-
7/30/2019 Galley - Inflammation and Immunity
1/119
Critical Care Focus10: Inflammation and
Immunity
EDITOR
DR. HELEN F. GALLEY
BMJ Books
-
7/30/2019 Galley - Inflammation and Immunity
2/119
Critical Care Focus
10: Inflammation and Immunity
-
7/30/2019 Galley - Inflammation and Immunity
3/119
-
7/30/2019 Galley - Inflammation and Immunity
4/119
Critical Care Focus
10: Inflammation and Immunity
EDITOR
DR HELEN F GALLEY
Senior Lecturer in Anaesthesia and Intensive Care
University of Aberdeen
EDITORIAL BOARD
PROFESSOR NIGEL R WEBSTER
Professor of Anaesthesia and Intensive Care
University of Aberdeen
DR PAUL G P LAWLER
Clinical Director of Intensive Care
University of Aberdeen
DR NEIL SONI
Consultant in Anaesthesia and Intensive Care
Chelsea and Westminster Hospital
DR MERVYN SINGER
Reader in Intensive Care
University College Hospital, London
-
7/30/2019 Galley - Inflammation and Immunity
5/119
BMJ Publishing Group 2003BMJ Books is an imprint of the BMJ
Publishing Group
All rights reserved. No part of this publication may be
reproduced, stored in aretrieval system, or transmitted, in any
form or by any means, electronic,
mechanical, photocopying, recording and/or otherwise, without
the prior writtenpermission of the publishers.
First published in 2003by BMJ Books, BMA House,Tavistock
Square,
London WC1H 9JR
www.bmjbooks.comwww.ics.ac.uk
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British
Library
ISBN 0-7279-1689-0
Typeset by Newgen Imaging Systems (P) Ltd, Chennai.Printed and
bound in Spain by GraphyCems, Navarra
-
7/30/2019 Galley - Inflammation and Immunity
6/119
v
Contents
Contributors vii
Preface viii
Introduction ix
1 Immunoparalysis 1
JEAN-MARC CAVAILLON, HELEN F GALLEY
2 Apoptosis and the inflammatory process 18NIGEL R WEBSTER
3 Virus interaction with host immunity 33
LAWRENCE S YOUNG
4 The double-edged role of the neutrophil in inflammatory
responses 47
PAUL G HELLEWELL
5 T cell immunity and sepsis 65
EGBERT PRAVINKUMAR
6 Metalloproteinases and inflammation 77
ANDREW J GEARING
7 Glucocorticoid therapy in septic shock 90
PIERRE-EDOUARD BOLLAERT
Index 99
-
7/30/2019 Galley - Inflammation and Immunity
7/119
Critical Care Focus series
Also available:
H F Galley (ed) Critical Care Focus 1: Renal Failure, 1999.
H F Galley (ed) Critical Care Focus 2: Respiratory Failure,
1999.
H F Galley (ed) Critical Care Focus 3:Neurological Injury,
2000.
H F Galley (ed) Critical Care Focus 4: Endocrine Disturbance,
2000.
H F Galley (ed) Critical Care Focus 5:Antibiotic Resistance and
Infection
Control, 2001.
H F Galley (ed) Critical Care Focus 6: Cardiology in Critical
Illness, 2001.
H F Galley (ed) Critical Care Focus 7:Nutritional Issues,
2001.
H F Galley (ed) Critical Care Focus 8: Blood and Blood
Transfusion, 2002.
H F Galley (ed) Critical Care Focus 9: The Gut, 2002.
-
7/30/2019 Galley - Inflammation and Immunity
8/119
vii
Contributors
Pierre-Edouard BollaertProfesseur des Universits, Service de
Ranimation Mdicale, Centre
Hospitalier Universitaire, Nancy, France
Jean-Marc Cavaillon
Unit dImmunology-Allergie, Institute Pasteur, Paris, France
Helen F Galley
Senior Lecturer in Anaesthesia and Intensive Care, University
of
Aberdeen, UK
Andrew J Gearing
Chief Executive Officer, Biocomm International, Melbourne,
Victoria,
Australia
Paul G Hellewell
Professor of Vascular Biology, University of Sheffield, UK
Egbert PravinkumarLecturer in Intensive Care Medicine,
University of Aberdeen, UK
Nigel R Webster
Professor of Anaesthesia and Intensive Care and Honorary
Consultant,
University of Aberdeen, UK
Lawrence S Young
Director of Institute and Head of Division of Cancer
Research,
UK Institute for Cancer Studies, University of Birmingham,
UK
-
7/30/2019 Galley - Inflammation and Immunity
9/119
viii
Preface to the Critical Care
Focus series
The Critical Care Focus series aims to provide a snapshot of
currentthoughts and practice, by renowned experts. The complete
series should
provide a comprehensive guide for all health professionals on
key issues in
todays field of critical care. The volumes are deliberately
concise and easy
to read, designed to inform and provoke. Most chapters are
produced from
transcriptions of lectures given at the Intensive Care Society
meetings and
represent the views of world leaders in their fields.
Helen F Galley
-
7/30/2019 Galley - Inflammation and Immunity
10/119
ix
Introduction
Immunoparalysis
Jean-Marc Cavaillon and Helen F Galley
Several studies indicate that depression of immune function
induced by
traumatic injury is aetiologically involved in the development
of infection
or sepsis. Nevertheless, the mechanisms behind the maintenance
of the
sustained suppression of immune function remain incompletely
understood. Alterations of immune responses have been regularly
reported
in patients with systemic inflammatory responses syndrome
(SIRS).
The observation that some patients have apparent immune
paralysisled to the concept of compensatory anti-inflammatory
response
syndrome or CARS. In this article, we describe this phenomenon
of
immunoparalysis but, although alterations in immune response
are
probably associated with an enhanced sensitivity to nosocomial
infections,
there is no clear demonstration that they are directly
responsible for poor
outcome in sepsis.
Apoptosis and the inflammatory process
Nigel R Webster
Cells that are damaged by injury undergo swelling and leakage of
cell
contents, leading to inflammation of surrounding tissues. This
process
is called necrosis. Cells that are induced to commit suicide, in
contrast,
shrink, and the mitochondrial membrane becomes breached such
that
release of cytochrome c occurs. Chromatin (DNA and protein) in
the
nucleus becomes degraded into small, membrane-wrapped fragments,
and
the phospholipid phosphatidylserine, which is normally hidden
within theplasma membrane, is exposed on the surface. This is then
bound by
receptors on phagocytic cells, such as macrophages, which engulf
the cell
fragments, leading to a quiet orderly removal of dead cells.
This pattern
-
7/30/2019 Galley - Inflammation and Immunity
11/119
x
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
of events is called programmed cell death or apoptosis. The
cellular
machinery of programmed cell death is as intrinsic to the cell
as, for
example, mitosis. This article will describe the regulation and
process of
apoptosis and its relevance to disease, including the
inflammatory response
in patients with sepsis.
Virus interaction with host immunity
Lawrence S Young
Resistance to and recovery from viral infections depends on
the
interactions between virus and host. The defences mounted by the
host
may act directly on the virus or indirectly on virus replication
by altering or
killing the infected cell. The non-specific host defences
function early inthe encounter with virus to prevent or limit
infection, while the specific
host defences function after infection in initiation of immune
responses
to subsequent challenges. Viruses have evolved complex
strategies to
manipulate host immune defences to their advantage, permitting
viral
replication without massive inflammatory responses integrating
their
needs with that of their host man. However, some persistent and
latent
viral infections can lead to serious disease and malignancy.This
article will
describe the hostvirus interactions and particularly focus on
the role of
latent infection with the EpsteinBarr virus in tumour
development thekiller within.
The double-edged role of the neutrophil in
inflammatory responses
Paul G Hellewell
Accumulation of leucocytes in tissues is essential for effective
host
defence. The major role of neutrophils is to phagocytose and
destroy
infectious agents but they can also cause host damage, and
neutrophil-
mediated injury has been implicated in several inflammatory
conditions
seen on the Intensive Care Unit (ICU). This article provides an
overview
of the vital role of neutrophils in host defence, and the
consequences of
host damage. An increased understanding of neutrophil biology is
likely to
result in intelligent intervention strategies.
T cell immunity and sepsis
Egbert Pravinkumar
Immune responses essential for defeating systemic microbial
infections
depend on intact innate and acquired immune responses.
Recognition
-
7/30/2019 Galley - Inflammation and Immunity
12/119
xi
molecules, inflammatory cells, and the cytokines allow host
tissues to
recognise invading microbes and to initiate intercellular
communication
between the innate and acquired immune systems. However,
activation of
innate immunity may also occur in the absence of microbial
recognition,
through expression of internal signals produced by tissue
ischaemia andnecrosis. Induction of the innate immune system can
have catastrophic
effects on patients with sepsis. Exaggerated production of
cytokines and
the induction of mediators such as nitric oxide, platelet
activation factor,
and prostaglandins have been implicated in the endothelial
changes and
induction of a procoagulant state, leading to hypotension,
inadequate organ
perfusion, and necrotic cell death, associated with multiorgan
dysfunction
syndrome. This article provides an overview of the T cell immune
system,
its regulation, and the influence of sepsis.
Metalloproteinases and inflammation
Andrew J Gearing
Matrix metalloproteinases (MMPs) are a large family of
zinc-containing
endoproteinases, which have similar structures but differ in
substrate
specificity, cellular sources, and inducibility. MMP activity is
controlled at
the transcriptional level and by a family of at least four
endogenous natural
inhibitors (tissue inhibitors) of MMPs called TIMPs. MMPs
cleaveprotein components of the extracellular matrix, membrane
receptors, and
cytokines, and have a role in cell extravasation. This article
describes the
action, regulation, and roles of MMPs in inflammatory and
immune
responses.
Glucocorticoid therapy in septic shock
Pierre-Edouard Bollaert
Recent findings highlighting the role of the ability of the
hypothalamic
pituitaryadrenal axis to respond appropriately to a septic
insult have led
to a reappraisal of the use of steroids in septic shock. Recent
work has
suggested that physiological doses of corticosteroids given for
a longer
duration may be beneficial in catecholamine-dependent septic
shock
leading to a more rapid withdrawal of vasopressor therapy and a
trend
toward improved survival. A recent multicentre study of patients
in septic
shock has suggested a reduction in mortality in patients with
relative
adrenal insufficiency receiving replacement therapy with a
combinationof hydrocortisone and fludrocortisone. This article
describes studies of
corticosteroid therapy in patients with septic shock and
comments on the
possible benefits of corticosteroid therapy in this
population.
INTRODUCTION
-
7/30/2019 Galley - Inflammation and Immunity
13/119
-
7/30/2019 Galley - Inflammation and Immunity
14/119
1
1: ImmunoparalysisJEAN-MARC CAVAILLON, HELEN F GALLEY
Introduction
Several studies indicate that depression of immune function
induced by
traumatic injury is aetiologically involved in the development
of infection
or sepsis. Nevertheless, the mechanisms behind the maintenance
of the
sustained suppression of immune function remain incompletely
under-
stood. Alterations of immune responses have been regularly
reported in
patients with systemic inflammatory response syndrome
(SIRS).
Trauma, haemorrhage, burns, surgery, or sepsis are associated
with events
such as tissue injury, blood loss, hypoxia, transfusion,
microbial infection, andbacterial translocation, which contribute
to an inflammatory response and
affect the quality of the immune response. Drugs (for example,
anaesthetics,
opioids) also influence immune responses (Figure 1.1). Depressed
immune
status including decreased blood cell counts, low expression of
surface
markers (for example, MHC Class II antigen), altered natural
killer (NK) cell
activity, reduced cellular cytotoxicity and antigen
presentation, poor
proliferation in response to mitogens, and depressed cytokine
production, are
seen in vitro, and illustrated in vivo by anergy to skin test
antigens. These
observations led Roger Bone to coin the concept of compensatory
anti-
inflammatory response syndrome or CARS.1 Bone postulated that
when the
SIRS response predominated it was associated with an organ
dysfunction and
cardiovascular compromise leading to shock; in contrast, when
CARS
predominated it was characterised by anti-inflammatory responses
associated
with a suppression of the immune system termed immunoparalysis.1
It was
initially accepted that the SIRS response occurred first and was
followed in
some patients by the CARS response. However, the two syndromes
most
probably occur concomitantly.2 In this article, we will describe
the
phenomenon of immunoparalysis in SIRS patients. Although
alterations in
immune response are probably associated with an enhanced
sensitivity to
nosocomial infections, there is no clear demonstration that they
are directly
responsible for poor outcome in sepsis. Indeed, since the
investigations of
-
7/30/2019 Galley - Inflammation and Immunity
15/119
2
immune function may depend upon numerous parameters (for
example,
nature of the activators, cell types used, initial compartment
of the cells, the
cytokine investigated), interpretation of findings is not
easy.
Measures of immune dysfunction
How can this modification of immune status be monitored?
Lymphocyte
and monocyte population changes and also HLA-DR expression are
simple
examples. Immune suppression can be assessed in vitro as poor
lymphocyte
proliferation in response to mitogens, reduced NK cell activity,
reduced
neutrophil function, reduced cytokine production, and in vivo
anergy to
skin test antigens (Figure 1.2).
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Figure 1.2 Approaches to monitoring immune status resulting from
trauma, haemorrhage, burns,surgery, or sepsis.
IMMUNE STATUS
Immune suppression
Lymphocyte
proliferation
Anergy to skin
test antigens
Natural killer
cell activity Cytokineproduction
Lymphocyte/monocyte
population changes
Anaesthesia
Opioids
Blood loss
Transfusion
Hypoxia
Tissue injury
Bacterial translocation
Inflammatory response
IMMUNE STATUS
Figure 1.1 Contributory factors to altered immune status,
resulting from trauma, haemorrhage,burns, surgery, or sepsis.
-
7/30/2019 Galley - Inflammation and Immunity
16/119
3
HLA-DR expression
Abnormal antigen presentation has been observed in SIRS
patients,3 and
decreased HLA-DR expression on monocytes may contribute to
this
defect.4
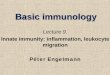
In a study by Hershman and colleagues,5
60 trauma patients wereretrospectively divided into three
groups: those with an uneventful recovery
(n 17), those with recovery after major sepsis (n 27), and those
who
did not survive (n 16). HLA-DR expression on peripheral
blood
monocytes was compared with that of 77 healthy volunteers.
After
the initial injury, there was a significant decrease from normal
in the three
groups of trauma patients, and this returned to normal after one
week in
the group of patients who recovered uneventfully. In those who
developed
sepsis, HLA-DR expression took three weeks to return to normal
and in
the patients who did not survive, expression never returned to
normal.Thisstudy demonstrated that monocyte HLA-DR antigen
expression was able
to distinguish those patients who survived severe trauma, from
those who
died (Figure 1.3). HLA-DR antigen expression correlated directly
with the
clinical course and identified a group of patients at high risk
of infection
and death following trauma.5 Low HLA-DR expression is now
widely
recognised as a good marker of the intensity of the immune
depression and
of increased risk of bacterial infection.6,7
IMMUNOPARALYSIS
uneventful recovery
major sepsis
death
80
60
40
%HLA-DRpo
sitivemonocytes
20
Days after injury
1 3 6 9 12 15 18
Figure 1.3 Percentage of monocytes expressing HLA-DR expression
in 60 trauma patients, 17 of
whom had an uneventful recovery, 27 developed sepsis and 16
died. Dotted line represents mean
HLA-DR expression in 77 healthy controls. Reproduced with
permission from Hershman Met al.5
-
7/30/2019 Galley - Inflammation and Immunity
17/119
4
Lymphocyte proliferation
Impaired lymphocyte transformation in SIRS patients was reported
more
than three decades ago.8 The impairment was proportional to the
severity
of the injury. In vitro lymphocyte proliferative response to
antigens andmitogens, and in mixed lymphocyte reactions, are all
significantly
decreased in trauma patients.8,9 The length of depressed
lymphocyte
responses may exceed two weeks, and lower responses and longer
depression
have been observed in patients who become infected.9,10
Natural killer cell activity
The ability of the cell to mount an NK cell response provides
another
means to monitor immune status. NK cell activity was studied in
burn andtrauma patients11 and was shown to be significantly
depressed over a very
long period of time for the more severely burned patients.
Patients with
lesser burns and traumatically injured patients had an altered
NK activity
for a shorter period. Interestingly, Blazar et al. further
showed that stress-
induced mediators (cortisol, epinephrine, glucagon) had the
capacity to
reduce NK activity in healthy volunteers.11 In the study by
Maturana
et al.,12 patients with septic shock (n 11) had also a markedly
lower NK
activity than healthy controls (n 10), independently of the
effector:target
cell ratio in the experimental system. In another study, NK cell
activityin patients with septic shock (n 20) was also lower than in
healthy
volunteers (n 15). Pre-incubation of peripheral blood
lymphocytes with
either interferon- (IFN) or interleukin-2 (IL-2) enhanced NK
cell
activity in healthy controls but not in patients with sepsis
indicating the
difficulty in reversing the depressed immune
responsiveness.13
Neutrophil functions
Although apoptosis of circulating neutrophils (PMN) is delayed
in patientswith SIRS or sepsis,14 function of the cells is altered.
This is the case of
phagocytosis and bactericidal activity15 and of migration.16 The
reduced
responsiveness of PMN to chemoattractant agents may reflect the
action of
nitric oxide,16 the decreased expression of certain chemokine
receptors,17
or a deactivation occurring in the bloodstream after interacting
with large
amounts of circulating chemokines as indicated, for example, by
the huge
amounts of IL-8 found associated to PMN in septic
patients.18
Delayed hypersensitivity
The in vitro evidence of immune depression is also reflected in
vivo by
tests of delayed type hypersensitivity. Several years ago,
Christou and
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
18/119
5
colleagues19 skin tested 727 surgical patients with recall
antigens prior to
operation. Patients who had normal skin test responses were of
similar age
and had equal degrees of surgical procedures performed compared
with
those patients who were anergic (that is, had depressed skin
test responses).
Postoperatively, sepsis, mortality, and death from sepsis were
significantlyhigher in the anergic population, reconfirming the
hypothesis that skin test
anergy in patients preoperatively is a signal of increased risk
for septic
complications and death in such patients. These authors20 also
reported
that surgical patients who were anergic to a battery of five
skin test antigens
had a two-fold higher rate of postoperative infection than those
who
reacted to only two antigens, and were more than five times more
likely to
die in the postoperative period.
Cytokine production
The analysis of sepsis and SIRS patients reveals a paradoxical
situation: an
overwhelming production of cytokines as assessed by their
concentrations
within the bloodstream21 and a profound reduction of the
capacity of
circulating cells to produce cytokines upon in vitro activation.
Among
pioneering work is the study by Wood and co-workers.22 They
studied the
production of IL-1 and IL-2 by peripheral blood mononuclear
cells from
23 burn patients and 23 matched controls. Serial measurements
were made
of IL-1 production by monocytes after stimulation with
lipopolysaccharide
(LPS), and of IL-2 production by lymphocytes after stimulation
with the
mitogen phytohaemagglutinin (PHA). Lymphocyte IL-2 production
from
12 patients with more than 30% body surface area burns revealed
lower
IL-2 production compared with patients with less than 30%
burns.
Patients with systemic sepsis also had lower IL-2 production
than non-
septic patients. IL-1 production was increased compared with
controls
early after injury, but was subsequently within the normal range
regardless
of burn size. The percentage of circulating helper T
lymphocytes, the
principal source of IL-2, was also reduced, although this did
not always
correlate with IL-2 production, which remained depressed after
recovery of
the T cell population. This study indicated that failure to
produce IL-2,
which is a powerful mediator of cellular immune responses, is an
important
mechanism underlying the defective cell-mediated immunity seen
in burn
patients.22 Surgery also leads to significant modulation of the
immune
system, and cytokine release in particular. Cabie et al.
investigated the
consequences of surgery on in vitro cytokine production by
human
monocytes stimulated by LPS.23 The responsiveness of cells
obtained the
day before, during and after surgery was compared in patients
undergoingabdominal aortic surgery (n 9), carotid surgery (n 4),
and spinal
surgery (n 4). A significant decrease in monocyte tumour
necrosis
factor- (TNF), interleukin-1 (IL-1), and IL-1 production
during
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
19/119
6
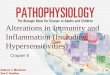
surgery was reported, whereas IL-6 production remained
unchanged.
By day 2 following surgery, a significant increase in
monocyte
responsiveness was observed and levels of cytokine production
were similar
to initial values (Figure 1.4).
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
ng/ml
TNF IL-1
10
8
6
4
2
0
ng/ml
15
12
9
6
3
0pre post pre post
Figure 1.4 Influence of surgery on in vitro monocyte tumour
necrosis factor (TNF) and
interleukin-1 (IL-1) production in nine patients undergoing
aortic surgery, four patients
undergoing surgery for atheromatous lesions of the carotid
artery,and four patients undergoing spinal
surgery. Isolated cells were stimulated for 24 hours with 2 g/ml
lipopolysaccharide (LPS).
Pre one day before surgery and post 3 hours into the surgical
procedure. Reproduced withpermission from Cabie A et al.23
Characterisation of the ex vivo cytokine
production in sepsis and SIRS
Inflammation is characterised by an interplay between pro- and
anti-
inflammatory cytokines. Cytokines are commonly classified in one
or theother category: IL-1, TNF, interferon- (IFN), IL-12, IL-18,
and
granulocyte-macrophage colony stimulating factor (GM-CSF) are
well
characterised as pro-inflammatory cytokines whereas IL-4, IL-10,
IL-13,
-
7/30/2019 Galley - Inflammation and Immunity
20/119
7
IFN, and transforming growth factor- (TGF) are recognised as
anti-
inflammatory cytokines. However, this dichotomy may be too
simplistic
and it should be remembered that the amount of cytokine
produced, the
target cell, the activating signal, the timing and sequence of
cytokine action,
and even the experimental model, are parameters that greatly
influencecytokine properties.24
There have been several studies investigating in vitro
stimulated cytokine
release in patients with sepsis, in stimulated whole blood or
isolated cell
preparations.
Monocyte-derived cytokines
Several years ago, Munoz et al. studied the capacity of
monocytes from
septic patients to produce cytokines in response to LPS.25
Monocyteproduction of IL-1, IL-1, IL-6 and TNF in patients with
sepsis
syndrome (n 23) or non-infectious shock (n 6) was measured
at
admission and at regular intervals during intensive care unit
(ICU) stay.
Reduced LPS-induced production of cytokines was most pronounced
in
patients with Gram-negative infections. Recovery of cytokine
production
was observed among surviving patients but not in non-surviving
patients.
The data suggest that complex regulatory mechanisms can
downregulate
the production of cytokines by monocytes during severe
infections.
The suppression of lymphocyte and monocyte responses may
reflectpotential defects in the upregulation of the IL-12 and IFN
pathway.These
cytokines exert protective effects during experimental
endotoxaemia
through upregulation of cellular immunity and phagocytic
functions and are
part of a positive regulatory feedback loop that enhances the
production of
the other. In a study by Ertel et al.,26 LPS-stimulated whole
blood from 25
critically ill patients and 12 healthy individuals was incubated
with either
recombinant human (rh) IL-12 or rhIFN.They found that, although
IFN
increased the release of IL-12 from LPS-stimulated whole blood
from
healthy subjects in a dose-dependent manner, this effect was not
seen incritically ill patients. IL-12 enhanced the secretion of IFN
in healthy
subjects, but was ineffective in critically ill patients.
Although the anti-
inflammatory cytokine, IL-10, but not IL-4, mimicked suppression
of the
IL-12-IFN pathway similar to that observed during critical
illness, the
release of anti-inflammatory cytokines (IL-4, IL-10, TGF) was
decreased
in LPS-stimulated blood from critically ill patients. This study
suggested
that deactivation of IL-12 and IFN-producing leukocytes occurred
in vivo.
Lymphocyte-derived cytokines
The T lymphocyte population comprises both T helper 1 (Th1) and
T helper 2
(Th2) subsets. Th1 cells produce cytokines predominantly
concerned with
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
21/119
8
pro-inflammatory responses (IFN, TNF, IL-2) and Th2 produce
cytokines concerned with anti-inflammatory responses (IL-4,
IL-10, and
IL-13). It has been regularly reported that the production of
Th1 cytokines
was mainly altered in SIRS patients, whereas this was not the
case for the
Th2 cytokines.27,28 However, the study of purified T cells from
37 severelyinjured trauma patients showed that T cell anergy was a
global depression of
both Th1 and Th2 cytokine profile. Interestingly, depressed T
cell
proliferation and depressed cytokine production correlate to
poor clinical
outcome.29 Muret et al. further illustrated that infectious and
non-infectious
SIRS exert a more subtle modulation on circulating cell
reactivity. They
investigated the production of IL-2, IL-4, IL-5, and IL-10 by
peripheral
blood mononuclear cells in 13 patients with sepsis and 13
patients with non-
infectious inflammation (patients undergoing cardiac surgery
with
cardiopulmonary bypass).30
Cytokine release after activation of lymphocyteswith either
concanavalin A (ConA), PHA, or anti-CD3 antibodies was
studied. ConA-induced IL-10 was reduced in both groups of
patients
compared with healthy controls. In sepsis patients, ConA-induced
IL-2,
IL-5, and IL-10 production was decreased but not that released
in response
to PHA or anti-CD3. In cardiac patients, only anti-CD3-induced
IL-10
production was reduced.These data indicate that subtle
modifications of the
reactivity of circulating cells occur during infectious and
non-infectious
inflammation, dependent on the cell stimulus. This suggests that
regulation
of both Th1 and Th2 responses is occurring in patients with
sepsis and SIRS,and that the cell stimulant used determines the
results achieved.
Neutrophil-derived cytokines
McCall and co-workers31 reported that neutrophils from patients
with
the sepsis syndrome were consistently resistant to LPS
stimulation such
that synthesis of IL-1 was depressed. This downregulation
occurred
concomitant with an upregulation in expression of the type 2
IL-1 receptor
(IL-1r2). Similar findings were not seen in uninfected patients
with severe
trauma or shock from other causes. In another study,32 Marie et
al. reported
depressed IL-8 release from neutrophils in patients who had
undergone
cardiac surgery with cardiopulmonary bypass and patients with
sepsis. Cells
were activated with either LPS or heat-killed streptococci.
Compared with
healthy controls, the release of IL-8 in both groups of patients
was
significantly reduced whether activated by LPS or by
heat-killed
streptococci.These observations suggest that stressful
conditions related to
inflammation, independently of infection, resulted in
hyporeactivity of
circulating neutrophils, suggestive of LPS tolerance. However,
in vitroexperiments suggested that neutrophils from healthy
controls (in contrast to
monocytes) could not be rendered tolerant to LPS. Interestingly,
while
IL-1 receptor antagonist (IL-1ra) was shown to be enhanced in
whole
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
22/119
9
blood assays in meningococcal infection,33 Marie et al. found
that the release
of IL-1ra by isolated PMN was diminished in SIRS patients.34
Not a universal defect
It is noteworthy that the diminished capacity of leukocytes from
SIRS
patients to produce cytokines as compared with healthy donors is
not
obtained with all activating signals. For example, McCall et
al.,31 in their
studies of patients with sepsis, failed to observe a decreased
capacity of
PMN to release IL-1 when they used heat-killed staphylococci,
while
immune-depression was revealed with LPS. In sepsis, IL-2, IL-5,
and
IL-10 production in response to conA was reduced, but not
when
phytohaemagglutinin or anti-CD3 were used.30
More recently, in cardiac arrest and resuscitated patients,
hyporeactivity,assessed in terms of TNF production, was observed
with LPS stimulation,
but not with heat-killed staphylococci (Adrie et al., personal
communication).
A similar dissociation between stimuli that reveal
hyporeactivity (LPS, CpG,
IL-1,TNF) and those that do not (for example, staphylococci,
streptococci)
has also been observed in trauma patients (Adib-Conquy et al.,
personal
communication). These observations suggest that differential
alteration of
signalling pathways may occur within the cells of SIRS patients,
depending
upon the nature of the activating agent and the nature of the
cytokine being
analysed.
Mechanisms of hyporesponsiveness of monocytes
Desensitising agents
The presence of deactivating or immunosuppressive agents within
the
bloodstream may contribute to the hyporeactivity of circulating
leukocytes.
IL-10 has been identified as a major functional deactivator of
monocytes in
human septic shock plasma,35 and TGF was shown in animal models
of
haemorrhagic shock and of sepsis to be the causative agent of
the depressed
splenocyte responsiveness.36,37 Furthermore, there is
accumulating
evidence for a strong interaction between components of the
nervous and
the immune systems, and numerous neuromediators have been shown
to
behave as immunosuppressors. Catecholamines suppress the
activity of
immunocompetent cells and are found at higher concentrations in
stressful
situations.38 Catecholamines are known to inhibit TNF
production39 and
to favour IL-10 release.40 Similarly,
alpha-melanocyte-stimulating
hormone contributes to immunosuppression by inducing IL-10
productionby human monocytes.41 In addition, vasoactive intestinal
peptide and
pituitary adenylate cyclase-activating polypeptide directly
inhibit endotoxin
induced pro-inflammatory cytokine secretion.42 SIRS is also
associated
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
23/119
10
with an activation of the hypothalamuspituitaryadrenal axis,
which leads
to the release of glucocorticoids, well known for their potent
ability to limit
cytokine production.43 Finally, prostaglandins are produced
during sepsis
and can also contribute to the downregulation of cytokine
production.44
Endotoxin neutralising molecules
As mentioned previously, the reduced capacity of monocytes to
produce
inflammatory cytokines has been established, particularly in
experimental
systems using LPS as a triggering agent. Since numerous recent
studies have
analysed the hyporeactivity phenomenon using whole blood
cultures, it is
possible that endotoxin-neutralising molecules have interfered
in these
studies. Indeed, Adrie et al. have shown that the hyporeactivity
to LPS was
both an intrinsic property of circulating monocytes, as well as
the reflectionof a specific neutralising activity within the plasma
of SIRS patients (personal
communication). It has been reported that plasma of septic
patients
contains large amounts of LPS binding protein (LBP), which can
either
inhibit the LPS molecules,45 or transfer LPS to lipoproteins,46
known for
their inhibitory activity towards LPS.47 Furthermore, sera from
septic
patients contain amounts of soluble CD14, which also favours the
shuttle of
LPS towards lipoproteins.48
Toll-like receptors
Toll-like receptors (TLR) are a family of receptors that
recognise
components of bacteria, virus, parasites, and fungi, and induce
a pro-
inflammatory response by several cell types. So far, 10 human
TLRs
differing in their specificity for microbial components have
been cloned,
which respond to various components, including LPS from
Gram-negative
bacteria, lipopeptides of Gram-positive cell walls, bacterial
DNA, and
flagella. TLR4 was identified as the receptor for LPS and
requires the
presence of an extracellular accessory protein called MD-2.
CD14
physically associates with LPS complexed with LBP and transfers
the
endotoxin to the TLR4 and MD-2 dimer; each component of this
complex
is required for efficient LPS-induced signalling.
Many parameters of immunoparalysis observed in SIRS patients
are
reminiscent of the endotoxin tolerance phenomenon, which
characterises the
refractoriness of cells or the inability of whole animals to
respond to a second
endotoxin challenge shortly after a first encounter.49 Because
recent studies
reported a downregulation of surface expression of TLR4 in
endotoxin-
tolerant macrophages,50,51 it was of interest to investigate the
expression ofthis molecule on the surface of monocytes from SIRS
patients. A decreased
expression of TLR4, but not TLR2, on CD14 positive cells was
found in
11 trauma patients compared with 6 healthy subjects (Adib-Conquy
et al.,
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
24/119
11
personal communication). However, this lower expression of TLR4
is not
sufficient to explain the decreased capacity of the cells to
respond to stimuli.
Indeed, while LPS-induced TNF is decreased, this was not the
case of LPS-
induced IL-1ra and IL-10. This latter observation suggests that
the defect
may occur at the different signalling pathways within the cell
rather than atthe initiation of the signalling cascade on the cell
surface.
Nuclear factor kappa B
Transcription factors are DNA-binding proteins which regulate
gene
expression. Nuclear factor kappa B (NFB) is one such
transcription factor
which is critical for maximal expression of many cytokines
involved in the
pathogenesis of inflammation. Activation and regulation of
NF
B is tightlycontrolled by a group of inhibitory proteins (IB),
which maintain NFB in
an inhibited state in the cytoplasm of effector cells.The
sequence of events
leading to NFB activation involves phosphorylation,
ubiquitination, and
proteolysis of IB, allowing exposure of a nuclear recognition
site. NFB
then migrates to the nucleus, binds to specific promoter sites,
and activates
transcription of target genes (for example,TNF, IL-1, IL-6,
IL-8). NFB,
part of the Rel/NF-B family of transcription factors, is
involved in the
regulation of immune and acute-phase responses at the
transcriptional level.
Rel proteins can be divided into two groups based on their
structures,
functions, and modes of synthesis. The first group of Rel
proteins consists
of p65 (also known as RelA), c-Rel, and RelB, each of which
contains one
or more transcriptional-activation domain necessary for gene
induction.The
second group consists of p105 and p100, which, upon
proteolytic
processing, give rise to p50 and p52, respectively. Members of
both groups
of Rel proteins can form homo- or heterodimers. Studies have
shown that
the transactivator form of NFB is the p65 unit, whereas the p50
unit has
shown no or minimal activation capacity.
To investigate the role of NFB in the mechanism of endotoxin
tolerance
in macrophages, Blackwell and co-workers52 used a rat alveolar
macrophage
cell line made endotoxin tolerant by exposure to low
concentrations of
LPS for 48 hours. This treatment induced a state of tolerance
such that
subsequent exposure to high-dose LPS resulted in decreased
production
of cytokines compared with LPS-sensitive cells. This decreased
cytokine
production was associated with impaired activation of NFB with
depletion
of both RelA and p50. This study suggested endotoxin tolerance
might be
mediated by depletion of RelA/p50, which could limit the amount
of
NFB available for activation and inhibit transcription of
NFB-dependent
genes. On the other hand, Ziegler-Heitbrock and colleagues
demonstratedthat endotoxin tolerance of monocytes was associated
with an increase of
the inactive p50 homodimer and a decrease of the p50/p65
active
heterodimer.53
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
25/119
12
Accordingly, Adib-Conquy et al. studied NFB expression and
dimer
characteristics in mononuclear cells of patients with sepsis and
major
trauma and healthy controls.54,55 The expression of p50/p65
heterodimer
was significantly reduced in all patients as compared with
controls. The
p50/p50 homodimer was reduced in the survivors of sepsis.
Subsequentin vitro stimulation of mononuclear cells with LPS did
not induce further
NFB nuclear translocation: the survivors of sepsis showed low
expression
of both p50/p65 and p50/p50, while non-survivors of sepsis
showed a
predominance of the inactive homodimer and a low
p50/p65:p50/p50
ratio when compared with controls. In the latter group of
patients there
was a negative correlation between plasma IL-10 levels and
the
p50/p65:p50/p50 ratio after in vitro LPS stimulation (r 0.8,
P 0.04). The reduced expression of nuclear NFB was not due to
its
inhibition by IB since very low expression of IB as well as low
levels ofp65 and p50, were found in the cytoplasm of mononuclear
cells from
sepsis patients when compared with controls. These results
demonstrate
that upon LPS activation, mononuclear cells of systemic
inflammatory
response syndrome patients show patterns of NFB expression
that
resemble those reported during LPS-tolerance: global
downregulation of
NFB in survivors of sepsis and presence of large amounts of the
inactive
homodimer in the non-survivors of sepsis.54
In trauma patients, after 1, 3, 5, and 10 days following
admission of
patients in the intensive care units, expression of both p50/p65
heterodimersand p50/p50 homodimers was significantly reduced
compared with
controls. After LPS stimulation in vitro, the p50/p65:p50/p50
ratio was
significantly lower in cells from trauma patients than from
healthy controls
and the ex vivo expression of IB was higher. Although no
direct
correlation was found between levels of IL-10 or TGF and NFB,
these
immunosuppressive cytokines were significantly elevated in the
trauma
patients by 10 days after admission. This long-term low basal
and LPS-
induced activation of NFB might be linked to
immunoparalysis.55
Signalling pathways
There are still very few studies in humans addressing whether
some
alterations of the signalling pathways might explain part of
the
immunodepression seen in circulating cells in SIRS patients.
Most
interestingly, Learn et al.56 reported that in septic patients
the repressed
production of IL-1 and the selective elevation of the secreted
form of
IL-1ra in response to LPS, was linked to a probable alteration
in the
interleukin-1 receptor-associated kinase (IRAK) signalling
pathway anda maintained efficient phosphatidylinositol
3-kinase-dependent signalling
pathway. In murine model of sepsis, it was reported that
inhibition of p59fyn
phosphorylation and kinase activity was associated with T
lymphocyte
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
26/119
13
IL-2 production and proliferation,57 whilst activation of MAPK
p38 was
associated with T cell immune dysfunction.58
Cells derived from inflammatory foci
The hyporesponsiveness of peripherally derived cells in terms of
the capacity
of the cells to produce cytokines is not a generalised
phenomenon, and cells
derived from inflammatory foci are, in contrast, activated. In a
baboon model
of inflammation, the capacity of alveolar macrophages after
unilateral lung
irradiation was studied.2 Over a 1 month period, bronchoalveolar
lavage
was undertaken in five baboons, macrophages were recovered
and
production of TNF was measured.This study showed a significant
increase
of spontaneous, LPS-, staphylococci- and streptococci-induced
TNF
release in macrophages from the inflamed lung compared with the
initialvalues. Macrophages from lungs of patients with acute
respiratory distress
syndrome (ARDS) also clearly demonstrated no deactivation of the
cells.
Schwartz et al.59 investigated activation of the transcription
factors NFB,
nuclear factor-IL-6 (NF-IL-6), cyclic adenosine monophosphate
(cAMP)-
responsive element binding protein, serum protein-1 (SP-1), and
activating
protein-1 (AP-1) in alveolar macrophages from six patients with
ARDS and
from six control patients without lung injury. Activation of NFB
in alveolar
macrophages observed in patients with ARDS had increased
compared with
control patients, but there was no increase in the activation of
the othertranscription factors. Moine and colleagues60 subsequently
showed
decreased cytoplasmic levels of p50, p65 and c-Rel in alveolar
macrophages
from patients with ARDS, consistent with enhanced migration of
liberated
NFB dimers from the cytoplasm to the nucleus.
When leukocytes are derived from the peritoneal cavity or the
gut
of patients suffering peritonitis,61 inflammatory bowel
diseases,62 or
endometriosis,63,64 LPS-induced cytokine production by
peritoneal
macrophages or mononuclear cells from the lamina propria was
enhanced
as compared with healthy controls. Following injection of
endotoxin, theproduction of IFN by intra-epithelial lymphocytes was
enhanced upon
stimulation as compared with control animals.65 A similar
enhanced
activity of intra-epithelial T lymphocytes after endotoxaemia
was observed
when cellular cytotoxicity and proliferation were monitored.
Altogether,
these examples illustrate that local inflammation is associated
with an
enhanced activity of resident and/or infiltrating leukocytes,
whilst systemic
inflammation is associated with a reduced activity of
circulating leukocytes.
Conclusion
Sepsis and non-infectious SIRS are paradoxically associated with
an
exacerbated production of cytokines, as assessed by their
presence in
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
27/119
14
biological fluids, and a diminished ability of circulating cells
to produce
cytokine upon in vitro activation.This might represent a
protective response
against an overwhelming dysregulation of the pro-inflammatory
process, but
on the other hand it may induce a state of immune paralysis
(endogenous
immunosuppression) leading to an increased risk of
subsequentnosocomial infections.66 However, cellular hyporeactivity
is not a global
phenomenon and some signalling pathways are unaltered and allow
the cells
to respond normally to certain stimuli. Furthermore, during
sepsis and
SIRS, cells derived from tissues or inflammatory foci are either
fully
responsive to ex vivo stimuli or even primed, in contrast to
cells derived from
haematopoietic compartments (blood), which are hyporeactive. In
addition
to cytokine production, NFB activity within leukocytes reflects
cellular
hyporeactivity. Thus the immunoparalysis reported in sepsis and
SIRS
patients, often revealed by a diminished capacity of leukocytes
to respondto LPS, is not a generalised phenomenon, and SIRS is
associated with a
compartmentalised responsiveness involving either anergic or
primed cells.
References
1 Bone RC, Grodzin CJ, Balk RA. Sepsis: a new hypothesis for
pathogenesis ofthe disease process. Chest1997;112:23543.
2 Cavaillon J-M, Adib-Conquy M, Cloz-Tayarani I, Fitting C.
Immuno-
depression in sepsis and SIRS assessed by ex vivo cytokine
production is nota generalized phenomenon: a review.J Endotoxin Res
2001;7:8593.
3 Polk HC Jr, George CD,Wellhausen SRet al. A systematic study
of host defense
processes in badly injured patients.Ann Surg1986;204:28299.4
Livingston DH, Appel SH,Wellhausen SR, Sonnenfeld G, Polk HC.
Depressed
interferon gamma production and monocyte HLA DR expression after
severeinjury.Arch Surg1988;123:130912.
5 Hershman MJ, Cheadle WG, Wellhausen SR, Davidson PF, Polk HC
Jr.Monocyte HLA-DR antigen expression characterizes clinical
outcome in thetrauma patient. Br J Surg1990;77:2047.
6 Cheadle WG, Hershman MJ, Wellhausen SR, Polk HC Jr. HLA-DR
antigen
expression on peripheral blood monocytes correlates with
surgical infection.Am J Surg1991;161:63945.
7 Van den Berk JMM, Oldenburger RHJ, van den Berg AP et al. Low
HLA-DRexpression on monocytes as a prognostic marker for bacterial
sepsis after livertransplantation. Transplantation
1997;63:18468.
8 Salo M, Merikanto J, Eskola J, Nieminen S, Aho AJ. Impaired
lymphocytetransformation after accidental trauma.Acta Chir
Scand1970;145:36772.
9 Keane RM, Birmingham W, Shatney CM, Winchurch RA, Munster
AM.Prediction of sepsis in the multitraumatic patients by assays of
lymphocyte
responsiveness. Surg Gynecol Obst1983;156:1637.10 Levy EM,
Alharbi SA, Grindlinger G, Black PH. Changes in mitogen
responsiveness lymphocyte subsets after traumatic injury:
relation todevelopment of sepsis. Clin Immunol
Immunopathol1984;32:22433.
11 Blazar BA, Rodrick ML, OMahony JB et al. Suppresion of
natural killer-cellfunction in humans following thermal and
traumatic injury. J Clin Immunol1986;6:2636.
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
28/119
15
12 Maturana P, Puente J, Miranda D, Sepulveda C, Wolf ME,
Mosnaim AD.Natural killer cell activity in patients with septic
shock.J Crit Care 1991;6:425.
13 Puente J, Carvajal T, Parra S et al. In vitro studies of
natural killer cell activity inseptic shock patients. Response to a
challenge with alpha-interferon andinterleukin-2. Int J Clin
Pharmacol Ther Toxicol1993;31:2715.
14 Jimenez MF,Watson WG, Parodo J et al. Dysregulated expression
of neutrophilapoptosis in the systemic inflammatory response
syndrome. Arch Surg1997;132:126370.
15 van Dijk WC, Verbrugh HA, van der Tol ME et al. Interactions
of phagocyticand bacterial cells in patients with bacteremia caused
by Gram-negative rods.
J Infect Dis 1980;141:4419.
16 Benjamin CF, Ferreira SH, Cunha FDQ. Role of nitric oxide in
the failure ofneutrophil migration in sepsis.J Infect Dis
2000;182:21423.
17 Cummings CJ, Martin TR, Frevert CW et al. Expression and
function of thechemokine receptor CXCR1 and CXCR2 in sepsis. J
Immunol 1999;162:23416.
18 Marie C, Fitting C, Cheval C et al. High levels of
leukocyte-associatedinterleukin-8 upon cell-activation and in
patients with sepsis syndrome. InfectImmun 1997;65:86571.
19 Christou NV. Host-defence mechanism in surgical patients: a
correlative studyof the delayed hypersensitivity skin-test
response, granulocyte function andsepsis. Can J
Surg1985;28:3946.
20 Christou NV, Meakins JL, MacLean LD. The predictive role of
delayedhypersensitivity in preoperative patients. Surg Gynecol
Obstet1981;152:297301.
21 Cavaillon J-M. Possibilities and problems of cytokine
measurements. In RedlH, Schlag G, eds. Cytokines in Severe Sepsis
and Septic Shock, Prog. Inflam. Res.,Basel: Birkhuser Publishing
Ltd. 1998, 95119.
22 Wood JJ, Rodrick ML, OMahony JB et al. Inadequate interleukin
2 production.A fundamental immunological deficiency in patients
with major burns. AnnSurg1984;200:31120.
23 Cabie A, Fitting C, Farkas JC et al. Influence of surgery on
in-vitro cytokineproduction by human monocytes. Cytokine
1992;4:57680.
24 Cavaillon J-M. Pro- versus anti-inflammatory cytokines: myth
or reality. Cell MolBiol2001;47:695702.
25 Munoz C, Carlet J, Fitting C, Misset B, Bleriot JP, Cavaillon
J-M. Dysregulationof in vitro cytokine production by monocytes
during sepsis. J Clin Invest1991;88:174754.
26 Ertel W, Keel M, Neidhardt Ret al. Inhibition of the defense
system stimulating
interleukin-12 interferon-gamma pathway during critical Illness.
Blood1997;89:161220.
27 OSullivan ST, Lederer, JA, Horgan AF, Chin DHL, Mannick JA,
Rodrick ML.Major injury leads to predominance of the T helper-2
lymphocyte phenotypeand diminished interleukin-12 production
associated with decreased resistanceto infection.Ann
Surg1995;222:48292.
28 Mack VE, McCarter MD, Naana HA, Calvano SE, Daly J-M.
Dominance of
T helper 2 type cytokine after severe injury.Arch
Surg1996;131:13039.29 Puyana JC, Pellegrini JD, De AK, Kodys K,
Silva WE, Miller CL. Both
T-helper-1- and T-helper-2-type lymphokines are depressed in
posttraumaanergy.J Trauma 1998;44:103745.
30 Muret J, Marie C, Fitting C, Payen D, Cavaillon J-M. Ex vivo
T-lymphocytederived cytokine production in SIRS patients is
influenced by experimentalprocedures. Shock 2000;13:16974.
31 McCall CE, Grosso-Wilmoth LM, LaRue K, Guzman RN, Cousart
SL.Tolerance to endotoxin-induced expression of the interleukin-1
beta gene in
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
29/119
16
blood neutrophils of humans with the sepsis syndrome. J Clin
Invest1993;91:85361.
32 Marie C, Muret J, Fitting C, Losser MR, Payen D, Cavaillon
J-M. Reducedex vivo interleukin-8 production by neutrophils in
septic and nonseptic systemicinflammatory response syndrome.
Blood1998;91:343946.
33 Van Deuren M,Van Der Ven-Jongekrijg H, Demacker PNM et al.
Differentialexpression of proinflammatory cytokines and their
inhibitors during the courseof meningococcal infections.J Infect
Dis 1994;169:15761.
34 Marie C, Muret J, Fitting C, Payen D, Cavaillon J-M.
Interleukin-1 receptorantagonist production during infectious and
non-infectious systemicinflammatory response syndrome. Crit Care
Med2000;28:227783.
35 Brandtzaeg P, Osnes L, vsteb R, Jo GB, Westwik AB, Kierulf P.
Netinflammatory capacity of human septic shock plasma evaluated by
a monocyte-based target cell assay: identification of
interleukin-10 as a major functionaldeactivator of human
monocytes.J Exp Med1996;184:5160.
36 Ayala A, Meldrum DR, Perrin MM, Chaudry IH.The release of
transforming
growth factor-beta following haemorrhage: its role as a mediator
of hostimmunosuppression. Immunology 1993;79:47984.
37 Ayala A, Knotts JB, Ertel W et al. Role of interleukin 6 and
transforming growthfactor-beta in the induction of depressed
splenocyte responses following sepsis.
Arch Surg1993;128:8994.38 Jones S, Romano F. Dose- and
time-dependent changes in plasma catecholamines
in response to endotoxin in conscious rats. Circ Shock
1989;28:5968.39 Severn A, Rapson NT, Hunter CA, Liew FY. Regulation
of tumor necrosis
factor production by adrenaline and by -adrenergic agonists. J
Immunol1992;148:34415.
40 van der Poll T, Coyle SM, Barbosa K, Braxton CC, Lowry SF.
Epinephrine
inhibits tumor necrosis factor-alpha and potentiates
interleukin-10 productionduring human endotoxemia.J Clin
Invest1996;97:71319.
41 Luger TA, Kalden DH, Scholzen TE, Brzoska T.
-melanocyte-stimulatinghormone as a mediator of tolerance
induction. Pathobiology 1999;67:31821.
42 Delgado M, Pozo D, Martinez C et al.Vasoactive intestinal
peptide and pituitaryadenylate cyclase-activating polypeptide
inhibit endotoxin-induced TNFproduction by macrophages: in vitro
and in vivo studies. J Immunol1999;162:235867.
43 Chrousos GP. The hypothalamicpituitaryadrenal axis and
immune-mediatedinflammation.N Engl J Med1995;332:135162.
44 Choudhry MA, Ahmad S, Ahmed Z, Sayeed MM. Prostaglandin E2
down-
regulation of T cell IL-2 production is independent of IL-10
during Gramnegative sepsis. Immunol Lett1999;67:12530.
45 Zweigner J, Gramm HJ, Singer OC, Wegscheider K, Schumann RR.
Highconcentration of lipopolysaccharide-binding protein in serum of
patients withsevere sepsis or septic shock inhibit the
lipopolysaccharide response in humanmonocytes.
Blood2001;98:38008.
46 Vreugdenhil ACE, Snoeck AMP, vant Veer C, Greve JWM, Buurman
WA.LPS-binding protein circulates in association with
apoB-containing lipoproteinsand enhances endotoxin-LDL/VLDL
interaction. J Clin Invest 2001;107:22534.
47 Cavaillon J-M, Fitting C, Haeffner-Cavaillon N, Kirsch J,
Warren HS.
Cytokine response by monocytes/macrophages to free and
lipoprotein-bound lipopolysaccharide. Infect Immun
1990;58:237582.
48 Kitchens RL,Thompson PA,Viriyakosol S, OKeefe GE, Munford RS.
PlasmaCD14 decreases monocyte responses to LPS by transferring
cell-bound LPS toplasma lipoproteins.J Clin
Invest2001;108:48593.
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
30/119
17
49 Cavaillon J-M.The non specific nature of endotoxin tolerance.
Trends Microbiol1995;3:3204.
50 Nomura F, Akashi S, Sakao Y et al. Endotoxin tolerance in
mouse peritonealmacrophages correlates with down-regulation of
surface Toll-like receptor 4expression.J Immunol2000;164:34769.
51 Medvedev AE, Kopydlowski KM, Vogel SN. Inhibition of
lipopolysaccharide-induced signal transduction in
endotoxin-tolerized mouse macrophages:dysregulation of cytokine,
chemokine, and Toll-like receptor 2 and 4 geneexpression.J
Immunol2000;164:556474.
52 Blackwell TS, Blackwell TR, Christman JW. Induction of
endotoxin tolerancedepletes nuclear factor-kappaB and suppresses
its activation in rat alveolar
macrophages.J Leukocyte Biol1997;62:88591.53 Ziegler-Heitbrock
L, Wedel A, Schraut W et al. Tolerance to lipopolysaccharide
involves mobilization of nuclear factorB with predominance of
p50homodimers.J Biol Chem 1994;269:170014.
54 Adib-Conquy M, Adrie C, Moine P et al. Nuclear factorB
expression in
mononuclear cells of septic patients resembles that observed in
LPS-tolerance.Am J Respir Crit Care Med2000;162:187783.
55 Adib-Conquy M, Asehnoune K, Moine P, Cavaillon J-M. Long term
impaired
expression of nuclear factorB and IB in peripheral blood
mononuclearcells of patients with major trauma.J Leukocyte
Biol2001;70:308.
56 Learn CA, Boger MS, Li L, McCall CE. The phosphatidylinositol
3 kinasepathway selectively controls sIL-1ra not interleukin-1
production in the septicleukocytes.J Biol Chem 2001;276:202349.
57 Choudhry MA, Uddin S, Sayeed MM. Prostaglandin E2 modulation
of p59fyn
tyrosine kinase in T lymphocytes during sepsis.J
Immunol1998;160:92935.58 Song GY, Chung CS, Chaudry IH, Ayala A.
MAPK p38 antagonism as a novel
method of inhibiting lymphoid immune suppression in
polymicrobial sepsis.Am J Physiol Cell Physiol2001;281:C6629.
59 Schwartz MD, Moore EE, Moore FA et al. Nuclear factor kappa B
is activatedin alveolar macrophages from patients with acute
respiratory distress syndrome.Crit Care Med1996;24:128592.
60 Moine P, McIntyre R, Schwartz MD et al. NF-kappaB regulatory
mechanismsin alveolar macrophages from patients with acute
respiratory distress syndrome.
Shock 2000;13:8591.61 Fieren MWJ, Van Den Bemd GJ, Bonta IL.
Endotoxin-stimulated peritoneal
macrophages obtained from continuous ambulatory peritoneal
dialysis patients
show an increased capacity to release interleukin-1 in vitro
during infectious
peritonitis. Eur J Clin Invest1990;B4537.62 Rugtveit J, Nilsen
EM, Bakka A, Carlsen H, Brandtzaeg P, Scott H. Cytokine
profiles differ in newly recruited and resident subsets of
mucosal macrophagesfrom inflammatory bowel disease.
Gastroenterol1997;112:1493505.
63 Rana N, Braun DP, House R, Gebel H, Rotman C, Dmowski WP.
Basal andstimulated secretion of cytokines by peritoneal
macrophages in women withendometriosis. Fertil
Steril1996;65:92530.
64 Wu MY, Ho HN, Chen SU, Chao KH, Chen CD, Yang YS. Increase in
theproduction of IL-6, IL-10 and IL-12 by LPS stimulated peritoneal
macrophagesfrom women with endometriosis.Am J Reprod
Immunol1999;41:10611.
65 Nssler NC, Stange B, Nussler AK et al. Upregulation of
intraepithelial
lymphocyte function in the small intestinal mucosa in sepsis.
Shock2001;16:4548.
66 Munford RS, Pugin J. Normal responses to injury prevent
systemicinflammation and can be immunosuppressive. Am J Respir Crit
Care Med2001;163:31621.
IMMUNOPARALYSIS
-
7/30/2019 Galley - Inflammation and Immunity
31/119
2: Apoptosis and the
inflammatory processNIGEL R WEBSTER
Introduction
Cells that are damaged by injury, such as by mechanical damage
or
exposure to toxic chemicals, undergo swelling, from disruption
of the
ability of the plasma membrane to control the passage of ions
and water,
with consequent leakage of cell contents, leading to
inflammation of
surrounding tissues.This process is called necrosis. Cells which
are induced
to commit suicide, in contrast, shrink, and the mitochondrial
membrane
becomes breached, such that release of cytochrome c occurs.
Chromatin
(DNA and protein) in the nucleus becomes degraded into
small,membrane-wrapped fragments, and the phospholipid
phosphatidylserine,
which is normally hidden within the plasma membrane, is exposed
on the
surface. This is then bound by receptors on phagocytic cells
such as
macrophages, which engulf the cell fragments, leading to a quiet
orderly
removal of dead cells. This pattern of events is called
programmed cell
death or apoptosis.The cellular machinery of programmed cell
death is as
intrinsic to the cell as, for example, mitosis. This article
will describe the
regulation and process of apoptosis and its relevance to
disease, including
the inflammatory response in patients with sepsis.
Identification of apoptosis
A series of careful observational studies in the 1950s and
1960s
demonstrated the importance of physiological cell death in
development. By
the 1970s, a process of cell death, characterised by a rigid set
of structural
changes, was also observed in a wide variety of physiological
circumstances:
negative selection in the immune system, cytotoxic T cell
killing, atrophy
induced by hormones and other stimuli, the growth and regression
oftumours, and tissue development after exposure to teratogens.
These distinctive structural changes characterising cell death
were
identical to those found in cell death during normal development
and
18
-
7/30/2019 Galley - Inflammation and Immunity
32/119
19
raised the possibility that a programmed death pathway, similar
to that in
development, might also occur in adult tissues in response to a
variety of
stimuli. This type of death was called apoptosis a term derived
from the
Greek word meaning the dropping of leaves from the trees. The
word
apoptosis is often mispronounced it derives from apo- and
-ptosis andtherefore the second p is silent. This term is applied
to a group of
characteristic structural and molecular events which separate
this type of
cell deletion from necrosis (Box 2.1). In contrast to necrosis,
which involves
a group of cells simultaneously, apoptosis may occur in a single
cell
surrounded by a group of viable cells. Apoptosis is a selective
process for
deletion of cells in various biological systems and, in a
similar manner to
proliferation, is tightly regulated, with both processes playing
essential roles
in the homeostasis of renewable tissues.13
APOPTOSIS AND THE INFLAMMATORY PROCESS
Box 2.1 Key facts about apoptosis
Normal process modelling in vertebrate development cell loss
accompanying atrophy in adult tissues deletion of B and T
lymphocytes occurs widely in tumours
Characteristic morphological changes
Characteristic biochemical changes
The process of apoptosis
Structurally, the dying cell loses contact with its neighbours,
undergoes a
dramatic process of bubbling, blebbing, and shrinkage, and
disintegrates
into a cluster of membrane-bound fragments. Inside, there are
compacted
organelles and prominent and characteristic chromatin
condensation.
Apoptotic cells in tissues are rapidly recognised and
phagocytosed by their
neighbours, or by specialised phagocytes, in whose phagosomes
they are
safely destroyed within a few hours.Tissues can shrink to half
their original
cell number in a day or two, with little disturbance in
structure, no
inflammatory process, and few accumulating dead cells.
Apoptosis versus necrosis
All of this is very different from the changes in cells exposed
to
severe toxicological injury or major degrees of hypoxia, where
damage to
-
7/30/2019 Galley - Inflammation and Immunity
33/119
20
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Box 2.2 Morphological features of apoptosis versus necrosis
Necrosis
Loss of membrane integrity
Swelling of cytoplasm and mitochondria
Ends with total cell lysis
No vesicle formation, complete lysis
Disintegration of organelles
Apoptosis
Mitochondria becomes leaky
Membrane blebbing, no loss of integrity
Aggregation of chromatin at the nuclear membrane
Shrinking of cytoplasm and condensation of nucleus
Ends with fragmentation of cell into smaller bodies
Formation of membrane bound vesicles (apoptotic bodies)
Box 2.3 Biochemical features of apoptosis versus necrosis
Necrosis
Loss of regulation of ion homeostasis
No energy requirement
Random digestion of DNA
Postlytic DNA fragmentation (late event of death)
Apoptosis Tightly regulated process
Energy (ATP)-dependent
Non-random fragmentation of DNA (ladder pattern)
Pre-lytic DNA fragmentation
Release of cytochrome c into cytoplasm by mitochondria
Activation of caspase cascade
Translocation of membrane phosphatidyl-serine
-
7/30/2019 Galley - Inflammation and Immunity
34/119
21
energy-dependent membrane ion pumps leads to progressive
cellular
swelling and rupture necrosis. When this occurs there is usually
an acute
inflammatory reaction, apparently stimulated by neutrophil
chemotactic
factors originating from intracellular proteins lost from the
necroticcells. The characteristic morphological and biochemical
features and
physiological significance of necrosis versus apoptosis are
given in Boxes 2.2,
2.3, and 2.4. Figure 2.1 shows a normal eosinophil and one
undergoing
apoptosis.
APOPTOSIS AND THE INFLAMMATORY PROCESS
Box 2.4 Physiological significance of apoptosis
versus necrosis
Necrosis
Affects groups of contiguous cells
Evoked by non-physiological disturbances
Phagocytosis by macrophages
Significant inflammatory response
Apoptosis
Affects individual cells
Induced by physiological stimuli (lack of growth factors,
hormonal environment) Phagocytosis by adjacent cells or
macrophages
No inflammatory response
A B
Figure 2.1 A transmission electron photomicrograph of (A) a
normal eosinophil and (B) an
eosinophil undergoing apoptosis showing aggregation of
chromatin, blebbing, and shedding of
intracytoplasmic granules.
-
7/30/2019 Galley - Inflammation and Immunity
35/119
22
Why do we need apoptosis?
There are two reasons why apoptosis is physiologically vital.The
first is the
role it plays in fetal development and other key processes. This
is most
eloquently seen in the change from a tadpole to a frog. The
resorption ofthe tadpole tail at the time of its metamorphosis into
a frog occurs by
apoptosis. In man the formation of the fingers and toes of the
fetus requires
the removal, by apoptosis, of the tissue between them. The
formation of
synapses between neurones requires that surplus cells be
eliminated by
apoptosis, and the sloughing off of the endometrium at the start
of
menstruation also occurs by apoptosis.
The second reason for apoptosis is the need to destroy cells
that
represent a threat to the integrity of the organism. This might
include, for
example, cells infected with viruses one of the methods by
whichcytotoxic T (Tc) lymphocytes kill virus-infected cells is by
inducing
apoptosis and some viruses are able to mount countermeasures
(see Chapter 3 in this volume). Apoptosis is also important in
cells with
DNA damage where disruption of proper embryonic development
leading
to birth defects can occur, or the cell can become cancerous.
Cells respond
to DNA damage by increasing their production of p53 a potent
inducer
of apoptosis. Mutations in the p53 gene an oncogene producing
a
defective protein, are often found in cancer cells, and
radiation and
chemotherapeutic agents used in cancer therapy induce apoptosis
in sometypes of cancer cells. Mice with both copies of p53 deleted
develop multiple
malignancies, and p53 mutation is associated with many human
cancers.
Following DNA damage, for example, by radiation, p53 levels
rise, and
proliferating cells arrest in the G1 phase of mitosis. This
allows time for
DNA repair prior to the next round of replication. This arrest
is mediated
by stimulation of expression of p21CIP1, a cyclin kinase
inhibitor.
Why can apoptosis be a problem?
Although the process of apoptosis is physiologically essential
for both
development and removal of dangerous cells, initiation of the
sequence
of events leading to cell death through apoptosis can lead to
both unwanted
removal of healthy cells, and propagation of inflammatory
responses
through release of cytokines (see description of the actions of
caspase
enzymes below).
Caenorhabditis elegans and the genetics of apoptosis
C. elegans is a hermaphrodite nematode worm with a life cycle
from egg to
sexual maturity of about 3 days. The genome of this organism has
been
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
-
7/30/2019 Galley - Inflammation and Immunity
36/119
23
fully sequenced and contains 19 099 genes. The adult
hermaphrodite
consists of exactly 959 somatic cells of very precisely
determined lineage
and function. Development control occurs through apoptotic
removal of
exactly 131 cells, and thus C. elegans is an ideal organism to
study the
genetics of apoptosis. It has been found that three key genes
triggerapoptosis: ced-3 and ced-4 (C.elegans cell death genes) and
egl-1 (C.elegans
egg laying defective gene) (Figure 2.2).
Ced-3 has a mammalian counterpart, originally known as
interleukin 1
converting enzyme or ICE, but now termed caspase 1 (Cys
catalytic Asp
targeting protease). Thirteen caspases are known in mammalian
systems
and have conserved sequence and subunit structure; of these four
play key
effector roles in apoptosis and four are initiators in the
activation process.4
Ced-4 acts as an adapter for caspase activation in C. elegans;
the
mammalian counterpart is called apoptosis activating factor
(Apaf-1).A fourth gene in C. elegans promotes survival, that is, it
acts as a negative
regulator of apoptosis, ced-9. The mammalian equivalent is the
BCL-2
family of genes. Bcl-2 and ced-9 proteins are 23% identical, and
bcl-2 can
substitute for ced-9 in C. elegans. However, in higher animals,
bcl-2 is a
member of a large family of closely related proteins, some of
which promote
survival and some death (Box 2.5). The similarities between
ced-3 and
ICE, ced-4 and Apaf-1, and between ced-9 and bcl-2 strongly
suggest that
programmed cell death in C. elegans parallels apoptosis in
higher animals,
but in a much more simplified form. Figure 2.2 shows the C.
elegans
apoptosis genes and their human equivalents.5
APOPTOSIS AND THE INFLAMMATORY PROCESS
Pro-apoptotic
ced-3
ced-4Anti-apoptotic
ced-9
caspase-1(ICE)
Apaf-1
BCL-2 gene family
Figure 2.2 A transmission electron micrograph of the nematode
worm Caenorhabditis elegans.
Its apoptosis genes ( left) with the mammalian equivalents
(right) are indicated.
Signals for apoptosis
The cascade of events leading to apoptosis takes place as a
result of either
the withdrawal of positive signals (that is, signals needed for
continuedsurvival), or the initiation of negative signals (that is,
those which instigate
cell death). Signals can arise within the cell or from so-called
death
activators binding to receptors at the cell surface.6
-
7/30/2019 Galley - Inflammation and Immunity
37/119
24
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Box 2.5 The bcl-2 protein family
Pro-apoptotic
Bad
Bak
Bax
Bcl-Xs
Bid
Bik
Anti-apoptotic
AL
Bcl-2
Bcl-W
Bcl-XL
Mcl-1
Withdrawal of positive signals
The continued survival of most cells requires that they receive
continuous
stimulation from other cells and, for many, continued adhesion
to the
surface on which they are growing. Some examples of positive
signals
include specific growth factors for neurones, and interleukin-2
(IL-2), an
essential factor for the mitosis of lymphocytes.
Receipt of negative signals
Internal signals
In a healthy cell, the outer membranes of mitochondria express
the protein
bcl-2 on their surface. The role of the mitochondrion in
apoptosis is
discussed further below. Bcl-2 is bound to a molecule of the
protein
Apaf-1, and internal damage in the cell causes bcl-2 to release
Apaf-1.This
results in leakage of cytochrome c from mitochondria into the
cytoplasm.
The released cytochrome c and Apaf-1 bind to molecules of
caspase 9.
The resulting complex of cytochrome c, Apaf-1 and caspase 9
(with ATP)
is called an apoptosome and these aggregate in the cytosol.
Caspase 9activates other caspases, which leads to digestion of
structural proteins in
the cytoplasm, degradation of chromosomal DNA, and
ultimately
phagocytosis of the cell (see caspases below).
-
7/30/2019 Galley - Inflammation and Immunity
38/119
25
External signals
External signals which initiate apoptosis include increased
levels of oxidants
within the cell or damage to DNA by these oxidants or other
agents, such as
ultraviolet light, x rays, and chemotherapeutic drugs. In
addition there are
several molecules that bind to specific receptors on the cell
surface and signalthe start of apoptosis. Signalling pathways link
key receptors to the caspase
proteolytic cascade.These death activators include tumour
necrosis factor
(TNF) which binds to the TNF receptor; lymphotoxin (also known
as
TNF) which also binds to the TNF receptor; and Fas ligand
(FasL), a
molecule that binds to the Fas cell-surface receptor (also
called CD95).
Fas expression and immune function
Fas is a transmembrane receptor protein which is very widely
distributed,
and is constitutively expressed in some cells for example,
liver, or induced
in cells such as lymphocytes on activation. The activating
ligand, Fas-L,
is expressed in a narrower range of cells, including
antigen-activated
T lymphocytes, testis, eye, and central nervous system.
Persistent and strong
stimulation of CD4T helper lymphocytes results in expression of
Fas-L.
During ablation of the immune repertoire in the fetal/neonatal
period, self-
antigen stimulation causes killing of self-reactive B
lymphocytes and self or
mutual killing of the Fas-L expressing T lymphocytes. The
development of
tolerance against a potential antibody represents a similar
process. Sometumours also express Fas-L constitutively for example,
melanoma and
lung tumours. This renders them resistant to immune intervention
any
visiting lymphocytes are induced to commit suicide through
apoptosis.
Expression of Fas-L in testis, eye, and central nervous system
gives rise to
the phenomenon of immune privilege, in which these tissues do
not reject
allografts, but kill invading lymphocytes instead.
Mechanism of Fas-L and TNF-induced apoptosis
When Fas binds Fas-L, changes occur in the cell membrane; its
cytoplasmic
domain contains a sequence called the death domain (DD), a
sequence
critically required for stimulated apoptosis.The changes in the
cell membrane
result in incorporation of an intracellular DD-containing
protein called
Fas-associated death domain (FADD) protein (synonymous with a
protein
previously named MORT1). The N-terminal region of FADD
contains
another domain referred to as death effector domain or DED.This
associates
with another DED at the N-terminus of pro-caspase-8 (the
pro-caspase
formerly known as pro-FLICE or MACH1, or Mort-associated
ced-3homologue). Recruitment into the complex results in
dimerisation of pro-
caspase-8, releasing the active caspase-8. Caspase-8 then
initiates the whole
effector protease cascade by acting on pro-caspase-3 to liberate
caspase 3.
APOPTOSIS AND THE INFLAMMATORY PROCESS
-
7/30/2019 Galley - Inflammation and Immunity
39/119
26
A similar sequence involves the TNF receptor (TNFR), signalled
by
TNF, and DR3 or Apo3 signalled by Apo3L. TNF binds to TNFR,
recruiting the DD protein TRADD, and acts as an intermediary for
binding
FADD, activating pro-caspase 8 in the same way as FAS.
However,
TRADD can also be occupied by another DD protein RIP, which
signalsto the nuclear factor B (NFB) and Jun pathways, which are
inhibitory
to apoptosis. TNF is expressed mainly in activated lymphocytes
and
macrophages, while TNFR is expressed ubiquitously. DR3 is
expressed by
spleen and thymus cells, and Apo3L by T cells. This complex
pathway is
represented in a simplified form in Figure 2.3.
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Apo2L
TRAIL
Death adaptor
ICE/
Caspase 1 Caspase 8
Caspase 3m
Bad, Bax
Cytochrome c
APOPTOSIS Nucleus
Bcl2/Bcl-XL
FADD TRADD TRAF 1
FLIPNFB
activation
FasL Apo3L TNF
DR4/
DR5
Fas/
CD95
DR3 TNF R1Free radicals
NO Steroids
+/
Figure 2.3 The complex pathway involved in the signalling of
apoptosis events.For explanation and
abbreviations/acronyms see text.
Caspases
Caspases are a group of proteases, named because they cleave
proteins
mostly each other at aspartic acid (Asp) residues. Caspases
initially exist
as immature pro-caspases (zymogens) and require processing to
be
activated, in a similar way to the proteins of the clotting or
complement
cascades. There are three basic domains in the immature form:
the pro-
domain, the large subunit, and the small subunit. Some caspases
are
initiators that is, their targets are downstream effector
caspases. The
initiator caspases have a large pro-domain, since these are
regulated by
proteins other than caspases.The effector caspases have small
pro-domains
since they are directly regulated by other caspases. In other
words, the
pro-domain is important for proteinprotein interactions. The
large
pro-domain interacts with other proteins in the cell, containing
caspaserecruitment domains (CARD domains). These interactions lead
to
the cleavage and activation of the inhibitor caspases, which
then go on to
cleave the effector caspases. Once activated the long pro-domain
caspases
-
7/30/2019 Galley - Inflammation and Immunity
40/119
27
may then cleave caspases with short pro-domains to achieve
their
activation.7
The full process of apoptosis in mammalian cells involves
several caspases,
some of which have specialised purposes; for example a whole
subgroup is
involved in cytokine activation rather than apoptosis (Figure
2.4).
APOPTOSIS AND THE INFLAMMATORY PROCESS
m
cytochrome c
cytochrome c
Apaf-1
pro-caspase 9
pro-caspase 3 caspase 3
APOPTOSIS
caspase 9
(ced-4 equivalent)
mitochondrion
Figure 2.4 A simplified representation of the role of caspases
in apoptosis.For abbreviations/acronyms
see text.
The initiator caspases include caspases 2, 8, 9, and 10, and act
on pro-
caspase 3. The effector caspases are 3, 6, and 7, which act on
proteins
involved in cell structure.The inflammatory caspases mentioned
earlier in
this chapter are 1, 4, 5, 11, 12, and 13. Substrates for these
enzymes are
pro-IL-1 and pro-IL-18. IL-18 is a relatively recently
elucidated cytokine,
which has similar effects to IL-1. Thus the signals for
apoptosis can also
result in propagation of inflammatory events via
pro-inflammatory
cytokine release. The net effects of caspases are outlined in
Box 2.6.
Box 2.6 Net effect of caspase activity
Halts cell cycle progression
Disables homeostatic and repair mechanisms
Initiates detachment of the cell from surrounding tissue
structure
Disassembles structured components Marks dying cell for
engulfment by other cells such as
macrophages
-
7/30/2019 Galley - Inflammation and Immunity
41/119
28
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Redundancy of caspases
Caspase-1 or ICE is not a single enzyme, but one of a family of
related
proteases, which are co-expressed.This appears to provide
redundancy for
an important function and circumvents what was once an
embarrassment,that caspase-1 knockout mice still undergo
apoptosis.
The role of mitochondria in apoptosis
Recently, the mitochondrion has been identified as playing a
central role in
apoptosis. Several findings support this idea: members of the
BCL-2 gene
family localise into the mitochondrial membrane and inhibit
apoptosis and
a mutant BCL-2, which cannot insert into the mitochondrial
membrane,is a less potent inhibitor of apoptosis. BCL-2/-XL can
also recruit Apaf-1
into the mitochondrial membrane and may prevent Apaf-1 from
activating
caspases, thereby inhibiting apoptosis. In addition some
mitochondrial
proteins induce apoptosis when leaked into the cytosol: during
apoptosis,
cytochrome c and apoptosis inducing factor (AIF) are released
from the
mitochondria and, with other factors, such as Apaf-1 and Apaf-3,
lead to
caspase activation and apoptosis. Increased levels of BCL-2 can
prevent
the release of these molecules, whereas caspase inhibitors
cannot. This
indicates the release of cytochromec
and AIF is downstream of BCL-2function but upstream of the
caspases. Apoptosis is also associated
with a change in the mitochondrial membrane potential, a
phenomenon
known as permeability transition. The permeability transition
can be
blocked by excess BCL-2 but not by inhibitors of caspases,
indicating that
the permeability transition is downstream of BCL-2 but
upstream
of caspase activation. BCL-2, bcl-XL, and another
apoptosis-related
gene, BAX, are capable of forming selective ion pores in
membranes, thus
forming channels in the mitochondrial membrane that could
regulate
permeability transition and the release of molecules such as
cytochrome c
and AIF.
Apoptosis and disease
Apoptosis and cancer
Cancer cells are known to use inhibition of apoptosis.8 For
example, one
of the two human papilloma viruses (HPV) that have been
implicated
in causing cervical cancer produces a protein (E6) which binds
andinactivates the apoptosis promoter p53. EpsteinBarr Virus (EBV),
the
cause of mononucleosis and a cause of Burkitts lymphoma,
secretes a
protein that stimulates cells to increase endogenous production
of bcl-2.
-
7/30/2019 Galley - Inflammation and Immunity
42/119
29
Both these actions make the cell more resistant to apoptosis and
therefore
enables cancer cells to continue to proliferate. Some B-cell
leukaemias and
lymphomas express high levels of bcl-2, thus blocking apoptotic
signals
that they may receive. Melanoma cells avoid apoptosis by
inhibiting the
expression of the gene encoding Apaf-1, and some cancer cells,
especiallylung and colon cancer cells, secrete elevated levels of a
soluble decoy
molecule that binds to FasL, preventing binding to Fas and
blocking
cytotoxic T cell killing mechanisms.
Apoptosis and AIDS
The hallmark of acquired immunodeficiency syndrome (AIDS) is
the
decline in CD4 T cell numbers. These cells are responsible,
directly
or indirectly (as T helper cells), for all immune responses.
Human
immunodeficiency virus (HIV) invades CD4 and one might assume
that
it is this infection by HIV that causes loss of CD4T cells.
However, fewer
than 1 in 100 000 CD4T cells in the blood of AIDS patients are
actually
infected with the virus and, although the mechanism is not
clear, apoptosis
appears to be involved. Since all T cells, both infected and
uninfected,
express Fas, expression of an HIV gene (termed Nef) in a
HIV-infected cell
causes the cell to express high levels of FasL at its surface
while preventing
an interaction with self-Fas preventing self-elimination.
However, when the
infected T cell encounters an uninfected cell (for example, in a
lymphnode), the interaction of FasL with Fas on the uninfected cell
kills it by
apoptosis.
Apoptosis and organ transplants
For many years it has been known that certain tissues including
the anterior
chamber of the eye and the testes are immunologically privileged
sites
such that antigens within these sites fail to elicit an immune
response fromhigh constitutive expression of high levels of FasL.
This finding raises the
possibility of a new way of preventing graft rejection. However,
animal
studies have produced mixed results. Allografts that have been
genetically
modified to express FasL have shown increased survival for
kidneys but not
for hearts or islets of Langerhans.
Apoptosis and sepsis
Apoptosis is also relevant to inflammatory responses in sepsis.
Theimmune/inflammatory balance in sepsis reflects the balance
between pro- and
anti-inflammatory responses, and the balance between
hypermetabolic/
hyperdynamic versus hypometabolic/hypodynamic responses.There is
also
APOPTOSIS AND THE INFLAMMATORY PROCESS
-
7/30/2019 Galley - Inflammation and Immunity
43/119
30
probably a balance between ischaemic or necrotic cell death and
apoptotic
cell death. Ultimately, the balance between all these components
probably
then governs death or survival of the patient (Figure 2.5).
CRITICAL CARE FOCUS 10: INFLAMMATION AND IMMUNITY
Hypermetabolic
Hyperdynamic
Hypometabolic
Hypodynamic
Exaggerated inflammatory
response
SEPSIS
Immune hyporesponsiveness
Ischaemic/
necrotic
Apoptotic
cell death