-
8/3/2019 Foramenal Location
1/6
48 oralhealth August 2004
E N D O D O N T I C S
P
redictable endodontic success
demands accurate determina-tion of, and strict adherence tothe
preparation length of the rootcanal space in order to create asmall
wound site and good healingconditions.1 Each portal of exit(POE) on
the root face has biolog-ic significance; this includesthe furcal
canals of bifurca-tions and trifurcations, lat-eral and accessory
arboriza-tions and the myriad of api-cal termini (Figs. 1A-D).
The ability to distinguishbetween the
inner-most(physiologic/histologic fora-men) and outer-most
(ana-tomic foramen) diameters of theapical terminus is essential to
thecreation of the Apical ControlZone.2 The Apical Control Zone isa
mechanical alteration of theapical terminus of the root canalspace
that addresses the rheologyof thermolabile filling materials,
offering resistance and matrix
style retention form against thecondensation pressures of
obtu-ration (Figs. 2A-C).
The determination of the in-strumentation finishing level isone
of the primary factors associ-
ated with the resolution of anendodontic infection both
clinical-ly and histologically.3,4 The major-ity of studies
postulate that opti-mal success rates occur wheninstrumentation,
debridement,disinfection and obturation arecontained within the
region of api-
cal narrowing (bracketed by the
minor apical diameter and apicalforamen.5,6,7 In teeth/roots
withapical periodontitis (AP) for exam-ple, a millimeter loss in
workinglength can increase the chance oftreatment failure by 14
percent.8
The Toronto Study notedthat the highest healingrate differential
(15 percent)was observed in teeth with
AP that were most likelyover-instrumented resulting
in transportation of contam-inated debris periapically.9
The evidence is indisputablethat electronic root canallength
measuring devices
provide significantly more accu-rate results than
radiographs10,11
and therefore offer greater controlof the creation of the
ApicalControl Zone (Fig. 3).
In 1942, Suzuki discoveredthat the electrical resistance
(sin-
The New Era of
Foramenal Location
Kenneth S. Serota, DDS, MMSc, Jorge Vera DDS,Frederick Barnett,
DMD, Yosef Nahmias, DDS, MSc
New modes ofdebridement and disinfection
are constantly arrivingin the endodonticarmamentarium.
-
8/3/2019 Foramenal Location
2/6
August 2004 oralhealth 49
gle current source) between an
instrument inserted into a rootcanal and an electrode attachedto
the oral mucosa registered aconsistent value. In 1962, Sunadausing
a direct current device witha simple circuit, demonstratedthat the
consistent electrical re-sistance between the periodon-tium and the
mucous membranewas 6.5 kOhms [DC Resistance].Through the 1970s,
frequencymeasurements were measuredthrough the feedback of an
oscil-
lator loop by calibration at theperiodontal pocket of each
tooth.This culminated with the effortsof Hasedgawa in 1979 with
theuse of high frequency waves and aspecially coated file which
couldrecord in conductive fluids.
In 1983, Ushiyama introducedthe voltage gradient methodwhere a
concentric bipolar elec-trode measured the current den-sity evoked
in a limited area of
the canal. Maximum potential
was reached when the electrodewas at the apical constriction.The
mid 80s saw the develop-ment of a relative value of fre-quency
response method wherethe apical constriction was pickedby filtering
the difference be-tween two direct potentials aftera 1 kHz
rectinlinear wave wasapplied to the canal space.
A Third Generation electronicforamenal locator (EFL) devel-
oped in the late 80s by Kobayashiused multi-channel
impedance/ratio based technology to simul-taneously measure the
imped-ance of two different frequencies,calculate the quotient of
theimpedance and express it interms of the position of the
elec-trode (file) in the canal. Thisformed the basis of the
technolo-gy used in the ROOT ZX (J.Morita USA, Inc. Irvine,
CA)where no calibration was re-
quired and a microprocessor cal-
culated the impedance quotient.
Fourth Generation EFLs (Ele-ments Diagnostic, SybronEndo,Orange,
CA) measure resistanceand capacitance separately ratherthan the
resultant impedance
value (impedance being a func-tion of resistance and
capaci-tance) [Fig. 4A]. There can be dif-ferent combinations of
values ofcapacitance and resistance thatprovide the same impedance
(and
thus the same foramenal read-ing); this can then be brokendown
into the primary compo-nents and measured separatelyensuring better
accuracy and lesschance for error. In addition, theElements unit
uses a lookupmatrix (Fig. 4B) rather than mak-ing any internal
calculations.
While calculations take place very quickly, they are still
rela-tively much slower than simply
E N D O D O N T I C S
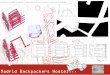
FIGURE 1AArrows indicate mul-tiple POEs associated with the
mesial-buccal and distal-buccalapices of a maxillary first
molar.
FIGURES 1B & CThe complexity of the root canal system has
been graphically evidencedsince the work of Hess in the 1920s.
Radical improvement in materials and techniques arenow enabling the
clinician to replicate that complexity as evidenced in the cleared
speci-men (1B) and the radiograph (1C). (Courtesy of Dr. William
Watson.)
FIGURE 1D(right) The number, shape and diameter of
thephysiologic foramena at the root apex mandate the continu-ing
pursuit of excellence in endodontics through
increasedsophistication in materials and methods and the alliance
of sci-entific innovation and clinical acumen. From Gutierrez
andAguayo, OS, OM, OP June 1995.
-
8/3/2019 Foramenal Location
3/6
looking up comparative values ina pre-calculated matrix (in
therange of 10-20x slower). Thisallows the unit to crunchthrough
much more data in agiven amount of time; a largersample size tends
to make theresults more accurate. Figure 5demonstrates the
technologic
protocol difference between 3rdand 4th generation
foramenallocators.
In the course of preparation ofthis paper, the importance of
regu-lation of battery power wasassessed.The Elements
Diagnosticcircuitry runs at 3.3 volts (commonfor electronics),
which is internallyregulated to remain extremelyconsistent. The
battery pack israted at a nominal 6 volts, 7.5 volts
with a full charge and no load.
As the battery pack is depleted,the voltage decreases to a
pointwhere the electronics cannot con-tinue to regulate the
operating
voltage to such a precise valueand therefore the signals
sentthrough the electrodes will not beas reliable either. The
device is setto automatically shut off whenbattery voltage is a
little abovethis threshold.
The ROOT ZX runs on AAalkaline or lithium batteries(mixing types
is to be avoided)
and will shut itself off after twen-ty minutes. There is a bar
graphon the face of the unit which indi-cates residual battery
power. Thequestion of the accuracy of sig-nals sent through the
electrode isin doubt if the battery powerlevel drops below the
first threeor four bars (authors observa-tion) [Fig. 7].
A paper point measurement,foramenal detection technique has
been advocated by Rosenberg.12 Itis designed to determine the
pointpositional location of the apical
foramen as well as three-dimen-sional information regarding
theslope of the foramen. A trial paperpoint is placed 1mm short of
theEFL determined length. If thepoint is retrieved dry, it
isadvanced further until fluid isnoted. The length of the segmentof
the point that is dry is noted.
This sequence is repeated asevidenced in Figs 6A, B & C
andthe maximum length of the point
50 oralhealth August 2004
E N D O D O N T I C S
FIGURE 2AThe definitions of the morphologicentities comprising
the regional terminus of the
apex are shown diagrammatically with super-imposition of the
histologic anatomy.
FIGURE 2BRetreatment of tooth #4.6 with K3 nickel-titanium
[NiTi] files(G Pack system). The goal is identification of the
histologic terminus of theroot canal space and the use of variable
tapered rotary NiTi instrumen-tation to create an apical control
zone and optimize the seal producedby the new generation of resin
thermoplastic root canal filling materialsand sealers. (Courtesy of
Dr. Gary Glassman.)
FIGURE 2CRetreatment of tooth #3.6 with K3 nickel-titanium
[NiTi] filesVarible Tip Varible Taper (VTVT) system. The K3 file
sequence after thetwo Orifice Openers/Body Shapers is: #35/.06,
#30/.04, #25/.06,#20/.04. In the majority of cases, the #25/.06 or
the #20/.04 willreach the desired working length on the first pass.
If not, the sequence isrepeated from the beginning. (Courtesy of
Dr. Fred Barnett.)
-
8/3/2019 Foramenal Location
4/6
that can be placed into the canaland remain dry reflects the
ori-entation of the cavosurface ofthe apical foramen (Fig. 6D).
There are several basic condi-tions that ensure accuracy ofusage
for all generations of fora-menal locators;
1) preliminary debridementshould remove most tissue ordebris
obstructions,
2) cervical leakage must beeliminated and excess fluidremoved
from the chamber asthis may cause inaccuratereadings,
3) extremely dry canals may re-sult in low readings [longworking
length],
4) long canals can produce highreadings [short
workinglengths],
4) lateral canals may give afalse foramenal reading, and
5) the use with open apices is con-traindicated. The residual
fluidin the canal should possess alow conductivity value. In
de-scending order of conductivitythese are; sodium
hypochlorite(NaOCl 5.25 percent), EDTA(17 percent), Smear
Clear(SybronEndo, Orange, CA),
saline, FileEze (UltradentProducts, S. Jordan, UT), andisopropyl
alcohol.
It is advisable to use a crowndown canal preparation
tech-nique13 and take the preliminaryelectronic measurement using
afile that is approximately bigenough to bind at the apical
con-
striction.14 A second workinglength measurement is
advisableafter flaring the coronal and mid-dle thirds as shortening
of workinglength occurs when instrumentingcurved canals; this
shortening can
vary from 0.22mm to 0.5mm. How-ever, once coronal flaring has
beendone little change in lengthoccurs.15,16 From a
medico-legal
52 oralhealth August 2004
E N D O D O N T I C S
FIGURE 3The subtraction approxima-tion technique; the average
disparity of0.5 to 1mm between the radiographicapex or terminus
(RT) and the cavosur-face point of exit of the root canal spaceused
as the standard for length determi-nation is fraught with
inaccuracy.(Courtesy of Dr. William Watson.)
FIGURE 4AFourth Generation forame-nal locator (Elements
Diagnostic,SybronEndo, Orange CA).
FIGURE 4BLookup matrix generatedfrom in-vivo studies (x-axis
capacitance,y-axis resistance, vertical z-axis is resul-tant
displayed location in the canal).
FIGURE 5
The graphic shows the technologic difference between the
operation ofthird and fourth generation foramenal locators.
-
8/3/2019 Foramenal Location
5/6
standpoint, a verification radi-ograph is recommended at
this
juncture. It is also advisable to doa final confirmation EFL
readingafter drying the canal and priorto obturation.
In the case of the third gener-ation ROOT ZX (Fig. 7),
theworking length of the canalused to calculate the length ofthe
filling material is actuallysomewhat shorter; the length ofthe
canal up to the apical seat(i.e. the end point of the
fillingmaterial) is found by subtract-ing 0.5 to 1.0mm from the
work-ing length indicated by the 0.5reading on the meter.
The meters 0.5 reading indi-cates that the tip of the file is
inthe vicinity of the apical fora-men (i.e. an average of 0.2
to0.3mm past the entrance to theapical constriction towards
theapex). The disparity betweenthe EFL reading of such unitsas the
Ultima EZ and the ROOTZX is demonstrated to be the+.0.5/-0.5
position indicated bythe 0.5 reading on the meter.
This finding has been consis-tently verified by
numerousinvestigators.17,18
A recent investigation of thefourth generation EFL, the
Ele-ments Diagnostic (Sybron Endo,Orange, CA) demonstrated
anunprecedented level of accuracyin usage. Length calibrationswere
performed on teeth to beextracted, the files cemented toposition
and the teeth cleared for
microscopic examination.19 In 22out of 22 cases where the
readingof the file was taken to 0.0 or intothe minus numbers and
with-drawn to the 0.5 mark on thescale, the file terminus was
con-sistent with the position of the api-cal constriction (Fig.
8A).
When the file was cementedafter going down to the 0.5 mark,in 20
out of 24 cases, the file waspositioned a distance of 0.5mm
from the external foramen (Fig.8B). Of note was the finding
thatwhen the device displayed aminus number, the file wasalways
beyond the apical con-striction and in most cases out ofthe root
structure (Fig. 8C).
CONCLUSION
Evolutionary technologic soph-istication is the hallmark of
allscientific and clinical endeavour.Endodontics is the bedrock of
allcomprehensive care. As such, it isimperative that predictable
endo-
August 2004 oralhealth 53
E N D O D O N T I C S
FIGURE 6BHydrostatics will cause peri-apical fluids to
accumulate on theoverextended paper point. (Courtesy of Dr.David
Rosenberg.)
FIGURE 6CThe angle of the paper pointdiscolouration reflects the
three dimension-al orientation of the cavosurface of the api-cal
foramen. (Courtesy of Dr. David Rosenberg.)
FIGURE 6DThe terminus of the canal isnot a point in space; it is
a multidimen-sional, topographically diverse plane.(Courtesy of Dr.
David Rosenberg.)
FIGURE 6AThe paper point is intro-duced coronal to the level of
the EFLdetermination. As it is shy of the cavo-surface of the canal
terminus, it shouldremain dry. (Courtesy of Dr. David
Rosenberg.)
FIGURE 7The Root ZX is a fully auto-matic, self-calibrating root
canal fora-menal locator.
FIGURE 8AWhen the file glide path isstopped at 0.5 on the
digital display,the units accuracy in determining theapical foramen
is less than 85 percent.
-
8/3/2019 Foramenal Location
6/6
dontic success is projected asclose to 100 percent as
biological-ly possible. Outcome assessment
studies indicate that formenalposition is a pivotal factor if
notthe pivotal factor in the mostfavourable end result. New modesof
debridement and disinfectionare constantly arriving in
theendodontic armamentarium. TheFourth Generation of
foramenallocators will ensure that theirusage in evolutionary
endodontic
protocols is optimized. OH
Drs. Serota, Vera, Barnett, Nahmias,
Watson and Glassman are membersof the cybercommunity ROOTS
www.rxroots.com.
Oral Health welcomes this original
article.
REFERENCES
1. Simon JHS. The apex: How critical is it? Gen Dent1994
42:330-4.
2. Serota KS, Nahmias Y, Barnett F, Brock M, Senia
ES.Predictable endodontic success. The apical control
zone. Dent Today. 2003 May;22(5):90-7.3. Chugal NM, Clive JM,
Spangberg LS. Endodontic
infection: Some biologic and treatment factors associ-ated with
outcome. Oral Surg Oral Med Oral PatholOral Radiol Endod. 2003
Jul;96(1):81-90.
4. Ricucci D, Langeland K. Apical limit of root
canalinstrumentation and obturation, Part II: A histologicalstudy.
Int Endod J 1998;31:394-409.
5. Dammaschke T, Steven D, Kaup M, Ott KH. Long-term survival of
root-canal-treated teeth: A retrospec-
tive study over 10 years. J Endod. 2003 Oct;29(10):638-43.
6. Kojima K, Inamoto K, et al. Success rate of endodon-tic
treatment of teeth with vital and nonvital pulps. Ameta-analysis.
Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2004
Jan;97(1):95-9.
7. Basmadjian-Charles CL, Farge P, Bourgeois DM,Lebrun T.
Factors influencing the long-term results ofendodontic treatment: a
review of the literature. IntDent J. 2002 Apr;52(2):81-6.
8. Vachey E, Lemagnen G, Grislain L, Miquel JL. Alter-natives to
radiography for determining root canallength. Odontostomatol Trop.
Sep 2003;26(103):15-8.
9. Friedman S, Abitbol S, Lawrence HP. TreatmentOutcome in
Endodontics: The Toronto Study. Phase I:Initial Treatment. J Endod
December 2003;29(12):787-793.
10. Pratten D, McDonald NJ. Comparison of radiographic
and electronic working lengths. 1996 J Endo
April1996;22(4):173-6.
11. Pommer O. In vitro comparison of an electronic rootcanal
length measuring device and the radiographicdetermination of
working length. Schweiz MonatsschrZahnmed. 2001;111(10):1165.
12. Rosenberg D. Paper Point Technique: Part II.Endodontic
Practice May 2004 7;(2):7-11.
13. Ibarrola JL, Chapman BL, Howard JH, Knowles KI,Ludlow MO.
Effect of preflaring on Root ZX apex loca-tors. J Endod September
1999;25(9):625-6.
14. Nguyen HQ, Kaufman AY, Komorowski RC, FriedmanS. Electronic
length measurement using small andlarge files in enlarged canals.
Int Endod J. 1996Nov;29(6):359-64.
15. Davis RD, Marshall JG, Baumgartner JC. Effect ofearly
coronal flaring on working length change incurved canals using
rotary Nickel-Titanium versus
stainless steel instrumentation. J Endod 2002;28:438-441.
16. Caldwell JL. Change in working length following
instru-mentation of molar canals. Oral Surg Oral Med OralPath 1976;
41:114-8.
17. Welk A, Baumgarnter C, Marshall G. An in vivo com-parison of
two frequency-based electronic apex loca-tors. J Endod August 2003;
29(8):497-500.
18. Shabahang S, Goon WW, Gluskin AH. An in vivo eva-lution of
ROOT ZX electronic apex locator. J EndodNovember 1996;
22(11):616-8.
19. Vera J, Gutierrez M. Accurate working lengthdetermination
using a fourth generation apex loca-tor (in press).
FIGURE 8BWhen the file reaches theperiodontal ligament, the
digital displayshows 0.0. When the file is withdrawn0.5mm, an
instrumentation terminuspoint consistent with the apical
constric-tion resulted 100 percent of the time.
FIGURE 8CWhen the file glidepath is extended into a
negativereading on the display, the filewas out of the canal in all
cases.
54 oralhealth August 2004
E N D O D O N T I C S