Embed Size (px)
Citation preview

Annual Meeting
Immunology/Transplantation and Nephrology PRNs’ Focus Session—Long-term Management of the Renal Transplant Recipient Activity No. 0217-0000-11-076-L01-P (Knowledge-Based Activity) Monday, October 17 1:30 p.m.–3:30 p.m. Convention Center: Rooms 319 & 320 Moderators: Heather A. Nyman, Pharm.D., BCPS Clinical Pharmacist, Dialysis, University of Utah Dialysis Program, Salt Lake City, Utah and Angela Q. Maldonado, Pharm.D., BCPS Clinical Assistant Professor of Pharmacotherapy, Washington State University; Kidney Transplant Pharmacist, Providence Hospital, Spokane, Washington Agenda 1:30 p.m. Introduction and Welcome
1:40 p.m. Mineral and Bone Disorder in Chronic Kidney Disease and
Kidney Transplantation Timothy M. Clifford, Pharm.D., BCPS Clinical Pharmacist Specialist–Transplant/Critical Care; Assistant Adjunct Professor, Pharmacy and Surgery, University of Kentucky, Lexington, Kentucky
2:15 p.m. Anemia Pre- and Post-renal Transplant—Shouldn’t the Allograft Be the Cure? Joanna Q. Hudson, Pharm.D., FASN, BCPS Associate Professor, The University of Tennessee, Departments of Clinical Pharmacy & Medicine (Nephrology), Memphis, Tennessee
2:50 p.m. The Pharmacokinetics and Pharmacodynamics of Drug Dosing in the Renal Allograft Recipient Ali Olyaei, Pharm.D. Professor of Medicine, Director of Clinical Research, Division of Nephrology and Hypertension, Oregon State University/Oregon Health & Sciences University, Portland, Oregon
3:25 p.m. Closing Remarks
Faculty Conflict of Interest Disclosures Timothy M. Clifford: no conflicts to disclose. Joanna Q. Hudson: speaker’s bureau for Amgen. Ali Olyaei: no conflicts to disclose.
Long-term Management of the Renal Transplant Recipient 1
Annual Meeting
Learning Objectives
1. Discuss the pathophysiology of mineral and bone disorder (MBD)in the CKD patient. 2. Discuss the prevalence of MBD in the kidney transplant recipient. 3. Describe the methods of diagnosing MBD, goals of management and monitoring parameters. 4. Recommend non-pharmacological and pharmacological treatment of MBD. 5. Discuss the pathophysiology of anemia both pre- and post-renal transplant. 6. Describe the goals of therapy and pharmacological management of anemia. 7. Describe the conflicting data on target hemoglobin with the use of erythropoiesis stimulating
agents. 8. Describe the various methods of estimating GFR in the renal allograft recipient. 9. Discuss the use of potentially nephrotoxic medications in the renal allograft recipient and how to
minimize nephrotoxicity. 10. Discuss how the varying degree of renal insufficiency affects the pharmacokinetics and
pharmacodynamics of the immunosuppressants.
Self-Assessment Questions Self-assessment questions are available online at www.accp.com/am
Long-term Management of the Renal Transplant Recipient 2

A i P d P t R lAnemia Pre- and Post-Renal Transplant – Shouldn’t theTransplant Shouldn t the
Allograft Be the Cure?
Joanna Hudson, Pharm.D., BCPS, FASN Associate Professor
Departments of Clinical Pharmacy & Medicine (Nephrology)Departments of Clinical Pharmacy & Medicine (Nephrology)The University of Tennessee
Memphis, TN

ObjectivesObjectives
• Discuss the pathophysiology of anemiaDiscuss the pathophysiology of anemia both pre- and post-renal transplant
• Describe the goals of therapy and pharmacological management of anemiap g g
• Describe the conflicting data on target fhemoglobin with the use of erythropoiesis
stimulating agents

Erythropoiesis in CKDErythropoiesis in CKDBone Marrow CirculationErythropoietin Iron
Circulation
Stem Cell BFU-E CFU-EPro-erythroblast Reticulocyte RBCs
0 15 19 21 250 15 19 21 25
Time to Mature Cell Development (days)JH Brook et al. Iron Metabolism in Health and Disease. 1st edition. London, England: W.B. Saunders; 1994.

Response to RBC Mass
Normal Kidney FunctionPatients with Anemia and
Kidney DiseasePatients on Dialysis
(U/li
ter)
104
105Normal Blood Donors
(U/li
ter)
104
105
Patients on Dialysis
Normal Blood DonorsPatients with Anemia
Patients with KidneysPatients without Kidneys
ropo
ietin
103
10
ropo
ietin
103
10
ma
Eryt
hr 102
101 ma
Eryt
hr 102
101
0 0.1 0.2 0.3 0.4 0.5 0.6
Plas
m
100
0 0.1 0.2 0.3 0.4 0.5 0.6
Plas
m100
Erslev AJ. N Engl J Med. 1991;324:1339-1344.
Hematocrit Hematocrit

Contributing Factors of Anemia A i d Wi h CKDAssociated With CKD
• Erythropoietin deficiency & resistancey p y• Chronic blood loss• Shortened RBC lifespan from 120 to ~60 days• Iron losses (iron deficiency)
– GI bleeding&– Reduced intake & absorption
• Malnutrition• Inflammatory conditions• Inflammatory conditions• Hemodilution• Secondary HyperparathyroidismSecondary Hyperparathyroidism• Other disease states (e.g. cancer, HIV)

Body Iron Distribution d P th H di l i P ti t
R ti l d th li l t
and Pathways: Hemodialysis Patient
Reticuloendothelial stores (low)
ferritin 50 to 800Gut
Transferrin Absorption0.5 mg/day
32
Tissue
1.5 mg = 50 µg/% (20% sat)
Erythroid marrow
200 mg32
mg/day
Loss:4 mg/day
Erythroid marrow
Red blood cells
36 mg/dayLoss:
1 mg/day
4 mg/dayNet loss: 4.5
mg/day
1500 mg (Hct 30)
Adapted from Bothwell et al. Iron Metabolism in Man. 2nd ed. 1979.

Clinical and Economic Impact of Anemia
Increased Decreased Q lit f
Increased Hospitalization
Mortality, Increased LVH1-3
Quality of Life4
and Lengthof Stay5
1. Harnett et al. Am J Kidney Dis. 1995;25(4 suppl 1):S3-S7.2. Ma et al. J Am Soc Nephrol. 1999;10:610-619.3. Levin et al. Am J Kidney Dis. 1996;27:347-354.4. Strippoli et al. J Am Soc Nephrol. 2004;15:3154-3165. 5. Jones et al. Kidney Int. 2004;65:757-767.

Lower HCT Associated With Increased Mortality i ESRD P ti tin ESRD Patients
1.331.331.41.4AllAll--cause deathcause death
1.121.12
1.001.00 0.960.96
1.251.25
1.111.111.001.00 0.970.9711
1.21.2
kk
AllAll--cause deathcause deathCardiacCardiac--related deathrelated death
0.60.6
0.80.8
elat
ive
Ris
elat
ive
Ris
0 20 2
0.40.4
0.60.6
*Re
*Re
00
0.20.2
< 27%< 27% 27% to < 30%27% to < 30% 30% to < 33%30% to < 33% 33% to < 36%33% to < 36%N 75 283N 75 283Hct Hct
**After adjustment for medical diseases.After adjustment for medical diseases.Ma et al. Ma et al. J Am Soc J Am Soc NephrolNephrol. 1999;10:610. 1999;10:610--619.619.
N = 75,283 N = 75,283

Anemia Post TransplantAnemia Post Transplant• At time of kidney transplantation almost all
patients have anemia of CKD
• Post-transplantation anemia (PTA) is estimated• Post-transplantation anemia (PTA) is estimated to occur in 30-40% of patients
• Anemia usually resolves by 3-6 months, but some patients have late PTA defined as anemia ≥ 6 to 12 months after transplant≥ 6 to 12 months after transplant
• Use of ESAs in kidney transplant recipients is y p prelatively low

Mechanisms of PTAMechanisms of PTA• Decreased RBC Production
D i d d (i t ACEI /ARB– Drug induced (immunosuppressants, ACEIs/ARBs, antimicrobial agents)
– Allograft dysfunction and rejectionAllograft dysfunction and rejection– Erythropoietin resistance (iron deficiency, infections,
aplastic anemia)
• Loss of RBCs– Surgical blood loss– GI blood loss
Frequent phlebotomy– Frequent phlebotomy

Mechanisms of PTAMechanisms of PTA• Increased RBC destruction
I di t d h l i (i i– Immune-mediated hemolysis (immunosuppression, PTLD)
– Microangiopathic hemolytic anemia (tacrolimus,Microangiopathic hemolytic anemia (tacrolimus, cyclosporine, sirolimus)
– Nonimmune hemolysis (G6PD deficiency – dapsone, t i / fl h l bi thi )trim/sufla, hemoglobinopathies)
• Other factors• Other factors– Donor and recipient factors– Limitations of iron indices in transplant populationLimitations of iron indices in transplant population– Elevated hepcidin levels

Immunosuppressive Medications and Anemia
• Antimetabolite medications (azathioprine MMFAntimetabolite medications (azathioprine, MMF, mycophenolic acid) bone marrow suppression
• mTOR inhibitors (sirolimus, everolimus) myelosuppression and other mechanismsye osupp ess o a d ot e ec a s s
• Hemolytic anemia with sirolimus and theHemolytic anemia with sirolimus and the calcineurin inhibitors tacrolimus and cyclosporine

Role of Hepcidin in Iron Metabolism
• Hormone produced primarily in the liver• Principal regulator or iron absorption and• Principal regulator or iron absorption and
distribution into tissues• hepcidin blocks iron absorption hepcidin blocks iron absorption• hepcidin increases iron absorption
Inflammation, Increased iron stores
Iron deficiency,Increased erythropoiesis
Hepcidin
Hepcidin

Prevalence of PTAPrevalence of PTA
MaleMale FemaleFemaleMild: Mild: HbHb > 12 > 12 -- 13 g/13 g/dLdL HbHb > 11 > 11 -- 12 g/12 g/dLdLModerate:Moderate: HbHb > 11 > 11 -- 12 g12 g//dLdL HbHb > 10 > 10 -- 11 11 g/g/dLdLSS HbHb ≤ 11 /≤ 11 /dLdL HbHb ≤ 10 /≤ 10 /dLdL
VanrenterghemVanrenterghem et al. et al. Am J TransplantAm J Transplant 2003;3:835.2003;3:835.
Severe: Severe: HbHb ≤ 11 g/≤ 11 g/dLdL HbHb ≤ 10 g/≤ 10 g/dLdL

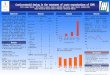
Prevalence of PTAPrevalence of PTA
ESA therapy was used in 5.2% of patients overall and in 18% of patients with ESA therapy was used in 5.2% of patients overall and in 18% of patients with severe anemia.severe anemia.
VanrenterghemVanrenterghem et al. et al. Am J TransplantAm J Transplant 2003;3:835.2003;3:835.

Prevalence of PTAPrevalence of PTA
Among pts with Hct < 30%
Mix et al. Mix et al. Am J TransplantAm J Transplant 2003;3:1426.2003;3:1426.
36% had iron studies46% received iron40% ESA

Association with GFRAssociation with GFR
Mix et al. Mix et al. Am J TransplantAm J Transplant 2003;3:1426.2003;3:1426.

Consequences in Transplant?Consequences in Transplant?
• Anemia significantly associated withAnemia significantly associated with– mortality (hazard ratio 1.69; 95% CI 1.15 – 2.5)1
– graft failure (hazard ratio 2.47; 95% CI 1.47-4.10)1g ( )– Left ventricular growth2
A i t l t d t ll t lit b t• Anemia not related to all-cause mortality but associated with 25% risk of allograft loss (hazard ratio 1 25; 95% CI 1 02-1 59)3ratio 1.25; 95% CI 1.02 1.59)
1 1 Molnar et al. Molnar et al. Am J TransplantAm J Transplant 2007;7:818. 2007;7:818. 2 2 RigattoRigatto et al. et al. J Am Soc J Am Soc NephrolNephrol 2003;2003;14:462. 14:462. 3 3 WinkelmayerWinkelmayer et al. et al. NephrolNephrol Dial Transplant Dial Transplant 2006;21:3559.2006;21:3559.

Consequences in Transplant?Consequences in Transplant?
• Not a clear consensus than anemia isNot a clear consensus than anemia is associated with increased mortality and adverse CV events in transplant population
Anemia may not directly cause adverse y youtcomes in transplant population, but may be a marker for an underlying pathologic process

Goals in Transplant PatientGoals in Transplant Patient
QUALITY OF TRANSFUSIONS
RISK OF ALLOGRAFT LOSSQLIFE
RISK OF ALLOGRAFT LOSS
Balance goals while minimizingBalance goals while minimizing the risks of treatment.

Approach to Prevention and TreatmentApproach to Prevention and Treatment
• Perioperatively: Consider iron for patientsPerioperatively: Consider iron for patients with transferrin saturation < 20% and serum ferritin < 200 ng/mLserum ferritin < 200 ng/mL
Consider ESA therapy when benefit• Consider ESA therapy when benefit outweighs risk

K/DOQI Guidelines for Anemia Management i th T l t P l tiin the Transplant Population
• Recommend that treatment guidelines for anemia in the ggeneral CKD population be followed in the transplant population
• ESAs Early Post-transplantation– Studies support that ESAs are effective in correcting anemia,
although higher doses may be required compared to dosesalthough higher doses may be required compared to doses pre-transplant
• ESAs Late Post-transplantation S s a e os a sp a a o– ESAs are effective and do not likely accelerate a decline in renal
function– May contribute to hypertension– May contribute to hypertension
Am J Kidney Dis. 2006;47(suppl 3):S1-S146.

Guidelines for Anemia of CKDCKD diagnosis CKD diagnosis
HbHb <12 g/<12 g/dLdL (females)(females)
Evaluate RBC, Evaluate RBC, reticulocytes, reticulocytes,
iron parametersiron parameters
Correct iron Correct iron deficiency deficiency
((oral,oral,Iron HbHb <13.5 g/<13.5 g/dLdL (males)(males) parenteralparenteral))deficient
Normal
Erythropoietic Erythropoietic Stimulating Agent Stimulating Agent
(ESA)(ESA)
Anemia correctedAnemia correctedNo
Measure Measure HbHb every every k il blk il bl
Hb < 1 g/dL 4 weeks after dose
changeHb > 1 g/dL in 2–wk
periodweek until stable, week until stable, then every 4 then every 4
weeksweeksIncrease dosesIncrease doses Decrease dosesDecrease doses
dose by 25%dose by 25%
change period
Adapted from: National Kidney Foundation. Am J Kidney Dis. 2001;37(suppl 1):S182-S237, Am J Kidney Dis. 2006;47(suppl 3):S1-S146 and Epoetin® PI June 2011.
by 25%by 25% dose by 25%dose by 25%

What is known about ESAs in the t l t l ti ?transplant population?
• ESA therapy post-transplant shortens time toESA therapy post transplant shortens time to achieve higher hematocrit and improves QOL1,2
• Observational studies in kidney transplant show evidence of increase mortality with Hb levels
b 12 5 /dL3above 12.5 g/dL3
• Medicare reimbursement polices affect therapyed ca e e bu se e t po ces a ect t e apy
1 1 Van Van LooLoo et al. et al. NephrolNephrol Dial Transplant 1996Dial Transplant 1996;11:815.;11:815.22McDevitt et al. McDevitt et al. Am J TransplantAm J Transplant 2005;5:1948.2005;5:1948.33Heinze et al. Heinze et al. BMJBMJ 2009;339:b4018. 2009;339:b4018.

Questions about ESAs in the transplant l ti ?population?
• Can we apply data from ESA studies in CKDCan we apply data from ESA studies in CKD population?
• When do we start treatment and how aggressive should we be?
• What is the target Hb?at s t e ta get b

Concerns with ESAs and Target Hb in CKD…

Mean monthly hemoglobin y g& mean EPO dose per week
United States Renal Data System (USRDS) 2006 Annual Data Report

Safety Information on ESAs:Supporting Studies
WARNINGS I d M t lit d S i C di l E tWARNINGS: Increased Mortality and Serious Cardiovascular Events
Study Patients Sponsor Published Target Hb(g/dL)
Besarab et al1Epoetin alfa Cardiac disease on hemodialysis Amgen 1998 14 ± 1* vs
10 ± 1
CHOIR2
Epoetin alfaAnemia associated with CKD not on dialysis
Ortho Biotech/
J & J2006 13.5* vs
11.3
CREATE3 Anemia associated with CKD not on F. CREATE3
Epoetin betaAnemia associated with CKD not on dialysis Hoffmann–
La Roche.2006 13-15 g/dL vs
10.5-11.5 g/dL
1 B b A t l N E l J M d 1998 339 584 590 CHOIR C ti f H l bi d O t i R l I ffi i1. Besarab A, et al. N Engl J Med. 1998;339:584-590.2. Singh AK, et al. N Engl J Med. 2006;355:2085-2098.3. Drüke, et al. N Eng J Med 2006:355:2071-84.
CHOIR = Correction of Hemoglobin and Outcomes in Renal InsufficiencyCREATE = Cardiovascular Risk Reduction by Early Anemia Treatment with Epoetin Beta

CHOIR Trial
1432 patients enrolled
Primary endpoints: time to composite death, MI, stroke, death, CHF hospitalization
p
715 assigned to high-Hb group (13.5 g/dL)
717 assigned to low-Hb group (11.3 g/dL)
• 312 completed 36 months or withdrew at study termination without having primary event
• 125 had a primary event278 ithd b f l
• 349 completed 36 months or withdrew at study termination without having primary event
• 97 had a primary event• 278 withdrew before early
termination of study 131 required renal
replacement therapy (RRT) 147 withdrew for other
• 271 withdrew before early termination of study 111 required RRT 160 withdrew for other reasons
reasons
Singh AK, et al. N Engl J Med. 2006;355:2085-98.

CHOIR StudySingh AK, et al N Engl J Med. 2006;355(20):2085-2098.g , g ; ( )
Primary Composite End Point30
High hemoglobin group
•N = 1432
20y of
Ev
ent
High-hemoglobin group
10roba
bilit
ym
posi
te E
Low-hemoglobin group
0
PrC
om
00 3 6 9 12 15 18 21 24 27 30 33 36 39
Month• 222 composite events (death MI hospitalization for CHF stroke)• 222 composite events (death, MI, hospitalization for CHF, stroke)
– High-Hb (13.5 g/dL): 125 events (18%)– Low-Hb (11.3 g/dL): 97 events (14%)– Hazard ratio (HR) = 1.34; 95% Confidence Interval (CI), 1.03 to 1.74 (P = 0.03)

CREATE Study
• 603 patients with CKD stage 3 or 4 randomly assigned to 1 of 2 groups:1 of 2 groups:
– Epoetin beta therapy targeted to Hb 13.0-15.0 g/dL– Epoetin beta therapy targeted to Hb 10.5-11.5 g/dL
• Primary endpoint was time to first cardiovascular event
• Secondary endpoints were LVMI, QOL, and progression of CKD
Drüeke TB, et al, for the CREATE Investigators. N Engl J Med. 2006;355(20):2071-2084.

Median Hemoglobin Levels in the Intention-to-Treat Population During the Study
1516
Group 1 (n=301)
(g/d
l)
1314
oglo
bin
1112
G 2 ( 302)
Hem
910 Group 2 (n=302)
08
0 6 12 18 24 30 36 42 48Months
Drüeke, T. et al., N Engl J Med 2006;355:2071-84.
0 6 12 18 24 30 36 42 48

Time to Primary End Point of First Cardiovascular Event
90100
Cardiovascular EventGroup 2 Lower Hb
708090
val (
%)
Group 1 Higher Hb
405060
ee S
urvi
58 events in group 1 vs. 47 events in group 2Hazard ratio 0 78; 95% CI 0 53 to 1 14; P = 0 20
203040
Even
t-Fr Hazard ratio 0.78; 95% CI 0.53 to 1.14; P = 0.20
010
0 6 12 18 24 30 36 42 48
E
0 6 12 18 24 30 36 42 48Month
Drüeke, T. et al., N Engl J Med 2006;355:2071-84.

CREATE Study
• There was no difference between the groups in the primary endpoint LVMI or progression ofthe primary endpoint, LVMI, or progression of CKD
• QOL increased significantly in both groups, but was significantly better in the higher Hb groupwas significantly better in the higher Hb group compared with the lower Hb group at yr 1
Drüeke TB, et al, for the CREATE Investigators. N Engl J Med. 2006;355(20):2071-2084.

Meta-Analysis of CKD Trials
p= 0.031
Phrommintiku, Haas, Elsik, Krum. Lancet 2007; 369:381-388.

FDA Reaction to Safety I f ti ESAInformation on ESAs
• FDA issued warning in late 2006 regarding new risks g g gassociated with use of ESAs
• FDA changed labeling for ESA on March 9, 2007g g
• The use of ESAs may increase the risk for death and for serious cardiovascular events when dosed to achieve a target hemoglobin of >12 g/dL
• FDA recommends using the lowest dose of ESAs that will ggradually raise the hemoglobin concentration to the lowest level sufficient to avoid the need for blood transfusion
FDA Web page. Information for healthcare professionals: erythropoiesis stimulating agents (ESA). Available at: http://www.fda.gov/cder/drug/InfoSheets/HCP/RHE2007HCP.htm. Accessed April 5, 2007.

Black Box Warning for ESAs in CKD
Renal failure: Patients experienced greater risks for death andRenal failure: Patients experienced greater risks for death and serious cardiovascular events when administered erythropoiesis-stimulating agents (ESAs) to target higher versus lower hemoglobin levels (13 5 vs 11 3 g/dL; 14 vs 10 g/dL) in two clinicalhemoglobin levels (13.5 vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Individualize dosing to achieve and maintain hemoglobin levels within the range of 10 to 12 g/dL.
Epogen® PI, Amgen Inc. - August 2008
K/DOQI- 2007 Update of Hb TargetK/DOQI 2007 Update of Hb Target
Adequate Hb
Lower limit of Hb(R d ti )
• In dialysis and nondialysis CKD patients i i ESA th th l t d Hb
Adequate Hb
(Recommendation) receiving ESA therapy, the selected Hbtarget should generally be in the range of 11-12 g/dL
Upper limit of Hb(G id li )
• In dialysis and nondialysis CKD patients receiving ESA therapy the Hb target(Guideline) receiving ESA therapy, the Hb target should not be above 13 g/dL– Strength of evidence = moderate
KDOQI. Am J Kidney Dis. 2007;50:471-530.
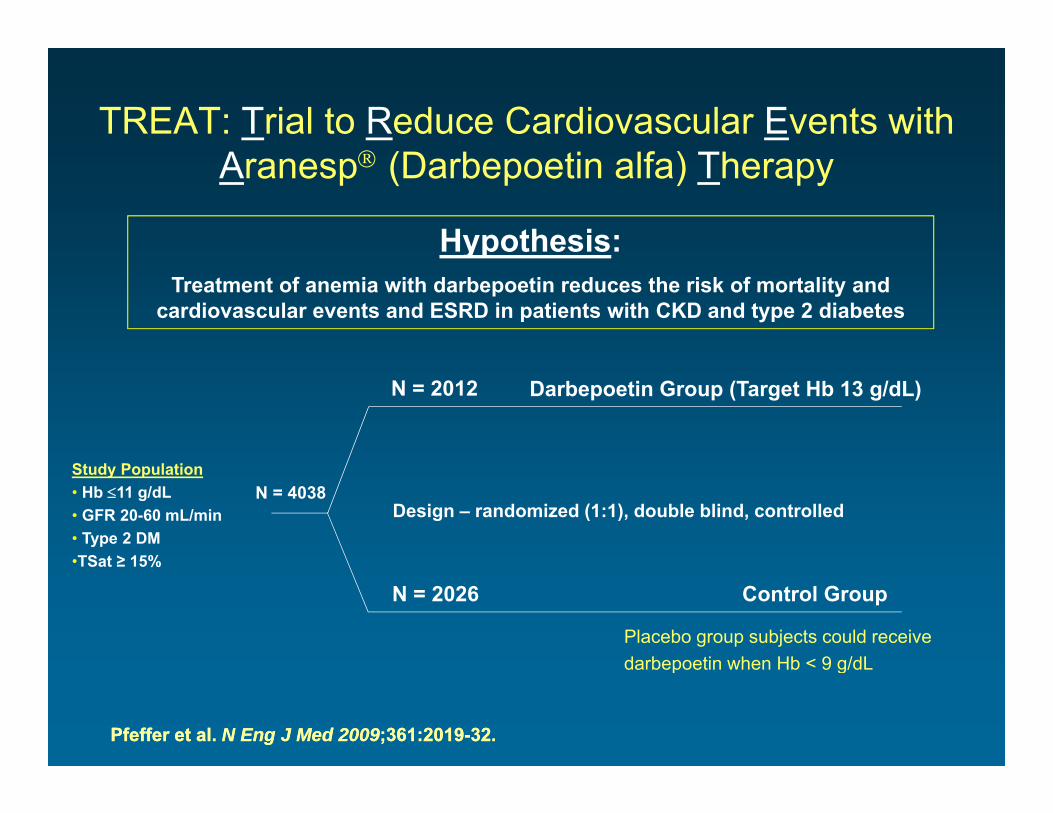
TREAT: Trial to Reduce Cardiovascular Events with Aranesp (Darbepoetin alfa) Therapy
Hypothesis: ypTreatment of anemia with darbepoetin reduces the risk of mortality and
cardiovascular events and ESRD in patients with CKD and type 2 diabetes
Darbepoetin Group (Target Hb 13 g/dL)N = 2012
Study Population• Hb 11 g/dL• GFR 20-60 mL/min• Type 2 DM•TSat ≥ 15%
Design – randomized (1:1), double blind, controlledN = 4038
Control Group•TSat ≥ 15%
N = 2026
Placebo group subjects could receive darbepoetin when Hb < 9 g/dL
PfefferPfeffer et al. et al. N Eng J Med 2009N Eng J Med 2009;361:2019;361:2019--32.32.
darbepoetin when Hb < 9 g/dL

TREAT EndpointsTREAT EndpointsPrimary Endpoints – Time to:
– Composite outcome of death from any cause or a CV event defined as:– Composite outcome of death from any cause or a CV event defined as:• Nonfatal myocardial infarction• Congestive heart failure• Stroke• Hospitalization for myocardial ischemia
– Composite of death or ESRD
Secondary Endpoints – Time to:
• DeathDeath from CV ca ses• Death from CV causes
• Rate of decline in eGFR • Change in patient reported fatigue (FACT-fatigue)
PfefferPfeffer et al. et al. N Eng J Med 2009N Eng J Med 2009;361:2019;361:2019--32.32.

TREAT End Points
PfefferPfeffer et al. et al. N Eng J Med 2009N Eng J Med 2009;361:2019;361:2019--32.32.Median Median HbHb 12.5 (1212.5 (12--12.8) in 12.8) in darbepoetindarbepoetin group; group; 10.6 (9.910.6 (9.9--11.3) in placebo group (p<0.0001).11.3) in placebo group (p<0.0001).

TREATTREAT• TREAT failed to meet its primary objectives of
demonstrating a reduction in all-cause mortality CVdemonstrating a reduction in all cause mortality, CV morbidity, or ESRD and in time to all-cause mortality or ESRD.
• There was an almost two-fold increase in risk of stroke (5% in treatment arm vs 2 6% in placebo arm)(5% in treatment arm vs. 2.6% in placebo arm)
• Among darbepoetin treated subjects with a past history g p j p yof cancer, there were more deaths due to all causes and due to cancer compared with the control group

“FDA Urges Lower Doses of A i D ”Anemia Drugs”
Reported that the FDA "said that three drugs that hadReported that the FDA said that three drugs that had been widely used to treat anemia in both kidney and cancer patients were so dangerous to the heart that doctors should consider avoiding the medicines altogether in some patients and using less of them in others." The FDA "concluded that there were no risk-free doses of Epogen (epoetin alfa), Aranesp (darbepoetin alfa) and Procrit (epoetin alfa), and that doctors should use the medicines only in patients suffering from severeuse the medicines only in patients suffering from severe anemia.
•
New York Times (6/24/2011)

Most Recent Black Box Warning for ESAs in CKDESAs in CKD
Chronic Kidney Disease:Chronic Kidney Disease: • In controlled trials, patients experienced greater risks for death, serious adverse
cardiovascular reactions, and stroke when administered erythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL.
• No trial has identified a hemoglobin target level, ESA dose, or dosing strategy that does not increase these risks.
• Use the lowest Epogen dose sufficient to reduce the need for red blood cell (RBC) transfusions .
Physicians and patients should weigh the possible benefits of decreasing transfusionsagainst the increased risks of death and other serious cardiovascular adverse events.
Epogen® PI , Amgen Inc. – June 2011

Labeling of ESAsLabeling of ESAsFor patients with CKD on dialysis:
• Initiate Epogen treatment when the hemoglobin level is less than 10 g/dLInitiate Epogen treatment when the hemoglobin level is less than 10 g/dL. • If the hemoglobin level approaches or exceeds 11 g/dL, reduce or interrupt the dose
For patients with CKD not on dialysis:
• Consider initiating Epogen treatment only when the hemoglobin level is less than 10 g/dL and the following considerations apply:
The rate of hemoglobin decline indicates the likelihood of requiring a RBC– The rate of hemoglobin decline indicates the likelihood of requiring a RBC transfusion and,
– Reducing the risk of alloimmunization and/or other RBC transfusion-related risks is a goal
• If the hemoglobin level exceeds 10 g/dL, reduce or interrupt the dose of Epogen, and use the lowest dose of Epogen sufficient to reduce the need for RBC transfusions.
Epogen® PI , Amgen Inc. – June 2011

QuestionsQuestions • Are negative outcomes associated with ESAs specifically
Hb l l b th?or Hb level or both?
• What is the Hb level at which QOL is maximixed, yet risk yis minimized?
• Is iron a contributing factor or would increased use beIs iron a contributing factor or would increased use be supported to achieve target Hb without increased use of ESAs?
• What to do with conflicting FDA warnings and K/DOQI anemia guidelines?

Considerations in the Transplant P l iPopulation
• Consider the risk of CV events and stroke inConsider the risk of CV events and stroke in transplant recipients before initiating an ESA
• If blood transfusions are likely to be needed given the decline in Hb consider potential benefit g pof ESAs at low Hb (< 10 g/dL?)
• Until further guidance is available in the transplant population consider recommendations for ESA use in CKD patients not on dialysis

Summary• Anemia of CKD is prevalent in patients post-kidney transplant
and a problem many practitioners will be faced with given the Sincrease in the population with ESRD.
• Iron supplementation and ESAs are essential for treatment of i f CKD h titi d t b i tanemia of CKD; however, practitioners need to be cognizant
of the limitations in using these agents.
• Recent evidence of mortality risk associated with higher Hb in• Recent evidence of mortality risk associated with higher Hb in select populations has raised many questions about the current strategies for anemia management.
• Whether the same risks of ESA use observed in the CKD population apply to kidney transplant patients has not been determined; however, there is enough information on ESAs t j tif ti h ki t t t d i i fto justify caution when making treatment decisions for individuals with anemia post transplant.