Embed Size (px)
Citation preview
This article was downloaded by: [Heriot-Watt University]On: 07 October 2014, At: 12:22Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number:1072954 Registered office: Mortimer House, 37-41 MortimerStreet, London W1T 3JH, UK
NeuropsychologicalRehabilitation: AnInternational JournalPublication details, including instructionsfor authors and subscription information:http://www.tandfonline.com/loi/pnrh20
From theory to therapyin aphasia: Where arewe now and where tonext?Wendy Best & Lyndsey NickelsPublished online: 22 Sep 2010.
To cite this article: Wendy Best & Lyndsey Nickels (2000) Fromtheory to therapy in aphasia: Where are we now and where to next?,Neuropsychological Rehabilitation: An International Journal, 10:3,231-247, DOI: 10.1080/096020100389147
To link to this article: http://dx.doi.org/10.1080/096020100389147
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy ofall the information (the “Content”) contained in the publicationson our platform. However, Taylor & Francis, our agents, and ourlicensors make no representations or warranties whatsoever asto the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publicationare the opinions and views of the authors, and are not the viewsof or endorsed by Taylor & Francis. The accuracy of the Content
should not be relied upon and should be independently verifiedwith primary sources of information. Taylor and Francis shall notbe liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with,in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and privatestudy purposes. Any substantial or systematic reproduction,redistribution, reselling, loan, sub-licensing, systematic supply,or distribution in any form to anyone is expressly forbidden.Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4

From theory to therapy in aphasia:Where are we now and where to next?
Wendy Best1 and Lyndsey Nickels1,2
1Birkbeck College, University of London, UK and2Macquarie University, Sydney, Australia
Language therapy for acquired aphasia has come under much scrutiny in recentyears, with debate focusing on whether or not it is effective and how best efficacycan be measured. In this paper, we argue that although the efficacy of manydifferent therapies has been clearly documented, there remain unanswered ques-tions. In particular, it is still difficult to predict which therapeutic task or approachwill be successful at remediating which particular disorders. We argue that this isparticularly true in the rehabilitation of anomia, whilst in other areas (e.g.,reading) the relationship between deficit, task, and outcome is easier to interpret.We discuss in detail the reasons for these differences arguing that specificity oftheoretical models, complexity of therapeutic tasks, and a lack of (reporting of)comprehensive assessment of linguistic deficits all contribute to the problem. Weconclude that research needs to perform a microanalysis of the interactionsbetween tasks and deficits.
INTRODUCTION
Language therapy for acquired aphasia has a long history (Howard & Hatfield,1987). The techniques used have been many and varied and some are still in usetoday. There has been much debate over the past few decades about whether or
Requests for reprints should be sent to Wendy Best, Department of Psychology, BirkbeckCollege, Malet Street, London WC1E 7HX (e-mail: [email protected]) or Lyndsey Nickels,Psychology Department, Macquarie University, Sydney, NSW 2109, Australia (e-mail:[email protected]).
We would like to acknowledge the help of RD, MF, JOW and PG and to thank them and theirrelatives for enthusiastic participation in the project. David Howard, Carolyn Bruce, and ClaireGatehouse were involved in the research with the computerised aid which was funded by the MRCand the Stroke Association. We would also like to thank the reviewers for helpful comments on anearlier draft. David Howard carried out the statistical analysis of the data for the study. LyndseyNickels was funded by a Wellcome Trust Fellowship during the preparation of this paper.
NEUROPSYCHOLOGICAL REHABILITATION, 2000, 10 (3), 231–247
Ó 2000 Psychology Press Ltdhttp://www.tandf.co.uk/journals/pp/09602011.html
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
not therapy for aphasia is effective. However, as Howard (1986) argues, thisquestion is inappropriate and probably unanswerable. Rather, we need toconsider whether a particular therapy can be shown to be effective inremediating an individual person’s aphasia (or aspect of that aphasia). Therehave now been many reports, published within a cognitive neuropsychologicalframework, that show just that—a specific therapy task results in a clearimprovement of a particular skill. For example, Hillis and Caramazza (1994)showed that matching a written word to the correct picture (from a large array)improved the ability of JJ, a person with aphasia, to find the names of pictures.Similiarly, De Partz (1986) showed that reteaching of the correspondencebetween letters and their realisation as sounds improved the reading ability ofSP (with acquired dyslexia). In this paper we use “efficacy” in this limitedsense of demonstrable improvement on a specific task, although generalisationto natural communication is obviously crucial.
Which therapy for which problem?
A key aim of research into the treatment of aphasic language is to be able todetermine which therapy is most appropriate to remediate which particularlanguage deficit. In other words if an aphasic person presents with problem X,then treatment Y is the most appropriate and this will produce result Z.
1How far
have we progressed towards this goal? We will take examples from twodifferent areas of language processing—disorders of word production(anomia) and disorders of reading (acquired dyslexia).
First, in the case of anomia, it has been clearly demonstrated that severaldifferent tasks can improve naming for some aphasic people (e.g., word–picture matching, Marshall, Pound, White-Thompson, & Pring, 1990; readingaloud, Miceli, Amitrano, Capasso, & Caramazza, 1996). Is it possible to predictwhich people with which levels of breakdown in word production (for a modelof speech production see, for example, Butterworth, 1989) will benefit from aparticular therapy task? Nickels and Best (1996a,b) addressed precisely thisissue, focusing particularly on word–picture matching. They found that fromthe (published) results of research, it was difficult to draw any clear con-clusions. There were anomic people who appeared to have similar levels ofbreakdown (e.g., lexical–semantic deficits) but yet responded differently totherapy. They conclude that “it is still not clear exactly how the treatments areworking, and how they relate to levels of deficit” (1996b, p. 134).
232 BEST AND NICKELS
1 Of course, we acknowledge that in clinical practice it is both the deficits and the areas ofrelative strength that are taken into account. However, in published research this is often over-looked with the emphasis being placed on the impairment(s).
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
The contrasts with the apparently clear findings from the remediation ofacquired surface dyslexia. Weekes and Coltheart (1996) have recently reporteda treatment study involving NW, a person with acquired dyslexia (specificallysurface dyslexia). NW’s difficulty in reading irregularly spelled words (e.g.,yacht, colonel, pint) was identified as being due to a deficit in visual wordrecognition. (He was poor at visual lexical decision making with pseudo-homophones; e.g., Which is the real word: turtle/tertle?) Previously, Byng andColtheart (1986; Coltheart & Byng, 1989) described a treatment programmeinvolving EE who also had a problem in visual word recognition (resulting insurface dyslexia). Therefore, Weekes and Coltheart treated NW’s difficulty inreading irregular words aloud using this same therapy technique. The treatmentinvolved pairing the written word with a picture representing the word meaning(a pictorial mnemonic)
2. The results of the therapy with NW were exactly the
same as those found by Byng and Coltheart for EE: After therapy, both EE andNW showed a specific treatment effect (treated words were read better thanuntreated words), and generalisation (untreated words were read better thanthey were before therapy). These results seem promising—two people whowere identified as having the same level of breakdown in reading, when giventhe same type of therapy, responded in the same way. However, what remainsto be seen is whether the same pattern of results will occur when the same tech-niques are applied to other people in further replication studies. Indeed,evidence from the rehabilitation of anomia (and other areas such as sentenceprocessing) suggests that the picture can become less clear as more case studiesare reported.
3
The problem of prediction
The example from Weekes and Coltheart (1996) illustrates the ideal—deter-mine the level of breakdown in language processing, identify a therapy that isappropriate for that level of breakdown, predict the pattern of change, andobtain these results. Unfortunately, predicting the results of therapy is notalways so straightforward. Nickels and Best (1996b) describe three people withanomia, all of whom were identified as having semantic deficits. All three were
FROM THEORY TO THERAPY IN APHASIA 233
2 Unlike Byng and Coltheart, Weekes and Coltheart also included a further aid—a letter string,whose pronunciation via conventional letter-sound rules was the pronunciation of the word beinglearned, was also printed on each card.
3 The difference between the domains of reading and word production may also be important.Reading is a late acquired skill (in comparison to word production) and may be “relatively”modular—and hence more predictable in its breakdown and subsequent remediation. In com-parison, word production relies heavily on many other domains and the complexity of interactionsbetween domains may be part of the difficulty in interpreting both disorders of word productionand the effects of therapy on this skill.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
given the same type of therapy—word–picture matching with semanticdistractors. Far from the results being predictable each of the three responded ina different way to the therapy. Why is it that the outcome of therapy can be sohard to predict? We will begin our discussion by using as an example a series ofstudies concerned with the remediation of reading in deep dyslexia.
Treatment of deep dyslexia
De Partz (1986) described a therapy programme for SP who was deep dyslexic.SP made semantic errors in reading aloud and was unable to read aloudnon-words or even provide a sound for a written letter. De Partz retaught SP toassemble the phonology of non-words (i.e. read them aloud) by using asequence of therapy tasks starting with the relearning of letter–sound(grapheme–phoneme) correspondences. At the conclusion of the therapy, SP’sreading of words has improved substantially (with a reduction in semanticerrors) and he was able to read aloud non-words (which had previously benimpossible). Nickels (1992, 1995) used the same technique with TC, anotherdeep dyslexic, who, like SP, was unable to read aloud non-words. However,although after therapy TC’s word reading was greatly improved and there was areduction in the incidence of semantic errors, he remained unable to readnon-words. This contrasts with SP who was able to read non-words aftertreatment.
Why did SP and TC show different patterns of improvement—in otherwords why were the results of therapy not predictable for TC? The first point tonote is that the therapy was effective for both SP and TC—they both showedimproved reading of words (and, more importantly, could use this to help theirspoken naming). However, this improvement had been achieved in differentways. After therapy SP, when unable to read aloud a word, would assemble thephonology of that word (using the taught grapheme–phoneme corres-pondences to identify the phonemes and then blend these together to form asyllable). In contrast, when TC was unable to read a word aloud he wouldidentify only the first phoneme of the word (using the taught grapheme–phoneme correspondences), this phoneme then served as a phonemic cue,enabling him to read the word aloud (by facilitating retrieval of the phonolog-ical form from the lexicon). Thus, the same therapy task was effective inimproving SP and TC’s reading by rather different means (assembling thephonology vs. self-cueing). It follows, then, that some of the difficulty inpredicting the results of therapy is because that even for those with apparentlythe same level of deficit, the same task can work in different ways (which maylead to different results).
There is a further lesson to be learned from these studies of the remediationof non-lexical reading, relating to the level of detail of the deficit analysiswhich precedes therapy. In order to read aloud non-words, it is not sufficient to
234 BEST AND NICKELS
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
know grapheme–phoneme correspondences, one must also be able to assemble(blend) the phonemes into a syllable. The reason that TC (Nickels, 1992) didnot benefit from relearning grapheme–phoneme correspondences in the sameway that SP (De Partz, 1986) had, was that he was unable to blend the resultingphonemes into syllables (and also unable to relearn this ability). Thus, for TCthere were two levels of disruption to the non-lexical reading route: Loss ofknowledge of grapheme–phoneme correspondences and impaired blendingprocedures. In other words, the initial assessment of TC’s reading problem wasnot sufficiently detailed to fully specify the nature of the breakdown innon-lexical reading. This, then, is a further complication in our attempts topredict the results of therapy: Although SP and TC did have identical deficits atone level, a more detailed analysis would have revealed that they were indeeddifferent. Berndt and Mitchum (1994; Mitchum & Berndt, 1991) demonstratethe advantages of, and necessity for, this more detailed analysis in anotherstudy aimed at remediating non-lexical reading. They identify that deepdyslexic, LR, had a number of difficulties in the component processes involvedin non-lexical reading and took these deficits into account in the therapeuticprocedure (readers are referred to the original papers for details).
Finally, the difference between SP and TC was not restricted to the fact thatTC had an additional blending deficit. His response to therapy was alsodifferent because of the effectiveness of phonemic cues in helping to produce aresponse. In other words, the presence of one strength (cueability) affected theresults of therapy as much as the absence of another skill (blending). If TC hadbeen unable to make use of a phonemic cue, obtaining the phonemes derivedfrom the letters of the written word would not have influenced his ability to saythat word aloud—in other words his reading would not have improved.
Clearly, the formula that was our original goal (problem X + treatment Y =result Z) needs amending. The situation is far more complex, and problem Xsimply cannot be considered in isolation.
4Rather, the amended formula might
read:
(problem X [+ skills a,b,c; – skills d,e,f] + treatment Y = result Z)
That is, given problem X in the presence of skills a, b, c and absence of skills d,e, f; then if you do therapy y, you should get result Z.
What we are arguing, therefore, is that to gain the maximum (clinical)benefit from research into remediation we need to be clear about the relation-ship between therapy and outcome. The earlier example, illustrates that we
FROM THEORY TO THERAPY IN APHASIA 235
4 We make a distinction between the broader strengths and weaknesses that are routinely takeninto account in clinical practice and the very specific linguistic skills (a, b, c) and deficits (d, e, f)that become clear only with very detailed analyses of language processing. Examples are given inthe main text.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
need detailed analyses of the language skills of the aphasic person, in order tobe able to interpret which skills impact on the results of therapy. At a grosslevel, therapy studies clearly do take a person’s skills into account—forexample, no clinician would use auditory word–picture matching as a therapytask with a person who had severe peripheral auditory and/or visual processingproblems. However, a more detailed analysis of impaired and retained skillshas often not been reported in the literature. We would suggest that without thisinformation, it is impossible to understand exactly why one person respondedin a certain way to a therapy, and why another person with (at a gross level) asimilar problem responded differently. For example, in early studies of thetreatment of anomia little attention was given to the other skills of the anomicpeople involved (e.g., Howard et al., 1985). This was despite the fact that thetherapy tasks used necessitated the use of many processing components notinvolved in word production (the problem being treated). For example,word–picture matching, one task that has been used in many studies, must alsoinvolve input processes in reading comprehension (where a written word isused), picture recognition processes, plus processes involved in reading aloud(where the word is read aloud before selection). Thus, differences in the patternof strengths and weaknesses of processes across these areas could impact on theeffect of this task on subsequent naming. Furthermore, in addition to the basicprocessing elements involved in a task, there are clearly other skills and factorsthat will impact on the effects of therapy: For example, to correctly performword–picture matching, the person must be able to “hold”, “compare”, and“decide” between the semantically related items. All these factors make it lesssurprising that Nickels and Best (1996a,b) found it difficult to interpret thepattern of results from using therapy of this kind with different anomic subjects.Moreover, word–picture matching is a relatively simple therapy task comparedto many that are used (e.g., cueing hierarchies).
We conclude by presenting data from a therapy study which illustrates manyof the points discussed above. This study began by using previous research todevelop a clear set of predictions regarding the efficacy of a therapy taskdepending on both the deficits and intact skills of some people with anomia.However, these predictions were not supported. Nevertheless, with the detailedanalysis of a broader range of skills and consideration of the processes involvedin the (complex) therapy task, the reason for the failure of these predictionsbecomes clearer.
TREATMENT STUDY
We present here an outline of a study that illustrates the main points of ourpaper. Detailed information on the treatment study is provided elsewhere (Best,Howard, Bruce, & Gatehouse, 1997).
236 BEST AND NICKELS
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4

Much of the research into treatment for anomia has focused on tasksinvolving semantic processing such as word-to-picture matching. In contrast,the focus of this study is on using orthographic cues to help word retrieval.
Bruce and Howard (1988) ask the question, why don’t aphasic speakers cuetheir own word finding? That is, why don’t they use any retained knowledge ofinitial letters to help access spoken word forms? Bruce and Howard workedwith 20 people with anomia and asked three questions which reflect three skillsnecessary to self-cue word finding:
1. Can people indicate the initial letters for words they cannot produce?2. Can they convert letters to sounds?3. Does naming benefit from phonemic cues (over and above extra time)?
Unsurprisingly, the participants did not all show the same pattern (e.g. onlyhalf benefited from initial phoneme cues). However, importantly, none of the20 people had all three skills that would be necessary in order to self-cue theirword finding. Five people had skills (1) and (3), i.e. they were able to point tothe correct initial letter for some words even when unable to produce the spokenform and they were better at finding words when initial phoneme (plus schwa)cues were provided. If they had possessed skill (2) they might have been able toconvert the initial letters into phonemes to cue their word finding.
In order to make the link between letters and sounds (step 2 above) Bruceand Howard (1987) devised a computerised aid that converted letters to sounds.They worked with the five people who were able to select initial letters forpictures they could not name and who benefited from initial phoneme cues.When taught to use the aid (in a picture naming paradigm) they found all fivepeople’s word finding improved (the pattern of improvement varied andreaders are referred to the original article for details).
In the 1990s a research project was set up to replicate and extend thesefindings. In particular, one aim of the study was to determine for whom the aidwas most appropriate in order to make recommendations for efficient use of theaid in clinical practice.
In relation to our formula
(problem X [+ skills a,b,c; – skills d,e,f] + treatment Y = result Z)
we worked with people with anomia (X), providing treatment with the comput-erised aid (Y) with the aim of improving word finding (Z). The difference fromthe original study was that people varied in the skills that they retained inrelation to their word finding. While Bruce and Howard included only peoplewho had both some letter knowledge and benefited from cues, we also includedpeople who did not have letter knowledge and some who did not benefit fromphonemic cues. Overall there are four possible combinations of these abilities(see Table 1).
FROM THEORY TO THERAPY IN APHASIA 237
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
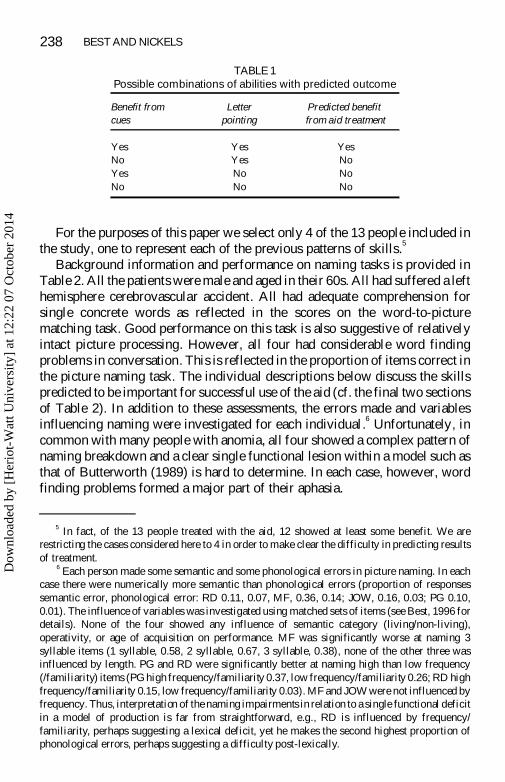
For the purposes of this paper we select only 4 of the 13 people included inthe study, one to represent each of the previous patterns of skills.
5
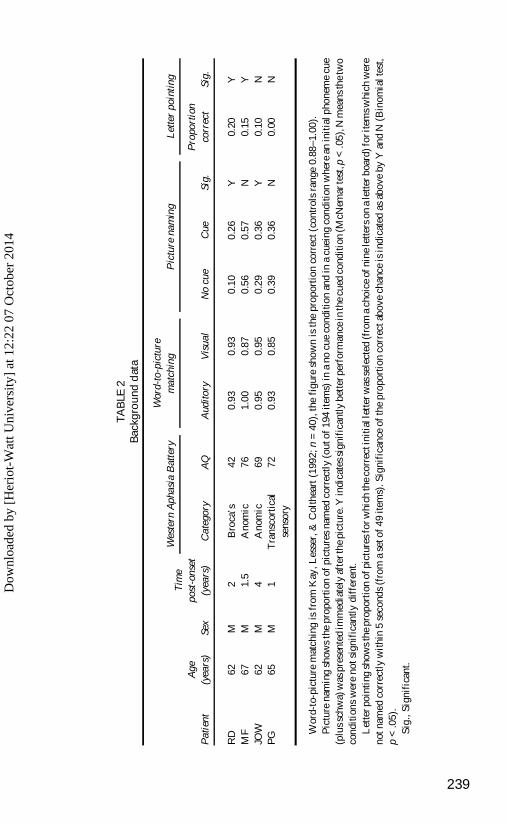
Background information and performance on naming tasks is provided inTable 2. All the patients were male and aged in their 60s. All had suffered a lefthemisphere cerebrovascular accident. All had adequate comprehension forsingle concrete words as reflected in the scores on the word-to-picturematching task. Good performance on this task is also suggestive of relativelyintact picture processing. However, all four had considerable word findingproblems in conversation. This is reflected in the proportion of items correct inthe picture naming task. The individual descriptions below discuss the skillspredicted to be important for successful use of the aid (cf. the final two sectionsof Table 2). In addition to these assessments, the errors made and variablesinfluencing naming were investigated for each individual.
6Unfortunately, in
common with many people with anomia, all four showed a complex pattern ofnaming breakdown and a clear single functional lesion within a model such asthat of Butterworth (1989) is hard to determine. In each case, however, wordfinding problems formed a major part of their aphasia.
238 BEST AND NICKELS
TABLE 1Possible combinations of abilities with predicted outcome
Benefit fromcues
Letterpointing
Predicted benefitfrom aid treatment
YesNoYesNo
YesYesNoNo
YesNoNoNo
5 In fact, of the 13 people treated with the aid, 12 showed at least some benefit. We arerestricting the cases considered here to 4 in order to make clear the difficulty in predicting resultsof treatment.
6 Each person made some semantic and some phonological errors in picture naming. In eachcase there were numerically more semantic than phonological errors (proportion of responsessemantic error, phonological error: RD 0.11, 0.07, MF, 0.36, 0.14; JOW, 0.16, 0.03; PG 0.10,0.01). The influence of variables was investigated using matched sets of items (see Best, 1996 fordetails). None of the four showed any influence of semantic category (living/non-living),operativity, or age of acquisition on performance. MF was significantly worse at naming 3syllable items (1 syllable, 0.58, 2 syllable, 0.67, 3 syllable, 0.38), none of the other three wasinfluenced by length. PG and RD were significantly better at naming high than low frequency(/familiarity) items (PG high frequency/familiarity 0.37, low frequency/familiarity 0.26; RD highfrequency/familiarity 0.15, low frequency/familiarity 0.03). MF and JOW were not influenced byfrequency. Thus, interpretation of the naming impairments in relation to a single functional deficitin a model of production is far from straightforward, e.g., RD is influenced by frequency/familiarity, perhaps suggesting a lexical deficit, yet he makes the second highest proportion ofphonological errors, perhaps suggesting a difficulty post-lexically.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
239
TAB
LE2
Bac
kgro
und
dat
a
Pat
ient
Age
(yea
rs)
Sex
Tim
epo
st-o
nset
(yea
rs)
Wes
tern
Aph
asia
Bat
tery
Wor
d-to
-pic
ture
mat
chin
gP
ictu
rena
min
gL
ette
rpo
inti
ng
Cat
egor
yA
QA
udit
ory
Vis
ual
No
cue
Cue
Sig.
Pro
port
ion
corr
ect
Sig.
RD
MF
JOW
PG
62 67 62 65
M M M M
2 1.5
4 1
Bro
ca’s
Ano
mic
Ano
mic
Tra
nsco
rtic
alse
nsor
y
42 76 69 72
0.93
1.00
0.95
0.93
0.93
0.87
0.95
0.85
0.10
0.56
0.29
0.39
0.26
0.57
0.36
0.36
Y N Y N
0.20
0.15
0.10
0.00
Y Y N N
Wor
d-to
-pic
ture
mat
chin
gis
from
Kay
,Les
ser,
&C
olth
eart
(199
2;n
=40
),th
efi
gure
show
nis
the
prop
orti
onco
rrec
t(co
ntro
lsra
nge
0.88
– 1.0
0).
Pic
ture
nam
ing
show
sth
epr
opor
tion
ofpi
ctur
esna
med
corr
ectl
y(o
utof
194
item
s)in
ano
cue
cond
itio
nan
din
acu
eing
cond
ition
whe
rean
init
ialp
hone
me
cue
(plu
ssch
wa)
was
pres
ente
dim
med
iate
lyaf
tert
hepi
ctur
e.Y
indi
cate
ssig
nifi
cant
lybe
tter
perf
orm
ance
inth
ecu
edco
nditi
on(M
cNem
arte
st,p
<.0
5),N
mea
nsth
etw
oco
nditi
ons
wer
eno
tsig
nifi
cant
lydi
ffer
ent.
Let
terp
oint
ing
show
sth
epr
opor
tion
ofpi
ctur
esfo
rwhi
chth
eco
rrec
tini
tial
lett
erw
asse
lect
ed(f
rom
ach
oice
ofni
nele
tters
ona
lette
rboa
rd)f
orit
emsw
hich
wer
eno
tnam
edco
rrec
tly
wit
hin
5se
cond
s(f
rom
ase
tof4
9ite
ms)
.Sig
nifi
canc
eof
the
prop
ortio
nco
rrec
tabo
vech
ance
isin
dica
ted
asab
ove
byY
and
N(B
inom
ialt
est,
p<
.05)
.S
ig.,
Sign
ific
ant.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
RD
RD’s skills matched those of the original 5 people who were treated with theaid (Bruce & Howard, 1987). He was able to select from initial letters forpictures he was unable to name. In addition, his naming was improved by initialphoneme cues. The prediction was that he could learn to use the aid to providethe missing link between these two skills (converting initial letters intophonemes which could act as phonemic cues) thereby improving wordfinding.
7
MF
MF’s naming did not benefit from phonemic cues. However, he was able tochose from initial letters at greater than chance rates for items he was unable toname. Thus, whilst he might be able to select an initial letter and convert this toa sound using the aid, the prediction was that this would not help word findingas his naming was not helped by phonological cues.
JOW
JOW’s skills show a double dissociation with those of MF. He did benefitfrom phonemic cues but was unable to chose from letters at greater than chancerates for items he was unable to name. So, the prediction was that JOW wouldbe unable to chose from the letters on the aid and would not be able to use this toimprove naming (Best et al., 1997 provide further details on this and other treat-ments for JOW’s anomia).
PG
PG had neither of the key skills one would predict would be required tobenefit from the aid. He neither selected initial letters for items he could notname nor benefited from phonemic cues. In this case the strong prediction canbe made of no benefit from treatment with the aid.
In summary, on the basis of detailed assessment of naming abilities and relatedskills only 1 of the 4 people described above (RD) would be predicted to benefitfrom treatment involving a computerised aid which converts letters to sounds.The remaining 3 people all lack one or both of the skills thought to be necessaryto benefit.
240 BEST AND NICKELS
7 In Bruce and Howard’s original study the aid not only improved word finding (treated itemswere named better than control items) but also acted as a prosthesis. That is, after treatment, fourpeople were better at naming with the aid present that without (the fifth’s performance approachedceiling). Thus, it is possible for the aid to be effective in two ways. It may improve word findingabilities per se, it may also be needed as a prosthesis to aid word finding.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
Treatment
A set of pictures was presented three times for baseline naming. From theoriginal set, a set of treatment items (n = 50) and set of control items (n = 50,not to be seen during treatment) were selected individually for each participant.The treatment and control items were matched for number correct acrossbaseline naming. Filler pictures (n = 50) which had had a high success rateduring baseline naming were also included in order to provide encouragement.
This version of the aid had nine letters available which when pressedproduced the appropriate phoneme (plus schwa). All the picture names beganwith one of these initial letters.
Treatment took place once a week, over 5 weeks, for about 1 hour on eachoccasion. During the first three sessions participants were instructed that theymust use the aid prior to naming the picture. During the final two sessions use ofthe aid was optional. The same sequence was followed for each of the treatedand filler pictures which were presented in a random order.
1. Press the initial letter—if failed go to step (4).2. Encourage repetition of the cue.3. Name the picture—if failed go to step (7).4. Therapist points to three of the letters for participant to press the correct
one—if failed go to step (7).5. Encourage repetition of cue.6. Name the picture—if failed go to step (7).7. Therapist says the name and asks for repetition.
Results
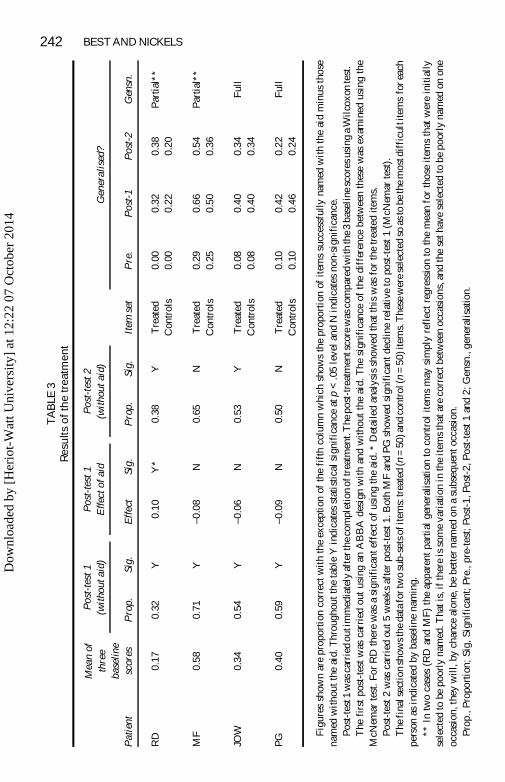
The results of treatment with the aid are shown in Table 3. The results were notas predicted. In all four cases there was significant benefit from the aid (asreflected in improved picture naming): Performance at post-test 1 was signifi-cantly better than baseline naming.
8
FROM THEORY TO THERAPY IN APHASIA 241
8 Clearly, the only change of real value is change in word finding in real-life conversation. Inthe case of JOW a change in connected speech was clear. He was rated blind, by experiencedtherapists, as significantly better at both finding words and transmitting a message, after treatment(see Best et al., 1997 for details). RD continues to show carryover from the treatment to wordfinding in conversation and himself feels the aid was of considerable benefit. Bruce (1996) notesthat RD continued to respond to phonological cues after treatment and suggests his problem mayrelate to initiating speech output. Treatment for his anomia has continued and he is now able towrite initial letters to cue his word finding in conversation. In both cases the change in conver-sation was apparent without the aid present. However, neither MF nor PG showed lastingfunctional benefit from the treatment. We do not wish to draw strong conclusions from thesefindings as the treatment lasted only five sessions and there was no treatment directed atcarry-over to conversation. Rather we would note that it is extremely positive that carry-over wasfound for RD and JOW.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
242 BEST AND NICKELST
AB
LE3
Res
ults
ofth
etr
eatm
ent
Pat
ient
Mea
nof
thre
eba
seli
nesc
ores
Pos
t-te
st1
(wit
hout
aid)
Pos
t-te
st1
Eff
ecto
fai
dP
ost-
test
2(w
itho
utai
d)
Item
set
Gen
eral
ised
?
Pro
p.Si
g.E
ffec
tSi
g.P
rop.
Sig.
Pre
.P
ost-
1P
ost-
2G
ensn
.
RD
0.17
0.32
Y0.
10Y
*0.
38Y
Tre
ated
Con
trol
s0.
000.
000.
320.
220.
380.
20P
artia
l**
MF
0.58
0.71
Y– 0
.08
N0.
65N
Tre
ated
Con
trol
s0.
290.
250.
660.
500.
540.
36P
artia
l**
JOW
0.34
0.54
Y– 0
.06
N0.
53Y
Tre
ated
Con
trol
s0.
080.
080.
400.
400.
340.
34F
ull
PG
0.40
0.59
Y– 0
.09
N0.
50N
Tre
ated
Con
trol
s0.
100.
100.
420.
460.
220.
24F
ull
Fig
ures
show
nar
epr
opor
tion
corr
ectw
ith
the
exce
ptio
nof
the
fift
hco
lum
nw
hich
show
sth
epr
opor
tion
ofit
ems
succ
essf
ully
nam
edw
ith
the
aid
min
usth
ose
nam
edw
itho
utth
eai
d.T
hrou
ghou
tthe
tabl
eY
indi
cate
sst
atis
tical
sign
ific
ance
atp
<.0
5le
vela
ndN
indi
cate
sno
n-si
gnif
ican
ce.
Pos
t-te
st1
was
carr
ied
outi
mm
edia
tely
afte
rthe
com
plet
ion
oftr
eatm
ent.
The
post
-tre
atm
ents
core
was
com
pare
dw
ith
the
3ba
seli
nesc
ores
usin
ga
Wil
coxo
nte
st.
The
firs
tpo
st-t
estw
asca
rrie
dou
tus
ing
anA
BB
Ade
sign
wit
han
dw
ithou
tth
eai
d.T
hesi
gnif
ican
ceof
the
diff
eren
cebe
twee
nth
ese
was
exam
ined
usin
gth
eM
cNem
arte
st.F
orR
Dth
ere
was
asi
gnif
ican
teff
ecto
fus
ing
the
aid.
*D
etai
led
anal
ysis
show
edth
atth
isw
asfo
rth
etr
eate
dite
ms.
Pos
t-te
st2
was
carr
ied
out5
wee
ksaf
ter
post
-tes
t1.B
oth
MF
and
PG
show
edsi
gnif
ican
tdec
line
rela
tive
topo
st-t
est1
(McN
emar
test
).T
hefi
nals
ecti
onsh
owst
heda
tafo
rtw
osu
b-se
tsof
item
s:tr
eate
d(n
=50
)and
cont
rol(
n=
50)i
tem
s.T
hese
wer
ese
lect
edso
asto
beth
em
ostd
iffi
cult
item
sfo
reac
hpe
rson
asin
dica
ted
byba
selin
ena
min
g.**
Intw
oca
ses
(RD
and
MF)
the
appa
rent
part
ial
gene
ralis
atio
nto
cont
rol
item
sm
aysi
mpl
yre
flec
tre
gres
sion
toth
em
ean
for
thos
eit
ems
that
wer
ein
itial
lyse
lect
edto
bepo
orly
nam
ed.T
hati
s,if
ther
eis
som
eva
riat
ion
inth
eit
ems
that
are
corr
ectb
etw
een
occa
sion
s,an
dth
ese
thav
ese
lect
edto
bepo
orly
nam
edon
one
occa
sion
,the
yw
ill,
bych
ance
alon
e,be
bett
erna
med
ona
subs
eque
ntoc
casi
on.
Pro
p.,P
ropo
rtio
n;Si
g,Si
gnif
ican
t;Pr
e.,p
re-t
est;
Post
-1,P
ost-
2,P
ost-
test
1an
d2;
Gen
sn.,
gene
rali
satio
n.
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
For RD the improvement had been predicted. However, MF, JOW, and PGall showed significant improvement after treatment despite not appearing tohave the skills required to benefit from the aid. The results were very encour-aging from one point of view, suggesting that it may be worth trying this type oftreatment for many people with anomia. However, the findings confirm that thesuccess or otherwise of treatments for anomia are hard to predict. With theseresults it is difficult to be clear about the theory of the therapy and impossible tomake sensible recommendations as to whom the aid may be suitable for.
Our predictions clearly need refining. In fact, in the individual cases, takingaccount of the full complexity of the treatment task, one can devise plausiblepost hoc explanations for the findings. The important point for this paper,however, is that, even in this study which included related skills in assessment,we still could not predict the outcome of treatment without further detailedanalysis.
One of the possible reasons for this is the complexity of the treatment. Thetreatment has many components including trying to name the picture, selectingfrom a choice of initial letters, hearing the letters converted to sounds, usingcues to access spoken word forms, and producing the words. One possibility isthat different components of the treatment were important for different people.
Microanalysis of the effects of treatment
RD
As it was predicted that RD would benefit and this turned out to be the case,perhaps in his case, additional consideration of how the treatment worked is notwarranted. In fact a close examination of the results (Table 3) is informative.RD’s naming improved greatly after treatment. In addition, he was better atnaming the pictures with the aid present than without. The effect was probablylimited to treated items (the partial generalisation to controls may be explainedby regression to the mean, see table legend for further explanation) but it was alasting effect. Thus RD was like the original aphasic people treated by Bruceand Howard (1987), the aid helped him access treated items and he was bestable to do this with the aid present as a prosthesis after treatment (see Bruce1996 for further discussion of the treatment of RD’s anomia).
MF
As MF did not benefit from phonemic cues, it had been predicted that treat-ment with the aid would not improve naming. However, the results showed asignificant improvement. As for RD the improvement in control items was lessthan for treated items and may simply reflect regression to the mean. Theimprovement was short lasting; MF’s performance had significantly declined 5weeks later. One reason for the item-specific, short-lasting effect of treatment,
243
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
would be that MF as predicted, did not benefit from cues and therefore the aidwas not useful to him. Instead, the final step in the treatment, repetition of thetargets, may have helped him. Perhaps he did not have difficulty in accessingthe word forms from a lexicon (the level at which cues could be of benefit) butrather with later stages of production. It is possible that he had accessed (at leastsome of) the phonological forms but could not assemble the phonology forproduction. There are two important lines of evidence in support of thisproposal. First, in treatment sessions 4 and 5, when not required to use the aid,MF never chose to press the letters. Second, MF’s naming was influenced bythe length of the stimuli, he was worse on longer items, in line with apost-lexical effect on production (for a detailed description of MF’s naming,see Best, 1996, but see also footnote 6).
JOW
As JOW could not select from nine initial letters for items he could not nameit had seemed unlikely that he would be able to benefit from treatment with theaid. In fact he showed a significant improvement which both generalised fullyto the untreated items and was maintained after the end of treatment. Onereason for the success of the treatment probably lies in the fact that JOW’snaming did benefit from a more restricted choice between three written letters.Also, in the treatment we incorporated a choice between a restricted set of threeletters on the occasions when participants were unable to select from all nineletters (step 4, in the treatment). Thus, to understand how the treatment mayhave worked for JOW, we need to carry out a microanalysis of the treatmenttask as well as of his linguistic deficits and strengths. For further discussion ofthe ways in which the aid treatment may have worked for JOW see Best et al.,1997.
PG
PG neither benefited from phonological cues nor was able to select initialletters for words he could not find. Thus, the significant effect of the aid treat-ment is particularly difficult to explain. The effect was short lasting (withsignificant deterioration by post-test 2). However, there was full generalisationto the control items. PG’s naming did not benefit from the aid being presentafter treatment. How then did it have its effect? One possibility is that, likeJOW, PG was able to select from a set of initial letters restricted to three and thathe was able to use orthographic information to address the speech outputlexicon directly (Howard & Harding, 1998). Perhaps the therapy generallyencouraged lexical access. One piece of information in line with this is thatPG’s naming was influenced by frequency and not be length which would fitwith a lexical level deficit (Bruce, 1996). In addition, there was a non-signifi-cant trend for items that were correct in post-test 1 to be higher frequency than
244 BEST AND NICKELS
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
those that PG failed to name in post-test 1 (using treated and control items thatwere never correct during baseline assessment, log of lemma frequency fromCelex database; correct x = 1.32, std = 0.48; incorrect x = 1.14, std = 0.62;unrelated t-test, t(69) = 1.37, p < .1, n.s.).
So, with a little creativity and a lot of detailed analysis it is possible to suggestplausible hypotheses for how the treatment may have worked in each case. Thisbrings us back, from our example, to the main focus of the paper. It is only withsuch detailed microanalysis of deficits, strengths, and tasks, that we will furtherunderstand treatments for aphasia. In addition, the results of treatment shouldbe examined relative to baseline scores and with respect to generalisation tountreated items or tasks, and maintenance of change. Finally, with respect toour “formula” for predicting the effects of treatment, we propose one furtherchange highlighting the importance of task analysis
(problem X [+ skills a,b,c; – skills d,e,f]+ treatment Y [with components i,j,k] = result Z).
This is not a new suggestion but is something that is often not provided inpublished treatment studies.
CONCLUSIONS
In summary, consideration of studies of the treatment of acquired dyslexia andanomia show that it is possible to find the elusive link between therapy andoutcome. So far this has been easier in the case of dyslexia but in both cases amicroanalysis of the task alongside linguistic skills and deficits is necessary.
The data from the aid study illustrate the level of detailed analysis necessaryto try to understand how a treatment works (particularly in the case of amulti-component treatment such as this). Nevertheless, clinically the resultsare very encouraging and suggest that this therapy may be able to help manypeople’s word-finding. Because of this, and despite the problems in predictingthe outcome, we would encourage therapists to include the aid (fairly easilyaccessible with today’s technology) along with the range of other techniquesavailable for the treatment of anomia.
Our understanding of treatment for aphasia will benefit from more studies inwhich there is detailed analysis of linguistic strengths and weaknesses and taskdemands. One way to achieve this would be using very simple treatment tasks(such as those used in facilitation studies) in research into treatment.
Clinically, in the meantime, therapists will continue to use a variety ofbroad-based tasks that work in different ways for different aphasic people butare very often effective. Examples of such treatments are semantically basedtasks such as word-to-picture matching (Nickels & Best, 1996a) and sentence
FROM THEORY TO THERAPY IN APHASIA 245
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
level tasks such as “mapping therapy” (Schwartz, Fink, & Saffran, 1995). Theuse of such treatments is justified in that they stand a very good chance ofworking for the maximum number of people. However, it is also important thatwe continue to develop our understanding of treatment and outcome so thatprecisely targeted therapy can be offered where possible.
REFERENCESBerndt, R.S., & Mitchum, C.C. (1994). Approaches to the rehabilitation of “Phonological
assembly”: Elaborating the model of nonlexical reading. In M.J. Riddoch & G.W. Humphreys(Eds.), Cognitive neuropsychology and cognitive rehabilitation. Hove, UK: LawrenceErlbaum Associates Ltd.
Best, W. (1996). When racquets are baskets but baskets are biscuits, where do the words comefrom? A single case study of formal paraphasic errors in aphasia. Cognitive Neuropsychology,13, 443–480.
Best, W., Howard, D., Bruce, C., & Gatehouse, C. (1997). A treatment for anomia; combiningsemantics, phonology and orthography. In S. Chiat, J. Marshall, & J. Law (Eds.), Languagedisorders in children and adults, psycholinguistic approaches to therapy. (pp. 102–129).London: Whurr.
Bruce, C. (1996). Sound effects: A new investigation of phonemic cues in aphasia. UnpublishedPhD Thesis, University College London.
Bruce, C., & Howard, D. (1987). Computer generated cues: An effective aid for naming inaphasia. British Journal of Disorders of Communication, 22, 191–201.
Bruce, C. & Howard, D. (1988). Why don’t Broca’s aphasics cue themselves? An investigationof phonemic cueing and tip-of-the-tongue information. Neuropsychologia, 26, 253–264.
Butterworth, B. (1989). Lexical access in speech production. In W. Marslen-Wilson (Ed.),Lexical representation and process. Cambridge, MA: MIT Press.
Byng, S., & Coltheart, M. (1986). Aphasia therapy research: Methodology requirements andillustrative results. In E. Hjelmquist & L.-G. Nilsson (Eds.), Communication and handicap:Aspects of psychological compensation and technical aids. New York: North HollandElsevier Science.
Coltheart, M., & Byng, S. (1989). A treatment for surface dyslexia. In X. Seron & G. Deloche(Eds.), Cognitive approaches in neuropsychological rehabilitation. Hillsdale, N.J.: Erlbaum.
De Partz, M-P. (1986). Reeducation of a deep dyslexic patient: Rationale of the method andresults. Cognitive Neuropsychology, 3, 149–177.
Hillis, A.E., & Caramazza, A. (1994). Theories of lexical processing and rehabilitation of lexicaldeficits. In M.J. Riddoch & G.W. Humphreys (Eds.), Cognitive neuropsychology andcognitive rehabilitation. Hove, UK: Lawrence Erlbaum Associates Ltd.
Howard, D. (1986). Beyond randomised controlled trials: The case for effective case studies ofthe effects of treatment in aphasia. British Journal of Disorders of Communication, 21,89–102.
Howard, D., & Harding, D. (1998). Self-cueing of word retrieval by a woman with aphasia: Why aletter board works. Aphasiology , 12, (4/5), 399–420.
Howard, D., Patterson, K.E., Franklin, S., Orchard-Lisle, V., & Morton, J. (1985). The treatmentof word retrieval deficits in aphasia: A comparison of two therapy methods. Brain, 108,817–829.
Howard, D., & Hatfield, M.H. (1987). Aphasia therapy. Hove, UK: Lawrence Erlbaum Associ-ates Ltd.
Kay, J., Lesser, R., & Coltheart, M. (1992). Psycholinguistic Assessment of Language Processingin Aphasia (PALPA). Hove, UK: Psychology Press.
246 BEST AND NICKELS
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4
Marshall, J., Pound, C., White-Thomson, M., & Pring, T. (1990). The use of picture/wordmatching tasks to assist word retrieval in aphasic patients. Aphasiology , 4, 167–84.
Miceli, G., Amitrano, A., Capasso, R., & Caramazza, A. (1996). The treatment of anomiaresulting from output lexical damage: Analysis of two cases. Brain & Language, 52, 150–174.
Mitchum, C.C., & Berndt, R.S. (1991). Diagnosis and treatment of “phonological assembly” inacquired dyslexia: An illustration of the cognitive neuropsychological approach. Journal ofNeurolinguistics, 6, 103–137.
Nickels, L.A. (1992). The autocue? Self-generated phonemic cues in the treatment of a disorderof reading and naming. Cognitive Neuropsychology, 9, 155–182.
Nickels, L.A. (1995). Reading too little into reading? Strategies in the rehabilitation of acquireddyslexia. European Journal of Disorders of Communication, 30, 37–50.
Nickels, L., & Best, W. (1996a). Therapy for naming disorders (Part 1): Principles, puzzles andprogress, Aphasiology , 10, 21–47.
Nickels, L., & Best, W. (1996b). Therapy for naming disorders (Part II): Specifics, surprises andsuggestions, Aphasiology , 10, 109–136.
Schwartz, M.F., Fink, R.B., & Saffran, E.M. (1995). The modular treatment of agrammatism.Neuropsychological Rehabilitation, 5, 93–127.
Weekes, B., & Coltheart, M. (1996). Surface dyslexia and surface dysgraphia: Treatmentstudies and their theoretical implications. Cognitive Neuropsychology, 13, 277–315.
Manuscript received October 1999
FROM THEORY TO THERAPY IN APHASIA 247
Dow
nloa
ded
by [
Her
iot-
Wat
t Uni
vers
ity]
at 1
2:22
07
Oct
ober
201
4