Embed Size (px)
Citation preview
Surgical procedure
G. Weber M.D., Ph.D
Professor of Surgery
Department of Surgical Research and Techniques Medical Faculty, Semmelweis University
Surgery
•is an ancient medical specialty •using operative manual and instrumental techniques •on a patient •to investigate and/or treat •a pathological condition (disease or injury)
An act of performing surgery: surgical procedure, operation, or simply surgery. In this context, the verb operate means to perform surgery.
Safe surgery
Pain – anaesthesia
Concept of infection
Discovery: Pain – anaesthesia
In October 16, 1846 the young William Morton got the opportunity from Prof. J. Warren, in Boston, to try his new miracle potion (ether) to anaesthetise a patient prior to a cervical tumor resection.
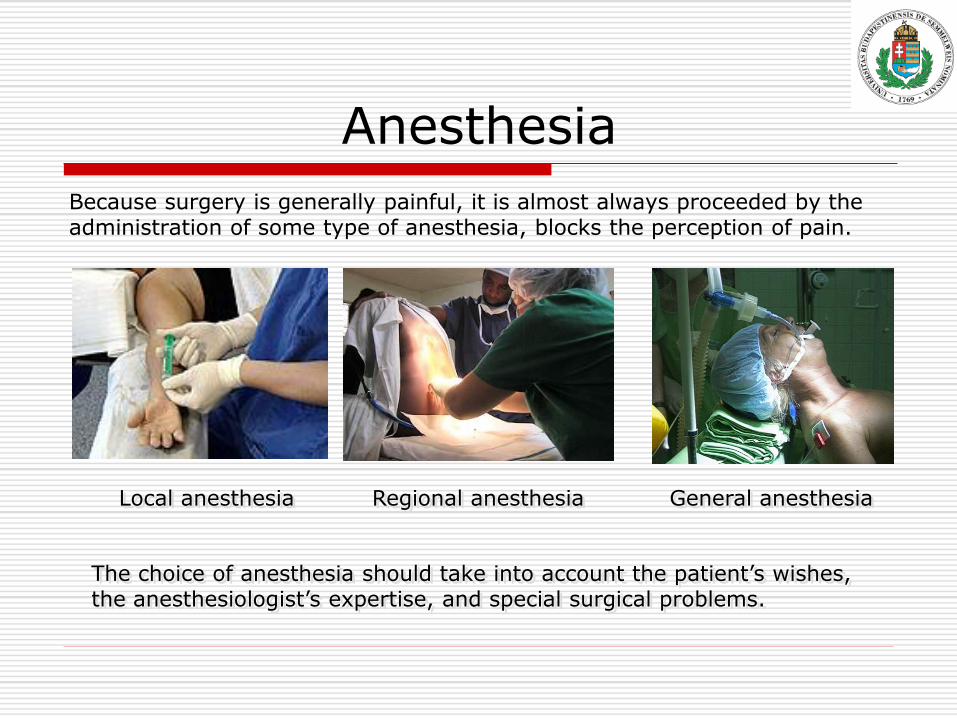
Anesthesia
Because surgery is generally painful, it is almost always proceeded by the administration of some type of anesthesia, blocks the perception of pain.
Local anesthesia Regional anesthesia General anesthesia
The choice of anesthesia should take into account the patient’s wishes, the anesthesiologist’s expertise, and special surgical problems.
Concept of infection
Ignaz Philipp Semmelweis (1818 – 1865) a Hungarian obstetrician who worked to identify the cause of puerperal sepsis. Semmelweis carefully compared mortality rates among obstetrical patients in two Viennese clinics.
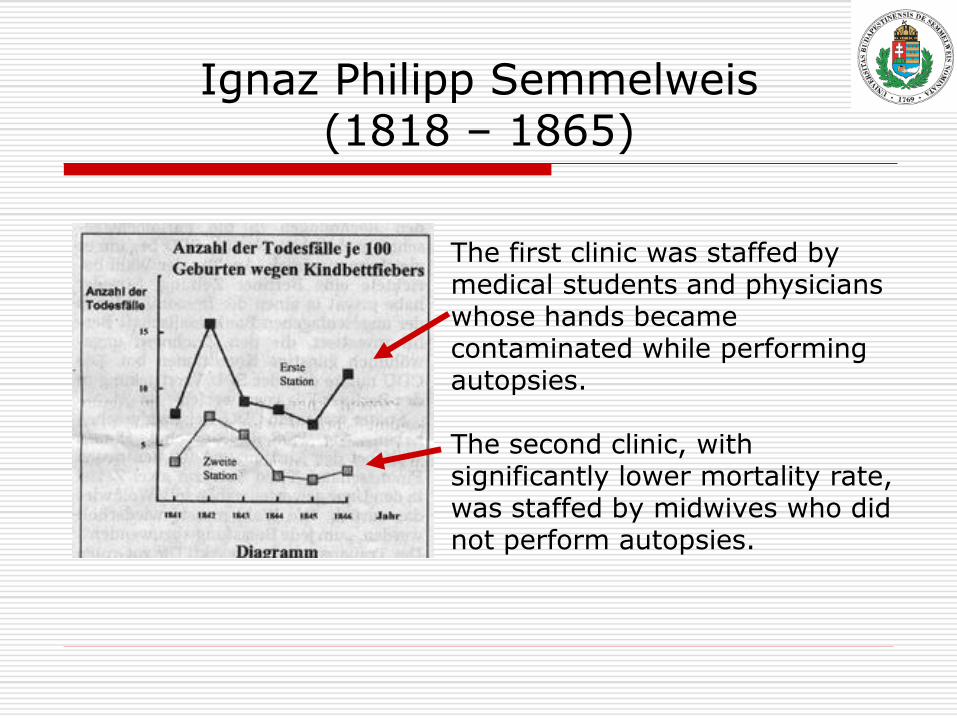
Ignaz Philipp Semmelweis (1818 – 1865)
The first clinic was staffed by medical students and physicians whose hands became contaminated while performing autopsies. The second clinic, with significantly lower mortality rate, was staffed by midwives who did not perform autopsies.
Ignaz Philipp Semmelweis (1818 – 1865)
The mortality rate of women declined from 18% to 2% in only 5 Months. Unfortunately, Semmelweis was unable to convince his colleagues of the importance of handwashing.
He implemented a program which required medical students to wash their hands in liquid chlorine after performing autopsies.
Surgical procedure
Based on timing: Three categories of surgery are known
emergency,
urgent,
elective.
The indication for surgery
Emergent procedure
(for example, a ruptured aortic aneurysm) leave very little time for evaluation.

The indication for surgery
Urgent procedure: ileus
require surgery soon, but the operation can usually be delayed some hours to accommodate further evaluation and improve- ment of existing pathology.
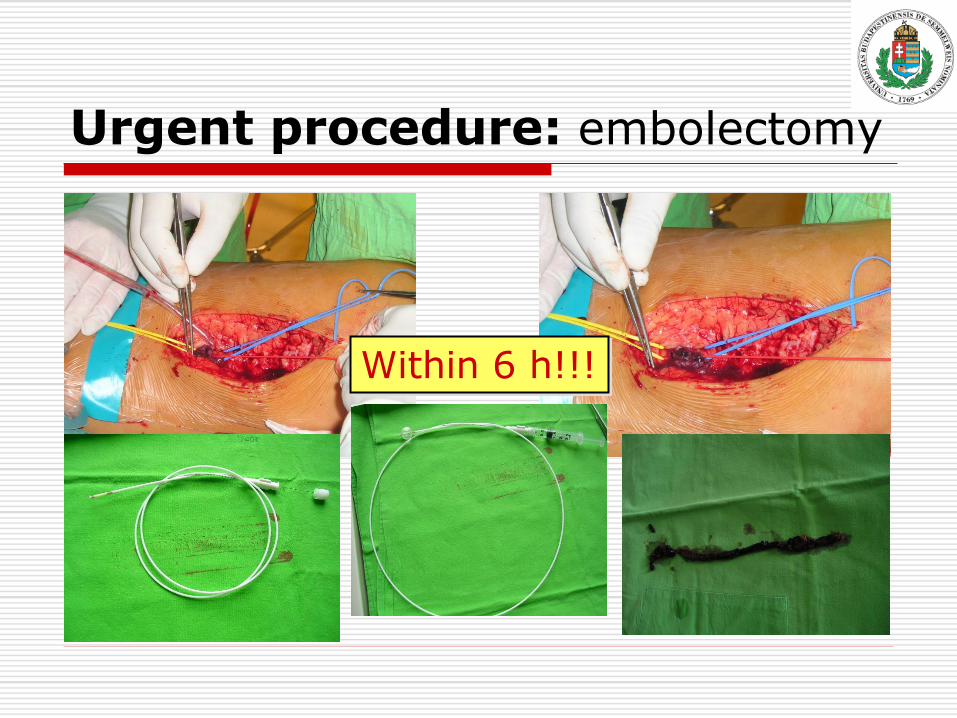
Urgent procedure: embolectomy
Within 6 h!!!
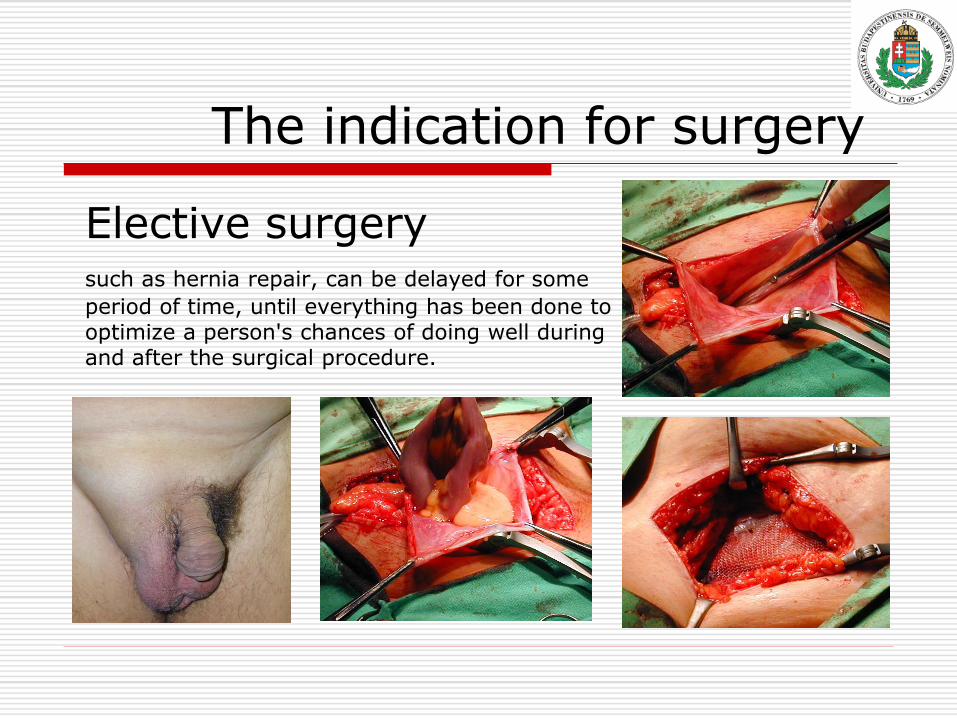
The indication for surgery
Elective surgery
such as hernia repair, can be delayed for some
period of time, until everything has been done to optimize a person's chances of doing well during and after the surgical procedure.
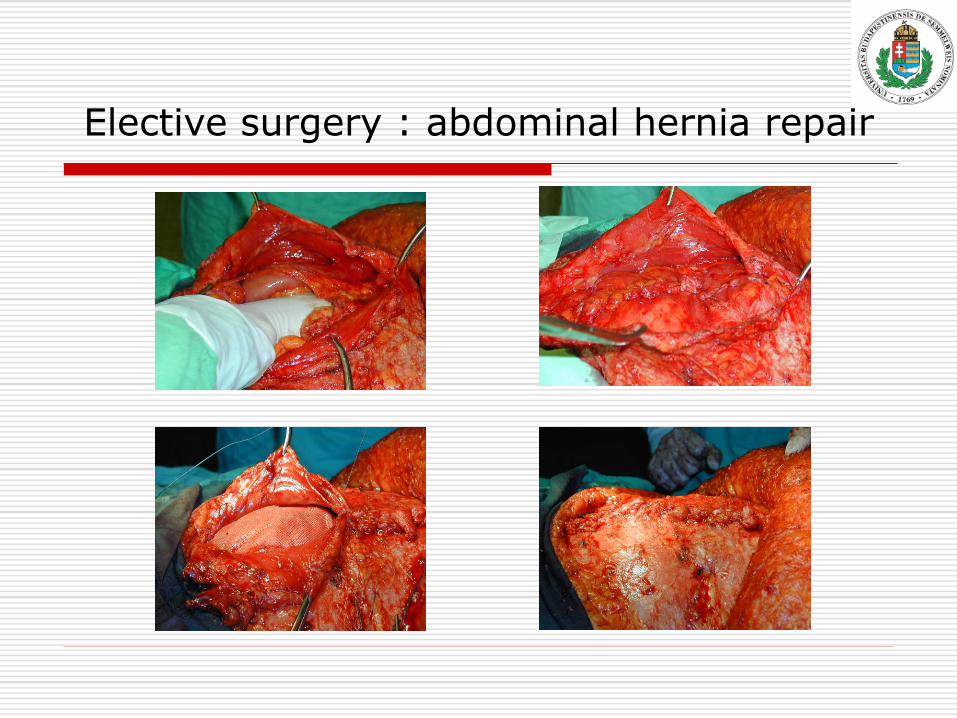
Elective surgery : abdominal hernia repair

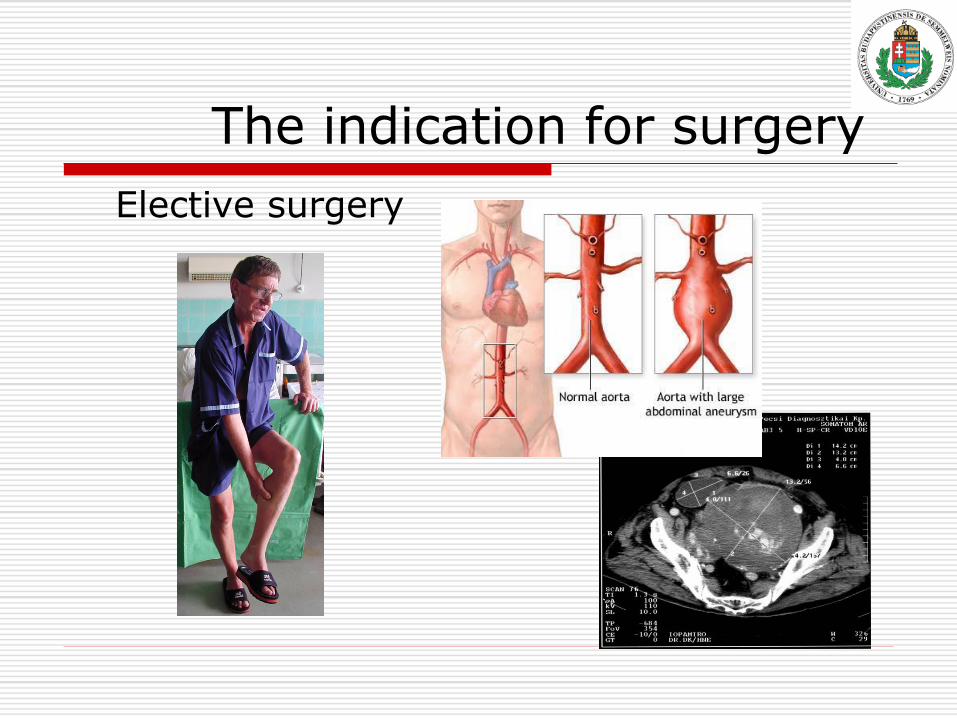
The indication for surgery
Elective surgery
The indication for surgery
Elective surgery
„Salus ægroti suprema lex”
the right operation is performed for the right reasons, accurately and expeditiously, on the right patient at the right time.
„The well-being of the patient is the most important law."
Pre-operative evaluation
Has two important goals:
For the patient to get a feeling of security and optimal peri-operative medical care, together with information concerning the surgery and anaesthesia.
For the surgeon and anaesthetist to get an objective picture of health and physical readiness for the operative procedure.
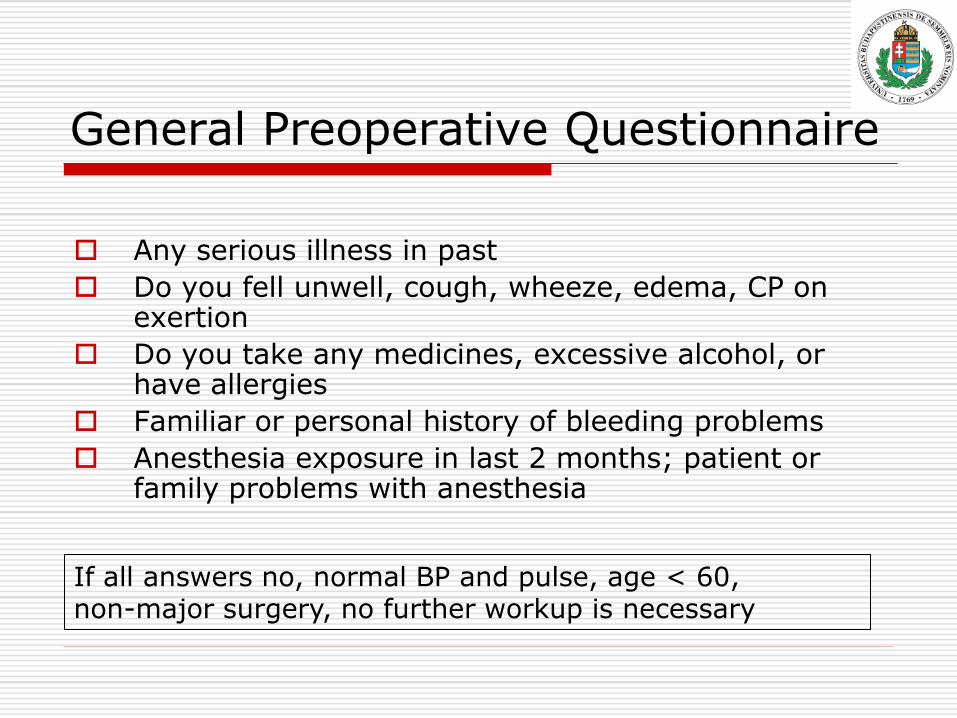
General Preoperative Questionnaire
Any serious illness in past
Do you fell unwell, cough, wheeze, edema, CP on exertion
Do you take any medicines, excessive alcohol, or have allergies
Familiar or personal history of bleeding problems
Anesthesia exposure in last 2 months; patient or family problems with anesthesia
If all answers no, normal BP and pulse, age < 60, non-major surgery, no further workup is necessary
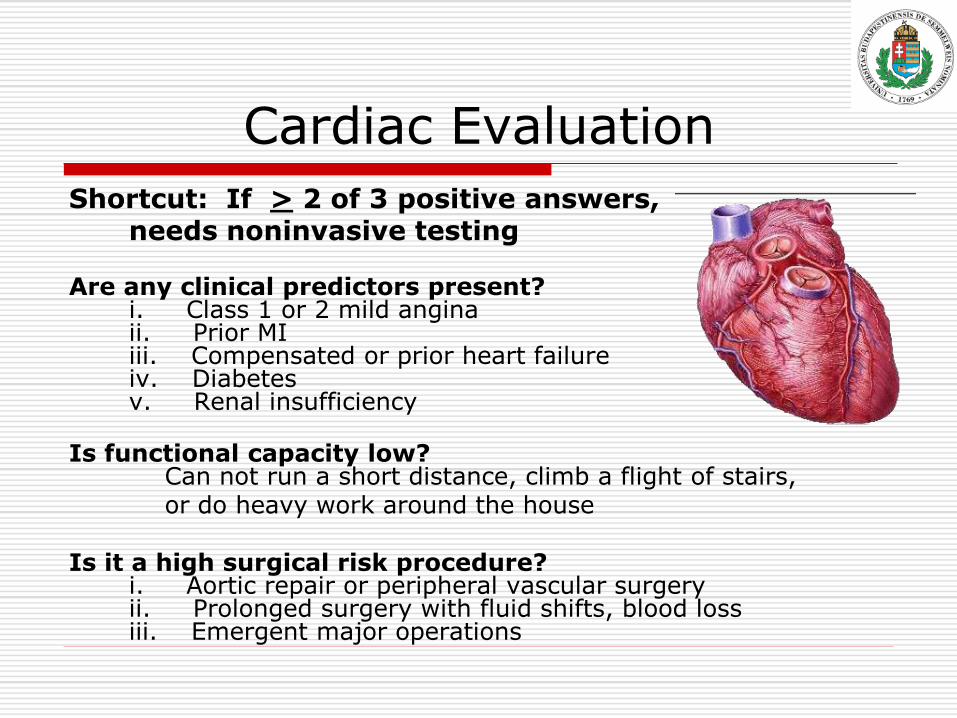
Cardiac Evaluation
Shortcut: If > 2 of 3 positive answers, needs noninvasive testing
Are any clinical predictors present?
i. Class 1 or 2 mild angina ii. Prior MI iii. Compensated or prior heart failure iv. Diabetes v. Renal insufficiency
Is functional capacity low? Can not run a short distance, climb a flight of stairs,
or do heavy work around the house Is it a high surgical risk procedure?
i. Aortic repair or peripheral vascular surgery ii. Prolonged surgery with fluid shifts, blood loss iii. Emergent major operations

Pre-operative evaluation
All organ systems should be evaluated by history, with emphasis on the cardiovascular, respiratory and central nervous system, liver, kidney and haematology as vital functions.
Pre-operative evaluation
PHYSICAL EXAMINATION
The emphasis in the preoperative examination is truly on a head to toe examination.
Patients should be examined in supine and recumbent positions for end organ pathology.
The extent of further investigations is decided by the history, the physical examination and the present therapy, the age of the patient, the type, extent and urgency of the planned operation.
Extent of surgery
High-risk procedure Emergency surgery Large blood loss Aortic or peripheral vascular surgery
Intermediate-risk procedure Abdominal or thoracic op. Head and neck surgery Carotid endarterectomy Orthopedic surgery Prostate surgery
Low-risk procedure Breast surgery Cataract surgery Superficial surgery Endoscopy
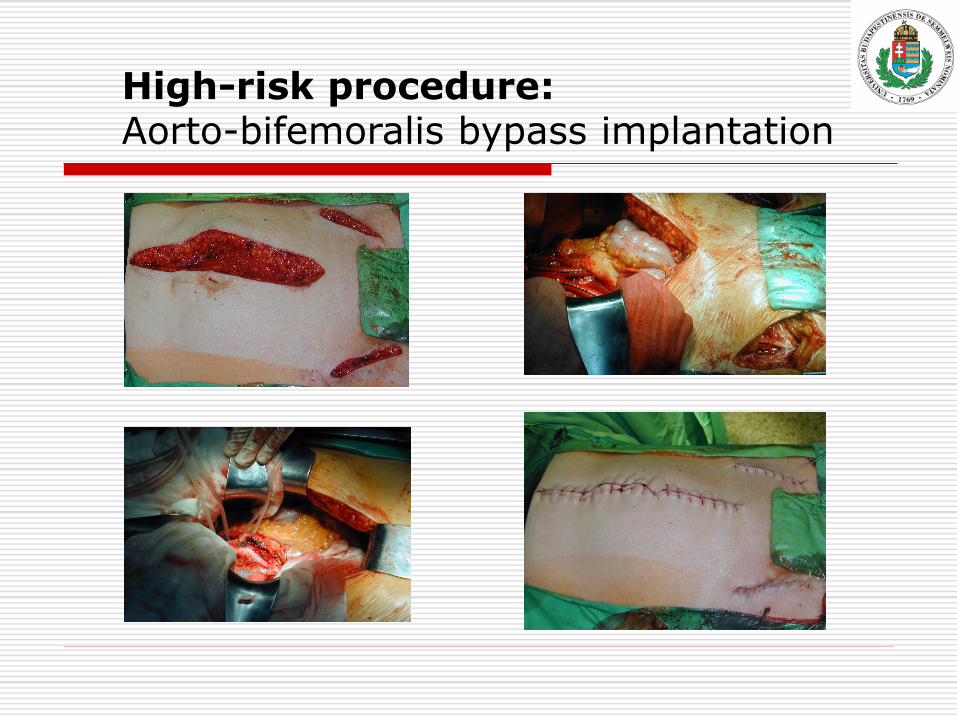
High-risk procedure: Aorto-bifemoralis bypass implantation
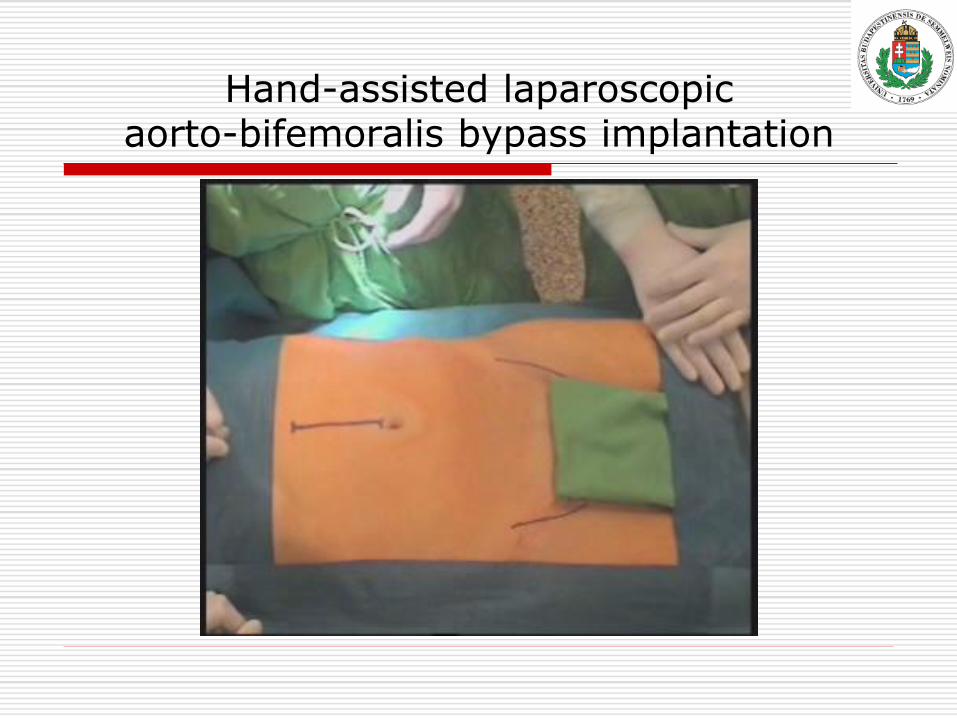
Hand-assisted laparoscopic aorto-bifemoralis bypass implantation
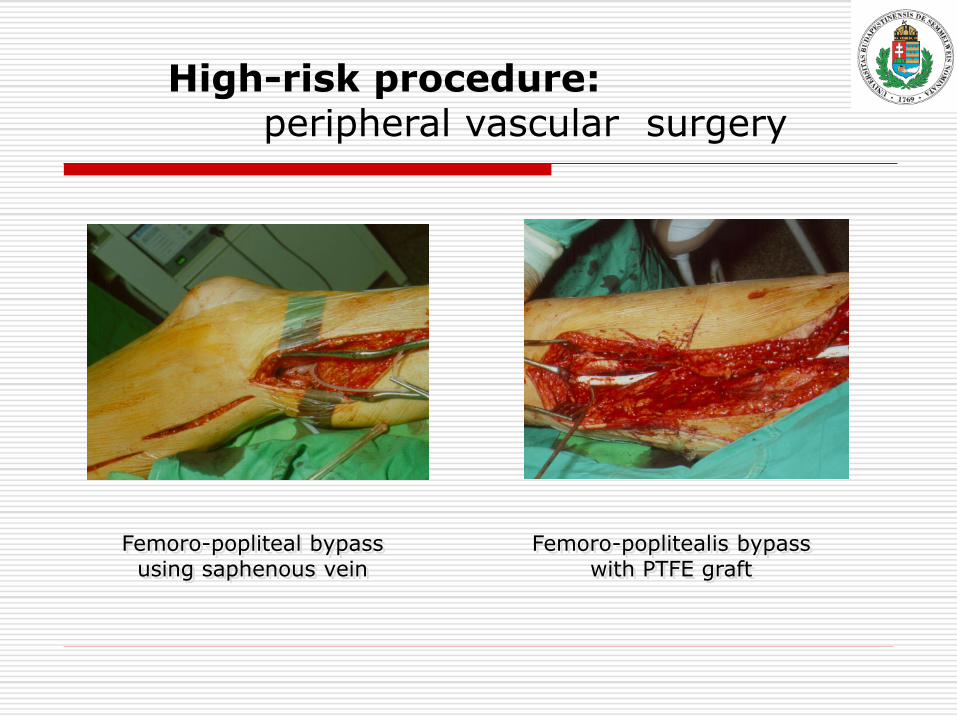
High-risk procedure: peripheral vascular surgery
Femoro-popliteal bypass using saphenous vein
Femoro-poplitealis bypass with PTFE graft
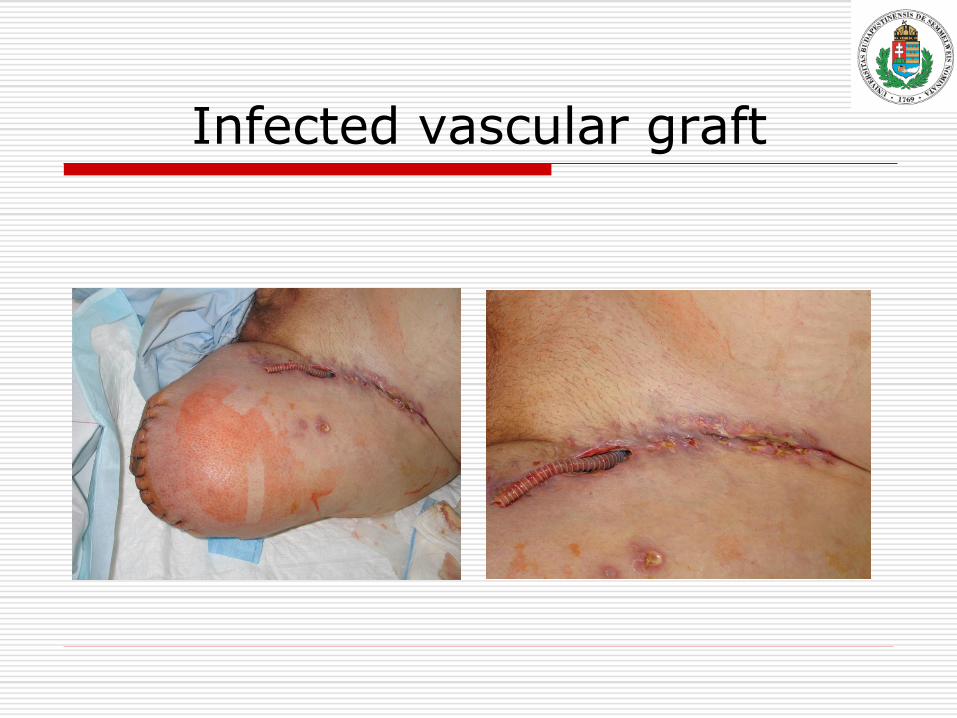
Infected vascular graft
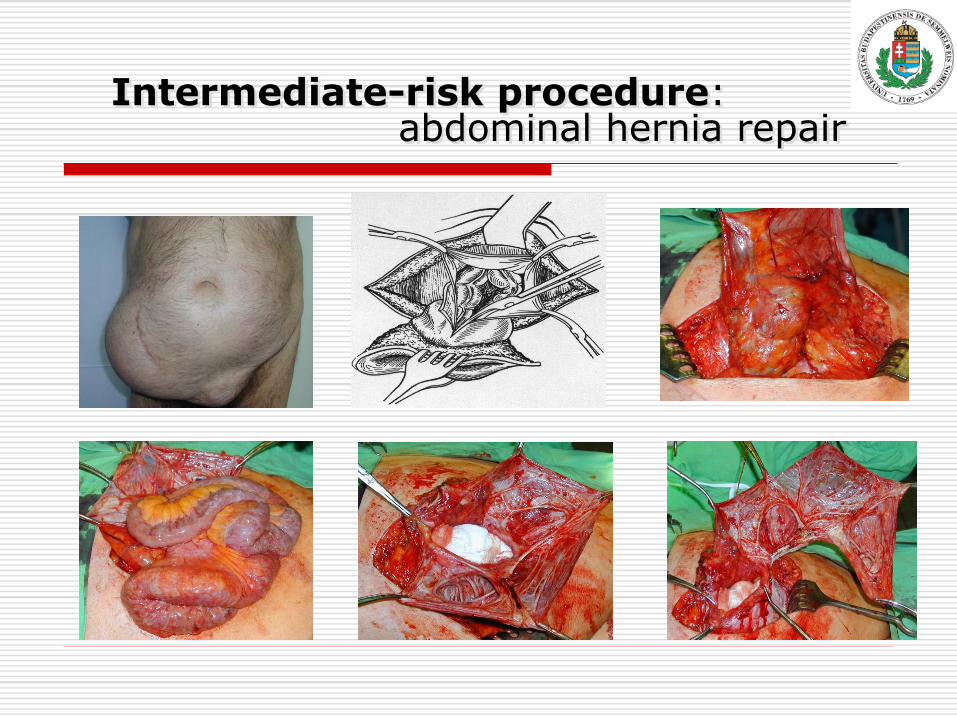
Intermediate-risk procedure: abdominal hernia repair
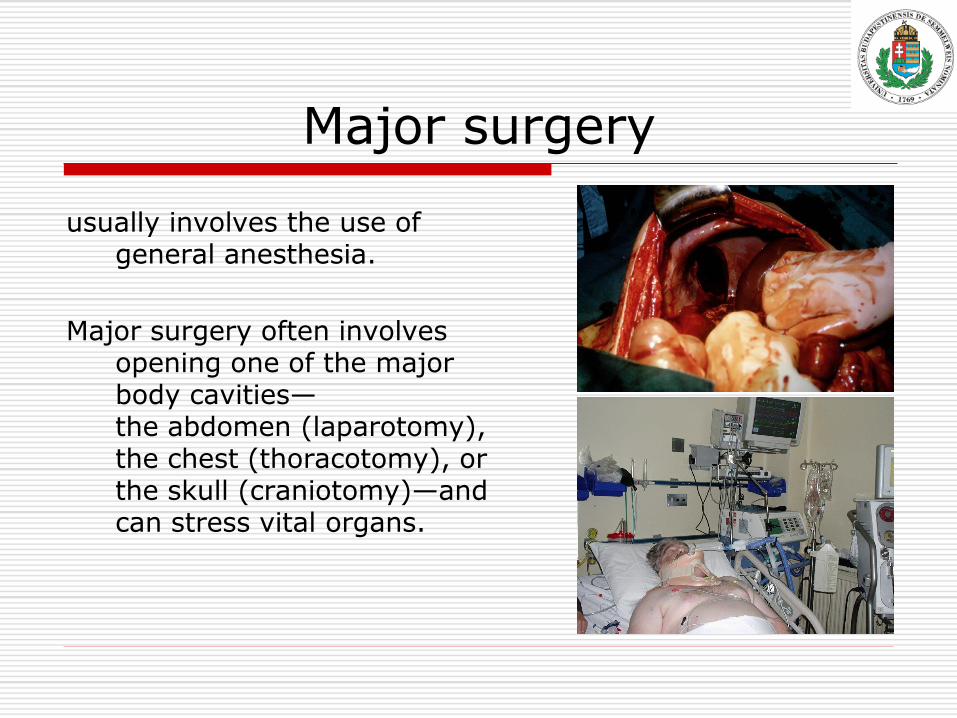
Major surgery
usually involves the use of general anesthesia.
Major surgery often involves opening one of the major body cavities— the abdomen (laparotomy), the chest (thoracotomy), or the skull (craniotomy)—and can stress vital organs.
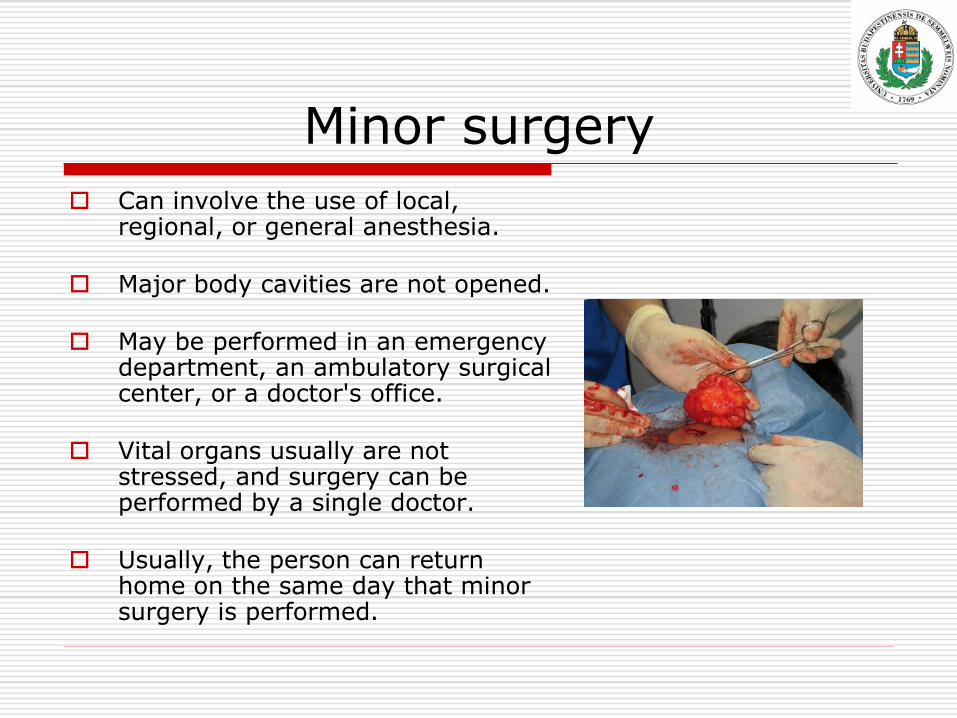
Minor surgery
Can involve the use of local, regional, or general anesthesia.
Major body cavities are not opened.
May be performed in an emergency department, an ambulatory surgical center, or a doctor's office.
Vital organs usually are not stressed, and surgery can be performed by a single doctor.
Usually, the person can return home on the same day that minor surgery is performed.
THE RISK ASSESSMENT
After taking the history, physical examination and special investigations, and integrating the results, the preoperative risk assessment is done.
The peri-operative risk consists of the anaesthetic and the surgical risk.
Both are difficult and must be seen separately as they influence each other.
THE RISK ASSESSMENT
The following factors have the largest influence on morbidity and mortality peri-operatively:
Pre-morbid conditions.
Type, extent, urgency and planned duration of the operation.
The anaesthetic technique (e.g. hypotensive anaesthesia).
The post-operative monitoring.
PATIENT’S INFORMED CONSENT
After risk assessment the surgeon works out the operative plan and discuss the plan with the patient.
The patient’s own choice should be taken into account if possible.
The patient has to give informed consent.
The surgeon has to inform the patient about the operative management, explain alternative techniques with their advantages and disadvantages.
Only if the patient is fully informed, can he give informed consent.
Second Opinion
The choice to undergo surgery is not always clear, and there may be several options for the kind of surgical procedure.
Thus, a person may seek the opinion of more than one doctor.
Some medical insurance plans require a second opinion for elective surgery.
Some experts advise establishing up front that the doctor giving the second opinion will not perform the operation, so that there is no conflict of interest.
Second Opinion
Others advise obtaining a second
opinion from a doctor who is not a surgeon, to eliminate any bias toward surgery when nonsurgical treatment is an option.
However, some experts recommend that another surgeon give the second opinion, believing that a surgeon knows more about the advantages and disadvantages of surgery than would a nonsurgeon.
„Salus ægroti suprema lex”
Sensitive communication of the nature and severity of the disease
clear explanation of the proposed treatment
A knowledgeable patient who participates in his or her treatment will get better faster.
A patient must not be allowed to give up hope.
Patient safety problems
A number of studies suggest that
approximately 10% of patients admitted to hospital suffer from some kind of harm.
Up to 98 000 hospital deaths occur in the USA as a result of medical error each year Kohn et al. To err is human: building a safer health system. Washington National Academy Press, 2000.
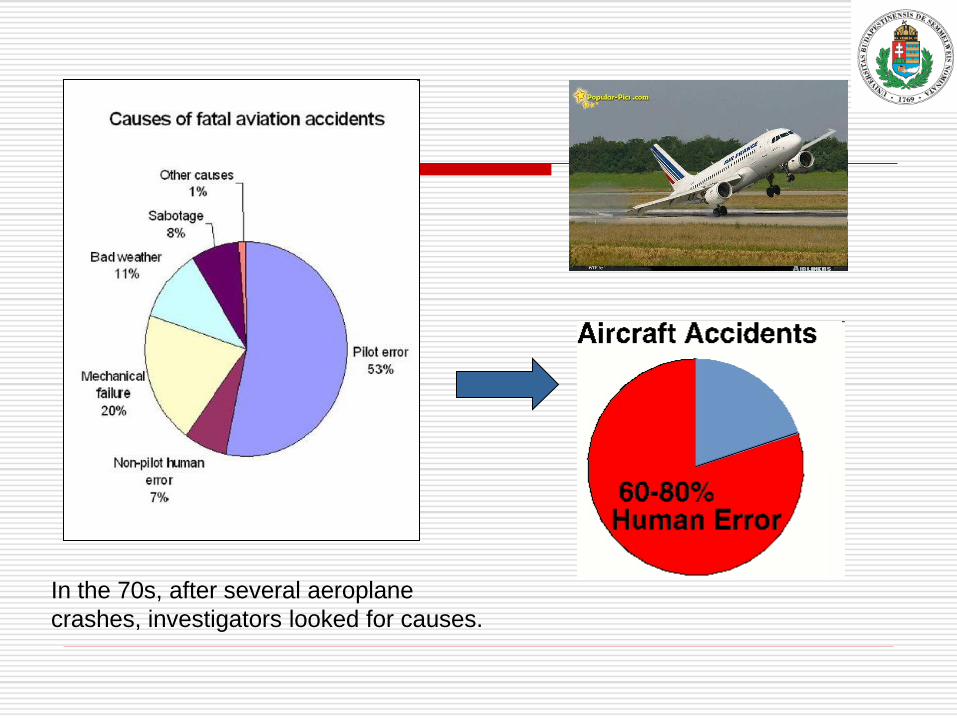
In the 70s, after several aeroplane
crashes, investigators looked for causes.
AEs in the OR from 35% to 66%
Evaluation of errors:
communication failures
are the major causes
Great impact of non-technical
skills on technical performance
and clinical outcomes
Adverse events
Substantial proportion of adverse events are attributed to poor teamworking and related skills – incl. situation awareness and coordination between team-members in the OR
Studies of safety in other high-risk industries
show that adverse events are primarily attributed to human failures, rather than technical malfunction
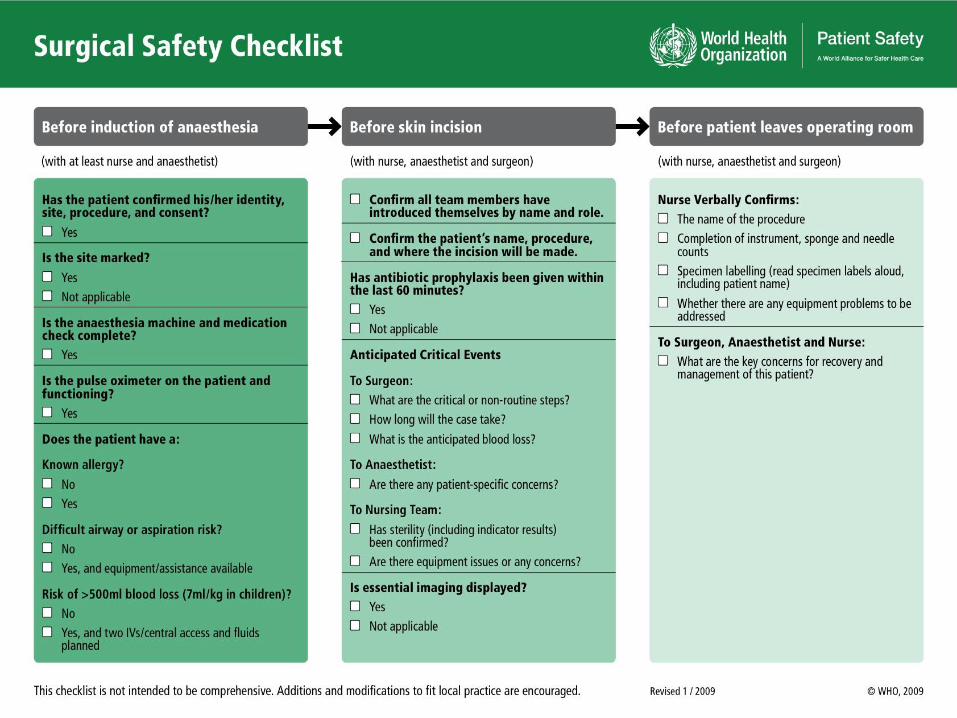
Surgical Safety Checklist
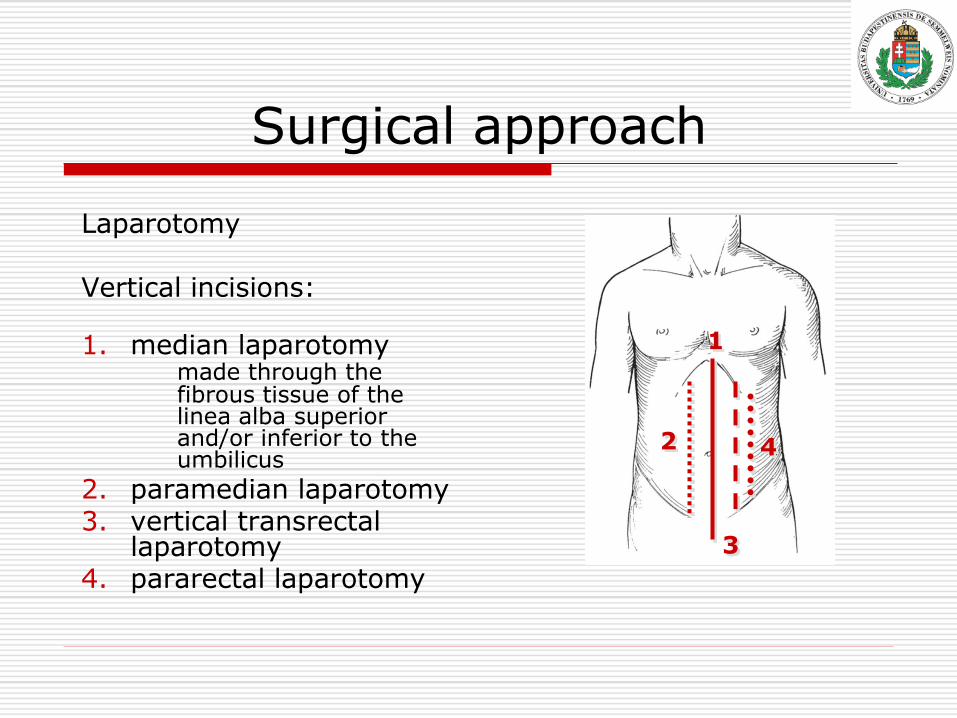
Surgical approach
Laparotomy Vertical incisions:
1. median laparotomy
made through the fibrous tissue of the linea alba superior and/or inferior to the umbilicus
2. paramedian laparotomy 3. vertical transrectal
laparotomy 4. pararectal laparotomy
1
2
3
4
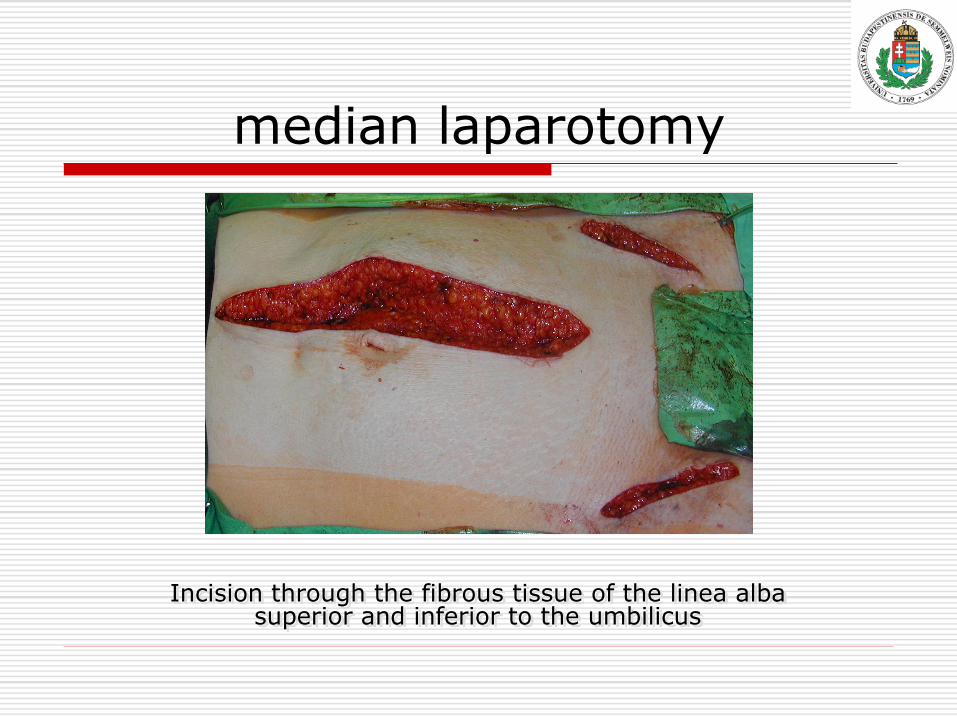
median laparotomy
Incision through the fibrous tissue of the linea alba superior and inferior to the umbilicus
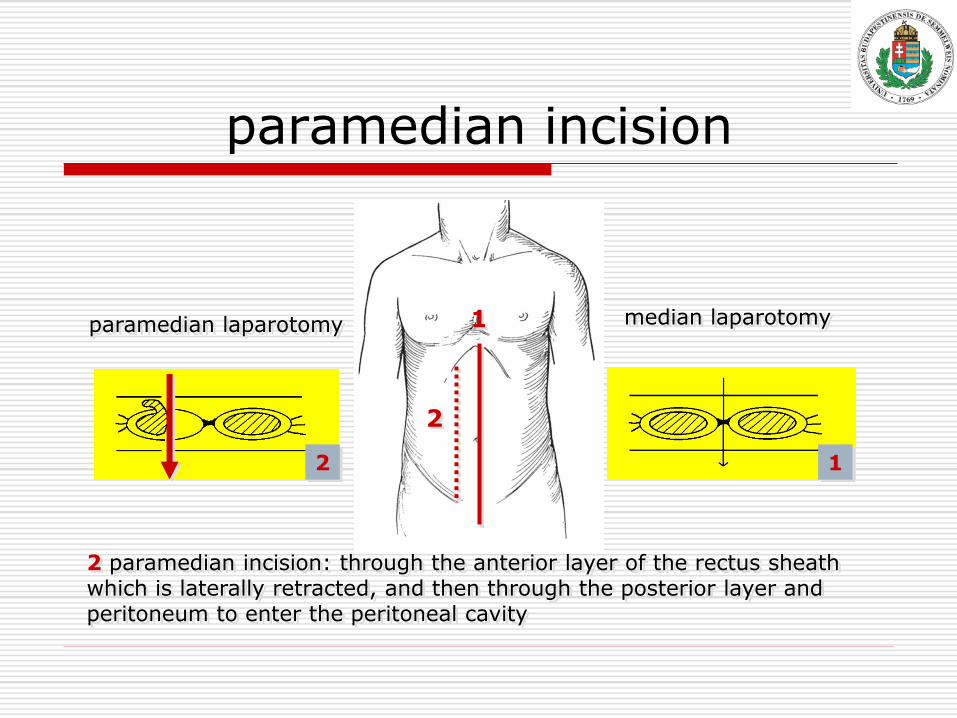
paramedian incision
1
2
1
2 paramedian incision: through the anterior layer of the rectus sheath which is laterally retracted, and then through the posterior layer and peritoneum to enter the peritoneal cavity
2
median laparotomy paramedian laparotomy
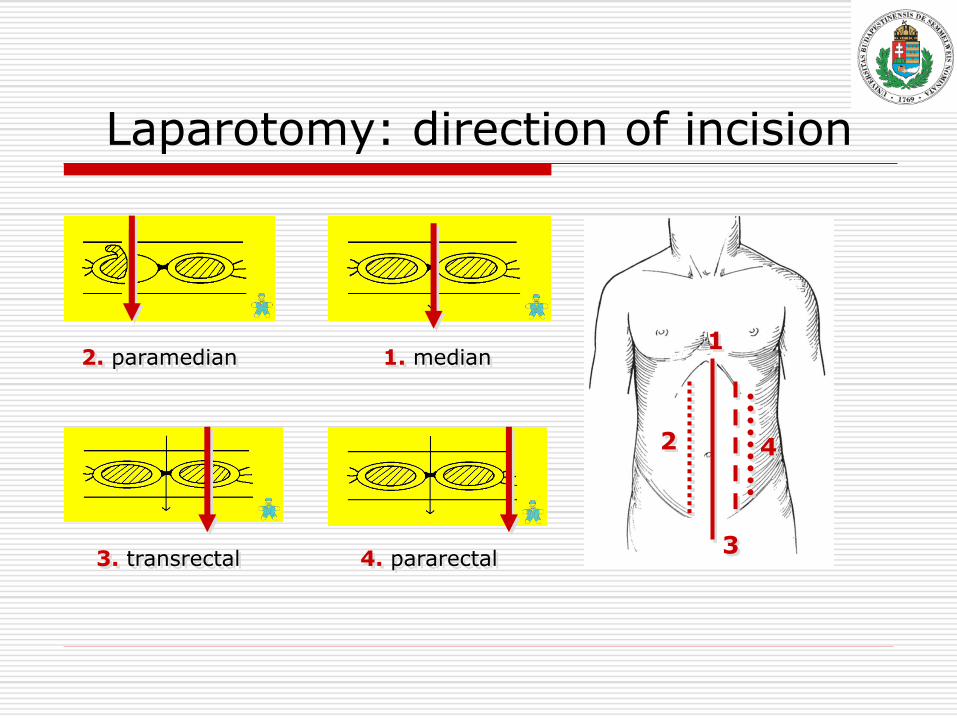
Laparotomy: direction of incision
1
2
3
4
2. paramedian 1. median
3. transrectal 4. pararectal
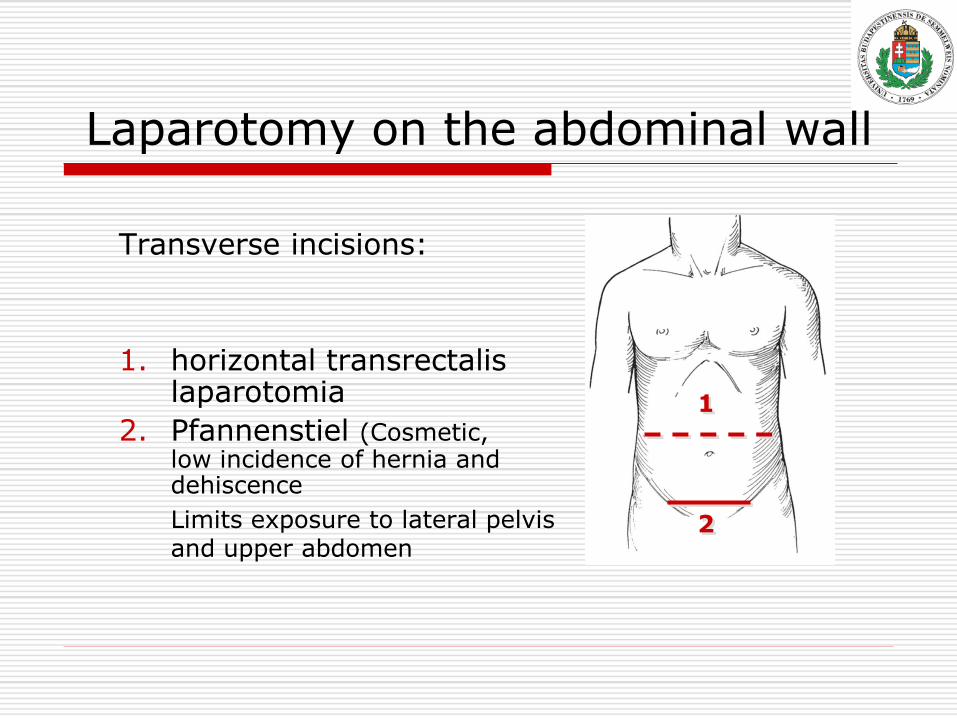
Laparotomy on the abdominal wall
Transverse incisions:
1. horizontal transrectalis laparotomia
2. Pfannenstiel (Cosmetic, low incidence of hernia and dehiscence
Limits exposure to lateral pelvis and upper abdomen
2
1
Laparotomy on the abdominal wall
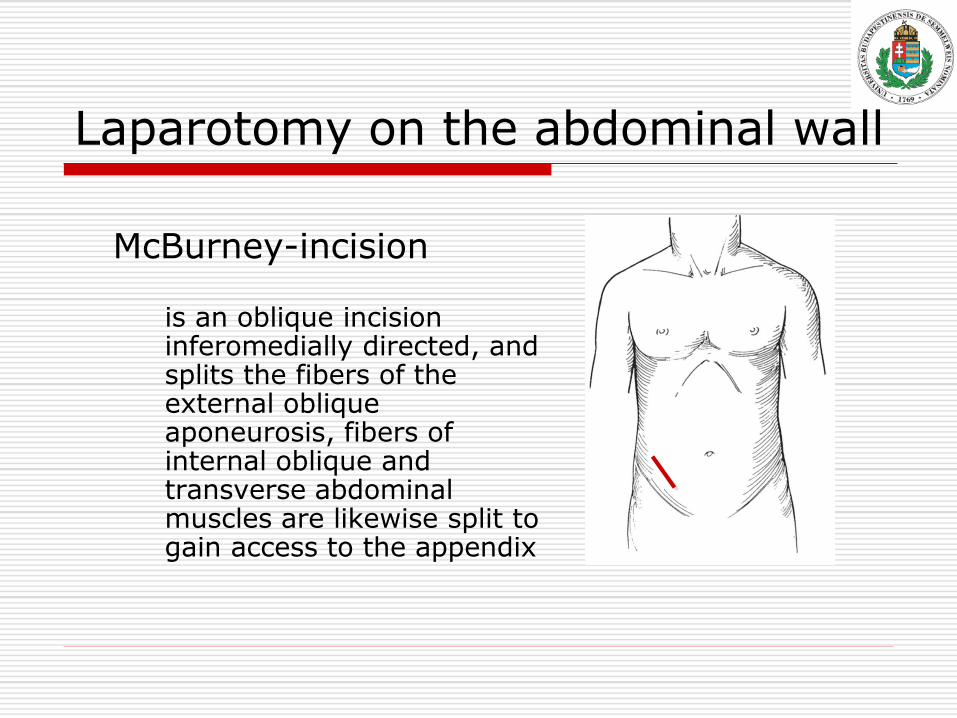
McBurney-incision
is an oblique incision inferomedially directed, and splits the fibers of the external oblique aponeurosis, fibers of internal oblique and transverse abdominal muscles are likewise split to gain access to the appendix
Laparotomy on the abdominal wall
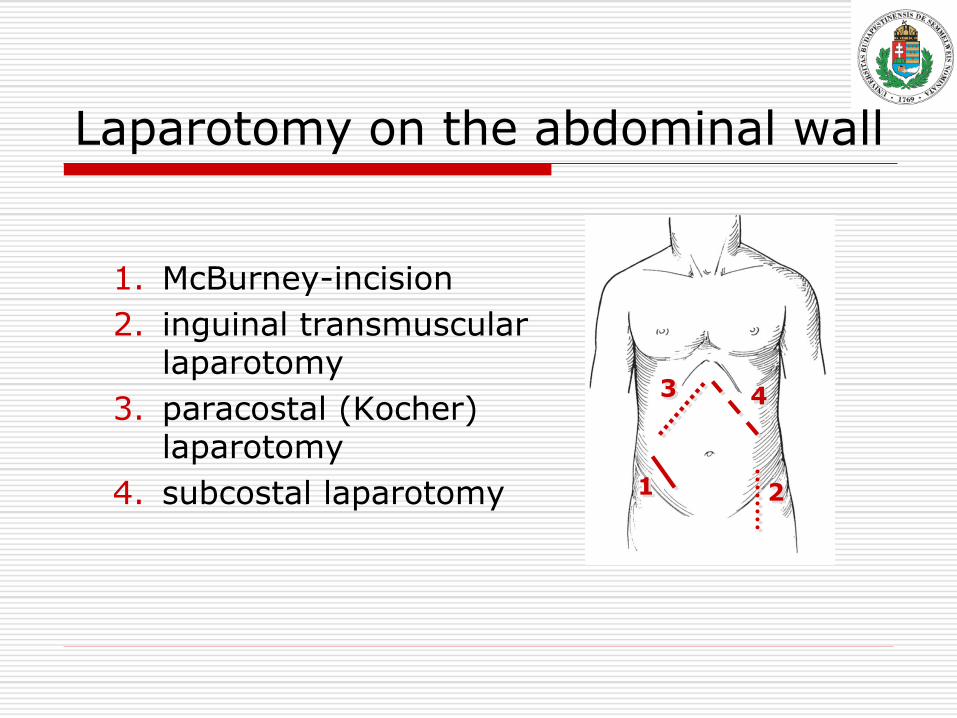
1. McBurney-incision
2. inguinal transmuscular laparotomy
3. paracostal (Kocher) laparotomy
4. subcostal laparotomy 1 2
4 3
Vertical vs transverse incision
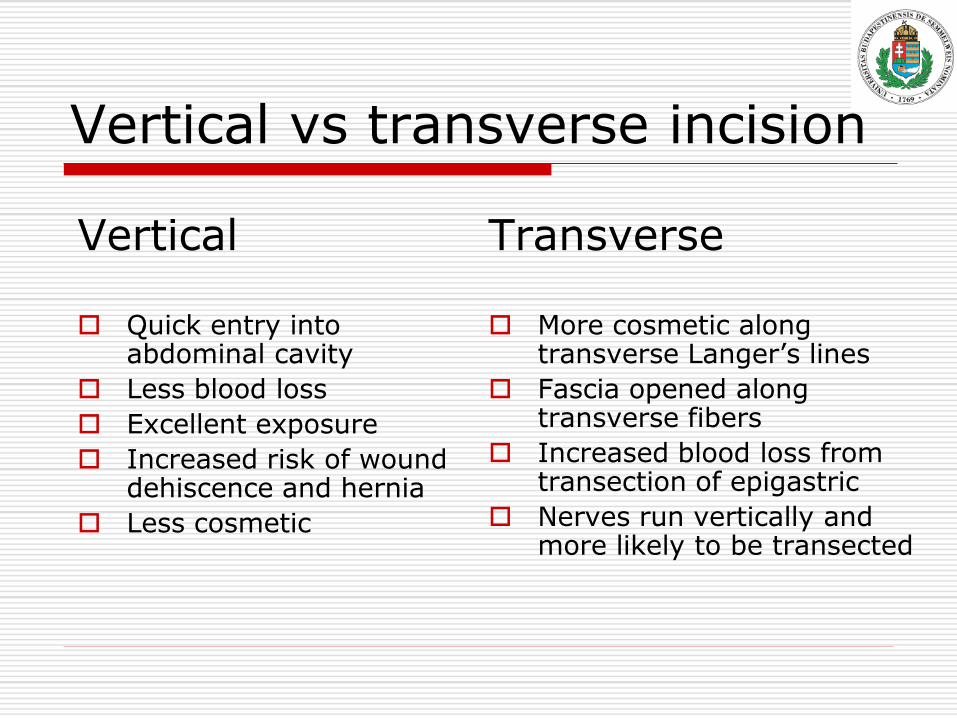
Vertical
Quick entry into abdominal cavity
Less blood loss
Excellent exposure
Increased risk of wound dehiscence and hernia
Less cosmetic
Transverse
More cosmetic along transverse Langer’s lines
Fascia opened along transverse fibers
Increased blood loss from transection of epigastric
Nerves run vertically and more likely to be transected

Thoracotomy
A: axillar thoracotomy B: extended axillar thoracotomy C: anterior intercostal thoracotomy D: Median sternotomy
Thoracotomy
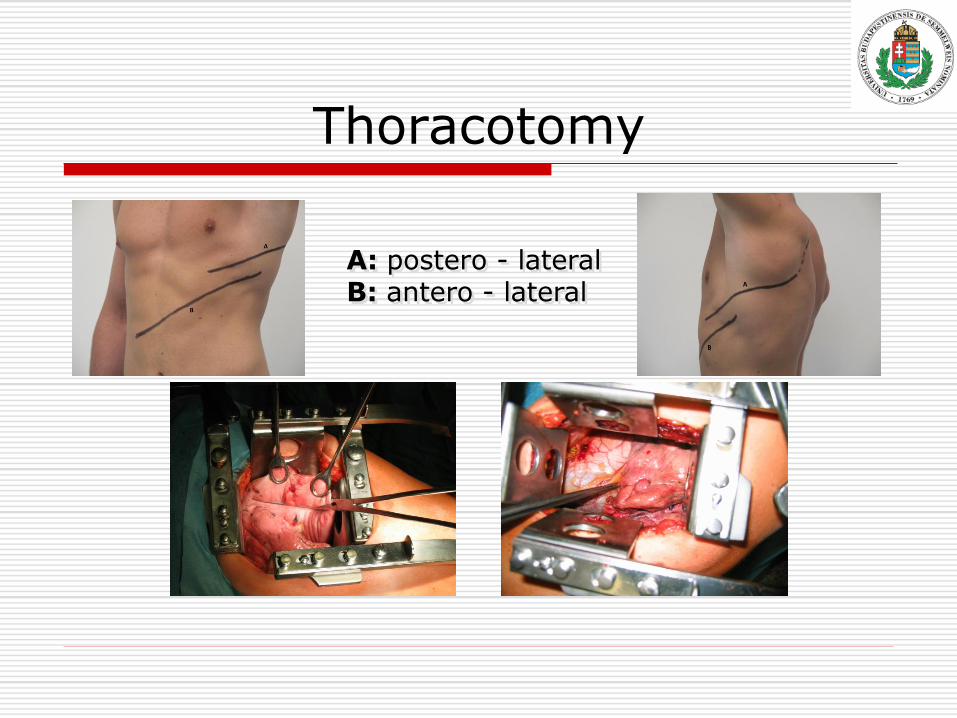
A: postero - lateral B: antero - lateral
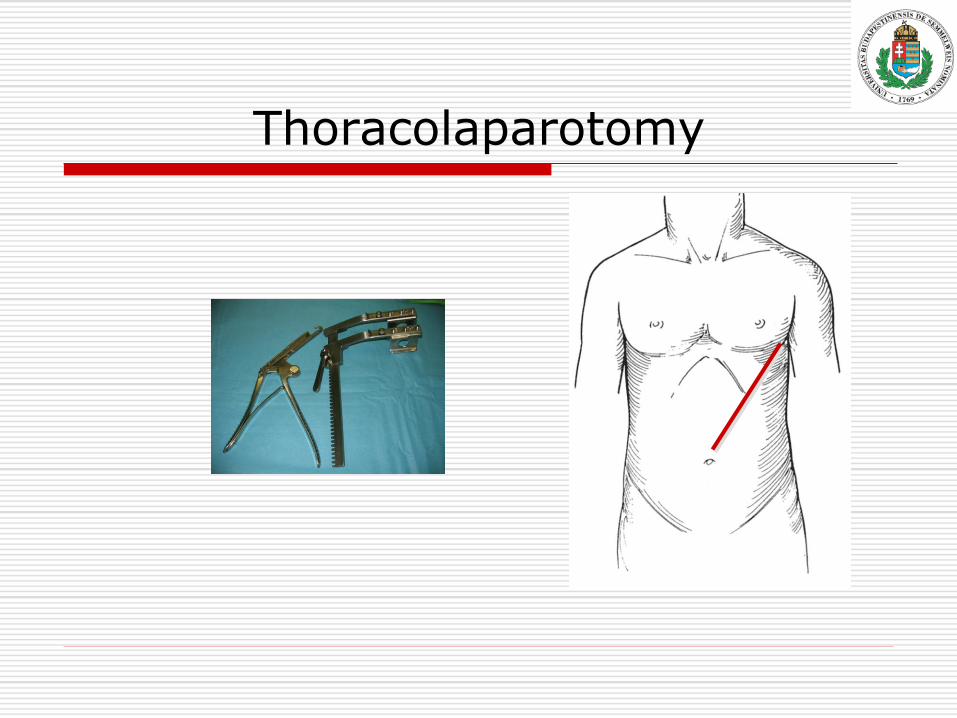
Thoracolaparotomy
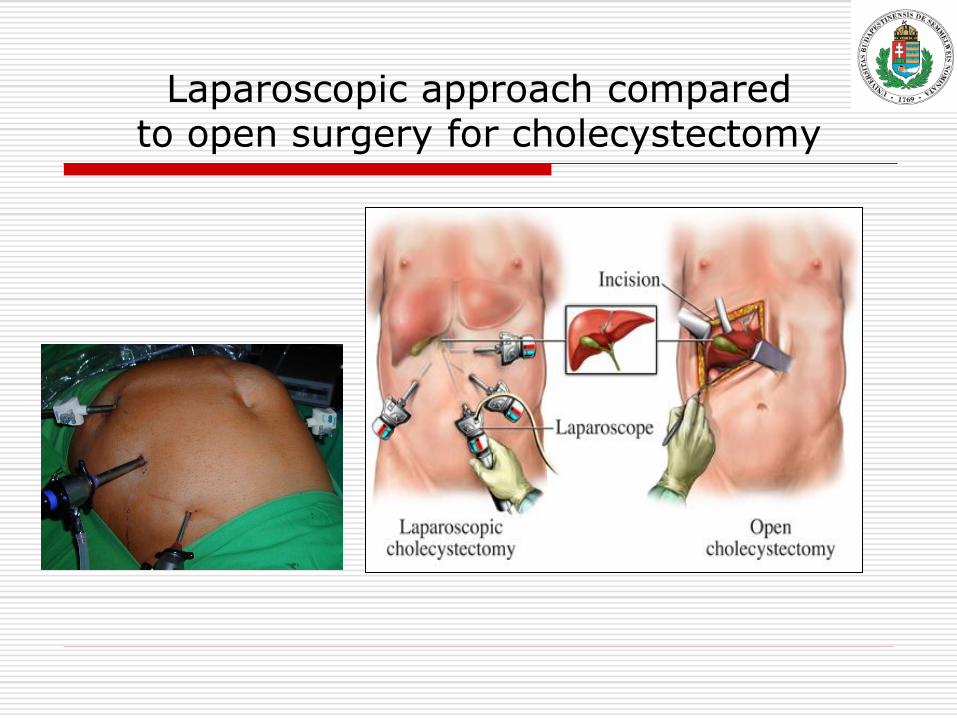
Laparoscopic approach compared to open surgery for cholecystectomy
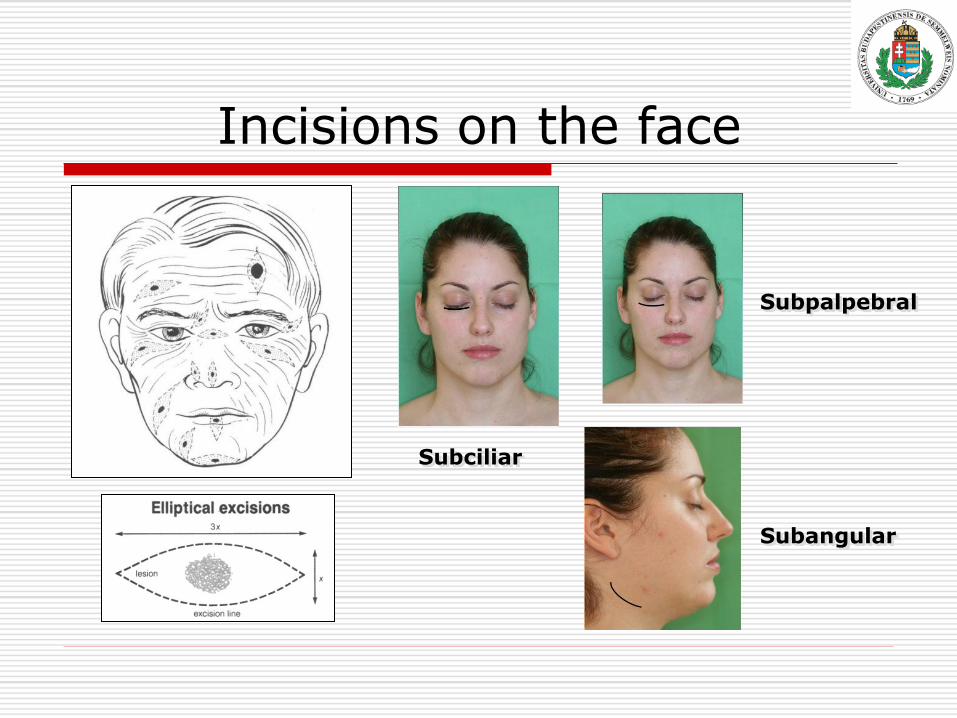
Incisions on the face
Subpalpebral
Subangular
Subciliar
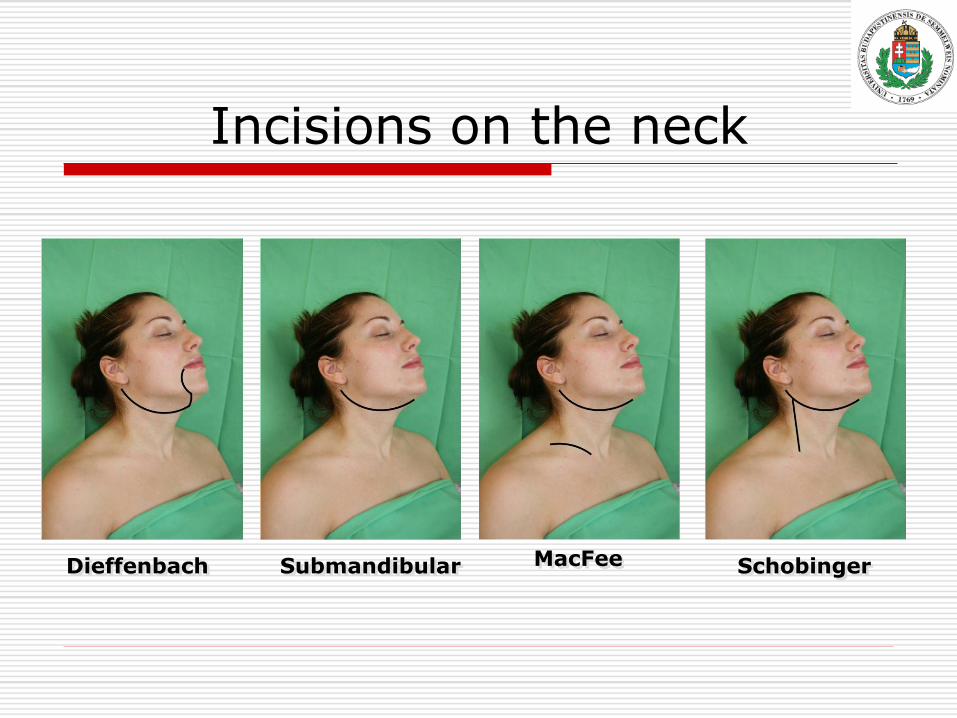
Incisions on the neck
Dieffenbach Submandibular MacFee Schobinger