Embed Size (px)
Citation preview


Gastric Cancer
Elshami Elamin, MDMedical Oncologist
Central Care Cancer Center
www.cccancer.com
Wichita, KS - USA
•04/20/23 •2

INTRODUCTION
Gastric cancer is defined as any malignant tumor arising from the region extending between the gastroesophageal (GE) junction and the pylorus.
The incidence and mortality of gastric cancer have been declining in most developed countries.
The age-adjusted risk fell 5% from 1985-1990.
•04/20/23 •3

Risk Factors Low vegetable, fruit Nitrates Coal mining, nickel, rubber Intestinal metaplasia Blood group A ?Gastrectomy Pernicious anemia
•04/20/23 •4

Pathology Adenoca: 95%
Intestinal Diffuse Mixed
Lymphoma Squmous Leimyosarcoma Carcinoid
•04/20/23 •5

Clinical Classification
Superficial Focal, fungating, polypoid Infiltrative, linitis plastica
•04/20/23 •6

Physical exam Hepatomegaly Ascites Virchow’s node (Lt. SCV)
Irish node (Lt. Ant. Axilla.)
Sister Mary Joseph nodule/sign (palpable nodule bulging into the umblicus)
Krukenberg’s tumor Blumer’s shelf
•04/20/23 •7

Staging
IA : T1 (invade lamina propria/submucosa) IB: T1, N1 (1-6 +ve)
T2 (invade muscularis/subserosa II: T1, N2 (7-15 +ve)
T2, N1 T3 (penetrate visceral peritoneum only)
IIIA: T2, N2 T3, N1 T4 (invade structures)
IIIB: T3, N2 IV: T1-3, N3 (>15 +ve)
T4, N1-3 OR M1
•04/20/23 •8

Prognostic factors
Aneuploidy: poor prognosis in patients with adenocarcinoma of the distal
stomach. High plasma levels of vascular endo-thelial growth factor (VEGF) presence of CEA in peritoneal washings
predict poor survival in surgically resected patients. intratumoral levels of dihydropyrimidine dehydrogenase (DPD)
low levels appear to predict better response to 5-FU based chemotherapy and longer survival.
The prognostic implications of tumor-suppressor genes and oncogenes are an area of active investigation.
Patients with cancers of the diffuse type worse than those with intestinal-type lesions.
•04/20/23 •9

•04/20/23 •10

•H&PH&P
•CBC/CMPCBC/CMP
•C-x-rayC-x-ray
•CTCT
•EGDEGD
•H. pyloriH. pylori
•BariumBarium
•EUSEUS
•PET/CT PET/CT
Locoregional
Locoregional
I - III
I - III
IVIV
•04/20/23 •11
Multi-
Disciplinary
eval

Locore
gio
nal I-
III
Locore
gio
nal I-
III
Operable
/Med fi
t
Operable
/Med fi
t
Inop
erable
Inop
erable
Unresectab
le/Med
unfit
Unresectab
le/Med
unfit
•04/20/23 •12

TREATMENT
Resection provides the only chance for cure. Radiotherapy and chemotherapy
potential roles as adjuncts to surgery patients with unresectable tumors.
Preoperative chemo and chemoradiation therapy are active areas of current investigation.
•04/20/23 •13

Confirmation of resectability
CT scan +/- EUS Laparoscopy
assess the extent of disease and resectability. adds to the accuracy of preoperative imaging
peritoneal spread or small liver metastases. peritoneal washings
Laparoscopic ultrasonography identify lesions with a high risk of recurrence
(T2b or >, N+), for which a preoperative chemotherapy protocol
may be available.
•04/20/23 •14

Extent of resection
Depends on: The site and extent of the primary cancer.
Subtotal gastrectomy is preferred over total gastrectomy comparable survival benefit but lower morbidity. A 5-cm proximal and distal resections margins.
If total gastrectomy is necessary: transection of the distal esophagus and proximal duodenum omentectomy
In Japan, there is a growing experience with more limited resections of early-stage gastric cancer.
Endoscopic Mucosal Resection (EMR) of non-ulcerated T1 N0 lesions
pylorus-preserving gastrectomy. Laparoscopic resections are also being performed more
frequently.
•04/20/23 •15

Extent of surgery
Routine or prophylactic splenectomy is not required
Splenectomy is acceptable if: Spleen or hilum is involved
•04/20/23 •16

Extent of lymphadenectomy
Regional lymphatics: Perigastric (paracardial, paragastric, parapyloric) (D1)
Retroperitoneal “second echelon” and LN along the named vessels:
celiac trunk, left gastric artery, hepatic artery, splenic artery, and splenic hilus (D2)
The goal is > 15 LN
•04/20/23 •17

Improved long-term survival rates for Japanese patients had been attributed to the extended lymphadenectomies routinely performed in this country (D2 or more).
Retrospective data had shown that D2 lymphadenectomy is safe and does not increase morbidity.
Two European randomized trials showed no sig differences in OS between D1 and D2
higher postop morbidity and mortality in the D2 due to a higher rate of splenectomy and/or partial pancreatectomy. When a subset of patients with N2 disease were studied in
long-term follow-up in the Dutch randomized trial, a survival advantage was shown with D2 dissection.
Extended lymphadenectomy should primarily be performed in specialized centers by experienced surgeons:
splenectomy and pancreatectomy should be avoided
•04/20/23 •18

Reconstruction
Billroth I BillrothII Roux-en-Y esophagojejunostomy
•04/20/23 •19

Surgical Surgical
outcomesoutcomes
RoRo
R1R1
R2R2
M1M1
ObserveObserve
T2T2
palliativepalliative
•04/20/23 •20
T3-4 or N+T3-4 or N+
Tis-T1Tis-T1
RT + chemoRT + 5FU/LV or RT + chemoRT + 5FU/LV or
ECF if given preopECF if given preop
Observe or chemoRT (high risk) or Observe or chemoRT (high risk) or ECF if given preopECF if given preop
RT + chemoRT + 5FU/LV RT + chemoRT + 5FU/LV
RT + chemoRT + 5FU/LV or RT + chemoRT + 5FU/LV or
Chemo or BSCChemo or BSC

•04/20/23 •21

•04/20/23 •22
Any role for Chemo/RT
<30% of locally advanced Gastric/GEJ adeno could be cure with surgery alone
Previous adj chemo failed to show clinical benefit

ADJUVANT THERAPY
The 5Y survival rate after “curative resection” 30-40%
A North American Intergroup trial randomizing resected patients (stages IB–IV[M0]) to receive chemoRT or observation:
sig improvement in median DFS (median 19 vs 30 m) and OS (26 vs 35 m)
Adj chemoRT (usually C.I. 5-FU) is the standard of care in the United State
•04/20/23 •23

•04/20/23 •24
INT-0116 (SWOG 9008)
Randomized lll Trial: Resectable adeno of stomach GEJ (lB-IVA)
5-FU/LVx5d--> RT+5-FU/LV during first 4d and last 3d of RT --> 2cycles of 5-FU/LVx5d
postop CT/RT improve DFS&OS in R0 (resected locally advanced) [standard of care]
•Adj Option
•Macdonald et al; N Engl J Med. 2001 Sep 6;345(10):725-30.

? Is D2 LND required ? D2 LND was performed in only 10% of the
patients in this trial.
Subgroup analysis revealed that outcome did not differ based upon the type of lymphadenectomy (P = .80).
Still, since only a small percentage of pts underwent the recommended D2 dissection, further research is necessary before firm conclusions can be made in this area.
•04/20/23 •25

Radiotherapy
Radiotherapy can decrease the rate of locoregional failure but has not been shown to improve survival as a single postop modality
Postop RT may be appropriate in patients who are not candidates for chemo
•04/20/23 •26

Chemotherapy
Randomized trials of surgery +/- chemo: No definite survival advantage, with the possible
exception of pts with widespread nodal involvement. One meta-analysis included both Western and Asian
studies: showed a sig survival benefit with the use of chemo in the Asian
trials, but there was no benefit in the Western studies, possibly due to differences in biology or drug metabolism.
No specific regimen could be recommended
•04/20/23 •27

•04/20/23 •28

Clinical > T2 or N +
•04/20/23 •29

European Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) by Cunningham and associates.
The 5Y survival rate for ECF + surgery was 36%, vs 23% for surgery
Chemo also enhanced resectability
•04/20/23 •30

•04/20/23 •31
The MAGIC TrialThe Medical Research Council Adjuvant Gastric Infusional
Chemotherapy
Operable adeno of the stomach, the lower third of the esophagus, and the GEJ ( 74% of pts had tumors in the stomach)
ECFx3->surg->ECFx3 (250 pts) vs Surgery alone (253 pts): 5Y survival: 36% vs 23% Chemo sig. improves resectability,PFS and OS
•Periop. option
•D. Cunningham, et al ; N Engl J Med. 2006 Jul 6;355(1):11-20.

Other options of ChemoRT
Docetaxel or Taxol + 5-FU/Xeloda
Cisplatin + 5-FU/Xeloda
•04/20/23 •32

•04/20/23 •33
Preoperative Chemotherapy vs Surgery Alone
FNLCC ACCORD 07-FFCD 9703, multicenter, randomized trial indicated benefit of preoperative chemotherapy vs surgery alone for resectable adenocarcinoma of stomach and lower esophagus[1]
Higher rate of R0 resection (87% vs 74%; P = .04) Higher 5-yr OS (38% vs 24%; P = .021) No increase in postoperative morbidity or mortality
Boige V, et al. ASCO 2007; Abstract 4510.

•04/20/23 •34

•ECF (n = 249) •ECX (n = 241)
•EOF (n = 235) •EOX (n = 239)
•Epirubicin 50 mg/m2 IV 3 weekly•Cisplatin 60 mg/m2 IV 3 weekly
•5-FU 200 mg/m2/day IV givencontinuously
•Epirubicin 50 mg/m2 IV 3 weekly
•Cisplatin 60 mg/m2 IV 3 weekly
•Capecitabine 625 mg/m2 BID PO
continuously
•Epirubicin 50 mg/m2 IV 3 weekly•Oxaliplatin 130 mg/m2 IV 3 weekly•5-FU 200 mg/m2/day IV given
continuously
•Epirubicin 50 mg/m2 IV 3 weekly
•Oxaliplatin 130 mg/m2 IV 3 weekly
•Capecitabine 625 mg/m2 BID PO
continuously
REAL-2: Phase III Capecitabine vs 5-FU and Oxaliplatin vs
Cisplatin
•Cunningham D, et al. N Engl J Med. 2008;358:36-46.

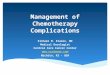
TAX325: Phase III Docetaxel/Cisplatin/5-FU (DCF) vs
Cisplatin/5-FU (CF) Primary endpoint: TTP from 4 → 6 mos Secondary endpoints: OS, RR, safety, QoL, clinical benefit
•Patients with advanced gastric
cancer and no previous palliative
chemotherapy•
(N = 457)
•DCF•Docetaxel 75 mg/m2 IV over 1 hr on Day 1
+•Cisplatin 75 mg/m2 IV over 1-3 hrs on Day
1 +•5-FU 750 mg/m2/day by CIV over 5 days
•q3w•(n = 227)
•CF•Cisplatin 100 mg/m2 IV over 1-3 hrs on Day
1 +•5-FU 1000 mg/m2/day by CIV over 5 days
•q4w•(n = 230)
•R
•Van Cutsem E, et al. J Clin Oncol. 2006;24:4991-4997.

•04/20/23 •37

•Trastuzumab + chemo associated with increased OS: • 11.1 months vs. 13.8 months (HR=0.74; 95% CI, 0.60-0.91)
•Trastuzumab + chemo associated with an improved overall response rate:
• 47.3% vs. 34.5% (P=.0017)
•The treatment was generally well tolerated with no unexpected adverse effects in the trastuzumab group
ToGa results
•04/20/23 •38

THANKS
•04/20/23 •39