Embed Size (px)
Citation preview
Anticoagulation:Focus on DOACs and Reversal
Sara Zochert, Pharm.D., BCPSApril 7, 2015

Objectives
1. Explain the role of direct oral anticoagulants (DOAC).
2. Identify situations where lab monitoring of DOACs is appropriate.
3. Discuss reversal of anticoagulation including reversal agents and lab monitoring.
4. Utilize validated nomograms to determine appropriate re-initiation of anticoagulation.
Anticoagulants
• Warfarin• Dabigatran (Pradaxa)• Rivaroxaban (Xarelto)• Apixaban (Eliquis)• Edoxaban (Savaysa)
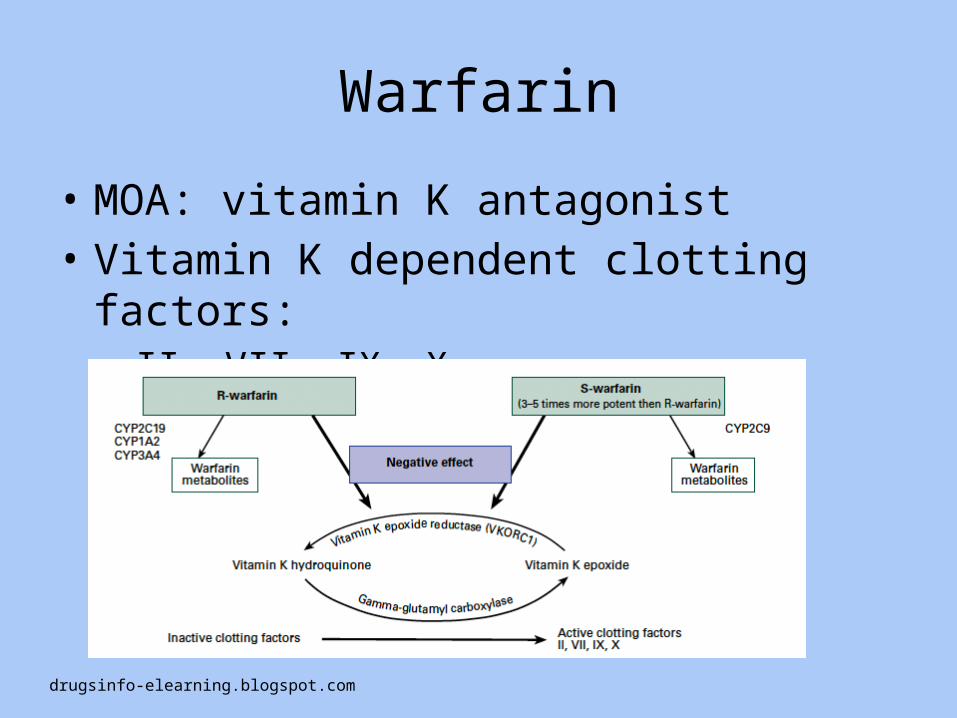
Warfarin
• MOA: vitamin K antagonist• Vitamin K dependent clotting factors:– II, VII, IX, X
drugsinfo-elearning.blogspot.com
Warfarin – Key Points
• Time to effect: 5 days• Long half life: avg. 36-42 hours• Dietary consistency– Vitamin K intake should be the same week to week
• Dosing affected by multiple factors– Gender, age, weight, liver function, diet, disease
states• Drug interactions (prescription and herbal)• INR monitoring requiredAnsell J, et al. CHEST. 2008; 133:160S-198S
Warfarin – INR monitoring
• Goal INR = 2-3• Indications for higher INR goal = 2.5-3.5 – Mechanical mitral valve replacement – Mechanical aortic valve replacement + additional risk
• Risk factors: Age >70, left atrial enlargement, poor left ventricular function, atrial fibrillation
• Indications for lower INR goal = 1.8-2.5– Post-orthopedic procedure– Hx of severe bleeding
Ansell J, et al. CHEST. 2008; 133:160S-198S
Warfarin
• Advantages– Old medication– Reversible– Inexpensive– Only anticoagulant option for heart valve replacements
• Disadvantages– Drug interactions– Food interactions– Lab monitoring– Bleeding
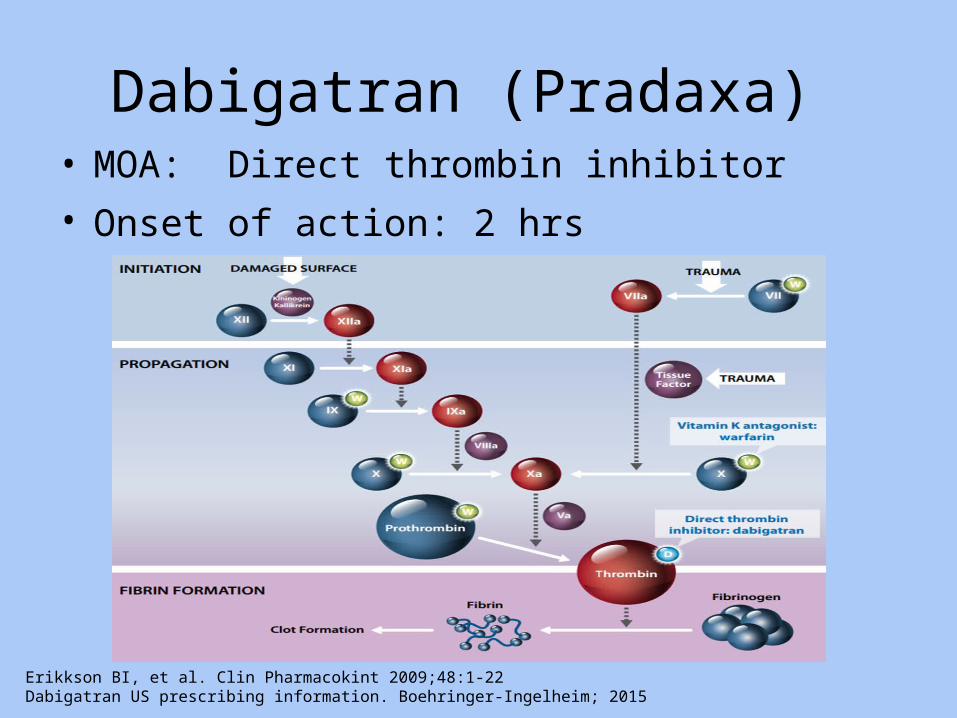
Dabigatran (Pradaxa) • MOA: Direct thrombin inhibitor• Onset of action: 2 hrs
Erikkson BI, et al. Clin Pharmacokint 2009;48:1-22Dabigatran US prescribing information. Boehringer-Ingelheim; 2015

Dabigatran
• Indications/Dose– Nonvalvular atrial fibrillation
• CrCl > 30 ml/min – 150 mg PO BID• CrCl 15-30 ml/min – 75 mg PO BID
– Treatment of VTE after 5-10 days of parenteral therapy• CrCl > 30 ml/min – 150 mg PO BID
– Prevention of recurrent VTE• CrCl > 30 ml/min – 150 mg PO BID
• Drug interactions– Avoid use with P-gp inducers (rifampin)– Reduce to 75 mg BID if CrCl 30-50 ml/min and on dronedarone or
ketoconazole• Dose must be taken at least 6 hours prior to next dose
Dabigatran US prescribing information. Boehringer-Ingelheim; 2015
Dabigatran – Key Points
• Two black box warnings1. Increased risk of thrombosis with discontinuation2. Spinal/epidural hematoma
• Do NOT use in patients with valve replacements– RE-ALIGN terminated early due to increased bleeding and thrombosis
• Superior to warfarin in prevention of CVA/systemic embolism (RE-LY)• Less ICH, but more GI bleeds compared to warfarin (RE-LY)• Most common side effect: Dyspepsia (>15%)• Do NOT open capsules
– Bioavailability increases by 75%– Cannot be administered via tubes
Dabigatran US prescribing information. Boehringer-Ingelheim; 2015Connolly SJ, et al. N Engl J Med 2009;361:1139-51
Dabigatran• Advantages
– Better CVA/systemic embolism prevention– No routine lab monitoring– No food interactions– Fewer drug interactions– Clearance not reduced in moderate hepatic failure– Less ICH
• Disadvantages– Renal dose adjustment– Dyspepsia– More GI bleeds– Not reversible– Cannot use in valve replacement patients
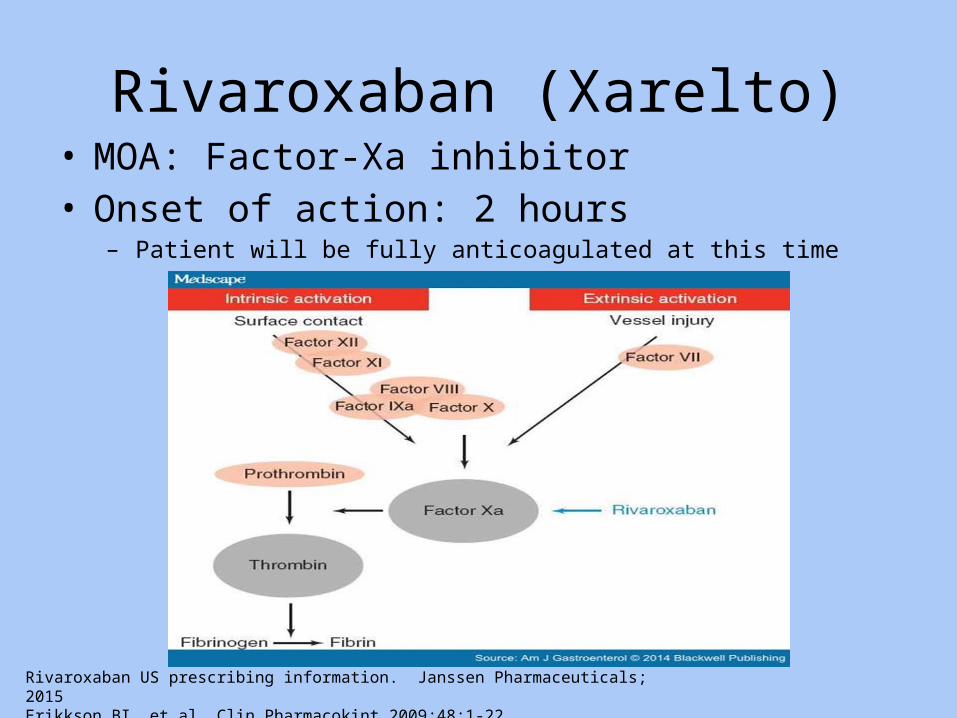
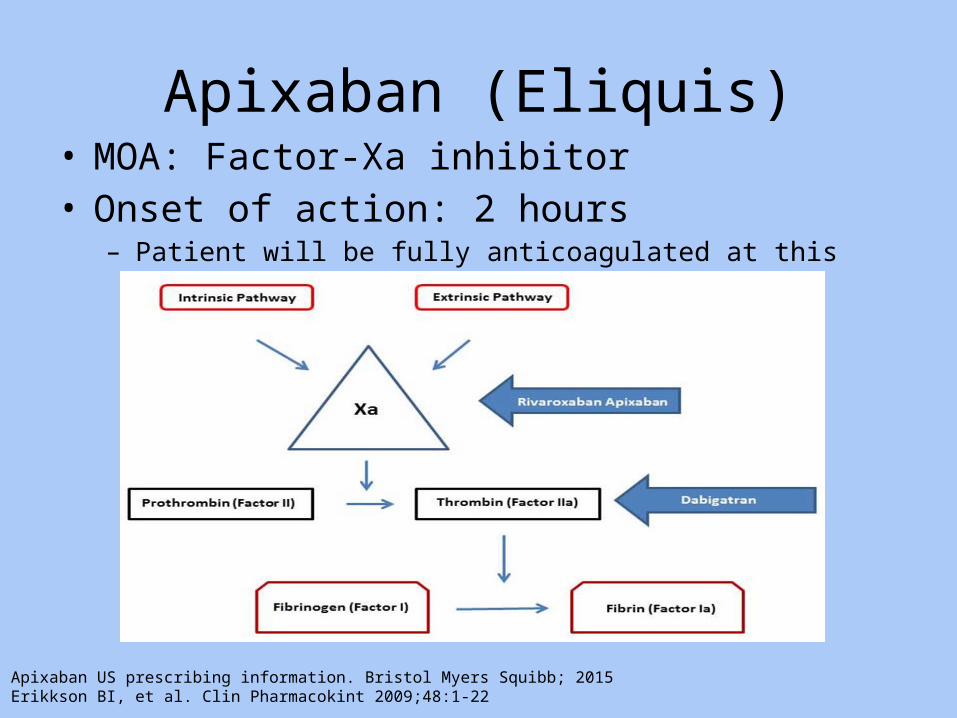
Rivaroxaban (Xarelto)• MOA: Factor-Xa inhibitor• Onset of action: 2 hours
– Patient will be fully anticoagulated at this time
Rivaroxaban US prescribing information. Janssen Pharmaceuticals; 2015Erikkson BI, et al. Clin Pharmacokint 2009;48:1-22
Rivaroxaban• Indications/Dose
– Nonvalvular atrial fibrillation• CrCl > 50 ml/min – 20 mg PO daily with evening meal• CrCl 15-50 ml/min – 15 mg PO daily with evening meal
– Treatment of VTE • 15 mg twice a day (12 hrs apart) with food for 21 days, then change to 20 mg once a day
with food.– During initial treatment patients can take 30 mg at one time, otherwise do not double up on doses
• No data on dosage adjustments for this indication– Prevention of recurrent VTE after 6 months of treatment
• 20 mg PO daily with food• No data on dosage adjustments for this indication
– VTE prophylaxis after knee/hip replacement surgery• CrCl > 30 ml/min – 10 mg PO daily (knees = 12 days, hips = 35 days)
• Drug Interactions: Avoid with strong CYP 3A4 inducers– Carbamazepine, phenytoin, rifampin, St. John’s Wort
Rivaroxaban US prescribing information. Janssen Pharmaceuticals; 2015
Rivaroxaban – Key Points
• Two black box warnings1. Increased risk of thrombosis with discontinuation2. Spinal/epidural hematoma
• Do NOT use in patients with valve replacements• Less ICH, but more GI bleeds (ROCKET-AF)• 15 and 20 mg doses should be given with food
– 10 mg doses can be with or without• Tablet may be crushed and given via gastric tube
– Post-gastric tube lead to decreased absorption• Will cause elevations in INR
– Cannot be used for bridging therapy
Rivaroxaban US prescribing information. Janssen Pharmaceuticals; 2015Patel MR et al. N Engl J Med 2011;365(10):883-891
Rivaroxaban
• Advantages– No lab monitoring– No food interactions– Fewer drug interactions– Less ICH– Once a day dosing
• Disadvantages– Renal dose adjustment– More GI bleeds– Not reversible– Cannot use in valve replacement patients
Apixaban (Eliquis)• MOA: Factor-Xa inhibitor• Onset of action: 2 hours
– Patient will be fully anticoagulated at this time
Apixaban US prescribing information. Bristol Myers Squibb; 2015Erikkson BI, et al. Clin Pharmacokint 2009;48:1-22
Apixaban• Indications/Dose
– Nonvalvular atrial fibrillation• 5 mg PO BID• Reduce to 2.5 mg PO BID if patient has 2 of the following:
– Age ≥ 80 years old– Weight ≤ 60 kg– SCr ≥ 1.5 mg/dL
– Treatment of VTE• 10 mg PO BID x 7 days, then 5 mg PO BID
– Prevention of recurrent VTE after 6 months of treatment• 2.5 mg PO BID
– VTE prophylaxis after knee/hip replacement surgery • 2.5 mg PO BID (knees = 12 days, hips = 35 days)
• Drug interactions– Reduce dose by 50% for patients taking strong dual inhibitors of CYP 3A4 and P-gp
• Ketoconazole, itraconazole, ritonavir, clarithromycin
– Avoid with strong CYP 3A4 inducers• Carbamazepine, phenytoin, rifampin, St. John’s Wort
• Do not double up on doses!Apixaban US prescribing information. Bristol Myers Squibb; 2015
Apixaban – Key Points
• Two black box warnings1. Increased risk of thrombosis with discontinuation2. Spinal/epidural hematoma
• Do NOT use in patients with valve replacements• Less major and non-major bleeding (ARISTOLE)• Superior to warfarin in prevention of CVA/systemic
embolism (ARISTOLE)• Tablet may be crushed and given via gastric tube, no data
on giving orally after crushing• Will cause elevations in INR
– Cannot be used for bridging therapyApixaban US prescribing information. Bristol Myers Squibb; 2015Granger C, et al. N Engl J Med 2011;365:981-92
Apixaban
• Advantages– No lab monitoring– No food interactions– Fewer drug interactions– Less bleeding– Better CVA/systemic embolism prevention
• Disadvantages– Dose adjustment non-traditional– Not reversible– Cannot use in valve replacement patients
Edoxaban (Savaysa)• Newly approved January 2015• Very similar to rivaroxaban and apixaban• Third black box warning
– Reduced efficacy with CrCl ≥ 95 ml/min• Indications/Dose
– Nonvalvular atrial fibrillation• CrCl 50-95 ml/min – 60 mg PO daily• CrCl 15-50 ml/min, less than 60 kg – 30 mg PO daily
– Treatment of VTE after 5-10 days of parenteral therapy • Same
• Less major bleeding, more GI bleeds (ENGAGE AF TIMI 48)• No data on crushing tablets• No data on reversal or lab monitoring
Edoxaban US prescribing information. Dalichi Sankyo; 2015Giugliano RP, et al. N Eng J Med 2013;369:2093-104
Direct Oral Anticoagulants (DOACs)
• Little data using with dual antiplatelet therapy (DAPT)– APPRAISE-2 trial (apixaban) terminated early due to increased bleeding
• Not well studied in patients receiving lytic therapy• Non-steroidal anti-inflammatory drugs (NSAIDs) should be
avoided due to increased bleeding risks• More GI bleeds than warfarin, except apixaban• Great option for patients without renal disease or valve
replacements• No routine lab monitoring required
– Bleeding, obesity, low body weight, borderline renal function
• No specific antidote availableDabigatran US prescribing information. Boehringer-Ingelheim; 2015Rivaroxaban US prescribing information. Janssen Pharmaceuticals; 2015Apixaban US prescribing information. Bristol Myers Squibb; 2015Edoxaban US prescribing information. Dalichi Sankyo; 2015
Management of bleeding
• Supportive– Fluid Resuscitation– PRBC transfusion– Maintenance of renal function
• DOACs are renally eliminated
– Identification of bleeding source– Mechanical compression– Surgical intervention– Activated charcoal
• Only useful for DOAC, if administered within the last 2 hours
• Reversal– Specific based on anticoagulant
Reversal of Anticoagulation
• Indications– Severe bleeding– Emergent/urgent procedures
• Minor bleeding/elevated INRs– Supportive– Hold doses
CHEST 2012; 141(2)(Suppl);e152S-e184S
Reversal - Warfarin
• Lab monitoring– PT/INR

Reversal - Warfarin
• Vitamin K (phytonadione)– Dose: 1-10 mg
• Usually not repeated, unless first dose was too low
– Route: • SubQ: Only for patients that are strict NPO due to slower absorption• IV: preferred method for active bleeding, emergent reversal
– Fastest– Adults high risk of anaphylaxis
• PO: 5 mg tablets, or give IV product orally
– Onset of action: 4-12 hrs IV, 12-24 hrs PO– Duration of action: Full effect in 24-48 hours– Warfarin resistance: Yes, dose dependent
Whitling AM. Arch Intern Med 1998; 158:2136-2140
Reversal - Warfarin
• Fresh Frozen Plasma (FFP)– Dose: 15 ml/kg (usually) 2-4 units
• May be repeated as needed
– Onset of action: 1-4 hrs, depending INR– Duration of action: 6 hours or less– Warfarin resistance: No
• Advantages– Rapid acting, no warfarin resistance
• Disadvantages– Short acting, risk of transfusion related reaction, requires
thawing, type and cross, INR will re-increase (if no Vitamin K given), fluid limiting
Holbrook A. CHEST 2012; 141(2)(Suppl);e152S-e184S
Reversal - Warfarin• Prothrombin complex concentrate (PCC)
– Kcentra: (II, VII, XI, X and Protein C and S) - FDA approval for reversal– Dose: Based on INR, one time only
• INR = 2 to <4: 25 IU of factor IX/kg IV, max 2500 IU• INR = 4 to 6: 35 IU of factor IX/kg IV, max 3500 IU• INR > 6: 50 IU of factor IX/kg IV, max 5000 IU• Administer slow IV push, max of 8.4 ml/minute
– Onset of action: 10 – 15 minutes– Duration of action: 12 or more hours– Warfarin resistance: No
• Advantages– Rapid acting, less fluid
• Disadvantages– Short duration, risk of thrombosis, cannot use in HIT patients, expensive, IV room
compounding, risk of transmissible infectious agents• MUST be given with Vitamin K!
Kcentra US prescribing information. CSL Behring; 2013
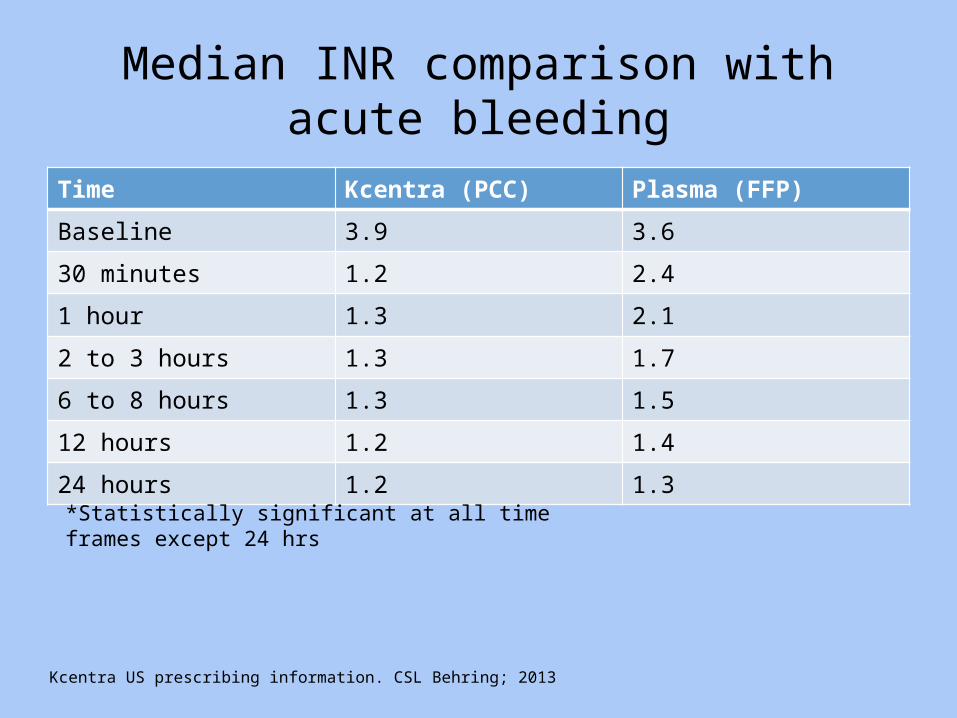
Median INR comparison with acute bleeding
Time Kcentra (PCC) Plasma (FFP)
Baseline 3.9 3.6
30 minutes 1.2 2.4
1 hour 1.3 2.1
2 to 3 hours 1.3 1.7
6 to 8 hours 1.3 1.5
12 hours 1.2 1.4
24 hours 1.2 1.3
*Statistically significant at all time frames except 24 hrs
Kcentra US prescribing information. CSL Behring; 2013
Reversal – Dabigatran (Pradaxa)
• Lab monitoring– Ecarin clotting time (ECT, dabigatran level)• No established therapeutic range
– Activated partial thromboplastin time (aPTT)• 1.5-2 x normal
– Thrombin Time
Kaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.UW Medicine alternative monitoring for antithrombotic agents. depts.washington.edu/anticoag/home
Reversal - Dabigatran
• Hemodialysis– 80% renally eliminated – Preferred method for emergent bleeding– Not an option for rivaroxaban or apixaban
• 60% of the drug will be removed during a 2-3 hour session
• May need continued therapy as drug re-distributes out of the tissues
• Check ECT/aPTT 1-2 hrs after dialysis is completed• May administer aPCC – immediately prior to placing line
Kaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.
Reversal - Dabigatran
• aPCC – First line therapy – FEIBA NF (activated factor VII, inactivated II, IX, X)
• Dose: 25 units/kg slow IV push at max rate of 2 units/kg/minute (over 15 minutes)– May repeat if needed
• Onset of action: 12 hours• Duration of action: 36 to 72 hours• Advantages
– Best option we have
• Disadvantages– Thrombosis risk, little data to support use, expensive, IV room
compounding, transmission of infectious agents Kaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.
Reversal - Dabigatran
• Recombinant active factor VIIa – Second line therapy– NovoSeven
• Dose: 20-40 mcg/kg slow IV push over 2-5 minutes– May repeat if needed
• Onset of action: 10-20 minutes• Duration of action: 4-6 hours• Advantages
– Feel like we are “doing something”
• Disadvantages– Increased risk of arterial thrombosis, no human studies available,
expense, IV room compoundingKaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.
Reversal – Rivaroxaban (Xarelto)
• Lab monitoring– Anti-factor Xa activity level (Rivaroxaban level)• No established therapeutic range
– Prothrombin Time (PT)– Activated partial thromboplastin time (aPTT)• PT is more sensitive
Kaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39. UW Medicine alternative monitoring for antithrombotic agents. depts.washington.edu/anticoag/home
Reversal - Rivaroxaban
• PCC – First line therapy– Kcentra (factor II, VII, IX, X and protein C and S)• Dose: 25 units/kg slow IV push, 8.4 ml/min
– May repeat if needed
• Onset of action: 10-15 minutes• Duration of action: 12 hours or more• Advantages
– Best option we have
• Disadvantages– Increased risk of thrombosis, lack of data, expense, IV room
compoundingKaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.
Reversal - Rivaroxaban
• Recombinant active factor VIIa – Second line therapy– NovoSeven
• Dose: 20-40 mcg/kg slow IV push over 2-5 minutes– May repeat if needed
• Onset of action: 10-20 minutes• Duration of action: 4-6 hours• Advantages
– Feel like we are “doing something”
• Disadvantages– Increased risk of arterial thrombosis, no human studies available,
expense, IV room compoundingKaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39.
Reversal – Apixaban (Eliquis)
• Lab monitoring– Anti-factor Xa activity level
• Special calibration compared to heparin, enoxaparin, rivaroxaban• No established therapeutic range
– Observed peak levels of 59-321 ng/ml (5 mg BID)
– PT – aPTT– Chromogenic anti-Xa assay• If available
Kaatz S, et.al. Am J Hematol. 87:S141-145, 2012 Miyares MA, et al. Am J Health- Syst Pharm. 2012;69:e28-39. Nutescu EA, et al. Am J Health-Syst Pharm. 2013;70:19914-29UW Medicine alternative monitoring for antithrombotic agents. depts.washington.edu/anticoag/home
Reversal - Apixaban
• See rivaroxaban reversal• PCC– KCentra
• NovoSeven
Current research
• Andexanet alfa– Anti-Xa inhibitor antidote– Phase III trials• 33 older healthy patients given apixaban 5 mg PO BID x
4 days• Randomized to andexanet alfa or placebo• Immediate and significant reversal shown
– FDA breakthrough therapy medication– Accelerated application submission expected end
of 2015Moll S. Updates of Antidotes for NOAC. Medpagetoday.com 11/10/14
Current research
• Aripazine– Binds to anticoagulants– Effective against• Heparin, LMWH, and all 4 DOAC
– Currently in Phase 1 trials• Patients given 1 dose of edoxaban, then aripazine• Reversal to within 10% of baseline 10 minutes after
administration
Moll S. Updates of Antidotes for NOAC. Medpagetoday.com 11/10/14

Current research
• Idarucizumab– Monoclonal antibody– Targets dabigatran• 3 phase I studies completed• Phase III study of patients with major bleeding or
needing emergent reversal is ongoing
Moll S. Updates of Antidotes for NOAC. Medpagetoday.com 11/10/14

Reversal SuggestionsMethod Dabigatran Rivaroxaban Apixaban
Oral activated charcoal
Yes Yes Yes
Hemodialysis Yes No No
FFP No No No
rFVIIa (NovoSeven) Unclear Unclear Unclear
3-factor PCC (Profilnine)
Unclear Unclear Unclear
4-factor PCC (Kcentra)
Unclear Possible Possible
Activated PCC (FEIBA)
Possible Possible Possible
Modified from Kaatz S, et al. Am J Hematol 2012; 87:S141-S145

Lab monitoringLab Dabigatran Rivaroxaban Apixaban
ECT Yes (best option) No No
aPTT Yes Yes Yes
TT Yes No No
INR/PT Yes Yes Yes
Anti-Xa activity No Yes (best option) Yes
Chromogenic anti-Xa assay(not widely available)
No Yes Yes
Diluted TT(not widely available)
Yes No No
Nutescu EA, et al. Am J Health-Syst Pharm 2013;70:1914-29
Resuming Anticoagulation
• Always a balance of:– Risk of thrombosis– Risk of bleeding
Risk factors for thrombosis
• Surgery• Trauma• Immobility• Malignancy• Cancer therapy• Venous compression• Previous VTE• Increased age• Pregnancy/Post-partum• Nephrotic syndrome• Acute medical illness
• Estrogen medications• Estrogen receptor
modulators• Erythropoiesis stimulating
agents• Inflammatory bowel disease• Myeloproliferative disorders• Central venous
catheterization• Thrombophilia
CHEST 2012; 141(2) (Suppl):e195S-e226S
Assessing Thrombosis Risk
• CHEST guidelines• CHADS2 score• CHADS2 – VASc score
CHEST guidelineHigh Risk for Thromboembolism Moderate Risk for
ThromboembolismLow risk for Thromboembolism
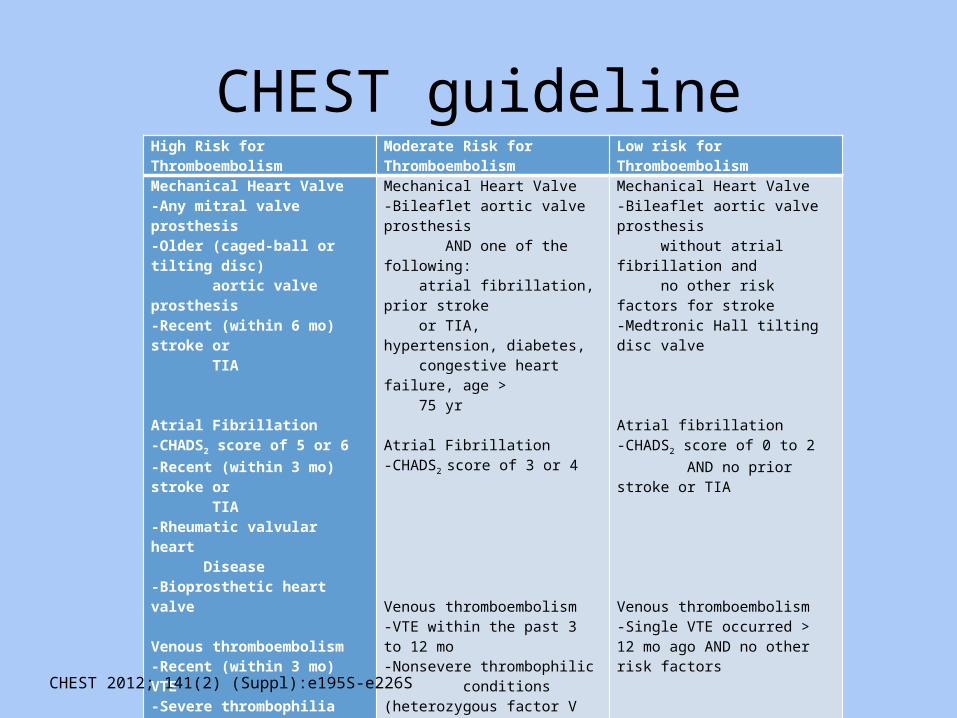
Mechanical Heart Valve-Any mitral valve prosthesis-Older (caged-ball or tilting disc) aortic valve prosthesis-Recent (within 6 mo) stroke or TIA Atrial Fibrillation-CHADS2 score of 5 or 6-Recent (within 3 mo) stroke or TIA-Rheumatic valvular heart Disease-Bioprosthetic heart valve Venous thromboembolism-Recent (within 3 mo) VTE-Severe thrombophilia (deficiency of protein C, protein S or antithrombin, antiphospholipid antibioties, or multiple abnormalities)
Mechanical Heart Valve-Bileaflet aortic valve prosthesis AND one of the following: atrial fibrillation, prior stroke or TIA, hypertension, diabetes, congestive heart failure, age > 75 yr Atrial Fibrillation-CHADS2 score of 3 or 4 Venous thromboembolism-VTE within the past 3 to 12 mo-Nonsevere thrombophilic conditions (heterozygous factor V Leiden mutation, heterozgyous factor II mutation)-Recurrent VTE-Active cancer (treated within 6 mo or palliative)
Mechanical Heart Valve-Bileaflet aortic valve prosthesis without atrial fibrillation and no other risk factors for stroke-Medtronic Hall tilting disc valve Atrial fibrillation-CHADS2 score of 0 to 2 AND no prior stroke or TIA Venous thromboembolism-Single VTE occurred > 12 mo ago AND no other risk factors
CHEST 2012; 141(2) (Suppl):e195S-e226S
Thrombosis Risk – Valve Replacements
• Type of valve– Mechanical > bioprosthetic
• Location of valve– Mitral > Aortic
• Additional risk factors– Multiple valves– Age > 70 yo– Atrial fibrillation– Left atrial enlargement– Left ventricle dysfunction– Hx of embolism
CHEST 2012; 141(2) (Suppl):e195S-e226S
Thrombosis Risk – Venous Thromboembolism
• Timing of clot– Highest risk in the first the 3 months– Decrease in risk after 1 year
• Location of clot– Pulmonary embolism > Deep vein thrombosis• Proximal > distal
• Number of clots– Bilateral > single side– Recurrent
CHEST 2012; 141(2) (Suppl):e195S-e226S
Thrombosis Risk – Atrial Fibrillation
• CHADS2 score– C = Congestive Heart Failure (or EF < 30%)– H = Hypertension– A = Age (≥ 75 year old)– D = Diabetes Mellitus– S = Stroke/TIA • Counts as 2 points
• High Risk = 5 or 6, Moderate Risk = 3 or 4, Low risk 0 to 2
Gage BF, et al. JAMA 2001 285: 2864-2870
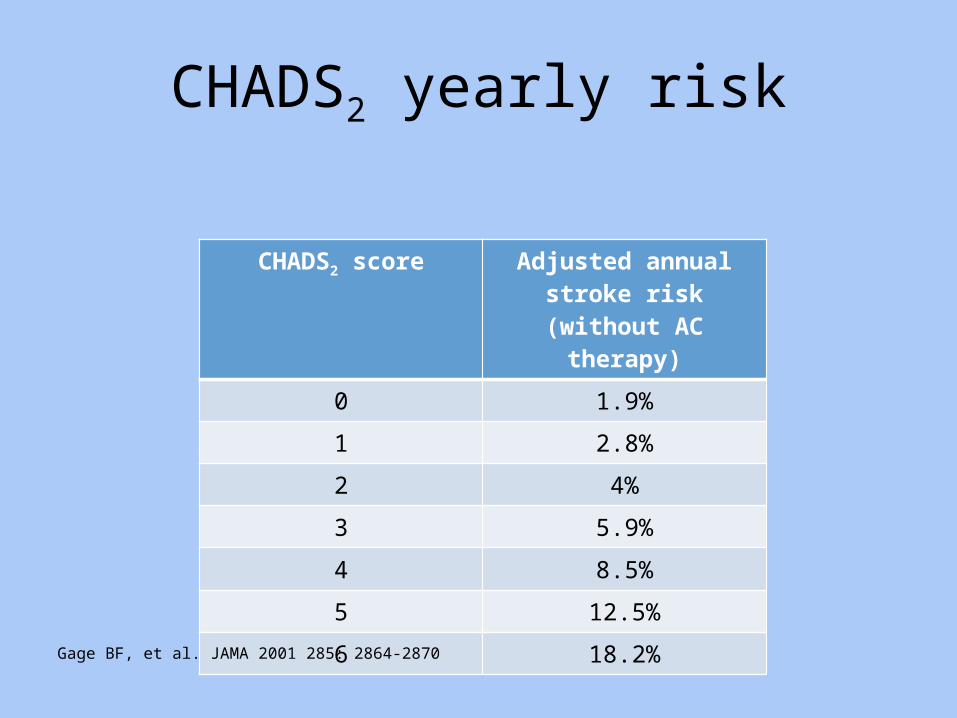
CHADS2 yearly risk
CHADS2 score Adjusted annual stroke risk (without AC therapy)
0 1.9%
1 2.8%
2 4%
3 5.9%
4 8.5%
5 12.5%
6 18.2%
Gage BF, et al. JAMA 2001 285: 2864-2870
Thrombosis Risk – Atrial Fibrillation
• CHADS2-VASc score– C = Congestive Heart Failure (or EF < 30%)– H = Hypertension– A = Age (> 75 years old)– D = Diabetes Mellitus– S = Stroke/TIA
• Counts as 2
– V = Vascular disease– A = Age (65-74)– S = Sex
• Female = 1 point
• High risk = 7 to 9, Moderate risk = 4 to 6, Low risk = 0 to 3
Lip GY et al. Chest 2010; 137: 263-72
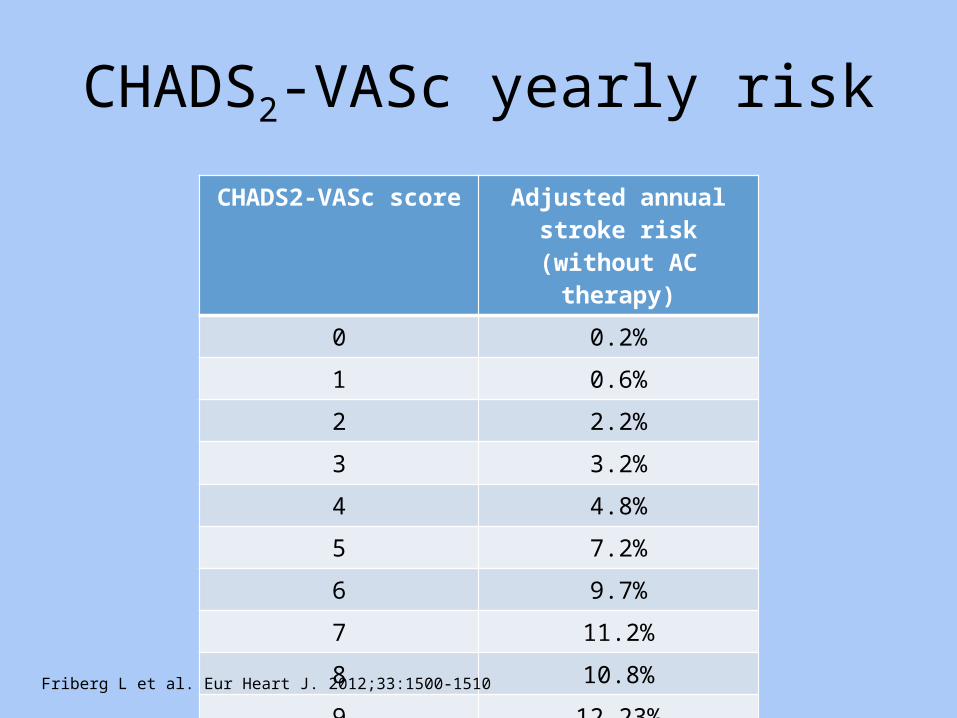
CHADS2-VASc yearly risk
CHADS2-VASc score Adjusted annual stroke risk (without AC therapy)
0 0.2%
1 0.6%
2 2.2%
3 3.2%
4 4.8%
5 7.2%
6 9.7%
7 11.2%
8 10.8%
9 12.23%
Friberg L et al. Eur Heart J. 2012;33:1500-1510
Risk factors for bleeding
• Hepatic disease• Renal disease• Alcoholism• Malignancy • Age > 70• Reduced platelet
count/function• Previous bleeding• Uncontrolled hypertension• Excessive fall risk
• Concurrent medications– Antiplatelets– NSAIDs– Heparin/LMWH– IIb/IIIa inhibitors
• Recent thrombolytic use• Recent invasive
procedure• Anemia• Stroke
CHEST 2012; 141(2)(Suppl):e44S-e88S
Bleeding Risk
• HAS-BLED score– H = hypertension, SBP > 160 mmHg– A = abnormal renal or liver function
• 1 point each
– S = stroke– B = bleeding history or predisposition– L = labile INRs– E = elderly ≥ 65 yo– D = drugs/alcohol
• Antiplatelets/NSAIDs• Alcohol use > 8 servings/week
Pisters R, et al. Chest.2010;138:1093-1100.
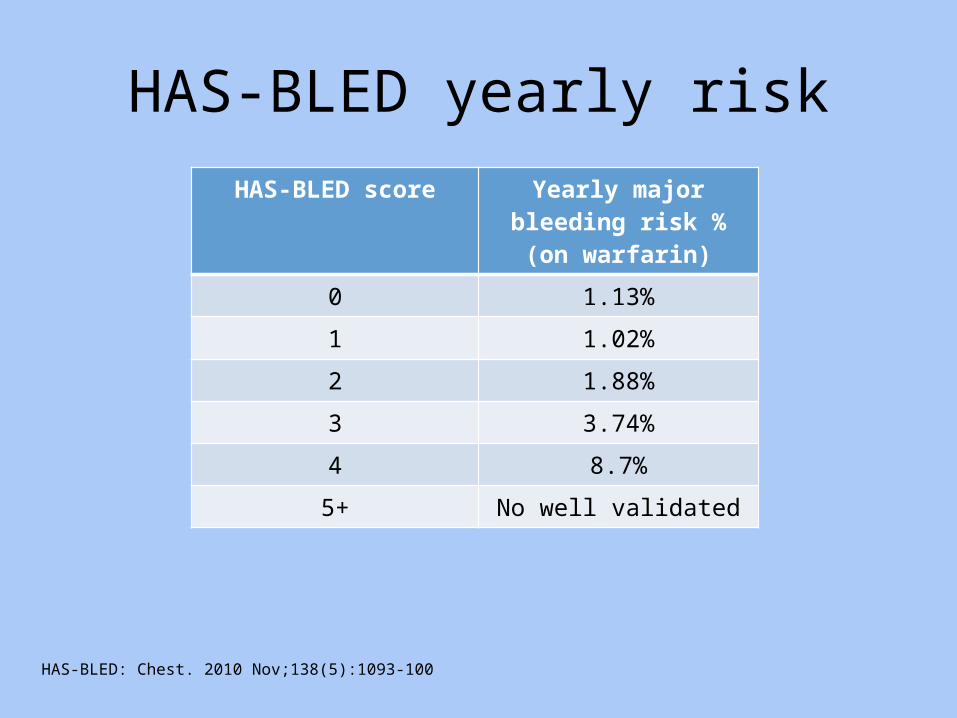
HAS-BLED yearly riskHAS-BLED score Yearly major bleeding risk
% (on warfarin)0 1.13%
1 1.02%
2 1.88%
3 3.74%
4 8.7%
5+ No well validated
HAS-BLED: Chest. 2010 Nov;138(5):1093-100
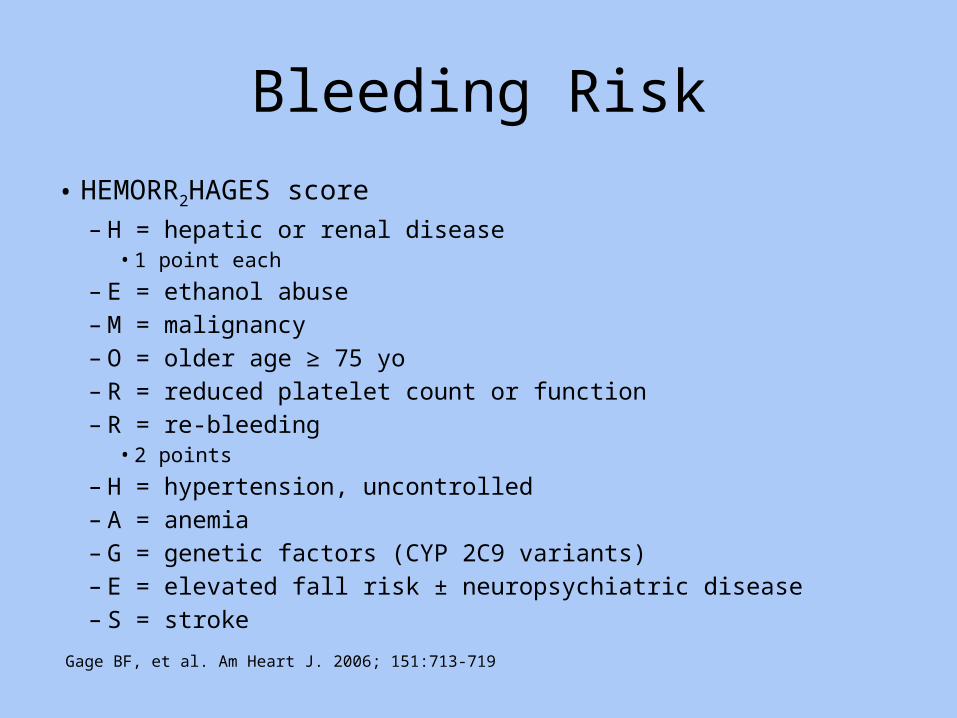
Bleeding Risk
• HEMORR2HAGES score– H = hepatic or renal disease
• 1 point each
– E = ethanol abuse– M = malignancy– O = older age ≥ 75 yo– R = reduced platelet count or function– R = re-bleeding
• 2 points
– H = hypertension, uncontrolled– A = anemia– G = genetic factors (CYP 2C9 variants)– E = elevated fall risk ± neuropsychiatric disease– S = stroke
Gage BF, et al. Am Heart J. 2006; 151:713-719
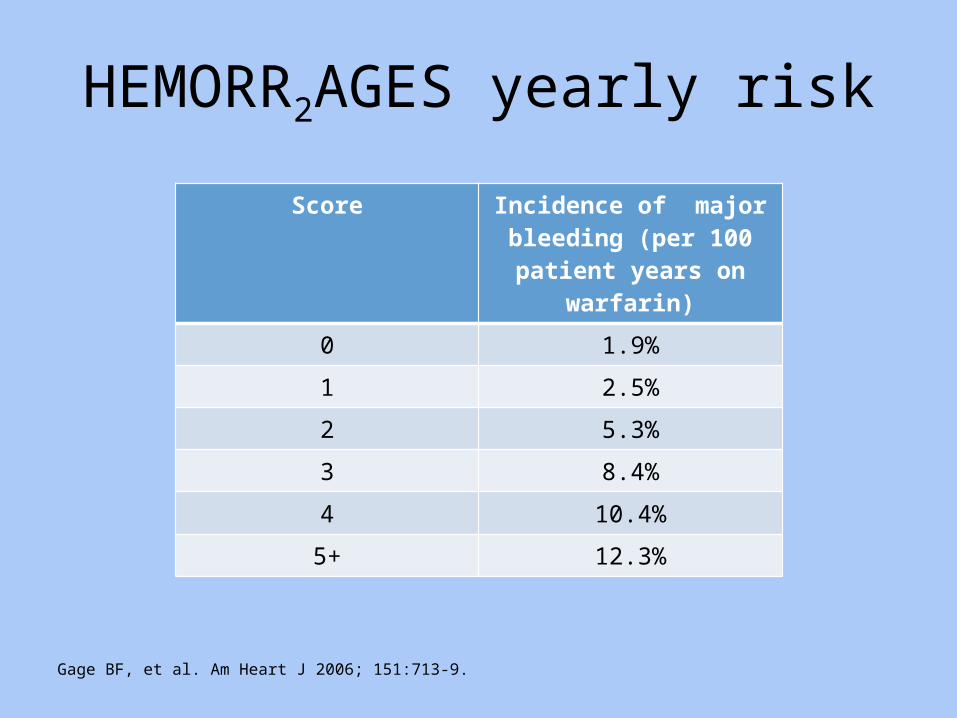
HEMORR2AGES yearly risk
Score Incidence of major bleeding (per 100 patient years on
warfarin)0 1.9%
1 2.5%
2 5.3%
3 8.4%
4 10.4%
5+ 12.3%
Gage BF, et al. Am Heart J 2006; 151:713-9.

Bleeding Risk
• AnTicoagulation and Risk factors In Atrial Fibrillation (ATRIA) score– Anemia = 3 points• Hgb < 13 for males, < 12 for females
– Severe renal disease = 3 points• GFR ≤ 30 ml/min or dialysis dependent
– Age ≥ 75 yo = 2 points– Any prior hemorrhage = 1 point– Hypertension history = 1 point
Fang, MC, et al. J Am Coll Cardiol. 2011;58:395-401http://www.mdcalc.com/atria-bleeding-risk-score/

ATRIA yearly riskAtria score Yearly major bleeding risk % (on warfarin)
0 1.09%
Low risk, 0.76%1 1.97%
2 2.44%
3 1.92%
4 9.13% Intermediate risk, 2.6%
5+ 6.45% High risk, 5.8%
http://www.mdcalc.com/atria-bleeding-risk-score/Roldan V, et al. CHEST 2013; 143(1):179–184

Patient Case
• Pt. admitted to hospital for evaluation of GI bleed after having blood in the stool for 2 days prior to admission.
• EGD and colonoscopy did not reveal a source of bleeding
• CHADS2 score = 5 and HAS-BLED score = 2• Should patient be re-started on anticoagulant
therapy?
GI bleeds
• Many patients will resume anticoagulation– Weigh risk of thrombosis vs. bleeding
• Consider waiting 7 days to resume• Consider starting heparin gtt first• Stop antiplatelets and NSAIDs if able• Change DOACs to warfarin due to less GI
bleeds– Apixaban is an exception
Witt DM, et al. Arch internal Med, 2012; 172(19):1484-1491Qureshi W, et al. Am J Cardiol 2014;113:662-668
Intracranial Hemorrhage (ICH)
• Data only available with warfarin and all retrospective• Goals in the first 4 hours
– INR less than 1.3– SBP less than 160 mmHg– Patients that met these goals had the best outcomes
• Location and size matter– Intraventricular involvement and large hematoma size have a poor prognosis– Deep hemispheric strokes (basal ganglia, thalamus, pons, or cerebellum)
• Associated with chronic arterial hypertension, consider resuming anticoagulation• 1 year risk of recurrence = 2.1%
– Superficial/lobular hemorrhages (frontal, parietal, temporal, occipital lobes)• Poor restart candidates• 1 year risk of recurrence = 15%
• Weigh risk of thrombosis vs. risk of recurrenceHart RG, et al. Stroke 2005;36:1588-1593Paciaroni M, et al. Thrombosis and Haemostasis 111(2014):14/18
Resuming after ICH
• High thrombosis risk patients should resume anticoagulation• Traumatic ICH may be lower recurrence risk• Imaging to rule out expansion is helpful• Control blood pressure• Consider starting heparin gtt first• Stop antiplatelets and NSAIDs if able• Change warfarin to DOAC due to less ICH• Optimal time to resume unknown
– 10 to 30 weeks in 1 study, 30 days in another• Ask the patient
Paciaroni M, et al. Thrombosis and Haemostasis 111(2014):14/18Majeed, et al. Stroke 2010;41:2860-2866Hart RG, et al. Stroke 2005;36:1588-1593
Resuming Anticoagulation
• Atrial fibrillation patients– Use nomograms
• Valve replacements– Mechanical – resume– Bioprosthetic – based on risk assessment
• Venous thromboembolism– Within 3 months or recurrent – resume– 3 months to 1 year – based on risk assessment– More than 1 year – likely stop anticoagulation
• These are all generalizations and each patient should be evaluated for thrombosis and bleeding risk factors!
Questions?





























