Embed Size (px)
Citation preview
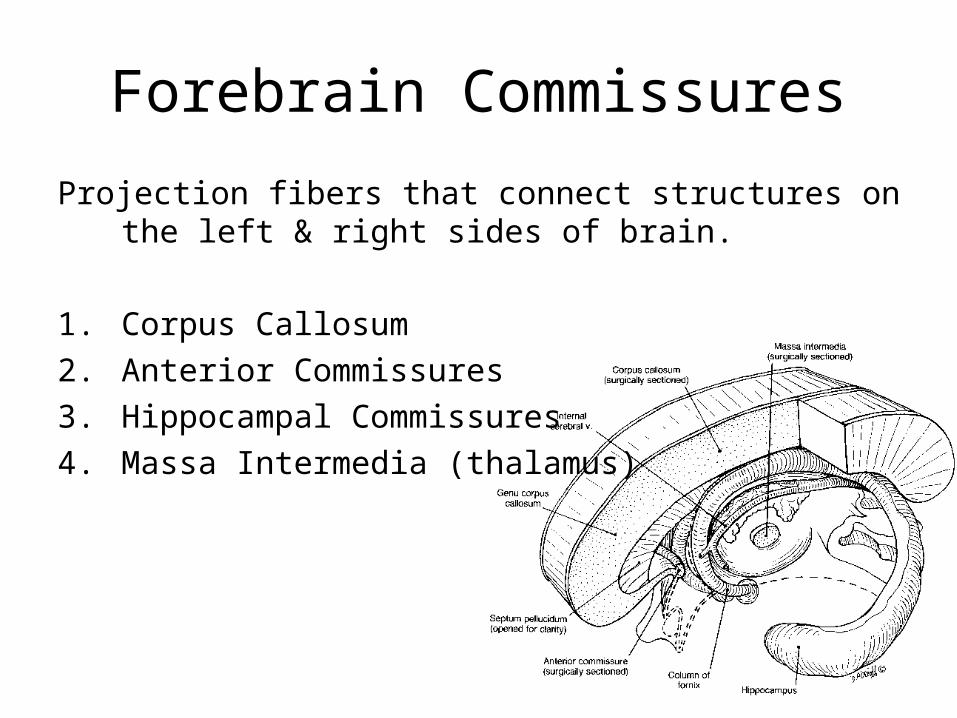
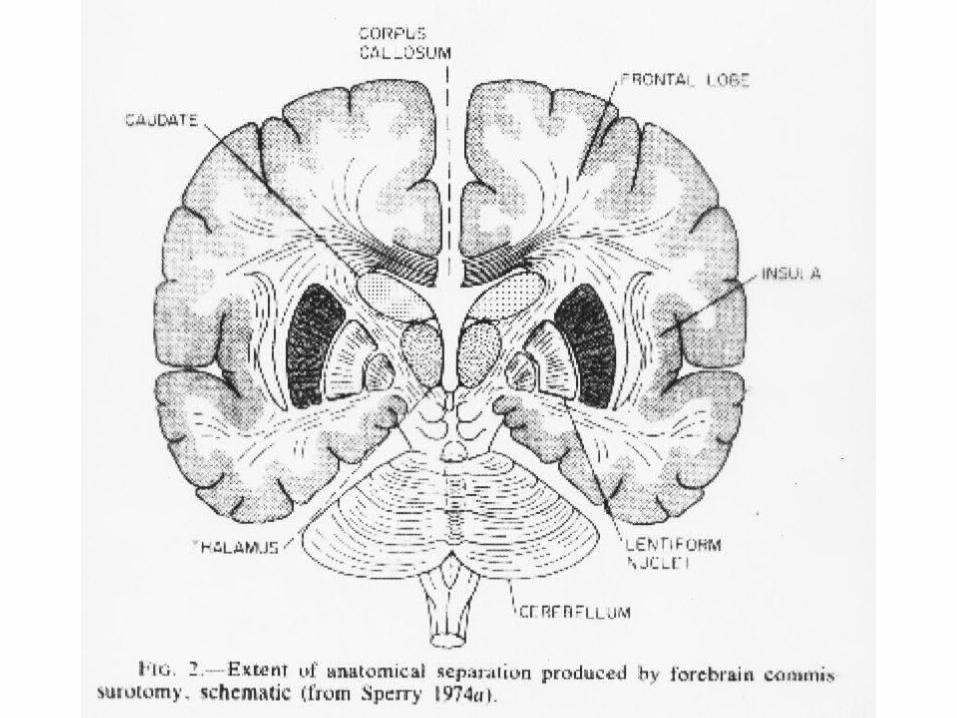
Forebrain Commissures
Projection fibers that connect structures on the left & right sides of brain.
1. Corpus Callosum
2. Anterior Commissures
3. Hippocampal Commissures
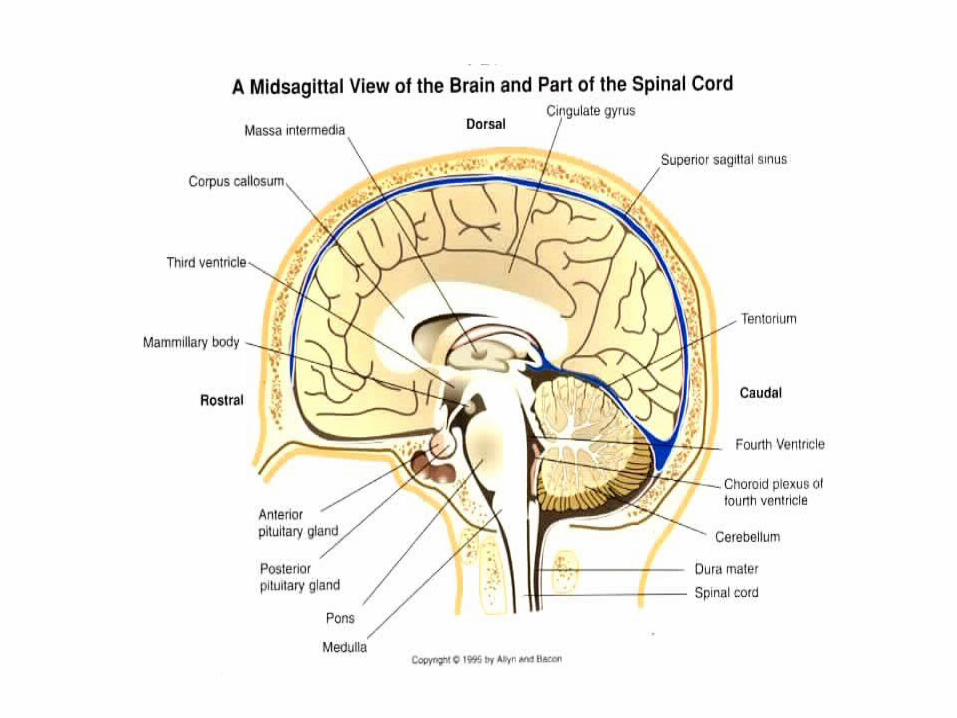
4. Massa Intermedia (thalamus)
Evolution of Commissures
1. Corpus Callosum1. Placental mammals only
2. Connect cortex only
3. 200 million fibers, ~95% myelinated
2. Anterior Commissures1. Large in Marsupials and callosal agenesis humans.
2. Connects orbitofrontal cortex, anterior temporal pole
3. Hippocampal Commissures 1. Connects hippocampi and entorhinal cortex
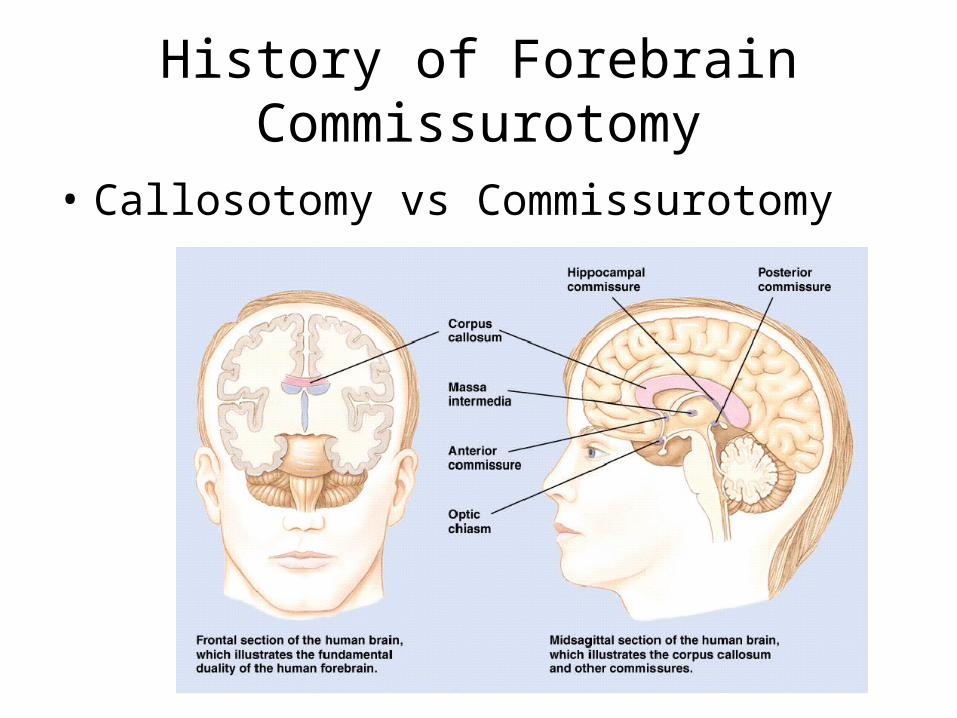
History of Forebrain Commissurotomy
• Callosotomy vs Commissurotomy
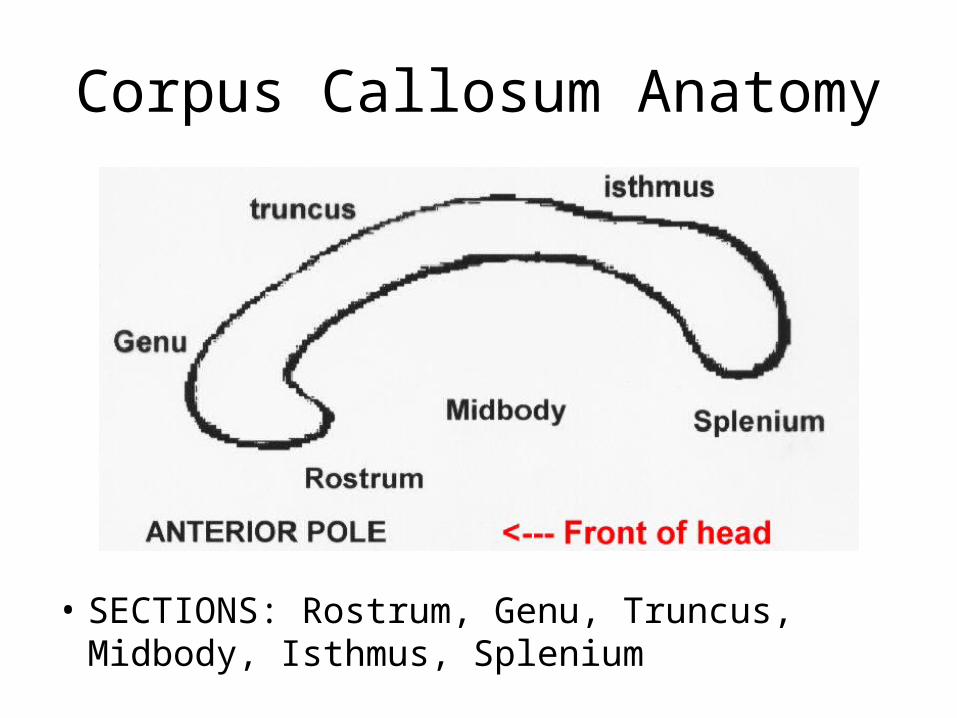
Corpus Callosum Anatomy
• SECTIONS: Rostrum, Genu, Truncus, Midbody, Isthmus, Splenium
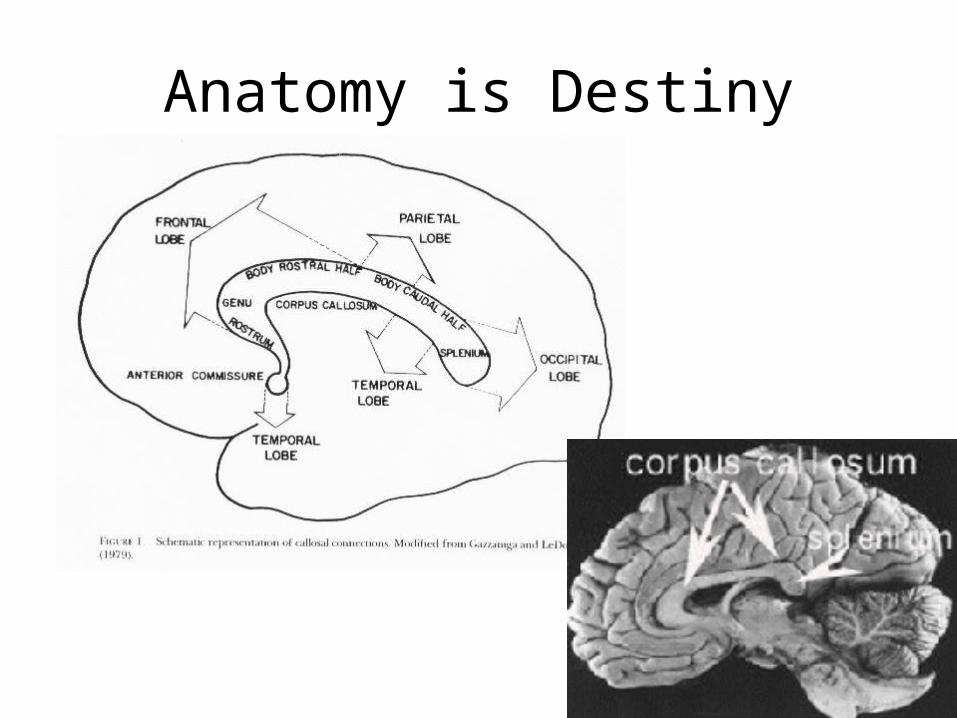
Anatomy is Destiny
Callosal Function
• For centuries, beliefs about callosal function consisted almost solely of inferences from its central location, widespread connections, and large size– larger than all descending and ascending tracts, taken together,
which connect the cerebrum with the outside sensory world.
• Thomas Willis (1664), de la Peyronie (1740), and Lancisi (1713), among others, thought the corpus callosum was a likely candidate for "the seat of the soul“
• (“or they used some other expression intended to cover that highest or ultimate liaison which brings coherent, vital unity to a complex assemblage,” Bogen, 1983).
Early neuroscience research on the CC
• Bubnoff & Heidenhain (1881) stimulated white matter of the motor cortex to produce convulsive movements in the unparalyzed ipsilateral limbs, and concluded that the excitation had spread to the opposite hemisphere via the corpus callosum.
• Horsley (1886) found that cutting the CC prevented the spread of such seizures.
• Spiegel (1931) however emphasized that seizures could spread through lower commissures; he cut all crossing fibers down to the hindbrain and still “general clonic convulsions developed following one-sided cortical stimulation,” suggesting a multiplicity of routes for seizure spread
• Erickson (1940) stimulated cortex of monkeys to produce seizures. Cut CC in 14, transcortical sections in another 10. Generalized seizure was prevented by CC cuts in 13 of the 14
Early information about the CC from TBI
• Zinn (1749) sectioned a dog’s CC. No detectable effect on motor or sensory function
• Bykov & Speransky (1924) in Pavlov’s lab found that conditioned responses to tactile stimuli spread to the homologous area on the opposite site of an animal – and cutting the CC prevented this
• Monkey commissurotomy experiments in 1930s revealed little obvious behavioral effects but it did stop spread of epileptic seizure activity.
Early information from TBI (cont’)
• Dandy (1936) neurosurgeon, sectioned CC to get at pineal tumors. “No symptoms follow its division. This simple experiment puts an end to all of the extravagant hypotheses on the functions of the corpus callosum.”
– However, Trescher & Ford (1937) reported alexia in LVF on Dandy patient. They concluded:“Special methods of examination are required to demonstrate the essential symptoms”
CommissurotomyCommissurotomy
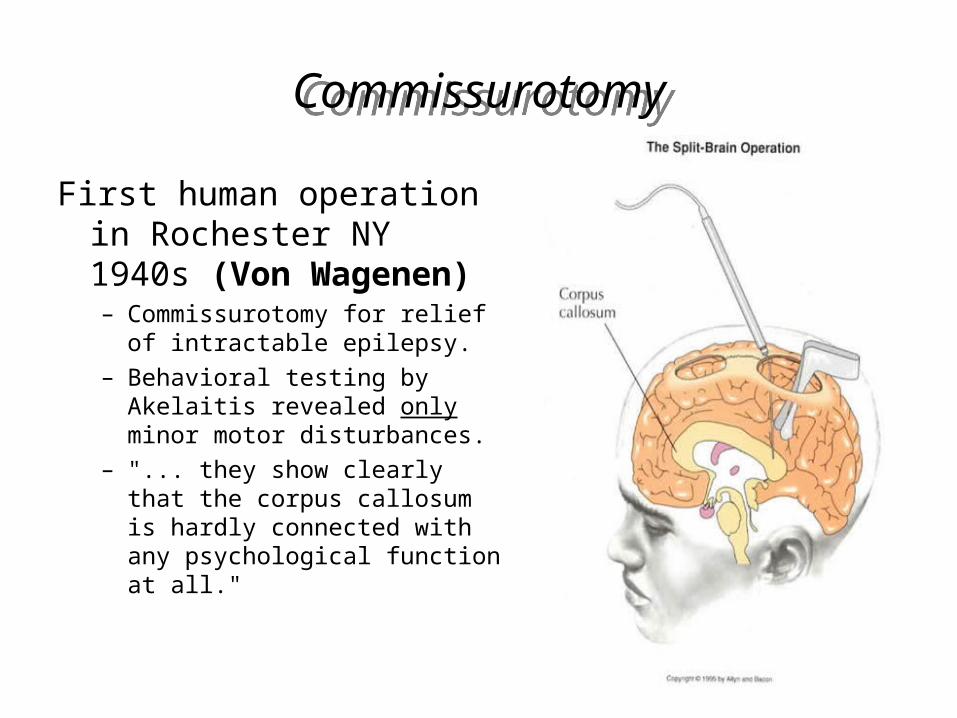
First human operation in Rochester NY 1940s (Von Wagenen)– Commissurotomy for relief of
intractable epilepsy.– Behavioral testing by Akelaitis
revealed only minor motor disturbances.
– "... they show clearly that the corpus callosum is hardly connected with any psychological function at all."
Van Wagenen Series
• Van Wagenen based his surgery to treat epilepsy on four lines of anecdotal evidence:
1. Two cases of callosal tumors1. CC tumors produced seizures early on, but they lessened
as the tumors grew larger2. Meningioma advanced into CC and reduced seizure
frequency in single case
2. Two cases of vascular insult which stopped seizures altogether
1. Postmortem study of man with 25y history of seizure which ceased 5 y before his death after hemorrhage destroyed much of his CC
2. Epilepsy cured in one individual after right-sided hemorrhage, destroying the presumed foci
Van Wagenen Series
• Short follow-up (WWII interrupted)– Mixed clinical results but favorable enough in terms
of seizure control to continue– Akelaitis (1944) studied patients but found little; only
slight motor impairments in bimanual tasks, no change in standard neuropsychological tests and psychological assessments• He was not prepared to ask the right questions• However, Case 3: “The muscles of my left side do not
coordinate very well with those of the rest of my body. For instance, I find myself trying to open a door with my right hand and at the same time trying to push it shut with the left; putting my dress on with the right and pulling it off with the left.” (Temporary effect which disappeared completely)
Enter Caltech: Roger Sperry; Joseph Bogen
•Sperry had been doing animal neuroscience research since 1939
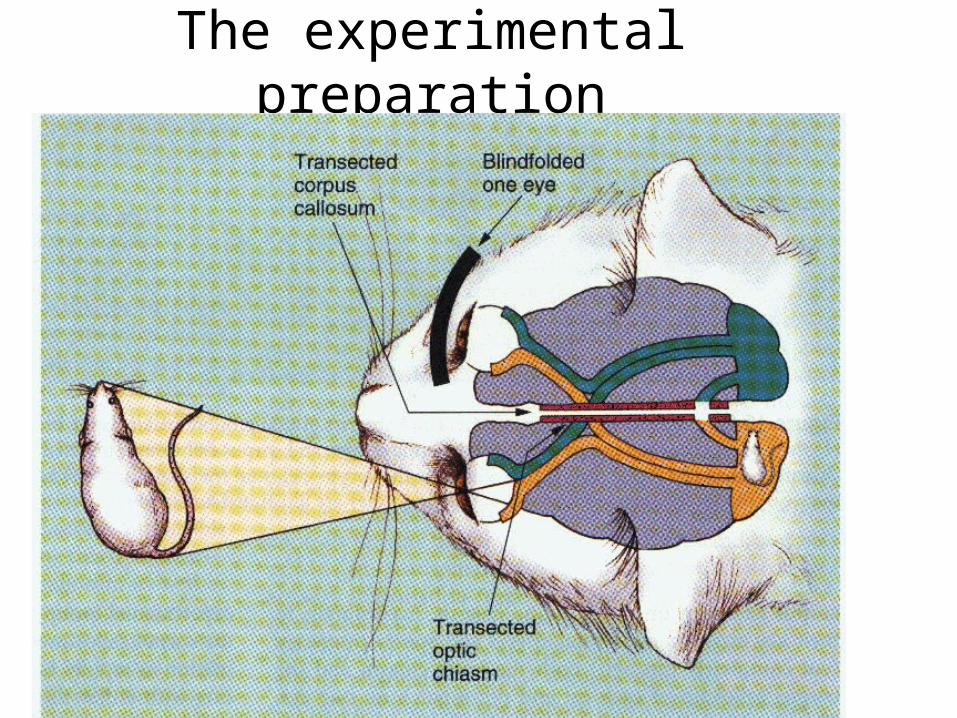
The experimental preparation
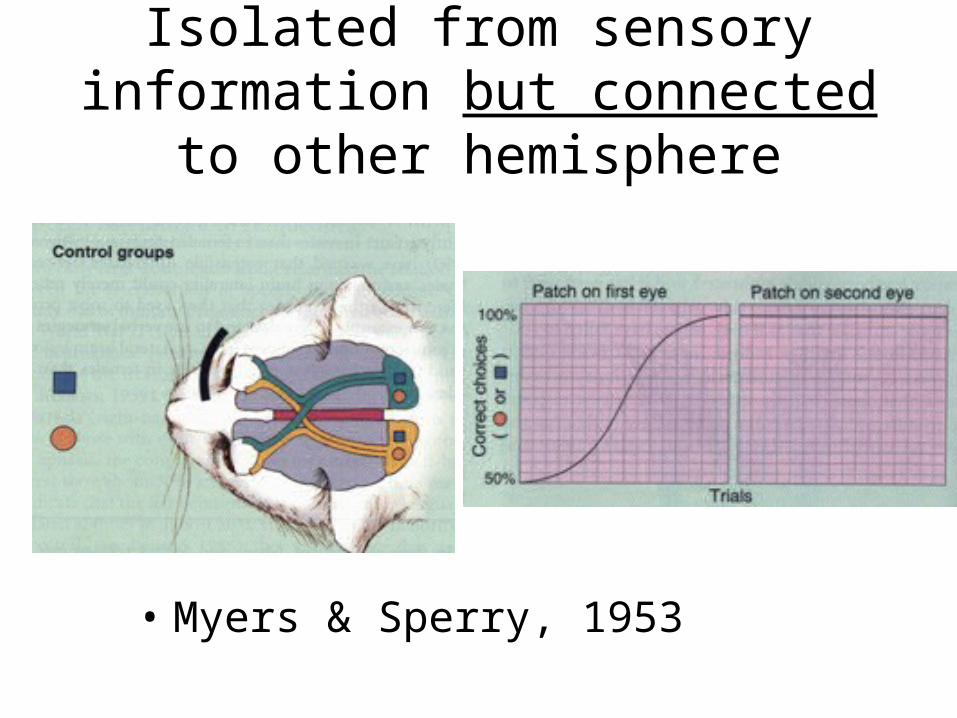
Isolated from sensory information but connected to other hemisphere
• Myers & Sperry, 1953
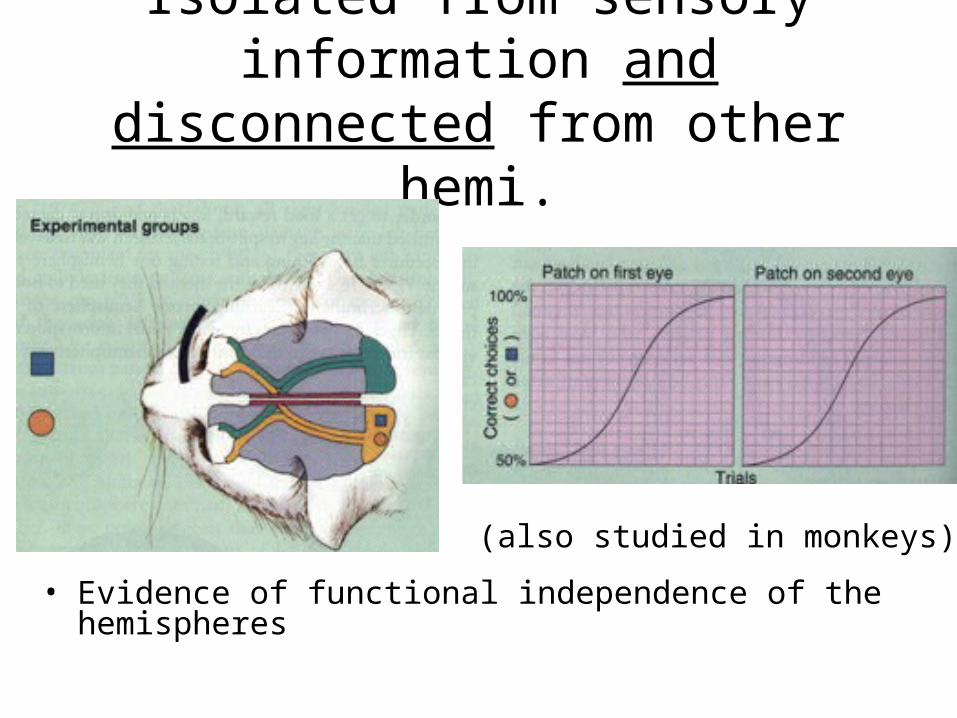
Isolated from sensory information and disconnected from other hemi.
• Evidence of functional independence of the hemispheres
(also studied in monkeys)
Vogel and Bogen, reintroduced callosotomy in 1962
For WJ: “This patient's desperate situation caused us to consider every possible approach to his problem. That the forebrain commissures contribute to the spread of seizures was shown by Erickson in 1940. But about the same time, Van Wagenen, et al. (1940) tried callosotomy on approximately 24 patients without major success, and the operation was largely abandoned. However, recent review of Van Wagenen's cases as described by Akelaitis (1944) led us to the following conclusions: (1) At least four of the patients had definite improvement. (2) Most of the remaining had only incomplete sectioning and only one of the many operative procedures included the anterior commissure, clearly important in cases suspected of having temporal foci (Frost, et al., 1958). We felt, therefore, that commissurotomy offered a reasonable chance of some improvement in this case. After the operation was practiced at postmortem several times, it became clear that adeqaute visualization required both a posterior and an anterior approach. Excellent exposure was obtained by using two openings, leaving the bone in place over the Rolandic veins and the nearby Pacchionian granulations. “
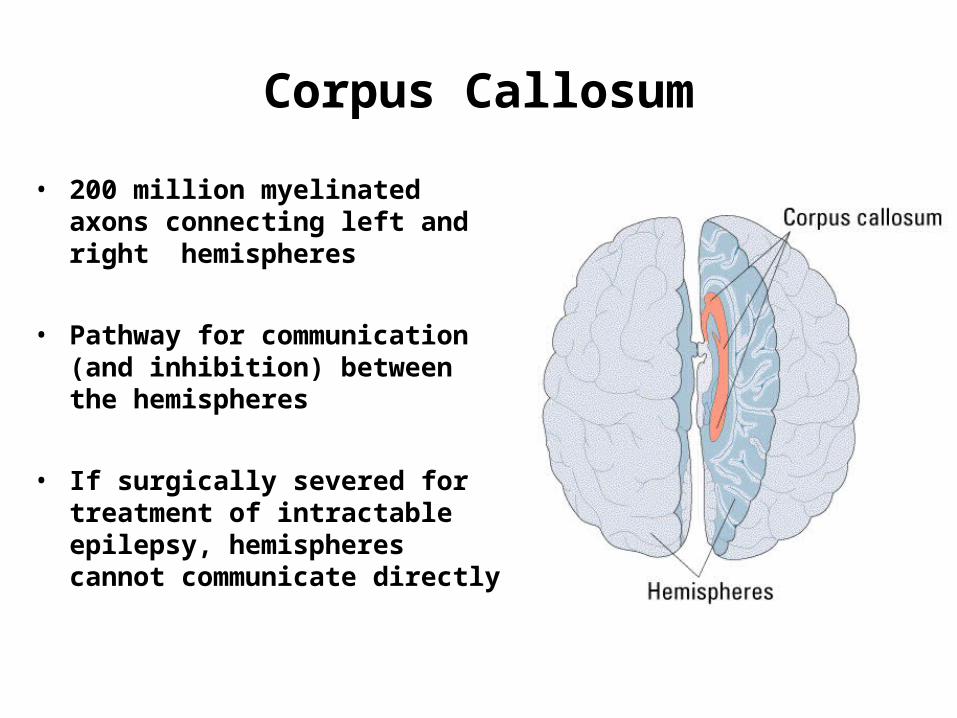
Corpus Callosum
• 200 million myelinated axons connecting left and right hemispheres
• Pathway for communication (and inhibition) between the hemispheres
• If surgically severed for treatment of intractable epilepsy, hemispheres cannot communicate directly
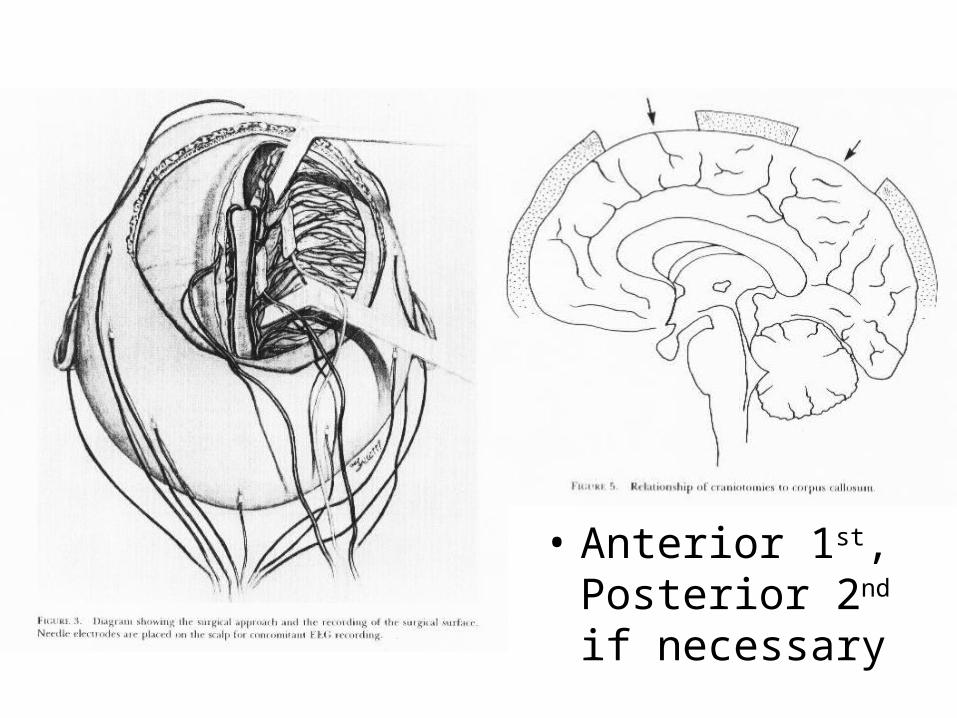
• Anterior 1st, Posterior 2nd if necessary
Wilson callosotomy series in NH
• Behavioral improvement (n=9)– For 8 of 9, falls per month dropped from 24 to only 2
(most dropped to 0). 9th patient revealed extensive brain damage
• EEG outcome (n=9)– 5 “cured” - no epileptic discharge during observation.– 3 more showed minimal discharge compared to pre-
operative baselines• so significant clinical improvement in 8 of 9
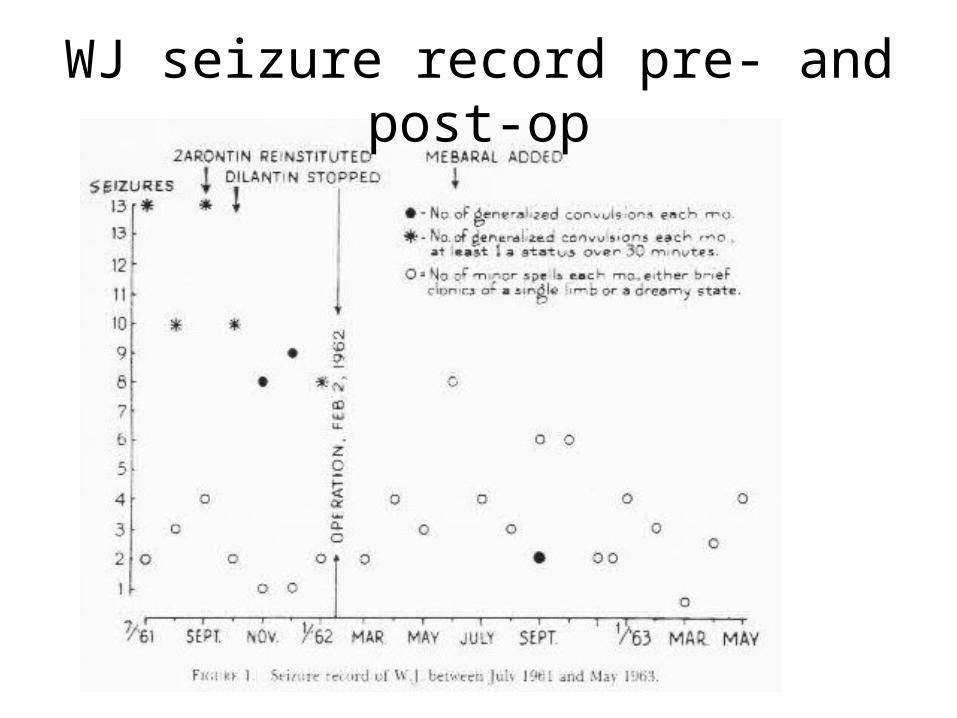
WJ seizure record pre- and post-op
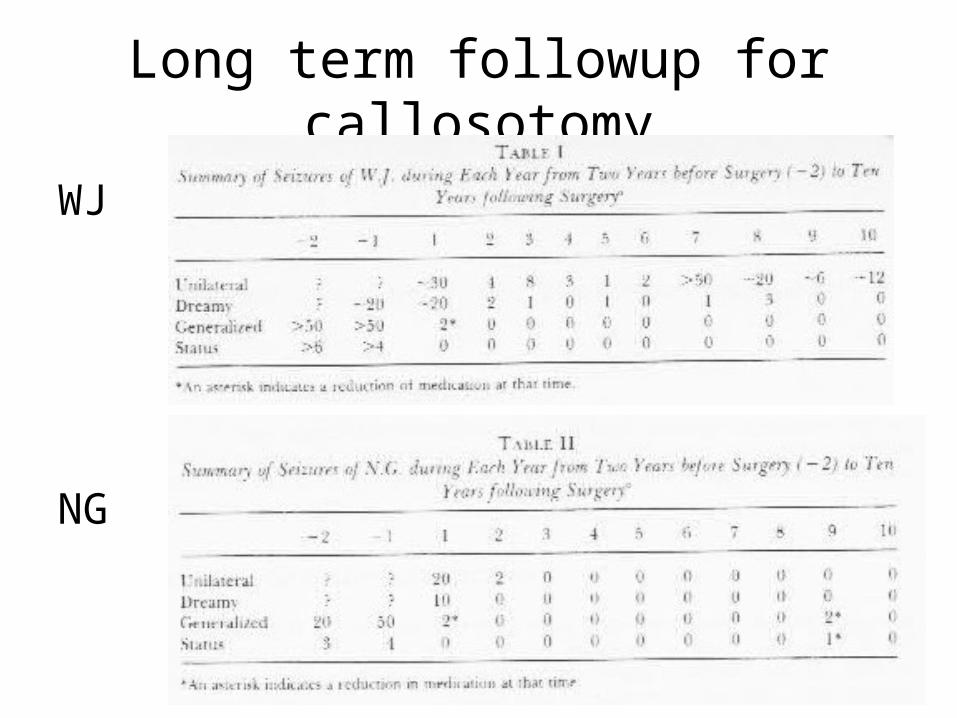
Long term followup for callosotomy
WJ
NG
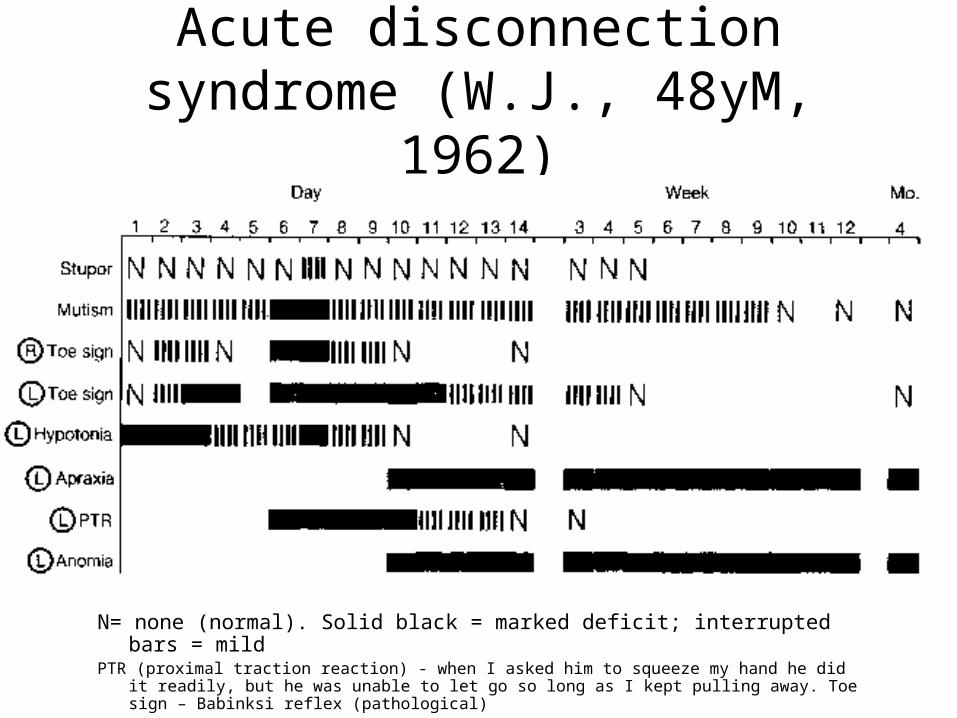
Acute disconnection syndrome (W.J., 48yM, 1962)
N= none (normal). Solid black = marked deficit; interrupted bars = mildPTR (proximal traction reaction) - when I asked him to squeeze my hand he did it readily,
but he was unable to let go so long as I kept pulling away. Toe sign – Babinksi reflex (pathological)
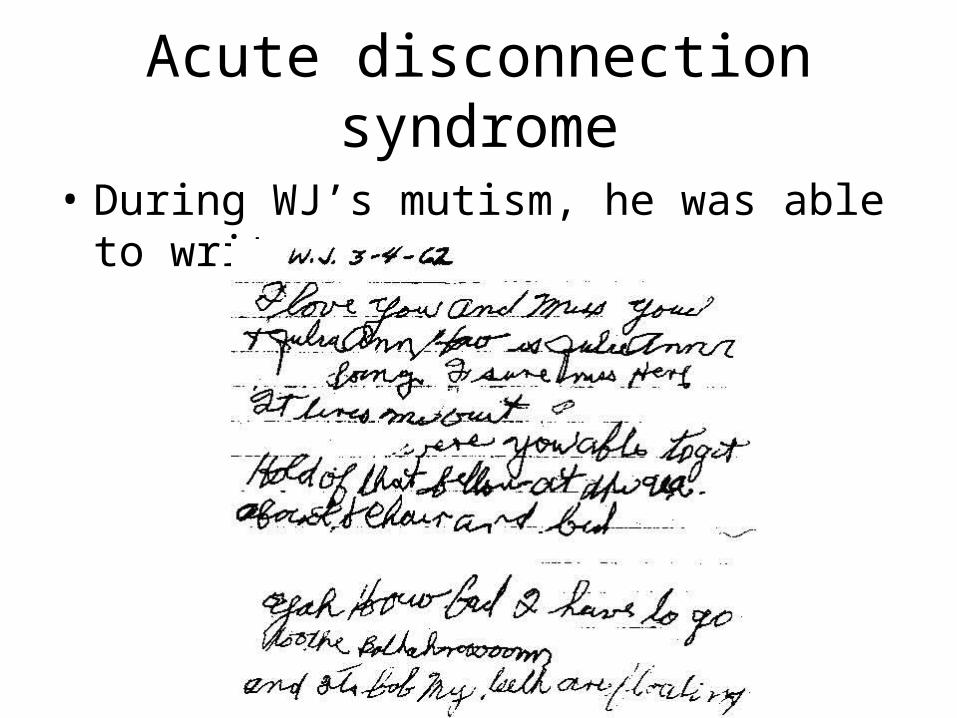
Acute disconnection syndrome
• During WJ’s mutism, he was able to write:
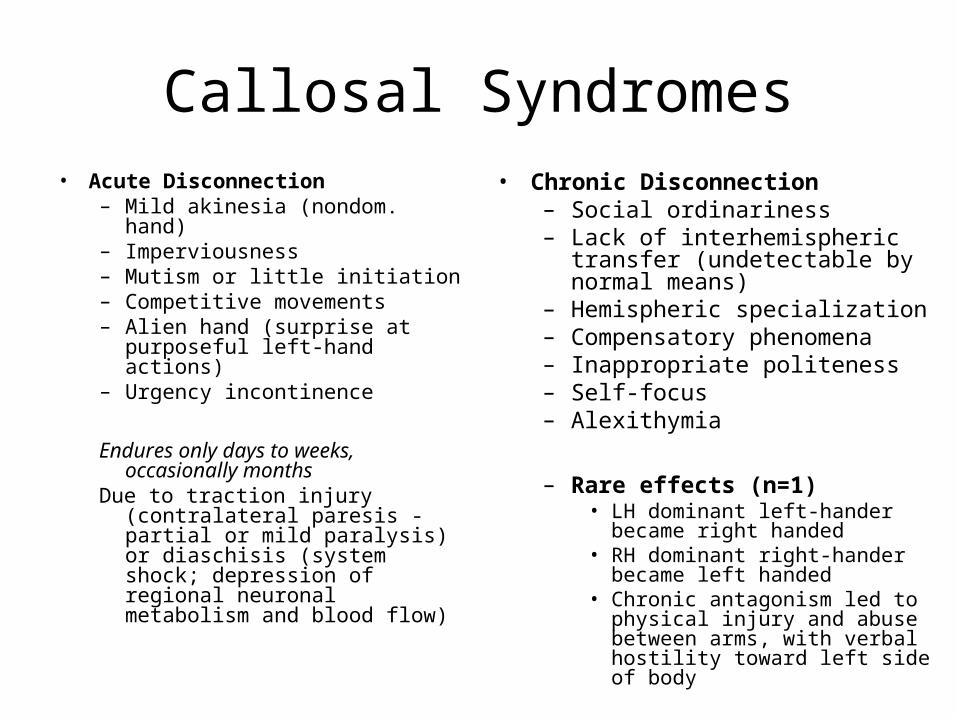
Callosal Syndromes• Acute Disconnection
– Mild akinesia (nondom. hand)– Imperviousness– Mutism or little initiation– Competitive movements– Alien hand (surprise at
purposeful left-hand actions)– Urgency incontinence
Endures only days to weeks, occasionally months
Due to traction injury (contralateral paresis - partial or mild paralysis) or diaschisis (system shock; depression of regional neuronal metabolism and blood flow)
• Chronic Disconnection– Social ordinariness– Lack of interhemispheric transfer
(undetectable by normal means)– Hemispheric specialization– Compensatory phenomena– Inappropriate politeness– Self-focus– Alexithymia
– Rare effects (n=1)• LH dominant left-hander became
right handed• RH dominant right-hander
became left handed• Chronic antagonism led to
physical injury and abuse between arms, with verbal hostility toward left side of body
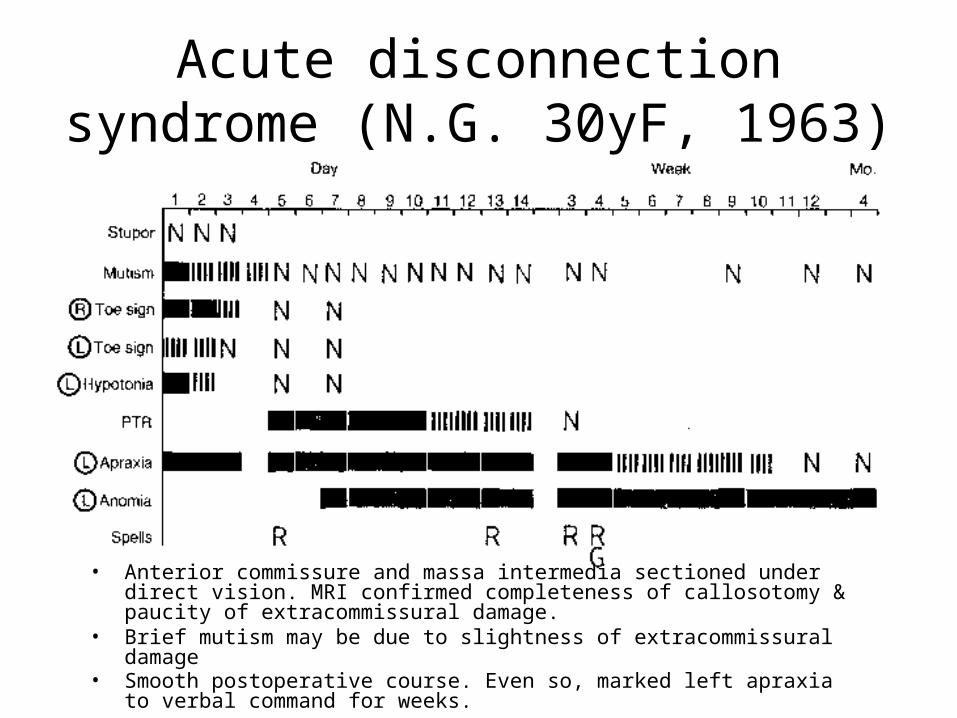
Acute disconnection syndrome (N.G. 30yF, 1963)
• Anterior commissure and massa intermedia sectioned under direct vision. MRI confirmed completeness of callosotomy & paucity of extracommissural damage.
• Brief mutism may be due to slightness of extracommissural damage • Smooth postoperative course. Even so, marked left apraxia to verbal
command for weeks.
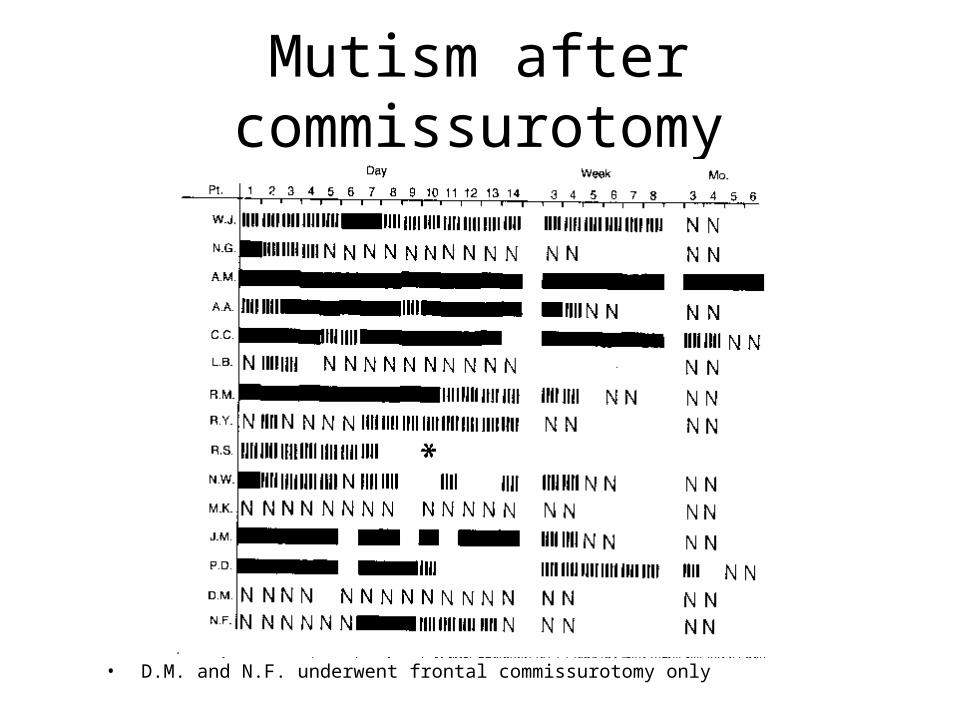
Mutism after commissurotomy
• D.M. and N.F. underwent frontal commissurotomy only
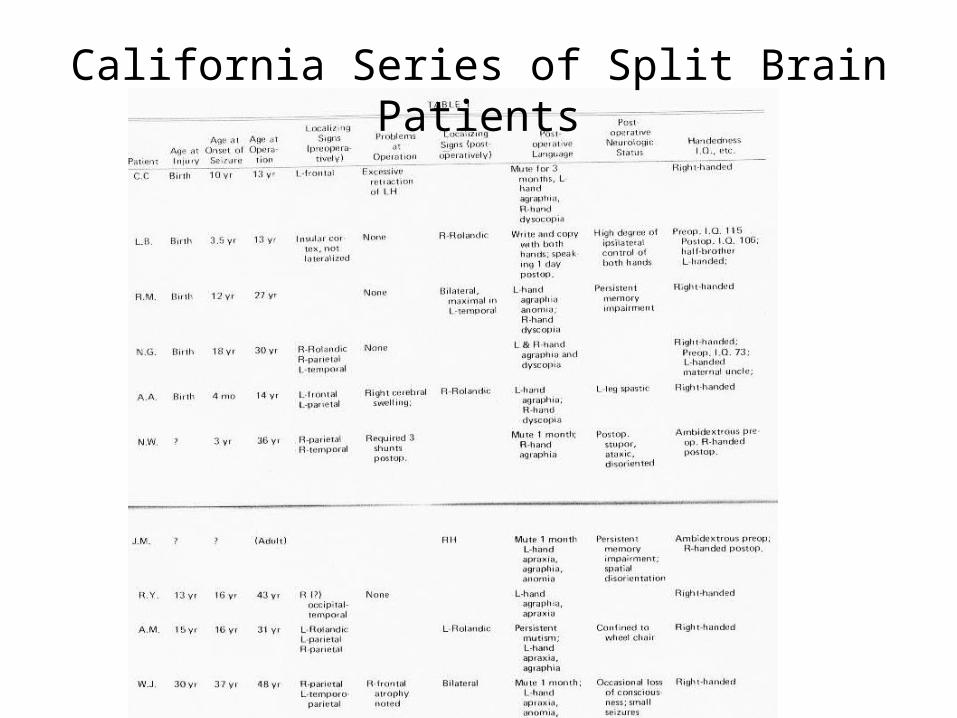
California Series of Split Brain Patients
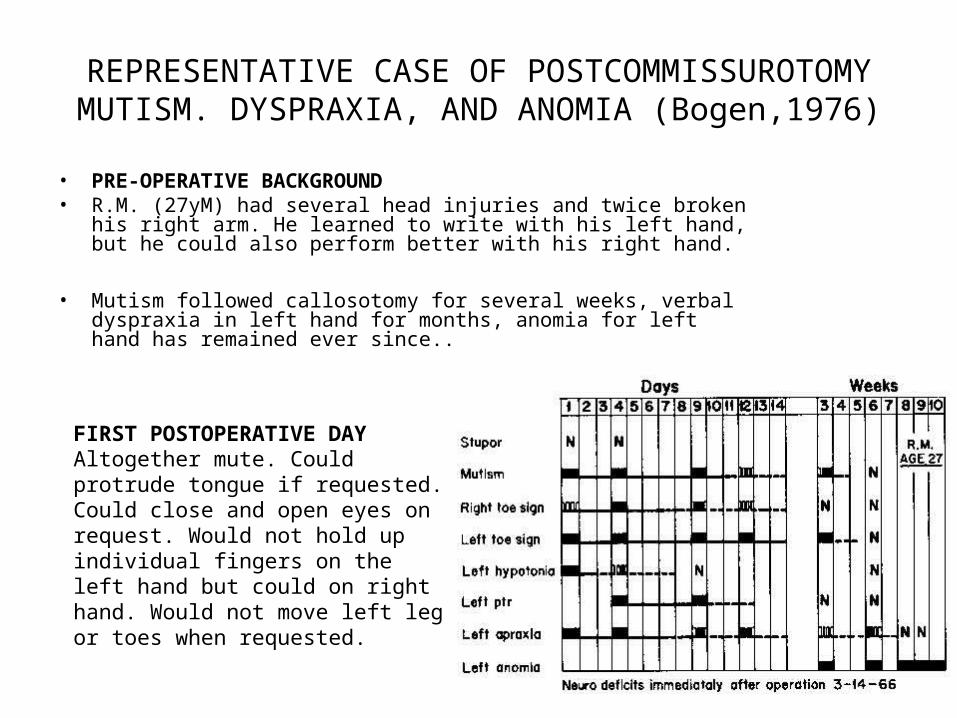
REPRESENTATIVE CASE OF POSTCOMMISSUROTOMY MUTISM. DYSPRAXIA, AND
ANOMIA (Bogen,1976)
• PRE-OPERATIVE BACKGROUND • R.M. (27yM) had several head injuries and twice broken his right arm.
He learned to write with his left hand, but he could also perform better with his right hand.
• Mutism followed callosotomy for several weeks, verbal dyspraxia in left hand for months, anomia for left hand has remained ever since..
FIRST POSTOPERATIVE DAYAltogether mute. Could protrude tongue if requested. Could close and open eyes on request. Would not hold up individual fingers on the left hand but could on right hand. Would not move left leg or toes when requested.
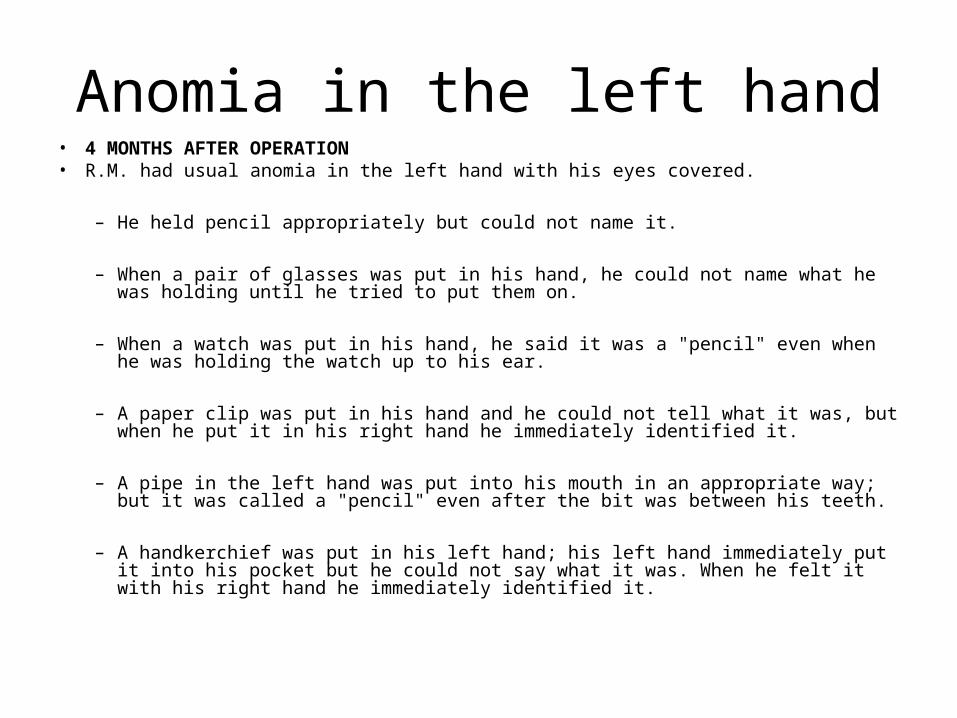
Anomia in the left hand• 4 MONTHS AFTER OPERATION • R.M. had usual anomia in the left hand with his eyes covered.
– He held pencil appropriately but could not name it.
– When a pair of glasses was put in his hand, he could not name what he was holding until he tried to put them on.
– When a watch was put in his hand, he said it was a "pencil" even when he was holding the watch up to his ear.
– A paper clip was put in his hand and he could not tell what it was, but when he put it in his right hand he immediately identified it.
– A pipe in the left hand was put into his mouth in an appropriate way; but it was called a "pencil" even after the bit was between his teeth.
– A handkerchief was put in his left hand; his left hand immediately put it into his pocket but he could not say what it was. When he felt it with his right hand he immediately identified it.
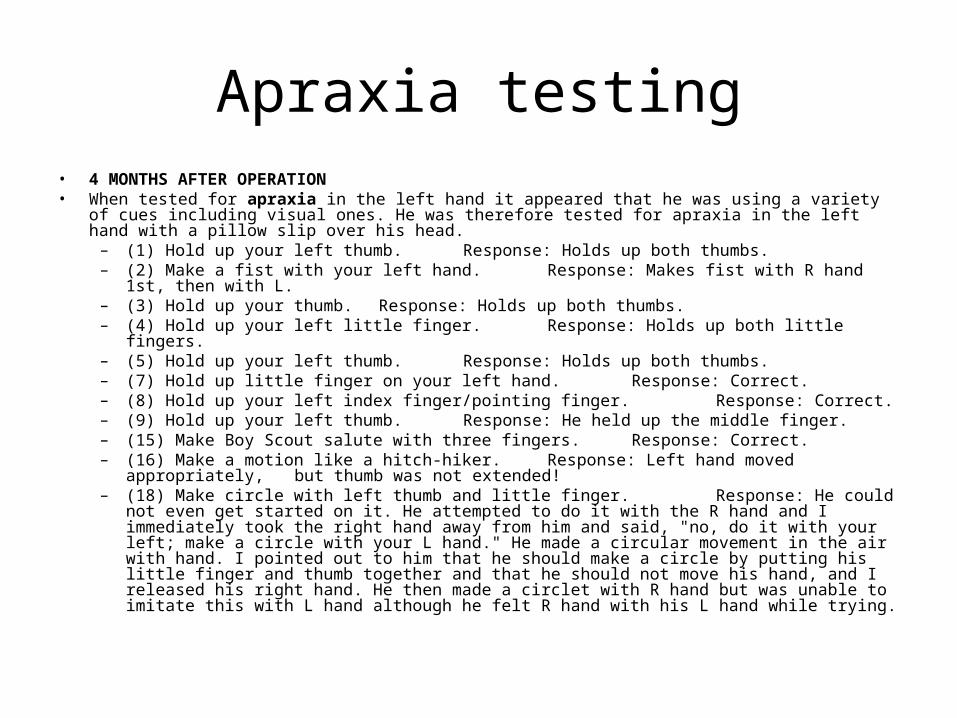
Apraxia testing• 4 MONTHS AFTER OPERATION• When tested for apraxia in the left hand it appeared that he was using a variety of cues including
visual ones. He was therefore tested for apraxia in the left hand with a pillow slip over his head. – (1) Hold up your left thumb. Response: Holds up both thumbs. – (2) Make a fist with your left hand. Response: Makes fist with R hand 1st, then with L. – (3) Hold up your thumb. Response: Holds up both thumbs. – (4) Hold up your left little finger. Response: Holds up both little fingers. – (5) Hold up your left thumb. Response: Holds up both thumbs. – (7) Hold up little finger on your left hand. Response: Correct. – (8) Hold up your left index finger/pointing finger. Response: Correct. – (9) Hold up your left thumb. Response: He held up the middle finger. – (15) Make Boy Scout salute with three fingers. Response: Correct. – (16) Make a motion like a hitch-hiker. Response: Left hand moved appropriately,
but thumb was not extended!
– (18) Make circle with left thumb and little finger. Response: He could not even get started on it. He attempted to do it with the R hand and I immediately took the right hand away from him and said, "no, do it with your left; make a circle with your L hand." He made a circular movement in the air with hand. I pointed out to him that he should make a circle by putting his little finger and thumb together and that he should not move his hand, and I released his right hand. He then made a circlet with R hand but was unable to imitate this with L hand although he felt R hand with his L hand while trying.
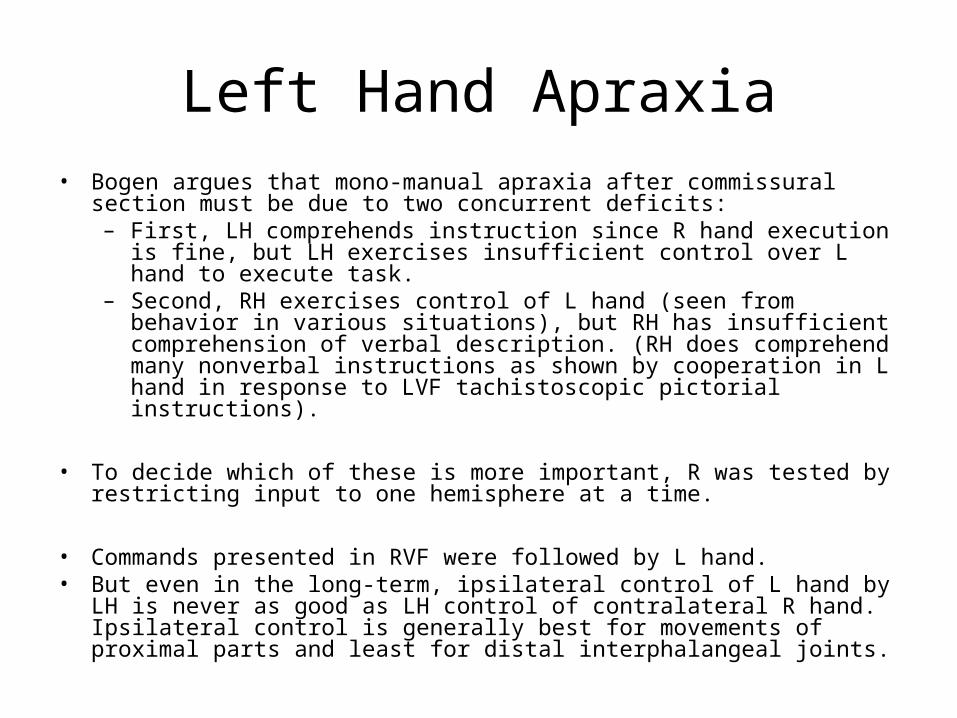
Left Hand Apraxia• Bogen argues that mono-manual apraxia after commissural section must be
due to two concurrent deficits:– First, LH comprehends instruction since R hand execution is fine, but LH
exercises insufficient control over L hand to execute task. – Second, RH exercises control of L hand (seen from behavior in various
situations), but RH has insufficient comprehension of verbal description. (RH does comprehend many nonverbal instructions as shown by cooperation in L hand in response to LVF tachistoscopic pictorial instructions).
• To decide which of these is more important, R was tested by restricting input to one hemisphere at a time.
• Commands presented in RVF were followed by L hand. • But even in the long-term, ipsilateral control of L hand by LH is never as good
as LH control of contralateral R hand. Ipsilateral control is generally best for movements of proximal parts and least for distal interphalangeal joints.
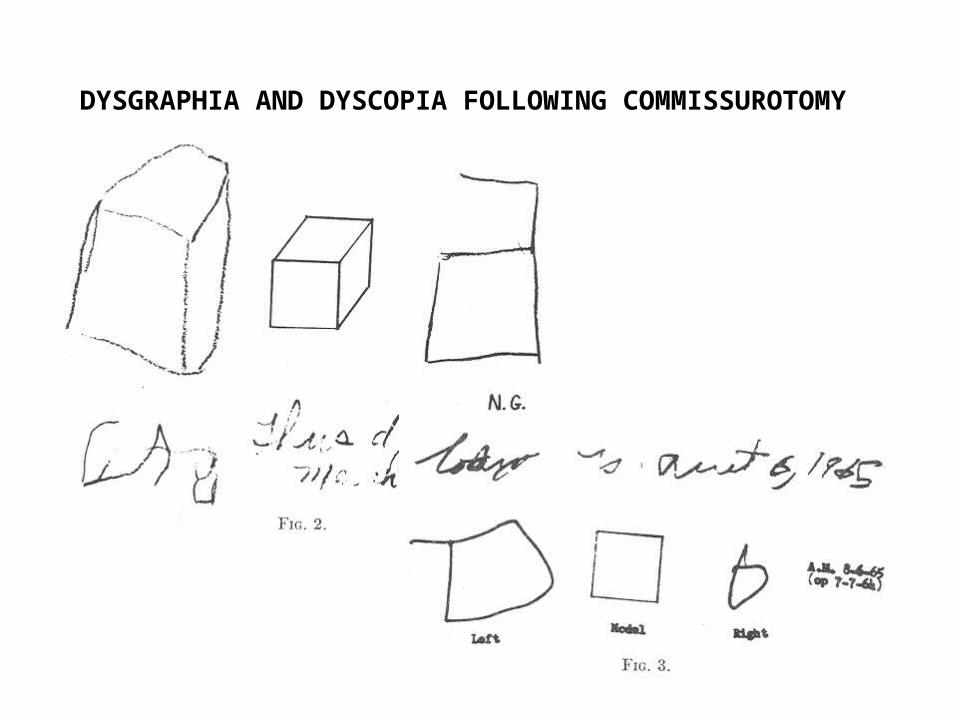
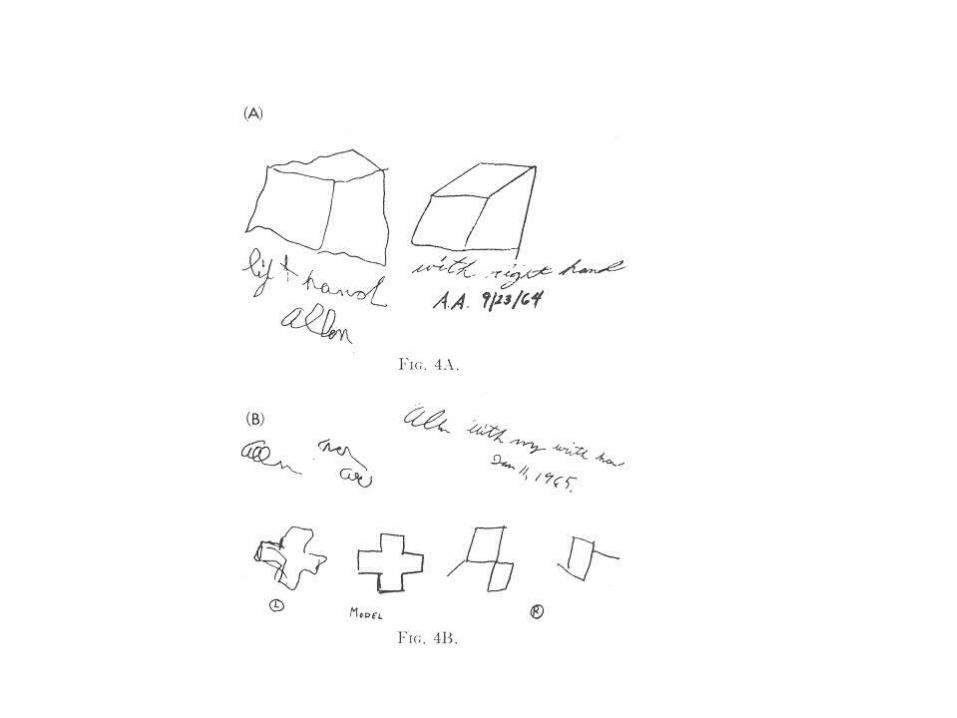
DYSGRAPHIA AND DYSCOPIA FOLLOWING COMMISSUROTOMY
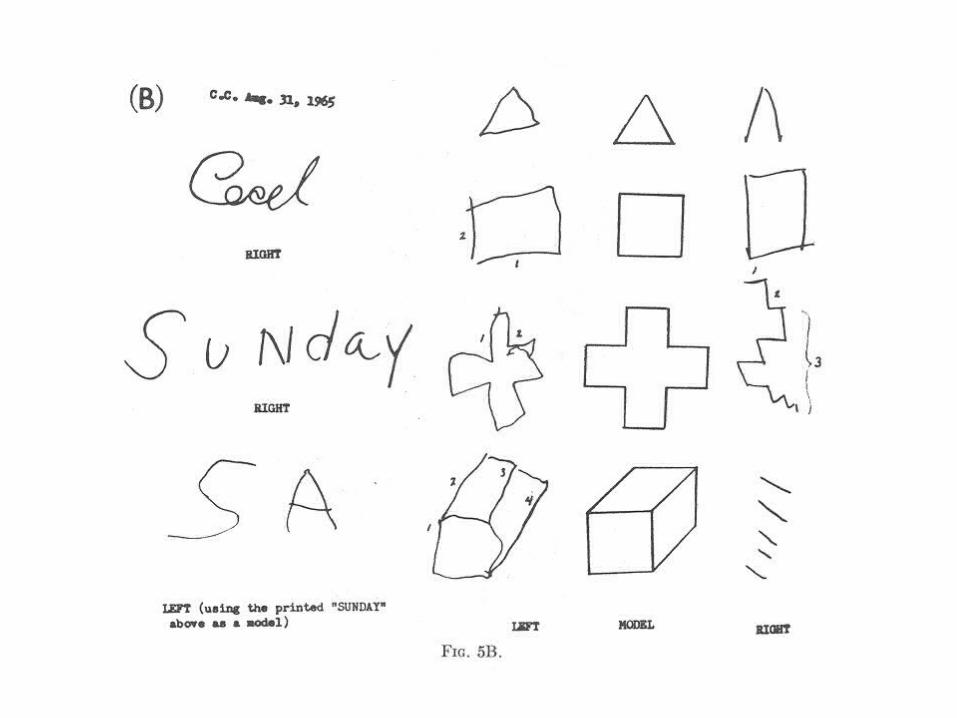
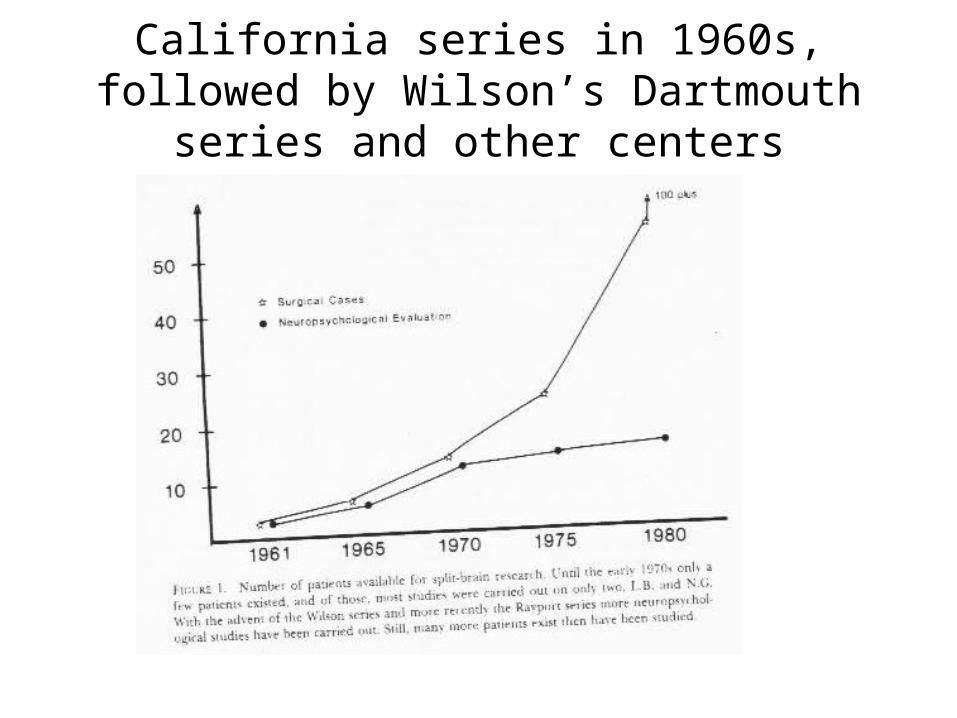
California series in 1960s, followed by Wilson’s Dartmouth series and other centers

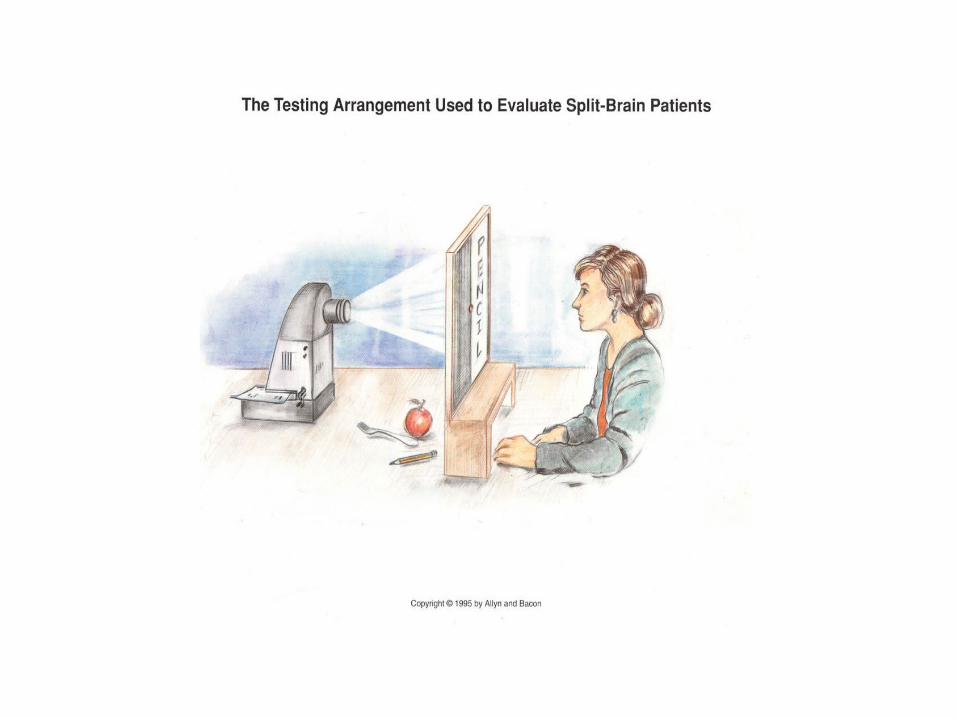
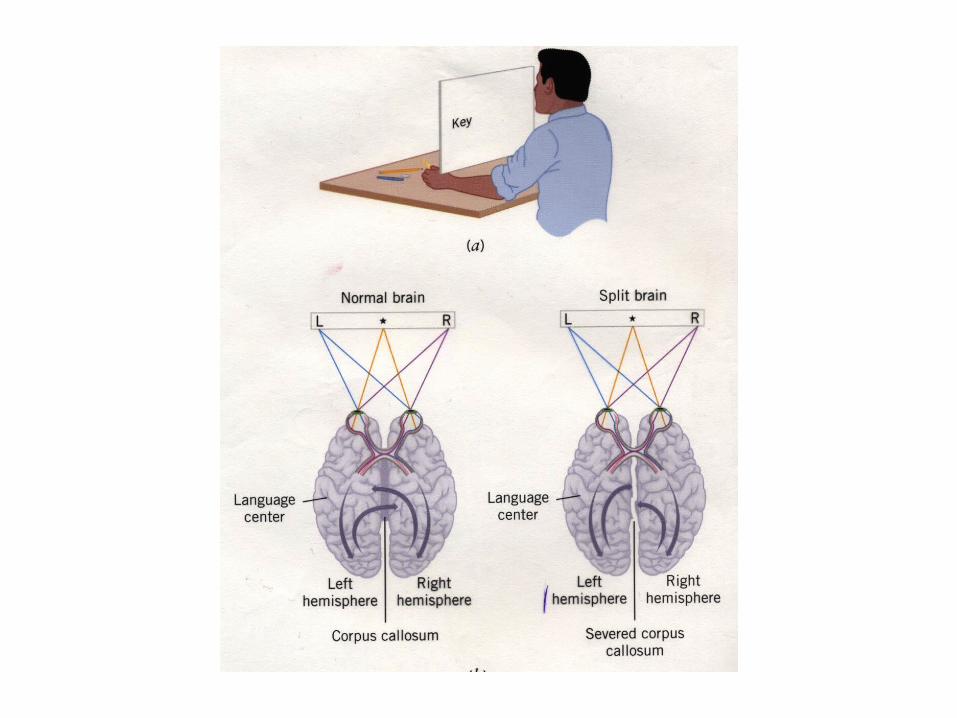
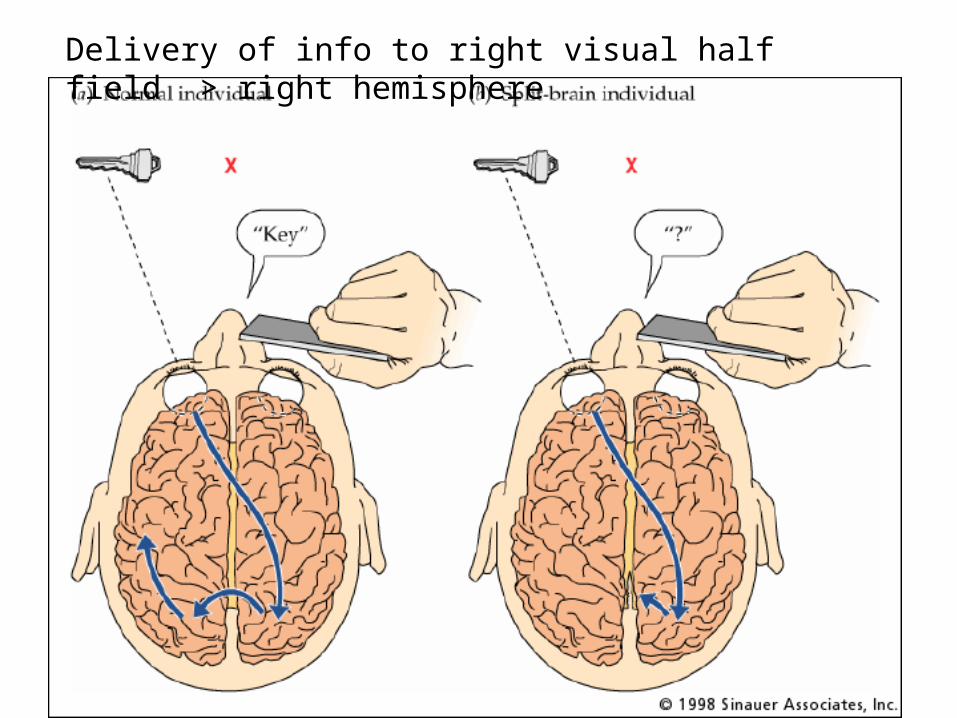
Delivery of info to right visual half field > right hemisphere
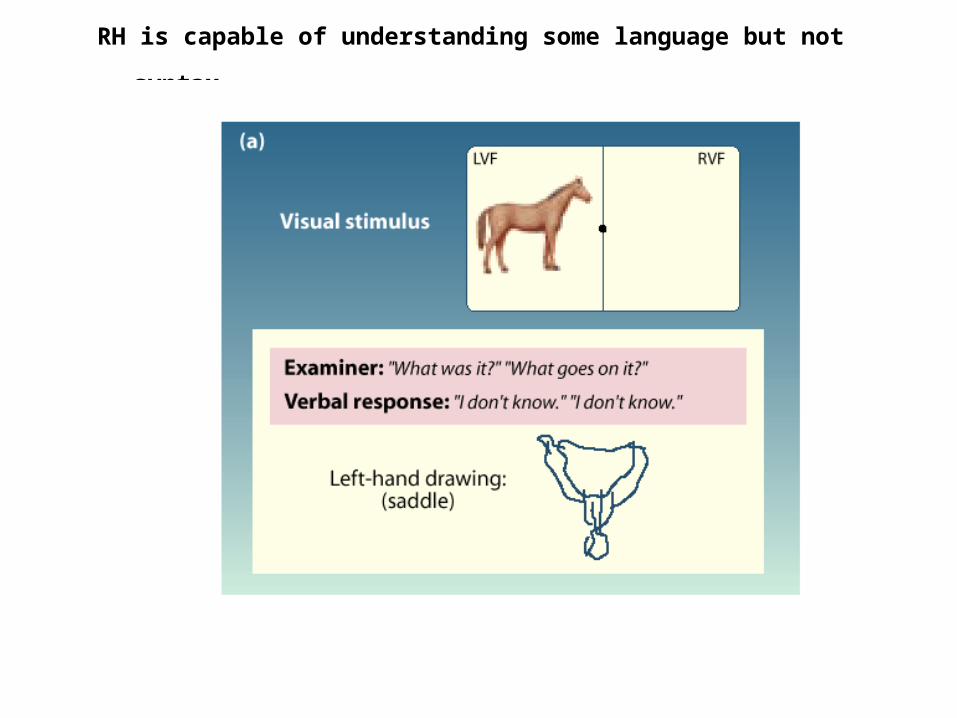
RH is capable of understanding some language but not
syntax
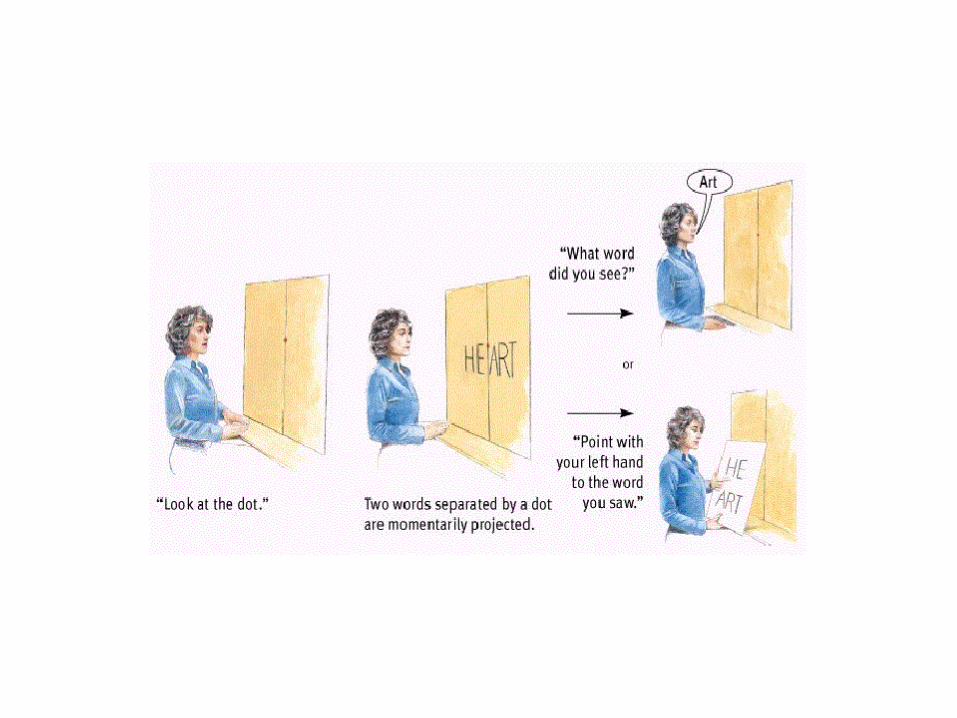
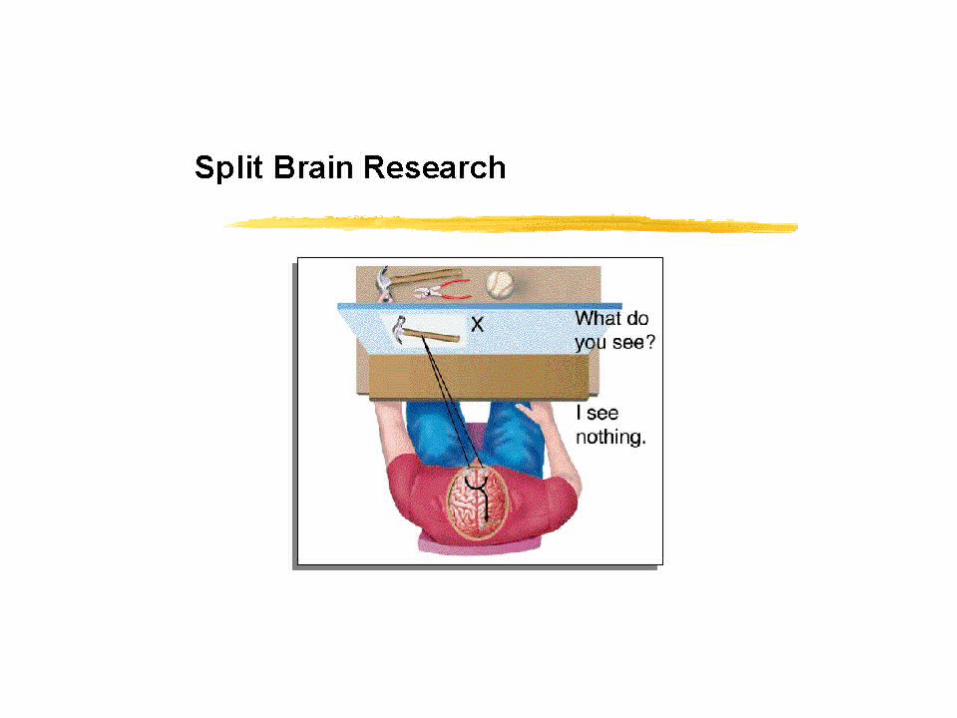
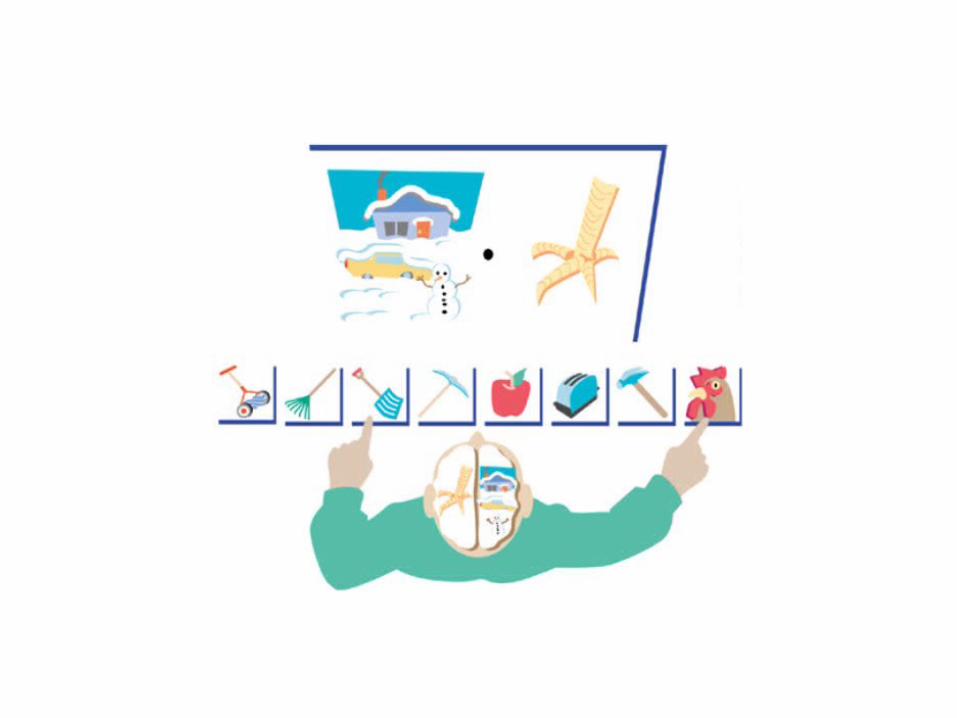
Results of Split brain research
LH has two output systems: right hand and mouth (speech)
RH has only one outputter, the left hand
Left hemisphere can name and point at items it saw in the RVF. The right hemisphere cannot name but can still point at items from the LVF.
Mystery of Right Hemisphere Language
• Focal damage in left hemisphere produces aphasias (Broca, Wernicke, etc), but removal of entire left hemisphere allows right hemisphere verbal functioning– Why?





























