Embed Size (px)
Citation preview

Frontier Cardiology
Imperial College Healthcare NHS Trust
with
Harrow Health
Iqbal Malik and Chris Jenner
wwwLondonCardioVascularCiniccouk
wwwLondonCardioVascularCiniccouk 1
wwwLondonCardioVascularCiniccouk 2
Interactive
No planned fire alarms
wwwLondonCardioVascularCiniccouk 3
Cover key topics
AF
IHD
Complex Cardiac Interventions
Cases
wwwLondonCardioVascularCiniccouk 4
900 Refreshments
930 Welcome and Introduction
950 Who to refer to MAU David Lubel
What does the report mean
1005 Holter abnormal Boon Lim
1030 Abnormal Echo Jamil Mayet
1100 Cases
wwwLondonCardioVascularCiniccouk 5
Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
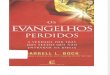
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
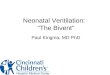
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
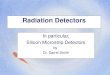
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 2
Interactive
No planned fire alarms
wwwLondonCardioVascularCiniccouk 3
Cover key topics
AF
IHD
Complex Cardiac Interventions
Cases
wwwLondonCardioVascularCiniccouk 4
900 Refreshments
930 Welcome and Introduction
950 Who to refer to MAU David Lubel
What does the report mean
1005 Holter abnormal Boon Lim
1030 Abnormal Echo Jamil Mayet
1100 Cases
wwwLondonCardioVascularCiniccouk 5
Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Interactive
No planned fire alarms
wwwLondonCardioVascularCiniccouk 3
Cover key topics
AF
IHD
Complex Cardiac Interventions
Cases
wwwLondonCardioVascularCiniccouk 4
900 Refreshments
930 Welcome and Introduction
950 Who to refer to MAU David Lubel
What does the report mean
1005 Holter abnormal Boon Lim
1030 Abnormal Echo Jamil Mayet
1100 Cases
wwwLondonCardioVascularCiniccouk 5
Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Cover key topics
AF
IHD
Complex Cardiac Interventions
Cases
wwwLondonCardioVascularCiniccouk 4
900 Refreshments
930 Welcome and Introduction
950 Who to refer to MAU David Lubel
What does the report mean
1005 Holter abnormal Boon Lim
1030 Abnormal Echo Jamil Mayet
1100 Cases
wwwLondonCardioVascularCiniccouk 5
Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

900 Refreshments
930 Welcome and Introduction
950 Who to refer to MAU David Lubel
What does the report mean
1005 Holter abnormal Boon Lim
1030 Abnormal Echo Jamil Mayet
1100 Cases
wwwLondonCardioVascularCiniccouk 5
Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Coronary disease AF Valves
1130 Rapid Access CPC Yvonne
1140 Rapid Access Arrhythmia Boon Lim
1150 Debate
Surgery is best for AVR Andy C
TAVI should be considered IM
1230 Lunch
wwwLondonCardioVascularCiniccouk 6
Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Complex Cardiac Interventions
130 New Cardiac Drugs Darrel Francis
145 PFOASDRDN IM
200 Defibs and Bivent Nick Peters
210 Heart failure in the house Darrel Francis
Cases to make your day
230 Chest Pain IM
240 Breathless Darrel Francis
250 Palpitation Nick Peters
wwwLondonCardioVascularCiniccouk 7
Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Thanks to BMI Clementine
Summary and Close 330-345
wwwLondonCardioVascularCiniccouk 8
wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 9
wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 10
wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 11
Iqbal Malik
ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

ST depression T wave inversion ST elevation
ESC NSTE-ACS Guidelines 2007
Acute Coronary Syndromes
ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

ST elevation
STEACS NSTEACS
troponins
myonecrosis no myonecrosis
Adapted from H White Lancet 2008
Aborted MI STEMI NSTEMI
Working
Diagnosis
Final
Diagnosis
unstable
angina
no ST elevation
ECG
aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

aspirin andor clopidogrelprasugelticagrelor
abciximab or tirofibaneptifibatide
UFH or LMWH or fondaparinux or bivalirudin
immediate or delayed angiogram
routine or selective invasive strategy
140 DIFFERENT
THERAPEUTIC
COMBINATIONS
Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Management of suspected NSTEACS
troponins (on presentation and after 6 to 12 hours) repeat ECG
Risk score assessment Bleeding risk assessment
bull early discharge
bull ETT
1 Initial Evaluation amp Treatment
History Examination ECG firstndashline medical therapy
2 Validation amp Risk Stratification
3 Definitive Treatment
Adapted from ESC guidelines Eur Heart J 2007 28 1598
NICE 2010
LOW
RISK
bull angiography
bull IIbIIIa inhibitor
HIGH
RISK
bull early discharge
bull CT angiography
LOW
RISK
12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

12
3
17
13
3
20
8
15
20
0
10
20
30
Death Stroke Urgent readmissionfor cardiac event
Pa
tie
nts
(
)
STEMI (2075)
NSTEMI (1856)
UA (2883)
Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Friday night admission
A+E SHO then medical team
A+E SHO then cardiology team on Monday
Cardiology team direct
wwwLondonCardioVascularCiniccouk 17
Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Tell LAS that you want your patients at a
cardiac centre
Minimum requirement
Have a cardiology junior resident-see pt 1st
Have a cardiologist able to see pt within 1 hr
Always see the cardiologist within 12 hrs
Have the cath lab open every weekend
wwwLondonCardioVascularCiniccouk 18
wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 19
wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 20
Iqbal Malik
wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 21
Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Increasing incidence
Symptomatic
Med Rx 50 2 year survival
Surgery Excellent
BUT
30 of symptomatic patient declined or not
referred
wwwLondonCardioVascularCiniccouk 22
40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

40 yr old with Bicuspid valve as Stenosis
Operate
75 year old with diabetes and coronary disease
Operate
85 year old with previous CABG
TAVI
wwwLondonCardioVascularCiniccouk 23
85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

85 year old with no comorbidity
TAVI
95 year old with multiple co morbidity
Medical Rx
wwwLondonCardioVascularCiniccouk 24
NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

NOT suitable for surgery
The surgeon though risk too high
3015 patients screened
358 (12) into RCT TAVI vs medical Rx (inc BAV)
Many with ldquocomorbidityrdquo
Porcelain aorta
Lungs
Chest wall problems etc
wwwLondonCardioVascularCiniccouk 25
Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Death Rates 30 day 1 year P
TAVI 5 28 ns
Conventional
medical
307 507 Plt0001
wwwLondonCardioVascularCiniccouk 26
1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

1 yr
death
readmission
1 yr
CVA
1 yr
NYHA III
TAVI 425 78 748
Medical 716 39 42
p plt0001 p=018 plt0001
wwwLondonCardioVascularCiniccouk 27
Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Aortic stenosis in your practice
Donrsquot be nihilistic Refer to a TAVI centre
AVR rates go up
TAVI via strict MDT
Number need to treat
3 wwwLondonCardioVascularCiniccouk 28
wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 29
Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Teamwork
Strong MDT
National data collection
End of surgery
wwwLondonCardioVascularCiniccouk 30
wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 31
TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

TAVI if high risk for surgery
Define by scores plus
wwwLondonCardioVascularCiniccouk 32
wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 33
wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 34
Iqbal Malik
Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Development of atrial septum
Braunwald
Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Embolic ischaemic stroke (cryptogenic)
Cerebralcutaneous decompression disease
Migraine with aura
Sleep Apnoea
High Altitude Pulmonary Odema
Chronic Fatigue
symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

symptoms beyond the fourth decade including
reduced functional capacity exertional shortness of
breath
Pulmonary HT(lt5)
Palpitations (atrial flutter AF)
Systemic embolism -AF
20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

20 of neurological events may be cardiac
40 of neurological events are cryptogenic Are these often cardiac
Rheumatic heart disease
AF
Cardiomyopathy (clot)
Aortic atheroma
Patent Foramen Ovale
GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

GJ Koullias et al Circulation 20041093056-3057
TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

TransCranial Doppler 86
Transthoracic Echo and contrast gt90
TOE and contrast gt90
Two modalities are better than one
MRI for ASD
Heckman et al
Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Not 1st line
If failed several medication
And
Have migraine with aura
PRIMA trial
RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

RESPECT (AGA)
PC-Trial (AGA)
VINTAGE-PFO
TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

TransCatheter Renal Denervation
Resistant HT
wwwLondonCardioVascularCiniccouk 49
wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 50
wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 51
wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 52
Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Deliver data nationally
Confirm good outcomes
Publish and do trials
Imperial does all this-please refer
wwwLondonCardioVascularCiniccouk 53
wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 54
Dr Iqbal Malik
PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

PAF NOT less risky that permanent AF
wwwLondonCardioVascularCiniccouk 55
wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 56
wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 57
wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 58
CHADS-2 =1
Lee et al JCE 2010
Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Camm et al EHJ 2010
bullAspirin has significant
risk of bleeding and
low dose should be
used
Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Lee et al JCE 2010
Smalll no of patients
Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Camm et al EHJ 2010
bullStudies now suggest a
bleed rate of 01-06
-Lower INR ranges
-Better control of
OAC
-Better hypertension
control
bullCaution with scoregt3
Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Dabigatran Pradaxa 110150 mg bd RELY
Direct thrombin inhibitor
Rivaroxaban Xarelto 20mg od ROCKET AF
Direct Xa inhibitor
Apixiban Eliquis 5 mg bd ARISTOTLE
Direct Xa inhibitor
Connolly et al NEJM 2009
Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Increased ldquofront-loadedrdquo risk
Lower long term risk
45 days warfarin post implant and
then TOE to assess integrity
Less inconvenience
Occlusion equivalent to warfarin
Holmes et al Lancet 2009
CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

CHA2DS2VAS score
Warfarin here to stay
Dagabitran role limited by cost
LAA closure if
Bleed risk
intolerance
wwwLondonCardioVascularCiniccouk 64
wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 65
69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

69 Male
Hx of exertional dyspnoea
Hx IHD
MI 1983
Normal ECG 2012
Angiogram 3VD
CABG x3 April 2012
ECG May 2012
wwwLondonCardioVascularCiniccouk 66
ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

ECG 2012
wwwLondonCardioVascularCiniccouk 67
Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Action
Nil-normal ECG
Refer for anigo-abnormal ECG
Other
Repeat ECG
Echo
Reassure
wwwLondonCardioVascularCiniccouk 68
Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Thanks to all our lecturers
Thanks to our sponsors
wwwLondonCardioVascularCiniccouk 69
IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

IHD
2 million sufferers
Medical therapy is good for most
ranolazine
ivabradine
ACS-STEMI
PPCI is best
Chest pain
RACPC 020 3312 3732
wwwLondonCardioVascularCiniccouk 70
CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

CHADS2VASC2 score
0 medical rx with nothing
1 warfarin or nothing
2 or more warafarin
Elderly will do well on warfarin
Warfarin is cost effective if
CHADS2gt1
Time with good treatment gt65
wwwLondonCardioVascularCiniccouk 71
Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Who to give a EBCT to
is there any reason not to take all ACS to a
Heart Attack Centre
Who should get a LAA closure device
wwwLondonCardioVascularCiniccouk 72
Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Exercise
wwwLondonCardioVascularCiniccouk 73
Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

Smoking
wwwLondonCardioVascularCiniccouk 74
wwwLondonCardioVascularCiniccouk 75

wwwLondonCardioVascularCiniccouk 75









![Darrel Duffie CDS Valuation]](https://img.pdfslide.us/doc/110x75/577d357f1a28ab3a6b909ab2/darrel-duffie-cds-valuation.jpg)