Embed Size (px)
Citation preview

Gastro-esophageal Reflux Surgical Management
Fahad Y. Bamehriz, MBBS, SBIS

Introduction
• GERD is a chronic disease of upper GI tract as a
cause of complex mechanisms defects, resulting in back flow of gastric contents to the
esophagus, that presents with GI and extra-GI manifestation.
• affecting up to 40% of people in the Western world.

Mechanisms for GERD
• By Orlando R,1- TLESR2- Hypotensive or incompetent LES3- Anatomic disruption of EGJ. Refluxate material: - Acid - Bile- Gas

Aim of treatment
– Control acute GERD symptoms
– Maintain the control
– Prevent long-term complications

Mechanism of action of fundoplication

Surgical options

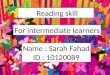
Nissen’s fundoplication

X-ray picture

Partial Toupet (posterior)fundoplication

Partial Anterior (Dor) fundoplication

Nissen Fundoplication

Step 1

Step 2

Step 3

Step 4

Step 5

Step 6

Step 7

Step 8

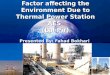
Picture of a partial ‘Toupet’ fundoplication

Partial Anterior (Dor) fundoplication

Peri-operative information
OR time is 1houre
Less pain medication
Hospital stay is 1 day
Back to regular activity within 5-7 days

Cosmetic appearance
open Laparoscopic

Complications • Complications, during or the after the operation in 5-
15% of cases • Serious problems is around 2-8% of patients, with
around 2% requiring a new operation• Difficulties swallowing persist for longer than 3 months in
only 10%. After 1 year, it’s around 2% • Diffuse abdominal complaints• Thee is about a 10% risk of reflux disease reoccurring • Despite all the risks to be taken into consideration, the
fact remains that in around 90% of reflux cases a long-lasting cure of reflux disease can be achieved.

Clinical data 1
• Dallemagne B et al (Surg Endosc. 2005 Dec 5):100 consecutive patients who underwent LAS by a single surgeon in
1993 Evaluations of the outcome were made 5 and 10 years after surgery
At 5 years, 93% of the patients were free of significant reflux
symptoms. At 10 years, 89.5% of the patients still were free of significant reflux
(93.3% after Nissen, 81.8% after Toupet). The GIQLI scores at 10 years were significantly better than the
preoperative scores of the patients under medical therapy with proton pump inhibitors.
Four patients underwent revision surgery: one patient for persistent dysphagia and three patients for recurrent reflux symptoms

Clinical dataPt F/U Dysp REC satisf
Pessaux 2005 1340 >5y 5.1% 10% 93%
Dan S 2005 141 5 y 12% 12% 91%
PointnerR
2005 89 5y 5% 2% 95%
Tucker L 2005 93 4y 2% 21% 94%
Anvari/bamehriz
2004 1023 5y 5 % 12% 89%
Dallemagne B
2005 100 10y 1 pt 3pt 96%

Clinical data 2
• Beher and colleagues (NEJM-1975),
surgery is superior to antacid therapy
. Spechler and coworkers (NEJM-1992),
surgery is superior to H² blockers
. Lundell (J Am Coll Surg-1999),
surgery is superior to PPI therapy

Clinical data 2
• Mahon D (Br J Surg-2005),
surgery is superior to PPI therapy
. Olberg P (Scand J Gast-2005),
surgery is more effective than medical care
. Cookson R( Br J Surg-2005),
surgery maybe cost saving after 8 years compared to PPI maintenance therapy

GERD& Barrett’s esophagus
• Surgical therapy:– Controls symptoms of GERD– Controls acid & bile reflux– May prevent or slow progression– May cause regression

Clinical data• Pope et al (N Eng J Med-1980), complete regression of IM in 4/10 patients. Low et al (Am J Gastr-1999),Complete regression in 2/14 pt partial regression in 10/14 ptDisappearance of dysplasia in 4/14 ptDe Meester (Ann Surg-1998),Complete regression and loss of IM in 4.4%

Clinical data
• Ortiz and colleagues (Br J Surg-1996),Randomized 27 pt (M) + 32 pt (S)Follow-up 5 yearsRegression of IM: 2/27 pt of medical arm 8/32 pt of surgical arm. Mc Callum et al (Gast-1991). Katz et al (Am J Gas-1998)

GERD & Pregnancy
• Two thirds of pregnant pt develop HB
• ? Progesterone, ? High intra A pressure
• Al-Amri SM (Eur J Obstet Gynecol Reprod Biol. 2002 ),
Pregnancy is associated with decreased LES pressure, more frequent episodes of reflux and upright reflux.

Clinical data
• Bamehriz (Surg End-2005), of 146 child-bearing age women, 25 pt became
pregnant after LNF 5of 25 patients (20 %) developed dyspepsia
during their pregnancy 1 patient (4%) developed acute intra-thoracic
herniation of the stomachHowever, for majority laparoscpic Nissen
fundoplication provides effective control of their reflux symptom during and after pregnacy

GERD &TLESR
• TLESR cause 70-100% of reflux episodes in normal person. 63-74% in GERD pt.
• PPI has no effect on TLESR
• Bamehriz et al (Surg Endo-2004),
73 pt with GERD +TLESR
TLESR is significantly reduced to a mean number of 0.19 per pt from 2.4 per pt
Only 8/73 pt had TLESR post LNF

LNF & NERD
• Kamolz,Pointner et al (Surg End-2005),
- 89/500 pt had NERD who underwent LNF
- Compared with EGD-positive GERD pt
- Follow-up was 5 years
- GIQLI was significantly better in NERD pt

GERD & Cough
• Anvari et al (Surg Endo-2005),
- 209 pt had GERD+ cough, underwent LNF
- 60% has 5 years follow-up
- Cough improved in 71% of pt at 5 years
- LNF is successful in the long-term control of GERD-related Cough.

Redo fundoplication
Pt number
FOLLOWUP
CONVERSION
MORTALITY
Pointner R
225 3 Y 10% 0.4%
Richardson WS
10 2Y 20% 0
Bamehriz F
28 2 Y 7% 0

Factors contributing to success of LNF

factors
• 1- typical GERD symptoms
• 2- well-respond to PPI therapy
• 3- abnormal 24 pH study
• All 3 factors = 95-98% success of LNF
• Only 2 factors= 70-80%
• Only 1 factor = < 50%

Summary
• PPI is still the first line of GERD therapy • Laparoscopic Nissen fundoplication remains an Laparoscopic Nissen fundoplication remains an
effective anti-reflux measure at 10 years effective anti-reflux measure at 10 years • Resumption of anti-secretory Rx not a measure Resumption of anti-secretory Rx not a measure
of surgical failure of surgical failure • Recurrence can be treated effectively with Recurrence can be treated effectively with
laparoscopic revision laparoscopic revision • Severe GERD symptoms and response to PPI Severe GERD symptoms and response to PPI
are good indicators of symptom outcomeare good indicators of symptom outcome

Final word
• Let the GERD patient decide about the treatment option
• What about YOUNG
PREGNANCY
POOR PATIENTS
BILE REFLUX
……………….ECT