Embed Size (px)
Citation preview

HEAD and NECK HEAD and NECK CANCERSCANCERS
Elshami Elamin, MDElshami Elamin, MD

MULTIDISCIPLINARY TEAM
Head and neck surgery Radiation oncology Medical oncology Plastic and
reconstructive surgery Specialized nursing care Dentistry/prosthodontics Physical medicine and
rehabilitation Speech and swallowing
therapy
Clinical Social work Nutrition support Pathology Diagnostic radiology Adjunctive services
Neurosurgery Ophthalmology Psychiatry Addiction Services

SUPPORT AND SERVICES Pain and symptom management Nutritional support:
Enteral feeding Dental care for RT effects
Oral supplements Xerostomia management Smoking cessation Tracheotomy care Social work and Case management Supportive Care

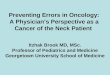
Lymphatic drainage of the head and neckand associated sites of primary tumors
Lymphatic drainage
Level I Submental: Lower lip, chin, anterior oral cavity (including
anterior one-third of the tongue and floor of the mouth) Submandibular: Upper and lower lips, oral tongue, floor of the
mouth, facial skin Level II
Oral cavity and pharynx (including soft palate, base of the tongue, and piriform sinus)
Level III Larynx, hypopharynx, and thyroid
Level IV Larynx, hypopharynx, thyroid, cervical esophagus, and trachea
Level V Nasopharynx, thyroid, paranasal sinuses, and posterior scalp Supraclavicular: Infraclavicular sites (including lungs,
esophagus, breasts, pancreas, GI tract, GU and gynecologic sources)

Ethmoid Sinus Tumors
Squamous cell carcinoma Undifferentiated carcinoma Adenocarcinoma Salivary gland tumor Esthesioneuroblastomas Sarcoma (nonrhabdomyosarcoma)

Ethmoid Sinus TumorsTreatment
T1, T2:• Complete surgical resection (preferred) or
Adj RT or Chemo/RT if adverse characteristics (positive margins and perineural invasion)
• Definitive RT T3, T4 resectable:
• Complete surgical resection Postoperative RT
Unresectable:• Chemo/RT or • RT or• Clinical trial (preferred)

Ethmoid Sinus TumorsTreatment
Incomplete excision (eg, polypectomy, endoscopic procedure)
Gross residual disease:• Surgery (preferred), if feasible
Adj RT
• RT or• Chemo/RT
No disease on physical exam, imaging, and/or endoscopy:
• RT or• Surgery, if feasible
Adj RT

Maxillary Sinus Tumors
Squamous cell carcinoma Undifferentiated carcinoma Adenocarcinoma Salivary gland tumor Esthesioneuroblastoma Sarcoma (nonrhabdomyosarcoma)

Maxillary Sinus TumorsTreatment
T1, N0 (all histologies): Complete surgical resection: Margin –ve:
• Observe Perineural invasion:
• Consider RT or• chemo/RT
Margin +ve:• reresection
Margin –ve RT Margin +ve chemo/RT
T2, N0 (SCC, Undifferentiated): Complete surgical resection:
• Margin -ve Consider RT• Perineural invasion Consider RT or chemo/RT• Margin +ve reresection
Margin –ve RT Margin +ve chemo/RT
T2, N0 (Adenoidcystic, other histologies) Complete surgical resection RT

Maxillary Sinus Tumors T3, N0, Operable T4 (all histologies):
Complete surgical resection:• Adverse characteristics:
Chemo/RT to primary and neck• No adverse characteristics:
RT to primary and neck (SCC and undifferentiated) T4, inoperable (all histologies):
Clinical trial or Definitive RT or Chemo/RT
Any T, N+, resectable: Surgical excision + neck dissection:
• Adverse characteristics: Chemo/RT to primary and neck
• No adverse characteristics: RT to primary and neck

Maxillary Sinus TumorsPRINCIPLES OF RT
Definitive RT: Primary and gross adenopathy:
• > 66 Gy Neck:
• Low-risk nodal stations: > 50 Gy
Postoperative RT: Primary:
• > 60 Gy Neck
• High-risk nodal stations: > 60 Gy
• Low-risk nodal stations: > 50 Gy

Salivary Gland Tumors (Parotid, Submaxillary, Minor salivary)
Characteristics of benign tumor: Mobile superficial lobe Slow growth Painless VII intact No neck nodes.

Salivary Gland Tumors (Parotid, Submaxillary, Minor salivary)
Untreated resectable: clinically benign (< 4 cm: T1, T2):
• Complete surgical excision: Benign or low G Observe Adenoid cystic RT to tumor bed and skull base Intermediate or high G RT to tumor bed and ips neck
Untreated resectable, clinically Suspicious (> 4 cm or deep lobe):
CT/MRI base of skull to clavicle FNA (salivary tumor):
• Surgical resection: Benign Observe Cancer see treatment

PAROTID GLAND
Superficial lobe: Node –ve:
• Parotidectomy Node +ve:
• Parotidectomy + neck dissection
Deep lobe: Node –ve:
• Total parotidectomy Node +ve:
• Total parotidectomy + neck dissection

PAROTID GLAND Completely excised:
No adverse characteristics• Observe
Adverse characteristics (Intermediate or high G, adenoid cystic, Close or +ve margins, neural/perineural invasion, Lymphatic/ vascular invasion, LN mets)
• Adj RT or Consider Chemo/RT
Incompletely excised, gross residual disease (No further surgical resection possible): Definitive RT or Chemo/RT

Other salivary gland tumors
Complete excision +/- LN dissection: No adverse characteristics:
• Observe Adverse characteristics (Intermediate or high G,
adenoid cystic, Close or +ve margins, neural/perineural invasion, Lymphatic/ vascular invasion, LN mets)
• Adj RT or Consider Chemo/RT

Salivary Gland Tumors (Parotid, Submaxillary, Minor salivary)
Previously treated incompletely resected: Negative P/E and imaging:
• Adj RT Gross residual disease:
• Surgical resection, if possible: Adj RT
• No surgical resection possible: Definitive RT or Chemo/RT
Not resectable: FNA or open biopsy
• Definitive RT or Chemo/RT

F/U
Physical exam:• Year 1 q 1–3 m• Year 2, q 2–4 m• Years 3–5 q 4–6 m• > 5 years q 6–12 m
Chest imaging as clinically indicated TSH every 6-12 m if neck irradiated CT scan/MRI- baseline

Salivary Gland TumorsRecurrence
Locoregional or distant, Resectable: Surgery + selected metastasectomy RT
Locoregional, Not resectable: RT or Chemo/RT or Chemotherapy or Best supportive care

Salivary Gland Tumors PRINCIPLES OF RADIATION THERAPY
Definitive RT: Unresectable or gross residual disease:
• Photon/electron therapy or neutron therapy Primary and gross adenopathy:
• > 70 Gy or• 19.2 nGy
Low-risk nodal stations: • 45-54 Gy or• 13.2 nGy
Postoperative RT: Photon/electron therapy or neutron therapy
• Primary: > 60 Gy or 18 nGy
• Neck: 45-54 Gy or 13.2 nGy

Cancer of the Lip
T1–2, N0: Surgery or RT
Resectable T3, T4, N0 and any T, N1-3: Surgery Adj RT +/- Chemo if high risk or RT or Chemo/RT if not surgical candidate
Unresectable: RT or Chemo/RT or best supportive care

Cancer of the Oral Cavity(Buccal mucosa, floor of mouth, anterior tongue,
alveolar ridge, retromolar trigone, hard palate)
H&P Biopsy Chest x-ray or Chest CT As indicated for evaluation:
Panorex CT/MRI Examination under anesthesia
Preanesthesia studies Dental evaluation Multidisciplinary consultation as indicated

Cancer of the Oral Cavity
T1–2, N0:- RT salvage surgery for residual dz OR excision of primary ± unilateral or bilateral
selective neck dissection adj RT +/-chemo (high risk pts);
High Risk:- Extracapsular nodal dz, +ve margins, multiple +ve LN or perineural/lymphatic/vascular invasion.
Resectable T3, N0: Excision of primary and reconstruction +
unilateral or bilateral selective neck dissection; Adj RT (optional) High Risk: Adj RT +/- chemo

Cancer of the Oral Cavity (Resectable T1-3, N1-3)
N1, N2a-b, N3:N1, N2a-b, N3: Excision of primary, ipsi comprehensive neck Excision of primary, ipsi comprehensive neck
dissection ± contra selective neck dissectiondissection ± contra selective neck dissection N2c (bilateral):N2c (bilateral):
Excision of primary and bilateral Excision of primary and bilateral comprehensive neck dissectioncomprehensive neck dissection
Adj Therapy:Adj Therapy: RT (optional)RT (optional) High Risk; RT +/- chemoHigh Risk; RT +/- chemo

Cancer of the Oral Cavity
Resectable T4, Any N:• Surgery (preferred for bone invasion) Chemo/RT or• Chemo/RT Surgery for residual dz (primary or LN)

Cancer of the Oropharynx(Base of tongue/tonsil/posterior pharyngeal wall/soft palate)
H&P Biopsy Chest x-ray or Chest CT CT with contrast or MRI recommended for primary
and neck Panorex as indicated Dental evaluation as indicated Speech & swallowing evaluation as indicated Examination under anesthesia with laryngoscopy Preanesthesia studies Multidisciplinary consultation as indicated

Cancer of the OropharynxT1-2, N0-1
Definitive RT (preferred) : surgery for residual dz
Concurrent chemo/RT (T1-T2, N1 only): surgery for residual dz
Excision of primary ± unilateral or bilateral neck dissection:
One +ve node without adverse features: Consider RT
Adverse features: RT or Chemo/RT (multiple +ve nodes only)

Cancer of the OropharynxT3-4, N0
Concurrent chemo/RT (preferred):• Salvage surgery if residual dz
Surgery + RT:• RT +/- Chemo if high risk or adverse features
Induction chemo followed by chemo/RT off protocol:
• Salvage surgery if residual dz
Multimodality clinical trial

Cancer of the Oropharynxany T3-4, N+ or any T, N2-3
Concurrent chemo/RT (preferred): or Induction chemo followed by chemo/RT off
protocol: Residual Primary tumor:
• Salvage surgery + neck dissection as indicated Residual neck mass Neck dissection CR but initial N2-3;
• Observe or Neck dissection
OR ---

Cancer of the Oropharynxany T3-4, N+ or any T, N2-3
Surgery: primary and neck: N1, N2a–b, N3;
• Excision of primary, ipsi neck dissection N2c;
• Excision of primary and bilateral neck dissection Adj RT or Chemo/RT
Multimodality clinical trial

PRINCIPLES OF RT
Conventional fractionation: 70 Gy (2 Gy/d) in 7 wks Altered fractionation: 72 Gy/6 weeks (1.8 Gy/d, 1.5 Gy/d boost daily
during last 12 treatment days) Hyperfractionation: 81.6 Gy/7 weeks (1.2 Gy bid) Primary and gross adenopathy
> 70 Gy (2 Gy/d) Neck
Low risk: 44-50 Gy (2 Gy/d) Postoperative RT:
• Primary: 60 Gy (2 Gy/d)• Neck
High-risk: 60 Gy (2 Gy/d) Low-risk:50 Gy (2 Gy/d)
Concurrent Therapy: Conventional RT + Cisplatin 100 mg/m q 3 wk Use of other fraction sizes and multiagent chemotherapy, has been
evaluated with no consensus on the optimal approach.

Cancer of the Oral Cavity OropharynxF/U
Physical exam:• Year 1, every 1-3 m• Year 2, every 2-4 m• Years 3-5, every 4-6 m• > 5 yr, every 6-12 m
Chest imaging as clinically indicated TSH every 6-12 m, if neck irradiated Speech and swallowing evaluation and
rehabilitation as indicated

Hypopharynx (laryngopharynx) entrance to the esophagus
Work-up H&P Biopsy Chest x-ray or Chest CT CT with contrast or MRI of primary and neck Examination under anesthesia with
laryngoscopy and esophagoscopy Preanesthesia studies Dental evaluation Multidisciplinary consultation as indicated

Cancer of the Hypopharynx
Early T stage not requiring total laryngectomy:
• Most T1, N0-1• Small T2, N0
Resectable advanced cancer requiring total laryngectomy:
• T1, N2-3• T2-4, Any N• Participation in clinical is preferred
Unresectable

Early T stage (not requiring total laryngectomy) Most T1, N0-1, small T2, N0
Definitive RT:• Neck dissection (selective vs comprehensive) if residual dz
Surgery: Partial laryngopharyngectomy + • Ipsi or bilateral selective neck dissection (N0)• Comprehensive neck dissection levels 1-5 (N1)
Adj RT or Chemo/RT if adverse features:• Extracapsular nodal spread• +ve margins• Multiple +ve nodes • Perineural/lymphatic/vascular invasion

T1, N2-3; T2-3, any N (if total laryngectomy required)
Induction chemotherapy x 2 cycles: CR of primary site:
• Definitive RT: Residual neck mass Neck dissection CR of neck if initial N2-3 Observe or neck dissection
PR of primary site:• Chemo x 1 cycle:
CR of primary definitive RT• Residual neck mass Neck dissection• CR of neck if initial N2-3 Observe or neck dissection
Residual primary savage surgery;• RT or chemoRT depending on adverse features
Less than PR of primary:• Surgery:
RT or chemoRT depending on adverse features

T1, N2-3; T2-3, any N (if total laryngectomy required)
Laryngopharyngectomy + selective (N0) or comprehensive (N+) neck dissection
• Adj RT or ChemoRT depends on adverse features
Concurrent chemoRT: CR of primary;
• Residual neck mass Neck dissection• CR of neck if initial N2-3 observe or neck
dissection PR of primary;
• Salvage surgery + neck dissection as indicated
Multimodality clinical trial

Hypopharynx T4, any N
Surgery + comprehensive neck dissection• Chemo/RT
Concurrent chemo/RT: CR of primary:
• Residual neck mass Neck dissection• CR of neck; N1 observe
if initial N2-3 observe or neck dissection
PR of primary:• Salvage surgery + neck dissection as indicated
Multimodality clinical trial

HypopharynxPRINCIPLES OF RADIATION THERAPY
Definitive RT Primary and gross adenopathy:
• > 70 Gy (2 Gy/d)• Neck; low risk > 50 Gy (2 Gy/d)
Postoperative RT: Primary: > 60 Gy (2 Gy/d) Neck;
• high-risk > 60 Gy (2 Gy/d)• Low-risk > 50 Gy (2 Gy/d)
Postoperative chemoRT for high risk: Concurrent Cisplatin 100 mg/m q 3 wks

Occult Primary Neck mass FNA
SCC Adenocarcinoma Anaplastic Epithelial tumors
WORK-up• Complete head and neck exam with attention to skin,
including nasopharyngoscopy• Chest x-ray• CT or MRI (skull base through thoracic inlet)• PET scan • Examination under anesthesia• Direct laryngoscopy and nasopharynx survey• If level IV, lower V nodes:
Bronchoscopy, EGD Chest/abdominal/pelvic CT

Occult Primary (NO primary found)
Adenocarcinoma (levels I–III): Comprehensive neck dissection + parotidectomy, if
indicated• RT to neck ± parotid bed
SCC: Comprehensive neck dissection
N1 Adj RT Extracapsular spread or N2, N3 RT or ChemoRT
Poorly diff or nonkeratinizing SCC or NOS or Anaplastic (Not thyroid) :
Comprehensive neck dissect Adj RT +/- chemo or RT or Chemo RT
• Residual dz Comprehensive neck dissect

Cancer of the Glottic Larynxwork-up
H&P Biopsy Chest x-ray or Chest CT CT with contrast and thin cuts through larynx, or MRI of primary and neck Examination under anesthesia with laryngoscopy Preanesthesia studies Dental evaluation as indicated Speech & swallowing evaluation as indicated Multidisciplinary consultation as indicated

Glottic Larynx Severe dysplasia/CIS
Clinical trial or Endoscopic removal (stripping/laser) or RT

Glottic LarynxTotal laryngectomy not required
(Most T1-2, any N)
RT to primary > 66 Gy or Partial laryngectomy/endoscopic
resection (selected superficial lesions) or Open partial laryngectomy
• N-ve N-ve observe observe• N+ve N+ve Neck dissection and/or RT

Glottic LarynxResectable requiring total laryngectomy
Most T3, any N
Concurrent chemoradiation: Primary and neck CR observe
• if initial N2-3 Observe or neck dissection Primary CR, neck PR Neck dissection Primary PR Salvage surgery + neck
dissection as indicated

Glottic LarynxResectable requiring total laryngectomy
Most T3, any N
Surgery:Surgery: N0:-N0:-
• Laryngectomy with ipsi thyroidectomy +/- unilat or bilateral Laryngectomy with ipsi thyroidectomy +/- unilat or bilateral selective neck dissectionselective neck dissection
N1:-N1:-• Laryngectomy with ipsi thyroidectomy, ipsi comprehensive Laryngectomy with ipsi thyroidectomy, ipsi comprehensive
neck dissection ± contral selective neck dissectionneck dissection ± contral selective neck dissection N2-3:-N2-3:-
• Laryngectomy with ipsi thyroidectomy, ipsi or bilateral Laryngectomy with ipsi thyroidectomy, ipsi or bilateral comprehensive neck dissectioncomprehensive neck dissection
Adj Therapy:Adj Therapy: If adverse features: If adverse features: (Extracapsular nodal spread +ve margins, multiple +ve LN or (Extracapsular nodal spread +ve margins, multiple +ve LN or
perineural/lymphovascular invasion)perineural/lymphovascular invasion)
• Adj RT +/- chemoAdj RT +/- chemo

Glottic LarynxT4
Selected T4: Consider concurrent chemoRT or Clinical trial for function preserving
• Primary and neck CR observe if initial N2-3 Observe or neck dissection
• Primary CR, neck PR Neck dissection• Primary PR Salvage surgery + neck
dissection as indicated

Glottic Larynx T4, Any N
N0:-N0:- Laryngectomy with ipsi thyroidectomy +/- unilat Laryngectomy with ipsi thyroidectomy +/- unilat
or bilateral selective neck dissectionor bilateral selective neck dissection
N1:- N1:- Laryngectomy with ipsi thyroidectomy, ipsi Laryngectomy with ipsi thyroidectomy, ipsi
comprehensive neck dissection ± contral comprehensive neck dissection ± contral selective neck dissectionselective neck dissection
N2-3:-N2-3:- Laryngectomy with ipsi thyroidectomy, ipsi or Laryngectomy with ipsi thyroidectomy, ipsi or
bilateral comprehensive neck dissectionbilateral comprehensive neck dissection
Adj chemo/RTAdj chemo/RT

Glottic LarynxPRINCIPLES OF RADIATION THERAPY
Definitive RT Primary and gross adenopathy:
• > 70 Gy (2 Gy/d) For early cancer of the glottic larynx, preferred dose is 2
Gy/d with total dose modification accordingly Neck
• Low-risk: > 50 Gy (2 Gy/d) Postoperative RT
Primary: > 60 Gy (2 Gy/d) Neck
• High-risk: > 60 Gy (2 Gy/d)• Low-risk > 50 Gy (2.0 Gy/day)
Postoperative chemoradiation for high pathologic risk features:
Concurrent Cisplatin at 100 mg/m q 3 wks

Glottic LarynxF/U
Physical exam: Year 1, every 1-3 m Year 2, every 2-4 m Years 3-5, every 4-6 m > 5 years, every 6-12 m
Chest imaging as clinically indicated TSH every 6-12 m, if neck irradiated Speech and swallowing evaluation and
rehabilitation as indicated

Supraglottic LarynxResectable not requiring total laryngectomy
Most T1–2, N0
Endoscopic resection ± selective neck dissection or
Open partial supraglottic laryngectomy ± selective neck dissection or
Definitive RT Adj Therapy:-
• One +ve LN without other adverse features Consider RT
• Adverse features: (+ve margins or extracapsular nodal) ChemoRT

Supraglottic LarynxResectable requiring laryngectomy (T3, N0; T4, N0)(No cartilage destruction, low-volume base-of tongue involvement)
Laryngectomy, ipsi thyroidectomy + ipsi or bilateral selective neck dissection
• N0 or one +ve LN without adverse features RT optional
• Adverse features RT or chemoRT
Concurrent chemoRT:• Primary site PR:
Salvage surgery + neck dissection as indicated

Supraglottic LarynxResectable T4, N0
Skin involvement, high-volume invasion of base of tongue; cartilage destruction
Laryngectomy, ipsi thyroidectomy + ipsi Laryngectomy, ipsi thyroidectomy + ipsi or bilateral selective neck dissectionor bilateral selective neck dissection
• Adj RT or chemoRTAdj RT or chemoRT
Or Cclinical trialOr Cclinical trial

Supraglottic LarynxNode positive disease
H&P Biopsy Chest x-ray or Chest CT CT with contrast and thin cuts through larynx or MRI of primary and neck recommended Examination under anesthesia with laryngoscopy Dental evaluation as indicated Speech & swallowing evaluation as indicated Multidisciplinary consultation as indicated

Supraglottic Larynx (N+ve) CLINICAL STAGING
1- Resectable; Not requiring total laryngectomy (T1–2, N+ and selected T3–4)
2- Resectable; Requiring total laryngectomy (Most T3–4, N+):
• Low-volume base-oftongue involvement• No cartilage destruction
3- High-volume T4, N+:• Cartilage destruction• Skin involvement• High-volume invasion of base of tongue
4- Unresectable

Supraglottic LarynxResectable; Not requiring total laryngectomy (T1–2, N+ and selected T3–4)
Definitive RT or Concurrent chemoRT:
• Primary site CR: Residual neck mass Neck dissection CR of neck Observe or Neck dissection if initial N2-3
• Primary site; residual tumor: Salvage surgery + neck dissection as indicated
Or Partial supraglottic laryngectomy and comprehensive neck dissection:
• Observe or RT+/-Chemo if adverse features

Supraglottic LarynxResectable; Requiring total laryngectomy (Most T3–4, N+)
Laryngectomy, ipsi thyroidectomy with comprehensive neck dissection:
• No adverse features Adj RT
• Adverse features Adj RT+/-Chemo
Or Concurrent chemoRT (preferred)• Primary site CR:
Residual neck mass Neck dissection CR of neck Observe or Neck dissection if initial N2-3
• Primary site; residual tumor: Salvage surgery + neck dissection as indicated

Supraglottic Larynx High-volume T4, N+
Laryngectomy, ipsi thyroidectomy with ipsi or bilateral neck dissection or
Clinical trial• Adj ChemoRT

Supraglottic LarynxPRINCIPLES OF RADIATION THERAPY
Definitive RT: Primary and gross adenopathy:
• > 70 Gy (2 Gy/day) Neck (Low-risk):
• > 50 Gy (2 Gy/day)
Postoperative RT: Primary:
• > 60 Gy (2 Gy/day) Neck (High-risk):
• > 60 Gy (2 Gy/day) Neck (Low-risk)
• > 50 Gy (2 Gy/day)
Postoperative chemoRT for high pathologic risk features: Concurrent single agent Cisplatin 100 mg/m q 3 wks

Cancer of the NasopharynxWORKUP
H&P Nasopharyngeal exam and biopsy Chest x-ray or Chest CT MRI with gadolinium of nasopharynx and base of
skull to clavicles and/or CT with contrast Dental evaluation as indicated Speech & swallowing evaluation as indicated Imaging for distant metastases (chest, liver, bones)
for N2-3 disease (PET scan and/or CT) Multidisciplinary consultation

Cancer of the NasopharynxT1, N0, M0
T2a, N0, M0
Definitive RT to nasopharynx Elective RT to neck

Cancer of the NasopharynxT1, N1-3; T2b-T4, any N
Concurrent ChemoRT: Cis 100 mg/m on d 1, 22, 43 RT ( 70 Gy) to primary and gross nodal dz Bilateral neck > 50 Gy
Then
Cis 80 mg/m d 1 + 5-FU 1,000 mg/m CI x 4 d repeat every 4 wk x 3
• Neck: CR Observe
• Neck: residual dz Neck dissection

Cancer of the NasopharynxAny T, any N, M1
Platinum-based combination chemo If CR:
• Definitive RT to primary and neck

Cancer of the Nasopharynx FOLLOW-UP
Physical exam: Year 1, every 1–3 mo Year 2, every 2–4 mo Year 3–5, every 4–6 mo > 5 years, 6–12 mo
TSH every 6-12 mo, if neck irradiated Speech and swallowing evaluation and
rehabilitation as indicated

Unresectable Head and Neck Ca M0; T4b, any N; or Unresectable N+
Clinical trial (preferred) PS 0-1:
Concurrent Cis or Carbo-based chemo + RT or Induction chemo followed by RT
• Residual neck disease: Neck dissection, if feasible + primary site controlled
PS 2: Induction chemo followed by RT or Definitive RT
• Residual neck disease: Neck dissection, if feasible + primary site controlled
PS 3: Definitive RT or Best supportive care

Recurrent Head and Neck Cancer
Locoregional recurr without prior RT: Resectable
• Surgery +/- RT Unresectable
Locoregional recurr or 2nd primary with prior RT: Resectable
• Surgery ± reirradiation• clinical trial preferred
Unresectable• Reirradiation • Chemotherapy or• clinical trial preferred
Distant mets: Clinical trial preferred PS 0–1
• Combination chemo or Single-agent chemo PS 2
• Single agent chemo or Best supportive care PS 3
• Best supportive care

PRINCIPLES OF CHEMOTHERAPY(SCC: Maxillary Sinus, Ethmoid Sinus, Lip, Oral Cavity, Oropharynx, Hypopharynx, Glottic larynx, Supraglottic larynx, Occult Primary)
Primary ChemoRT: Cisplatin alone 5-FU/hydroxyurea Cis/Taxol Cis/5-FU Carbo/5-FU
Postoperative Chemoradiation: Cisplatin alone
Induction chemo (followed by chemoRT): Carbo/Taxol Docetaxel/cisplatin/5-FU

PRINCIPLES OF CHEMOTHERAPYNasopharynx
ChemoRT followed by adj chemo Cis + RT followed by Cis/5-FU

PRINCIPLES OF CHEMOTHERAPY Unresectable Recurrent Head and Neck Cancers
Combination therapy Cis or carbo + 5-FU Cis or carbo + taxane Cis/cetuximab
Single agent Cisplatin Carboplatin Paclitaxel Docetaxel 5-FU Methotrexate Ifosfamide Bleomycin Gemcitabine (nasopharyngeal) Cetuximab

THANKSTHANKS