Embed Size (px)
Citation preview

NORTH OF SCOTLAND PLANNING GROUP
Shaping the Future of Restorative Dentistry
for the North of Scotland
A Report from the NHS Tayside Workshop
June 2010

This report provides the reader with an insight in to the events of the NHS Grampian Restorative Dentistry Workshop which took place in Inverness on 21 st July 2010. It summarises the presentations, the facilitated sessions and the outcomes from the day and gives an indication as to the further work required to inform the debate to “Establish a Regional Service for Restorative Dentistry in the North of Scotland”.
Intentionally, the report does not contain any recommendations for the North of Scotland Planning Group. Recommendations will form part of a full and final report which draws on the evidence base and the findings from consultation across all six North of Scotland Boards. It is anticipated that the full and final report will be
presented to NoSPG by the end of 2010.
oOo

CONTENTS
1. Programme
2. Invitee List
3. Introduction
4. Current Service – The NHS Tayside Perspective Dr E Connor, Clinical Lead, Integrated Dental Services
4.1 What the Data Tells us 4.2 The Consultant Perspective 4.3 The Primary Care Perspective and Patient Stories 4.4 NHS Tayside Dental Laboratory 4.5 Voice of the Staff 4.6 Stakeholder Reflections
5. Mapping the Patient Journey
6. Future State
Appendices
Appendix 1 Opportunities Summary

Chaired/Facilitated By
Dr E. Connor, Clinical Lead, NHS Tayside
Present
Dr Anne Shearer, Consultant in Restorative Dentistry, NHS Tayside Dr Brendan J Scott, Consultant in Restorative Dentistry, NHS Tayside Helen Strachan, Regional Manager, NoS OH&D
Apologies
Ms Karen Wright, Integrated Dental Services Manager

3. Introduction
The Restorative Dentistry service across the North of Scotland is struggling to meet demand and the North Boards are experiencing considerable pressures to comply with the Scottish Government’s 18/52 referral to treatment standards.
At their meeting on 14 th April 2010, members of the North of Scotland Planning Group (NoSPG) reaffirmed their commitment to the North of Scotland Oral Health and Dentistry work stream. With regard to services for Restorative Dentistry, members agreed that quick fix solutions were not an option and that “A Regional Service should be formally established for Restorative Dentistry” thus ensuring:
• Public Value for money • HEAT Targets (Health, Efficiency, Access, Treatment) are met • Service Quality Outcomes are uniform and agreed across the North • Compliance with the18/52 Referral to Treatment (RTT) standard • Unified corporate and clinical governance issues are addressed • There is equity of service across the North • A unified approach to the delivery of Restorative Dentistry Services across the North
Clinical Benefits
The perceived clinical benefits of a regional approach to the delivery of Restorative Dentistry services include:
• Support to Clinicians – decisionmaking – emergency management – skill sharing – inclusivity
• Patient and Access Benefits – less travel to access expertise – more rapid access – better distribution and utilisation of resource – shorter waiting times
• Educational Benefits – shared learning – common learning pathways – development and maintenance of skills – inclusivity and the sense of belonging to a wider network
• Governance – setting standards – audit – improving and adjusting standards
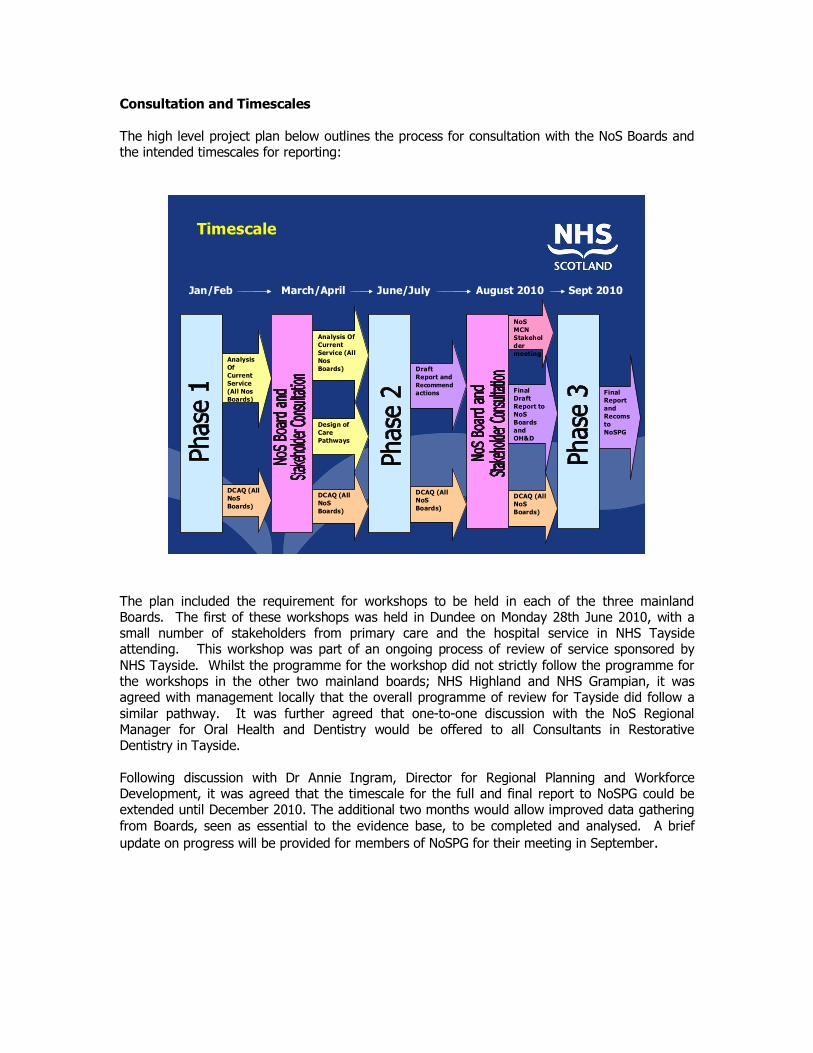
Consultation and Timescales
The high level project plan below outlines the process for consultation with the NoS Boards and the intended timescales for reporting:
North of Scotland Planning Group
North of Scotland Planning Group
Timescale
Analysis Of Current Service (All Nos Boards)
DCAQ (All NoS Boards)
Analysis Of Current Service (All Nos Boards)
Design of Care Pathways
DCAQ (All NoS Boards)
NoS MCN Stakehol der meeting
Draft Report and Recommend actions
DCAQ (All NoS Boards)
Final Draft Report to NoS Boards and OH&D
DCAQ (All NoS Boards)
Jan/Feb March/April June/July August 2010 Sept 2010
Final Report and Recoms toNoSPG
The plan included the requirement for workshops to be held in each of the three mainland Boards. The first of these workshops was held in Dundee on Monday 28th June 2010, with a small number of stakeholders from primary care and the hospital service in NHS Tayside attending. This workshop was part of an ongoing process of review of service sponsored by NHS Tayside. Whilst the programme for the workshop did not strictly follow the programme for the workshops in the other two mainland boards; NHS Highland and NHS Grampian, it was agreed with management locally that the overall programme of review for Tayside did follow a similar pathway. It was further agreed that onetoone discussion with the NoS Regional Manager for Oral Health and Dentistry would be offered to all Consultants in Restorative Dentistry in Tayside.
Following discussion with Dr Annie Ingram, Director for Regional Planning and Workforce Development, it was agreed that the timescale for the full and final report to NoSPG could be extended until December 2010. The additional two months would allow improved data gathering from Boards, seen as essential to the evidence base, to be completed and analysed. A brief update on progress will be provided for members of NoSPG for their meeting in September.

4. The Current Service
4.1 Dr E Connor, Clinical Lead, Integrated Dental Services
The Restorative Dental Service in NHS Tayside is under considerable strain with demand in the form of referrals to the service far outstretching the available capacity. Dr Connor asked the question, “How can we work together to ensure that patients have appropriate access to secondary care dental services?”
She defined the role of a Dental Hospital as being:
• To provide a clinical environment in which the dental team members & dental specialists of the future are trained
• To provide clinical care for patients
In comparison, the role of Hospital Dental Services was:
• Consultant led services • To provide advice, including treatment planning, for patients and their primary care
practitioner • To provide NHS treatment for patients that requires specialist knowledge and skills that
would not normally be expected of the GDP
Dr Connor continued:
Setting the context for Setting the context for developing referral guidelines developing referral guidelines
l Clinical capacity – available staff & clinical space
l Government targets for treatment l Financial constraints
18 week RTT 18 week RTT – – what is this? what is this?
l Government requirement of NHS Boards l Patient will start definitive treatment within 18 weeks of referral from GDP to consultant led service
l For dentistry – by December 2011 l Current target: l New referrals should have an initial appointment within 12 (9) weeks of referral
When does 18 RTT apply? When does 18 RTT apply?
l For all patients referred for specialist care
l For all patients who require any inpatient care e.g. a GA
When does 18 RTT not apply? When does 18 RTT not apply?
l Self referrals l Patients who treated by the undergraduates.

The number of referrals made to all Services at Dundee Dental Hospital are as follows:
• April 08 – March 09 5324 • April 09 – March 10 6137
The number of New Patient referrals by specialty was reported as follows:
NP referrals by specialty NP referrals by specialty
l June 08 – May 09
l Oral surgery 1505 l Oral medicine 739 l Ortho. 462 l Restorative 2062 l Paediatrics 588
l June 09 – May 10
l 1820 21% l 916 24% l 581 26% l 2376 15% l 665 13%
Additional data relating to the Restorative Dentistry Service was provided by Ms Karen Wright, Clinical Services Manager, Integrated dental Services for NHS Tayside after the meeting. The Data Templates revealed the following:
DEMAND
2008/9 2009/10 Ave Total referrals 2073 2270 Removals Net Demand
REFERRAL SOURCE
The source of referrals includes Dentists in Primary Care, Consultants in the Acute Sector, and others. The distribution of referrals from these sources was illustrated as follows:
2008/9 2009/10 Ave %
Dentists 2024 2202
Consultants
Others 49 68
Total 2073 2270
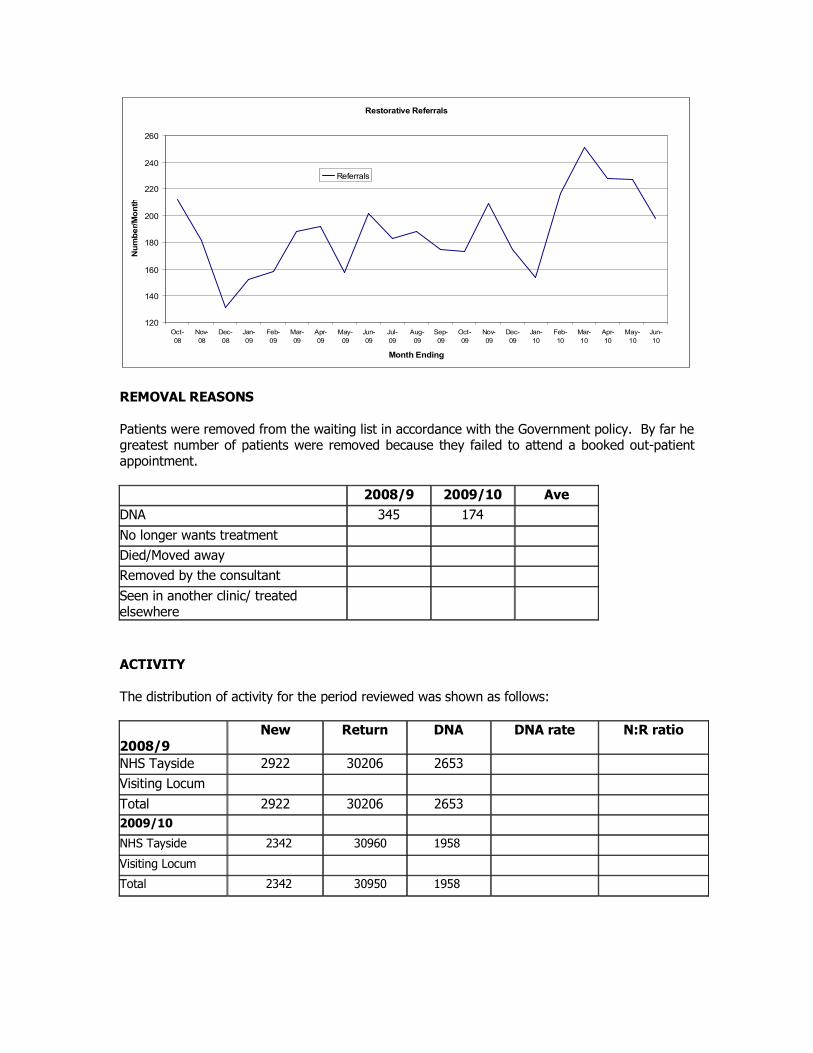
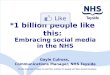
Restorative Referrals
120
140
160
180
200
220
240
260
Oct 08
Nov 08
Dec 08
Jan 09
Feb 09
Mar 09
Apr 09
May 09
Jun 09
Jul 09
Aug 09
Sep 09
Oct 09
Nov 09
Dec 09
Jan 10
Feb 10
Mar 10
Apr 10
May 10
Jun 10
Month Ending
Num
ber/M
onth
Referrals
REMOVAL REASONS
Patients were removed from the waiting list in accordance with the Government policy. By far he greatest number of patients were removed because they failed to attend a booked outpatient appointment.
2008/9 2009/10 Ave DNA 345 174 No longer wants treatment Died/Moved away Removed by the consultant Seen in another clinic/ treated elsewhere
ACTIVITY
The distribution of activity for the period reviewed was shown as follows:
2008/9 New Return DNA DNA rate N:R ratio
NHS Tayside 2922 30206 2653 Visiting Locum Total 2922 30206 2653 2009/10
NHS Tayside 2342 30960 1958
Visiting Locum
Total 2342 30950 1958

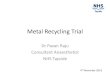
Waiting Times for a First New Outpatient Appointment
Restorative Dentistry Patients Waiting > 9 weeks
0
100
200
300
400
500
600
Jan 09
Feb 09
Mar 09
Apr 09
May 09
Jun 09
Jul09 Aug 09
Sep 09
Oct 09
Nov 09
Dec 09
Jan 10
Feb 10
Mar 10
Apr 10
May 10
Jun 10
Month Ending
Patient Num
bers
>9 wks
Treatment Waiting Times
ProstheticsTreatment Hopper(Waiting Times)
0
50
100
150
200
MidFeb 10 End Feb 10 End Mar 10 End Apr 10 End May 10 End Jun 10
Period Ending
Num
ber o
f Patients Waitin
g Treatm
ent
2yrs +
12 yrs
3952 wks
2639 wks
1826 wks
1218 wks
912 wks
69 wks
36 wks
03 wks
ConservationTreatment Hopper(Waiting Times)
0
100
200
300
400
End Feb 10 End Mar 10 End Apr 10 End May 10 End Jun 10
Period Ending
Num
ber o
f Patients Waitin
g Treatm
ent
2yrs +
12 yrs
3952 wks
2639 wks
1826 wks
1218 wks
912 wks
69 wks
36 wks
03 wks

NB With regard to the data templates above, it is believed that, where there is no return documented, this is due entirely to the fact that the information is not currently recorded for dental specialties.
Validation of the waiting lists has been taking place along with subtypes being added to patients to separate review from treatment patients.
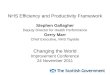
4.2 Restorative Referrals – Dr A Shearer, Consultant in Restorative Dentistry
Dr Connor identified the 12 Consultants in Restorative Dentistry working at Dundee Dental Hospital. These are:
• Professor WP Saunders Professor DNJ Ricketts • Dr J Radford Dr M Lyons • Dr BJ Scott Dr J Drummond • Dr RG Chadwick Dr A Hall • Dr P Maillou Mr CJ Allan • Dr S Manton Dr AC Shearer
The majority of these consultants (10) are employed by NES in a teaching role and providing two service sessions per week. Of the remaining two Consultants, one works fulltime for the NHS and the other works on a parttime basis.
Referrals to the Restorative Dentistry Service at Dundee Dental School were illustrated as per the graph opposite.
Restorative referrals 20092010
0
50
100
150
200
250
300
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May 2010 2009
2152 in 2009, x in 5 months of 2010

Referrals for the period April to June 2010, excluding removal Prosthodontics, appear as follows:
Restorative referrals 2010 (excluding removable prosthodontics)
0
50
100
150
200
250
Jan Feb Mar Apr May June
Others Perio Endo
Following discussion with the Consultants in Restorative Dentistry at DDH, it was agreed that the use of a standard letter of referral to the service should be adopted. A copy of the proposed letter template was provided and is attached at appendix 1.
DUNDEE DENTAL HOSPITAL AND SCHOOL Restorative Referral
1.Referrer details Name ………………………………………………………… Title Mr/Miss/Mrs/Dr (please circle) Address ……………………………………………………… Tel No ………………………………… ……………………………………………………………….. Postcode ………………………………… ………………………………………………………………………………………………………………...
2.Patient details Name …………….……………………………………………. Title Mr/Miss/Mrs/Dr (please circle) Address ……………………………………………………….. Tel No ………………………………… ………………………………………………………………… Postcode ………………………………… ………………………………………………………………………………………………………………..
3.Scheduling Information Minimum notice required to attend: ……………………………………………………………………… Known times patient unable to attend: ………………………………………………………………………
4.Predominant dental problem (tick the most appropriate box) Perio Treatment Planning Surgical Endodontics Implants Post Removal Toothwear Crown and Bridge failure RCT Caries Dental Aesthetics/Appearance Pain Missing teeth (Fixed Prosthodontics) Missing teeth (Removable Prosthodontics) Routine Care (undergraduate clinic) Other Please specify………………………….
5.Give an account of the problem and its history:
6.Detail any relevant medical history and list all current medications:
7. List all special investigations carried out in connection with the referral Radiographs Yes No Study Casts Yes No
(send in if relevant –these must be provided for crown and br idge referrals )
View | Date | Dietary HistoryYes No I Detail main findings below: | ____________________________________ | | ____________________________________
(These must be provided for endodontic referrals. ____________________________________ Where provided these should be attached to the referral)
Relevant Clinical Photographs Yes No (These should be attached to the referral) Describe what these show: _____________________________________________________ ______________________________________________________________________________
8.Social History (where relevant to referral) a) Does the patient smoke? Yes No
If yes – how many cigarettes per day? ______________ for how many years? ______________
b) Does the patient drink alcohol? Yes No If yes – how many units are consumed weekly?______________
9.In your view is this referral for (tick most appropr iate) Specialist opinion/advice Justify if treatment requested___________ Specialist treatment _____________________________________ Undergraduate patient clinic
10. If this referral is to a preferred Consultant Clinic indicate his/her name below: ______________________________________________________________________________
It was further proposed that guidelines for referral to the service should be introduced (appendix 2). The following supporting information was provided:
• The role of the restorative dentistry service is to provide a diagnostic, treatment planning and advice service to referring practitioners.
• A small number of patients may be accepted for treatment by consultants, specialists or specialist trainees if specialist treatment is required.
• Other patients may be suitable for training of undergraduates, postgraduates and staff in training.
• Patients accepted for specialist treatment are expected to continue to see their GDP for routine dental examinations and treatment.
• All patients will be referred back to the referring practitioner on completion of treatment.
• The intention of the consultants in restorative dentistry is to work in partnership with the referring clinician.
• All referrals are triaged by senior clinical staff according to the urgency and nature of the case as described in the letter from the referring dentist or doctor.
Endodontics
• All endodontic referrals must include dated and relevant, good diagnostic quality radiograph(s).
• The tooth or teeth in question should be potentially restorable and functional. • Patients referred for endodontics should have good oral hygiene, no active caries or
active periodontal disease and no other teeth requiring restoration.
Periodontics
• All periodontal referrals must include a BPE score or other detailed periodontal charting. Recent radiographs showing alveolar bone levels should be included.
• Before referral, patients should be made aware of the reduced response to periodontal therapy in smokers.
• Patients who simply have chronic gingivitis will not normally be accepted for treatment. • When appropriate, pre and posttreatment charts can be sent to the GDP for
information to inform future monitoring and maintenance of the patient. • Patients who do not maintain good levels of oral hygiene will be returned to the referring
GDP for palliative periodontal care.
Fixed Prosthodontics
• A full diagnostic and advisory service is available. Dated study models should be given to the patient to bring to the consultation appointment.
• Patients requiring multiple units involving changes to the dynamic occlusion may be accepted for treatment at the discretion of the consultant.
• Patients referred for fixed prosthodontics should have good oral hygiene, no active caries or active periodontal disease and no other teeth requiring restoration.
Toothwear
• A full diagnostic and advisory service is available. Toothwear referrals should include evidence of dietary history where appropriate. Dated study models should be given to the patient to bring to the consultation appointment.
• Patients requiring prolonged and/or complex care may be accepted for treatment, at the discretion of the consultant.
• Patients referred for management of toothwear should have good oral hygiene, no active caries or active periodontal disease and no other teeth requiring restoration.
4.3 Fixed Implant Approaches Dr Brendan J Scott, Consultant in Restorative Dentistry
Dr Scott addressed those present on the subject of his specialist interest, Implantology. Demand for implants is growing across Scotland, not just in Tayside. Dr Scott offered the following by way of background information:
Provision of Services:
• Usually carried out in multidisciplinary teams • Oral Surgery / Restorative Dentistry / Laboratories • May also involve orthodontists • Historically 2 parallel teams have provided implants with some crossover between
members • Balance between service commitment and training e.g. SpRs • Undergraduate students observe at diagnostic and treatment clinics
Removable Implant Approaches:
• Edentulous patients who have major problems in wearing prostheses
• Usually because of compromised anatomy e.g. atrophic mandibular ridge
• Tolerance problems – e.g. maxillary denture
Fixed Implant Approaches:
• Edentulous patients in certain circumstances – malignancy, trauma
• Dentate patients with tooth loss in certain circumstances
• Has to be a good rationale as many restorative specialists would say that other options can give an equally good result e.g. adhesive bridgework
• Dentate patients in certain circumstances – long saddles
Facilities available in Dundee Dental Hospital include, scanning, the production of stents, Cone Beam Imaging and 3 dimensional assessment.
Dr Scott introduced a proposal for referral criteria for Implantology, to be used by all referring clinicians in Tayside. He stated that the criteria were sourced from other institutions and Consultants in Dental Public Health.
Implant Referral Criteria
• It is recognised that the potential demand for this modality of treatment is increasing, through a greater awareness of both health care professionals and patients themselves.
• However it should be recognised that there are a wide range of options available to patients for replacing missing teeth and the supporting tissues, of which the dental implant modality is but one.
• Furthermore, for many patients, more conventional forms of treatment will often provide an equally acceptable treatment outcome.
• It would simply not be possible to provide dental implants to replace missing teeth for every patient purely because they want a fixed solution as opposed to one involving a removable prosthesis
• Patients with congenital or inherited disorders such as hypodontia, cleft palate and amelogenesis or dentinogenesis imperfecta.

• Patients who have sustained tooth, alveolar bone or soft tissue loss through ablative surgery from head and neck malignancy or pathological lesions resulting in altered oral anatomy.
• Patients who have sustained usually accidental trauma resulting in the loss of teeth (subject to the constraints above and dependent on the circumstances that the tooth/teeth were lost).
• Patients who have a severe intolerance to wearing removable prostheses. This could be due to either severe alveolar ridge resorption (usually the mandibular arch) or a severe gag reflex (usually the maxillary arch)
• Patients with an edentulous ridge opposed by teeth with a good prognosis, where there is a likelihood of further alveolar resorption occurring (especially where maxillary teeth remain)
“When will we not usually provide implants and in particular a fixed solution?”
• Large area of tissue loss • Multiple saddles • Periodontal disease • Uncertain prognosis of remaining dentition
With regard to followup, hygiene and maintenance, Dr Scott proposed that this could be done in the primary care dental setting by the GDP or DCP, as appropriate. However, he identified that, as a result of the wide range of implant solutions available, components used in the hospital setting might not be available except where the GDP used that particular implant system. In the event of complications arising, e.g. screw loosening, the same difficulties would be likely to arise. The solution, he thought, was to ensure a ready supply of suitably trained and experienced clinicians.
Future challenges:
• Implant holidays – Patients having dental treatment abroad who seek followup repair or remedial assistance back in the U.K.
• Medico legal difficulties • The number of implant systems in use worldwide (Estimated total number of
manufacturers = 138, total number of implants = 464) • Resources • The increasing price of gold • Economic climate • Local priorities in HS Tayside
4.4 NHS Tayside Dental Laboratory Services Mr David Hoban, Senior Dental Laboratory Technician
The NHS Tayside Dental Laboratories provide technical services for Orthodontics, Paediatrics, Oral Medicine and Oral surgery as well as restorative services including Prosthetics, Periodontal, Conservation and Integrated Oral Care. There are 3 specialist laboratories based in Dundee Dental Hospital and School, covering Orthodontics, Prosthetics and Conservation with a

technician based in Perth Royal Infirmary providing orthodontic technical services including orthognathic planning for surgical patients.
Maxillofacial services are covered by two technicians one based in Perth Royal Infirmary and one in Ninewells hospital. The maxillofacial service is managed separately from the dental services.
Restorative Department
(includes Prosthetics, Periodontal, Conservation and Integrated Oral Care)
NHS Consultants 3 Hon Consultants / Professors 11 Clinical Lecturers 10 Total Clinical Sessions per month not known SPRs 1 Staff Grade/ Specialty Dentist 3
Orthodontic Department
NHS Consultants 2 Hon Consultants / professors 2 Clinical Lecturers 2 SPRs 6 Total Clinic Sessions per month not known
Assoc Specialist 1 Staff Grade Spec Dentist 1 FTTA 1
Paediatric Department
NHS Consultants 1 Hon Consultants / professors 2 Total Clinic sessions per month not known Clinical Lecturers 2 Staff Grade Spec Dentist 1
Oral Medicine, Oral Surgery, Radiology, Dental A&E
NHS Consultants 5 Hon Consultants / Professors 1 Clinical Lecturers 1 SPRs 1 Total Clinical Sessions per month not known Assoc Specialist 1 Staff Grade Spec Dentist 1
GDPs all P/T 26 SHO /DF1/DF2 12 all departments
Clinics also staffed by Undergraduate students 3 rd to 5 th year.

The laboratories are staffed 1 as follows: Dundee Dental Hospital:
Orthodontic Laboratory Dental Laboratory Services Manager 1 Advanced Dental Technicians 2 Dental Technician 1 Total 4
Conservation Laboratory
Dental Laboratory Manager 1 Advanced Dental Technicians 4 Total 5
Prosthetic Laboratory
Dental Laboratory Manager 1 Advanced Dental Technicians 9 Specialist Dental Technicians 2 Dental Technicians 2 Vacancy 1 Total 15
Perth Royal Infirmary:
Advanced Dental Technician 1 Total 1
Dental Laboratory Staff Total 25
The laboratories in Dundee and Drumhar Health Centre, Perth, are currently training 5 dental technician students funded by NES. The course is a pilot scheme and 5 of our advanced dental technicians are dedicated mentors to the students, this is in addition to their day to day duties.
Services Provided by the laboratories
Prosthetics
• Full and Partial Dentures • Chrome Cobalt Dentures • Implant retained dentures • Bite rehabilitation appliances • Obturators • Duplicate Dentures • Various types of stents • Research as required
Crown and Bridge
• Gold post and core crowns • Gold shell crowns • Porcelain Fused to Metal (PFM) • Crowns • Implant retained crowns • Resin retained bridges • Veneers • Diagnostic Wax ups • Surgical stents
1 All Laboratory Staff are full time employees.
• Pressable Ceramics • Zirconia crowns and bridges CAD CAM • Bite rehabilitation appliances • Research as required
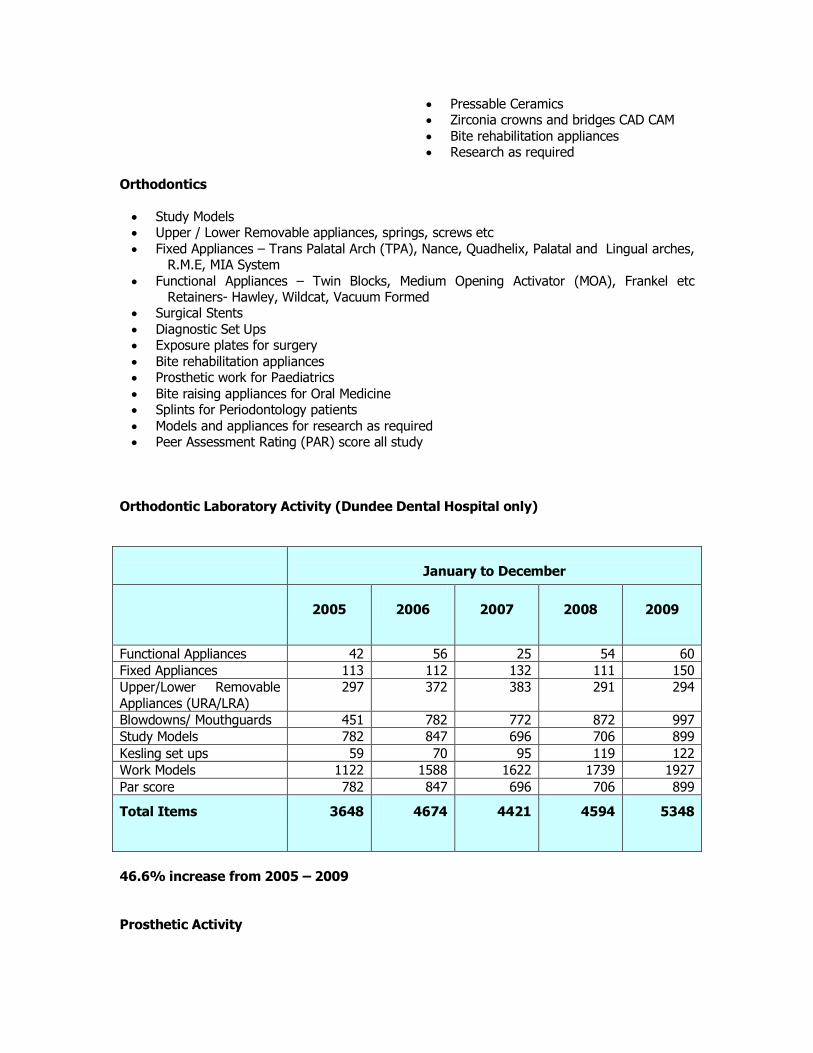
Orthodontics
• Study Models • Upper / Lower Removable appliances, springs, screws etc • Fixed Appliances – Trans Palatal Arch (TPA), Nance, Quadhelix, Palatal and Lingual arches,
R.M.E, MIA System • Functional Appliances – Twin Blocks, Medium Opening Activator (MOA), Frankel etc
Retainers Hawley, Wildcat, Vacuum Formed • Surgical Stents • Diagnostic Set Ups • Exposure plates for surgery • Bite rehabilitation appliances • Prosthetic work for Paediatrics • Bite raising appliances for Oral Medicine • Splints for Periodontology patients • Models and appliances for research as required • Peer Assessment Rating (PAR) score all study
Orthodontic Laboratory Activity (Dundee Dental Hospital only)
January to December
2005 2006 2007 2008 2009
Functional Appliances 42 56 25 54 60 Fixed Appliances 113 112 132 111 150 Upper/Lower Removable Appliances (URA/LRA)
297 372 383 291 294
Blowdowns/ Mouthguards 451 782 772 872 997 Study Models 782 847 696 706 899 Kesling set ups 59 70 95 119 122 Work Models 1122 1588 1622 1739 1927 Par score 782 847 696 706 899
Total Items 3648 4674 4421 4594 5348
46.6% increase from 2005 – 2009
Prosthetic Activity

January to December
2005 2006 2007 2008 2009
6912 7178 7608 7875 7875
14% increase from 20052009
Conservation Figures
April to March
2004/2005 2005/2006 2006/2007 2007/2008 2008/2009 2009/ 2010
6075 5706 7028 7804 5832 6718
10.5% increase
Medical Health Regulatory Authority (MHRA) (Previously known as the Medical Devices Agency (MDA)
The dental laboratories in NHS Tayside were removed from the register in 2002 as they do not supply or fit dental appliances or prosthesis other than to their own patients.
OnetoOne discussions
Invitations to participate in 1:1 semistructured interviews were sent to all Restorative Dentistry Consultants in NHS Tayside (12). Six of the Consultants (50%) accepted the invitation. The findings are summarised as follows:
General
Issues with funding in the primary care service were identified as a major barrier to progress. The view was expressed by some respondents that some dentists refer patients to the hospital dentistry service (a) because the procedure takes multiple visits and multiple appointment slots to complete and (b) the fee structure in primary care renders treatment by dentists financially nonviable.
Service Issues
All of the respondents interviewed identified pressures on the service to achieve the 18 week Referral to Treatment Standard. Some respondents commented on the inappropriateness of the Standard in relation to Restorative Dentistry (and Orthodontics), stating that the standard might be achieved for a first new outpatient appointment. However, it was thought that the complex and longitudinal nature of treatment for many Restorative Dentistry patients slowed the rate at
which patients could be removed from the treatment waiting list thus setting the service up to fail.
Endodontics and Periodontics were cited as being the two monospecialties where demand was greatest. Some respondents felt that Dentists should be doing more root canal work in primary care rather than referring to the specialist hospital service. Others thought that Periodontics was as waste of tax payers money on the basis that behaviours related to poor oral hygiene spanning many years would not change as a result of specialist intervention.
Many of the respondents thought that there was a role for Dentists with Special Interest in the monospecialties of Restorative Dentistry, which was not being met.
Dental Care Professionals (DCP’s)
The majority of respondents considered that there were opportunities to be explored for developing the role of Dental Care Professionals (DCP’s) (Dental Therapists, Technicians, Nurses etc). Most thought that these opportunities existed predominantly in primary care and were not sure where enhanced skills roles would fit in a hospital dental service where treatment needs are complex. It was noted, however, that Dental Therapists do currently manage Periodontal patients in DDH.
Data
Most of the Consultants interviewed reported that they do receive data relating to waiting times though some said that this had only recently become available. There was a view amongst some respondents that recording outcome codes following assessment of the patient in clinic was bureaucratic and not supported by any additional resource. Others noted that the profile of Restorative Dentistry was not clear and saw outcome coding as a useful tool to providing that clarity. A number of respondents referred to difficulties with IT systems which they considered were unfit for purpose given the focus on improved data quality and data collection.
Training and Education
All of the Honorary Consultants interviewed spoke of the need to ensure that a broad range of referrals are received by the hospital dental services to support the training and education of undergraduate students. Some identified this group of students as the future cohort of dentists in primary care and that the training they receive is fundamental to the service they will provide in future years. They considered it essential therefore that opportunities for treating “bread and butter” cases should continue.
The issue about the fee structure in primary care was again expressed, this time as a reason for difficulties in retaining SpR’s to the NHS once they have gained their CCST.
(f) The Future
Thoughts for the future of Restorative Dentistry for the North of Scotland were mixed. There was strong support for a plan to provide clarity around what should and should not be treated in a hospital based Restorative Dentistry service – what should be included in the core service? Also, stakeholders largely agreed on the need for robust referral criteria and protocols standardised across the North, supported by an agreed referral template containing core data sets. All of the respondents considered training and education to be the key factor to determining how Restorative Dentistry services could be designed in the future.

Helen M Strachan Regional Manager North of Scotland Oral Health and Dentistry Final at 15.10.10

Appendix 1


Appendix 2