Embed Size (px)
Citation preview

Dr. Stefanie Keulen Prof. Dr. Philippe Paquier Prof. Dr. Jo Verhoeven Prof. Dr. Peter Marië[email protected]
FOREIGN ACCENT SYNDROME: WHAT CAN THE SLT EXPECT TO SEE IN CLINICAL PRACTICE?
Université Libre de Bruxelles (BE)
Vrije Universiteit Brussel (BE)
University of Groningen (NL)
Université Libre de Bruxelles (BE)
Vrije Universiteit Brussel (BE)
Universiteit Antwerpen (BE)
Universiteit Antwerpen (BE)
City University London (UK)
Vrije Universiteit Brussel (BE)
ZNA General Hospital , Antwerp
(BE)

13-4-2018 | 2
DEFINITION
FOREIGN ACCENT SYNDROME
FAS can be described as a motor speech disorder that causes patients to speak their mother tongue with an accent that is perceived as non-native (by their immediate environment, by medical staff)
- First report: Pierre Marie (1907)
- Second report: Arnold Pick (1919)
- Third report: Georg Monrad-Krohn (1947)
…
- Whitaker (1982): operational criteria for the diagnosis of FAS
> anecdotal
> +ling. characteris.
> + neuroanatomy ;
+ psychological impact
Monrad Krohn’spatient Astrid L.: FAS after severehemorrhagic stroke affecting the fronto-temporo-parietal region(1947)

13-4-2018 | 3
WHITAKER’S OPERATIONAL CRITERIA
1)The accent is considered by the patient, by acquaintances andby the investigator, to sound foreign
2) It is unlike the patient’s native dialect before the cerebralinsult
3) It is clearly related to central nervous system damage (as opposed to an hysteric reaction, if such exist)
4) And there is no evidence in the patient’s background of beinga speaker of a foreign language (this is not like cases of polyglot aphasia).
(Whitaker 1982, pp. 197-198)
FOREIGN ACCENT SYNDROME

13-4-2018 | 4
PROBLEMS FACING WHITAKER’S CRITERIA
Problematic retrospective interpretation of Whitaker’s criteria (1982)
Problematic prospective interpretation of FAS:
1. … Subjectivity of the defining criteria
2. … Not just damage to CNS
3. … Bilingual and polyglot speakers
FOREIGN ACCENT SYNDROME

13-4-2018 | 5
TYPOLOGY
• Verhoeven and Mariën (2010): introduction of taxonomic distinction between:
• Neurogenic FAS (acquired & developmental)
• Psychogenic FAS
• Mixed FAS
• Neurogenic is most frequently reported
• Psychogenic (or functional?) is increasingly reported in the past decades
FOREIGN ACCENT SYNDROME

13-4-2018 | 6
TYPOLOGY
FOREIGN ACCENT SYNDROME
05
10152025303540455055606570
1900-1920 1920-1940 1940-1960 1960-1980 1980-2000 2000-2017
Overview of neurogenic / psychogenic cases published in the past decades
Neurogenic FAS Psychogenic/functional FAS
Systematic review 112 cases publishedbetween 1907-2017 (only authentic!):
Neurogenic (n=87)
Psychogenic/functionalFAS (n=18)

13-4-2018 | 7
NEUROGENIC FAS
• 77.68% acquired, neurogenic FAS
• Different etiologies reported, though most common = stroke (almost 54% of all cases)
• Stroke-based FAS or “vascular FAS” (n=60) allows for lesion localization
FOREIGN ACCENT SYNDROME
Stroke (53.7%)
Trauma (13.39%)
Tumor (2.68%)
Multiple sclerosis (2.68%)
Primary Progressive Aphasia (1.79%)
Paediatric Autoimmune NeuropsychiatricDisorder associated with Streptococcus(0.89%)Vasculitis (0.89%)
Garcin's syndrome (0.89%)
Vascular dementia (0.89%)

13-4-2018 | 8
NEUROGENIC FAS
FOREIGN ACCENT SYNDROME Reported lesion locationsBasal ganglia (53.3%)
Frontal lobe (L) (46.7%)
Parietal lobe (L) (33.3%)
Insular region (L) (21.67%)
Temporal region (L) (16.67%)
Pons (11.67%)
Frontal operculum (8.33%)
Temporal lobe (R) (8.33%)
Cerebellum (5%)
Frontal lobe (R) (5%)
Parietal lobe (R) (5%)
Corpus Callosum (3.3%)
Insular region (R) (3.3%)
Stroke-based FAS (n=60):
Over half of the lesionlocations comprised(structural):
• Basal ganglia• Frontal lobe (L) (esp.
BA 4 & 6)• Parietal lobe (L)
But… diaschisis (SPECT)

NEUROGENIC FAS
FOREIGN ACCENT SYNDROME
Insights into stroke-based FAS (n=60)
Demographics & comorbid speech and language disorders:
• Significantly more women than men (>< stroke incidence?)
• First report: relatively young age: average age of 51 years (median = 53, SD= 12.8 y) (cfr. functional cases?)
• 41.7% initially mute (implication SMA, Broca, insula?)
• FAS-onset: usually in the acute phase (63.3%)
0
5
10
15
20
25
30
35
40
Acute phase (upuntil 3 weeks post-
stroke)
Lesion phase (3weeks - 3 months
post-stroke)
Chronic phase (> 3months post-
stroke)
Onset period notmentioned
FAS AoS dysarthria aphasia
stroke
13-4-2018 | 9
N=60

13-4-2018 | 10
NEUROGENIC FAS
FOREIGN ACCENT SYNDROME
Insights into stroke-based FAS (n=60)
• « Crossed FAS » incidence is quite high: 6.67%
Cognition:
• Cognitive impairments were identified in 15% of all stroke cases (n=9/60) (neurocognitive exams were only reported in 45% of the stroke patients).
• 9 patients with cognitive deficits (6/9: aphasic!)• Acalculia and working memory
• Patients with frontoparietal, cerebellar and basal ganglia lesions
stroke
13-4-2018 | 11
NEUROGENIC FAS
FOREIGN ACCENT SYNDROME
Insights into stroke-based FAS (n=60)
Remission:
• Almost 20% of all stroke patients remitted (1d - 3y)• Most of these patients (66.6%) also had comorbid speech or language disorders• 30% of these patients had persisting FAS (lesion phase)
• Aphasia: severity , than remission chances Wade et al. (1986): 18% remission, if aphasia is persistent in lesionphase
• Most of these patients had focal damage located in the frontal lobe, in or near(pre)central gyrus, inferior frontal gyrus or pons (9/12)
• Only three had basal ganglia involvement
stroke

13-4-2018 | 12
WHAT DOES THE TYPICAL NEUROGENIC FAS PATIENT LOOK LIKE?
• Monolingual, right-handed female, early fifties
• Stroke, affecting basal ganglia, SMA, (pre)motor cortex
• Mute initially, with FAS emerging within three weeks after stroke
• Often accompanied by other speech disorders (… which may initially cover up the accent)
• Patient is usually aware of the accent (reports of anosognosia are rare)
• Total remission: 20% of the patients
FOREIGN ACCENT SYNDROME

13-4-2018 | 13
PSYCHOGENIC SPEECH DISORDERS
FOREIGN ACCENT SYNDROME
Diagnostic process: psychogenic speech disorders
Some pitfalls and critiques:
• Speech disorder + psychological disturbance ≠ always “psychogenic speech disorder” “functional” ?
• Exclusion criteria• Requires elaborate knowledge on what are accepted neurological
manifestations (clinical experience)
What characterizes the psychogenic FAS patient?

13-4-2018 | 14
PSYCHOGENIC (?)
Demographics:
• More women than men (3.5:1) (preponderance women psychiatric disturbances? - WHO)
• Mean age is quite young: 45y (Median=45y 6m; SD=11y) & fallsinto the age range in whichpsychiatric disturbances are usually withheld
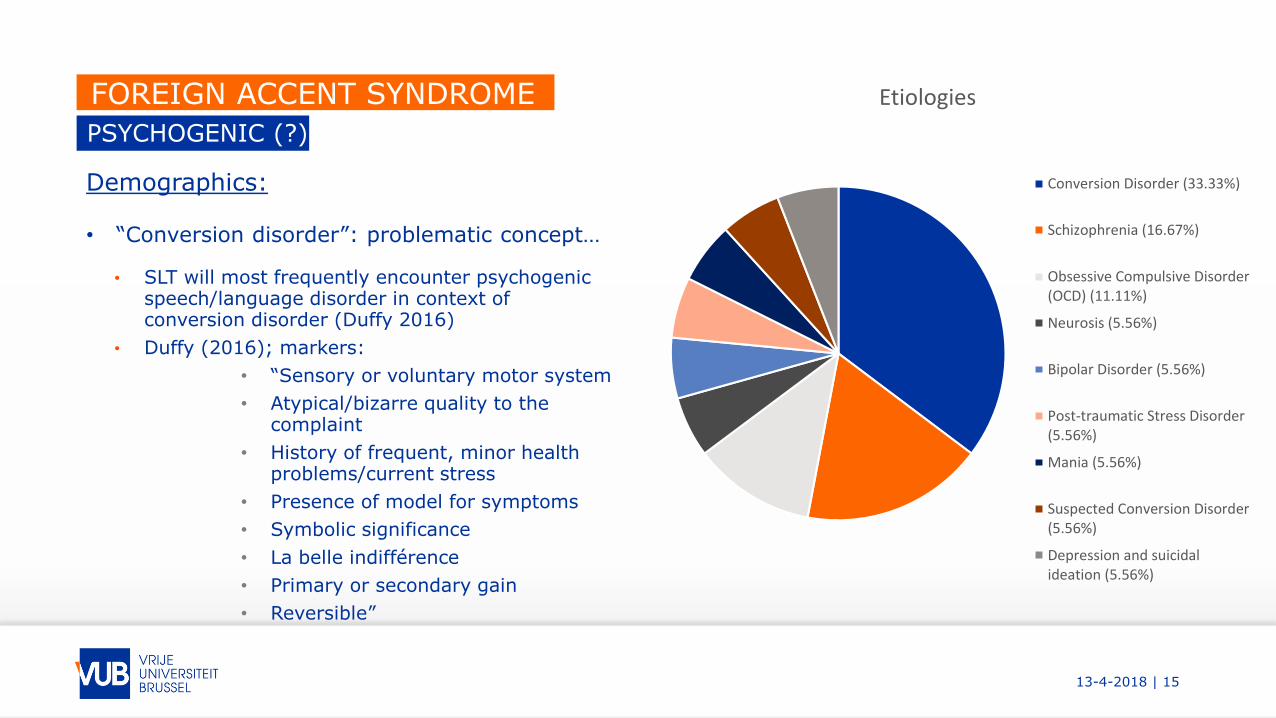
FOREIGN ACCENT SYNDROME Etiologies
Conversion Disorder (33.33%)
Schizophrenia (16.67%)
Obsessive Compulsive Disorder(OCD) (11.11%)
Neurosis (5.56%)
Bipolar Disorder (5.56%)
Post-traumatic Stress Disorder(5.56%)
Mania (5.56%)
Suspected Conversion Disorder(5.56%)
Depression and suicidal ideation(5.56%)
13-4-2018 | 15
PSYCHOGENIC (?)
Demographics:
• “Conversion disorder”: problematic concept…
• SLT will most frequently encounter psychogenicspeech/language disorder in context of conversion disorder (Duffy 2016)
• Duffy (2016); markers:
• “Sensory or voluntary motor system
• Atypical/bizarre quality to thecomplaint
• History of frequent, minor health problems/current stress
• Presence of model for symptoms
• Symbolic significance
• La belle indifférence
• Primary or secondary gain
• Reversible”
FOREIGN ACCENT SYNDROME Etiologies
Conversion Disorder (33.33%)
Schizophrenia (16.67%)
Obsessive Compulsive Disorder(OCD) (11.11%)
Neurosis (5.56%)
Bipolar Disorder (5.56%)
Post-traumatic Stress Disorder(5.56%)
Mania (5.56%)
Suspected Conversion Disorder(5.56%)
Depression and suicidalideation (5.56%)

13-4-2018 | 16
PSYCHOGENIC (?)
Comorbid speech and language disorders:
- For 7/18 patients speech was qualified as “telegraphic” or “agrammatic-like” (in absenceof aphasia)- Two patients were initially mute
Psychopathology:
In cases were psychopathology was not already established (n=5), the hypothesis of psychiatric disorder was reported to be formally assessed in 5 studies (MMPI, BDI, DIS-Q, …)
three studies reported to have included malingering tests in their protocol (one: Cottingham & Boone, 2011: inconclusive…)
FOREIGN ACCENT SYNDROME

13-4-2018 | 17
PSYCHOGENIC (?)
Cognition:
Deficits concerned mnestic functioning, attention and executive functioning, processing speed, intelligence, fine motor skills, and visuospatial skills
mostly reported in patients with conversion disorder (“cogniform disorder” ?, Delis & Wetter, 2007)
Only 3 study included cognitive malingering tests (test of memory malingering: TOMM, Tombaugh, 1996)…
Remission:
38.89% of the psychogenic/functional patients remitted• 4 patients: remission pharmacologically induced• 3 patients: spontaneous remission
FOREIGN ACCENT SYNDROME

13-4-2018 | 18
FOREIGN ACCENT SYNDROME
« TRUELY » FUNCTIONAL OR PSYCHOGENIC?
NEUROLOGICAL?
All cases demonstrate neurologically inexplicable symptoms• Unaccompanied by typical « comorbid » neurological
speech and/or language disorders (dysarthria, AoS, aphasia)
• Accent-onset is either associated with an exarcerbation, or is situated months after incident associated with FAS (>< acute onset in stroke-based FAS)
• Symptom evolution: « fluctuating » (not only speech, also other neurological symptoms: e.g. immobility of legs chair test, give-way weakness, …)
• Dissociations in terms of linguistic modalities (writing vs. speaking - in absence of aphasia)
• « automatic » speech versus complex speech
ORAL MECHANISM?
Not consistently tested…
• 5 patients were tested: twohad difficulties with oral praxis upon testing (BDAE)
DISTRACTIBLE?
Reports indicate that speech issubject to distractibility
• Emotional breakthroughsinduce accent changes (… and usually for the better)
• Possibility to consciouslymanipulate accent (voluntaryaccent change)
Duffy (2016, p. 381): questions that can provide diagnostic assistance, as to diagnose patient with psychogenic disorder

13-4-2018 | 19
FOREIGN ACCENT SYNDROME
« TRUELY » FUNCTIONAL OR PSYCHOGENIC?
FATIGUE?
« Most MSD ‘s do not fatigue dramatically over the course of examination » (Duffy 2013, p. 337)
Accent is almost withoutexception reported to becomemore exaggerated when fatigue increases
(cfr. muscle tone)
REVERSIBLE?
Better prognosis, reportedfluctuations
Schizophrenia, OCD, bipolardisorder: accent remitted afterpharmacological aid.
Fluctuations are reported in all patients (not necessarilyreported with fatigue)

13-4-2018 | 20
FOREIGN ACCENT SYNDROME
WHAT DOES THE TYPICAL PSYCHOGENIC/FUNCTIONAL FAS PATIENT LOOK LIKE?
• Monolingual, right-handed female, mid-forties
• Often there is a history of psychopathology
• Formal psychodiagnostic tests to confirm presence of psychopathology
• FAS onset is related to exacerbation in context of psychiatric disorders (e.g. schizophrenia), and in absence of a confirmed psychopathology: delayed onset vis-à-vis « traumatic event »
• Reported comorbid language symptoms are pseudo-agrammatism, jargon-speech, language mixingand switching, change of register
• Total remission: 39% of the patients (within follow-up period)

13-4-2018 | 21
FOREIGN ACCENT SYNDROME
THANK YOU FOR YOUR ATTENTION!
QUESTIONS? REMARKS?...
… EMAILS?: [email protected]





























