts of specimen also
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
Reference Values PMN-Elastase
Stool 62 ng/ml
Serum 19 - 78 ng/ml
PMN-Elastase (ELISA)
Sample volume 100 µlMatrix Stool, Serum, Plasma, Seminal plasma, SynoviaDetection limit 0.12 ng/mlCalibrators 0.12 - 3.3 ng/mlIncubation time 3x1 h; 10-20 minTests 96 Cat. No. K 6840
also available as 1-point-calibration test (Cat. No. K 6830)
18
Secretory IgA (sIgA)Secretory IgA consists of two IgA monomers, which are connected to each other by a J-chain and contain a secretory component. They are produced in plasma cells located in the lamina propria of the mucous membranes and are found in body secretions, such as saliva, tears, nasal mucus, tracheobronchial mucus, gastrointesti-nal secretions, breast milk and colostrum.
The formation of secretory IgA occurs independently of the serum IgA synthesis. Therefore, a lack of serum IgA does not necessarily mean a lack of secretory IgA.
Neonates and infants are supplied with sIgA through breast milk and are therefore passively immunized against gastrointestinal infections.
Conclusions concerning the endogenic defence of the intestinal mucosa can be drawn from the concentration of the sIgA in stool. A deficiency of sIgA points to a diminished activity of the mucosa immune system, whereas increased sIgA values indicate increased activity and a local inflammation of the intestinal mucosa.
Indications
• Proof of an imbalanced immunological barrier of the intestinal mucosa • Autoimmune diseases
ReferencesMohan R et al. (2008) Pediatr Res 64(4):418-22.Michalsen A et al. (2005) BMC Complement Altern Med 5:22Hofman LF et al.(2002) Clin Chem Vol 48(6) Suppl A169Noel N et al. (2001) Abstract P 155 Clin Chem Vol 47 (6), Suppl A47Schütz B (1998) Biol Med 27:31-36Brandtzaeg P (1981) Clin Exp Immunol 44:221-231
Reference Values sIgA (Age > 16 years)
Stool 510 - 2040 µg/mlSaliva 102 - 471µg/ml
For Research only: For Research only:
2.Inflammatoryboweldiseases
sIgA (ELISA)
Sample volume 100 µlMatrix Stool (100 mg), body liquidsDetection limit 13.4 ng/mlCalibrators 22.2 – 600 ng/mlIncubation time 1 h; 1 h; 10-20 minTest principle ELISATests 96 Cat. No. K 8870
also available as 1-point-calibration test
(Cat. No. K 8880)
sIgA-1 (ELISA)
Sample volume 100 mgMatrix StoolCalibrators 3,3-100 UIncubation time 1 h; 1 h; 15 minTests 96Cat. No. K 6863
sIgA-2 (ELISA)
Sample volume 100 mgMatrix StoolCalibrators 3,3-100 UIncubation time 1 h; 1 h; 15 minTests 96Cat. No K 6864

19
TNFa Tumour�Necrosis�Factor�alpha (TNFa) belongs to the pro-inflammatory cytokines that encourage and uphold infection reactions. Cytokines, produced by macro-phages and t-cells, play a central role in both acute and chronic infections.
The TNFa concentration is raised in the affected joints in many rheumatic diseases (rheumatoid arthritis, chronic poly-arthritis, ankylosing spondylitis i.e. M. Bechterew disease) and plays a significant role in the joint destruction and in the courses of other diseases. Even in Crohn’s disease, an overproduction of TNFa can be observed that obviously affects the course of the disease.
In the 1990’s, pharmaceutical companies developed bio-technologically produ-ced medications that aimed at hindering TNFa (“TNFa blockers”) and therewith pro-duced a positive effect on the various disease symptoms (Feldmann et al. 2001).
ReferencesFeldmann M et al. (2001) Annu Rev Immunol 19:163-196
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
TNFa (ELISA)
Sample volume 100 mlMatrix Serum, Stool (100 mg), Cell Culture Supernatant, PlasmaCalibrators 16-500 pg/mlIncubation 2h, 1h, 1h, 10-20 minTests 96Cat. No. K 9610
20
TNFa-Blocker Therapy Monitoring1. Drug-level determination
Tumor Necrosis Factor alpha (TNFa) belongs to the pro-inflammatory cytokines that establish and sustain inflammation reactions. Cytokines, produced by macrophages and T-cells, play a central role in both acute and chronic inflammations.
The TNFa concentration is elevated in the affected joints in many rheumatic di-seases (rheumatoid arthritis, chronic poly-arthritis, ankylosing spondylitis i.e. M. Bechterew disease, psoriasis) and plays a significant role in joint destruction as well as in other manifestations of the diseases. Even in Crohn’s disease, an overproduction of TNFa has been observed, obviously affecting the activity of the disease.
In the 1990’s, pharmaceutical companies developed biotechnologically produced drugs that are aimed to neutralize TNFa (“TNFa blockers”) and expected to have a positive effect on the various symptoms of the diseases.In 1998, the first TNFa blockers were approved for use in the therapy of rheumatoid arthritis. Since then other TNFa blockers have been marketed:
• Infliximab (Remicade®), • Adalimumab (Humira®).
The two TNFa blockers are approved for treatment of rheumatoid arthritis as well as ankylosing spondylitis and psoriasis. Although the TNFa blockers differ in respect to their chemical structures and mechanisms of action, the pharmacological effects are the same for both substances. They are comparable in their effectiveness in fa-cilitating improvement in clinical symptoms of rheumatoid arthritis, but in Crohn’s disease, Infliximab has proved to be the most effective one.
The therapeutic effect of the anti TNFa antibodies on chronic inflammations, i.e. Crohn’s disease or rheumatoid arthritis, depends on the serum concentration of the corresponding pharmaceutical. In many patients, the treatment is of limited value, because of a fast degradation of the pharmaceutical or generation of antibodies against it. For a better control of the therapy, drug level monitoring is necessary.
Our ELISA test can be used for monitoring anti-TNFa-antibodies (e.g. Remicade®, Humira®) and provides a basis for possible preventive strategies.
Indication:
• Continuous TNFa Blocker therapy monitoring
2.Inflammatoryboweldiseases
With our ELISA test, anti-TNFa-therapeutic antibodies can be
detected
As an orientation:
To ensure clinical effectiveness of the TNFa inhibitor, the serum level should be at/above 12 mg/
ml in week 4 and at/above 5 mg/ml in week 8.
TNFa-Blocker-Monitoring(drug-level, e.g. Remicade®)
Sample volume 100 mlMatrix SerumIncubation 1h, 1h, 10-20minTest principle ELISATests 96Cat. No. K 9655
TNFa-Blocker-Monitoring(drug-level, e.g. Humira®)
Sample volume 100 mlMatrix SerumIncubation 4h, 1h, 10-20minTest principle ELISATests 96Cat. No. K 9657
21
2. ADA (anti-drug-antibodies) determination
Problems in the therapy with TNFa antibodies occur when the human organism de-velops antibodies against the therapeutical antibody i.e. against the TNFa-blocker (among others). In a cohort study 61%�of�M.�Crohn�patients�treated�with�Inflixi-mab� reacted� with� the� development� of� antibodies� against� Infliximab� (Baert et al. 2003). The presence of antibodies in 7-19% of patients could be associated with infusion reactions. Allergic reactions, and also therapy failure, could be attributed to the development of such antibodies. Through the parallel administration of immu-no-suppressants (mostly Methotrexat) a reduction of antibody development could, at least, be achieved (Colombel et al. 2004).
Our ELISAs enable the detection of human antibodies against: • Adalimumab (fully humanistic antibody to TNFa, e.g. Humira®) • Infliximab (chimeric, monoclonal antibody to TNFa, e.g. Remicade®) • Etanercept (genetically produced variant of TNF receptors, e.g. Enbrel®)
Indications:
Therapy monitoring for therapy with antibodies against TNFa or therapy with TNFa-receptors
ReferencesSeow et al. (2009) Gut, publ. online, doi:10.1136/gut.2009.183095Bendtzen et al. (2009) Scand J Gastroenterol 44:774-781Ainsworth et al. (2008) Am J Gastroenterol 103:944-948Radstake et al. (2008) Ann Rheum Dis, publ. online, doi:10.1136/ard.2008.092833Baert F et al. (2007) Acta Gastroenterol Belg. Apr-Jun;70(2):163-70Bender N et al. (2006) Rheumatol Int, publ. online, doi:10.1007/s00296-006-0183-7Baert F et al. (2003) N Engl J Med 348 : 601-608Bender N et al. (2006) Rheumatol Int 2006 Sep 28 [Epub ahead of print]Colombel J et al. (2004) Gastroenterology 126: 19-31Cohen R D et al. (2000) Am J Gastroenterol 95 : 3469-3477
2.Inflammatoryboweldiseases 2.Inflammatoryboweldiseases
Our ELISAs enable the de-tection of human antibody against therapeutical anti-bodies / TNF receptors
Bender et al. (2006) found out that adalimumab is immunogenic and induces antibodies in a high rate in adalimumab-treated patients
TNFa-Blocker-ADA (anti-drug-antibodies, e.g. Enbrel®)
Sample volume 5 mlMatrix SerumIncubation o.N., 1h, 5-10minTest principle ELISATests 96Cat. No. K 9653
TNFa-Blocker-ADA (anti-drug-antibodies, e.g. Remicade®)
Sample volume 5 mlMatrix SerumIncubation o.N., 1h, 5-10minTest principle ELISATests 96Cat. No. K 9650
TNFa-Blocker-ADA (anti-drug-antibodies, e.g. Humira®)
Sample volume 5 mlMatrix SerumIncubation o.N., 1h, 5-10minTest principle ELISATests 96Cat. No. K 9652

22
Zonulin Zonulin is a novel human protein analogue to the Vibrio cholerae derived Zonula occludens toxin, which participates�in�tight�junctions�between�cells�of�the�wall�of�the�digestive�tract. Zonulin binds to a specific receptor on the surface of intestinal epithelia and triggers a cascade of biochemical events which induces tight�junction�disassembly and a subsequent permeability increase of the intestinal epithelia, al-lowing some substances to pass through and activate immune reactions.
A. Fasano and his co-workers found out that the zonulin-zonulin-receptor-system is more activated in celiac�disease and type 1 diabetes mellitus patients. Patients with active celiac disease showed higher levels of zonulin and anti-zonulin antibo-dies compared to non-celiac patients and patients in remission, who were eating a gluten-free diet.
In addition, it was reported that many people who suffer from celiac disease also suffer from other autoimmune disorders. It is suggested that increased levels of zo-nulin are a contributing�factor�to�the�development�of�celiac�disease�and�other�autoimmune�disorders such as insulin dependent diabetes, multiple sclerosis, and rheumatoid arthritis.
ReferencesWang W et al. (2000) J Cell Sci 113 Pt 24: 4435-40. Fasano A (2001) Gut 49: 159-62.Fasano A et al.(2000) Lancet 355(9214): 1518-19.Thomas KE et al. (2006) J Immunol 176: 2512-21. Freemark M et al. (2003) Diabetes Care 26: 1932-39.Lazzarotto F et al. (2003) Diabetes Care 26: 248-49.Watts T et al. (2005) Proc Nat Acad Sci USA 102(8): 2916-21.Sapone A et al. (2006) Diabetes 55: 1443-9.De Magistris MT (2006) 24 Suppl 2: S2-60-1Hilbig H et al. (2008) Poster presented at the CIMT Meeting, 15.-16.05.2008, Mainz, GermanyWex T et al. (2009) Peptides 30(6):1082-7
2.Inflammatoryboweldiseases
ELISA for the detection of tight junctions now
available for your research
Zonulin* (ELISA)
Sample volume 50 µl Matrix Serum, EDTA-Plasma Stool (100 mg)Standards 0.97–1000 ng/mlIncubation time 1.5 h, 1.5 h, 1.5 h, 10 minCat. No. K 5600
* For Research only

23
2.Inflammatoryboweldiseases
3. Exocrinepancreaticfunction
The pancreas is an important exocrine gland of the digestive system. It secretes en-zymes and their precursors for the cleavage of proteins, sugars, nucleic and fatty acids. This enzymatic "cocktail" enables the decomposition of food in the small in-testine.
Next to this basic exocrine function, the pancreas acts as an endocrine gland by re-leasing hormones that regulate the blood sugar level into the circulation, e.g. insulin and glucagon.
Immundiagnostik offers assays for the analysis of the exocrine pancreatic functions which can be used for diagnosis and therapy monitoring of diseases, such as exocri-ne pancreas insufficiency or chronic pancreatitis.
24
ChymotrypsinChymotrypsin is a serine protease, which is secreted as anexcretory enzyme from the pancreas after food intake into the duodenum. Here food proteins are hydrolytically cleaved, preferentially next to aromatic residues. A small part of the active form of the enzyme is exreted in the stool. In pancreas insufficiency secondary to a chronic pancreatitis, the secretion of the enzyme is reduced markedly. In the past an exocrine pancreatic insufficiency within the scope of a chronic pancreatitis was diagnosed e.g. by determining faecal elastase or chymotrypsin activity in stool. The colorimetric determination of chymotrypsin activity, however, is less reliable because the enzyme´s activity is influenced by enzyme inhibitors in stool. Our ELISA allows the determination of the chymotrypsin concentration in stool. Besides the determination of the chymotrypsin concentration, we offer a photo-metric test for the determination of chymotrypsin activity in stool.
Indications
• Chronic pancreatitis • Exocrine pancreas insufficiency
ReferencesGoldberg et al. (1971) Comp Biochem Physiol B38: 697Kaspar P et al. (1984) Clin Chem 30:1753 – 1757Stein et al. (1996) Clin Chem 42:222 – 6
3.Exocrinepankcreasfunction
Determination of the chy-motrypsin concentration:
The enzyme substituti-on does not have to be
discontinued before taking the stool sample (no false
normal values in continued substitution)
Long storage of stool samples
(up to 10 days at bei RT)
Chymotrypsin Concentration (ELISA) Sample volume 100 mgMatrix Stool (100 mg)Standards 15.6 – 1000 mg/mlIncubation time 1 h; 1 h; 1 h; 30 minTests 96 Cat. No. K 6910
Chymotrypsin Activity (photometric) Sample volume 100 mgMatrix Stool Tests 20 Cat. No. K 6990
25
3.Exocrinepankcreasfunction 3.Exocrinepankcreasfunction
Pancreatic AmylaseLike lipase and elastase, pancreatic amylase is synthesised in the pancreas. In the case of chronic pancreatitis, pancreatic amylase concentration is decreased. Some forms of disease (alcoholism, accidental trauma, fibrosis), are associated with a pancreatic insufficiency.In the routine laboratory pancreatic amylase has proved itself to be a genuine alter-native to elastase-I in stool diagnosis with apparently higher clinical specificity and sensitivity.
Indications
• Chronic pancreatitis
ReferencesBishop M. et al. (1996) Pancreas 13:226-30Katschinsky M. et al. (1997) Pancreas 15 :1991-200
Sandwich ELISA technology with a highly specific antibody pair (no cross-reaction to salivary amylase and porcine amylase)
Good stability of Pancreatic amylase in stool
Reference Values Pancreatic Amylase
Serum 26 - 325 µg/l
Stool < 124 mg/l
Pancreatic Amylase (ELISA)
Sample volume 100 µlMatrix Serum, Stool (100 mg)Calibrators 440 - 28000 mU/lIncubation time 1h; 30 min; 15 minTests 96 Cat. No. K 6410

26
Pancreatic LipaseThe pancreatic lipase (triacylglycerol acylhydrolase) is a specific pancreatic enzyme which hydrolyzes primarily glycerol ester of long chain fatty acid. The activity of this enzyme is elevated in patients with acute pancreatitis. The determination of pancre-atic lipase is therefore an important parameter for the detection and differentiation of pancreatic diseases, esp. in combination with the determination of the pancreatic amylase.Conventional turbidimetric methods to assess lipase activity are complex, non-speci-fic and exhibit a low sensitivity. In contrast, our ELISA detects human pancreatic lipase in serum quantitatively and with high specificity.
ReferencesLott JA et al. (1986) Clin Chem 32:1290Lott JA et al. (1986) Clin Enzymol: 245Tietz NW (1986) Clin Chem 32:301-307Tietz NW (1987) Clin Chem 33: 624Panteghini M et al. (1989) Clin Chem 35:417Verduin PA (1973) Clin Chi Acta 46:11-19
Pancreatic Lipase (ELISA)
Sample volume 100 µl�Matrix Stool (100 mg), SerumCalibrators 10 - 400 U/lIncubation time 30 min; 10 minTests 96 determinationsCat. No. K 6495
3.Exocrinepankcreasfunction
27
4. Foodintolerances
Food intolerances include enzyme defects (e.g. lactose or histamine intolerance) as well as immunological intolerances (e.g. gluten intolerance).
Often, these intolerances are caused by gene defects and are therefore congenital. In addition, they can be caused by diseases or diet.
Depending on the kind of food intolerance, different methods are used for diagno-sis. Next to provocation tests and bowel biopsies, a number of laboratory parame-ters in urine, serum/plasma or stool along with DNA-analysis tools enable a reliable detection of food intolerances.
Immundiagnostik offers specific assays for the detection and differentiation of various intolerances.
A special focus of Immundiagnostik is the basic understanding of gluten intolerance and the supply of comprehensive laboratory analysis tools for the detection of even atypic and silent forms.
3.Exocrinepankcreasfunction

28
EDN (Eosinophil-derived Neurotoxin)EDN (eosinophil derived neurotoxin, eosinophil protein x, EPX) measuring in stool is recommended for diagnosing�a�food�allergy�with�an�immediate�reaction or to test the clinical efficiency of an elimination diet. EDN measurements also support an exa-mination of the integrity of the intestinal mucous, when looking into an inflammable intestinal disease, investigating Colon Carcinoma or for the diagnosis of an intestinal parasite.The classic ways of diagnosing an allergy (determine allergy specific IgE antibodies and the prick-test) are only limitedly reliable when used to determine a food allergy.For example a normal IgE level and a negative result from the prick-test doesn’t rule out an intestinal food allergy. In this case, an EDN measurement in stool is recommended. EDN, a cationic glycoprotein, which is released by activated eosinophiles, has strong cytotoxic characteristics and plays a large part in virus prevention. It is released by the eosinophile granules in places where eosinophiles are mainly to be found, in the skin, lungs, urogenital and gastrointestinal tracts, that is, in the organs which act as an entry point for pathogen. The accumulation of EDN in the intestine is associated with tissue damage.Measuring EDN in stool can serve as an objective parameter for a current clinical or sub-clinical cronic inflammation which is noticeable in the gastrointestinal area. With Colitis ulcerosa and Crohn’s disease, the EDN measurement helps the evaluation of a disease’s activity and the prediction of it possible.
Indications
• Proof of a food allergy with immediate reaction • Assessment of an elimination diet • Proof of damaged integrity of the intestinal mucous membrane caused by an invasive disease (e.g. CED, CC etc.) • Proof of intestinal parasites
ReferencesMagnusson J et al. (2003) Clin Exp Allergy 33 : 1052-1059Bengtsson U et al. (1997) J Allergy Clin Immunol :100 : 216-221Bischoff SC et al. (1997) Dig Dis Sci 42(2) 394-403Petersen CGB et al. (2002) Am J Gastroenterol 97(7) 1755-1762
4.Foodintolerances
EDN (ELISA) Sample volume 100 µlMatrix Serum, Urine, Plasma, Stool (100 mg)Detection limit 0.125 ng/mlStandards 0.6 – 40 ng/mlIncubation time 1 h, 1 h, 10 minTests 96 Cat. No. K6811
Proof of a food allergy with immediate reaction
A non-invasive examination of the
intestinal eosophile activity.
Validated in stool, urine, serum, plasma
Stable in stool for seven days
29
Glutensensitivity
Gliadin / Transglutaminase AntibodiesCeliac disease/ gluten intolerance is a chronic gastrointestinal disease with a prevalence of about 1:250 in Europe.
The definition of gluten intolerance has to be revised due to new data regarding its prevalence. The classic diagnosis of fully developed celiac disease by biopsy-proven villous atrophy only represents the tip of the iceberg.The iceberg model of Logan clearly indicates that the majority of patients with gluten intolerance do not present with fully developed celiac disease. The early diagnosis and the subsequent initiation of a gluten-free diet is instrumental in preventing a total atrophy of the intestinal mucous layer.
In patients presenting with long-term, unspecific abdominal complaints secondary to gluten intolerance, the quality of life can be improved considerably after an early diagnosis and a timely initiation of a gluten-free diet. Gluten intolerance is, next to its classic symptoms, associated with other autoimmune diseases (rheumatoid arthritis, dermatitis herpetiformis Duhring or diabetes mellitus) or with a risk of miscarriage.We offer a unique product line for the purpose of evaluating unspecific abdominal complaints, especially when gluten intolerance is suspected. Beside the assays for the determination of anti-transglutaminase�IgA�antibodies�from�serum, we offer tests for the determination of anti-transglutaminase�sIgA/IgA�from�faeces. The tissue transglutaminase and also the epidermal transglutaminase have been proven to be associated with gluten intolerance. The epidermal transglutaminase especially is associated with extraintestinal manifestations like Dermatitis herpetiformis Duhring.Gluten intolerance is caused by gliadins or analogous proteins in cereals. It is well known that this (auto-)immunological disease strikes individuals with a special genetic profile: there is a strong association with specific risk alleles encoding the heterodimeric HLA-DQ2 molecule (>90 % of the patients) or respectively the HLA-DQ8 molecule. The MutaGEL HLA-DQ 2+8 test allows the individual HLA-DQ� genotyping by amplification of the encoding allels (for 24 determinations). For this purpose, only a small sample of EDTA-blood is necessary for the preliminary extraction of DNA (reagents not included). The subsequent processing with molecular biological methods leads to specific amplification products detectable by gel-electrophoresis.
Indications
• Poor appetite and failure to gain weight • Iron-deficiency anaemia• Neurological disturbances (e.g., depression, lethargy)• Infertility• Recurrent abortions (Untreated pregnant women are
at risk of miscarriage and at risk of having a baby with a congenital malformation)
• Dermatitits herpetiformis Duhring• Rheumatoid arthritis symptoms
4.Foodintolerances 4.Foodintolerances(Glutensensitivity)
Classic celiac diseases: only the tip of the iceberg (Logan's iceberg model)
Reference Values Anti-Transglutaminase
Serum ≥ 7 AU positive
Stool > 100 U/l positives
Reference Values Anti-Gliadin
Serum ≥ 18 AU positive
Stool > 100 U/l positives
30
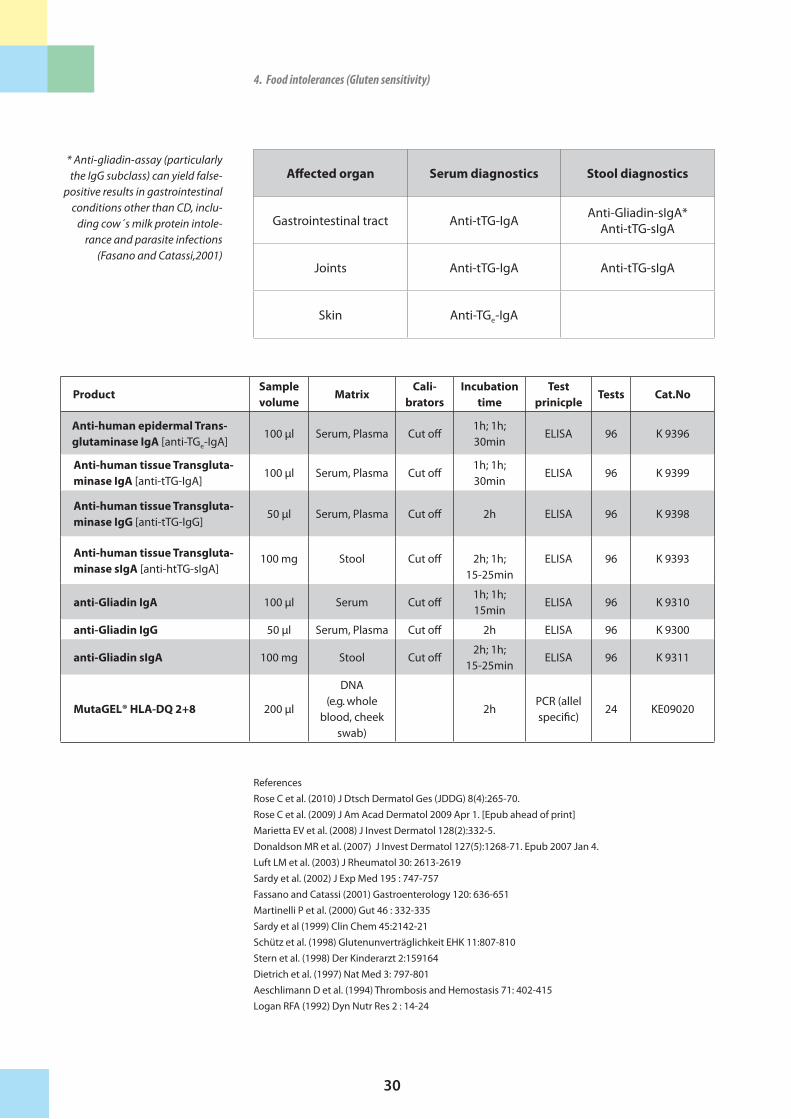
Affected�organ Serum�diagnostics Stool�diagnostics
Gastrointestinal tract Anti-tTG-IgA Anti-Gliadin-sIgA*Anti-tTG-sIgA
Joints Anti-tTG-IgA Anti-tTG-sIgA
Skin Anti-TGe-IgA
ReferencesRose C et al. (2010) J Dtsch Dermatol Ges (JDDG) 8(4):265-70.Rose C et al. (2009) J Am Acad Dermatol 2009 Apr 1. [Epub ahead of print]Marietta EV et al. (2008) J Invest Dermatol 128(2):332-5. Donaldson MR et al. (2007) J Invest Dermatol 127(5):1268-71. Epub 2007 Jan 4.Luft LM et al. (2003) J Rheumatol 30: 2613-2619Sardy et al. (2002) J Exp Med 195 : 747-757Fassano and Catassi (2001) Gastroenterology 120: 636-651Martinelli P et al. (2000) Gut 46 : 332-335Sardy et al (1999) Clin Chem 45:2142-21Schütz et al. (1998) Glutenunverträglichkeit EHK 11:807-810Stern et al. (1998) Der Kinderarzt 2:159164Dietrich et al. (1997) Nat Med 3: 797-801Aeschlimann D et al. (1994) Thrombosis and Hemostasis 71: 402-415Logan RFA (1992) Dyn Nutr Res 2 : 14-24
4.Foodintolerances(Glutensensitivity)
���ProductSample�volume
MatrixCali-�
bratorsIncubation�
timeTest��
prinicpleTests Cat.No
Anti-human�epidermal�Trans-�glutaminase�IgA [anti-TGe-IgA]
100 µl Serum, Plasma Cut off1h; 1h; 30min
ELISA 96 K 9396
Anti-human�tissue�Transgluta-minase�IgA [anti-tTG-IgA]
100 µl Serum, Plasma Cut off1h; 1h; 30min
ELISA 96 K 9399
Anti-human�tissue�Transgluta-minase�IgG [anti-tTG-IgG]
50 µl Serum, Plasma Cut off 2h ELISA 96 K 9398
Anti-human�tissue�Transgluta-minase�sIgA [anti-htTG-sIgA]
100 mg Stool Cut off 2h; 1h; 15-25min
ELISA 96 K 9393
anti-Gliadin�IgA 100 µl Serum Cut off1h; 1h; 15min
ELISA 96 K 9310
anti-Gliadin�IgG 50 µl Serum, Plasma Cut off 2h ELISA 96 K 9300
anti-Gliadin�sIgA 100 mg Stool Cut off2h; 1h;
15-25minELISA 96 K 9311
MutaGEL®�HLA-DQ�2+8 200 µl
DNA (e.g. whole
blood, cheek swab)
2hPCR (allel specific)
24 KE09020
* Anti-gliadin-assay (particularly the IgG subclass) can yield false-
positive results in gastrointestinal conditions other than CD, inclu-
ding cow´s milk protein intole-rance and parasite infections
(Fasano and Catassi,2001)
31
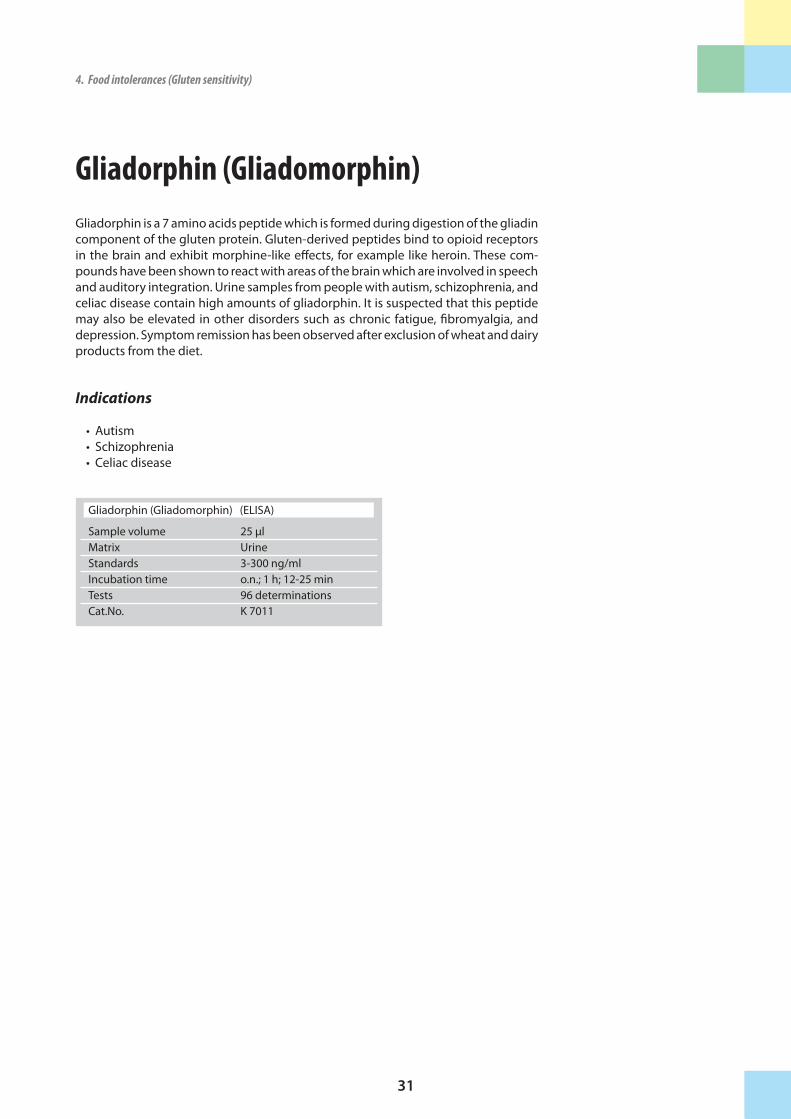
Gliadorphin (Gliadomorphin)Gliadorphin is a 7 amino acids peptide which is formed during digestion of the gliadin component of the gluten protein. Gluten-derived peptides bind to opioid receptors in the brain and exhibit morphine-like effects, for example like heroin. These com-pounds have been shown to react with areas of the brain which are involved in speech and auditory integration. Urine samples from people with autism, schizophrenia, and celiac disease contain high amounts of gliadorphin. It is suspected that this peptide may also be elevated in other disorders such as chronic fatigue, fibromyalgia, and depression. Symptom remission has been observed after exclusion of wheat and dairy products from the diet.
Indications
• Autism • Schizophrenia • Celiac disease
4.Foodintolerances(Glutensensitivity) 4.Foodintolerances(Glutensensitivity)
Gliadorphin (Gliadomorphin) (ELISA)
Sample volume 25 µlMatrix UrineStandards 3-300 ng/mlIncubation time o.n.; 1 h; 12-25 minTests 96 determinationsCat.No. K 7011

32
Lactoseintolerance
MutaGEL® LaktasePatients with lactose intolerance are not able to digest milk sugar (lactose) taken in with food. Due to this fact, these persons subsequently suffer under malabsorption problems like nausea, flatulence, diarrhoea or stomach pain.
The most important reason for lactose intolerance is founded in a genetical lack of the enzyme lactase which is responsible for the degradation of milk sugar in the organism. This common gene defect is very easy to detect by analysing the T/C base replacement at position -13910 from the regulatory region of the lactase gene. If this point mutation is homozygous, a lactase deficiency and subsequent lactose intole-rance is predetermined. The manifestation of the disease occurs with about 20 years of age and the prevalence of the homozygous mutation in Germany is more than 15 %.
The kit “MutaGEL® Laktase” allows the detection of the common T13910C polymor-phism in the lactase gene LCT.
Indications
• Nausea, cramps, bloating, gas, and diarrhea, which begin about 30 minutes to 2 hours after drinking or eating fluids, foods containing lactose
ReferencesTag CG et al. (2007) Clin Chem 53(1):146-48Buning C et al. (2003): Scand J Gastroenterol 38: 538-542.Enattah NS et al. (2002): Nat Genet 30: 233-237.
4.Foodintolerances(Lactoseintolerance)
MutaGEL® Laktase (AS)
Sample volume 200 µlMatrix DNA (e.g. from EDTA- whole blood, cheek swab)Test principle PCR (allel specific)Tests 96 DeterminationsCat. No. KE 09009
33
Fructoseintolerance
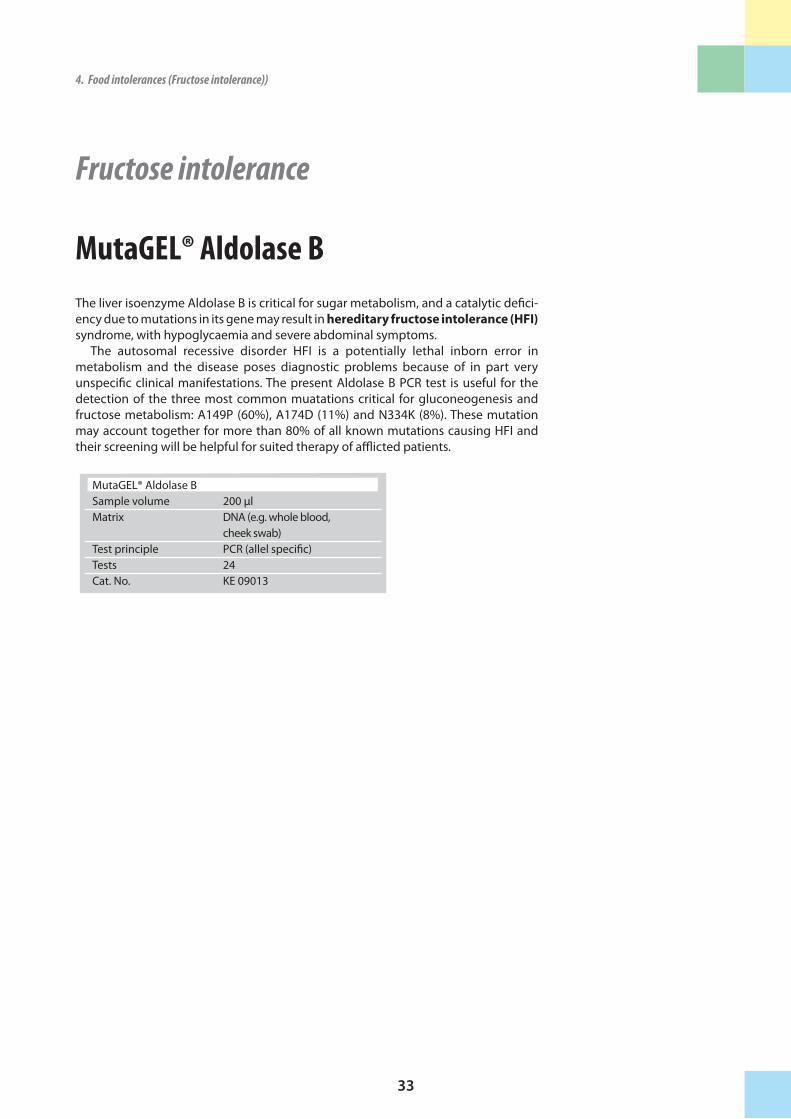
MutaGEL® Aldolase BThe liver isoenzyme Aldolase B is critical for sugar metabolism, and a catalytic defici-ency due to mutations in its gene may result in hereditary�fructose�intolerance�(HFI) syndrome, with hypoglycaemia and severe abdominal symptoms.
The autosomal recessive disorder HFI is a potentially lethal inborn error in metabolism and the disease poses diagnostic problems because of in part very unspecific clinical manifestations. The present Aldolase B PCR test is useful for the detection of the three most common muatations critical for gluconeogenesis and fructose metabolism: A149P (60%), A174D (11%) and N334K (8%). These mutation may account together for more than 80% of all known mutations causing HFI and their screening will be helpful for suited therapy of afflicted patients.
4.Foodintolerances(Lactoseintolerance) 4.Foodintolerances(Fructoseintolerance))
MutaGEL® Aldolase BSample volume 200 µlMatrix DNA (e.g. whole blood, cheek swab)Test principle PCR (allel specific)Tests 24 Cat. No. KE 09013
34
Histaminintolerance
Diamine Oxidase (DAO)
Diamine� oxidase� (DAO) is a histamine-metabolizing enzyme. Although DAO is found practically in the whole body, the most important site of its action is the inte-stine. The enzymatic activity of DAO determines the histamine degradation speed. In the case of DAO deficiency or inhibition, incorporated or endogenous histamine cannot be degraded quickly enough, and the symptoms of histamine intolerance are presented. Millions of people suffer from gastrointestinal problems, migraine, irrita-tions of nasal mucosa and other allergy-like symptoms after consumption of certain nutrients. Too much histamine in the body can be the reason for this wide range of symptoms. Another possibility for reduced DAO function could be the intake of activity-inhibiting substances, such as alcohol or medication.
Histamine induced food intolerance is not IgE-mediated. Determination of the DAO activity in serum or plasma is a suitable marker for diagnosis of histamine into-lerance and the associated symptoms.
With our easy-to-use, reliable and standardised test kit it is possible to quantify the biological activity of DAO in the circulation. Only 50 µl of serum are needed for the test, results are available within 3 hours.
Indications:
Detection of histamine intolerance Monitoring of a histamine-free diet
ReferencesInfvesson G et al. (1969) Scand J Clin Lab Invest 24: 163-168Sessa A et al. (1994) Agents and Actions 43: 69-77Wantke F et al. (1993) Clin Exp Allergy 23: 982-985Wantke F et al. (1999) Inflammation Research 48: 169-170
4.Foodintolerances(Histaminintolerance))
NH2
HistaminNH
N
Histamin
DAO 3H (REA) Sample volume 100 µlMatrix SerumCalibrators 2.1 - 80 U/mlIncubation time 2,5 hTests 96 Cat. No. K 8220
DAO (ELISA) Sample volume 25 µlMatrix Serum, PlasmaIncubation time 2 h, 1 h, 1 h, 10-20 minTests 96 Cat. No. K 8500

35
Histamin
4.Foodintolerances(Histaminintolerance)) 4.Foodintolerances(Histaminintolerance))
Histamin* (ELISA)
Sample volume 100 mgMatrix StoolCalibrators 10–2560 ng/mlIncubation time 15 min; 30 min; 10 min;
15 minTests 96Cat. No. K 6861
* For Research Use only
New for your research: Our ELISA for the quantitativedetermination of HIstamin in Stool
36
5. Infectiousdiseases
Infections of the intestinal tract with bacteria, viruses or parasites can cause life threa-tening acute diarrhea. In addition, frequent or chronic infections play a role in the pa-thogenesis of a number of intestinal diseases. For routine screening, Immundiagnostik offers a comprehensive, automatable assay portfolio (ELISA, PCR) for pathogen detec-tion.
Microscopic picture of the yeast Candida albicans
37
Helicobacter pylori Antigen
Helicobacter pylori (H. pylori) is a spiral-shaped bacterium that can be found in the human stomach and duodenum. In order to be able to survive in the extremely acid environment of the stomach, H. pylori bacteria produce urease which in turn metabo-lises urea into bicarbonate and ammonia. Particularly, the highly corrosive ammonia affects the gastric mucosa adversely and might cause severe damage. Besides a possi-ble gastritis, an H. pylori infection could eventually lead to a duodenal ulcer or a gastric tumour, resulting from the persisting immune response to the infection. Traditional diagnosis of an H. pylori infection requires invasive measures such as gas-troscopy and biopsy, which for most patients are rather burdensome. Alternatively, measuring H. pylori antibodies in serum or the 13C-urease breath test provides infor-mation on a possible H. pylori infection.
Our Helicobacter pylori Antigen ELISA offers a tool for the detection of the H. pylori antigen in faeces. The advantages of a faecal antigen test are obvious: • non-invasive sample collection • cost efficient alternative to the golden standard of gastroscopy • equivalent sensitivity and specifity to the 13C-urease breath test • for follow-up of treatment more useful than serological test since a com- parison of pro- and post-treatment is necessary
Indications
• Initial diagnosis of a H. pylori infection• Follow-up of treatment
References Gisbert JP et Pajares JM (2004) Helicobacter 4: 347-368Uemura N et al. (2001) N Engl J Med 345: 784-89
Also available at Immundiagnostik for serum und plasma samples:
• Helicobacter pylori IgA ELISA (KBE-HLAK09)
• Helicobacter pylori IgA CLIA (KBC-HLAK09)
• Helicobacter pylori IgG ELISA (KBE-HLGK08)
• Helicobacter pylori IgG CLIA (KBC-HLGK08)
5.Infectiousdiseases
Optimal patient screening: Combination of Helicobacter pylori antigen detection and determination of antibiotic resistance
Helicobacter pylori antigen (ELISA) Sample volume 100 mgMatrix StoolCalibrators Cut offIncubation time 1 h; 1 h; 1h, 15 minTests 96Cat. No. K 6920

38
5.Infectiousdiseases
MutaPLATE® NorovirusSample volume 200 µlMatrix RNA (Stool)Test principle real time RT-PCR (for open system)
Tests 96 Cat. No. KG1934196
MutaREAL® NorovirusSample volume 200 µlMatrix RNA (Stool)Test principle real time RT-PCRTests 96 Cat. No. KG2934196
New:
MutaREX® NorovirusSample volume 200 µlMatrix RNA (Stool)Test principle real time RT-PCR (+ extraction control)
Tests 96 Cat. No. KG290196
New:
Norovirus
Gastrointestinal infections can cause life threatening diseases ultimately leading to death. It was recently shown, that the genetic heterogeneous group of Noroviruses (formally known as Norwalk-like viruses) are the major cause of non-bacterial gas-troenteritis worldwide. Human Noroviruses are small, non-enveloped viruses with a ssRNA (single stranded) genome.
Noroviruses belong to the family of Caliciviridae and are divided into genotype I and II. These viruses are resistant against higher temperatures (60°C), acid (pH 3) and chlorit (10mg/L). The viruses are transmitted via contaminated food and water but also from person-to-person and are highly contagious.
LiteratureLopman BA et al. (2003) Viral gastroenteritis outbreaks in Europe, 1995-2000. Emerg Infect Dis Jan 9(1):90-6Marshall JA et al. (2006) Laboratory Diagnosis of Norovirus. Clin Lab 52:571-81
MutaPLEX® NorovirusSample volume 200 µlMatrix RNA (Stool)Test principle real time RT-PCR (for open system)
(+ extraction control)
Tests 32 Cat. No. KG190132
39
EnterovirusHuman Enteroviruses are small RNA viruses which belong to the family of picornaviri-dae. The ubiquitous pathogen is responsible for about 500 million infections per year worldwide. The 64 serotypes are divided in the following groups:
* Polioviruses Typ 1-3 * Coxsackieviruses with subgroups A and B * Echoviruses * Enteroviruses 68-71
In moderate climates there is a seasonal accumulation of enterovirus infections in late summer and fall. Transmission of enteroviruses occur via the faecal-oral route. Airborne infections are also common. The viruses are transmitted between humans through stool or through saliva-contaminated objects and are excreted during the acute disease phase. In addition, virus particles can be detected up to several weeks after the symptoms have subsided. The median incubation time for most enterovirus infections is 3-5 days.
Diseases caused by enteroviruses are very complex and can be life threatening, es-pecially for children. Among them are febrile illness, conjunctivitis, herpangina, hand foot and mouth disease, gastroenteritis, generalized skin rashes, meningitis, pneu-monia, myocarditis, pericarditis, hepatitis, encephalitis, paralyses, fetal damage up to severe neonatal diseases with pneumonia, myocarditis and meningoencephalitis.
Enteroviruses are excreted mainly in stool and, depending on the virus type, through the pharyngeal route. In acute disease, the diagnosis should prefererrably be based on PCR pathogen detection.
Our PCR kits are screening tests for the qualitative determination of human enterovi-rus RNA (Polio-, Coxsackie A-, Coxsackie B- and echoviruses) in clinical samples (stool, whole blood, plasma, respirational tract samples, cerebrospinal fluid).
5.Infectiousdiseases 5.Infectiousdiseases
MutaREAL® EnterovirusSample volume 200 µlMatrix RNA (biol. liquids)Test principle real time RT-PCRTests 96 Cat. No. KG2900296
MutaPLEX® EnterovirusSample volume 200 µlMatrix RNA (biol. liquids)Test principle real time RT-PCR
for open systems + extraction control
Tests 96 Cat. No. KG190296
New:
MutaREX® EnterovirusSample volume 200 µlMatrix RNA (biol. liquids)Test principle real time RT-PCR + extraction
controlTests 96 Cat. No. KG290296
New:
MutaPLATE® EnterovirusSample volume 200 µlMatrix RNA (biol. liquids)Test principle real time RT-PCR
for open systemsTests 96 Cat. No. KG1900296
Highest quality standard of our PCR kits: 2010 evaluated by the international panel "Quality Control for Molecular Dia-gnostics" with best result (100%)
The CE-marked kits are optimized for enterovirus detection in stool

40
Salmonella sp. Salmonella are the main cause for food intoxications: In more than 65% of all cases, egg products, meat and poultry are the common foods which transmit salmonella. Therefore, the European regulations specify that none of the roughly 2000 known salmonella subtypes must be detected in a 25 g food sample. Until now, the necessary analysis has been performed with bacteriological cultures which take up to 5 days.
The PCR offers a far more sensitive and time saving alternative (one day) to the conventional microbiological analysis of Salmonella sp. in various food samples. In addition, the PCR allows the pathogen detection in stool samples and is thereofore ideal for a clinical setting.
5.Infectiousdiseases
MutaREAL® SalmonellaSample volume 200 µlMatrix DNA (Food, Stool)Test principle real time RT-PCRTests 96 Cat. No. KV2900196

41
D-Arabinitol The yeast Candida albicans is present in most human mucous membranes of the mouth and pharynx, the genital area and the intestinal tract. If the immune system is weakened or the physiological bacterial intestinal flora disrupted, the yeast mul-tiplies and leads to a generalized candidiasis. Typical symptoms of a candidiasis include general weakness, recurring vaginal infections, fungal skin infections, fatigue, memory impairments, irritability, headaches, poor concentration, joint aches and flatulence.
A systemic candidiasis is often diagnosed late. As a consequence of the multipli-cation of the yeast in the circulation, multiple organs can be affected. Complications include endocarditis, endophthalmitis or osteomyelitis.During a systemic candidiasis, pathogen detection occurs in blood, liquor, joint fluid and endotracheal samples and bronchial lavages.
An additional possibility to diagnose invasive yeast infections is the determination of D-Arabinitol in serum or urine. D-Arabinitol is a characteristic yeast metabolite. While Candida ssp. produce exclusively D-Arabinitol, the human metabolism gene-rates L-Arabinitol. D-Arabinitol serum levels rise during an invasive candidiasis, when the yeast multiplies in the organism.
Apart from the gas chromatographic determination easy-to-use tests have been missing so far. Our Arabinitol test is a straight-forward colorimetric enzyme assay for the manual and automatic analysis of D-Arabinitol in serum or urine.
Indications
• Detection of a Candida infection
• Determination of the severity of a Candida infection
• Therapy monitoring
• Choice of the appropriate medication
5.Infectiousdiseases 5.Infectiousdiseases
D-Arabinitol Sample volume 10 µlMatrix Serum, UrineTest principle colorimetricCalibrators 20-100 µmol/lTests 125 Cat. No. KMD-ARAB
Colorimetric test:• Simple handling• Automatable
42
More tests for the detection of viral and bacterial infections
(determination in stool) on request:
Serazym�Adenovirus HW/E-017 96 determinationsKit for automate HW/E-017-A2 2 x 96 determinations
Serazym�Astrovirus HW/E-045 96 determinationsKit for automate HW/E-045-A2 2 x 96 determinations
Serazym�Rotavirus HW/E-020 96 determinationsKit for automate HW/E-020-A2 2 x 96 determinations
Serazym�Giardia�lamblia�Kit for automate HW/E-038 96 determinations
Serazym�Entamoeba�histolyticaKit for automate HW/E-018 96 determinations
Serazym�Clostridium�difficile��Toxin�A/B� HW/E-040 96 determinationsKit for automate HW/E-040-A2 2 x 96 determinations
Serazym�Verotoxin�1+2 HW/E-030 96 determinations Kit for automate HW/E-030-A2 2 x 96 determinations
Serazym�Campylobacter HW/E-093 96 determinations.Kit for automate HW/E-093-A2 2 x 96 determinations
5.Infectiousdiseases
43
5.Infectiousdiseases
Appendix: Stool sample preparation systems
We can spare you the cumbersome and unpleasant stool weighing procedure: Our special, cost-eff ective sample tube enables the preparation of a defi ned sample solu-tion with minimal stool contact. For sample collection, the dip stick with screw cap is used to collect the sample (15 mg), excessive stool is stripped off at the cone-shaped insert (s. Fig.). The stool sample is now ready for storage or dilution with buff er. The resulting sample suspension can be used with our ELISAs for the determination of a respective parameter in stool.
The sample tubes can be ordered empty or fi lled with buff er for the preparation of a defi ned stool sample suspension.
Fig.: Practical preparation of stool samples
• time saving• hygienic• minimal stool contact• suited for direct use on automates
Stool sample preparation systems
unfi lled Cat. No. K 6998SAS
with buff er (dilution 1:50) Cat. No. K ....SASP1
with buff er (dilution 1:100) Cat. No. K ...SASP2] .... = Cat. Nr. of the respective ELISA test for the determination of a parameter in stool.
Stool sample tube
Stool sample
Dipstick

Immundiagnostik AGStubenwald-Allee 8a D-64625 BensheimTel.: +49 (0) 62 51/70 19 00 Fax: +49 (0) 62 51/84 94 [email protected] www.immundiagnostik.com
q Product List
q Catalogue "Immunochemicals, Antibodies, Antigens"
q Manuals of these products:
Brochures:
q Skeletal�System�
q Oxidative�Stress�
q Cardiovascular�and�Renal�Systems
q Orthomolecular�Medicine
q Molecular�Biology
q HPLC-Applications�/�LC-MS/MS-Applications
Phone:�
� Fax:
� Date:
� E-Mail:
FAX-Reply� +�49�(0)�62�51�-�84�94�30
Name/Address:� �
� � �
� � � �� � �� �� �
� � � �
Please�send�me�the�following�informative�material:
Gas
troi
ntes
tinal
Dis
ease
s / A
pril
201
1