Embed Size (px)
Citation preview
P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42Food Allergens
J. I. Boye, A. O. Danquah, Cin Lam Thang, and X. Zhao
IntroductionFood Hypersensitivity
Food AllergyImmediate Hypersensitivity ReactionsDelayed Hypersensitivity Reactions
Food IntoleranceMetabolic Food DisordersAnaphylactoid Responses
Milk AllergensMilk ProteinMajor Milk Allergens
Caseinsβ-Lactoglobulinα-LactalbuminBovine Serum AlbuminLactoferrin
Milk Allergen Cross-ReactivitiesThreshold DoseEffect of Processing on the Allergenicity of Cow’s Milk
ProteinsHeat treatmentHydrolysisRadiationHigh-Pressure Treatment
Egg AllergensPrevalence, Symptoms and ThresholdsMajor Egg AllergensThresholds of Clinical Reactivity to Eggs
Soya bean AllergensMajor Soya AllergensPrevalence, Symptoms and ThresholdEffect of Processing on Soya AllergensSoya Allergen Cross-Reactivities
Peanut and Tree Nut AllergensPrevalence and ThresholdMajor Peanut and Tree Nut AllergensProcessing-Induced Changes in Peanut and Tree Nut
Allergenic Proteins
Fish and Shellfish AllergensAllergens in Cereals
Celiac DiseaseIgE-Mediated Cereal AllergyFoods to Avoid for Gluten-Sensitive Enteropathy
Patients and IgE-Mediated Cereal-Allergic PatientsSesame and Mustard Allergens
Sesame AllergyMustard Seed Allergy
Minor Food AllergensManagement of Food AllergyMethods for Detecting Allergens
ELISA-Based Detection MethodsSandwich ELISACompetitive ELISALFA and Dipstick Tests
Proteomic ApproachDNA-Based Allergen Detection Methods
Polymerase Chain Reaction (PCR) withGel Electrophoresis
PCR with ELISAReal-Time PCR
ConclusionAcknowledgementReferences
Abstract: The management of allergens along the food value chainand the diagnosis of food allergic diseases continue to pose seriouschallenges to the food industry as well as health care professionals.Of the over 170 foods known to provoke allergic reactions, ninefoods (and their derived products) are today considered to be majorallergens accounting for over 90% of all food allergic reactions.These priority allergens include milk, eggs, soya beans, peanuts,tree nuts (e.g. almonds, walnuts, pecans, cashews, Brazil nuts, hazelnuts, pistachios, pine nuts, macadamia nuts, chestnuts and hick-ory nuts), seafood such as fish (i.e. both saltwater and freshwater
Food Biochemistry and Food Processing, Second Edition. Edited by Benjamin K. Simpson, Leo M.L. Nollet, Fidel Toldra, Soottawat Benjakul, Gopinadhan Paliyath and Y.H. Hui.C© 2012 John Wiley & Sons, Inc. Published 2012 by John Wiley & Sons, Inc.
798

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 799
finfish), crustaceans (e.g. shrimp, prawns, crab, lobster and crayfish)and molluscs (e.g. snails, oysters, clams, squid, octopus and cuttle-fish), gluten-containing cereals (i.e. wheat, rye, barley and theirhybridised strains and products), sesame and mustard. Symptomsof food allergic reactions and the threshold dose required to pro-voke allergic reaction markedly vary among sensitised individuals.Food production practices, processing conditions and matrix effectscan also modify the molecular structure of food allergens and theirpotential immunogenic properties which can make allergens diffi-cult to detect even when present in foods. This chapter provides anoverview of the different types of food hypersensitivities includ-ing a distinction between food allergies and food intolerance, theproperties of the nine priority food allergens, current approaches forthe management of food allergens and a summary of some of thecurrent methods used in food allergen detection.
INTRODUCTIONHumans require food to survive. In addition to basic nutri-tion, food consumption provides a sense of satisfaction andculinary pleasure and also serves as a source of social enter-tainment. However, for a small percentage of the population,consumption of certain foods even in small quantities can re-sult in life-threatening allergic reactions. Approximately 4–8%of young children and 2–4% of adults in developed countriessuffer from food allergies (Kanny et al. 2001, Munoz-Furlonget al. 2004, Sampson 2004, Sicherer et al. 2004, Breitenederand Mills 2005). Although over 170 foods are known to causefood allergies, nine foods (and their derived products) are to-day considered to be major allergens accounting for over 90%of all food allergic reactions. These priority allergens includemilk, eggs, soya beans, peanuts, tree nuts (e.g. almonds, wal-nuts, pecans, cashews, Brazil nuts, hazel nuts, pistachios, pinenuts, macadamia nuts, chestnuts and hickory nuts), seafood suchas fish (i.e. both saltwater and freshwater finfish), crustacea (e.g.shrimp, prawns, crab, lobster and crayfish) and molluscs (e.g.snails, oysters, clams, squid, octopus and cuttlefish), gluten-containing cereals (i.e. wheat, rye, barley and their hybridisedstrains and products), sesame and mustard.
Food allergy is thus emerging as a growing public health prob-lem. Unfortunately, the management of food allergens along thefood value chain and the diagnosis of food allergic diseases con-tinue to pose a challenge to the food industry as well as healthcare professionals. The factors responsible for this are varied.Multiple foods can induce food allergic reactions, and the thresh-old dose required to provoke allergic reaction markedly variesfor different patients; thus, small quantities of foods can cause se-vere reactions in sensitised individuals, whereas other sensitisedindividuals can tolerate quantities of the allergen that are ordersof magnitude higher. Additionally, symptoms of food allergiesvary tremendously among sensitised individuals, and food pro-duction practices, processing conditions and matrix effects canalter the molecular structure of food allergens and their potentialimmunogenic properties and detection. In this chapter, we willprovide an overview of the different types of food hypersensi-tivities, including a distinction between food allergies and food
intolerance, the properties of the nine priority food allergens,current approaches for the management of food allergens and asummary of some of the current methods used for food allergendetection.
FOOD HYPERSENSITIVITYFood Allergy
Food allergy is an immunological reaction resulting from theingestion, inhalation or atopic contact of food. Immunologicalreactions can be mediated by IgE antibodies or other immunecells such as T cells. Some workers define food allergy specifi-cally as being those immunological responses mediated by im-munoglobulin E (IgE) antibodies, whereas others use the broaderdefinition of immunological response, which include T-cell me-diated responses as well. In this chapter, the latter definition willbe used.
In general, any protein-containing food can elicit an aller-gic response in sensitised individuals. Allergenic proteins infoods may be enzymes, enzyme inhibitors, structural proteinsor binding proteins with varied biological functions (Stewartand Thompson 1996, Valenta et al. 1999, Chapman et al. 2000,Martin and Chapman 2001). The pathogenesis of food allergybegins with a sensitisation phase during which time the bodyrecognises one or more proteins in a particular food source asa foreign invader and begins to mount an immune-defensive re-sponse. Subsequent consumption of the offending food can resultin an allergic response that may manifest in one of two forms,that is, immediate or delayed response as described below.
Immediate Hypersensitivity Reactions
Immediate hypersensitivity reactions are mediated by a specificclass of antibodies known as IgE. Symptoms of an IgE-mediatedfood allergy develop within a few minutes to a few hours afteran individual has ingested the offending food (Taylor 2000).During the sensitisation phase, the body produces IgE antibod-ies, which recognise allergenic fragments from the offendingfood. After production, IgE antibodies circulate in the bloodand bind to basophiles and to the surface of mast cells (Taylor2000). Mast cells and basophiles contain granules packed withpotent inflammatory mediators such as histamine, cytokines andother chemotactic factors. When an allergic person encountersan allergen to which the person has previously produced IgEantibodies, the allergen combines with the IgE antibody on thesurface of the mast cells and basophiles. This triggers a com-plex series of reactions that result in the release of histamineand other chemical mediators (prostaglandin D2, tryptase, hep-arin, etc.) from the granules inside the mast cells and basophiles(Taylor and Lehrer 1996, Lu et al. 2007). Histamine as well asthe other chemical mediators has been shown to be the agentsresponsible for producing symptoms of allergy. The release ofsome of these mediators occurs rapidly, within 5 minutes afterthe interaction between the allergen and the IgE antibody (Taylor2000). Once released, these compounds enter the blood stream

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
800 Part 8: Food Safety and Food Allegens
and bind to ‘receptors’ on other cells in the body, causing typicalallergic symptoms.
The severity of an allergic reaction depends on how sensitisedthe person is and the amount of the allergenic component in-gested. Histamine released from mast cells is usually completewithin 30 minutes after the allergen–IgE antibody interaction.The release of mediators (other than histamine) is slower andtheir effects are more prolonged. Allergic reactions may, thus,sometimes occur in two phases. The first stage or first symptomsdisappear on their own or with medication only to recur in 4–6hours. Reactions may range from mild to severe life-threateningconditions, and may manifest as gastrointestinal disorders (nau-sea, vomiting, diarrhoea and abdominal cramping), or involvethe skin, leading to urticaria or hives, dermatitis, eczema, an-gioderma, pruritis or itching. It may also involve the respiratorytract, in which case the individual may suffer from rhinitis,asthma or laryngeal oedema. Systemic anaphylaxis representsthe most dramatic and potentially catastrophic manifestation ofimmediate hypersensitivity. Virtually, every organ in the bodycan be affected, although reactions involving the pulmonary, cir-culatory, cutaneous, neurological and gastrointestinal tract arethe most common (Anderson 1986).
About 1–2% of the total population are affected by IgE-mediated food allergies (Chafen et al. 2010). The most vul-nerable group are infants and young children, with 5–8% infantsunder 3 years being affected (Sampson and McCaskill 1985,Motala and Lockey 2004, Sicherer 2010). More than 170 dif-ferent foods have been implicated in immediate hypersensitivityreactions (Hefle et al. 1996, Taylor 2000).
Delayed Hypersensitivity Reactions
Unlike the immediate hypersensitivity reactions describedabove, symptoms associated with delayed hypersensitivity in-duced by T-cells may appear after several hours to even daysfollowing consumption of the offending food. Delayed allergicreactions to food are relatively more difficult to identify un-less the suspected food is eliminated from the diet for at leastseveral weeks and then slowly reintroduced followed by moni-toring for the onset of any physical, emotional or mental changes(Anderson 1986). These reactions are mediated by tissue-boundimmune cells, and the acuteness of the reaction may be less thanthat of the immediate reactions (Taylor 2000). An example ofdelayed hypersensitivity reaction to food is celiac disease (CD),which is described in greater detail below.
Food Intolerance
Food intolerances are abnormal reactions to food or food compo-nents that do not involve the immune system (Breneman 1987).They are generally less severe, shorter in duration and morelocalised than immunological reactions. Food intolerances arethe most common types of food sensitivities and specific ex-amples include the metabolic food disorders and anaphylactoidresponses described below.
Metabolic Food Disorders
Metabolic food disorders arise from inherited genetic deficien-cies that reduce the capacity of afflicted individuals to efficientlymetabolise food components. One such example is lactose in-tolerance, which is caused by an inherited deficiency of thedigestive enzyme lactase, which hydrolyses lactose in milk andmilk products into galactose and glucose for further process-ing within the body. As a result, the undigested lactose cannotbe absorbed by the small intestine and passes into the colonwhere bacteria metabolise it into carbon dioxide (CO2) and wa-ter (H2O), leading to bloating, abdominal cramping and frothydiarrhoea (Taylor 2000).
Another example is phenylketonuria, a metabolic disorder inwhich afflicted individuals are deficient in the hepatic enzymephenylalanine hydroxylase, which metabolises phenylalanineinto tyrosine. Thus, phenylalanine and phenylpyruvate accumu-late in the body, and if left untreated, it could affect the centralnervous system and cause mental retardation and/or brain dam-age in infants and children.
A third example of food intolerance due to a genetic defi-ciency is favism, where individuals are intolerant to fava beansor the pollen from the Vicia faba plant. Persons with this intoler-ance have an inherited deficiency of the erythrocyte glucose-6-phosphate dehydrogenase (G6PDH) enzyme, which is essen-tial to protect erythrocyte membranes against oxidative damage(Taylor 2000). This deficiency is crucial as several endoge-nous oxidants present in broad beans, for example, vicine andconvicine, are capable of damaging erythrocyte membranesin G6PDH-deficient individuals, resulting in acute haemolyticanaemia with pallor, fatigue, dyspnoea, nausea, abdominal and/or back pain, fever and chills. It may even lead to more serioussymptoms such as haemoglobinuria, jaundice and renal failure,but these situations are rare. Symptoms occur quite rapidly, usu-ally within 5–24 hours following consumption of fava beans.
Anaphylactoid Responses
Anaphylactoid responses are due to the non-immunologic re-lease of chemical mediators, such as histamine, from mast cells(Sampson et al. 1992). The specific substances that cause thisreaction are not well known, and the reactions are often confusedwith true food allergies because they display similar symptoms.Anaphylactic shock is one of the most startling symptoms asso-ciated with food allergies, and such food intolerances, and mayaffect the gastrointestinal tract, skin, respiratory tract and thecardiovascular system. It can cause severe hypotension, and ifnot treated properly, it may lead to death within minutes afteringesting the offending food (Taylor 2000).
The rest of this chapter will focus on describing some of theproperties of the nine most common food allergens and methodsfor detecting allergens.
MILK ALLERGENSMilk is a nutritional biological fluid secreted from the mammarygland of female mammalians, and it is primarily intended to
P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 801
provide nutritional requirements of neonates. Human milk andthe milks of dairy animals, such as cows, goats, sheep and buf-faloes, have been extensively studied. Humans are the onlyknown mammals that consume the milk of other mammals,particularly from cows. In fact, cow’s milk and cow’s milk-associated food have been deeply rooted as an important partof the human diet, and the dairy industry plays a huge role insupporting nutrition of humans and continues to be a backboneof the agri-food sector in many countries.
In developed countries, bovine milk and milk-derived prod-ucts contribute about 19% of total dietary protein intake and 73%of calcium intake (Tome et al. 2004). However, for some people,consumption of cow’s milk and cow’s milk-derived food has tobe avoided due to milk allergy. Recent studies have indicatedthat prevalence and persistence of cow’s milk allergy (CMA) inindustrialised countries may be increasing. In North America,incidence of CMA is estimated at 2.5% in children and about1% in the adult population with a 75% outgrowing rate at theage of 16 (Sicherer and Sampson 2010).
Milk Protein
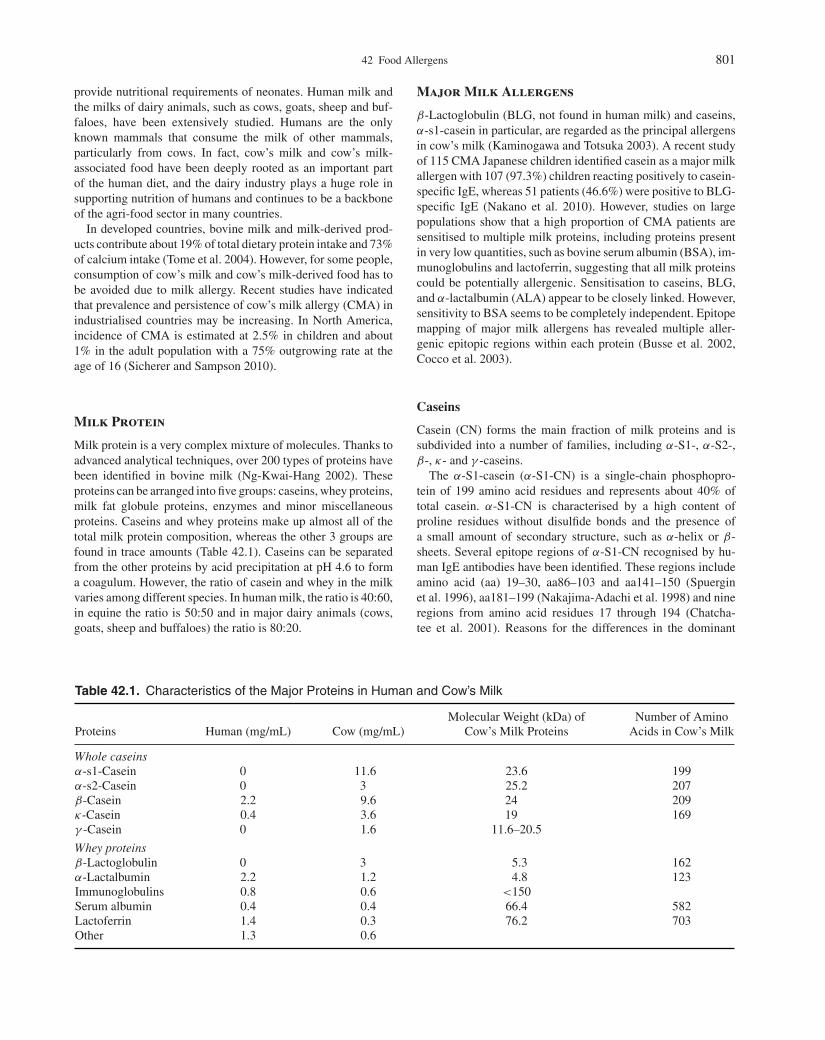
Milk protein is a very complex mixture of molecules. Thanks toadvanced analytical techniques, over 200 types of proteins havebeen identified in bovine milk (Ng-Kwai-Hang 2002). Theseproteins can be arranged into five groups: caseins, whey proteins,milk fat globule proteins, enzymes and minor miscellaneousproteins. Caseins and whey proteins make up almost all of thetotal milk protein composition, whereas the other 3 groups arefound in trace amounts (Table 42.1). Caseins can be separatedfrom the other proteins by acid precipitation at pH 4.6 to forma coagulum. However, the ratio of casein and whey in the milkvaries among different species. In human milk, the ratio is 40:60,in equine the ratio is 50:50 and in major dairy animals (cows,goats, sheep and buffaloes) the ratio is 80:20.
Major Milk Allergens
β-Lactoglobulin (BLG, not found in human milk) and caseins,α-s1-casein in particular, are regarded as the principal allergensin cow’s milk (Kaminogawa and Totsuka 2003). A recent studyof 115 CMA Japanese children identified casein as a major milkallergen with 107 (97.3%) children reacting positively to casein-specific IgE, whereas 51 patients (46.6%) were positive to BLG-specific IgE (Nakano et al. 2010). However, studies on largepopulations show that a high proportion of CMA patients aresensitised to multiple milk proteins, including proteins presentin very low quantities, such as bovine serum albumin (BSA), im-munoglobulins and lactoferrin, suggesting that all milk proteinscould be potentially allergenic. Sensitisation to caseins, BLG,and α-lactalbumin (ALA) appear to be closely linked. However,sensitivity to BSA seems to be completely independent. Epitopemapping of major milk allergens has revealed multiple aller-genic epitopic regions within each protein (Busse et al. 2002,Cocco et al. 2003).
Caseins
Casein (CN) forms the main fraction of milk proteins and issubdivided into a number of families, including α-S1-, α-S2-,β-, κ- and γ -caseins.
The α-S1-casein (α-S1-CN) is a single-chain phosphopro-tein of 199 amino acid residues and represents about 40% oftotal casein. α-S1-CN is characterised by a high content ofproline residues without disulfide bonds and the presence ofa small amount of secondary structure, such as α-helix or β-sheets. Several epitope regions of α-S1-CN recognised by hu-man IgE antibodies have been identified. These regions includeamino acid (aa) 19–30, aa86–103 and aa141–150 (Spuerginet al. 1996), aa181–199 (Nakajima-Adachi et al. 1998) and nineregions from amino acid residues 17 through 194 (Chatcha-tee et al. 2001). Reasons for the differences in the dominant
Table 42.1. Characteristics of the Major Proteins in Human and Cow’s Milk
Proteins Human (mg/mL) Cow (mg/mL)Molecular Weight (kDa) of
Cow’s Milk ProteinsNumber of Amino
Acids in Cow’s Milk
Whole caseinsα-s1-Casein 0 11.6 23.6 199α-s2-Casein 0 3 25.2 207β-Casein 2.2 9.6 24 209κ-Casein 0.4 3.6 19 169γ -Casein 0 1.6 11.6–20.5
Whey proteinsβ-Lactoglobulin 0 3 5.3 162α-Lactalbumin 2.2 1.2 4.8 123Immunoglobulins 0.8 0.6 <150Serum albumin 0.4 0.4 66.4 582Lactoferrin 1.4 0.3 76.2 703Other 1.3 0.6

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
802 Part 8: Food Safety and Food Allegens
epitopic regions reported by different researchers may be dueto racial (Kaminogawa and Totsuka 2003), dietary, breed andenvironmental differences.
The α-s2-casein is comprised of 207 amino acids and has onedisulfide bond (Wal 1998). The α-S2-CN family accounts for12.5% of the casein fraction and is the most hydrophilic amongall caseins due to the presence of clusters of anionic groups. TenIgE-binding regions have been identified between amino acidpositions 31–200 of α-s2-casein (Busse et al. 2002).
β-Casein (β-CN) represents 35% of the total caseins and isquite complex because of the action of native milk protease plas-min. Plasmin cleaves β-CN and thereby generates γ 1-, γ 2-, andγ 3-CN fragments. β-CN is the most hydrophobic componentamong casein fractions. Six major and three minor IgE-bindingepitopes, as well as eight major and one minor IgG-bindingregions, have been identified on β-CN (Chatchatee et al. 2001).
κ-CN accounts for 12.5% of the total casein fraction. Eightmajor IgE-binding epitopes, as well as two major and two minorIgG-binding epitopes, have been detected in κ-casein (Chatcha-tee et al. 2001).
β-Lactoglobulin
Bovine BLG is the most abundant whey protein and represent50% of total whey proteins. It has no homologous counterpartin human milk. It possesses three disulfide bridges. BLG is rela-tively resistant to proteases and acid hydrolysis. BLG belongs tothe lipocalin superfamily and is capable of binding a wide rangeof molecules, including retinol, β-carotene, saturated and unsat-urated fatty acids and aliphatic hydrocarbons (Breiteneder andMills 2005). BLG epitopes reported as markers for persistentCMA include aa1–16, aa31–48, aa47–60, aa67–78 and aa75–86(Jarvinen et al. 2001, Inoue et al. 2001).
α-Lactalbumin
Bovine ALA is characterised by four disulfide bridges and pos-sesses a high-affinity binding site for calcium, which stabilisesits secondary structure.
Bovine ALA shows a 72% amino acid sequence homologyto human ALA and is, thus, an ideal protein for the nutritionof human infants. Four different linear IgE-binding peptides,aa1–16, aa3–26, aa47–58 and aa93–102, have been identifiedby epitope mapping in children who outgrow CMA later in life(Jarvinen et al. 2001).
Bovine Serum Albumin
BSA accounts for about 5% of total whey proteins and is phys-ically and immunologically very similar to human blood serumalbumin. BSA has 17 disulfide bonds and most of the disulfidebonds are protected in the core of the protein and are there-fore not easily accessible (Restani et al. 2004). This may be thereason for its relatively stable tertiary structure. IgE-binding epi-topes identified for BSA have been inconsistent among studies(Karjalainen et al. 1992).
Lactoferrin
Lactoferrin (LF) is a milk-specific iron-binding protein. Al-though LF in cow’s milk is homologous to human LF, the contentis lower than that of human’s milk. Its main function is to defendthe host against infections and inflammations due to its abilityto sequester iron from the environment, thereby removing thisessential nutrient for bacterial growth (Ward et al. 2002). De-spite its low concentration in bovine milk, LF-specific IgE havebeen detected in 45% of CMA patients (Wal 1998).
Milk Allergen Cross-Reactivities
Different species of milk-producing ruminants have the sameor closely related milk proteins with relatively similar ratios ofcasein and whey (Monaci et al. 2006). Furthermore, considerablyhigh amino acid sequence homology (varying from 87–96%)exists among major milk proteins of cow, goat and ewe (Table42.2). As a result, IgE cross-reactivity among the milk of goat,ewe and cow has been reported for most CMA patients. IgEsensitisation to sheep and goat casein has been found to be ashigh as 93–98% in children with IgE-mediated CMA (Besleret al. 2002a). In general, the milk of other ruminants is not agood alternative for CMA patients.
Cross-reactivity between cow’s milk allergens and soya beanproteins has also been reported. Allergic reactions to soya beanwas observed in about 17–47% of children with CMA (Hillet al. 1999). Cross-reactivity between soya bean and casein wasconfirmed by Rozenfeld et al. (2002), who showed that glycinin-like protein (two polypeptides, A5-B3) from soya bean were ableto bind casein-specific monoclonal antibodies.
Threshold Dose
There is limited data on the threshold dose required to provoke amilk allergy reaction. Several research groups using double blindplacebo controlled food challenges with milk protein have useddoses varying from 0.6 to 180 mg to induce allergic reactions inCMA patients (Monaci et al. 2006). However, these studies wereprimarily intended for diagnostic purpose and not necessarily fordetermining the lowest provoking dose. Severe adverse reactions
Table 42.2. Comparisons of the Amino Acid SequenceHomology of the Major Proteins Found in Cow’s Milkand That of Goat and Ewe
Sequence Homology (%)
Milk Proteins Cow vs Goat Cow vs Ewe
β-Lactoglobulin 96 96α-Lactalbumin 95 94α-s1-Casein 87 89α-s2-Casein 88 89β-Casein 90 90κ-Casein 85 84
Source: Adapted from Wal 2004.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 803
have been reported after eating food contaminated with traceamounts of milk protein, including breast milk from motherswho consume cow’s milk (Gerrard and Shenassa 1983), meattreated with casein to enhance texture (Yman et al. 1994), frozendesserts that contain trace amounts of whey protein (Laoprasertet al. 1998) and lactose-containing medications that containedresidual milk protein (Nowak-Wegrzyn et al. 2004).
Bindslev-Jensen et al. (2002) developed a statistical approachto estimate threshold levels of four major food allergens. Theyreported that the threshold dose required for a person to developan adverse reaction using a million CMP susceptible popula-tion is 0.005 mg of cow’s milk or 7×10−5 mg of milk pro-tein (Bindslev-Jensen et al. 2002). Other workers have reportedthreshold levels ranging between 3 and 180 mg (Morisset et al.2003a, Taylor et al. 2002).
Effect of Processing on the Allergenicity ofCow’s Milk Proteins
Processing techniques are routinely applied to raw milk in orderto reduce or eliminate microorganisms and enhance shelf life.Some of the techniques such as homogenisation, pasteurisationand sterilisation do not modify protein structure significantly,whereas others such as hydrolysis and irradiation do. In gen-eral, results from several studies have shown that cow’s milkallergenicity could be decreased, increased or unchanged byprocessing treatments such as pasteurisation or sterilisation andhomogenisation (Host and Samuelsson 1988).
Heat treatment
The effect of heating on milk protein allergenicity remains con-troversial. Pasteurised milk has been reported to have higher al-lergenicity than raw or homogenised milk (Host and Samuelsson1988). Caseins are more thermostable, whereas BLG manifestsa thermolabile behaviour (Wal 2004). However, BLG may beprotected from denaturation when heated due to possible inter-actions with caseins. Currently, heat denaturation is not acceptedas a satisfactory process to reduce the allergenicity of milk pro-tein. On the contrary, application of heat treatment could lead tothe formation of neo-allergens.
Hydrolysis
Hydrolysis of milk proteins reduces their allergenicity to vary-ing degrees. Several cow’s milk proteins, for example BLG,are relatively resistant to degradation by proteolytic enzymes,while others are considered very labile (e.g. caseins). Boza et al.(1994) obtained an extensively hydrolysed hypoallergenic in-fant formulae by using a combination of ultrafiltration processand hydrolysis with enzymes from bacterial/fungal origin withbroad specificity. Extensively hydrolyzed formulas (eHF) suc-cessfully protect the development of allergy symptoms in themajority of CMA infants (Walker-Smith 2003). However, eveneHFs (molecular weight (MW) less than 1.5 kDa) can still in-duce allergic response in infants with atopic family background(Nentwich et al. 2001) and CMA infants (De Boissieu et al.
1997). Moreover, eHF have also been criticised for their poorfunctionality (Crittenden and Bennett 2005).
Radiation
Lee et al. (2001) reported that the application of gamma irra-diation to α-casein and BLG altered the epitope structure ofboth milk proteins, probably due to agglomeration of the milkproteins and consequent decrease in solubility. Further researchis needed to clearly elucidate the effect of irradiated milk onallergenicity.
High-Pressure Treatment
High pressure may reveal potentially immunogenic hydrophobicregions to enzymes, resulting in better hydrolysis. Bonomi et al.(2003) reported that enzymatic hydrolysis under high pressure(600 MPa) produced non-immunogenic peptides. Other work-ers have, however, reported an increase in antigenicity of milkproteins on high-pressure treatment in the absence of hydrolysis(Kleber et al. 2004, 2007). Thus, as with irradiation, further re-search will be useful to ascertain the effect of high pressure onmilk protein allergenicity.
EGG ALLERGENSEgg protein is used as a protein nutritional standard because itis highly nutritional and has all the essential amino acids in theright amounts required by the human body. Moreover, with theexception of vitamin C, eggs serve as a good source of vitaminsA, D, E, K, as well as the B vitamins. Whole egg and egg-derived ingredients also possess excellent functional properties(e.g. gelation, emulsification and foaming), which has resulted intheir extensive use in the formulation of various food products.
Egg consists of the white and yolk, both of which containallergenic proteins. Whole egg contains 12.8–13.4% protein,10.5–11.8% fat, 0.3–1% carbohydrate and 0.8–1.0% ash on a wetbasis (Breeding and Beyer 2000). Proteins found in egg whiteare ovalbumin, conalbumin, ovomucoid, lysozyme, ovomucinand other minor albumen proteins such as avidin, ovoglobulins,flavoprotein and ovoinhibitors. The egg yolk proteins are richin lipoproteins and phosophoproteins and primarily comprise oflipovitellin, lipovitellenin, vitellin, vitellenin, phosvitin, trans-ferrin, γ -globulin, serum albumin and α2-glycoprotein.
Prevalence, Symptoms and Thresholds
Although the majority of people can tolerate eggs in their diet,a small percentage of the population, mostly children, suffer se-vere allergic reactions after consuming egg. Symptoms of eggallergic reactions include vomiting, diarrhoea, gastrointestinalpain, urticaria, angiodema, atopic dermatitis, asthma and rhico-conjunctivitis (Martorell Aragones et al. 2001).
Egg allergy prevalence in the general population is estimatedbetween 1.6 and 3.2%, making egg the second most importantcause of food allergic reactions next to peanut (Arede et al. 2000,Mine and Yang 2008 and references within). In children, egg

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
804 Part 8: Food Safety and Food Allegens
allergy is the most commonly occurring food hypersensitivitywith symptoms usually becoming evident in the child’s first year.
Major Egg Allergens
Egg white is more allergenic than the egg yolk. Ovalbumin andovocumoid, the two most potent egg allergens together makeup about 65% of the composition of egg white proteins. Oval-bumin has a MW of 44.5 kDa and contains 385 amino acids.Using pooled sera from 18 egg-allergic patients, Mine and Rupa(2003) identified five IgE binding linear epitopes in the primarystructure of the protein. Four of the five epitopes were exposedat the surface of the protein.
Ovomucoid, the other major allergen, is a 28 kDa MW proteincomprising 186 amino acids. The protein has three structurallydistinct domains (Domain I, II and III), which are cross-linkedby disulfide bonds. Several linear sequences representing aller-genic epitopes recognised by both IgE and IgG antibodies havebeen identified (Zhang and Mine 1998, Mine and Zhang 2002).Ovomucoid also contains 20–25% carbohydrate moieties. Mostreports indicate that the carbohydrate moieties are not immuno-genic; however, some studies suggest that the carbohydrate re-gion in the third domain is immunologically active (Mine andRupa 2004). Ovomucoid is relatively stable to digestion, andheat and allergenic fragments have been detected even after di-gestion by pepsin.
Other reported egg allergens are ovotransferrin (MW 76 kDa)and lysozyme (MW 14.3 kDa). Aabin et al. (1996) reporteda higher frequency of reactivity for ovotransferrin (53%) thanfor ovomucoid (38%) and ovalbumin (32%), suggesting that itmay be a more important allergen than the latter two. The sameauthors reported frequency of reactivity of 15% for lysozyme.Very few studies have reported on the allergenicity of egg yolkproteins; however, some of the allergenic proteins identified inegg yolk include apovitellenin I, apovitellenin VI and phosvitin(Walsh et al. 1988, 2005).
Thresholds of Clinical Reactivity to Eggs
Reported thresholds of clinical reactivity to eggs range between0.13 and 6.5 mg of hen’s egg protein (Morisset et al. 2003a,Taylor et al. 2004). As with other allergens, there are currentlyno cures for egg allergy, and the best management tool is thereading of food labels and avoidance of foods containing eggor egg-derived ingredients. The use of multiple definitions foreggs and egg ingredients (e.g. albumin, albumen, conalbumin,egg nog, egg yolk, egg white, lecithin, livetin, lysozyme, oval-bumin, ovoglobulin, ovomacroglobulin, ovomucin, ovomucoid,ovomucin, ovovitellin, ovotransferrin and vitellin) in the pastmade egg avoidance challenging. Today, most countries in NorthAmerica as well as in Europe require the use of the commonnames of priority allergens when they are used as ingredients infoods or are likely to be present in foods in spite of best effortsto control their presence. Fortunately, most children outgrowtheir egg allergy by school age (Heine et al. 2006). Egg allergy,however, tends to persist in children with positive skin tests,multiple allergies and/or who have more severe reactions (e.g.
respiratory symptoms, angiodema and multisystemic reactions)or other atopic diseases such as asthma (Ford and Taylor 1982,Mine and Yang 2008).
SOYA BEAN ALLERGENSSoya bean (Glycine max) is a legume belonging to the fabaceaefamily and the glycine genus. On a dry basis, soya beans contain35–40% protein, 17–23% lipid, 31% carbohydrate and 4–5%minerals. Soya bean is considered as one of the most nutritionalplant sources of food providing a well-balanced amino acidprofile and good supplies of omega 3 and omega 6 fatty acids.The history of the seed dates as far back as 3000–5000 years,with its origins somewhere in Asia.
Consumption of soya bean and soya bean foods has beenlinked to many health benefits. Various studies have reported as-sociations between soya bean consumption and reduced riskof cardiovascular disease, cancer, diabetes, bone loss andmenopausal symptoms amongst others (Friedman and Brandon2001, Hori et al. 2001, Chen et al. 2003, Zhang et al. 2003,Stephenson et al. 2005, Anderson 2008). These reports have fu-elled the growth of soya foods in Western countries. In October1999, the Food and Drug Administration of the United Statesapproved a health claim linking the consumption of 25 gramsof soya protein a day (as part of a diet low in saturated fattyacids) to reduced cardiovascular disease risk (FDA 1999). Formanufacturers to make this claim, products must provide at least6.25 grams of soya protein per serving. Soya flour and soya pro-tein ingredients are therefore increasingly being used in manyfood products.
Unfortunately, soya bean is listed in Canada, the United States,Australia and the European Union as a priority allergen, requir-ing labelling when it is used as an ingredient in foods. Symp-toms of soya bean allergy are similar to the other major allergensand include cutaneous, respiratory as well as gastrointestinal re-sponses. Although the majority of allergic responses occur oningestion, allergic reactions on inhalation of soya bean and soyabean byproducts has also been reported (Gonzalez et al. 1992,1995, Codina et al. 1997).
Major Soya Allergens
Over 17 different allergens have been identified in soya bean.These include soya bean glycinin (11S), β-conglycinin (7S),soya bean vacuolar protein (Gly m Bd 30K or P34), the Kunitztrypsin inhibitor (KTI), Gly m Bd 28K, soya bean profilin(Gly m 3), soya bean hull proteins (Gly m 1.0101, Gly m1.0102, Gly m 2) and the pathogensis-related (PR) soya beanprotein SAM22 (Gly m 4) (Wilson et al. 2005, L’Hocine andBoye 2007, Boye et al. 2010).
Glycinin and β-conglycinin have been studied extensivelyas they are the major soya bean storage proteins and repre-sent over 70% of the proteins found in soya (Liu 1997). Theyare both globulins belonging to the cupin superfamily (Breit-eneder and Radauer 2004) and have complex quaternary struc-tures with conserved amino acid sequence homology. Glycinin

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 805
(MW ∼ 300 kDa) has a hexameric structure with each monomercomprising an acidic and basic subunit linked by disulfide bonds.β-conglycinin (MW ∼ 150 kDa) has a trimeric structure withthe three major subunits α, α′ and β having MWs of 76, 72and 53 kDa, respectively (Liu 1997, Krishnan 2000). Variousstudies have shown that all glycinin and β-conglycinin subunitsbind IgE from soya bean-allergic patients although a few studieshave found an absence of binding to some subunits (Pedersenand Djurtoft 1989, Krishnan et al. 2009, Boye et al. 2010).
The soya bean vacuolar protein (P34; MW of 34 kDa), whichis an oil body-associated protein, is also a major soya allergen.Over 65% of soya bean-allergic patients reportedly react to it(Ogawa et al. 1991, 1993). The KTI, which is a 21 kDa belongingto the plant defence system, is another important allergen. KTIexerts its effect by inhibiting the activity of proteases such astrypsin. Although the major allergenic epitopes have not beenidentified, reports suggest that it may be a culprit in soya bean-induced occupational respiratory disorders (Baur et al. 1996)along with the soya bean hydrophobic lipid transfer proteinsidentified in soya bean hulls (Gonzalez et al. 1992, 1995).
Prevalence, Symptoms and Threshold
Prevalence rates of soya allergy range between 0.3% and 0.4%(Becker et al. 2004, Sicherer and Sampson 2006). The exactamount of soya proteins required to induce an allergic responseis, however, not known. Reported threshold levels vary signif-icantly and range between 0.0013 and 500 mg of soya protein(Bindslev-Jensen et al. 2002, Ballmer-Weber et al. 2007).
Effect of Processing on Soya Allergens
In general, processing treatments such as thermal treatment,microwaving, irradiation, hydrolysis and fermentation have notbeen shown to remove soya bean allergenicity. Some treatmentsmay cause modifications in proteins structure and hide aller-genic epitopes reducing but not eliminating their immunogenic-ity, whereas other treatments cause unfolding of the proteins,allowing greater exposure of hidden allergenic epitopes and in-creasing the immunogenic properties of the proteins (Davis andWilliams 1998, Soler-Rivas and Wichers 2001).
Soya bean is processed into products such as soya beverages,tofu, edamame, miso, natto and tempeh. The beans can also beprocessed to obtain soya oil, soya flour, soya lecithin, soya fibre,soya protein concentrate (>65% protein on dry basis), soya pro-tein isolate (>90% protein on dry basis), textured soya productsand soya hydrolysates or hydrolysed vegetable protein, whichare used in a wide variety of products. Other novel applicationsinclude soya ice cream and soya yogurt. Allergenicity of soyafoods is linked to the presence of residual soya proteins in thesefoods, so unless the soya ingredient used is highly refined (e.g.refined soya bean oil), it is likely to contain allergenic proteinand must be labelled when used in foods. Studies conductedon soya lecithin have generally reported little or no allergy riskto sensitised individuals (Awazuhara et al. 1998); however, hy-drolysed and fermented soya products tend to retain some oftheir allergenic properties (Hefle et al. 2005, L’Hocine and Boye
2007). Appropriate caution therefore needs to be exercised inthe consumption of processed soya foods.
Soya Allergen Cross-Reactivities
Although not confirmed clinically, a high cross-reactivityhas been reported for different legumes (soya bean, peanut,lentils and beans; Yunginger 1990, Eigenmann et al. 1996,Kalogeromitros et al. 1996). This may be explained by thehigh amino acid sequence homology, which frequently occursin plant proteins belonging to the same family. Clinical co-reactivity rates in peanut-allergic patients for soya using placebo-controlled challenges range between 1% and 6.5% (Burks et al.1988). Additionally, coexisting clinical reactivity has been re-ported between soya bean and cow’s milk for some allergicpatients ranging between 5% and 50% depending on the spe-cific group of patients studied (Host and Halken 1990, Burkset al. 1994).
PEANUT AND TREE NUT ALLERGENSPeanuts and tree nuts contain some of the most potent foodallergens. Prevalence rates of 0.8–1.5% for peanut allergy inthe UK and US population and about 0.6% for tree-nut allergyin the US population have been reported (Grundy et al. 2002,Sicherer et al. 2003). Nuts and tree nuts belong to different plantspecies; however, they are frequently discussed together as theirpresence, handling and use in the food chain as well as theallergic responses they induce are often similar.
Peanut (Arachis hypogea) is a legume belonging to the fam-ily Leguminosae. It grows under the ground in peanut podscontaining the peanut seed. Tree nuts, on the other hand, areedible seeds that grow on trees. Examples of tree nuts that areof most concern as allergens are hazelnut (Corylus avellana),almond (Prunus dulcis), pistachio (Pistachia vera), macadamianuts (Macadamia integrifolia), cashew (Anacardium occiden-tale), walnut (Juglans regia), pine nut (Pinus pinea), pecans(Carya illinoinensis) and Brazil nut (Bertholetia excelssa).
Prevalence and Threshold
Prevalence rates of peanut and tree nut allergies vary for differentpopulations but appear to be higher in Western societies such asin Europe and North America. Reported rates vary from 0.2 to1.7 for peanut and 0.1 to 1.4 for tree nuts (Sicherer et al. 2003).Allergic responses following ingestion of peanut and tree nutsby allergic patients range from oral pruritus, nausea, vomiting,urticaria, angiodema, bronchospasm, bronchitis, hypotension,anaphylaxis and death in some instances. The reaction oftenoccurs within minutes to a few hours after food consumption, andthe severity of the response may be exacerbated by preexistingasthma (Sampson 2002, Sicherer et al. 2003).
Threshold doses for clinical reactivity reported in the literaturerange from 100 µg to 10 mg for peanut and 20 µg to 7.5 mg fortree nuts (Hourihane et al. 1997, FDA 2006). Cross-reactivitiesbetween peanut, soya bean as well as other tree nuts have beenreported (de Leon et al. 2003).

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
806 Part 8: Food Safety and Food Allegens
Major Peanut and Tree Nut Allergens
The major allergens identified in peanut are Ara h 1 (glycopro-tein, vicilin, MW 63.5 kDa), Ara h 2 (glycoprotein, conglutin,MW 17.5 kDa), Ara h 3 (legumin, MW ∼ 60 kDa), Ara h 4(legumin, MW 37 kDa), Ara h 5 (profilin, MW 14–15 kDa), Arah 6 (conglutin, MW 14.5 kDa), Ara h 7 (conglutin, MW 15.8kDa) and Ara h 8 (pathogenesis-related protein, MW 16.9 kDa;Wen et al. 2007, Rajamohamed and Boye 2010). Ara h 1 and Arah 2 are classified as major allergens and are recognised by thesera of >90% of peanut-allergic patients. Ara h 3, Ara h 4, Ara h5, Ara h 6, Ara h 7 and Ara h 8 are less frequently recognised bythe sera of peanut allergic individuals and are classified as minorallergens (Wen et al. 2007, Rajamohamed and Boye 2010).
Allergenic proteins in tree nuts vary depending on the type ofnuts. In a voluntary survey report on tree nut allergy conductedby Sicherer et al. (2001), 46% of tree-nut-allergic individualsreacted to multiple tree nuts, and 54% reacted to single treenuts with the highest reactions being reported toward walnut(34%), cashew (20%) and almond (15%) and lower allergicresponses to pecan (9%), pistachio (7%), hazelnut, Brazil nut,macadamia nut, pine nut and hickory (less than 5% each). Table42.3 provides a list of some of the major proteins identified intree nuts and their properties (Rajamohamed and Boye 2010).
Processing-Induced Changes in Peanut andTree Nut Allergenic Proteins
Processing induces changes in peanut and tree nut proteins,which can modify their allergenic properties. Many research
studies have found, for example, that roasting increases the im-munogenic properties of peanut compared to frying and boiling.Using sera of peanut-allergic patients, Beyer et al. (2001) foundlower IgE-binding intensities of Ara h 1, Ara h 2 and Ara h 3 infried and boiled peanuts compared to roasted peanuts. Similarly,Maleki et al. (2000) found significant increases in the allergenicproperties of roasted peanut compared to raw peanut. On thecontrary, Koppelman et al. (1999) reported no change in theallergenicity of Ara h 1on heat treatment. Hansen et al. (2003)also reported that dry roasting of hazelnut reduced its aller-genicity compared to raw hazel nut. Differences in the effect ofthe thermal treatment on the molecular structure of the proteinsand their solubility may explain the variations in the responsesreported.
FISH AND SHELLFISH ALLERGENSFish and shellfish represent one of the most common sources offood allergens in the adult population. Fish and shellfish speciesknown to cause allergic reactions include but are not limited tocod, flounder, grouper, haddock, halibut, hake, herring, mack-erel, pike, sole, snapper, trout, crabs, lobsters, prawns, shrimps,crayfish, octopus, squid, clams, mussels, oysters, scallops andsnails.
The major allergen in fish is parvalbumin (Gad c 1), a 12kDa protein (O’Neil et al. 1993). Tropomyosin, with a MWof ∼36 kDa, is the major allergen found in shrimp, lobster,crab and molluscs such as squid, oyster, snail, mussels, clamand scallops (Daul et al. 1993a, 1993b). Both parvalbumin
Table 42.3. Major Tree-Nut Allergens and Their Characteristics
Tree Nuts AllergenMolecular
Weight (kDa) Protein FamilyAllergen
TypeIdentifiedEpitopes
AllergenStability References
Cashew Ana o 1 50 Vicilin (7S) Major 11 Thermostable 51, 54Ana o 2 33 and 53 Legumin (11S) Major 22 Thermostable 53, 54Ana o 3 12 Albumin (2S) Major 16 Thermostable 52, 54
Walnut Jug r 1 14 Albumin (2S) Major 3 NR 55, 56Jug r 2 44–47 Vicilin (7S) Major NR NR 57Jug r 3 9 LTP NR NR NR 58Jug r 4 NR Legumin (11S) NR NR NR 58, 76
Hazelnut Cor a 1 18 PR-10 Major NR Thermolabile 59, 61Cor a 2 14 Profilin Major NR NR 59Cor a 8 9 LTP Major NR NR 63Cor a 9 35–40 Legumin (11S) Major NR NR 63
Cor a 11 47 Vicilin (7S) NR NR NR 63Brazil nut Ber e 1 9 Albumin (2S) Major NR Thermostable
and resistantto proteolysis
64, 65
Ber e 2 22 and 35 Legumin (11S) Minor NR NR 67Almond NR 45 Vicilin (7S) Major NR NR 70
NR 20–22 and38–42
Legumin (11S) Major NR NR 68, 69
NR 12 Albumin (2S) Major NR NR 70
Source: Adapted from Rajamohamed and Boye 2010.MW, molecular weight; NR, - not reported; PR, pathogenesis-related protein family; LTP, lipid transfer protein.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 807
and tropomyosin are muscle cell proteins. To date, eight majorIgE-binding epiopes have been identified in shrimp tropomyosin(Lehrer et al. 2003).
Exposure, including handling, consumption and inhalation ofair-borne particles from fish and fish ingredients, can induceallergic reaction in sensitised individuals. Seafood-induced al-lergic reactions are generally similar to responses induced bymany of the other allergenic foods. A study conducted using30 shrimp-sensitive and 37 fish-allergic individuals reported al-lergic symptoms ranging from generalised itching, urticaria toswelling of the lips and tongue (Lehrer et al. 2003). Other re-ported symptoms include difficulty breathing, gastrointestinaldistress and anaphylactic shock (O’Neil et al. 1993, Daul et al.1993a, 1993b).
Additionally, occupational reactions among a variety ofseafood workers (e.g. fish and prawn workers, seafood pro-cessing workers, fishermen, canners, restaurant cooks and otherworkers in the seafood industry) have been reported. Cartieret al. (1984) showed that workers in the seafood industry wereexposed to occupational allergens through direct contact withseafood products as well as inhalation of bits of seafood or wa-ter droplets generated during processing. Out of the 303 crabworkers investigated, 18% reported rhinitis or conjunctivitis,about 24% some sort of skin rash and over a third reported ofasthma.
Very little work has been done on the effect of process-ing on the allergenicity of seafood. As with other allergens,highly refined products from seafoods that do not contain resid-ual proteins (e.g. refined fish oils, gelatine and isinglass) donot pose a risk to allergic consumers. However, processingtechniques that leave seafood protein fragments in the finishedproduct may pose serious allergenic risk to sensitised individ-uals. As consumers and the food industry become increasinglyaware of the health benefits of fish, consumption and utili-sation of fish and fish products is likely to increase, whichcould increase the allergen risk for fish- and shellfish-sensitisedindividuals.
ALLERGENS IN CEREALSCertain cereal grains contain proteins that induce immune-mediated responses in individuals who are predisposed to CD orwho have specific cereal allergy. As the mechanisms involvedin celiac disease are distinctly different from those involved inIgE-mediated cereal allergy, they will be discussed separately.
Celiac Disease
CD also sometimes known as gluten-sensitive enteropathy orgluten intolerance is an abnormal immunological response togluten/gliadin, which frequently results in a diseased state char-acterised by damage of the lining of the gut (villous atrophy). Inthese individuals, the T lymphocytes in the small intestines re-spond abnormally to gluten, causing inflammation and damageto the absorptive epithelium of the small intestine, resulting inmalabsorption and disorders such as diarrhoea, bloating, weight
loss, anaemia, weakness and muscle cramps. In children, CDleads to growth retardation and underweight. Symptoms lingerfor some days even after the offending food is avoided due tothe fact that the damaged intestine requires time to heal. Mortal-ity rate has not been reported but patients are likely to developmalignant lymphomas (Ferguson 1997).
CD occurs more commonly in Caucasians than in Blacks,Asians and Hispanics according to present knowledge. Whetherthis is due to under-diagnosis or true biosocial/genetic differ-ence is not clear. Reported prevalence rates are 1:200–400in Europe, 1:133 in America, 1:100–300 in a UK study and1:120 in a Belfast study (Rostami et al. 1999, Gomez et al.2001, Fasano and Catassi 2001, Fasano et al. 2003, GarcıaNovo et al. 2007). CD appears to be genetic with 10% preva-lence rates reported among first-degree relatives of CD patientsand 70–100% concordance rates amongst twins. Higher preva-lence rates are reported in women likely due to higher rates ofdiagnoses.
The primary offending foods for celiacs are wheat, barley andrye. The major proteins present in these cereals are albumins,globulins, gliadin (prolamin) and glutenin (glutelin) and the of-fending protein for celiacs is the gluten fraction in these cereals,which are the prolamins and glutelins, particularly the prolamins(i.e. hordein (barley), secalin (rye) and gliadin (wheat)). Severalrepeating peptide sequences (e.g. QQPFP, QQQP, QQPY, QPYP,PSQQ) in the primary structure of these proteins have beenblamed (Osman et al. 2001, Kahlenberg et al. 2006, Darewiczet al. 2008). Although the mechanism involved in the pathogen-esis of the disease is unclear, tissue transglutaminase is believedto play a key role in the deamidation of glutamine converting itto glutamic acid, which allows the immune cells to bind, provok-ing continued immune response (Anderson et al. 2000, Mazzeoet al. 2003). The principal organ targeted is the gut (i.e. smallintestine); however, damage to other parts of the body such asthe skin (dermatitis herpetiformis), the teeth and the liver hasbeen reported (Lohi 2010). Severity of the disease increases sig-nificantly with delays in diagnosis (i.e. age of diagnosis) and thedegree of susceptibility increase with the rate of gluten consump-tion (quantity). Tolerance thresholds for the general populationof CD patients are not known but some workers have reportedvalues ranging between 10 and 100 mg gluten (Collin et al. 2004,Hischenhuber et al. 2006, Catassi et al. 2007).
IgE-Mediated Cereal Allergy
IgE-mediated cereal allergy is distinctly different from CD. Thistype of allergy is an immediate-type hypersensitivity occurringminutes to hours after consumption of the offending food. Symp-toms are similar to those described for the other allergens andinclude oral allergy syndrome (e.g. swelling of lips), respira-tory difficulties (e.g. asthma), skin reaction (e.g. eczema, atopicdermatitis) and gastrointestinal distress (e.g. nausea, diarrhoea,vomiting and cramps). There is no accurate data available on theprevalence, but as is the case for the other allergens, genetic sus-ceptibility has been suggested (Becker et al. 2004). Severity ofIgE-mediated cereal allergy depends on the immune state of thepatient (degree of sensitisation/tolerance) and the concentration

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
808 Part 8: Food Safety and Food Allegens
of antigen in the food consumed. The proteins responsible forthis type of allergy can be the albumins, globulin, gliadins orglutenins and will vary depending on the individual and the spe-cific allergenic food. Offending foods include buckwheat, rice,corn, millet, wheat, oats, rye and barley (Cantani 2008). Buck-wheat and rice allergies are more frequently observed in Asiathan in Europe or North America (Taylor and Hefle 2001, Ku-mar et al. 2007). The pathway for sensitisation and cereal allergyelicitation is by ingestion (mouth) and/or inhalation (nose) (e.g.baker’s asthma). Wheat allergy is responsible for up to 30% ofoccupational asthma in the bakery industry.
Another type of cereal allergy is exercise-induced cereal al-lergy. Symptoms in this case appear only after food allergenconsumption is followed by exercise. Wheat, as well as shellfishand nuts, is mostly associated with this type of allergy (Romanoet al. 2001, Beaudouin et al. 2006, Porcel et al. 2006).
Foods to Avoid for Gluten-SensitiveEnteropathy Patients and IgE-MediatedCereal-Allergic Patients
As with the other allergens, there are presently no cures forCD. Major foods to avoid include barley, wheat, durum, farina,kamut, rye, semolina, spelt and triticale. Oats was previouslyincluded in the list of gluten-containing foods; however, sev-eral recent studies suggest that quantities of oats of up to 50g/day are harmless to the majority of gluten-sensitive individu-als (Janatuinen et al. 1995, 2000, 2002, Lundin et al. 2003). Amajor challenge for the industry is that commercial oats is veryfrequently contaminated with high amounts of wheat, barley orrye (Thompson 2004, 2005) as these crops are often grown inthe same regions and in close proximity. Furthermore, a smallpercentage of CD patients may react to oat proteins. The mech-anisms at play in this instance and the specific proteins in oatsto which these patients react still remain to be clarified. Asgluten-containing cereals are often used as ingredients in foodformulation, other foods to avoid include hydrolyzed vegetableprotein, flavouring, malt, maltodextrin, malted barley, malt vine-gar and starch from gluten sources, especially if these containresidual amounts of gluten proteins.
Many countries have adopted the gluten-free Codex Alimen-tarius Standards (Joint FAO/WHO Food Standards Programmeand Codex Alimentarius Commission 2008), which sets a max-imum limit of 20 ppm for gluten-free foods that are naturallyfree from gluten and 100 ppm for gluten-free foods that havebeen rendered gluten-free through processing.
For IgE-mediated cereal allergy, foods to avoid will dependon the particular allergy. Major challenges for cereal-allergic in-dividuals are cross-reactivity and cross-contamination of foods.Food ingredients that are particularly problematic if not prop-erly labelled are starches, spices, seasonings, sauces, flavourings,colourings, some vinegars, hydrolysed plant protein, syrups (e.g.brown rice syrup), beverages (e.g. beer, ale, etc.). Other poten-tial hidden sources of cereals or cereal ingredients are cosmetics,pillows, toy stuffings and certain medications when products de-rived from these are used as ingredients.
SESAME AND MUSTARD ALLERGENSSesame Allergy
Sesame (Sesamum indicum) is a herbaceous plant of the Ped-aliaceae family originating from India, which is now grown inmany countries. It is also known as Benne, Gingelly, Til or Teel,Simsim and Ajonjoli and is now a common ingredient used ex-tensively in everyday foods because of its high nutritional value(Perkins 2000). Sesame proteins are rich in methionine (Dalalet al. 2002, Wolff et al. 2003). Common sesame products in-clude biscuits, crackers, breadsticks, rice cakes, etc., as well asprepacked delicatessen and processed foods such as noodles,dips, soups, sausages, samosas, processed meats, vegeburgers,chutneys, etc., (Perkins 2000, Allergyexpert 2010).
Sesame seeds, which may be used whole or crushed, are ex-tremely potent allergens, causing severe allergic reactions insusceptible individuals. The first case of sesame allergy wasreported in 1950 (Gangur et al. 2005). More recently, a studyof Australian children showed that allergic reactions to sesameranked fourth behind reactions to egg, milk, and peanuts, andsesame was also found to be the third most common allergy-inducing food in Israeli children (Gangur et al. 2005). Anotherrecent study showed that sesame allergy in Israeli children wasmore common than peanut allergy (More 2009). Sesame allergyseems to affect people of all ages, which imply that this foodallergy is not commonly outgrown. The symptoms of sesameallergy can include urticaria, angioedema, asthma, atopic der-matitis, oral allergy syndrome, allergic rhinitis and anaphylaxis.
One of the major sesame seed allergens is the 9 kDa, 2S albu-min (Pastorello et al. 2001). Beyer et al. (2002) also identified10 IgE-binding proteins in sesame, four of which had MWs of7, 34, 45 and 78 kDa. Wolff et al. (2003) have also reported a14 kDa sesame allergenic protein belonging to the 2S albuminfamily.
Sesame products are used in a wide variety of food productsand may represent hidden allergens in foods. Fatal anaphylacticreactions have occurred as a result of consuming sesame (Ganguret al. 2005). Unrefined sesame oil may be used in food products,which may trigger allergic reactions in susceptible individuals.The oil resists rancidity and is popular with Oriental chefs. Inthe bakery industry, workers have reported allergic reactions,which include asthma, to sesame products. In addition to its usein the food industry, sesame and sesame products are used inthe pharmaceutical and cosmetic industries. Sesame productsused in cosmetics and ointments may cause allergic dermatitis,an inflammatory condition of the skin, in sensitised individuals.Contact dermatitis as a result of direct exposure to cosmetics orpharmaceutical products containing sesame allergens has beenreported. Specific instances of sesame allergy resulting in skinrashes and inflammation after baking with sesame seeds andskin rashes from cosmetics that contain sesame oil have alsobeen reported (Stoppler and Marks 2005).
As sesame allergens are similar in biochemical structure topeanut allergens, people with sesame allergy may be at risk ofhaving allergic reactions as a result of eating peanuts and vice-versa (Gangur et al. 2005). Cross-reactivity may also exist withrye, kiwi, poppy seed and various tree nuts (such as hazelnut,

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 809
black walnut, cashew, macadamia and pistachio), but clinicalstudies are lacking.
While the number of reports of sesame allergy has steadilyincreased, it is still not clear whether this increase is in the num-ber of reactions or an increased rate of detection and reportingof these allergic reactions (Stoppler and Marks 2005).
Mustard Seed Allergy
The mustard plant belongs to the family Brassicaceae with cab-bage, cauliflower, broccoli, Brussel sprout, turnip and radish(Monreal et al. 1992). Mustard is often consumed as a condi-ment prepared from the mustard seed. The powder is made froma mixture of two species, Sinapis alba L. (yellow mustard) andBrassica juncea L. (oriental mustard). The varieties Brassicanigra and Brassica juncea are used for food products. In addi-tion to mustard powder, mustard is also usually found in saladdressing, mayonnaise, soups and sauces (Ensminger et al. 1983).
Mustard allergy is now considered to be a very common foodallergy, accounting for about 1.1% of food allergies in children(Morisset et al. 2003b) and ranks fourth in children’s food al-lergies after eggs, peanuts and cow’s milk (Rance et al. 2000).The major allergen of yellow mustard is Sin a 1, which has beenfound to be resistant to heating and proteolysis (Dominguez et al.1990, Gonzalez de la Pena et al. 1996, Rance et al. 2000). Bra j 1is the major allergen in oriental mustard with a structure similarto that of Sin a 1 (Gonzalez de la Pena et al. 1991, Caballeroet al. 1994).
Mustard allergy can cause a wide array of symptoms. Ranceet al. (2000) reported that allergic reactions to mustard startearly in life and are probably linked to early consumption ofbaby foods. Mustard-allergic patients will react to any foodthat comes from the mustard plant, including jars of mustard,mustard powder, mustard leaves, seeds and flowers, sproutedmustard seeds, mustard oil and foods that contain these (Bock2008).
Common symptoms of mustard allergy include difficulty inbreathing, shortness of breath and other breathing complications,a rash or hives, itchy skin or general skin irritation. In some se-vere cases, it can lead to anaphylaxis, and if left untreated, ana-phylaxis can lead to anaphylactic shock and even death. Someof the common symptoms of anaphylaxis include constriction ofairways in the throat and lungs, anaphylactic shock, severe dropin blood pressure, heightened pulse and heavy heartbeat, dizzi-ness, nausea and abdominal pain, confusion and disorientation,and loss of consciousness. Panconesi et al. (1980) reported thefirst case of mustard-induced anaphylaxis after the subject hadconsumed pizza.
Incidents of cross-reactions have been rarely reported. How-ever, single cases have been described of cross-allergy tocauliflower, broccoli, cabbage and Brazil nuts, which may belinked to sequence homology of some proteins (Moneret-Vautrin2006). One of the major challenges of mustard allergy is thatmany foods contain mustard even when it would seem unlikely(e.g. lunchmeat and hot dogs). Thus, careful reading of labelson processed foods is important for mustard-allergic patients.
MINOR FOOD ALLERGENSAs previously indicated, over 170 foods are known to provokeallergic reactions in humans (Taylor 2000). In addition to thenine major priority allergens, other minor food allergens and/oremerging allergens include lupin, pea, chickpea, lentil, fruits(e.g. apple, apricot, avocado, banana, cherry, grape, kiwi, mango,melon, peach, pear, pineapple and strawberry) and vegetables(celery, carrot, eggplant, lettuce, potato, pumpkin and tomato).The reader is referred to the following references for furtherreading (Pereira et al. 2002, Fernandez-Rivas 2003, Fernandez-Rivas et al. 2008, Harish Babu et al. 2008, Towell 2009, Skypala2009, Jappe and Vieths 2010).
MANAGEMENT OF FOOD ALLERGYMany of the priority food allergens such as milk, eggs, nuts andsoya bean are commonly used in food processing (e.g. processedbeef, sausages, salad dressings, breads, cakes, soups and sauces)and pharmaceutical products (e.g. casein hydrolysates as “drug”carriers) due to their desirable properties (Monaci et al. 2006).Extensive use of these foods as ingredients in various prod-ucts increases the chances of their presence as hidden allergens,particularly when they are undeclared or present as a result ofcross-contact.
As there are currently no cures for food allergy, the best man-agement tool is the reading of food labels and avoidance of foodscontaining allergens or allergen-derived ingredients. As a result,many countries presently require the use of the common namesof priority allergens when they are used as ingredients in foods.
A major development in the last decade has been the use ofprecautionary allergen labelling to warn allergic consumers ofthe likely presence of allergens. Unfortunately, consumers withfood allergy have become less avoidant to products with advi-sory labels, such as “may contain” or “shared equipment” due totheir misuse (Hefle et al. 2007). Pieretti et al. (2009) studied theuse of advisory labels in the United States and found that 17% of20,241 manufactured foods contained advisory labels. Thus, theunregulated use of advisory labels has become a source of con-fusion and frustration, which could eventually pose challengesfor allergic consumers (Pieretti et al. 2009).
Recent emergence of the hygiene hypothesis (Yazdanbakhshet al. 2002) brings a new approach for the management of al-lergic diseases. Several epidemiological studies have suggestedthat allergic diseases are more common in industrialised nationsand urban areas compared to developing countries and rural ar-eas. Less frequent microbial exposures in the developed worldhas been regarded as an important predisposing factor for havinghigher allergic population in these regions. To compensate theinadequate exposure of microbial load, probiotics (live bacteria,usually Lactobacillus and Bifidobacterium) are now being addedin some infant formula along with oligosaccharides (prebiotics;Matricardi et al. 2003). The goal is to achieve the developmentof regulatory T cell or balanced Th1/Th2 activity, which couldeventually prevent allergy development (Cross et al. 2001, Pri-oult et al. 2004). Further research will be required to confirm thepurported effects.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
810 Part 8: Food Safety and Food Allegens
Another area of interest is specific oral tolerance induction(SOTI). Taking milk as an example, about 15% of children withmilk allergy maintain the susceptibility permanently in theirlife. Strict avoidance of cow’s milk and cow’s milk derivativesremains the gold standard for allergen management for suchCMA patients. For these patients, however, the likelihood ofexposing the offending allergen unintentionally always remainsand thus total avoidance cannot be guaranteed. Similar concernsexist for patients with persistent peanut and tree nut allergies.SOTI is a promising approach particularly for patients with per-sistent food allergy. Staden et al. (2007) reported that SOTItreatment (using a daily dose of CMP, starting from 0.002 mgCMP) remarkably increased the threshold dose for allergic reac-tion in CMA patients. As a result, the patient could be protectedagainst potentially fatal allergic reactions when small amountsof the hidden allergen are accidentally ingested. Since this ap-proach uses the specific offending allergen to induce tolerance,development of mild to moderate side effects (such as itchingin the mouth, nausea and wheals, etc.) is very common. Closesupervision by an experienced professional is, therefore, neces-sary for SOTI treatment. Similar promising studies have beenreported for peanut (Blumchen et al. 2008, Clark et al. 2009,Jones et al. 2009).
For the food industry, food allergen testing has become anincreasingly important tool for the management and control ofallergens during food production and processing. The rest ofthe chapter provides a brief summary of some of the methodscurrently available for allergen detection.
METHODS FOR DETECTING ALLERGENSTable 42.4 provides examples of some of the commonly usedmethods for food allergen detection. Food allergens may bedetected either by the presence of the target allergen itself orby using a marker in the target food. The method of choicewill depend on factors such as food matrix interference, natureand quantity of the target allergen, the desired level of detection,specificity and time and resources required for running the assay.The threshold dose for sensitised individuals to manifest allergicreactions is quite low and variable among individuals (Bindslev-Jensen et al. 2002). However, it is commonly agreed that foodallergen detection methods should be sensitive enough to detect1–100 mg of analyte (allergen) per kg of processed food (Pomset al. 2004). Increasing numbers of rapid and user-friendly testkits to detect different food allergens are now commerciallyavailable with sensitivities ranging from 0.05 to 10 mg/kg (Table42.5).
Protein-based food allergen detection methods include im-munoblotting, rocket immunoelectrophoresis, enzyme aller-gosorbent test, enzyme-linked immunosorbent assay (ELISA),protein microarray and biosensors. More recently developedDNA-based methods are available as supplementary and com-plementary methods to protein-based methods and are particu-larly useful in species differentiation and detection of geneticallymodified food (Mustorp et al. 2008). This chapter will focus onELISA-based detection, lateral-flow assays (LFA) and dipstick
test, proteomic approaches and DNA-based allergen detectionmethods.
ELISA-Based Detection Methods
Among the growing number of food allergen detection tech-niques, ELISA has gained prominence and has become an exten-sively used technique due to its high sensitivity and specificity,availability of automation and user friendliness. Some ELISAsare designed to detect specific allergens (e.g. BLG, Ara h1 (amajor peanut allergen) and shrimp tropomyosin), whereas otherELISAs detect mixtures of proteins from the allergenic source(e.g. total milk, egg, peanut and almond-soluble proteins; Tayloret al. 2009). Detection is based on binding of an allergen or aspecific marker protein with an antibody specifically generatedto recognise and bind to these proteins. This binding complexis visualised by a colourimetric assay when the enzymes, whichare labelled to the allergen specific antibody, interact with thesubstrate solution. The concentration of the allergen can be quan-tified by obtaining optical density (OD) values with a microplatereader and plotting these values using a standard curve.
There are certain limitations of ELISA-based detection meth-ods, however (Yeung 2006). ELISAs are based on aqueous sys-tems and they do not work well in detecting insoluble proteins orallergens derived from edible oil-producing foods. In addition,ELISA may not detect oleosins, a family of protein involved inthe formation of oil bodies in peanut and sesame (Pons et al. 2002and Leduc et al. 2006) and soya lecithin containing more than50 ppm residual protein (Taylor et al. 2009). ELISAs also failto distinguish certain closely related foods. For example, walnutantisera react with pecan (Niemann et al. 2009) and mustard an-tisera react to rapeseed (Lee et al. 2008). These may be caused bythe presence of cross-reactive epitopes or proteins between twofoods (Taylor et al. 2009). Regardless of the above-mentionedlimitations, ELISA is still a very powerful tool and remainsthe method of choice for food allergen detection. ELISA-basedfood allergen detection methods are developed using either thesandwich ELISA or competitive ELISA format.
Sandwich ELISA
In this assay, as indicated by its self-explanatory name, an al-lergen of interest is captured between two allergen-specific an-tibodies. The first allergen-specific antibody is immobilised onthe solid phase to capture the allergen, and the second allergen-specific antibody is labelled with enzyme to detect the capturedallergen. Allergens need to have enough binding sites, for ex-ample, large molecules such as proteins, to allow binding of thetwo allergen-specific antibodies (Schubert-Ullrich et al. 2009).
Competitive ELISA
This assay is based on the competitive binding of unknown ana-lyte (allergen) in a sample of interest and a known analyte (aller-gen) to the allergen-specific antibody. The antigen of interest inthis case is incubated in the presence of the unlabelled antibody.Antibody/antigen complexes are formed and the solution is then

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 811
Table 42.4. Commonly Used Food Allergen Detection Methods
PrincipleLimit of
Detection Advantages/Disadvantages References
Protein-based methodsRocket immunoelec-
trophoresis(RIE)
Binding of allergen to humanIgE or antibodies raised inanimal followed byobservation in gel
2.5 mg/kg Not widely used due to thelaborious procedure.Semi-quantitative.
Besler et al.2002b
EAST inhibition Binding of specific IgEantibodies to food allergensbound to a solid phasefollowed by measurement
1 mg/kg Mainly used for clinicaldiagnosis.
Limited commercial productsavailable due to reliance onhuman sera.
Quantitative.
Nordlee andTaylor1995
SDS-PAGE andimmunoblotting
Proteins are denatured andseparated according to theirmolecular mass. The proteinsare then transferred onto amembrane and detected withlabelled human IgE orantibody raised in animals.
5 mg/kg Complex and time-consumingprocedure.
Reliance on human sera.
Scheibe et al.2001
Dot immunoblotting Reaction between sampleprotein extracts andenzyme-labelled specificantibodies on a nitrocellulosemembrane.
Intensity of dotis proportionalto the amountof allergen.
Semi-quantitative but simpleand inexpensive.
Blais andPhillippe2000
ELISA Detects allergens bycolourimetric reaction formedby the binding of allergen andspecific enzyme-labelledantibody.
0.05–10 mg/kg Most widely used method.High specificity and sensitivity.Rapid ELISA kits for major
allergens are commerciallyavailable.
Schubert-Ullrichet al. 2009
Flow-throughMicroarray
Immobilised allergen specificantibodies on a microarraychip react with allergens.
1.3 ng/mL forovalbumin
Powerful tool but still ininfancy stage for foodallergen detection.
Shriver-Lakeet al. 2004
Optical biosensors,e.g., surface plasmonresonance (SPR)
Interaction of immobilisedmolecules (e.g.allergen-specific antibodies)on a sensor surface and atarget molecule (e.g.allergens) in solution.
1–12.5 mg/kg Interaction is measured byeither a resonance angle orrefractive index value.
No need to use labelledmolecules.
Yman et al.2006
DNA-based methodsPCR with gel
electrophoresisAmplification of a specific DNA
fragment followed by agarosegel electrophoresis andvisualisation by staining orsouthern blotting.
<10 mg/kg Qualitative.Target DNA is less affected
than protein duringprocessing and extractionfrom food matrices.
Results do not truly representactual allergen exposure.
Poms et al.2001
Real-time PCR Uses a target-specificoligonucleotide probe with areporter dye and a quencherdye attached.
<10mg/kg Requires costly laboratoryequipments.
Allows for gel-free detection.RT-PCR kits are available for
various food allergens.
Oliver andVieths 2004
DNA-ELISA Amplified product of specificDNA fragment is linked witha specific protein labelledDNA probe coupled with aspecific enzyme-labelledantibody.
<10mg/kg Semi-quantitative. Poms et al.2004
Source: Adapted from Poms et al. 2004.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
812 Part 8: Food Safety and Food Allegens
Table 42.5. Examples of Some Commercially Available Test Kits for Food Allergen Detection
Allergenic Food Target Allergens Test Format and LOD (mg/kg food) Testing Time (min) Manufacturer
Milk Milk protein ELISA (<5) 30 NeogenCasein ELISA (0.5) 30 R-Biopharm
β-Lactoglobulin ELISA (0.1) 45 ELISA SystemsEggs Egg-white protein ELISA (0.6) 35 R-Biopharm
Egg-white protein LFA (LOD: not specified) <10 Tepnel BioSystemsEgg protein ELISA (<5) 30 Neogen
Peanuts Peanut protein LFA (<5) 10 NeogenPeanut protein LFA (1) <10 Tepnel BioSystems
Ara h1 LFA (5) 10 R-BiopharmNuts Almond protein LFA (1) <10 Tepnel BioSystems
Hazelnut protein LFA (5) 10 R-BiopharmSoya beans Soya protein ELISA (<5) 30 NeogenCrustacean Tropomyosin ELISA (1) 60 ELISA SystemsCereals Gliadin, secalins, hordeins ELISA (2) 30 R-Biopharm
Gluten Dipstick (10–20) <15 HallmarkGliadin LFA (2.5) 5 R-Biopharm
Molluscs Not specified LFA (5) <10 Tepnel BioSystems
Source: Adapted from Schubert-Ullrich et al. 2009.LOD, limit of detection; ppm, milligram of allergenic food/kg of target food sample.
added to an antigen-coated well followed by washing to removeany unbound material. The higher the concentration of antigenin the sample, the lower will be the amount of free antibody ableto bind to the antigen in the well. The allergen concentrationin the sample in this assay is therefore inversely proportionalto OD values obtained after adding the substrate. CompetitiveELISA assay is known for its ability to detect relatively smallproteins (Poms et al. 2004). Today, continuous developments intechnology allows the possibility of enzyme labelling of eitherthe analyte or the analyte-specific antibody.
LFA and Dipstick Tests
Both of these tests are modified versions of ELISA and aredesigned to meet the growing need of portable, reliable, userfriendly and cost-effective methods that can detect trace amountof allergens in suspected foods within a short period of time(Schubert-Ullrich et al. 2009). Although quantification is pos-sible in principle by using special strip test readers, commer-cially available LFA and dipstick test are primarily intendedfor qualitative or semi-quantitative purposes (yes or no). Table42.5 shows some of the commercially available tests based onELISA, LFA and dipstick methods.
LFAs or strip tests are immunochromatographic tests with amobile phase that allows movement of the allergen–antibodycomplex and/or the sample along a test strip. This techniqueis based on an immunochromatographic procedure that utilisesantigen–antibody properties and enables rapid detection of theanalyte (Rong-Hwa et al. 2010). For LFAs using a sandwichELISA, an allergen-specific detection antibody, deposited on themembrane, is solubilised upon introduction of a liquid sampleand moves along with the sample until it reaches the zone where
a capture antibody has been immobilised. At that point, theallergen–antibody complex is trapped. The presence or absenceof allergen is determined with the colour development pattern.Competitive ELISA format can also be applied in LFA tests.LFAs results can be obtained within 3–15 minutes after runningthe assay (Schubert-Ullrich et al. 2009).
Dipstick tests are also based on a similar principal as LFA butwith no mobile phase. Instead, an incubation phase is requiredin the dipstick test. Oliver et al. (2002) used dipstick assay todetect peanut and hazelnut allergens and reported that resultsof the dipstick assays and the corresponding ELISA were inconcordance. Although most dipstick tests are based on sand-wich ELISA format, application of competitive ELISA has beenreported. Depending on the time needed for incubation, foodallergen detection time, using dipstick test, could vary from10 minutes to 3 hours (Schubert-Ullrich et al. 2009).
Proteomic Approach
Recently, proteomics has gained much attention especially forthe detection and identification of IgE-binding allergens in com-plex mixtures. Proteomics is useful for identification and char-acterisation of proteins, including their post-translational mod-ifications, protein conformations (native, denatured, folding in-termediates) and protein–protein interactions (Leadbeater andWard 1987, Alomirah et al. 2000).
A proteomic analysis usually consists of sample collection andpreparation, protein separation using electrophoresis or chro-matography and protein identification and characterisation us-ing mass spectrometry. Successful identification of proteins de-pends on many factors such as the sensitivity of the mass spec-trometer, the completeness of the database, post-translational

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 813
modifications and more (Monaci et al. 2006). Many technolo-gies, including protein separation via two-dimensional elec-trophoresis or liquid chromatography (LC), mass spectrometryand arrays (to map protein–protein interactions), are applied inproteomic-based studies. Shefcheck and Musser (2004) showeduseful application of LC-based proteins separation with MSanalysis (LC-MS/MS) to detect peanut allergen Ara h1 in icecream with a detection level of 10 mg/kg. Proteomic studies canoffer more detailed information about allergens (Shefcheck andMusser 2004), help in the identification of new allergens (Yuet al. 2003) and provide objective evaluation of changes inducedby genetic modification (Herman et al. 2003). However, therequirement of a highly skilled operator, the high cost of massspectrometers, the length of time required for sample preparationand analysis, and the need for separate protocols and optimisa-tion for each sample prevent current proteomic approaches to beused for routine detection of food allergens. Nevertheless, pro-teomics remains a promising tool in allergen studies due to itsgreat potential for detection and identification of food allergensin complex mixtures. Recent developments in mass spectrometerinstrumentation and software offer ultra-high throughput, highsensitivity, and high-resolution capabilities (Chassaigne et al.2009). Currently, attempts to couple more efficient protein sepa-ration (microfluidic) and detection technologies with MS analy-sis are progressing. Proteomic approaches could therefore soonbe widely applicable for detection and identification of foodallergens.
DNA-Based Allergen Detection Methods
Detection of allergens in food, by traditional protein-based de-tection methods, can sometimes be very difficult, as they are of-ten present in minute amounts and are masked by the food matrix(Keck-Gassenmeier et al. 1999). DNA-based allergen detectionmethods have emerged as an alternative and complementarymethod to detect allergens where effective protein-based aller-gen detection methods are unavailable. DNA-based tests alsopossess high accuracy and sensitivity and, in general, are able towithstand harsh processing conditions better than correspondingallergenic proteins (Mustorp et al. 2008). On the other hand, insome food, DNA are partially or totally degraded and conse-quently false-negative results could occur, while the food maystill contain the allergen. In addition, some food matrix com-ponents may reduce DNA amplification efficiency. DNA-basedmethods, in comparison to ELISA-based methods, are relativelymore complicated, require more equipment and have lengthierprotocols. For this reason, DNA-based methods have been con-sidered impractical for routine detection. They may, however,be desirable for use by regulatory agencies and in institutionswhere there is easy access to appropriate equipment.
The sensitivity of the DNA-based methods strongly dependson the amount and on the quality of the template DNA since theDNA encoding the allergen in the food samples may be presentin low amounts and may also be degraded as a result of process-ing (Holzhauser et al. 2006). Three DNA-based approaches arecurrently available to detect food allergens.
Polymerase Chain Reaction (PCR) withGel Electrophoresis
The assay involves DNA extraction from food, amplification ofspecific DNA fragment using primers that bind selectively tocomplementary parts of the DNA to be amplified, followed byagarose gel electrophoresis (Besler 2001). PCR consists of threesteps, determined by different temperatures in every cycle ofamplification: denaturation of double strands DNA, annealingof the primers and extension of the primers by the enzyme Taqpolymerase (Poms et al. 2004). The amplified product is loadedto run agarose gel electrophoresis and visualised by staining thegel. PCR with gel electrophoresis approach is good for qualita-tive detection of allergen in the food.
PCR with ELISA
This assay is a combination of a highly specific DNA-basedmethod with the relatively simple and highly sensitive ELISAassay for semi-quantitative analysis (Poms et al. 2004). As inother PCR-based methods, extraction and purification of DNAfrom a food sample and amplification of specific DNA fragmentencoding to suspected allergen using primers in a thermocy-cler are prerequisite for PCR-ELISA assay. The ELISA compo-nent of the test involves immobilisation of the amplified PCRproduct on a solid phase (a microplate), denaturation of doublestrand, hybridisation with specific probe, detection of the probewith enzyme-conjugated antibody and observation of the en-zymatic colour reaction after addition of substrate (Holzhauseret al. 2002). The DNA concentration can be determined viaabsorbance obtained from an enzyme–substrate reaction.
Real-Time PCR
Real-time PCR allows gel-free detection ‘in real time’ with highaccuracy by using a target-specific oligonucleotide probe with areporter dye and a quencher dye attached (Desjardin et al. 1998).Oliver and Vieths (2004) reported real-time PCR method to be assensitive as sandwich ELISA in detecting peanut allergens in 33food samples. Many different types of real-time PCR assay kitsare commercially available to detect many of the priority foodallergens (Poms et al. 2004), including kits for detecting allergenencoding genes from mustard, sesame and celery (Mustorp et al.2008).
CONCLUSIONFood allergy will likely continue to be an important food safetyissue in the coming decades. Although substantial progress hasbeen made in the field in the last 20 years, much still remainsunknown. One area still requiring significant work is the ques-tion of the minimum eliciting dose required to provoke reactionsin sensitised individuals. Increasing prevalence rates along withthe possibility of severe allergic reactions after exposure to verylow level of allergens in sensitised consumers continue to bea concern. Although exact threshold doses for food allergensare not known at present, levels of detection offered by current

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
814 Part 8: Food Safety and Food Allegens
commercial allergens detection kits appear to be adequate forallergic consumer protection. There continues to be a need, how-ever, for more sensitive and easily applicable analytical meth-ods and improved understanding of the sources of cross-contactalong the food value chain.
Currently, ELISA-based rapid allergens detection kits includ-ing LFA and dipstick are extensively used to detect suspectedmajor allergens in processed foods. They will likely remain themethod of choice in the food industry for a while, because oftheir fast and easy usage. Other methods such as surface plas-mon resonance on automated platforms or protein microarraysin combination with immunochemical analytical approaches canprovide rapid, efficient and simultaneous detection of multipleallergens in multiple samples (Moreno-Bondi et al. 2003 andSchubert-Ullrich et al. 2009). However, application of thesenovel techniques to food allergen analyses is still limited andwill hopefully grow. Similarly, use of proteomics approach toidentify and detect food allergens is expected to increase as mi-crofluidic system-based protein separation and analysis systemsbecome available as handheld devices in the near future. It isalso anticipated that DNA-based food allergen detection meth-ods will continue to be used as a valuable reinforcement tool inthe ongoing effort to manage food allergens in the food supply.
ACKNOWLEDGEMENTThe help of Dr. Sahul H. Rajamohamed in the preparation andrevision of this manuscript is gratefully acknowledged.
REFERENCES
Aabin B et al. 1996. Identification of IgE-binding egg white proteins:comparison of results obtained by different methods. Int ArchAllergy Immunol 109(1): 50–57.
Allergyexpert. Available at www.allergyexpert.com. Accessed onMarch 3, 2010.
Alomirah HF et al. 2000. Applications of mass spectrometry to foodproteins and peptides. J Chromatogr A 893: 1–21.
Anderson JA. 1986. The establishment of common language con-cerning adverse reactions to food and food additives. J AllergyClin Immunol 78(1): 140–143.
Anderson JW. 2008. Beneficial effects of soy protein consumptionfor renal function. Asia Pacific J Clin Nutr 17(Suppl 1): 324–328.
Anderson RP et al. 2000. In vivo antigen challenge in celiac dis-ease identifies a single transglutaminase-modified peptide as thedominant A-gliadin T-cell epitope. Nature Med 6(3): 337–342.
Arede A et al. 2000. Food allergy pattern in children from SouthernEurope. Allergy 55(63): 52–57.
Awazuhara H et al. 1998. Antigenicity of the proteins in soylecithin and soy oil in soybean allergy. Clin Exp Allergy 28(12):1559–1569.
Ballmer-Weber BK et al. 2007. Clinical characteristics of soybeanallergy in Europe: a double-blind, placebo-controlled food chal-lenge study. J Allergy Clin Immunol 119(6): 1489–1496.
Baur X et al. 1996. Characterization of soybean allergens causingsensitization of occupationally exposed bakers. Allergy 51(5):326–330.
Beaudouin E et al. 2006. Food-dependent exercise-induced anaphy-laxis – update and current data. Eur Ann Allergy Clin Immunol38(2): 45–51.
Becker W et al. 2004. Opinion of the scientific panel on dieteticproducts, nutrition and allergies on a request from the commis-sion relating to the evaluation of allergenic foods for labellingpurposes (Request nr EFSA-Q-2003–016). Eur Food Saf Author-ity J 32: 1–197.
Besler M. 2001. Determination of allergens in foods. Trends AnalChem 20: 662–672.
Besler M et al. 2002a. Allergen data collection: goat’s milk (Capraspp.). Available at www.food-allergens.de/. Internet Symp FoodAllergens 4(2): 119–124.
Besler M et al. 2002b. Determination of hidden allergens in foodsby immunoassays. Available at www.food-allergens.de/. InternetSymp Food Allergens 4(1): 1–18.
Beyer K et al. 2001. Effects of cooking methods on peanut aller-genicity. J Allergy Clin Immunol 107: 1077–1081.
Beyer K et al. 2002. Identification of sesame seed allergens by2-dimensional proteomics and Edman sequencing: seed storageproteins as common food allergens. J Allergy Clin Immunol 110:154–159.
Bindslev-Jensen C et al. 2002. Can we determine a threshold levelfor allergenic foods by statistical analysis of published data in theliterature? Allergy 57: 741–746.
Blais BW, Phillippe LM. 2000. A cloth-based enzyme immunoassayfor detection of peanut proteins in foods. Food Agric Immunol12: 243–248.
Blumchen K et al. 2008. Rush specific oral tolerance induction inpeanut allergic patients with high risk of anaphylactic reactions.J Allergy Clin Immunol 121(2): S136.
Bock T. 2008. What are the symptoms of mustard allergy.Available at http://ezinearticles. com/?What-Are-the-Symptoms-of-Mustard-Allergy?andid=1682496. Accessed on March 2,2010.
Bonomi F et al. 2003. Reduction of immunoreactivity of bovine β-lactoglobulin upon combined physical and proteolytic treatment.J Dairy Res 70: 51–59.
Boye JI et al. 2010. Processing foods without soybean ingredients.In: JI Boye, S Godefroy (eds.) Allergen Management in the FoodIndustry, Chapter 13. John Wiley & Sons, New York.
Boza JJ et al. 1994. Nutritional value and antigenicity of twomilk protein hydrolysates in rats and guinea pigs. J Nutr 124:1978–1986.
Breeding CJ, Beyer RS. 2000. Eggs. In: L Genevieve et al.(eds) Food Chemistry: Principles and Applications. Sci-ence Technology Systems, West Sacramento, CA, pp. 421–431.
Breiteneder H, Mills EN. 2005. Molecular properties of food aller-gens. J Allergy Clin Immunol 115: 14–23.
Breiteneder H, Radauer CA. 2004. Classification of plant food al-lergens. J Allergy Clin Immunol 113(5): 821–830.
Breneman JC. 1987. Handbook of Food Allergies. Marcel Dekker,New York.
Burks AW Jr et al. 1988. Allergenicity of major component proteinsof soybean determined by enzyme-linked immunosorbent assay(ELISA) and immunoblotting in children with atopic dermati-tis and positive soy challenges. J Allergy Clin Immunol 11(6):1135–1142.
P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 815
Burks AW et al. 1994. Prospective oral food challenge study oftwo soybean protein isolates in patients with possible milk or soyprotein enterocolitis. Pediatr Allergy Immunol 5(1): 40–45.
Busse PJ et al. 2002. Identification of sequential IgE-binding epi-topes on bovine alpha (s2)- casein in cow’s milk allergic patients.Int Arch Allergy Immunol 129: 93–96.
Caballero T et al. 1994. Relationship between pollinosis and fruitor vegetable sensitization. Pediatr Allergy Immunol 5: 218–222.
Cantani A. 2008. Pediatric Allergy, Asthma and Immunology.Springer-Verlag, Berlin, Heidelberg and New York, p. 628.
Cartier A et al. 1984. Occupational asthma in snow crab-processingworkers. J Allergy Clin Immunol 74(3 Pt 1): 261–269.
Catassi C et al. 2007. A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patientswith celiac disease. Am J Clin Nutr 85(1): 160–166.
Chafen JJ et al. 2010. Diagnosing and managing common foodallergies: a systematic review. JAMA 12(18): 1848–1856.
Chapman MD et al. 2000. Recombinant allergens for diagnosis andtherapy of allergic disease. J Allergy Clin Immunol 106: 409–418.
Chassaigne H et al. 2009. Resolution and identification of ma-jor peanut allergens using a combination of fluorescence two-dimensional differential gel electrophoresis, Western blotting andQ-TOF mass spectrometry. J Proteomics 72: 511–526.
Chatchatee P et al. 2001. Identification of IgE and IgG bindingepitopes on β- and κ-casein in cow’s milk allergic patients. ClinExp Allergy 31: 1256–1262.
Chen ST et al. 2003. Effect of dietary protein on renal function andlipid metabolism in five-sixths nephrectomized rats. Br J Nutr89(4): 491–497.
Clark AT et al. 2009. Successful oral tolerance induction in severepeanut allergy. Allergy 64(8): 1218–1220.
Cocco RR et al. 2003. Mutational analysis of major, sequential IgE-binding epitopes in alpha s1-casein, a major cow’s milk allergen.J Allergy Clin Immunol 112: 433–437.
Codina R et al. 1997. Purification and characterization of a soybeanhull allergen responsible for the Barcelona asthma outbreaks. II:purification and sequencing of the Gly m 2 allergen. Clin ExpAllergy 27(4): 424–430.
Collin P et al. 2004. The safe threshold for gluten contaminationin gluten-free products. Can trace amounts be accepted in thetreatment of coeliac disease? Aliment Pharmacol Ther 19(12):1277–1283.
Crittenden RG, Bennett LE. 2005. Cow’s milk allergy: a complexdisorder. J Am Coll Nutr 24: S582–S591.
Cross M et al. 2001. Anti-allergy properties of fermented foods: animportant immunoregulatory mechanism of lactic acid bacteria?Int Immunopharmacol 1: 891–901.
Dalal I et al. 2002. Food allergy is a matter of geography after all:sesame as a major cause of severe IgE-mediated food allergicreactions among infants and young children in Israel. Allergy 57:362–365.
Darewicz M et al. 2008. Celiac disease – background, molecular,bioinformatics and analytical aspects. Food Rev Int 24: 311–329.
Daul CB et al. 1993a. Hypersensitivity reactions to crustacean andmolluscs. Clin Rev Allergy 11: 201–222.
Daul CB et al. 1993b. Common crustacean allergens: identifica-tion with shrimp-specific allergens. In: D Kraft, A Sehon (eds.)
Molecular Biology and Immunology of Allergens. CRC Press,Baton Rouge, pp. 291–293.
Davis PJ, Williams SC. 1998. Protein modification by thermal pro-cessing. Allergy 53(46, Suppl): 102–105.
De Boissieu D et al. 1997. Allergy to extensively hydrolyzed cow’smilk proteins in infants: identification and treatment with anamino acid-based formula. J Pediatr 131: 744–747.
de Leon MP et al. 2003. Immunological analysis of allergenic crossreactivity between peanut and tree nuts. Clin Exp Allergy 33:1273–1280.
Desjardin LE et al. 1998. Comparison of the ABI 7700 system (Taq-Man) and competitive PCR for quantification of IS6110 DNA insputum during treatment of tuberculosis. J Clin Microbiol 36:1964–1968.
Dominguez J et al. 1990. Purification and characterization of anallergen of mustard seed. Ann Allergy 64: 352–357.
Eigenmann PA et al. 1996. Identification of unique peanut andsoy allergens in sera adsorbed with cross-reacting antibodies.J Allergy Clin Immunol 98(5 Pt 1): 969–978.
Ensminger AH et al. 1983. Foods and Nutrition Encyclopedia. PegusPress, Clovis, CA.
Fasano A, Catassi C. 2001. Current approaches to diagnosis andtreatment of celiac disease: an evolving spectrum. Gastroenterol-ogy 120(3): 636–651.
Fasano A et al. 2003. Prevalence of celiac disease in at-risk andnot-at-risk groups in the United States: a large multicenter study.Arch Intern Med 163(3): 286–292.
FDA. 1999. Food labeling: health claims; soy protein and coronaryheart disease. The United States Food and Drug Adminstration,Department of Health and Human Services. Federal Register 64:57699–57733.
FDA. 2006. The United States Food and Drug Administration,Department of Health and Human Services, Threshold WorkingGroup. Approaches to establish thresholds for major foodallergens and for gluten in food. Available at http://www.fda.gov/Food/LabelingNutrition/FoodAllergensLabeling/GuidanceComplianceRegulatoryInformation/ucm106108.htm. Accessedon November 28, 2011
Ferguson A. 1997. Gluten-sensitive enteropathy (celiac disease). In:DD Metcalfe et al. (eds.) Food Allergy – Adverse Reactions toFoods and Food Additives, 2nd edn. Wiley-Blackwell, Malden,MA, pp. 287–301.
Fernandez-Rivas M. 2003. Cross-reactivity between fruit and veg-etables. Allergol Immunopathol 31(3): 141–146.
Fernandez-Rivas M et al. 2008. Allergies to fruits and vegetables.Pediatr Allergy Immunol 19(8): 675–681.
Ford RP, Taylor B. 1982. Natural history of egg hypersensitivity.Arch Dis Childhood 57: 649–652.
Friedman M, Brandon DL. 2001. Nutritional and health benefits ofsoy proteins. J Agric Food Chem 49(3): 1069–1086.
Gangur V et al. 2005. Sesame allergy: a growing food allergy ofglobal proportions. Ann Allergy Asthma Immunol 95: 4–11.
Garcıa Novo MD et al. 2007. Prevalence of celiac disease in ap-parently healthy blood donors in the autonomous community ofMadrid. Revista Espanola de Enfermedades Digestivas 99(6):337–342.
Gerrard JW, Shenassa M. 1983. Sensitization to substances in breastmilk: recognition, management and significance. Ann Allergy 51:300–302.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
816 Part 8: Food Safety and Food Allegens
Gomez JC et al. 2001. Prevalence of celiac disease in Argentina:screening of an adult population in the La Plata area. Am J Gas-troenterol 96(9): 2700–2704.
Gonzalez de la Pena MA et al. 1991. Isolation and characterizationof a major allergen from oriental mustard seeds, Brajl. Int ArchAllergy Appl Immunol 96: 263–270.
Gonzalez de la Pena MA et al. 1996. Expression in Escherichia coliof Sin a 1, the major allergen from mustard. Eur J Biochem 237:827–832.
Gonzalez R et al. 1992. Purification and characterization of majorinhalant allergens from soybean hulls. Clin Exp Allergy 22(8):748–755.
Gonzalez R et al. 1995. Soybean hydrophobic protein and soybeanhull allergy. Lancet 346(8966): 48–49.
Grundy JR et al. 2002. Rising prevalence of allergy to peanut inchildren: data from 2 sequential cohorts. J Allergy Clin Immunol110(5): 784–778.
Hansen KS et al. 2003. Roasted hazelnuts – allergenic activity evalu-ated by double-blind, placebo-controlled food challenge. Allergy58: 132–138.
Harish Babu BN et al. 2008. A cross-sectional study on the preva-lence of food allergy to eggplant (Solanum melongena L.) re-veals female predominance. Clin Exp Allergy 38(11): 1795–1802.
Hefle SL et al. 1996. Allergenic foods. Crit Rev Food Sci Nutr 36:S69–S89.
Hefle SL et al. 2005. Soy sauce retains allergenicity through thefermentation production process. J Allergy Clin Immunol 115(2,Suppl): S32.
Hefle SL et al. 2007. Consumer attitudes and risks associated withpackaged foods having advisory labelling regarding the presenceof peanuts. J Allergy Clin Immunol 120: 171–176.
Heine RG et al. 2006. The diagnosis and management of egg allergy.Curr Allergy Asthma Reports 6: 145–152.
Herman EM et al. 2003. Genetic modification removes an immun-odominant allergen from soybean. Plant Physiol 132: 36–43.
Hill DJ et al. 1999. The natural history of intolerance to soy andextensively hydrolyzed formula in infants with multiple foodprotein intolerance (MFPI). J Pediatr 135: 118–121.
Hischenhuber C et al. 2006. Review article: safe amounts of glutenfor patients with wheat allergy or coeliac disease. Aliment Phar-macol Ther 23(5): 559–575.
Holzhauser T et al. 2002. Detection of potentially allergenic hazel-nut (Corylus avellana) residues in food: a comparative study withDNA PCR-ELISA and protein sandwich-ELISA. J Agric FoodChem 50: 5808–5215.
Holzhauser T et al. 2006. Polymerase chain reaction (PCR) meth-ods for the detection of allergenic foods. In: SJ Koppelman, SLHefle (eds.) Detecting Allergens in Food. Woodhead Publishing,Cambridge, pp. 125–143.
Hori G et al. 2001. Soy protein hydrolyzate with bound phospho-lipids reduces serum cholesterol levels in hypercholesterolemicadult male volunteers. Biosci Biotechnol Biochem 65(1): 72–78.
Host A, Halken S. 1990. A prospective study of cow milk allergyin Danish infants during the first 3 years of life: clinical coursein relation to clinical and immunological type of hypersensitivityreaction. Allergy 45(8): 587–596.
Host A, Samuelsson EG. 1988. Allergic reactions to raw, pasteur-ized, and homogenized/pasteurized cow milk: a comparison. A
double-blind placebo-controlled study in milk allergic children.Allergy 43: 113–118.
Hourihane JO et al. 1997. An evaluation of the sensitivity of sub-jects with peanut allergy to very low doses of peanut protein:a randomized, double-blind, placebo-controlled food challengestudy. J Allergy Clin Immunol 100: 596–600.
Inoue R et al. 2001. Identification of beta-lactoglobulin-derivedpeptides and class II HLA molecules recognized by T cells frompatients with milk allergy. Clin Exp Allergy 31: 1126–1134.
Janatuinen EK et al. 1995. A comparison of diets with and with-out oats in adults with celiac disease. N Engl J Med 333(16):1033–1037.
Janatuinen EK et al. 2000. Lack of cellular and humoral immuno-logical responses to oats in adults with coeliac disease. Gut 46(3):327–331.
Janatuinen EK et al. 2002. No harm from five year ingestion of oatsin coeliac disease. Gut 50(3): 332–335.
Jappe U, Vieths S. 2010. Lupine, a source of new as well as hiddenfood allergens. Mol Nutr Food Res 54(1): 113–126.
Jarvinen KM et al. 2001. IgE and IgG binding epitopes on alpha-lactalbumin and beta-lactoglobulin in cow’s milk allergy. Int ArchAllergy Immunol 126: 111–118.
Joint FAO/WHO Food Standards Programme and Codex Al-imentarius Commission. 2008. Report of the 30th Sessionof the Codex Committee on Nutrition and Foods for Spe-cial Dietary Uses, 30 June – 5 July 2008, Geneva, Switzer-land. ALINORM 08/31/26. Available at http://www. codexal-imentarius.net/download/report/687/al08_26e.pdf. Accessed on28 November 2011
Jones SM et al. 2009. Clinical efficacy and immune regulationwith peanut oral immunotherapy. J Allergy Clin Immunol 124(2):292–300.
Kahlenberg F et al. 2006. Monoclonal antibody R5 for detection ofputatively coeliac-toxic gliadin peptides. Eur Food Res Technol222(1–2): 78–82.
Kalogeromitros D et al. 1996. Anaphylaxis induced by lentils. AnnAllergy Asthma Immunol 77(6): 480–482.
Kaminogawa S, Totsuka M. 2003. Allergenicity of milk proteins.In: PF Fox (ed.) Advanced Dairy Chemistry, Volume 1, Proteins.Elsevier Science Publications, London, pp. 648–674.
Kanny G et al. 2001. Population study of food allergy in France. JAllergy Clin Immunol 108: 133–140.
Karjalainen J et al. 1992. A bovine albumin peptide as a possibletrigger of insulin-dependent diabetes mellitus. N Engl J Med 327:302–307.
Keck-Gassenmeier B et al. 1999. Determination of peanut tracesin food by a commercially available ELISA test. Food AgricImmunol 11: 243–250.
Kleber N et al. 2004. The antigenic response of β-lg is modulatedby thermally induced aggregation. Eur Food Res Technol 219(2):105–110.
Kleber N et al. 2007. Antigenic response of bovine beta lactoglob-ulin influenced by ultra high pressure treatment and temperature.Innovative Food Sci Emerg Technol 8(1): 39–45.
Koppelman SJ et al. 1999. Heat induced conformational changesof Ara h 1, a major peanut allergen, do not affect its allergenicproperties. J Biol Chem 274(8): 4770–4777.
Krishnan HB. 2000. Biochemistry and molecular biology of soy-bean seed storage protein. J New Seeds 2(3): 1–25.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 817
Krishnan HB et al. 2009. All three subunits of soybean β-conglycinin are potential food allergens. J Agric Food Chem57(3): 938–943.
Kumar R et al. 2007. Rice (Oryza sativa) allergy in rhinitis andasthma patients: a clinico-immunological study. Immunobiology212(2): 141–147.
L’Hocine L, Boye JI. 2007. Allergenicity of soybean: new devel-opments in identification of allergenic proteins, cross-reactivitiesand hypoallergenization technologies. Crit Rev Food Sci Nutr47(2): 127–143.
Laoprasert N et al. 1998. Anaphylaxis in a milk-allergic child fol-lowing ingestion of lemon sorbet containing trace quantities ofmilk. J Food Prot 61: 1522–1524.
Leadbeater L, Ward FB. 1987. Analysis of tryptic digests of bovineβ-casein by reversed-phase high-performance liquid chromatog-raphy. J Chromatogr 397: 435–443.
Leduc V et al. 2006. Identification of oleosins as major allergens insesame seed allergic patients. Allergy 61: 349–356.
Lee JW et al. 2001. Effects of gamma-radiation on the allergenicand antigenic properties of milk proteins. J Food Prot 64: 272–276.
Lee PW et al. 2008. Sandwich enzyme-linked immunosorbent as-say (ELISA) for detection of mustard in foods. J Food Sci 73:T62–T68.
Lehrer SB et al. 2003. Seafood allergy and allergen: a review. MarBiotechnol 5: 339–348.
Liu K. 1997. Soybeans: Chemistry, Technology and Utilization.Chapman and Hall, New York, pp. 28–35.
Lohi S. 2010. Prevalence and prognosis of coeliac disease: a specialfocus on undetected condition. Ph.D. Dissertation, Submitted toFaculty of Medicine of the University of Tampere, Finland.
Lu Y et al. 2007. Immunological characteristics of monoclonalantibodies against shellfish major allergen tropomyosin. FoodChem 100: 1093–1099.
Lundin KE et al. 2003. Oats induced villous atrophy in coeliacdisease. Gut 52(11): 1649–1652.
Maleki SJ et al. 2000. The effects of roasting on the allergenic prop-erties of peanut proteins. J Allergy Clin Immunol 106: 763–768.
Martin D, Chapman M. 2001. Prediction of the allergenicity of amolecule. J Allergy Clin Immunol 41: 13–16.
Martorell Aragones A et al. 2001. Allergy to egg proteins. AllergolImmunopathol 29: 84–95.
Matricardi PM et al. 2003. Microbial products in allergy preventionand therapy. Allergy 58: 461–471.
Mazzeo MF et al. 2003. Identification of transglutaminase-mediated deamidation sites in a recombinant alpha-gliadin byadvanced mass-spectrometric methodologies. Protein Sci 12(11):2434–2442.
Mine Y, Rupa P. 2003. Fine mapping and structural analysis of im-munodominant IgE allergenic epitopes in chicken egg ovalbumin.Prot Eng 16: 747–752.
Mine Y, Rupa P. 2004. Immunological and biochemical propertiesof egg allergens. World Poult Sci J 60: 321–330.
Mine Y, Yang M. 2008. Recent advances in the understanding ofegg allergens: basic, industrial, and clinical perspectives. J AgricFood Chem 56: 4874–4900.
Mine Y, Zhang JW. 2002. Identification and fine mapping of IgGand IgE epitopes in ovomucoid. Biochem Biophys Res Commun292: 1070–1074.
Monaci L et al. 2006. Milk allergens, their characteristics and theirdetection in food. Eur Food Res Technol 223: 149–179.
Moneret-Vautrin A. 2006. Allergenic foods: mustard. Available athttp://www.anaphylaxis.eu/uk_mustard.html.
Monreal P et al. 1992. Two anaphylactic reactions to ingestion ofmustard sauce. Ann Allergy 69: 317–320.
More D. 2009. Sesame seed allergy. Available at http://allergies.about.com/od/otherfoodallergies/a/sesameallergy.htm. Accessedon November 28, 2011.
Moreno-Bondi MC et al. 2003. Multi-analyte analysis system usingan antibody-based biochip. Anal Bioanal Chem 375: 120–124.
Morisset M et al. 2003a. Thresholds of clinical reactivity to milk,egg, peanut and sesame in immunoglobulin E-dependent aller-gies: evaluation by double-blind or single-blind placebo con-trolled oral challenges. Clin Exp Allergy 33: 1046–1051.
Morisset M et al. 2003b. Prospective study of mustard allergy: firststudy with double-blind placebo-controlled food challenge trials(24 cases). Allergy 58(4): 295–299.
Motala C, Lockey R. 2004. Food Allergy. World Allergy Organi-zation Allergic Diseases Resource Centre. Available at http://www.worldallergy.org/professional/allergic_diseases_center/foodallergy/
Munoz-Furlong A et al. 2004. Prevalence of self-reported seafoodallergy in the U.S. J Allergy Clin Immunol 113: S100.
Mustorp D et al. 2008. Detection of celery (Apium graveolens), mus-tard (Sinapis alba, Brassica juncea, Brassica nigra) and sesame(Sesanum indicum) in food by real time PCR. Eur Food ResTechnol 226: 771–778.
Nakajima-Adachi H et al. 1998. Determinant analysis of IgE andIgG antibodies and T cells specific for bovine alpha s1-caseinfrom the same patients allergic to cow’s milk: existence of alphas1-casein-specific B cells and T cells characteristic in cow’s milkallergy. J Allergy Clin Immunol 101: 660–671.
Nakano T et al. 2010. Sensitization to casein and β-lactoglobulin(blg) in children with cow’s milk allergy (CMA). Arerugi 59:117–122.
Nentwich I et al. 2001. Cow’s milk-specific cellular and humoral im-mune responses and atopy skin symptoms in infants from atopicfamilies fed a partially (pHF) or extensively (eHF) hydrolyzedinfant formula. Allergy 56: 1144–1156.
Ng-Kwai-Hang KF. 2002. Heterogeneity, fractionation and isola-tion. In: H Roginski et al. (eds.) Encyclopaedia of Dairy Sciences.Academic Press, London, pp. 1881–1894.
Niemann L et al. 2009. Detection of walnut residues in foods usingan enzyme-linked immunosorbent assay. J Food Sci 74: T51–T57.
Nordlee JA, Taylor SL. 1995. Immunological analysis of food al-lergens and other food proteins. Food Technol 2: 129–132.
Nowak-Wegrzyn A et al. 2004. Contamination of dry powder in-halers for asthma with milk proteins containing lactose. J AllergyClin Immunol 113: 558–560.
O’Neil C et al. 1993. Allergic reactions to fish. Clin Rev Allergy 11:183–200.
Ogawa T et al. 1991. Investigation of the IgE binding proteinsin soybeans by immunoblotting with the sera of the soybean-sensitive patients with atopic dermatitis. J Nutr Sci Vitaminol37(6): 555–565.
Ogawa T et al. 1993. Identification of the soybean allergenic protein,Gly m Bd 30K, with the soybean seed 34-kDa oil-body-associatedprotein. Biosci Biotechnol Biochem 57(6): 1030–1033.

P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
818 Part 8: Food Safety and Food Allegens
Oliver S, Vieths S. 2004. Development of a real-time PCR anda sandwich ELISA for detection of potentially allergenic traceamounts of peanut (Arachis hypogaea) in processed foods. JAgric Food Chem 52: 3754–3760.
Oliver S et al. 2002. Development and validation of two dipsticktype immunoassays for determination of trace amounts of peanutand hazelnut in processed foods. Eur Food Res Technol 215:431–436.
Osman AA et al. 2001. A monoclonal antibody that recognizes apotential coeliac-toxic repetitive pentapeptide epitope in gliadins.Eur J Gastroenterol Hepatol 13(10): 1189–1193.
Panconesi E et al. 1980. Anaphylactic shock from mustard afteringestion of pizza. Contact Dermatitis 6: 294–295.
Pastorello EA et al. 2001. The major allergen of sesame seeds(Sesamum indicum) is a 2S albumin. J Chromatogr B Biomed SciAppl 756: 85–93.
Pedersen HS, Djurtoft R. 1989. Antigenic and allergenic propertiesof acidic and basic peptide chains from glycinin. Food AgricImmunol 1(2): 101–109.
Pereira MJ et al. 2002. The allergenic significance of legumes.Allergol Immunopathol 30(6): 346–353.
Perkins MS. 2000. Sesame allergy. Available at www.allergyuk.org/fs_sesame.aspx. Accessed on February 24, 2010.
Pieretti MM et al. 2009. Audit of manufactured products: use of al-lergen advisory labels and identification of labeling ambiguities.J Allergy Clin Immunol 124: 337–341.
Poms RE et al. 2001. Increased sensitivity for detection of specifictarget DNA in milk by concentration in milk fat. Eur Food ResTechnol 213: 361–365.
Poms RE et al. 2004. Methods for allergen analysis in food: a review.Food Addit Contam 21: 1–31.
Pons L et al. 2002. The 18 kDa peanut oleosin is a candidate aller-gen for IgE-mediated reactions to peanuts. Allergy 57(72): 88–93.
Porcel S et al. 2006. Food-dependent exercise-induced anaphy-laxis to pistachio. J Investig Allergol Clin Immunol 16(1): 71–73.
Prioult G et al. 2004. Stimulation of interleukin-10 production byacidic beta-lactoglobulin-derived peptides hydrolyzed with Lac-tobacillus paracasei NCC2461 peptidases. Clin Diagn Lab Im-munol 11: 266–271.
Rajamohamed SH, Boye JI. 2010. Processing foods without peanutsand tree nuts. In: JI Boye, S Godefroy (eds.) Allergen Man-agement in the Food Industry, Chapter 11. John Wiley & Sons,New York.
Rance F et al. 2000. Mustard allergy in children. Allergy 55(5):496–500.
Restani P et al. 2004. Characterization of bovine serum albuminepitopes and their role in allergic reactions. Allergy 59: 21–24.
Romano A et al. 2001. Food-dependent exercise-induced anaphy-laxis: clinical and laboratory findings in 54 subjects. Int ArchAllergy Immunol 125(3): 264–272.
Rong-Hwa S et al. 2010. Gold nanoparticle-based lateral flow assayfor detection of staphylococcal enterotoxin B. Food Chem 118:462–466.
Rostami K et al. 1999. High prevalence of celiac disease in appar-ently healthy blood donors suggests a high prevalence of undiag-nosed celiac disease in the Dutch population. Scand J Gastroen-terol 34(3): 276–279.
Rozenfeld P et al. 2002. Detection and identification of a soy beancomponent that cross reacts with caseins from cow’s milk. ClinExp Immunol 130: 49–58.
Sampson HA. 2002. Peanut allergy. N Engl J Med 346(17):1294–1299.
Sampson HA. 2004. Update on food allergy. J Allergy Clin Immunol113: 805–819.
Sampson HA, McCaskill CC. 1985. Food hypersensitivity andatopic dermatitis: evaluation of 113 patients. J Pediatr 107:669–675.
Sampson HA et al. 1992. Fatal and near-fatal anaphylactic reac-tions to food in children and adolescents. N Engl J Med 327(6):380–384.
Scheibe B et al. 2001. Detection of trace amounts of hidden aller-gens: hazelnut and almond proteins in chocolate. J ChromatogrB Biomed Sci Appl 756: 229–237.
Schubert-Ullrich P et al. 2009. Commercialized rapid immunoan-alytical tests for determination of allergenic food proteins: anoverview. Anal Bioanal Chem 395: 69–81.
Shefcheck KJ, Musser SJ. 2004. Conformation of the aller-genic protein Ara h 1 in a model matrix using liquid chro-matography/tandem mass spectrometry. J Agric Food Chem 52:2785–2790.
Shriver-Lake LC et al. 2004. Applications of array biosensor fordetection of food allergens. J AOAC Int 87: 1498–1502.
Sicherer SH. 2010. Food allergies. eMedicine. Available athttp://emedicine.medscape.com/article/135959-overview.
Sicherer SH, Sampson HA. 2006. 9. Food allergy. J Allergy ClinImmunol 117(2 Suppl Mini-Primer): S470–S475.
Sicherer SH, Sampson HA. 2010. Food allergy. J Allergy Clin Im-munol 125: S116–S125.
Sicherer SH et al. 2001. A voluntary registry for peanut and tree-nutallergy: characteristics of the first 5149 registrants. J Allergy ClinImmunol 108: 128–132.
Sicherer SH et al. 2003. Prevalence of peanut and tree nut allergyin the United States determined by means of a random digitdial telephone survey: a 5-year follow-up study. J Allergy ClinImmunol 112(6): 1203–1207.
Sicherer SH et al. 2004. Prevalence of seafood allergy in the UnitedStates determined by a random telephone survey. J Allergy ClinImmunol 114: 159–165.
Skypala I. 2009. Fruits and vegetables. In: I Skypala, C Venter (eds.)Food Hypersensitivity: Diagnosing and Managing Food Allergiesand Intolerance. Blackwell Publishing, Oxford, pp. 147–165.
Soler-Rivas C, Wichers HJ. 2001. Impact of (bio)chemical and phys-ical procedures on food allergen stability. Allergy 56(67): 52–55.
Spuergin P et al. 1996. Allergenic epitopes of bovine alpha s1-caseinrecognized by human IgE and IgG. Allergy 51: 306–312.
Staden U et al. 2007. Specific oral tolerance induction in food allergyin children: efficacy and clinical patterns of reaction. Allergy 62:1261–1269.
Stephenson TJ et al. 2005. Effect of soy protein-rich diet on renalfunction in young adults with insulin-dependant diabetes melli-tus. Clin Nephrol 64(1): 1–11.
Stewart GA, Thompson PJ. 1996. The biochemistry of commonaeroallergens. Clin Exp Allergy 26: 1020–1044.
Stoppler MC, Marks JW. 2005. Sesame seed allergy: agrowing problem? Available at www.medicinenet.com/script/main/art.asp. Accessed on February 24, 2010.
P1: SFK/UKS P2: SFK
BLBS102-c42 BLBS102-Simpson March 21, 2012 14:27 Trim: 276mm X 219mm Printer Name: Yet to Come
42 Food Allergens 819
Taylor SL. 2000. Emerging problems with food allergens. Food NutrAgric 26: 14–29.
Taylor SL, Hefle SL. 2001. Food allergies and other food sensitiv-ities – an application of the Institute of Food Techologists’ ex-pert panel on food safety and nutrition. Food Technol 55(9): 68–83.
Taylor SL, Lehrer SB. 1996. Principles and characteristics of foodallergens. Crit Rev Food Sci Nutr 36: S91–S118.
Taylor SL et al. 2002. Factors affecting the determination of thresh-old doses for allergenic foods: how much is too much? J AllergyClin Immunol 109(1): 24–30.
Taylor SL et al. 2004. Consensus protocol for the determination ofthe threshold doses for allergenic foods: how much is too much?Clin Exp Allergy 34: 689–695.
Taylor SL et al. 2009. Allergen immunoassays – considerationsfor use of naturally incurred standards. Anal Bioanal Chem 395:83–92.
Thompson T. 2004. Gluten contamination of commercial oatproducts in the United States. N Engl J Med 351(19): 2021–2022.
Thompson T. 2005. Contaminated oats and other gluten-free foodsin the United States. J Am Diet Assoc 105(3): 348–349.
Tome D et al. 2004. Nutritional value of milk and meat productsderived from cloning. Cloning Stem Cells 6: 172–177.
Towell R. 2009. Peanuts, legumes, seeds and tree nuts. In: I Skypala,C Venter (eds.) Food Hypersensitivity: Diagnosing and ManagingFood Allergies and Intolerance. Blackwell Publishing, Oxford,pp. 166–182.
Valenta R et al. 1999. The recombinant allergen-based concept ofcomponent resolved diagnostics and immunotherapy (CRD andCRIT). Clin Exp Allergy 29: 896–904.
Wal JM. 1998. Cow’s milk allergens. Allergy 53: 1013–1022.Wal JM. 2004. Bovine milk allergenicity. Ann Allergy Asthma Im-
munol 93: 2–11.Walker-Smith J. 2003. Hypoallergenic formulas: are they really
hypoallergenic? Ann Allergy Asthma Immunol 90: 112–114.
Walsh BJ et al. 1988. New allergens from hen’s egg white and eggyolk: in vitro study of ovomucin, apovitellenin I and VI, andphosvitin. Int Arch Allergy Appl Immunol 87: 81–86.
Walsh BJ et al. 2005. Detection of four distinct groups of hen eggallergens binding IgE in the sera of children with egg allergy.Allergol Immunopathol 33: 183–191.
Ward PP et al. 2002. Lactoferrin and host defense. Biochem CellBiol 80: 95–102.
Wen HW et al. 2007. Peanut allergy, peanut allergens, and meth-ods for the detection of peanut contamination in food products.Compr Rev Food Sci Food Saf 6(2): 47–58.
Wilson S et al. 2005. Allergenic proteins in soybean: processing andreduction of P34 allergenicity. Nutr Rev 63(2): 47–58.
Wolff N et al. 2003. Allergy to sesame in humans is associatedprimarily with IgE antibody to a 14 kDa 2S albumin precursor.Food Chem Toxicol 41(8): 1165–1174.
Yazdanbakhsh M et al. 2002. Allergy, parasites, and the hygienehypothesis. Science 296: 490–494.
Yeung J. 2006. Enzyme-linked immunosorbent assays (ELISAs)for detecting allergens in foods. In: K Stef, H Sue (eds.) De-tecting Allergens in Food. Woodhead Publishing, Cambridge,pp. 109–124.
Yman IM et al. 1994. Analysis of food proteins for verification ofcontamination or mislabelling. Food Agric Immunol 6: 167–172.
Yman IM et al. 2006. Food allergen detection with biosensor im-munoassays. J AOAC Int 89: 856–861.
Yu CJ et al. 2003. Proteomics and immunological analysis of a novelshrimp allergen (Pen m 2). J Immunol 170: 445–453.
Yunginger JW. 1990. Classical food allergens. Allergy Asthma Proc11(1): 7–9.
Zhang JW, Mine Y. 1998. Characterization of IgE and IgG epitopeson ovomucoid using egg white allergic patient’s sera. BiochemBiophys Res Commun 253: 124–127.
Zhang X et al. 2003. Soy food consumption is associated with lowerrisk of coronary heat disease in Chinese women. J Nutr 133(9):2874–2878.